Intestinal Disorders • Gastroenteritis • Irritable bowel syndrome (IBS) • Inflammatory bowel disease (IBD) • Crohn disease • Ulcerative colitis • Appendicitis • Diverticulitis • Intestinal obstruction • Intussusception • Volvulus • Ileus • Hemorrhoids

Intestinal Disorders Gastroenteritis Irritable bowel syndrome (IBS) Inflammatory bowel disease (IBD) Crohn disease Ulcerative colitis Appendicitis Diverticulitis.
Jan 02, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Intestinal Disorders
• Gastroenteritis• Irritable bowel syndrome (IBS)• Inflammatory bowel disease (IBD)
• Crohn disease• Ulcerative colitis
• Appendicitis
• Diverticulitis• Intestinal obstruction
• Intussusception• Volvulus• Ileus• Hemorrhoids

Disorders of the Intestines Infection
Etiology/pathophysiology Invasion of the alimentary canal by
pathogenic microorganisms Most commonly enters through the mouth in
food or water Person-to-person contact Fecal-oral transmission Long-term antibiotic therapy can cause an
overgrowth of the normal intestinal flora (C. difficile)
Disorders of the Intestines Infection (continued)
Clinical manifestations/assessment Diarrhea Rectal urgency Tenesmus Nausea and vomiting Abdominal cramping Fever
Disorders of the Intestines Infection (continued)
Diagnostic tests Stool culture
Medical management/nursing interventions Antibiotics Fluid and electrolyte replacement Kaopectate Pepto-Bismol

Disorders of the Intestines Irritable bowel syndrome
Etiology/pathophysiology Episodes of alteration in bowel function Spastic and uncoordinated muscle
contractions of the colon Clinical manifestations/assessment
Abdominal pain Frequent bowel movements Sense of incomplete evacuation Flatulence, constipation, and/or diarrhea

Disorders of the Intestines Irritable bowel syndrome (continued)
Diagnostic tests History and physical examination
Medical management/nursing interventions Diet and bulking agents Medications
Anticholinergics Milk of Magnesia, fiber, or mineral oil Opioids Antianxiety drugs

Gastrointestinal Surgery
Mechanical vs. Chemical Digestion
The Esophagus & Stomach
The Small Intestines
The Large Intestine
The Rectum
Accessory Organs of Digestion
The Liver, Gallbladder, & Biliary Tract
The Pancreas
The Spleen
Mechanical vs. Chemical Digestion

The Esophagus & Stomach
Anatomy & Physiology
Pathophysiology
Surgical Intervention

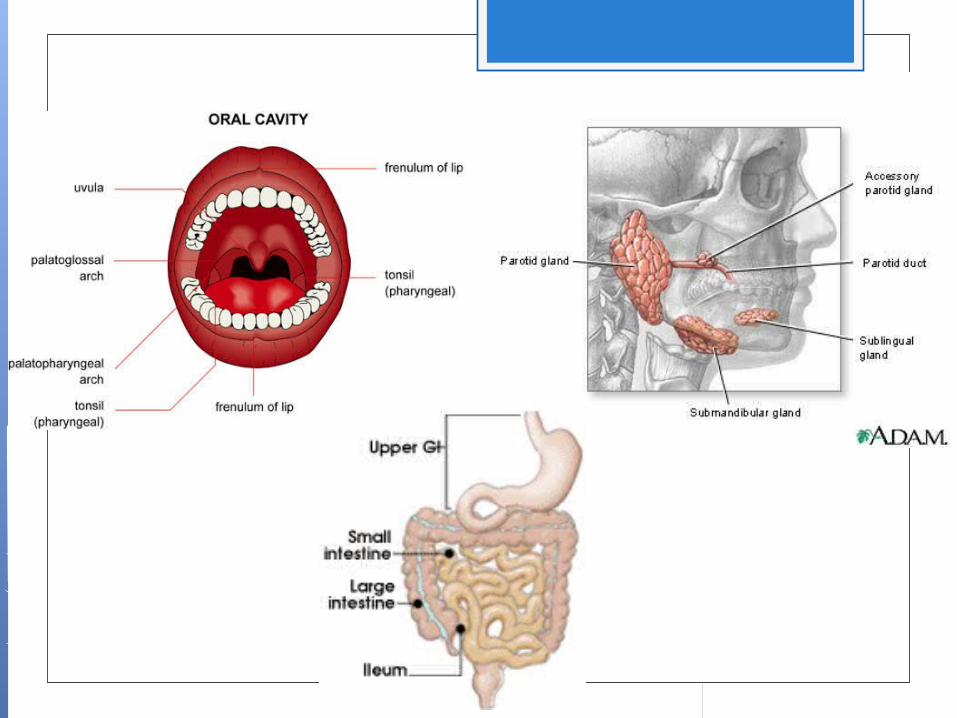
The esophagus is a thin narrow tube that acts like a conveyorbelt carrying food from the pharynx to the stomach. It is about25-30cm in length.
The stomach is like a churning pot, with a very thick layer ofmucosa called Rugae. Unlike the rest of the G.I. tract, the stomachhas three distinct layers of muscle.
Pathophysiology GERD
(gastroesohageal Reflux Disease
Barrett's Esophagus
Hiatal Hernia
Esophageal Varices
Gastric Ulcers
Stomach Carcinoma

GERD (gastroesophageal reflux disease) – is a condition where the acid of the stomach comes in contact with the delicate linings of the esophagus do to decreased tone of the LES (lower esophageal sphincter). GERD is a chronic condition which is initially treated with over the counter antacids, as well as prescription drugs. In many cases surgery may be indicated.

Barrett’s Esophagus – if GERD goes untreated, dysplasia (Barrett’s esophagus) may result. In some cases a Barrett’s esophagus may result in erosion of the esophagus or worse yet carcinoma.

Esophageal Varices – is a dilation and protrusion of the veins within the mucosa lining of the esophagus. Varicosing of these veins is thought to mainly be caused by portal hypertension. They may also develop do to esophageal erosion. The mode of treatment involves the placement of a Blakemore-Sangston tube, sclerotherapy, and in some cases partial esophagectomy.

Gastric Ulcers – A gastric ulcer develops when there are high amounts of HCL (hydrochloric acid) present in the stomach over a long period of time. An ulceration is literally the burning of the mucosa in the G.I. tract. Other factors leading to gastric ulcers are due to excessive alcohol, drug use,and stress. In some cases a Partial Gastrectomy may be indicated.

Surgery of the Stomach and Esophagus Nissen Fundoplication
Esophageal Myotomy
Vagotomy
Partial Gastrectomy
Total Gastrectomy
Gastric Bypass

Nissen Fundoplication – A common way to treat reflux (GERD) is by performing a stomach wrap. Nissen Fundoplication has also been successful at treating hiatal hernia.

Esophageal Myotomy (Heller Procedure) – An esophageal myotomy is indicated for patients who have an motitliy disorders of the esophagus. Achalasia for example is where there is an absence of muscular contractions in the lower half of the esophagus. Surgery is needed to incise the lower esophageal sphincter allowing food to pass into the stomach.

Vagotomy – An indication to perform vagotomy is when the stomach is producing to much hydrochloric acid (HCL). When there is excessive acid secretion within the stomach, an individual as at risk of developing a gastric ulcer. The goal of surgery is to create a partial split in the nerve trunks.

Partial Gastrectomy – Indicated for confined conditions of the stomach like gastric ulcer, a partial gastrectomy focuses on removing only a part of the stomach. Continuity is restored by either reattaching the stomach to the duodenum ( Gastroduodenostomy ) or in some cases where the disease process has effected the duodenum a connection between the stomach and jejunum would be done ( Gastrojejunostomy ).
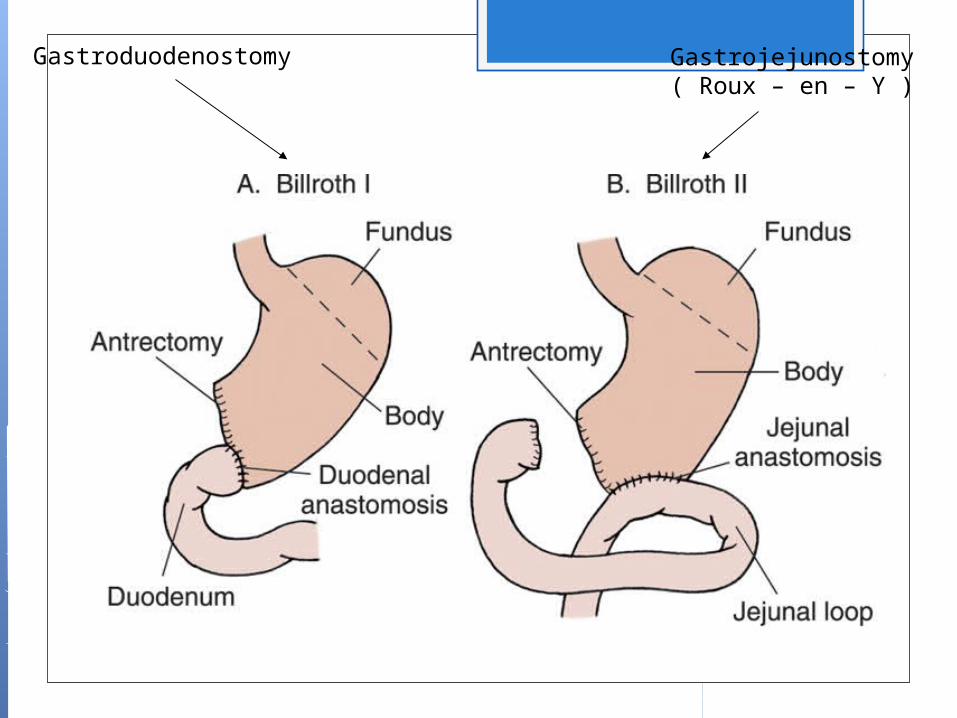
Gastroduodenostomy Gastrojejunostomy( Roux – en – Y )
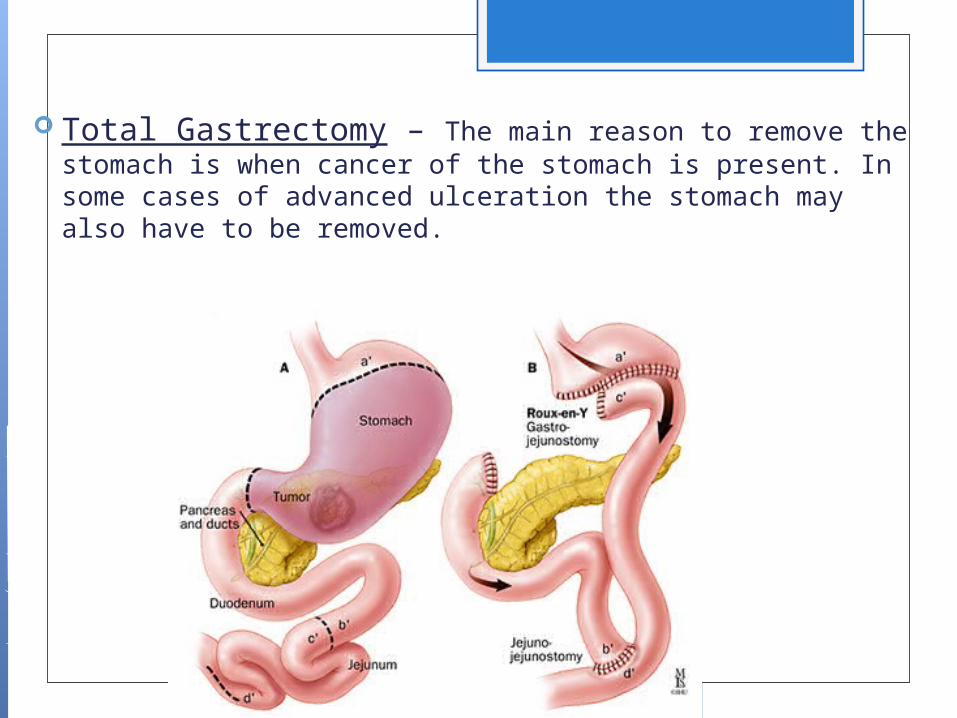
Total Gastrectomy – The main reason to remove the stomach is when cancer of the stomach is present. In some cases of advanced ulceration the stomach may also have to be removed.
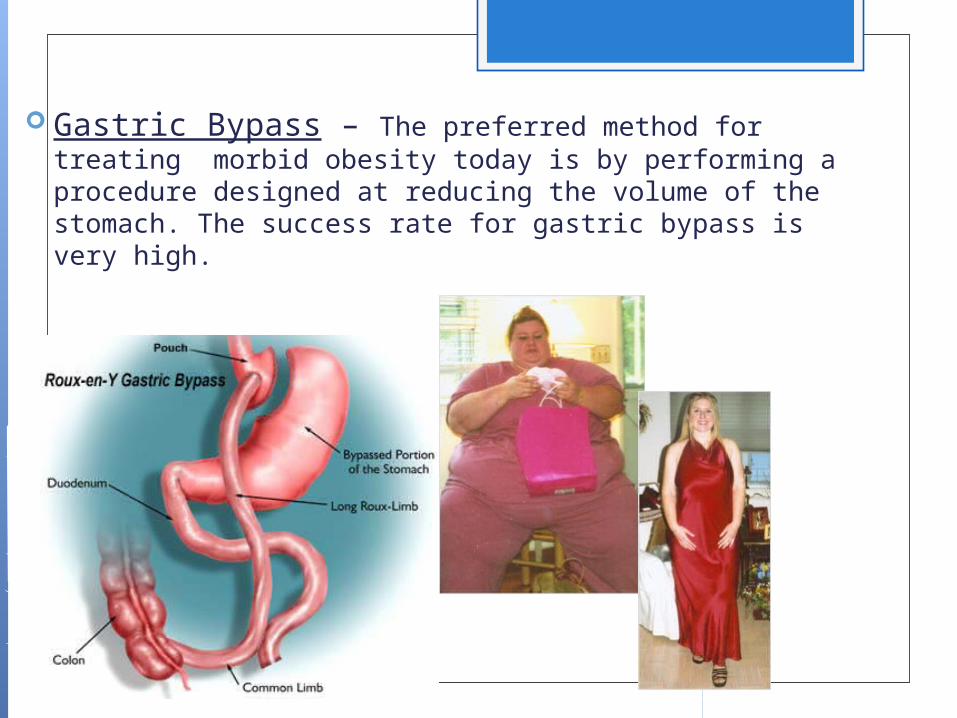
Gastric Bypass – The preferred method for treating morbid obesity today is by performing a procedure designed at reducing the volume of the stomach. The success rate for gastric bypass is very high.
The Intestinal Tract Anatomy & Physiology
Pathophysiology
Surgical Intervention
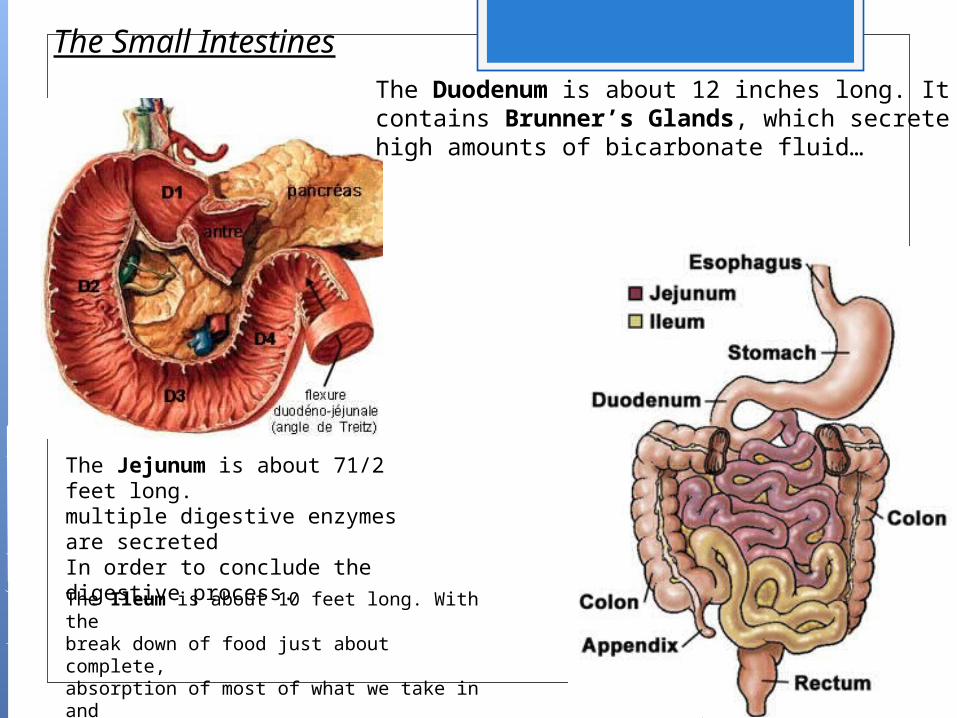
The Duodenum is about 12 inches long. It contains Brunner’s Glands, which secretehigh amounts of bicarbonate fluid…
The Jejunum is about 71/2 feet long.multiple digestive enzymes are secretedIn order to conclude the digestive process.
The Ileum is about 10 feet long. With thebreak down of food just about complete, absorption of most of what we take in anddigest is now absorbed into the blood stream.
The Small Intestines
DISORDERS OF INTESTINES
The Small Intestines
NEC (necrotizing enterocolitis)
Crohn’s Disease
Meckel’s Diverticulum
Intussusception
Volvulus
The Large Intestines
Appendicitis
Diverticulitis
Polyps
Hirschsprung’s Disease
Colon Cancer

Necrotizing Enterocolitis (NEC) – Seen in the newborn, NEC is best defined as a premature gut. When the layers of the intestines are underdeveloped they begin to separate or fall apart. The problem then causes gases to develop inside the linings of the bowel wall. In many cases if caught early, antibiotics are usually effective. In more severe cases the bowel often dies requiring it to be resected.
X-ray showing profoundPneumatosis Intestinalis

Meckel’s Diverticulum – The term diverticulum means abnormal or pouching of bowel. Most meckel’s diverticuli occur in the ileocecal region of the G.I. tract. It is believed that this form of diverticulum is left over from your umbilical cord when you were a fetus. The goal of treatment is surgical resection only when they are symptomatic.
Related Documents