Introduction: It is the classic hepatobiliary manifestation of IBS. It is generally chronic progressive. Frequently present with asymptomatic, anicteric.
Jan 01, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


Introduction:• It is the classic hepatobiliary manifestation of IBS.• It is generally chronic progressive. • Frequently present with asymptomatic, anicteric cholestasis, but
many develop progressive biliary strictures with time, leading to recurrent cholangitis, biliary cirrhosis& end-stage liver disease.
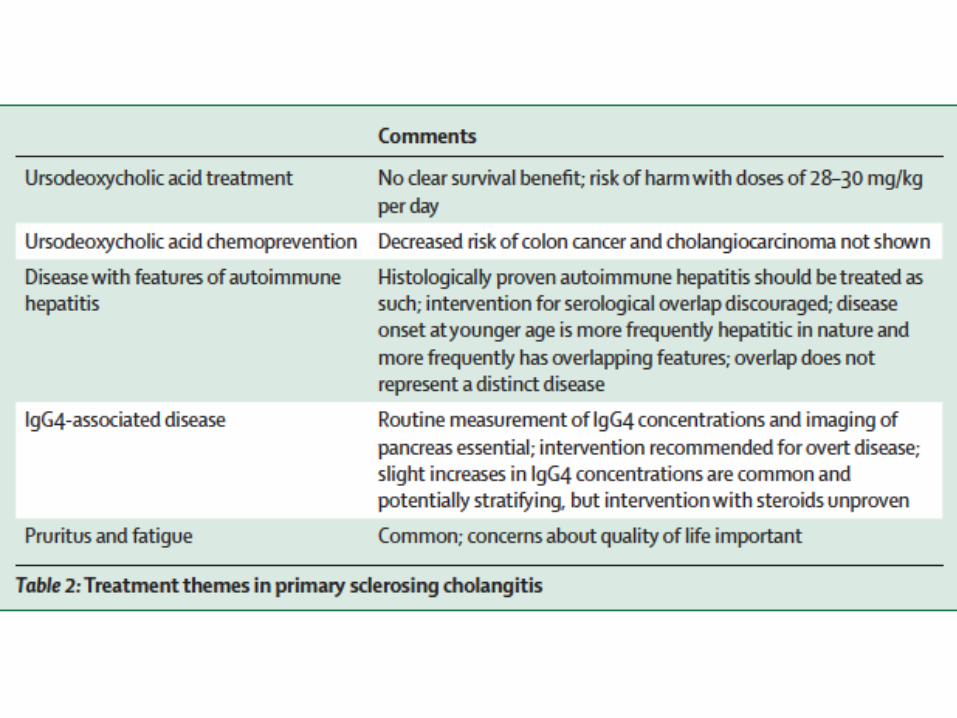
• Medical treatment does not slow the progression & many patients need liver transplantation, after which recurrent disease is a risk.
• The increased incidence of hepatobiliary cancer, not related to the underlying severity of biliary fibrosis, is of particular concern.
• Risk of colorectal cancer is also increased in patients with coexistent IBD.
• Treatment of is confined to supportive measures• Advances in pathobiology suggest that new stratified approaches
will soon be available.

Epidemiology:• The incidence varies geographically & is as high as 1.3 /100 000
people / year in northern Europe,Prevalence varies 16.2 /100 000.• Affects both sexes and all age groups>60% of patients are men.• The median age at onset is 30–40 years, usually non-smokers.• 60–80% has IBD (30–50% in S Europe & Asia), 75% UC, 83% with UC
had a pancolitis, 13% a leftsided colitis, 4% proctitis only, 95% of those with CD had an ileocolitis & 5% ileitis only.
• Patients with coexistant IBD are more likely to be male& asymptomatic at presentation&have both intrahepatic/ extrahepatic bile duct strictures than are those with PSC only.
• The prevalence of PSC in colitis varies, but not >10%.• CD compared with UC,more likely to be women,have small bile
duct disease &a less severe course.• Clinically progressive disease has been associated with mild
ulcerative colitis& a reduced need for colectomy.

Epidemiology:• PSC without colitis : colitis or immune activation in the gut might
simply be too mild to be diagnosed by available techniques.• >50% need liver transplantation within 10–15 years of symptom
development, as a result of reduced quality and quantity of life related to biliary obstruction, cholangitis, secondary biliary cirrhosis, & hepatobiliary malignant disease.

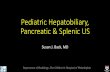
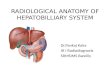
Strictures:• 10–20% have dominant strictures—ie, stenosis of 1.5 mm or less
in CBD or of 1 mm or less in the hepatic duct—many of whom have recurrent bacterial cholangitis.
• Patients with dominant strictures have significantly worse survival than do those without dominant strictures.
• Although most dominant strictures are benign, as much as 25% could be malignant.
• Some patients present with cholelithiasis, gallbladder carcinoma, pancreatitis, or colorectal cancer.
• PSC is an independent risk factor for CRC in IBD (*4 increased risk)& cumulative risk increases with disease duration (risk of CRC or dysplasia of 9%, 31%, 50% after 10, 20, 25 years, respectively, in patients with PSC a& UC vs 2%, 5%, and 10% in those with UC only).

MRCP:• MRCP is the diagnostic test of choice, alongside ultrasonography
to exclude secondary causes & assess the gallbladder.• MRI showed a sensitivity of 0.86&specificity of 0.94.• Strictures, dilatations,pruning of bile ducts are present in both the
intrahepatic&extrahepatic bile ducts of roughly 75% of patients& disease is extrahepatic in 5% of patients.

Secondary causes :• Secondary or radiological mimics:• Biliary calculi. Cholangiocarcinoma. Biliary tract surgery.• Caroli’s dis ease• Chronic biliary infection• Biliary toxin exposure• Chronic portal-vein thrombosis• Ischaemic stricturing• Cholestatic drug-induced liver injury • Cholangiopathy of critical care.• Autoimmune pancreatitis.• Slight increases in IgG4 noted in >10% in the absence of clear
evidence of AIP & these have a progressive disease phenotype & have no consistent benefits from treatment.

Malignancy:• PSC associated with an increased risk of cholangiocarcinoma, GB
cancer& CRC (in patients with colitis). • Advanced fibrosis or cirrhosis are at increased risk of HCC.• 2/3 CC are diagnosed at the same time as, or within the first year
after, diagnosis of PSC , yearly incidence of is 0.5–1.5%&lifetime risk is at least 10–15%.
• CC can occur as an intrahepatic mass or a hilar tumour. • Benign & malignant disease are difficult to distinguish& even the
combination of tumour markers, various imaging modalities (MRI, CT, endoscopic ultrasonog raphy) biliary brush cytology (including cytogenetic testing when available) cannot ensure early diagnosis.

Malignancy:• High-grade dysplasia on brush cytology has high sensitivity,
specificity&positive predictive value for diagnosis, and, when combined with carbohydrate antigen 19-9, sensitivity increases further.
• Brush cytology necessitates ERCP or PTC which are associated with intrinsic risks.
• EUS with FNA has greater sensitivity / specificity for the diagnosis of distal CC than do ERCP& brush cytology.
• Fluorescence in-situ hybridisation, in which DNA probes are used to identify chromosomal changes& digital image analysis, are novel techniques to measure DNA proliferation that might im prove the diagnostic yield of cytology.
• Other: cholangioscopy-guided biopsies& intra ductal E/S.• Urine bio markers by capillary electrophoresis mass spec
trometry has generated a CC-specific peptide marker .

Malignancy:• Gallbladder cancer develops in 2% &> 50% of gallbladder polyps
detected by ultrasonography could be malignant.• Thus yearly ultrasonography &a low threshold for
cholecystectomy is recommended, but ?true cost-effectiveness unclear.








BO5s:1
• Primary sclerosing cholangitis is characterized by all except:
• A. Usually present with asymptomatic anicteric cholestasis.• B. Medical treatments can slow the progression of the disease.• C. The treatment of advanced disease is liver transplantation.• D. There is risk of recurrence after liver transplantation.• E. Risk of CRC is only in those with coexistent IBD.

BO5s:1
• Primary sclerosing cholangitis is characterized by all except:
• A. Usually present with asymptomatic anicteric cholestasis.• B. Medical treatments can slow the progression of the disease.• C. The treatment of advanced disease is liver transplantation.• D. There is risk of recurrence after liver transplantation.• E. Risk of CRC is only in those with coexistent IBD.

BO5s:2
• Primary sclerosing cholangitis in contrast with primary biliary cirrhosis is charcterized by:
• A. Affecting more males.• B. Affecting younger ages.• C. Associated with IBD.• D. Associated with autoimmune pancreatitis.• E. Responds to UDCA.

BO5s:2
• Primary sclerosing cholangitis in contrast with primary biliary cirrhosis is charcterized by:
• A. Affecting more males.• B. Affecting younger ages.• C. Associated with IBD.• D. Associated with autoimmune pancreatitis.• E. Responds to UDCA.

BO5s:3
• Primary sclerosing cholangitis associated with UC compared with that associated with Crohn’s disease is characterized by all except:
• A. More severe course.• B. More diffuse disease.• C. Affecting more women.• D. More diffuse colonic disease.• E. Affects more females.

BO5s:3
• Primary sclerosing cholangitis associated with UC compared with that associated with Crohn’s disease is characterized by all except:
• A. More severe course.• B. More diffuse disease.• C. Affecting more women.• D. More diffuse colonic disease.• E. About 10%.

BO5s:4
• Primary sclerosing cholangitis is associated with all these cancers except:
• A. Cholangiocarcinoma.• B. Gall bladder cancer.• C. HCC.• D. Pancreatic cancer.• E. CRC.

BO5s:4
• Primary sclerosing cholangitis is associated with all these cancers except:
• A. Cholangiocarcinoma.• B. Gall bladder cancer.• C. HCC.• D. Pancreatic cancer.• E. CRC.

BO5s:5
• Colitis associated with primary sclerosing cholangitis is characterized by all except:
• A. Starts earlier in life.• B. Starts before PSC.• C. More total colitis than localized.• D. Less rectal sparing.• E. More affecting the right side.

BO5s:5
• Colitis associated with primary sclerosing cholangitis is characterized by all except:
• A. Starts earlier in life.• B. Starts before PSC.• C. More total colitis than localized.• D. Less rectal sparing.• E. More affecting the right side.
Related Documents