Brief Communication Intraplaque Hemorrhage in Cardiac Allograft Vasculopathy C. Castellani 1 , A. Angelini 1 , O. J. de Boer 2 , C. M. van der Loos 2 , M. Fedrigo 1 , A. C. Frigo 1 , L. B. Meijer-Jorna 3 , X. Li 2 , H. J. P. Ploegmakers 2 , F. Tona 1 , G. Feltrin 1 , G. Gerosa 1 , M. Valente 1 , G. Thiene 1 and A. C. van der Wal 2, * 1 Department of Cardiac, Thoracic and Vascular Sciences, University of Padua, Padua, Italy 2 Department of Pathology, Academic Medical Center/ University of Amsterdam, Amsterdam, The Netherlands 3 Symbiant Pathology Expert Center, Alkmaar, The Netherlands Corresponding author: Allard C. van der Wal, [email protected] Plaque hemorrhage, inflammation and microvessel density are key determinants of plaque vulnerability in native coronary atherosclerosis (ATS). This study investigates the role of intraplaque hemorrhage (IPH) and its relation with inflammation and microvessels in cardiac allograft vasculopathy (CAV) in posttrans- planted patients. Seventy coronary plaques were obtained from 12 patients who died because of CAV. For each patient we collected both native heart and the allograft, at the time of transplantation and autopsy, respectively. Intralesion inflammation, microvessels and IPH were assessed semi-quantitatively. IPH was observed in 21/35 (60%) CAV lesions and in 8/35 (22.9%) native ATS plaques, with a strong association between fibrocellular lesions and IPH (p ¼ 0.0142). Microvessels were detected in 26/35 (74.3%) of CAV lesions with perivascular leakage as sign of endothelial damage in 18/26 (69.2%). IPH was strongly associated with microvessels (p < 0.0001). Inflammation was present in 31/35 (88.6%) of CAV lesions. CAV IPHþ lesions were characterized by presence of both fresh and old hemorrhage in 12/21 (57.1%). IPH, associated with microvessel damage and inflammation, is an important feature of CAV. Fresh and old intralesion hemorrhage suggests ongoing remodeling processes promoting the lesion progression and vulnerability. Keywords: Atherosclerosis, cardiac allograft vascul- opathy, cardiac transplantation, inflammation, intra- plaque hemorrhage, microvessels Abbreviations: AHA, American Heart Association; ATS, atherosclerosis; CAV, cardiac allograft vasculopathy; DCM, dilated cardiomyopathy; GFA, glycophorin A; ICM, ischemic cardiomyopathy; IPH, intraplaque hemorrhage; SMCs, smooth muscle cells; vWF, von Willebrand factor Received 05 July 2013, revised 11 September 2013 and accepted for publication 23 September 2013 Introduction Cardiac allograft vasculopathy (CAV) still represents the Achilles’ heel of transplant procedures, accounting for its increasing incidence in approximately 10% every year in the long-term clinical follow-up (1). CAV is recognized as a concentric thickening of the coronary artery wall due to diffuse proliferation of smooth muscle cells (SMCs) in the intima layer (neointima) (2). Its pathogenesis is complex and can be related to different risk factors (3). A tight correlation between acute rejection and the development of CAV has been extensively reported (3). However, the exact pathophysiological origin of CAV is not fully under- stood (4,5). Previous studies have shown that inflammation and oxidative stress in native coronary atherosclerosis (ATS) contribute to rapidly progressive plaque destabiliza- tion (6–8). Recently several groups have also demonstrated that intraplaque hemorrhage (IPH) is associated with the development of ATS lesions and plaque instability (9–11). Moreover, there is evidence in patients who died suddenly from acute coronary syndromes that IPH may represent a potent atherogenic stimulus both biochemically and mechanically (12). Red blood cells are rich in phospholipids and free cholesterol, and their accumulation within the plaque plays a key role in promoting lesion instability through necrotic core expansion and inflammatory cell infiltration (12–14). IPH correlates positively with both inflammation and the presence of microvessels (15). Pathological examination of unstable lesions has demonstrated that IPH is closely associated with neoangiogenesis at site of microvessel leakage (16). For the first time we had the possibility to study and compare in the same patients, CAV from explanted hearts at autopsy with native coronary ATS from hearts removed at transplantation. In this setting, the aim of our study was to investigate whether and to what extent IPH plays a role in the American Journal of Transplantation 2014; 14: 184–192 Wiley Periodicals Inc. C Copyright 2013 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/ajt.12517 184

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Brief Communication
Intraplaque Hemorrhage in CardiacAllograft Vasculopathy
C. Castellani1, A. Angelini1, O. J. de Boer2,C. M. van der Loos2, M. Fedrigo1, A. C. Frigo1,L. B. Meijer-Jorna3, X. Li2, H. J. P. Ploegmakers2,F. Tona1, G. Feltrin1, G. Gerosa1, M. Valente1,G. Thiene1 and A. C. van der Wal2,*
1Department of Cardiac, Thoracic and Vascular Sciences,University of Padua, Padua, Italy2Department of Pathology, Academic Medical Center/University of Amsterdam, Amsterdam, The Netherlands3Symbiant Pathology Expert Center, Alkmaar, TheNetherlands�Corresponding author: Allard C. van der Wal,[email protected]
Plaque hemorrhage, inflammation and microvesseldensity are key determinants of plaque vulnerabilityin native coronary atherosclerosis (ATS). This studyinvestigates the role of intraplaque hemorrhage (IPH)and its relation with inflammation and microvesselsin cardiac allograft vasculopathy (CAV) in posttrans-planted patients. Seventy coronary plaques wereobtained from 12 patients who died because of CAV.For each patient we collected both native heart and theallograft, at the time of transplantation and autopsy,respectively. Intralesion inflammation, microvesselsand IPH were assessed semi-quantitatively. IPH wasobserved in 21/35 (60%) CAV lesions and in 8/35(22.9%) native ATS plaques, with a strong associationbetween fibrocellular lesions and IPH (p¼0.0142).Microvessels were detected in 26/35 (74.3%) of CAVlesionswith perivascular leakage as sign of endothelialdamage in 18/26 (69.2%). IPH was strongly associatedwith microvessels (p< 0.0001). Inflammation waspresent in 31/35 (88.6%) of CAV lesions. CAV IPHþlesions were characterized by presence of both freshand old hemorrhage in 12/21 (57.1%). IPH, associatedwith microvessel damage and inflammation, is animportant feature of CAV. Fresh and old intralesionhemorrhage suggests ongoing remodeling processespromoting the lesion progression and vulnerability.
Keywords: Atherosclerosis, cardiac allograft vascul-opathy, cardiac transplantation, inflammation, intra-plaque hemorrhage, microvessels
Abbreviations: AHA, American Heart Association; ATS,atherosclerosis; CAV, cardiac allograft vasculopathy;DCM, dilated cardiomyopathy; GFA, glycophorin A;ICM, ischemic cardiomyopathy; IPH, intraplaquehemorrhage; SMCs, smooth muscle cells; vWF, vonWillebrand factor
Received 05 July 2013, revised 11 September 2013 andaccepted for publication 23 September 2013
Introduction
Cardiac allograft vasculopathy (CAV) still represents the
Achilles’ heel of transplant procedures, accounting for
its increasing incidence in approximately 10% every year in
the long-term clinical follow-up (1). CAV is recognized as a
concentric thickening of the coronary artery wall due to
diffuse proliferation of smooth muscle cells (SMCs) in the
intima layer (neointima) (2). Its pathogenesis is complex
and can be related to different risk factors (3). A tight
correlation between acute rejection and the development
of CAV has been extensively reported (3). However, the
exact pathophysiological origin of CAV is not fully under-
stood (4,5). Previous studies have shown that inflammation
and oxidative stress in native coronary atherosclerosis
(ATS) contribute to rapidly progressive plaque destabiliza-
tion (6–8).
Recently several groups have also demonstrated that
intraplaque hemorrhage (IPH) is associated with the
development of ATS lesions and plaque instability (9–11).
Moreover, there is evidence in patients who died suddenly
from acute coronary syndromes that IPH may represent
a potent atherogenic stimulus both biochemically and
mechanically (12).
Red blood cells are rich in phospholipids and free
cholesterol, and their accumulation within the plaque plays
a key role in promoting lesion instability through necrotic
core expansion and inflammatory cell infiltration (12–14).
IPH correlates positively with both inflammation and the
presence of microvessels (15). Pathological examination of
unstable lesions has demonstrated that IPH is closely
associated with neoangiogenesis at site of microvessel
leakage (16).
For the first time we had the possibility to study and
compare in the same patients, CAV from explanted hearts
at autopsy with native coronary ATS from hearts removed
at transplantation.
In this setting, the aim of our study was to investigate
whether and to what extent IPH plays a role in the
American Journal of Transplantation 2014; 14: 184–192Wiley Periodicals Inc.
�C Copyright 2013 The American Society of Transplantationand the American Society of Transplant Surgeons
doi: 10.1111/ajt.12517
184

progression of CAV in patients transplanted for dilated
cardiomyopathy (DCM) or ischemic cardiomyopathy (ICM).
Materials and Methods
Selection of patients, inclusion criteria
We selected 12 patients from the heart transplant registry at Padua
University who died because of CAV, onwhom autopsywas performed, and
from whom both the native heart and the graft removed at autopsy were
available for histopathology. Patients’ written consent for keeping the native
heart and further use for research purposes was obtained at transplantation.
The hearts retrieved at autopsywere kept for diagnostic and further research
purposes according to the permission of the family and by ethical committee
approval about research on archived materials (Padova Hospital, Ethical
Committee, June 2011).
Four of these patients had been transplanted because of DCM while
the other eight were transplanted for ICM. Overall we were able to evaluate
24 hearts. All major epicardial arteries were assessed macroscopically by
transverse sections every 0.5 cm and themost severe lesions from the three
main epicardial coronary arteries were identified. Among the most severe
lesions we included the culprit lesions responsible for the cardiac death. A
total of 70 lesions were included in the study, of which 35 were from native
hearts and 35 from posttransplant hearts.
Plaque histomorphological classification
Different types of lesion classification have been proposed in the literature
by Virmani et al (17). However at present, there is no internationally
acknowledged histological classification for the different types of CAV
lesions, but only a clinical and angiographic classification (18). Therefore, we
used the classification of native ATS as proposed by the American Heart
Association (AHA) (19,20) butwith somemodifications tomake it suitable for
CAV. Classification was carried out by two pathologists blindly.
Plaque morphologies are classified as follows:
(1) Early lesions including fatty streaks and intimal thickening (correspond-
ing to AHA classification I–III lesions).
(2) Fibrocellular lesions: concentric or eccentric fibromuscular intimal
hyperplasia with more than 50% of its area occupied by nucleated
cells (not included in AHA classification, and considered peculiar to
CAV).
(3) Fibrolipid lesions: concentric or eccentric lesions containing a necrotic
core with cholesterol clefts and extracellular lipid deposits covered by a
fibrous cap (AHA type IV).
(4) Fibrotic lesions: concentric or eccentric lesions composed of collagen
rich tissue, cellularity less than 50% and without significant lipid
deposition (AHA class Vc).
(5) Complicated lesions: lesions with intraplaque hematoma and/or super-
imposed mural thrombus (AHA class VI).
Four groups have been identified: (1) native hearts from DCM patients
(12 lesions); (2) transplanted hearts in DCM patients (12 CAV lesions); (3)
native hearts from ICM patients (23 lesions); (4) transplanted hearts in ICM
patients (23 CAV lesions).
Histological and immunohistochemical methods
Formalin-fixed coronary segments were embedded in paraffin and 4- to
5-mm sections were stained with hematoxylin and eosin, Azan-Mallory
staining for histomorphologic evaluation of the lesions.
Immunohistochemical single and double stains were performed on serial
sections as previously described (21), using mouse monoclonal anti
CD68, anti-mouse monoclonal SMA-1 (reactive with vascular SMCs),
CD31 (reactive with endothelial cells and platelets), anti-rabbit von
Willebrand factor (vWF; reactive with vWF), anti-LCA (reactive with
leucocytes) and anti-glycophorin-A (reactive with erythrocytes and erythro-
cyte membrane remnants). All antibodies were purchased from Dakopatts
(Glostrup, Denmark).
(Immuno) histological assessment of plaque inflammation and
plaque hemorrhage
(1) IPH: IPHwas evaluated using glycophorin A (GFA) immunostain (22) and
Perls iron stain. IPH was classified as either recent-onset (extravascular
located clusters of GFAþ intact erythrocytes), old (deposits of GFAþerythrocyte membrane fragments or iron stain) or ongoing (lesions with
simultaneous presence of recent and old IPH). Plaque hemorrhage was
scored as 0 (absent) and 1 (present) in all cases.
(2) Inflammation: The topographic localization in lesions, of the CD68þ and
LCAþ areas, was scored as superficial (adjacent to the lumen) or deep
(inside the lesion). Inflammation was semi-quantitatively scored as 0:
absent, 1: present. The ratio between immunopositive staining macro-
phages and SMCswas scored as CD68/SMA< 10%, CD68/SMA¼ 10–
50% and CD68/SMA >50% in all plaques.
(3) Presence of microvessels: CD31 positive microvessels were scored as
follows: 0: absent, 1: <10% vessels and 2: >10% vessels.
(4) Microvascular dilatation and endothelial leakage: Dilatation of vessels
was evaluated as 0: absent, 1: present. Leakage of microvessels
was assessed by presence of a rim of perivascular staining with anti-
vWF as reported previously (12) and was scored as either 0: absent
(only staining of endothelial cells), 1: present (additional staining of
perivascular tissue).
Statistical analysis
Data are presented as counts and percentages. Association of morphologic
plaque characteristics was analyzed with chi-square or Fisher’s exact
test. The statistical significance was set at the 5% level. The analyses
were conducted with SAS 9.2 (SAS Institute, Inc., Cary, NC) for
Windows.
Results
Clinical profile of patientsClinical characteristics of all patients who were trans-
planted for either DCM or ICM are presented in Table 1.
Histomorphological classification of lesions in nativehearts and in transplanted heartsHistomorphological classification of the lesions in native
ATS and CAV is reported in Table 2.
In the DCM hearts, only rarely were ATS plaques detected
(9 lesions in 12 samples, of which 7 were early lesions).
In ICM hearts, 23 lesions were found, which were all
advanced plaques (including 1 lesion complicated by
thrombosis). By contrast, nearly all lesions studied from
the 12 autopsy hearts (CAV lesions) were advanced
plaques, of which 4 were complicated by thrombosis.
See Table 3 for details.
Intraplaque Hemorrhage in CAV
185American Journal of Transplantation 2014; 14: 184–192

IPH in CAV lesions versus native plaquesIn the allografts from DCM and ICM patients, altogether 21
out of 35 (60%) CAV lesions showed signs of either fresh
(presence of extracellular intact erythrocytes) or old (GFA
immunopositive erythrocyte remnants, membrane frag-
ments and/or iron deposits) IPH, while in the native ATS,
which were derived from the explant hearts of the same
patients, IPH was present in 8 of 35 (22.9%) lesions
(Figure 1A–C, p¼ 0.0016). Fresh IPH was present in 4/35
(11.4%) of CAV lesions and in 3/35 (8.6%) in ATS plaques
(Figure 1D). Old hemorrhageswere present in 5/35 (14.3%)
of CAV lesions versus 2/35 (5.7%) in ATS plaques
(Figure 1D–F). Fresh and old IPH, as ongoing IPH, were
present in 12/21 (57.1%) CAV lesions compared to 3/8
(37.5%, Figure 1D) ATS.
In CAV lesions IPH co-localized in the necrotic core with
extracellular lipid material, close to numerous cholesterol
clefts. Fresh and old IPH were localized in different sites in
12/21 (57.1%) plaques.
The incidence of IPH in CAV lesions did not differ
significantly from culprit (55.6%) and nonculprit (78.6%,
p¼ 0.2656) lesions.
IPH, microvessels, inflammation and endothelialleakage in CAV lesions versus native plaquesIntraplaque CD31-immunopositive microvessels were
present in 23/35 (65.7%) of the native ATS. Only in
8/23 (34.8%) of these cases the microvessels showed
a rim of perivascular immunostaining with anti-vWF anti-
body, indicating endothelial leakage as previously reported
(9,23).
In CAV lesions, 26 out of 35 (74.3%, p¼ 0.4339 vs. ATS
microvessels) showed presence of intimal microvessels,
and 18/26 (69.2%) of thempresented perivascular anti-vWF
immmunostaining, indicating vessel leakage (Table 4).
Inflammation was identified as areas with CD68þ and
LCAþ cells, indicating presence of macrophages and
leukocytes. Inflammation was present in 31/35 (88.6%)
of the CAV lesions and in 25/35 (71.4%) of the ATS lesions
(Table 4, p¼0.1102 vs. ATS lesions). In the ATS plaques, it
was not possible to define the presence of inflammation in
one early lesion. A superficially located inflammatory infil-
trate was more commonly found in CAV lesions (26/35,
74.3%) than in ATS lesions (14/35, 40%, p¼ 0.0047).
Inflammatory infiltrates that were located deep inside the
lesions were found both in CAV (25/35, 71.4%) and in ATS
lesions (19/35, 54.3%) with no statistically significant
differences between them (Table 4). Superficial and deep
inflammation together were found in 20/35 (57.1%)
CAV lesions compared to 6/35 (17.1%) ATS plaques
(p¼0.0121). Moreover, in CAV lesions, the IPH events
were strongly associated with presence of microvessels,
20/21 (95.2%) IPH positive plaques (p¼0.0009) as in ATS
group (p¼ 0.0316).
In CAV lesions areas with IPH frequently co-localized with
microvessels and perivascular anti-vWF immunostaining
and with inflammatory cells at the same sites within the
plaques (Figure 2).
Table 1: Baseline clinical characteristics
pt
Age at
HT (yrs)
Indication
to HT
Survival
(yrs) Hypertension Diabetes Smoking
Donor
age (yrs)
PRA
(%)
Mismatch
(AB and DR)
Ischemic
time (min)
Total
rejection
score
Severe
rejection
score
1 21 DCM 13 y n n 11 na 5/12 (42%) 120 1 0.18
2 55 DCM 18 y y n 20 na 2/12 (17%) 120 1.3 0.09
3 45 DCM 17 n n n 28 0 4/12 (33%) 180 0.41 0.06
4 27 DCM 17 n n n 16 na 4/12 (33%) 120 0.46 0.04
5 59 ICM 1.3 n n n 41 na 3/12 (25%) 60 1.4 0.13
6 63 ICM 6 y y n 19 0 4/12 (33%) 180 0.6 0.27
7 40 ICM 3.3 n n n 27 0 4/12 (33%) 120 1.57 0.19
8 47 ICM 1.5 n n n 58 0 6/12 (50%) 60 1.19 0.19
9 51 ICM 1.1 y n n 27 0 2/12 (17%) 180 1.65 0.3
10 53 ICM 10 y y n 16 0 3/12 (25%) 120 2.6 0.36
11 52 ICM 1.2 y n n 40 0 na 180 1.38 0.62
12 59 ICM 3.6 n n n 30 0 4/12 (33%) 120 1 0.73
DCM, dilated cardiomyopathy; HT, heart transplantation; ICM, ischemic cardiomyopathy; min, minutes; n, no; na, not available; PRA, panel
reactive antibodies; pt, patient; y, yes; yrs, years.
Table 2: Plaque classification scheme and morphology of ATS
and CAV plaques
Plaque classification
Native ATS
(n¼35),
n (%)
CAV
(n¼35),
n (%)
Total
(n¼70),
n (%)
1. No lesions 3 (8.6) 0 (0) 3 (4.3)
2. Early lesions 7 (20) 3 (8.6) 10 (14.3)
3. Fibrocellular lesions 3 (8.6) 17 (48.6) 20 (28.6)
4. Fibrotic lesions 8 (22.9) 3 (8.6) 11 (15.7)
5. Fibrolipid lesions 13 (37.1) 8 (22.9) 21 (30)
6. Complicated lesions 1 (2.9) 4 (11.4) 5 (7.1)
ATS, native atherosclerotic plaques in explant hearts; CAV, cardiac
allograft vasculopathy plaques in graft hearts at autopsy.
Castellani et al
186 American Journal of Transplantation 2014; 14: 184–192

IPH, microvessels, inflammation and vessel leakagein relation to plaque morphologyPresence of IPH, neoangiogenesis, inflammation and
vessel leakage in CAV lesions were also evaluated in
relation to the specific type of plaque morphology (Table 4).
IPH was found in 11/17 (64.7%) of fibrocellular lesions, the
lesion type specific for CAV. Three out 11 of these lesions
(27.3%) had fresh IPH, 2/11 (18.2%) had old IPHwhile 6/11
(54.5%) had features of both fresh and old IPH in the
same lesion. Moreover, 13/17 (76.5%) fibrocellular lesions
also showed presence of microvessels, 15/17 (88.2%) had
inflammatory infiltrates, and 11/17 (64.7%) had perivascular
anti-vWF immunostaining (Figure 3).
Moreover there was a strong association between
fibrocellular lesions and IPH (p¼0.0142).
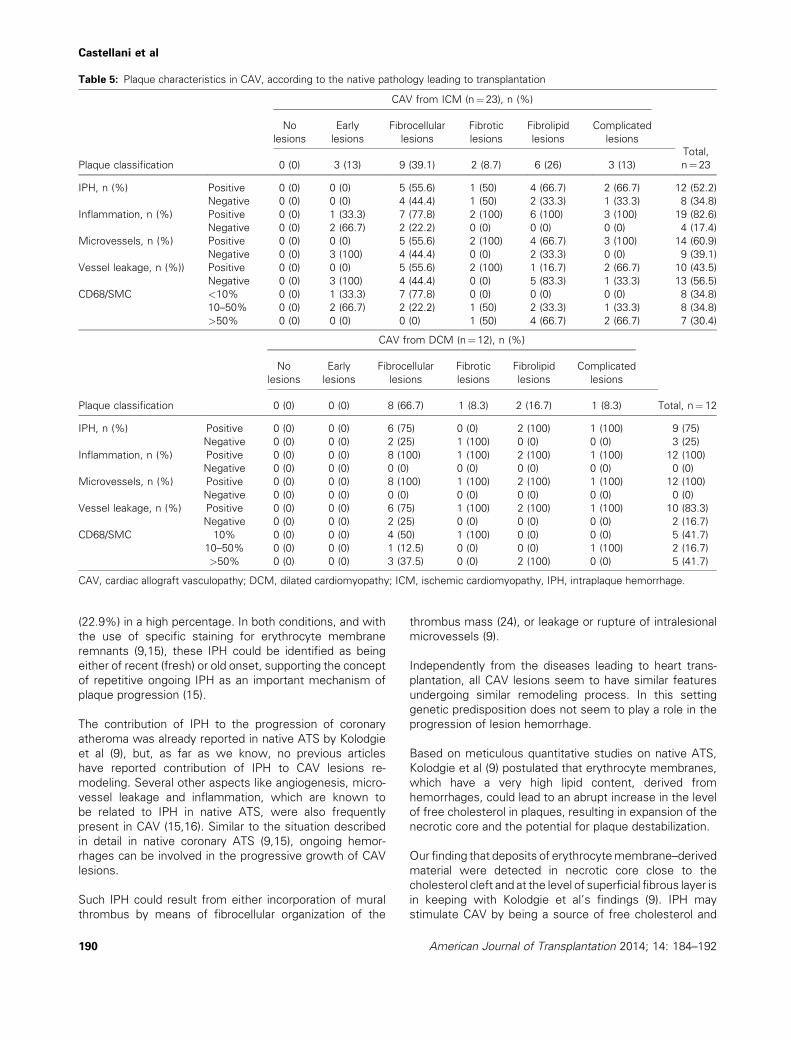
Relation of CAV lesions phenotype and the nativepathology leading to transplantationIPH was detected in more than half of CAV lesions (52.2%)
from ICM patients. CAV lesions from ICM and DCM
Figure 1: Analysis of intraplaque hemorrhage (IPH). (A) The graph shows the percentage (%) of IPH in native atherosclerotic (ATS)
lesions and in cardiac allograft vasculopathy (CAV). IPH is present in 21/35 (60%) of CAV lesions compared to ATS 8/35 (22.9%, p¼0.0016);
(B) graph shows the percentage of IPH in CAV and ATS lesions separated in fresh, old and for both fresh and old staining. Fresh IPH was
present in 4/35 (11.4%) of CAV lesions and in 3/5 (8.6%) in ATS plaques. Old hemorrhagewas present in 5/35 (14.3%) of CAV lesions versus
2/35 (5.7%) in ATS plaque lesions. Fresh and old IPH, as ongoing IPH phenomenon,were present in 12/21 (57.1%) CAV lesions compared to
ATS with 3/8 (37.5%); (C) immunostaining for glycophorin A antibody that identifies fresh staining for IPH. Original magnification 40�; (D)
immunostaining for glycophorin A, antibody that identify staining for IPH. Original magnification 40�.
Table 3: Plaque classification scheme and morphology according to the native pathology leading to transplantation
Plaque classification
DCM (n¼12) ICM (n¼23)
Native ATS, n (%) CAV, n (%) Native ATS, n (%) CAV, n (%)
1. No lesions 3 (25) 0 (0) 0 (0) 0
2. Early lesions 7 (58.3) 0 (0) 0 (0) 3 (13)
3. Fibrocellular lesions 0 (0) 8 (66.7) 3 (13) 9 (39.1)
4. Fibrotic lesions 0 (0) 1 (8.3) 8 (34.8) 2 (8.7)
5. Fibrolipid lesions 2 (16.7) 2 (16.7) 11 (47.8) 6 (26.1)
6. Complicated lesions 0 (0) 1 (8.3) 1 (4.3) 3 (13)
CAV, cardiac allograft vasculopathy lesions in allograft at autopsy; DCM, lesions from patients transplanted because of dilated
cardiomyopathy; ICM, lesions from patients transplanted because of ischemic cardiomyopathy; native ATS, native atherosclerotic plaques
in explanted hearts.
Intraplaque Hemorrhage in CAV
187American Journal of Transplantation 2014; 14: 184–192

Table 4: Plaque classification scheme and morphology
Plaque classification
CAV (n¼35), n (%)
Total
(n¼35)
No
lesions
Early
lesions
Fibro
cellular
lesions
Fibrotic
lesions
Fibrolipid
lesions
Complicated
lesions
0 (0) 3 (8.6) 17 (48.6) 3 (8.6) 8 (22.9) 4 (11.4)
IPH, n (%) Positive 0 (0) 0 (0) 11 (64.7) 1 (33.3) 6 (75) 3 (75) 21 (60)
Negative 0 (0) 3 (0) 6 (35.3) 2 (66.6) 2 (25) 1 (25) 14 (40)
Inflammation, n (%) Positive 0 (0) 1 (33.3) 15 (88.2) 3 (100) 8 (100) 4 (100) 31 (88.6)
Negative 0 (0) 2 (66.6) 2 (11.8) 0 (0) 0 (0) 0 (0) 4 (11.4)
Microvessels, n (%) Positive 0 (0) 0 (0) 13 (76.5) 3 (100) 6 (75) 4 (100) 26 (74.3)
Negative 0 (0) 3 (100) 4 (23.5) 0 (0) 2 (25) 0 (0) 9 (25.7)
Vessel leakage, n (%) Positive 0 (0) 0 (0) 11 (64.7) 3 (100) 3 (37.5) 3 (75) 20 (57.1)
Negative 0 (0) 3 (100) 6 (35.3) 0 (0) 5 (62.5) 1 (25) 15 (42.9)
CAV, cardiac allograft vasculopathy; IPH, intraplaque hemorrhage.
Figure 2: Overviewof IPH,microvessels andendothelial leakage inCAV lesions. (A) Hematoxylin and eosin (H&E) of a cross-section of
a cardiac allograft vasculopathy (CAV) lesion. The bar indicates 500mm. (B) Detail of the black insert in (A). Immunostaining for glycophorinA,
showing extravasation of intact erythrocytes, indicating fresh hemorrhage. The bar indicates 100mm. (C) Detail of the black insert in (A).
Immunostaining for CD31 indicates presence ofmicrovessels in the plaque. Note as areaswith intraplaque hemorrhage (IPH) in CAV lesions
frequently co-localized with presence of microvessels. Bar indicates 100mm. (D) Detail of the black insert in (A). Immunostaining for von
Willebrand factor (vWF): leakage of microvessels is identified by the presence of diffuse perivascular vWF deposits. Note as areas with IPH
in CAV lesions co-localized also with microvessel and vessel leakage. Bar indicates 100mm.
Castellani et al
188 American Journal of Transplantation 2014; 14: 184–192

presented both fresh and old hemorrhage with a mean
percentage of 40%and 16%, respectively. Hemorrhage co-
localized with lipid and necrotic core in these lesions.
Inflammation was a common pattern in most of the CAV
lesions (78.3% and 50% from ICM and DCM). No
differences were identified between superficial and deep
inflammation (Table 5).
Discussion
The main result of our study is that IPH, which is regularly
observed in native ATS and considered responsible for
episodes of sudden plaque growth (9–11), is also an
important feature in CAV. Such IPH could be observed in
our study both in CAV lesions (60%) and in native ATS
Figure 3: Intraplaque hemorrhage localization. (A) Hematoxylin and eosin (H&E) stain of a cross-section of a cardiac allograft
vasculopathy lesion (2�); insert shows intraplaque hemorrhage. (B) Details of black insert in (A), immunostained for glycophorin A, showing
erythrocytes fragments, which indicates old hemorrhage. Bar indicates 100mm. (C) Perls staining for detection of iron (black deposits),
indicating old hemorrhage that co-localizedwith glycophorin A, in erythrocytemembrane. Bar indicates 100mm. (D) Adjacent tissue section
immunostained for von Willebrand factor showing leakage of vessels. Bar indicates 100mm. (E) Immunostaining for SMA/CD68, showing
the presence of inflammation around necrotic core. Bar indicates 100mm.
Intraplaque Hemorrhage in CAV
189American Journal of Transplantation 2014; 14: 184–192
(22.9%) in a high percentage. In both conditions, and with
the use of specific staining for erythrocyte membrane
remnants (9,15), these IPH could be identified as being
either of recent (fresh) or old onset, supporting the concept
of repetitive ongoing IPH as an important mechanism of
plaque progression (15).
The contribution of IPH to the progression of coronary
atheroma was already reported in native ATS by Kolodgie
et al (9), but, as far as we know, no previous articles
have reported contribution of IPH to CAV lesions re-
modeling. Several other aspects like angiogenesis, micro-
vessel leakage and inflammation, which are known to
be related to IPH in native ATS, were also frequently
present in CAV (15,16). Similar to the situation described
in detail in native coronary ATS (9,15), ongoing hemor-
rhages can be involved in the progressive growth of CAV
lesions.
Such IPH could result from either incorporation of mural
thrombus by means of fibrocellular organization of the
thrombus mass (24), or leakage or rupture of intralesional
microvessels (9).
Independently from the diseases leading to heart trans-
plantation, all CAV lesions seem to have similar features
undergoing similar remodeling process. In this setting
genetic predisposition does not seem to play a role in the
progression of lesion hemorrhage.
Based on meticulous quantitative studies on native ATS,
Kolodgie et al (9) postulated that erythrocyte membranes,
which have a very high lipid content, derived from
hemorrhages, could lead to an abrupt increase in the level
of free cholesterol in plaques, resulting in expansion of the
necrotic core and the potential for plaque destabilization.
Our finding that deposits of erythrocytemembrane–derived
material were detected in necrotic core close to the
cholesterol cleft and at the level of superficial fibrous layer is
in keeping with Kolodgie et al’s findings (9). IPH may
stimulate CAV by being a source of free cholesterol and
Table 5: Plaque characteristics in CAV, according to the native pathology leading to transplantation
Plaque classification
CAV from ICM (n¼23), n (%)
Total,
n¼23
No
lesions
Early
lesions
Fibrocellular
lesions
Fibrotic
lesions
Fibrolipid
lesions
Complicated
lesions
0 (0) 3 (13) 9 (39.1) 2 (8.7) 6 (26) 3 (13)
IPH, n (%) Positive 0 (0) 0 (0) 5 (55.6) 1 (50) 4 (66.7) 2 (66.7) 12 (52.2)
Negative 0 (0) 0 (0) 4 (44.4) 1 (50) 2 (33.3) 1 (33.3) 8 (34.8)
Inflammation, n (%) Positive 0 (0) 1 (33.3) 7 (77.8) 2 (100) 6 (100) 3 (100) 19 (82.6)
Negative 0 (0) 2 (66.7) 2 (22.2) 0 (0) 0 (0) 0 (0) 4 (17.4)
Microvessels, n (%) Positive 0 (0) 0 (0) 5 (55.6) 2 (100) 4 (66.7) 3 (100) 14 (60.9)
Negative 0 (0) 3 (100) 4 (44.4) 0 (0) 2 (33.3) 0 (0) 9 (39.1)
Vessel leakage, n (%)) Positive 0 (0) 0 (0) 5 (55.6) 2 (100) 1 (16.7) 2 (66.7) 10 (43.5)
Negative 0 (0) 3 (100) 4 (44.4) 0 (0) 5 (83.3) 1 (33.3) 13 (56.5)
CD68/SMC <10% 0 (0) 1 (33.3) 7 (77.8) 0 (0) 0 (0) 0 (0) 8 (34.8)
10–50% 0 (0) 2 (66.7) 2 (22.2) 1 (50) 2 (33.3) 1 (33.3) 8 (34.8)
>50% 0 (0) 0 (0) 0 (0) 1 (50) 4 (66.7) 2 (66.7) 7 (30.4)
Plaque classification
CAV from DCM (n¼12), n (%}
Total, n¼12
No
lesions
Early
lesions
Fibrocellular
lesions
Fibrotic
lesions
Fibrolipid
lesions
Complicated
lesions
0 (0) 0 (0) 8 (66.7) 1 (8.3) 2 (16.7) 1 (8.3)
IPH, n (%) Positive 0 (0) 0 (0) 6 (75) 0 (0) 2 (100) 1 (100) 9 (75)
Negative 0 (0) 0 (0) 2 (25) 1 (100) 0 (0) 0 (0) 3 (25)
Inflammation, n (%) Positive 0 (0) 0 (0) 8 (100) 1 (100) 2 (100) 1 (100) 12 (100)
Negative 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
Microvessels, n (%) Positive 0 (0) 0 (0) 8 (100) 1 (100) 2 (100) 1 (100) 12 (100)
Negative 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
Vessel leakage, n (%) Positive 0 (0) 0 (0) 6 (75) 1 (100) 2 (100) 1 (100) 10 (83.3)
Negative 0 (0) 0 (0) 2 (25) 0 (0) 0 (0) 0 (0) 2 (16.7)
CD68/SMC 10% 0 (0) 0 (0) 4 (50) 1 (100) 0 (0) 0 (0) 5 (41.7)
10–50% 0 (0) 0 (0) 1 (12.5) 0 (0) 0 (0) 1 (100) 2 (16.7)
>50% 0 (0) 0 (0) 3 (37.5) 0 (0) 2 (100) 0 (0) 5 (41.7)
CAV, cardiac allograft vasculopathy; DCM, dilated cardiomyopathy; ICM, ischemic cardiomyopathy, IPH, intraplaque hemorrhage.
Castellani et al
190 American Journal of Transplantation 2014; 14: 184–192

macrophage activation. Our lesions are representative of
the heterogeneity of CAV lesions. Lipid could result from
lipid insudation from blood or from disrupted erythrocytes
membranes.
IPH frequently occurs in ATS, and pathological studies have
demonstrated that IPH and plaque rupture are associated
with increased microvessel density (9). In our study, IPH
was strongly associated with presence of microvessels.
IPH derived from microvascular disruption or leakage is
considered to contribute to necrotic core expansion, which
precedes plaque instability and rupture (9,25). Repeated
hemorrhage events, in our study, occurred in at least
one-third of patients with previous IPH.
Iron accumulation due to hemoglobin breakdown can act as
a catalyst in the formation of free radicals that modify LDL
cholesterol and foam cells (26). Thus, iron accumulation
deposits are not only a histological marker of previous
hemorrhage but also a possible source of reactive oxygen
species, and could activate the redox state inducing
inflammatory reaction and activating matrix metallopro-
teases, leading to coronary plaque instability via reactive
oxygen species generation (26).
CAV is a process that negatively affects survival after heart
transplantation. The concentric growth is generally believed
to be caused by the influx and growth of SMCs originating in
the tunica media of the coronary arteries (6).
In this work, we also identified infiltrating inflammatory
cells both superficial and deep in the plaque. There was no
difference in plaque inflammation phenotype between ATS
and CAV. Moreover in CAV lesions, both superficial and
deep inflammation were found in 57.1% compared to ATS
lesions with only 19.4%.
Limitation of the Study
For the first time we had the possibility to study and
compare within the same group of patients CAV from
explanted hearts at autopsy with native coronary ATS from
the heart removed at transplantation. The inclusion criteria
adopted in this study led to a relatively constrained data set,
with an overall number of lesions analyzed around 70. Even
though the limited amount of data available suggests
caution in extrapolating general patterns from this study,
our results provide new insight on the mechanisms
underlying the formation of CAV lesions. Further work
will be needed to expand the current database and better
assess the statistical significance of these results.
Conclusions
Findings from this study suggest the importance of
repeated hemorrhage into the plaque as an additional
mechanism of CAV progression.
Neoangiogenesis combined with endothelial leakage
was a constant feature in CAV lesions. Incorporation of
luminal thrombi cannot be entirely excluded. However,
microvessels were constantly present in association with
hemorrhage while plaque fissure was absent.
Repeated IPH and the resulting consequences related
to trapped erythrocytes and activated macrophages may
be important factors in the rapid progression of CAV.
Understanding the mechanism by which plaque angiogen-
esis, vessel growth and IPHoccur in CAVmay help to define
a better therapeutic and preventive strategy.
Imaging modalities such as contrast-enhanced ultrasound
and dynamicMRI have the potential to evaluate intraplaque
neovascularization and IPH noninvasively, improving our
stratification of ‘‘high-risk’’ patients (10,27,28). IPH may
serve as surrogate for events that are stronger than intima-
media thickness (29). Using microbubbles as vehicles
for targeted drug therapy could be foreseen as future
therapeutic intervention (30).
Acknowledgments
This work was supported by a research grant from University of Padua
(nos. CPDR099073, CPDA108809, 60A07-5074 and 60A07-8587).
Disclosure
The authors of this manuscript have no conflicts of interest
to disclose as described by the American Journal of
Transplantation.
References
1. Stelik J, Edwards LB, Kucheryavaya AY, et al. The registry of the
international society for heart and lung transplantation: 29th official
adult heart transplant report—2012. J Heart Lung Transplant 2012;
31: 1052–1064.
2. Schmauss D, Weis M. Cardiac allograft vasculopathy. Circulation
2008; 117: 2131–2141.
3. Rahmani M, Cruz RP, Granville DJ, McManus BM. Allograft
vasculopathy versus atherosclerosis. Circ Res 2006; 99: 801–815.
4. Caforio AL, Tona F, Fortina AB, et al. Immune and nonimmune
predictors of cardiac allograft vasculopathy onset and severity:
Multivariate risk factor analysis and role of immunosuppression.
Am J Transplant 2004; 4: 962–970.
5. Costanzo MR, Naftel DC, Pritzker MR, et al. Heart transplant
coronary artery disease detected by coronary angiography: A
multiinstitutional study of preoperative donor and recipient risk
factors: Cardiac Transplant Research Database. J Heart Lung
Transplant 1998; 17: 744–753.
6. van Loosdregt J, van Oosterhout MFM, Bruggink AH, et al. The
chemokine and chemokine receptor profile of infiltrating. Cells in
the wall of arteries with cardiac allograft vasculopathy is indicative
of a memory T-helper 1 response. Circulation 2006; 114: 1599–
1607.
Intraplaque Hemorrhage in CAV
191American Journal of Transplantation 2014; 14: 184–192

7. Van der Wal AC, Becker AE, van der Loos CM, Das PK. Site of
intimal rupture or erosion of thrombosed coronary atherosclerotic
plaques is characterized by an inflammatory process irrespective
of the dominant plaque morphology. Circulation 1999; 89: 36–44.
8. Hosono M, de Boer OJ, van der Wal AC, et al. Increased
expression of T cell activation markers (CD25, CD26, CD40L
and CD69) in atherectomy specimens of patients with unstable
angina and acute myocardial infarction. Atherosclerosis 2003; 168:
73–80.
9. Kolodgie FD, Gold HK, Virmani R, et al. Intraplaque haemorrhage
and progression of coronary atheroma. N Engl J Med 2003; 349:
2316–2325.
10. Hellings WE, Peeters W, Moll FL, et al. Composition of carotid
atherosclerotic plaque is associated with cardiovascular outcome:
A prognostic study. Circulation 2010; 121: 1941–1950.
11. Takaya N, Yuan C, Chun B, et al. Presence of intraplaque
haemorrhage stimulates progression of carotid atherosclerotic
plaques: A high resolution magnetic resonance imaging study.
Circulation 2005; 111: 2768–2775.
12. Virmani R, Kolodgie FD, Burke AP, et al. Atherosclerotic plaque
progression and vulnerability to rupture: Angiogenesis as a source
of intraplaque haemorrhage. Arterioscler Thromb Vasc Biol 2005;
25: 2054–2061.
13. Yeagle PL. Cholesterol and the cell membrane. Biochim Biophys
Acta 1985; 822: 267–287.
14. Kockx MM, Cromheeke KM, Knaapen MW, et al. Phagocytosis
and macrophage activation associated with hemorrhagic micro-
vessels in human atherosclerosis. Arterioscler Thromb Vasc Biol
2003; 23: 440–446.
15. Li X, van der Meer JJ, van der Loos CM, et al. Microvascular
endoglin (CD105) expression correlates with tissue markers for
atherosclerotic plaque vulnerability in an ageing population with
multivessels coronary artery disease. Histopathology 2012; 61:
88–97.
16. Fleiner M, Kummer M, Mirlacher M, et al. Arterial neovasculariza-
tion and inflammation in vulnerable patients: Early and late signs of
symptomatic atherosclerosis. Circulation 2004; 110: 2843–2850.
17. Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM. Lessons
from sudden coronary death. A comprehensive morphological
classification scheme for atherosclerotic lesions. Arterioscler
Thromb Vasc Biol 2000; 20: 1262–1275.
18. Mehra MR, Crespo-Leiro MG, Dipchand A, et al. International
society for heart and lung transplantation working formulation of a
standardized nomenclature for cardiac allograft vasculopathy—
2010. J Heart Lung Transplant 2010; 29: 717–727.
19. Stary HC, Chandler CA, Glagov S, et al. A definition of initial, fatty
streak and intermediate lesions of atherosclerosis. A report from
committee on vascular lesions of the council on atherosclerosis,
American Heart Association. Circulation 1994; 89: 2462–2478.
20. Stary HC, Chandler CA, Dinsmore RE, et al. A definition of
advanced types of atherosclerotic lesions and a histological
classification of atherosclerosis. A report from committee on
vascular lesions of the council on atherosclerosis, American Heart
Association. Artheriosclerorosis Thromb Vasc Biol 1995; 15: 1512–
1531.
21. de Boer OJ, van der Loos CM, Teeling P, van der Wal AC,
Teunissen MB. Immunohistochemical analysis of regulatory T cell
markers FOXP3 and GITR on CD4þ CD25þ T cells in normal skin
and inflammatory dermatoses. J Histochem Cytochem 2007; 55:
891–898.
22. Andersson LC, von Willebrand E, Jokinen M, Karhi KK, Gahmberg
CG. Glycophorin A as an erythroid marker in normal and malignant
hematopoiesis. Haematol Blood Transfus 1981; 26: 338–344.
23. Meijer-Jorna LB,Mekkes JR, van derWal AC. Platelet involvement
in cutaneous leukocytoclasic vasculitis. J Cutan Pathol 2002; 29:
176–180.
24. van der Wal AC, Li X, de Boer OJ. Tissue factor expression in the
morphology spectrum of vulnerable atherosclerosic plaques.
Semin Thromb Hemost 2006; 32: 40–47.
25. Castellani C, van der Wal AC, De Boer OJ, et al. Virtual histology
and themorphologic assessment of cardiac allograft vasculopathy.
Am J Transplant 2012; 13: 1109.
26. Yuan XM, Brunk UT, Olsson AG. Effect of iron and hemoglobin-
loaded human monocyte-derived macrophages on oxidation and
uptake of LDL. Arterioscler Thromb Vasc Biol 1995; 15: 1345–
1351.
27. Moguillansky D, Leng X, Carson A, et al. Quantification of plaque
neovascularization using contrast ultrasound: A histologic valida-
tion. Eur Heart J 2011; 32: 646–653.
28. Dong L, Kerwin WS, Chen H, et al. Carotid artery atherosclerosis:
Effect of intensive lipid therapy on the vasa vasorum—Evaluation
by using dynamic contrast-enhancedMR imaging. Radiology 2011;
260: 224–231.
29. ten Kate GL, Sijbrands EJ, Valkema R, et al. Molecular imaging of
inflammation and intraplaque vasa vasorum: A step forward
to identification of vulnerable plaques? J Nucl Cardiol 2010; 17:
897–912.
30. Chen ZY, Yan Lin Y, Yang F, Jiang L, Ge SP. Gene therapy for
cardiovascular disease mediated by ultrasound and microbubbles.
Cardiovasc Ultrasound 2013; 11: 11–14.
Castellani et al
192 American Journal of Transplantation 2014; 14: 184–192
Related Documents











