44.3 Intracranial tumours Oxford Textbook of Surgery 44.3 Intracranial tumours Jeffrey J. Olson, Daniel L. Barrow, Mark R. Gilbert and Nelson Oyesiku Tumors of the nervous system Introduction Primary brain tumors Glioblastoma multiforme and anaplastic astrocytoma Astrocytoma Oligodendroglioma and anaplastic oligodendroglioma Ependymoma Medulloblastoma Neuronal and mixed neuronal and glial tumors: ganglioglioma and neurocytoma Tumors of the skull base that arise separately from the nervous system General comments

Intracranial Brain Tumor
Oct 31, 2015
intrakranial brain tumor
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
44.3 Intracranial tumours
Oxford Textbook of Surgery
44.3 Intracranial tumours
Jeffrey J. Olson, Daniel L. Barrow, Mark R. Gilbert and Nelson Oyesiku
Tumors of the nervous system
Introduction
Primary brain tumors
Glioblastoma multiforme and anaplastic astrocytoma
Astrocytoma
Oligodendroglioma and anaplastic oligodendroglioma
Ependymoma
Medulloblastoma
Neuronal and mixed neuronal and glial tumors: ganglioglioma and neurocytoma
Tumors of the skull base that arise separately from the nervous system
General comments
Chordoma
Esthesioneuroblastoma
Nasopharyngeal carcinoma
Glomus tumor
Neurofibromas and schwannomas
Neurofibromatosis
Diagnosis
Treatment
Pineal tumors
Introduction
Clinical presentation
Diagnosis
Tumor types
Treatment
Meningiomas and choroid plexus tumors
Meningiomas
Choroid plexus tumors
Pituitary tumors
Clinical problems
Diagnosis and treatment
Endocrine-inactive tumors
Prolactinomas
Acromegaly
Cushing disease
Gonadrotropin-secreting adenomas
TSH-secreting adenomas
Future directions in pituitary surgery
Intracranial epidermoid tumors
Craniopharyngioma
Brain metastases
Introduction
Diagnostic evaluations
Treatment
Outcome
Primary lymphoma of the central nervous system
Introduction
Diagnosis
Management
Further reading
Tumors of the nervous system
Introduction
General classification
Neoplasms of the nervous system are a very heterogeneous group of diseases. Though often grouped together in one discussion, the range of surgical techniques used to deal safely and effectively with the variety of tissue consistencies, anatomic locations, and adjacent tissues is necessarily extensive and provides some of the greatest challenges in neurosurgery. The World Health Organization (WHO) classification allows one to see this more directly. The summary in Table 1 demonstrates the various types and sites of origin of these lesions.Table 1 New information on cytogenetics, molecular biology, and proliferative capacity offers to extend our appreciation of the differences in the origin and progression of brain tumors. Though many other classifications are available, the discussions below will rely primarily on the WHO system. Consistent usage of classifications allows comparison between reports of different series and coherent discussions of lesions between clinicians.

Table 1 Histologic classification of tumors of the central nervous system
The WHO classification refers to primary brain tumors as those that arise from the cells of the central nervous system. Brain tumors are a small component of cancer overall, with an autopsy frequency of 1 to 2 per cent. The neuroepithelial tumors are those of the glia and neurones; they account for 50 to 60 per cent of primary intracranial tumors in adults. Of these, the relative incidence of tumor types is: glioblastoma 50 per cent, anaplastic astrocytoma 30 per cent, oligodendroglioma 6 per cent, nonanaplastic astrocytoma 5 per cent, ependymal tumor 4 per cent, medulloblastoma 2 per cent; the neurocytomas, pineal-cell tumors, subependymal giant-cell tumors, pilocytic astrocytomas, and choroid plexus tumors account for 1 per cent or less each. Meningiomas comprise about 20 per cent of intracranial tumors. Overall, metastases account for approximately one-half of all intracranial neoplasms.
Initial management
More often than not, the individual with a tumor affecting the nervous system presents to the physician they consider their primary caregiver, be they a family physician, internist, or surgeon. The majority present with new neurologic deficits, changes in mental status, headaches, or deformities that are gradual in onset, often over days to months, as is described in greater detail below. An example of a more urgent presentation would in the emergency room after a new seizure. The initial steps in the management of these patients are important. In each of them a simple neurologic exam will guide further evaluation. Imaging studies of the appropriate portion of the central nervous system are based on the findings of the physical examination and history. Where obtundation, rapidly progressive deficits, or difficulty in controlling seizures are present, admission to hospital is necessary. If images show a significant mass effect and this appears to be due to vasogenic edema, corticosteroids, usually in the form intravenous dexamethasone, are begun. H2-blockers are started prophylactically. When seizures are present, anticonvulsants such as phenytoin or phosphenytoin are begun. Where the individual cannot drink or eat, intravenous fluids with half-normal saline are necessary. Free water or dextrose in water is not advisable, as these may enhance brain edema. The majority of patients are neurologically stable and their admission is unnecessary. Oral corticosteroids, H2-blockers, and anticonvulsants can be used in preference to intravenous preparations. Whether or not admission is required, a key component in early management is to find a neurosurgeon or neurologist willing to manage the patient's immediate problems and plan methods of diagnosis and treatment.
Aspects of clinical presentation

Because of the diversity of these lesions, blanket statements about their signs and symptoms cannot be made. In general, though, symptoms arise from malfunction of that part of the nervous system where the tumor is arising or from compression of adjacent structures. The common general symptoms at presentation include changes in mental status, headaches, vertigo, dizziness, and alteration of level of consciousness. Changes in mental status, such as altered concentration, memory, affect, personality, initiative, abstract reasoning, and confusion, are often indolent and may occur in 15 to 20 per cent of patients with brain tumors at presentation. Other symptoms, such as weakness, sensory changes, visual abnormalities, aphasias, gait instability and focal seizure activity, are examples of symptoms that have localizing value. Approximately 10 to 20 per cent of adults with the new onset of seizures have brain tumors.
Headache is not universal in those with brain tumors. Contrary to popular expectation, only 70 per cent of patients with primary brain tumors will have a headache of some sort at the time of diagnosis: in 35 per cent it the first symptom; only about 15 per cent have all of the usual characteristics of headache supposedly related to raised intracranial pressure, such as increased intensity in the morning, association with nausea, exacerbation by postural change, and pain that arouses one from sleep.
General diagnostic methods
The clinical examination yields clues to the localization of a lesion within the central nervous system but falls short of providing the detailed information necessary to plan a surgical approach. Visualization of central nervous tumors is centered around computed tomography (CT) and magnetic resonance imaging (MRI). Where the presentation is a precipitous decline in neurologic status, suggesting acute hydrocephalus or intracranial hemorrhage, a CT scan is indicated. Once these patients have been stabilized, and in most others who have a more gradual onset of symptoms, MRI without and with contrast-enhancing agents will yield the most information about the lesion. The multiplanar representation of the lesion seen in various imaging sequences allows the surgeon to appreciate the tumor mass, its surrounding edema, and its relation to normal structures.
Angiography can be of use in selected circumstances: these include preoperative evaluation of tumor vasculature, the assessment of normal arterial and venous anatomy adjacent to or within the tumor, preoperative embolization, and ruling out the presence of arteriovenous malformations and aneurysms in patients presenting with hemorrhage. Other diagnostic techniques, such as electroencephalography, positron-emission tomography and nuclear brain scanning, do not often assist the surgeon in determining how to proceed. Although imaging studies are of great value in localizing the lesion, actual diagnosis is dependent on obtaining adequate tissue for histologic evaluation. Studies that can be diagnostic include cytology of cerebrospinal fluid and endocrine evaluation, which may be diagnostic in carcinomatosis metastatic to the central nervous system and pituitary adenoma, respectively.
Primary brain tumors
In adults the most common form of primary brain tumor, known as the glioblastoma multiforme, is also the most malignant. Less commonly encountered is the anaplastic astrocytoma, which is not as aggressive but is still ultimately lethal. The astrocytoma and oligodendroglioma are more indolent, but could be considered benign with malignant potential as they often go on to devastating

progression years after diagnosis. The less common histologic types must be recognized, as some have extraordinarily benign courses while others require aggressive intervention to obtain even temporary control.
The discussions of the tumors below include aspects of management beyond surgery alone. Because many brain tumors require surgical intervention or at least surgical decision-making, a neurosurgeon will often supervise the overall care of these patients. Thus, the neurosurgeon must be familiar with all the aspects of their care.
Glioblastoma multiforme and anaplastic astrocytoma
Clinical presentation
The glioblastoma multiforme is generally a rapidly growing lesion that makes itself known by causing malfunction of the central nervous system at its site of origin and, because it can attain significant size rapidly, by compression of surrounding normal tissue. The less common anaplastic astrocytoma may be somewhat slower in its proliferation, but often has a similar set of presenting characteristics. In contrast to the neurologic deficits from processes such as ischemia, the onset of which is relatively sudden, those from brain tumors tend to be gradually progressive. Fewer than 20 per cent of patients have had symptoms for less than 1 month and fewer than 10 per cent for longer than a year. Symptoms of increased intracranial pressure, including lethargy, confusion, headache, nausea and vomiting, may be the first presentation. On neurologic examination the site of origin can sometimes be discerned. For example, a lesion arising in the left frontal lobe may be associated with expressive aphasia and a right hemiparesis. A lesion of the temporal lobe may present with seizure activity and a superior quadrantanopia. Parietal lesions can be subtle, with only minor cognitive abnormalities and contralateral sensory changes. Occipital lesions are almost always associated with some degree of deficit in the visual field, even if not appreciated by the patient. Lesions of the diencephalon, brainstem, and cerebellum may be symptomatic when small because of the compact nature of the functionally important neurones and fibers in these regions. Increased intracranial pressure can be discerned by ophthalmoscopic examination to determine whether or not papilledema is present. Seizures are an occasional mode of presentation in these more malignant tumors, but not so frequently as with less aggressive types of the same family of tumors. These symptoms and signs are not pathognomonic for brain tumors, but rather signify the presence of any destructive or mass-producing intracranial lesion. One must keep in mind that, in the appropriate clinical setting, brain abscess, inflammatory disease, or even ischemia can produce such a presentation.
Diagnosis
The clinical examination is an interesting and rewarding exercise in neurologic localization but will not necessarily be diagnostic by itself. In a patient with objective signs of neurologic changes and/or increased intracranial pressure, MRI is the optimal method for characterizing the anatomy of the lesion. The glioblastoma multiforme tends to have the more bizarre appearance, with irregularly enhancing margins, cystic and necrotic areas associated with mass effect, and varying amounts of edema (Fig. 1). Anaplastic astrocytomas can have any of these characteristics but are, in general, more homogeneous in appearance. Importantly, it is not uncommon to see an anaplastic astrocytoma with no contrast enhancement (Fig. 2). Thus enhancement by itself is not the essential
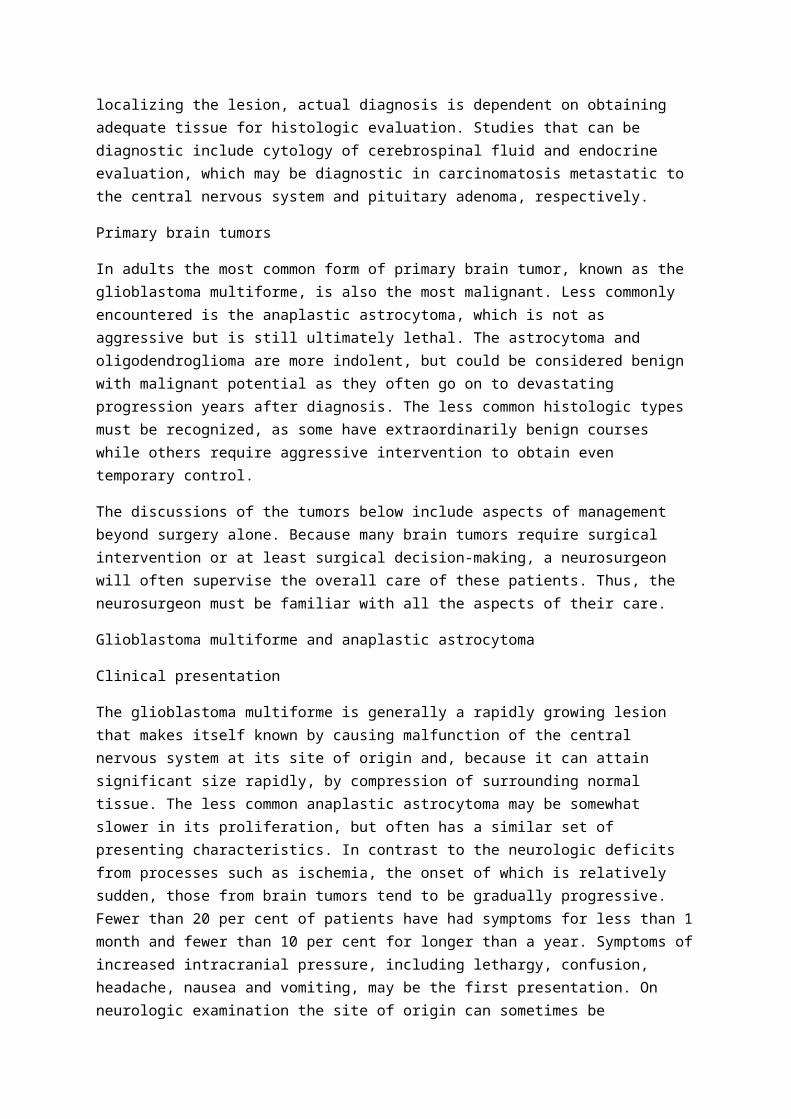
feature of malignancy. As mentioned above, some individuals will present with sudden changes in consciousness, or new seizure activity. In these cases CT will be the most useful in determining if the process needs emergency surgical or medical intervention. Angiography, electroencephalography, and imaging based on radionuclides rarely provide information that alters the surgical approach or subsequent therapy. Lumbar puncture is rarely diagnostic and, especially when increased intracranial pressure is shown by imaging, may be dangerous. Ultimately, diagnosis is based on histologic evaluation, in which the WHO system serves as the standard. The presence of necrosis differentiates glioblastoma from anaplastic astrocytoma. In recurrent masses in patients who have had radiation therapy, positron-emission tomography may assist in differentiating tumor recurrence from radiation necrosis. The most common histologic correlate is the presence of necrosis within the lesion, though some grading systems outside of the standard WHO system may allow this diagnosis to be made without the presence of necrosis. When there is mesenchymal differentiation within the lesion, the tumor may be designated a gliosarcoma (Fig. 3); these sometimes may actually follow a more aggressive course than glioblastoma.
Fig. 1. Glioblastoma multiforme. Axial T1-weighted gadolinium-enhanced MRI showing a right temporo-occipital lesion with irregular rim enhancement, central hypointensity suggestive of necrosis, and edema extending anteriorly into the temporal lobe. The two apparent components of this tumor on this image merged lower in the temporal lobe.
Fig. 2. Anaplastic astrocytoma. (a) Axial T1-weighted gadolinium-enhanced MRI demonstrating a right mesial frontal mass with faint gyriform enhancement and decreased signal intensity of the associated gyral white-matter tracts. (b) Axial FLAIR (TR 7000,TE 130) MRI better demonstrating the edema and infiltrative nature of this lesion, with involvement of not only the corpus callosum but also the left frontal lobe.
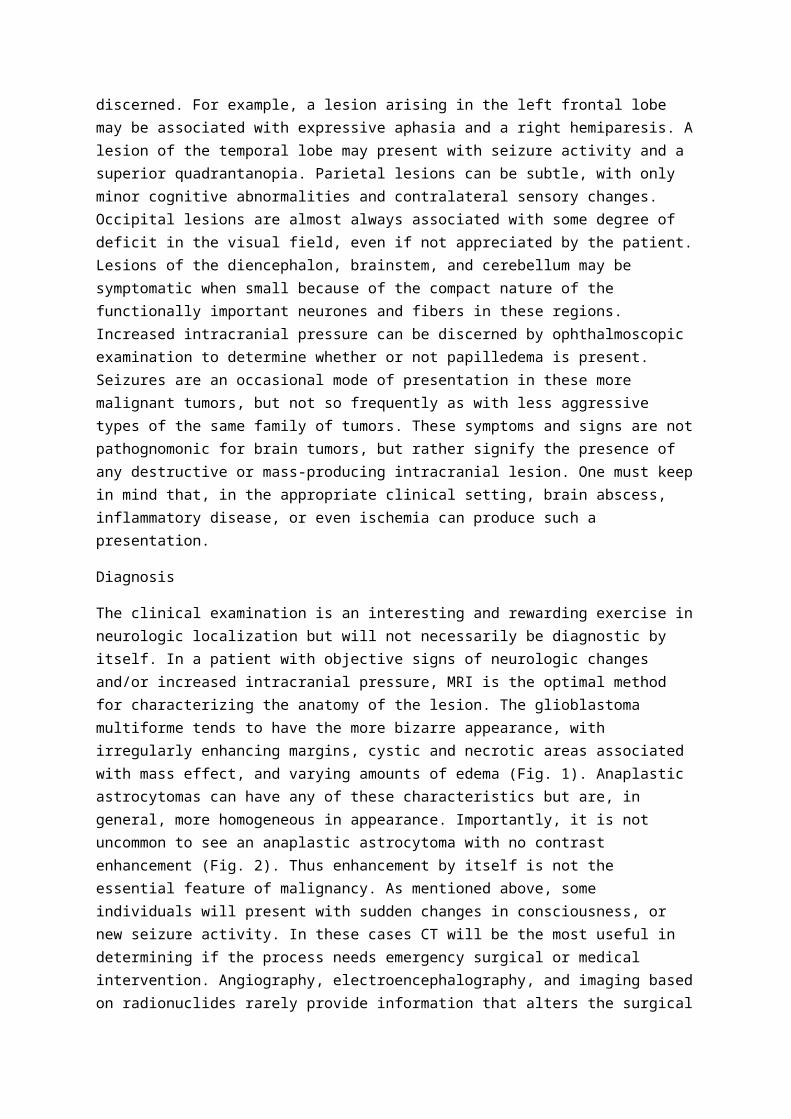
Fig. 3. Gliosarcoma. Axial T1-weighted gadolinium-enhanced MRI of a left parieto-occipital tumor with mass effect on the corpus callosum and obliteration of the normal contours of the lateral ventricle on that side. There is an irregular rim of enhancement with decreased central signal, suggestive of extensive necrosis. The radiographic appearance is similar to that of glioblastoma.
Treatment
Though various therapies are available for these difficult lesions, it is important for the surgeon to recognize that the most important prognostic factors for survival are the histology of the tumor, the patient's age, and their performance status at the time of diagnosis. Knowing this helps the surgeon keep the risks and benefits of the proposed therapies in proper perspective.
Upon finding an intracranial lesion that one suspects is a tumor it is the surgeon's responsibility to obtain a diagnosis and, when necessary and deemed safe, decompress surrounding normal tissue. Small lesions without mass effect and lesions in the thalamus, hypothalamus, and upper brainstem can usually be diagnosed safely with stereotactic methods. The needle-biopsy specimens can be informative, with the key to success with these procedures being an experienced neuropathologist. Lesions compressing the surrounding normal tissue that contain significant cystic fluid, necrotic material, or solid tumor can benefit from craniotomy and resection. It is with the resection of the margins, where visually imperceptible infiltration into the normal tissue occurs, that new neurologic deficits are most likely to be induced. Measures to maximize the accuracy of tumor identification and avoid entering the adjacent normal tissue include the use of awake craniotomy, preoperative electrocorticography, intraoperative sensory-evoked potentials for mapping, image-guided surgical techniques, and frame-based stereotactics. Standard bipolar cautery and suction account for most of the resection in these lesions, but speed can be added by the judicious use of ultrasonic dissection devices. It is important to maintain hemostasis as the resection proceeds and to confirm it upon completion of the resection of all tissues that can be clearly identified as tumor. The surgeon must keep in mind that cure is not possible with surgery alone. Though, under selected circumstances, outcome is associated with the degree of resection, the primary goal of surgery is to obtain diagnosis and decompression.

External radiation is the single most effective form of therapy for these lesions. Multifractioned X-irradiation in fractions of 1.8 to 2 Gy/day to a total dose of approximately 60 Gy to primary region of the tumor can usually be offered to all individuals with this diagnosis. Toxicity does occur and needs to be balanced with prognosis. Radionuclide brachytherapy and stereotactic radiation can be used as additional methods of treatment for recurrent tumors.
Cytotoxic chemotherapy has a role in the treatment of these tumors, particularly in newly diagnosed cases in younger individuals with good performance status. No single agent has demonstrated anything near curative potential, but BCNU (carmustine; 1,3-bis(2-chloroethyl)-1-nitrosourea) and cisplatin have reliable, though small, response profiles in glioblastoma multiforme. For anaplastic astrocytoma a combination of procarbazine, CCNU (lomustine; 1-(2-chloroethyl)-3-cyclohexyl-nitrosourea), and vincristine has been advocated, but prospective data suggest that the ability of this combination to add value to radiation may be limited. In selected cases these agents may have a greater impact when given before, rather than during or after, radiation. On recurrence, the implantation of biodegradable polymers that release BCNU into a tumor bed may augment the value of surgical debulking.
Because these standard forms of therapy are associated with poor prognosis, this group of patients has provided fertile ground for investigational treatment agents and routes of administration. A wide variety of alternative cytotoxic agents has been evaluated, demonstrating no clear advantage over the agents mentioned above. Treatments based on molecular biologic information and using immunologic agents, biologic-response modifiers, RNA (oligonucleotides), and DNA (genes or fragments thereof) are under active study. It is encouraging that patients with glioblastoma had a three times greater 5-year survival (12 per cent compared to 4.5 per cent) when treated as part of an investigative rather than standard protocol.
It must be kept in mind that these lesions are frequently heterogeneous histologically, with some areas appearing relatively low grade while others are completely consistent with glioblastoma multiforme. It is recommended that the lesion be treated as indicated by its most aggressive-appearing portion.
The surgeon must become an advocate for the patient's best interests. Knowing the patient's age, overall health, and the tumor's location and probable histologic type, the surgeon can inform the patient and the family about treatment options and the likelihood of side-effects and success.
Upon completion of treatment, vigilance is necessary to detect recurrence or progression. Neurologic examination and imaging, usually MRI without and with gadolinium-based contrast agents, should be performed at regular intervals.
Astrocytoma
Clinical presentation
The growth pattern of these lesions tends to be more indolent than that of their more malignant counterparts. Because of this, the brain may be more tolerant of their presence and this alters their presentation. Rather than symptomatic increases in intracranial pressure and focal neurologic deficits, generalized or focal seizures are a much more common form of presentation. Seizure

activity may antedate the clinical diagnosis by months or years. Gradually progressive cognitive changes can also develop and signal the presence of astrocytoma.
Diagnosis
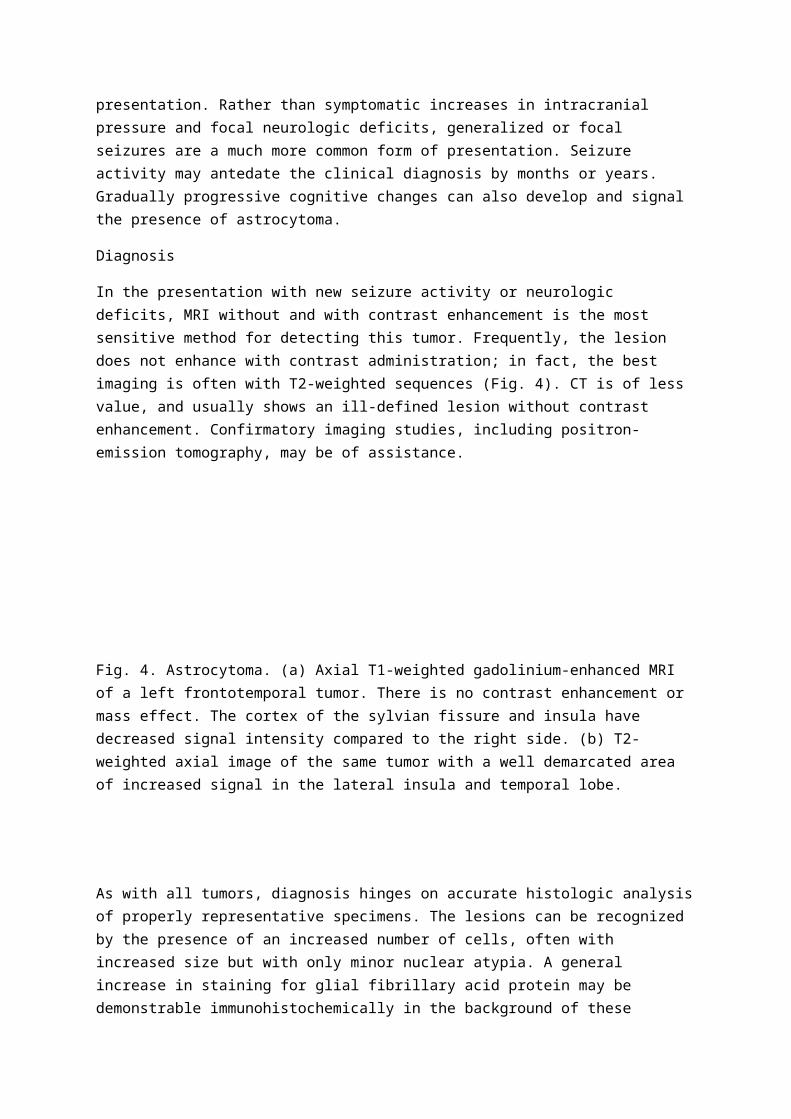
In the presentation with new seizure activity or neurologic deficits, MRI without and with contrast enhancement is the most sensitive method for detecting this tumor. Frequently, the lesion does not enhance with contrast administration; in fact, the best imaging is often with T2-weighted sequences (Fig. 4). CT is of less value, and usually shows an ill-defined lesion without contrast enhancement. Confirmatory imaging studies, including positron-emission tomography, may be of assistance.
Fig. 4. Astrocytoma. (a) Axial T1-weighted gadolinium-enhanced MRI of a left frontotemporal tumor. There is no contrast enhancement or mass effect. The cortex of the sylvian fissure and insula have decreased signal intensity compared to the right side. (b) T2-weighted axial image of the same tumor with a well demarcated area of increased signal in the lateral insula and temporal lobe.
As with all tumors, diagnosis hinges on accurate histologic analysis of properly representative specimens. The lesions can be recognized by the presence of an increased number of cells, often with increased size but with only minor nuclear atypia. A general increase in staining for glial fibrillary acid protein may be demonstrable immunohistochemically in the background of these lesions. Three histologic patterns of astrocytoma may be seen, termed fibrillary, gemistocytic, and protoplasmic. Based on autopsy and retrospective clinical series, as many as half of all astrocytomas may have a malignant or anaplastic component at the time of diagnosis. Two-thirds will go on to recur, with clinical behavior and a pathologic appearance consistent with malignancy. The molecular events associated with this progression are under active investigation and appear to include loss of chromosome 19q or 10. Additionally, loss, alteration, or amplification of platelet-derived growth factor, retinoblastoma protein, and even epidermal growth factor may be steps on the way to anaplastic change in an astrocytoma.
The juvenile pilocytic astrocytoma is not commonly seen in adults, and when found is often associated with good prognosis. Astrocytomas may be mixed in the sense that they can have a combination of astrocytic and oligodendroglial cells. In mixed tumors, prognosis is dependent on the most aggressive component. Variants are recognized, such as the pleomorphic xanthoastrocytoma, a tumor usually occurring superficially in the cerebrum, with pleomorphic neoplastic astrocytes, some of which have lipid inclusions. Though the cells of the pleomorphic xanthoastrocytoma appear

aggressive, the prognosis is better than for anaplastic astrocytoma. The subependymal giant-cell astrocytoma arises almost exclusively in tuberous sclerosis.
Treatment
Although these lesions may be discovered by imaging, a tissue diagnosis is still obligatory in most cases for the most accurate possible prediction of prognosis. No prospective analysis of the extent of surgical resection is available to guide the surgeon in making a decision to biopsy, resect subtotally, or attempt to resect completely. Thus the surgeon's judgement and experience are essential in these decisions. In lesions involving functionally important areas it is reasonable to use stereotactic biopsy to obtain a diagnosis and proceed with a treatment plan. For lesions with mass effect and in more quiescent regions of the brain, more aggressive resection can be entertained. Complete resection of small lesions seems to be associated with better tumor control. Difficult-to-control seizure activity can also be improved with resection. Whether in eloquent or silent areas of the brain, accuracy of resection can be augmented with stereotactic techniques, electrophysiologic mapping, and electrocorticography.
When a significant amount of tumor is left behind after biopsy or attempted resection, radiation therapy may be added to control the residue, but there is a risk of inducing cognitive deficits and an alternative is to delay radiation until there is objective imaging evidence of tumor progression. Where surgical resection is demonstrably complete on postoperative imaging, one option is to withhold radiation until there is objective imaging evidence of tumor progression. In a prospective study the timing of the addition of radiation, either at the time of diagnosis or of progression, did not seem to affect survival. That study, as well as retrospective reviews, provide evidence that radiation early after subtotal resection may prolong survival. Additional histologic investigation, such as on the tumor's proliferative capacity as measured by 5-bromodeoxyuridine or Ki-67 labeling, may detect more aggressive tumors and may justify the use of radiation early after incomplete resection. Chemotherapy has been investigated in the treatment of these lesions, but it has been difficult to show any benefit from its addition and it is not considered standard care. Agents under investigation that induce tumor differentiation may ultimately prove to be useful alternatives to standard cytotoxic chemotherapy.
In some of the more unusual variants, such as pleomorphic xanthoastrocytoma or subependymal giant-cell tumor, surgery with the goal of complete resection is the primary therapy, with repeat resection or radiation the options for treatment of any recurrence.
Upon completion of the initial phase of treatment, vigilance is necessary for recurrence or progression. Neurologic examination and imaging, usually MRI without and with gadolinium-based contrast agents, should be performed at regular intervals. Dedifferentiation can be expected at the time of progression. Surgery may be indicated for decompression and to determine whether the lesion has taken on the characteristics of an anaplastic astrocytoma or glioblastoma, thus guiding further treatment planning.
Oligodendroglioma and anaplastic oligodendroglioma
Clinical presentation
The oligodendroglioma arises from its myelin-producing namesake. Though of biologic interest, this fact does not seem to alter the presentation much from that of an astrocytoma. Oligodendrogliomas tend to be lesions of the frontal lobes and of younger adults (peak incidence, 26 to 46 years of age). They present more frequently with seizures and headaches than do astrocytomas. Many of these lesions may have been present for a significant period of time before becoming symptomatic. Therefore, due to the plasticity of the brain, they can occasionally attain large size without the symptoms of increased intracranial pressure. Ultimately, cognitive fall-off will occur, and headache or other focal deficits will be the reason for seeking medical attention in at least 50 per cent of patients. In some instances, possibly due to the neoplastic capillary bed, presentation may be with spontaneous intracranial hemorrhage.
The anaplastic counterpart of the oligodendroglioma can present much like the anaplastic astrocytoma. Symptoms of increased intracranial pressure are more likely to be seen here. In general, the onset of symptoms is faster than with its less aggressive counterpart. Also, focal neurologic deficits, rather than just seizures or changes in mental status, will be a part of presentation in many patients.
Diagnosis
The clinical presentation of new seizures without obvious cause in an adult justifies the use of sophisticated imaging. MRI will show these lesions well, particularly those with little or no contrast enhancement. The T2-weighted images tend to have well-delineated margins, implying that some of these lesions may be less infiltrative than their astrocytic counterparts. The oligodendroglioma has a significant propensity for calcification; this can be seen well in a CT scan, but, of itself, calcification does not differentiate oligodendroglioma from astrocytoma and therefore a search for this finding alone does not justify obtaining a CT.
A nidus of contrast enhancement in a lesion with otherwise homogeneous, nonenhancing characteristics suggests an oligodendroglioma with an anaplastic component. Cystic components as well as calcification can be seen here.
Histologic analysis of oligodendrogliomas shows monotonous fields of cells somewhat larger than normal oligodendrogliocytes, with round nuclei. Formalin-fixed tissue undergoes acute swelling and dissolution of cytoplasmic contents giving an artefactual honey-comb appearance, sometimes thought of as characteristic of this tumor type. Microcalcifications and a branching capillary network are often seen. Anaplastic lesions have a more heterogeneous cell population with frequent mitotic figures. Not uncommonly, oligodendrogliomas may be mixed with astrocytic tumor cells, termed oligoastrocytoma or mixed glioma.
Seizures are an important component of the natural history. Once the lesion has been detected by imaging, the surgeon learns little else by the addition of electroencephalography. On the other hand, patients with known residual oligodendroglioma after initial treatment who are experiencing poor seizure control may benefit from electroencephalography. Identification of a residual seizure focus in or adjacent to the tumor may indicate the need for additional resection, possibly with intraoperative electrocorticography, with the goal being seizure control.
Treatment
It has been suggested that the central component of an oligodendroglioma is more purely tumorous than that of an astrocytoma, whose infiltrative nature is more likely to encompass some normal brain. Because of this, homogeneous, nonenhancing brain lesions in safely approachable areas, consistent with oligodendroglioma, may be good candidates for surgical resection. Complete resection of these lesions, when possible, results in improved long-term control. As with the astrocytoma, a small deep lesion may best be diagnosed by stereotactic biopsy. The addition of radiation at initial diagnosis or on progression is an option that should be decided from the aggressiveness of the presentation, the amount of residual tumor, and possibly the proliferative index. When the histologic appearance is of oligodendroglioma without anaplasia and total resection is confirmed by postoperative images, careful observation with regularly spaced MRI may be warranted as follow-up management. Tumors known to be anaplastic oligodendroglioma always warrant radiation therapy.
The anaplastic oligodendroglioma does seem to have a greater propensity to grow. When this diagnosis is obtained, the use of standard or intensive doses of procarbazine, CCNU, and vincristine in addition to radiation has been advocated. Their use prior to radiation has been proposed, and documented responses have occurred. These lesions are also sensitive to radiation and this is recommended as a standard part of their treatment, whether or not chemotherapy is added.
Upon completion of treatment, vigilance is necessary for recurrence or progression. Neurologic examination and imaging, usually MRI without and with gadolinium-based contrast agents, should be performed at regular intervals.
Ependymoma
Clinical presentation
These lesions arise from the ependymal cells lining the cerebrospinal fluid-containing spaces in the central nervous system. They are relatively uncommon, accounting for about 5 per cent of tumors in the adult central nervous system and 10 per cent in children. Approximately half of these lesions develop in the first two decades of life. The majority occur in the cranium, predominantly in the posterior fossa in children and supratentorially in adults, but they are certainly seen also in the spinal canal.
Focal neurologic deficits related to the location of the lesion may occur. There may be extension into normal periventricular tissue but it is important to recognize that many of these lesions frequently extend into the ventricular system, obstructing cerebrospinal fluid dynamics and causing symptoms of hydrocephalus and increased intracranial pressure. Infratentorially, in addition to symptoms of hydrocephalus, there may be new cranial-nerve palsies or cerebellar dysfunction. Ependymoma can seed the subarachnoid space, both intracranially and along the spinal canal, and present with symptoms localizing to sites remote from that of its origin.
Primary spinal lesions, or lesions that develop by seeding from cranial lesions, tend to have indolent myelopathies. These are often painless presentations including gait instability, incoordination in the upper or lower extremities, and sensory alterations that do not follow strict dermatomal patterns. Some are associated with syrinx formation above and below the lesion, whereby the patients may have suspended sensory losses. Hyper-reflexia or clonus may be detected, as well as up-going toes

to various maneuvers. Ependymoma in the spine, particularly in the cauda equina, may be associated with pain. If the neurologic examination demonstrates any more than expected from a simple radiculopathy, then imaging studies are warranted to assess the possible presence of this neoplasm.
Diagnosis
As with other primary tumors of the central nervous parenchyma, MRI is the most sensitive method for detecting any abnormality. Symptomatic lesions can be rather small when sited near the foramen of Monroe, aqueduct of Sylvius, or foramen magnum. Any extension into the ventricular system suggests that ependymoma should be placed higher in the differential diagnosis of the lesion. Once the diagnosis is made, MRI of the spinal canal, and lumbar puncture if necessary, are indicated to look for leptomeningeal spread.
On MRI, intraspinal ependymomas tend to show a very focal expansion of the spinal cord (one to two segments) and the enhancement will be fairly intense and homogeneous (Fig. 5). In patients over 20 years of age the probability that a spinal intramedullary tumor with these findings will be an ependymoma is about 60 per cent. A more diffuse widening, with or without cystic changes and heterogeneous enhancement, suggests astrocytoma. There may be extension proximally and distally through the central canal. The myxopapillary variant of ependymoma can attain huge proportions and encompass the entire cauda equina before detection. Often, intraoperative inspection reveals that these tumors are actually arising from the conus or filum terminale.
Fig. 5. Spinal ependymoma. Sagittal T1-weighted gadolinium-enhanced image of the lumbar spine: an enhancing lesion occupying the majority of the spinal canal from L1 to L4 is associated with a cystic component in its rostral end. At surgery this lesion was found to arise at the conus and followed the filum terminale.
Treatment
Small intracranial lesions can be diagnosed by stereotactic biopsy. More often, symptoms from hydrocephalus and mass effect are present; craniotomy is then indicated for diagnosis and resection. Often the lesion can be approached through an adjacent sulcus in a functionally less important region. The site of origin must be visualized in order to attain total resection. When the lesion arises from the floor of the fourth ventricle, some may be left behind if differentiating between tumor and

normal parenchyma proves difficult and there is a chance of causing mechanical damage to the brainstem. Local radiation therapy is nearly always used as an adjuvant, with or without total resection. If histologic evidence of anaplasia is present, radiation is more strongly advised. When tumor regrowth occurs, chemotherapy with BCNU, dibromodulcitol, ifosfamide, VP-16, or platinum-based compounds has been described, though no standard regimen with a reliable response rate has been developed.
The first choice in the treatment of leptomeningeal spread is craniospinal irradiation; this is a particularly difficult option in children because of its extensive toxicity. Chemotherapy, either systemic or intrathecal, has been used in children with this form of the disease, but again, no standard regimen has been clearly established.
Primary intramedullary ependymomas of the spinal cord can be approached surgically, both for diagnosis and for decompression of the surrounding normal tissue. The surgical technique involves identification of the site where the lesion has become most superficial and its exposure via a midline myelotomy. Microscopic assistance is essential, and monitoring of somatosensory or motor-evoked potentials helps in identifying, but does not guarantee the preservation of, the functional integrity of the cord during the procedure. Piecemeal resection of these lesions from the inside out minimizes the manipulation and traction of normal tissue. Microscopic extensions of the tumor rostrally or caudally, or poorly defined extensions into the spinal cord, may not be resectable, requiring the addition of radiation in the early postoperative period or at the time of recurrence. The myxopapillary variant of these tumors, with its characteristic myxoid and mucinous background, is benign in character, found primarily in the conus, filum and cauda equina, and best treated by total surgical resection. Also, the subependymoma, usually seen in the fourth ventricle, is a low-grade lesion that, once recognized histologically, is treated surgically without additional radiation (Fig. 6).
Fig. 6. Subependymoma. (a) Sagittal T1-weighted MRI demonstrating a mass at the caudal end of the fourth ventricle extending to the top of the cisterna magna with mild mass effect on the medulla and the inferior vermis. (b) Axial T1-weighted gadolinium-enhanced MRI of a minimally enhancing lesion in the caudal fourth ventricle; note the relatively clear delineation of the tumor from the floor of the fourth ventricle.
Medulloblastoma
Clinical presentation

Seventy per cent of medulloblastomas occur in individuals younger than 16 years of age. The peak occurrence is at 7 years of age. In adults, 80 per cent develop between 21 and 40 years of age, and more often in men than women. Medulloblastoma is the most common and best characterized of the primitive neuroectodermal tumors. It is most often a lesion in the midline of the posterior fossa, involving the vermis, and inducing symptoms of increased intracranial pressure, such as headaches, nausea, occasional vomiting, and lethargy, by its shear size and sometimes from hydrocephalus. Also, symptoms due to cranial-nerve, brainstem or cerebellar malfunction, such as diplopia, altered facial motion and sensation, difficulty with swallowing, ataxia or dysmetria, may occur. Because of their malignant nature, medulloblastomas tend to show symptoms that have been present over a period of only weeks to months.
Diagnosis
In patients with symptoms of cerebellar, cranial-nerve, and brainstem malfunction and/or increased intracranial pressure suggesting disease of the posterior fossa, MRI with and without gadolinium or CT with and without contrast are indicated. Medulloblastomas are generally solid, intensely enhancing lesions, in or adjacent to the vermis, and compressing the surrounding normal tissue. As the age of patient at presentation increases, there is the likelihood of greater involvement of the cerebellar hemispheres. Images confirm the presence of a lesion in the posterior fossa that appears to be relatively separate from the cerebellum itself. Additionally, approximately one-third of patients will have nodular or diffuse leptomeningeal and ependymal spread at the time of diagnosis. Because of this, proper treatment planning requires that all patients with this diagnosis should have spinal imaging to look for leptomeningeal spread and cytologic sampling of cerebrospinal fluid if the imaging is negative. In younger patients, systemic involvement is not uncommon and bone-marrow studies are indicated.
Treatment
Surgery for diagnosis and the relief of intracranial pressure by tumor debulking is the initial step in nearly all patients. At the same sitting, the surgeon may choose to place a ventriculostomy to avoid intra- or postoperative intracranial hypertension or hydrocephalus. Fortunately, in those with complete resections, less than one-third will need permanent ventriculoperitoneal shunts. Though radical resections can be accomplished, surgical removal is not curative. In adults, once the wound is well healed, radiation therapy supplemented with chemotherapy can be added. Regular follow-up with neurologic examination and imaging is necessary in view of the propensity of these lesions to recur.
Considerable experience has been gained with these tumors in children. Essential to their treatment is the use of chemotherapy alone in children of less than 2 years of age with good risk. A number of agents have been used in this effort, with no single regimen being superior in every clinical situation. Therefore, the enrolment of such patients into research protocols where available will speed the delineation of the best regimens. Radiation is delayed if possible in order to protect the immature nervous system from its toxicity. Radiation is used more aggressively, in doses on par with those for malignant gliomas in older children and adults.
Neuronal and mixed neuronal and glial tumors: ganglioglioma and neurocytoma

Clinical presentation
Presentation tends to be nonspecific, but a significant proportion of gangliogliomas present with seizure activity, either generalized or focal, with symptoms appropriate to the site of origin. The epilepsy may be new or long standing. The neurocytoma is more likely to be associated with headache and symptoms of increased intracranial pressure. The neurocytoma and ganglioglioma occur most often in those below 30 years of age. These lesions generally grow slowly and may also be associated with gradual alterations in mental status appreciated only in retrospect.
Diagnosis
An individual with new onset of seizures or an unexplained fall off in cognitive abilities should undergo a neurologic examination to determine if any localizing abnormalities are present; this should be followed by MRI with and without gadolinium to evaluate the site of the abnormality. Neurocytomas will usually be associated with the lateral or third ventricles, often deforming the septum pellucidum. When in this location they are sometimes called central neurocytomas. Those that occur away from the ventricles may be called cerebral neurocytomas (Fig. 7). These lesions are usually homogeneous in density and may not enhance.
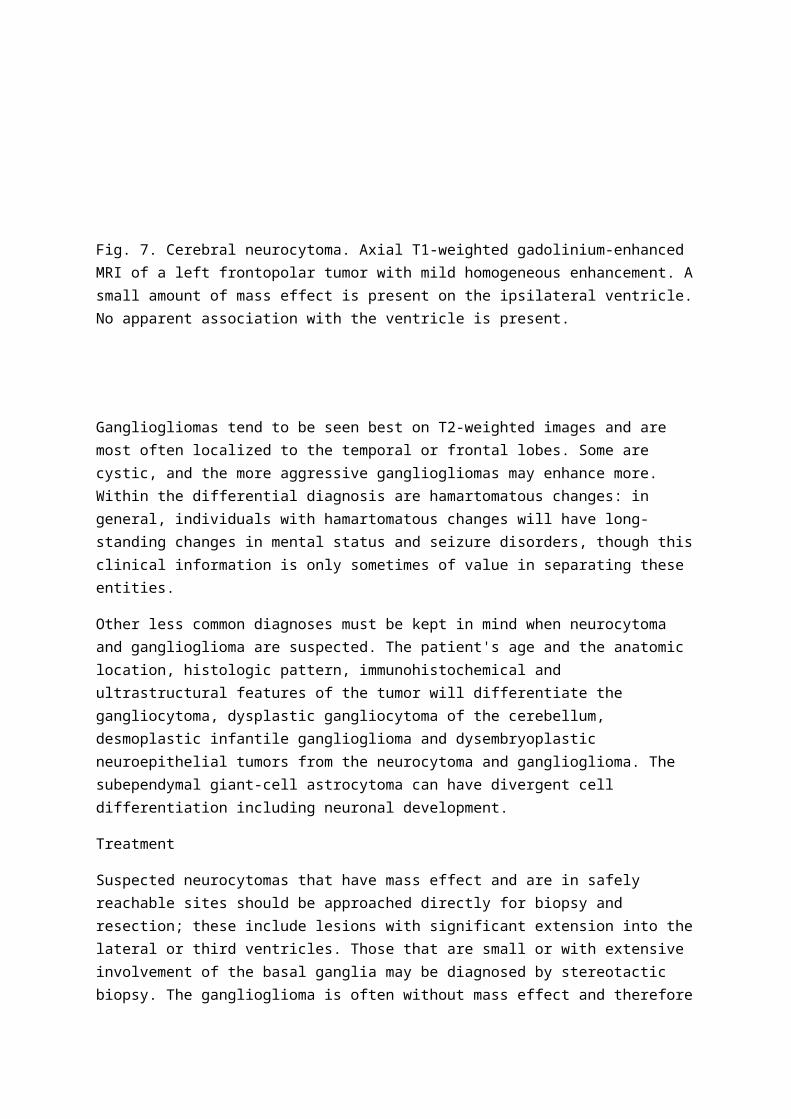
Fig. 7. Cerebral neurocytoma. Axial T1-weighted gadolinium-enhanced MRI of a left frontopolar tumor with mild homogeneous enhancement. A small amount of mass effect is present on the ipsilateral ventricle. No apparent association with the ventricle is present.
Gangliogliomas tend to be seen best on T2-weighted images and are most often localized to the temporal or frontal lobes. Some are cystic, and the more aggressive gangliogliomas may enhance more. Within the differential diagnosis are hamartomatous changes: in general, individuals with hamartomatous changes will have long-standing changes in mental status and seizure disorders, though this clinical information is only sometimes of value in separating these entities.
Other less common diagnoses must be kept in mind when neurocytoma and ganglioglioma are suspected. The patient's age and the anatomic location, histologic pattern, immunohistochemical and ultrastructural features of the tumor will differentiate the gangliocytoma, dysplastic gangliocytoma of the cerebellum, desmoplastic infantile ganglioglioma and dysembryoplastic neuroepithelial tumors from the neurocytoma and ganglioglioma. The subependymal giant-cell astrocytoma can have divergent cell differentiation including neuronal development.
Treatment
Suspected neurocytomas that have mass effect and are in safely reachable sites should be approached directly for biopsy and resection; these include lesions with significant extension into the lateral or third ventricles. Those that are small or with extensive involvement of the basal ganglia may be diagnosed by stereotactic biopsy. The ganglioglioma is often without mass effect and therefore stereotactic biopsy is often used. On examination of preliminary or frozen sections the neurocytoma appears to be composed of a homogeneous population of cells. On this basis, and because fine calcification is sometimes present, a preliminary diagnosis of oligodendroglioma may be made. The ganglioglioma will show a more heterogeneous field of cells with greater fibrillary background. The cells of these tumors can be identified as having neuronal, ganglionic, and astrocytic characteristics by immunohistochemistry and electron microscopy. The malignancy of the glial components of the ganglioglioma determines the propensity for recurrence.
Once diagnosis and/or resection has been accomplished, the next step depends on the proliferative nature of the lesions. The neurocytoma tends to grow slowly and can have an excellent prognosis after complete resection, and therefore its postoperative management is often simple observation with regular imaging and neurologic examinations. However, even in the neurocytoma, there can be significant postoperative residue in a tumor with mitotic activity and a high proliferative index as measured by MIB-1. In these there may be a role for more aggressive options, such as early repeat resection or more frequent postoperative imaging to detect progression early. X-irradiation is generally reserved for lesions that fail a second attempt at resection, detected by biopsy at recurrence as having some component of malignant glioma.
Regular electroencephalography may have a role in the chronic management of those with difficult-to-control seizures. In such a patient with ganglioglioma, craniotomy with electrocorticography to guide the resection can assist successfully in improving the seizure disorder. In the ganglioglioma with an aggressive or anaplastic glial component, radiation may be indicated at initial diagnosis.
Tumors of the skull base that arise separately from the nervous system
General comments
The skull base, particularly including the clivus, the petrous portions of the temporal bones, the sphenoid, the ethmoid, and the orbital roofs, serves as an interface between diseases treated by surgeons in other disciplines and those usually the province of the neurosurgeon. The anatomy of this location is heterogeneous in the sense that numerous important structures lie in and adjacent to these bones. Thus the surgeon must be familiar with the location and course of the primary vascular structures, including the internal carotid, vertebral and basilar, and meningeal arteries, the sphenoparietal, superior and inferior petrosal, transverse and sigmoid sinuses, the jugular bulb, and the cavernous sinus. Any of the 12 cranial nerves can become involved in operations at these sites. Additionally, the pituitary gland and its stalk should be respected. The paranasal sinuses, parts of the auditory and vestibular apparatus, and of the visual apparatus, are all found in association with tumors of this location. The preservation of these normal structures, and the maintenance of a reasonable cosmetic appearance but eradicating a tumor, are the primary challenges to working in this area.

Each type of tumor has a particular propensity to arise in certain regions and a characteristic tissue consistency. Approaches to these areas and techniques for their removal vary widely and have been the subject of much innovation. Tumor control is often obtained with multimodal management utilizing not only surgery but also radiation and embolization. The purpose here is to discuss considerations that are common in the care of patients with these lesions rather than provide an exhaustive list of possible approaches in each case.
Chordoma
Clinical presentation
Cranial and spinal chordomas putatively develop from the remnants of the embryonic notochord. Clinically, they arise in the ventral midline along the clivus, upper vertebral bodies, and sacrum (the most common site of origin). They occur most often in the third to fifth decades of life. Forty per cent arise from the clivus and the single most common complaint is headache. Presentation may be with new cranial neuropathy or radiculopathy, depending on the site of tumor origin. Motor symptoms and endocrine involvement are less common. These are unencapsulated lesions that compress and deform neurologic structures but remain separate from the nervous system. They are not separate from bone and are locally invasive. The symptoms, with or without pain, are often slow to develop, though sudden new symptoms can occur after local trauma.
Diagnosis
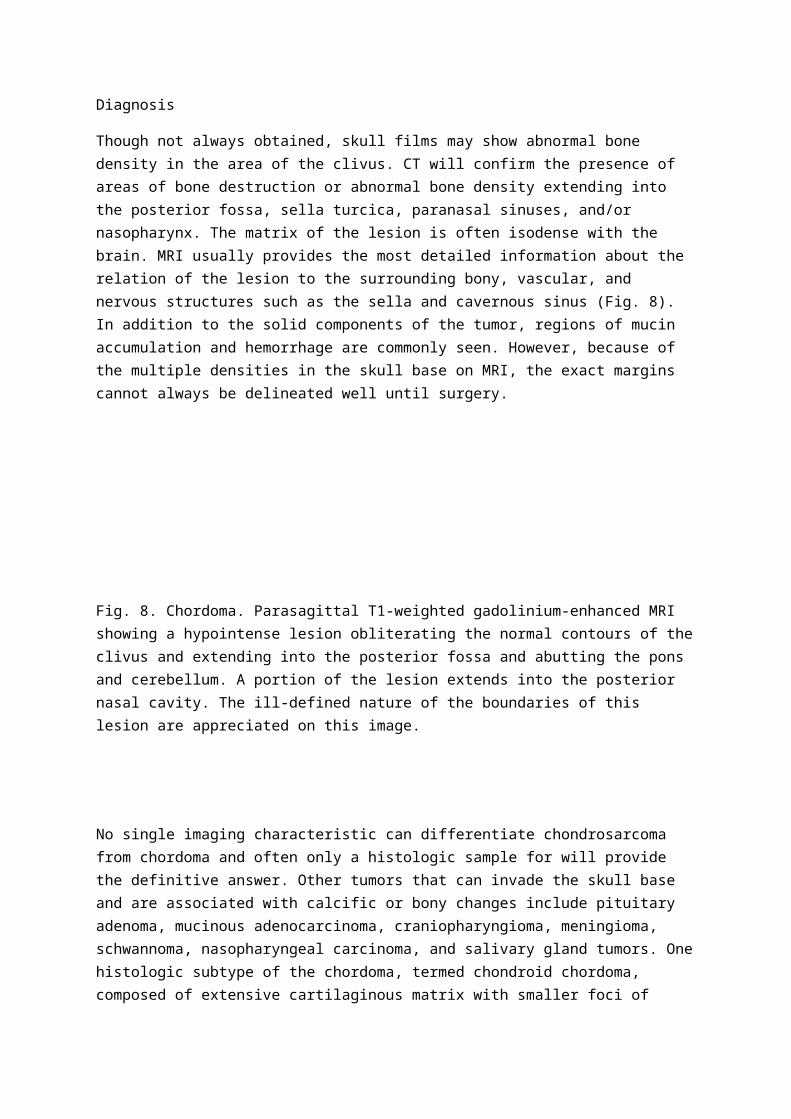
Though not always obtained, skull films may show abnormal bone density in the area of the clivus. CT will confirm the presence of areas of bone destruction or abnormal bone density extending into the posterior fossa, sella turcica, paranasal sinuses, and/or nasopharynx. The matrix of the lesion is often isodense with the brain. MRI usually provides the most detailed information about the relation of the lesion to the surrounding bony, vascular, and nervous structures such as the sella and cavernous sinus (Fig. 8). In addition to the solid components of the tumor, regions of mucin accumulation and hemorrhage are commonly seen. However, because of the multiple densities in the skull base on MRI, the exact margins cannot always be delineated well until surgery.
Fig. 8. Chordoma. Parasagittal T1-weighted gadolinium-enhanced MRI showing a hypointense lesion obliterating the normal contours of the clivus and extending into the posterior fossa and abutting the pons and cerebellum. A portion of the lesion extends into the posterior nasal cavity. The ill-defined nature of the boundaries of this lesion are appreciated on this image.

No single imaging characteristic can differentiate chondrosarcoma from chordoma and often only a histologic sample for will provide the definitive answer. Other tumors that can invade the skull base and are associated with calcific or bony changes include pituitary adenoma, mucinous adenocarcinoma, craniopharyngioma, meningioma, schwannoma, nasopharyngeal carcinoma, and salivary gland tumors. One histologic subtype of the chordoma, termed chondroid chordoma, composed of extensive cartilaginous matrix with smaller foci of chordoma, reportedly has better survival with less locally aggressive behavior.
When the tumor abuts the internal carotid it may be necessary to sacrifice that artery in order to obtain resection or intraoperative hemostasis, so a preoperative angiogram with balloon-test occlusion is useful. Additionally, a preoperative study of the venous anatomy will alert the surgeon to the dominant venous drainage pathways should it become necessary to consider sacrificing veins during the surgical procedure.
Unusually, where an exophytic component of the lesion involves the posterior nasopharynx, the diagnosis may be made via an endoscopic biopsy done by an otolaryngologist.
Treatment
Surgical management remains the primary form of therapy for these lesions; the clearest indications are for lesions with compression of the spinal cord, brainstem, or supratentorial structures. The approach to the lesion depends on the predominant location. Location can be classified by the tumor's primary nidus as upper, middle and lower clival. The majority are best approached anteriorly via extended frontal, transnasal, transmaxillary, or transoral approaches; not infrequently a combination of these must be used to reach an entire lesion; less frequently, a component of the lesion extending laterally can best be approached by a temporal, transpetrous, transcondylar, suboccipital, or retropharyngeal pathway. The tumor will insinuate itself into many of the bony recesses in the skull base, repositioning or enveloping vascular and neurologic structures. Thus microscopic dissection is necessary, with supplemental image-guided techniques if possible. Often the majority of the operation is extradural. Intradural extensions may require removal of a component of a portion of the dura, with repair by grafting and fibrin glue at completion of the resection. Temporary diversion of cerebrospinal fluid may be necessary. In anteriorly extending lesions with no significant alteration of the contours of the spinal canal or posterior fossa, transnasal endoscopic biopsy of the mass can be carried out.
In small lesions with no clearly defined site for needle or endoscopic biopsy, a surgical approach for open biopsy is indicated. Plans for resection must be made at the same time. Accurate knowledge of histologic type is important, as metastatic carcinomas and aggressive primary bone tumors can arise in these areas.
Where observation by scanning is chosen, the surgeon must be careful not to allow too long an interval between scans in the early stages of follow-up. The patient must be alerted to symptoms that may develop which would suggest the need for earlier follow-up imaging. When progression is noted, tissue diagnosis is still necessary even if resection is not used, to confirm the appropriateness of X-irradiation or proton-beam radiation.

The principles of care for spinal chordomas are the same: complete surgical resection when possible, including reconstruction of the spine as necessary, with supplemental irradiation where there is incomplete resection or progression. Metastasis reportedly occurs in up to 30 per cent of spinal chordomas, with widespread sites of involvement.
It is important to obtain images in the early postoperative period to establish a baseline for future reference. Not infrequently, resection of all but the smallest of midline lesions is incomplete, and the residue will be prone to slow but inexorable progression. To deal with this likelihood, nonsurgical options such as standard X-irradiation, stereotactic or proton-beam radiation can then be considered to control the lesion. Conventional radiation, though it does not seem to improve overall survival time, may prolong disease-free survival. Proton-beam radiation, though not commonly available, seems to have the most benefit in these lesions over the long term. Even with surgery and radiation the patient is committed to a lifetime of follow-up in view of this tumor's propensity for recurrence. No reliable chemotherapy regimens have been identified as yet.
Esthesioneuroblastoma
Clinical presentation
This tumor, sometimes referred to as olfactory neuroblastoma, is thought to arise from the olfactory neuroepithelium at the top of the nasal cavity, which explains its primary site of central nervous involvement, the midline of the anterior fossa. The portion of the neoplasm extending into the ethmoid sinuses, frontal sinus, and superior portions of the nasal airway will often present with symptoms of sinusitis. The tumor can also extend superiorly, lifting or transgressing the basal frontal dura mater, and this is where the neurosurgeon's input is most useful. As the compression usually occurs at the base of the frontal lobes, symptoms can include changes in mental status or an alteration or decrease in the sense of smell or taste. As some of these lesions invade the medial aspect of the orbit, diplopia, exophthalmos, or alterations in visual acuity may be noted.
Diagnosis
These individuals most often present to an otolaryngologist. The symptoms of sinusitis are unresponsive to standard conservative measures and medications. Skull films are often normal or will show fullness of the ethmoid and frontal sinus. CT will demonstrate lytic lesions in the cribriform and ethmoids on ‘bone windows'. Additionally, there will be a homogeneously enhancing soft-tissue mass in this region, usually asymmetric with variable amounts of tumor above and below the cribriform. MRI, particularly in the coronal plane, generally shows the tumor to better advantage (Fig. 9). As mentioned above, the persistent nasal mass will often mean that biopsy is done via this route, resulting in a histologic diagnosis prior to neurosurgical involvement. The histologic appearances are not uniform and, by utilizing the presence of lobar architecture, mitotic activity, nuclear pleomorphism, rosettes, and necrosis, a pathologic grading system has been designed that predicts reasonably well both outcome and the need for adjuvant therapy.

Fig. 9. Esthesioneuroblastoma. Coronal T1-weighted gadolinium-enhanced MRI of a large lesion with homogeneous enhancement in the superior nasal, ethmoid, and cribriform region. The usual thin, hypointense line showing the bony base of the olfactory groove is missing. The tumor extends bilaterally into the anterior fossa, with hypointense portions extending well into the frontal lobes.
Treatment
Surgery is the primary treatment for these lesions. In small lesions lying entirely below the cribriform, endoscopic resection is optimal. With clear evidence of defects in the skull base in a lesion primarily involving the nose and sinus, it is still prudent to be prepared for intracranial inspection and repair if necessary. Certainly, with a clearly intracranial tumor mass, a frontal craniotomy is necessary to address dural involvement or transdural invasion. The size of this approach depends on the size and location of the tumor. The surgeon must be able to see the normal structures of the skull base around the lesion. The tumor is usually separate from the brain, but large lesions are often infiltrative, requiring careful dissection between them and adjacent edematous brain. A graft of temporalis fascia, pericranium, or fascia lata can be used to repair the dura. Circumferential osteotomies will allow removal of the tumor. An attached and vascularized pericranial graft is then laid over the anterior skull base, covering the exenterated and occluded frontal sinus and the tumor defect in the ethmoids and cribriform, and anchored to the basal frontal dura behind the repair of the primary defect. The space between the pericranial flap and primary dural repair may be filled with fibrin glue. A brief period of cerebrospinal fluid diversion via a ventriculostomy or lumbar drain will assist in allowing the repair to heal well.
Gross total resection of a small esthesioneuroblastoma can be ascertained by the surgeon and the patient may be followed with CT or MRI at regular intervals. If microscopic or gross tumor is clearly still left behind, or if significant malignant changes are present on histologic analysis, then fractionated radiation doses of 55 to 65 Gy over 6 to 7 weeks can be used. Lesions with a significant degree of anaplasia may be treated with intravenous cytotoxic agents. No specific regimen is clearly superior but a combination of Adriamycin and cisplatin has some efficacy. Regular follow-up examinations and imaging should be maintained to observe for recurrence at or near the tumor bed.
Nasopharyngeal carcinoma
Clinical presentation
As many as 25 per cent of nasopharyngeal carcinomas affect the skull base. They tend to occur more often in males, and with a mean age of onset of 62 years in men and 72 years in women. As with other neoplasms of this region, presentation is usually associated with nasal congestion, nasal and pharyngeal drainage, epistaxis, and facial or frontal pain that may have been acute or, more commonly, indolent in onset. Lesions with which the neurosurgeon is involved are often invasive and
may have spread into the orbit and intracranial space. Orbital involvement may be associated with exophthalmos, diplopia, erythema and chemosis, and visual obscuration. Intracranial invasion is most often frontal, but may be via the cavernous sinuses into the middle fossa or even through the clivus to the posterior fossa. The symptoms induced by intracranial invasion depend on the site of brain involvement. In general, frontal involvement will be associated with changes in mental status. Involvement of the middle fossa may be preceded by alterations of function in the nerves in the cavernous sinus. Once temporal damage has occurred, the patient may develop seizure activity or alterations in mental status. Invasion of the posterior fossa is uncommon, but when it occurs, cranial-nerve symptoms may be the first evidence, as these structures are injured as they leave the posterior fossa. Difficulties with balance and coordination may occur, owing to cerebellar dysfunction or hydrocephalus.
Diagnosis
An irregularly enhancing, nasal or sinus mass on CT, usually with variable degrees of bone destruction seen on properly ‘windowed' images, will suggest this diagnosis. The most common route of intracranial extension is through the foramen lacerum. From here the tumor has direct access to the cavernous sinus and orbital apex. During this process, dysfunction of the IIIrd, IVth, Vth, and VIth cranial nerves can be seen. It is believed that another route of tumor spread is along the nerves in and around the skull base. Therefore, enlargement and erosion of normally occurring foramina containing abnormal soft-tissue densities can also suggest this diagnosis. MRI will best delineate any involvement of the cranial nerves, cavernous sinus, sella, and brain. The tumor tissue is usually homogeneous on T1-weighted images and hyperintense on T2-weighted sequences (Fig. 10). MRI can also assist in differentiating inspissated mucus from tumor within sinuses. Direct transnasal biopsy of the lesion to confirm the diagnosis will be possible in the majority of cases.
Fig. 10. Nasopharyngeal carcinoma. (a) Axial t1-weighted gadolinium-enhanced MRI of a tumor arising the right ethmoid, deforming the medial aspect of the orbit and growing up against the gyri of the basal frontal lobe. (b) A parallel axial T1-weighted gadolinium-enhanced image of the same tumor at a more inferior level, showing invasion of the orbit.
Histologic types of cancer in this location, in descending order of incidence, include squamous-cell carcinoma, adenocarcinoma, anaplastic carcinoma, salivary or adenoid cystic carcinoma, and metastatic tumors such as melanoma or lymphoma. Imaging by itself does cannot separate these types easily, indicating the need for biopsy to define more exactly the management and prognosis.
Treatment
If the patient is otherwise healthy and without debilitating systemic metastases, surgical resection is indicated. The goal of surgery is to obtain complete resection with tumor-free margins. Surgical planning includes determination of the approach, method of resection, and reconstruction.
Approaches to the anterior skull base include the trans-septal (trans-sphenoidal), transethmoidal, transmaxillary, extended frontal, anterior craniofacial, facial translocation, transoral, and the transmandibular–transcervical routes. Lateral extensions of the tumor may require approaches via the middle fossa, infratemporal fossa, or orbitozygomatic routes. In many cases the invasive nature of the tumor will have resulted in it becoming intertwined with structures of the orbit or cavernous sinus in a manner that is not amenable to complete surgical resection. The dura serves as an effective barrier to many of these tumors. Where the dura is crossed and there is clearly involvement of brain parenchyma, there is cerebral edema and mass effect. Neurosurgical involvement is indicated to resect this portion of the lesion if aggressive management is chosen. Resection by craniotomy or in a combined craniofacial resection may add to the palliative effort in these cases. Extensive invasion of the cavernous sinus with involvement of the carotids may preclude anything more than a biopsy. Also, orbital exenteration is indicated only if it is fairly certain that complete resection is being obtained. Large resections of the skull base will require repair with vascularized tissue to avoid leakage of cerebrospinal fluid.
As these lesions are rarely cured surgically, subsequent radiation to the tumor bed is necessary. In fact, part of the neurosurgeon's role is often to determine that no, or only limited, surgical intervention is warranted and to follow-up and perform well-documented neurologic examinations in an attempt to detect clinical signs of early tumor progression. Stereotactic radiation provides a method for focal radiation of tumor residues after initial surgery or at the time of recurrence. Chemotherapy may have a role; cisplatin and 5-fluorouracil have been used.
Survival depends on the stage or extent of involvement of the surrounding tissue. Greater extension is associated with shorter survival. Recurrences are frequent, with progression-free survival at 10 years being as low as 7 per cent for adenoid cystic carcinoma. With multimodal management, 5-year survival is approximately 20 to 40 per cent, depending on the histologic type of tumor.
Glomus tumor
Clinical presentation
Glomus jugulare tumors arise from cells in the adventitia of the jugular bulb and along Jacobson's and Arnold's nerves within the tympanic cleft. They are the most common tumor of the middle ear and second to the acoustic neuroma for tumors of the temporal bone. The mean age at presentation is 52 to 55 years and there is a female predominance. It must be kept in mind that these lesions can be bilateral or multicentric and, in rare cases, familial, where a modified autosomal-dominant transmission may be present. It appears that the genetic abnormality may be localized on chromosome 11q at 11q23 and 11q13.1.
Because these tumors often involve the middle ear, conductive hearing loss, ear pain, bloody discharge, and tinnitus can occur. As an alternative to tinnitus, the patient may note a pulsatile sound that corresponds with a mastoid bruit found on examination and reflects the vascular nature

of these lesions. The surgeon may even be able to observe the lesion behind or transgressing the tympanic membrane or the external auditory canal. The glomus jugulare involves the jugular foramen and its contents, resulting in symptoms due to dysfunction of the glossopharyngeal and vagal nerves, and occlusion of the jugular vein and sigmoid sinus. Problems with swallowing and an alteration in vocal quality are the main clinical changes related to the glomus tumor. Interestingly, palsies of the IXth and Xth nerves are seen with another tumor in the differential diagnosis, schwannoma of the jugular foramen. Glomus tumors can involve the VIIth and VIIIth nerves or the contents of the middle ear, causing facial weakness and hearing loss. Shoulder weakness or aching from involvement of the accessory nerve can occur. Additionally, with large lesions, compression of the cerebellum or of vestibular nerves, or invasion of the vestibular apparatus, will result in ataxia and incoordination. Because glomus tumors grow slowly, the symptoms from venous occlusion tend to be minimal.
These lesions are also called paragangliomas, implying origin from paraganglionic cells of the neural crest. Early classifications mention chromaffin and nonchromaffin paragangliomas, based on tissue reaction with chromic acid, but this reaction is not always reliable and terminology based on location is clearer. Glomus tumors have been identified at various locations. The glomus tympanicum is not uncommon and arises from cells on the promontory of the cochlea in the hypotympanum; therefore it is more likely to result in altered hearing. Also, there is the glomus vagale, arising from receptor cells along the course of the vagus nerve, and the glomus caroticum (carotid body tumor or chemodectoma), arising at the division of the common carotid artery.
Diagnosis
Clinical examination will confirm the presence of abnormalities in voice quality, palatal movement, pharyngeal sensation, and gross alterations in hearing. Laryngoscopy and audiometry can better confirm these findings. CT using a ‘soft-tissue window' with and without contrast and ‘bone windows' will delineate these lesions well. MRI may assist in sorting out the relation between the tumor and structures outside of the jugular foramen and within the posterior fossa, which becomes important with larger lesions. On T1-weighted images, mixed hypointense and isointense signals will be noted. The hypointense components are the flow voids of vascular channels and the isointense portions reflect solid tumor. This mixture of intensities, sometimes called a salt-and-pepper pattern, is the result of the tumor's extensive vascularity. Gadolinium enhancement is usually heterogeneous. As implied, glomus jugulare tumors can be very vascular and an angiographic blush of the jugular foramen region fed by the external carotid is characteristic (Fig. 11).
Fig. 11. Glomus jugulare. Left common carotid angiogram in modified lateral view showing contributions from branches of the external carotid artery to a tumor blush in the region of the jugular foramen; this pattern is characteristic.
As many of these symptoms will first lead the patient to the otolaryngologist, they will usually be seen by the neurosurgeon in consultation. Sometimes, larger lesions will have been biopsied via the external auditory canal, though most otolaryngologists recognize these and understand that this can result in significant hemorrhage in some cases.
Some of these tumors (approximately 1 per cent) are hormonally active, and urine and serum assays for catecholamines, vanillylmandelic acid, and metanephrine should be part of the evaluation; positive results will influence the anesthetic management of the patient.
Treatment
Because of their vascularity, preoperative embolization 1 to 2 days before surgery may ease dissection and decrease blood loss in larger lesions. This vascular intervention will also clarify the relation between the tumor and the carotid. In these larger lesions, upper cervical dissection to isolate the jugular, carotids, and IXth to XIIth cranial nerves serves as an initial step, followed by a mastoidectomy with exposure of the VIIth nerve, sigmoid sinus, and semicircular canals. Monitoring of the facial nerve and auditory-evoked potentials is useful during the dissection. The resection of the lesion, usually along with the sigmoid sinus and jugular bulb, is then carried out. An attempt is made to preserve the cranial nerves, and any attachments to the carotid artery are carefully dissected. Unresectable attachments to the carotid are best left and coagulated rather than risk injury to the artery. Intracranial portions of the lesion are resected via presigmoid or retrosigmoid approaches. Dural closure is important to avoid leakage of cerebrospinal fluid. In some cases, larger defects or sites that have already been radiated may need closure with rotational or vascularized muscle grafts.
In smaller lesions without intracranial extension, transpetrous resection without invasion of the posterior fossa is reasonable; the work within the petrous bone must preserve the VIIth nerve and the middle and inner ear. Where there is compression of the contents of the posterior fossa, neurosurgical intervention is necessary to stop progression of the neurologic deficit. Imaging studies will often show that, even with lesions having significant involvement of the posterior fossa, cure can only be obtained by removal of the portions of the tumor in the jugular foramen, mastoid, middle ear, and upper cervical soft tissues.
These lesions are radiosensitive. Its use is controversial in some circles, but offers a good alternative in patients who are unable to undergo surgery, have significant postoperative residues, or who suffer recurrence. Fractionated radiation in larger tumors and stereotactic radiation in lesions less than 3 cm in diameter can arrest growth and even result in regression. The patient must be told of the possibility of injury to the surrounding structures with this form of therapy, even if there is no incision. This method is particularly appealing in patients with other medical infirmities and in the presence of measurable recurrence.
Even after resection, the surgeon must be aware of the possibility of recurrence. Therefore postoperative imaging, at least annually, is necessary.
Neurofibromas and schwannomas
Neurofibromas and schwannomas are histologically benign neoplasms that arise from nerve sheaths, most commonly from sensory nerve roots. Neurofibromas appear grossly as a fusiform enlargement of the nerve whereas schwannomas are more clearly delineated from the nerve root. Therefore, surgical resection of schwannomas may be accomplished without sacrifice of the associated nerve root, a result that is almost impossible to achieve with a neurofibroma.
In the absence of neurofibromatosis, nerve-sheath tumors are almost invariably schwannomas and only rarely neurofibromas. Within the spinal axis, nerve-sheath tumors are distributed fairly evenly, being more prevalent in the thoracic region. They occur most commonly in an intradural, extramedullary location and present with pain in the distribution of the involved nerve root, followed by progressive myelopathy with continued growth.
Intracranially, schwannomas most commonly arise from the vestibular nerve. Although the most accurate term for these neoplasms is vestibular schwannoma, the term ‘acoustic neuroma' is firmly entrenched in the neurosurgical literature. The most common presentation of the acoustic neuroma is progressive, unilateral hearing loss due to compression of the adjacent cochlear nerve. Tinnitus is another common early symptom. With progressive growth, the tumor may compress the adjacent trigeminal nerve and brainstem. Nerve-sheath tumors may occur on other cranial nerves such as the trigeminal or glossopharyngeal.
Neurofibromatosis
The neurofibromatoses are genetic disorders associated with a high incidence of tumors of the nervous system including neurofibromas, schwannomas, meningiomas, and gliomas. Two types of neurofibromatosis have been well characterized and the genetic abnormalities identified. Both neurofibromatosis type I and type II are transmitted in an autosomal-dominant manner with high penetrance. The genes for each type have been cloned and protein sequences identified.
Type I is the most common, occurring approximately once in every 4000 births. Previously known as peripheral neurofibromatosis or von Recklinghausen's disease, its most common manifestations are multiple cutaneous neurofibromas, café au lait marks, axillary freckling, Lisch nodules of the iris, skeletal abnormalities, and an increased incidence of childhood gliomas including optic gliomas, ependymomas as well as meningiomas, hamartomas, and primitive neuroectodermal tumors. Tumors of spinal nerve roots in patients with type I neurofibromatosis are commonly asymptomatic, multiple, and more often neurofibroma than schwannoma. Plexiform neurofibromas are peripheral nerve tumors composed of Schwann cells, fibroblasts, and connective tissue; these may degenerate into malignant neurofibrosarcomas in patients with type I.
Neurofibromatosis type II is much less common than type I, occurring once in every 100 000 births. Previously called central neurofibromatosis, the hallmark of this condition is bilateral acoustic neuromas. Meningiomas, sporadic unilateral acoustic neuromas, sporadic spinal schwannomas, and ependymomas are found with higher incidence in patients with type II.
Diagnosis
Both intracranial and intraspinal nerve-sheath tumors are best seen by MRI, with and without gadolinium. In spinal lesions these studies demonstrate the relation of the tumor to the spinal cord, to bony structures, and, in high cervical lesions or lesions in the foramen magnum, its relation to the vertebral arteries (Fig. 12). MRI elegantly demonstrates the extraspinal component of neurofibromas that extend through the neural foramina in a dumbbell shape. Nerve-sheath tumors usually enhance homogeneously after the administration of gadolinium.
Fig. 12. (a) Axial and (b) sagittal MRI demonstrates a schwannoma ventral to the upper cervical spinal cord causing significant compression; this study illustrates the relation of the tumor to surrounding important structures.
Intracranial nerve-sheath tumors such as acoustic neuromas are best visualized by MRI with and without contrast; this is very helpful in determining the relation of the tumor to important structures and in planning surgical approaches (Fig. 13).
Fig. 13. (a) Gadolinium-enhanced axial T1-weighted MRI of a right-sided acoustic neuroma. There is compression of the pons and cerebellum and the fourth ventricle is shifted to the left. The tumor extends into the internal auditory canal and has a heterogeneous signal internally. (b) Gadolinium-enhanced coronal T1-weighted MRI of the same lesion showing that the tumor extends all way up to the tentorium and occupys the usual location of the middle cerebellar peduncle.
Treatment
Most tumors of spinal nerve sheaths are benign and complete surgical excision is potentially curative. For symptomatic patients with a reasonable life expectancy, surgical treatment offers a high likelihood of success and an opportunity to eliminate a potential source of progressive myelopathy. Frequently, patients with neurofibromatosis will have multiple asymptomatic tumors that can be simply observed by serial MRI.
For intracranial tumors, such as acoustic neuroma, there is a variety of treatment options. Small, asymptomatic or minimally symptomatic tumors may be observed by serial MRI, particularly in the elderly patient. Different surgical approaches may be considered for acoustic neuromas, chosen on the basis of several factors including tumor size and configuration, opportunity for preservation of hearing, and surgeon's experience. The translabyrinthine operation is a versatile approach for managing acoustic tumors: one of its primary advantages is early and accurate visualization and preservation of the facial nerve, but it is always associated with hearing loss on the side of the tumor. Translabyrinthine approaches are often used for the resection of small to medium-sized tumors in patients without useful hearing. A retromastoid suboccipital craniotomy is an excellent approach for tumors of all sizes and is the procedure of choice when preservation of hearing is attempted. Small lesions within the internal auditory canal in patients with functional hearing may also be resected via the middle fossa.
Stereotactic radiosurgery is another option in the management of acoustic tumors for selected, high-risk patients. It involves the delivery to the tumor, in a single session, of a high dose of targeted radiation such that the surrounding neural structures receive a low dose. Its primary advantage is that it is minimally invasive. Its disadvantages are the long interval to the desired effects of the radiation, the relatively low cure rate, and the low but definite risk of radiation injury to the brainstem and adjacent cranial nerves.
Pineal tumors
Introduction
The pineal gland is a small, midline organ situated in the quadrigeminal plate cistern attached to the posterior roof of the third ventricle. The gland is divided by connective tissue septa into lobules consisting of pineocytes, which are specialized neuroepithelial cells with neurosecretory properties. The physiologic importance of the pineal gland remains unclear, although it is believed to have a role in circadian rhythms and reproduction. Despite its small size, the diversity of cell types that constitute the gland and adjacent structures results in a large variety of neoplasms. Although many different neoplastic and non-neoplastic mass lesions occur in this region, pineal tumors represent only about 1 per cent of all brain tumors and 3 to 10 per cent of brain tumors in childhood.
Clinical presentation
Because of the strategic anatomic location of the pineal gland, the presenting symptoms and signs of pineal mass lesions are similar regardless of the histopathologic features. Growth of a mass lesion in this region frequently results in compression of the aqueduct of Sylvius, resulting in obstructive hydrocephalus. Lesions causing hydrocephalus present with the features of increased intracranial pressure, including headache, nausea and vomiting, and lethargy. Infiltration or compression of the midbrain results in Parinaud's syndrome, the classic syndrome associated with tumors of the pineal
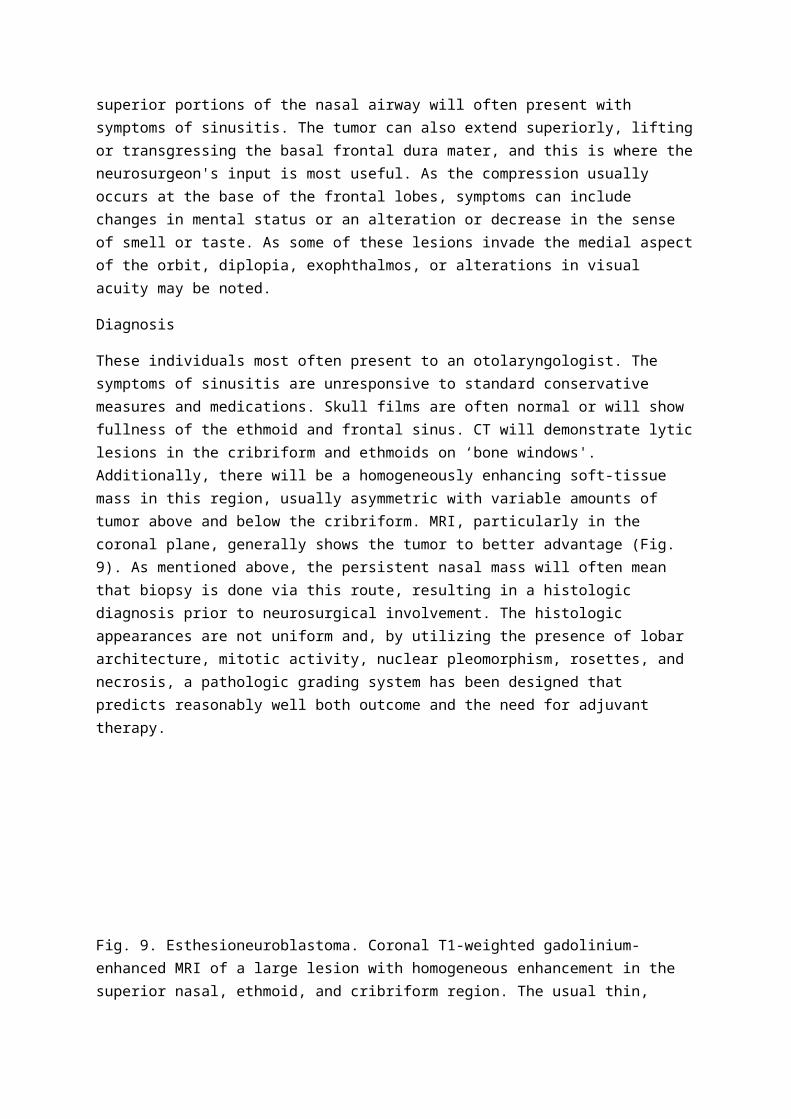
region. Parinaud's syndrome includes paralysis of upward gaze and ocular convergence, and pupillary abnormalities characterized by non-reactivity to light but constriction to accommodation. Endocrine disturbances, including precocious puberty, hypogonadism, diabetes insipidus, and anterior pituitary insufficiency, are frequently associated with tumors of the pineal region.
Diagnosis
The diagnostic investigation of masses in the pineal region has been revolutionized by MRI. This noninvasive study clearly demonstrates all the mass lesions that arise in this region, the extent of tumor compression or invasion, and the precise relation to surrounding anatomic structures in multiple planes. Because certain pineal tumors have a predilection for metastasis within the cerebrospinal fluid spaces, evaluation of the spinal axis by MRI is recommended to look for these ‘drop metastases'.
In general, the precise diagnosis of a tumor of the pineal region cannot be made from imaging studies. Histologic diagnosis is essential, since each different tumor arising in this region has an optimal method of treatment.
Tumor types
Tumors arising within the pineal region can be classified into five major groups of mass lesions: pineal parenchymal tumors, tumorsof the supporting glial cells, germ-cell tumors, mesenchymaltumors (meningiomas), and non-neoplastic masses.
Pineal parenchymal tumors
Tumors arising from the pineal parenchyma constitute approximately 15 to 30 per cent of all tumors of the pineal region. They include:
1.
pineoblastomas: highly malignant, primitive neoplasms with a propensity for local infiltration and dissemination in cerebrospinal fluid;
2.
pineocytomas: tumors with primarily benign cytologic features and little tendency to invade the surrounding brain or spread within the neuraxis (Fig. 14);
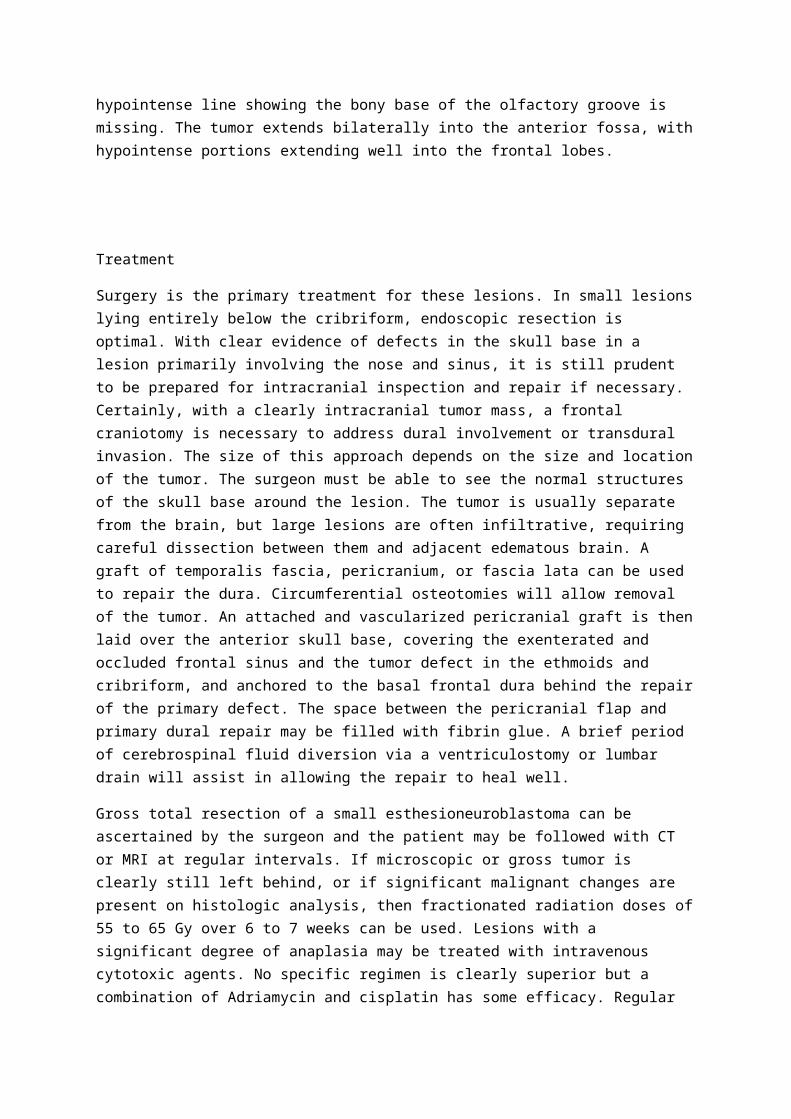
Fig. 14. Axial, primarily T2-weighted MRI of a pineocytoma: this tumor is located posterior to the third ventricle, anterior to the cerebellar vermis, and just to the right of the midline; note the significant vascular flow voids adjacent to the lesion and the relatively clear delineation between tumor and normal parenchyma.
3.
mixed pineocytoma–pineoblastomas: neoplasms that exhibit features of both of the aforementioned lesions.
Glial tumors
Gliomas, particularly astrocytomas, arise from the supporting glial cells present within the pineal gland or from structures adjacent to the pineal gland; they account for 10 to 35 per cent of tumors in the pineal region. Glial tumors arising here include benign astrocytomas, anaplastic astrocytomas, glioblastomas, ependymomas, oligodendrogliomas, and papillomas of the choroid plexus.
Meningiomas
Meningiomas of the pineal region typically arise from the falx, tentorium, or the velum interpositum, a fold of arachnoid that forms at the roof of the third ventricle. These lesions typically expand into the pineal region and posterior third ventricle.
Germ-cell tumors
Germ-cell tumors that occur in the region of the pineal gland are indistinguishable from those arising in the testicle and ovary; they comprise the largest group of neoplasms in the pineal region, accounting for nearly 50 per cent. They occur most commonly during the first two decades of life and are more common in males than females. The six major types of germ-cell tumors in approximate order of increasing malignancy are mature and immature teratomas, germinomas, malignant teratomas, embryonal carcinomas, endodermal sinus tumors, and choriocarcinomas.
Germinomas, which are similar histologically to testicular seminomas, are the most common germ-cell tumor affecting the pineal region. They are locally invasive and tend to spread through the ventricular system and subarachnoid spaces via the cerebrospinal fluid. Although these tumors have malignant characteristics, they are exquisitely radiosensitive and long-term survival or cure can be accomplished. Other germ-cell tumors are highly malignant. Although they may show an early response to radiation therapy, they are usually fatal.
Non-neoplastic lesions
Cysts of the pineal region are relatively common findings at autopsy. With the advent of MRI, these lesions have been diagnosed with greater frequency. They are typically benign and almost always an incidental finding. On rare occasions they will enlarge and result in obstructive hydrocephalus.
Treatment
Prior to the advent of microsurgical techniques, surgical approaches to the pineal region were fraught with high morbidity and mortality. Standard treatment typically consisted of ventricular shunting to relieve hydrocephalus, followed by an empiric course of radiation. Because of the high incidence of germinomas, this approach was associated with some successes.
In the modern microsurgical era, tumors of the pineal region can be approached directly with a very low operative morbidity. Those patients who present with symptomatic hydrocephalus should undergo placement of a ventriculoperitoneal shunt to relieve the hydrocephalus. Lesions are most commonly approached by an infratentorial, supracerebellar method that exposes the pineal region through the posterior fossa over the superior surface of the cerebellar vermis. Approximately one-third of pineal tumors are benign and curable with surgery alone. If the intraoperative biopsy demonstrates a germinoma, the treatment of choice is radiation therapy. Other highly malignant germ-cell tumors are typically treated by subtotal resection, followed by radiation therapy. Chemotherapy is now often instituted, based on experience with tumors of gonadal origin arising elsewhere in the body.
Certain malignant germ-cell tumors are associated with tumor markers in cerebrospinal fluid. Concentrations of a-fetoprotein, normally produced by the fetal yolk sac, may be elevated in patients with endodermal sinus tumors or embryonal carcinomas. Human chorionic gonadotrophin is normally produced by syncytiotrophoblasts of the placenta and is commonly elevated in the cerebrospinal fluid of patients with choriocarcinoma or embryonal carcinoma. Although cytologic evaluation of cerebrospinal fluid, tumor markers, and radiographic features can inform predictions of a diagnosis, this can be accomplished accurately only by pathologic examination of tumor tissue. These markers in cerebrospinal fluid are useful in following patients for evidence of recurrence of disease or response to treatment.
Despite the advantages of direct surgical approaches to pineal tumors, there are several circumstances in which a stereotactic biopsy is the preferred treatment. It is most appropriate for patients who are elderly or in whom significant medical complications increase the risk of open craniotomy. Patients with disseminated tumors at the time of presentation are often best managed by stereotactic biopsy to establish a diagnosis, followed by adjuvant therapy including radiation and/or chemotherapy.
Meningiomas and choroid plexus tumors
Meningiomas are neoplasms that arise from the meningeal coverings of the brain or spinal cord. They originate from the arachnoidal cap cells, commonly in association with the arachnoid villi at the dural venous sinuses and their tributaries, the foramina of the cranial nerves, the cribriform plate, and the medial middle fossa. The overwhelming majority of meningiomas are benign and most grow very slowly.
Meningiomas

Etiology
Various environmental and genetic factors are proposed as potential contributors to the pathogenesis of meningiomas. Prior head trauma has been associated with these tumors, but several case–control studies have failed to show a correlation. A clear connection between radiation and meningiomas has been established. Significant evidence suggests that the growth of meningiomas may be influenced by female sex hormones, providing a rationale for clinical trials of estrogen and progesterone inhibitors.
Clinical features
Although meningiomas may arise anywhere within the intracranial or intraspinal cavities, there are specific locations where they are more common. The clinical presentation of meningioma depends upon the location, the rate of tumor growth, and the extent of peritumoral edema. Compression of adjacent brain and neural structures may produce global or focal neurologic symptoms and signs. A meningioma occurring in a relatively silent area of the brain may become rather large before producing symptoms, whereas a relatively small tumor may produce significant neurologic deficits if it is in a functionally important area.
Convexity meningiomas arising from the dura over the surface of the brain cause symptoms by compressing the adjacent cerebral hemispheres and may produce headache, focal neurologic deficits, or seizures.
Parasagittal meningiomas involve the superior sagittal sinus and adjacent dura and falx; patients frequently present with focal motor or sensory seizures, or leg weakness. Progressive enlargement of these lesions may eventually occlude the superior sagittal sinus.
Falx meningiomas arise from the falx cerebri and only secondarily invade the superior sagittal sinus; their presentation is similar to that of parasagittal meningiomas.
Meningiomas of the sphenoid wing may arise anywhere along the sphenoid ridge. In the lateral sphenoid wing they usually present with slowly progressive, painless exophthalmos. In the mid-portion of the sphenoid wing they may compress the frontal and temporal lobes, and present with headaches and/or seizures. Meningiomas of the medial sphenoid wing may involve the anterior clinoid process and present with unilateral loss of vision. Secondary involvement of the superior orbital fissure or cavernous sinus may produce cranial-nerve palsies.
Meningiomas of the cavernous sinus may originate within the sinus itself or invade this structure secondarily from other adjacent locations. Diplopia and facial numbness or pain are manifestations of involvement of the intracavernous cranial nerves. Meningiomas of the optic sheath present with progressive, painless, ipsilateral visual loss.
Meningiomas of the olfactory groove may reach large size before clinical detection because of slow growth compressing the frontal lobes; this may result in changes in mental status, decreased visual acuity, or seizures. Anosmia is often present.
Meningiomas arising from the tuberculum sellae typically present with visual symptoms due to lateral displacement of the optic nerves; these lesions commonly present with headache and changes in mental status.
Meningiomas may arise from any site along the tentorium. If the growth is primarily supratentorial, patients most commonly present with headaches and/or seizures. Primarily, infratentorial growth will result in cerebellar, brainstem or cranial-nerve deficits, or hydrocephalus.
Meningiomas may arise from any level of the clivus. Clival meningiomas may grow along the petrous bone or into the cavernous sinus and middle fossa. Symptoms and signs result from cranial-nerve dysfunction, cerebellar and/or brainstem compression, and intracranial hypertension.
Meningiomas of the cerebellopontine angle present with cerebellar symptoms and signs, and hearing loss.
Meningiomas of the foramen magnum are most commonly located anterolateral to the medulla and typically present with progressive quadriparesis and dysfunction of the lower cranial nerves.
Intraventricular meningiomas are rare and most commonly occur in the trigone of the lateral ventricle. Headache is the most common symptom of these lesions. With progressive enlargement, they may produce intracranial hypertension due to direct compression of the adjacent brain and development of hydrocephalus.
Spinal meningiomas typically present with focal back pain and progressive paresis below the level of the lesion. As compression of the spinal cord advances, patients develop sphincter disturbances.
Diagnosis
Meningiomas have a characteristic appearance on both CT and MRI. MRI has become the procedure of choice for diagnosis of most meningiomas: this noninvasive study elegantly demonstrates the lesion in multiple planes, its relation to surrounding neural structures, and any associated edema (Fig. 15). Some meningiomas are associated with significant hyperostosis or frank invasion of the Haversian canals of adjacent bone, best seen on CT.
Fig. 15. (a) Contrast-enhanced axial T1-weighted MRI of a meningioma of the medial sphenoid wing; (b) T2-weighted MRI of the same case—note the extensive hyperintense signal abnormality in the temporal lobe adjacent to the tumor.
Magnetic resonance angiography is useful in defining the relation of meningiomas to the arterial circulation and in disclosing the presence of invasion or occlusion of venous sinuses. Occasionally, catheter angiography is indicated to define better the vascular relations of a meningioma, or for preoperative embolization of highly vascular lesions.
Treatment
With modern, noninvasive imaging many meningiomas are diagnosed when they are minimally symptomatic or as incidental findings during an evaluation for unrelated symptoms. Particularly in elderly patients these lesions may not require treatment, and serial MRI or CT can be used to follow tumor growth or the progression of symptoms.
The primary treatment for most symptomatic meningiomas is surgical resection. Factors influencing safety, ease, and outcome of surgical removal include tumor location, size, consistency, and vascular and neural involvement. To minimize the likelihood of recurrence the neurosurgeon must resect not only the entire neoplasm but also all involved dura, soft tissue, and bone. Meningiomas of the convexity have the greatest potential for total removal and cure because of the relative ease of exposure and the opportunity to resect a wide margin of dura. Meningiomas involving the anterior sagittal sinus may be managed by ligation and excision of the sinus, if involved. Involvement of the posterior two-thirds of the superior sagittal sinus often requires extensive efforts to reconstruct the sinus and maintain its patency if not already occluded by the tumor.
Variuos approaches that involve more extensive removal of bone to minimize retraction of the brain are useful in the management of meningiomas involving the anterior, middle, and posterior skull base. Spinal meningiomas are generally approached through a laminectomy with dural opening, with careful microsurgical resection of the lesion and its dural attachment.
Although the surgical goal for meningiomas is complete removal of the tumor and involved dura, this objective should be tempered with good judgement and the primary aim of preserving and improving neurologic function. In some patients, total removal of the meningioma carries the risk of significant morbidity, and extensive but subtotal removal may be followed by resolution of symptoms for many years without significant recurrence.
A number of studies have shown the effectiveness of radiation therapy in reducing the likelihood and rapidity of recurrence following subtotal resection. Although less conclusive, there are reports of the effectiveness of radiation therapy in meningiomas considered inoperable because of their location or the patient's poor health. More recently, stereotactic radiosurgery has been used with promising results on relatively small tumors considered inoperable or high risk, and for residual tumor in functionally important areas.
Although little information is available on the efficacy of traditional chemotherapeutic agents for meningiomas, the antiestrogen tamoxifen and the antiprogesterone mifepristone have produced some encouraging early results in selected cases.
Choroid plexus tumors
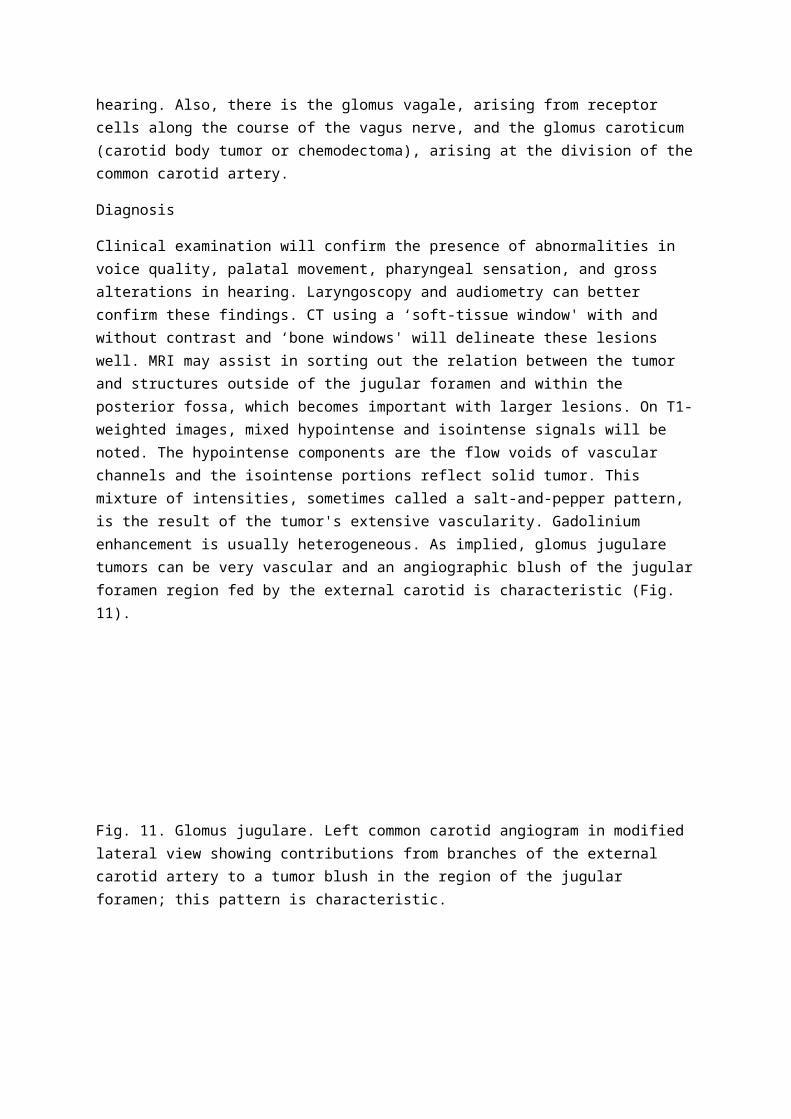
Tumors of the choroid plexus may occur anywhere within the ventricular system where choroid plexus exists. The majorityoccur in the atrium of the lateral ventricle, a smaller number within the fourth ventricle, and rarely in the third ventricle. Choroid plexus tumors characteristically occur in young children. Although they account for 10 to 20 per cent of all brain tumors occurring during the first year of life, they represent only 3 per cent of all brain tumors of childhood. Tumors of the choroid plexus include benign papillomas, or malignant carcinomas that invade the brain and tend to disseminate within the cerebrospinal fluid.
Tumors of the choroid plexus most commonly present with hydrocephalus, which may be due to an overproduction of cerebrospinal fluid by the tumor, direct obstruction of the fluid pathways, or impairment of the fluid absorption due to episodes of subarachnoid hemorrhage.
These lesions are best diagnosed by MRI or CT. On CT, papillomas of the choroid plexus are often hyperdense with calcification, and demonstrate homogeneous enhancement after contrast injection. Carcinomas are more heterogeneous in density, with homogeneous contrast enhancement and evidence of tumor necrosis or cyst formation. These lesions and their relation to the ventricle and adjacent neural structures are elegantly demonstrated on MRI.
Surgery is the treatment of choice for papillomas and carcinomas of the choroid plexus. Complete removal of either of these types of lesion may be associated with long disease-free survival. Because of the tendency for leptomeningeal spread, these patients must be monitored closely, and those with carcinomas may require radiotherapy and chemotherapy for control of disease.
Pituitary tumors
Clinical problems
Pituitary adenomas may present in one of three ways: (1) as an endocrinopathy, i.e. the abnormal release or suppression of hormones, causing an alteration in the body's hormonal function; or (2) as a mass lesion with growth of the tumor compressing neural or vascular structures; or (3) as a combination of those two.
Tumors that arise in the pituitary may be described as endocrine active (functional) or endocrine inactive (non-functional). The most common endocrine-active tumors are those that secrete prolactin, and the next most common are growth hormone- and adrenocorticotrophic hormone (ACTH)-producing tumors. Only occasional tumors produce luteinizing, follicle-stimulating, or thyroid-stimulating (TSH) hormones. The most common adjacent neural structure affected is the optic chiasm, causing bitemporal hemianopia.
Diagnosis and treatment
Pituitary adenomas may be treated surgically, medically, or with radiation. In many instances the therapeutic end-point is control rather than cure of the endocrinopathy. The goals of treatment in patients with functional pituitary adenomas are (1) to decompress any neural structures compromised by the tumor mass and (2) to restore and maintain normal hormone secretion.
Endocrine evaluation

Pituitary endocrine function can be assessed systematically. A normal morning serum cortisol usually reflects an intact hypothalamic–pituitary–adrenal axis. The pituitary–thyroid axis can be assumed intact if the serum thyroxine (T4) (total or free) is normal. Laboratory assessment may also include measurement of serum luteinizing and follicle-stimulating hormones and sex steroids (estradiol in women; testosterone in men). Prolactin should be assayed in all patients with pituitary tumors, especially apparently nonfunctional tumors. Growth hormone and somatomedin-C levels are required if there is clinical suspicion of acromegaly. Growth hormone deficiency may be clinically significant in adults and should be evaluated in all children with pituitary or hypothalamic lesions.
Imaging studies
MRI has become the primary modality for diseases of the sellar and parasellar region. The most definitive study using MRI involves thin coronal, sagittal, and axial slices combined with administration of gadolinium. With this technique, the normal pituitary gland, cavernous sinus, and infundibulum enhance immediately. Microadenomas do not enhance immediately and therefore show up as areas of decreased signal intensity.
Treatment
Surgery is the preferred treatment for most pituitary tumors. The two most common procedures used are trans-sphenoidal adenomectomy and craniotomy. The goals of surgery are: (1) to decompress neural structures, particularly the optic nerves; (2) to correct the endocrine dysfunction; (3) to obtain a histologic diagnosis; and (4) to remove the tumor completely, if feasible.
The trans-sphenoidal approach is favored by most surgeons because it is safer and more effective than craniotomy. Trans-sphenoidal adenomectomy is the procedure of choice for pituitary adenomas that cause Cushing disease and acromegaly, and for some prolactinomas. Morbidity and mortality are low when the trans-sphenoidal procedure is done by an experienced surgeon.
Hydrocortisone (100 mg) is given intravenously before surgery and tapered postoperatively. The primary considerations in the postoperative period are fluid and electrolyte balance, and corticosteroid coverage. Most instances of postoperative diabetes insipidus after trans-sphenoidal surgery are transient and resolve spontaneously.
Currently, there are no cytotoxic drugs that cure pituitary adenomas. Therefore the options for treating these lesions medically are limited to attempts to (1) reduce the excessive amounts of hormone associated with certain hypersecretory tumors, and (2) reduce the size of certain others.
Because trans-sphenoidal adenomectomy has produced such excellent results in the treatment of pituitary adenomas, radiation usually is reserved for adjunctive treatment with recurrent or residual tumors. Use of radiation as the primary treatment usually is reserved for patients who cannot undergo surgery for medical reasons or for those who refuse surgery.
Endocrine-inactive tumors
Clinical presentation
The symptoms of endocrine-inactive tumors usually relate to loss of pituitary hormonal function and mass effect because patients commonly have tumors that have grown to considerable size before being recognized.
A careful history taken from a patient with an endocrine-inactive tumor who is being examined because of loss of vision almost always reveals symptoms consistent with loss of endocrine function that considerably predate the onset of that loss. In women these symptoms may include early menopause or infertility, and in men the symptoms include lack of potency or infertility. Both men and women may experience excessive fatigue, inability to tolerate temperature extremes, and decreased hair growth. Headache is not an uncommon symptom and when present has one of two basic components: pain referred to the vertex of the skull, reflecting pressure on to the diaphragm of the sella, or pain referred to the retro-orbital and supraorbital areas from pressure on the ophthalmic division of the trigeminal nerve.
Prolactinomas
Clinical presentation
Women with prolactinomas usually see a physician because they have experienced amenorrhea, galactorrhea, or infertility. Hyperprolactinemia also suppresses gonadal function in men, but because of insidious onset, denial, or reluctance, decreased libido or erectile impotence do not often bring men to their physicians. This delay may account in part for the disproportionate number of macroprolactinomas (larger than 10 mm in diameter) in men, whereas these account for only 5 to 10 per cent of all prolactinomas in women.
Physical examination in sexually developed women reveals galactorrhea in more than 85 per cent of patients. Abnormal physical findings in men include galactorrhea, gynecomastia, and testicular atrophy. If the serum prolactin is above 200 ng/l the patient almost certainly has a prolactinoma.
Management
Surgical
The most successful cure rates (60–70 per cent) are reported by centers in which an experienced surgeon performs the surgery, and when the tumors are microadenomas and the prolactin is below 200 ng/ml. When surgery is successful, galactorrhea stops, normal menstrual cycles resume, and the prolactin normalizes below 25 ng/ml.
Medical
Various hormone treatments have been used for prolactin-secreting tumors, but the most common drug treatment is the ergot derivative bromocriptine. The most common side-effects are nausea and vomiting, dizziness, and sedation. More recently, carbegoline (Dostinex) has become available; this has the advantage of weekly or twice-weekly dosing compared with daily dosing for bromocriptine.
Acromegaly

Acromegaly is an uncommon condition, with an incidence of 500 to 1000 cases each year in the United States. It accounts for approximately 10 per cent of all pituitary tumors. Acromegaly poses a significant risk to health and may shorten life expectancy if left untreated.
Clinical presentation
The most common manifestations of acromegaly are swelling of soft tissue and skin thickening. Headache, excessive perspiration (hyperhidrosis), altered menses, decreased libido, and dysesthesias (e.g. carpal tunnel syndrome) resulting from nerve entrapment are all common complaints.
Endocrine evaluation
Basal concentrations of growth hormone, and of somatomedin-C or insulin-like growth factor-I, are elevated. Somatomedin-C provides an essential means of confirming the diagnosis of acromegaly.
Management
Surgical
The optimal surgical treatment is selective, total removal of the growth hormone-secreting pituitary adenoma.
Medical
Currently the mainstay of drug therapy for acromegaly is octreotide, which is given by subcutaneous injection.
Cushing disease
Cushing disease is a pituitary-dependent excess secretion of ACTH. It affects women more often than men, and poses a significant threat to health and life expectancy. Adult sufferers complain of weakness, weight gain, easy bruising, pyschologic changes, excess body hair, oligomenorrhea, change in facial shape and color, and bone pain.
Physical examination reveals centripetal obesity, muscle wasting, thin skin with ecchymoses and telangiectasias, intertriginous fungal infections, and facial plethora. Often a fine, downy hirsutism in the ‘sideburn' area, violaceous stretch marks, and acne are present. Men have a reduction in testicular size, impotence, and loss of body hair. Diabetes and hypertension are very common, and signs of congestive heart failure with edema may be present.
Diagnostic studies
Measuring free cortisol in a 24-h sample (i.e., urinary free cortisol) from an unstressed patient provides a reliable indication of cortisol production. Another useful screening test for Cushing syndrome is the overnight dexamethasone suppression test. Plasma ACTH is elevated in patients with Cushing disease and in those with an ectopic source of ACTH.

Sampling from the petrosal sinus was developed to establish a pituitary origin for Cushing disease in patients with negative MRI and to lateralize the tumor within the gland by establishing a differential in ACTH concentrations between the left and right sinuses draining the pituitary gland.
Medical management
Currently, ketoconazole is the most effective drug available for treating Cushing disease.
Gonadrotropin-secreting adenomas
Clinical presentation
Because they cause relatively few symptoms, gonadotropin-secreting adenomas frequently go undetected. Most of these tumors occur in middle-aged men; they are uncommon in women of reproductive age. Headaches and visual problems are common symptoms.
TSH-secreting adenomas
Clinical presentation
Tumors that secrete TSH are the least common adenomas, accounting for less than 1 per cent. They are usually macroadenomas and manifest with compressive symptoms. Some patients have hyperthyroidism with goiter.
Future directions in pituitary surgery
Endoscopy is being used in surgery to improve visualization. Intraoperative ultrasonography and MRI are also available for real-time assessment of tumor resection. Molecular analysis of pituitary tumorigenesis is an active area of research.
Intracranial epidermoid tumors
Epidermoid tumors are congenital neoplasms that grow through desquamation of keratin, cholesterol, and cellular debris. They are histologically benign, but rare malignant degeneration does occur. Intracranial epidermoid tumors account for approximately 1 to 2 per cent of all brain tumors; the most common locations are parachiasmal and in the cerebellopontine angle; they may also occur in the calvarium. The natural history of the intracranial tumors is a slow, relentless progression of symptoms. They are rarely asymptomatic. Specific signs and symptoms depend upon the location of the tumor. Seizures are a common presenting symptom. They may also present with recurrent episodes of aseptic meningitis.
MRI has revolutionized the diagnosis of these tumors. In T1 images the epidermoid is well defined and separable from normal tissues; in T2 images the tumors have high signal intensity. They rarely enhance.
Supratentorial tumors
Patients with suprasellar tumors typically present with visual complaints.
Infratentorial tumors
Tumors of the cerebellopontine angle may present with hearing loss, dizziness, or trigeminal paresthesias.
Treatment
The goal of surgery is total removal: the real issue is the difficulty of removing every bit of capsule; if the entire capsule is not removed, recurrence is the rule. The second major problem with surgery is the noxious nature of the cholesterol/keratin material that constitutes the bulk of the tumor. If this material escapes into the subarachnoid space, the result can be a meningitis that may be highly disabling and can produce permanent cranial-nerve deficits.
Craniopharyngioma
Craniopharyngiomas are epithelial tumors derived from the vanishing hypophyseal duct during the formation of Rathke's pouch. They may be intrasellar, suprasellar, intraventricular, or in combinations of these locales. Because of their central location they may be anatomically related to many neural and vascular structures. Inferiorly, the pituitary gland and stalk may be in close proximity. Anteriorly, the suprasellar cistern contains the optic nerves and chiasm, the carotid arteries and their branches. Superiorly, the hypothalamus, and posteriorly, the midbrain and cranial nerves III, IV, V, and VI may be encountered, as well as the basilar artery and its branches. These tumors comprise 2.5 to 4 per cent of all brain tumors and about half occur in childhood.
Clinical features
The majority of patients with craniopharyngiomas present with ophthalmologic symptoms. Other clinical symptoms include headaches, seizures, or neurologic deficits.
Surgical treatment
A number of surgical routes have been used to reach these tumors, including the subfrontal, transcortical–transventricular, transcal-losal, trans-sphenoidal, subtemporal, pterional, and stereotactic approaches. The route selected depends on the location and anatomic relations of the tumor, and the preference of the surgeon.
Endocrinologic compromise and its management
The activity of the hypothalamic–pituitary axis should be assessed to determine the extent of hormonal disturbance before and after surgery. Endocrinologic compromise may be neurohypophyseal or adenohypophyseal. Neurohypophyseal compromise is usually manifested by disturbances in fluid and electrolyte balance; specifically, the disorders of diabetes insipidus and the syndrome of inappropriate antidiuretic hormone secretion.
Adenohypophyseal
Deficiencies may be of ACTH or thyrotropin (TSH); these must be replaced in the preoperative and perioperative period. Long-term replacement is also frequently necessary.
Radiation
Postoperative radiation may be useful in treating residual tumor. In children this should be used judiciously because of deleterious effects on intelligence. Radiation may be delivered as interstitial intracavitary therapy or conventional external radiotherapy. Total removal of craniopharyngiomas is often not achievable; therefore, radiation serves as an important adjuvant treatment.
Brain metastases
Introduction
The spread of systemic cancer to the nervous system has been estimated to occur in 20 to 40 per cent of patients. Direct spread into the brain parenchyma is by far the most common, although nearly 10 per cent of patients have extension of tumor into the leptomeninges (neoplastic meningitis) or dura. The actual incidence of central nervous metastases has been difficult to determine because of variability in the methods of assessment (clinical, radiographic, or autopsy) used to make the diagnosis. More recent studies, using modern imaging techniques, are yielding the highest incidences.
The frequency of spread to the central nervous system varies with the type of cancer (Table 2). Some, such as malignant melanoma, have a distinct predilection to metastasize to brain; in many series malignant melanoma is the third most common histologic type of brain metastasis despite the relatively low incidence of this tumor. Lung cancer, particularly small cell, is the most common primary. Breast cancer, a very common cancer with an often prolonged survival, frequently spreads to the central nervous system. Prostate cancer, despite its high incidence and prolonged survival, rarely produces brain metastases.
Table 2 Brain metastases by primary tumor type
Brain metastases are most commonly hematogenous, which provides a reasonable explanation for their frequent development at the gray–white junction, a ‘watershed' zone in the cerebral vasculature (Fig. 16). The location of metastatic lesions generally follows the volume of blood flow, with 90 per cent in the supratentorial region and 10 per cent developing infratentorially. The exceptions to this are the retroperitoneal cancers, such as uterine, cervical and bladder, which frequently spread to the posterior fossa, attributed to tumor infiltration of Batson's venous plexus in the pelvis. Renal-cell carcinoma, although retroperitoneal, does not preferentially spread to the posterior fossa. A second potential mechanism of spread to the brain is via the subarachnoid space
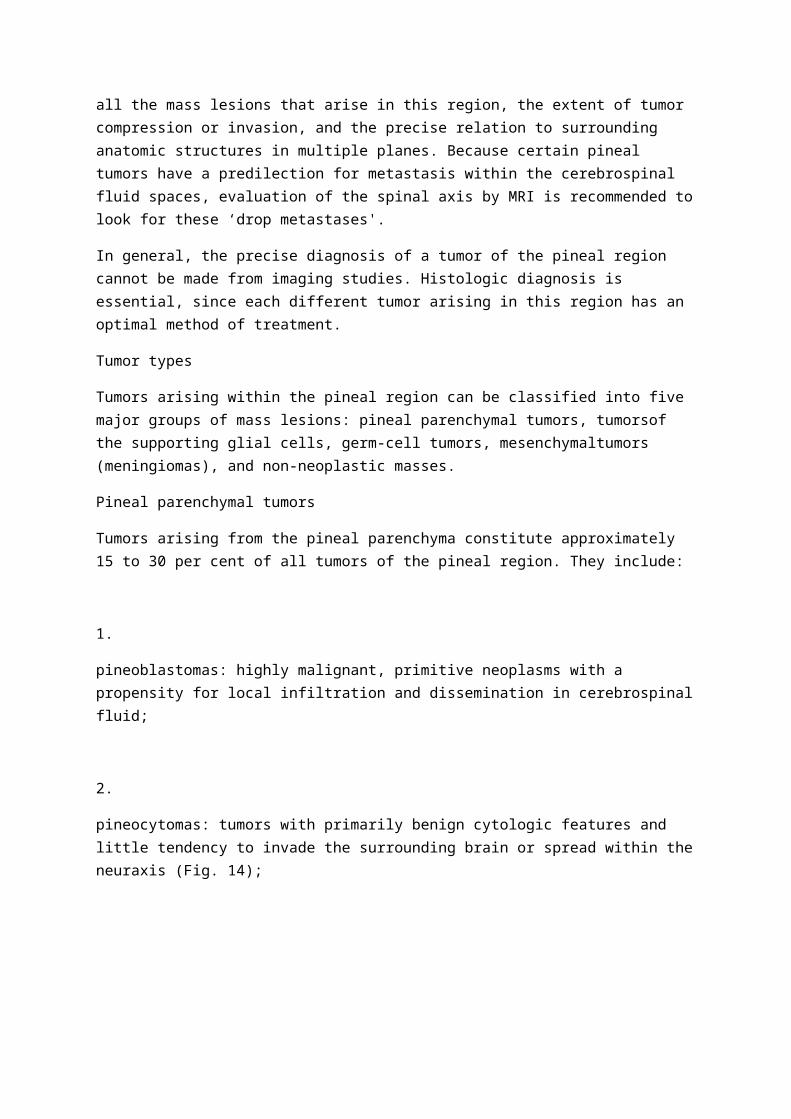
(leptomeningeal dissemination). The detection of tumor nodules adjacent to cerebrospinal fluid, such as in brain sulci or in the wall of a ventricle, suggests that the tumor is from a deposit evolving from leptomeningeal dissemination (Fig. 17).
Fig. 16. Multiple metastases in a 52-year-old man with metastatic malignant melanoma; the lesions are at the gray–white junction.
Fig. 17. Multiple brain metastases in a 54-year-old man with metastatic melanoma; the tumor nodules arise from sulci, indicating that these lesions arise from a deposit of tumor from the leptomeninges.
Diagnostic evaluations
Clinical symptoms and signs are dependent upon the location of the lesion(s) and the rapidity of growth or change in size. A slow-growing tumor may cause only subtle neurologic or cognitive changes despite achieving a large size, whereas a rapidly growing tumor or acute hemorrhage may cause sudden neurologic symptoms. Multiple lesions are more likely to cause changes in the sensorium or cognitive function.
Radiologic imaging is essential in diagnosing brain metastases. Contrast-enhanced MRI has proved to be the most effective modality (Fig. 16). Double-dose contrast CT, although less sensitive, can also be used. Nearly all brain metastases will enhance with contrast material, although very small lesions may be detected only as a T2 signal abnormality on MRI.
The need for pathologic confirmation of metastatic tumor depends upon the clinical setting. Patients with multiple enhancing brain lesions and a known systemic malignancy generally do not require biopsy. Patients without known cancer should have pathologic confirmation prior to treatment. Patients with established systemic cancer and a single brain lesion should have either a resection or stereotactic biopsy to confirm the diagnosis. A recent series demonstrated that 11 per cent of patients with known systemic cancer and a solitary enhancing brain lesion did not have a brain metastases.
Treatment
Supportive care includes the use of corticosteroids to decrease peritumoral edema. Anticonvulsants are generally reserved for patients with known seizures or with metastatic lesions from melanoma, renal-cell carcinoma or choriocarcinoma, tumors that have a high likelihood of spontaneous hemorrhage.
The treatment of brain metastases is determined by several critical factors: (1) number of lesions; (2) extent of the systemic malignancy; and (3) performance status. Several other factors, including the responsiveness of the tumor to chemotherapy and/or radiation, are also potentially important.
Patients with a solitary metastases (one brain lesion, no active systemic cancer) benefit from surgical resection of the tumor and would likely benefit from radiosurgery if the lesion is not surgically accessible. Current recommendations include postoperative whole-brain radiotherapy. Patients with a single brain metastasis but active systemic disease may benefit from resection or radiosurgery if the anticipated survival from the systemic disease exceeds 4 to 6 months.
Patients with multiple brain metastases are commonly treated with whole-brain radiotherapy. Surgical resection of one of the lesions, if it is large and causing mass effect or compromising neurologic function, may be indicated. No consensus exists on the optimal treatment schema, although most treatment programs administer 3000 cGy to the whole brain in 300-cGy fractions. Some radiotherapists recommend a more prolonged course (4400–5000 cGy) in 200-cGy fractions for patients with a better prognosis (age under 60 years, limited systemic disease, Karnofsky performance status above 70). Although these treatment strategies have similar efficacy, the convenience of fewer treatments is offset by an increase in risk for neurotoxicity, especially in patients with a better prognosis. Radiosurgery is now being investigated as a treatment for patients with three or fewer metastatic lesions. There are reports of surgical resection of multiple metastases, but the efficacy has been variable.
Chemotherapy is reportedly effective in patients with sensitive tumors. There are reports of response rates greater than 50 per cent for combined chemotherapy treatment of germ-cell tumors, lymphomas, breast cancer, and small-cell lung cancer. Delivery of the chemotherapeutic drugs to the brain lesions has been adequate, likely because of the local disruption of the blood–brain barrier, evident by contrast enhancement.
Outcome
The recent advances in imaging modalities as well as radiotherapy and surgical techniques has improved the outcome for patients with brain metastases. Early reports state an average survival of 1 month with no treatment, 2 months with corticosteroids and supportive care. Current treatment

approaches have resulted in improved control of brain metastases; less than half of the patients die as a result of the brain lesions. Newer approaches to treatment, such as local chemotherapy or brachytherapy, and expanding the role of radiosurgery, will likely further improve treatment and outcome for these patients.
Primary lymphoma of the central nervous system
Introduction
Primary lymphoma of the central nervous system was once considered a rare neoplasm, but there has been a marked increase in its incidence in both immunocompetent and immunocompromised patients. Current epidemiologic studies report a threefold increase in incidence in immunocompetent individuals over the past 10 years, and a 4 to 6 per cent incidence in patients with acquired immune deficiency syndrome (AIDS).
The origin of the tumor cells is uncertain. Hypotheses include the malignant transformation of a lymphocyte clone that has cell-surface adhesion molecules specific for central nervous infiltration or that systemic immunity limits an otherwise systemic lymphoma to the central nervous system. Rarely does the tumor spread outside the central nervous system.
The majority of primary lymphomas of the central nervous system are of B-cell origin. The histologic classifications commonly seen include diffuse large-cell, immunoblastic, lymphoblastic, or small non-cleaved cells. The pathogenesis of the tumor is uncertain and no genetic predisposition has yet been established. In patients with immunodeficiency, a high percentage of tumors have a portion of the Epstein–Barr virus in the tumor cell genome; this is only rarely found in primary lymphoma of the central nervous system from immunocompetent patients.
Diagnosis
Patients often present with global neurologic symptoms including headache and alterations in mentation or level of conscious. The signs and symptoms at presentation in immunocompetent patients is somewhat different from patients with AIDS-related primary lymphoma of the central nervous system (Table 3). The symptoms often develop subacutely, over days to weeks, underscoring the rapid growth of the tumor. A complete physical examination is essential to exclude evidence of systemic lymphoma, which would preclude the diagnosis of primary lymphoma of the central nervous system.
Table 3 Signs and symptoms of lymphoma of the central nervous system

Brain imaging by contrast-enhanced CT or MRI is essential for making the diagnosis. More than 80 per cent of these tumors are enhancing; 50 per cent show a homogeneous enhancing pattern in contradistinction to metastatic cancer or primary glial neoplasms, where a ring enhancing pattern is most common (Fig. 18). The tumor is often multifocal and, although it can develop in all regions of the central nervous system, the most common location is periventricular.
Fig. 18. Axial T1-weighted gadolinium-enhanced MRI showing a homogeneously enhancing, primary lymphoma of the central nervous system presenting in the splenium of the corpus callosum.
Systemic evaluation for evidence of tumor outside the central nervous system is controversial. Some advocate CT scans of the chest, abdomen and pelvis, along with examination of bone marrow. Others argue that the yield is extremely low and therefore that extensive testing is unnecessary.
Pathologic diagnosis is critical to confirm the presence of lymphoma. The tumor is characteristically vasocentric, with infiltration of the blood-vessel wall (Fig. 19). Currently, stereotactic biopsy is the preferred method of obtaining tissue. The diagnosis can be confirmed from the small sample of tissue using immunohistochemistry to prove the monoclonal nature of the cells. Extensive resection has not improved outcome, but is associated with loss of neurologic function. These tumors can be extremely responsive to corticosteroids; reports indicate a 20 per cent rate of complete tumor resolution with steroid treatment. Subsequent biopsy then reveals only necrosis and gliosis. Therefore, in suspected cases of primary lymphoma of the central nervous system, steroids should be withheld until the biopsy is complete unless tumor-associated mass effect is severe.
Fig. 19. Histopathology of lymphoma of the central nervous system. The tissue section is stained with hematoxylin–eosin, demonstrating the infiltration of malignant lymphocytes into the wall of a blood vessel and surrounding brain parenchyma.
Staging requires determination of the extent of involvement of the central nervous system. The tumor has a high propensity to infiltrate into the leptomeninges (60–100 per cent) and, although cranial-nerve palsies and other signs of leptomeningeal tumor are unusual at the time of diagnosis, failure to treat this tumor adequately will result in future relapse. In addition, ocular involvement is common, with infiltration of the vitreous. Therefore, all patients should undergo slit-lamp examination with possible vitreal biopsy to evaluate for tumor.
Management
As mentioned above, surgical resection has little role in the management of primary lymphoma of the central nervous system. External-beam radiotherapy has been proved to benefit patients; median survival increases from 2 to 3 months with supportive care to 12 months with radiotherapy. Many treatment algorithms exist, although most recommend whole-brain radiotherapy using 4000 to 5000 cGy. Some treatment plans also include a boost of 1200 to 1500 cGy to the tumor bed.
Chemotherapy has been shown to benefit patients with primary lymphoma of the central nervous system. The initial studies utilized chemotherapy for patients with recurrent disease after radiotherapy; more recently, preradiation chemotherapy has been utilized. All studies reported to date are small series using a variety of regimens. No prospective, randomized (phase III) study has been completed. The current regimens incorporate treatment for tumor behind the blood–brain barrier and tumor in the leptomeninges. Often, therapy requires direct intrathecal delivery by lumbar puncture or intraventricular delivery via a reservoir and intraventricular catheter system. Treatment of ocular involvement is not well established. Some chemotherapeutic agents (methotrexate, cytosine arabinoside) penetrate the vitreous, but most protocols recommend subsequent radiotherapy to the posterior two-thirds of the eye.
The optimal treatment for primary lymphoma of the central nervous system is evolving. Multiple studies suggest that there are several prognostic factors such as age (under 50 years), absence of immunodeficiency state, and good performance status that correlate with better outcome. Several series report survival in excess of 5 years in some patients with good prognostic factors. Some current studies are examining the role of chemotherapy, withholding radiotherapy until there is tumor relapse in an effort to reduce the neurotoxicity of the radiation treatment.
Further reading
General information
Burger PC. Classification, grading and patterns of spread of malignant gliomas. In: Apuzzo MLJ, ed. Malignant cerebral glioma, pp. 3–18. American Association of Neurological Surgeons, Park Ridge IL, 1990.
Jaeckle KA. Clinical presentation and therapy of nervous system tumors. In: Bradley WG, Darhoff RB, Fenichel GM, Marsden CD, ed. Neurology in clinical practice, pp. 1008–30. Butterworth-Heinemann, Boston, 1991.
Kleihues P, Burger PC, Scheithauer BW. World Health Organization international histological classification of tumours. Histological typing of tumours of the central nervous system, 2nd edn. Springer, Berlin, 1993.
Kleihues P, Cavenee WK. WHO classification of tumors of the nervous system. In: Kleihues P, Cavenee WK, eds. World Health Organization classification of tumours. Pathology and genetics. Tumours of the nervous system. IARC Press, Lyon, 2000
Kraemer DL, Bullard DE. Clinical presentation of the brain tumor patient. In: Morantz RA, Walsh JW, eds. Brain tumors: a comprehensive text, pp. 183–212. Marcel Dekker, New York, 1994.
Leeds NE, Kumar AJ. Diagnostic imaging: magnetic resonance imaging and computed tomography. In: Levin VA, ed. Cancer in the nervous system, pp. 13–49. Churchill Livingstone, New York, 1996.
Wen PY, Schiff D. Clinical evaluation of patients with astrocytomas. In: Black PM, Schoene WC, Lampson LA, ed. Contemporary issues in neurological surgery: astrocytomas: diagnosis, treatment, and biology, pp. 26–36. Blackwell Scientific, Boston, 1993.
Primary brain tumors
Evans RG. The role of radiation therapy in the treatment of adult brain tumors. In: Morantz RA, Walsh JW, ed. Brain tumors, pp. 643–57. Marcel Dekker, New York, 1994.
Loeffler JS, Alexander E, III. The role of radiotherapy in the management of astrocytomas. In: Black PM, Schoene WC, Lampson LA, ed. Contemporary issues in neurological surgery. astrocytomas: diagnosis, treatment and biology, pp. 73–85. Blackwell Scientific, Boston, 1993.
Maciunas RJ. Adjunctive management of gliomas. In: Tindall GT, Cooper PR, Barrow DL, ed. The practice of neurosurgery, pp. 671–82. Williams and Wilkins, Baltimore, 1996.
Roth JG, Elvidge AR. Glioblastoma multiforme: a clinical survey. Journal of Neurosurgery 1960; 17: 736–50.
Salcman M. Glioblastoma and malignant astrocytoma. In: Kaye AH, Laws ER, Jr. ed. Brain tumors: an encyclopedic approach, pp. 449–78. Churchill Livingstone, Edinburgh, 1995.
Astrocytoma
Berger MS, Leibel SA, Bruner JM, Finlay JL, Levin VA. Primary central nervous system tumors of the supratentorial compartment. In: Levin VA, ed. Cancer in the nervous system, pp. 57–126. Churchill Livingstone, New York, 1996.
Kepes JJ, Louis DN, Paulus W. Pleomorphic xanthoastrocytoma. In: Kleihues P, Cavenee WK, ed. Tumours of the nervous system. Pathology and genetics, pp. 34–6. International Agency for Research on Cancer, Lyon, 1997.

Kleihues P, Davis RL, Ohgaki H, Cavenee WK. Low-grade diffuse astrocytomas. In: Kleihues P, Cavenee WK, ed. Tumours of the nervous system. Pathology and genetics, pp. 10–13. International Agency for Research on Cancer, Lyon, 1997.
Weistler OD, Lopez BS, Crino PB. Tuberous sclerosis and subependymal giant cell astrocytoma. In: Kleihues P, Cavenee WK, ed. Tumours of the nervous system. Pathology and genetics, pp. 182–4. International Agency for Research on Cancer, Lyon, 1997.
Oligodendroglioma and anaplastic oligodendroglioma
Bullard DE. Surgical aspects and general management of oligodendrogliomas. In: Apuzzo MLJ, ed. Benign cerebral glioma, Vol. II, pp. 397–412. American Association of Neurological Surgeons, Park Ridge IL, 1995.
Reifenberger G, Kros JM, Schiffer D, Collins VP. Oligodendroglioma, anaplastic oligodendroglioma. In: Kleihues P, Cavenee WK, ed. Tumours of the nervous system. Pathology and genetics, pp. 38–44. International Agency for Research on Cancer, Lyon, 1997.
Shaw EG, Scheithauer BW, O'Fallon JR, Tazelaar HD, Davis DH. Oligodendrogliomas: the Mayo Clinic experience. Journal of Neurosurgery 1992; 76(3): 428–34.
Ependymoma
Constantini S, Epstein FJ. Primary spinal cord tumors. In: Levin VA, ed. Cancer in the nervous system, pp. 127–37. Churchill Livingstone, New York, 1996.
Duncan JA, III, Hoffman HJ. Surgical aspects and general management of ependymomas. In: Apuzzo MLJ, ed. Benign cerebral glioma, Vol. II, pp. 413–26. American Association of Neurological Surgeons, Park Ridge IL, 1995.
Medulloblastoma
Berger MS, Magrassi L, Geyer R. Medulloblastoma and primitive neuroectodermal tumors. In: Kaye AH, Laws ER, Jr, ed. Brain tumors, pp. 561–74. Churchill Livingstone, Edinburgh, 1995.
Giangaspero F, Bigner SH, Giordana MT, Kleihues P, Trojanowski JQ. Medulloblastoma. In: Kleihues P, Cavenee WK, ed. Tumours of the nervous system. Pathology and genetics, pp. 96–103. International Agency for Research on Cancer, Lyon, 1997.
Wisoff JH, Epstein JH. Management of pediatric brain tumors. In: Morantz RA, Walsh JW, ed. Brain tumors: a comprehensive text, pp. 581–611. Marcel Dekker, New York, 1994.
Neuronal and mixed neuronal and glial tumors: ganglioglioma and neurocytoma
Chen TC, Gonzalez-Gomez I, McComb JG. Uncommon glial tumors. In: Kaye AH, Laws ER, Jr, ed. Brain tumors, pp. 525–57. Churchill Livingstone, Edinburgh, 1995.
Silver JM, Rawlings CE, Rossitch ER, Zeidman SM, Friedman AH. Gangliomas: a clinical study with long-term follow-up. Surgical Neurology 1991; 35: 261–6.

Chordoma
Eriksson B, Gunterberg B, Kindblom LG. Chordoma, a clinicopathologic and prognostic study of a Swedish national series. Acta Orthopaedica Scandinavica 1981; 52: 49–58.
Forsyth PA et al. Intracranial chordomas: a clinicopathological and prognostic study of 51 cases. Journal of Neurosurgery 1993; 78: 741–7.
Gay E, Sekhar LN, Wright DC. Chordomas and chondrosarcomas of the cranial base. In: Kaye AH, Laws ER, Jr, ed. Brain tumors, pp. 777–94. Churchill Livingstone, Edinburgh, 1995.
Sundaresan N, Krol G, Hughes JEO, Hough L. Tumors of the spine: diagnosis and management. In: Tindall GT, Cooper PR, Barrow DL, ed. The practice of neurosurgery, pp. 1303–22. Williams and Wilkins, Baltimore, 1996.
Esthesioneuroblastoma
Ebersold MJ, Olsen KD, Roote RL, Buckner JC, Quast LM. Esthesioneuroblastoma. In: Kaye AH, Laws ER, Jr, ed. Brain tumors, pp. 825–38. Churchill Livingstone, Edinburgh, 1995.
Hyams VJ, Batsakis JG, Michaels L. Tumors of the upper respiratory tract and ear. Atlas of tumor pathology, 2nd series, Fascicle 25, pp. 240–8. Armed Forces Institute of Pathology, Washington DC, 1988.
Nasopharyngeal carcinoma
Cacayorin ED, Petro GR, Kieffer SA. Radiology of skull-base neoplasms. In: Long DM, ed. Contemporary issues in neurological surgery: surgery for skull base tumors, pp. 1–30. Blackwell Scientific, Boston, 1992.
Danks RA, Kaye AH. Carcinoma of the paranasal sinuses. In: Kaye AH, Laws ER, Jr, ed. Brain tumors, pp. 809–24. Churchill Livingstone, Edinburgh, 1995.
Rousseau GL, Sekhar LN. Surgery of cranial base tumors. In: Morantz RA, Walsh JW, ed. Brain tumors: a comprehensive text, pp. 451–91. Marcel Dekker, New York, 1994.
Glomus tumor
Batnitzky S, Eckard DA. The radiology of brain tumors: general considerations and neoplasms of the posterior fossa. In: Morantz RA, Walsh JW, ed. Brain tumors: a comprehensive text, pp. 213–72. Marcel Dekker, New York, 1994.
Ebersold MJ, Morita A, Olsen KD, Quast LM. Glomus jugulare tumors. In: Kaye AH, Laws ER, Jr, ed. Brain tumors, pp. 795–807. Churchill Livingstone, Edinburgh, 1995.
P>Holliday MJ. A two-staged planned removal of glomus tumors. In: Long DM, ed. Contemporary issues in neurological surgery: surgery for skull base tumors, pp. 247–53. Blackwell Scientific, Boston, 1992.
Soffer D. Paraganglioma. In: Kleihues P, Cavenee WK, ed. Tumours of the nervous system. Pathology and genetics, pp. 80–2. International Agency for Research on Cancer, Lyon, 1997.
Neurofibromas and schwannomas
Eisenberg MB, Catalano PJ. Management of acoustic schwannomas. In: Tindall GT, Cooper PR, Barrow DL, ed. The practice of neurosurgery, pp. 995–1004. Williams and Wilkins, Baltimore, 1996.
Freeman TB, Cahill DW. Management of intradural extramedullary tumors. In: Tindall GT, Cooper PR, Barrow DL, ed. The practice of neurosurgery, pp. 1323–34. Williams and Wilkins, Baltimore, 1996.
Pineal tumors
Apuzzo MLJ. Surgery of the third ventricle. Williams and Wilkins, Baltimore, 1987.
Bruce JN, Stein BM. Management of pineal tumors. In: Tindall GT, Cooper PR, Barrow DL, ed. The practice of neurosurgery, pp. 875–87. Williams and Wilkins, Baltimore, 1996.
Neuwelt EA, O'Neill OR, Roman-Goldstein S, Shults T. Clinical features and imaging of pineal region tumors. In: Tindall GT, Cooper PR, Barrow DL, ed. The practice of neurosurgery, pp. 857–74. Williams and Wilkins, Baltimore, 1996.
Meningiomas and choroid plexus tumors
Al-Mefty, O. Operative atlas of meningiomas. Lippincott Raven, Philadelphia, 1998.
DeMonte F, Al-Mefty, O. Management of meningiomas. In: Tindall GT, Cooper PR, Barrow DL, ed. The practice of neurosurgery, pp. 691–714. Williams and Wilkins, Baltimore, 1996.
Halliday Al, Harsh GR, IV. Meningiomas: clinical features. In: Tindall GT, Cooper PR, Barrow DL, ed. The practice of neurosurgery, pp. 683–90. Williams and Wilkins, Baltimore, 1996.
Brain metastases
Berk L. An overview of radiotherapy trials for the treatment of brain metastases. Oncology 1995; 9: 1205–19.
Black PM. Solitary brain metastases. Radiation, resection or radiosurgery? Chest 1993; 103 (Suppl.): 367–9S.
Buckner JC. The role of chemotherapy in the treatment of patients with brain metastases from solid tumors. Cancer and Metastases Reviews 1991; 10: 335–341.
Coia LR, Aaronson N, Linggood R, Loeffler J, Priestman TJ. A report of the consensus workshop panel on the treatment of brain metastases. International Journal of Radiation, Oncology, Biology, Physics 1992; 23: 223–7.
DeAngelis LM. Management of brain metastases. Cancer Investigation 1994; 12: 156–65.
Patchell RA. The treatment of brain metastases. Cancer Investigation 1996; 14: 169–77.
Shiau C-Y et al. Radiosurgery for brain metastases: relationship of dose and pattern of enhancement to local control. International Journal of Radiation, Oncology, Biology, Physics 1997; 37: 375–83.
Primary central nervous system lymphoma
DeAngelis LM. Primary central nervous system lymphoma. Recent Results in Cancer Research 1994; 135: 155–69.
DeAngelis LM. Current management of primary central nervous system lymphoma. Oncology 1995; 9: 63–71.
Ferreri AJM, Reni M, Villa E. Primary central nervous system lymphoma in immunocompetent patients. Cancer Treatment Reviews 1995; 21: 415–46.
Fine HA, Mayer RJ. Primary central nervous system lymphoma. Annals of Internal Medicine 1993; 119: 1093–104.
Reni M, Ferreri AJM, Garancini MP, Villa E. Therapeutic management of primary central nervous system lymphoma in immunocompetent patients: results of a critical review of the literature. Annals of Oncology 1997; 8: 227–234.
Related Documents

![Near Real-Time Computer Assisted Surgery for Brain Shift ...bmlweb.vuse.vanderbilt.edu/~migami/PUBS/jtehm2014.pdf · patient’s brain [26], tumor and intracranial support struc-tures,](https://static.cupdf.com/doc/110x72/5c9f25d188c993362d8ce81d/near-real-time-computer-assisted-surgery-for-brain-shift-migamipubsjtehm2014pdf.jpg)









