1 INTRODUCTION India is a land of immense biodiversity in which two (Eastern Himalayas and The Western Ghats of India) out of twenty five hot spots of the world are located. This country is perhaps the largest producer of medicinal herbs and is rightly called the botanical garden of the world. It is generally estimated that in India over 6000 plants are used in traditional, folk and herbal medicine, representing about 75% of the medicinal needs of the Third World countries. Medicinal herbs as potential source of therapeutic aids has attained a significant role in health system all over the world for both humans and animals not only in the diseased condition but also as potential material for maintaining proper health. The market share of herbal products made in developing countries remains comparatively low due to lack of research and development and the huge investments in making standardized products. Though India has a rich biodiversity, the growing demand is putting a heavy strain on the existing resources. While the demand for medicinal plants is growing, some of them are increasingly being threatened in their natural habitat. For meeting the future needs cultivation of medicinal plant has to be encouraged. Today there are at least 120 distinct chemical substances derived from plants that are considered as important drugs currently in use in one or more countries in the world. Indeed, molecules derived from natural sources (so-called natural products), including plants, marine organisms and microrganisms, have played, and continue to play, a dominant role in the discovery of leads for the development of conventional drugs for various diseases. In terms of a modern research endeavor, drug development from plants must necessarily imply a multi- displinary approach. Plants are used medicinally worldwide as sources of many potent drugs. Traditional medical practitioners use a variety of herbal preparations to treat different kinds of diseases including microbial infections. (Gunther, 1952; Chopra, 1956; Gopalan, 1984; Bauddhaloka, 2005). The World Health Organisation (WHO) estimated that 80% of the population of developing countries relies on traditional medicines, mostly plant drugs, for their primary

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
INTRODUCTION
India is a land of immense biodiversity in which two (Eastern Himalayas and The
Western Ghats of India) out of twenty five hot spots of the world are located. This country
is perhaps the largest producer of medicinal herbs and is rightly called the botanical
garden of the world. It is generally estimated that in India over 6000 plants are used in
traditional, folk and herbal medicine, representing about 75% of the medicinal needs of
the Third World countries. Medicinal herbs as potential source of therapeutic aids has
attained a significant role in health system all over the world for both humans and animals
not only in the diseased condition but also as potential material for maintaining proper
health. The market share of herbal products made in developing countries remains
comparatively low due to lack of research and development and the huge investments in
making standardized products.
Though India has a rich biodiversity, the growing demand is putting a heavy strain
on the existing resources. While the demand for medicinal plants is growing, some of
them are increasingly being threatened in their natural habitat. For meeting the future
needs cultivation of medicinal plant has to be encouraged. Today there are at least 120
distinct chemical substances derived from plants that are considered as important drugs
currently in use in one or more countries in the world. Indeed, molecules derived from
natural sources (so-called natural products), including plants, marine organisms and
microrganisms, have played, and continue to play, a dominant role in the discovery of
leads for the development of conventional drugs for various diseases. In terms of a modern
research endeavor, drug development from plants must necessarily imply a multi-
displinary approach. Plants are used medicinally worldwide as sources of many potent
drugs. Traditional medical practitioners use a variety of herbal preparations to treat
different kinds of diseases including microbial infections. (Gunther, 1952; Chopra, 1956;
Gopalan, 1984; Bauddhaloka, 2005).
The World Health Organisation (WHO) estimated that 80% of the population of
developing countries relies on traditional medicines, mostly plant drugs, for their primary
2
health care needs. Also, modern pharmacopoeia still contains at least 25% drugs derived
from plants and many others which are synthetic analogues built on prototype compounds
isolated from plants. Demand for medicinal plant is increasing in both developing and
developed countries due to growing recognition of natural products, being non-narcotic,
having no side-effects, easily available at affordable prices and sometimes the only source
of health care available to the poor. Medicinal plant sector has traditionally occupied an
important position in the socio cultural, spiritual and medicinal arena of rural and tribal
lives of India. Medicinal plants as a group comprise approximately 8000 species and
account for around 50% of all the higher flowering plant species of India. Millions of rural
households use medicinal plants in a self-help mode. Over one and a half million
practitioners of the Indian System of Medicine in the oral and codified streams use
medicinal plants in preventive, promotive and curative applications. There are estimated to
be over 7800 manufacturing units in India. In recent years, the growing demand for herbal
product has led to a quantum jump in volume of plant materials traded within and across
the countries. An estimate of the EXIM Bank puts the international market of medicinal
plants related trade at US $ 60 billion per year growing at the rate of 7% only (WHO,
2000).
Medicinal plants are important for pharmacological research and drug
development, not only when plant constituents are used directly as therapeutic agents, but
also as starting materials for the synthesis of drugs or as models for pharmacologically
active compounds. A significant number of modern pharmaceutical drugs are thus based
on or derived from medicinal plants. The need to document plant uses and attempt to
confirm their efficacy remains urgent. The term ethnopharmacology loosely describes the
field covering observation, identification, description and experimental investigation of
the effect of indigenous drugs and its ingredients is truly an interdisciplinary field of
research. Traditional medicine is a powerful source of biologically active compounds.
Ethnopharmacology has become a scientific backbone in the development of active
therapeutics based upon traditional medicine of various ethnic groups.
Ethnopharmacology is the survey of plants of a particular region or cultural tribe
depending on their use in traditional system by choosing a specific therapeutic target.

3
Screening program based on ethnopharmacological information has more success rate
than random screening (Papiya Bigoniya and Rana, 2008). Pharmacognosy is closely
related to botany and chemistry, both originated from the earlier scientific studies on
medicinal plants. A field concerned with the description and identification of drugs both in
whole state and powder along with their history, commerce, collection, preparation and
storage (Trease and Evans, 2008).
Medicinal herbs are moving from fringe to mainstream use with a greater number
of people seeking remedies and health approaches free from side effects caused by
synthetic chemicals. Recently, considerable attention has been paid to utilize eco-friendly
and bio-friendly plant-based products for the prevention and cure of different human
diseases. Considering the adverse effects of synthetic drugs, the western population is
looking for natural remedies which are safe and effective (Dubey et al., 2004). It is
documented that 80% of the world’s population has faith in traditional medicine,
particularly plant drugs for their primary healthcare. India is sitting on a gold mine of
well-recorded and traditionally well-practiced knowledge of herbal medicine. This country
is perhaps the largest producer of medicinal herbs and is rightly called the botanical
garden of the world. There are very few medicinal herbs of commercial importance which
are not found in this country. India officially recognizes over 3000 plants for their
medicinal value. It is generally estimated that over 6000 plants in India are in use in
traditional, folk and herbal medicine, representing about 75% of the medicinal needs of
the Third World countries (Rajshekharan, 2002).
Undoubtedly, the plant kingdom still holds many species of plants containing
substances of medicinal value which have yet to be discovered. India is a land of immense
biodiversity in which two out of eighteen hot spots of the world are located. India is also
one of the twelve mega biodiversity countries in the world. The total number of plant
species of all groups recorded from India is 45,000 (the total number may be even close to
60,000, as several parts of India are yet to be botanically explored). Of these, seed-bearing
plants account for nearly 15,000–18,000. India enjoys the benefits of varied climate, from
alpine in the Himalaya to tropical wet in the south and arid in Rajasthan. Such climatic

4
conditions have given rise to rich and varied flora in the Indian subcontinent. In order to
promote Indian herbal drugs, there is an urgent need to evaluate the therapeutic potentials
of the drugs as per WHO guidelines. Ironically, not many Indian products are available in
standardized form, which is the minimum requirement for introducing a product in the
western market (WHO, 2000).
The primary benefits of using plant derived medicines are that they are relatively
safer than synthetic alternatives, offering profound therapeutic benefits and more
affordable treatment. The use of medicinal plants in developing countries as a normative
basis for the maintenance of good health has been widely observed. Furthermore, the
increasing reliance on the use of medicinal plants in the industrialized societies has been
traced to the extraction and development of several drugs and chemotherapeutics from
these plants as well as from traditionally used rural remedies. Moreover, in these societies,
herbal remedies have become more popular in the treatment of minor ailments and also on
account of the increasing costs of personal health maintenance (Okigbo et al., 2009).
Some of the useful plant drugs include vinblastine, vincristine, taxol,
podophyllotoxin, camptothecin, digitoxigenin, gitoxigenin, digoxigenin, tubocurarine,
morphine, codeine, aspirin, atropine, pilocarpine, capscicine, allicin, curcumin,
artemesinin and ephedrine among others. In some cases, the crude extract of medicinal
plants may be used as medicaments. On the other hand, the isolation and identification of
the active principles and elucidation of the mechanism of action of a drug is of paramount
importance. Hence, works in both mixture of traditional medicine and single active
compounds are very important. Where the active molecule cannot be synthesized
economically, the product must be obtained from the cultivation of plant material. About
121 (45 tropical and 76 subtropical) major plant drugs have been identified for which no
synthetic one is currently available. The scientific study of traditional medicines,
derivation of drugs through bioprospecting and systematic conservation of the concerned
medicinal plants are thus of great importance (Joy et al., 2001).
5
Phytochemical investigations in plants
Successful determination of biologically active compound from plant material is
largely dependent on the type of solvent used in the extraction procedure. Properties of a
good solvent in plant extractions include low toxicity, ease of evaporation at low heat,
promotion of rapid physiologic absorption of the extract, preservative action and inability
to cause the extract to complex or dissociate. As the end product in extraction will contain
traces of residual solvent, the solvent should be non-toxic and should not interfere with the
bioassay. Variation in extraction methods are usually depend on the length of the
extraction period, solvent used, pH of the solvent, temperature, particle size of the plant
tissues and the solvent-to-sample ratio. Another common method is serial exhaustive
extraction which involves successive extraction with solvents of increasing polarity from a
non polar (hexane) to a more polar solvent (methanol) to ensure that a wide polarity range
of compound could be extracted. Other researchers employ soxhlet extraction of dried
plant material using organic solvent (Das, 2010).
The classical method of obtaining constituents of dried plant tissue is to
continuously extract the powdered material in soxhlet apparatus with a range of solvents
to obtain wide range of compounds. Identification of plant constituents can be achieved
from its response to color test, solubility, spectral characteristics and spot formation in
TLC (thin layer chromatography) and PC (paper chromatography). Nowadays, precoated
plates of commercial manufacture are usually employed since these have more uniform
and provide more reproducible results. The most recent being TLC plates coated with
same fine microparticles of silica that are used in HPLC (high performance thin layer
chromatography). Such chromatography is called HPTLC and it usually gives more
efficient and rapid separations than conventional silica layers at shorter time with better
resolution. The basic difference between TLC and HPTLC lies in particle and pore size of
the sorbents. The criteria for phytochemical identification are based on chromatographic
and spectral comparison, the extent of which depends on the class of the compound
(Harbone, 1998; Kokate, 2008).

6
Secondary metabolites are a group of compounds that do not get involved in
primary metabolism of the plant. But these compounds are now recognized to be involved
in adaptional and survival mechanism. They are produced in specially designed secondary
metabolic pathways. These compounds help the plants to face adversities, enemies and
competition. Studies on the dynamics of secondary metabolism indicated that here is a
definite turnover of these compounds evidenced by diurnal variation, seasonal variation
and different stages of development. Alkaloids are defensive agents dettering the
herbivore due to their bitter taste; volatile oils act as pheromone for pollination by insects
and protect the plant from microbes, competition, etc; diterpenes or triterpenes perform
wound healing and antimicrobial functions. Phenols act as antioxidant and protect cellular
membranes and tissues containing lipids against oxidation. Anthrocyanins and flavonoids
act as pollinator guide for insects as they are responsible for attractive coloration in
flowers. All sulfur containing compounds are antimicrobial in nature. Cardiac glycosides
are used by plants to protect from herbivore can be used in heart treatment. There are three
major classes of secondary metabolites, the largest group being that of alkaloids followed
by terpenoids and phenolics. Gums and mucilages are polysaccharides but considered as
secondary metabolite due to their function (Daniel, 2006).
Pharmacological action of different alkaloids (Daniel, 2006)
Scientific name Family Pharmacological action
Alkaloid
Papaver somnifreum Papaveraceae Analgesic and narcotics
Morphine and codeine
Campthoteca acuminata Nyssaceae Antitumor agents Campthotecin Strychnos toxifera Loganiaceae Muscle paralyzer Tubocurarine Erythroxylum coca Erythroxylaceae Local anesthetics Cocaine Mandragora officinarum Solanaceae Antispasmodic Atropine and
hyoscine Chinchona officinalis Rubiaceae Cardiac repressant Quinine
Alkaloids have been divided into three major classes depending on the precursors
and the final structure. The true alkaloids are derived from amino acids, are basic and
contain nitrogen in a heterocyclic ring for example, nicotine. Common alkaloid ring
structures include the pyridines, pyrroles, indoles, pyrrolidines, isoquinolines, and
7
piperidines (Ncube et al., 2008). Alkaloids are basic plant products possessing nitrogen
containing heterocyclic ring system and exhibiting marked pharmacological activity.
Alkaloids form a heterogenous group and have an alkaline nature due to nitrogen. The
degree of basicity depends on position of nitrogen and other functional groups. They are
usually water insoluble and their salts exist in crystalline form. Almost all alkaloids absorb
UV lignt and have characteristic absorption spectra. Alkaloids are usually toxic at high
concentration and their physiological activity depends on the dosage. They are associated
with different pharmacological actions (Harbone, 1998; Daniel, 2006).
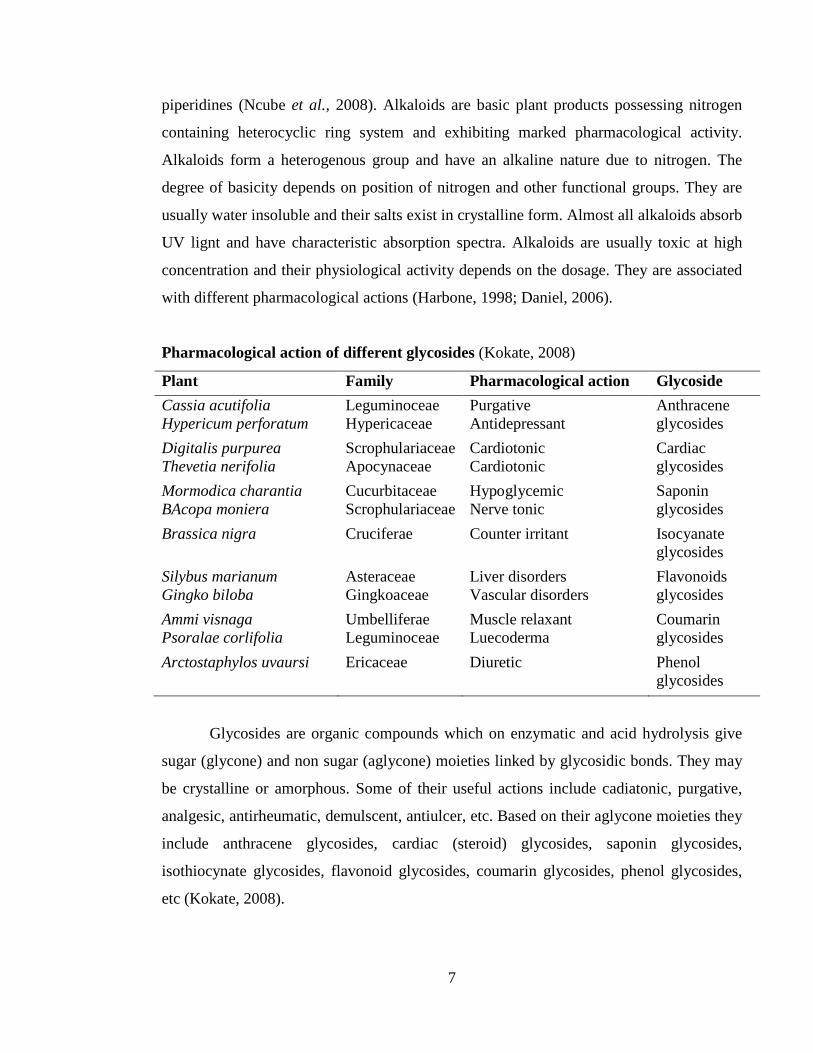
Pharmacological action of different glycosides (Kokate, 2008)
Plant Family Pharmacological action Glycoside Cassia acutifolia Hypericum perforatum
Leguminoceae Hypericaceae
Purgative Antidepressant
Anthracene glycosides
Digitalis purpurea Thevetia nerifolia
Scrophulariaceae Apocynaceae
Cardiotonic Cardiotonic
Cardiac glycosides
Mormodica charantia BAcopa moniera
Cucurbitaceae Scrophulariaceae
Hypoglycemic Nerve tonic
Saponin glycosides
Brassica nigra Cruciferae Counter irritant Isocyanate glycosides
Silybus marianum Gingko biloba
Asteraceae Gingkoaceae
Liver disorders Vascular disorders
Flavonoids glycosides
Ammi visnaga Psoralae corlifolia
Umbelliferae Leguminoceae
Muscle relaxant Luecoderma
Coumarin glycosides
Arctostaphylos uvaursi
Ericaceae
Diuretic
Phenol glycosides
Glycosides are organic compounds which on enzymatic and acid hydrolysis give
sugar (glycone) and non sugar (aglycone) moieties linked by glycosidic bonds. They may
be crystalline or amorphous. Some of their useful actions include cadiatonic, purgative,
analgesic, antirheumatic, demulscent, antiulcer, etc. Based on their aglycone moieties they
include anthracene glycosides, cardiac (steroid) glycosides, saponin glycosides,
isothiocynate glycosides, flavonoid glycosides, coumarin glycosides, phenol glycosides,
etc (Kokate, 2008).
8
Terpenoids are based on isoprene molecule (C5 molecule) with different modes of
ring closure, unsaturation and functional groups and are lipid soluble located mostly in
cytoplasm of plant cell. Some are also found to be associated with growth regulating
properties. Terpenoids are classified based on carbon chain into hemiterpenoids (C5),
monoterpenoids (C10), sesquiterpenoids (C15), diterpenoids (C20), sesterterpenoids
(C25), triterpenoids (C30), tertaterpenoids (C40) and polyterpenoids. The terpenoid
essential oil includes monoterpenes and sesquiterpenes, found to be used in perfume and
food industry. Triterpenoids are a heterogeneous collection of biochemical substances
which are derived from squalene (acyclic C30 hydrocarbon) by ring closure and
substitution. They are crystalline compounds and exist as alcohols, aldehydes or
carboxylic acids. Triterpenoids are divided into triterpenes, steroids, saponins and cardiac
glycosides. Saponins are glycoside of triterpenes and sterols. The sugar component
consists of oligosaccharides with 2-5 sugar unit, gluconic acid and aglycone. Sapogenics,
the aglycone may be triterpenes. The foam formation during plant extraction can be
attributed to saponins which have the ability to haemolyse blood cells. Saponins are more
polar then sapogenics due to attachment to glycosidic linkages. Saponins are employed as
expectorant, antitussive and antimicrobial agents (Harbone, 1998; Daniel, 2006).
The term phenolic compound embraces a wide range of plant substances which
possesses a common aromatic ring bearing one or more hydroxyl constituents. These
compounds have a single aromatic ring and include all phenolic alcohols, aldehydes,
ketones and their glycosides. Phenolic substances are water soluble since they are
combined with sugar as glycosides and located in cell vacuoles. Polymeric substances like
lignins, melanins and tannins are polyphenols and occasionally phenolic units are
encountered in proteins, alkaloids and terpenoids. Phenolics are effective antioxidants and
antimicrobial agents. Detection of simple phenols by development of the intense green,
purple, blue or black colors in presence of ferric chloride can be obtained. Majority of
phenolic compounds and flavonoids can be detected with their colors of fluorescence in
UV (since they are aromatic) light. Phenolic compounds are visibly colored and hence can
be easily isolated and purified. This group includes metabolites derived from the
condensation of acetate units (tepernoids), those produced by the modification of aromatic
9
amino acids (phenylpropanoids and coumarins), flavonoids, isoflavonoids and tannins.
Flavones, flavonoids and flavonols have been known to be synthesized by plants in
response to microbial infection so it is not surprising that they have been found, in vitro, to
be effective antimicrobial substances against a wide array of microorganisms (Bennet and
Wallsgrove, 1994).
The flavonoids form the largest group but simple monocyclic phenols,
phenylpropanoids and phenolic quinones exist in considerable numbers. Flavonoids are
water soluble phenolic compound derived from the parent substance flavone. They have
conjugated aromatic system and hence show absorption bands in UV and visible region.
Flavonoids are present in combination with glycosides and also in free state. The mixtures
of different flavonoid class of compounds (anthocyanins, proanthocyanidins, flavonols,
flavones, gycoflavones, biflavonyls, chalcones, aurones, neoflavanoids, flavonones and
isoflavonones) which give different colors and fluorescence with chemical and UV
treatment. The different classes are bases on oxidation pattern of C3, additional oxygen
heterocyclic rings and glycosylation. The spectra of properties exhibited by these
compounds include coloring of flowers and fruits, accessory pigments in photosynthesis,
astringency, estrogenic, etc (Harbone, 1998; Daniel, 2006).
Tannins are polyphenols having astringent taste and occur widely in vascular
tissues and associated with woody tissues. They react with proteins to form stable water
soluble polymers hence are capable to transform raw animal skin to leather. Plants rich in
tannins have astringent taste and thus act as major barrier to herbivores. Two main types
of tannins are condensed (flavolans) tannins found in ferns, gynosperms and angiosperms
while hydrolysable tannins found in dicots. Hydrolysable tannins are water soluble simple
phenolic acids esterified with sugar molecules while condensed tannins are water
insoluble polyphenols. Tannins have antifungal, antioxidant properties and are used as
medical astringents. Quinones are aromatic ketones and widely distributed in bark, roots,
etc. They exhibit structural and color variations, thus are largest class of natural coloring
compounds. They are found to be associated with purgative and cathartic action. They are
classified into benzoquinones, naphthaquinones, anthraquinones (mono, bi and tri cyclic
10
ring system, respectively) and isoprenoid quinines. Coumarins are formed by lactonization
of o-hydroxy cinnamic acid. They exist in aromatic form and also associated with
glycosides. Furanocoumarins and pyranocoumarins have a furan or pyrano ring attached
to benzene ring of coumarins. Furanocoumarins are associated with spasmolytic and
vasodilating effects. Lignans are dimers formed by condensation or two cinnamic acid or
cinnamyl alcohols through β-carbons of their aliphatic side chains and found to be
extensively used as antioxidants and antimicrobial agents. They are used in treating
malagncies and associated with cathartic action (Harbone, 1998; Daniel, 2006).
Gums and mucilages include all hydrocolloids of plant and are anionic or non
inonic polysaccharides of many monosaccharides. Gums are pathologic compounds
produced in response to injury by gummosis to for a colloid of cell wall and their
ingredients which serve as act as protective layer on wounded tissue. They are amorphous,
translucent and water soluble compounds. Mucilages on the other hand are natural plant
products for the inhibition and retention of water since they form slimy mass with water.
They are esters of sulphuric acid wherin ester groups are polysaccharide complex. But
from a chemical point of view, gums and mucilages are almost identical and serve as
laxatives (Harbone, 1998; Daniel, 2006; Kokate, 2008).
Primary metabolites include carbohydrates, proteins and lipids, since they are
continuously synthesized and utilized. But their storage in tissue without any reason hence
marked as secondary metabolites. Carbohydrates are the major source of energy in plants
made entirely of carbon. They are polyhydroxy aldehydes or ketones and their derivatives.
They are classified as monosaccharide, disaccharides and polysaccharides based on
number of carbon. They are present in tannins, saponins and cardiac glycosides. Dietary
fibres consisit of pectin, cellulose, lignins, etc. They have important effects on gut
functions, ability to absorb water, constipation, diverticular diseases and appendicitis. The
plant world is made of 300 amino acids, wherein 20-26 form proteins while rest are non
protein amino acids. The non proteins occur free or as peptides and exhibit various
biological activity. They are classified into D-amino acids, non α-amino acids,
dicarboxylic acids, amides, sulfur containing amino acids, hydoxy amino acids,
11
heterocyclic and alicyclic amino acids. They form important constituents of enzymes and
vitamins (Harbone, 1998; Daniel, 2006).
The identification of biologically active compounds is an essential requirement for
quality control and dose determination of plant-based drugs. A medicinal herb can be
viewed as a synthetic laboratory as it produces and contains a number of chemical
compounds. These compounds are responsible for medical activity of the herb, are usually
secondary metabolites. For example, alkaloids which are nitrogenous principles of organic
compounds combine with acids to form crystalline salts. In addition, herbs may contain
saponins, resins, oleoresins, lactones and volatile oils. Complete phytochemical
investigations of most of the medicinally important herbs of India have not been carried
out so far. This would be beneficial in standardization and dose determination of herbal
drugs. Further, there should be a quality control test for the entire preparation to ensure the
quality of the drug. There is no doubt that most herbs exhibit their effects on a variety of
constituents and the idea of synergy within and between them is also gaining acceptance.
It is not well-documented in most of the herbal medicines whether they are acting truly in
a synergistic way or by additive effects. Clinical evaluation is also difficult, without
knowing the extent to which synergy occurs within the herbal preparations. Some of the
components of the crude drugs may not have any biological activity, Ginger (Zingiber
officinale) is another example of a chemically unstable range of compounds being
responsible for the activity and probably acting synergistically (Dubey et al., 2004). St
John’s wort (Hypericum perforatum, family Hypericaceae) thus represents a good
example of a herb which may exhibit synergism and polyvalent action.
The isolation of physiologically active principles of indigenous plant materials and
the elucidation of their chemical structure and therapeutic status is most frustrating, may
be due to the lack of contribution between botanist, pharmacologist, chemist and
clinicians, because it is only through their cooperation that new therapeutic agents can be
established. Hence drugs of plant origin have failed to acquire full measure of their
importance in the pharmaceutical industry. In this context, American pharmaceutical
industry suggested that 47.2% of the total number of prescription in United States during
12
1960 were based on natural products while 52.8% on synthetic drugs. It is quite evident
that studies on medicinal plants continue to offer vast and attractive field of research for
chemist and presently serve as mainstay for providing a big reservoir of physiologically
active constituents for human welfare. Interest in medicinal plants was recorded as a result
of isolation of new alkaloids from Rauwolfia serperntina which gained importance in the
treatment of cardiovascular diseases and mental ailments. Reserpine has been extensively
used in the treatment of hypotension and as an aid in psychotherapy. Discovery of life
saving drugs like vinblastine and vincristine from Vinca rosea, for treatment of of certain
types of cancers including leukemia and Hodkin’s disease have strengthened interest in
active principles of medicinal plants. These investigations have served dual purpose of
isolating new medicinally important substances and providing basis of therapeutic studies
directed towards the synthesis of drugs modeled on the chemical structure of natural
products (Ayatollahi and Malik, 1991).
Plants with antimicrobial activity
Plant derived substances have recently become of great interest owing to their
versatile applications. Medicinal plants have been used for centuries as remedies for
human diseases and offer a new source of biologically active chemical compound as
antimicrobial agent. Medicinal plants are the richest bio-resources of drugs of traditional
medicinal systems, modern medicines, nutraceuticals, food supplements, folk medicines,
pharmaceuticals, intermediate and chemical entitled for synthetic drugs. It has been
estimated that 14 - 28% of higher plant species are used medicinally and that 74% of
pharmacologically active plant derived components were discovered after following up on
ethno medicinal use of the plants. Recently the acceptance of traditional medicine as an
alternative form of health care and the development of microbial resistance to the
available antibiotics has led authors to investigate the antimicrobial activity of medicinal
plants. Substantial use of chemical pesticides induces problems of health and
environmental hazards in agricultural system. So, for human and plants natural products of
antimicrobial activity are best biorational alternatives today. Over the last two decades,
intensive effort has been made to discover chemically useful antibacterial or antifungal
drugs of plant origin. Medicinal plant based antimicrobials represent a vast untapped

13
source of pharmaceuticals and further exploration of plant antimicrobials need to occur for
treatment of infectious diseases both in plants and humans while simultaneously for
mitigating many of the side effects that are often associated with synthetic antimicrobials.
Out of the several hundred thousand medicinal plant species around the globe, only a
small portion has been investigated both phytochemically and pharmacologically (Das et
al., 2010).
Existence of humans on the earth is made possible because of the vital role played
by the plant kingdom. Besides providing basic requirements of man, the plants offer
unique protection to mankind by providing innumerable drugs to prevent and treat various
disorders. Drugs used in modern medicine were initially used in crude form in traditional
or folk healing practices. The benefits of plant derived medicines are that they are
relatively safer than synthetic alternatives, offering profound therapeutic benefits and
more affordable treatment. Phytomedicines represent vast untapped sources of drugs
effective in treating infectious diseases simultaneously mitigating many of the side effects
of synthetic antimicrobials (Iwu et al., 1999). In a constant attempt to improve the quality
of life, men have used plants as source of food, shelter, clothing, cosmetic, medicine and
for seeking relief from hardship of life. Some plants are known as medicinal because they
contain active substances that cause certain reaction from relenting to the cure of diseases
of man (Sliva-Junor, 1994).
Knowledge of medicinal plants sometimes means the only therapeutic resource (Di
Stasi, 1996) of some communities and ethnic group (Odunbaku et al., 2008). Infectious
diseases are a major cause of morbidity and mortality worldwide (WHO, 2004). Clinical
microbiologists have two reasons to be interested in the topic of antimicrobial plant
extracts. First, it is very likely that these phytochemicals will find their way into the
arsenal of antimicrobial drugs prescribed by physicians; several are already being tested in
humans. It is reported that, on average, two or three antibiotics derived from
microorganisms are launched each year. After a downturn in that pace in recent decades,
the pace is again quickening as scientists realize that the effective life span of any
antibiotic is limited. Worldwide spending on finding new anti-infective agents (including

14
vaccines) is expected to increase 60% from the spending levels in 1993. New sources,
especially plant sources, are also being investigated. Second, the public is becoming
increasingly aware of problems with the over prescription and misuse of traditional
antibiotics. In addition, many people are interested in having more autonomy over their
medical care. A multitude of plant compounds (often of unreliable purity) is readily
available over-the-counter from herbal suppliers and natural-food stores, and self-
medication with these substances is common place. The use of plant extracts, as well as
other alternative forms of medical treatments, is enjoying great popularity in the late
1990s. Earlier in this decade, approximately one-third of people surveyed in the United
States used at least one “unconventional” therapy during the previous year. It was reported
that in 1996, sales of botanical medicines increased 37% over 1995 (Cowan, 1999).
Medicinal plants have been used for centuries as remedies for human diseases and
offer a new source of biologically active chemical compound as antimicrobial agent.
Medicinal plants are the richest bio-resources of drugs of traditional medicinal systems,
modern medicines, nutraceuticals, food supplements, folk medicines, pharmaceuticals,
intermediate and chemical entitled for synthetic drugs (Hammer et al., 1999). The
evaluation for antimicrobial agent of plant origin begins with thorough biological
evaluation of plant extracts to ensure efficacy and safety followed by identification of
active principles, dosage formulations, efficacy and pharmacokinetic profile of the new
drug. Many plants have been used because of their antimicrobial traits and antimicrobial
properties of plants have been investigated by a number of researchers worldwide. Ethno
pharmacologists, botanists, microbiologists and natural product chemists are searching the
world for phytochemicals which could be developed for treatment of infectious diseases
(Tanaka et al., 2006).

15
List of plants with antimicrobial activity (Cowan, 1999)
Common name Scientific name Compound Class Activity
Aloe Aloe barbadensis, Aloe vera Latex Complex mixture Corynebacterium,
Salmonella, Streptococcus
Apple Malus sylvestris Phloretin Flavonoid derivative General
Basil Ocimum basilicum Essential oils Terpenoids Salmonella, bacteria
Bay Laurus nobilis Essential oils Terpenoids Bacteria, fungi
Betel pepper Piper betel Catechols, eugenol Essential oils General
Black pepper Piper nigrum Piperine Alkaloid Fungi, Lactobacillus, Micrococcus, E. coli, E. faecalis
Blueberry Vaccinium spp. Fructose Monosaccharide E. coli
Buchu Barosma setulina Essential oil Terpenoid General
Buttercup Ranunculus bulbosus Protoanemonin Lactone General
Ceylon cinnamon
Cinnamomum verum
Essential oils, others Terpenoids, tannins General
Chili peppers, paprika
Capsicum annuum Capsaicin Terpenoid Bacteria
Clove Syzygium aromaticum Eugenol Terpenoid General
Fava bean Vicia faba Fabatin Thionin Bacteria
Garlic Allium sativum Allicin, ajoene Sulfoxide General
Henna Lawsonia inermis Gallic acid Phenolic Staphylococcus aureus
Olive oil Olea europaea Hexanal Aldehyde General
Onion Allium cepa Allicin Sulfoxide Bacteria, Candida
Papaya Carica papaya Latex Mix of terpenoids, organic acids, alkaloids General
Peppermint Mentha piperita Menthol Terpenoid General
Periwinkle Vinca minor Reserpine Alkaloid General
Quinine Cinchona sp. Quinine Alkaloid Plasmodium spp.
Turmeric Curcuma longa Curcumin Terpenoids Bacteria, protozoa
Plants have limitless ability to synthesize aromatic secondary metabolites, most of
which are phenols or their oxygen-substituted derivatives. Important subclasses in this
group of compounds include phenols, phenolic acids, quinones, flavones, flavonoids,
flavonols, tannins and coumarins. These groups of compounds show antimicrobial effect
16
and serves as plant defense mechanisms against pathogenic microorganisms (Das et al.,
2010). Antimicrobial activity of Cassia alata was noticed against E. coli and fungi
(Ikenebomeh et al., 1988). Water extract of Senna alata showed antimicrobial activity
against B. subtilis only but other reports of antimicrobial activity exists (Adebayo et al.,
1991, Ibrahim and Osman 1995).
Standard criteria for in vitro evaluation of antimicrobial activity of plants differ
among authors. Results obtained from antimicrobial efficacy of plant extract is often
difficult to compare with published results due to the influence of several factors, that is,
environment and climatic conditions during plant growth, choice of plant extracts, choice
of extraction methods and antimicrobial tests employed and on test microorganisms
(Nostro et al., 2000 and Hammer et al., 1999). The beneficial medicinal effect of plant
materials basically results from the secondary products present in the plant and is not
usually attributed to a single compound but a combination of the metabolites (Parekh et
al., 2005). Because of available antimicrobials failure to treat infectious diseases, many
researchers have focused on the investigation of natural products as source of new
bioactive molecules. A variety of methods are found for this purpose and since not all of
them are based on same principles, results obtained will also be profoundly influenced not
only by the method selected, but also by the microorganisms used to carry out the test, and
by the degree of solubility of each test compound. The test systems should ideally be
simple, rapid, reproducible, inexpensive and maximize high sample throughput in order to
cope with a varied number of extracts and fractions. The complexity of the bioassay must
be defined by laboratory facilities and quality available personnel. The currently available
screening methods for the detection of antimicrobial activity of natural products fall into
three groups, including bioautographic, diffusion, and dilution methods. The
bioautographic and diffusion methods are known as qualitative techniques since these
methods will only give an idea of the presence or absence of substances with antimicrobial
activity. On the other hand, dilution methods are considered quantitative assays once they
determine the minimal inhibitory concentration. Antimicrobial activities reported in the
literature have been evaluated with diverse sets of methodologies, degrees of sensitivity,

17
amount of test compounds and microbial strains, often difficult to compare (Cowan,
1999).
Plants with antihelmintic activity
The World Health Organization estimates that a staggering two billion people
harbor parasitic worm infections. Parasitic worms also infect livestock and crops, affecting
food production with a resultant economic impact. Despite this prevalence of parasitic
infections, the research on anthelmintic drug is poor. As per WHO, only few drugs are
frequently used in the treatment of helminthes in human beings. Anthelmintics from the
natural sources may play a key role in the treatment of these parasite infections (Aswar
Manoj et al., 2008). Helminth infections are among the most common infections in
humans, affecting a large population of the world. Although the majority of infections due
to worms are generally limited to tropical regions and pose a great threat to health and
contribute to the prevalence of malnutrition, anaemia, eosinophilia and pneumonia
(Bundy, 1994). Parasitic diseases cause severe morbidity affecting mainly population in
endemic areas with major economic and social consequences (Tagbota and Townson,
2001). The gastro-intestinal helminthes becomes resistant to currently available
antihelmintic drugs therefore there is a foremost problem in treatment of helminthes
diseases (Sondhi et al., 1994), hence there is an increasing demand towards natural
antihelmintics.
Parasitic worms also infect livestock and crops, affecting food production with a
resultant economic impact. Also of importance is the infection of domestic pets. Indeed,
the animal market is a major economic consideration for animal health, thus companies
are undertaking drug discovery programmes. Despite the prevalence of parasitic worms,
anthelmintic drug discovery is poor in relation of the pharmaceutical industry. The simple
reason is that the nations which suffer most from these tropical diseases have little money
to invest in drug discovery or therapy. It comes as no surprise therefore that the drugs
available for human treatment were first developed as veterinary medicines. There is thus
a pitifully small repertoire of chemotherapeutic agents available for treatment. In some
respects, this situation has been exacerbated by the remarkable success of ivermectin over

18
the last twenty years (Geary, 2005), which has decreased motivation for anthelmintic drug
discovery programmes (Geary Patel et al., 1999). This prompts concern, as anthelmintic
resistance has been widely reported in livestock and it may also only be a matter of time
before this phenomenon occurs in parasites of humans.
Helminth infections are among the most common infections in man, affecting a
large proportion of population all over the world. In developing countries they pose a large
threat to public health and contribute to the prevalence of malnutrition, anaemia,
eosinophilia and pneumonia. Although the majority of infections caused due to worms are
generally limited to tropical regions. Parasitoses have been of concern to the medical field
for centuries and the helminthes still cause considerable problems for human beings and
animals. During the past few decades, despite numerous advances made in understanding
the mode of transmission and the treatment of these parasites, there are still no efficient
products to control certain helminths and the indiscriminate use of some drugs has
generated several cases of resistance. Furthermore, it has been recognized recently that
anthelmintic substances having considerable toxicity to human beings are present in foods
derived from livestock, posing a serious threat to human health (Patel et al., 2011). Some
workers have reported antihelmintic activity in the essential oils of Piper betle Linn.,
Anancardium occidentale Linn. and seed oils of Gynandropsis gynandra Linn., Impatiens
balsamina Linn., Celastrus peniculata Willd., Embelia ribes Burm. F. and Mucuna prurita
Hook. against the earthworm Pheretima Posthuma (Mali and Mehta, 2008).
Plants with potential anthelmintic activity (Behnke et al., 2008)
Species Enzymes known to be contained Papaya papain, chymopapain, caricain, glycyl endopeptidase Fig ficin, ficain Pineapple ananain, fruit bromelain, stem bromelain, comosain Kiwi fruit Actinidain Egyptian milkweed Asclepain Cowhage Mucunain

19
Plants providing protection against hepatic and renal disorders.
Several chemicals have been known to induce hepatotoxicity. Carbontetrachloride
(CCl4), Galactosamine, d-Galactosamine/Lipopolysachharide (GalN/LPS), Thioacetamide,
antitubercular drug paracetamol, arsenic etc are used to induce experimental
hepatotoxicity in laboratory animals. Liver injury due to CCl4 in rats was first reported in
1936 (Cameron et al., 1936) and has been widely and successfully used by many
investigators (Handa et al., 1990; Shirwaiker et al., 1996). Carbon tetrachloride is
metabolized by cytochrome P-450 in endoplasmic reticulum and mitochondria with the
formation of CCl3O*, a reactive oxidative free radical, which initiates lipid peroxidation
(Zimmerman et al., 1976; Agarwal et al., 1983).
CCl4 CCl3O- + O-
Administration of a single dose of CCl4 to a rat produces, within 24 hrs, a
centrilobular necrosis and fatty changes (Cameron et al., 1936). The poison reaches its
maximum concentration in the liver within 3 hrs of administration. Thereafter, the level
falls and by 24 hrs there is no CCl4 left in the liver (Dawkins, 1963). The development of
necrosis is associated with leakage of hepatic enzymes into serum. Dose of CCl4 that
induces hepatotoxicity ranges from 0.1 to 3 ml/kg administered intraperitoneally.
Nature has provided an excellent storehouse of remedies to cure all the ailments of
mankind. In ancient days, almost all the medicines used were from natural sources,
particularly from plants. Plants continue to be an important source of new drugs even
today. The importance of botanical, chemical and pharmacological evaluation of plant-
derived agents used in the treatment of human ailments has been increasingly recognized
in the last decades. Herbal remedies are widely used for the treatment and prevention of
various diseases and often contain highly active multitude of chemical compounds.
Modern research is now focusing greater attention on the generation of scientific
validation of herbal drugs based on their folklore claim. In this modern era, a large number
of Indian population still relies on the traditional system of medicine, which is mostly
20
plant based. Free radical initiating auto oxidation of cellular membrane lipids can lead to
cellular necrosis and is now accepted to be important in connection with a variety of
pathological conditions. Liver is an aerobic organ which generates reactive oxygen species
that induce oxidative tissue damage. These radicals react with cell membranes and induces
lipid per oxidation or causes inflammation, which may result as important pathological
mediators in many clinical disorders such as heart disease, diabetes, gout and cancer.
Reduction of these radicals by antioxidant molecules is crucial for the protection of cells
against various disorders. Development of life threatening diseases like cancer and also
liver disorders are linked to the availability of these antioxidants (Vadivu et al., 2008).
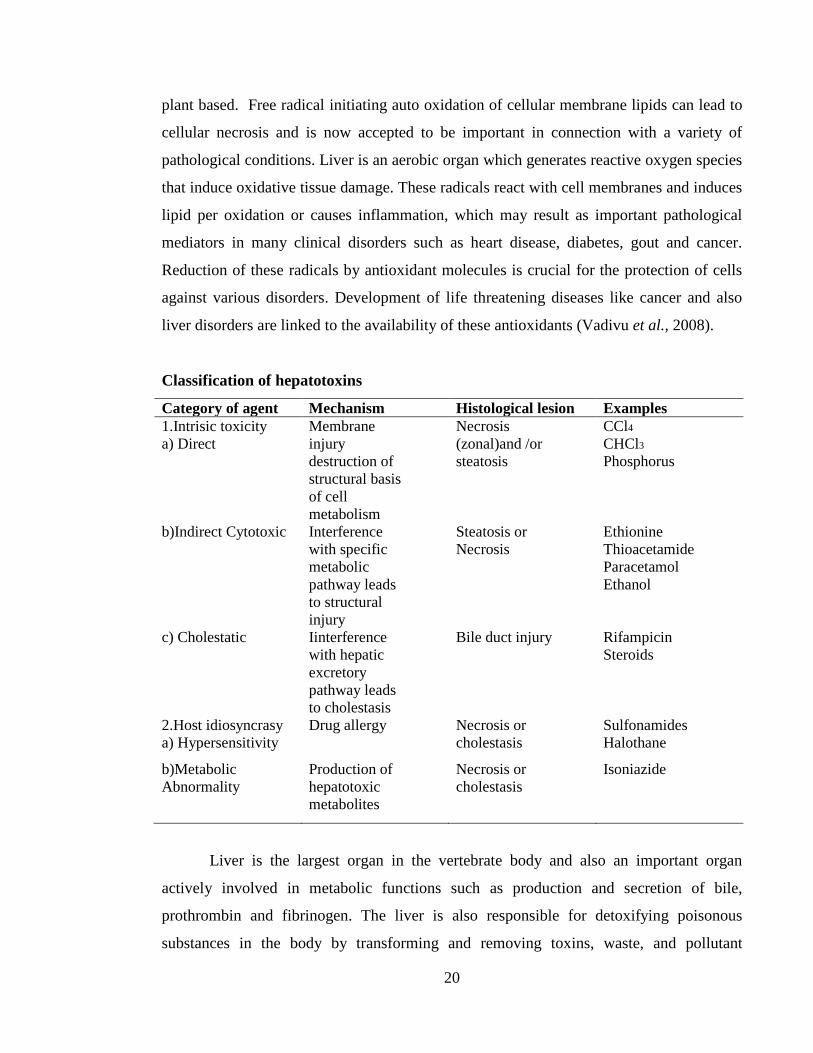
Classification of hepatotoxins
Category of agent Mechanism Histological lesion Examples 1.Intrisic toxicity a) Direct
Membrane injury destruction of structural basis of cell metabolism
Necrosis (zonal)and /or steatosis
CCl4
CHCl3
Phosphorus
b)Indirect Cytotoxic Interference with specific metabolic pathway leads to structural injury
Steatosis or Necrosis
Ethionine Thioacetamide Paracetamol Ethanol
c) Cholestatic Iinterference with hepatic excretory pathway leads to cholestasis
Bile duct injury
Rifampicin Steroids
2.Host idiosyncrasy a) Hypersensitivity
Drug allergy Necrosis or cholestasis
Sulfonamides Halothane
b)Metabolic Abnormality
Production of hepatotoxic metabolites
Necrosis or cholestasis
Isoniazide
Liver is the largest organ in the vertebrate body and also an important organ
actively involved in metabolic functions such as production and secretion of bile,
prothrombin and fibrinogen. The liver is also responsible for detoxifying poisonous
substances in the body by transforming and removing toxins, waste, and pollutant
21
xenobiotics. A large number of medicinal preparations are recommended for the treatment
of liver disorders and quite often claimed to offer significant relief which would not be
possible in absence of reliable liver-protective drugs in modern medicine, (Jain et al.,
2009). Carbon tetrachloride also known as tetra chloromethane is known to have
hepatotoxic effects. On exposure, the liver is inflamed and the hepatocytes destroyed
(Sanni et al., 2007). Though CCL4 is a potent hepatotoxin, in addition to hepatic problems
CCL4 also causes disorders in kidney. Exposure to CCL4 causes acute and chronic renal
injuries (Manna et al., 2006). Herbal drugs are prescribed widely even when their
biologically active components are unknown because of their effectiveness, fewer side
effects and relatively low cost (Krishna Mohan et al., 2007). Certain toxic chemicals and
medicines can cause damage to organs, which has been recognized as a toxicological
problem. However, herbal medicines are known to play an important role in the treatment
of various ailments. Many traditional practitioners have claimed that numerous medicinal
plants and their formulations can be effectively used for the alleviation of different types
of liver and kidney diseases (Vadivu et al., 2008). Casuarina equisetifolia, Cajanus cajan,
Glycosmis pentaphylla, Bixa orellana, Argemone mexicana, Physalis minima, Caesalpinia
bonduc were observed to provide dose-dependent protection against CCl4 induced
hepatocellular injury (Ahsan et al., 2009).
Alterations in kidney structure and function are frequently found in severe liver
disease and once liver function falls below a critical threshold, sodium retention occurs
followed by ascites, associated with profound disturbances of splachnic and systemic
hemodynamics which in turn may affect renal function (Schrier, 1988; Weinberg, 1991).
As disease progresses, constriction of intrarenal vascular system favors marked sodium
and water retention, leading to refractory ascites, a progressive rise in plasma creatinine
levels and reduction of renal clearances (decompensated cirrhosis). Persistent renal
hypoxia may also induce tubular damage (Gentilini et al., 1999). Development of renal
failure in patients with liver failure is frequent, it occurs in approximately in 55% of the
patients. This complication may result when the cirrhotic individual is exposed to
xenobiotics, either therapeutic drugs or environmental pollutants, especially heavy metals.
Renal function is rarely restored in the absence of hepatic recovery (Moore, 1999).
22
Administration of carbon tetrachloride (CCl4) to rats results in a reproducible experimental
model of cirrhosis that resembles the disease in humans and provides a tool to study liver-
kidney interrelationships (Mclean et al., 1969; Perez, 1983). Previously experimental
model of acute liver and renal damage was produced by intragastric administration of a
single dose of CCl4 to cirrhotic rats. In this experimental model there were hemodynamic
and renal functional alterations similar to those observed in the human with
decompensated cirrhosis. This model is useful to study the pathogenesis of renal failure
associated with liver damage when the hepatic function decrease after an acute liver
damage (Rincon et al., 1999).
In spite of tremendous advances in modern medicine no effective drugs are
available, which stimulates liver functions and offer protection to the liver from the
damage or help to regenerate hepatic cells. In absence of reliable liver-protective drugs in
modern medicine, a large number of medicinal preparations are recommended for the
treatment of liver disorders and quite often claimed to offer significant relief. Attempts are
being made globally to get scientific evidences for these traditionally reported herbal
drugs (Jain et al., 2009). In view of severe undesirable side effects of synthetic agents,
there is growing focus to follow systematic research methodology and to evaluate
scientific basis for the traditional herbal medicines that are claimed to possess
hepatoprotective activity. A single drug cannot be effective for all types of severe liver
diseases. Therefore, indigenous medicinal plants are being investigated (Samundram et
al., 2009).
In the status of normal metabolism, the levels of oxidants and antioxidants in
humans are maintained in balance, which is important for sustaining optimal physiological
conditions. Overproduction of oxidants in certain conditions can cause an imbalance,
leading to oxidative damage to large biomolecules such as lipids, DNA, and proteins (Jie
Sun et al). Oxidative stress results from either a decrease of natural cell antioxidant
capacity or an increased amount of reactive oxygen species (ROS) in organisms. When the
balance between oxidants and antioxidants in the body is shifted by the overproduction of
free radicals, it will lead to oxidative stress and DNA damage. When left unrepaired, it can
23
cause base mutation, single- and double-strand breaks, DNA cross-linking, and
chromosomal breakage and rearrangement (Yi-Fang Chu et al., 2002). The importance of
natural antioxidants has been clarified by studies which have demonstrated that the
consumption of foods rich in such phytochemicals can exert beneficial effects upon
human health, possibly by interfering in the processes involved in reactive oxygen and
nitrogen species mediated pathologies. This has resulted in resurgence in phyto-
pharmacognosy with extensive attention upon the role that plant secondary metabolites
may have in preventative medicine (Damein-Dorman et al., 2003).
Plants having hepatoprotective activity (Khabiya and Joshi, 2010)
Plant Scientific name Plant Part Holy Milk Thistle Silybum marianum Seed, fruits Amla Phyllanthus niruri Whole plant Indian bearberry Berberis aristata Root stem bark Turmeric Curcuma longa Rhizome Liquorice Glycyrrhiza glabra Root Tulsi Ocimum sanctum Whole plant, roots, seed.
Plants with antidiabetic activity
Diabetes mellitus has been known since ages and the sweetness of diabetic urine
has been mentioned in Ayurveda by Sushruta. Its pharmacotherapy however is over 80
years old. The word diabetes was coined by a Greek physician in the first century A.D. In
the 17th century, Willis observed that the urine of diabetics as wonderfully sweet as if
imbued with honey or sugar. The presence of sugar in the urine of diabetics was
demonstrated by Dobson in 1755. Diabetes is a chronic disease affecting around 2-3 % of
the population worldwide. Unfortunately, after the introduction of sulfonylurea and
metformin about 50 years back no major lead has been obtained in this direction of finding
a proper drug for diabetes. Plant materials which are being used as traditional medicine for
the treatment of diabetes are considered one of the good sources for a new drug or a lead
to make a new drug. Plant extract or different folk plant preparations are being prescribed
by the traditional practioners and also accepted by the users for diabetes like for any other
diseases in many countries especially in third world countries. Now a days more than 400
plants are being used in different forms for hypoglycaemic effects all the claims

24
practitioners or users are neither baseless nor absolute. Therefore, a proper scientific
evaluation for screening of plant by pharmacological tests followed by chemical
investigations is necessary. Diabetes mellitus is wide spread disorder, which has long been
in the history of medicine. Before the advent of insulin and oral hypoglycaemic drugs the
major form of treatment involved the use of the plants. But now from the last two decades
there has been a new trend in the preparation and marketing of herbal drugs. Further it has
been estimated that in the U.S. 25% of all prescription dispensed from community
pharmacies contain plant extracts (Wadkar et al., 2008).
On the basis of etiology two main categories of diabetes are recognized, viz.
primary diabetes and secondary diabetes. Primary diabetes is divided into two types i.e.
Juvenile onset diabetes which is also referred as Type 1 or Insulin dependent diabetes
mellitus (IDDM) and Maturity onset diabetes which is also referred as Type II / Non-
insulin dependent diabetes mellitus (NIDDM). In Juvenile onset diabetes there is a
profound decrease in the number of b cells in the islet of Langerhans and thus there is
absolute deficiency of insulin. The main treatment for this type is insulin. The NIDDM
patients are usually obese and the treatment is usually dietary, though supplementary oral
hypoglycaemic drugs. It is diagnosed by blood or urinary glucose measurement. Insulin
resistances as well as loss of insulin secretion contribute to the onset of disease. The
symptoms of secondary diabetes are pancreatic dysfunction (pancreatitis,
pancreatectomy), hormonal imbalance (eg : acromegaly, pheochromacytoma), Cushing’s
syndrome, glucagonoma, and drugs or chemical induced reactions (eg: glucocorticoids,
anticancer agents, streptozotocin or diazoxide, thiazide, some psychoactive agents).
Diagnosis of early Diabetes Mellitus in diabetes are hyperglycemia, glycosuria, loss of
weight due to increased breakdown of fat and tissue protein, increased production of
ketone bodies by liver and their incomplete utilization by the tissue leading to their
accumulation in blood (Ketosis) and elimination in urine (Ketonuria), lowering of PH of
blood due to circulating keto acids (acidosis), dehydration due to elimination of large
amounts of water with glucose in urine, increased levels of lipid, fatty acids and
cholesterol in blood (lipemia) and increased tendency to develop cataract in the eye and
atheromatous and artherosclerotic lesions of blood vessels (Wadkar et al., 2008).

25
Diabetes mellitus is a metabolic disorder of the endocrine system. The disease is found
in all parts of the world and is rapidly increasing worldwide. People suffering from
diabetes cannot produce or properly use insulin, so they have high blood glucose. Type 2
diabetes, non–insulin-dependent diabetes mellitus, in which the body does not produce
enough insulin or properly use it, is the most common form of the disease, accounting for
90%–95% of cases. Type 2 is nearing epidemic proportions as a result of an increased
number of elderly people and a greater prevalence of obesity and sedentary lifestyle. The
cause of diabetes is a mystery, although both genetic and environmental factors such as
obesity and lack of exercise appear to play a role. According to World Health
Organization projections, the diabetic population is likely to increase to 300 million or
more by the year 2025. Currently available therapies for diabetes include insulin and
various oral antidiabetic agents such as sulfonylureas, biguanides, a-glucosidase
inhibitors, and glinides, which are used as monotherapy or in combination to achieve
better glycemic regulation. Many of these oral antidiabetic agents have a number of
serious adverse effects; thus, managing diabetes without any side effects is still a
challenge. Therefore, the search for more effective and safer hypoglycemic agents has
continued to be an important area of investigation. The hypoglycemic effect of several
plants used as antidiabetic remedies has been confirmed, and the mechanisms of
hypoglycemic activity of these plants are being studied. New natural products reported
from 2001 to 2004 with antidiabetic potential that have potent medicinal activities with
diverse structures (Jung et al., 2006).
Diabetes mellitus is a disease in which blood vessels of glucose (sugar) are high
because the body does not produce or properly use insulin. There are two major forms of
diabetes mellitus. Type 1 diabetes develops when the pancreas does not produce insulin.
Type 2 diabetes occurs when the body cell resist insulin’s effect (Microsoft Encarta,
2009). This condition leads to elevated levels of blood glucose. The normal range of blood
glucose level for blood glucose level is between 70-110mg/dl. Insulin is a hormone that
helps to maintain normal blood glucose level by making the body’s cell absorbs glucose
(sugar) so that it can be as a source of energy. In people with diabetes glucose levels build

26
up in the blood and urine causing excessive urination, thirst, hunger and problems with
fats and protein metabolism because the body cannot convert glucose into energy, it
begins to break down stored fats for fuel. This produces increasing amounts of acidic
compounds in the blood called ketone bodies which interfere with cellular respiration
energy producing process in cells. Alloxan induces diabetes mellitus in rats. Alloxan, a
beta cytotoxin, induces diabetes in a wide variety of animal species through damage of
insulin secreting cell. These animals develop characteristic similar to type 1 diabetes in
humans. Hypercholesterolemia and hypertriglyceridemia are common complications of
diabetes mellitus (Rerup, 1999).
Coopertein and Watkins (1978), Lazarow (1964) have shown that alloxan probably
exerts toxic effect on the beta-cells by selectively interacting with certain components of
the plasma membrane. This results in an altered permeability which permits the diffusion
of extra cellular fluid markers such as D-mannitol and insulin into the surrounding
incubation medium. However, the fact that only beta-cell components of intermediate cells
are affected by alloxan suggests that there is no comparable damage to their plasma
membrane as occurs in the beta-cell (Cooperstein, 1964), but is consistent with the
possibility that alloxan interacts with the membranes of the beta-cell cytoplasmic
organelle. In intermediate cells this imitates the remarkably selective recognition and an
autophary of these organelles. The same considerations probably apply to the effects of
streptozotoxia on the intermediate cells. Alloxan is known to induce diabetic renal
changes as well as causing nephrotoxic alterations however. No ultra structural study has
been performed to differentiate diabetic verses toxic effect of tubules and glomerulus
(Andrew et al, 1992).
Diabetes mellitus is a debilitating and often life-threatening disorder with
increasing incidence throughout the world. Diabetic complications arise partly from
glycosylation damage to structural and functional proteins and reflect chronic failure to
maintain blood glucose homeostasis. Other complications such as diabetic nephropathy,
diabetic retinopathy, diabetic neuropathy and diabetic cardiomyopathy prevail as a result
of hyperglycemia. A scientific investigation of traditional herbal remedies for diabetes
27
may provide valuable leads for the development of alternative drugs and strategies.
Alternatives are clearly needed for better management of diabetes because of high cost
and poor availability of current therapies for many rural populations, particularly in
developing countries. Diabetic nephropathy is one of the microvascular complications of
diabetes. The pathophysiology involves an interaction between metabolic and
hemodynamic factors. Metabolic factors include advanced glycation, increased formation
of polyols and activation of protein kinase-C. Hemodynamic factors include systemic
hypertension, intraglomerular hypertension and the role of vasoactive hormones, such as
anglotensin II. Clinical course progresses from microalbuminuria to overt proteinuria and
then to renal failure. The field of herbal medicines research has been gaining significant
importance in the last few decades and the demand to use natural products in the treatment
of diabetes is increasing worldwide. The available literature shows that there are more
than 400 plant species showing antidiabetic activity. Although some of these plants have
great reputation in Ayurveda, the indigenous Indian system of medicine, many remain to
be scientifically established (Rao and Nammi, 2006). Diabetes mellitus is one of the
common metabolic disorders and 1.3% of the population suffers from this disease
throughout the world. Insulin and oral hypoglycemic agents like sulphonylureas and
biguanides are still the major players in the management of the disease. Due to lack of
insulin, hyperglycemia and glycosuria almost invariably occur. The search for a curative
agent against this disease resulted in the introduction of several hypoglycemic agents.
Some of which are used therapeutically. However, various harmful side effects and weak
effectiveness of them made their use limited and the search to find more effective agents
continues. Investigation in the plant kingdom culminated in the discovery of many herbal
hypoglycemic agents (Tatiya et al., 2011).
Traditional medicines from readily available medicinal plants offer great potential for
the discovery of new antidiabetic drugs. Many traditional plant treatments for diabetes
exist, a hidden wealth of potentially useful natural products for diabetes control.
Nonetheless, few traditional antidiabetic plants have received scientific or medical
scrutiny, despite recommendations by the World Health Organization in 1980 that this
should be undertaken. Medicinal plants that are the most effective and the most commonly
28
studied in relation to diabetes and its complications are: Gentiana olivieri griseb
(Gentianaceae), Bauhinia forficata koeingii (Leguminosae), Eugenia jambolana L.
(Myrtaceae), Lactuca indica L. (Compositae), Mucuna pruriens Bak. (Leguminosae),
Tinospora cordifolia W. (Menispermaceae), Momordica charantia L. (Cucurbitaceae),
Aporosa lindleyana Baill (Euphorbiaceae), Cogent db, Myrtus communis L. (Myrtaceae),
Rhizoma Polygonati Odorati (Liliaceae), and Terminalia pallida Brand. (Combretaceae).
Most of these plants have shown varying degrees of hypoglycemic and anti-
hyperglycemic activity. Among active medicinal herbs, Momordica charantia L.
(Cucurbitaceae), Pterocarpus marsupium Roxb. (Leguminoceae), and Trigonella foenum
greacum L. (Leguminosae) have been reported to be beneficial for treatment of type 2
diabetes (Jung et al., 2006).
Some plants having hypoglycemic activity (Grover, 2002; Srinivasa, 2005)
Plant Plant Part Type of Test Sample Trigonella foenum-gracecum seed Alcohol ,water extract Nephoelepsis tuberose bulb juice Costus specious rhizome juice Plantago ovata husk Powder Allium sativum bulb juice Hemidesmus indicus root alcoholic extract Allium cepa bulb juice
Plants with anticancer activity
Cancer, a major public health problem worldwide, is a group of diseases
characterized by uncontrolled growth and spread of abnormal cells. It affects all people,
the young and old, the rich and poor, men, women and children. Cancer is one of the
leading causes of death in the world and its incidence is still increasing, particularly in
developing countries. It is the second leading cause of death in developed countries, and is
among the three leading causes of death for adults in developing countries (Parkin et al.,
2001). External factors such as tobacco, chemicals, radiation, infectious organisms and
internal factors such as inherited mutations, hormones and immune status can be able to
cause cancer. These risk factors may act together or in sequence to initiate or promote
carcinogenesis (American Cancer Society, 2005). Many different types of chemical

29
exposures can increase the incidence of tumors in humans (Wogan et al., 2004). The only
types of radiation proven to cause human cancer are high-frequency ionizing radiation and
ultraviolet radiation. Exposure to sunlight causes almost all cases of basal and squamous
cell skin cancer and is a major cause of skin melanoma (Moan et al., 2008). Cancers
triggered by infections are more prevalent in the developing world. Both DNA and RNA
viruses were documented as a causative factor of experimental carcinogenesis (Shillitoe,
1991). More than 100 oncogenes have been identified to date, and many among them have
been implicated in carcinogenesis, including ras, c-myc, erb-B2 and epidermal growth
factor receptor (Duesberg and Liu, 2003; Carbone and Pass, 2004). Cancer can be treated
by surgery, radiation therapy, chemotherapy and immunotherapy. Cancers that are most
often cured are breast, cervix, prostate, oral, colon and skin, if they are diagnosed early.
Improving the quality of life of patients living with cancer and dying from cancer is
therefore an urgent humanitarian need. Indian sub-continent is rich in its diversity of flora,
being a tropical country with a large spread of rain forests and river basins. It is
floristically rich with about 33 percent of its botanical wealth (over 15,000 species of
higher plants) being endemic. Numerous bioactive compounds have been isolated from
plant sources and several of them are currently in clinical trials. Plant-derived compounds
have been a vital source of varied clinically useful anti-cancer agents: Camptothecin
derivatives (Kepler et al., 1969), Topotecan and Irinotecan, Etoposide, derived from
Epipodophyllotoxin (Utsugi et al., 1996), and Paclitaxel (taxol) (Cragg and Newman,
2005). Furthermore, other potent molecules include Vinca rosea alkaloids (Vinblastine,
Vincristine) (Johnson et al., 2001), Flavopiridol, a semi-synthetic analogue of the
chromone alkaloid and Rohitkine, a pyridoindole alkaloid derived from leaves of
Ochrosia species (Arguello et al., 1998). The research on anticancer drug development is
largely dependent on exploring potential phytochemicals.
Polycyclic aromatic hydrocarbons (PAHs) are products formed by incomplete
combustion of organic matter. Sources of PAHs include industrial and domestic oil
furnaces, gasoline, and diesel engines. PAHs are widely distributed in our environment
and are implicated in various types of cancer. Enzymatic activation of PAH’s leads to the
generation of active oxygen species such as peroxides and superoxide anion radicals,
30
which induce oxidative stress in the form of lipid peroxidation. The PAH 7,12-dimethyl-
benz(a)anthracene (DMBA) acts as a potent carcinogen by generating various reactive
metabolic intermediates leading to oxidative stress. It is therefore imperative to search
alternative drugs for the treatment of liver disease to replace the currently used drugs of
doubtful efficacy and safety (Bishayee et al., 2000). Most tumor initiating agents either
generate or are metabolically converted to electrophilic reactants which bind covalently to
cellular DNA (Slaga et al., 1987; DiGiovannio, 1992). For a number of PAH's, including
DMBA the ultimate carcinogen is so called Bay-region dihydrodiol epoxide, produced
during cellular metabolism (Harry, 2001). Free radicals and these modified DNA bases
have been strongly implicated in carcinogenesis in general (Floyd, 1990; Mollins, 1993).
A high correlation has been found to occur between the dose of administered DMBA and
the levels of total DNA adducts in liver and target organ epithelial cells. Presumably this
is due to the fact that liver cells have a greater capacity of metabolizing PAHs, as
compared with the target cells for tumorigenicity, which become more readily saturated
(Izzotti et al., 1999). DMBA is the most well known polycyclic aromatic hydrocarbon that
is used as a chemical inductor of model mammary carcinogenesis (Huggins et al., 1961).
The main advantage of using DMBA as chemical carcinogen in rodent model is that it
closely mimics human breast disease. Both of these cancers arise from ductal epithelial
cells. Histopathological characterization of DMBA-induced mammary hyperplastic,
premalignant and malignant lesions shows that rat mammary adenocarcinomas and the
most common human breast carcinomas share several histological and morphological
similarities (Costa et al., 2002).
Chemical carcinogen like DMBA binds with DNA which is considered to be
essential for its tumor inducing ability. Inhibitory effect of any chemopreventive agent
against DMBA induced tumorigenesis correlates with decreased binding of DMBA to
DNA. Cell proliferation has important role in carcinogenesis as cancer proceeds through
inactivation of negative regulators of cell proliferation and activation of positive regulators
of cell proliferation (Coleman and Tsongalis, 2006). Toxic manifestation of DMBA is
associated with its oxidative metabolism leading to the formation of reactive metabolites
(epoxides and quinines) capable of generating free radicals. Metabolism of PAHs like
31
7,12-dimethyl benz(a)anthracene by the mixed function oxidases system (MFO) often
results in the formation of oxy-radicals “O2−, 1O2, H2O2, OH,” which bind covalently to
nucleophillic sites on cellular macromolecules thereby eliciting cancerous responses (Giri
et al., 1995). Oxidative stress induced due to the generation of free radicals and/or
decreased antioxidant level in the target cells and tissues has been suggested to play an
important role in carcinogenesis (Huang et al., 1999). Increased incidence of oxidative
stress and lipid peroxidation are implicated in carcinogenic processes (Khanzode
Khanzode 2004).
Cancer cachexia is a common clinical problem that substantially impacts upon the
quality of life and survival of cancer patients. The pathophysiology of this syndrome
implicates tumour induced metabolic changes and immune response. Clinical
manifestations include anorexia, chronic nausea and change in body image. (Nayak,
2002). Vinblastine isolated from the Catharanthus rosesus (Farnsworth and Blowster,
1967) is used for the treatment of Hodgkins, choriocarcinoma, non-hodgkins lymphomas,
leukemia in children, testicular and neck cancer. Vincristine is recommended for acute
lymphocytic leukemia in childhood advanced stages of hodgkins, lymophosarcoma, small
cell lung, cervical and breast cancer (Farnsworth and Bingel, 1977). Among several
potential benefits of ayurvedic medicine, relief from cancer cachexia is the most valuable.
Herbs used in cancer therapy provide not only total healing, but also reduces the side
effects and cancer associated complications. It also avoids the need for supplemental
therapy to manage cancer. Each herbal product contains multiple active principles that
may operate synergistically, producing therapeutic benefits and lowering the risks on
adverse effects. The anorexia or weight loss could be effectively managed by Withania
somnifera, Sida cordifolia, Asparagu sracemosa, Vitis vinifera, Plumbago zeylenica,
Tinospora cordifolia, Zingiber officinale, Coptidis rhizoma, etc. These herbs have been
shown to improve appetite, food intake, malnutrition, fatigue and sensation of well-being
which could elicit body weight gain. These herbs may even stimulate the flow of digestive
juices, thereby improving digestion and increasing the appetite. Aegle marmelos,
Holarrhena antidysenterica, Punica granatum, Cyperus rotundus, Emblica officinalis, and
Plumbago zeylanica can be used as anti-diarrhoeals when diarrhoea becomes one of the

32
complications of cancer cachexia. Terminalia chebula could be useful against chronic
constipation and digestive disorders which are common in cancer patients resulting in loss
of appetite. Eclipta prostrata, Emblica officinalis, Withania somnifera and Piper longum
can be directed to correct nausea and vomiting (Nayak, 2002). Among the above-
mentioned herbs, Withania somnifera (Agarwal et al., 1999) and Tinospora cordifolia
(Mathew, 1999) are also proven to be powerful immunostimulants, which could increase
body resistance power during cancer associated immuno suppression. The therapy
includes recommendations for lifestyle and use of specific foods and herbs which are very
helpful not only in preventing the progression of the disease but also makes the patients
feel better and comfortable in overcoming the symptoms. Allium sativum (garlic) could be
helpful to manage pain and ache. Bacopa monniera strengthens mental faculties and helps
to manage insomnia or sleeplessness due to stress (Bakhru, 2000). An herbal combination
of Withania sominifera, Asparagus racemosa, Hydrocotyle asiatica, Nardostachys
jatamamsi, Elettaria cardamomum, Tribulus terrestris, Zingiber officinalis and Eclipta
alba could also be useful in the treatment of anxiety, tension and insomnia. Ocimum
sanctum is beneficial against stress and depression during cancer. Curcuma longa,
Zingiber officinale, Glycyrrhiza glabra, Terminalia chebula, Ocimum sanctum and
Adhatoda vasica are used to control cough and shortness of breathe especially for lung
cancer patients (Nayak, 2002). Thus, ayurvedic therapeutic regimen rejuvenates the body
tissues, tones up the systems and act as a tonic to the body against cancer cachexia. This
kind of orientation toward total healing and health promotion makes approach to cancer
therapy promising.
Nutritional supplement and/or diet modification alone may not be sufficient to
control risk of mammary cancer. Thus there is a necessity to combine dietary factors/life
style factors with well known chemopreventive agents and use them in combinations for
cancer prevention. A single chemopreventive agent is unlikely to be effective for the
prevention of cancer. There is convincing evidence that the combination approach does
indeed provide greater efficacy than the administration of individual agent at higher doses.
It really holds better promise to use multiple agents that can hit multiple targets in
carcinogenesis. This particular combination chemoprevention approach is more preferred

33
because: (a) combination treatment can hit more than one critical molecular target, (b)
lower dose requirement lessening the concern of associated toxicities, and (c) acceptability
in human (Larson et al., 2004). Dietary and endogenous antioxidants prevent cellular
damage by reacting with and eliminating oxidizing free radicals. However, in cancer
treatment, a mode of action of certain chemotherapeutic agents involves the generation of
free radicals to cause cellular damage and necrosis of malignant cells. So a concern has
logically developed as to whether exogenous antioxidant compounds taken concurrently
during chemotherapy could reduce the beneficial effect of chemotherapy on malignant
cells. The importance of this concern is underlined by a recent study which estimates 23
percent of cancer patients take antioxidants (VandeCreek et al., 1999). The study of
antioxidant use in cancer treatment is a rapidly evolving area. Antioxidants have been
extensively studied for their ability to prevent cancer in humans (Singh and Lippman,
1998). It was suggested that antioxidants might interfere with the oxidative mechanisms of
alkylating agents (Labriola and Livingston, 1999). Antioxidants have been shown to
increase cell death by this mechanism (Chinery et al., 1997; Mediavilla et al., 1999).
34
List of herbs commonly used in cancer treatment
No. Name of the herb Method and use
1 Vitis vinifera The mixture of Terminalia chebula, grape juice and
sugar cane juice has been used (Hartwell, 1969).
Resveratrol, a natural product derivative from grape
juice has been proved to possess cancer
chemopreventive activity (Jang, 1997).
2 Baliospermum montanum The paste comprising of Baliospermum montanum,
Plumbago zeylanica, Euphorbia neriifolia, Calotropis
procera, jaggery, Semecarpus anacardium applied
over the tumours (Bhishagratha, 1991).
3 Moringa oleifera The paste of Moringa oleifera seeds, Solanum
xanthocarpum, Sinapis dichotoma, Holarrhena
antidysenterica and Nerium odorum roots prepared
with buttermilk is used for arbuda tumours (Murthy.
2001).
4 Ficus bengalensis Application of mixture of Ficus bengalensis and
Saussurea lappa pacify tumour growth on bone
(Murthy, 2001).
5 Curcuma domestica The Curcuma domestica powder in combination with
Symplocos racemosa, Soymida
febrifuga, is mixed with honey and this is used as an
external remedy (Murthy, 2001).

35
Bridelia retusa Spreng.
Plant Description
Bridelia species belong to the family Euphorbiaceae, and comprise approximately
60-70 species distributed in Asia, Africa and Australia. Chemical and pharmacological
studies of Bridelia species have resulted in the identification of flavonoids, sesquiterpenes,
triterpenoids, and phenolic compounds, as well as a wide variety of biological activities
including antiamebic, antianemic, antibacterial, anticonvulsant, anti-diabetic,
antidiarrhoeal, antihelmintic, anti-inflammatory, antimalarial, antinociceptive, antiviral,
and hypoglycemic activities (Ngueyem et al., 2009; Khiev et al., 2010).
Bridelia retusa Spreng (Bridelia airyshawii) is a moderate sized tree or a shrub
belonging to Euphorbiaceae family growing up to 18-20 meters in height with conical
spines 7 cm long when young. Bridelia retusa (airyshawii) commonly known as Asana,

36
Kasai or Khaja is a shrub, found to be distributed through out the hotter parts of India. The
tree is dioceious with leaves 7.5- 15 cm long, simple, alternate, ovate, elliptic or oblong
acute or acuminate, pubescent and with prominent veins, and are used as fodder. Stem is
armed and the dark grey bark is used for tanning (Tatiya et al., 2011 and Shahid et al.,
2009). The flowers are greenish yellow in color with lateral appearing from May to July
(Jain S. K., Pal D. C. 1982). Flowers are in axillary spikes, small and unisexual (Shahid et
al., 2009). Fruits drupes, 5 mm in diameter, and edible, purple black in color and contains
a single, 5 mm in diameter, reddish brown seed. Fruit ripens in December to January (Jain
and Pal, 1982). The seeds have brownish papery testa and 1 or 2 seeds with fairly thick
bony shells.
Synonyms and classification (Jain and Pal, 1981; Trease and Evans, 2008)
Synonyms Classification
Hindi Khaja Kingdom Plant
Kannada
Malayalam
Asana
Kukaryim
Division
Phylum
Angiosperms
Dicotelydon
Marathi
Sanskrit
Tamil
Telugu
Kantakauchi
Mahavira
Mulluvengai
Bontayegi
Subclass
Order
Family
Archichlamydae
Geraniales
Euphorbeaceae

37
Habitat and Ecology
The species are found growing throughout India; in Southeast Asia usually have
primary and secondary forest vegetation either as big trees or as smaller trees or shrubs. It
is found to be growing throughout India up to an altitude of 1,000 m except in very dry
regions (Banerjee and Kulkarni, 2009), in Himalayas from Nepal to the hills of Assam,
Meghalaya, Manipur, Arunachal Pradesh, and also in South-India and Sri Lanka (Tatiya et
al., 2011; Shahid et al., 2009).
Medicinal Properties
Various plants from this family have been investigated for their medicinal
properties. B. retusa and B. ferruginea are known to contain compounds that possess
antifungal and anti-inflammatory properties (Jayasinghe et al., 2003; Olajide et al., 2003).
The roots and bark of Bridelia species have been used for the treatment of headache,
abnormal pain, indigestion, astringent, and purgative (Mostafa et al., 2006). Previous
studies on Bridelia species have reported the occurrence of sesquiterpenes, megastigmane
glucosides in B. glauca (Sueyoshi et al., 2006), flavonoids in B. ferruginea and B.
tomemtosa (Addae-Mensah and Achenbach, 1985; Hui, et al., 2006), phenolic derivatives
in B. ferruginea B. retusa and B. ndellensis (Cimanga et al., 1999; Jayasinghe et al., 2003;
Mostafa et al., 2006), and triterpenoids in B. monoica, B. tomemtosa and B. ovata (Hui
and Fung, 1968; Boonyaratavej, 1990; Boonyaratavej et al., 1992) as the chemical
constituents, as well as biological activities including snake venom phosphodiesterase-I
inhibitory (Mostafa et al., 2006), antibacterial (Ramesh et al., 2001), and antifungal
(Jayasinghe et al., 2003) activities. The LD50 of the B. retusa (EE4965000) administered
by i.p. was observed as 1 gm/kg when investigated in mice (CSIR, 1971).
Plant pacifies vitiated vata, pitta, diarrhea, dysentery, hemorrhoids, hemorrhage,
menorrhagia, leucorrhea, arthritis, diabetes, wounds, ulcers and poison. Plant also has
contraceptive action. Decoction of stem bark with country liquor is used for diarrhea, ear
38
ache and prevents pregnancy. Extract from the stem bark has antiviral, anticancer and
hypotensive properties. Paste of the stem bark is applied to wounds and bark juice taken
internally in case of snake bite (Joshi, 2006). Bridelia retusa is used in the indigenous
system of medicine for treatment of rheumatism and as an astringent and it also pacifies
vitiated vata, pitta, diarrhea, dysentery, hemorrhoids, hemorrhage, menorrhagia,
leucorrhea, arthritis, diabetes, wounds, ulcers and poison (Shahid et al., 2009). A survey
of ethno medicinal records revealed that the bark is pungent, bitter, heating; useful in
‘vata’ lumbago, hemiplegia. The bark is good for the removal of urinary concretions .The
root and the barks are valuable astringents. The bark is used as a liniment with gingerly oil
in rheumatism (Banerjee and Kulkarni, 2009). The bark extract is used by the tribal to
develop sterility and it is used as a contraceptive. One or two drops of fruit extract are
poured in ear to cure earache (Tatiya et al., 2011). Bark is a valuable astringent and used
in the form of a liniment in rheumatism. It exhibited antiviral, hypoglycemic, hypotensive,
antifertility activity and removal of urinary concretions properties in pharmacological
trials. It is reported as anti inflammatory activity in animal model (Mehare and Hatapakki,
2003; Tatiya et al., 2011). Earlier work was reported for wound healing activity on leaves
of Bridelia retusa (Udegbunam et al., 2011).
Phytochemical analysis has revealed the presence of steroids, triterpenoids, tannins
and flavonoids as major constituents by Tatiya et al. (2011). The presence
phytoconstituents reported by Banerjee and Kulkarni (2009) includes steroids,
carbohydrates, flavanoids, tannins, phenols, glycosides triterpenoids and saponins while
absence of alkaloids, reducing sugar, proteins, amino acids, gums and resins were
detected. The bark of Bridelia retusa was screened for estimation of phytochemical
standards like: phenolic, flavonoid, tannins, carbohydrates and mucilage content. In
addition to its acetone fraction i.e. tannins rich fraction, were also subjected to in vitro
antioxidant activity using standard procedures. The effects of extracts of Bridelia
ferruginea on Bacillus subtilis, Eschericia coli, Staphylococcus aureus, Aspergillus niger
and Fusarium solani were examined and the results revealed that methanol extract was the
most effective on Bacillus substilis and Escherichial coli while ethanol extract was most
effective on Staphylococcus aureus. In the fungal isolates the ethanol extracts had the

39
highest growth inhibition though the values obtained were considerably lower than those
of the control experiments (Jose and Kayode, 2009).
Phytochemical standards analysis of B. retusa revealed the presence of bioactive
components comprising phenolics (2.92-3 g of GAE/100 g of dry sample), total tannins
(33-43 % w/w as tannic acid equivalence), proanthocyanidin content (2.98-4 % w/w as
catechin equivalent), ellagic acid (0.135 % w/w), mucilage (3-4 % w/w), flavonoids (257
mg of Rutin equivalence/100 g dry plant) and carbohydrates (7 – 7.1g /100g of plant). The
acetone exhibited IC50 values of 47.20, 110.76, 48.81 44.15 and 50.42 μg/ml, respectively
in DPPH (1,1 Diphenyl-2-picryl-hydrazyl free radical scavenging activity), ALP (anti-
lipid peroxidation effect), hydroxyl, hydrogen peroxide and nitric oxide radical inhibition
assays while acetone had effective reducing power. The results showed that tannins rich
fractions of bark had strong antioxidant activity by inhibiting DPPH, ALP, reducing
power, hydroxyl radical and hydrogen peroxide and nitric oxide scavenging. These results
suggest strong antioxidant potentials of the acetone extracts of Bridelia retusa. These
bioactive compounds may be responsible for antioxidant properties of B.retusa that form
the basis of their use in herbal medicine in India (Tatiya and Saluja, 2010).
Extract of Bridelia retusa leaves was investigated as corrosion inhibitor of mild
steel in 1 N H2SO4 using conventional weight loss, electrochemical polarizations,
electrochemical impedance spectroscopy and scanning electron microscopic studies. The
weight loss showed that the extract of Bridelia retusa leaves had excellent corrosion
inhibitor and electrochemical polarizations data revealed the mixed mode of inhibition.
While the results of electrochemical impedance spectroscopy showed that the change in
the impedance parameters, charge transfer resistance and double layer capacitance, with
the change in concentration of the extract was due to the adsorption of active molecules
leading to the formation of a protective layer on the surface of mild steel. Scanning
electron microscopic studies provided the confirmatory evidence of improved surface
condition, due to the adsorption, for the corrosion protection (Patel et al., 2010).

40
List of antifugal sesquiterpenes reported from B. retusa (Jayasingh et al., 2003).
In certain studies carried out using aqueous and alcohol extracts of the bark of
Bridelia retusa (Linn.) Spreng (Euphorbiaceae) were investigated for acute anti-
inflammatory activity in carrageenan-induced rat paw oedema. Both the extracts exhibited
significant dose-dependent inhibition of rat paw oedema in dose of 50 mg/kg, orally and
100 mg/kg, orally, when compared to control group. The activity was compared with a
standard drug, diclofenac (15 mg/kg, orally) sodium (Mehare and Hatapakki, 2003).
Wound healing property of B. ferruginnea has been reported with significantly enhanced
41
wound contraction and epithelization (Udegbunam et al., 2011). Aqueous and alcoholic
extracts of its bark were investigated earlier for acute antiinflammatory activity in
carrageenan-induced rat paw oedema (Tatiya et al., 2011).
Antifertility activity of previous investigation of ethyl acetate and methanol
extracts of Aegle marmelos and Bridelia retusa and isolation of alkaloids from A.
marmelos and fatty acids and flavonoid from B. retusa (Gurulingappa, 2002, 2005, 2009).
In the type 2 diabetic model rats, the ethanol extract of stem bark of Bridelia ndellensis
showed an anytihyperglycemic effect comparable to that of glibenclamide when fed
simultaneously with glucose (Sokeng et al., 2005). The results of this study suggest that
Bridelia ferruginea bark extract achieved a reduction in plasma glucose levels especially
in glucose induced hyperglycemic rats. This implies that the methanol extract has anti-
diabetic properties and may thus be useful in the management and treatment of diabetes
mellitus (Kolawole et al., 2006). The methanolic stem bark extract of B. grandis, has
hypoglycaemic effects in type 2 diabetic mice (Njamen et al., 2011). The ethanolic
extracts of six plants including Bridelia ovate showed cytotoxic activity against lung and
prostate cancer cell lines (Saetung et al., 2005). B. cambodiana Gagnep. methanolic
extract was found to be cytotoxic against HL-60 cell line (Khiev et al., 2009).
In Pharmacological trials the bark of Bridelia retusa exhibited anti-viral,
hypoglycemic and hypotensive properties. According to Ayurveda, the bark is good for
removal of urinary concretions, useful in lumbago and hemiplegia. The bark is used as
liniment with gingelly oil in rheumatism (Kirtikar and Basu, 1999). The bark is
documented to be used ethno botanically to promote antifertility. The presence of
triterpene ketone (4- desmethyl eupha 7, 24 (28) - diene-3-one) in the bark has been
reported and also contains 16-40% of tannins (Chopra and Nayer, 1992). Phenolics
including tannins are the natural products present in abundant amount and possess various
biological properties related to antioxidant mechanisms (Christel et al., 2000). The bark of
B. retusa exhibited variations in their contents of phytoconstituents depending upon the
geographical location from where they were collected which was evident and supported
from their extractive values and total polyphenol content. The methanolic extract of the

42
plant collected from Maharashtra and Andhra Pradesh regions and the plant collected from
the region of Maharashtra was found to be superior with respect to extraction yield and
radical scavenging activity. These differences may possibly be related to the natural
climatic differences which occur over a particular geographical area to be influenced by
several climatic factors (Banerjee and Bonde, 2011). Therefore, the need to investigate the
pharmacological properties of this plant becomes necessary Hence, the present
investigation was undertaken to elucidate phytochemical and pharmacological
investigation of stem bark extract of Bridelia retusa S. with emphasis on qualitative
phytochemical screening, antimicrobial, antihelminthic, invivo antioxidant,
hepatoprotective, nephroprotective, antidiabetic and anticancer activity of the stem bark
extracts.
Related Documents