Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery (Review) Kumar S, Wong PF, Leaper DJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2009, Issue 4 http://www.thecochranelibrary.com Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery (Review) Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Intra-peritoneal prophylactic agents for preventing adhesions
and adhesive intestinal obstruction after non-gynaecological
abdominal surgery (Review)
Kumar S, Wong PF, Leaper DJ
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2009, Issue 4
http://www.thecochranelibrary.com
Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
13ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
13REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
15CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
22DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 HA/CMC membrane Versus Control, Outcome 1 Incidence of adhesions. . . . . . 23
Analysis 1.2. Comparison 1 HA/CMC membrane Versus Control, Outcome 2 Extent of adhesions. . . . . . . 23
Analysis 1.3. Comparison 1 HA/CMC membrane Versus Control, Outcome 3 Adverse events (Overall). . . . . . 24
Analysis 1.4. Comparison 1 HA/CMC membrane Versus Control, Outcome 4 Wound infection. . . . . . . . 24
Analysis 1.5. Comparison 1 HA/CMC membrane Versus Control, Outcome 5 Intra-abdominal or pelvic infection. . 25
Analysis 1.6. Comparison 1 HA/CMC membrane Versus Control, Outcome 6 Anastomotic leak. . . . . . . . 25
Analysis 1.7. Comparison 1 HA/CMC membrane Versus Control, Outcome 7 Fistula. . . . . . . . . . . . 26
Analysis 1.8. Comparison 1 HA/CMC membrane Versus Control, Outcome 8 Ileus. . . . . . . . . . . . 26
Analysis 1.9. Comparison 1 HA/CMC membrane Versus Control, Outcome 9 First episode of Intestinal obstruction (All
causes). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Analysis 1.10. Comparison 1 HA/CMC membrane Versus Control, Outcome 10 First episode of Intestinal obstruction
(Adhesive) needing surgery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Analysis 2.1. Comparison 2 Ferric Hyaluranate gel Versus Control, Outcome 1 Adverse events (Overall). . . . . 28
Analysis 2.2. Comparison 2 Ferric Hyaluranate gel Versus Control, Outcome 2 Protracted Ileus. . . . . . . . 29
Analysis 2.3. Comparison 2 Ferric Hyaluranate gel Versus Control, Outcome 3 Anastomotic leak. . . . . . . . 29
Analysis 2.4. Comparison 2 Ferric Hyaluranate gel Versus Control, Outcome 4 Wound infection. . . . . . . . 30
Analysis 2.5. Comparison 2 Ferric Hyaluranate gel Versus Control, Outcome 5 Mortality. . . . . . . . . . . 30
30WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
31INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iIntra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
[Intervention Review]
Intra-peritoneal prophylactic agents for preventing adhesionsand adhesive intestinal obstruction after non-gynaecologicalabdominal surgery
Senthil Kumar1, Peng F Wong2, David J Leaper3
1Directorate of Surgery, Queens Hospital, Romford, UK. 2Department of Surgery, University Hospital of North Tees, Hardwick, UK.3Department of Wound Healing, Cardiff University, Cardiff, UK
Contact address: Senthil Kumar, Directorate of Surgery, Queens Hospital, Rom Valley way, Romford, Essex, RM7 0AG, UK.
[email protected]. (Editorial group: Cochrane Colorectal Cancer Group.)
Cochrane Database of Systematic Reviews, Issue 4, 2009 (Status in this issue: Unchanged)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
DOI: 10.1002/14651858.CD005080.pub2
This version first published online: 21 January 2009 in Issue 1, 2009.
Last assessed as up-to-date: 2 August 2008. (Help document - Dates and Statuses explained)
This record should be cited as: Kumar S, Wong PF, Leaper DJ. Intra-peritoneal prophylactic agents for preventing adhesions and
adhesive intestinal obstruction after non-gynaecological abdominal surgery. Cochrane Database of Systematic Reviews 2009, Issue 1. Art.
No.: CD005080. DOI: 10.1002/14651858.CD005080.pub2.
A B S T R A C T
Background
Intra-abdominal adhesions are common and challenge patients, surgeons and other healthcare providers. They are potentially preventable
and several agents that act as barriers between adjacent peritoneal surfaces have been evaluated for prophylaxis. Efficacy, judged by
systematic reviews, has only been undertaken in gynaecological surgery.
Objectives
To determine efficacy and safety of peritoneal adhesion prophylaxis on incidence, distribution and adhesion-related intestinal obstruction
after non-gynaecological surgery.
Search strategy
The Cochrane Central Register of Controlled Trials, the Cochrane Colorectal Cancer Group specialised register, MEDLINE (1966-
2008), and EMBASE (1971-2008) were searched.
Selection criteria
Blinded and non-blinded, randomised and quasi-randomised clinical trials were considered.
Data collection and analysis
Two authors individually conducted the searches and assessed the quality of studies for inclusion which were analysed using the Revman
Analyses software 5.0.0 provided by the Cochrane collaboration. Meta-analysis used a random effects model.
Main results
Seven randomised trials were eligible; six compared hyaluronic acid/carboxymethyl membrane (HA/CMC) and one 0.5% ferric
hyaluronate gel against controls.
1Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
juliob
Resaltado
HA/CMC reduced the incidence of adhesions (OR 0.15 (95% CI: 0.05, 0.43); p=0.0005) with reduced extent (WMD -25.9% (95%
CI: -40.56, -11.26); p=0.0005) and severity. There was no reduction of intestinal obstruction needing surgical intervention (odds ratio:
0.84 (95% CI: 0.24, 2.7) with comparable overall morbidity and mortality.
The study of 0.5% ferric hyaluronate gel was prematurely terminated and no valid conclusions could be made but there was a higher
incidence of overall morbidity (OR 5.04; 95% CI: 1.1, 22.9) and ileus (OR: 9.29; 95% CI: 1.57, 54.77; p=0.01).
Authors’ conclusions
Implications for practice
There is evidence that the use of HA/CMC membrane reduces incidence, extent and severity of adhesions which may, theoretically, have
implications in re-operative abdominal surgery. There is no evidence that the incidence of intestinal obstruction or need for operative
intervention is reduced. HA/CMC appears to be safe but there may be a risk of leak when wrapped around an anastomoses. HA/CMC
may be considered for intra-abdominal, adhesion prophylaxis at a surgeon’s discretion and clinical context.
Implications for research
Further research is needed to explore the effectiveness of other agents in abdominal surgery in general. Synergism, using agents which
target different aspects of adhesiogenesis, with exploration effectiveness in a wide range of emergency and elective surgery should be
considered. Longer term outcomes of recurrent intestinal obstruction and chronic pain, identification of high risk groups of patients
with evaluation of cost-effectiveness are required.
P L A I N L A N G U A G E S U M M A R Y
The use of hyaluronic acid/carboxymethyl cellulose (HA/CMC) membrane, reduces the incidence, extent and severity of
adhesions in the abdomen.
Adhesions in the abdomen cause abnormal bonding between adjacent peritoneal surfaces and are common after operations in the
abdomen. They are composed of fibrous tissue but also contain blood vessels, fat and nerves. They result in a spectrum of problems
that affect the patient (intestinal blockage, infertility and possibly pain); the surgeon (difficulties in access and dissection, prolongation
of operative time, increase in blood loss, predisposition to bowel injury); the health care provider (increased cost due to readmissions
and litigation). Prevention is the key. This review focus on the evaluation of the safety and efficacy of two preventive agents applied
in the abdomen during general surgical operations, Hyaluronic acid /carboxymethyl cellulose membrane and 0.5% ferric hyaluronate
gel.
There is evidence to suggest that use of Hyaluronic acid/carboxymethyl cellulose membrane reduces the incidence, severity and extent
of adhesions.However, it does not reduce the incidence of subsequent intestinal obstruction or need for surgery to treat the obstruction,
when it occurs. It appears to be safe with no significant increase in adverse effects or deaths when compared to control. There is
limited data on 0.5% ferric hyaluronate gel with only one study available. This study did not report on the efficacy of the gel as it was
prematurely terminated because of a significantly higher rate of adverse effects in the patients who were treated with this gel.
B A C K G R O U N D
Intra-abdominal adhesions are usually iatrogenic, affect both gen-
ders and all ages. They may occur in up to 95% of patients who
had undergone a previous laparotomy (Ellis 1997). This contrasts
with a 10% incidence in patients without a prior laparotomy (
Menzies 1990). Pelvic adhesions that follow trans-abdominal gy-
naecological surgery have long been implicated in causing pain
and infertility. Similarly, patients presenting to the general sur-
geon display a spectrum of adhesion related problems or morbid-
ity. The treating surgeon often faces difficulties with access and
obscured normal anatomy which may lead either to an inability
to apply minimal access surgery, prolongation of operative time (
Coleman 2000) or result in potentially serious organ injury such
as inadvertent enterotomy (Van der Krabben 2000). Adhesions are
estimated to account for about a third of all bowel obstructions
and two-thirds of small bowel obstructions in the western world (
Menzies 1992; Menzies 1993).
2Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
juliob
Resaltado
juliob
Resaltado

Certain surgical operations have been reported to carry a higher
than usual risk of adhesion-related complications. A 25 % inci-
dence of adhesive obstruction has been reported in a series of 1005
ileo-anal pouch procedures (Fazio 1995). Total or subtotal colec-
tomy (Lockhart-Mummery1967; Nieuwenhuijzen 1998) and ap-
pendicectomy (Cox 1993) are other high risk procedures in terms
of their propensity to lead to adhesive intestinal obstruction. In
neonates, surgery for gastroschisis and malrotation are reported to
carry a 15% risk of post-operative adhesive intestinal obstruction (
Wilkins 1986). Managing adhesions and adhesion related compli-
cations is expensive in terms of time (Menzies 2001; Parker 2001),
effort and finances (Ray 1998; Jeekel 1997; Menzies 2001; Wilson
1998) and impacts not only on the patient and the treating physi-
cian but also the health care system at large. The prolongation in
hospital stay, re-admissions, repeated surgical interventions and
litigation impose an enormous burden on the health care systems
globally, making adhesion prevention an important area of health
care intervention research.
As once established, adhesions follow an unpredictable temporal
course, which is attended by a lifetime risk of recurrent symp-
toms, complications, re-admissions and repeat surgery, prevention
seems to be the most viable strategy yet. Peritoneal injury, the at-
tendant inflammation, imbalance in plasmin system and proxim-
ity of injured surfaces are the crucial elements in adhesion for-
mation. Hence, preventive strategies have been designed targeting
these steps individually or in combination. Injury limitation, a vi-
tal aspect of prophylaxis is largely a surgical endeavour achieved by
meticulous attention to operative technique and tissue handling.
However, as injury can only be minimised and not completely
abolished, adjuncts to injury limitation techniques are necessary to
reduce the risk of adhesions. Systemic and intraperitoneal pharma-
cological strategies like anti-inflammatories, anticoagulants, agents
targeting the plasmin cascade and hormones have not met with
much success clinically (diZerega 1994; Risberg 1997).
A number of fluid and solid phase (membranes, sheets) agents
that primarily act as barriers to contact between two adjacent peri-
toneal surfaces, have been evaluated clinically for their potential
for adhesion prophylaxis. Examples of fluid agents include 4%
Icodextrin (Adept®, ML laboratories plc.,UK) and Hyaluronic
acid-phosphate buffered saline (Sepracoat®, Genzyme Corp.,
USA). Examples of solid phase agents include, Hyaluronic
acid /Carboxymethyl cellulose membrane (Seprafilm®, Genzyme
Corp., USA), Oxidised regenerated cellulose (Interceed®, John-
son&Johnson medical Inc., USA), and expanded Polytetraflu-
oroethylene (Gore-tex®, WL Gore& Associates, USA ). These
agents differ in their chemical composition, biodegradability, tis-
sue interactions and hence the adverse effect profiles.
An intervention such as adhesion prophylaxis, that is likely to have
a wide impact on day to day surgical practice and on the health
care economics needs to be scrutinised for safety and efficacy with
specific reference to the context in which it is used and in relation
to relevant outcomes.Barrier and non-barrier agents in prophylaxis
of adhesions have been evaluated for efficacy by systematic reviews,
but only in the context of gynaecological surgery (diZerega 2002),
usually with respect to their effect on fertility rates and pain (
Ahmad 2008, Metwally 2006).
The purpose of the current review is to provide an evidence based
appraisal of the safety and efficacy of intra-peritoneal agents in
general surgical operations from randomised controlled trials that
have assessed adhesion reformation (severity, distribution and fre-
quency) and /or adhesion related intestinal obstruction as the main
outcome measure.
O B J E C T I V E S
Primary objective:
To determine the efficacy of intra-peritoneal prophylactic agents
in reducing the incidence, distribution and severity of adhesions
in non-gynaecological abdominal surgery.
Secondary objectives:
To determine the effect of intra-peritoneal prophylactic agents on
the incidence and outcome of adhesion related intestinal obstruc-
tion.
To determine the safety and adverse effect profile of intra-peri-
toneal prophylactic agents in non-gynaecological intra-abdominal
surgery.
To detect any changes in health related quality of life from the use
of intra-peritoneal prophylactic agents in this subset of patients.
M E T H O D S
Criteria for considering studies for this review
Types of studies
Inclusion criteria:
Randomised and Quasi-randomised clinical trials addressing the
safety and/or efficacy of prophylactic intraperitoneal agents in pre-
vention of adhesions and adhesion related complications were in-
cluded.
Both blinded and non-blinded studies were considered.
Only parallel group and factorial designs were considered.
Only studies involving non-gynaecological abdominal surgery in-
volving the peritoneal contents were evaluated for inclusion.
In studies reporting on efficacy, the patients required to have had
the intra-peritoneal adhesions assessed at a second operation -
either open or laparoscopic.
3Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Types of participants
Inclusion criteria:
Patients of all ages and both genders were included.
Patients who underwent a non-gynaecological abdominal surgery
either open or laparoscopic, involving the use of a prophylactic
intra-peritoneal agent for adhesion prevention, during the course
of the surgery.
Exclusion criteria:
Patients undergoing primarily a transabdominal gynaecological
surgery .This would be defined for the purpose of this review as
any transabdominal primary operative intervention on the female
reproductive tract. However, patients who had a primary general
surgical operation but also had to undergo a surgical procedure on
the female reproductive tract during the course of the operation
were considered to be included in the review.
Types of interventions
Intra-operative intra-peritoneal incorporation or instillation of a
solid phase agent (membranes or sheets) or a fluid agent respec-
tively, with a view to prevent intra-abdominal adhesions and ad-
hesion related complications.
The prophylactic agent studied should have been compared with
either no intervention or against a placebo or against another pro-
phylactic agent.
Both open and minimal access surgeries involving the intraperi-
toneal contents and employing the interventions were considered.
There was no restriction as to the grade or level of experience of
the operating surgeon performing the interventions.
Types of outcome measures
Inclusion criteria:
Primary outcome measure:
1.The incidence, distribution and severity of adhesions assessed
during the course of a second open surgical or laparoscopic oper-
ation
Secondary outcome measures:
1.The incidence and outcome of adhesion-related intestinal ob-
struction.
2.Incidence and outcome of adhesion related re-admissions
3.Local, regional and systemic complications arising from the use
of fluid and membrane agents
4.Patient reported health related quality of life recorded by a vali-
dated generic or specific quality of life assessment tool.
Exclusion criteria for outcome measures:
1. Where the main outcome study of the study was pain
2. Where the main outcome measure of the study was fertility
Search methods for identification of studies
The following bibliographic electronic medical databases were
searched for publications addressing the above clinical problem
1.The Cochrane Central Register of Controlled Trials (CEN-
TRAL)
2.The Cochrane Colorectal Cancer Group specialised register (SR-
COLOCA)
3.MEDLINE from 1966 to 2008 (April)
4.EMBASE from 1971 to 2008 (April)
Two authors individually conducted the searches.The following
search strings were used where appropriate, without language re-
strictions.
Strategy A:
1.Adhesi$ - LIMIT to human studies
2.Abdo$ OR Intraabdominal
3.Peritoneal OR Intraperitoneal
4.COMBINE 2 OR 3
5.COMBINE 1AND 4
6.Prevent$ OR Prophyla$
7.COMBINE 5 AND 6
The titles and abstracts when available were scrutinised to select
relevant controlled studies addressing the safety and efficacy of the
use of these agents in non-gynaecological abdominal surgery.
Strategy B:
The following text words were used individually to identify studies
reporting results from the specific use of the respective products
1.“SEPRAFILM”
2.“SEPRACOAT”
3.“INTERCEED”
4.“ADEPT”
5.“ICODEXTRIN”
6.“GORETEX”
7. “SURGIWRAP”
8. “DEXTRAN”
9. “HYSCON”
10. “CARBOXYMETHYLCELLULOSE”
11. “ HYALURONAN”
12. “ HYALURONIC ACID”
13. “ POLYTETRAFLUOROETHYLENE”
14. “ OXIDISED REGENERATED CELLULOSE”
15. “ PHOSPHATIDYLCHOLINE”
16.COMBINE 1 OR 2 OR 3 OR 4 OR 5 OR 6 OR 7 OR 8 OR
9 OR 10 OR 11 OR 12 OR 13 OR 14 OR 15.
17.Adhesi$
18.COMBINE 16 AND 17
The search was limited to human studies
The titles and abstracts when available were scrutinised to select
relevant controlled studies addressing the safety and efficacy of the
use of these agents in non-gynaecological abdominal surgery.
Strategy C:
1.Adhes$ LIMIT to human studies
2.Intestinal obstruction OR Bowel obstruction
3.COMBINE 1 and 2
4.Complications
5.COMBINE 1 and 4
4Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

6 COMBINE 3 OR 5, avoid duplicates
7.Prevent$ OR Prophyl$
8.COMBINE 6 AND 7.
The titles and abstracts when available were scrutinised to select
relevant controlled studies addressing the safety and efficacy of the
use of these agents in non-gynaecological abdominal surgery.
Reference lists of retrieved full text articles were searched for rele-
vant additional studies.
The manufacturers of the prophylactic agents mentioned above
were contacted when necessary to acquire information about any
published trials known to them that could be of relevance.
The health technology assessment (HTA) database was also
searched for relevant publications.
Data collection and analysis
STUDY SELECTION
Two reviewers (SK and PFW) conducted a methodical search of
the electronic bibliographic medical databases and other sources as
outlined in the search strategy. Trials were considered for inclusion
in the review if they fulfilled the following criteria:
1. Prospective randomised or quasi-randomised controlled trials
in humans.
2.The procedure performed was an intra-peritoneal non-gynaeco-
logical surgery, either open or laparoscopic.
3.The trial compared an agent against either no treatment or an
appropriate placebo or against another prophylactic agent.
4.Trial addressed the safety and/or efficacy of the intra-peritoneal
prophylactic agents.
After initial screening of the title and abstract, the full-text article
of the studies were retrieved in the following situations:
1.Study fulfils criteria on initial screening of the abstract and title
2.Study may potentially fulfil criteria but there is not enough in-
formation in the abstract alone to justify inclusion.
3.No abstract is available but the title suggests a potential that the
study may fulfil criteria.
The full text article was then scrutinised independently by two re-
viewers to confirm that the study justified inclusion. A specifically
designed structured flow chart with a set of check lists incorpo-
rated was used in the selection procedure.
QUALITY ASSESSMENT:
Quality assessment was by a component based system incorporat-
ing aspects of internal validity outlined below. Composite scoring
systems for quality assessment were not used.The domains consid-
ered towards quality assessment, were selected to detect any poten-
tial for selection bias, detection bias and attrition bias. The studies
were scrutinised for details regarding the following components
of quality:
1. Randomisation:
Good quality: True randomisation ( Computer generated random
number sequences, sequences from validated random number ta-
bles, coin tossing, casting dice, shuffling cards or similar methods
)
Poor quality: Quasi-randomisation (based on date of birth, hos-
pital number, date of admission, alternating sequence or similar
methods ).
2.Allocation concealment:
Good quality: sequentially labelled sealed, opaque envelopes; Cen-
tralised randomisation revealed by telephoning before assignment
or similar methods.
Poor quality: unsealed or non-opaque envelopes, open allocation
schedule, all procedures based on quasi-randomisation.
3.Blinding:
Good quality: Assessor or observer is blinded to the intervention
that the patient has had.
Poor quality: Assessor not blinded; Only the patient and or the
surgeon applying the intervention is blinded ; No blinding used.
4.Handling of attrition:
Good quality: Analysis on an intention to treat basis; patients lost
to follow-up, drop outs, protocol violations reported and causes
discussed; proportion of patient attrition < 15% (Chalmers 1981).
Poor quality: Participant attrition poorly described or analysed.
Attrition rate > 15% of total recruited.
Studies were assigned an overall grade as follows: A (All criteria for
good quality are met, low risk of bias; would be classified as a good
quality study), B (One or more criteria of good quality only partly
met, moderate risk of bias; would be classified as an intermediate
quality study), C (One or more criteria for good quality not met,
high risk of bias; would be classified as a poor quality study).
The grading however was not used to weight the summary out-
comes in the meta-analysis.
DATA COLLECTION :
Data extraction from the studies was standardised by specially
designed forms and was double checked by a second reviewer
independently. It was not possible to blind the reviewers to the
source of the articles (authors, institution, journal, funding). The
data collected was in relation to the following characteristics:
Methods:
-Setting: Geographical location; single centre or multicenter
-Type of randomisation: True, Quasi-.
-Method of randomisation : Generation of sequence; allocation
concealment.
-Extent of blinding: Patient; surgeon employing the intervention;
observer; non-blinded; unclear; not stated.
-Power calculations: Not applicable; not stated; unclear; provided;
if provided then statement of power.
-Size of the study: Total patients recruited; total included in anal-
ysis; whether size appropriate to a priori statement of study size.
-Methods employed to deal with attrition and missing data
-Type of adhesion assessment: second look laparoscopy; second
5Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

look laparotomy.
-Time of adhesion assessment in relation to the index surgery.
-Duration of the study.
-Duration of follow-up.
Participants:
-Age and gender distribution.
-Type of underlying abdominal pathology (peritonitis or not; be-
nign or malignant; Inflammatory or non-inflammatory bowel
pathology ; mixed, unclear; not stated).
Intervention:
-Setting: Type of surgery- laparoscopic or open; emergency or
elective; mixed.
-Agent(s) used and comparator: agent Vs none; agent Vs placebo;
agent Vs agent.
-Dose or size of agent used.
-Area of application: General peritoneal cavity; all surgical sites;
identified raw areas or peritoneal defects; around anastomosis; un-
der the laparotomy wound; unclear; not stated.
Outcome measures and results:
1.Incidence of adhesions
2.Distribution/ extent of adhesions.
3.Severity/type of adhesions
4..Incidence of morbidity attributable to adhesions or interven-
tion.
5.Incidence of mortality attributable to adhesion or intervention.
6.Incidence of re-admissions
7.Incidence of clinical bowel obstruction.
8.Incidence of operative intervention attributable to adhesions.
9.Quality of life scores
DATA ANALYSIS AND SYNTHESIS:
The statistical package Metaview of Revman 4.2.6, provided by the
Cochrane collaboration was used to analyse and synthesise data.
For dichotomous data such as presence or absence of adhesions,
incidence of morbidity and mortality attributable to adhesions,
incidence of intestinal obstruction and incidence of re-admissions
, the impact of the intervention is expressed as an odds ratio with
95% confidence intervals. For continuous data such as extent of
adhesions measured as absolute area (square millimetres or square
centimetres) or as a proportion or percentage of wound area, the
effect size was estimated by computing the weighted mean differ-
ence with 95% confidence intervals.
The tables of comparison are for the following outcomes:
1.Incidence of adhesions
2.Extent of adhesions
3.Incidence of morbidity (overall and specific)
4.Incidence of mortality
5.Incidence of intestinal obstruction (overall and those needing
surgical intervention)
A meta-analysis was performed where appropriate. There were
too few studies (7) satisfying the inclusion criteria to explore the
potential for publication bias by a funnel plot of sample size plotted
against the odds ratio of primary outcome. Statistical heterogeneity
was tested by inspection of the forest plot and computation of the
chi square statistic for heterogeneity with the probability of a type
I error set at 10% ( P value <0.1 considered significant). Meta-
analysis when appropriate, was performed assuming a random
effects model (Dersimonian and Laird method).
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
NUMBER AND TYPES OF STUDIES
A total of 12 studies reporting on the use of intra-abdominal agents
for adhesion prophylaxis in general surgical operations were iden-
tified, of which 5 were excluded. Four of the five excluded studies
were excluded because they were non-randomised clinical studies
(Kudo 2004; Arnbjornsson 1983; Wang 1994; Salum 2001). One
other study (Beck 1997) was excluded because it was a dual pub-
lication of identical data previously published (Becker 1996). All
7 included studies were prospective randomised controlled trials.
However, there were 2 publications (Beck 2003; Fazio 2006), from
one clinical trial reporting on different outcomes which meant
that there were a total of 8 publications from 7 clinical trials
TYPES OF INTERVENTION
Six of the seven
studies involved Hyaluronic acid/Carboxymethylcellulose mem-
brane (Seprafilm) as the intervention agent against a control group
which did not receive any specific anti-adhesion prophylaxis (Beck
2003; Becker 1996; Cohen 2005; Fazio 2006; Kusunoki 2005;
Tang 2003; Vrijiland 2002). The only other study used 0.5% Fer-
ric hyaluranate gel (Intergel) as adhesion prophylaxis in the inter-
vention group while the control group received distilled water (
Tang 2006).
NUMBER OF PATIENTS
There was a wide variation among the studies in the total num-
bers of patients recruited. This ranged from only 32 patients in
one study (Tang 2006) to 1791 patients in another (Beck 2003).
Only two of the other five studies, recruited more than a hundred
patients (Becker 1996; Cohen 2005).
TYPES OF PATIENTS
All studies involved adult patients of both genders and excluded
pregnant patients. Three studies recruited patients who underwent
a wide range of abdominopelvic resective surgery (involving small
bowel, large bowel and rectum) (Beck 2003; Fazio 2006; Tang
2006) while the others included only a more limited group of pa-
tients defined on the basis of the underlying pathology or type of
surgery. Two studies limited their recruitment to patients undergo-
ing colectomy and ileoanal pouch procedure for ulcerative colitis
6Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
or familial adenomatous polyposis (Becker 1996; Cohen 2005).
One study included only patients who had rectal cancer who un-
derwent preoperative radiotherapy followed by staged surgery (
Kusunoki 2005). Another study recruited only patients who un-
derwent a rectal resection and needed an ileostomy (Tang 2003)
while one restricted recruitment to patients undergoing Hartmann
resection for sigmoid diverticulitis or obstructing recto-sigmoid
lesions (Vrijiland 2002).
TYPES OF OUTCOMES
Five out of the 8 included publications reported on outcomes
which included aspects of both efficacy and safety (Becker 1996;
Cohen 2005; Tang 2003; Tang 2006; Vrijiland 2002) while two
studies reported on efficacy alone (Fazio 2006; Kusunoki 2005)
and one publication on safety alone (Beck 2003). Efficacy of pro-
phylactic agents was reported in 7 trials. The relevant outcome
measures studied were their effect on the incidence of adhesions
in 3 publications (Becker 1996; Vrijiland 2002; Cohen 2005), ex-
tent of adhesions in 3 publications (Becker 1996; Cohen 2005;
Kusunoki 2005), the severity of adhesions in 5 publications (
Becker 1996; Cohen 2005; Kusunoki 2005; Tang 2003; Vrijiland
2002), incidence of bowel obstruction in 2 publications (Fazio
2006; Tang 2006) and their effect on the quality of life in one
study (Tang 2006).
The safety profile of the agents used were reported in 6 publi-
cations. The relevant outcome measures studied were mortality,
overall morbidity and specific morbidity such as wound infection,
anastomotic leak, fistula and intra-abdominal abscess.
Risk of bias in included studies
Of the 7 prospective randomised controlled trials included, 5 were
multi centre trials involving eight (Vrijiland 2002), eleven (Becker
1996), twelve (Cohen 2005), sixteen (Beck 2003) and twenty two
(Fazio 2006) centres. Three trials were based in single institutions
(Tang 2003; Kusunoki 2005; Tang 2006). Sample size calculation
was described in 4 studies (Beck 2003; Becker 1996; Fazio 2006;
Tang 2006). Generation of the randomisation sequence was by
using standard random number tables in one study (Beck 2003;
Fazio 2006) and by a computer generated sequence in 2 studies
(Vrijiland 2002; Tang 2006). In 4 studies the exact method of
generation of the random sequence was not mentioned (Becker
1996; Cohen 2005; Kusunoki 2005; Tang 2006). Allocation con-
cealment was by the use of sealed envelopes in 3 studies (Vrijiland
2002; Tang 2003; Kusunoki 2005), and by resorting to telephon-
ing a remote point of central randomisation at the time of inter-
vention in 1 study (Tang 2006).
Allocation concealment was not clearly evident in 4 studies (Beck
2003; Fazio 2006; Becker 1996; Cohen 2005). Blinded outcome
evaluation to minimise bias was described in 5 studies (Beck 2003;
Fazio 2006; Becker 1996; Cohen 2005; Tang 2006).
Only five studies prospectively defined at least some of the key
outcomes (Fazio 2006; Kusunoki 2005; Tang 2003; Tang 2006;
Vrijiland 2002). Analysis was on an intention to treat basis in 3
studies (Vrijiland 2002; Cohen 2005; Tang 2006).
The period of follow up varied depending on the outcome re-
ported. For example, studies reporting on safety related outcomes
such as morbidity had a shorter follow up than those reporting
on efficacy related outcomes such as the incidence of adhesions
or bowel obstruction. The period of follow up was clearly stated
in 4 publications - Beck 2003 (1 month follow up for adverse
events); Tang 2003 (median follow up of 22.8 months in phase I
and 9.6 months in phase II for adverse events); Fazio 2006 (Mean
follow up of 3.5 years for intestinal obstruction), and Tang 2006
(1 year follow up for intestinal obstruction). The follow up period
for safety related outcomes was not clearly evident in 3 studies (
Becker 1996; Cohen 2005; Vrijiland 2002). In studies reporting
on the efficacy of agents in preventing the incidence and or severity
of adhesions, there was a wide variation in the duration between
the index surgery and the second surgery used for assessment of
adhesions. In Becker 1996, the duration was from 8-12 weeks;
in Cohen 2005 it was 8-14 weeks; Kusunoki 2005 states that the
second surgery was performed at least 3 months after the index
surgery, but does not provide further details; Vrijiland 2002 re-
ports a median duration of 5 months in the intervention group
and 4 months in the control group between index surgery and
assessment; Tang 2003 report two different phases in the trial.
In phase I, the intervention group had ileostomy closure at three
weeks from index surgery, while the control group had the closure
performed at 6-12 weeks. In phase II both the intervention and
control groups had ileostomy closure at 3 weeks.
Attrition of patients either due to exclusion after recruitment or
loss to follow up had a wide variation depending on the outcome
being studied and the duration of follow up. Three studies had no
attrition and were able to report outcomes on all recruited patients
(Beck 2003; Cohen 2005; Fazio 2006). Two studies had low attri-
tion rates of 4.4% (Becker 1996) and 4.8% (Kusunoki 2005). The
other three studies had a much higher degree of attrition, Tang
2003 (38%), Vrijiland 2002 (41%) and Tang 2006 (12.5% at 3
months and 62.5% at 1 year). In one study (Fazio 2006), 90 pa-
tients were excluded post-randomisation, from the final analysis.
The excluded patients were analysed as a different subgroup and
results reported separately from the main cohort of patients in the
study. The reason stated is that these 90 patients, had adhesive
intestinal obstruction, at recruitment while the others did not.
However exclusion after randomisation is likely to introduce bias
and as shown in the analysis, including this subgroup of patients
in the meta-analysis significantly affects the point estimate of the
effect (Analysis 1.10).
Overall 5 studies could be described as grade B studies (interme-
diate quality) (Beck 2003; Fazio 2006; Becker 1996; Cohen 2005;
Kusunoki 2005). Three other studies were assigned grade C (poor
quality) mainly because of a high attrition rate (Vrijiland 2002;
Tang 2003; Tang 2006).
7Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Effects of interventions
The results may be summarised in two broad categories: those
relating to the efficacy of the agents and those pertaining to their
safety.
A. EFFICACY:
[1] INCIDENCE OF ADHESIONS
Data was available for the use of only one agent- Hyaluronic
acid/carboxymethyl cellulose membrane. The only study which
used 0.5% Ferric hyaluronate gel did not report on its effect on
the incidence of adhesions (Tang 2006).
Hyaluronic acid/carboxymethylcellulose membrane
(seprafilm) versus control:
Three studies reported on the effect of use of Hyaluronic
acid/carboxymethyl cellulose membrane on the incidence of ad-
hesions (Becker 1996; Vrijiland 2002; Cohen 2005). There were
a total of 97 events amongst 164 patients in the treatment group
compared to 158 events amongst 171 patients in the control arm.
The use of hyaluronic acid/carboxymethyl cellulose membrane re-
duced the incidence of adhesions significantly [OR 0.15 (95% CI:
0.05, 0.43); p=0.0005].
[2] EXTENT OF ADHESIONS
Three studies using Hyaluronic acid/carboxymethylcellulose
membrane as the interventional agent, reported on the extent of
adhesions as a relative measure such as the proportion of either
the main wound length or peristomal area involved by adhesions (
Becker 1996; Fazio 2006; Kusunoki 2005). In two studies the ex-
tent of adhesions was measured on an interval scale as a percentage
of the main laparotomy wound and data analysed comparing dif-
ferences between means or median among the two groups (Becker
1996; Cohen 2005). Becker and colleagues found the mean extent
of adhesions in the intervention group (n=85) to be 23% (s.d. 34)
compared to 63% (s.d. 34) in the control group (n=90) [ p<0.01;
student’s t test]. Cohen and colleagues, reported a mean of 31%
involvement of the main laparotomy wound with adhesions in
the intervention group compared to 65% in the control group.
The mean distribution and error bars representing standard de-
viation were provided in this publication. The measured differ-
ences between the two groups however, were analysed using a non-
parametric method and are reported to be statistically significant
[p<0.001; Mann-Whitney test].
Data from these two studies were used in the meta-analysis. The
use of hyaluronic acid/carboxymethyl cellulose membrane signif-
icantly reduced the extent of adhesions to the midline wound
[WMD -25.9%(95%CI: -40.56, -11.26); p=0.0005]
In one other study (Kusunoki 2005), the adhesions were measured
on an ordinal scale with the extent of adhesions in individual
patients given a grading of 0 (no adhesions), 1 (covering up to 25%
of the length of the wound or peristomal area), 2 (covering 25-
50% of the length of the wound or peristomal area), 3 (covering
more than 50% of the length of the wound or peristomal area).
The extent of midline and peristomal adhesions were measured
in 30 patients in the intervention group and 29 patients in the
control group. When midline adhesions were compared, 26 out
of 30 patients in the intervention group had a grade of 0, while
15 out of 29 patients in control group had grade 2 adhesions.
The differences between the groups were statistically significant
(p<0.01; Mann-Whitney test). Comparing peristomal adhesions,
18 of 30 patients in the interventional group had grade 1 adhesions
while 23 out of 29 patients in the control group had grade 2 or
3 adhesions. The differences between the groups was statistically
significant (p ,0.01; Mann-Whitney test).
[3] SEVERITY OF ADHESIONS
Five studies using Hyaluronic acid/carboxymethylcellulose mem-
brane as the interventional agent reported on the severity of adhe-
sions (Becker 1996; Vrijiland 2002; Tang 2003; Kusunoki 2005;
Cohen 2005). There was a wide variation in the methods and def-
initions used to assess severity which precluded meta-analysis.
Becker 1996 used a three point grading system (grades 1-3) which
assessed thickness and vascularity . There were 90 patients in
the control group and 85 in the intervention group. The use
of Hyaluronic acid/carboxymethylcellulose membrane was asso-
ciated with significantly less severe adhesions as assessed by their
grading system (p<0.01; Wilcoxon rank sum test).
Vrijiland 2002 used the product of an estimate of severity (which
was graded from 1-4) and the distribution of adhesions to give a
composite score which was used as the comparative measure. The
median composite severity score for the whole of the midline in-
cision was significantly lower in the intervention group (18) when
compared to the control group (50) [p=0.002 ; Mann-Whitney
test].
Tang 2003 classified peristomal adhesions by severity into 3 groups
(grades 1-3). Each of the 4 quadrants around the stoma was scored
separately and a total score was calculated by summation. In Phase
one of the trial, assessment was performed 3 weeks after index
surgery in the intervention group (n=26) while the assessment
in the control group was at 6 weeks or after (n=39). There were
no differences in the mean adhesion severity scores between the
two groups in this phase (p=0.84; student’s t test). In the second
phase of the study, a subsequently recruited cohort of patients were
assessed at 3 weeks after index surgery in both groups (n= 21 in the
intervention group and n= 22 in the control group). The mean
adhesion severity score was significantly less in the intervention
group (p=0.02; student’s t test).
Kusunoki 2005 graded the severity of adhesions based on thick-
ness an vascularity into four groups (grades 0-3). There were 30
patients in the intervention group and 29 patients in the control
group. Both midline adhesions and peristomal adhesions were sig-
nificantly less severe in the intervention group (p<0.01; Mann-
Whitney test).
Cohen 2005 used a four point grading system (grades 0-3). There
were 58 patients in the intervention group and 60 patients in the
control group. In the intervention group, 19 patients had grade 2
8Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

adhesions and 6 patients had grade 3 adhesions compared to 25
and 21 patients respectively in the control group. These differences
in severity were reported to be statistically significant ( p<0.001;
Wilcoxon rank sum test).
[4] INCIDENCE OF RE-ADMISSIONS
None of the included studies had provided specific data on the
incidence of re-admissions in the patients studied.
[5] INCIDENCE OF BOWEL OBSTRUCTION AND OPER-
ATIVE INTERVENTION FOR BOWEL OBSTRUCTION
Overall three out of the eight publications reported on the inci-
dence of bowel obstruction as an outcome measure.
Hyaluronic acid/carboxymethylcellulose mem-
brane (seprafilm) versus control: Two studies reported on the
incidence of intestinal obstruction (Kusunoki 2005; Fazio 2006).
Kusunoki 2005 followed up their patients for 24-66 months (me-
dian 43.6 months) while Fazio 2006 reported a follow up of be-
tween 24-60 months (mean 42 months). Two types of incidences
were reported. All causes bowel obstruction includes a diagnosis of
bowel obstruction in patients in the follow up period, arrived on
the basis of clinical, radiological and/ or operative criteria. Bowel
obstruction attributable to adhesions includes only the subset of
patients who either required a laparotomy or laparoscopy to diag-
nose or treat bowel obstruction and hence had objective operative
evidence to support the adhesive aetiology of obstruction. Fazio
2006 presented their results in two subgroups. Ninety patients
who had adhesive intestinal obstruction at recruitment have been
analysed as a separate subgroup - with a higher incidence of ad-
hesive obstruction in the treatment group (8/42) compared to the
control group (4/48). This essentially means a post-randomisation
exclusion of 90 patients from the initial recruitment cohort of pa-
tients. The authors of this review, feel that such post randomisa-
tion exclusion is inappropriate and introduces a significant bias to
the results (as borne out by the forest plot 1.10.1, which clearly
illustrates the effect of excluding and including this subgroup of
90 patients in the meta-analysis). For the purposes of this review,
the authors have included the data on the subgroup of 90 patients
in the meta-analysis.
The total incidence of intestinal obstruction of all causes was 111
out of 912 patients in the intervention group compared to 111 out
of 938 patients in the control group. The differences between the
two groups was not statistically significant [OR: 0.84 (95% CI:
0.34, 2.08)]. Similarly, in the subgroup of adhesive intestinal ob-
struction needing surgical intervention, the incidence of intestinal
obstruction in the treatment group (24 out of 914) and the control
group (36 out of 939) were not statistically significant [OR: 0.84
(95% CI: 0.24, 2.7)].
0.5% Ferric Hyaluronate gel: One study reported the incidence
of intestinal obstruction during follow up (Tang 2006). The study
was underpowered due to premature termination. Even amongst
the recruited patients, the attrition rate in the study for evaluation
of this particular outcome measure was unacceptably high. Of the
total of 32 patients recruited in the study only 20 patients (10
patients in each arm of the study) completed 1 year follow up for
evaluation of the incidence of intestinal obstruction. One patient
in the treatment group was found to satisfy the criteria set out in
the study, for intestinal obstruction during the one year of follow
up reported. So no valid conclusions can be drawn from this study
on the effect of adhesion prophylaxis on the incidence of adhesive
obstruction.
[6] INCIDENCE OF OPERATIVE INTERVENTION OF
OTHER CAUSES, ATTRIBUTABLE TO ADHESIONS
None of the included studies had provided data specifically relat-
ing to adhesion related operative intervention apart from those
presenting with intestinal obstruction discussed above. Though
one study set out to evaluate the need for adhesiolysis during fol-
low up, as an outcome measure (Tang 2006), this did not mate-
rialise as the study was terminated prematurely. None of the 20
patients followed up for 1 year needed adhesiolysis. In summary,
the recruitment was small (total of 32 patients), follow up short
(1 year), attrition rate for follow up high (37.5%) and the event
rate too low (zero) to draw any valid conclusions.
[7] QUALITY OF LIFE MEASURES
Quality of life is an important patient reported outcome increas-
ingly used to assess effectivenes of interventions. However, it would
be a difficult one to measure in the context of adhesions due to a
number of confounding factors. Only one trial attempted to study
the effect of adhesion prophylaxis on the quality of life (Tang 2006)
using the Gastrointestinal Quality Of Life Index tool. Though
baseline measurements were available for 29 patients (n=15 for
treatment group and n=14 for control group), the attrition rate
was high with only a total of 11 patients ( n=5 for treatment group
and n=6 for control group) completing the quality of life ques-
tionnaire at the end of 1 year. Moreover, only 3 patients completed
all three sets of questionnaires (i.e. baseline, 6 months and 1 year).
Because of the high attrition rate and the non-availability of indi-
vidual patient data, no definite conclusions can be drawn on the
effect of the intervention on the quality of life.
B. SAFETY
Six studies reported on at least one aspect of safety. Five of these
studies used Hyaluronic acid / carboxymethyl cellulose and the
results were reported at the end of the study period as planned. One
study evaluated the safety of 0.5% Hyaluranate gel against placebo
(Tang 2006). Though the study was intended to recruit about
700 patients, the high incidence of morbidity in the intervention
group resulted in a premature termination of the trial within 6
weeks of commencement after recruitment of only 32 patients.
[1] INCIDENCE OF OVERALL MORBIDITY
A total of 4 studies reported on overall adverse events seen in the
intervention and the control groups. The specific list of compli-
cations for which the patients were evaluated for, varied between
different studies, but was applied equally between the two arms
9Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

within a study. The overall morbidity included both abdominal
(such as abdominal abscess, anastomotic leak) as well as extra-ab-
dominal (such as fever, pulmonary embolism) adverse events.
Hyaluranate/CMC membrane: Three studies recruiting a total of
2094 patients, were available for evaluation of safety of HA/CMC
membrane. The total event rate in all three studies together was
relatively high at 759 (36.2%). There was no significant clinical
or statistical heterogeneity amongst the studies. There was a total
of 390 events amongst 1032 patients in the intervention group
and a total of 369 events in 1062 patients in the control group.
The incidence of overall morbidity was comparable between the
intervention and control groups [OR: 1.19; 95% CI: 0.97, 1.46;
p=0.10].
0.5% Ferric Hyaluranate gel: one study evaluated the safety of
0.5% hyaluranate gel against placebo (Tang 2006). There were a
total of 32 patients of which 17 were in the intervention group. At
30 day follow up, complications were 5 times more common in
the intervention group when compared to the control group [OR
5.04; 95%CI:1.1; 22.9]. This resulted in the premature termina-
tion of the study, within 6 weeks of initiation.
[2] INCIDENCE OF ABDOMINAL OR PELVIC INFEC-
TION
Hyaluranate/CMC membrane: Three studies reported on the
incidence of post-operative intra-abdominal or pelvic infection
after the use of Hyaluranate/CMC membrane (Becker 1996; Beck
2003; Cohen 2005). A total of 53 patients out of 1032 experienced
pelvic or abdominal infection in the intervention group compared
to 34 out of 1062 patients in the control group. These differences
did not reach statistical significance [OR: 1.92; 95% CI: 0.95,
3.92; p=0.07].
0.5% Ferric Hyaluranate gel: One study which used 0.5% ferric
hyaluranate gel reported occurrence of peritonitis in one patient
(of 17) in the intervention group while none were recorded in the
control group. However, there were no instances of intra-abdom-
inal or pelvic abscesses in the study.
[3] INCIDENCE OF ANASTOMOTIC LEAKS
The incidence of anastomotic leaks was reported in a total of 5
studies.
Hyaluranate/CMC membrane: Four studies using hyalu-
ranate/CMC membrane specifically reported on the incidence of
anastomotic leak (Becker 1996; Beck 2003; Tang 2003; Cohen
2005). The study by Tang reported two different phases in the
trial. In Phase I the intervention group had the ileostomy closed
at 3 weeks while the control group had the ileostomy closed at
6-12 weeks. As the radiologically evaluated anastomotic leak rate
is bound to be higher at 3 weeks when compared to 6-12 weeks,
potentially introducing a time bias between the two groups, pa-
tients from the phase I of the study were not included in the meta-
analysis of anastomotic leaks. However, in Phase II in the trial,
the intervention and control groups were treated similarly, with
ileostomy closure being performed at 3 weeks in both groups.
Data from Phase II of this trial was considered for meta-analysis.
In the study by Beck 2003, which was by far the largest study in
the group, there was a higher incidence of anastomotic leak and
leak related events (fistula, peritonitis, abdominopelvic abscess,
systemic sepsis) in the intervention group (76/882=8.6%) when
compared to the control group (46/909= 5.1%). In the subgroup
where HA/CMC membrane was wrapped around the anastomo-
sis, the incidence of these events was particularly high (39/289=
13.5%) and the difference was statistically significant when com-
pared to control in this particular study (Beck 2003).
When data from all three contributing studies was considered in
the meta-analysis, there was a total of 43 anastomotic leaks in 1066
patients in the treatment arm compared to 26 anastomotic leaks in
1098 patients in the control arm. The observed higher incidence
of anastomotic leak in the intervention group was not statistically
significant [OR: 1.61; 95%CI: 0.69, 3.71; p=0.27].
0.5% Ferric Hyaluranate gel: One study reported the incidence
of anastomotic leak when 0.5% ferric hyaluranate gel was com-
pared with control (Tang 2006). There were 5 anastomotic leaks
among 17 patients in the treatment group compared to 1 anas-
tomotic leak in 15 patients in the control group. The observed
fivefold increase in anastomotic leak in the treatment group was
however not statistically significant [OR: 5.83; 95% CI: 0.6, 57.1;
p=0.13].
[4] INCIDENCE OF ILEUS OR EARLY POSTOPERATIVE
OBSTRUCTION
Data on the incidence of ileus or early postoperative obstruction
not specifically attributed to adhesions was available in 5 studies.
Hyaluranate/CMC membrane: Four studies reported on the ef-
fect of use of this membrane agent on the incidence of ileus (Becker
1996; Beck 2003; Tang 2003; Cohen 2005). A total of 58 patients
out of 1113 developed ileus in the treatment arm compared to 57
out of 1148 patients in the control arm. These differences were not
statistically significant [OR: 1.05; 95% CI: 0.72, 1.53; p=0.79].
0.5% Ferric hyaluranate gel: The only study which reported on
the use of 0.5% Ferric hyaluranate gel found a nine fold higher
incidence of ileus in the intervention group (10 out of 17) com-
pared to the control group (2 out of 15) (Tang 2006). The dif-
ferences were statistically significant [OR: 9.29; 95% CI: 1.57,
54.77; p=0.01].
[5] INCIDENCE OF WOUND INFECTION
Incidence of wound infection was reported in a total of 5 studies.
Hyaluranate/CMC membrane: Four studies used Hyaluronic
acid/carboxymethyl cellulose membrane (Becker 1996; Vrijiland
2002; Beck 2003; Cohen 2005). A total of 49 wound infections
occurred in 1053 patients in the intervention group compared to
43 wound infections in 1083 patients in the control group. The
observed differences in wound infection between the intervention
and control groups were not statistically significant [OR 1.18;
95% CI: 0.77, 1.80; p=0.46].
10Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

0.5% Ferric hyaluranate gel: One study (Tang 2006) reported
wound infection rates when 0.5% Ferric hyaluronate gel was used
as the agent. This was an underpowered study as it had to be
prematurely terminated. There were 6 infections in 17 patients in
the intervention group compared to 3 infections in 15 patients
in the control group. There were no significant differences in the
incidence of wound infection between the two groups [OR: 2.18;
95% CI: 0.44, 10.9; p=0.34].
[6]INCIDENCE OF OVERALL MORTALITY
Overall mortality was reported in a total of 2 studies.
Hyaluranate/CMC membrane: In one study using Hyalu-
ranate/CMC membrane (Becker 1996), there was one mortality
among 91 patients in the treatment group (1%) and none among
92 patients in the control group. The differences were not statis-
tically significant.
0.5% Ferric hyaluranate gel: In one study using 0.5% ferric
hyaluranate gel (Tang 2006), there was one mortality each in
the treatment group (n=17; 5.8%) and the control group (n=15;
6.6%). These differences were not statistically significant.
D I S C U S S I O N
Peritoneal injury which occurs during laparotomy almost invari-
ably results in the formation of adhesions. It has been estimated
that up to a third of the adult population in the western world,
may be harbouring adhesions which carry a lifelong potential for
complications. The resultant burden to the patient, the surgeon
and the health care system on a global scale is high. From this per-
spective, research in peritoneal adhesions especially its prevention,
should be given a high priority. Methods to prevent adhesions may
be broadly grouped into surgical techniques and adjuncts. Sur-
gical techniques include such poorly defined suggestions such as
gentle peritoneal handling to more specific interventions such as
avoiding peritoneal closure, use of starch free gloves and avoiding
spillage of gall stones. However, these surgical techniques alone
are not completely effective on their own and hence the search
for adjuncts. Adjuncts may further be classified into physical (or
mechanical) types and chemical categories. The physical group
of agents are applied intraperitoneally and primarily act by form-
ing a barrier between adjacent peritoneal surfaces. They may be
membranes or sheets which have only a local effect where they
are applied (such as Hyaluronic acid/Carboxymethyl cellulose; ex-
panded poly-tetrafluoro ethylene; Oxidised regenerated cellulose)
or fluid agents which diffuse to coat a larger surface area of the peri-
toneum (such as 4% icodextrin solution and 0.5% ferric hyalu-
ranate gel). The chemical group of agents are more heterogenous
and have an effect by chemically interfering with adhesio genesis.
Examples include ani-inflammatory agents, anti-coagulants, anti-
fibrotic agents and proteolytic agents.
This review is limited to the evaluation of intra-peritoneally ap-
plied membrane and fluid agents. Over the last five decades, more
than a hundred different natural and synthetic agents have been
evaluated in animal experiments for their prophylactic potential.
While a large proportion of these pre-clinical studies have reported
beneficial effects, only a few of these agents have been evaluated in
clinical studies in humans. Most of the earlier studies in humans
were initially in the context of gynaecological operations and are
extensively reviewed elsewhere. It is only in the last decade that
clinical studies evaluating prophylactic agents in general surgical
operations started to emerge. To date, data on only two intra-
peritoneal agents namely hyaluronic acid/carboxymethyl cellulose
membrane and 0.5% ferric hyaluronate gel is available, in the con-
text of randomised controlled studies in general surgical opera-
tions. We found only a total of eight published randomised clin-
ical trials of prophylactic agents, seven of which used hyaluronic
acid/carboxymethyl cellulose membrane and one which reported
on 0.5% ferric hyaluranate gel. The probable reason for the scarcity
of published randomised trials in this field is, because of the fact
that, assessing the efficacy of adhesion prevention involves a sec-
ond invasive procedure such as laparoscopy or laparotomy, while
assessing some of the outcomes such as the effect on intestinal
obstruction needs long term follow up of the order of many years.
This also probably accounts for the generally small numbers of
patients recruited in individual studies as observed in the current
review, in which, despite the fact that five of the seven included
studies were multicentre studies, involving up to 22 centres, bar-
ring one study which recruited more than a thousand patients, the
total patients recruited in the individual studies was low resulting
in a median of 96 patients among the included studies. Absence
of blinding in a trial is known to be a source of bias and causes
overestimation of effects. Only four out of seven studies described
blinded outcome assessment. Though blinding may be difficult to
achieve in surgical patients because of the logistics involved and
is likely to be more expensive to implement, it would be a worth-
while means to achieve more accurate results. None of the studies
satisfied all the criteria for good quality studies as stated in the pro-
tocol. Five out of the seven studies were of intermediate quality,
while the other two were considered poor quality mainly due to
the high attrition rates in these studies. Trials in future, should aim
to clearly state the methods used to randomise, to conceal alloca-
tion and to achieve blinding in more detail. Similarly, they should
provide details of sample size calculations, should be adequately
powered to answer the key questions being addressed by the study.
Calculation of sample size and power should take into account
the attrition of patients during the course of the study, which was
unacceptably high in three of the seven studies included in the
review. The lack of explicit definitions in the outcome in some
studies and wide variations in the methods used to measure some
of the outcomes (such as severity of adhesions) made comparisons
amongst the studies difficult.
In a randomised clinical study, it is important that the interven-
11Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

tion and the control group are otherwise treated identically. Most
studies achieved this at the point of intervention and assessment.
However, Tang 2003, had an initial phase in the study (phase I),
where the intervention group were assessed early at 3 weeks while
the control group were assessed between 6-12 weeks. Such dif-
ferential treatment may potentially introduce bias and hence this
phase of the study has been discounted when analysing outcomes
such as leak rates. Variable follow up is another element which
may potentially affect reporting of outcomes. As discussed in the
section on methodological quality, there was a wide variation in
follow up and in some studies there was lack of clarity as to the
duration of follow up. There is a need for consensus among the
researchers as to the minimum acceptable follow up period for
various outcomes and future studies should aim to achieve this
for all patients available for analysis in the intervention and the
control groups.
When comparing the effect of membrane agents on leak rates, it
may be more relevant to compare the rates between patients in
whom the membrane was in contact with the anastomosis with
those in whom it was not (the control group). However, this was
not achieved in the studies that reported on leak rates. Becker 1996
and Cohen 2005 used the membrane only in contact with the
midline wound, while Tang 2003 used the membrane around the
stoma. In Beck 2003, there were patients in the intervention group
who did not have the membrane wrapped around the anastomosis.
The leak rate for this subgroup was similar to the control group.
But the leak rate was significantly higher for the subgroup which
had the membrane wrapped around the anastomosis. Because the
randomisation was not stratified by placement of the membrane,
the differences could not be explored further. The leak rates were
only compared between the intervention group as a whole and the
control group and these were not significantly different.
The results of this review should be interpreted in the light of
the shortcomings discussed above. In summary, from the avail-
able evidence, the use of Hyaluronic acid/Carboxymethyl cellu-
lose membrane reduced the incidence of adhesions [OR 0.15
(95% CI: 0.05, 0.43); p=0.0005] and was associated with a re-
duced extent of adhesions [WMD -25.9%(95%CI: -40.56, -
11.26); p=0.0005] and severity of adhesions. However, the use
of Hyaluronic acid/Carboxymethyl cellulose membrane did not
reduce the incidence of intestinal obstruction [odds ratio: 0.84
(95% CI: 0.34, 2.08)]. With respect to the incidence of adhe-
sive intestinal obstruction (needing surgical intervention), there
was no significant difference between the intervention and control
groups [Odds ratio: 0.84 (95% CI: 0.24, 2.7)].
On the basis of currently available evidence, Hyaluronic
acid/Carboxymethyl cellulose membrane has an acceptable safety
profile.The overall morbidity and mortality were comparable be-
tween the hyaluronic acid/carboxymethyl cellulose membrane
groups and the control groups as was the specific morbidity such
as wound infection, intra-abdominal sepsis, anastomotic leak and
prolonged ileus. There are concerns regarding the higher incidence
of anastomotic leak in a subgroup of patients where the membrane
is directly wrapped around the anastomosis (Beck 2003). How-
ever, this has not been specifically studied in a randomised trial.
No valid conclusions could be drawn on the efficacy of 0.5%
ferric hyaluranate gel, the only other agent on which data relevant
to the subject of this review is available. While there were no
differences in the mortality rates between the intervention and
control groups, there was a high incidence of overall morbidity in
the intervention group [OR 5.04; 95%CI:1.1; 22.9]. While the
rates of wound infection, intra-abdominal abscess and anastomotic
leak were comparable, there was a higher incidence of ileus in the
intervention group [OR: 9.29; 95% CI: 1.57, 54.77; p=0.01] .
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
Based on the currently available data considered in this systematic
review, there is evidence that the use of HA/CMC membrane,
reduces the incidence, extent and severity of adhesions. This may
have implications in re-operative abdominal surgery in terms of
time, ease of access, blood loss, visceral injury and cost, but these
outcomes were beyond the remit of this review. With respect to
symptomatic long term outcomes, however, there is currently no
evidence that use of HA/CMC membrane, reduces the incidence
of intestinal obstruction or the need for operative intervention
in adhesive intestinal obstruction in the first few years following
the index abdominal surgery. HA/CMC membrane appears to be
safe, though there are concerns that it may increase the risk of
anastomotic leak when wrapped around the anastomosis. Hence,
in the absence of an ideal or alternative agent of proven efficacy
in general surgical patients, HA/CMC may be considered in the
prophylaxis of intra-peritoneal adhesions, at the discretion of the
surgeon, tailored to the individual clinical context.
0.5% Ferric hyaluranate gel, has an unacceptably high morbidity,
based on the limited data available, and hence cannot be recom-
mended.
Implications for research
a. Evidence on effectiveness of other agents in general surgery
Currently Hyaluronic acid/Carboxymethylcellulose (HA/CMC)
membrane remains the only agent on which evidence of effective-
ness as an anti-adhesio genesic agent is available in general surgical
patients. However, HA/CMC has certain shortcomings. It is suit-
able only for open surgery and it needs to be applied with some
degree of precision on to the raw surfaces to be effective. It does
not prevent adhesions in regions of the peritoneum which may
harbour areas of injury not be macroscopically visible, areas which
therefore, are not protected. Fluid agents such as 4% icodextrin
12Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

circumvent many of these problems and there is evidence from at
least one study in gynaecological surgery of its efficacy in prevent-
ing adhesions (diZerega 2002). Studies in general surgical opera-
tions are ongoing and would perhaps clarify its role in future. A
plethora of other pharmacological and physical (membrane and
fluid) agents have been shown to be effective in pre-clinical animal
experiments, but only a selected few have been tested in human
studies. Even fewer agents have been tried in randomised clini-
cal trials, mostly in gynaecological surgery. Adequately powered,
prospective, blinded, randomised controlled clinical trials in gen-
eral surgical patients using agents which have proven efficacy in
preclinical studies, may potentially uncover useful therapeutic op-
tions.
b. Evidence of synergism
The potential for synergistic effects of a combination of different
types of adhesion prevention strategies, such as anti-inflammatory
strategies, fibrinolytic strategies and barrier agents applied together
has been demonstrated in animal experiments. The clinical value
of using a combination of strategies in general surgical patients
undergoing laparotomy may be worth investigating.
c. Evidence on other clinically important effects
Though it is evident that film barrier agents reduce the incidence
and severity of adhesions, currently there is lack of evidence that
this translates to a reduction in symptomatic long term outcomes
such as incidence of intestinal obstruction and the proportion
needing surgical intervention for adhesive obstruction. If there
was indeed a small benefit from the barrier agents, which was
missed in the available studies (type II error), then this will need a
large, adequately powered study to uncover the effect. As adhesive
disease is common, even small risk reductions have the potential to
translate to significant benefits when applied on a global scale.The
other clinically significant long term outcome is chronic pain,
on which there is no data available at present on the efficacy of
prophylactic agents in general surgical patients.
d. Evidence of effectiveness in a range of operations
Generalised peritonitis results in a higher incidence of adhesion
related re-admission and re-operation. Data on safety and efficacy
of anti-adhesio genetic agents used in the context of pathologies
leading to generalised peritonitis is worth pursuing. Similarly use
of prophylactic agents in other types of surgery such as small bowel
resections for Crohns disease and a range of laparoscopic surgical
procedures would be valuable. If noninvasive tools for evaluation
of adhesions such as magnetic resonance imaging are validated in
assessing adhesions then a broader range of surgical interventions
and consequently a larger subgroup of patients could be studied.
e. Identification of high risk groups
It is known that adhesions and adhesion related complications are
more frequent after certain types of surgery such as pelvic surgery.
However, at present there is no validated system to identify indi-
vidual patients with an increased risk of adhesions and related com-
plications during the perioperative period. Future studies should
focus on collecting good quality, prospective data (epidemiolog-
ical, clinical, biochemical, cellular and biomolecular) which may
then be used to predict the risk in individual patients. Risk pre-
diction may help in prognostication, planning service needs and
targeting anti-adhesive therapy.
f. Cost effectiveness
Economic analysis in the field of peritoneal adhesion prevention
is understandably difficult for many reasons including controlling
for the number of potential confounding factors in the periop-
erative period, the difficulty in measuring the economic impact
accurately and the length of follow up required. Nevertheless as
economic analysis may be useful in resource planning it is perhaps
worthwhile exploring the cost effectiveness in a carefully chosen
index procedure which is amenable to standardisation.
A C K N O W L E D G E M E N T S
None
R E F E R E N C E S
References to studies included in this review
Beck 2003 {published data only}
Beck DE, Cohen Z, Fleshman JW, Kaufman H, van Goor H, Wolff
BG for the adhesion study group steering committee. A prospective,
randomised, multicenter, controlled study of the safety of seprafilm
adhesion barrier in abdominopelvic surgery of the intestine. Dis
Colon Rectum 2003;46:1310–19.
Becker 1996 {published data only}
Becker JM, Dayton MT, Fazio VW, Beck DE, Stryker SJ, Wexner
SD, et al.Prevention of postoperative abdominal adhesions by a
sodium hyaluronate based bioresorbable membrane: a prospective,
randomised, double-blind multicenter study. J Am Coll Surg 1996;
183(4):297–306.
Cohen 2005 {published data only}
Cohen Z, Senagore A, Dayton M, Koruda M, Beck DE, Wolff BG,
et al.Prevention of postoperative abdominal adhesions by a novel,
Glycerol/sodium hyaluronate/ carboxymethylcellulose- based biore-
sorbable membrane: a prospective, randomised, evaluator blinded
multicenter study. Dis Colon Rectum 2005;48:1130–39.
Fazio 2006 {published data only}
Fazio VW, Cohen Z, Fleshman JW, van Goor H, Bauer JJ, Wolff
BG, et al.Reduction in adhesive small-bowel obstruction by seprafilm
13Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ahesion barrier after intestinal resection. Dis Colon Rectum 2006;49
(1):1–11.
Kusunoki 2005 {published data only}
Kusunoki M, Ikeuchi H, Yanagi H, Noda M, Tonouchi H, Mohri Y,
et al.Bioresorbable hyaluronate-carboxymethylcellulose membrane
(Seprafilm) in surgery for rectal carcinoma: a prospective randomised
clinical trial. Surgery today 2005;35(11):940–5.
Tang 2003 {published data only}
Tang CL, Seow-Choen F, Fook-Chong S, Eu KW. Bioresorbable ad-
hesion barrier facilitates early closure of the defunctioning ileostomy
after rectal excision: a prospective, randomised trial.. Dis Colon Rec-
tum 2003;46(9):1200–7.
Tang 2006 {published data only}
Tang CL, Jayne DG, Seow-Choen F, Ng Y-Y, Eu K-W, Mustapha N.
A randomised controlled trial of 0.5% ferric hyaluronate gel (Intergel)
in the prevention of adhesions following abdominal surgery. Annals
of Surgery 2006;243:449–455.
Vrijiland 2002 {published data only}
Vrijiland WW, Tseng LNL, Eijkman HJM, Hop WCJ, Jakimowicz JJ,
Leguit P, et al.Fewer intraperitoneal adhesions with use of hyaluronic
acid-carboxymethylcellulose membrane: a randomised clinical trial.
Ann Surg 2002;235(2):193–99.
References to studies excluded from this review
Arnbjornsson 1983 {published data only}
Arnbjornsson E, Goransson G. The effect of intraperitoneal fluid on
the prevention of small intestinal obstruction after appendicectomy.
Ann Chir Gynaecol 1983;72:250–52.
Beck 1997 {published data only}
Beck DE. The role of seprafilm bioresorbable membrane in adhesion
prevention. Eur J Surg 1997;Suppl 577:49–55.
Kudo 2004 {published data only}
Kudo FA, Nishibe T, Miyazaki K, Murashita T, Nishibe M. Use of
bioresorbable membrane to prevent postoperative small bowel ob-
struction in transabdominal aortic aneurysm surgery. Surgery Today
2004;34:448–51..
Salum 2001 {published data only}
Salum MR, Lam DT, Wexner SD, Pikarsky A, Baig MK, Weiss EG,
et al.Does limited placement of bioresorbable membrane of modified
sodium hyaluronate and carboxymethyl cellulose (Seprafilm) have
possible short term beneficial effects?. Dis Colon Rectum 2001;44(5):
706–12.
Wang 1994 {published data only}
Wang RQ, Chen JZ, Ren GY. Intraperitoneal perfusion of compound
injection of salvia miltiorrhiza with dachengqi decoction in treating
adhesive intestinal obstruction. Zhongguo Zhong Xi Yi Jie He Za Zhi
1994;14(10):595–97.
Additional references
Ahmad 2008
Ahmad G, Duffy JM, Farquhar C, Vandekerckhove P, Watson A,
Wiseman D. Barrier agents for adhesion prevention after gynaeco-
logical surgery. Cochrane Database of Systematic Reviews 2008, Issue
2:. [DOI: 10.1002/14651858.CD000475.pub2]
Chalmers 1981
Chalmers TC, Smith H Jr, Blackburn B, Silverman B, Schroeder
B, Reitman D, Ambroz A. A method for assessing the quality of
a randomised controlled trial. Control Clin Trials 1981;2:31–49.
[MEDLINE: 7261638]
Coleman 2000
Coleman MG, McLain AD, Moran BJ. Impact of previous surgery on
time taken for incision and division of adhesions during laparotomy.
Dis Colon Rectum 2000;43:1297–9. [MEDLINE: 11005501]
Cox 1993
Cox MR, Gunn IF, Eastman MC, Hunt RF, Heinz AW. The operative
aetiology and types of adhesions causing small bowel obstruction.
Aust N Z J Surg 1993;63(11):848–52. [MEDLINE: 8216061]
diZerega 1994
diZerega GS. Contemporary adhesion prevention. Fertil Steril 1994;
61:219–35. [MEDLINE: 8299773]
diZerega 2002
diZerega GS, Verco SJS, Young P, Kettle M, Koback W, Martin D,
Senfilippo J, Peers EM, Scrimgeour A, Brown CB. A randomised
controlled pilot study of the safety and efficacy of 4% icodextrin so-
lution in the reduction of adhesions following laparoscopic gynaeco-
logical surgery. Human Reproduction 2002;17:1031–1038.
Ellis 1997
Ellis H. The clinical significance of adhesions: Focus on intesti-
nal obstruction.. Eur J Surg 1997;577 (suppl):5–9. [MEDLINE:
9076446]
Fazio 1995
Fazio VW, Ziv Y, Church JM, Oakley JR, Lavery IC, Milsom JW,
Schroeder TK. Ileal pouch-anal anastamoses complications and func-
tion in 1005 patients. Ann Surg 1995;222:120–7. [MEDLINE:
7639579]
Jeekel 1997
Jeekel H. Cost implications of adhesions as highlighted in a European
study. Eur J Surg Suppl 1997;S79:43–5.
Lockhart-Mummery1967
Lockhart Mummery HE. Intestinal polyposis: the present position.
Proc Roy Soc Med 1967;60:381–4. [MEDLINE: 6021668]
Menzies 1990
Menzies D, Ellis H. Intestinal obstruction from adhesions- how big
is the problem?. Ann R Coll Surg Engl 1990;72:60–3. [MEDLINE:
2301905]
Menzies 1992
Menzies D. Peritoneal adhesions. Incidence, cause and prevention.
Ann Surg 1992 1992;24(1):29–45. [MEDLINE: 1727325]
Menzies 1993
Menzies D. Postoperative adhesions: their treatment and relevance
in clinical practice. Ann R Coll Surg Engl 1993;75:147–53. [MED-
LINE: 8323205]
Menzies 2001
Menzies D, Parker M, Hoare R, Knight A. Small bowel obstruction
due to postoperative adhesions: treatment patterns and associated
costs in 110 hospital admissions. Ann R Coll Surg Engl 2001;83:
40–6. [MEDLINE: 11212449]
14Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Metwally 2006
Metwally M, Watson A, Lilford R, Vandekerckhove P. Fluid and
pharmacological agents for adhesion prevention after gynaecological
surgery. Cochrane Database of Systematic Reviews 2006 Apr 19, Issue
2:. [DOI: CD001298]
Nieuwenhuijzen 1998
Nieuwenhuijzen M, Reijnen MM, Kuijpers JH, van Goor H. Small
bowel obstuction after total or subtotal colectomy: a 10 year retro-
spective review. Br J Surg 1998;85:1242–5. [MEDLINE: 9752868]
Parker 2001
Parker MC, Ellis H, Moran BJ, Thompson JN, Wilson MS, Menzies
D, McGuire A, Lower AM, Hawthorn RJ, O’Briena F, Buchan S,
Crowe AM. Postoperative adhesions: Ten-year follow-up of 12,584
patients undergoing lower abdominal surgery. Dis Colon Rectum
2001;44:822–30. [MEDLINE: 11391142]
Ray 1998
Ray NF, Denton WG, Thamer M, Henderson SC, Perry S. Abdom-
inal adhesiolysis: inpatient care and expenditure in the united states
in 1994. J Am Coll Surg 1998;186(1):1–9. [MEDLINE: 9449594]
Risberg 1997
Risberg B. Adhesions: Preventive strategies. Eur J Surg 1997;577:
32–9. [MEDLINE: 9076450]
Van der Krabben 2000
Van Der Krabben AA, Dijkstra FR, Nieuwenhuijzen M, Reijnen
MM, Schaapveld M, Van Goor H. Morbidity and mortality of inad-
vertent enterotomy during adhesiotomy. Br J Surg 2000;87:467–71.
[MEDLINE: 10759744]
Wilkins 1986
Wilkins BM, Spitz L. Incidence of post-operative adhesive obstruc-
tion following neonatal laparotomy. Br J Surg 1986;73:762–4.
[MEDLINE: 3756446]
Wilson 1998
Wilson MS, Hawkswell JA, McCloy RF. The natural history of adhe-
sional small bowel obstruction: Counting the cost. Br J Surg 1998;
85:1294–8. [MEDLINE: 9752881]∗ Indicates the major publication for the study
15Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
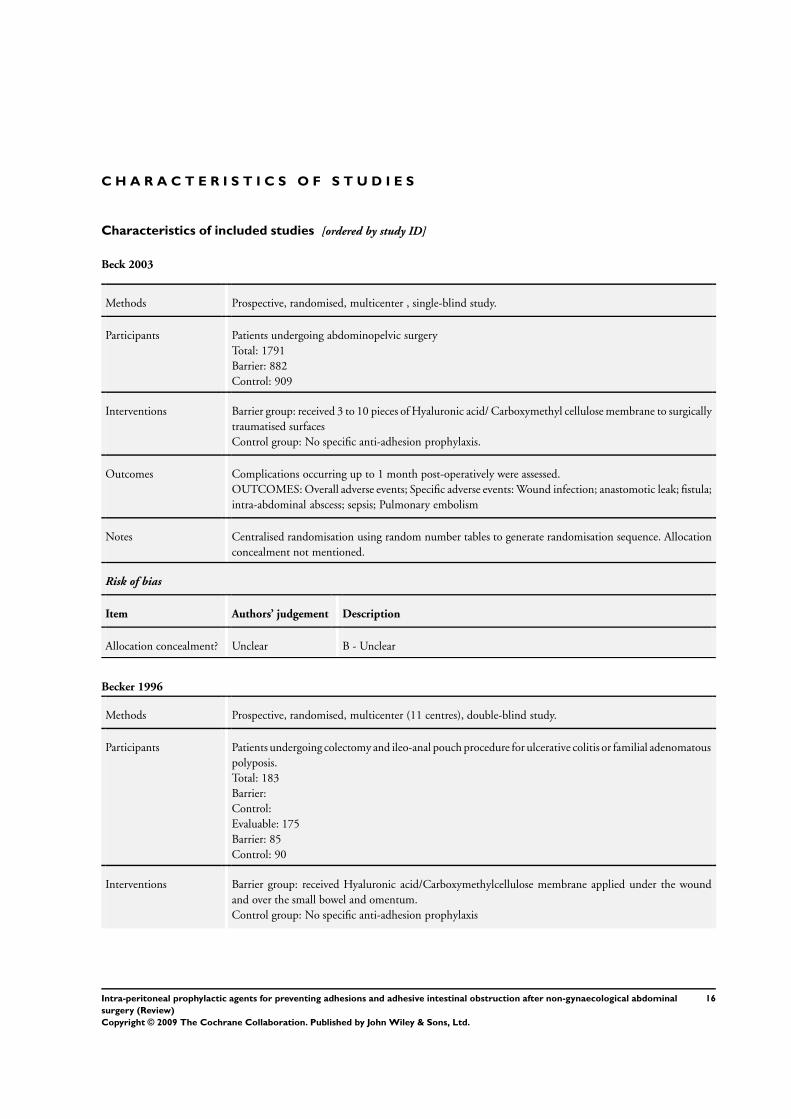
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Beck 2003
Methods Prospective, randomised, multicenter , single-blind study.
Participants Patients undergoing abdominopelvic surgery
Total: 1791
Barrier: 882
Control: 909
Interventions Barrier group: received 3 to 10 pieces of Hyaluronic acid/ Carboxymethyl cellulose membrane to surgically
traumatised surfaces
Control group: No specific anti-adhesion prophylaxis.
Outcomes Complications occurring up to 1 month post-operatively were assessed.
OUTCOMES: Overall adverse events; Specific adverse events: Wound infection; anastomotic leak; fistula;
intra-abdominal abscess; sepsis; Pulmonary embolism
Notes Centralised randomisation using random number tables to generate randomisation sequence. Allocation
concealment not mentioned.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Becker 1996
Methods Prospective, randomised, multicenter (11 centres), double-blind study.
Participants Patients undergoing colectomy and ileo-anal pouch procedure for ulcerative colitis or familial adenomatous
polyposis.
Total: 183
Barrier:
Control:
Evaluable: 175
Barrier: 85
Control: 90
Interventions Barrier group: received Hyaluronic acid/Carboxymethylcellulose membrane applied under the wound
and over the small bowel and omentum.
Control group: No specific anti-adhesion prophylaxis
16Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
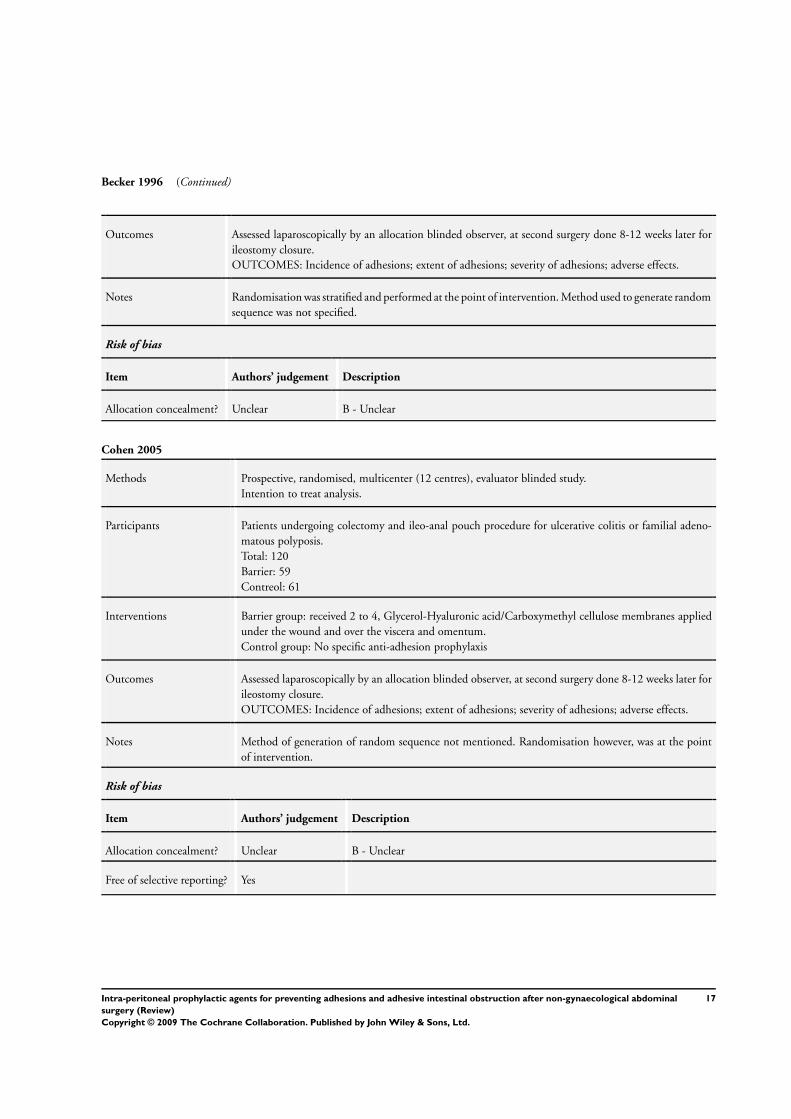
Becker 1996 (Continued)
Outcomes Assessed laparoscopically by an allocation blinded observer, at second surgery done 8-12 weeks later for
ileostomy closure.
OUTCOMES: Incidence of adhesions; extent of adhesions; severity of adhesions; adverse effects.
Notes Randomisation was stratified and performed at the point of intervention. Method used to generate random
sequence was not specified.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Cohen 2005
Methods Prospective, randomised, multicenter (12 centres), evaluator blinded study.
Intention to treat analysis.
Participants Patients undergoing colectomy and ileo-anal pouch procedure for ulcerative colitis or familial adeno-
matous polyposis.
Total: 120
Barrier: 59
Contreol: 61
Interventions Barrier group: received 2 to 4, Glycerol-Hyaluronic acid/Carboxymethyl cellulose membranes applied
under the wound and over the viscera and omentum.
Control group: No specific anti-adhesion prophylaxis
Outcomes Assessed laparoscopically by an allocation blinded observer, at second surgery done 8-12 weeks later for
ileostomy closure.
OUTCOMES: Incidence of adhesions; extent of adhesions; severity of adhesions; adverse effects.
Notes Method of generation of random sequence not mentioned. Randomisation however, was at the point
of intervention.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Free of selective reporting? Yes
17Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
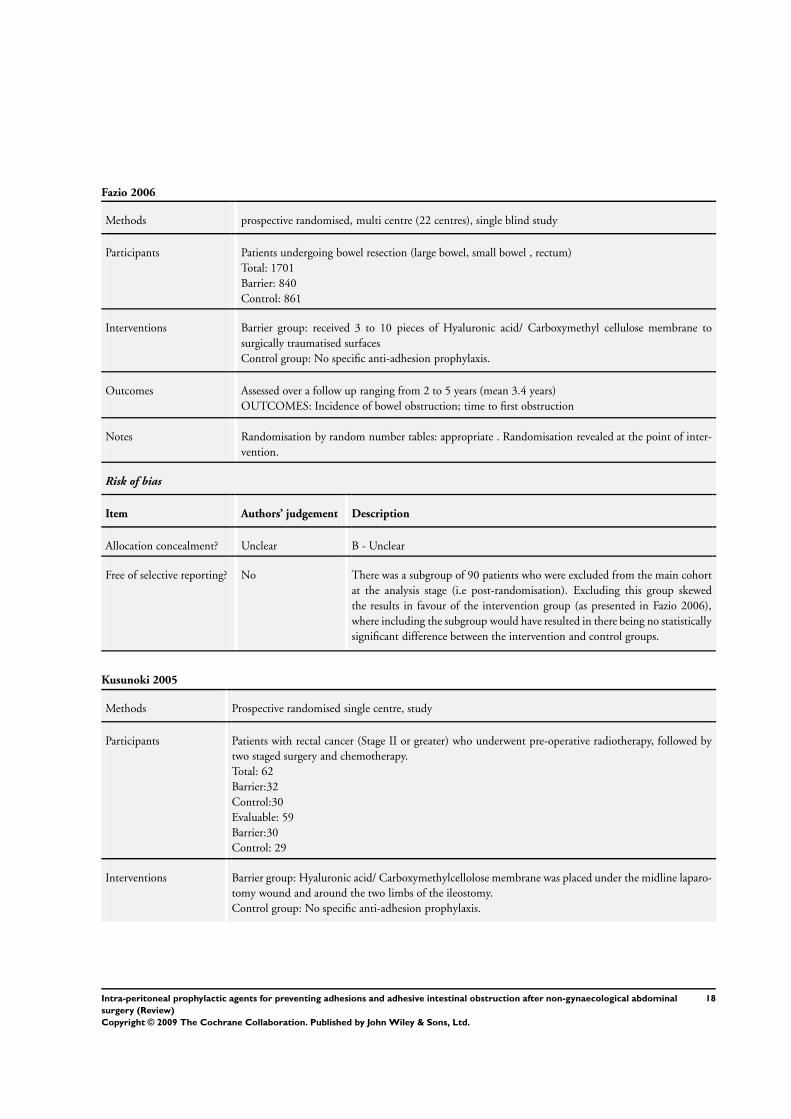
Fazio 2006
Methods prospective randomised, multi centre (22 centres), single blind study
Participants Patients undergoing bowel resection (large bowel, small bowel , rectum)
Total: 1701
Barrier: 840
Control: 861
Interventions Barrier group: received 3 to 10 pieces of Hyaluronic acid/ Carboxymethyl cellulose membrane to
surgically traumatised surfaces
Control group: No specific anti-adhesion prophylaxis.
Outcomes Assessed over a follow up ranging from 2 to 5 years (mean 3.4 years)
OUTCOMES: Incidence of bowel obstruction; time to first obstruction
Notes Randomisation by random number tables: appropriate . Randomisation revealed at the point of inter-
vention.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Free of selective reporting? No There was a subgroup of 90 patients who were excluded from the main cohort
at the analysis stage (i.e post-randomisation). Excluding this group skewed
the results in favour of the intervention group (as presented in Fazio 2006),
where including the subgroup would have resulted in there being no statistically
significant difference between the intervention and control groups.
Kusunoki 2005
Methods Prospective randomised single centre, study
Participants Patients with rectal cancer (Stage II or greater) who underwent pre-operative radiotherapy, followed by
two staged surgery and chemotherapy.
Total: 62
Barrier:32
Control:30
Evaluable: 59
Barrier:30
Control: 29
Interventions Barrier group: Hyaluronic acid/ Carboxymethylcellolose membrane was placed under the midline laparo-
tomy wound and around the two limbs of the ileostomy.
Control group: No specific anti-adhesion prophylaxis.
18Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
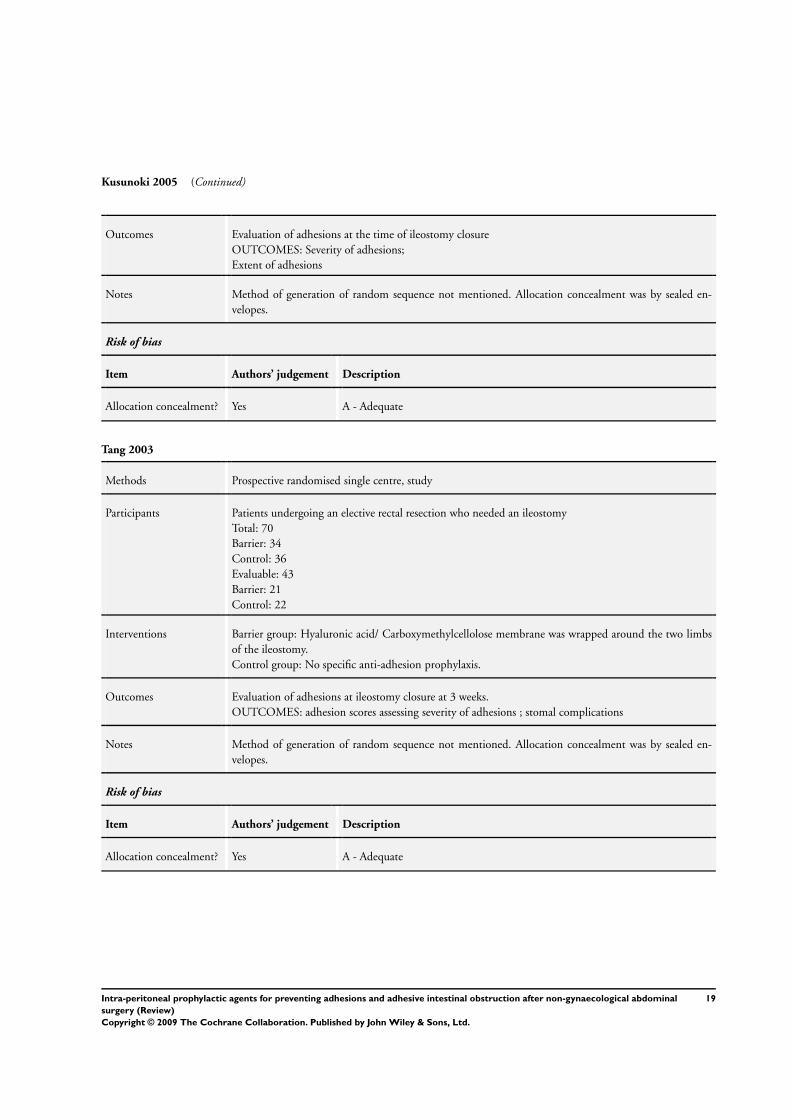
Kusunoki 2005 (Continued)
Outcomes Evaluation of adhesions at the time of ileostomy closure
OUTCOMES: Severity of adhesions;
Extent of adhesions
Notes Method of generation of random sequence not mentioned. Allocation concealment was by sealed en-
velopes.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
Tang 2003
Methods Prospective randomised single centre, study
Participants Patients undergoing an elective rectal resection who needed an ileostomy
Total: 70
Barrier: 34
Control: 36
Evaluable: 43
Barrier: 21
Control: 22
Interventions Barrier group: Hyaluronic acid/ Carboxymethylcellolose membrane was wrapped around the two limbs
of the ileostomy.
Control group: No specific anti-adhesion prophylaxis.
Outcomes Evaluation of adhesions at ileostomy closure at 3 weeks.
OUTCOMES: adhesion scores assessing severity of adhesions ; stomal complications
Notes Method of generation of random sequence not mentioned. Allocation concealment was by sealed en-
velopes.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
19Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
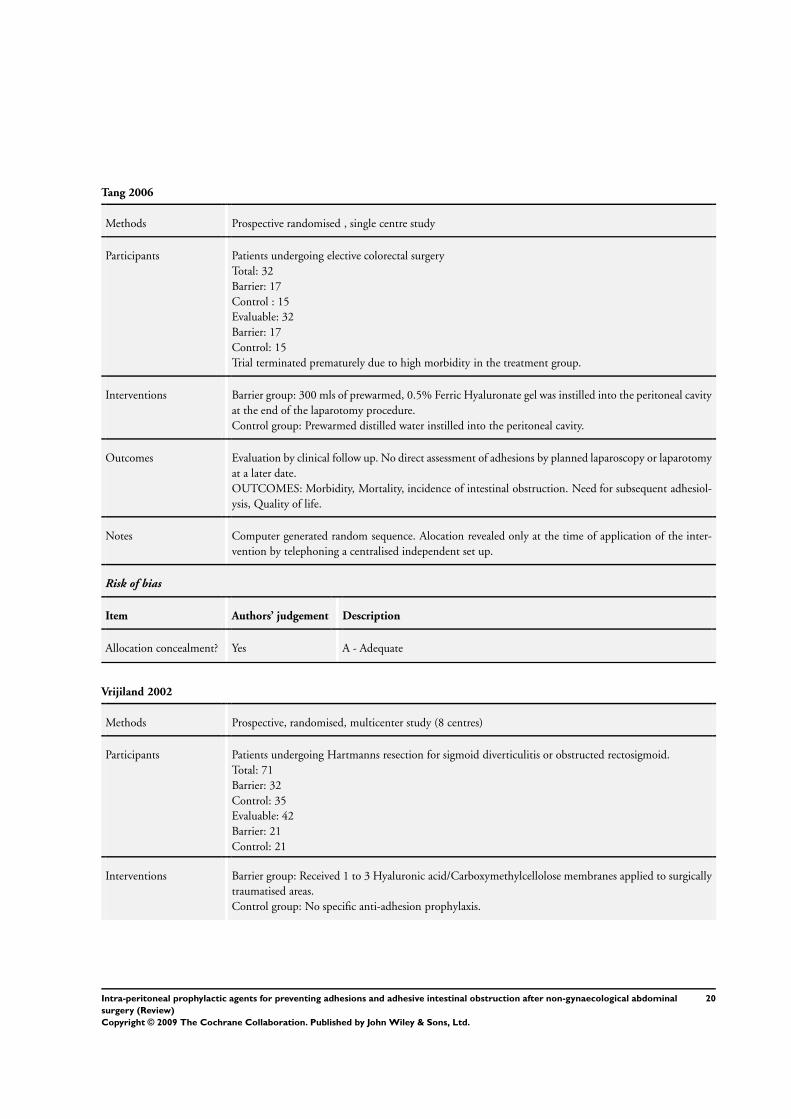
Tang 2006
Methods Prospective randomised , single centre study
Participants Patients undergoing elective colorectal surgery
Total: 32
Barrier: 17
Control : 15
Evaluable: 32
Barrier: 17
Control: 15
Trial terminated prematurely due to high morbidity in the treatment group.
Interventions Barrier group: 300 mls of prewarmed, 0.5% Ferric Hyaluronate gel was instilled into the peritoneal cavity
at the end of the laparotomy procedure.
Control group: Prewarmed distilled water instilled into the peritoneal cavity.
Outcomes Evaluation by clinical follow up. No direct assessment of adhesions by planned laparoscopy or laparotomy
at a later date.
OUTCOMES: Morbidity, Mortality, incidence of intestinal obstruction. Need for subsequent adhesiol-
ysis, Quality of life.
Notes Computer generated random sequence. Alocation revealed only at the time of application of the inter-
vention by telephoning a centralised independent set up.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
Vrijiland 2002
Methods Prospective, randomised, multicenter study (8 centres)
Participants Patients undergoing Hartmanns resection for sigmoid diverticulitis or obstructed rectosigmoid.
Total: 71
Barrier: 32
Control: 35
Evaluable: 42
Barrier: 21
Control: 21
Interventions Barrier group: Received 1 to 3 Hyaluronic acid/Carboxymethylcellolose membranes applied to surgically
traumatised areas.
Control group: No specific anti-adhesion prophylaxis.
20Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
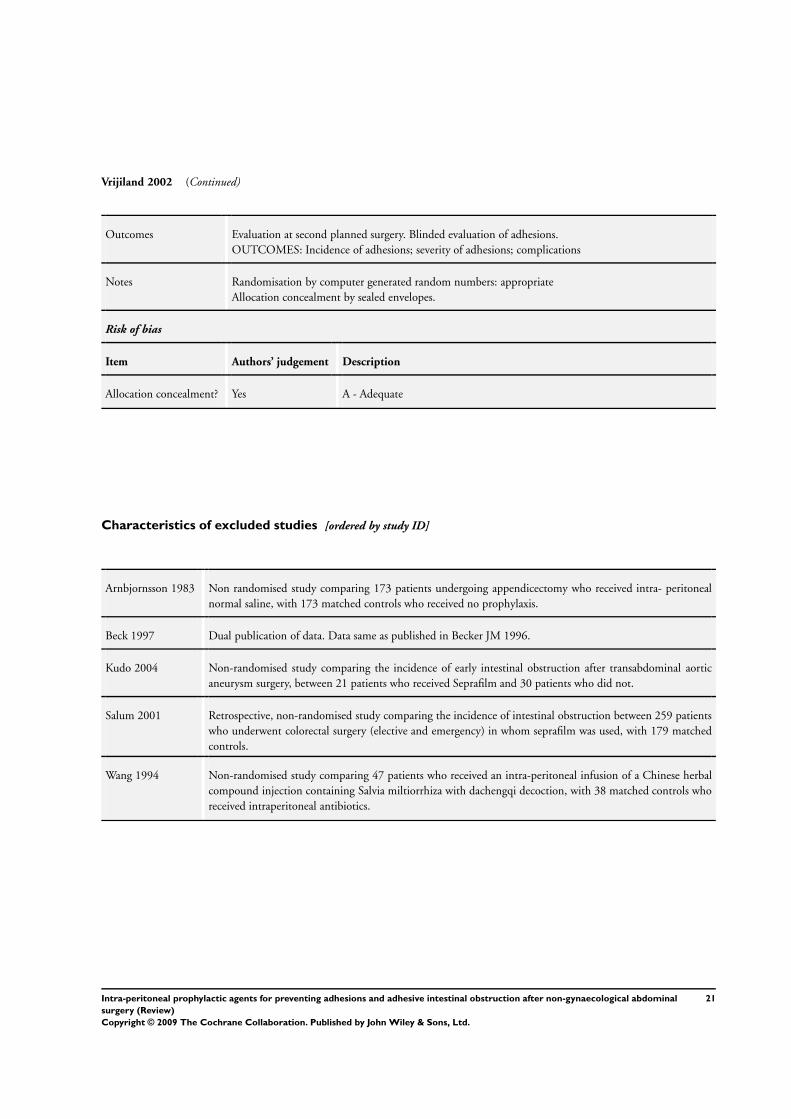
Vrijiland 2002 (Continued)
Outcomes Evaluation at second planned surgery. Blinded evaluation of adhesions.
OUTCOMES: Incidence of adhesions; severity of adhesions; complications
Notes Randomisation by computer generated random numbers: appropriate
Allocation concealment by sealed envelopes.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
Characteristics of excluded studies [ordered by study ID]
Arnbjornsson 1983 Non randomised study comparing 173 patients undergoing appendicectomy who received intra- peritoneal
normal saline, with 173 matched controls who received no prophylaxis.
Beck 1997 Dual publication of data. Data same as published in Becker JM 1996.
Kudo 2004 Non-randomised study comparing the incidence of early intestinal obstruction after transabdominal aortic
aneurysm surgery, between 21 patients who received Seprafilm and 30 patients who did not.
Salum 2001 Retrospective, non-randomised study comparing the incidence of intestinal obstruction between 259 patients
who underwent colorectal surgery (elective and emergency) in whom seprafilm was used, with 179 matched
controls.
Wang 1994 Non-randomised study comparing 47 patients who received an intra-peritoneal infusion of a Chinese herbal
compound injection containing Salvia miltiorrhiza with dachengqi decoction, with 38 matched controls who
received intraperitoneal antibiotics.
21Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
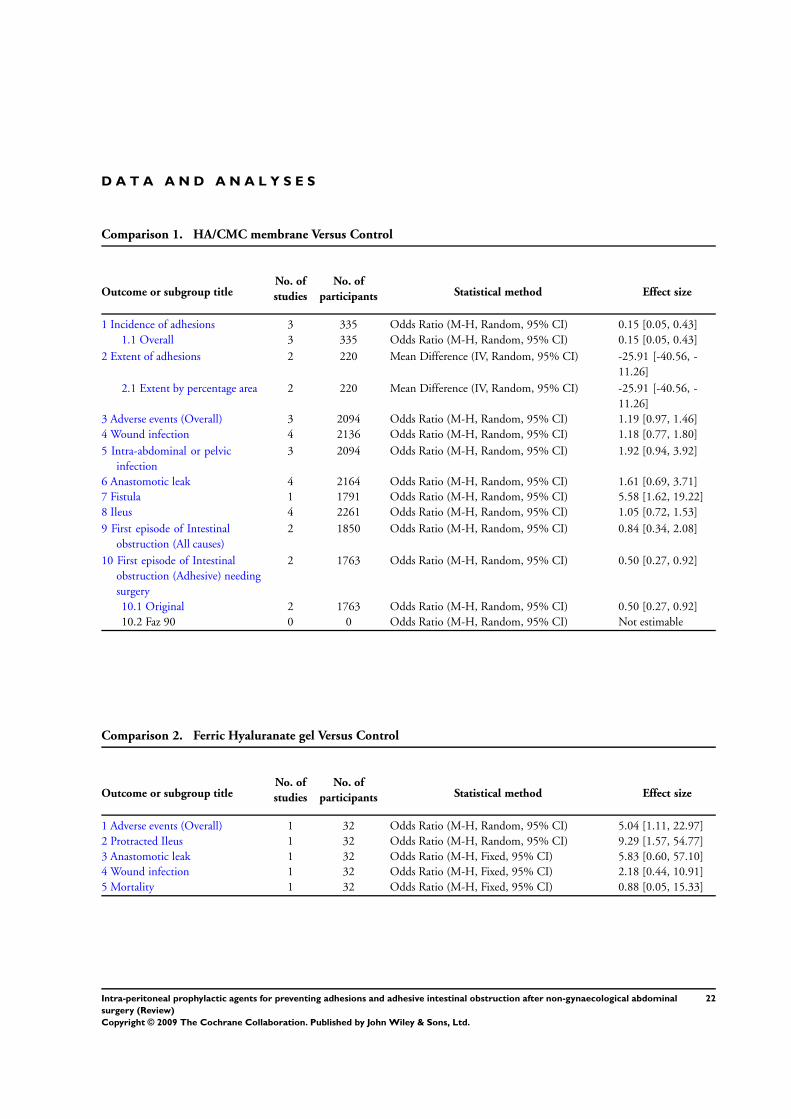
D A T A A N D A N A L Y S E S
Comparison 1. HA/CMC membrane Versus Control
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Incidence of adhesions 3 335 Odds Ratio (M-H, Random, 95% CI) 0.15 [0.05, 0.43]
1.1 Overall 3 335 Odds Ratio (M-H, Random, 95% CI) 0.15 [0.05, 0.43]
2 Extent of adhesions 2 220 Mean Difference (IV, Random, 95% CI) -25.91 [-40.56, -
11.26]
2.1 Extent by percentage area 2 220 Mean Difference (IV, Random, 95% CI) -25.91 [-40.56, -
11.26]
3 Adverse events (Overall) 3 2094 Odds Ratio (M-H, Random, 95% CI) 1.19 [0.97, 1.46]
4 Wound infection 4 2136 Odds Ratio (M-H, Random, 95% CI) 1.18 [0.77, 1.80]
5 Intra-abdominal or pelvic
infection
3 2094 Odds Ratio (M-H, Random, 95% CI) 1.92 [0.94, 3.92]
6 Anastomotic leak 4 2164 Odds Ratio (M-H, Random, 95% CI) 1.61 [0.69, 3.71]
7 Fistula 1 1791 Odds Ratio (M-H, Random, 95% CI) 5.58 [1.62, 19.22]
8 Ileus 4 2261 Odds Ratio (M-H, Random, 95% CI) 1.05 [0.72, 1.53]
9 First episode of Intestinal
obstruction (All causes)
2 1850 Odds Ratio (M-H, Random, 95% CI) 0.84 [0.34, 2.08]
10 First episode of Intestinal
obstruction (Adhesive) needing
surgery
2 1763 Odds Ratio (M-H, Random, 95% CI) 0.50 [0.27, 0.92]
10.1 Original 2 1763 Odds Ratio (M-H, Random, 95% CI) 0.50 [0.27, 0.92]
10.2 Faz 90 0 0 Odds Ratio (M-H, Random, 95% CI) Not estimable
Comparison 2. Ferric Hyaluranate gel Versus Control
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Adverse events (Overall) 1 32 Odds Ratio (M-H, Random, 95% CI) 5.04 [1.11, 22.97]
2 Protracted Ileus 1 32 Odds Ratio (M-H, Random, 95% CI) 9.29 [1.57, 54.77]
3 Anastomotic leak 1 32 Odds Ratio (M-H, Fixed, 95% CI) 5.83 [0.60, 57.10]
4 Wound infection 1 32 Odds Ratio (M-H, Fixed, 95% CI) 2.18 [0.44, 10.91]
5 Mortality 1 32 Odds Ratio (M-H, Fixed, 95% CI) 0.88 [0.05, 15.33]
22Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
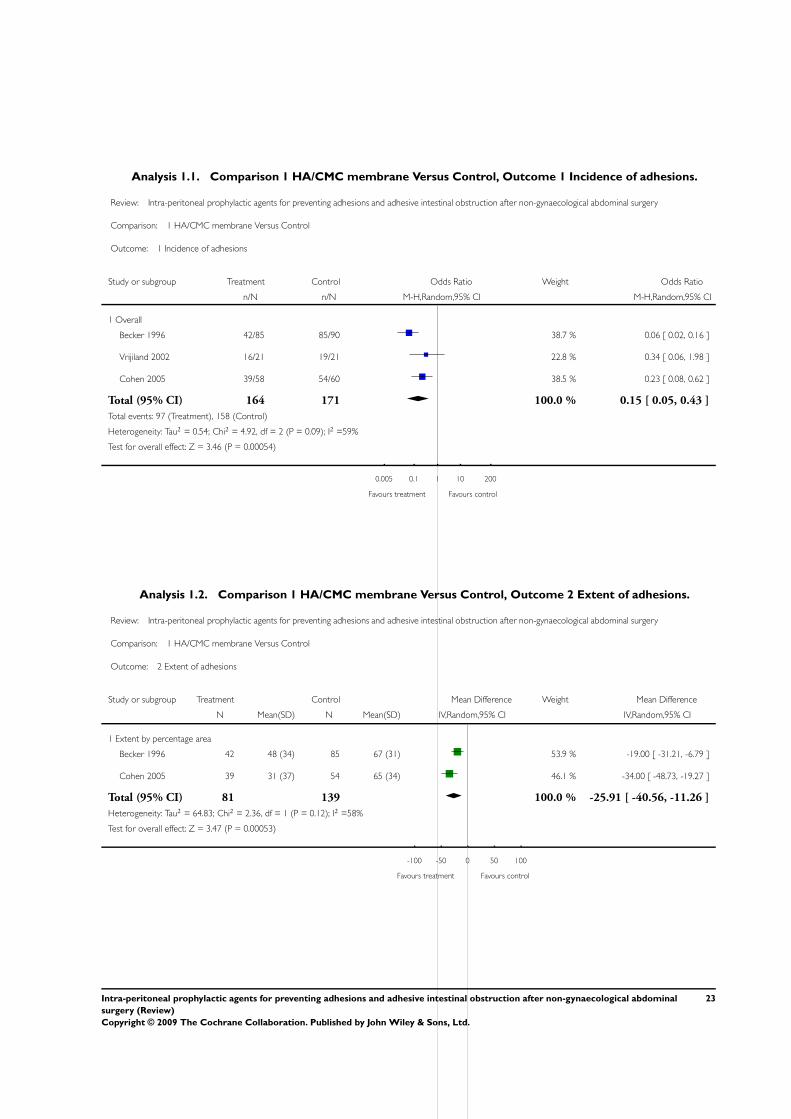
Analysis 1.1. Comparison 1 HA/CMC membrane Versus Control, Outcome 1 Incidence of adhesions.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 1 HA/CMC membrane Versus Control
Outcome: 1 Incidence of adhesions
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
1 Overall
Becker 1996 42/85 85/90 38.7 % 0.06 [ 0.02, 0.16 ]
Vrijiland 2002 16/21 19/21 22.8 % 0.34 [ 0.06, 1.98 ]
Cohen 2005 39/58 54/60 38.5 % 0.23 [ 0.08, 0.62 ]
Total (95% CI) 164 171 100.0 % 0.15 [ 0.05, 0.43 ]
Total events: 97 (Treatment), 158 (Control)
Heterogeneity: Tau2 = 0.54; Chi2 = 4.92, df = 2 (P = 0.09); I2 =59%
Test for overall effect: Z = 3.46 (P = 0.00054)
0.005 0.1 1 10 200
Favours treatment Favours control
Analysis 1.2. Comparison 1 HA/CMC membrane Versus Control, Outcome 2 Extent of adhesions.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 1 HA/CMC membrane Versus Control
Outcome: 2 Extent of adhesions
Study or subgroup Treatment Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
1 Extent by percentage area
Becker 1996 42 48 (34) 85 67 (31) 53.9 % -19.00 [ -31.21, -6.79 ]
Cohen 2005 39 31 (37) 54 65 (34) 46.1 % -34.00 [ -48.73, -19.27 ]
Total (95% CI) 81 139 100.0 % -25.91 [ -40.56, -11.26 ]
Heterogeneity: Tau2 = 64.83; Chi2 = 2.36, df = 1 (P = 0.12); I2 =58%
Test for overall effect: Z = 3.47 (P = 0.00053)
-100 -50 0 50 100
Favours treatment Favours control
23Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
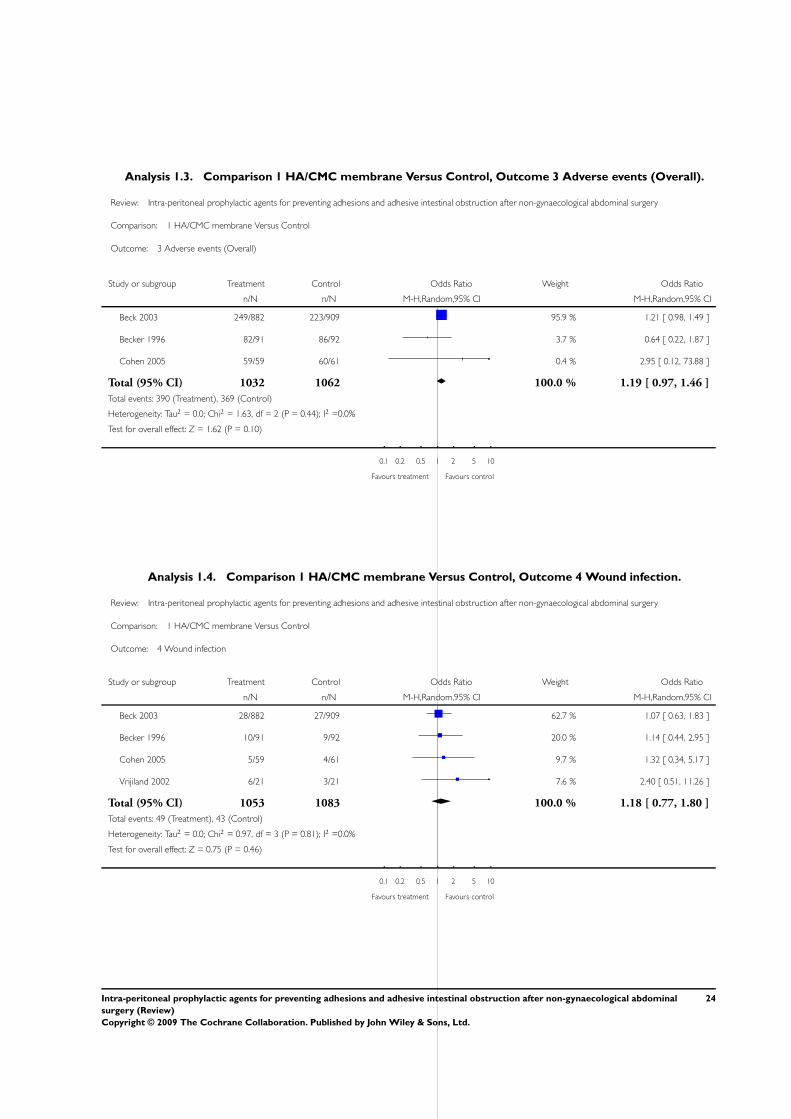
Analysis 1.3. Comparison 1 HA/CMC membrane Versus Control, Outcome 3 Adverse events (Overall).
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 1 HA/CMC membrane Versus Control
Outcome: 3 Adverse events (Overall)
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Beck 2003 249/882 223/909 95.9 % 1.21 [ 0.98, 1.49 ]
Becker 1996 82/91 86/92 3.7 % 0.64 [ 0.22, 1.87 ]
Cohen 2005 59/59 60/61 0.4 % 2.95 [ 0.12, 73.88 ]
Total (95% CI) 1032 1062 100.0 % 1.19 [ 0.97, 1.46 ]
Total events: 390 (Treatment), 369 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 1.63, df = 2 (P = 0.44); I2 =0.0%
Test for overall effect: Z = 1.62 (P = 0.10)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
Analysis 1.4. Comparison 1 HA/CMC membrane Versus Control, Outcome 4 Wound infection.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 1 HA/CMC membrane Versus Control
Outcome: 4 Wound infection
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Beck 2003 28/882 27/909 62.7 % 1.07 [ 0.63, 1.83 ]
Becker 1996 10/91 9/92 20.0 % 1.14 [ 0.44, 2.95 ]
Cohen 2005 5/59 4/61 9.7 % 1.32 [ 0.34, 5.17 ]
Vrijiland 2002 6/21 3/21 7.6 % 2.40 [ 0.51, 11.26 ]
Total (95% CI) 1053 1083 100.0 % 1.18 [ 0.77, 1.80 ]
Total events: 49 (Treatment), 43 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.97, df = 3 (P = 0.81); I2 =0.0%
Test for overall effect: Z = 0.75 (P = 0.46)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
24Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
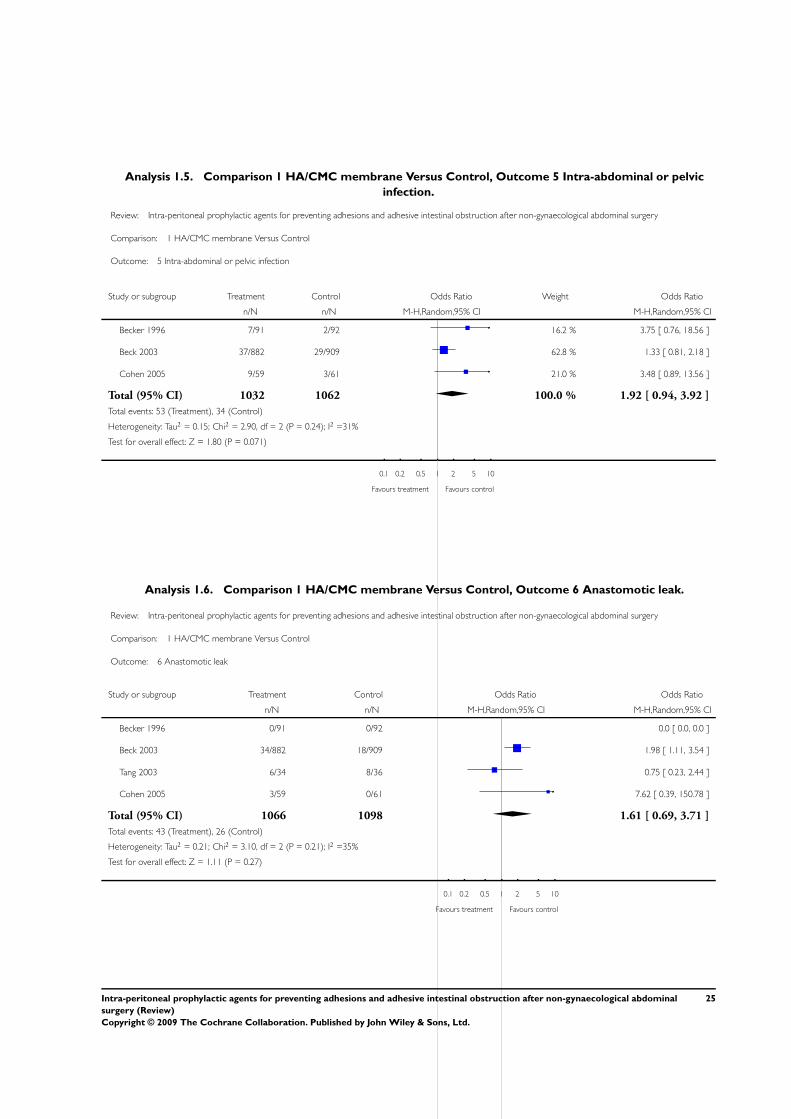
Analysis 1.5. Comparison 1 HA/CMC membrane Versus Control, Outcome 5 Intra-abdominal or pelvic
infection.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 1 HA/CMC membrane Versus Control
Outcome: 5 Intra-abdominal or pelvic infection
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Becker 1996 7/91 2/92 16.2 % 3.75 [ 0.76, 18.56 ]
Beck 2003 37/882 29/909 62.8 % 1.33 [ 0.81, 2.18 ]
Cohen 2005 9/59 3/61 21.0 % 3.48 [ 0.89, 13.56 ]
Total (95% CI) 1032 1062 100.0 % 1.92 [ 0.94, 3.92 ]
Total events: 53 (Treatment), 34 (Control)
Heterogeneity: Tau2 = 0.15; Chi2 = 2.90, df = 2 (P = 0.24); I2 =31%
Test for overall effect: Z = 1.80 (P = 0.071)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
Analysis 1.6. Comparison 1 HA/CMC membrane Versus Control, Outcome 6 Anastomotic leak.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 1 HA/CMC membrane Versus Control
Outcome: 6 Anastomotic leak
Study or subgroup Treatment Control Odds Ratio Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Becker 1996 0/91 0/92 0.0 [ 0.0, 0.0 ]
Beck 2003 34/882 18/909 1.98 [ 1.11, 3.54 ]
Tang 2003 6/34 8/36 0.75 [ 0.23, 2.44 ]
Cohen 2005 3/59 0/61 7.62 [ 0.39, 150.78 ]
Total (95% CI) 1066 1098 1.61 [ 0.69, 3.71 ]
Total events: 43 (Treatment), 26 (Control)
Heterogeneity: Tau2 = 0.21; Chi2 = 3.10, df = 2 (P = 0.21); I2 =35%
Test for overall effect: Z = 1.11 (P = 0.27)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
25Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
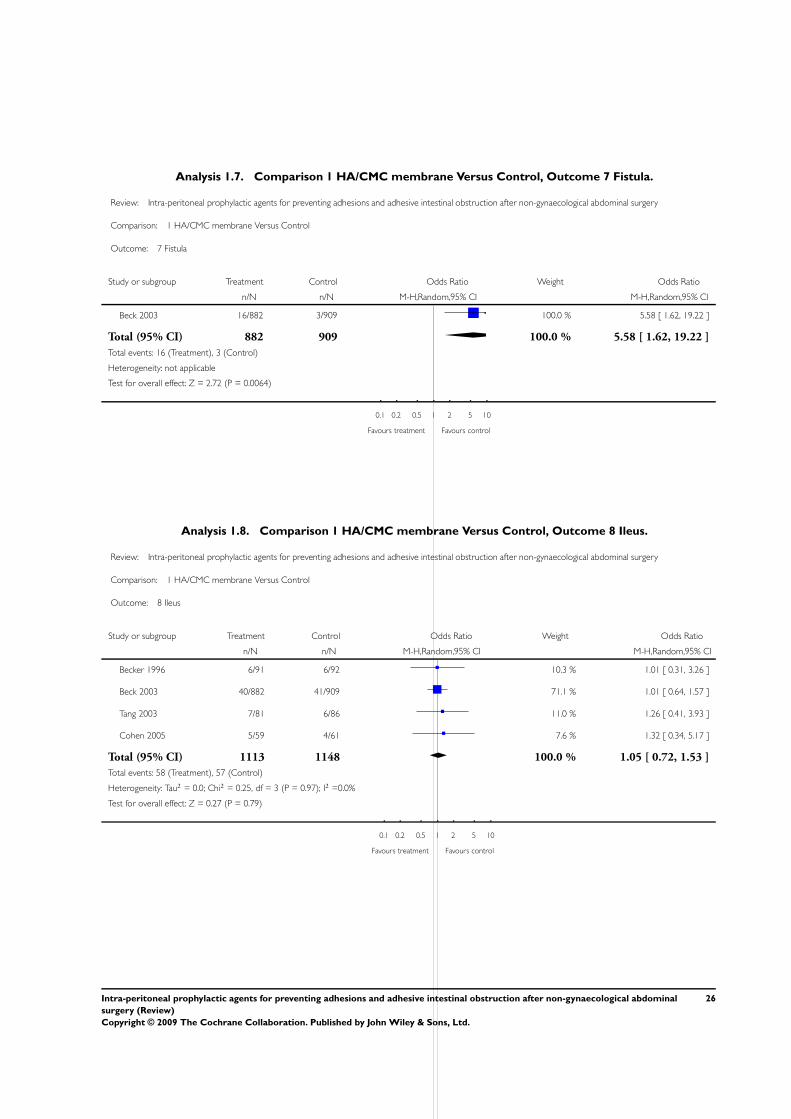
Analysis 1.7. Comparison 1 HA/CMC membrane Versus Control, Outcome 7 Fistula.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 1 HA/CMC membrane Versus Control
Outcome: 7 Fistula
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Beck 2003 16/882 3/909 100.0 % 5.58 [ 1.62, 19.22 ]
Total (95% CI) 882 909 100.0 % 5.58 [ 1.62, 19.22 ]
Total events: 16 (Treatment), 3 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.72 (P = 0.0064)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
Analysis 1.8. Comparison 1 HA/CMC membrane Versus Control, Outcome 8 Ileus.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 1 HA/CMC membrane Versus Control
Outcome: 8 Ileus
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Becker 1996 6/91 6/92 10.3 % 1.01 [ 0.31, 3.26 ]
Beck 2003 40/882 41/909 71.1 % 1.01 [ 0.64, 1.57 ]
Tang 2003 7/81 6/86 11.0 % 1.26 [ 0.41, 3.93 ]
Cohen 2005 5/59 4/61 7.6 % 1.32 [ 0.34, 5.17 ]
Total (95% CI) 1113 1148 100.0 % 1.05 [ 0.72, 1.53 ]
Total events: 58 (Treatment), 57 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.25, df = 3 (P = 0.97); I2 =0.0%
Test for overall effect: Z = 0.27 (P = 0.79)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
26Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
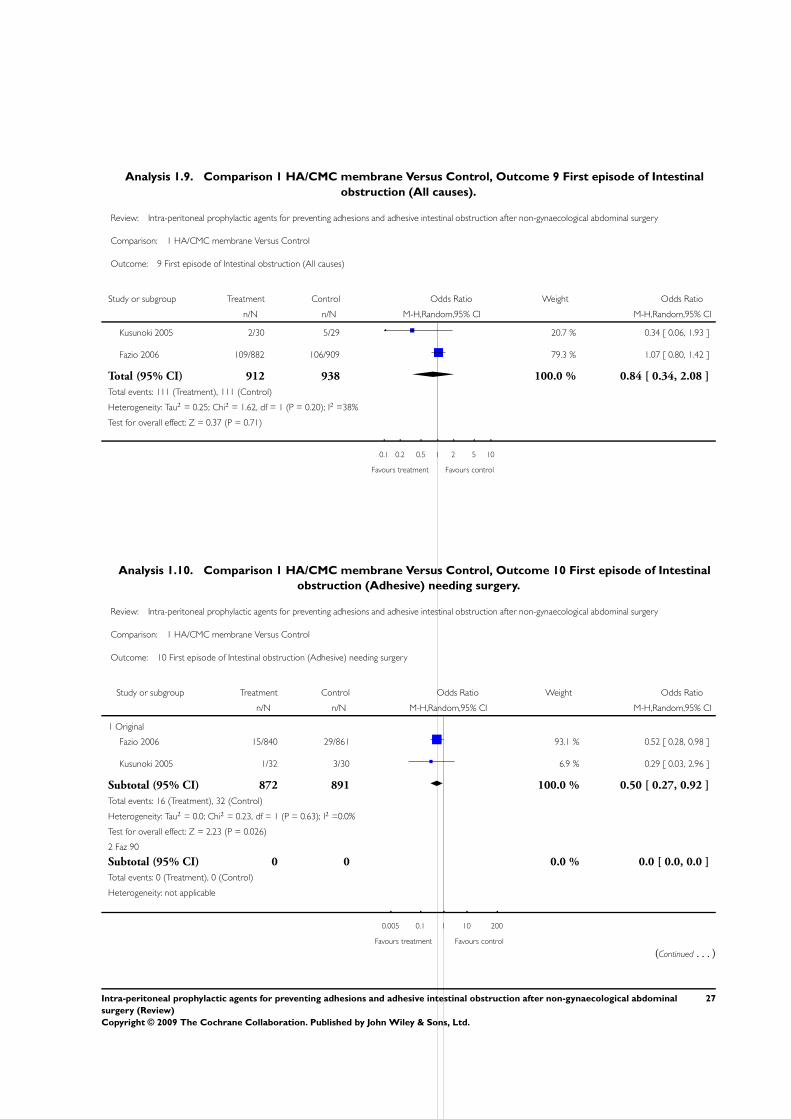
Analysis 1.9. Comparison 1 HA/CMC membrane Versus Control, Outcome 9 First episode of Intestinal
obstruction (All causes).
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 1 HA/CMC membrane Versus Control
Outcome: 9 First episode of Intestinal obstruction (All causes)
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Kusunoki 2005 2/30 5/29 20.7 % 0.34 [ 0.06, 1.93 ]
Fazio 2006 109/882 106/909 79.3 % 1.07 [ 0.80, 1.42 ]
Total (95% CI) 912 938 100.0 % 0.84 [ 0.34, 2.08 ]
Total events: 111 (Treatment), 111 (Control)
Heterogeneity: Tau2 = 0.25; Chi2 = 1.62, df = 1 (P = 0.20); I2 =38%
Test for overall effect: Z = 0.37 (P = 0.71)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
Analysis 1.10. Comparison 1 HA/CMC membrane Versus Control, Outcome 10 First episode of Intestinal
obstruction (Adhesive) needing surgery.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 1 HA/CMC membrane Versus Control
Outcome: 10 First episode of Intestinal obstruction (Adhesive) needing surgery
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
1 Original
Fazio 2006 15/840 29/861 93.1 % 0.52 [ 0.28, 0.98 ]
Kusunoki 2005 1/32 3/30 6.9 % 0.29 [ 0.03, 2.96 ]
Subtotal (95% CI) 872 891 100.0 % 0.50 [ 0.27, 0.92 ]
Total events: 16 (Treatment), 32 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.23, df = 1 (P = 0.63); I2 =0.0%
Test for overall effect: Z = 2.23 (P = 0.026)
2 Faz 90
Subtotal (95% CI) 0 0 0.0 % 0.0 [ 0.0, 0.0 ]
Total events: 0 (Treatment), 0 (Control)
Heterogeneity: not applicable
0.005 0.1 1 10 200
Favours treatment Favours control
(Continued . . . )
27Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
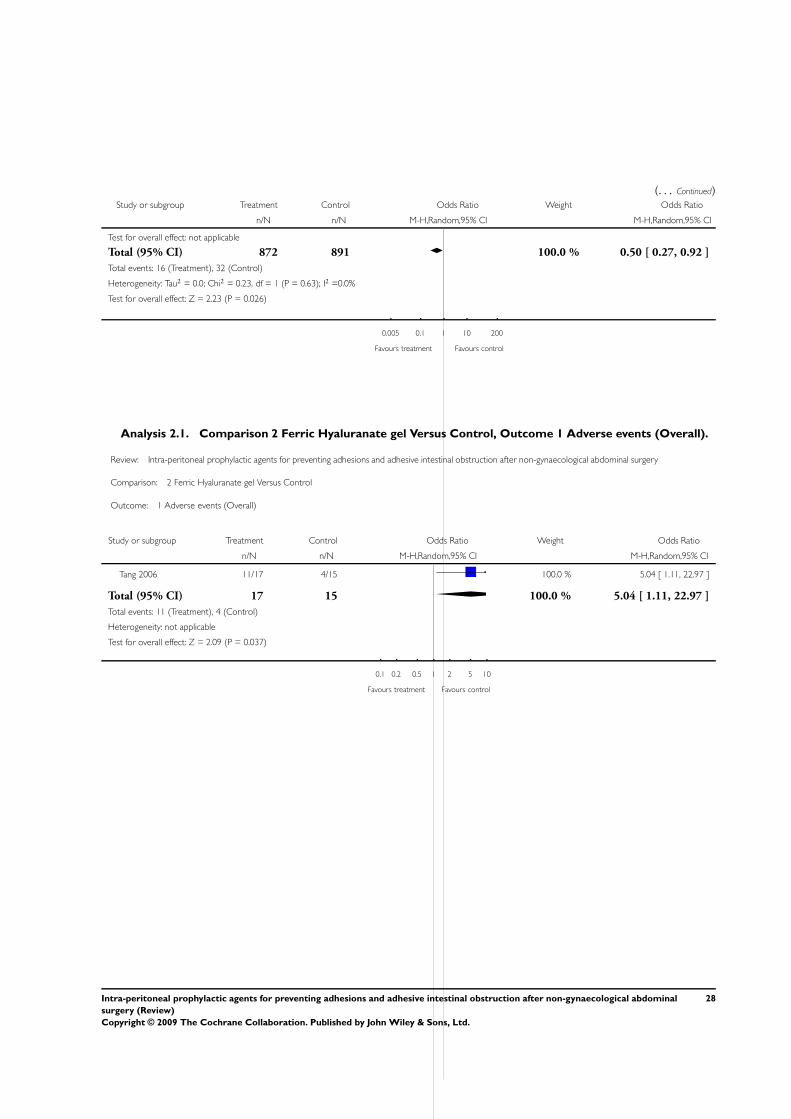
(. . . Continued)Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Test for overall effect: not applicable
Total (95% CI) 872 891 100.0 % 0.50 [ 0.27, 0.92 ]
Total events: 16 (Treatment), 32 (Control)
Heterogeneity: Tau2 = 0.0; Chi2 = 0.23, df = 1 (P = 0.63); I2 =0.0%
Test for overall effect: Z = 2.23 (P = 0.026)
0.005 0.1 1 10 200
Favours treatment Favours control
Analysis 2.1. Comparison 2 Ferric Hyaluranate gel Versus Control, Outcome 1 Adverse events (Overall).
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 2 Ferric Hyaluranate gel Versus Control
Outcome: 1 Adverse events (Overall)
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Tang 2006 11/17 4/15 100.0 % 5.04 [ 1.11, 22.97 ]
Total (95% CI) 17 15 100.0 % 5.04 [ 1.11, 22.97 ]
Total events: 11 (Treatment), 4 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.09 (P = 0.037)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
28Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
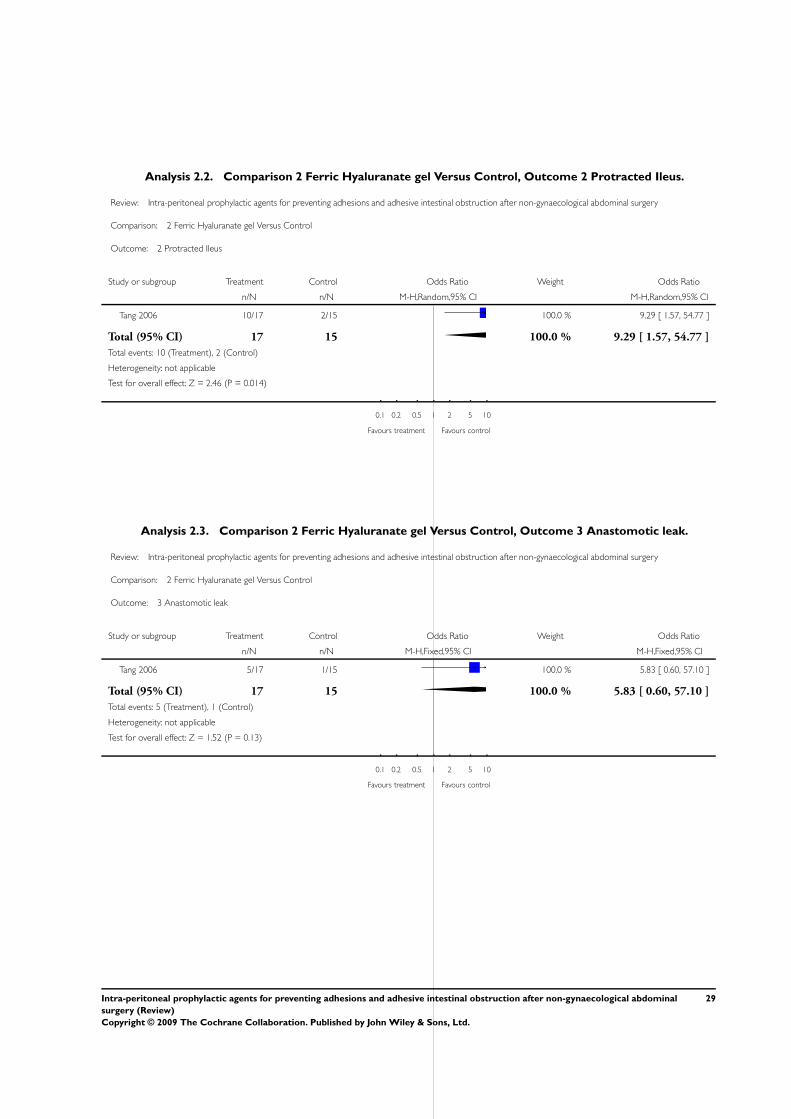
Analysis 2.2. Comparison 2 Ferric Hyaluranate gel Versus Control, Outcome 2 Protracted Ileus.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 2 Ferric Hyaluranate gel Versus Control
Outcome: 2 Protracted Ileus
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Random,95% CI M-H,Random,95% CI
Tang 2006 10/17 2/15 100.0 % 9.29 [ 1.57, 54.77 ]
Total (95% CI) 17 15 100.0 % 9.29 [ 1.57, 54.77 ]
Total events: 10 (Treatment), 2 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 2.46 (P = 0.014)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
Analysis 2.3. Comparison 2 Ferric Hyaluranate gel Versus Control, Outcome 3 Anastomotic leak.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 2 Ferric Hyaluranate gel Versus Control
Outcome: 3 Anastomotic leak
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Tang 2006 5/17 1/15 100.0 % 5.83 [ 0.60, 57.10 ]
Total (95% CI) 17 15 100.0 % 5.83 [ 0.60, 57.10 ]
Total events: 5 (Treatment), 1 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 1.52 (P = 0.13)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
29Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
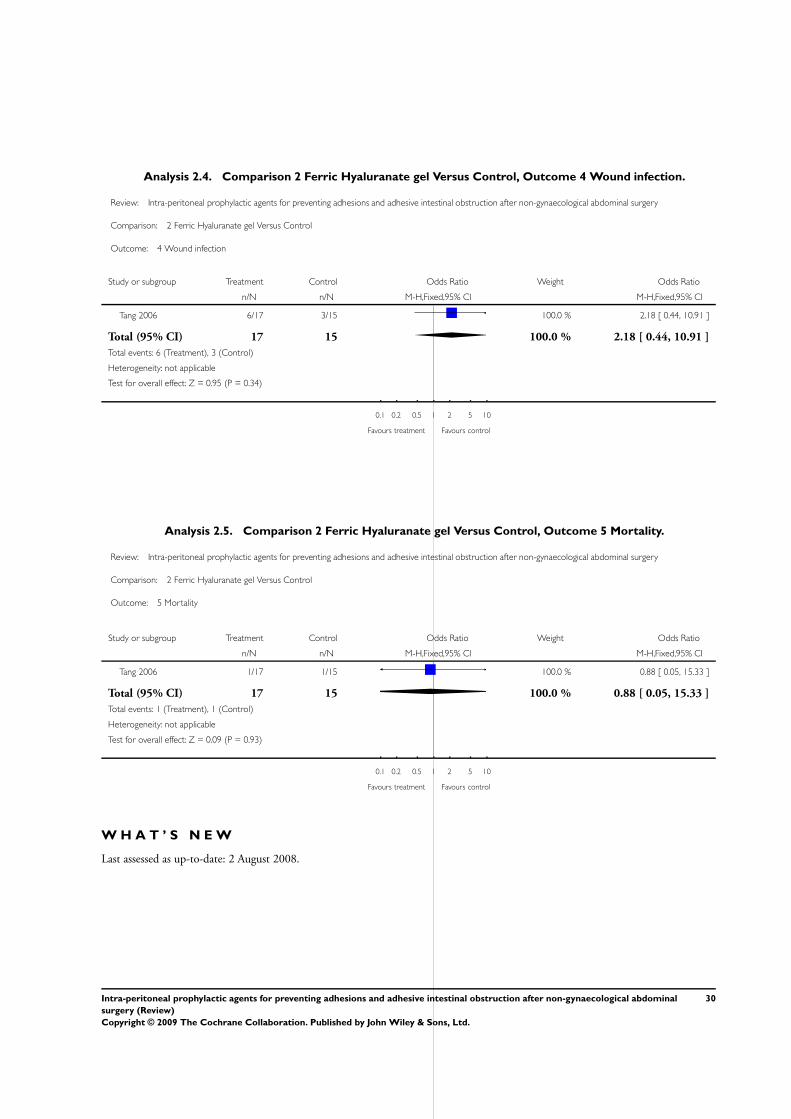
Analysis 2.4. Comparison 2 Ferric Hyaluranate gel Versus Control, Outcome 4 Wound infection.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 2 Ferric Hyaluranate gel Versus Control
Outcome: 4 Wound infection
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Tang 2006 6/17 3/15 100.0 % 2.18 [ 0.44, 10.91 ]
Total (95% CI) 17 15 100.0 % 2.18 [ 0.44, 10.91 ]
Total events: 6 (Treatment), 3 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.95 (P = 0.34)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
Analysis 2.5. Comparison 2 Ferric Hyaluranate gel Versus Control, Outcome 5 Mortality.
Review: Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal surgery
Comparison: 2 Ferric Hyaluranate gel Versus Control
Outcome: 5 Mortality
Study or subgroup Treatment Control Odds Ratio Weight Odds Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Tang 2006 1/17 1/15 100.0 % 0.88 [ 0.05, 15.33 ]
Total (95% CI) 17 15 100.0 % 0.88 [ 0.05, 15.33 ]
Total events: 1 (Treatment), 1 (Control)
Heterogeneity: not applicable
Test for overall effect: Z = 0.09 (P = 0.93)
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
W H A T ’ S N E W
Last assessed as up-to-date: 2 August 2008.
30Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
23 October 2008 Amended Copy edited version for publication
3 August 2008 Amended Substantive amendment
H I S T O R Y
Protocol first published: Issue 1, 2005
Review first published: Issue 1, 2009
8 June 2004 New citation required and conclusions have changed Substantive amendment
C O N T R I B U T I O N S O F A U T H O R S
SK: Development of protocol, literature search, contacting authors, publishers and other sources of information where necessary,
choosing relevant papers for review, critical appraisal of included and excluded studies, data extraction and analysis, writing the final
version of the review.
PFW: Literature search, critical appraisal of included and excluded studies, data extraction and analysis, participate in writing the final
version of the review.
DJL: Oversee the drafting of the protocol, Scrutinise papers and participate in decisions regarding inclusion and exclusion of studies,
supervise data extraction and analysis, participate and supervise the writing of the final version of he review.
D E C L A R A T I O N S O F I N T E R E S T
There was no potential or actual conflict of interest perceived by the authors. This review did not receive any external funding.
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
In the protocol it was stated that, for inclusion in the review, the length of follow up for studies reporting on long term outcomes
should be at least 5 years. This was ideal. But among the available studies which satisfied all other criteria for inclusion, there were no
studies with follow up of 5 years of more. Hence, in the review, it was decided to include studies even with a follow up shorter than the
ideal of 5 years, as stated in the protocol.
Similarly, for studies reporting on short term outcomes, pertaining to safety, studies with a shorter follow up less than the ideal of 1
year, were also included in the review.
31Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

I N D E X T E R M SMedical Subject Headings (MeSH)
∗Membranes, Artificial; Abdomen [∗surgery]; Hyaluronic Acid [administration & dosage; adverse effects; ∗analogs & derivatives;∗therapeutic use]; Intestinal Obstruction [∗prevention & control]; Postoperative Complications [∗prevention & control]; Randomized
Controlled Trials as Topic; Tissue Adhesions [prevention & control]
MeSH check words
Humans
32Intra-peritoneal prophylactic agents for preventing adhesions and adhesive intestinal obstruction after non-gynaecological abdominal
surgery (Review)
Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Related Documents