Intra-arterial administration of Bone- marrow mononuclear cells in patients with critical limb ischemia – a randomized placebo-controlled trial PROVASA D.H.Walter, H. Krankenberg, J. Balzer, C. Kalka, I. Baumgartner, M. Schlüter, T.Tonn, F.Seeger S.Dimmeler, E.Lindhoff-Last, A.M.Zeiher MVZ Prof. Mathey, Prof. Schofer, Hamburg, Cardiology - Angiology and Radiology, Frankfurt Inselspital Bern Blutspendedienst Hessen ClinicalTrials.gov number : NCT00282646

Intra-arterial administration of Bone- marrow mononuclear cells in patients with critical limb ischemia – a randomized placebo-controlled trial PROVASA.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Intra-arterial administration of Bone-marrow mononuclear cells in patients with
critical limb ischemia –a randomized placebo-controlled
trial PROVASA
Intra-arterial administration of Bone-marrow mononuclear cells in patients with
critical limb ischemia –a randomized placebo-controlled
trial PROVASA
D.H.Walter, H. Krankenberg, J. Balzer, C. Kalka, I. Baumgartner, M. Schlüter, T.Tonn, F.Seeger S.Dimmeler, E.Lindhoff-
Last, A.M.Zeiher
MVZ Prof. Mathey, Prof. Schofer, Hamburg, Cardiology - Angiology and Radiology, Frankfurt
Inselspital BernBlutspendedienst Hessen
ClinicalTrials.gov number : NCT00282646
D.H.Walter, H. Krankenberg, J. Balzer, C. Kalka, I. Baumgartner, M. Schlüter, T.Tonn, F.Seeger S.Dimmeler, E.Lindhoff-
Last, A.M.Zeiher
MVZ Prof. Mathey, Prof. Schofer, Hamburg, Cardiology - Angiology and Radiology, Frankfurt
Inselspital BernBlutspendedienst Hessen
ClinicalTrials.gov number : NCT00282646
I do not have any potential conflict of interest

Intra-arterial Application of Bone-Marrow Mononuclear Cells
Isolation of mononuclear cells (Ficoll)
BSD HessenGMP Facility
Bone-marrow(50 ml,
Local anesthesia)
*
Intracoronary
In PAOD: no randomized placebo controlled trials available
PROVASABackground
*
REPAIR AMI
Schächinger V et al.
NEJM 2006
Critical limb ischemia
Rutherford 4-6
*
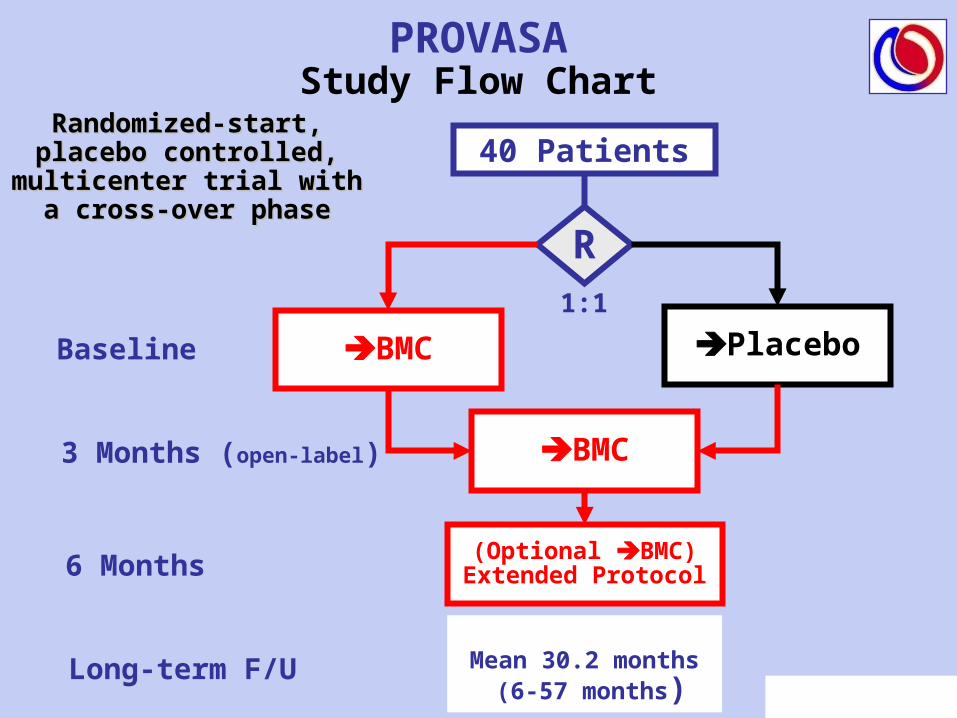
PROVASAStudy Flow Chart
40 Patients
R
BMC Placebo
BMC
(Optional BMC)Extended Protocol
Baseline
3 Months (open-label)
6 Months
1:1
Long-term F/U Mean 30.2 months (6-57 months)
Randomized-start, Randomized-start, placebo controlled, placebo controlled,
multicenter trial with a multicenter trial with a cross-over phasecross-over phase
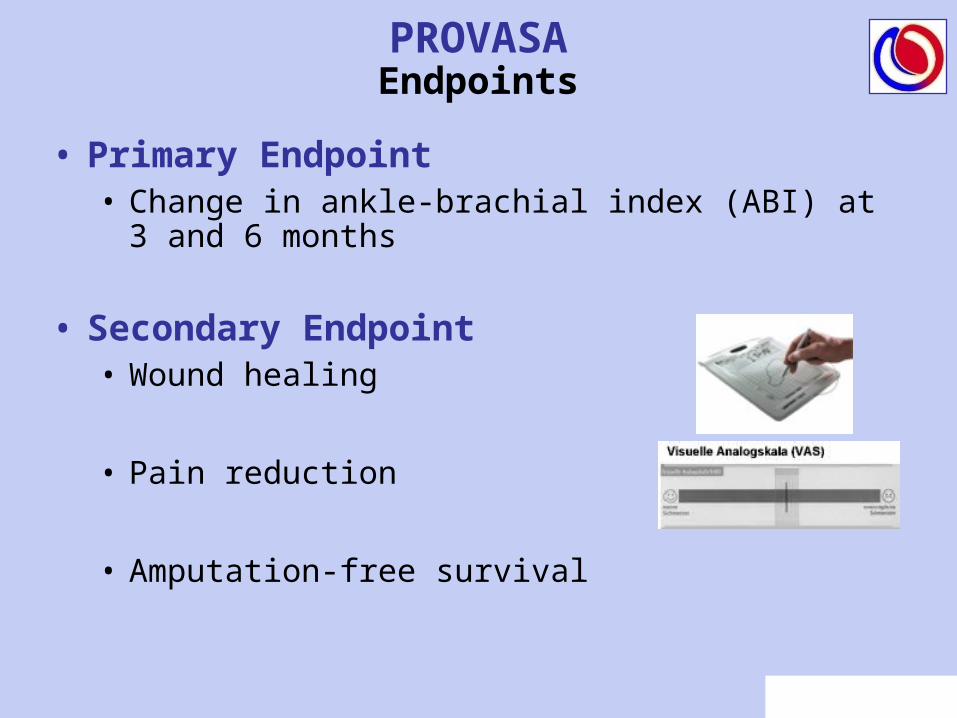
PROVASAEndpoints
• Primary Endpoint• Change in ankle-brachial index (ABI) at 3 and 6
months
• Secondary Endpoint• Wound healing
• Pain reduction
• Amputation-free survival

PROVASAInclusion/Exclusion Criteria
• Patients with Fontaine III or IVwho were not candidates for interventional or surgical revascularization or who failed to respond to interventional or surgical procedures.
• PAOD or thrombangitis obliterans (TAO)
• Exclusion:prior PTA or Bypass < 3 months
• Creatinine > 2.0 mg/dl at time ot treatment
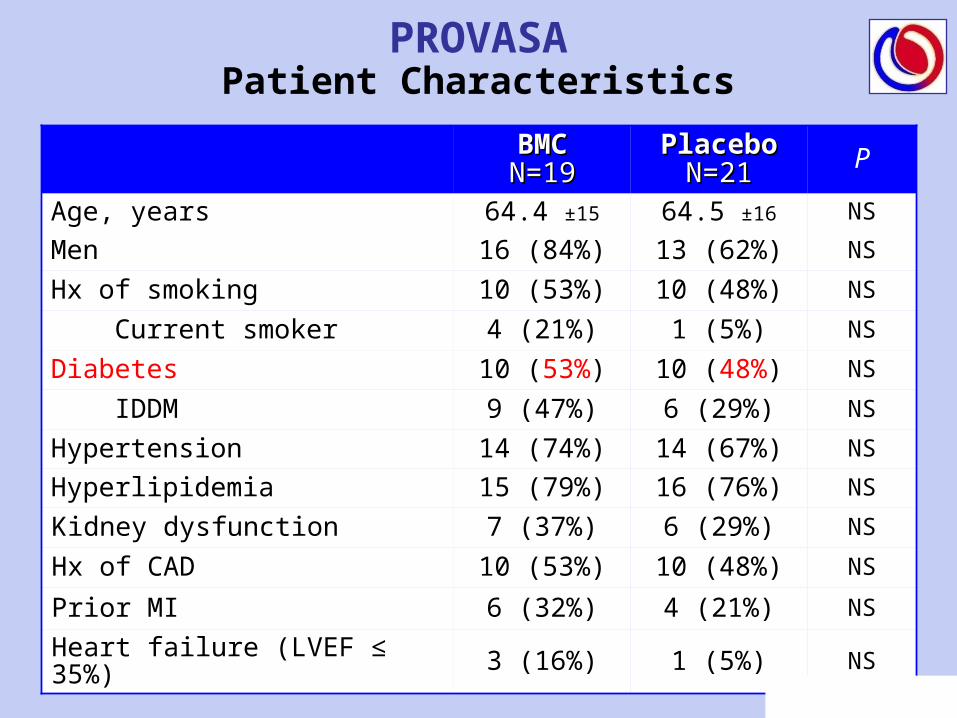
PROVASAPatient Characteristics
BMCBMCN=19N=19
PlaceboPlaceboN=21N=21 P
Age, years 64.4 ±15 64.5 ±16 NS
Men 16 (84%) 13 (62%) NS
Hx of smoking 10 (53%) 10 (48%) NS
Current smoker 4 (21%) 1 (5%) NS
Diabetes 10 (53%) 10 (48%) NS
IDDM 9 (47%) 6 (29%) NS
Hypertension 14 (74%) 14 (67%) NS
Hyperlipidemia 15 (79%) 16 (76%) NS
Kidney dysfunction 7 (37%) 6 (29%) NS
Hx of CAD 10 (53%) 10 (48%) NS
Prior MI 6 (32%) 4 (21%) NS
Heart failure (LVEF ≤ 35%) 3 (16%) 1 (5%) NS
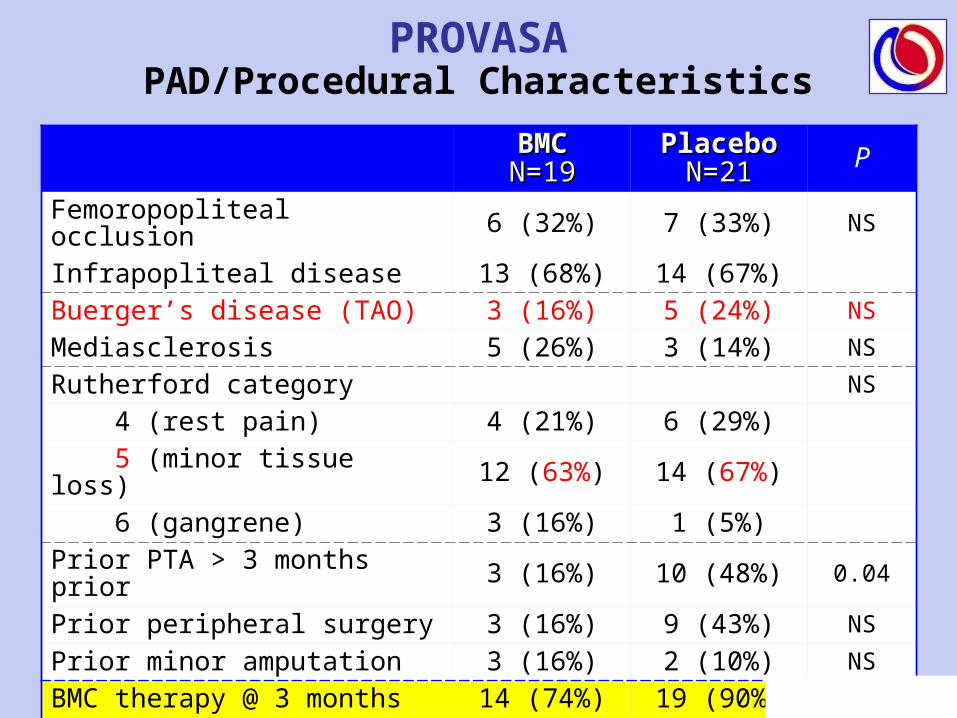
PROVASAPAD/Procedural Characteristics
BMCBMCN=19N=19
PlaceboPlaceboN=21N=21 P
Femoropopliteal occlusion 6 (32%) 7 (33%) NS
Infrapopliteal disease 13 (68%) 14 (67%)Buerger’s disease (TAO) 3 (16%) 5 (24%) NS
Mediasclerosis 5 (26%) 3 (14%) NS
Rutherford category NS
4 (rest pain) 4 (21%) 6 (29%) 5 (minor tissue loss) 12 (63%) 14 (67%) 6 (gangrene) 3 (16%) 1 (5%)Prior PTA > 3 months prior 3 (16%) 10 (48%) 0.04
Prior peripheral surgery 3 (16%) 9 (43%) NS
Prior minor amputation 3 (16%) 2 (10%) NS
BMC therapy @ 3 months 14 (74%) 19 (90%) NS
BMC therapy > 6 months 5 (26%) 6 (29%) NS
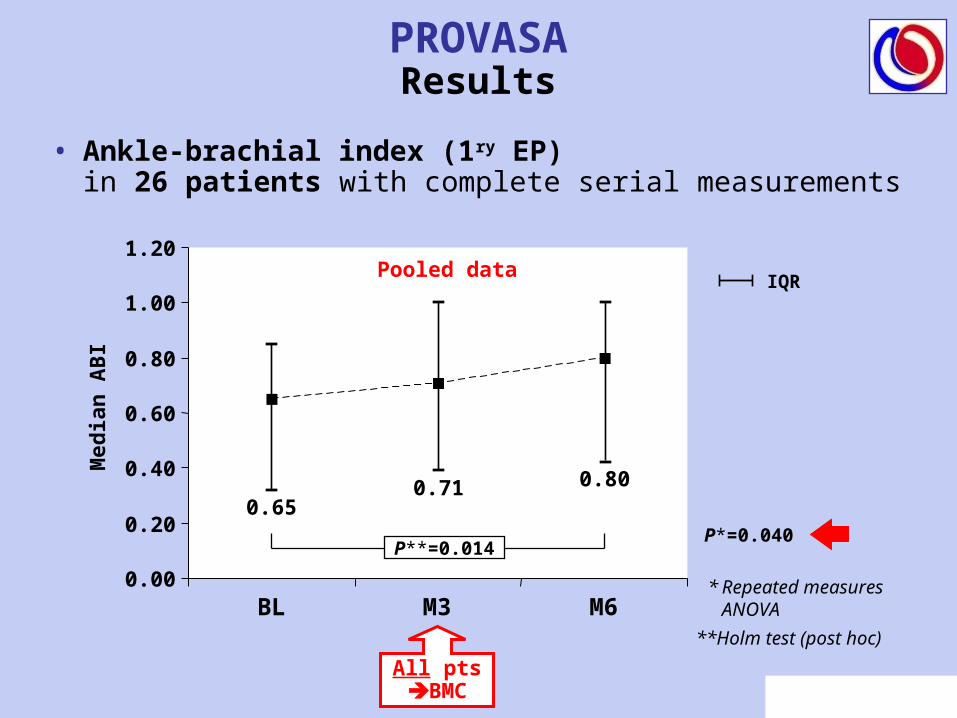
PROVASAResults
• Ankle-brachial index (1ry EP)in 26 patients with complete serial measurements
0.00
0.20
0.40
0.60
0.80
1.00
1.20
BL M3 M6
Med
ian
AB
I
IQR
0.800.710.65
P*=0.040
* Repeated measures ANOVA
All ptsBMC
P**=0.014
**Holm test (post hoc)
Pooled data
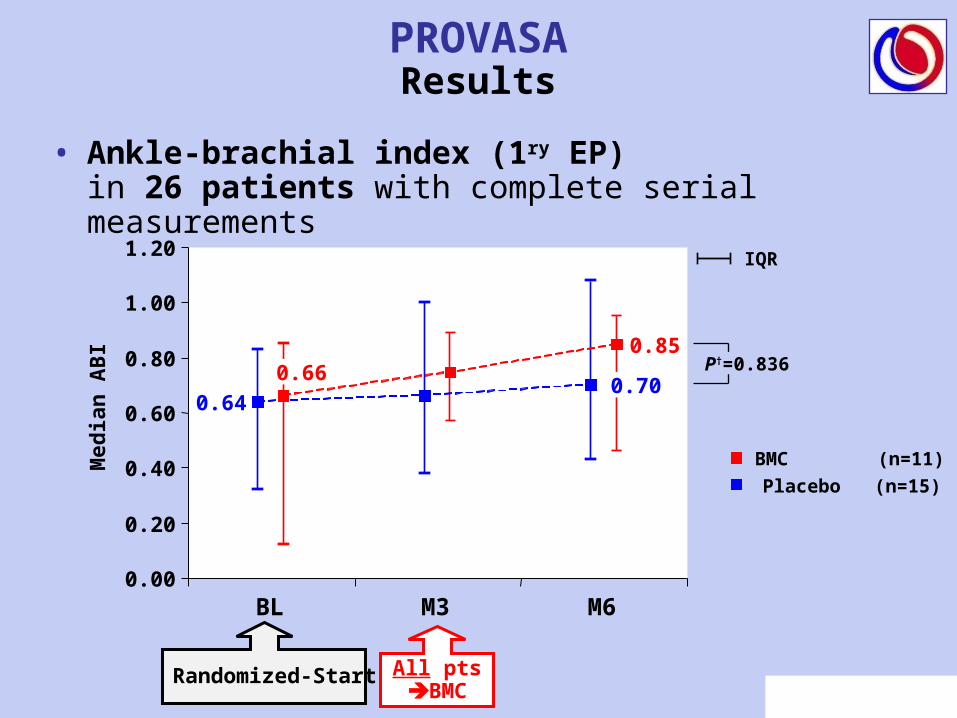
PROVASAResults
• Ankle-brachial index (1ry EP)in 26 patients with complete serial measurements
0.00
0.20
0.40
0.60
0.80
1.00
1.20
BL M3 M6
Med
ian
AB
I
IQR
BMC (n=11)
Placebo (n=15)
0.85
0.700.64
0.66
All ptsBMC
P†=0.836
Randomized-Start
PROVASAThe Primary Endpoint Dilemma
• ABI values were not useful as primary endpoint
• Changes in ABI do not correlate well with ulcer healing and limb salvage
• In patients with thrombangiitis obliterans (TAO) as well as in patients with extensive mediasclerosis, ABI values do not reflect the degree of distal ischemia and tissue necrosis.
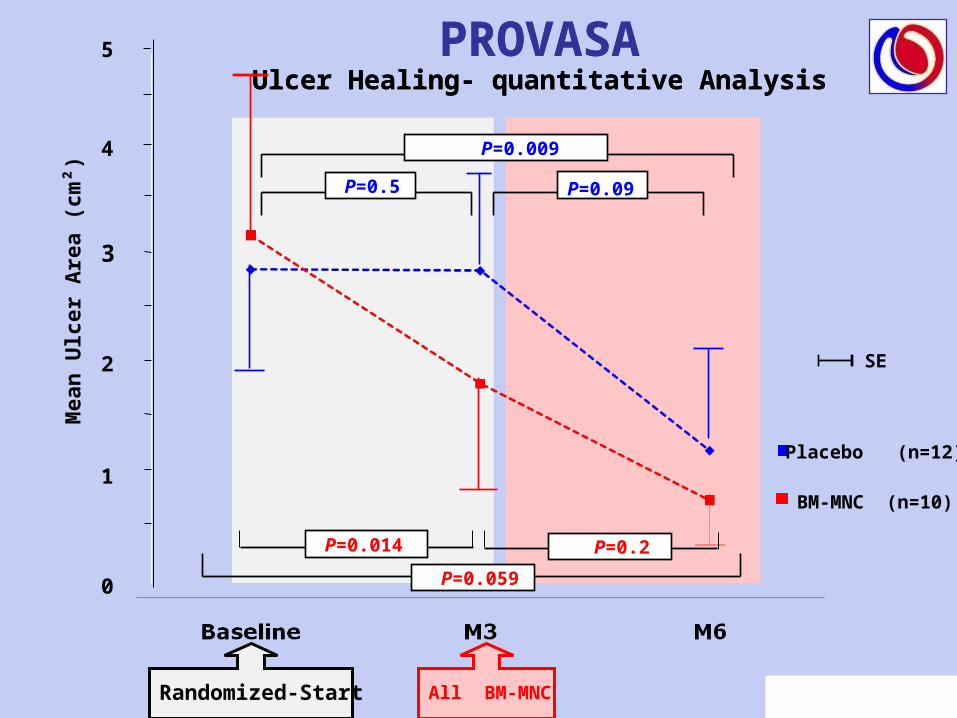
PROVASAUlcer Healing- quantitative Analysis
PROVASAUlcer Healing- quantitative Analysis
Figure 3A
4
0
1
2
3
5
BM-MNC (n=10)
Placebo (n=12)
P=0.014
All BM-MNCRandomized-Start
Mea
n U
lcer
Are
a (c
m²)
P=0.009
P=0.5
SE
P=0.2
P=0.059
P=0.09
Mea
n R
edu
ctio
n o
f U
lcer
Are
a (c
m²)
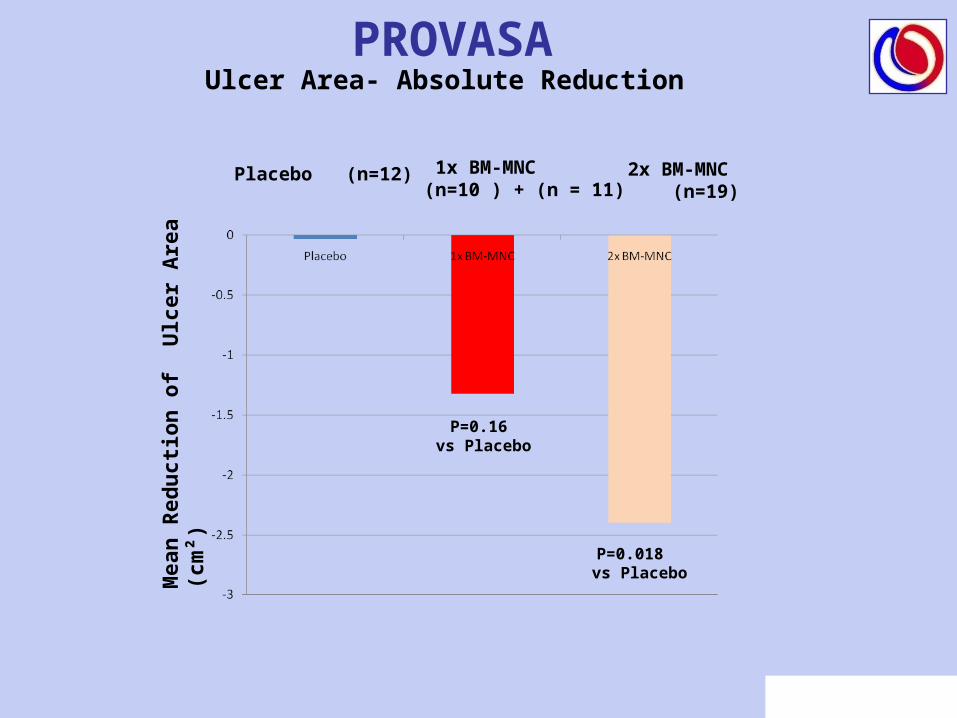
1x BM-MNC (n=10 ) + (n = 11)
Placebo (n=12) 2x BM-MNC (n=19)
P=0.16 vs Placebo
P=0.018 vs Placebo
PROVASAUlcer Area- Absolute Reduction

PROVASAPatients with Complete Ulcer Healing
NS
P=0.037All BMC vs. PlaceboMean time to ulcer
healing 10.9 months
All ptsBMC
• No difference in complete ulcer healing within 3 months between BMC vs Placebo
• Complete healing of ulcers 20/30 patients (66.6%)
• 20/21 (95%) complete healing in patients with stable ulcers, 17/21 (81%) after repeated BMC !
PROVASAUlcer healing

PROVASAPain Analysis-Serial Values
BM-MNC (n=10)
Placebo (n=15)
P=0.02
All BM-MNCRandomized-Start
Pai
n s
cale
P=0.13
M6M3BL
SE
P=0.004 P=0.3
P=0.002
P=0.009 P=0.343
P=0.014

PROVASAPain Analysis-Absolute Reduction
1x BM-MNC (n=15 ) + (n = 10)
Placebo (n=15) 2x BM-MNC (n=10)
Pai
n s
cale
P=0.002 vs Placebo
P=0.1 vs Placebo
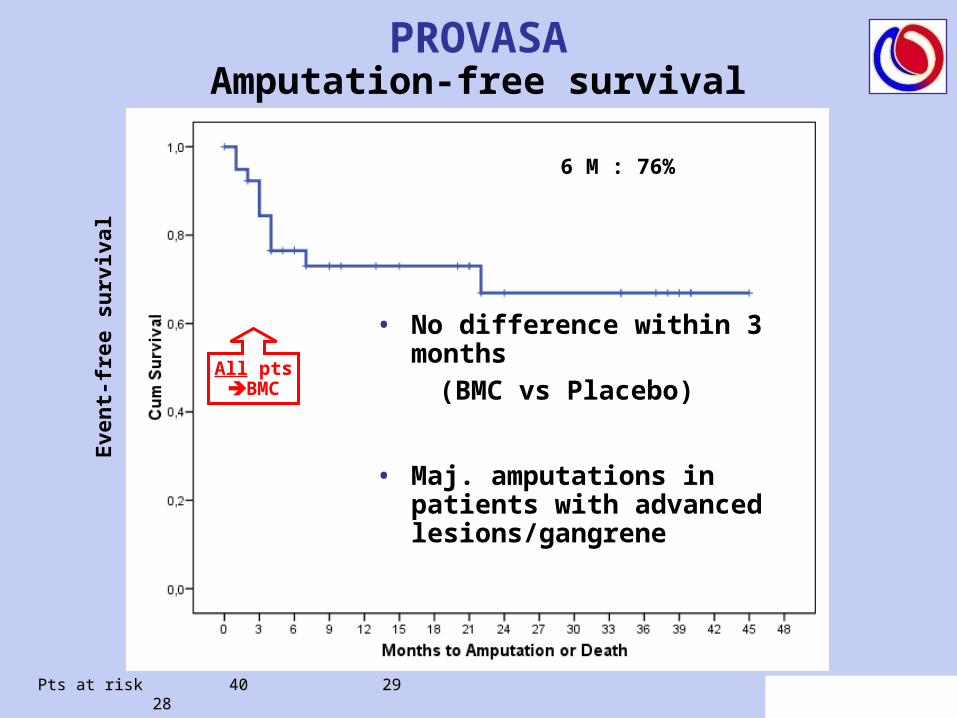
PROVASAAmputation-free survival
Pts at risk 40 29 28 Pts at risk 40 29 28
All ptsBMC
• No difference within 3 months
(BMC vs Placebo)
• Maj. amputations in patients with advanced lesions/gangrene
Eve
nt-
free
su
rviv
al
6 M : 76%
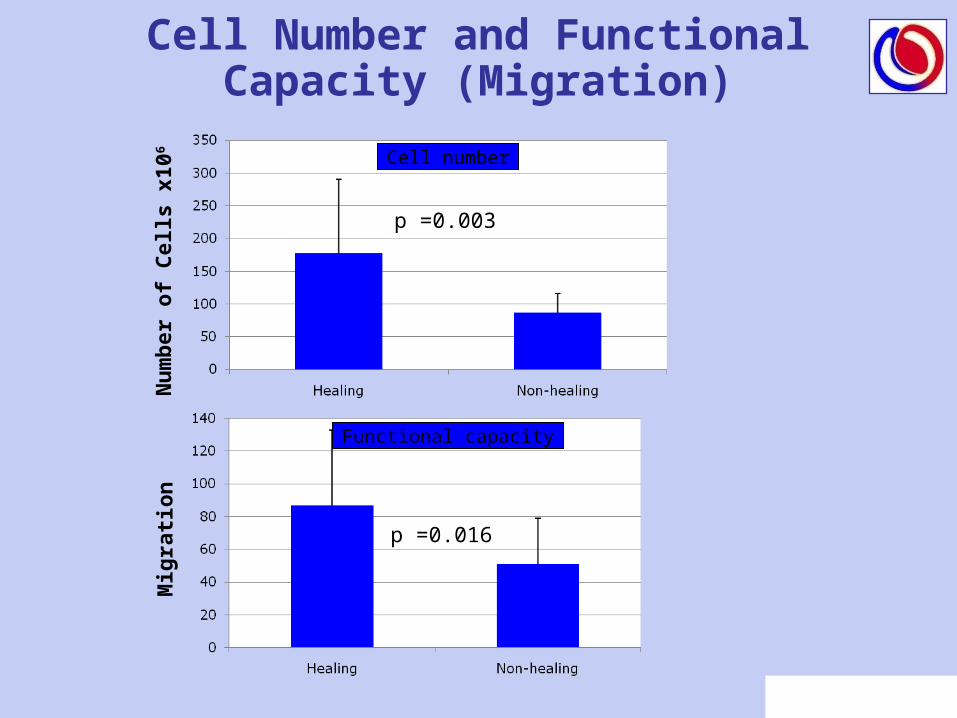
Cell Number and Functional Capacity (Migration)
Cell number
Functional capacity
Mig
rati
on
Nu
mb
er o
f C
ells
x10
6
p =0.016
p =0.003

Factor P Exp (B)Hazard 95% CI
Age 0.7 1.01 1.01 - 1.07
Ulcer size 0.5 0.9 0.65 - 1.25
EF 0.08 1.09 0.99 - 1.20
Pain at baseline 0.12 0.82 0.65 - 1.05
Creatinine < 1.4 mg/dl 0.11 6.13 0.66 - 56
Buerger’s disease (TAO) 0.8 1.26 0.17 - 9.0
Cell number 0.003 1.02 1.008 - 1.038
Repeated BM-MNC (≥ 2 applications)
0.018 6.17 1.35 - 28
Cell function 0.049 0.99 0.98 – 1.00
Multivariate AnalysisClinical Improvement (Healing or Pain Reduction)Clinical Improvement (Healing or Pain Reduction)
Repeated BM-MNC administration as well as the number and functionality of administered BM-MNC were significant independent predictors for clinical improvement

PROVASAConclusions (1)
• Intraarterial administration of BM-MNC significantly promotes ulcer healing and reduces rest pain until 3 months versus Placebo
• Successful ulcer healing associated with improved limb salvage requires repeated administration of functionally competent BM-MNC
• Patients with thrombangiitis obliterans generally responded well, critically ill patients with extensive gangrene and impending amputation did not derive any benefit.

PROVASAConclusions (2)
• Thus, large scale randomized trials are warranted to assess the clinical effect of repeated BM-MNC administration in patients with critical limb ischemia with stable ulcers and/or rest pain.
• Complete ulcer healing occurred at a mean of 10.9 months after BM-MNC administration
• To assess potential clinical benefits of cell therapy in patients with critical limb ischemia, a follow-up period of at least 18 months will be required.
FrankfurtKardiologie:
D. Walter (Coordinator)A. Zeiher (PI)S. Dimmeler
Angiologie:
A. Kopalla E. Lindhoff-Last
Radiologie:
J. Balzer,
Institut für Transfusionsmedizin
BSD Hessen:T. Tonn
Hamburg
H. KrankenbergM. Schlüter
D. Walter (Coordinator)
Bern
C. Kalka
I.Baumgartner
PROVASABack-up slides
Responders
• Younger age • Better ejection fraction • Smaller ulcer size (< 2.3 cm² , p =0.038)• Less rest pain at baseline• Better renal function (creatinine < 1.4 mg/dl) • TAO (all 8 TAO) responders versus 18 of 32 (56%)
atherosclerotic PAOD improved clinically by BM-MNC treatments (P=0.02 TAO vs. PAOD).
• Patients with gangrene (Rutherford 6) did not respond at all.

All BM-MNCRandomized-Start
BM-MNC (n=6)
Placebo (n=10)
TC
O2 (
mm
Hg
)
P=0.52
P=0.17
P=0.14
P=0.032 P=0.018
P=0.058
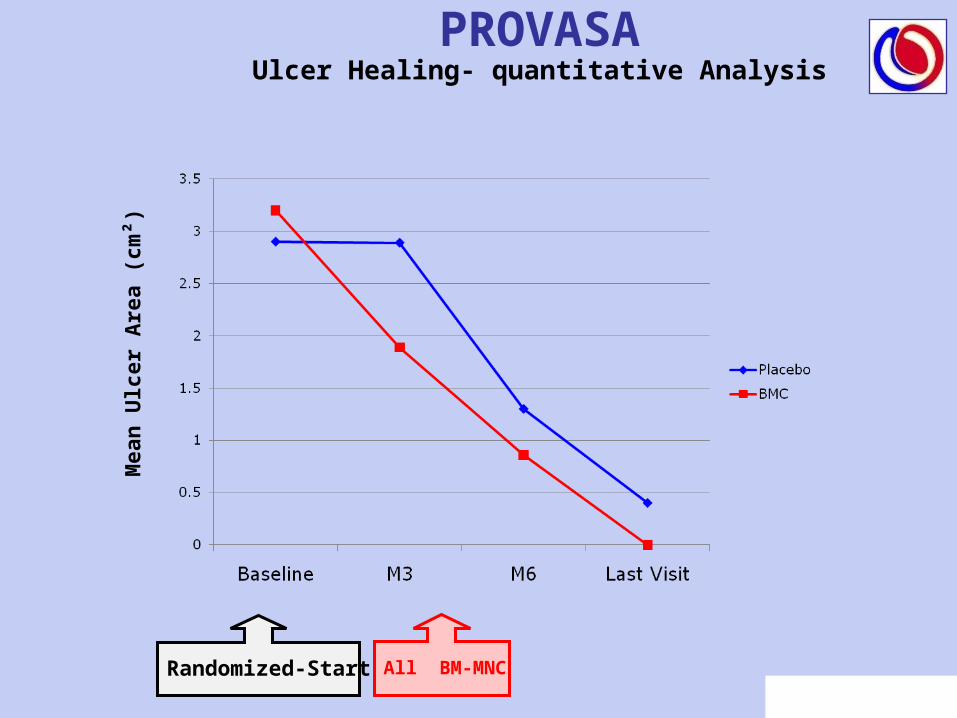
PROVASAUlcer Healing- quantitative Analysis
Mea
n U
lcer
Are
a (c
m²)
All BM-MNCRandomized-Start
Related Documents











