HPB Surgery, 1996, Vol. 9, pp. 61-69 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V. Published in The Netherlands by Harwood Academic Publishers GmbH Printed in Malaysia C Intestinal Endotoxins as o-Factors of Liver InJury in Obstructive Jaundice B. BLENT MENTES, ERTAN TATLICIOLU, GLEN AKYOL,* 3MER ULUOGLU,* NEDIM SULTAN,** ERDAL YILMAZ, MURAT ELEBI,*** FERIT TANERI,* and ZAFER FERAHKI SE *From the Departments of Surgery, Pathology, and **Microbiology, Gazi University Medical School and from the Department of Physiology, Ankara University Medical School, Ankara, Turkey (Received February 24, 1994) The concept of endotoxin-mediated rather than direct liver injury in biliary obsruction was investigated using the experimental rat model of bile duct ligation (BDL) and small bowel bacterial overgrowth (SBBO). Small identical doses of intravenous endotoxin (bacterial LPS) caused a significantly more severe liver injury in rats with BDL, compared with sham-operated rats, suggesting the possible contribution of LPS in this type of liver damage. BDL was then combined with surgically created jejunal self-filling blind loops, which resulted in SBBO. Plasma LPS level increased significantly, and once again a more severe liver injury, determined by liver histology and serum gamma-glutamyl transpeptidase levels, was observed compared with the control group of rats with BDL+self-emptying blind loops.The data presented suggest that small amounts of exogenous LPS and/or the ordinarily innocous amounts of LPS constantly absorbed from the intestinal tract may be critical in the hepatic damage caused by obstruction of the biliary tract. KEY WORDS: Endotoxins; bile duct obstruction extrahepatic; liver injury INTRODUCTION There is considerable evidence suggesting a relation- ship between endotoxins (bacterial lipopolysaccha- rides-LPS), cytokines, macrophage functions, and pathogenesis of liver injury in both acute and chronic liver diseases 1-4. Whereas LPS may directly damage hepatocytes, a large number of LPS mediators origi- nating from the monocyte/macrophage line are thought to work in concert with LPS at the cellular level and cause liver injury in defined circumstances 5- 12. The initial injury in a variety of liver injuries is to the Kupffer cells (KCs), and this injury impairs the ability of the liver to detoxify the ordinarily innocuous amounts of LPS, including those constantly absorbed Address for correspondence: B. Biilent Mentes, M.D. Naci (akir Mah, 2. Sokak No:23/4 06450, Dikmen,Ankara, Turkey. from the gastrointestinal tract 13-15,1,3,4. This KC depres- sion brings about the consequent enhancement of en- dotoxic activity, and even minimal amounts of LPS might precipitate hepatic injury 1,4. Extrahepatic bile duct obstruction and cholestasis have the well-known potential for liver injury, progres- sion to cirrhosis and hepatocellular failure as evidenced by the study of the natural history of progressive cholestatic disorders16-18. Systemic endotoxemia is regu- larly found in those patients who have chronic extrahe- patic bile duct obstruction 19,2. Prolonged biliary ob- struction is associated with a significant depression of the reticuloendothelial system (RES) phagocytic func- tion and significantly higher mortality following endot- oxin challenge21. The depressed function of the RES may allow spillover of even minute amounts of exog- 22 23 enous or gut-originated LPS into the circulation ,. The concept of LPS as a key factor in liver injury has been studied in a number of experimental and clinical 61

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
HPB Surgery, 1996, Vol. 9, pp. 61-69Reprints available directly from the publisherPhotocopying permitted by license only
(C) 1996 OPA (Overseas Publishers Association)Amsterdam B.V. Published in The Netherlands
by Harwood Academic Publishers GmbHPrinted in Malaysia
CIntestinal Endotoxins aso-Factors of Liver InJury in
Obstructive JaundiceB. BLENT MENTES, ERTAN TATLICIOLU, GLEN AKYOL,* 3MERULUOGLU,* NEDIM SULTAN,** ERDAL YILMAZ, MURAT ELEBI,***
FERIT TANERI,* and ZAFER FERAHKISE*From the Departments of Surgery, Pathology, and **Microbiology, Gazi University Medical School and from the
Department of Physiology, Ankara University Medical School, Ankara, Turkey
(Received February 24, 1994)
The concept of endotoxin-mediated rather than direct liver injury in biliary obsruction wasinvestigated using the experimental rat model of bile duct ligation (BDL) and small bowelbacterial overgrowth (SBBO). Small identical doses of intravenous endotoxin (bacterial LPS)caused a significantly more severe liver injury in rats with BDL, compared with sham-operatedrats, suggesting the possible contribution of LPS in this type of liver damage. BDL was thencombined with surgically createdjejunal self-filling blind loops, which resulted in SBBO. PlasmaLPS level increased significantly, and once again a more severe liver injury, determined by liverhistology and serum gamma-glutamyl transpeptidase levels, was observed compared with thecontrol group of rats with BDL+self-emptying blind loops.The data presented suggest thatsmall amounts of exogenous LPS and/or the ordinarily innocous amounts of LPS constantlyabsorbed from the intestinal tract may be critical in the hepatic damage caused by obstructionof the biliary tract.
KEY WORDS: Endotoxins; bile duct obstruction extrahepatic; liver injury
INTRODUCTION
There is considerable evidence suggesting a relation-ship between endotoxins (bacterial lipopolysaccha-rides-LPS), cytokines, macrophage functions, andpathogenesis of liver injury in both acute and chronicliver diseases1-4. Whereas LPS may directly damagehepatocytes, a large number of LPS mediators origi-nating from the monocyte/macrophage line arethought to work in concert with LPS at the cellularlevel and cause liver injury in defined circumstances5-
12. The initial injury in a variety ofliver injuries is to theKupffer cells (KCs), and this injury impairs the abilityof the liver to detoxify the ordinarily innocuousamounts of LPS, including those constantly absorbed
Address for correspondence: B. Biilent Mentes, M.D. Naci (akirMah, 2. Sokak No:23/4 06450, Dikmen,Ankara, Turkey.
from the gastrointestinal tract13-15,1,3,4. This KC depres-sion brings about the consequent enhancement of en-dotoxic activity, and even minimal amounts of LPSmight precipitate hepatic injury1,4.
Extrahepatic bile duct obstruction and cholestasishave the well-known potential for liver injury, progres-sion to cirrhosis and hepatocellular failure as evidencedby the study of the natural history of progressivecholestatic disorders16-18. Systemic endotoxemia is regu-larly found in those patients who have chronic extrahe-patic bile duct obstruction19,2. Prolonged biliary ob-struction is associated with a significant depression ofthe reticuloendothelial system (RES) phagocytic func-tion and significantly higher mortality following endot-oxin challenge21. The depressed function of the RESmay allow spillover of even minute amounts of exog-
22 23enous or gut-originated LPS into the circulation ,.The concept ofLPS as a key factor in liver injury has
been studied in a number of experimental and clinical
61

62 B. BfQLENT MENTES et al.
liver injuries24’6’’4. In spite of the large body of knowl-edge about endotoxemia associated with obstructivejaundice, most of the studies have focused on thesystemic effects ofendotoxemia or extrahepatic mani-festations such as renal failure4,2-22.
In the present study, the effect of a small dose ofexogenously administered LPS on liver injury wasinvestigated, as the first step, in rats with extrahepaticbile duct obstruction. Extrahepatic bile duct obstruc-tion was then combined with jejunal self-filling blindloops (SFBLs) in order to create small bowel bacterialovergrowth (SBBO). The resultant liver injury andplasma a LPS levels were evaluated and comparedwith appropriate controls in order to discuss the pro-posed complementary role ofgut-originated endotox-ins as key factors in liver injury caused by extrahepaticbile duct obstruction.
METHODS
Experimental Design and Surgical Procedures
Male Wistar rats, 12-20 weeks old and weighing200-250 grams(g) were obtained from Gazi Univer-sity Surgical Research Center. Animals were alloca-ted to one of six groups:Group l(n=6): Sham operation (sham for bile duct
ligation).Group 2(n=8): Sham operation and 13 days later
given intravenous (iv)LPS.Group 3(n=8): Bile duct ligation (BDL) for 14 days.Group 4(n=8): BDL for 14 days and iv LPS on the
13th day.Group 5(n=8): BDL + Jejunal self-filling blind loop
(SFBL) for 14 days.Group 6(n=8): BDL + jujunal self-emptying blind
loop (SEBL) for 14 days.
Rats were anesthetised with ketamine hydrochloride,50 milligram (mg)/kilogram (kg) body weight intra-muscularly (im) after an overnight fast. Operationswere performed via an uppermidline incision understrict sterile conditions. BDL consisted ofdissection ofthe supraduodenal portion of the common bile ductand division between 5/0 vycril ligatures. In the shamoperation, the ligature was placed around the com-mon bile duct and then removed.
In groups 5 and 6, BDL was combined with SFBLand SEBL, respectively. A modification ofthe methodof Cameron et al.25 was used and 10 centimeter (cm)jejunal SFBLs were created about 10 cm distal to theligament of Treitz using a side-to-side anastomosis
technique with continuous 8/0 polydiaxanone (PDS)sutures. This experimental model of SFBL has beenpreviously shown to result in SBBO within one weekfollowing surgery26,27. The control group for this modelconsisted of rats with SEBLs, in which the correspond-ing jejunal segments were constructed using the samesurgical techniques, but in an isoperistaltic fashion toempty aborally.
Postoperatively, all rats were kept in a temperature-controlled environment and allowed water and stan-dard laboratory rodent chow ad libitum. 14 days later,all rats were again anaesthetised with ketamine hydro-chloride im. Under strict sterile conditions, laparatomywas performed through the previous midline incision. Asecond set of sterile instruments was used for eachanimal after the skin was traversed with the first set.Peritoneal cultures were taken with a sterile applicatorstick and cardiac blood was a;pirated sterilely. Liverspec.imens from various sites were then obtained forhistology. Last of all, luminal contents ofjejunal loopswere flushed with 10 milliliter (mL) saline and collectedfor anaerobic culture. (See below for technical details).
Endotoxin Challenge
Rats of groups 2 and 4 were challenged with iv LPS onthe 13th postoperative day, that is 24 hours beforesacrifice. Lyophilized and gamma-irradiated LPS fromE. coli 055:B5 (Sigma Chemical Co. St. Louis, Mo) wasgiven through the tail vein following fresh reconstitu-tion with pyrogen-free water and calibration to providemicrogram LPS per gram (g) body weight in mL of
diluent. Rats in groups and 3 received iv injections ofmL pyrogen-free water only.
Quantification ofBacterial Endotoxin in Plasma
An advanced method for optimization of detection ofbacterial LPS in plasma with the Limulus test, describedby Roth et al.28 was used. All glassware was renderedendotoxin-free by washing, with alkaline detergent (E-Toxa-Clean, Sigma), autoclaving for 45 minutes (min),and heating at 190C for 4 hours (h). Endotoxin-freeplasma was obtained from a healthy volunteer. In brief,endotoxin stock solutions (E.coli LPS B, 055:B5) withvarious concentrations were prepared in pyrogen-free0.15 mol/liter (L) NaC1 (Sigma). volume ofeach stocksolution was added to 9 volumes of endotoxin-freeplasma and endotoxin-spiked plasma samples were thusprepared. In order to obtain maximal detection of lowconcentrations of LPS, plasma samples were dilutedfourfold with 0.15 mol/L NaC1 followed by heating at

ENDOTOXINS IN BILIARY OBSTRUCTION 63
60C for 30 min. A 0.2 mL sample of plasma (endo-toxin-free, endotoxin-spiked, or plasma to be tested)was mixed with 0.6 mL 0.15 mol/L NaC1 and incubatedin a cork-stoppered tube at 60C for 30 min. A 0.05 mlsample of this diluted-heated plasma was then incu-bated with 0.05 mL sample of Limulus lysate (E-Toxate, Sigma) for 30 min in a 37C water bath. 0.2 mLof chromogenic substrate (S-2423 AB Kabi, Vitrum,Molndal, Sweden) was then added to each assay tube,and incubated for an additional 10 min at 37C. Reac-tions were stopped by 0.15 mL of 50% acetic acid, andabsorbance was measured at 405 nm in a spectro-photometer. The results were expressed in picrogram(pg)/mL.
Liver Histology
Specimens ofliver were fixed in 10% buffered formalin,then processed for histological examination andstained using hematoxylen and eosin (H&E), periodicacid-Schiff(PAS) with diastase digestion, methyl greenpyronine, Gomoris reticuline, Masson’s trichrome, orphosphothungistic acid hematoxylen (PTAH) in orderto assess hepatic abnormalities including necrosis,hydropic degeneration, regenerative activity, decreas-ing glycogen content of hepatocytes, polymorpho-nuclear cell (PMNC) infiltration and mononuclear cellinfiltration in the portal tracts, pseudoductular prolif-eration, interlobular duct changes, fibroblastic activ-ity, KC abnormalities, PMNC and, mononuclear cellinfiltration in the sinusoids, sinusoidal vascular con-gestion, portal vascular congestion, sinusoidal vascu-lar thrombosis, portal vascular thrombosis, phlebitisof portal and central veins, and arterial wall changes.Each parameter of each rat was graded by two blindedobservers semiquantatively depending on the degree ofthe abnormality: grade 0-absent, grade 1-mild, grade2-moderate, and grade 3-severe. A scoring system simi-lar to that of Lichtman and associates29 was used. Themeans and standard deviations (SD) were calculated,and the parameters were scored from 0 to 4 for eachgroup according to the corresponding mean values ofsham-operated rats. A score of 1 was obtained forexample, when the mean value exceeded the mean +SD derived from the sham-operated rats.
Bacterial Cultures
Peritoneal fluid and cardiac blood samples were imme-diately inoculated on blood agar, EMB agar andprereduced brain-heart infusion (BHI) agar plates. Lu-minal contents ofthejejunal loops or corresponding 10
cm jejunal segments were flushed with 10 mL saline,diluted in thioglycollate broth from 10-1 to 10-1, andinoculated on blood agar and BHI plates. Anaerobicculture plates were kept in anaerobic jars (Oxoid) con-taining gas-generating kit and catalyzer. All specimenswere inoculated at 37C for 72h. Total anaerobic bac-terial colony-forming units (CFU) per mL of luminalcontents were then determined in order to confirm thedevelopment of SBBO in SFBLs within the time limitsofthis study. Luminal contents were not subcultured toidentify the involved anaerobic species.Gamma-glutamyl transpeptidase (GGT) levels weremeasured with a Beckman Astra-8 Enzyme Auto-analyzer in serum obtained by centrifugation of thecardiac blood samples at 4000 revolutions per min for10 min. The results were expressed in U/L.
Statistical Analysis
The results are presented as mean values +SEM. Mann-Whitnney-U test was used for all comparisons, and apvalue of less than 0.05 was considered to represent asignificant difference. Comparisons of the histologicalparameters were performed using Kruskal-Wallis test.
RESULTS
Rats in which complications, such as intraabdominalbleeding, intestinal obstruction, or anastomotic leak-age, developed were excluded from the study. All suchcomplications and deaths occurred within the first 72 hpostoperatively, and never after. When harvestinglaparatomy was performed 14 days later, SFBLs weregrossly dilated and were filled with fecaloid material incontrast with SEBLs.
Bacterial Counts and Plasma LPS Levels
Aerobic and anaerobic cultures of peritoneum andblood were negative in all animals. Luminal bacterialconcentrations and differential counts, as well as
Table 1 Plasma LPS and serum GGT levels of the study groups
LPS(pg/mL) GGT (U/L)
Group SHAM A 32.10 + 9.6 8.33 + 1.6Group 2 SHAM + LPS 8.67 + 1.5Group 3 BDL 142.77 + 20.5 24.86 + 1.9Group 4 BDL + LPS 57.50 + 5.2Group 5 BDL + SFBL 352.63 +_ 115.3 60.29 + 4.1Group 6 BDL + SEBL 86.19 _+ 15.7 21.67 + 2.1

64 B. BLENT MENTES et al.
bacterial cultures ofliver, spleen and mesenteric lymphnodes, had been well-documented in previous investi-gations, and SFBLs had been shown to result in SBBOwith week following surgery26,27,29. In accordance, ratswith SFBLs were shown to have 108-9 colony-formingunits (CFU) of anaerobic bacteria per mL of the loopcontent. SEBLs contained approximately 103-4 bacte-ria/mL.
The numerical data regarding plasma LPS andserum GGT levels are shown in Table 1. BDL resultedin significantly elevated plasma LPS concentrationscompared with those of the sham-operated group(p < 0.05). When BDL was combined with SEBL,plasma LPS levels were similar to those of BDL rats(p > 0.05). On the contrary, plasma LPS levels of ratswith BDL combined with SFBL were significantlyhigher than those of BDL rats (p < 0.05), indicatingthat SBBO in animals with BDL resulted in even higherlevels of endotoxemia. Groups 2 and 4 were not testedfor plasma LPS concentrations because of the exist-ence of recent exogenous LPS administration.
Histological and Biochemical Evidence
ofLiver Injury
Sham-operated rats (group 1) had random, small mono-nuclear aggregates, minimal round cell infiltrationaround bile ducts, and mild congestion affecting bothportal and central veins (data not shown). The scoresobtained for each involved parameter according to thecorresponding mean value ofthe sham-operated groupare given in Table 2. Although simply suggestive of the
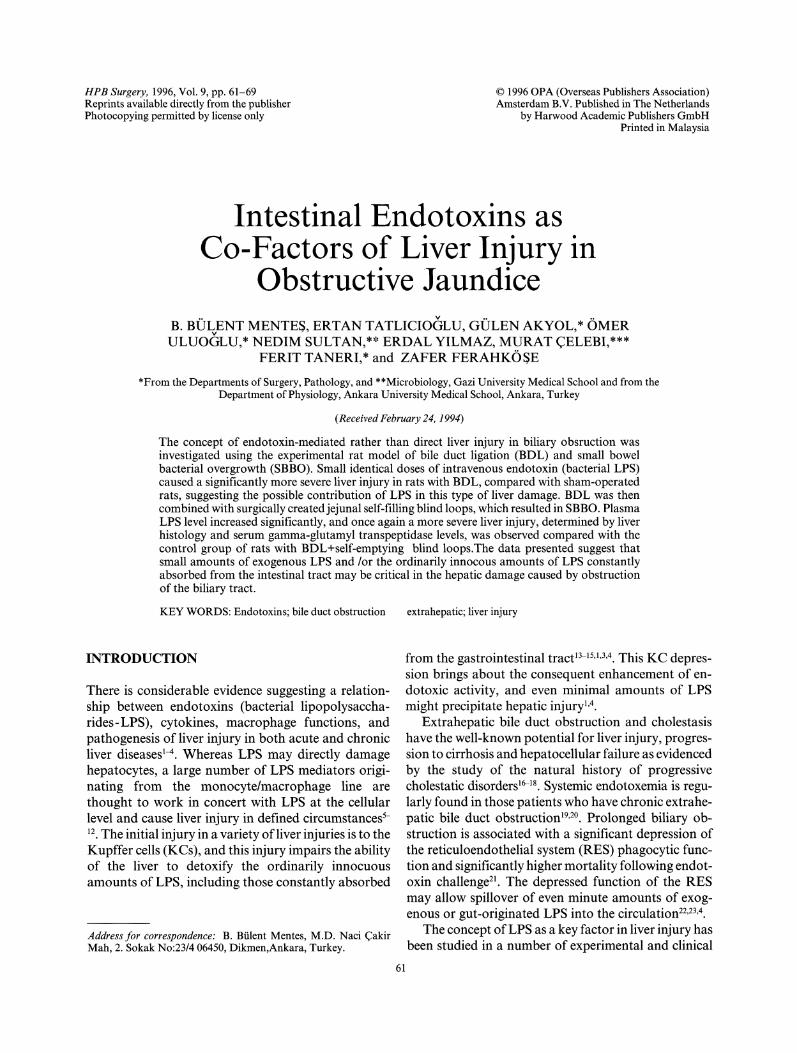
resultant degree of liver injury (Figure 1), the totalscores should be interpreted cautiously because eachparameter has a different pathological meaning and de-serves special discussion, rather than simple cumulation.
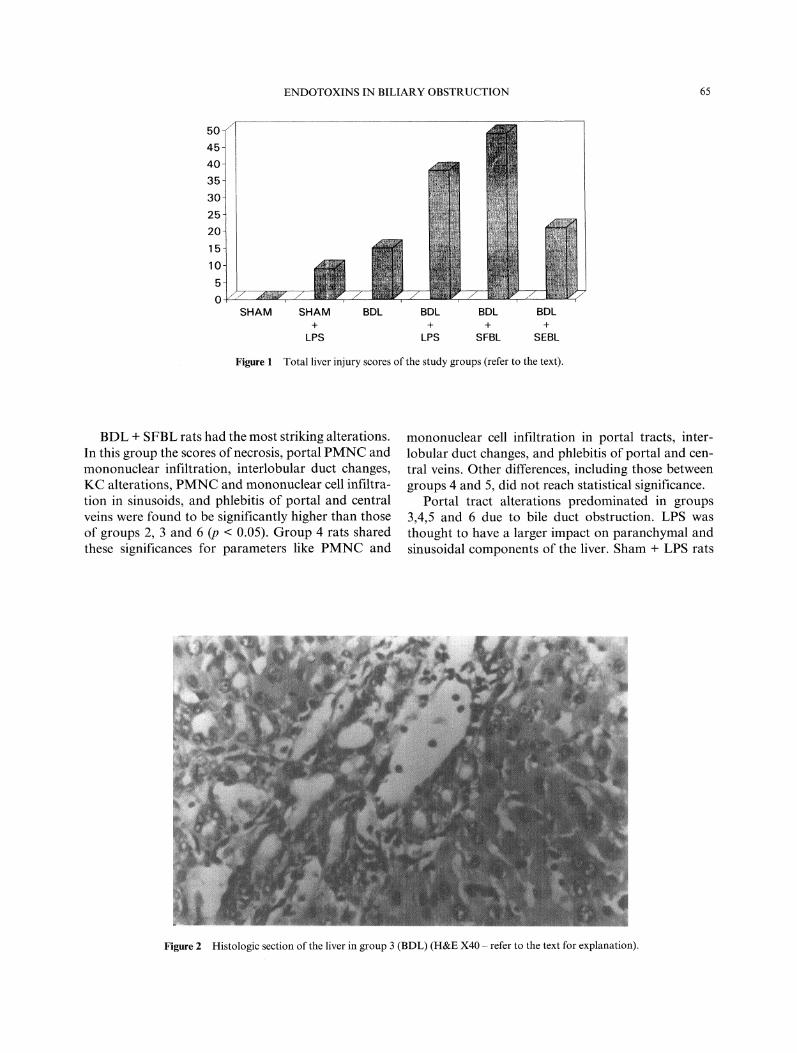
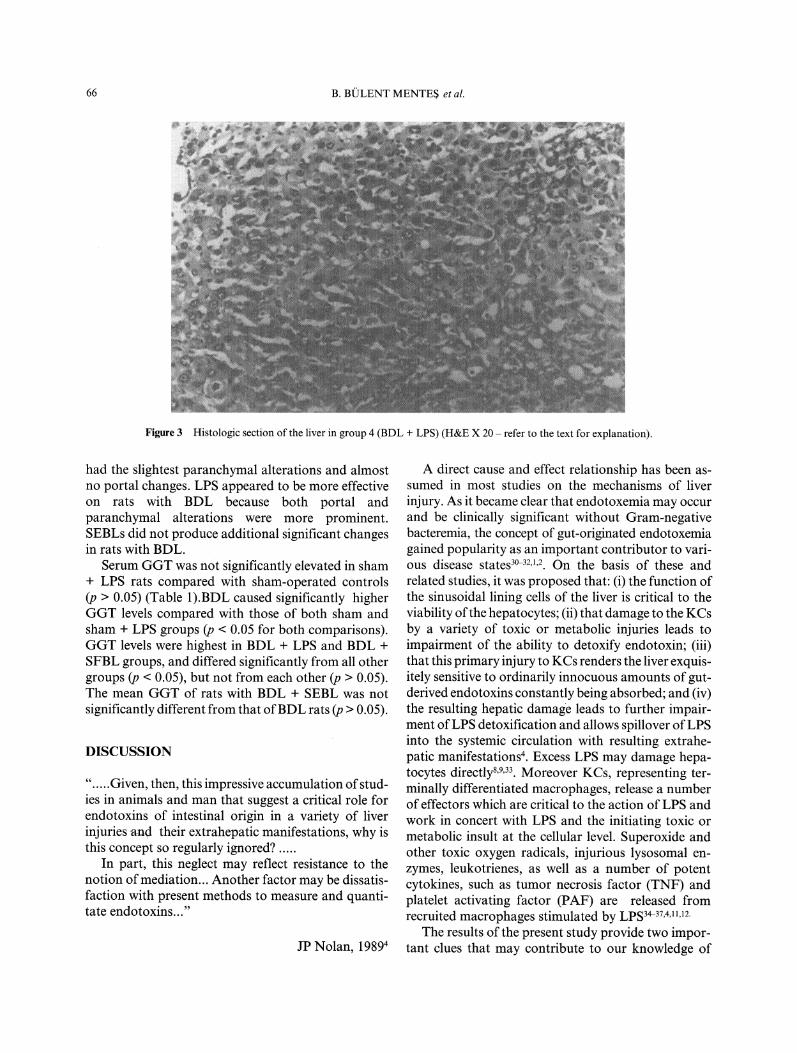
Sham + LPS rats (group 2) had rounded KCs, mildPMNC infiltration in sinusoids, and mild mononuclearcell infiltration in portal tracts and sinusoids. In group3 (BDL), mild hepatocyte necrosis with eosinophilicdegeneration, enlarged portal tracts, pseudoductularproliferation, denser mononuclear infiltration, and por-tal vascular congestion were noticed (Figure 2). WhenBDL was combined with iv LPS (group 4), more severeportal and paranchymal alterations were noted (Figure3). Pseudoductular proliferation was more prominent,and tended to make spurs into the paranchyme. Fibro-blastic activity appeared to accompany this prolifera-tion. Inflammation of duct epithelia and portal veinswere apparent. KCs appeared more rounded with atendency to bulge into sinusoids, and they were stronglyPAS (+) after diastase digestion. Sinusoidal PMNCand mononuclear cell infiltration was dense. Focalparanchymal necrosis and PMNC were aggregatesextensive. Rarely, PTAH (+) eosinophilic materialwith linear configuration was seen and considered tobe fibrin. Central vein inflammation was seen in somerats. Group 5 (BDL + SFBL) also had more severealterations (Figure 4). Group 6 (BDL + SEBL) hadportal alterations predominantly. The inflammation inportal tracts were not as striking as it was in group 5.Mild paranchymal necrosis, PMNC infiltration, KCprominence, sinusoidal inflammation, and occasionalplatelet thrombosis were seen in most of the rats.
Table 2 The histological scores obtained for the involved parameters according to the corresponding mean values of the sham-operatedgroup
PARAMETERS SHAM+LPS BDL BDL+LPS BDL+SFBL BDL+SEBL
necrosis 0 2 3hydropic degeneration 2 2regenerative activity 0 2 2decreasing glycogen content 2portal PMNC infiltration 0 3 4portal mononuclear cell infiltration 2 4 4 2pseudoductular proliferation 0 2 3interlobular duct changes 0 3 4fibroblastic activity 0 2 3 2KC abnormalities 3 4 2sinusoidal PMNC infiltration 0 3 4sinusoidal mononuclear cell infiltration 3 4sinusoidal congestion 2portal vascular congestion 0 2sinusoidal thrombosis 0 2portal vascular thrombosis 0 0 0portal-central venous phlebitis 4 4arterial wall changes 0 0 0 0TOTAL 9 15 38 49 21
ENDOTOXINS IN BILIARY OBSTRUCTION 65
40
35
30
25
20
15
10
5
0SHAM SHAM BDL BDL BDL BDL
+ + + +LPS LPS SFBL SEBL
Figure 1 Total liver injury scores of the study groups (refer to the text).
BDL + SFBL rats had the most striking alterations.In this group the scores of necrosis, portal PMNC andmononuclear infiltration, interlobular duct changes,KC alterations, PMNC and mononuclear cell infiltra-tion in sinusoids, and phlebitis of portal and centralveins were found to be significantly higher than thoseof groups 2, 3 and 6 (p < 0.05). Group 4 rats sharedthese significances for parameters like PMNC and
mononuclear cell infiltration in portal tracts, inter-lobular duct changes, and phlebitis of portal and cen-tral veins. Other differences, including those betweengroups 4 and 5, did not reach statistical significance.
Portal tract alterations predominated in groups3,4,5 and 6 due to bile duct obstruction. LPS wasthought to have a larger impact on paranchymal andsinusoidal components of the liver. Sham + LPS rats
Figure 2 Histologic section of the liver in group 3 (BDL) (H&E X40 refer to the text for explanation).
66 B. BLENT MENTES et al.
Figure 3 Histologic section of the liver in group 4 (BDL + LPS) (H&E X 20 refer to the text for explanation).
had the slightest paranchymal alterations and almostno portal changes. LPS appeared to be more effectiveon rats with BDL because both portal andparanchymal alterations were more prominent.SEBLs did not produce additional significant changesin rats with BDL.
Serum GGT was not significantly elevated in sham+ LPS rats compared with sham-operated controls(p > 0.05) (Table 1).BDL caused significantly higherGGT levels compared with those of both sham andsham + LPS groups (p < 0.05 for bothcomparisons).GGT levels were highest in BDL + LPS and BDL +SFBL groups, and differed significantly from all othergroups (p < 0.05), but not from each other (p > 0.05).The mean GGT of rats with BDL + SEBL was notsignificantly different from that ofBDL rats (p > 0.05).
DISCUSSION
". Given, then, this impressive accumulation ofstud-ies in animals and man that suggest a critical role forendotoxins of intestinal origin in a variety of liverinjuries and, their extrahepatic manifestations, why isthis concept so regularly ignored?
In part, this neglect may reflect resistance to thenotion of mediation... Another factor may be dissatis-faction with present methods to measure and quanti-tate endotoxins..."
JP Nolan, 19894
A direct cause and effect relationship has been as-sumed in most studies on the mechanisms of liverinjury. As it became clear that endotoxemia may occurand be clinically significant without Gram-negativebacteremia, the concept of gut-originated endotoxemiagained popularity as an important contributor to vari-ous disease states3-32,1,-. On the basis of these andrelated studies, it was proposed that: (i) the function ofthe sinusoidal lining cells of the liver is critical to theviability ofthe hepatocytes; (ii) that damage to the KCsby a variety of toxic or metabolic injuries leads toimpairment of the. ability to detoxify endotoxin; (iii)that this primary injury to KCs renders the liver exquis-itely sensitive to ordinarily innocuous amounts of gut-derived endotoxins constantly being absorbed; and (iv)the resulting hepatic damage leads to further impair-ment ofLPS detoxification and allows spillover ofLPSinto the systemic circulation with resulting extrahe-patic manifestations4. Excess LPS may damage hepa-tocytes directly8,9,33. Moreover KCs, representing ter-minally differentiated macrophages, release a numberof effectors which are critical to the action of LPS andwork in concert with LPS and the initiating toxic ormetabolic insult at the cellular level. Superoxide andother toxic oxygen radicals, injurious lysosomal en-zymes, leukotrienes, as well as a number of potentcytokines, such as tumor necrosis factor (TNF) andplatelet activating factor (PAF) are released fromrecruited macrophages stimulated by LPS34-37,4,11,12.
The results of the present study provide two impor-tant clues that may contribute to our knowledge of
ENDOTOXINS IN BILIARY OBSTRUCTION 67
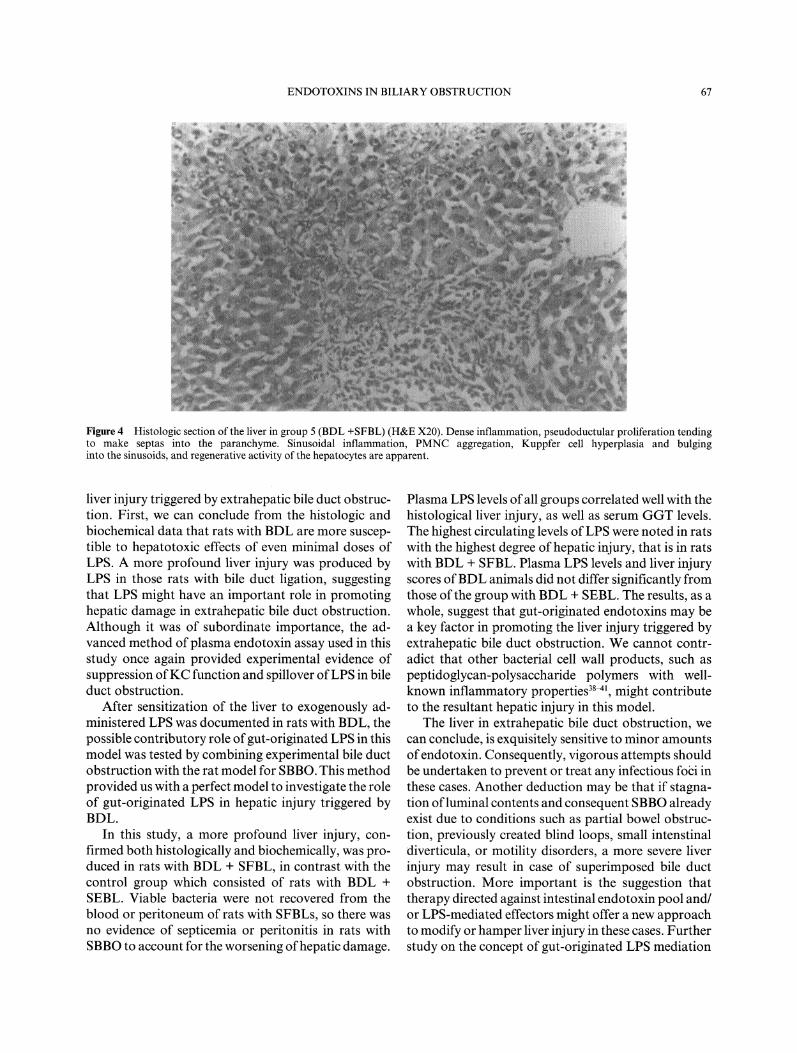
Figure 4 Histologic section of the liver in group 5 (BDL +SFBL) (H&E X20). Dense inflammation, pseudoductular proliferation tendingto make septas into the paranchyme. Sinusoidal inflammation, PMNC aggregation, Kuppfer cell hyperplasia and bulginginto the sinusoids, and regenerative activity of the hepatocytes are apparent.
liver injury triggered by extrahepatic bile duct obstruc- Plasma LPS levels of all groups correlated well with thetion. First, we can conclude from the histologic and histological liver injury, as well as serum GGT levels.biochemical data that rats with BDL are more suscep- The highest circulating levels ofLPS were noted in ratstible to hepatotoxic effects of even minimal doses of with the highest degree of hepatic injury, that is in ratsLPS. A more profound liver injury was produced byLPS in those rats with bile duct ligation, suggestingthat LPS might have an important role in promotinghepatic damage in extrahepatic bile duct obstruction.Although it was of subordinate importance, the ad-vanced method ofplasma endotoxin assay used in thisstudy once again provided experimental evidence ofsuppression ofKC function and spillover ofLPS in bileduct obstruction.
After sensitization of the liver to exogenously ad-ministered LPS was documented in rats with BDL, thepossible contributory role ofgut-originated LPS in thismodel was tested by combining experimental bile ductobstruction with the rat model for SBBO. This methodprovided us with a perfect model to investigate the roleof gut-originated LPS in hepatic injury triggered byBDL.
In this study, a more profound liver injury, con-firmed both histologically and biochemically, was pro-duced in rats with BDL + SFBL, in contrast with thecontrol group which consisted of rats with BDL +SEBL. Viable bacteria were not recovered from theblood or peritoneum of rats with SFBLs, so there wasno evidence of septicemia or peritonitis in rats withSBBO to account for the worsening ofhepatic damage.
with BDL + SFBL. Plasma LPS levels and liver injuryscores ofBDL animals did not differ significantly fromthose ofthe group with BDL + SEBL. The results, as awhole, suggest that gut-originated endotoxins may bea key factor in promoting the liver injury triggered byextrahepatic bile duct obstruction. We cannot contr-adict that other bacterial cell wall products, such aspeptidoglycan-polysaccharide polymers with well-known inflammatory properties3-41, might contributeto the resultant hepatic injury in this model.
The liver in extrahepatic bile duct obstruction, wecan conclude, is exquisitely sensitive to minor amountsofendotoxin. Consequently, vigorous attempts shouldbe undertaken to prevent or treat any infectious foizi inthese cases. Another deduction may be that if stagna-tion ofluminal contents and consequent SBBO alreadyexist due to conditions such as partial bowel obstruc-tion, previously created blind loops, small intenstinaldiverticula, or motility disorders, a more severe liverinjury may result in case of superimposed bile ductobstruction. More important is the suggestion thattherapy directed against intestinal endotoxin pool and/or LPS-mediated effectors might offer a new approachto modify or hamper liver injury in these cases. Furtherstudy on the concept of gut-originated LPS mediation
68 B. BILENT MENTES et al.
ofhepatic injury is required to elucidate the responsiblemechanisms and the involved LPS-mediated effectorsfor a better understanding of hepatic injury associatedwith bile duct obstruction.
ACKNOWLEDGEMENTS
The study was presented at the 1st European Congress of WordAssociation of Hepato-Pancreato-Biliary Surgery, 8-11 June 1993,Paris, France.The study received support for suture materials from Ethicon Lim-ited, International Division, Edinburgh, UK.
REFERENCES
1. Bhagwandeen, B.S., Apte, M., Manwarring, L., Dickeson, J.(1987) Endotoxin induced hepatic necrosis in rats on an alcoholdiet. Journal ofPathlogy, 15, 7-53.
2. van Deventer, S.J.H., ten Cate, J.W., Tytgat, G.N.J. (1988)Intestinal endotoxemia- clinical significance. Gastoroenterology,94, 825-831.
3. Nolan, J.P., Camara, D.S. (1989) Intestinal endotoxins as co-factors in liver injury. Immunological Investigation, 18(1-4),325-337.
4. Nolan, J.P. (1989) Intestinal endotoxins as mediators of liverinjury- an idea whose time has come again. Hepatology, 10(5),887-891.
5. Utili, R., Abernathy, C.O., Zimmerman, H.J. (1976) Cholestaticeffects of Escherichia coli endotoxin on the isolated perfused ratliver. Gastroenterology, 70, 248-253
6. Ferluga, J., Allison, A.C. (1978) Role of mononuclear infiltrat-ing cells in pathogenesis of hepatitis. Lancet, ii 610-611.
7. Bradfield, J.W.B., Wells, M. (1978) Liver disease caused bylysosomal enzymes released from Kupffer cells. Lancet, ii 836.
8. McGivney, A., Bradley, S.G. (1979) Action of bacterial endot-oxin and lipid A on mitochondrial enzyme activities of cells inculture and subcellular fractions. Infection and Immunity, 25664-671.
9. Pagani, R., Portoles, M.T., Diza-Laviada, I., Municio, A.M.(1988) Morphological damage induced by E. coli lipopoly-saccharide in cultured hepatocytes: Iocalization and bindingproperties. British Journal ofExperimental Pathology, 69, 537-549.
10. Arthur, M.J.P., Kowalski-Saunders, P., Wright, R. (1988) Effectof endotoxin on release of reactive oxygen intermediates by rathepatic macrophages.
11. Tiegs, G., Wendel, A. (1988) Leukotriene-mediated liver injury.Biochemical Pharmacology, 37, 2569-2573.
12. Thiele, D. (1989) Tumor necrosis factor, the acute phase responseand the pathogenesis of alcoholic liver disease. Hepatology, 9,497-499.
13. Nolan, J.P. (1975) The role ofendotoxin in liver injury. Gastroen-terology, 69, 1346-1356.
14. Nolan, J.P. (1981) Endotoxin, reticuloendothelial function andliver injury. Hepatology, 1,458-461.
15. Mills, L.R., Scheuer P.J.(1985) Hepatic sinusoidal macrophagesin alcoholic liver disease. Journal ofPathology, 147, 127-132.
16. Cameron, G.R., Hasan, S.M. (1958) Disturbance andstructure and function in the liver as the results ofbiliary obstruc-tion. J Pathology and Bacteriology, 75, 333-349.
17. Dickson, E.R., Grambsch, P.M., Fleming, T.R., Fisher, L.D.,Langworthy, A. (1989) Prognosis in primary biliary cirrhosis:model for decision making. Hepatology, 10, 1-7.
18. Wiesner, R.H., Grambsch, P.M., Dickson, E.R., Ludwig, J.,MacCarty, R.L., Hunter, E.B., Fleming T.R., Fisher, L.D., Bea-ver, S.J., LaRusso, N.F. (1989) Primary sclerosing cholangitis:natural history, prognostic factors and survival analysis.Hepatology, 10, 430-436.
19. Pain, J.A., Bailey, M.E. (1987) Measurement of operativeplasma endotoxin livels injaundiced and non-jaundiced patients.European Surgical Reseach, 19, 207-216.
20. Wait, R.B., Kahng, K.U. (1989) Renal failure complicatingobstructivejaundice. American Journal ofSurgery, 157, 256-263.
21. Holman, J.M. Jr, Rikkers, L.F. (1982) Biliary obstruction andhost defense failure. Journal ofSurgical Research, 32, 208-213.
22. Katz, S., Grosfeld, J.L., Gross, K., Plager, D.A., Ross, D.,Rosenthal, R.S., Hull, M., Weber, T.R. (1984) Impaired bacte-rial clearance and trapping in obstructive jaundice. Annals ofSurgery, 199, 14-20.
23. Pain, J.A., Bailey, M.E. (1986) Experimental and clinical studyof tactulose in obstructive jaundice. British Journal of Surgery,73, 775-778.
24. Nolan. J.P., Leibowitz, A.I. (1978) Endotoxin and the liver III.Modification of acute carbon tetrachloride injury by polymixinB an antiendotoxin. Gastroenterology 75, 445-449.
25. Cameron, D.G., Watson, G.M., Witts, L.J. (1949) The experi-mental production of macrocytic anemia by operations on theintestinal tract. Blood, 4, 803-815.
26. King, C.E., Toskes. P.P. (1981) Protein-loosing enteropathy inthe human and experimental rat blind loop syndrome. Gastroen-terology, 80, 504-509.
27. Lichtman, S.N., Shermann, P., Forstner, G. (1986) Productionof secretory lgA in rat self filling blind loops: local slgA immuneresponse to luminal bacterial flora. Gastroenterology, 91, 1495-1502.
28. Roth, R.I., Levin, F.C., Levin, J. (1990) Optimization of detec-tion of bacterial endotoxin in plasma with the Limulustest. Journal of Laboratory and Clinical Medicine, 116, 153-161.
29. Lichtman, S.N., Sartor, R.B., Keku, J., Schwab, J.H. (1990)Hepatic inflammation in rats with experimental small bowelbacterial overgrowth. Gastroenterology, 98, 414-423.
30. Broitman, S.A., Gottlieb, L.S., Zamcheck, M. (1964) Influenceof neomycin and ingested endotoxin in the pathogenesis of cho-line deficiency cirrhosis in the adult rat. Journal ofExperimentalMedicine, 119, 633-641.
31. Hyland, G., Stein, T., Wise, L. (1977) Abnormalities of liverfunction following extensive jejunoileal bypass and resection inrats. Surgery, 81,578--582.
32. Editorial Lancet (1982) Endotoxin and Cirrhosis.Lancet, 1, 318-319.
33. Pagani, R., Portoles, M.T., Bosch, M.A., Diaz-Lavida, I.,Municio, A.M. (1987) Direct and mediated Escherichia colilipopolysaccharide action in primary hepatocyte cultures. Euro-pean Journal of Cell Biology, 43, 243-246.
34. Arthur, M.J.P., Kowalski-Saunders, P., Wright, R. (1986)Corynobacterium parvum- elicited hepatic macrophages dem-onstrate enhanced respiratory burst activity compared with resi-dent Kupffer cell in the rat. Gastroenterology, 91, 174-181.
35. Arthur, M.J.P., Kowalski-Saunders, P., Wright, R. (1988)Effect of endotoxin on release of reactive oxygen inter-mediates by rat hepatic macrophages. Gastroenterology, 95,1588-1594.
36. Beutler, B., Cerami, A. (1987) Cachectin: more than a tumornecrosis factor. New EnglandJournal OfMedicine, 316, 379-385.
37. Caramelo, C., Fernandez-Gallardo, S., Santos, J.C., Inarrea, P.,Sanchez Crespo, M., Lopez-Novoa, J.M., Hernado, L. (1987)Increased levels of platelet activating factor in blood from pa-tients with cirrhosis of the liver. European Journal of ClinicalInvestigation, 17, 7-11.
38. Stimpson, S.A., Schwab, J.H., Janusz, M.J., Anderle, S.K.,Brown, R.R., Cromartie, W.J. (1986) Acute and chronic inflam-mation induced by peptidoglycan structures and polysaccharide

ENDOTOXINS IN BILIARY OBSTRUCTION 69
complexes. In Biological Properties of Peptidoglycan, edited byPH Seidl and KH Schleifer, pp. 273-290. Berlin: de Gruyter
39. Sartor, R.B., Cromartie, W.J., Powell, D.W., Schwab, J.H.(1985) Granulamatous enterocolitis induced in rats by purifiedbacterial cell wall fragments. Gastroenterology, $9, 587-595.
40. Wahl, S.M., Hunt, D.A., Allen, J.B., Wilder, R.L., Paglia, L.,
Hand, A.R. (1986) Bacterial cell wall induced hepatic granulo-mas. Journal ofExperimental Medicine, 163, 884-902.
41. Lichtman, S.N., Keku, J., Schwab, J.H., Sartor, R.B. (1991)Hepatic injury associated with small bowel bacterial overgrowthin rats is prevented by metronidazole and tetracycline. Gastroen-terology, 100, 513-519.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com
Related Documents











