Intraosseous Vascularization of Anterior Mandible: A Radiographic Analysis Roberto Di Bari, DDS,* Roberto Coronelli, MD, DDS, and Andrea Cicconetti, MD* Abstract: The anterior mandible was initially considered a safe zone from a surgical point of view. Over time, serious complications re- sulting from dental implantology procedures have been reported. This has led to a greater focus on vascularization of the interforaminal re- gion. The purpose of this article was to evaluate the anterior man- dibular region in relation to the presence of canals perforating the buccal and lingual cortical plates. DICOM (Digital Imaging and Communications in Medicine) files of 100 cone beam computed tomography scans were analyzed by imaging software. All radiographic cross-sections between the mental foramina were examined to detect the presence and location of per- forating buccal or lingual canals. Lingual perforating canals are pre- sent in 98% of the cohort. The most common site is the symphysis region. The presence of 2 lingual canals cranially and caudally to the genial apophysis has been found in 39%. Vestibular perforating canals are absent in 61%. The anterior mandible has several lingual perforating canals, which are variable in number and location. Imaging software is a valuable aid in presurgical planning. Because of the higher prevalence of per- forating canals in the symphysis region, this site should be preserved. Key Words: CBCT (cone beam computed tomography) imaging, mandibular symphysis, vascularization, computed tomography, perforating canals (J Craniofac Surg 2014;25: 872Y879) T he anterior mandibular region is of particular anatomical interest in oral surgery for implant rehabilitation. It is also considered a valid intraoral donor site of autologous bone for reconstructive patient needs. 1 Previous studies have analyzed the vascularization of the anterior region of the mandible in relation to the hemorrhagic risk during oral surgery. 2 The purpose of this article was to evaluate this site in relation to the presence of perforating canals. Differently from the available literature, this study was performed using high-resolution cone beam computed tomography (CBCT) images and three-dimensional reconstructions. The study aimed to analyze both lingual and buccal perforating canals. Perforating canals were analyzed in relation to location (horizontal and vertical position), patient’s sex, age, and class of edentulism. MATERIALS AND METHODS One hundred CBCT scans, all obtained with the same x-ray apparatus (GENDEX GXCB-500; Gendex Dental Systems, Des Plaines, IL) and the same acquiring parameters, were analyzed. The cohort of 100 CBCT scans was composed of 61 female and 39 male patients. The ages of the patients ranged from 19 to 91 years with subjects belonging to each band (Fig. 1). For each case, the dental formula was described, and the edentulism class was evaluated by the Kennedy classification for partial edentulism (Table 1). DICOM (Digital Imaging and Communications in Medicine) files of each CBCT scan were imported on SimPlant (SimPlant 3-D Pro; Materialize, Leuven, Belgium). The software accepts the impor- tation of DICOM format images: the first standard format for sharing and viewing any kind of medical image. Once imported, images were processed in axial, sagittal, and paraxial sections. The images were real x-ray representations of jaw bones (reproduction scale 1:1) and allowed accurate measurements of anatomical structures. DICOM images related to the mandibular region (230 images on 432) were loaded through the “Image Selector” function of SimPlant. Three-dimensional reconstruction of the mandibular region was obtained through the function “Segmentation” of the software; the “scattering” (linked to dentures or metal restorations in the mouth) was removed. The three-dimensional reconstruction was redirected to have the mandible parallel to the floor. Then, using the function “create a panoramic curve, ” a referral scout view in relation was selected to which the software had rebuilt all the cross sections (1-mm step). At this point, another tool, “create a nerve” was used to highlight the path of the left and right mandibular canal both in cross section and in the three-dimensional reconstruction. Anterior mandible was defined as the region between the mental foramina, considering a margin of 5 mm medially to them (Fig. 2). All cross sections were analyzed to detect the presence and location of buccal or lingual perforating canals. For each case, the number of lingual and buccal perforating canals was recorded. Regarding canal position, distances from the bottom edge of the cortex (h inf ) and from the top edge of the alveolar process (h sup ) were measured (Fig. 3). Because of the nature of retrospective study, the present work did not require a specific institutional review board approval. The current study followed the Declaration of Helsinki on medical pro- tocol and ethics. RESULTS Data on number of perforating canals are presented in Table 2. Depending on the situations encountered, patients were divided into 4 groups and 13 subgroups, characterized by an acronym, as follows: & Patients without canals, with a single homonym subgroup L0+V0Vpatients without canals & Patients with only lingual canals, with 3 subgroups CLINICAL STUDY 872 The Journal of Craniofacial Surgery & Volume 25, Number 3, May 2014 From the *Department of Oral and Maxillofacial Sciences, School of Dentistry, Sapienza University of Rome; and †Dr. Coronelli Dental Clinic, Rome, Italy. Received August 10, 2013. Accepted for publication September 30, 2013. Address correspondence and reprint requests to Roberto Di Bari, DDS, Via Simone Martini, 125-00142, Rome, Italy; E-mail: [email protected] The authors report no conflicts of interest. Copyright * 2014 by Mutaz B. Habal, MD ISSN: 1049-2275 DOI: 10.1097/01.scs.0000436735.60042.49 Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Intraosseous Vascularization of AnteriorMandible: A Radiographic Analysis
Roberto Di Bari, DDS,* Roberto Coronelli, MD, DDS,� and Andrea Cicconetti, MD*
Abstract: The anterior mandible was initially considered a safe zonefrom a surgical point of view. Over time, serious complications re-sulting from dental implantology procedures have been reported. Thishas led to a greater focus on vascularization of the interforaminal re-gion. The purpose of this article was to evaluate the anterior man-dibular region in relation to the presence of canals perforating thebuccal and lingual cortical plates.
DICOM (Digital Imaging and Communications in Medicine) filesof 100 cone beam computed tomography scans were analyzed byimaging software. All radiographic cross-sections between the mentalforamina were examined to detect the presence and location of per-forating buccal or lingual canals. Lingual perforating canals are pre-sent in 98% of the cohort. The most common site is the symphysisregion. The presence of 2 lingual canals cranially and caudally to thegenial apophysis has been found in 39%. Vestibular perforating canalsare absent in 61%.
The anterior mandible has several lingual perforating canals, whichare variable in number and location. Imaging software is a valuableaid in presurgical planning. Because of the higher prevalence of per-forating canals in the symphysis region, this site should be preserved.
Key Words: CBCT (cone beam computed tomography) imaging,mandibular symphysis, vascularization, computed tomography,perforating canals
(J Craniofac Surg 2014;25: 872Y879)
The anterior mandibular region is of particular anatomical interestin oral surgery for implant rehabilitation. It is also considered
a valid intraoral donor site of autologous bone for reconstructivepatient needs.1 Previous studies have analyzed the vascularizationof the anterior region of the mandible in relation to the hemorrhagicrisk during oral surgery.2
Thepurposeof this articlewas to evaluate this site in relation to thepresence of perforating canals. Differently from the available literature,this study was performed using high-resolution cone beam computedtomography (CBCT) images and three-dimensional reconstructions.The study aimed to analyze both lingual and buccal perforating canals.
Perforating canals were analyzed in relation to location (horizontal andvertical position), patient’s sex, age, and class of edentulism.
MATERIALS AND METHODSOne hundred CBCT scans, all obtained with the same x-ray
apparatus (GENDEX GXCB-500; Gendex Dental Systems, DesPlaines, IL) and the same acquiring parameters, were analyzed.
The cohort of 100 CBCT scans was composed of 61 femaleand 39 male patients. The ages of the patients ranged from 19 to91 years with subjects belonging to each band (Fig. 1). For eachcase, the dental formula was described, and the edentulism classwas evaluated by the Kennedy classification for partial edentulism(Table 1).
DICOM (Digital Imaging and Communications in Medicine)files of each CBCT scan were imported on SimPlant (SimPlant 3-DPro; Materialize, Leuven, Belgium). The software accepts the impor-tation of DICOM format images: the first standard format for sharingand viewing any kind of medical image. Once imported, images wereprocessed in axial, sagittal, and paraxial sections. The images werereal x-ray representations of jaw bones (reproduction scale 1:1) andallowed accurate measurements of anatomical structures. DICOMimages related to the mandibular region (230 images on 432) wereloaded through the “Image Selector” function of SimPlant.
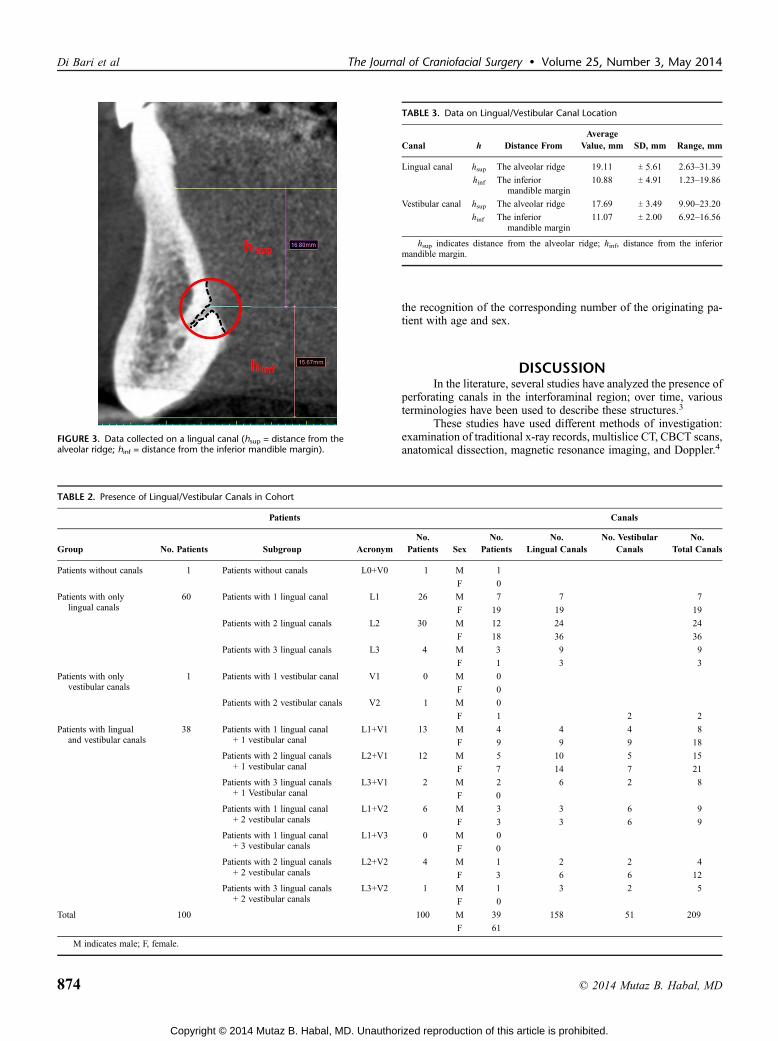
Three-dimensional reconstruction of the mandibular regionwas obtained through the function “Segmentation” of the software;the “scattering” (linked to dentures or metal restorations in the mouth)was removed. The three-dimensional reconstruction was redirected tohave the mandible parallel to the floor. Then, using the function“create a panoramic curve,” a referral scout view in relation wasselected to which the software had rebuilt all the cross sections (1-mmstep). At this point, another tool, “create a nerve”was used to highlightthe path of the left and right mandibular canal both in cross sectionand in the three-dimensional reconstruction. Anterior mandible wasdefined as the region between the mental foramina, considering amargin of 5 mm medially to them (Fig. 2). All cross sections wereanalyzed to detect the presence and location of buccal or lingualperforating canals. For each case, the number of lingual and buccalperforating canals was recorded. Regarding canal position, distancesfrom the bottom edge of the cortex (hinf) and from the top edge ofthe alveolar process (hsup) were measured (Fig. 3).
Because of the nature of retrospective study, the present workdid not require a specific institutional review board approval. Thecurrent study followed the Declaration of Helsinki on medical pro-tocol and ethics.
RESULTSData on number of perforating canals are presented in Table 2.
Depending on the situations encountered, patients were divided into4 groups and 13 subgroups, characterized by an acronym, as follows:& Patients without canals, with a single homonym subgroupL0+V0Vpatients without canals& Patients with only lingual canals, with 3 subgroups
CLINICAL STUDY
872 The Journal of Craniofacial Surgery & Volume 25, Number 3, May 2014
From the *Department of Oral andMaxillofacial Sciences, School of Dentistry,SapienzaUniversityofRome; and†Dr.CoronelliDentalClinic,Rome, Italy.
Received August 10, 2013.Accepted for publication September 30, 2013.Address correspondence and reprint requests to Roberto Di Bari, DDS, Via
Simone Martini, 125-00142, Rome, Italy; E-mail: [email protected] authors report no conflicts of interest.Copyright * 2014 by Mutaz B. Habal, MDISSN: 1049-2275DOI: 10.1097/01.scs.0000436735.60042.49
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

L1Vpatients with 1 lingual canalL2Vpatients with 2 lingual canalsL3Vpatients with 3 lingual canals& Patients with only vestibular canals, with 2 subgroupsV1Vpatients with 1 vestibular canalV2Vpatients with 2 vestibular canals& Patients with lingual and vestibular canals, with 7 subgroupsL1+V1Vpatients with 1 lingual canal + 1 vestibular canalL2+V1Vpatients with 2 lingual canals + 1 vestibular canalL3+V1Vpatients with 3 lingual canals + 1 vestibular canalL1+V2Vpatients with 1 lingual canal + 2 vestibular canalsL1+V3Vpatients with 1 lingual canal + 3 vestibular canalsL2+V2Vpatients with 2 lingual canals + 2 vestibular canalsL3+V2Vpatients with 3 lingual canals + 2 vestibular canals
On the cohort of 100 patients, 209 canals were detected, in-cluding 158 lingual canals and 51 vestibular canals, distributed amongthe various groups and subgroups as described in the list. Both patientsand the detected canals were also divided according to sex of the pa-tients themselves between the various groups and subgroups.
The lingual canals have been identified in 98% of the cohort;there are no lingual canals in only 2% of the cohort. Vestibular per-forating canals are less frequent: no canal in 61% of cases. In thesymphysis region, a single lingual canal was present in 45%. Amiddle
symphysis structure characterized by 2 lingual perforating canals (lo-cated, respectively, cranially and caudally to genial apophysis) wasfound in 39% of cases. A slightly higher occurrence in males (on av-erage, 2.3 canals for male) than in females (on average, 1.9 canals forfemale) was recorded. Data on location of perforating canals arepresented in Table 3.
The distance of lingual perforating canals from the higheralveolar margin (hsup) is 19.11 (SD, 5.61)mm (range, 2.63Y31.39mm)on average, with a minimum value of hsup (2.63 mm) recorded inedentulous patient. The distance of lingual perforating canals fromthe lower margin (hinf) is, on average, 10.88 (SD, 4.91) mm (range,1.23Y19.86 mm). The distance between vestibular canals and theupper alveolar edge (hsup) is, on average, 17.69 (SD, 3.49) mm (range,9.90Y23.20 mm). The distance between vestibular canals and the in-ferior mandible margin (hinf) is, on average, 11.07 (SD, 2.00) mm(range, 6.92Y16.56 mm).
In Figure 4, the position of lingual perforating canals has beenrelated to the upper alveolar ridge (hsup) and patient’s age: the 158perforating lingual canals were numbered in such a way as to allow
FIGURE 1. Composition of the cohort by age and sex. The 100 patients, marked with an identification number, were ordered in ascending age; the figure shows anearly linear distribution of patients’ age in the considered range of 19Y91 years.
TABLE 1. Classification of the Cohort According to the Class of Edentulism
Class of Edentulism No. Cases
Full dentition 43
Class IVpartially edentulous 14
Class IIVpartially edentulous 12
Class IIIVpartially edentulous 30
Edentulous 1
Total no. cases 100FIGURE 2. Lateral limits (5 mm) from mental holes.
The Journal of Craniofacial Surgery & Volume 25, Number 3, May 2014 Intraosseous Vascularization of Mandible
* 2014 Mutaz B. Habal, MD 873
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
the recognition of the corresponding number of the originating pa-tient with age and sex.
DISCUSSIONIn the literature, several studies have analyzed the presence of
perforating canals in the interforaminal region; over time, variousterminologies have been used to describe these structures.3
These studies have used different methods of investigation:examination of traditional x-ray records, multislice CT, CBCT scans,anatomical dissection, magnetic resonance imaging, and Doppler.4
FIGURE 3. Data collected on a lingual canal (hsup = distance from thealveolar ridge; hinf = distance from the inferior mandible margin).
TABLE 3. Data on Lingual/Vestibular Canal Location
Canal h Distance FromAverage
Value, mm SD, mm Range, mm
Lingual canal hsup The alveolar ridge 19.11 T 5.61 2.63Y31.39
hinf The inferiormandible margin
10.88 T 4.91 1.23Y19.86
Vestibular canal hsup The alveolar ridge 17.69 T 3.49 9.90Y23.20
hinf The inferiormandible margin
11.07 T 2.00 6.92Y16.56
hsup indicates distance from the alveolar ridge; hinf, distance from the inferiormandible margin.
TABLE 2. Presence of Lingual/Vestibular Canals in Cohort
Patients Canals
Group No. Patients Subgroup AcronymNo.
Patients SexNo.
PatientsNo.
Lingual CanalsNo. Vestibular
CanalsNo.
Total Canals
Patients without canals 1 Patients without canals L0+V0 1 M 1
F 0
Patients with onlylingual canals
60 Patients with 1 lingual canal L1 26 M 7 7 7
F 19 19 19
Patients with 2 lingual canals L2 30 M 12 24 24
F 18 36 36
Patients with 3 lingual canals L3 4 M 3 9 9
F 1 3 3
Patients with onlyvestibular canals
1 Patients with 1 vestibular canal V1 0 M 0
F 0
Patients with 2 vestibular canals V2 1 M 0
F 1 2 2
Patients with lingualand vestibular canals
38 Patients with 1 lingual canal+ 1 vestibular canal
L1+V1 13 M 4 4 4 8
F 9 9 9 18
Patients with 2 lingual canals+ 1 vestibular canal
L2+V1 12 M 5 10 5 15
F 7 14 7 21
Patients with 3 lingual canals+ 1 Vestibular canal
L3+V1 2 M 2 6 2 8
F 0
Patients with 1 lingual canal+ 2 vestibular canals
L1+V2 6 M 3 3 6 9
F 3 3 6 9
Patients with 1 lingual canal+ 3 vestibular canals
L1+V3 0 M 0
F 0
Patients with 2 lingual canals+ 2 vestibular canals
L2+V2 4 M 1 2 2 4
F 3 6 6 12
Patients with 3 lingual canals+ 2 vestibular canals
L3+V2 1 M 1 3 2 5
F 0
Total 100 100 M 39 158 51 209
F 61
M indicates male; F, female.
Di Bari et al The Journal of Craniofacial Surgery & Volume 25, Number 3, May 2014
874 * 2014 Mutaz B. Habal, MD
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

Only dissective studies provide the vascular-nervous contentof perforating canals, but the study of their characteristics (frequency,location, diameter, etc) requires a number of analyzed cases that canhardly be obtained with such studies.
Radiographic studies allow a wider cohort. Traditional x-rayexaminations do not allow a precise identification of the perforat-ing canals, because of beam orientation: canals are visible only whenthe beam direction coincides with that of the same canals.5
Multislice CTand CBCT images are not affected by this factorand are thus more useful to canal detection.6 The development andwidespread use ofCBCT technology combine a highly accurate surveywith a low biological cost to the patient.4 The resolution distinguishingelement of CBCT is the voxel (three-dimensional pixel). The smallestis the voxel, and the most defined is the cone beam imaging.7
Studied CBCT scans have excellent resolution (voxel size, 0.2 mm).Several studies tested the dimensional accuracy of CBCT
and the validity of linear and volumetric measurements obtained onthem. Most of them experienced no significant statistical differ-ences in accuracy between CBCT and multislice CT; other studiesconfirmed the congruence between linear measurements performedon CBCT images and measures on anatomical dry mandible.8Y11
A three-dimensional image was created for each analyzedcase, achieved through an appropriate density value threshold(Figs. 5A, B). Even if recent studies demonstrate the reliability of
these images,12 all measurements were, however, performed on radio-graphic cross section.
The study of Maloney et al13 tests the hypothesis that linear(vertical and horizontal) measures calculated using a radiographicmachine software (I-CAT; Imaging Science International,Hatfield, PA)and SimPlant are as accurate as the criterion standard, represented bymeasures obtained through a digital gauge on mandibular anatomicalsections. They found no statistically significant differences between thevarious methods. These data confirm the validity of the measurementmethod adopted in present protocol.
At first, anterior mandibular region has been defined. In ac-cordance with the indications emerged in previous works, a surgicaloperation must provide a safety margin of 5 mm medially to themental foramina to prevent iatrogenic injury to nervous structures.14
To obtain a greater clinical significance the same parameters werechosen. On 100 CBCT scans, 3 cases of unilateral double mentalforamen were found. In such cases, the mesial foramen was chosen asreference margin15 (Fig. 6).
FIGURE 4. Lingual canal’s position related with patient age (cases sorted in order of age). The figure shows the typical pattern of the trend: the distance of the canalfrom the alveolar ridge decreases with the age of the patient due to the physiological/pathological resorption of alveolar bone. This trend is not evident with chart datarelated to hinf because of substantial stability of the mandibular lower margin.
FIGURE 5. A and B, Masks obtained by different thresholding values. FIGURE 6. Twin mental holes.
The Journal of Craniofacial Surgery & Volume 25, Number 3, May 2014 Intraosseous Vascularization of Mandible
* 2014 Mutaz B. Habal, MD 875
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

The interforaminal region was initially considered a safe zonefrom a surgical point of view. However, in the literature, serious com-plications resulting from dental implantology procedures have beenreported.2 This may occur during implant’s placement, when theaccidental perforation of the lingual cortical plate is caused, withinjury to adjacent vascular structures.16 The bleeding causes infarctionof the connective tissues of the floor of the mouth. The resultinglifting of the tongue causing upper airway obstruction may neces-sitate an emergency tracheotomy.17
Some authors believe that injury to the intrabone canalswithout lingual plate perforation can also cause bleeding that exposesthe patient to increased risk of death. This occurs, in particular, inthe case of severe mandibular atrophy, if the patient takes anticoag-ulants for a prolonged period of time, or if he has coagulopathy orhypertension.2,4,18
According to Vandewalle et al,3 the artery present in the per-forated canal is of sufficient size to cause severe bleeding, whendamaged during oral surgery. According toGahleitner et al,6 the vesselpresent in the bone canal is proportional to the original sublingualartery and is therefore able to determine significant intraoperativebleeding. To confirm these observations, Lustig et al19 clearly de-fine how the blood flow within these vessels has an arterial originand is directed toward the bone: the blood flowwas detected in 0.7 to3.7 mL/min. The study of Eiseman et al20 performed with Doppler
and duplex ultrasound technique indicates that there is a decrease inmandibular blood flow as age increases.
In the study of vascularization of the mandible, 2 importantfactors must be taken into account: the edentulism class and the ageof the patient. The latter is linked to increased incidence of athero-sclerosis in the elderly: this leads to a general reduction in bloodsupply.20
However, in the mandible, an important role is played bythe presence of dental elements, as the alveolar ridge is uniquelyvascularized by dental branches of the inferior alveolar artery21: whenthe tooth is lost, the dental alveolar bone loses the nutritional intake too.Multiple dental extractions can also cause inferior alveolar arterythrombosis resulting in ischemia and atrophy of tissues placed down-stream vascular disruption.
Castelli et al22 demonstrated the development of a collateralcirculation after proximal obstruction of the inferior alveolar artery.A collateral blood supply comes from the sublingual branch of thelingual artery, from 2 branches of the facial artery (submental andinferior labial) and from the hyoid artery. As these arteries are re-sponsible for perforating vessels in the interforaminal region, it isreasonable to expect an increased flow and therefore an increasedrisk of bleeding in patients with severe atrophy.
Some studies show that excessive bleeding during implantplacement can affect the healing process, resulting in the proliferationof endothelial cells of blood vessels on the implant surface with im-pairment of the osteointegration process.4,23
Finally, the nerve ending lesions within the canals were corre-lated to the incidence of postoperative neurosensory disorders.3 Thecirculation of the anterior mandible is mediated by 3 major arteries:the inferior alveolar artery (and its branch,mylohyoid artery), the facialartery (and its branch, submental artery), and the lingual artery (andits branch, sublingual artery).4
In fact, it is believed that both the facial and lingual arteriescan be damaged as a result of incidents during oral surgery. In an
TABLE 4. Elements of Neurovascular Bundle (Lingual Canals)
Neurovascular Bundle (Lingual Canals) Vascular Element Nervous Element
Superior lingual canal Lingual artery Lingual nerve
Inferior lingual canal Submental artery Mylohyoid nerve
FIGURE 7. A and B, Single lingual canal in three-dimensional mask (A) andradiographic cross section (B).
FIGURE 8. A and B, Superior and inferior lingual canal in three-dimensionalmask (A) and radiographic cross section (B). FIGURE 9. Sublingual region anatomy.
Di Bari et al The Journal of Craniofacial Surgery & Volume 25, Number 3, May 2014
876 * 2014 Mutaz B. Habal, MD
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

emergency situation, it remains a controversial choice to performexternal binding of either artery. Manual compression of the ante-gonial landmark at the bottom edge of the mandible helps to dis-tinguish which of the 2 arteries was injured. If compression of theantegonial landmark stops the bleeding, then the facial/submentalartery is most likely the cause.18
Several authors have studied mouth floor vascularization inrelation to the interforaminal region, and studies confirm that thevascular structures potentially involved are the submental branch ofthe facial artery and the sublingual branch of the lingual artery.16
Scientific studies based on anatomical dissection or by usingCT examinations confirm that terminal vessels of the sublingualand submental arteries can penetrate the lingual cortical plate of theinterforaminal region.24
The main investigated factors were number of canals, locali-zation, diameter, intraosseous direction, content, correlation betweenpresence of canal and sex of the patient, and correlation betweencanal position and age of the patient.
In this work, the lingual canals have been identified in 98%of the cohort. Previous studies found a frequency of canals in themedian portion ranging between 85% and 99%.5,25,26 The study ofVandewalle et al3 on macroanatomical evaluation of 354 dried man-dibles reveals a similar percentage.
Generally, radiographic-based examinations reveal an inci-dence lower than anatomical studies: high-resolution x-ray imageanalysis and three-dimensional reconstruction offered by SimPlanthave allowed a greater correspondence with anatomical and dis-section studies.
In this work, the lingual foramen diameters have not beenevaluated, as in the literature there are overlapping data. Longoniet al27 refer to a diameter between 0.3 and 1.1 mm (mean value,0.6 [SD, 0.2] mm). Gahleitner et al6 distinguish the vessel diameterdepending on their position: middle position (0.7 [SD, 0.3] mm) andpremolar position (0.6 [SD, 0.2] mm). Lustig et al19 refer to a diameterof 0.18 to 1.8 mm. Vandewalle et al3 performed a very thorough in-vestigation on the lingual foramen located in the upper position inrespect to the genial apophysis, recording diameter data substan-tially similar to those described previously. According to the studyby Vandewalle et al,3 the shape of the entering foramen appearsgenerally funnel shaped or round. The length of the intraosseouscanal course has not been studied in this article, but Romanoset al23 indicate a value between 5 and 15 mm with a mean value of10.55 mm. Tepper et al26 describe the intraosseous course distinguishing
between the middle and side canals: median canals show a buccal-to-lingual course, whereas side canals have a ventral direction. The currentstudy confirms these data. In the middle section, when multiple vesselsare present, their intraosseous course frequently appears convergent,thus forming anastomoses between them.
An accurate study of perforating bone canals must providea distinction according to their location. The literature shows thatauthors have chosen different criteria for topographic grouping ofcanals from time to time. More frequently, the horizontal positionof the canals was placed in relation to dental elements present inthat region: thus, there are canals in premolar, lateral incisors, andin the middle section or symphysis region.
In the current study, a similar classification was used. How-ever, vessels in the premolar region were not studied, because of alimit of 5 mm from the mental foramina. The study of Gahleitneret al6 reported an incidence of perforating canals in the premolararea of 34% (right side) and 38% (left side). The investigativemethod of the current study appears similar to that adopted byLongoni et al.27 In their article, they studied the number, location,and size of lingual perforating canals; the analysis was carried outon a cohort of 100 dry mandibles, and the results were comparedwith those obtained by radiographic analyses performed on CTof the same mandibles.
According to the study of Longoni et al,27 most mandibles(45%) present a single lingual canal in the symphysis region; othertypical location is the lateral incisor region (Figs. 7A, B). The presentwork reveals the recurrence (39%) of a middle symphysis structurecharacterized by 2 lingual perforating canals located, respectively,cranially and caudally to genial apophysis (Figs. 8A, B). This patternemerges also in the work of Liang et al25: their dissective exami-nation indicates that the upper perforating canal is a terminal branchof the sublingual artery, whereas the lower is a terminal branch of thesubmental artery (Table 4; Fig. 9). Another pattern is the verticalposition of the canal, which could be related with the upper alveolarridge or with the lower margin of the mandible.
In the present work, both of these values have been recorded:hsup and hinf. The distance of lingual perforating canals from the higheralveolar margin (hsup) is 19.11 (SD, 5.61)mm (range, 2.63Y31.39mm)on average; this result is obviously of surgical interest but is highlyinfluenced by the presence or absence of dental elements and by thedegree of resorption of the edentulous sites. Confirming that, a
FIGURE 11. Position of neurovascular bundles in edentule mandible.
FIGURE 10. A and B, Mandibular canal’s position in edentule (A) and dentate(B) mandible.
The Journal of Craniofacial Surgery & Volume 25, Number 3, May 2014 Intraosseous Vascularization of Mandible
* 2014 Mutaz B. Habal, MD 877
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

minimum value of hsup (2.63 mm) was recorded in the edentulouspatient (Figs. 10A, B) (Fig. 11).
The studies of Rosano et al28 and Loukas et al29 describe anaverage distance of a perforating canals from the alveolar margin of10.3 mm. This difference is related to the class of edentulism of thecohort. The medium hsup evaluated in the current study registers avalue halfway between upper and lower perforating canal distancefrom the genial apophysis in 39% of cases. If only the values ofthe upper perforating canals were considered, similar values to thoseof the studies listed above would be obtained.
Figure 4 shows the typical pattern of the trend: the distanceof the canal from the alveolar ridge decreases with the age of thepatient due to the physiological/pathological resorption of alveolarbone. This trend is not evident with chart data related to hinf becauseof substantial stability of the mandibular lower margin. The dis-tance of perforating canals from the lower margin (hinf) is, on av-erage, 10.88 (SD, 4.91) mm (range, 1.23Y19.86 mm). This value isthe same as that recorded by Vandewalle et al3 (10.6 [SD, 1.6] mm)and Gahleitner et al6 (10.0 [SD, 5.5] mm).
The choice of the implant length must then be correlated withthe presence and location of perforating canals: bicorticalism is nolonger considered a key factor,30 and data are emerging supportingthe use of short implants.31
In the study of Romanos et al,4 no differences emerged in thefrequency of perforating canals between male and female patients.
In the current study, a slightly higher occurrence inmale patients(on average, 2.3 canals for male patients) than in female patients (onaverage, 1.9 canals for female patients) was recorded.
Vandewalle et al3 suggest differences between ethnic groups.The substantial overlap of the present work’s results (Italian cohort)with thoseofVandewalle et al3 (Indian cohort) doesnot seem to supportthis hypothesis.
The presence of buccal perforating canals was also investi-gated (Figs. 12A, B). These canals appear smaller than lingual ones.The distance between these buccal vessels and the upper alveolaredge is, on average, 17.69 (SD, 3.49) mm (range, 9.90Y23.20 mm).
The anterior mandibular region has many lingual perforatingcanals, which are variable in number and position. A careful radio-graphic assessment and a surgical safeguarding of this region appearadvisable, especially of the lingual plate (there are no lingual canals inonly 2% of the cohort). Particular attention is reserved for edentulous,periodontopathic, and elderly patients: marginal alveolar bone resorp-tion causes a relative superficialization of perforating canals, increasingthe chance to intercept them during surgery. Vestibular perforatingcanals are less frequent: they do not represent a serious surgical risk (nocanal in 61% of cases).
All surgical intervention for bone grafting or placing implantsshould be preceded by a thorough radiographic analysis of the anteriormandibular region. A careful choice of implant length is required. Inrelation to the higher prevalence of vascular structures near themidlineregion, this should possibly be preserved.
REFERENCES1. Misch CM, Misch CE, Resnik RR, et al. Reconstruction of maxillary
alveolar defects with mandibular symphysis grafts for dentalimplants: a preliminary procedural report. Int J Oral Maxillofac Implants1992;7:360Y366
2. Jo J, Kim SG, Oh JS. Hemorrhage related to implant placement in theanterior mandible. Implant Dent 2011;20:e33Ye37
3. Vandewalle G, Liang X, Jacobs R, et al. Macroanatomic and radiologiccharacteristics of the superior genial spinal foramen and its bonycanal. Int J Oral Maxillofac Implants 2006;21:581Y586
4. Romanos GE, Gupta B, Crespi R. Endosseous arteries in the anteriormandible: literature review [review]. Int J Oral Maxillofac Implants2012;27:90Y94
5. McDonnell D, Reza Nouri M, Todd ME. The mandibular lingualforamen: a consistent arterial foramen in the middle of the mandible.J Anat 1994;184(pt 2):363Y369
6. Gahleitner A, Hofschneider U, Tepper G, et al. Lingual vascular canalsof the mandible: evaluation with dental CT. Radiology2001;220: 186Y189
7. Spin-Neto R, Gotfredsen E, Wenzel A. Impact of voxel size variationon CBCT-based diagnostic outcome in dentistry: a systematicreview. J Digit Imaging 2013;26:813Y830
8. De Vos W, Casselman J, Swennen GRJ. Cone-beam computerizedtomography (CBCT) imaging of the oral and maxillofacial region:a systematic review of the literature. Int J Oral Maxillofac Surg2009;38:609Y625
9. Kamburoglu K, Kolsuz E, Kurt H, et al. Accuracy of CBCTmeasurements of a human skull. J Digit Imaging 2011;24:787Y793
10. Torres MG, Campos PS, Segundo NP, et al. Accuracy of linearmeasurements in cone beam computed tomography with different voxelsizes. Implant Dent 2012;21:150Y155
11. Suomalainen A, Vehmas T, Kortesniemi M, et al. Accuracy of linearmeasurements using dental cone beam and conventional multislicecomputed tomography. Dentomaxillofac Radiol 2008;37:10Y17
12. Munetaka N, Hidetoshi A, Akiko H, et al. Morphometric analysis ofmandibular trabecular bone using cone beam computed tomography: anin vitro study. Int J Oral Maxillofac Implants 2010;25:1093Y1098
13. Maloney K, Batidas J, Freeman K, et al. Cone beam computedtomography and SimPlant Materialize Dental Software versus directmeasurement of the width and height of the posterior mandible: ananatomic study. J Oral Maxillofac Surg 2011;69:1923Y1929
14. Greenstein G, Tarnow D. The mental foramen and nerve: clinical andanatomical factors related to dental implant placement: a literaturereview. J Periodontol 2006;77:1933Y1943
15. Katakami K, Mishima A, Shiozaki K, et al. Characteristics ofaccessory mental foramina observed on limited cone-beam computedtomography images. J Endod 2008;34:1441Y1445
16. Katsumi Y, Tanaka R, Hayashi T, et al. Variation in arterial supply tothe floor of the mouth and assessment of relative hemorrhagerisk in implant surgery. Clin Oral Implants Res 2013;24:434Y440
17. Mason ME, Triplett RG, Alfonso WF. Life-threatening hemorrhagefrom placement of a dental implant. J Oral Maxillofac Surg1990; 48:201Y204
18. Woo BM, Al-Bustani S, Ueeck BA. Floor of mouth haemorrhageand life-threatening airway obstruction during immediate implantplacement in the anterior mandible [published online ahead of printJuly 7, 2006]. Int J Oral Maxillofac Surg 2006;35:961Y964
19. Lustig JP, London D, Dor BL, et al. Ultrasound identification andquantitative measurement of blood supply to the anterior part of themandible. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2003;96:625Y629
20. Eiseman B, Johnson LR, Coll JR. Ultrasound measurement ofmandibular arterial blood supply: techniques for defining ischemia in the
FIGURE 12. A and B, Vestibular canal in three-dimensional mask (A) andradiographic (B) cross section.
Di Bari et al The Journal of Craniofacial Surgery & Volume 25, Number 3, May 2014
878 * 2014 Mutaz B. Habal, MD
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

pathogenesis of alveolar ridge atrophy and tooth loss in the elderly?J Oral Maxillofac Surg 2005;63:28Y35
21. Braun P. Quelque points d’anatomie sur la vascularization arterelles dumaxillaire inferieur. Rev Odontostomatol (Bordeaux) 1955;13:98
22. Castelli WA, Najlet CE, Diaz Perez R. Interruption of the arterial inferioralveolar flow and its effect on mandible collateral circulation anddistal tissue. J Dent Res 1975;54:708Y715
23. Romanos GE, Gupta B, Davids R, et al. Distribution of endosseousbony canals in the mandibular symphysis as detected with conebeam computed tomography. Int J Oral Maxillofac Implants2012;27: 273Y277
24. Hofschneider U, Tepper G, Gahleitner A, et al. Assessment of the bloodsupply to the mental region for reduction of bleeding complicationsduring implant surgery in the interforaminal region. Int J Oral MaxillofacImplants 1999;14:379Y383
25. Liang X, Jacobs R, Lambrichts I, et al. Lingual foramina on themandibular midline revisited: a macroanatomical study. Clin Anat2007; 20:246Y251
26. Tepper G, Hofschneider UB, Gahleitner A, et al. Computed tomographicdiagnosis and localization of bone canals in the mandibularinterforaminal region for prevention of bleeding complications duringimplant surgery. Int J Oral Maxillofac Implants 2001;16:68Y72
27. Longoni S, Sartori M, Braun M, et al. Lingual vascular canals of themandible: the risk of bleeding complications during implant procedures.Implant Dent 2007;16:131Y138
28. Rosano G, Taschieri S, Gaudy JF, et al. Anatomic assessment ofthe anterior mandible and relative hemorrhage risk in implant dentistry:a cadaveric study. Clin Oral Implants Res 2009;20:791Y795
29. Loukas M, Kinsella CR Jr, Kapos T, et al. Anatomical variation inarterial supply of the mandible with special regard to implant placement.Int J Oral Maxillofac Surg 2008;37:367Y371
30. Givol N, Chaushu G, Halamish-Shani T, et al. Emergency tracheostomyfollowing life-threatening hemorrhage in the floor of the mouthduring immediate implant placement in the mandibular canine region.J Periodontol 2000;71:1893Y1895
31. Karthikeyan I, Desai SR, Singh R. Short implants: a systematicreview. J Indian Soc Periodontol 2012;16:302Y312
The Journal of Craniofacial Surgery & Volume 25, Number 3, May 2014 Intraosseous Vascularization of Mandible
* 2014 Mutaz B. Habal, MD 879
Copyright © 2014 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Related Documents











