Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know when to suspect an ICH. Know the necessary immediate medical management. Be aware of the common early complications of ICH. Hypertensive hemorrhage Amyloid angiopathy Hemorrhagic conversion of CVA Vascular malformation/ Aneurysm/ Cavernoma Hemorrhagic tumor Subdural hematoma Venous sinus thrombosis

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Intracranial Hemorrhage � What Do Need to Know?
Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado
Objectives � Know the common types of ICH. � Know how they can be differentiated. � Know when to suspect an ICH. � Know the necessary immediate medical
management. � Be aware of the common early
complications of ICH.
� Hypertensive hemorrhage � Amyloid angiopathy � Hemorrhagic conversion of CVA � Vascular malformation/ Aneurysm/
Cavernoma � Hemorrhagic tumor � Subdural hematoma � Venous sinus thrombosis

Diagnosis � SUSPECT ICH WHEN---
� Headache that is prominent complaint. 80% with ICH and only 25%with ischemic CVA
� Among patients who can respond, 85% with aneurysmal SAH report sudden onset of the worst headache of their lives!
� Nausea and vomiting 50% with ICH and 2% with ischemic CVA
� Decreased level of consciousness-
� These symptoms reflect increased intracranial pressure and are common to all types of ICH
Diagnosis ICH � CT will identify and help classify the ICH
etiology. Each ICH type has a recognizable pattern. � HTN- Small/end vessel (perforators) or
microaneuryms (Charcot-Bouchard) The bleeds are commonly located in Putamen, Thalamus, Pons, Cerebellum.
� Amyloid Angiopathy- Protein deposition in small to medium cortical and leptomeningial vessels. (Not associated with systemic amyloidosis.) These bleeds tend to be more cortically located.
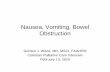
HTN Hemorrhage Location
Neurosurg Focus 15(4): Article 1; 2003

Hypertensive Stroke
Hypertensive Stroke
Cerebral Amyloid Angiopathy � Can present single or mulitple spontaneous
intracerebral hemorrhages or as progressive dementia.
� Usually in patients >60 years of age, thereafter increasing prevalence.
� Younger patients in familial types. � Correlation with Alzheimer Disease? � 30-40% recurrence rate on intracerebral
hemorrhage � Hemorrhage usually in frontal or parietal cortical or
subcortical matter. Infrequently in basal ganglia, cerebellum or brain stem.
EMedicine.com

Amyloid Angiopathy
Hemorrhagic transformation of ischemic CVA � Occurs in about 10% � 2 types petichial or parenchymal
� Petichial more common confined to the area of ischemia this may be due to leakage of blood cells through damaged capillaries without frank vessel rupture
� Parenchymal hematomas are more likely due to vessel rupture and are larger

Hemorrhagic MCA infarct
Subarachnoid Hemorrhage � 42 year old woman presents to clinic with history of sudden
onset of the worst headache of her life 2 days ago. � Headache largely resolved. � Sentinel headaches as high as 20%. � Ask about associated symptoms- Increased ICP and
meningismus. nausea/vomiting 77% stiff neck- 35%, photophobia brief loss of consciousness- 53% focal neurologic deficits including the cranial nerves radicular type leg pains or back pain

Work up for SAH � CT scan reliable within first 3 days, the earlier
the better. But even if done within first 48 hours may miss up to 5%.
� With a negative CT but a suspicious history or exam -> CTA or LP. CTA should reliably identify aneurysms above 2 mm in size. Role of CTA varies by institution.
� Role of lumbar puncture varies by institution but recommended if CT negative and history is concerning. � Presence of xanthrocromia
Subarachnoid
SAH/ CTA

Case 1
Hemorrhagic Tumor
Treatment � Hurry! � Treatment requires the same vigilance as the
ischemic strokes being evaluated for tPA. � 73% will increase in size over 3 hours. � Up to 38% have hematoma expansion > 1/3
on repeat CT within 3 hours! Size matters! � Mortalities range for 35-52% � Approximately half in the first 48 hours!
Coagulopathies
� Patients taking oral anticoagulants (OACs) � 12% to 14% of patients with ICH � Goal is to get INR to 1.4 within 2 hours
� Patients with qualitative or quantitative platelet abnormalities. Goal is >100,000
� Recognition of an underlying coagulopathy provides an opportunity to target correction in the treatment strategy, Xa inhibitors and direct thrombin inhibitors

Review of Coagulation Cascade 22
Reversal of Oral Anticoagulants: Warfarin � Vitamin K antagonist
� inhibits coagulation factors II, VII, IX and X � Half-life: 20-60 h (variable) � Urgent reversal à reduce mortality, limit
hemorrhage expansion and improve outcomes � Goal INR <1.5
� Reversal Agents: � Vitamin K (IV > PO > subq) � FFP � 4-factor PCC (Kcentra)
Neurocrit Care. 2016; 24:6-46
23
Direct Xa Inhibitors Xa Inhibitor Half-life
Rivaroxaban (Xarelto)* 5-9 h, 11-13 h in elderly
Apixaban (Eliquis) 8-12 h
Edoxaban (Savaysa) 10-14 h
Fondaparinux 17-20 h *DH preferred DOAC
} No reversal agent currently available } Andexanet alpha
} Consider 4-PCC 1500 units } No standard dose recommendation in
literature } Doses up to 50 units/kg Neurocrit Care. 2016; 24:6-46
24

Reversal of Oral Anticoagulants: Direct Thrombin Inhibitor
� Dabigatran (Pradaxa) � Half life: 12-17h � Lab test: n/a
� Consider INR, aPTT, Thrombin Time, ACT
� Reversal Agent: Idarucizumab (Praxbind) � Monoclonal antibody that binds free and thrombin-bound
dabigatran � Onset: Immediate � Duration: at least 24 hours � Dosing: 5g IVP over 10 minutes (available as 2.5g in 50mL
vials)
Neurocrit Care. 2016; 24:6-46. Dabigatran Package Insert. 2015
25
Seizure Prophylaxis � 2010 guidelines recommended against it but there has been no
change in use. � Levetiracetum- fewer side effects- Study showed that dilantin
associated with worse outcomes at 3 months but not levetiracetum. Some studies with it showing improved cognitive outcomes at discharge and fewer seizures.
� Typical dose 500 BID
� Taylor S, Heinrichs RJ, Janzen JM, Ehtisham A. Levetiracetam is associated with improved cognitive outcome for patients with intracranial hemorrhage. Neurocrit Care. 2011;15:80-84
� Szaflarski JP, Sangha KS, Lindsell CJ, Shutter LA. Prospective, randomized, single-blinded comparative trial of intravenous levetiracetam versus phenytoin for seizure prophylaxis. Neurocrit Care. 2010;12:165-172
Xa Inhibitors � Andexxa-4 Ongoing multicenter trial � Bind Xa inhibitors so they cannot interact
with Factor Xa

Blood Pressure
� Blood pressure (BP) is frequently ( often markedly) elevated in patients with acute ICH � Stress activation of the neuroendocrine system
� Sympathetic nervous system � Renin-angiotensin axis � Glucocorticoid system
� Increased intracranial pressure � Hypertension may contribute adverse outcomes
due to � Hematoma expansion- There is more than double the risk
of death and dependency in patient with SBP > 140-150 range in the first 12 hours.
� Perihematoma edema
Blood Pressure
� Blood pressure (BP) is frequently ( often markedly) elevated in patients with acute ICH � Stress activation of the neuroendocrine system
� Sympathetic nervous system � Renin-angiotensin axis � Glucocorticoid system
� Increased intracranial pressure � Hypertension may contribute adverse outcomes
due to � Hematoma expansion- There is more than double the risk
of death and dependency in patient with SBP > 140-150 range in the first 12 hours.
� Perihematoma edema
Treatment of SAH � All the same considerations apply.
� Treat intracracranial pressure � Control blood pressure � Reverse any coagulopathy
� Prevent Re-Bleed/ secure the aneursym ASAP � Clipping of coiling

Generic ICH orders � Q 1 hour neuro checks- tell the nursing staff what
you are looking for. � Remember that agitation and increases in BP are
early signs of increased intracranial pressure. � HOB 30 degrees � Control BP generally < 140 systolic � Correct coags ASAP � Prophylaxis for seizure Kepra (lobar bleeds) � treat fevers � Fluids/O2 to maintain normal status
When things are going badly � Neurologic decline
� Protect airway/ control BP � Expansion of the clot #1 MUST REPEAT A CT
SCAN � Seizure � Hydrocephalus � Vasospasm � Other metabolic
Obstructive Hydrocephalus

Craniotomy and supratentorial hematoma evacuation
Cochrane Database of Systematic Reviews 2007 Issue 2
Case 1 � HPI: 67 y.o. man in A fib on Xeralto,
presents to ED with history of headaches for 2 days and trouble with vision.
� PMHx: A fib, HTN,
� PE: headache not severe � 189/100, HR 87 � A & O X3, no motor or sensory deficits � Right homonymous hemianopsia
Case 1

Case 1 � Immediate management?
� While in ED develops significant decline in mental status?
� Treatment? Additional work-up?
Case 1
Case 2 � HPI: 74 y.o. man with artificial valve,
pacer, DM, HTN, OSA on coumadin. Had a fall about a month ago without LOC. Has progressively increasing headaches and balance problems. Fell twice over last week.
� PE: A & O X 3, headache 5/10, pronation with LUE, otherwise intact

Case 2
Case 2
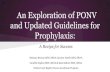
Case 3 • 32 y.o. female with sudden onset of left arm
weakness and poor coordination 12 hours prior to admission. Sx’s relatively stable since.
• (+) history of HA starting 3-4 days ago “like a band across my forehead”. HA slowly progressive over last 24 hours with onset of nausea, stiff neck and photophobia.
• Seen in outside ER with CT scan

CT (+) Gad
Related Documents