DOI 10.1378/chest.109.6.1514 1996;109;1514-1519 Chest Alfredo Perez-Romo Arroliga, Antonio Padua, Arnulfo Portales, Alejandro Villarreal and Ruben Delgado, Raul Cicero, Carlos Ibarra-Perez, Alejandro C. Carlos Jerjes-Sánchez, Alicia Ramirez-Rivera, Jose J. Elizalde, in Hemothorax and Empyema Treatment Streptokinase as an Adjunctive Intrapleural Fibrinolysis With http://chestjournal.chestpubs.org/content/109/6/1514 and services can be found online on the World Wide Web at: The online version of this article, along with updated information ISSN:0012-3692 ) http://chestjournal.chestpubs.org/site/misc/reprints.xhtml ( without the prior written permission of the copyright holder. No part of this article or PDF may be reproduced or distributed 3300 Dundee Road, Northbrook, IL 60062. All rights reserved. Copyright1996by the American College of Chest Physicians, Physicians. It has been published monthly since 1935. is the official journal of the American College of Chest Chest 1996 BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS by guest on July 26, 2011 chestjournal.chestpubs.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DOI 10.1378/chest.109.6.1514 1996;109;1514-1519Chest
Alfredo Perez-RomoArroliga, Antonio Padua, Arnulfo Portales, Alejandro Villarreal andRuben Delgado, Raul Cicero, Carlos Ibarra-Perez, Alejandro C. Carlos Jerjes-Sánchez, Alicia Ramirez-Rivera, Jose J. Elizalde, in Hemothorax and Empyema
TreatmentStreptokinase as an Adjunctive Intrapleural Fibrinolysis With
http://chestjournal.chestpubs.org/content/109/6/1514
and services can be found online on the World Wide Web at: The online version of this article, along with updated information
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
without the prior written permission of the copyright holder.No part of this article or PDF may be reproduced or distributed3300 Dundee Road, Northbrook, IL 60062. All rights reserved. Copyright1996by the American College of Chest Physicians,Physicians. It has been published monthly since 1935.
is the official journal of the American College of ChestChest
1996 BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from

Intrapleural Fibrinolysis WithStreptokinase as an AdjunctiveTreatment in Hemothorax and Empyema"A Multicenter Trial
By the Collaborative Group Investigators of Intrapleural Fibrinolysis:Carlos Jerjes-Sdnchez, MD, FCCP (Chair);Alicia Ramirez-Rivera, MD, FCCP; Jose J. Elizalde, MD, FCCP;Ruben Delgado, MD; Raul Cicero, MD, FCCP;Carlos Ibarra-Perez, MD, FCCP; Alejandro C. Arroliga, MD, FCCP;Antonio Padua, MD; Arnulfo Portales, MD; Alejandro Villarreal, MD;and Alfredo Perez-Romo, MD
To test the efficacy of intrapleural fibrinolytic therapy in patients with loculated pleural effusions,we conducted an open, prospective, and multicenter trial among five hospitals in Mexico. We en¬
rolled patients with hemothorax or empyema, clotted and/or loculated, thatwas not resolved throughconventional pleural drainage with chest tube and antibiotics in patients with empyema. All patientsreceived repeated doses of 250,000 IU of streptokinase through chest tube. Effectiveness criteriawere before and after intrapleural streptokinase (IPSK) drainage, and poststreptokinase radio-graphic and respiratory function test improvement. Forty-eight patients were studied; there were
30 patients with empyemas, 14 with hemothorax, and 4 patients with malignant pleural effusionswithout lung trapping. Successful fibrinolysis was obtained in 44 patients, with complete resolutionof the pleural collection and adequate radiologic and spirometric improvement. In three of fourpatients with multiloculated malignant hemothorax with high-yielding pleural drainage, IPSKallowed successful lysis ofloci and an adequate pleurodesis was achieved. Onlyfour patients requiredsurgical treatment. The overall success rate in our series was 92%, similar to previous reports. Theresults in this first prospective and multicentric trial suggest that intrapleural fibrinolysis is an ef¬fective and safe adjunctive treatment in patients with heterogeneous pleural coagulated and locu¬lated collections to restore the pulmonary function assessed by respiratory function tests and can
obviate surgery in mostcases. (CHEST 1996; 109:1514-19)
Key words: empyema; hemothorax; intrapleural fibrinolysis; intrapleural streptokinase; loculated pleural effusion
Abbreviation: IPSK=intrapleural streptokinase
r|1he treatment of choice of proteinaceous pleural-*- space collections, whether hemorrhagic or puru¬lent, is pleural drainage. Evacuation alone with simple*From the Hospital de Cardiologia, Centro Medico Nacional (Dr.Jerjes-Sanchez), Hospital General de Mexico, SSA (Drs. Ramirez-Rivera, Delgado, Cicero, and Perez-Romo), Hospital AmericanBritish Cowdray (Dr. Elizalde), Hospital de Oncologia, CentroMedico Nacional (Dr. Ibarra-Perez), Cleveland Clinic Foundation(Dr. Arroliga), and Hospital de Especialidades 71, IMSS, Torreon,Coahuila (Drs Padua, Portales, and Villarreal).'Dr. Jerjes-Sanchez is now Head of the Emergency Care Depart¬ment and Dr. Ramirez-Rivera is now Clinical Research Coordi¬nator of the Respiratory Care Department, Hospital de Cardiolo¬gia, Neumologia y Angiologia (Especialidades 34), Monterrey,Nuevo Leon, Mexico.Manuscript received September 25, 1995; revision accepted Janu¬ary 25, 1996.Reprint requests: Dr. Jerjes-Sdnchez, Paseo de los Descubridores209, Cumbres 3er Sector, CP 64190, Monterrey NL, Mexico
closed thoracotomy, adequate management of chesttube, and antibiotics when indicated are often enoughin early stages to restore pulmonary function and pre¬vent long-term pleural fibrosis and lung entrapment.In late stages, decortication is usually performed. As an
alternative to surgical aggressive therapy, intrapleuralfibrinolysis has been used with favorable results.1"11This conservative medical treatment may reduce mor¬
bidity secondary to surgical procedures and may resultin significant medical cost savings.4We are reporting a multicenter trial with 48 con¬
secutive patients with loculated hemothorax and em¬
pyema in whom intrapleural streptokinase (IPSK) was
used as an adjunctive treatment after failure of chesttube drainage.
1514 Clinical Investigations
1996 BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from

Materials and Methods
Primary End Point
To evaluate the role of intrapleural fibrinolysis in clotted or loc¬ulated pleural collections, and to investigate if major surgical pro¬cedures can be avoided, a prospective, open, and multicenter trialwas carried out in five hospitals in Mexico.
Inclusion and Exclusion Criteria
Patients were included if they had clotted hemothorax or locu¬lated empyema, or malignant loculated pleural effusion withoutlung trapping that did not resolve after pleural drainage with closedthoracotomy. Patients were also included if they had empyema or
hemothorax that developed within 30 days or loculated effusion.Patients with empyema or hemothorax after pneumonectomy, prioror present bronchopleural fistula, or who were in the first 48 hpostsurgery or following trauma were not included. Consent was
obtained from the patients, and the protocol was approved by theethics committee of the Hospital General de Mexico.
Therapeutic RegimenStreptokinase, 250,000 IU, was diluted in 100 mL of saline solu¬
tion and administered through a chest tube. The chest tube was
clamped for 4 h, and patients were rotated in several positions toallow a better distribution of IPSK. After the 4 h, the clamp was
removed and the drained material was measured subtracting theinjected volume. The procedure was repeated every day untilradiographic improvement was achieved or until pleural drainagewas less than 100 mL in 24 h. At that time, the chest tube was re¬
moved.
Criteria for EffectivenessWe quantified the amount of pleural drainage. The radiologic
improvement after administration of IPSK was quantified. Thecriteria for improvement were defined as follows: maximum (nor¬mal or near-normal chest radiograph); moderate (a clearance of 50to 80% of pleural opacities); minimal (<50% of clearance of pleu¬ral opacities); or none (no change). Other criteria for effectivenesswere the radiologic appearance at 2, 6, and 9 weeks after the lastdose of IPSK and spirometry at 2 and 6 weeks after the last doseof IPSK.
All patients had determination of coagulation parameters, liverfunction tests, and creatinine before and after IPSK.
Statistical AnalysisStudent's t test and analysis of variance were used. All data are
expressed as mean±SD.
Results
From October 1993 to April 1995, 49 consecutivepatients were enrolled. One patient with chronic renalfailure and empyema was excluded owing to bron¬chopleural fistula on the second day of IPSK. The re¬
maining 48 patients represent the basis of our report.Patients' demographic data, etiology, pleural drain¬
age, number of loci, length of treatment, and compli¬cations are depicted in Table 1. Regarding pleuralspace management, in cases of empyema (30/48), di¬agnosis was supported by aspiration of frank pus, pHless than 7.0, and pleural glucose levels less than 40mg/dL. All patients were receiving antibiotic therapy atthe time of drainage by chest tube. Antibiotic choicewas initially empiric but was modified on the basis of
Table 1.Characteristics of 48 Patients With IPSK
Variable Patients
Age, 15-79 yr 43.88±14.06Gender, F/M 11/37Right-side effusion 24/48Left-side 24/48
EtiologyEmpyema 30/48
Postpneumonic 15Infected hemothorax 11Infected transudate 2
Sterile hemothorax 14/48Traumatic 12Iatrogenic 2
Malignant hemothorax 4/48Breast adenocarcinoma 2
Bronchogenic carcinoma 2Loculated effusions 30/48
No. of loci (2 to 9) 3.50+1.63Interval between diagnosis and SK*
2 to 30 d 11.65±8.31Time without drainage
1 to 14 d 3.0+2.50Daily drainage in benign effusions (44 patients)Pre-SK (0-70 mL) 26.44±16.941st day post-SK (50-1,100 mL) 380.67±204.07
Required doses of SK2 to 10 5.10±1.99
ComplicationsPleuritic pain 3/48Transient neurologic signs 2/48Low-grade fever 2/48Rash 1/48Hemorrhage 0/48
Successful fibrinolysis 44/48
*SK=streptokinase.
subsequent pleural fluid culture results (Table 2). Inthree patients, the causal agent was not identified.Empyema was considered coagulated or loculatedwhen the chest tube failed to drain pleural fluid, andopacities on chest radiography persisted and/or were
demonstrated through chest CT. In sterile nonmalig-Table 2.Pleural Fluid Culture Results
Microorganism No. of Cases
Bacteroides spStaphylococcus aureus
Pseudomonas aeruginosaBacteroides fragilisStreptococcus pneumoniaeKlebsiella pneumoniaeKlebsiella spPeptostreptococcusEnterobacter aerogenesEnterobacter spStreptococcus viridansEscherichia coliFusobacterium plus S pneumoniaeMycobacterium tuberculosis plus S viridansAspergillus fumigatus plus P aeruginosaTotal 27
CHEST/109/6/JUNE, 1996 1515
1996 BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from
600, .ml
500J SK * p < 0-001
400. TI 1
iilllllliU01 23456 789 10
days
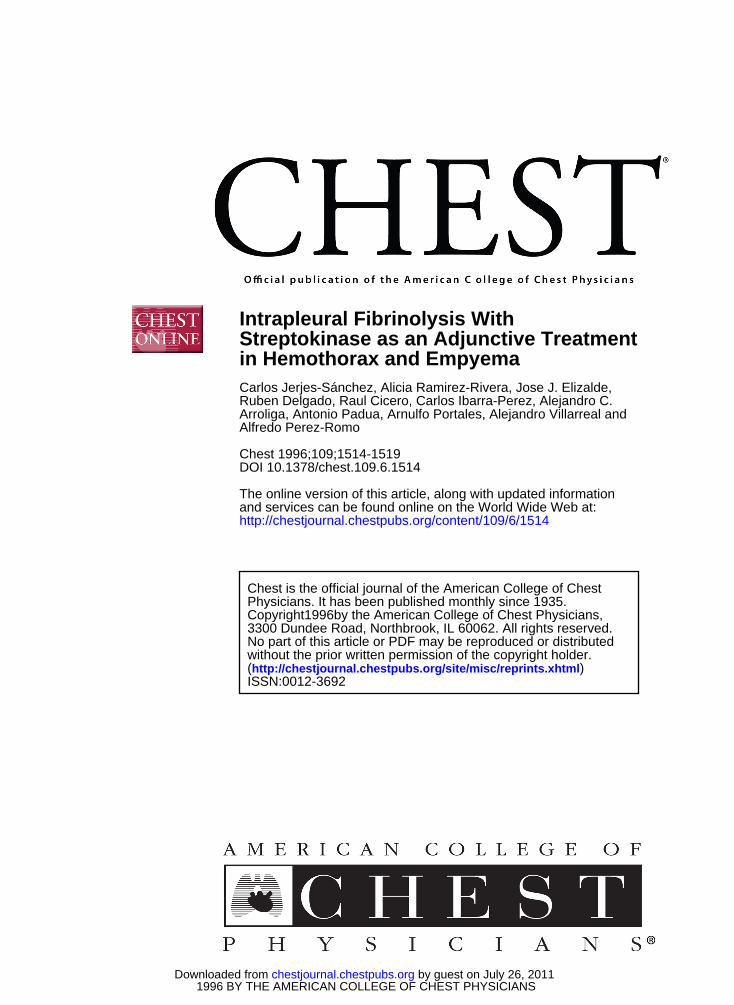
Figure 1. Volume of pleural drainage. Figure shows pleuraldrainage ofnearly zero obtained before IPSK was administered, andraised notoriously from the first day of treatment until the fourthday, and then slowly decreased until the tenth day in these 44 pa¬tients.
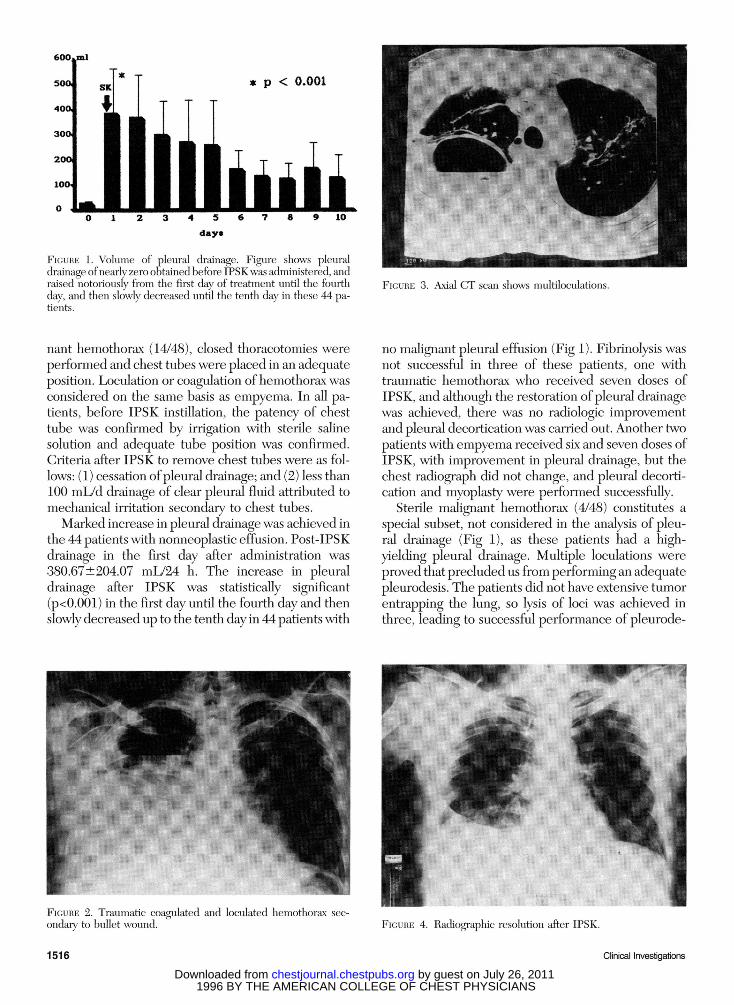
Figure 3. Axial CT scan shows multiloculations.
nant hemothorax (14/48), closed thoracotomies were
performed and chest tubes were placed in an adequateposition. Loculation or coagulation ofhemothorax wasconsidered on the same basis as empyema. In all pa¬tients, before IPSK instillation, the patency of chesttube was confirmed by irrigation with sterile salinesolution and adequate tube position was confirmed.Criteria after IPSK to remove chest tubes were as fol¬lows: (1) cessation ofpleural drainage; and (2) less than100 mL/d drainage of clear pleural fluid attributed tomechanical irritation secondary to chest tubes.Marked increase in pleural drainage was achieved in
the 44 patients with nonneoplastic effusion. Post-IPSKdrainage in the first day after administration was
380.67±204.07 mL/24 h. The increase in pleuraldrainage after IPSK was statistically significant(p<0.001) in the first day until the fourth day and thenslowly decreased up to the tenth day in 44 patients with
no malignant pleural effusion (Fig 1). Fibrinolysis wasnot successful in three of these patients, one withtraumatic hemothorax who received seven doses ofIPSK, and although the restoration of pleural drainagewas achieved, there was no radiologic improvementand pleural decortication was carried out. Another twopatients with empyema received six and seven doses ofIPSK, with improvement in pleural drainage, but thechest radiograph did not change, and pleural decorti¬cation and myoplasty were performed successfully.
Sterile malignant hemothorax (4/48) constitutes a
special subset, not considered in the analysis of pleu¬ral drainage (Fig 1), as these patients had a high-yielding pleural drainage. Multiple loculations were
proved that precluded us from performing an adequatepleurodesis. The patients did not have extensive tumorentrapping the lung, so lysis of loci was achieved inthree, leading to successful performance of pleurode-
Figure 2. Traumatic coagulated and loculated hemothorax sec¬
ondary to bullet wound. Figure 4. Radiographic resolution after IPSK.
1516 Clinical Investigations
1996 BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from
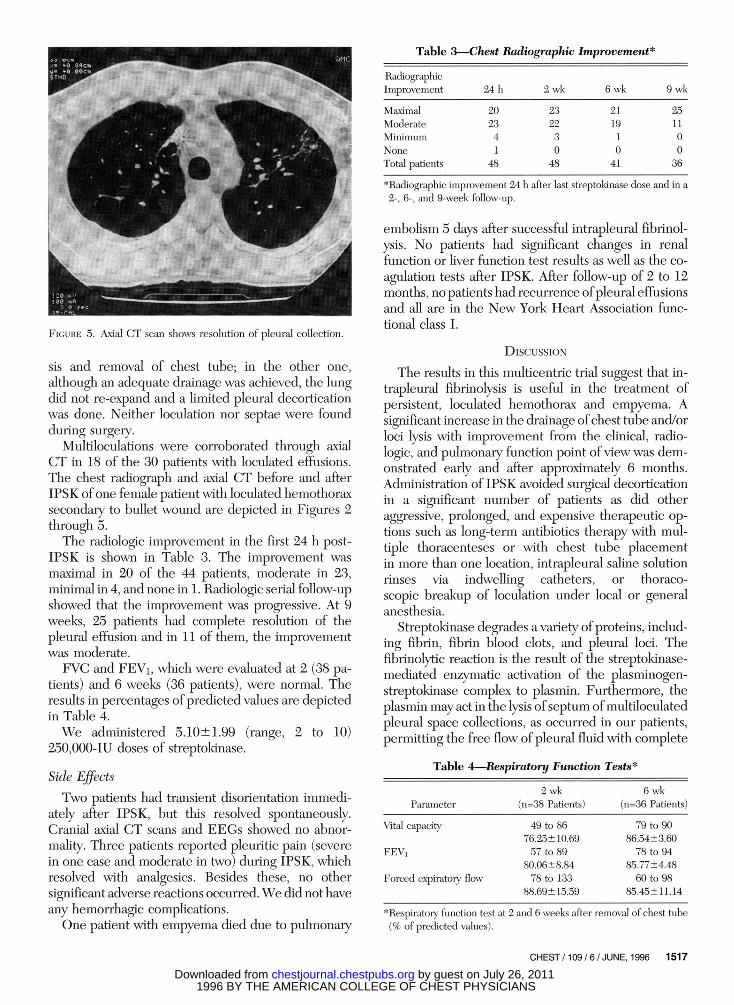
Table 3.Chest Radiographic Improvement*
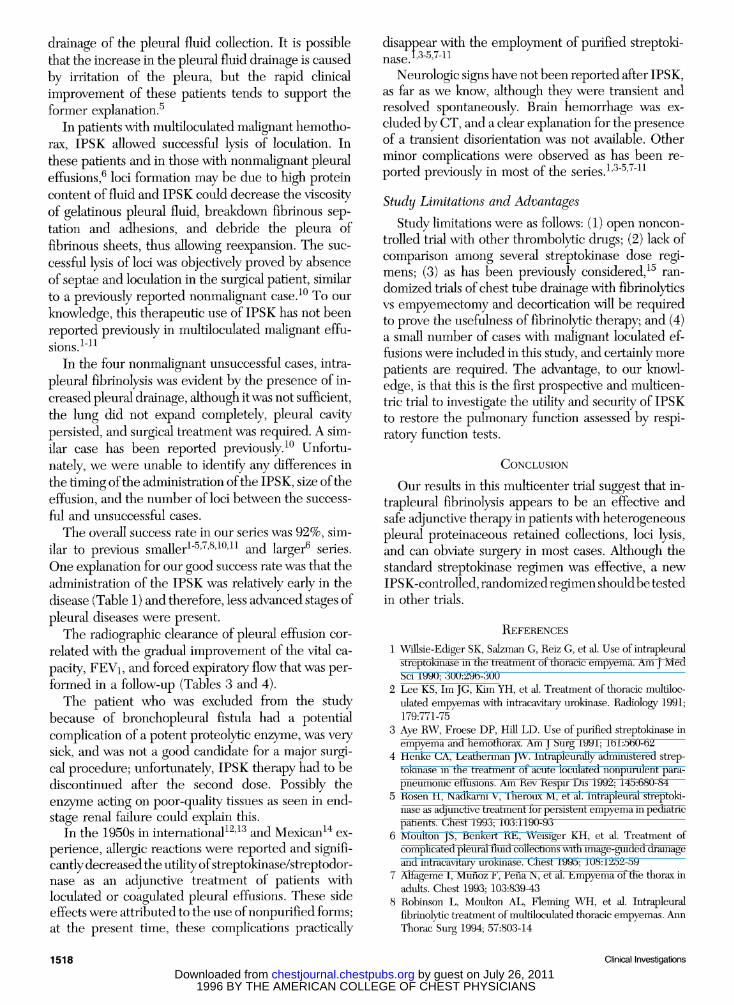
Figure 5. Axial CT scan shows resolution of pleural collection.
sis and removal of chest tube; in the other one,although an adequate drainage was achieved, the lungdid not re-expand and a limited pleural decorticationwas done. Neither loculation nor septae were foundduring surgery.
Multiloculations were corroborated through axialCT in 18 of the 30 patients with loculated effusions.The chest radiograph and axial CT before and afterIPSK ofone female patient with loculated hemothoraxsecondary to bullet wound are depicted in Figures 2through 5.The radiologic improvement in the first 24 h post-
IPSK is shown in Table 3. The improvement was
maximal in 20 of the 44 patients, moderate in 23,minimal in 4, and none in 1. Radiologic serial follow-upshowed that the improvement was progressive. At 9weeks, 25 patients had complete resolution of thepleural effusion and in 11 of them, the improvementwas moderate.FVC and FEVi, which were evaluated at 2 (38 pa¬
tients) and 6 weeks (36 patients), were normal. Theresults in percentages ofpredicted values are depictedin Table 4.We administered 5.10±1.99 (range, 2 to 10)
250,000-IU doses of streptokinase.Side EffectsTwo patients had transient disorientation immedi¬
ately after IPSK, but this resolved spontaneously.Cranial axial CT scans and EEGs showed no abnor¬mality. Three patients reported pleuritic pain (severein one case and moderate in two) during IPSK, whichresolved with analgesics. Besides these, no othersignificant adverse reactions occurred. We did not haveany hemorrhagic complications.One patient with empyema died due to pulmonary
RadiographicImprovement 24 h 2 wk 6 wk 9wk
MaximalModerateMinimumNoneTotal patients
202341
48
232230
48
211910
41
251100
36
*Radiographic improvement 24 h after last streptokinase dose and in a
2-, 6-, and 9-week follow-up.
embolism 5 days after successful intrapleural fibrinol¬ysis. No patients had significant changes in renalfunction or liver function test results as well as the co¬
agulation tests after IPSK. After follow-up of 2 to 12months, no patients had recurrence ofpleural effusionsand all are in the New York Heart Association func¬tional class I.
DiscussionThe results in this multicentric trial suggest that in¬
trapleural fibrinolysis is useful in the treatment ofpersistent, loculated hemothorax and empyema. Asignificant increase in the drainage ofchest tube and/orloci lysis with improvement from the clinical, radio-logic, and pulmonary function point of view was dem¬onstrated early and after approximately 6 months.Administration of IPSK avoided surgical decorticationin a significant number of patients as did otheraggressive, prolonged, and expensive therapeutic op¬tions such as long-term antibiotics therapy with mul¬tiple thoracenteses or with chest tube placementin more than one location, intrapleural saline solutionrinses via indwelling catheters, or thoraco¬scopic breakup of loculation under local or generalanesthesia.
Streptokinase degrades a variety of proteins, includ¬ing fibrin, fibrin blood clots, and pleural loci. Thefibrinolytic reaction is the result of the streptokinase-mediated enzymatic activation of the plasminogen-streptokinase complex to plasmin. Furthermore, theplasmin may act in the lysis ofseptum of multiloculatedpleural space collections, as occurred in our patients,permitting the free flow of pleural fluid with complete
Table 4.Respiratory Function Tests*
Parameter2 wk
(n=38 Patients)6 wk
(n=36 Patients)Vital capacity
FEVi
Forced expiratory flow
49 to 8676.25 ±10.6957 to 89
80.06±8.8478 to 133
88.69± 15.59
79 to 9086.54±3.60
78 to 9485.77±4.4860 to 98
85.45+11.14
*Respiratory function test at 2 and 6 weeks after removal of chest tube(% of predicted values).
CHEST /109 / 6 / JUNE, 1996 1517
1996 BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from
drainage of the pleural fluid collection. It is possiblethat the increase in the pleural fluid drainage is causedby irritation of the pleura, but the rapid clinicalimprovement of these patients tends to support theformer explanation.5
In patients with multiloculated malignant hemotho¬rax, IPSK allowed successful lysis of loculation. Inthese patients and in those with nonmalignant pleuraleffusions,6 loci formation may be due to high proteincontent of fluid and IPSK could decrease the viscosityof gelatinous pleural fluid, breakdown fibrinous sep-tation and adhesions, and debride the pleura offibrinous sheets, thus allowing reexpansion. The suc¬
cessful lysis of loci was objectively proved by absenceof septae and loculation in the surgical patient, similarto a previously reported nonmalignant case.10 To our
knowledge, this therapeutic use of IPSK has not beenreported previously in multiloculated malignant effu¬sions. l-n
In the four nonmalignant unsuccessful cases, intra¬
pleural fibrinolysis was evident by the presence of in¬creased pleural drainage, although it was not sufficient,the lung did not expand completely, pleural cavitypersisted, and surgical treatment was required. A sim¬ilar case has been reported previously.10 Unfortu¬nately, we were unable to identify any differences inthe timing ofthe administration ofthe IPSK, size oftheeffusion, and the number of loci between the success¬
ful and unsuccessful cases.
The overall success rate in our series was 92%, sim¬ilar to previous smaller1"5'7'8'10'11 and larger6 series.One explanation for our good success rate was that theadministration of the IPSK was relatively early in thedisease (Table 1) and therefore, less advanced stages ofpleural diseases were present.The radiographic clearance of pleural effusion cor¬
related with the gradual improvement of the vital ca¬
pacity, FEVi, and forced expiratory flow that was per¬formed in a follow-up (Tables 3 and 4).The patient who was excluded from the study
because of bronchopleural fistula had a potentialcomplication of a potent proteolytic enzyme, was verysick, and was not a good candidate for a major surgi¬cal procedure; unfortunately, IPSK therapy had to bediscontinued after the second dose. Possibly theenzyme acting on poor-quality tissues as seen in end-stage renal failure could explain this.
In the 1950s in international12'13 and Mexican14 ex¬
perience, allergic reactions were reported and signifi¬cantly decreased the utility ofstreptokinase/streptodor-nase as an adjunctive treatment of patients withloculated or coagulated pleural effusions. These sideeffects were attributed to the use ofnonpurified forms;at the present time, these complications practically
disappear with the employment of purified Streptoki¬nase. i'3"5'7"11
Neurologic signs have not been reported after IPSK,as far as we know, although they were transient andresolved spontaneously. Brain hemorrhage was ex¬
cluded by CT, and a clear explanation for the presenceof a transient disorientation was not available. Otherminor complications were observed as has been re¬
ported previously in most of the series.1,3"5'7"11
Study Limitations and AdvantagesStudy limitations were as follows: (1) open noncon-
trolled trial with other thrombolytic drugs; (2) lack ofcomparison among several streptokinase dose regi¬mens; (3) as has been previously considered,15 ran¬
domized trials of chest tube drainage with fibrinolyticsvs empyemectomy and decortication will be requiredto prove the usefulness of fibrinolytic therapy; and (4)a small number of cases with malignant loculated ef¬fusions were included in this study, and certainly morepatients are required. The advantage, to our knowl¬edge, is that this is the first prospective and multicen-tric trial to investigate the utility and security of IPSKto restore the pulmonary function assessed by respi¬ratory function tests.
ConclusionOur results in this multicenter trial suggest that in¬
trapleural fibrinolysis appears to be an effective andsafe adjunctive therapy in patients with heterogeneouspleural proteinaceous retained collections, loci lysis,and can obviate surgery in most cases. Although thestandard streptokinase regimen was effective, a new
IPSK-controlled, randomized regimen shouldbe testedin other trials.
References1 Willsie-Ediger SK, Salzman G, Reiz G, et al. Use of intrapleural
streptokinase in the treatment of thoracic empyema. Am J MedSci 1990; 300:296-300
2 Lee KS, Im JG, Kim YH, et al. Treatment of thoracic multiloc¬ulated empyemas with intracavitary urokinase. Radiology 1991;179:771-75
3 Aye RW, Froese DP, Hill LD. Use of purified streptokinase in
empyema and hemothorax. Am J Surg 1991; 161:560-624 Henke CA, Leatherman JW. Intrapleurally administered strep¬
tokinase in the treatment of acute loculated nonpurulent para¬pneumonic effusions. Am Rev Respir Dis 1992; 145:680-84
5 Rosen H, Nadkarni V, Theroux M, et al. Intrapleural streptoki¬nase as adjunctive treatment for persistent empyema in pediatricpatients. Chest 1993; 103:1190-93
6 Moulton JS, Benkert RE, Weisiger KH, et al. Treatment ofcomplicated pleural fluid collections with image-guided drainageand intracavitary urokinase. Chest 1995; 108:1252-59
7 Alfageme I, Munoz F, Peria N, et al. Empyema of the thorax inadults. Chest 1993; 103:839-43
8 Robinson L, Moulton AL, Fleming WH, et al. Intrapleuralfibrinolytic treatment of multiloculated thoracic empyemas. AnnThorac Surg 1994; 57:803-14
1518 Clinical Investigations
1996 BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from
9 Fraedrich G, Hofmann D, Effenhauser P, et al. Instillation of fi-brinolytics in the treatment of pleural empyema. Thorac Cardio¬vasc Surg 1982; 30:36-8
10 Taylor RFH, Rubens MB, Pearson MC, et al. Intrapleuralstreptokinase in the management of empyema. Thorax 1994;49:856-59
11 Bourus D, Shiza S, Panagou P, et al. Role of streptokinase in thetreatment of acute loculated parapneumonic pleural effusionsand empyema. Thorax 1994; 49:852-55
12 Sherry S, Tillet WS, Read T. The use of streptokinase-streptodor-
nase in the treatment of hemothorax. J Thorac Surg 1950;20:393-419
13 Tillet WS, Sherry S, Read T. The use of streptokinase-streptodor-nase in the treatment of post-pneumonic empyema. J ThoracSurg 1951; 21:275-97
14 Pacheco CR, Cicero RS. El uso de la esteptoquinasa y estrep-todornasa en el hemotorax extrapleural coagulado. Rev Med Tu¬berc y Ap Res 1951; 11:35-43
15 Sahn SA. Management ofcomplicated parapneumonic effusions.Am Rev Respir Dis 1993; 148:813-17
CHEST / 109 / 6 / JUNE, 1996 1519
1996 BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from
DOI 10.1378/chest.109.6.1514 1996;109; 1514-1519Chest
Perez-RomoAntonio Padua, Arnulfo Portales, Alejandro Villarreal and AlfredoDelgado, Raul Cicero, Carlos Ibarra-Perez, Alejandro C. Arroliga,
Carlos Jerjes-Sánchez, Alicia Ramirez-Rivera, Jose J. Elizalde, RubenTreatment in Hemothorax and Empyema
Intrapleural Fibrinolysis With Streptokinase as an Adjunctive
July 26, 2011This information is current as of
http://chestjournal.chestpubs.org/content/109/6/1514Updated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/109/6/1514#related-urlsThis article has been cited by 22 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlbe found online at: Information about reproducing this article in parts (figures, tables) or in its entirety canPermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
"Services" link to the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the
Citation Alerts
PowerPoint slide format. See any online figure for directions. articles can be downloaded for teaching purposes inCHESTFigures that appear in Images in PowerPoint format
1996 BY THE AMERICAN COLLEGE OF CHEST PHYSICIANS by guest on July 26, 2011chestjournal.chestpubs.orgDownloaded from
Related Documents











