Interventions to Modify Health Care Provider Adherence to Asthma Guidelines: A Systematic Review abstract BACKGROUND AND OBJECTIVE: Health care provider adherence to asthma guidelines is poor. The objective of this study was to assess the effect of interventions to improve health care providers’ adher- ence to asthma guidelines on health care process and clinical out- comes. METHODS: Data sources included Medline, Embase, Cochrane CENTRAL Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature, Educational Resources Information Center, PsycINFO, and Research and Development Resource Base in Continuing Medical Education up to July 2012. Paired investigators independently assessed study eligibility. Investigators abstracted data sequentially and inde- pendently graded the evidence. RESULTS: Sixty-eight eligible studies were classified by intervention: decision support, organizational change, feedback and audit, clinical pharmacy support, education only, quality improvement/pay-for- performance, multicomponent, and information only. Half were ran- domized trials (n = 35). There was moderate evidence for increased prescriptions of controller medications for decision support, feedback and audit, and clinical pharmacy support and low-grade evidence for organizational change and multicomponent interventions. Moderate evidence supports the use of decision support and clinical pharmacy interventions to increase provision of patient self-education/asthma action plans. Moderate evidence supports use of decision support tools to reduce emergency department visits, and low-grade evidence suggests there is no benefit for this outcome with organizational change, education only, and quality improvement/pay-for-performance. CONCLUSIONS: Decision support tools, feedback and audit, and clinical pharmacy support were most likely to improve provider adherence to asthma guidelines, as measured through health care process out- comes. There is a need to evaluate health care provider-targeted interventions with standardized outcomes. Pediatrics 2013;132:517– 534 AUTHORS: Sande O. Okelo, MD, PhD, a Arlene M. Butz, ScD, RN, CRNP, b Ritu Sharma, BSc, c Gregory B. Diette, MD, MHS, b Samantha I. Pitts, MD, MPH, b Tracy M. King, MD, MPH, b Shauna T. Linn, BA, c Manisha Reuben, BS, c Yohalakshmi Chelladurai, MBBS, MPH, c and Karen A. Robinson, PhD b,c a David Geffen School of Medicine and Mattel Children’ s Hospital, University of California at Los Angeles, Los Angeles, California; and b School of Medicine and c Bloomberg School of Public Health Baltimore, Johns Hopkins University, Baltimore, Maryland KEY WORDS asthma, systematic review, guidelines ABBREVIATIONS CI—confidence interval ED—emergency department ICS—inhaled corticosteroids OR—odds ratio RCT—randomized controlled trial SOE—strength of evidence Dr Okelo developed the protocol, completed data collection and data synthesis, drafted the manuscript, and critically reviewed the manuscript; Dr Butz, Ms Sharma, Drs Diette, Pitts, and King, Ms Linn, Ms Reuben, and Dr Chelladurai developed the protocol, completed data collection and data synthesis, and critically reviewed the manuscript; Dr Robinson developed the protocol, completed data collection and data synthesis, drafted the manuscript, and critically reviewed the manuscript; and all authors approved the final manuscript as submitted. www.pediatrics.org/cgi/doi/10.1542/peds.2013-0779 doi:10.1542/peds.2013-0779 Accepted for publication Jun 20, 2013 Address correspondence to Karen A. Robinson, PhD, Medicine, Epidemiology, and Health Policy and Management, Johns Hopkins University, 1830 E. Monument St, Suite 8068, Baltimore, MD 21287. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2013 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: Agency for Healthcare Research and Quality contract number: HHSA 290 2007 10061 I. The authors of this article are responsible for its contents, including any clinical or treatment recommendations. No statement in this article should be construed as an official position of Agency for Healthcare Research and Quality or of the US Department of Health and Human Services. POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose. PEDIATRICS Volume 132, Number 3, September 2013 517 REVIEW ARTICLE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Interventions to Modify Health Care ProviderAdherence to Asthma Guidelines: A Systematic Review
abstractBACKGROUND AND OBJECTIVE: Health care provider adherence toasthma guidelines is poor. The objective of this study was to assessthe effect of interventions to improve health care providers’ adher-ence to asthma guidelines on health care process and clinical out-comes.
METHODS: Data sources included Medline, Embase, Cochrane CENTRALRegister of Controlled Trials, Cumulative Index to Nursing and AlliedHealth Literature, Educational Resources Information Center, PsycINFO,and Research and Development Resource Base in Continuing MedicalEducation up to July 2012. Paired investigators independently assessedstudy eligibility. Investigators abstracted data sequentially and inde-pendently graded the evidence.
RESULTS: Sixty-eight eligible studies were classified by intervention:decision support, organizational change, feedback and audit, clinicalpharmacy support, education only, quality improvement/pay-for-performance, multicomponent, and information only. Half were ran-domized trials (n = 35). There was moderate evidence for increasedprescriptions of controller medications for decision support, feedbackand audit, and clinical pharmacy support and low-grade evidence fororganizational change and multicomponent interventions. Moderateevidence supports the use of decision support and clinical pharmacyinterventions to increase provision of patient self-education/asthmaaction plans. Moderate evidence supports use of decision support toolsto reduce emergency department visits, and low-grade evidence suggeststhere is no benefit for this outcome with organizational change, educationonly, and quality improvement/pay-for-performance.
CONCLUSIONS: Decision support tools, feedback and audit, and clinicalpharmacy support were most likely to improve provider adherence toasthma guidelines, as measured through health care process out-comes. There is a need to evaluate health care provider-targetedinterventions with standardized outcomes. Pediatrics 2013;132:517–534
AUTHORS: Sande O. Okelo, MD, PhD,a Arlene M. Butz, ScD,RN, CRNP,b Ritu Sharma, BSc,c Gregory B. Diette, MD, MHS,b
Samantha I. Pitts, MD, MPH,b Tracy M. King, MD, MPH,b
Shauna T. Linn, BA,c Manisha Reuben, BS,c YohalakshmiChelladurai, MBBS, MPH,c and Karen A. Robinson, PhDb,c
aDavid Geffen School of Medicine and Mattel Children’s Hospital,University of California at Los Angeles, Los Angeles, California;and bSchool of Medicine and cBloomberg School of Public HealthBaltimore, Johns Hopkins University, Baltimore, Maryland
KEY WORDSasthma, systematic review, guidelines
ABBREVIATIONSCI—confidence intervalED—emergency departmentICS—inhaled corticosteroidsOR—odds ratioRCT—randomized controlled trialSOE—strength of evidence
Dr Okelo developed the protocol, completed data collection anddata synthesis, drafted the manuscript, and critically reviewedthe manuscript; Dr Butz, Ms Sharma, Drs Diette, Pitts, and King,Ms Linn, Ms Reuben, and Dr Chelladurai developed the protocol,completed data collection and data synthesis, and criticallyreviewed the manuscript; Dr Robinson developed the protocol,completed data collection and data synthesis, drafted themanuscript, and critically reviewed the manuscript; and allauthors approved the final manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-0779
doi:10.1542/peds.2013-0779
Accepted for publication Jun 20, 2013
Address correspondence to Karen A. Robinson, PhD, Medicine,Epidemiology, and Health Policy and Management, Johns HopkinsUniversity, 1830 E. Monument St, Suite 8068, Baltimore, MD 21287.E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: Agency for Healthcare Research and Quality contractnumber: HHSA 290 2007 10061 I. The authors of this article areresponsible for its contents, including any clinical or treatmentrecommendations. No statement in this article should beconstrued as an official position of Agency for HealthcareResearch and Quality or of the US Department of Health andHuman Services.
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
PEDIATRICS Volume 132, Number 3, September 2013 517
REVIEW ARTICLE

In the United States, an estimated 24.6million people (8.2%) currently haveasthma,1 resulting in .14 millionmissed school days every year, and∼679 000 childhood emergency de-partment (ED) visits.2 Asthma is thethird leading cause of pediatric hospi-talizations.2
A number of guidelines have beenpublished (eg, the National AsthmaEducation and Prevention Program Ex-pert Panel Report 3: Guidelines for theDiagnosis and Management of Asthma,also known as EPR-33), and followingguideline treatment recommendationsimproves clinical outcomes.4–6 How-ever, health care providers do notroutinely follow asthma guideline rec-ommendations,7,8 resulting in substan-dard care and poor health outcomes.9–14
One of the shortcomings of asthmaguidelines is the limited extent to whichhealth careproviders are providedwithtools to followtherecommendedcare.15
There have been provider-targetedinterventions,16–21 but most interven-tions have been patient-focused.22–25
There is no consensus on the mosteffective provider-targeted interven-tions to improve adherence to guide-lines.
The objective of our systematic reviewwas to assess whether interventionstargeting health care providers im-prove adherence to asthma care guide-linesandsubsequently improveoutcomes.We considered health care process out-comes, such as patients receiving appro-priate treatment, and clinical outcomes,such as hospitalizations.
METHODS
We followed the Agency for HealthcareResearch and Quality Methods Guidefor Effectiveness and Comparative Ef-fectiveness Reviews (available at www.effectivehealth care.ahrq.gov/methodsguide.cfm). Our protocol and the fullreport were subject to review.26,27
Data Sources and Searches
We searched Medline, Embase, theCochraneCentral Registerof ControlledTrials, Cumulative Index to Nursing andAllied Health Literature, EducationalResources Information Center, Psy-cINFO, and Research and DevelopmentResource Base in Continuing MedicalEducation through July 2012. No limitswere imposed based on language ordate of publication. We also completedbackward citation searching by usingScopus for each eligible article.
Study Selection
Search results were screened inde-pendently by 2 trained investigators.Disagreements about eligibility wereresolved through discussion. We in-cluded randomizedand nonrandomizedstudies. We excluded studies that wereconducted in inpatientorEDsettingsonly.Potentially eligible articles not in Englishwere identified but not included in thedata abstraction and synthesis. We se-lected the most common outcomes usedinpractice, thosereliedonbyclinicianstoguide decision-making, and those en-dorsedby theNational InstitutesofHealthWorkshop on Asthma Outcomes.28 Thesecritical outcomes are prescription ofasthma controller medicines, provisionof asthma action plan/self-managementeducation, ED visits/hospitalizations, andmissed days of school or work.29
Data Extraction and QualityAssessment
One reviewer completed data abstrac-tion and a second reviewer confirmedaccuracy. Reviewers completed risk ofbias assessment independently. Weresolved disagreements through dis-cussion and, as needed, through con-sensus among the investigators.
Risk of Bias Assessment
We used the Cochrane Collaboration’stool for assessing risk of bias.30 Forpre-post studies, we added relevant
criteria from the Cochrane EffectivePractice and Organization of Care check-list.31 Specifically, the questions ask if theintervention was likely to affect datacollection and if the intervention wasindependent of other changes.
Data Synthesis and Analysis
Heterogeneity in the studies, includingthe measures of outcomes, populationincluded, and specifics of the inter-ventions, precluded quantitative syn-thesis. Qualitative synthesis was basedon these categories of interventions:
1. decision support interventions arehealth information technology–-and/or paper-based interventionsdesigned to support/facilitate healthcare provider decision-making;
2. organizational change interven-tions are designed to change theway in which an organization pro-vides care (eg, having an asthma“champion”);
3. feedback and audit interventionsprovide performance data to healthcare providers about their quality ofcare;
4. clinical pharmacy support inter-ventions target pharmacists’ deliv-ery of care;
5. education only interventions arefocused on educating health careproviders about the content ofguidelines;
6. quality improvement/pay-for-performance interventions are focusedon quality improvement initiativesor pay-for-performance;
7. multicomponent interventions usemore than 1 type of intervention,with no intervention clearly thepredominant intervention;
8. information-only interventions pro-vide only information to health careproviders about guideline recom-mendations (eg, provide a pocketguide to guidelines).
518 OKELO et al
For studies that used.1 intervention,wedetermined the predominant interven-tion. Studies in which this interventionwas unclear were discussed amongteam members to reach consensus.Some studies used multicomponentinterventions with no predominant in-tervention.
We chosemagnitudes of effect felt to beclinically meaningful. Magnitude of ef-fect was considered as small (,10%change or difference), moderate (10%–30% change or difference), and large(.30% change or difference).
We graded the strength of evidence(SOE) for each outcome by using theMethods Guide for Conducting Com-parative Effectiveness Reviews.32 We
considered 4 domains: risk of bias, di-rectness, consistency, and precision.Our judgments were first based on theability to make a conclusion (if not ableto make a conclusion, then “insuffi-cient” was assigned) and then on theconfidence in the conclusion (classifiedas low,moderate, or highwith increasingcertainty). Investigators graded the evi-dence, and this was reviewed by the leadauthor. Any disagreements were dis-cussed with the full team.
For pediatric health care providers, it ispertinent toknowifasthma interventionshave included children because thesepatients often have different naturalhistory, developmental considerations,environmental exposures, advocacy
concerns as minors, and phenotypesthanadults. In termsofproviderbehavior,there is no distinction in guidelines re-garding asthma diagnosis and manage-ment. Thus, for this summary, weconsidered studies of all providers buthave noted those described as beingconducted in a pediatric population.
RESULTS
Results of Literature Searches
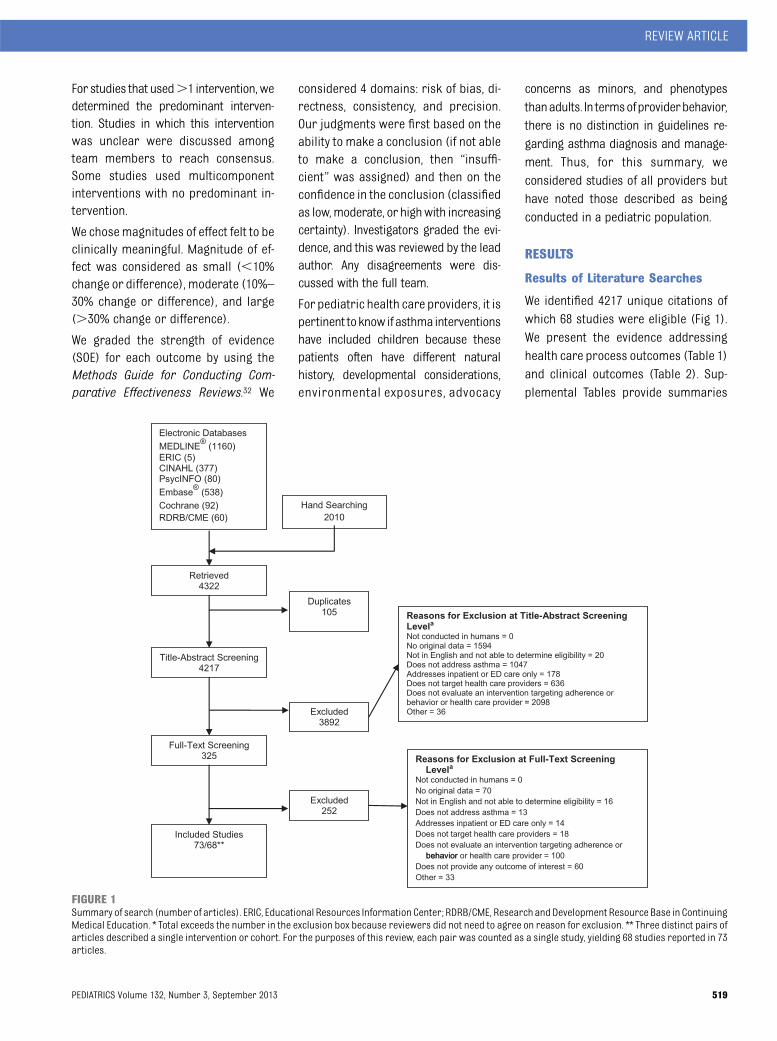
We identified 4217 unique citations ofwhich 68 studies were eligible (Fig 1).We present the evidence addressinghealth care process outcomes (Table 1)and clinical outcomes (Table 2). Sup-plemental Tables provide summaries
FIGURE 1Summary of search (number of articles). ERIC, Educational Resources Information Center; RDRB/CME, ResearchandDevelopment Resource Base in ContinuingMedical Education. * Total exceeds the number in the exclusion box because reviewers did not need to agree on reason for exclusion. ** Three distinct pairs ofarticles described a single intervention or cohort. For the purposes of this review, each pair was counted as a single study, yielding 68 studies reported in 73articles.
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 519
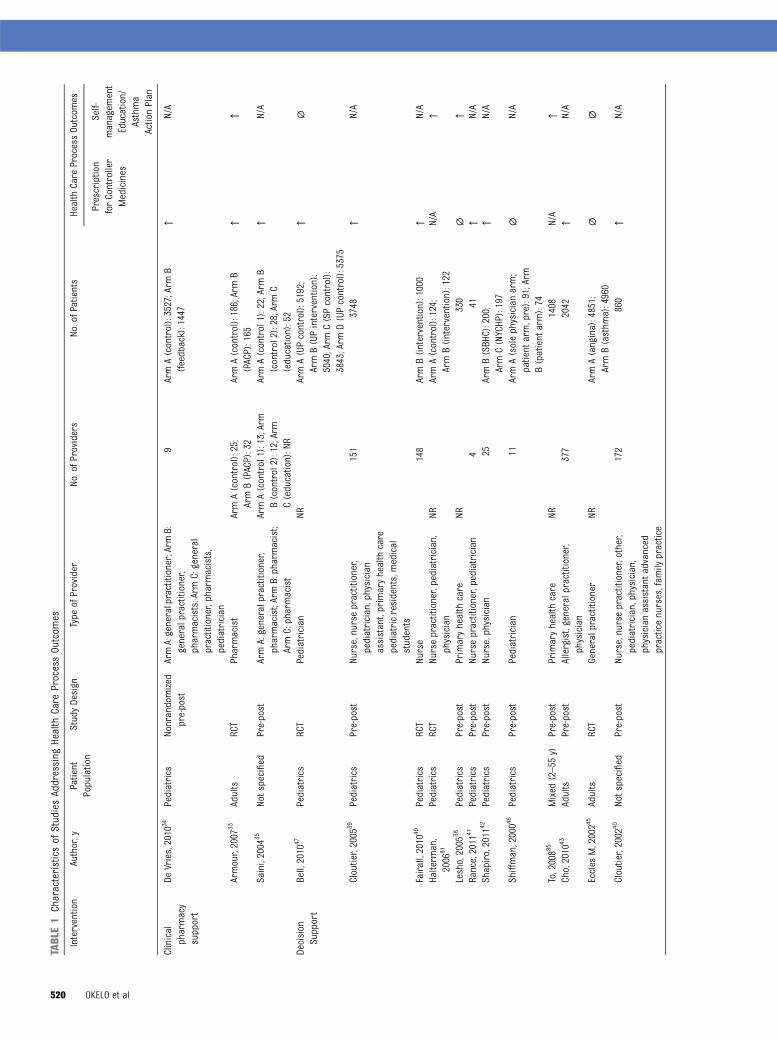
TABLE1
Characteristicsof
StudiesAddressing
Health
Care
ProcessOutcom
es
Intervention
Author,y
Patient
Population
StudyDesign
Type
ofProvider
No.ofP
roviders
No.ofPatients
Health
Care
ProcessOutcom
es
Prescription
forController
Medicines
Self-
managem
ent
Education/
Asthma
ActionPlan
Clinical
pharmacy
support
DeVries,2010
34Pediatrics
Nonrandomized
pre-post
ArmA:generalpractitioner;Arm
B:generalpractitioner,
pharmacists;Arm
C:general
practitioner,pharmacists,
pediatrician
9ArmA(control):3527;Arm
B(feedback):1447
↑N/A
Armour,2007
33Adults
RCT
Pharmacist
ArmA(control):25;
ArmB(PACP):32
ArmA(control):186;ArmB
(PACP):165
↑↑
Saini,2004
35Notspecified
Pre-post
ArmA:generalpractitioner,
pharmacist;ArmB:pharmacist;
ArmC:pharmacist
ArmA(control1):13;Arm
B(control2):12;Arm
C(education):NR
ArmA(control1):22;ArmB
(control2):28;ArmC
(education):52
↑N/A
Decision
Support
Bell,2010
47Pediatrics
RCT
Pediatrician
NRArmA(UPcontrol):5192;
ArmB(UPintervention):
5040;Arm
C(SPcontrol):
3843;Arm
D(UPcontrol):5375
↑∅
Cloutier,2005
39Pediatrics
Pre-post
Nurse,nursepractitioner,
pediatrician,physician
assistant,primaryhealth
care
pediatricresidents,medical
students
151
3748
↑N/A
Fairall,2010
49Pediatrics
RCT
Nurse
148
ArmB(intervention):1000
↑N/A
Halterm
an,
2006
81Pediatrics
RCT
Nursepractitioner,pediatrician,
physician
NRArmA(control):124;
ArmB(intervention):122
N/A
↑
Lesho,2005
38Pediatrics
Pre-post
Primaryhealth
care
NR330
∅↑
Rance,2011
41Pediatrics
Pre-post
Nursepractitioner,pediatrician
441
↑N/A
Shapiro,2011
42Pediatrics
Pre-post
Nurse,physician
25ArmB(SBH
C):200;
ArmC(NYCHP):197
↑N/A
Shiffman,20004
6Pediatrics
Pre-post
Pediatrician
11ArmA(solephysicianarm;
patient
arm,pre):91;Arm
B(patient
arm):74
∅N/A
To,20088
5Mixed
(2–55
y)Pre-post
Primaryhealth
care
NR1408
N/A
↑Cho,2010
43Adults
Pre-post
Allergist,generalpractitioner,
physician
377
2042
↑N/A
Eccles
M,20024
5Adults
RCT
Generalpractitioner
NRArmA(angina):4851;
ArmB(asthm
a):4960
∅∅
Cloutier,2002
40Notspecified
Pre-post
Nurse,nursepractitioner,other,
pediatrician,physician,
physicianassistantadvanced
practicenurses,fam
ilypractice
172
860
↑N/A
520 OKELO et al

TABLE1
Continued
Intervention
Author,y
Patient
Population
StudyDesign
Type
ofProvider
No.ofProviders
No.ofPatients
Health
Care
ProcessOutcom
es
Prescription
forController
Medicines
Self-
managem
ent
Education/
Asthma
ActionPlan
Davis,2010
48Notspecified
Pre-post
Physicianfamily
medicine
residents
NR180
↑N/A
Horswell,2008
36Notspecified
Pre-post
Physician
NRNR
↑↑
Kattan,20065
Notspecified
RCT
Nursepractitioner,physician
assistant,primaryhealth
care
ArmA(standardpractice):
NR;Arm
B(decision
support):435
ArmA(standardpractice):
466;ArmB(decisionsupport):471
↑N/A
Martens,20074
4Notspecified
RCT
Generalpractitioner
ArmA(Control):54;Arm
B(Guidelines
andinvolved
indevelopm
ent):53
ArmA:24
160;ArmB:35
748
∅N/A
McCow
an,20018
2Notspecified
RCT
Generalpractitioner
NRArmA(control):330;ArmB
(decisionsupport):147
N/A
∅
Mitchell,2005
37Notspecified
RCT
Generalpractitioner
270
NR∅
N/A
Newton,2010
84Notspecified
Pre-post
Nurse,physicianpractice
managers,otherstaff
NRNR
N/A
↑
Ruoff,2002
19Notspecified
Pre-post
Family
physicians
ArmA:17;Arm
B:17
ArmA:122;ArmB:122
N/A
↑Ragazzi,2010
83Notspecified
Pre-post
Nurse,pediatrician
26–28
NRN/A
↑Educationonly
Davis,2004
57Pediatrics
Pre-post
Primaryhealth
care
20NR
↑N/A
Blackstien-
Hirsch,
2000
58
Pediatrics
Pre-post
Physician
59195
∅N/A
Shah,20115
0Pediatrics
RCT
Generalpractitioner
150
ArmA(control):107
ArmB(PACE):110
↑↑
Brow
nR,2004
18Pediatrics
RCT
Pediatrician
ArmA(Control):11;Arm
B(Education):12
ArmA(control):122;Arm
B(education):157
∅∅
Clark,1998
52Pediatrics
RCT
Pediatrician,physician
ArmA(control):37;Arm
B(education):37
637
↑↑
Stergachis,
2002
53Pediatrics
RCT
Pharmacist
ArmA(control):NR
;Arm
B(education):35
ArmA(control):177;Arm
B(education):153
∅N/A
Sulaiman,20108
7Pediatrics
RCT
Generalpractitioner
ArmA(control):18;Arm
B(educationand
guidelines):18;Arm
C(guidelines):15
ArmA(control):121;ArmB
(educationandguidelines):
156;ArmC(guidelines):134
N/A
∅
Prem
aratne,
1999
54Mixed
(15–50
y)RCT
Nursepracticenurses
NRArmA(control):14
410;Arm
B(education):9900
∅N/A
Holton,2011
86Adults
RCT
Generalpractitioner
ArmA(control):45;Arm
B(spirometry
training):127
ArmA(control):157;Arm
B(spirometry
training):240
N/A
∅
Smeele,19995
1Adults
RCT
Generalpractitioner
ArmA(control):17;Arm
B(education):17
ArmA(control):223;Arm
B(education):210
∅N/A
Cowie,20015
6Notspecified
Pre-post
NRNR
ArmA(basiceducation):NR;
ArmB(intermediateeducation):
NR;Arm
C(intensive
education):NR
∅N/A
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 521

TABLE1
Continued
Intervention
Author,y
Patient
Population
StudyDesign
Type
ofProvider
No.ofProviders
No.ofPatients
Health
Care
ProcessOutcom
es
Prescription
forController
Medicines
Self-
managem
ent
Education/
Asthma
ActionPlan
Mahi-Taright,
2004
55Notspecified
Pre-post
Generalpractitioner
5049
∅N/A
Feedback
and
audit
SchneiderA.,
2008
67Mixed
RCT
Generalpractitioner
96ArmA(traditionalquality
circle):NR
;Arm
B(benchmark
quality
circle):NR
;Arm
C(com
binedarms):256
∅↑
Suh,2001
65Mixed
(4–55
y)Pre-post
NRNR
ArmA(intermittentasthm
a):
566;ArmB(persistent
asthma):1050
↑N/A
Sondergaard,
2002
69Mixed
(6–45
y)RCT
Generalpractitioner
ArmA(control):141;Arm
B(individualpatient
count
datafeedback):77;Arm
C(aggregatedatafeedback):74
6437
∅N/A
Veninga,1999
59Adults
RCT
Generalpractitioner
ArmA(Netherlands):181;Arm
B(Sweden):204;ArmC
(Norway):199;ArmD
(Slovakia):81
NR↑
N/A
Feder,1995
60Adults
RCT
Generalpractitioner
NRArmA(diabeteseducation):NR;
ArmB(education,reminders
andaudit):NR
↑↑
Veninga,2000
61Adults
RCT
Generalpractitioner
ArmA(UTI):91;Arm
B(educationandfeedback):90
ArmA(UTI):NR
;Arm
B(educationandfeedback):NR
↑N/A
Baker,2003
66Notspecified
RCT
Generalpractitioner
ArmA(guidelines
only):27;
ArmB(guidelines
with
auditcriteria):27;ArmC
(guidelines
with
audit
criteriaandfeedback):27
ArmA(guidelines
only):483;Arm
B(guidelines
with
auditcriteria):
510;ArmC(guidelines
with
audit
criteriaandfeedback):489
↑∅
Coleman,20036
3Notspecified
Pre-post
Pharmacistp
rescriber
NRArmA(patient
specificinform
ation:
prescriberswith
patientson
“high
dose”):510;Arm
B(patient-specific
inform
ation:prescriberswith
patientson
“low
dose”):135
∅↑
Richman,20006
4Notspecified
Pre-post
Pediatrician
29228
Nostatistical
testingof
results
for
thisoutcom
e
↑
Herborg,2001
68Notspecified
Non-RCT
Generalpractitioner,other,
pharmacistpharm
acyassistant
ArmA(control):64;Arm
B(TOM
):75
NR↑
N/A
522 OKELO et al
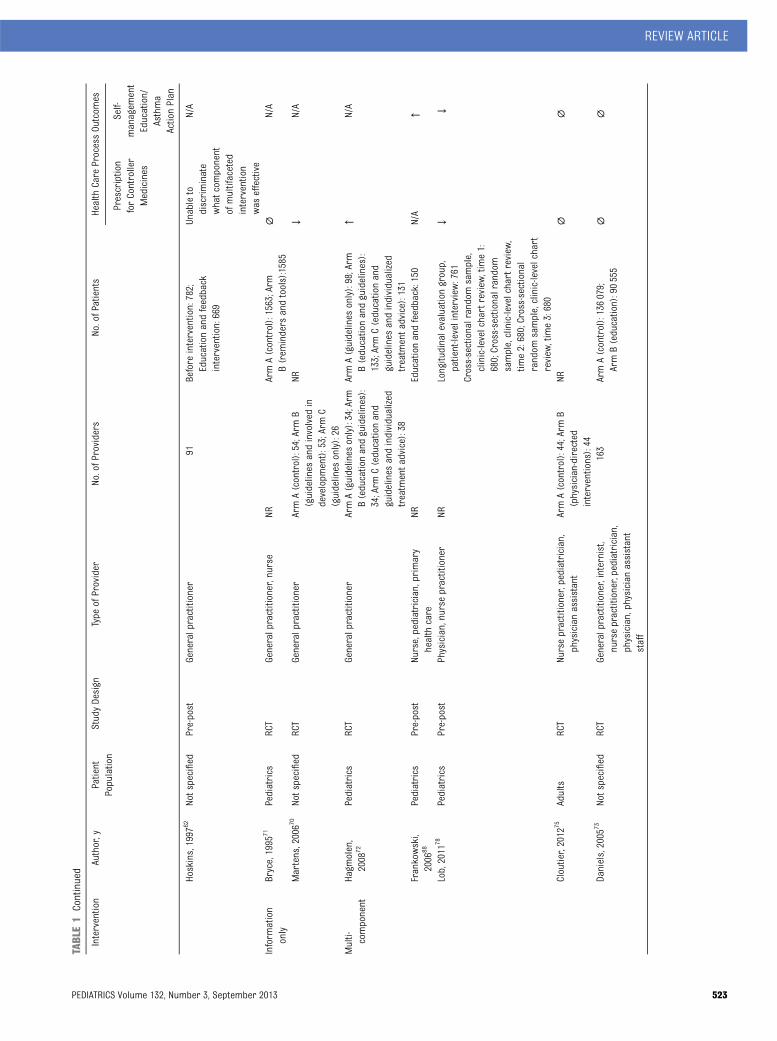
TABLE1
Continued
Intervention
Author,y
Patient
Population
StudyDesign
Type
ofProvider
No.ofProviders
No.ofPatients
Health
Care
ProcessOutcom
es
Prescription
forController
Medicines
Self-
managem
ent
Education/
Asthma
ActionPlan
Hoskins,1997
62Notspecified
Pre-post
Generalpractitioner
91Before
intervention:782;
Educationandfeedback
intervention:669
Unableto
discriminate
whatcom
ponent
ofmultifaceted
intervention
was
effective
N/A
Inform
ation
only
Bryce,1995
71Pediatrics
RCT
Generalpractitioner,nurse
NRArmA(control):1563;Arm
B(rem
inders
andtools):1585
∅N/A
Martens,20067
0Notspecified
RCT
Generalpractitioner
ArmA(control):54;Arm
B(guidelines
andinvolved
indevelopm
ent):53;ArmC
(guidelines
only):26
NR↓
N/A
Multi- component
Hagm
olen,
2008
72Pediatrics
RCT
Generalpractitioner
ArmA(guidelines
only):34;Arm
B(educationandguidelines):
34;Arm
C(educationand
guidelines
andindividualized
treatm
entadvice):38
ArmA(guidelines
only):98;Arm
B(educationandguidelines):
133;ArmC(educationand
guidelines
andindividualized
treatm
entadvice):131
↑N/A
Frankowski,
2006
88Pediatrics
Pre-post
Nurse,pediatrician,primary
health
care
NREducationandfeedback:150
N/A
↑
Lob,2011
78Pediatrics
Pre-post
Physician,nursepractitioner
NRLongitudinalevaluationgroup,
patient-levelinterview
:761
↓↓
Cross-sectionalrandomsample,
clinic-levelchartreview
,time1:
680;Cross-sectionalrandom
sample,clinic-levelchartreview
,tim
e2:680;Cross-sectional
random
sample,clinic-levelchart
review
,time3:680
Cloutier,2012
75Adults
RCT
Nursepractitioner,pediatrician,
physicianassistant
ArmA(control):44;Arm
B(physician-directed
interventions):44
NR∅
∅
Daniels,2005
73Notspecified
RCT
Generalpractitioner,internist,
nursepractitioner,pediatrician,
physician,physicianassistant
staff
163
ArmA(control):136079;
ArmB(education):90555
∅∅
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 523

TABLE1
Continued
Intervention
Author,y
Patient
Population
StudyDesign
Type
ofProvider
No.ofProviders
No.ofPatients
Health
Care
ProcessOutcom
es
Prescription
forController
Medicines
Self-
managem
ent
Education/
Asthma
ActionPlan
Lundborg,19997
4Notspecified
RCT
Generalpractitioner
ArmA(control):104;Arm
B(educationandfeedback):
100
ArmA(control):1333;Arm
B(educationandfeedback):1121
∅N/A
Yawn,2008
77Notspecified
Pre-post
Nursepractitioner,physician,
physicianassistant
Educationandfeedback:211
Educationandfeedback:840
↑↑
Bender,20117
6Notspecified
Pre-post
Nurse,physician,physician
assistantmedicalassistants,
practicemanagers,office
staff
372
15508
↑↑
Organizational
change
Finkelstein,
2005
79Pediatrics
RCT
Pediatricmedicalprovider
228
ArmA(control):1531;Arm
B(PLE
intervention):2003;Arm
C(planned
care
intervention):
1635
∅N/A
Glasgow,20038
9Pediatrics
RCT
Generalpractitioner
ArmA(control):12;Arm
B(intervention):12
ArmA(control):73;ArmB
(intervention):101
N/A
↑
Patel,2004
90Mixed
(4–55
y)Pre-post
Physicians,nurses
NR451
N/A
↑Thyne,2007
80Notspecified
Pre-post
“Pediatricmedicalproviders,”
“urgentcareclinicians”
NRArmA(time1,2002–2003):NR
;ArmB(time2,2003–2004):NR
;ArmC(time3,2004–2005):NR
↑N/A
Quality
improvem
ent
Fox,2007
92Pediatrics
Pre-post
Nurse,nursepractitioner,
physiciancaregivers,
administrativestaff
NRChartreviewsample:280;
Interviewsample:405
N/A
↑
Homer,20059
1Pediatrics
RCT
Nurse,physicianfrontoffice
staff
NRArmA(control):337;Arm
B(learningcollaborative):294
N/A
∅
Mangione-Sm
ith,
2005
93Notspecified
Pre-post
“Health
care
providers”
NRArmA(control):126;Arm
B(learningcollaborative):385
N/A
↑
NR,notreported;NYCHP,New
York
Children’sHealthProject;PACE,Physician
AsthmaCareEducation;PACP,Pharm
acyAsthmaCareProgram;PLE,PeerLeader
Education;SBHC,SouthBronxHealthCenter;SP,suburban
practice;TOM,therapeuticoutcom
esmonitoring;UP,urbanpractice;UTI,urinarytractinfection.↑,Statisticallysignificantincrease
inoutcom
eofinterest.↓,Statisticallysignificantdecrease
inoutcom
eofinterest.∅
,Difference
betweeninterventionandcontrolgroupsor
betweenpre-and
postinterventionnotstatisticallysignificant.
524 OKELO et al
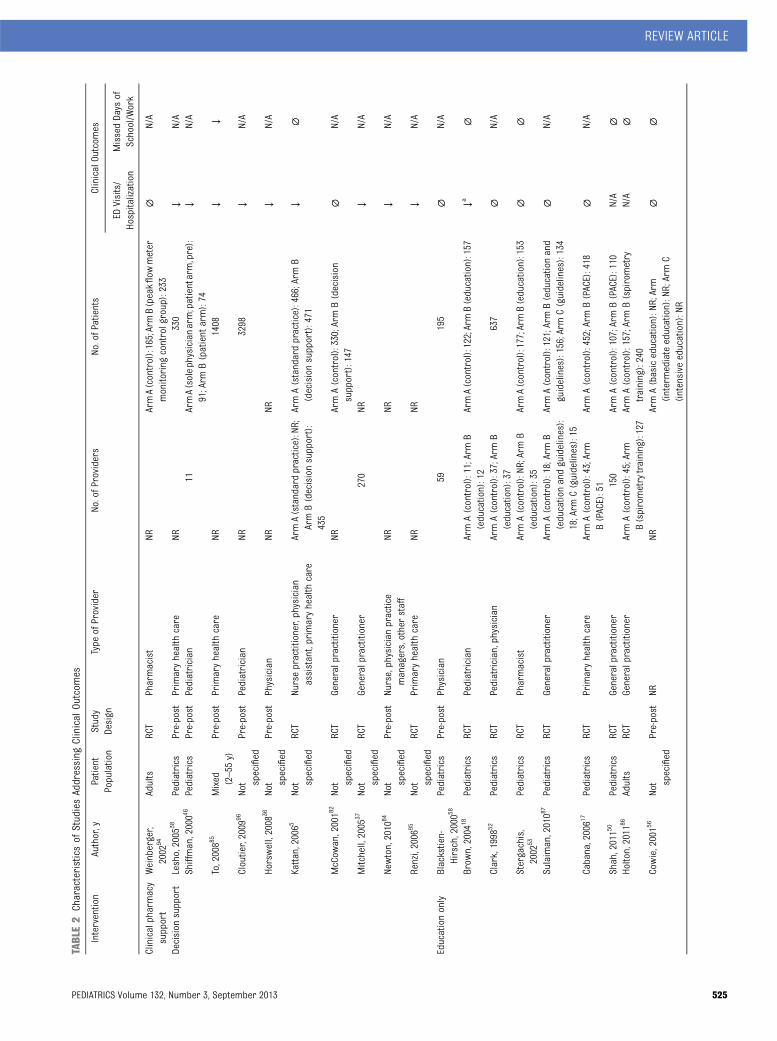
TABLE2
Characteristicsof
StudiesAddressing
Clinical
Outcom
es
Intervention
Author,y
Patient
Population
Study
Design
Type
ofProvider
No.ofProviders
No.ofPatients
ClinicalOutcom
es
EDVisits/
Hospitalization
MissedDays
ofSchool/Work
Clinicalpharmacy
support
Weinberger,
2002
94Adults
RCT
Pharmacist
NRArmA(control):165;ArmB(peakflow
meter
monitoring
controlgroup):233
∅N/A
Decision
support
Lesho,2005
38Pediatrics
Pre-post
Primaryhealth
care
NR330
↓N/A
Shiffman,20004
6Pediatrics
Pre-post
Pediatrician
11ArmA(solephysicianarm;patientarm,pre):
91;Arm
B(patient
arm):74
↓N/A
To,20088
5Mixed (2–55
y)Pre-post
Primaryhealth
care
NR1408
↓↓
Cloutier,2009
96Not specified
Pre-post
Pediatrician
NR3298
↓N/A
Horswell,2008
36Not specified
Pre-post
Physician
NRNR
↓N/A
Kattan,20065
Not specified
RCT
Nursepractitioner,physician
assistant,primaryhealth
care
ArmA(standardpractice):NR;
ArmB(decisionsupport):
435
ArmA(standardpractice):466;Arm
B(decisionsupport):471
↓∅
McCow
an,20018
2Not specified
RCT
Generalpractitioner
NRArmA(control):330;ArmB(decision
support):147
∅N/A
Mitchell,2005
37Not specified
RCT
Generalpractitioner
270
NR↓
N/A
Newton,2010
84Not specified
Pre-post
Nurse,physicianpractice
managers,otherstaff
NRNR
↓N/A
Renzi,2006
95Not specified
RCT
Primaryhealth
care
NRNR
↓N/A
Educationonly
Blackstien-
Hirsch,20005
8Pediatrics
Pre-post
Physician
59195
∅N/A
Brow
n,2004
18Pediatrics
RCT
Pediatrician
ArmA(control):11;Arm
B(education):12
ArmA(control):122;ArmB(education):157
↓a∅
Clark,1998
52Pediatrics
RCT
Pediatrician,physician
ArmA(control):37;Arm
B(education):37
637
∅N/A
Stergachis,
2002
53Pediatrics
RCT
Pharmacist
ArmA(control):NR
;Arm
B(education):35
ArmA(control):177;ArmB(education):153
∅∅
Sulaiman,20108
7Pediatrics
RCT
Generalpractitioner
ArmA(control):18;Arm
B(educationandguidelines):
18;Arm
C(guidelines):15
ArmA(control):121;ArmB(educationand
guidelines):156;ArmC(guidelines):134
∅N/A
Cabana,20061
7Pediatrics
RCT
Primaryhealth
care
ArmA(control):43;Arm
B(PACE):51
ArmA(control):452;ArmB(PACE):418
∅N/A
Shah,20115
0Pediatrics
RCT
Generalpractitioner
150
ArmA(control):107;ArmB(PACE):110
N/A
∅Holton,2011
86Adults
RCT
Generalpractitioner
ArmA(control):45;Arm
B(spirometrytraining):127
ArmA(control):157;ArmB(spirometry
training):240
N/A
∅
Cowie,20015
6Not specified
Pre-post
NRNR
ArmA(basiceducation):NR;Arm
(intermediateeducation):NR;ArmC
(intensive
education):NR
∅∅
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 525

TABLE2
Continued
Intervention
Author,y
Patient
Population
Study
Design
Type
ofProvider
No.ofProviders
No.ofPatients
ClinicalOutcom
es
EDVisits/
Hospitalization
MissedDays
ofSchool/Work
Feedback
and
audit
Schneider,2008
67Mixed
RCT
Generalpractitioner
96ArmA(traditionalqualitycircle):NR
;Arm
B(benchmarkquality
circle):NR
;Arm
C(com
binedarms):256
∅N/A
Richman,20006
4Not specified
Pre-post
Pediatrician
29228
∅∅
Inform
ationonly
Bryce,1995
71Pediatrics
RCT
Generalpractitioner,nurse
NRArmA(control):1563;Arm
B(rem
indersand
tools):1585
∅N/A
Multicom
ponent
Lob,2011
78Pediatrics
Pre-post
Physician,nursepractitioner
NRLongitudinalevaluationgroup,patient-level
interview:761;Cross-sectionalrandom
sample,clinic-levelchartreview
,time1:
680;Cross-sectionalrandomsample,
clinic-levelchartreview
,time2:680;
Cross-sectionalrandomsample,clinic-
levelchartreview
,time3:680
↓↓
Organizational
change
Finkelstein,
2005
79Pediatrics
RCT
Pediatricmedicalprovider
228
ArmA(control):1531;Arm
B(PLE
intervention):2003;ArmC(planned
care
intervention):1635
∅N/A
Glasgow,20038
9Pediatrics
RCT
Generalpractitioner
ArmA(control):12;Arm
B(intervention):12
ArmA(control):73;Arm
B(intervention):101
∅∅
Patel,2004
90Mixed (4–55
y)Pre-post
Physicians,nurses
NR451
↓N/A
Thyne,2007
80Not specified
Pre-post
“Pediatricmedicalproviders,”
“urgentcare
clinicians”
NRArmA(time1,2002–2003):NR
;Arm
B(time
2,2003–2004):NR
;Arm
C(time3,2004–
2005):NR
↓bN/A
Quality
improvem
ent
Homer,20059
1Pediatrics
RCT
Nurse,physicianfront
office
staff
NRArmA(control):337;ArmB(learning
collaborative):294
∅N/A
Mangione-Sm
ithR.,20059
3Not specified
Pre-post
“Health
care
providers”
NRArmA(control):126;ArmB(learning
collaborative):385
∅∅
NR,notreported;PACE,PhysicianAsthmaCare
Education;PLE,Peer
Leader
Education.↑,Statisticallysignificantincrease
inoutcom
eofinterest.↓,Statisticallysignificantdecrease
inoutcom
eofinterest.∅
,Difference
betweeninterventionandcontrol
groups,orbetweenpre-andpost-interventionnotstatisticallysignificant.
aReductioninED
visitforsubgroup
oflow-incomeparticipantsonlybutreductioninannualrateofhospitalizationforentiregroup.
bReductioninED
visitbutP
valuenotreported
instudy.
526 OKELO et al

of the evidence by outcome. Twenty-fiveof the 68 studies were conducted inpediatric-only populations. The tablesindicate if the patient population in-cluded children only, adults only,a mixture of children and adults, or ifthe patient population is unknown.
Outcome: Prescription ofController Medicines
Clinical Pharmacy Support
We identified 3 studies.33–35 In a ran-domized controlled trial (RCT), phar-macists trained in risk assessment,medication adherence, and spirometryreported increased dispensation ofasthma controller medicines (oddsratio [OR]: 3.80; 95% confidence in-terval [CI]: 1.40–10.32; P = .01).33 In 2non-RCTs,34,35 clinical pharmacy sup-port increased controller medicationprescribing by 20%35 and 6%34 (P, .05for both studies). In the controlled pre-post study, the intervention was a spe-cialized asthma service provided bycommunity pharmacies: patient appoint-ments, assessment and intervention ofpatient medication needs, and goal-setting with the patient.35 In the latterstudy, pharmacists were encouraged tomeet with local practitioners to discusspediatric asthma care guidelines.34
SOE: moderate.
Decision Support
Fifteen studies were identified that in-cluded the provision of asthma guide-lines in a more accessible format (eg,“pocket” versions),36–38 use of a specificalgorithm, pathway, or flow sheet,37–40
a structured template for taking a his-tory,41,42 a reminder system to raiseawareness about the patient’s asthmastatus,5,43,44 and computer systems.36,43–48
Ten of the studies reported significant-ly increased prescribing of asthmacontroller medicines,5,36,39–43,47–49 from2% to 34%, and 5 reported no statisti-cally significant effect.37,38,44–46
SOE: moderate.
Education Only
The 10 education-only interventions weidentified18,50–58 included small-groupasthma education programs,51 struc-tured training,58 seminars,52 and grandrounds.58 Certain interventions alsoemphasized more general skills, suchas training in communication.50,52 Thestudies reported increased prescribingof 3.5% to 50.3%, although statisticallysignificant increases were reported onlyin 3 of the studies.
SOE: low.
Feedback and Audit
We identified 11 studies; most assesseda multifaceted intervention combinedwith provider education,59–65 prioritizedreview criteria for audit,66 benchmark-ing (comparison with peers or otherpractices),66,67 or pharmacy monitoringof fill data and feedback.68,69
Increased prescribing of asthma con-trollermedicineswasreported forRCTsusing (1) targeted key guideline mes-sages (eg, “use inhaled corticosteroids[ICS] promptly”; 5%–12% increase, P =.05),59 (2) prioritized guideline reviewcriteria on a card,66 (3) prompts forannual review of asthma manage-ment,60 or (4) individualized feedbackon prescribing and decision strate-gies.61 The 2 RCTs reporting no effecton prescribing of asthma controllermedications involved mailed feedbackof prescribing data69 and a trial ofperformance feedback (a “benchmark”group, whose prescribing behaviorwas compared with a performancebenchmark or with other prescribers,versus a traditional or individualfeedback group, which did not receivecomparison with other prescribers).67
The observed effects between 3 groups(guidelines alone, prioritized guidelinereview criteria, and review criteria plusfeedback on actual prescribing behav-ior) was a 15.9% increase in controllerprescribing in the review criteria plusfeedback group, compared with an 11%
increase in the review criteria only andno change (0%) in the guideline onlygroup.66 A positive but nonsignificant2.7% difference (95% CI: –14.4 to 19.7)was noted in the proportion of patientsin practices with asthma “prophylaxis”compared with practices provided withdiabetes guidelines.60
Three of 5 pre-post studies reportedincreased prescribing of controllermedications (52%–104%): change inprescribing over time (52%), a 104.4%in patients with intermittent asthmabut a decrease by 10.8% in patientswith persistent asthma.
SOE: moderate.
Information Only
Two RCTs were assessed informationonly.70,71 One study, which randomizedpatients to have asthma managementinformation and treatment guidelinesinserted into their medical records forprovider use, reported no benefit.71 Thesecond study randomly selected pro-viders to participate in developing localasthma guidelines mailed to providersin both intervention and comparisongroups.70 Intervention providerswrote 8fewer prescriptions per 1000 patients(P, .01).
SOE: insufficient.
Multicomponent
We identified 7 studies of multicompo-nent interventions.72–78 All interventionsincluded information, education, and atleast 2 of the following: organizationalchange, decision support, and feed-back and audit. Two of the 3 pre-poststudies reported 25% to 49% increasesin prescribing rates.76,77 Three of the 4RCTs reported no statistically signifi-cant effects.
SOE: low.
Organizational Change
The 2 studies of organizational changefocused on pediatric providers.79,80 An
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 527

RCT assessed the use of an asthmanurse educator,79 and the pre-poststudy evaluated use of a communityhealth worker.80 The RCT reported nosignificant increase in prescriptionsfor ICS or asthma controller medi-cations (4%–16%).79 In the pre-poststudy, investigators observed a 12%increase in ICS prescriptions (noP value reported).80
SOE: low.
Quality Improvement and Pay-for-Performance
No studies were identified.
SOE: insufficient.
Outcome: Self-ManagementEducation and Asthma Action Plans
Clinical Pharmacy Support
We identified 1 RCT in which patients ofpharmacists in the Pharmacy AsthmaCare Program had increased asthmaaction plan possession (40.4%; 95% CI:31.9–48.9; P, .001); however, there areno data for the control group.33
SOE: moderate.
Decision Support
We identified 10 studies19,36,38,45,47,81–85
that includedcomputerizedsupport,36,45,47,82,84
a flow sheet/algorithm,19,85 and/or theprovision of guidelines.38 Two of the 3studies focused on pediatricians.81,83
Seven studies reported statisticallysignificant increase in the provision ofpatient education/asthma action plansof 14% to 84% (all reported as statis-tically significant).19,36,38,81,83–85 Three ofthe 4 RCTs reported no significant dif-ference.45,47,82
SOE: moderate.
Education Only
Of the 5 RCTs of education-only inter-ventions,18,50,52,86,87 1 focused on pedia-tricians and used small-group asthmaeducation programs, structured train-ing, and interactive seminars. Two
studies increased use of asthma actionplans by 10% (P = .03)52 and 15% (P =.046).50 The other 3 studies reported noincrease.18,86,87
SOE: low.
Feedback and Audit
Five studies evaluated feedback andaudit.60,63,64,66,67 Significant increasesin provision of self-managementeducation/asthma action plans (1%–40%) were reported in 4 studies.60,63,64,67
For peak flow meter use, one studyreported a 3.6% decrease, while asecond study reported a minimal in-crease of 0.7% (95% CI: –15.2 to 16.7)after practices received asthma guide-lines.60 A moderate increase was notedfor inhaler technique, 12.9% (95% CI:1.9 to 23.9),51 and a small increase inchange of asthma action plan use(7.6%) in a benchmarking feedbackgroup.67
SOE: low.
Information Only
No studies were identified.
SOE: insufficient.
Multicomponent
Of the 6 studies we reviewed,73,75–78,88
most included an educational compo-nent but also included (1) training incommunication techniques with pro-vision of a spirometer and training inuse of the spirometer76; (2) laminatedposters of guidelines and medicationswith feedback on asthma action planuse and monthly calls from an in-tervention team to troubleshoot com-munication problems88; (3) asthma kits(peak flow meters, spacers, educa-tional materials) and systems-levelchanges (flow sheets and standingmedication orders)73; (4) systematicuse of a patient questionnaire and anasthma management algorithm77; (5)an asthma coordinator and feedbackon performance as part of continuousquality improvement efforts; or (6) an
educational toolbox with seminars,teleconferences, mini fellowships, opin-ion leader visits, clinician-specific feed-back, and pay for performance.75 Thepre-post studies reported increasesin the provision of action plans(27%–46%).76–78,88 Both RCTs reportednonsignificant increases in patienteducation/asthma action plans (7% in1 study; relative risk = 1.82 in the otherstudy).73,75
SOE: low.
Organizational Change
We identified 2 studies.89,90 A pre-poststudy (instituting a registry to trackasthma patients and an asthma casemanager) reported a 10% increase inpatient education (P, .001) and a 14%increase in asthma action plan dis-pensations (P , .001).90 In the RCT (arestructured clinical protocol for howasthma patients are cared for duringambulatory care encounters; “3+ visitplan”), there was a 10% increase in theprovision of asthma education (P =.01).89
SOE: low.
Quality Improvement and Pay-for-Performance
Three studies, each including pediatrichealth care providers, were identi-fied.91–93 Two studies assessed par-ticipation in a Breakthrough SeriesCollaborative,91,93 and 1 study asses-sed a combination of continuous qualityimprovement and the addition of acommunity health worker.92 One ofthese studies showed a difference of33% in the intervention arm.93 Two ofthe 3 studies showed a 28% to 32% in-crease in the proportion of patientswhohad received an asthma action plan.92,93
These 2 studies enrolled practices thathad already joined a quality improve-ment initiative93 or were part of a dem-onstration project.92
The RCT showed no significant effect,witha3%lowerrate for the intervention
528 OKELO et al

versus control group.91 However, therewere decreases in participation and inoutcome reporting over time. In thecontrolled pre-post study, documentedself-management education increasedby 21%.93
SOE: low.
Outcome: ED Visits/Hospitalizations
Clinical Pharmacy Support
In an RCT, pharmacists were providedwith patient specific clinical data,training about asthma management,patient educational materials, resourceguides, and pragmatic strategies.94 Pa-tients of intervention pharmacists weremore likely to have a reduction in EDvisits/hospitalizations compared withpatients seen by pharmacists who re-ceived peak flowmeter instruction only(OR: 2.16; 95% CI: 1.76–2.63) but notcompared with patients of the usualcare control group (OR 1.08; 95% CI:0.93–1.25).94
SOE: insufficient.
Decision Support
For the 10 studies addressing this out-come,5,36–38,46,82,84,85,95,96 decision sup-port interventions included computersystems,36,46,82,84 checklists,95 supple-mental feedback protocols,5 and struc-tured pathways/algorithms.37,96 Severalstudies included children.5,37,46,85,96
Nine studies reported a reduction in EDvisits or hospitalizations5,36–38,46,84,85,95,96
(5%–60%) among pre-post studies (allstatistically significant) and 1% to 7%among the RCTs.5,37,95
SOE: moderate.
Education Only
We identified 7 studies17,18,52,53,56,58,87
involving interactive seminars, struc-tured training, and medical grandrounds. One study reported statisti-cally significant reduction in ED visits(only in a subgroup of low-incomeparticipants; –1.23 visits per year,
P = .001) and in the overall annualhospitalization rate.18
SOE: low.
Feedback and Audit
We identified 2 studies: (1) an RCT ofa traditional quality circle interventionof provider feedback on individualperformance and the aggregate per-formance of the provider group wascompared with a benchmark qualitycircle intervention (feedback on pro-viders’ individual performance wasexplicitly compared with a performancebenchmark)67; and (2) a pre-post studycomparing individual providers’ prac-tice patterns with their peers plus pro-viding asthma education to office staff.64
Patients in the benchmark quality circlehad a 6.7-point decrease in ED visits,although patients in the traditional qual-ity circle intervention had a 12.2-pointdecrease (P = .064).67
No significant change in ED visits (1%decrease) or hospitalizations (2% de-crease) was reported in the pre-poststudy.64
SOE: insufficient.
Information Only
The 1 study identified randomized pa-tients to have information about as-thma guidelines inserted in theirmedical records for provider use; eachprovider thusmanagedpatients in bothintervention and control arms simul-taneously.71 No differences in rates ofED visits or hospitalizations were ob-served between intervention and con-trol arms of the study.
SOE: insufficient.
Multicomponent
One study included quality improve-ment, decision support, organizationalchange, and feedback-and-audit.78 Thisstudy reported a 69% reduction in EDvisits and hospitalizations. However,44% of the patient sample was lost to
follow-up, and significant heterogene-ity in results was seen across partici-pating sites.
SOE: insufficient.
Organizational Change
We identified 4 studies,79,80,89,90 whichincluded restructured asthma carevisits,89 supplemental trained person-nel, and provider education.79,80,90
Three studies focused on pediatricproviders.79,80,89
Only 1 of 4 studies, a pre-post study,reported a significant reduction in EDvisits: a 41% reduction in ED visits and54% reduction in hospitalizations (P,.001 for both).90 The other pre-poststudy reported a 4% reduction in hos-pitalizations (no P value reported).80
The 2 RCTs reported 1% (P. .05)79 and7% (P = .06)89 reductions.
SOE: low.
Quality Improvement and Pay-for-Performance
One RCT91 and 1 controlled pre-poststudy93 evaluated a Breakthrough Se-ries Collaborative quality improvementstrategy among pediatric providersin community health centers. Neitherstudy showed a significant reduction ineither outcome. However, in the RCT,when analyses were limited to the 9practices that attended all 3 learningsessions, significant reductions in EDvisits were reported.91
SOE: low.
Outcome: Missed Days of Work/School
Clinical Pharmacy Support
No studies identified.
SOE: insufficient.
Decision Support
An RCTreported no reduction inmissedschool (0.05 days; P = .4) after mailingpatient-specific asthma morbidity infor-mation to their health care provider.5
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 529

A pre-post study reported a 49% re-duction (P , .001) in school absentee-ism and a 51% reduction in the odds ofmissed work (OR: 0.49; 95% CI: 0.34–0.71) after using an asthma care map,a treatment flowchart, program stand-ards, management flowchart, and ac-tion plan.85 Both studieswere conductedin a pediatric population.
SOE: insufficient.
Education Only
Five studies evaluated the effect ofprovider education onmissed school ormissed work.18,50,53,56,86 Three RCTsused structured training, seminars,and workshops for health care pro-viders to examine the effects onmissedschool. They reported small but sta-tistically nonsignificant reductions inmissed school (0.6–4 days). To evaluatethe impact on missed work, 2 RCTs50,86
and 1 pre-post study56 provided work-shops and training in how to performspirometry, and 1 study comparedasthma program development witha nurse educator program to continu-ing education. All studies reportedsmall, statistically nonsignificant reduc-tions in missed school or work.
SOE: insufficient.
Feedback and Audit
We identified 1 pre-post study thatprovided asthma education to officestaff and observed an 11% reduction inschool days missed and a 0% reductionin parent workdays missed.64
SOE: insufficient.
Information Only
No studies were reviewed.
SOE: insufficient.
Multicomponent
One study implemented decision sup-port, organizational change, and feed-back and audit. This study foundsignificant reductions inmissed days ofschool (53%) andwork (72%). However,
44% of the patient sample was lost tofollow-up, and significant heterogeneityin results was reported.78
SOE: insufficient.
Organizational Change
One RCTof organizational change basedon restructuring the clinical protocolforpatient careduringambulatorycareencounters (“3+ visit plan”)89 did notreduce missed school days (OR: 0.8;95% CI: 0.5–1.2; P = .3).
SOE: low.
Quality Improvement and Pay-for-Performance
One controlled pre-post study reportedthat patients of providers participatingin the Breakthrough Series Collabora-tivequality improvementstrategyshowedno significant reduction in the meannumber of school days or parentalworkdays missed.93
SOE: insufficient.
DISCUSSION
Of the 68 studies we identified, a mi-nority of studies focused on pediatrichealth care providers or involved chil-dren (14 studies assessing clinicaloutcomes; 24 studies assessing healthcare process outcomes). We acknowl-edge that there are a number of ways inwhich providing care for children isdifferent fromproviding care foradults:(1) physiology; (2) disease presen-tation, natural history, and morbidity;(3) the need to consider congenital,genetic, and developmental issues; and(4) support structure, including thatchildren are minors so parents area necessary element to any medicaldecision-making process. However,there are a few reasons that findings ofprovider-targeted asthma interven-tions should be applicable across thehealth care provider spectrum: (1)asthma guideline recommendationsgenerally do not distinguish different
types of providers; (2) a number ofprovider behaviors in asthma careare universal (eg, assessing asthmacontrol/severity; prescribing controllermedications for persistent asthma;providing self-management education);(3) the goals for patient outcomes arethe same (eg, reducing acute care visitsfor exacerbations; limiting missedschool/work); and (4) the mainstaytreatment options are the same (eg,inhaled steroids and short-actingbronchodilators). Therefore, for pedi-atricians, as with other providers, it isreasonable that the decision to chooseand implement a given intervention toimprove their adherence to asthmaguidelines be based on (1) the data onthe effectiveness of the intervention, (2)the feasibility of implementing the in-tervention within their own practicesetting, and (3) the sustainability of theintervention. There is always a need forpediatric-focused studies, but we be-lieve that the findings of our reviewmayprovide lessons for all providers.
Decision support, feedback/audit, andeducation only were the most commoninterventionsandwere tested foreachofthe outcomes we evaluated. Conversely,organizational change, clinical phar-macysupport, quality improvement/pay-for-performance, information only, andmulticomponent strategies were lessconsistently tested (see Table 3). Evi-dence suggests that some of the inter-ventions are not effective in achievingspecific outcomes: education to in-crease prescribing of asthma controllermedications or to reduce ED visits/hospitalizations; organizational changeto reduce ED visits/hospitalizations or toreduce missed days of school/work; andquality improvement to reduce ED visits/hospitalizations. Notably, these findingswere limited by having only a few studies,typically nonrandomized, on which todraw conclusions. Most of the studiesused a pre-post design, whichmore oftenreported abeneficial effect than theRCTs.
530 OKELO et al
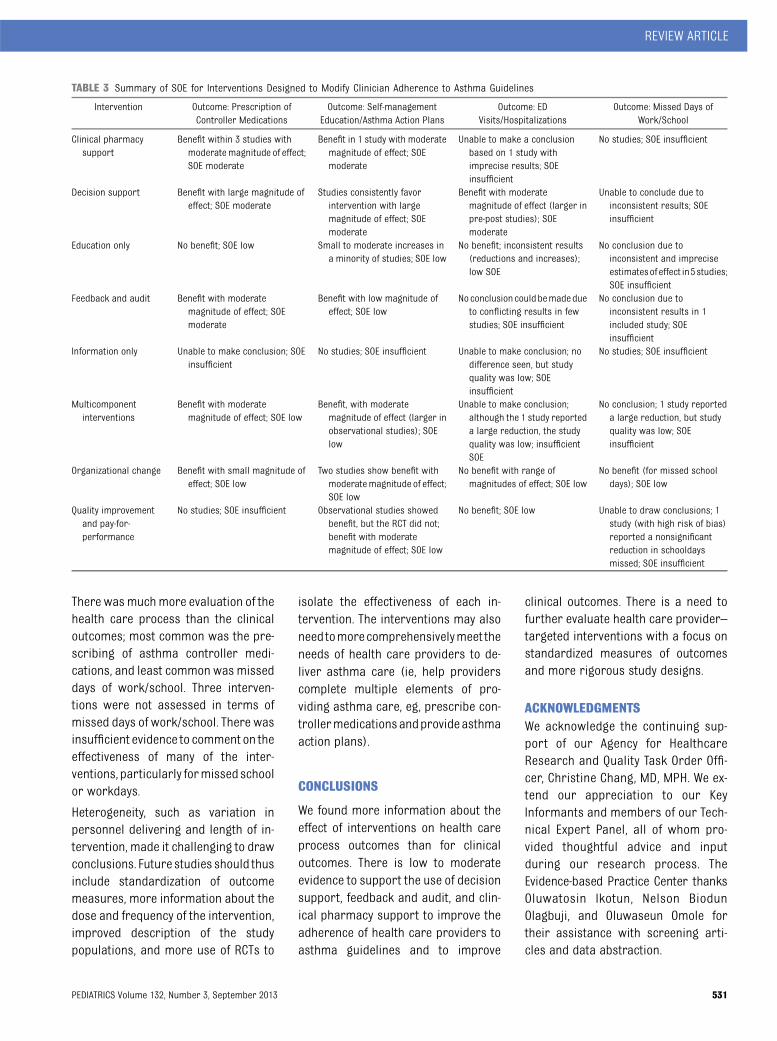
There wasmuchmore evaluation of thehealth care process than the clinicaloutcomes; most common was the pre-scribing of asthma controller medi-cations, and least common was misseddays of work/school. Three interven-tions were not assessed in terms ofmissed days of work/school. There wasinsufficient evidence to comment on theeffectiveness of many of the inter-ventions, particularly formissedschoolor workdays.
Heterogeneity, such as variation inpersonnel delivering and length of in-tervention, made it challenging to drawconclusions. Future studies should thusinclude standardization of outcomemeasures, more information about thedose and frequency of the intervention,improved description of the studypopulations, and more use of RCTs to
isolate the effectiveness of each in-tervention. The interventions may alsoneedtomorecomprehensivelymeet theneeds of health care providers to de-liver asthma care (ie, help providerscomplete multiple elements of pro-viding asthma care, eg, prescribe con-trollermedicationsandprovideasthmaaction plans).
CONCLUSIONS
We found more information about theeffect of interventions on health careprocess outcomes than for clinicaloutcomes. There is low to moderateevidence to support the use of decisionsupport, feedback and audit, and clin-ical pharmacy support to improve theadherence of health care providers toasthma guidelines and to improve
clinical outcomes. There is a need tofurther evaluate health care provider–targeted interventions with a focus onstandardized measures of outcomesand more rigorous study designs.
ACKNOWLEDGMENTSWe acknowledge the continuing sup-port of our Agency for HealthcareResearch and Quality Task Order Offi-cer, Christine Chang, MD, MPH. We ex-tend our appreciation to our KeyInformants and members of our Tech-nical Expert Panel, all of whom pro-vided thoughtful advice and inputduring our research process. TheEvidence-based Practice Center thanksOluwatosin Ikotun, Nelson BiodunOlagbuji, and Oluwaseun Omole fortheir assistance with screening arti-cles and data abstraction.
TABLE 3 Summary of SOE for Interventions Designed to Modify Clinician Adherence to Asthma Guidelines
Intervention Outcome: Prescription ofController Medications
Outcome: Self-managementEducation/Asthma Action Plans
Outcome: EDVisits/Hospitalizations
Outcome: Missed Days ofWork/School
Clinical pharmacysupport
Benefit within 3 studies withmoderatemagnitude of effect;SOE moderate
Benefit in 1 study with moderatemagnitude of effect; SOEmoderate
Unable to make a conclusionbased on 1 study withimprecise results; SOEinsufficient
No studies; SOE insufficient
Decision support Benefit with large magnitude ofeffect; SOE moderate
Studies consistently favorintervention with largemagnitude of effect; SOEmoderate
Benefit with moderatemagnitude of effect (larger inpre-post studies); SOEmoderate
Unable to conclude due toinconsistent results; SOEinsufficient
Education only No benefit; SOE low Small to moderate increases ina minority of studies; SOE low
No benefit; inconsistent results(reductions and increases);low SOE
No conclusion due toinconsistent and impreciseestimatesof effect in5studies;SOE insufficient
Feedback and audit Benefit with moderatemagnitude of effect; SOEmoderate
Benefit with low magnitude ofeffect; SOE low
Noconclusion couldbemadedueto conflicting results in fewstudies; SOE insufficient
No conclusion due toinconsistent results in 1included study; SOEinsufficient
Information only Unable to make conclusion; SOEinsufficient
No studies; SOE insufficient Unable to make conclusion; nodifference seen, but studyquality was low; SOEinsufficient
No studies; SOE insufficient
Multicomponentinterventions
Benefit with moderatemagnitude of effect; SOE low
Benefit, with moderatemagnitude of effect (larger inobservational studies); SOElow
Unable to make conclusion;although the 1 study reporteda large reduction, the studyquality was low; insufficientSOE
No conclusion; 1 study reporteda large reduction, but studyquality was low; SOEinsufficient
Organizational change Benefit with small magnitude ofeffect; SOE low
Two studies show benefit withmoderatemagnitude of effect;SOE low
No benefit with range ofmagnitudes of effect; SOE low
No benefit (for missed schooldays); SOE low
Quality improvementand pay-for-performance
No studies; SOE insufficient Observational studies showedbenefit, but the RCT did not;benefit with moderatemagnitude of effect; SOE low
No benefit; SOE low Unable to draw conclusions; 1study (with high risk of bias)reported a nonsignificantreduction in schooldaysmissed; SOE insufficient
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 531

REFERENCES
1. Centers for Disease Control and Preven-tion. Vital signs: asthma prevalence, dis-ease characteristics, and self-managementeducation: United States, 2001—2009.MMWR Morb Mortal Wkly Rep. 2011;60(17):547–552
2. Akinbami L; Centers for Disease Controland Prevention National Center for HealthStatistics. The state of childhood asthma,United States, 1980–2005. Adv Data. 2006;(381):1–24
3. National Asthma Education and PreventionProgram. Expert Panel Report 3 (EPR-3):Guidelines for the diagnosis and manage-ment of asthma—summary report 2007.J Allergy Clin Immunol. 2007;120(suppl 5):S94–S138
4. Evans R III, Gergen PJ, Mitchell H, et al. Arandomized clinical trial to reduce asthmamorbidity among inner-city children:results of the National Cooperative Inner-City Asthma Study. J Pediatr. 1999;135(3):332–338
5. Kattan M, Crain EF, Steinbach S, et al. Arandomized clinical trial of clinician feed-back to improve quality of care for inner-city children with asthma. Pediatrics. 2006;117(6). Available at: www.pediatrics.org/cgi/content/full/117/6/e1095
6. Szefler SJ, Mitchell H, Sorkness CA, et al.Management of asthma based on exhalednitric oxide in addition to guideline-basedtreatment for inner-city adolescents andyoung adults: a randomised controlled tri-al. Lancet. 2008;372(9643):1065–1072
7. Wisnivesky JP, Lorenzo J, Lyn-Cook R, et al.Barriers to adherence to asthma manage-ment guidelines among inner-city primarycare providers. Ann Allergy AsthmaImmunol. 2008;101(3):264–270
8. Halterman JS, Aligne CA, Auinger P,McBride JT, Szilagyi PG. Inadequate therapyfor asthma among children in the UnitedStates. Pediatrics. 2000;105(1 pt 3):272–276
9. Halterman JS, Yoos HL, Kaczorowski JM,et al. Providers underestimate symptomseverity among urban children withasthma. Arch Pediatr Adolesc Med. 2002;156(2):141–146
10. Cabana MD, Slish KK, Nan B, Lin X, ClarkNM. Asking the correct questions to assessasthma symptoms. Clin Pediatr (Phila).2005;44(4):319–325
11. Cabana MD, Bruckman D, Meister K, Bradley JF,Clark N. Documentation of asthma severityin pediatric outpatient clinics. Clin Pediatr(Phila). 2003;42(2):121–125
12. Ortega AN, Gergen PJ, Paltiel AD, BauchnerH, Belanger KD, Leaderer BP. Impact of site
of care, race, and Hispanic ethnicity onmedication use for childhood asthma. Pe-diatrics. 2002;109(1). Available at: www.pediatrics.org/cgi/content/full/109/1/e1
13. Akinbami LJ, Moorman JE, Garbe PL, SondikEJ. Status of childhood asthma in theUnited States, 1980–2007. Pediatrics. 2009;123(suppl 3):S131–S145
14. Flores G, Snowden-Bridon C, Torres S, et al.Urban minority children with asthma:substantial morbidity, compromised qualityand access to specialists, and the im-portance of poverty and specialty care.J Asthma. 2009;46(4):392–398
15. Bracha Y, Brottman G, Carlson A. Physi-cians, guidelines, and cognitive tasks. EvalHealth Prof. 2011;34(3):309–335
16. Bratton SL, Cabana MD, Brown RW, et al.Asthma educational seminar targetingMedicaid providers. Respir Care. 2006;51(1):49–55
17. Cabana MD, Slish KK, Evans D, et al. Impactof physician asthma care education onpatient outcomes. Pediatrics. 2006;117(6):2149–2157
18. Brown R, Bratton SL, Cabana MD, Kaciroti N,Clark NM. Physician asthma educationprogram improves outcomes for childrenof low-income families. Chest. 2004;126(2):369–374
19. Ruoff G. Effects of flow sheet implementa-tion on physician performance in themanagement of asthmatic patients. FamMed. 2002;34(7):514–517
20. Lozano P, Finkelstein JA, Carey VJ, et al.A multisite randomized trial of the effectsof physician education and organizationalchange in chronic-asthma care: health out-comes of the Pediatric Asthma Care PatientOutcomes Research Team II Study. ArchPediatr Adolesc Med. 2004;158(9):875–883
21. Halterman JS, McConnochie KM, Conn KM,et al. A randomized trial of primary careprovider prompting to enhance preventiveasthma therapy. Arch Pediatr Adolesc Med.2005;159(5):422–427
22. Butz AM, Eggleston P, Huss K, Kolodner K,Vargas P, Rand C. Children with asthma andnebulizer use: parental asthma self-carepractices and beliefs. J Asthma. 2001;38(7):565–573
23. Coffman JM, Cabana MD, Yelin EH. Doschool-based asthma education programsimprove self-management and health out-comes? Pediatrics. 2009;124(2):729–742
24. Teach SJ, Crain EF, Quint DM, Hylan ML,Joseph JG. Improved asthma outcomes ina high-morbidity pediatric population:results of an emergency department-based
randomized clinical trial. Arch PediatrAdolesc Med. 2006;160(5):535–541
25. Wise RA, Bartlett SJ, Brown ED, et al. Ran-domized trial of the effect of drug pre-sentation on asthma outcomes: theAmerican Lung Association Asthma ClinicalResearch Centers. J Allergy Clin Immunol.2009;124(3):436–444, 444e1–8
26. Interventions to Modify Healthcare ProviderAdherence to Asthma Guidelines. Researchprotocol. Available at: http://effective-healthcare.ahrq.gov/ehc/products/372/993/AsthmaAdherenceGuidelines_20120302.pdf.Accessed July 16, 2013
27. Okelo SO, Butz AM, Sharma R, et al. Inter-ventions to Modify Adherence to AsthmaGuidelines. Evidence Report (prepared bythe Johns Hopkins University Evidence-basedPractice Center, under Contract No. HHSA290 2007 10061 I). Comparative EffectivenessReviews No. 95. Rockville, MD: Agency forHealthcare Research and Quality; 2013
28. Akinbami LJ, Sullivan SD, Campbell JD,et al. Asthma outcomes: healthcare utiliza-tion and costs. J Allergy Clin Immunol.2012;129(suppl 3):S49–S64
29. Guyatt G, Oxman AD, Sultan S, et al. GRADEguidelines 11—making an overall rating ofconfidence in effect estimates for a singleoutcome and for all outcomes. J Clin Epi-demiol. 2012;66(2):15–17
30. Higgins JPT, Green S, eds. Cochrane Hand-book for Systematic Reviews of Inter-ventions Version 5.1.0 [updated March2011]. The Cochrane Collaboration; 2009.Available at: http://www.cochrane-hand-book.org. Accessed July 16, 2013
31. Cochrane Effective Practice and Organiza-tion of Care Group. Data collection checklist.2002. Available at: http://epoc.cochrane.org/sites/epoc.cochrane.org/files/uploads/datacollectionchecklist.pdf. Accessed July 16,2013
32. Owens DK, Lohr KN, Atkins D, et al. AHRQseries paper 5: grading the strength ofa body of evidence when comparing med-ical interventions—agency for healthcareresearch and quality and the effectivehealth-care program. J Clin Epidemiol.2010;63(5):513–523
33. Armour C, Bosnic-Anticevich S, Brillant M,et al. Pharmacy Asthma Care Program(PACP) improves outcomes for patients inthe community. Thorax. 2007;62(6):496–502
34. de Vries TW, van den Berg PB, Duiverman EJ,de Jong-van den Berg LT. Effect of a minimalpharmacy intervention on improvement ofadherence to asthma guidelines. Arch DisChild. 2010;95(4):302–304
532 OKELO et al

35. Saini B, Krass I, Armour C. Development,implementation, and evaluation of a com-munity pharmacy-based asthma care model.Ann Pharmacother. 2004;38(11):1954–1960
36. Horswell R, Butler MK, Kaiser M, et al. Dis-ease management programs for the un-derserved. Dis Manag. 2008;11(3):145–152
37. Mitchell EA, Didsbury PB, Kruithof N, et al. Arandomized controlled trial of an asthmaclinical pathway for children in generalpractice. Acta Paediatr. 2005;94(2):226–233
38. Lesho EP, Myers CP, Ott M, Winslow C,Brown JE. Do clinical practice guidelinesimprove processes or outcomes in primarycare? Mil Med. 2005;170(3):243–246
39. Cloutier MM, Hall CB, Wakefield DB, Bailit H.Use of asthma guidelines by primary careproviders to reduce hospitalizations andemergency department visits in poor, mi-nority, urban children. J Pediatr. 2005;146(5):591–597
40. Cloutier MM, Wakefield DB, Carlisle PS,Bailit HL, Hall CB. The effect of EasyBreathing on asthma management andknowledge. Arch Pediatr Adolesc Med.2002;156(10):1045–1051
41. Rance K, O’Laughlen M, Ting S. Improvingasthma care for African American childrenby increasing national asthma guidelineadherence. J Pediatr Health Care. 2011;25(4):235–249
42. Shapiro A, Gracy D, Quinones W, ApplebaumJ, Sarmiento A. Putting guidelines intopractice: improving documentation of pedi-atric asthma management using a decision-making tool. Arch Pediatr Adolesc Med.2011;165(5):412–418
43. Cho SH, Jeong JW, Park HW, et al. Effec-tiveness of a computer-assisted asthmamanagement program on physician ad-herence to guidelines. J Asthma. 2010;47(6):680–686
44. Martens JD, van der Weijden T, Severens JL,et al. The effect of computer reminders onGPs’ prescribing behaviour: a cluster-randomised trial. Int J Med Inform. 2007;76(suppl 3):S403–S416
45. Eccles M, McColl E, Steen N, et al. Effect ofcomputerised evidence based guidelineson management of asthma and angina inadults in primary care: cluster randomisedcontrolled trial. BMJ. 2002;325(7370):941
46. Shiffman RN, Freudigman M, Brandt CA,Liaw Y, Navedo DD. A guideline imple-mentation system using handheld com-puters for office management of asthma:effects on adherence and patient out-comes. Pediatrics. 2000;105(4 pt 1):767–773
47. Bell LM, Grundmeier R, Localio R, et al.Electronic health record-based decisionsupport to improve asthma care: a cluster-
randomized trial. Pediatrics. 2010;125(4).Available at: www.pediatrics.org/cgi/content/full/125/4/e770
48. Davis AM, Cannon M, Ables AZ, Bendyk H.Using the electronic medical record toimprove asthma severity documentationand treatment among family medicineresidents. Fam Med. 2010;42(5):334–337
49. Fairall L, Bachmann MO, Zwarenstein M,et al. Cost-effectiveness of educationaloutreach to primary care nurses to in-crease tuberculosis case detection andimprove respiratory care: economic evalu-ation alongside a randomised trial. TropMed Int Health. 2010;15(3):277–286
50. Shah S, Sawyer SM, Toelle BG, et al. Im-proving paediatric asthma outcomes in pri-mary health care: a randomised controlledtrial. Med J Aust. 2011;195(7):405–409
51. Smeele IJ, Grol RP, van Schayck CP, van denBosch WJ, van den Hoogen HJ, Muris JW.Can small group education and peer reviewimprove care for patients with asthma/chronic obstructive pulmonary disease?Qual Health Care. 1999;8(2):92–98
52. Clark NM, Gong M, Schork MA, et al. Impactof education for physicians on patientoutcomes. Pediatrics. 1998;101(5):831–836
53. Stergachis A, Gardner JS, Anderson MT,Sullivan SD. Improving pediatric asthmaoutcomes in the community setting: doespharmaceutical care make a difference?J Am Pharm Assoc (Wash). 2002;42(5):743–752
54. Premaratne UN, Sterne JA, Marks GB, WebbJR, Azima H, Burney PG. Clustered rando-mised trial of an intervention to improvethe management of asthma: Greenwichasthma study. BMJ. 1999;318(7193):1251–1255
55. Mahi-Taright S, Belhocine M, Aït-Khaled N.Can we improve the management ofchronic obstructive respiratory disease?The example of asthma in adults. Int JTuberc Lung Dis. 2004;8(7):873–881
56. Cowie RL, Underwood MF, Mack S. The im-pact of asthma management guidelinedissemination on the control of asthma inthe community. Can Respir J. 2001;8(supplA):41A–45A
57. Davis RS, Bukstein DA, Luskin AT, Kailin JA,Goodenow G. Changing physician pre-scribing patterns through problem-basedlearning: an interactive, teleconferencecase-based education program and reviewof problem-based learning. Ann AllergyAsthma Immunol. 2004;93(3):237–242
58. Blackstien-Hirsch P, Anderson G, Cicutto L,McIvor A, Norton P. Implementing continu-ing education strategies for family physi-cians to enhance asthma patients’ qualityof life. J Asthma. 2000;37(3):247–257
59. Veninga CCM, Lagerløv P, Wahlström R,et al; Drug Education Project Group. Evalu-ating an educational intervention to im-prove the treatment of asthma in fourEuropean countries. Am J Respir Crit CareMed. 1999;160(4):1254–1262
60. Feder G, Griffiths C, Highton C, Eldridge S,Spence M, Southgate L. Do clinical guide-lines introduced with practice based edu-cation improve care of asthmatic anddiabetic patients? A randomised controlledtrial in general practices in east London.BMJ. 1995;311(7018):1473–1478
61. Veninga CCM, Denig P, Zwaagstra R, Haaijer-Ruskamp FM. Improving drug treatment ingeneral practice. J Clin Epidemiol. 2000;53(7):762–772
62. Hoskins G, Neville RG, Smith B, Clark RA.Does participation in distance learning andaudit improve the care of patients withacute asthma attacks? The General Practi-tioners in Asthma Group. Health Bull(Edinb). 1997;55(3):150–155
63. Coleman CI, Reddy P, Laster-Bradley NM,Dorval S, Munagala B, White CM. Effect ofpractitioner education on adherence toasthma treatment guidelines. Ann Phar-macother. 2003;37(7-8):956–961
64. Richman MJ, Poltawsky JS. Partnership forexcellence in asthma care: evidence-baseddisease management. Stud Health TechnolInform. 2000;76:107–121
65. Suh DC, Shin SK, Okpara I, Voytovich RM,Zimmerman A. Impact of a targeted asthmaintervention program on treatment costs inpatients with asthma. Am J Manag Care.2001;7(9):897–906
66. Baker R, Fraser RC, Stone M, Lambert P,Stevenson K, Shiels C. Randomised con-trolled trial of the impact of guidelines,prioritized review criteria and feedback onimplementation of recommendations forangina and asthma. Br J Gen Pract. 2003;53(489):284–291
67. Schneider A, Wensing M, Biessecker K,Quinzler R, Kaufmann-Kolle P, Szecsenyi J.Impact of quality circles for improvementof asthma care: results of a randomizedcontrolled trial. J Eval Clin Pract. 2008;14(2):185–190
68. Herborg H, Soendergaard B, Jorgensen T,et al. Improving drug therapy for patientswith asthma—part 2: use of antiasthmamedications. J Am Pharm Assoc (Wash).2001;41(4):551–559
69. Søndergaard J, Andersen M, Vach K, KragstrupJ, Maclure M, Gram LF. Detailed postal feed-back about prescribing to asthma patientscombined with a guideline statement showedno impact: a randomised controlled trial. EurJ Clin Pharmacol. 2002;58(2):127–132
REVIEW ARTICLE
PEDIATRICS Volume 132, Number 3, September 2013 533

70. Martens JD, Winkens RA, van der Weijden T,de Bruyn D, Severens JL. Does a joint de-velopment and dissemination of multidis-ciplinary guidelines improve prescribingbehaviour: a pre/post study with concur-rent control group and a randomised trial.BMC Health Serv Res. 2006;6:145
71. Bryce FP, Neville RG, Crombie IK, Clark RA,McKenzie P. Controlled trial of an audit fa-cilitator in diagnosis and treatment ofchildhood asthma in general practice. BMJ.1995;310(6983):838–842
72. Hagmolen of ten Have W, van den Berg NJ,van der Palen J, van Aalderen WM, BindelsPJ. Implementation of an asthma guidelinefor the management of childhood asthmain general practice: a randomised con-trolled trial. Prim Care Respir J. 2008;17(2):90–96
73. Daniels EC, Bacon J, Denisio S, et al.Translation squared: improving asthmacare for high-disparity populations througha safety net practice-based research net-work. J Asthma. 2005;42(6):499–505
74. Lundborg CS, Wahlström R, Oke T, TomsonG, Diwan VK. Influencing prescribing forurinary tract infection and asthma in pri-mary care in Sweden: a randomized con-trolled trial of an interactive educationalintervention. J Clin Epidemiol. 1999;52(8):801–812
75. Cloutier MM, Tennen H, Wakefield DB, BrazilK, Hall CB. Improving clinician self-efficacydoes not increase asthma guideline use byprimary care clinicians. Acad Pediatr. 2012;12(4):312–318
76. Bender BG, Dickinson P, Rankin A, WamboldtFS, Zittleman L, Westfall JM. The ColoradoAsthma Toolkit Program: a practice coachingintervention from the High Plains ResearchNetwork. J Am Board Fam Med. 2011;24(3):240–248
77. Yawn BP, Bertram S, Wollan P. Introductionof asthma APGAR tools improve asthmamanagement in primary care practices.J Asthma Allergy. 2008;(August 31):1–10
78. Lob SH, Boer JH, Porter PG, Núñez D, Fox P.Promoting best-care practices in childhoodasthma: quality improvement in communityhealth centers. Pediatrics. 2011;128(1):20–28
79. Finkelstein JA, Lozano P, Fuhlbrigge AL,et al; Pediatric Asthma Care Patient Out-comes Research Team. Practice-level effectsof interventions to improve asthma carein primary care settings: the PediatricAsthma Care Patient Outcomes ResearchTeam. Health Serv Res. 2005;40(6 pt 1):1737–1757
80. Thyne SM, Marmor AK, Madden N, HerrickG. Comprehensive asthma management forunderserved children. Paediatr PerinatEpidemiol. 2007;21(suppl 3):29–34
81. Halterman JS, Fisher S, Conn KM, et al.Improved preventive care for asthma:a randomized trial of clinician prompting inpediatric offices. Arch Pediatr Adolesc Med.2006;160(10):1018–1025
82. McCowan C, Neville RG, Ricketts IW, WarnerFC, Hoskins G, Thomas GE. Lessons froma randomized controlled trial designed toevaluate computer decision support soft-ware to improve the management ofasthma. Med Inform Internet Med. 2001;26(3):191–201
83. Ragazzi H, Keller A, Ehrensberger R, IraniAM. Evaluation of a practice-based in-tervention to improve the management ofpediatric asthma. J Urban Health. 2011;88(suppl 1):38–48
84. Newton WP, Lefebvre A, Donahue KE, BaconT, Dobson A. Infrastructure for large-scalequality-improvement projects: early les-sons from North Carolina Improving Per-formance in Practice. J Contin Educ HealthProf. 2010;30(2):106–113
85. To T, Cicutto L, Degani N, McLimont S,Beyene J. Can a community evidence-basedasthma care program improve clinicaloutcomes?: a longitudinal study. Med Care.2008;46(12):1257–1266
86. Holton C, Crockett A, Nelson M, et al. Doesspirometry training in general practiceimprove quality and outcomes of asthmacare? Int J Qual Health Care. 2011;23(5):545–553
87. Sulaiman ND, Barton CA, Liaw ST, et al. Dosmall group workshops and locally adaptedguidelines improve asthma patients’ healthoutcomes? A cluster randomized controlledtrial. Fam Pract. 2010;27(3):246–254
88. Frankowski BL, Keating K, Rexroad A, et al;Community collaboration. Community col-laboration: concurrent physician andschool nurse education and cooperationincreases the use of asthma action plans.J Sch Health. 2006;76(6):303–306
89. Glasgow NJ, Ponsonby AL, Yates R, Beilby J,Dugdale P. Proactive asthma care in child-hood: general practice based randomisedcontrolled trial. BMJ. 2003;327(7416):659
90. Patel PH, Welsh C, Foggs MB. Improvedasthma outcomes using a coordinated careapproach in a large medical group. DisManag. 2004;7(2):102–111
91. Homer CJ, Forbes P, Horvitz L, Peterson LE,Wypij D, Heinrich P. Impact of a qualityimprovement program on care and out-comes for children with asthma. ArchPediatr Adolesc Med. 2005;159(5):464–469
92. Fox P, Porter PG, Lob SH, Boer JH, Rocha DA,Adelson JW. Improving asthma-relatedhealth outcomes among low-income, mul-tiethnic, school-aged children: results ofa demonstration project that combinedcontinuous quality improvement and com-munity health worker strategies. Pediatrics.2007;120(4). Available at: www.pediatrics.org/cgi/content/full/120/4/e902
93. Mangione-Smith R, Schonlau M, Chan KS,et al. Measuring the effectiveness of a col-laborative for quality improvement in pe-diatric asthma care: does implementingthe chronic care model improve processesand outcomes of care? Ambul Pediatr. 2005;5(2):75–82
94. Weinberger M, Murray MD, Marrero DG,et al. Effectiveness of pharmacist care forpatients with reactive airways disease:a randomized controlled trial. JAMA. 2002;288(13):1594–1602
95. Renzi PM, Ghezzo H, Goulet S, Dorval E,Thivierge RL. Paper stamp checklist toolenhances asthma guidelines knowledgeand implementation by primary care phy-sicians. Can Respir J. 2006;13(4):193–197
96. Cloutier MM, Grosse SD, Wakefield DB,Nurmagambetov TA, Brown CM. The eco-nomic impact of an urban asthma man-agement program. Am J Manag Care. 2009;15(6):345–351
534 OKELO et al
Related Documents











