Surgical Innovation 17(2) 142–158 © The Author(s) 2010 Reprints and permission: http://www. sagepub.com/journalsPermissions.nav DOI: 10.1177/1553350610370968 http://sri.sagepub.com International Multicenter Trial on Clinical Natural Orifice Surgery—NOTES IMTN Study: Preliminary Results of 362 Patients Ricardo Zorron, MD,PhD, 1 Chinnusamy Palanivelu, MD, 2 Manoel Passos Galvão Neto, MD, 3 Almino Ramos, MD, 3 Gustavo Salinas, MD, 4 Jens Burghardt, MD, 5 Luis DeCarli, MD, 6 Luiz Henrique Sousa, MD, 7 Antonello Forgione, MD, 8,18 Raffaele Pugliese, MD,PhD, 8,18 Alcides J Branco, MD, 9 T. S. Balashanmugan, MD, 10 Camilo Boza, MD, 11 Francesco Corcione, MD, 12 Fausto D’Ávila Avila, MD, 13 Néstor Arturo Gómez, MD, 14 Paulo Ayrosa Galvão Ribeiro, MD, 3 Susana Martins, MD, 15 Marcos Filgueiras, MD, 1 Klaus Gellert, MD, 5 Anibal Wood Branco, MD, 9 William Kondo, MD, 9 Jose Inacio Sanseverino, MD, 6 José Américo G. de Sousa, MD, 7 Lil Saavedra, MD, 4 Edwin Ramírez, MD, 4 Josemberg Campos, MD, 16 K. Sivakumar, MD, 10 Pidigu Seshiyer Rajan, MD, 2 Priyadarshan Anand Jategaonkar, MD, 2 Muthukumaran Ranagrajan, MD, 2 Ramakrishnan Parthasarathi, MD, 2 Palanisamy Senthilnathan, MD, 2 Mohan Prasad, MD, 2 Diego Cuccurullo, MD, 17 and Verena Müller, MD 5 Abstract Objectives: Natural orifice translumenal endoscopic surgery (NOTES) is evolving as a promising alternative for abdominal surgery. IMTN Registry was designed to prospectively document early results of natural orifice surgery among a large group of clinical cases. Methods: Sixteen centers from 9 countries were approved to participate in the study, based on study protocol requirements and local institutional review board approval. Transgastric and transvaginal endoscopic natural orifice surgery was clinically applied in 362 patients. Intraoperative and postopera- tive parameters were prospectively documented. Results: Mean operative time for transvaginal cholecystectomy was 96 minutes, compared with 111 minute for transgastric cholecystectomy. A general complication rate of 8.84% was recorded (grade I-II representing 5.8%, grade III-IV representing 3.04%). No requirement for any analgesia was found in one fourth of cholecystectomy and appendectomy patients. Conclusions: Results of clinical applications of NOTES in the IMTN Study showed the feasibility of different methods of this new minimally invasive alternative for laparoscopic and open surgery. Keywords natural orifice surgery, NOTES, laparoscopy, minimally invasive surgery, natural orifice translumenal endoscopic surgery, prospective study, multicenter study, cholecystectomy, appendectomy Introduction Natural orifice translumenal endoscopic surgery (NOTES) is an evolving concept of combination of techniques of mini- mally invasive surgery with flexible endoscopy, potentially representing a major paradigm shift to scarless surgery. With the aim of avoiding incision-related complications, researchers have made efforts to create even less invasive access by means of translumenal surgery. In the pioneering descriptions on endoscopic transgastric (TG) surgery,

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Surgical Innovation17(2) 142 –158© The Author(s) 2010Reprints and permission: http://www. sagepub.com/journalsPermissions.navDOI: 10.1177/1553350610370968http://sri.sagepub.com
International Multicenter Trial on Clinical Natural Orifice Surgery—NOTES IMTN Study: Preliminary Results of 362 Patients
Ricardo Zorron, MD,PhD,1 Chinnusamy Palanivelu, MD,2 Manoel Passos Galvão Neto, MD,3 Almino Ramos, MD,3 Gustavo Salinas, MD,4 Jens Burghardt, MD,5 Luis DeCarli, MD,6 Luiz Henrique Sousa, MD,7 Antonello Forgione, MD,8,18 Raffaele Pugliese, MD,PhD,8,18 Alcides J Branco, MD,9 T. S. Balashanmugan, MD,10 Camilo Boza, MD,11 Francesco Corcione, MD,12 Fausto D’Ávila Avila, MD,13 Néstor Arturo Gómez, MD,14 Paulo Ayrosa Galvão Ribeiro, MD,3 Susana Martins, MD,15 Marcos Filgueiras, MD,1 Klaus Gellert, MD,5 Anibal Wood Branco, MD,9 William Kondo, MD,9 Jose Inacio Sanseverino, MD,6 José Américo G. de Sousa, MD,7 Lil Saavedra, MD,4 Edwin Ramírez, MD,4 Josemberg Campos, MD,16 K. Sivakumar, MD,10 Pidigu Seshiyer Rajan, MD,2 Priyadarshan Anand Jategaonkar, MD,2 Muthukumaran Ranagrajan, MD,2 Ramakrishnan Parthasarathi, MD,2 Palanisamy Senthilnathan, MD,2 Mohan Prasad, MD,2 Diego Cuccurullo, MD,17 and Verena Müller, MD5
AbstractObjectives: Natural orifice translumenal endoscopic surgery (NOTES) is evolving as a promising alternative for abdominal surgery. IMTN Registry was designed to prospectively document early results of natural orifice surgery among a large group of clinical cases. Methods: Sixteen centers from 9 countries were approved to participate in the study, based on study protocol requirements and local institutional review board approval. Transgastric and transvaginal endoscopic natural orifice surgery was clinically applied in 362 patients. Intraoperative and postopera-tive parameters were prospectively documented. Results: Mean operative time for transvaginal cholecystectomy was 96 minutes, compared with 111 minute for transgastric cholecystectomy. A general complication rate of 8.84% was recorded (grade I-II representing 5.8%, grade III-IV representing 3.04%). No requirement for any analgesia was found in one fourth of cholecystectomy and appendectomy patients. Conclusions: Results of clinical applications of NOTES in the IMTN Study showed the feasibility of different methods of this new minimally invasive alternative for laparoscopic and open surgery.
Keywordsnatural orifice surgery, NOTES, laparoscopy, minimally invasive surgery, natural orifice translumenal endoscopic surgery, prospective study, multicenter study, cholecystectomy, appendectomy
Introduction
Natural orifice translumenal endoscopic surgery (NOTES) is an evolving concept of combination of techniques of mini-mally invasive surgery with flexible endoscopy, potentially representing a major paradigm shift to scarless surgery. With the aim of avoiding incision-related complications, researchers have made efforts to create even less invasive access by means of translumenal surgery. In the pioneering descriptions on endoscopic transgastric (TG) surgery,

Zorron et al. 143
Kalloo, Kantsevoy, and coworkers showed the possibilities of transpassing the gastric wall and operating in an animal model using a perorally introduced flexible endoscope via a sterile overtube in the abdominal cavity.1,2 Other research-ers described TG cholecystectomy, tubal ligation, oopho-rectomy, gastroenterostomy, and splenectomy in animal experiments.3-6 Human TG appendectomy was also clini-cally presented in meetings by Rao and Reddy using avail-able endoscopic instruments since 2005.7,8 Transvaginal (TV) NOTES provides easy access, direct vision closure, availability of instruments, and a well-known access with reasonable disinfection possibility. In fact, world experience in human, restricted to ethically approved studies, is grow-ing, particularly in the field of TV and TG access.9,10
Although human casuistic of natural orifice surgery is becoming more widely used, isolated studies have still small numbers of patients worldwide, and the design of larger series and comparative studies to evaluate early results and indications of natural orifice surgery techniques is desirable. IMTN Study (International Prospective Multicenter Trial on Clinical NOTES) is designed as a multi-institutional prospective documentation registry started in Brazilian centers in July 2007, and accepting international data since then, aiming to provide information regarding early post-operative results and complications of natural orifice surgery worldwide. Preliminary prospective data collected from 362 patients for TV and TG NOTES are described.
MethodsBrazilian and international natural orifice surgery cases were registered in a prospective database. Inclusion criteria for
accepting the authorized centers were the following: (a) must prove work as a multidisciplinary team including gastroenterology/endoscopy specialist, (b) must have previ-ous animal research with veterinary facility, (c) flexible endoscopic experience, and (d) local institutional review board approval for human trials in the pretended field of natural orifice surgery. IMTN Registry started accepting NOTES cases from Brazilian centers since July 2007, and since then several international centers were invited and joined the prospective documentation of TV, TG, and trans-colonic cases. Latin American research centers joined the IMTN Study in 2007, and other international centers, such as India, Italy, and Germany, were also accepted in the study in 2008. The main reason for not including prospective results from other countries that also actively initiated human NOTES experience is that these centers were reporting their results in their own prospective registry (eg, NOSCAR). The database accepted statements of individually approved human trials and signed informed consent by the institutional ethical committees in each center for natural orifice surgery clinical trials and by personal statement from each study local coordinator; all methods were in accordance with the Helsinki Declaration, revision 1989. The IMTN Clinical Trial database is registered under the Protocol ID 0209.0.314.000-08, ClinicalTrials.gov ID NCT00995735 in a free, publicly accessible, nonprofit electronically search-able database administered by the National Library of Medi-cine (located at http://www.clinicaltrials.gov).
International centers and responsible coordinators par-ticipating in the IMTN Study are listed in Table 1. All par-ticipants included their prospective results of new cases every 3 months by electronic input, and late results were
1University Hospital Teresopolis HCTCO-FESO, Rio de Janeiro, Brazil2GEM Hospital and Postgraduate Institute, Coimbatore, India3Hospital Santa Rita, São Paulo, Brazil4Clínica de Día Avendaño, Lima, Peru5Sana Clinical Center Berlin, Berlin, Germany6Hospital Irmandade Santa Casa da Misericordia, Porto Alegre, Brazil7SOUSAGROUP Hospital Femina, Goiania, Brazil8Niguarda Ca’ Granda Hospital, Milan, Italy9Cruz Vermelha Hospital Curitiba, Parana, Brazil10PSG Hospital, Coimbatore, India11Pontificia Universidad Católica del Chile, Santiago, Chile12Hospital UOC General and Laparoscopic Surgery, Naples, Italy13Hospital Poza Rica, Poza Rica, Mexico14Universidad de Guayaquil, Guayaquil, Ecuador15Foster City, CA, USA16University Recife, Recife, Brazil17NOC Chirugia Generale e Laparoscopica, Naples, Italy18AIMS – Advanced International Mini-invasive Surgery Academy, Milan, Italy
Corresponding Author:Ricardo Zorron, MD, PhD, Department of Surgery, University Hospital Teresopolis HCTCO-FESO, NOTES Research Group, Rio de Janeiro, BrazilEmail: [email protected]
144 Surgical Innovation 17(2)
included before the completion of the statistics. Thirty-day results were the main goal for the study, which included all early postoperative complications. Many participants also
sent single-port surgery experiences, but these cases were not computed in the study. Study protocol criteria of inclu-sion were patients with low ASA risk (I-II), who could
Table 1. Participating Centers of IMTN Study
Participating Center/Department Country Responsible Local Coordinators
1. Department of Surgery, University Hospital Teresopolis HCTCO-FESO, Rio de Janeiro
Brazil Coordinator: Ricardo Zorron
Marcos Filgueiras, Luis Carlos Maggioni, Monica Soldan 2. Department of Surgery, Hospital Irmandade
Santa Casa da Misericordia Porto AlegreBrazil Coordinator: Luiz DeCarli
Fernando Cirme Lima, Marcus Tang, Sergio Pioneer, Jose Inácio Sanseverino, Idílio Zanin Jr, Rodrigo Menguer, Andre Bigolin
3. Department of Surgery, Cruz Vermelha Hospital Curitiba, Parana
Brazil Coordinator: Alcides J. Branco
Aníbal Wood Branco, Rafael Noda, William Kondo, Nilton Kawahara
4. Department of Surgery, Gastrobeso Center, Hospital Santa Rita, São Paulo
Brazil Coordinator: Manuel Galvao
Almino Ramos, Paulo Ayrosa 5. Department of Surgery and Endoscopy,
SOUZAGROUP Hospital Femina, GoianiaBrazil Coordinator: Luiz Henrique de Sousa
José Américo Gomides de Sousa, Murilo Miranda de Sousa, Vitor Miranda de Sousa, Ana Patricia Miranda de Sousa
6. Department of Surgery, Universidade de Recife
Brazil Coordinator: Josemberg Campos
7. Clinica de Dia Avendaño, Lima Peru Coordinator: Gustavo SalinasLil Saavedra, Edwin Ramirez
8. Department of Surgery, PSG Hospital, Coimbatore
India Coordinator: T. S. Balashanmugan
K. Sivakumar 9. Department of Surgery, GEM Hospital and
Postgraduate Institute, CoimbatoreIndia Coordinator: Chinnusamy Palanivelu
Pidigu Seshiyer Rajan, Priyadarshan Anand Jategaonkar, Muthukumaran Ranagrajan, Ramakrishnan Parthasarathi, Palanisamy Senthilnathan, Mohan Prasad
10. Department of General and Emergency Surgery, Niguarda Ca’ Granda Hospital, Milan, Italy and AIMS – Advanced International Mini-invasive Surgery Academy, Milan, Italy
Italy Coordinator: Antonello Forgione
Raffaele Pugliese11. Department of Surgery, HOSPITAL UOC
General and Laparoscopic Surgery, AO Monaldi, Naples
Italy Coordinator: Francesco Corcione
Diego Cuccurullo12. Department of General Surgery, Sana
Clinical Center Berlin (Evangelisch-Freikirchliches Krankenhaus Rüdersdorf, Berlin)
Germany Coordinator: Jens Burghardt
Klaus Gellert, Verena Müller, Hendrick Freund, Mathias Federlein13. Department of Surgery, Hospital Poza Rica Mexico Coordinator: Fausto D’Ávila Ávila
José Lemus, Daniel Tsin14. Hospital “Kennedy,” Policentro, Facultad de
Medicina, Universidad de GuayaquilEcuador Coordinator: Néstor Arturo Gómez
15. Department of Surgery, Pontifícia Universidad Católica del Chile
Chile Coordinator: Camilo Boza
16. Hospital Universitario Abel Santamaria Cuadrado, Pinar del Rio
Cuba Coordinator: Raul Castro Perez

Zorron et al. 145
choose natural orifice procedure instead of laparoscopy. Inclusion criteria of the patients in most centers were based on mild preoperative symptoms and short duration of dis-ease. Patients with previous history of hysterectomy were avoided because of possibility of failure of TV access. Patients with previous abdominal surgery were commonly avoided, but some centers accepted a high rate of abdominal operations, not considering previous operations as contra-indication for NOTES. The research groups consisted of multidisciplinary teams of surgeons, gastroenterologists, endoscopists, gynecologists, and veterinary surgeons for the experimental background. Flexible endoscopes were previously submitted to sterilization by ethylene oxide, and in some centers, high-level disinfection was obtained by immersion in glutaraldhyde 2% or peracetic acid 3% solu-tion. A veterinary hospital facility was available, and natural orifice surgery technical possibilities were tested by the study groups in each international participant. At the begin-ning of recruitment for the study, 2 centers were not approved to join IMTN Study based on absence of 1 or more preconditions.
Intraoperative and postoperative data were prospec-tively documented until the 30th-day postoperative follow-up. Long-term postoperative data are also collected for future evaluation. Postoperative complications were pro-spectively recorded based on scores grading initially pro-posed by Clavien et al in 199211 and modified by Dindo et al in 2004.12 Mild discomfort, pain, and other postopera-tive symptoms were recorded as side effects. Conversion from NOTES to laparoscopic surgery was defined as unplanned installation of trocars and use of laparoscopic optic and dissection. Conversion to open surgery was defined of unplanned abdominal incision to perform the operation or specimen extraction. Hybrid NOTES tech-nique was defined as use of 1 or more laparoscopic trocars for assistance, because main dissection and visualization was performed by natural orifice access.
Surgical TechniqueTransvaginal Surgery
Patients were submitted to general anesthesia and installed in a Lloyd–Davies position. Disinfection of the vagina was achieved by topical iodopovidone or chlorhexidine solution, and urinary catheter was installed. Most of the participating centers recommended antibiotic prophylaxis. Usually, a single dose of intravenous bolus of either 2 g cefalexin or a combination of 400 mg metronidazol and 400 mg cipro-floxacin were given at the induction of anesthesia. Some specialists used previous abdominal insufflation with CO2 performed after introduction of a Veress needle in the left
subcostal abdomen or in the umbilicus, to allow a safe entry into the abdominal cavity through the vagina. Other groups in the study achieved good results by accessing directly the cavity through a direct view vaginal access. Incision of vaginal posterior sac was done after traction of the cervix with a conventional instrument. The operator was positioned between the legs of the patient, and the first assistant behind and holding the controls of the endoscope. A second assis-tant took position on the left side of the patient if laparo-scopic assistance was used. Insufflation of the cavity with CO2 was maintained by most groups using a laparoflator to provide control of the pressure, either by TV trocar or through a Veress needle. After insufflation, the orientation of the endoscope in the cavity was possible by initial local-ization of the abdominal wall and abdominal organs using a reverse Trendelemburg position.
Transvaginal Access and Closure—Method 1: Direct Vision Open AccessOpening of the posterior vaginal sac was done under direct vision with conventional instruments and facilitated access to the peritoneal cavity. A Sims speculum was inserted in the vagina, and the posterior lip of the cervix was grasped by a Pozzi clamp. The vaginal walls were retracted by 2 lateral retractors, and anterior traction was given to the cervix to stretch the posterior fornix. The vaginal mucosa in the posterior cul-de-sac was opened at the cervico-vaginal junction by a semilunar 2.5-cm incision. The posterior mar-gin was grasped by an Allis forceps, and sharp dissection was performed with scissors. The posterior cul-de-sac peri-toneum was identified and opened. CO2 was insufflated through the smallest working channel of the endoscope using a laparoscopic insufflator. Vaginal wound was closed using absorbable running suture under direct vision.
Transvaginal Access and Closure—Method 2: Laparoscopic Camera AssistanceThe surgeon was placed standing between the patient’s legs; the first and second assistants stand on the left and right sides of the patient, respectively. In this setting, 2 visualization systems, one for the abdominal laparoscopic camera and the other for the TV flexible endoscope, were used. The procedure started with a Veress puncture through an incision in the umbilicus to avoid a visible scar. Pneu-moperitoneum was then induced through the Veress needle. A 5-mm trocar is inserted, and a 5-mm laparoscopic optic used to inspect the abdominal cavity. To avoid the risk of injuring pelvic organs, the team performed a thorough examination of the pelvis, looking for adhesions that might prohibit the TV cul-de-sac puncture. In patients who had

146 Surgical Innovation 17(2)
had a previous hysterectomy, or unknown endometriosis, adhesions obliterating the pouch of Douglas contraindi-cated the further vaginal insertion of the trocar and conver-sion to formal laparoscopy was usually indicated. After inventory, a longer 10- to 12-mm laparoscopic trocar was inserted in the vaginal posterior cul-de-sac under laparo-scopic guidance. The endoscope was progressed after extraction of the laparoscopic trocar. Vaginal wound closure was performed in the same way as described previously, and the diameter of the wound was smaller (1-1.5 cm) than the direct vaginal access (2-3 cm).
Transvaginal CholecystectomyFour distinct techniques for NOTES TV cholecystectomy were described by the different centers, regarding pure natural orifice surgery or combined hybrid techniques to allow efficiency and safety for the procedures.
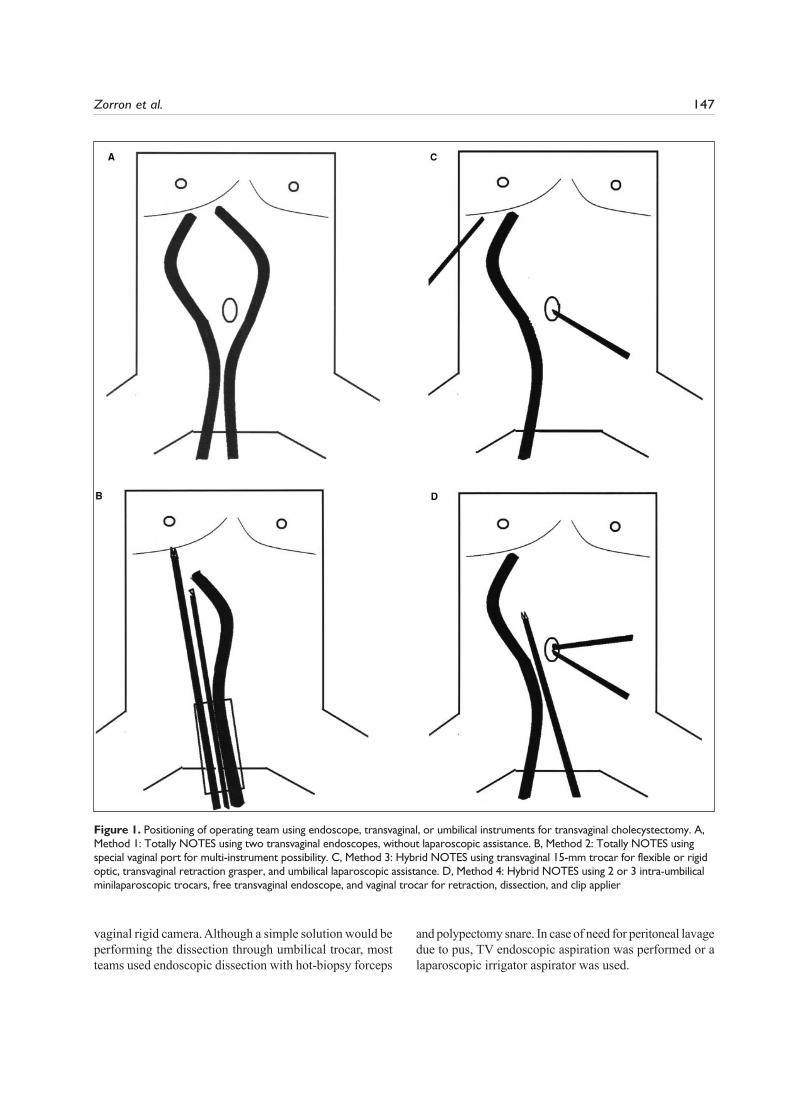
Method 1: Totally NOTES dual scope method. After pos-terior colpotomy using direct view and conventional instruments, safe open access to the peritoneal cavity was obtained. The ideal final incision diameter was 2.5 cm for the introduction of 2 endoscopes (Figure 1A). The first endoscope (single-channel gastroscope) with the insuf-flation tube attached was inserted in the orifice created. After pneumoperitoneum with CO2 was achieved, the sec-ond endoscope (double-channel colonoscope) was inserted through the same orifice. Abdominal pressure was main-tained between 9 and 10 mm Hg of CO2 and controlled by a laparoscopic insufflator. There was no use of laparoscopic camera or instruments in any case. The endoscope for retraction and insufflation was situated on the right, and an endoscopic strange body extraction grasper was used to keep the gallbladder retracted under tension, providing triangulation of instruments.
After retraction with the first endoscope, the second operating/visualization 2-channel endoscope was posi-tioned about 4 to 5 cm close to the retracted gallbladder with orientation of the first endoscope. After orientation and after the endoscope passed the pelvic organs, the position of the patient was changed to a reverse Tren-delemburg position, allowing visualization of the upper abdomen. Dissection of Calot’s Triangle was performed using endoscopic instruments such as hot-biopsy forceps, polipectomy snare, and endoscopic hook. Cystic duct and artery were dissected and clipped using endoscopic clips, 2 proximal and 1 distal. After transection of the duct and artery with endoscopic scissors, the gallbladder was dissected from the liver bed using polipectomy snare, the instrument also used for vaginal extraction of the specimen. After delivery of the gallbladder, pneumoperi-toneum was aspirated before the exit of the second endoscope.
Method 2: Transvaginal multipurpose port with flexible surgery (Figure 1B). In one group, main vaginal access and dissection was obtained by a TV port (local adapted trocar) that permitted independent entry of the flexible endoscope (double-channel colonoscope), insufflation channel from a laparoflator, and semiflexible instruments used for retrac-tion, cutting, and clipping using TV laparoscopic titanium clips. Dissection was accomplished by flexible endoscopic instruments available such as as polipectomy snares and hot-biopsy forceps. After TV extraction of the specimen and port, pneumoperitoneum was aspirated transvaginally, and closure was performed using absorbable sutures.
Method 3: Hybrid NOTES with transvaginal and abdominal laparoscopy. Laparoscopy was used in this technique for purposes such as safe access, visualization, and dissection, usually accomplished by endoscopic instruments or lapa-roscopy (Figure 1C). Avoiding maximally the difficult endo-scopic dissection and instrumentation, this method allowed for faster operations in a similar laparoscopic critical view.
Method 4: Transvaginal trocars (flexible or rigid optic) com-bined with umbilical minilaparoscopy. Pneumoperitoneum was achieved by umbilical Veress needle puncture, and abdominal pressure was maintained between 8 and 15 mm Hg of CO2 and controlled by a laparoscopic insufflator. After insufflation, opening of the posterior vaginal cul-de-sac was performed by direct vision and dissection through vaginal speculum and use of monopolar incision and long scissors.
After colpotomy, a 1- or 2-channel gastroscope was introduced in the abdominal cavity. After orientation and after endoscope passed the pelvic organs, the position of the patient was changed to a reverse Trendelemburg, allow-ing visualization of the upper abdomen. By retroflected view, a specially designed long trocar (10 mm) was placed in the vagina, parallel to the endoscope. Two 3-mm trocars were placed intra-umbilically under direct endoscopic vision (Figure 1D). Dissection of Calot’s Triangle was per-formed using endoscopic instruments such as hot-biopsy forceps, polipectomy snares, endoscopic hook, and the umbilical 3-mm instruments. Cystic duct and artery were dissected and clipped using long laparoscopic clipator through the vaginal trocar. After transection of the duct and artery, the gallbladder was dissected from the liver bed using endoscopic hook or polipectomy snare. Extraction of the specimen was achieved by long laparoscopic graspers inserted in the vaginal trocar.
Transvaginal AppendectomyNOTES appendectomies through vaginal access were per-formed using direct access to the cavity with or without umbilical laparoscopic assistance. Usually the appendix could be managed without endoscopic retroflection, or using
Zorron et al. 147
vaginal rigid camera. Although a simple solution would be performing the dissection through umbilical trocar, most teams used endoscopic dissection with hot-biopsy forceps
and polypectomy snare. In case of need for peritoneal lavage due to pus, TV endoscopic aspiration was performed or a laparoscopic irrigator aspirator was used.
Figure 1. Positioning of operating team using endoscope, transvaginal, or umbilical instruments for transvaginal cholecystectomy. A, Method 1: Totally NOTES using two transvaginal endoscopes, without laparoscopic assistance. B, Method 2: Totally NOTES using special vaginal port for multi-instrument possibility. C, Method 3: Hybrid NOTES using transvaginal 15-mm trocar for flexible or rigid optic, transvaginal retraction grasper, and umbilical laparoscopic assistance. D, Method 4: Hybrid NOTES using 2 or 3 intra-umbilical minilaparoscopic trocars, free transvaginal endoscope, and vaginal trocar for retraction, dissection, and clip applier

148 Surgical Innovation 17(2)
Transgastric Surgery
The patient was submitted to general anesthesia and installed in a Lloyd–Davies position. Disinfection of the gastric lumen was achieved by intraoperative washing with clorohexidine solution, but some centers used no special cleaning besides aspiration. Use of esophageal overtubes usually protected against esophageal trauma due to instrumentation, but they were not widely used. As laparoscopic gastric suture was the method of choice to close the gastric wound after the procedure, insertion of an umbilical laparoscopic optic was the first step of the operations, allowing safe translumenal entrance of the endoscope in the abdominal cavity. Speci-mens were extracted without special bags, and when the specimen diameter exceeded the diameter of the esophagus, open conversion by umbilical opening and extraction was the solution. Usually 3 trocars were used to close the gastric wound, but in 2 centers, one trocar was used for a 3-mm camera and another 5-mm trocar was used to perform the sutures using external knotting. Endoscopic closure was used early by some of the groups using endoscopic clips for gastric closure in TG cases, but this early casuistic was not included by the study, as it started with prospective registry later. Other TG closure methods and technology were not available for use by any of the contributing centers.
Transgastric cholecystectomies were performed using either endoscopic dissection or by laparoscopic dissection. One 3-mm umbilical trocar was placed at the umbilicus for guiding the endoscope’s safe transgatric exit under vision and, later, for retracting the fundus. At the end of the proce-dure, one more 3-mm trocar was inserted in the right para-rectus region. Two centers reported the use of 2 and 3 trocars. The gastrotomy wound was sutured “single handedly” by inserting a needle holder through this trocar and a 3-mm laparoscope through the umbilical trocar. This closure was also monitored by the endoscope, which was withdrawn and kept in the gastric lumen while the bytes were taken. The use of an additional trocar in the right pararectus region allowed the achievement of a secured gastrotomy closure.
Transgastric appendectomies were performed using ini-tially a 3- or 5-mm umbilical trocar in the beginning of the surgery for guiding the operating endoscope’s TG exit into the peritoneal cavity under vision. The same trocar was later used for retracting the appendix. All the steps were usually performed without using any other extra trocars till the extraction of the specimen. At that juncture, a 5-mm right pararectal trocar was inserted for securely closing the gastrotomy wound by deploying extracorporeal knots.
Special MethodsTransvaginal cases for cancer staging were less complex procedures, usually using only the endoscope without
laparoscopic assistance and performing retraction and biopsies using endoscopic hot-biopsy forceps through the working channels. TV nephrectomy, TV sleeve gastrec-tomy, and more complex cases were performed with sig-nificant laparoscopic dissection because of lack of advanced endoscopic technology, such as long and flexible stapler devices and graspers.
International centers reported new cases performed every 3 months, and the prospective database was maintained in the leading center by the main author responsible (RZ). Operative and postoperative data including operative time, blood loss, intraoperative complications, intra-abdominal pressures, end-tidal (expiratory) CO2, reasons for conver-sion to laparoscopic or open surgery, length of postoperative hospital stay, morbidity, 30-day morbidity and mortality, general data, and reason for reoperation were also collected. Statistical differences in categorical variables were analyzed by the F2 test, and differences in continuous variables were analyzed by Student’s t test.
ResultsA total of 362 patients were prospectively documented until June 30, 2009. Indications for NOTES surgery and the method of access were different between the centers, with the majority performing TV access, and only 4 centers reporting TG procedures also (see Table 2). TV NOTES cholecystectomy was the main indication in the study (240 cases), followed by TV appendectomy (37), TG cholecys-tectomy (29), TV colectomy (13), TV sleeve gastrectomy (5), TV cancer staging (8), TG appendectomy (14), TV nephrectomy (4), TV hepatic cyst extraction (1), and TV gynecologic surgery (11). Overall, the complication rate
Table 2. Indications and Access for NOTES Surgery in 362 Patients
Patients
Type of Procedure n Percentage
TV cholecystectomy 240 66.3TV appendectomy 37 10.2TG cholecystectomy 29 8.01TG appendectomy 14 3.87TV rectosigmoidectomy 12 3.31TV gynecologic surgery 11 3.03TV cancer staging 8 2.2TV sleeve gastrectomy 5 1.38TV nephrectomy 4 1.10TV right colectomy 1 0.28TV hepatic cyst 1 0.28Total 362 100
Note: NOTES= natural orifice translumenal endoscopic surgery; TV= transvaginal; TG, transgastric.
Zorron et al. 149
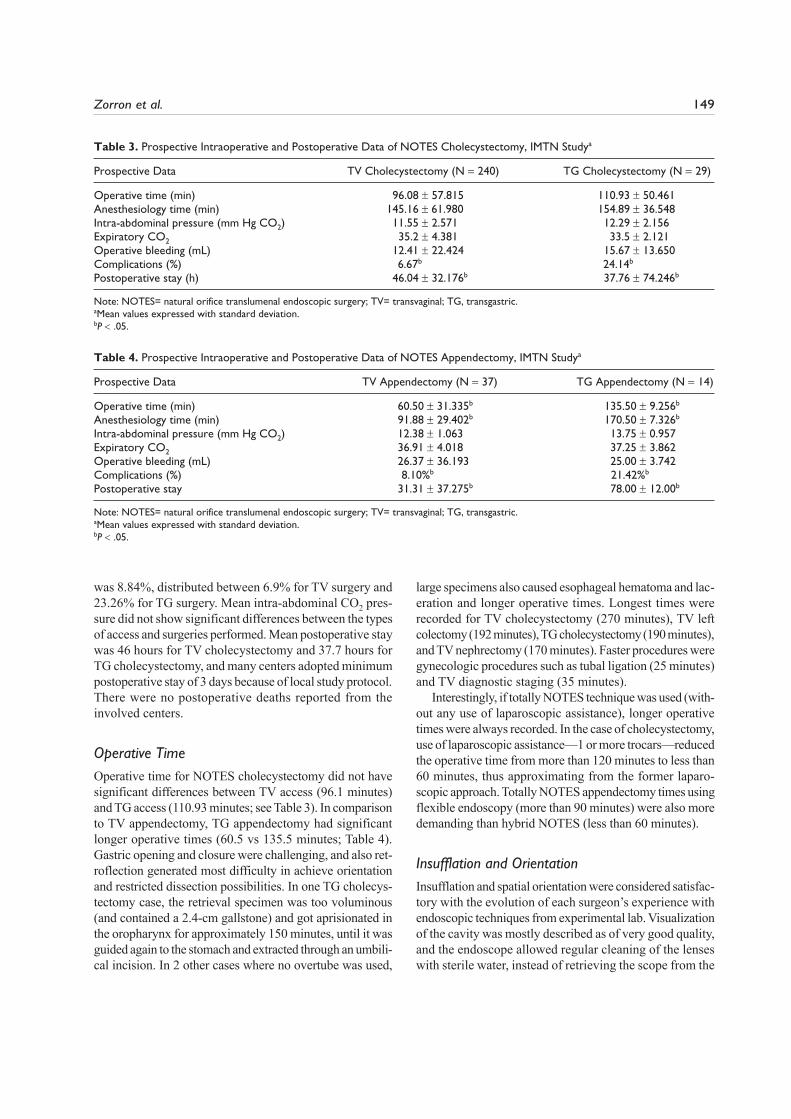
was 8.84%, distributed between 6.9% for TV surgery and 23.26% for TG surgery. Mean intra-abdominal CO2 pres-sure did not show significant differences between the types of access and surgeries performed. Mean postoperative stay was 46 hours for TV cholecystectomy and 37.7 hours for TG cholecystectomy, and many centers adopted minimum postoperative stay of 3 days because of local study protocol. There were no postoperative deaths reported from the involved centers.
Operative TimeOperative time for NOTES cholecystectomy did not have significant differences between TV access (96.1 minutes) and TG access (110.93 minutes; see Table 3). In comparison to TV appendectomy, TG appendectomy had significant longer operative times (60.5 vs 135.5 minutes; Table 4). Gastric opening and closure were challenging, and also ret-roflection generated most difficulty in achieve orientation and restricted dissection possibilities. In one TG cholecys-tectomy case, the retrieval specimen was too voluminous (and contained a 2.4-cm gallstone) and got aprisionated in the oropharynx for approximately 150 minutes, until it was guided again to the stomach and extracted through an umbili-cal incision. In 2 other cases where no overtube was used,
large specimens also caused esophageal hematoma and lac-eration and longer operative times. Longest times were recorded for TV cholecystectomy (270 minutes), TV left colectomy (192 minutes), TG cholecystectomy (190 minutes), and TV nephrectomy (170 minutes). Faster procedures were gynecologic procedures such as tubal ligation (25 minutes) and TV diagnostic staging (35 minutes).
Interestingly, if totally NOTES technique was used (with-out any use of laparoscopic assistance), longer operative times were always recorded. In the case of cholecystectomy, use of laparoscopic assistance—1 or more trocars—reduced the operative time from more than 120 minutes to less than 60 minutes, thus approximating from the former laparo-scopic approach. Totally NOTES appendectomy times using flexible endoscopy (more than 90 minutes) were also more demanding than hybrid NOTES (less than 60 minutes).
Insufflation and OrientationInsufflation and spatial orientation were considered satisfac-tory with the evolution of each surgeon’s experience with endoscopic techniques from experimental lab. Visualization of the cavity was mostly described as of very good quality, and the endoscope allowed regular cleaning of the lenses with sterile water, instead of retrieving the scope from the
Table 3. Prospective Intraoperative and Postoperative Data of NOTES Cholecystectomy, IMTN Studya
Prospective Data TV Cholecystectomy (N 240) TG Cholecystectomy (N 29)
Operative time (min) 96.08 r 57.815 110.93 r 50.461Anesthesiology time (min) 145.16 r�61.980 154.89 r 36.548Intra-abdominal pressure (mm Hg CO2) 11.55 r 2.571 12.29 r 2.156Expiratory CO2 35.2 r 4.381 33.5 r 2.121Operative bleeding (mL) 12.41 r 22.424 15.67 r 13.650Complications (%) 6.67b 24.14b
Postoperative stay (h) 46.04 r 32.176b 37.76 r 74.246b
Note: NOTES= natural orifice translumenal endoscopic surgery; TV= transvaginal; TG, transgastric.aMean values expressed with standard deviation.bP � .05.
Table 4. Prospective Intraoperative and Postoperative Data of NOTES Appendectomy, IMTN Studya
Prospective Data TV Appendectomy (N 37) TG Appendectomy (N 14)
Operative time (min) 60.50 r 31.335b 135.50 r 9.256b
Anesthesiology time (min) 91.88 r 29.402b 170.50 r 7.326b
Intra-abdominal pressure (mm Hg CO2) 12.38 r 1.063 13.75 r 0.957Expiratory CO2 36.91 r 4.018 37.25 r 3.862Operative bleeding (mL) 26.37 r 36.193 25.00 r 3.742Complications (%) 8.10%b 21.42%b
Postoperative stay 31.31 r 37.275b 78.00 r 12.00b
Note: NOTES= natural orifice translumenal endoscopic surgery; TV= transvaginal; TG, transgastric. aMean values expressed with standard deviation.bP � .05.

150 Surgical Innovation 17(2)
cavity. Laparoscopic transumbilical camera was used in some instances for TV surgery, and all cases of TG surgery, allowing safety and faster orientation than direct orificial access. TG endoscopic retroflected visualization was cor-rected by changing the positioning of the endoscope, chang-ing the positioning of the monitor, or correcting the “mirror effect” by computer software. CO2 was the gas of choice to insufflate NOTES surgery, and pressures of 5 to 15 mm Hg were used, with no difference between TV and TG cases. Also, mean CO2 pressures less than 10 mm Hg were not constantly used (Tables 3 and 4). Accidentally, in 2 cases air was insufflated by the operator of the endoscope, leading to abdominal pressures of nearly 30 mm Hg for short peri-ods, with no morbidity associated. In the cases when any abdominal trocar was inserted, insufflation trough the trocar or a Veress needle was preferred. Translumenal endoscopic insufflation was obtained usually by attaching a laparoflator to a working channel of the endoscope, by tying an insuf-flation tube to the endoscope, by a special vaginal port that allowed insufflation, or by insertion of a vaginal trocar. Of these methods, the method using working channels to insuf-flate CO2 was the only to introduce special problems because of low flux and sometimes bad exposition due to obstruction of the channel by fluids and low inflow.
Surgeon Versus GastroenterologistMain subjective questioning regarding the multidisci-plinary aspect of the team showed predominance of the surgeon performing the operation, with a gastroenterolo-gist responsible for part of dissecting, cutting, and clipping in a few centers. A minority of the NOTES teams were not composed of any gastroenterologist-endoscopist, as the surgeon was a skilled endoscopist or colonoscopist himself in these centers.
ConversionConversion to full laparoscopy was defined as insertion of unplanned trocars and significant use of laparoscopic dissection, clipping, or camera, and occurred in 6 patients due to difficult exposure, bleeding of appendiceal or cystic vessels, or adhesions from previous surgery. Conversion to open surgery occurred in 3 cases in the study. In the first, TG access led to important hemorrhage from epiploic ves-sels and required open conversion and ligature control, with no postoperative morbidity. In 2 other patients submitted to TG cholecystectomy with large stones (!2.4 cm), extrac-tion of the specimen through the mouth was an important issue. In one of them, after an uneventful procedure, the team tried to retrieve the specimen, which was stuck in the proximal esophagus/oropharynx. The gallbladder and stone remained blocked in place, and many methods were tried
to solve the problem, such as laringoscopy with tentative transoral grasping, breaking the stone, and variable delivery maneuvers. The solution was to return the gallbladder to the stomach and to the abdominal cavity and then to extract the specimen through an umbilical open incision.
ComplicationsIntraoperative complications occurred in 5.8% patients, and postoperative complications occurred in 3.04% of the patients (see Tables 5 and 6). The prospective docu-mentation grade of surgical complications followed the scores initially proposed by Clavien in 199211 and modi-fied in 2004 (Clavien–Dindo classification12). Complica-tions were recorded in 32 patients (8.84%) and stratified in grades I to IV according to the Clavien–Dindo clas-sification and were represented by intraoperative and postoperative complications. Reoperations were necessary for 5 patients because of the following: (a) Peritonitis—in 1 case of TG cholecystectomy, the patient was readmitted on the fifth postoperative day due to diffuse abdominal pain and distension. Laparoscopy was performed and diffuse peritonitis due to Streptococcus faecalis was found, but without gastric fistulae and clean cystic duct stump and gastric closure site. Abdominal fluid aspiration and washing with saline solution was performed, with good postoperative course. (b) Esophageal perforation—in 1 patient, the passage of a large calculi with an inflamed gallbladder led to perforation of the proximal esophagus and thoracic operation and longer intensive care unit lon-ger admission (grade IVa). (c) Biliary fistula described below in 2 cases, but in only 1 case leading to laparoscopic reoperation.
Comparing TG and TV surgery, the former had signifi-cantly more grade I-II (9.3%) and grade III-IV (13.95%) complications than TV surgery (5.33% and 1.57%, respec-tively; see Table 7). Nevertheless, smaller numbers of cases for each procedure of TG NOTES were recorded than TV cases.
Intraoperative BleedingDuring NOTES procedures, intraoperative hemorrhage during dissection or direct artery lesion occurred in 5 cases of TV cholecystectomy (treated in 1 case by endoscopic clips and with laparoscopic clips in 4 cases), in 1 case of TG appendectomy, and in 3 cases of TV appendectomy (all treated by laparoscopic clips). One case of intraoperative gastric perforation in a NOTES TV cholecystectomy occurred due to adhesions to the anterior gastric wall of a chronically inflamed gallbladder. TV dissection of the fibro-sis caused perforation that was intraoperatively recognized and laparoscopically sutured.

Zorron et al. 151
Biliary Leak
In 2 patients submitted to TV cholecystectomy, biliary leak occurred and no case was related to use of endoscopic clips. In 1 case, the patient was readmitted on the fifth postoperative day and was successfully treated by lapa-roscopic drainage and antibiotics and dismissed after 8 days. The finding was that the double layers of laparo-scopic suturing in the first operation were disrupted. The
second patient had 2 proximal laparoscopic clips applied during the NOTES procedure, and biliary leak and biloma was diagnosed on the first postoperative day. The patient was successfully treated by nasobiliary stenting and per-cutaneous drainage of the fluid collection under tomo-graphic guidance.
No deaths were registered by the centers in this study, and no definitive untreated sequel occurred by the time of closing of these preliminary data.
Table 5. Intraoperative Complications of NOTES Procedures, IMTN Study
Type of Complication Number Original Procedure Evolution Gradea
Cystic artery bleeding 5 TV cholecystectomy Intraoperative laparoscopic or endoscopic treatment
I
Appendix vessels bleeding 4 3 TV appendectomies; 1 TG appendectomy
Intraoperative laparoscopic or endoscopic treatment
I
Gastric access bleeding (epiploic vessels)
1 TG cholecystectomy Conversion to open surgery, suturing IIIb
Gastric wall perforation (inflammatory adhesions)
1 TV cholecystectomy Laparoscopic suturing IIIb
Bowel serosal laceration 1 TV cholecystectomy Intraoperative suturing IIIbEsophageal hematoma � esophageal
laceration due to large stone impaction (24 mm)
2 TG cholecystectomy Extraction by umbilical incision for specimen retrieval
IIIb
Esophageal perforation and mediastinitis
1 TG cholecystectomy Conservative, TPN, conversion to laparoscopy, dismissed after 16 days
IVa
Abdominal wall injury 1 TG appendectomy Conversion to laparoscopic surgery IIIbVaginal laceration 3 TV cholecystectomy Conservative IIntra-abdominal hypertension 2 1 TV cholecystectomy; 1 TV
cancer stagingDesufflation and fluid therapy I
Total 21 (5.8%)
Note: NOTES= natural orifice translumenal endoscopic surgery; TV= transvaginal; TG, transgastric.aGrade classification of surgical complications according to Dindo et al.12
Table 6. Postoperative Complications of NOTES Procedures, IMTN Study
Type of Complication Number Original Procedure Evolution Gradea
Umbilical port infection 1 TG cholecystectomy Conservative IIPeritonitis 1 TG cholecystectomy Streptococcus faecalis, laparoscopic
reoperation, drainage, antibiotics, good PO course
IIIb
Biliary leak 2 TV cholecystectomy using laparoscopic clips or suture
1 nasobiliary drainage, 1 laparoscopic reoperation and drainage
IIIa, IIIb
Prolonged ileus 1 TG appendectomy Conservative IEsophageal hematoma 1 TG cholecystectomy Conservative IIDyspareunia 1 TV cholecystectomy Conservative IVaginal granuloma 1 TV cholecystectomy Conservative IUrinary tract infection 2 1 TV cholecystectomy; 1 TV
rectosigmoidectomyAntibiotic therapy II
Subcutaneous and mediastinal enphysema
1 1 TV nephrectomy Conservative IVa
Total 11 (3.04%)
Note: NOTES= natural orifice translumenal endoscopic surgery; TV= transvaginal; TG, transgastric.aGrade classification of surgical complications according to Dindo et al.12

152 Surgical Innovation 17(2)
Postoperative Analgesia
Despite there being no control from study protocol to unify individual analgesia prescription, analgesia was given by patient’s request, and prospective data were documented. From the patients submitted to NOTES cholecystectomy and appendectomy (N 320, with 17 missing data), no requirement for any analgesia was found in 23.6% of NOTES cholecystectomy and 23.5% of NOTES appendec-tomy (see Table 8). About analgesia, there is difficult to compare as there is no control group in the study. Parameters were crossed to identify potential reasons for no pain, and there were no relations with regard to operative times. Most of the cases with no pain medication also used hybrid sur-gery with at least 1 laparoscopic trocar.
DiscussionNatural orifice surgery is an emerging alternative to stan-dard laparoscopy, combining endoscopic flexible tech-niques to diagnose and treat abdominal pathology. NOTES surgery is promising in achieving no scar surgery; com-pletely avoiding incision-related complications such as hernias, postoperative pain, wound infection, adherences, and intestinal obstruction; and providing good cosmetic result and possibly with less postoperative pain.13-15 More than this, the adoption of future flexible platforms to per-form therapeutic procedures, with many surgeons becom-ing skilled in flexible endoscopy and gastroenterologists replacing complex procedures by simple endoscopic ones, may change the current system of care, separated into com-partments by skill sets rather than target organs.16
Early experimental studies, mostly using TG access, evidenced technical difficulties, infection, and orientation issues related to the lack of adequate flexible platform and instruments for these specific procedures.17,18 Because of limitations of technology for TG access there is need for industry to develop new devices, especially endoscopic suture devices to avoid danger of postoperative leakage and peritonitis. Transcolonic, transurethral, and transesoph-ageal accesses were described, currently still restricted to experimental animal experience.19-24
To discuss the needs and possibilities of the emerging translumenal flexible procedures, a working group repre-senting societies ASGE (American Society of Gastroin-testinal Endoscopy) and SAGES (Society of American Gastrointestinal and Endoscopic Surgeons) met in New York in 2005.25 The group named NOSCAR (Natural Ori-fice Consortium for Assessment and Research) identified barriers that needed to be transposed for the development of translumenal surgery and suggested a list of steps and guidelines. This consortium of surgical endoscopists has established taxonomy, delineated the current limitations to NOTES, and motivated a unified plan of research to propel NOTES into human practice. Important aspect from this early discussion identified several inherent technical challenges to natural orifice surgery, including creating a viscerotomy, orientation, insufflation, infection, manipulat-ing intra-abdominal organs, and safely closing the vis-cerotomy. Following the directives, safe process of gaining experience with translumenal access, allied to safe closure by new devices, should be the natural way to slowly apply NOTES to clinical use.
Instead of other NOTES proposal accesses, however, TV natural orifice surgery may be a potentially less hazard-ous alternative for diagnostic and therapeutic purposes.26 Although TV NOTES can possibly benefit only around 50% of human population, it is now the preferred access published by most researchers in clinical series. Also, TV NOTES access allows the passage of endoscope and instru-ments through the natural orifice without retroflection or closure issues and has been performed for abdominal thera-peutic purposes for many years. Culdoscopy was described by Decker and Cherry in the 1940s,27 and with its evolution to TV hydrolaparoscopy, procedures usually performed
Table 7. Grade I-II and Grade III-IV Complications of TV and TG NOTES Procedures, IMTN Study
Type of Complication Number of Cases Grade I-II Complications Grade III-IV Complications Total
TV NOTES surgery 319 17 (5.33%) 5 (1.57%) 22 (6.9%)TG NOTES surgery 43 4 (9.3%) 6 (13.95%) 10 (23.26%)Total 362 21 (5.8%) 11 (3.04%) 32 (8.84%)
Note: NOTES= natural orifice translumenal endoscopic surgery; TV= transvaginal; TG, transgastric.aGrade classification of surgical complications according to Dindo et al.12
Table 8. Postoperative Use of Analgesia After NOTES Procedures
Zero Analgesiaa Total Percentage
NOTES cholecystectomy 68 289 23.6NOTES cppendectomy 12 51 23.5
Note: NOTES= natural orifice translumenal endoscopic surgery. aZero analgesia refers to patients who did not require any postoperative analgesic medication.

Zorron et al. 153
for investigation and treatment of infertility.28 Bueno described in 1949 the first case of successful performance of incidental vaginal appendectomy at the time of vaginal hysterectomy,29 and Reiner, in 1980, presented his experi-ence with 100 consecutive appendectomies done inciden-tally at the time of vaginal surgery30; and currently, many operations have been described for open TV surgery, including larger series of appendectomy. Laparoscopic extraction of specimens through the vagina (such as gall-bladder, colon, spleen, and kidney) has also been previously described.31-33 Using a hybrid procedure, Tsin and cowork-ers described vaginal cholecystectomy and other operations after simultaneous hysterectomy with a vaginal trocar and formal laparoscopic instruments through the anterior abdominal wall, naming the procedures as “culdolaparos-copy.”34 These previous clinical experiences using vaginal (contaminated) access to perform abdominal (sterile) operations showed small rates of infectious complications and few concerns about compromising fertility due to the access. TV NOTES may possibly represent the safest and most applicable way for natural orifice routes, relatively independent development of technology, with a potential benefit of controllable access and easy closure.
Recent publications and presentations in scientific meet-ings described the first clinical human applications of the new method, after institutional review board approval, for human trials on NOTES in different countries. Since the publication of successful NOTES TV cholecystectomy in early 2007,35-38 other groups published their initial clinical results of the technique, sometimes conjoined with laparos-copy for retraction or for camera purposes.39-49 TG appen-dectomy was also clinically presented in meetings by Rao and coworkers using available endoscopic instruments since 2005,8 and the first TV NOTES appendectomy was first described by Palanivelu et al,50 and later by Bernhardt et al.51 Lacy et al first described a case of hybrid TV sigmoid-ectomy for cancer (MA-NOS),52 Burghardt et al for right colectomy,53 and Ramos et al presented a first series of TV NOTES sleeve gastrectomy.54 Successful TG PEG rescue was described by Marks et al,55 and initial human application for TG pancreatic cancer staging and TV cancer staging has also been reported.9,56,57 Only 5 groups previously reported clinical TG surgery for cholecystectomy, appendectomy, and cancer staging with good results in a small number of cases.8,44,56,58,59 Frequently, procedures such as TG pancreatic debridement by Seifert et al60 and transanally endoscopic microsurgery performed by Buess et al61 were correctly referred as pioneering NOTES techniques.
The International Prospective Multicenter Trial on Clini-cal NOTES Registry started accepting participant centers from July 2007 as there was a need to understand technique improvements and postoperative results of NOTES cases. Inclusion was conditioned to centers having institutional
research committee approval, adequate experimental lab and resources, endoscopic experience, and availability of a multidisciplinary team. The preliminary results reported here will be followed for a minimum period of 6 years, and partial results will be published in intervals of 2 years.
Before adequate NOTES platforms become available, postoperative time will remain longer than when standard laparoscopic techniques are used. Despite lack of adequate technology for natural orifice surgery, totally NOTES sur-gery was first described in the literature by Sousa et al,46 using a technique with 2 vaginal endoscopes, and by Gumbs et al43 and Davila et al,49 using rigid TV retraction. In the present study, TG and TV NOTES cholecystectomy took a mean of 96.1 and 110.9 minutes, respectively, and TG and TV NOTES appendectomy, respectively, 135.5 and 60.5 minutes. This time was significantly decreased in the case of introduction of 1 or more trocars for retrac-tion or dissection, clearly showing that technical and instru-mental development is needed for NOTES procedures. Orientation and visualization were not significant issues, as all the multidisciplinary groups have had previous NOTES techniques tested in the animal experimental set. Laparoscopic assistance representing hybrid surgery was necessary in many cases of advanced procedures, in all cases of TG surgery, and always represented economy in operative and anesthesiology time, if compared with totally NOTES cases. The performance of first entrance by gas-trotomy using the endoscope was accompanied by lapa-roscopic visualization for safety and allowed low incidence of puncture accidents. Gastrotomy closure was always performed by laparoscopic suture, sometimes with innova-tive methods using only 2 trocars (one for 3-mm optic and one 5-mm for one-hand suture by external knotting.), ensur-ing safe recovery without compromising on cosmesis, until reliable, universally approved, safe, and cost-effective methods of closure will be available. Although 1 episode of postoperative peritonitis occurred after TG surgery, it was not related to inadequate closure or fistulae, and no TV cases became infected. Vaginal opening was accompanied by laparoscopic umbilical guidance in a few centers, and most centers using direct vision vaginal access did not report access-related complications. Vaginal wound was effec-tively closed transvaginally in all cases using absorbable sutures under direct view.
Analgesic requirement is an important field of research for NOTES clinical trials, as it may indicate better results than standard laparoscopic and open therapy. Studies com-paring laparoscopic with open cholecystectomy demon-strated less pain scores and less analgesic needs for laparoscopic surgery.62-64 Laparoscopic surgery has also shown to have lower stress response and less impaired immune functions when compared with open surgery in the past,65,66 and improvements in immunologic function

154 Surgical Innovation 17(2)
in natural orifice surgery is at least expected to approximate these results, but early experimental research does not support it yet.67 A prospective study comparing NOTES cholecystectomy and standard laparoscopic cholecystec-tomy in 46 patients registered less need for analgesia,68,69 although further prospective randomized trials should be performed to better compare postoperative pain. The expec-tation is that an expressive percentage of NOTES patients may not need any postoperative pain medication, as shown in our preliminary multicenter study results. Absorption of CO2 measured by end-tidal CO2 may also represent a trend and differences in further studies. Although collected from a few patients in this study, significant increase in end-tidal CO2 can be seen in the laparoscopic group when compared with natural orifice surgery patients, as well as higher CO2 intra-abdominal pressure for laparoscopy when compared with the NOTES group.68,69 Other unpublished reports suggested lower intra-abdominal pressures needed for NOTES compared with laparoscopy; in some cases the procedure was possible using 5to 6 mm Hg CO2, possibly because of less need of exposure and insufflation.70 Although these findings could also contribute to lower analgesia needs in natural orifice surgery, these suggestions were not confirmed in the present IMTN study, because the centers reported mostly same pressures used at lapa-roscopy. Recent experimental studies provided initial information for understanding the physiologic issues of insufflation and infection in natural orifice surgery.71-73
The intraoperative complications rate was 5.48%, and the postoperative complication rate was 2.87%. In larger series of laparoscopic cholecystectomy, biliary duct iath-rogenic lesions are encountered in 0.2% to 3% of the cases, but most individual centers reported a rate of 0.3%.74-79 Major complications are reported in 2% to 4% of the cases, and minor complications range from 5% to 7% for lapa-roscopic cholecystectomy. The mortality rate for laparo-scopic cholecystectomy is estimated to be as low as 0.1%.77 TV NOTES procedures had less grade I-II and grade III-IV complication rates than TG NOTES operations in this study, although the small number of cases might bias sta-tistical significance analysis. Although there were no reports of deaths in the IMTN registry, at least 1 patient had a possibility of fatal postoperative course due to esoph-ageal perforation and mediastinitis. Grade III-IV compli-cations occurred in 10 patients (2.76%), represented by intraoperative bleeding, bowel injury (intraoperatively recognized and treated), biliary fistula, and esophageal injury. Postoperative peritonitis by S faecalis occurred after 1 case of TG cholecystectomy, although with no gastric closure site leak. Biliary leaks occurred in 2 patients after TV surgery, but were not due to endoscopic clip failure, which were not used in the cases. Failures were due to cystic duct inefficient closure by laparoscopic clips or
sutures. There was no iathrogenic biliary injury reported. Infection is a concern from the very beginning of the natural orifice concept,80 but was rarely reported in this study. With the exception of 1 peritonitis case reported, estab-lished means of gastric and vaginal disinfection, steriliza-tion of the instruments, and high-level disinfection of the flexible endoscopes proved to be satisfactory in this casu-istic in avoiding surgical infection.
The choice of the orifice access showed significant dif-ferences in operative complication rates. TG surgery reported significantly higher rates of grade I-II (9.3%) and grade III-IV (13.95%) complications than TV surgery (5.33% and 1.57%, respectively). A longer learning curve for TG surgery is expected. Because of the lack of instru-ments to perform adequate dissection and retraction, the need for retroflection, the need for flexible endoscopy skills, and the small size of the esophageal lumen surely contribute to higher operative times and complications than TV NOTES. The use of gastroesophageal overtubes could prevent esophageal injuries, as well as avoiding technical difficulties for specimen retrieval, but still the instrumental and ports to be invented by industry will have more restrictions in size and shape than vaginal and colonic NOTES access.
The preliminary results of the IMTN Study represent the first large series application of NOTES in the literature. In most clinical cases, the access was easily created and intra-abdominal procedure was performed without technical or orientation difficulty, even in cases in which retroflection visualization from the endoscope was needed. Operative time was longer than a standard laparoscopic operation, but possibly might be shortened with more adequate instru-ments in the future. Interestingly, if “pure NOTES” (totally NOTES) is used, without laparoscopic assistance, operative time is significantly longer than with any laparoscopic assistance for retraction or visualization. The desired tri-angulation was not possible using the endoscope, and more in-line dissection technique was frequently described by the centers for dissection. The difficulties in applying trac-tion, lack of multiplanar instrumentation, and limited size of the working channels of the endoscope are other obsta-cles. Closure of the vaginal wound was not a problematic issue of the approach and was done externally under direct vision using conventional instruments. Closure of TG access, however, was still an issue, and the procedures could only be performed using laparoscopic closure of gastric access using 1 or 2 laparoscopic trocars. As the experienced surgeon knows, a hostile pelvis due to adhesions, previous pelvic infections, and endometriosis is more common than a hostile upper abdomen, possibly making TG access more attractive, especially for the general surgeon with upper endoscopy experience. However, large specimen retrievals are not expected to be solved by the TG approach, as the
Zorron et al. 155
esophagus allows only a maximal instrumental (or speci-men) diameter of around 2 cm. TV NOTES approaches have less potential for complications such as fistula and peritonitis when compared with other translumenal accesses. Potential disadvantages of NOTES surgery are the neces-sary use of antibiotics and bladder catheterization and risk of infection and morbidity of gastric, vaginal, and colonic access, even with longer operative times.
Based on the preliminary results of the study, initial general recommendations of the IMTN NOTES Study Group are the following:
1. Suggested taxonomy for NOTES procedures. Totally NOTES (T-NOTES) are procedures per-formed through any natural orifice without per-cutaneous assistance. Hybrid NOTES implies use of laparoscopy for retraction and visualization, but with significant dissection performed through the natural orifice. NOTES-assisted laparoscopy means operations performed by laparoscopy with low natural orifice instrumentation contribution (retraction or visualization), such as culdolapa-roscopy. NOSE refers to natural orifice specimen extraction, as previously published.81 A differen-tiation between NOTES performed by flexible endoscopy (FLEX-NOTES) and those performed by rigid instruments (RIG-NOTES) seems impor-tant, as flexible instruments are not accepted everywhere for intra-abdominal surgical arsenal and because of difficulties in reliable device sterilization.
2. Choice of the natural orifice access. The group recommends that all further clinical trials for TG and TV approaches, under institutional review board approval, be performed by a multidisci-plinary team with a skilled endoscopist and with previous extensive animal experience in translu-menal techniques before human series. Transco-lonic, transesophagic, and transurethral accesses are not suitable yet for clinical studies, as there is a lack of experimental data and technical devel-opment for its safe use in trials.
3. Single access surgery. Umbilical laparoscopic surgery (laparoendoscopic single site surgery [LESS], single access surgery [SAS], single port access [SPA], or transumbilical endoscopic sur-gery [TUES]) is not natural orifice surgery, as the umbilicus is a natural scar, not orifice, and pro-duces somatic pain rather than visceral pain. Regarding this evolving concept, potential advan-tages in NOTES regarding avoidance of incision-related complications and somatic pain are absent in SAS. As it is recognized as laparoscopy
performed through a single trocar, there is, in our view, no restriction for its use in clinical trials.
4. Feasibility and safety. Basic TG and TV NOTES procedures are feasible with the available instru-ments, taking possibly longer operative times than laparoscopy until new endoscopic technology arises. TV surgery is feasible and safe for uncom-plicated indications, although TG surgery needs evolution of technology for more wide clinical applications. Gastric opening wound still needs laparoscopic closure and preoperative gastric lavage with antiseptics for patient’s safety. The use of overtubes to perform TG NOTES could minimize esophageal complications. The deter-mination of safety of each procedure can only be assured after the next steps of IMTN Study with larger numbers of patients per procedure and lon-ger follow-up times.
5. Learning curve. TG NOTES showed a more haz-ardous learning curve and more initial complica-tions than TV surgery, due to the difficulty in navigation, spatial orientation, small size of the viscera (esophagus) allowed for operative work, and need for a safe entry and closure of the gastric wall. These barriers possibly will slow the accep-tance and development of clinical TG surgery, as the access has a limitation for instruments and specimen extraction sizes.
6. Sterilization and preparation. Although the occur-rence of postoperative infectious complications was relatively low in the study, efforts have to be directed to produce flexible endoscopes able to be sterilized under available and cost-effective methods. Intraoperative gastric lavage with chlo-rohexidine and traditional vaginal disinfection can minimize infection.
7. Contraindications. Cases shall be well selected and performed by a skilled team in flexible endos-copy to avoid long operative times and misorienta-tion. Previous abdominal and pelvic surgeries as well as adhesions are no longer contraindications. Advanced and emergency procedures should be avoided in the early phase of technological devel-opment. For TV access, previous hysterectomy, vaginal infection, pregnancy, endometriosis, and virgin patients constitutes contraindications. Oncologic NOTES procedures are not supported yet by the literature, but possibly will follow the same pattern of acceptance as laparoscopy. Natural orifice tumor implant possibilities are issues for future research.
8. Indications. None of the procedures performed worldwide in the study showed evidence of being
156 Surgical Innovation 17(2)
superior to laparoscopic surgery. Advantages sug-gested in this study, such as lower intra-abdominal pressures, less pain demonstrated by a percentage of patients showing no use of postoperative anal-gesia, and less incision complications, may be considered for future research.
NOTES seems to be evolving as a feasible, safe, and reasonable option for transabdominal surgery, with the potential to avoid incision-related complications completely. However, caution is necessary, as complications faced during the early days of laparoscopic surgery should not be repeated. Despite long operative times, these preliminary results of the IMTN Trial showed acceptable complication rates in all international centers, low postoperative hospital stay, and good cosmetic and pain requirement results, especially for TV surgery. Future prospective clinical trials comparing NOTES with laparoscopy may be needed. More important than this and perhaps crucial to indicate widespread use translumenal surgery will again be the ability of surgeons and endoscopists to replace complex surgical procedures with simple endoscopic ones and the identification of novel therapeutic targets. Therefore, it is expected that more clini-cal studies may reproduce the study results, thus stimulating also the call for prospective randomized studies comparing natural orifice surgery with standard laparoscopy.
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
FundingThe author(s) received no financial support for the research and/or authorship of this article.
References 1. Kalloo AN, Singh VK, Jagannath SB, et al. Flexible trans-
gastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Gastroin-test Endosc. 2004;60:287-292.
2. Kantsevoy SV, Jagannath SB, Niiyama H, et al. Endoscopic gastrojejunostomy with survival in a porcine model. Gastro-intest Endosc. 2005;62:287-292.
3. Park PO, Bergström M, Ikeda K, Fritscher-Ravens A, Swain P. Experimental studies of transgastric gallbladder surgery: cholecystectomy and cholecystogastric anastomosis. Gastrointest Endosc. 2006;61:601-606.
4. Wagh MS, Merrifield BF, Thompson CC. Survival studies after endoscopic transgastric oophorectomy and tubectomy in a porcine model. Gastrointest Endosc. 2006;63:473-478.
5. Bergstrom M, Ikeda K, Swain P, Park PO. Transgastric anas-tomosis by using flexible endoscopy in a porcine model. Gastrointest Endosc. 2006;63:307-312.
6. Kantsevoy SV, Hu B, Jagannath SB, et al. Transgastric endoscopic splenectomy: is it possible? Surg Endosc. 2006; 20:522-525.
7. Hochberger J, Lamadé W. Transgastric surgery of the abdo-men: the dawn of a new era? Gastrointest Endosc. 2005;62: 293-295.
8. Rao GV, Reddy DN, Banerjee R. NOTES: human experience. Gastrointest Endosc Clin N Am. 2008;18:361-370.
9. Bergman S, Melvin WS. Natural orifice translumenal endo-scopic surgery. Surg Clin North Am. 2008;88:1131-1148.
10. Sodergreen MH, Clark J, Athanasiou T, Teare J, Yang GZ, Darzi A. Natural orifice translumenal endoscopic surgery: critical appraisal of applications in clinical practice. Surg Endosc. 2009;23:680-687.
11. Clavien P, Sanabria J, Strasberg S. Proposed classification of complication of surgery with examples of utility in cholecys-tectomy. Surgery. 1992;111:518-526.
12. Dindo D, Demartines N, Clavien PA. Classification of sur-gical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205-209.
13. Malik A, Mellinger JD, Hazey JW, Dunkin BJ, MacFadyen BV. Endoluminal and transluminal surgery: current status and future possibilities. Surg Endosc. 2006; 20:1179-1192.
14. McGee MF, Rosen MJ, Marks J, et al. A primer on natural orifice transluminal endoscopic surgery: building a new para-digm. Surg Innov. 2006;13:86-93.
15. Giday S, Magno P, Kalloo AN. NOTES: the future. Gastro-intest Endosc Clin N Am. 2008;18:387-395.
16. Pasricha PJ, Krummel TM. NOTES and other emerging trends in gastrointestinal endoscopy and surgery: the change that we need and the change that is real. Am J Gastroenterol. 2009;104:2384-2386.
17. Sclabas GM, Swain P, Swanstrom LL. Endoluminal methods for gastrotomy closure in natural orifice transenteric surgery (NOTES). Surg Innov. 2006;13:23-30.
18. Swanstrom LL, Kozarek R, Pasricha PJ, et al. Development of a new access device for transgastric surgery. J Gastroin-test Surg. 2005;9:1129-1137.
19. Pai RD, Fong DG, Bundga ME, Odze RE, Rattner DW, Thompson CC. Transcolonic endoscopic cholecystectomy: a NOTES survival study in a porcine model (with video). Gastrointest Endosc. 2006;64:428-434.
20. Whiteford M, Denk EM, Swanstrom L. Feasibility of radical sigmoid colectomy performed as natural orifice translume-nal endoscopic surgery (NOTES) using transanal endoscopic microsurgery. Surg Endosc. 2007;21:1870-1874.
21. Lima E, Rolanda C, Pêgo JM, et al. Third-generation chole-cystectomy by natural orifices: transgastric and transvesical combined approach. J Urol. 2007;178:2648-2654.
22. Sumiyama K, Gostout CJ, Rajan E, Bakken TA, Knipschield MA. Transesophageal mediastinoscopy by
Zorron et al. 157
submucosal endoscopy with mucosal flap safety technique. Gastrointest Endosc. 2007;65:679-683.
23. Fritscher-Ravens A, Patel K, Kahle E, et al. Natural orifice transluminal endoscopic surgery (NOTES) in the mediasti-num: long-term survival animal experiments in transesopha-geal access, including minor surgical procedures. Endoscopy. 2007;39:870-875.
24. Willingham FF, Gee DW, Lauwers GY, Brugge WR, Rattner DW. Natural orifice transesophageal mediastinos-copy and thoracoscopy. Surg Endosc. 2008;22:1042-1047.
25. Rattner D, Kalloo, A. ASGE/SAGES Working Group on Natural Orifice Translumenal Endoscopic Surgery. Surg Endosc. 2006;20:329-333.
26. Zorron R. Techniques of transvaginal access for NOTES. Tech Gastrointest Endosc. 2009;11:75-83.
27. Decker A, Cherry TH. Culdoscopy: a new method in the diagnosis of pelvic disease—preliminary report. Am J Surg. 1944;64:40-44.
28. Christian J, Barrier BF, Schust D, Miedema BW, Thaler K. Culdoscopy: a foundation for natural orifice surgery—past, present and future. J Am Coll Surg. 2008;207:417-422.
29. Bueno B. Primer caso de apendicectomia por via vaginal. Tokoginec Pract (Madrid). 1949;8:152-154.
30. Reiner IJ. Incidental appendectomy at the time of vaginal surgery. Texas Med. 1980;76:46-50.
31. Delvaux G, Devroey P, De Waele B, Willems G. Transvaginal removal of gallbladders with large stones after laparoscopic cholecystectomy. Surg Laparosc Endosc. 1993;3:307-309.
32. Breda G, Silvestre P, Giunta A, Xausa D, Tamai A, Gherardi L. Laparoscopic nephrectomy with vaginal delivery of the intact kidney. Eur Urol. 1993;24(1):116-117.
33. Zornig C, Emmermann A, von Waldenfels HA, Felixmüller C. Colpotomy for specimen removal in laparoscopic surgery. Chirurg. 1994;65:883-885.
34. Tsin DA, Colombero L, Mahmood D, Padouvas J, Manolas P. Operative culdolaparoscopy: a new approach combining operative culdoscopy and minilaparoscopy. J Am Assoc Gynecol Laparosc. 2001;8:438-441.
35. Zorron R, Filgueiras M, Maggioni LC, et al. NOTES. Transvaginal cholecystectomy: report of the first case. Surg Innov. 2007;14:279-283.
36. Marescaux J, Dallemagne B, Perretta S, Wattiez A, Mutter D, Coumaros D. Report of transluminal cholecystectomy in a human being. Arch Surg. 2007;142:823-826.
37. Zornig C, Emmermann A, von Waldenfels HA, Mofid H. Laparoscopic cholecystectomy without visible scar: com-bined transvaginal and transumbilical approach. Endoscopy. 2007;39:913-915.
38. Branco Filho AJ, Noda RW, Kondo W, et al. Initial experi-ence with hybrid transvaginal cholecystectomy. Gastrointest Endosc. 2007;66:1245-1248.
39. Ramos AC, Murakami A, Galvão Neto M, et al. NOTES transvaginal video-assisted cholecystectomy: first series. Endoscopy. 2008;40:572-575.
40. DeCarli L, Zorron R, Branco A, et al. New hybrid approach for NOTES transvaginal cholecystectomy: preliminary clini-cal experience. Surg Innov. 2009;16:181-186.
41. Forgione A, Maggioni D, Sansonna F, et al. Transvaginal endoscopic cholecystectomy in human beings: preliminary results. J Laparoendosc Adv Surg Tech A. 2008;18:345-351.
42. Zorron R, Maggioni LC, Pombo L, Oliveira AL, Carvalho GL, Filgueiras M. NOTES transvaginal chole-cystectomy: preliminary clinical application. Surg Endosc. 2008;22:542-547.
43. Gumbs AA, Fowler D, Milone L, et al. Transvaginal natural endoscopic surgery cholecystectomy: early evolution of the technique. Ann Surg. 2009;249:908-912.
44. Horgan S, Cullen JP, Talamini MA, et al. Natural orifice surgery: initial clinical experience. Surg Endosc. 2009;23: 1512-1518.
45. Fischer LJ, Jacobsen G, Wong B, et al. NOTES laparo-scopic-assisted transvaginal sleeve gastrectomy in humans—description of preliminary experience in the United States. Surg Obes Relat Dis. 2009;5:633-636.
46. Sousa LH, Sousa JAG, Sousa MM, et al. Totally NOTES (T-NOTES) transvaginal cholecystectomy using two endoscopes: preliminary report. Surg Endosc. 2009;23:2550-2555.
47. Noguera J, Dolz C, Cuadrado A, Olea J, Vilella A, Morales R. Hybrid transvaginal cholecystectomy, NOTES, and mini-laparoscopy: analysis of a prospective clinical series. Surg Endosc. 2009;23:876-881.
48. Palanivelu C, Rajan PS, Rangarajan M, et al. Transvaginal endoscopic cholecystectomy in humans: preliminary report of a case series. Am J Gastroenterol. 2009;104:843-847.
49. Davila F, Tsin DA, Dominguez G, Davila U, Jesus R, Gomez de Arteche A. Transvaginal cholecystectomy with-out abdominal ports. JSLS. 2009;13:213-216.
50. Palanivelu C, Rajan PS, Rangarajan M, Parthasarathi R, Senthilnathan P, Prasad M. Transvaginal endoscopic appen-dectomy in humans: a unique approach to NOTES—world’s first report. Surg Endosc. 2008;22:1343-1347.
51. Bernhardt J, Gerber B, Schober HC, Kähler G, Ludwig K. NOTES—case report of a unidirectional flexible appendec-tomy. Int J Colorectal Dis. 2008;23:547-550.
52. Lacy AM, Delgado S, Rojas OA, Almenara R, Blasi A, Llach J. MA-NOS radical sigmoidectomy: report of a transvaginal resection in the human. Surg Endosc. 2008;22:1717-1723.
53. Burghardt J, Federlein M, Müller V, Benhidjeb T, Elling D, Gellert K. Minimal invasive transvaginal right hemicolectomy: report of the first complex NOS (natural orifice surgery) bowels operation using a hybrid approach. Zentralbl Chir. 2008;133:574-576.
54. Ramos AC, Zundel N, Neto MG, Maalouf M. Human hybrid NOTES transvaginal sleeve gastrectomy: initial experience. Surg Obes Relat Dis. 2008;4:660-663.
55. Marks JM, Ponsky JL, Pearl JP, McGee MF. PEG rescue: a practical NOTES technique. Surg Endosc. 2007;21:816-819.
158 Surgical Innovation 17(2)
56. Hazey JW, Narula VK, Renton DB, et al. Natural orifice transgastric endoscopic peritoneoscopy in humans: initial clinical trial. Surg Endosc. 2008;22:16-20.
57. Zorron R, Soldan M, Filgueiras M, Maggioni LC, Pombo L, Oliveira AL. NOTES: transvaginal for cancer diagnostic staging: preliminary clinical application. Surg Innov. 2008; 15:161-165.
58. Auyang ED, Hungness ES, Vaziri K, Martin JA, Soper NJ. Human NOTES cholecystectomy: transgastric hybrid tech-nique. J Gastrointest Surg. 2009;13:1149-1150.
59. Dallemagne B, Perretta S, Allemann P, Asakuma M, Marescaux J. Transgastric hybrid cholecystectomy. Br J Surg. 2009;96:1162-1166.
60. Seifert H, Wehrmann T, Schmitt T, Zeuzem S, Caspary WF. Retroperitoneal endoscopic debridement for infected peri-pancreatic necrosis. Lancet. 2000;19:653-655.
61. Buess G, Kipfmüller K, Ibald R, et al. Clinical results of transanal endoscopic microsurgery. Surg Endosc. 1988;2: 245-250.
62. Barkun JS, Barkun AN, Sampalis JS, et al. Randomised controlled trial of laparoscopic versus mini cholescytec-tomy. The McGill Gallstone Treatment Group. Lancet. 1992;340:1116-1119.
63. McMahon AJ, Russell IT, Baxter JN, et al. Laparoscopic versus minilaparotomy cholecystectomy: a randomised trial. Lancet. 1994;343:135-138.
64. Kunz R, Orth K, Vogel J, et al. Laparoscopic cholecystec-tomy versus mini-lapcholecystectomy. Results of a pro-spective, randomized study [in German]. Chirurg. 1992;63: 291-295.
65. Glaser F, Sannwald GA, Buhr HJ, et al. General stress response to conventional and laparoscopic cholecystectomy. Ann Surg. 1995;221:372-380.
66. Kloosterman T, von Blomberg BM, Borgstein P, Cuesta MA, Scheper RJ, Meijer S. Unimpaired immune functions after laparoscopic cholecystectomy. Surgery. 1994;115:424-428.
67. Bingener J, Krishnegowda NK, Michalek J. Immuno-logic parameters during NOTES compared with laparos-copy in a randomized blinded porcine trial. Surg Endosc. 2009;23:178-181.
68. SAGES 2009 Annual Meeting; April 22-25, 2009; Phoenix, AZ.
69. Zorrón R, DeCarli L, Branco A, et al. NOTES transvaginal cholecystectomy: prospective clinical comparative study with laparoscopy. Surg Endosc. In press.
70. NOSCAR. 2nd International Conference on NOTES; Boston, MA, July 13-14, 2007.
71. McGee MF, Rosen MJ, Marks J, et al. A reliable method for monitoring intraabdominal pressure during natural orifice translumenal endoscopic surgery. Surg Endosc. 2007;21:672-676.
72. Meireles O, Kantsevoy SV, Kalloo AN, et al. Comparison of intraabdominal pressures using the gastroscope and laparo-scope for transgastric surgery. Surg Endosc. 2007;21:998-1001.
73. Bergström M, Swain P, Park PO. Measurements of intraperi-toneal pressure and the development of a feedback control valve for regulating pressure during flexible transgastric sur-gery (NOTES). Gastrointest Endosc. 2007;66:174-178.
74. Larson G, Vitale G, Casey J, et al. Multipractice analysis of laparoscopic cholecystectomies in 1,093 patients. Am J Surg. 1992;163:221-226.
75. Rossi RL, Schirmer WJ, Braasch JW, Sanders LB, Munson JL. Laparoscopic bile duct injuries: risk factors, recognition and repair. Arch Surg. 1992;127:596-601.
76. MacMahon AJ, Fullarton G, Baxter JN, O’Dwyer PJ. Bile duct injury and bile leakage in laparoscopic cholecystectomy. Br J Surg. 1995;82:307-313.
77. Quinn SF, Sangster W, Standage B, Schuman E, Gross G. Biliary complications related to laparoscopic cholecystecto-mies: radiologic diagnosis and management. Surg Laparosc Endosc. 1992;2:279-286.
78. Strasberg SM, Hertl M, Soper NJ. An analysis of the prob-lem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180:101-125.
79. Steiner CA, Bass EB, Talamini MA, Pitt HA, Steinberg EP. Surgical rates and operative mortality for open and laparo-scopic cholecystectomy in Maryland. N Engl J Med. 1994; 330:403-408.
80. Kantsevoy SV. Infection prevention in NOTES. Gastrointest Endosc Clin N Am. 2008;18:291-296.
81. Palanivelu C, Rangarajan M, Jategaonkar PA, Anand NV. An innovative technique for colorectal specimen retrieval: a new era of “natural orifice specimen extraction” (NOSE). Dis Colon Rectum. 2008;51:1120-1124.
Copyright of Surgical Innovation is the property of Sage Publications, Inc. and its content may not be copied oremailed to multiple sites or posted to a listserv without the copyright holder's express written permission.However, users may print, download, or email articles for individual use.
Related Documents











