INTERNATIONAL JOURNAL FOR PSYCHOTHERAPY IN AFRICA ISSN: 2550-7257 (Print) ISSN: 2550-7249 (Online) Fifth Edition, Number 1 July, 2020 Published by the School of Psychotherapy and Health Sciences (SPHS), Okija Campus, Nigeria. Affiliated to Sigmund Freud University, Vienna, Austria

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
INTERNATIONAL
JOURNAL
FOR
PSYCHOTHERAPY
IN AFRICA
ISSN: 2550-7257 (Print)
ISSN: 2550-7249 (Online)
Fifth Edition, Number 1
July, 2020
Published by the
School of Psychotherapy and Health Sciences (SPHS),
Okija Campus, Nigeria.
Affiliated to Sigmund Freud University, Vienna, Austria
International Journal for Psychotherapy in Africa (5:1)
ii
EDITORIAL BOARD
Prof. S.N. Madu
Chukwuemeka Odumegwu Ojukwu University, Nigeria - Editor-in-Chief
Prof. P. A. Agashua
Nigerian Defense Academy, Kaduna, Nigeria - Associate Editor
Prof. H. Osinowo
University of Ibadan, Nigeria - Member
Prof. Z. Knight
University of Johannesburg, South Africa - Member
Dr. G. Madubuike
School of Psychotherapy & Health Sciences, Nigeria - Member
Dr. Alh. M. Tafida
Nasarawa State University, Nigeria - Member
Mr. P. Egwu
School of Psychotherapy & Health Sciences, Nigeria - Editorial Secretary
EDITORIAL ADDRESS
Editorial Secretary
International Journal for Psychotherapy in Africa (IJPA)
School of Psychotherapy and Health Sciences (SPHS),
Okija Campus,
P. O. Box 33, Okija, Anambra State, Nigeria.
Mobile: 09063927862
Email: [email protected]; [email protected]
Web Address: www.sphs.com.ng
© School of Psychotherapy and Health Sciences (SPHS), Okija Campus, Nigeria
International Journal for Psychotherapy in Africa (5:1)
iii
Editorial Brief
nternational Journal for Psychotherapy in Africa is published by the School of
Psychotherapy and Health Sciences, Okija, Nigeria, with the editorial policy to address
issues that border on people’s psychological health and psychotherapy in African. The
journal publishes contributions that advance the frontier of knowledge in psychotherapy
in Africa, submitted by trained psychotherapists, psychologists, and other scholars from
related disciplines, whose research works and practical experience unraveled new knowledge
in the area of psychotherapy. The emphasis for the journal is on empirical papers; however, it
also accepts theoretical papers, review articles, short communications and interactions
containing fair commentary. Priority is given to articles that are relevant to Africa, and that
address psychotherapeutic issues and methods for the enhancement of psychological wellness
of Africans.
The need for psychotherapeutic intervention is very vital in many countries of Africa.
In these days of corona virus (COVID-19) pandemic which locked down the whole world,
the countries of Africa are least prepared to face the psychological effects of the pandemic.
They are least prepared for the needed psychotherapeutic intervention during and post
COVID-19. The trauma, stigma, depression and other forms of psychological ill-health are
likely to take many African countries unaware. In addition to that, many of the countries are
being challenged by various forms of conflict and insecurity problems like terrorism, and
insurgency, the aftermath of which many innocent individuals, families and communities are
displaced of their natural residences; and are physically and mentally tormented. In the face
of this condition, the International Journal for Psychotherapy in African holds it as a
responsibility to invite scholars to contribute their knowledge of Psychotherapeutic
intervention models that will be of great help in assisting victims of this pandemic and
menace.
This fifth edition of the International Journal for Psychotherapy in African contains many
scholarly and vibrant research articles in areas of Psychotherapeutic Implications of COVID-
19 Pandemic, Psychotherapy Training in Africa, Acceptance and Commitment Therapy,
Suicidal Ideation, Post-traumatic Stress, Insurgencies, Internal Displacement of Persons,
Spirituality and Psychotherapy, and Traditional Healing, among others. The scholars cross-
pollinated knowledge on their psychotherapy models and expressed the need for
psychotherapy for mental wellness in African.
The editorial board wishes to thank all the authors of the articles and all those who helped in
one way or the other to make this publication a reality.
Prof. Sylvester Ntomchukwu Madu
Editor-in-Chief
I

International Journal for Psychotherapy in Africa (5:1)
iv
Editorial Mission and Policies
nternational Journal for Psychotherapy in Africa (IJPA) is published by the School of
Psychotherapy and Health Sciences (SPHS), Okija Campus, Nigeria. The institution is
affiliated to Sigmund Freud University, Vienna, Austria.
The journal is geared to dissemination of research out-put and cross-pollination of ideas
among psychotherapists world-wide about psychotherapy in Africa. It is a peer-reviewed
indexed journal and the articles can be accessed online through Google Scholar. It accepts
original articles, empirical investigations, position papers, as well as short book reviews of
not more than 1500 words.
Authors interested in publishing articles in IJPA are encouraged to submit their manuscripts
electronically by email attachment to the Editorial Secretary. Manuscripts should not exceed
20 typed pages, and should be accompanied by an abstract of not more than 150 words. Five
key words for identifying the paper on web search should be supplied immediately below the
abstract. Manuscripts should be typed in MS Word, Times New Romans, 12 font size and
should be on double spaced A4 size paper. The author’s named, institutional affiliation, and
address should appear on the title page separated from the manuscript, to ensure anonymity in
the review process. The title of the paper should appear on all the pages of the manuscript.
The journal adopts the latest edition of American Psychological Association (APA) format.
Acknowledgement should normally come at the end of references. Contributors should
ensure that papers submitted are not under consideration for publication in any other research
outlet. An editorial decision on the manuscripts will be taken as soon as possible and
communicated on the contributors. One complimentary copy of the journal in which the
author’s article appears will be forwarded to the first author immediately on publication. The
journal appears once a year, but articles are welcome throughout the year. All articles for
publication, requests for advertisement, and other enquiries should be forwarded to the
Editorial Secretary. The assessment fee per article is N5,000.00. Authors of accepted papers
are required to pay a publication fee of N25, 000.00. After payment, a scanned copy of
payment evidence should be forwarded to the journal’s email addresses. All payments should
be made to the bank account as stated below:
Account Name: School of Psychotherapy and Health Sciences.
Bank Name: Access Bank.
Account Number: 0084829949.
For Additional information, contact:
Prof. S.N. Madu
Mobile: +234(0)7062883630
Email: [email protected]; [email protected]
I
International Journal for Psychotherapy in Africa (5:1)
v
Contents
1 – 10 Challenges Facing Psychotherapists In Africa
In The Hit Of The Novel Coronavirus 2019
(Covid-19) Global Pandemic By: Sylvester Ntomchukwu Madu;
Valentine Ucheagwu
11 – 21 Psychological Intervention To Break
The Cycle Of Violence And Accelerate Public Safety,
Security And Development (With Special Reference To Africa) By: Chioma Ihuoma Igboegwu
22 – 34 The Relevance Of Acceptance And Commitment Therapy (ACT)
In The Treatment Of Emotional Numbing Among The
Adolescents: A Narrative Review By: Uchenna E. Enem
Bahago Samaila
35 – 43 Diagnosis And Treatment Of Mental Illness By Vhavenda
Traditional Healers In Vhembe District, South Africa By: Salome Thilivhali Sigida;
Nare Judy Masola
44 – 53 Psychotherapy Training In Africa South Of Sahara By: Sylvester Ntomchukwu Madu
54 – 69 Post-Traumatic Stress Disorder And Depression In
Personnel Of Nigeria Police Force: Implications For Psychotherapy
By: Chioma Ihuoma Igboegwu

International Journal for Psychotherapy in Africa (5:1)
vi
70 – 83 Personality Trait, Drug use and Abuse as Predictors of
Suicidal Intention Among Youths: A Focus for Psychotherapy
By: Charity Justin Takyun
Okwoli Matthew James
Maryam Abubakar
84 – 97 Posttraumatic Stress Disorder Among Trafficked Victims,
Role Of Self-Esteem, Demographic Factors And Relevance
Of Psychotherapy By: Ezeakor Adolphus I.
Okpala Michael O.
98 – 107 Integration Of Spirituality Into Psychotherapy –
A Potential Model For Nigeria B: Richard Uwakwe
108 – 115 English Language Students And Their Coping Styles
During Lockdown As A Result Of The Novel Coronavirus 2019
(Covid-19) Global Pandemic By: Bridget Ngozi Madu
116 – 121 Genuineness In Client Centered Psychotherapy:
It’s Relevance To The Nigerian Society During
The Convid-19 Global Pandemic
By: Promise Chinedu Uwakwe
122 – 135 Gender Differences In Attitude To The
Skin Disease-Atopic Dermatitis Among Adolescents:
The Role Of Cognitive Behavioral Therapy
By: Charity Justin Takyun
Aleksandra Surenovich Kocharyan
Madu, S.N. & Ucheagwu, V. (2020). Challenges Facing Psychotherapists in Africa in the Hit of The Novel
Coronavirus 2019 (Covid-19) Global Pandemic, International Journal for Psychotherapy in Africa 5(1):1-10
1
Challenges Facing Psychotherapists In Africa
In The Hit Of The Novel Coronavirus 2019
(Covid-19) Global Pandemic
Sylvester Ntomchukwu Madu Department of Psychology, Chukwuemeka Odumegwu Ojukwu University,
Igbariam Campus, Nigeria.
Valentine Ucheagwu Department of Psychology, Madonna University,
Okija Campus, Nigeria.
Abstract To fully understand the challenges facing psychotherapists in Africa in the hit of the
Novel Coronavirus 2019 (COVID-19) global pandemic, the paper visited/reflected the
origin and transmission of the virus, the global epidemiology, and the resultant adoption
of international and national lockdown limiting heavily movements of people and goods
to prevent further spread of the virus. The lockdown, however, has seriously affected the
interpersonal relationships and freedom of gathering. It is also expected that it will have
adverse mental and psychological effects leading to behavioural, emotional, social/family
problems. Increased incidence of stress reactivity and anxiety, reality denial, depression,
isolation, loneliness and lack of social support, undesirable marital adjustment and
irritability, trauma, self-injurious behaviours like suicidal ideation and drug addiction,
unhealthy eating behaviours and resultant increase in weight, and Obsessive Compulsive
Disorder, increased neuropsychological symptoms, are some of the expected adverse
effects of the lockdown. The ability to adequately address all these anticipated problems
pose a big challenge to the few qualified psychotherapists in Africa. There are also very
few institutions for the training of psychotherapist in Africa south of Sahara. The speed
with which the virus is spreading also calls for short-term acquisition of hands-on
psychotherapeutic skills. African governments are therefore called upon to address the
above-mentioned shortage as a matter of urgency. The few psychotherapists available in
Africa are also called upon to look into the above psychologically unhealthy situation
from the point of view of crisis intervention.
Key words: Corona virus (COVID-19), Pandemic, Challenges, Psychotherapists, Africa.
Introduction
Origin and Transmission of COVID -19
In December 2019, a cluster of pneumonia
cases, caused by a newly identified β-
coronavirus, occurred in Wuhan, China.
This coronavirus was initially named as
the 2019-novel coronavirus (2019-nCoV)
on 12 January 2020 by World Health
Organization (WHO) and was officially

International Journal for Psychotherapy in Africa (5:1)
2
named corona virus disease 2019
(COVID-19) (Yan-Rong and Colleagues,
2020). The Coronavirus Study Group
(CSG) of the International Committee had
proposed to name the new coronavirus as
severe acute respiratory syndrome (SARS-
CoV-2). COVID-19 belongs to a β-
coronavirus, which is enveloped non-
segmented positive-sense RNA virus
(subgenus sarbecovirus,
Orthocoronavirinae subfamily) (Zhu et.
al., 2020). Coronaviruses (CoV) are
divided into four genera, including α−/
β−/γ−/δ-CoV. Yan-Rong and colleagues
(2020) argued that α- and β-CoV are able
to infect mammals, while γ- and δ-CoV
tend to infect birds. Previously, six CoVs
have been identified as human-susceptible
virus, among which α-CoVs HCoV-229E
and HCoV-NL63, and β-CoVs HCoV-
HKU1 and HCoV-OC43 with low
pathogenicity, causing mild respiratory
symptoms similar to a common cold,
respectively (Yang-Rong, et. al., 2020).
Above all, the other two known β-CoVs:
SARS-CoV and MERS-CoV lead to
severe and potentially fatal respiratory
tract infections. It was found that the
genome sequence of SARS-CoV-2 is
96.2% identical to a bat CoV RaTG13,
whereas it shares 79.5% identity to SARS-
CoV (Yan-Rong et. al., 2020). Based on
virus genome sequencing results and
evolutionary analysis, bat has been
suspected as natural host of virus origin,
and SARSCoV-2 might be transmitted
from bats via unknown intermediate hosts
to infect humans (Yan-Rong et. al., 2020).
It is clear now that SARS-CoV-2 could
use angiotensin-converting enzyme 2
(ACE2), the same receptor as SARS-CoV
to infect humans.
COVID-19 pandemic which started
first in Wuhan, China, since 12 December
2019, is possibly related to a seafood
market. Several studies suggested that bat
may be the potential reservoir of SARS-
CoV-2 (Giovanetti et. al., 2020;
Paraskevis et. al., 2020). On virus genome
sequencing, the COVID-19 was analyzed
throughout the genome to Bat CoV
RaTG13 and showed 96.2% overall
genome sequence identity (Zhou et. al.,
2020) suggesting that bat CoV and human
SARS-CoV-2 might share the same
ancestor, although bats are not available
for sale in this seafood market (Wu and
Colleagues, 2020). Protein sequences
alignment and phylogenetic analysis
showed that similar residues of receptors
were observed in many species, which
provided more possibility of alternative
intermediate hosts, such as turtles,
pangolin and snacks (Li and Co-workers,
2020). In other words, there is potential
transmission from animals to humans that
may not be limited to bats alone. There is
possibility of intermediate hosts by some
domestic animals. At present, the mode of
transmission is through human to human
transmission via respiratory droplets.
Guan and co-workers (2020) stated
that sampled 1099 laboratory-confirmed
cases in China, reported that common
clinical manifestations of COVID-19
included fever (88.7%), cough (67.8%),
fatigue (38.1%), sputum production
(33.4%), shortness of breath (18.6%), sore
throat (13.9%), and headache (13.6%).
Their reports are similar to those of the
Centre for Disease Control (US) and other
clinical symptom reports from other parts
of the world. Liang and colleagues (2020)
showed different clinical characteristics of
corona virus disease cases between
children and their families in China.
COVID-19 in children is mainly caused
by family transmission, and their

Madu, S.N. & Ucheagwu, V. (2020). Challenges Facing Psychotherapists in Africa in the Hit of The Novel
Coronavirus 2019 (Covid-19) Global Pandemic, International Journal for Psychotherapy in Africa 5(1):1-10
3
symptoms are mild, and prognosis is better
than adults. However, their PCR result in
stool showed longer time than their
families. Because of the mild or
asymptomatic clinical process, it is
difficult for pediatricians and public health
staff to recognize early the presence of
COVID in children.
Global Epidemiology of COVID-19
The COVID-19 outbreak has quickly
turned into a pandemic, with hundreds of
thousands of cases reported globally.
Centre for Disease Control estimated the
prevalence of COVID-19 in the US as at
April 5, 2020 to be at 304,826 cases with
total deaths of 7,616. Italy has been
viewed as the worst hit in the global
pandemic. Italian civil protection
authorities as at March, 13 said the
number of infections has soared by more
than 2,500 in 24 hours while virus-related
deaths make the largest single-day jump of
250 taking the total number of infected in
Italy to 17,660 and the number of related
deaths to 1,266. With Italy at the epicentre
of Europe’s outbreak, the virus is now
present in all 27 EU countries with more
than 22,000 cases of COVID-19 having
been confirmed across Europe. Africa is
gradually witnessing a surge in COVID-19
with North Africa having the highest cases
of 6400 infections (603 deaths/1100
recoveries) as at April 13, 2020 followed
by West Africa with 3400 cases (84
deaths/664 recoveries), Southern Africa
2300 cases (35 deaths/452 recoveries),
then Central and East Africa with 1200
cases (38 and 28 deaths/ 129 and 187
recoveries) of infection respectively
(Africa CDC, April 13, 2020). On country
basis, South Africa has the highest number
of infection with 2,173 cases followed by
Egypt with 2,065 cases and then Algeria
and Morocco with 1,914 and 1,661 cases
respectively (Africa CDC, April 13,
2020). Nigeria with largest African
economy has recorded the infection cases
of 627 (21 deaths and 170 recoveries) on
19th April 2020 (Nigerian Centre for
Disease Control/NCDC, 2020). As there is
currently no known vaccine or treatment
for COVID-19, most African countries
have adopted precautions as directed by
WHO to contain the wide spread of the
virus. Among the precautions were
observing personal hygiene practices
particularly washing hands with soap
under running water, maintaining social
distancing, wearing of face masks,
sneezing in your inner flexed arm/elbow
or with disposable tissue paper. Africa
Center for Disease Control has also
advised that people should get influenza
vaccines if such is available in their
community.
At the wake of the pandemic, some
countries have adopted international and
national lockdowns limiting heavily
movements of people and goods to
prevent further spread of the virus. The
lockdown has seriously affected the
interpersonal relationships and freedom of
gathering. For example, in Nigeria, all
churches, mosques, schools at all levels,
and markets were closed to forestall
further spread of the virus.
Psychological Consequences of COVID-
19 Pandemic in Developing African
Nations
COVID-19 pandemic undoubtedly comes
with lots of social and psychological
distress particularly in resource poor
settings. People are worried about their
health and possibility of being infected
with the virus. The poor health care
facilities and corrupt nature of many

International Journal for Psychotherapy in Africa (5:1)
4
African countries leave many people
anxious and in doubt about their health
and over all protection. Psychologists and
mental health professionals have been
speculating the likely psychological
consequences that may follow COVID-19
pandemic and the subsequent measures
taken by countries to contain it. The
following sections discuss the possible
psychological consequences of the
pandemic.
COVID-19 Outbreak and Mental
Health in Africa
COVID-19 and Defense Mechanisms
To maintain psychological homeostasis,
Freud (1949) proposed the concept of
defense mechanism. Defense mechanisms
are psychological shock absorbers that
make individuals withstand stress and
pressures of life. They are mental
operations that enable the mind to reach
compromise solutions to conflicts that are
unable to resolve. These mental operations
can relieve the individual of the anxieties
following conflicts. But when defense
mechanisms are not well controlled by the
individual, it may subsequently lead to
psychological disturbances. The COVID-
19 outbreak in Africa may likely lead to
denial of reality as a form of defense
mechanism or true reality testing as a
positive adjustment.
When reality denial is a form of
defense mechanism, individuals are most
likely to underplay the pandemic and its
consequences. Denial of reality is seen in
some forms of mild psychological
disturbances where individuals deny the
existence of a known diagnosed illness
even at the expense of their lives. Low
level of education, health awareness and
ignorance about health in Africa may help
increase the possibility of denial of
COVID-19. A general observation by the
authors as to the way people respond to
lockdown instructions in some areas in
Nigeria show that many citizens are even
not aware of the consequences of the virus
or are in total denial about the virus
infection in the country. For example, we
hear the common man in Nigeria saying
that COVID-19 is ‘not real’; some say ‘it
is all about politics’; and others say it is ‘a
Whiteman’s/rich man’s disease’. In such
situations, necessary precautions that
should help prevent the spread of the virus
are undermined. At present, there are no
known research evidences from Africa on
denial of reality to COVID-19. Our
presentations are only experiential as we
await the outcome of researches on mental
health during the COVID-19 outbreak in
Africa.
Reality testing in the face of
COVID-19 leads the nation to a better
understanding of the disease progression
and possible ways to reduce spread of the
virus. However, there are failures to
reality testing and denial. When
individuals over exaggerates the realities
of situation, there is tendency of anxiety
and panic. The present situation in Nigeria
shows some signs of over exaggeration of
situation in many elite locations. Many
posts from social media particularly the
WhatsApp show extreme exaggeration of
the situation. WhatsApp social media is
full of posts on different remedies that
cure COVID-19. Anxious and uniformed
public are likely to key into these remedies
and possibly use them. Such unguarded
use may create more harm and complicate
the already heated polity. Over
exaggeration of reality can further lead to
anxiety, depression, panic and somatic
symptoms. When people over perceive the

Madu, S.N. & Ucheagwu, V. (2020). Challenges Facing Psychotherapists in Africa in the Hit of The Novel
Coronavirus 2019 (Covid-19) Global Pandemic, International Journal for Psychotherapy in Africa 5(1):1-10
5
consequences of COVID-19 outbreak,
they are more likely to become anxious
and apprehensive about their health and
those of their loved ones. Implications of
such anxieties and poor mindfulness on
mental and physical health have been
studied by Branstrom, Duncan and
Moskowitz (2011).
COVID-19 and Social Psychology of
Mental Health
Major precautions against the spread of
COVID-19 is social distance and
appropriate hygiene behaviours. It is well
known that humans are social animal and
live day to day in social interactions with
others. Among the ways humans maintain
social interactions include activities in
work places, religious and social
gatherings and schools. Human social
interactions are known to play
fundamental roles in mental health.
Abbasa and Co-workers (2019) showed
the moderating role of social support for
marital adjustment and mental health.
Their study emphasized positive
contributions of social support to marital
adjustment and significant negative
association between social support and
major mental health index including
anxiety, depression and stress reactivity.
In the hit of COVID-19 outbreak, people
are heavily advised to maintain social
isolation and avoid public gatherings
which may undermine social support.
Some studies in mental health show
negative consequences of social isolation
on physical and mental health particularly
in the elderlies. Leigh-Hunt and
colleagues (2017) in their meta-analysis of
public health consequences of social
isolation and loneliness identified a
significant association between social
isolation and loneliness with increased all-
cause mortality and social isolation with
cardiovascular disease. Narrative
systematic reviews suggest associations
with poorer mental health outcomes, with
less strong evidence for behavioural and
other physical health outcomes. Courtin
and Knapp (2017) reviewed studies on
social isolation, loneliness and health in
old age. Their finding showed that social
isolation and loneliness are significant
predictors of depression and
cardiovascular health in the population
reviewed. Tanand Colleagues (2017)
examined the relations between loneliness
and health related quality of life (HR-
QoL) among community dwelling older
citizens. Their findings showed that
participants who were lonely experienced
a lower HR-QoL than participants who
were not lonely. Emotional loneliness and
social loneliness were both associated with
a lower physical and mental HR-QoL.
Although social isolation is not the same
as loneliness, strong relationship exists
between the two factors. Interestingly,
COVID-19 has been shown to affect more
the elderly population and people with co-
existing chronic illnesses. Social isolation
is known to affect more the elderly group
although the mechanisms of action are not
yet understood. The ageing population is
at greater risk for social isolation
prescription for containing the spread of
the virus and may be more at risk with the
mental consequences of the COVID-19
pandemic.
Aside from the direct mental health
consequences of social isolation, the
indirect consequences are also important
to sustaining mental health. The present
lockdown in many countries of Africa is
likely to affect the economic development
and living standards of the people. Such
lockdown for many citizens came

International Journal for Psychotherapy in Africa (5:1)
6
unprepared and many African
governments have no plans prior to the
outbreak. This creates many psychological
imbalances for the public including
uncertainty about future, anxiety over
survival, depression over closure of works
and businesses and irritability following
continuous lockdown.
COVID -19 and Infected Patients
Patients with COVID-19 infection are
faced with some psychological
disturbances. The individual is worried
over possible survival and trauma
associated with social isolation. The sick
person is not only battling with Cov-2 but
is also battling with psychological
consequences following isolation. The
psychological consequences are necessary
factors to be managed alongside the
symptoms of Cov-2 so as to quicken the
recovery of the patients. It is known that
social isolation comes with loneliness,
anxiety and depression. These
psychological symptoms particularly
depression have been shown to
compromise immunity through their
endocrine systems mechanisms like the
pro-inflammatory cytokines and
corticosteroids stimulations (Coe, 2010;
Kiecolt-Glaser, Derry & Fagundes, 2015)
and is known to influence health and
recovery. Equally, the families of the
patients are not also immune to the
psychological consequences of the
diagnoses. The family members are
shocked and traumatized over the situation
and may be disposed to depression and
stigmatization. The psychological
strengths to look after the affected family
member and to bear the transient loss of
the quarantined family member are
important.
COVID-19: Depression, Trauma, and
Illness Anxiety in the Public
COVID-19 pandemic has also
psychological consequences in the
uninfected public. Illness anxiety is a
concept that describes apprehension
following illness people have no control
over. Because there is no cure for the
disease now, a lot of people are anxious
over their health and what they can do to
contain the virus. Such apprehension
could lead to survival behaviour where
people do things to keep safe. Such
survival acts could lead to self-injurious
behaviours like the cases of chloroquine
toxicity and increased cases of drug
addiction we hear from the social media.
Illness anxiety can as well co-exist with
depression even then complicating the
situation.
COVID-19 and Nuclear Family
Relations
Social isolation in the hit of corona virus
pandemic has created some changes in
nuclear family relations. Because people
are most likely to stay indoors, extensive
time is shared between couples and among
siblings. There are much time for parents
to interact with themselves and their
children. Because we live in a world
preoccupied with work, many families
have little time to share with their
children. The way the relationship
between couples are managed this time
determines to a significant extent how the
social isolation could impact on their
health. Couples with good understanding
can enjoy the quarantine period, take time
to discuss and rebuild their relationships.
However, couple with poor marital
relations can have their marital discord
escalated and consequently create more
problems for themselves. Because many

Madu, S.N. & Ucheagwu, V. (2020). Challenges Facing Psychotherapists in Africa in the Hit of The Novel
Coronavirus 2019 (Covid-19) Global Pandemic, International Journal for Psychotherapy in Africa 5(1):1-10
7
couple are more likely to stay at home,
increased sexual relations may be
encountered in sexually active couples.
Some people in Nigeria have even
reported in the social media of achieving
long expected pregnancies, while others
have talked about having unexpected and
unwanted pregnancies, as a result of the
lockdown. The extent to which these bring
psychological health or distress is to be
studied. Unwanted pregnancies and
consequent psychological consequences
may further be a problem for couples not
observing family planning during this
period.
Because people are compelled to
stay at home, there are tendencies of poor
regulation of eating behaviour, sedentary
life styles and consequent increase in
weight and other metabolic syndromes.
Some children are terribly bored,
especially those living in township
flats/condominiums with little space for
playing. Some parents who are not used to
staying at home with their children are
irritated by the children’s boredom. Many
workers are facing joblessness, and others
are losing job-identity. Increased drug
abuse and addiction among adolescents
and adults are expected. Physical,
emotional, psychological and sexual abuse
of children and women would be on the
increase. Some of these are possible
outcome that the public may face as a
result of social change following COVID-
19 pandemic. These issues are worth
deliberating by psychotherapists and
further provide people with possible
adaptive behaviours
Neuropsychological consequences
following COVID-19 Infection
Neurological symptoms have been
reported in some patients with SARS-2
infection. Among the symptoms were
headache, dizziness, and loss of
consciousness. Mao and co-workers
(2020) examined retrospectively
symptoms presented by COVID-19
patients for neurological symptoms.
Compared to 214 patients studied, 78
(36.4%) had neurologic manifestations.
Patients with more severe infection had
neurologic manifestations, such as acute
cerebrovascular diseases, impaired
consciousness and skeletal muscle injury.
There is every possibility that Cov-2
crosses blood brain barriers as evidence
has shown the detection of SARS corona
virus RNA in cerebrospinal fluids of
patients (Hung et. al., 2003; Lau and
colleagues, 2004). There is need to study
the neuropsychological consequences
following COVID-19 infection since there
are mounting evidence of neurological
symptoms. Neuropsychological
assessment post SARS recovery will be
helpful to ascertain future brain-behaviour
issues arising from the SARS infection.
Challenges for Psychotherapists in
Africa
The need for increase opportunities for
psychotherapy training in Africa
Due to the scarcity of properly trained
psychotherapists in Africa in general on
the one hand, and the increasing incidence
of emotional problems resulting from
poverty and underdevelopment, child
abuse and neglect, trauma resulting from
different forms of crime and abuse of
human dignity, insecurity problems like
terrorism, insurgency, kidnapping and
hijacking, increasing stress-provoking
lifestyles, tribal and national wars and
conflicts, westernization and globalisation,
and the HIV/AIDS pandemic, different

International Journal for Psychotherapy in Africa (5:1)
8
forms of cancer, and all sorts of abuse of
human dignity, on the other hand, Madu
(2016) called for urgent need for
establishment of institutions for formal
psychotherapy training in Africa. Now,
with the COVID-19 global pandemic, with
its expected effects on mental health,
behavioural, emotional, social/family
problems, and neurological consequences
(as described above), the need for training
opportunities for psychotherapists in
Africa has become more urgent than ever.
There is an urgent need for increased
number of psychotherapists to address the
problems as mentioned above. The School
of Psychotherapy and Health Sciences in
Okija, Nigeria, (www.sphs.com.ng)
(which is the first of its kind in Africa
South of Sahara) can only do as much as it
can cope with. More of such efforts are
therefore urgently needed.
Short-term psychotherapy skills-
acquisition
Normally, full-term psychotherapy
training lasts for years. For example,
based on the personal training experience
of the authors, in most parts of Europe
and America, full formal training in
psychoanalysis last for a minimum of
seven years, five years for any form of
Behaviour therapy/Behaviour
modification, four years for Client-
Centred Psychotherapy, and the same for
Gestalt therapy, etc. The speed with which
COVID-19 is spreading in Africa, with its
resultant mental, emotional and social
adverse effects, one cannot wait for such a
long-term training, before addressing them
psychotherapeutically. No African nation
was prepared for the pandemic. Therefore,
short-term training programmes on hands-
on psychotherapeutic skills are needed for
crisis and trauma intervention among
survivors of the corona virus, as well as
for the families and relatives of victims
and survivors of the virus. The issue of
stigmatisation of survivors as well as
relatives of survivors and victims’
families, need to be addressed by
psychotherapists now and after the
pandemic.
Conclusion and Recommendation
Many mental health, emotional,
behavioural and neuropsychological
problems are being envisaged to come
now as a result of the COVID-19 spread
and pandemic in Africa and thereafter.
These demand for urgent
psychotherapeutic training opportunities
which are rare to find in Africa, since
there are only a handsfull of fully trained
psychotherapists in Africa south of
Sahara. Therefore, short-term
psychotherapy skills-acquisition is a sine
qua non if Africa is to outlive the Corona
virus pandemic and maintain
psychological balance thereafter.
It is therefore recommended that
governments in Africa should have
political goodwill and offer financial
support to institutions of higher learning
that have the capacity to train
psychotherapists. This should be
considered as equally important as the
palliatives being given to cushion the
adverse effects of the lockdown as a result
of the COVID-19 pandemic. While the
governments are playing their own role,
the few psychotherapists available in
Africa should look into the above
psychologically unhealthy situation from
the point of view of crisis intervention.
Madu, S.N. & Ucheagwu, V. (2020). Challenges Facing Psychotherapists in Africa in the Hit of The Novel
Coronavirus 2019 (Covid-19) Global Pandemic, International Journal for Psychotherapy in Africa 5(1):1-10
9
References
Abbasa, J., Aqeelb, M., Abbasc, J.,
Shaherc, B., Jaffarc, A., Sundasb, J.,
Zhangc, W. (2019). The moderating
role of social support for marital
adjustment, depression, anxiety, and
stress: Evidence from Pakistani
working and nonworking women.
Journal of Affective Disorders, Vol.
244, 231-238.
Africa Centre for Disease Control and
Prevention, (13 April, 2020).
COVID-19 case update. Addis
Ababa, Ethiopia. Africa CDC.
Branstrom, R., Duncan, L., & Moskowitz,
J.T. (2011). The association between
dispositional mindfulness,
psychological wellbeing and
perceived health in a Swedish
population based sample. British
Journal of Health Psychology, 16,
300-316
Coe, C.L. (2010). All roads lead to
psychoneuroimmunology. In J.M.
Suls, K.W. Davidson and R.M.
Kaplan (eds.), Handbook of health
psychology and behavioural
medicine. New York: The Guilford
Press.
Courtin and Knapp (2017). Social
Isolation, loneliness and health in
old age: A scoping review. Health
Soc Care Community, 25,3,799-812
Freud, S. (1949). A general introduction to
psychoanalysis. New York: Garden
City Publishing.
Giovanetti, M., Benvenuto, D., Angeletti,
S., & Ciccozzi, M. (2020). The first
two cases of 2019-nCoV in Italy:
where they come from? J Med
Virol., 1–4. https://
doi.org/10.1002/jmv.25699
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou
CQ, He JX, et al. (2020). Clinical
characteristics of coronavirus
disease 2019 in China. N Engl J
Med. https://doi.org/10.
1056/NEJMoa2002032. Accessed
19/04/20.
Hung, E.C., Chim, S.S., Chan, P.K. et al.
(2003). Detection of SARS
coronavirus RNA in the
cerebrospinal fluid of a patient with
severe acute respiratory syndrome.
Clinical Chemistry 49,2108-2109.
Kiecolt-Glaser, J.K., Derry, H.M., &
Fagundes, C.P. (2015).
Inflammation: Depression fans the
flames and feasts on the heat. Am. J.
of Psychiatry, 172,11, 1075-1091
Leigh-Hunt, N., Bagguley, D., Bash, K.,
Turner, V., Turnbull, S., Valtorta, N.
&Caan, N. (2017). An overview of
systematic reviews on the public
health consequences of social
isolation and loneliness. Public
Health, Vol. 152, 157-171
Liu Z, Xiao X, Wei X, Li J, Yang J, Tan
H, et al. Composition and
divergence of coronavirus spike
proteins and host ACE2 receptors
predict potential intermediate hosts
of SARS-CoV-2. J Med Virol. 2020.
https://doi.org/10. 1002/jmv.2572
Liang, Su., Xiang, Ma., Huafeng, Yu.,
Zhaohua, Z., Pengfei, B., Yuling, H.,
Jing, S., Yanqin, L., Chun, Y., Jin,
G., Zhongfa, Z. & Zhongtao, G.
(2020). The different clinical
characteristics of corona virus
disease cases between children and
their families in China – the
character of children with COVID-
19. Emerging Microbes &
Infections, 9,1, 707-713.
Lau, K.K., Yu, W.C., Chu, C.M., Lau,
S.T., Sheng, B., &Yuen, K.Y.
(2004). Possible central nervous
International Journal for Psychotherapy in Africa (5:1)
10
system infection by SARS
coronavirus. Emerging infectious
diseases, 10,342.
Madu, S. N. (2016). Psychotherapy
Training in Nigeria, International
Journal for Psychotherapy in Africa
1(1):7-13.
Mao, L., Jin, H., Wang, M., Hu, Y., Chen,
S., He, Q., Chang, J., Hong, C.,
Zhou, Y., Wang, D., Miao, X., & Li,
Y. (2020). Neurologic
mmanifestations of hospitalized
patients with coronavirus disease
2019 in Wuhan, China. JAMA
Neurol.
doi:10.1001/jamaneurol.2020.1127.
Accessed 19/04/20.
Nigerian Centre for Disease Control
(NCDC) (2020). COVID-19 case
update (11.50pm, 19/04/20).
Twitter/Facebook:@NCDCgov/Covi
d19.NCDC.gov.ng. Accessed
19/04/20.
Paraskevis, D., Kostaki, E.G.,
Magiorkinis, G., Panayiotakopoulos,
G., Sourvinos, G., Tsiodras, S.
(2020). Full-genome evolutionary
analysis of the novel corona virus
(2019-nCoV) rejects the hypothesis
of emergence as a result of a recent
recombination event. Infect Genet
Evol.,79:104212
Tan, S.S., Fierloos, I.N., Zhang, X.,
Koppelaar, E., Alhambra-Borras, T.,
Rentoumis, T., Williams, G.,
Rukavina, T., Staveren, R.V.,
Garces-Ferrer, J., Franse, C.B., &
Raat, H. (2020). The Association
between Loneliness and Health
Related Quality of Life (HR-QoL)
among Community-Dwelling Older
Citizens. International Journal of
Environmental Research and Public
Health, 17, 600;
doi:10.3390/ijerph17020600.
Accessed 19/04/20.
Wu, F., Zhao, S., Yu, B., Chen, Y.M.,
Wang, W., Song, Z.G., et al. (2020).
A new coronavirus associated with
human respiratory disease in China.
Nature, https://
doi.org/10.1038/s41586-020-2008-3
Yan-Rong, G., Qing-Dong, C., Zhong-Si,
H., Yuan-Yang, T., Shou-Deng, C.,
Hong-Jun, J., Kai-Sen, T., De-Yun,
W. & Yan,Y. (2020). The origin,
transmission and clinical therapies
on coronavirus disease 2019
(COVID-19) outbreak – an update
on the status. Military Medical
Research,
7,11,https://doi.org/10.1186/s40779-
020-00240-0. Accessed 19/04/20.
Yin, Y., &Wunderink, R.G. (2018).
MERS, SARS and other
coronaviruses as causes of
pneumonia. Respirology, 23(2),130–
137.
Zhou, P., Yang, X.L., Wang, X.G., Hu, B.,
Zhang, L., Zhang, W., et al. (2020).
A pneumonia outbreak associated
with a new coronavirus of probable
bat origin. Nature. 2020.
https://doi.org/10.1038/s41586-020-
2012-7. Accessed 19/04/20.
Zhu, N., Zhang, D., Wang, W., Li, X.,
Yang, B., Song, J., et al. (2020). A
novel coronavirus from patients with
pneumonia in China, 2019. N Engl J
Med., 382(8), 727–33.
Igboegwu, C.I. (2020). Psychological Intervention to Break the Cycle of Violence and Accelerate
Public Safety, Security and Development (With Special Reference to Africa),
International Journal for Psychotherapy in Africa 5(1):11-21
11
Psychological Intervention To Break The Cycle Of
Violence And Accelerate Public Safety, Security And
Development (With Special Reference To Africa)
Chioma Ihuoma Igboegwu 18011 Pomelo Lane, Pflugerville, Texas 78660, USA
Abstract Pervasive and unrelenting violence threatens the safety and security of women and
children, present day survival and collective future of the people in various communities
and nations, across the globe. This tragic crisis has become one of the most serious
issues compelling the increasing attention of governments, at all levels, scholars in
traumatic stress studies, psychology, psychiatry, contemporary medicine, human
development, military and police administrators. Countries and communities are being
destroyed by violence. Images and accounts of violence pervade the media; it is on the
streets, homes, schools, workplaces and institutions. It has become a universal scourge
that tears at the fabric of society. In a world desperate to comprehend, address and
arrest the seemingly ever-enlarging explosion of violence and its psychological
aftermath, the Three-Dimensional Psychological Intervention Strategy (3-DPIS) Model
has been developed to explain the underlying factors that perpetuate violence in society
and the 3-DPIS Model to holistically address these factors and break the vicious circle
(Igboegwu, 2016).
Key words: Violence, post-traumatic stress, psychological intervention model.
Introduction
Research study on prisoners suggests that
there is a link between traumatic incident
exposure and violence perpetration
(Neller, Denney, Robert, Pietz&
Thomlinson, 2006). Foa, Ehlers, Clark,
Tolin and Orsillo (1999) explains that
chronic and prolonged exposure to
violence may develop into a
dysfunctional routine creating a link
between experiences of violence as
victims and later experiences of violence
as a perpetrator (Garbarino, 2002). While
Muller (2015) revealed that police
personnel with (vs. without) post-
traumatic stress disorder (PTSD) are at
great risk for police brutality. Research
evidence further shows that individuals
with (vs. without) PTSD have more
violent marriages and are at a higher risk
of violence towards and by their partners
(Jordan, Marmar, Fairbank, Sclenger,
Kulka, Hough & Weiss, 1992).
Despite a proliferation of research
and a large and growing evidence base to
effectively meet the needs of those

International Journal for Psychotherapy in Africa (5:1)
12
exposed to trauma, there are gaps in
knowledge, policies, institutional
capacities, due to neglect of the
psychological dimension of social and
criminal justice, public safety and
development policy agenda (Igboegwu,
2006, 2013, 2018 & 2019). These gaps
produce diverse categories of
psychologically disoriented, destabilized
and disillusioned populations and weak
institutions within which violence and its
psychological consequences thrive (Foa,
Ehlers, Clark, Tolin & Orsillo, 1999).
This cycle of violence in society can
have severe psychological consequences
in the lives of children. Deficits in the
socio-cultural environment can exacerbate
traumatic memories of children with a
history of child abuse, neglect and/or
survival of armed conflict. The adverse
mental health impact of childhood trauma
can predispose them to violence
perpetration later in life. Child abuse can
lead to suicidal ideation and attempts, as
well as the abuse of others and violent
arrests (Lansford, Miller-Johnson, Berlin,
Dodge, Bates & Pettit, 2007). Violent
conflicts and wars not only adversely
affect military and police personnel, but
hold adverse implications for the
psychological development of children in
cities, towns, villages, and private spaces.
It has adverse mental health impact on
civilians in the armed conflict
environment and creates vulnerabilities
that can lead to the problem of
intergenerational transmission of trauma
and violence among military, police and
civilian armed conflict survivors.
Attitudes and beliefs about violence
also cause direct harm as well as
determine the social and cultural use of
violence and destruction to discharge the
hopelessness, despair, and the frustration
and shame of lacking education and
employment (Igboegwu, 2013; Brandy,
2018). This can be observed in the rise in
violent conflicts and crime, including
widespread schoolyard bullying, shooting,
militancy, terrorism and escalating gun
murders.
Igboegwu (2009) explains that gaps
in the knowledge, policies, institutional
capacities and consequent deficits in the
social and criminal justice administration;
as well as internal security and
development strategies of stakeholders at
the local community, national, regional
and international levels have produced
diverse categories of psychologically
destabilized, disoriented and disillusioned
populations. These populations include
prisoners, ex-prisoners, street children,
militants, ex-militants, survivors of armed
conflict trauma, childhood trauma, gender-
based and domestic violence (GBDV), as
well as criminal, terrorist, drugs, human
and arms trafficking groups, as well as
women, children, youths and elderly, at
risk, world -wide. She further explains that
it is within these highlighted gaps in the
various sectors that violence thrives. Thus,
police and military personnel are deployed
to combat seemingly endless violence in
the society.
Igboegwu (2019) also revealed a
high prevalence of psychological
consequences of trauma, such as post-
traumatic stress disorder and depression,
in active duty Nigeria police personnel.
According to the study, Nigeria Police
personnel aged 25-34 years had the
highest occurrence of PTSD (49.2%)
followed by Nigeria Police personnel aged
35-44 years (39.3%), while Nigeria Police
personnel aged 45-54 years had the lowest
occurrence of PTSD (31.2%). In addition,
Nigeria Police personnel aged 35-44 years

Igboegwu, C.I. (2020). Psychological Intervention to Break the Cycle of Violence and Accelerate
Public Safety, Security and Development (With Special Reference to Africa),
International Journal for Psychotherapy in Africa 5(1):11-21
13
had the highest occurrence of depression
(33.7%) followed by Nigeria Police
personnel aged 25-34 years (28.8%), while
Nigeria Police personnel aged 45-54 years
had the lowest occurrence of depression
(12.5%). Comparatively, the highest
PTSD occurrence was among Nigeria
Police personnel aged 25-34 years, while
the highest depression occurrence was
among the police personnel aged 35-44
years. The least PTSD and depression
occurrences were however, among the
police personnel aged 45-54 years.
It is important to note that combat-
related psychological disorders, such as
PTSD and depression, among police
personnel do not only affect the personnel,
but their families, communities and the
general public. Combat-related
psychological disorders, such as PTSD
and depression, can lead to poor decision-
making, disciplinary problems, excessive
use of sick leave, severe difficulty in
regulating affect, which can impact
negatively on the quality of life as well as
the relationships of the security personnel.
There are also attention difficulties that
can undermine learning and employment
and thus complicate the reintegration of
the military and police returnee from
combat duty deployment with his/her
family and community. In addition, there
can be negligent accidental bullet
discharge, alcohol/drug dependence,
explosive anger, interpersonal violence,
including gender-based and domestic
violence (GBDV), murder and suicide.
Thus, deficits in the social and
criminal justice system, public safety,
security and development sectors as well
as adverse socio-cultural environment
created by these sectors produce diverse
categories of psychologically disoriented,
destabilized, disillusioned civilian trauma
survivors, who are unable to find the
means to actualize their potential. They
therefore become frustrated, resentful and
vulnerable to violent conflicts and crime,
militancy and terrorism, while the police
and military personnel deployed to quell
the unrelenting violence also sustain
psychological injuries due to critical
incident exposure associated with combat
operations and missions (Igboegwu, 2013,
2019).
The adverse mental health impact of
armed conflict, such as PTSD, and co-
morbidities, such as depression, are
predictive of violence, human rights
violations, gender-based and domestic
violence (GBDV), breeches of
international humanitarian laws (IHL) and
breeches of national and local laws and
norms that constitute what is acceptable
use of force by active duty military and
police personnel as well as intervention
forces.
Who, then, will build the city if the
people are not first built? This is a
common axiom that points to the
undisputable fact that the builders of a city
build in vain, if the people are not first
built! It is upon this premise that the
author of this article developed the Three-
Dimensional Psychological Intervention
Strategy (3-DPIS) Model for the bridging
of gaps in knowledge, policies and
institutional capacities, in order to
mobilize the cooperation of stakeholders
at the community level, national, regional
and international levels for mainstreaming
of the psychological dimension of social
and criminal justice, public safety, health,
security and development sectors, in order
to transform and empower institutions and
communities to break the cycle of
violence in the society.
International Journal for Psychotherapy in Africa (5:1)
14
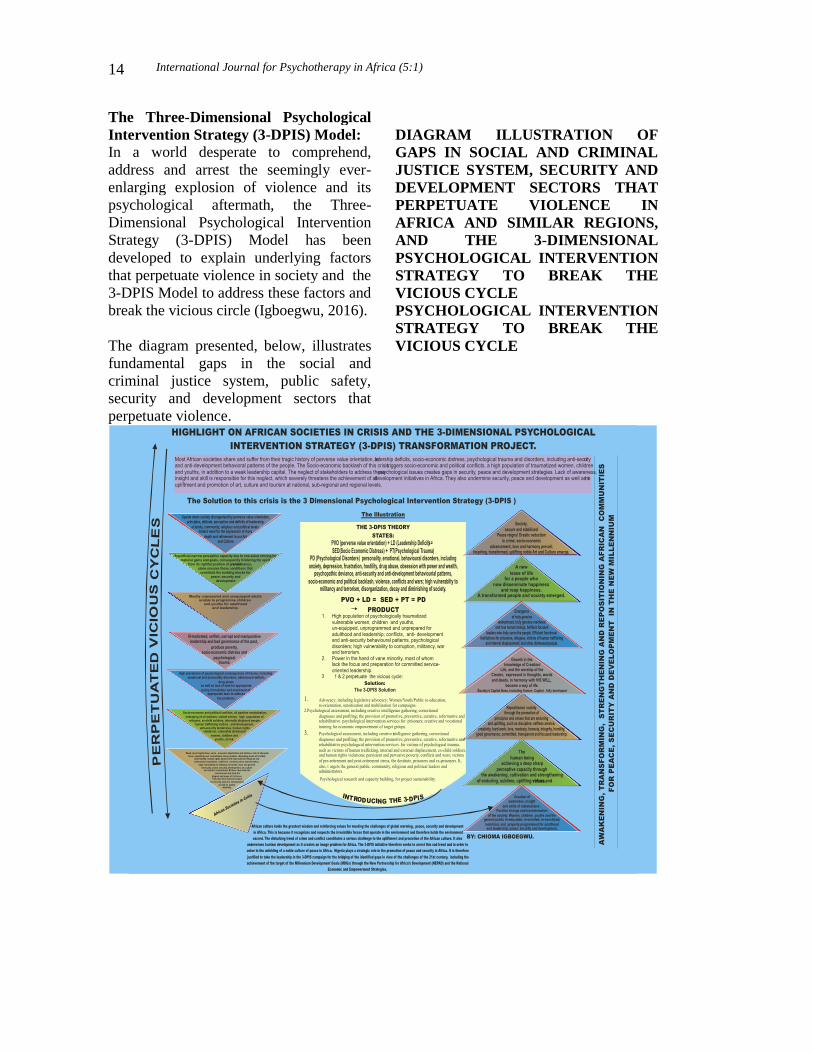
The Three-Dimensional Psychological
Intervention Strategy (3-DPIS) Model:
In a world desperate to comprehend,
address and arrest the seemingly ever-
enlarging explosion of violence and its
psychological aftermath, the Three-
Dimensional Psychological Intervention
Strategy (3-DPIS) Model has been
developed to explain underlying factors
that perpetuate violence in society and the
3-DPIS Model to address these factors and
break the vicious circle (Igboegwu, 2016).
The diagram presented, below, illustrates
fundamental gaps in the social and
criminal justice system, public safety,
security and development sectors that
perpetuate violence.
DIAGRAM ILLUSTRATION OF
GAPS IN SOCIAL AND CRIMINAL
JUSTICE SYSTEM, SECURITY AND
DEVELOPMENT SECTORS THAT
PERPETUATE VIOLENCE IN
AFRICA AND SIMILAR REGIONS,
AND THE 3-DIMENSIONAL
PSYCHOLOGICAL INTERVENTION
STRATEGY TO BREAK THE
VICIOUS CYCLE
PSYCHOLOGICAL INTERVENTION
STRATEGY TO BREAK THE
VICIOUS CYCLE

Igboegwu, C.I. (2020). Psychological Intervention to Break the Cycle of Violence and Accelerate
Public Safety, Security and Development (With Special Reference to Africa),
International Journal for Psychotherapy in Africa 5(1):11-21
15
The 3-DPIS Theory was inspired and
developed through 32 years of observing
and working with prisoners in the Nigeria
Prisons Service, pioneering psychological
services for prisoners in Nigeria, research
study on military and police populations,
in addition to being a survivor of the
Nigerian/Biafran bitter civil war as a child
(Igboegwu, 2006; 2018, 2019 ).
The Equation.
The problem of violence in the society can
be represented in an equation as follows:
PVO + LD →SED → PD →Violence and
its psychological aftermath.
The 3-DPIS Theory states that in any
environment, community, nation or region
of the world, where there is perverse value
orientation (PVO) and leadership deficits
(LD), there will, certainly, be socio-
economic distress (SED), a wide range of
psychological disorder (PD), including
emotional and personality disorders, as
well as behavior deficits, anti-social, anti-
security, anti-development behavior
patterns (Igboegwu, 2006). The adverse
socio-cultural environment created by this
problem will lead to weak institutions and
vulnerabilities that rekindle and
exacerbate traumatic memories of trauma
survivors, thereby leading to the insidious
mental health crisis that perpetuates
violence in society (Igboegwu, 2006;
2019). This is the root of violent conflicts
and crime, proliferation of small arms and
illicit weapons, prison over-population,
proliferation of criminal, militant, terrorist
networks, high populations of internally
displaced people and refugees, vulnerable
women, children and youths, at risk,
diverse categories of disillusioned,
disoriented and destabilized populations,
including civilians, police and military
populations. The diverse categories of
psychologically disoriented, destabilized
and disillusioned populations and weak
constitute the weak social capital that
perpetuates the vicious circle in such a
society. These crises diminish society and
make it vulnerable to disintegration.
The Problem: PVO + LD = SED + PD
• Perverse value orientation (PVO),
distorted values, ignoring the things
that matter to development and the
values that promote the unfolding or
development of the potentials of
human beings; Leadership deficits,
failure of leaders, at all levels, due to
the one-sided striving for material
gains and goals, earthly power and
domination, in line with the principle
of manipulation and exploitation of
the weak by the strong, which has
triggered social and economic distress
(SED) and psychological disorder(PD)
leading to the backlash effect of a
global security and development crisis.
• Africa and other similar regions of the
world have a tragic history of socio-
economic distress, psychological
trauma and the consequent emotional,
personality and behavioural disorders,
including anti-security and anti-
development behaviour patterns of the
people.
• The backlash effect of this problem
triggers violent conflicts, violent
crimes, militancy, extremism,
terrorism and illegal hazardous
migration. Millions of psychologically
International Journal for Psychotherapy in Africa (5:1)
16
traumatized women, children and
youths, including refugees, the
internally displaced, ex-child soldiers,
victims of human trafficking, human
rights abuses in various nations in
Africa and other distressed regions,
are stranded.
• Heavy casualties, decimation of huge
populations, unacceptable waste of
human and material resources being
recorded constitute an emergency that
calls for the bridging of gaps in the
social and criminal justice, public
safety, internal security and
development strategies of the affected
nations, including Nigeria and the
entire Africa region.
The Backlash Effects
The backlash effect of the tragedy
includes: socio-economic and political
conflicts; Persistent migration of people
from their homeland; Infiltration of
criminals, including armed and terrorist
groups across national and regional
borders; prison over-population; Human,
arms and drug trafficking; Drug addiction,
violent crimes, kidnappings, political
assassinations, etc; Illegal oil bunkering
and oil pipe line vandalism; Destruction of
national and foreign investments; General
insecurity of foreigners and nationals,
alike; arms proliferation; Youth militancy,
terrorism, extremism and wars; and
pandemics, including the COVID-19.
Governments of African nations ,
and other conflict-torn regions of the
world are relentlessly making the effort to
reinforce security, peace, and development
through the enactment and enforcement
of laws, as well as the establishment of
structures, such as the following: The
Sustainable Development Goals (SDGs);
The New Partnership for Africa’s
Development (NEPAD); Reinforcement of
Military and Paramilitary institutions;
Prison Reforms, Security Sector Reform;
Human Rights Laws; The mobilization of
Military and Police Forces; Global
Terrorism Strategy; and Disarmament,
Demobilization and Rehabilitation
Programs.
Important as the highlighted efforts
are, by themselves, alone, the cycle of
violence cannot be broken, unless, the
underlying psychological issues that
perpetuate violence in the communities,
nations and regions of the world are
addressed through the mainstreaming of a
holistic psychological intervention
strategy, as a priority agenda of
governments, at all levels.
During and after COVID-19
pandemic, the adverse psychological
consequences of neglect of the
psychological dimension of social and
criminal justice, public safety, internal
security and development, including
health, education, women, children and
youth development, as a priority agenda,
at the community level, national, regional
and international levels, will be
exacerbated in various families,
communities and nations across the globe.
COVID-19 pandemic will heighten the
level of mental health crisis and violence
being perpetuated across the globe as a
result of this neglect of the psychological
dimension of these critical sectors, at all
levels, across the globe. Thus, the urgent
the need for collective action through the
mobilization of communities, national,
regional and international cooperation for
mainstreaming of the psychological
Igboegwu, C.I. (2020). Psychological Intervention to Break the Cycle of Violence and Accelerate
Public Safety, Security and Development (With Special Reference to Africa),
International Journal for Psychotherapy in Africa 5(1):11-21
17
dimension, as a priority agenda, in the
highlighted sectors through the Three-
Dimensional Psychological Intervention
Strategy (3-DPIS) Model.
Through this intervention, the
vicious circle of violence will be broken,
public safety, internal security and
development, including health, education,
women, children and youth development,
will be accelerated at the family level,
community, national, regional and
international levels. The 3-DPIS is also
crucial in dealing with the corona virus
(COVID-19) pandemic prevention,
recovery and restoration of health.
Three Pillars of 3-DPIS
The 3-Dimensional Psychological
Intervention Strategy (3-DPIS) Model to
break the cycle of violence in the society
is comprised of the following three Pillars: 1. Advocacy, including legislative
advocacy;
women/children/youths/public re-
education, reorientation,
sensitization and mobilization
campaign for peace, security and
development, including the
mobilization and sensitization of
women and girls, especially, since
women and children are most
vulnerable when their communities
are torn apart by violence; and
integrating the use of psychological
science, art and culture, in
facilitation of the 3-DPIS
implementation.
2i. Psychological assessment and
intervention services for
psychologically traumatized
populations, including military,
police personnel and veterans and
their families, civilian counterparts;
civilian armed conflict survivors and
COVID-19 pandemic survivors,
including women, children, youths,
elderly, at risk, health/rescue
workers and journalists and
paramilitary personnel; preventive,
promotive, curative, reformative and
rehabilitative psychological
intervention services, including
creative/vocational skill
development and post amnesty
psychological rehabilitation.
2ii. Psychological assessment,
correctional diagnoses, promotive,
preventive, curative, reformative and
rehabilitative psychological services
for offender reformation,
rehabilitation and mental health of
prisoners, including
creative/vocational skill
development and economic
empowerment in order to integrate
them into the development and
democratic agenda of their
communities.
2iii. Psychological assessment and
promotive, preventive, curative,
reformative and rehabilitative
psychological services, including
creative/vocational skill
development and economic
empowerment/skill development for
psychologically traumatized women,
children and youths, including
displaced people, ex-street children,
ex-child soldiers, ex-combatants and
victims of human trafficking.

International Journal for Psychotherapy in Africa (5:1)
18
3. Institutional capacity building,
psychological research and
partnership to ensure project
sustainability
A special component of the 3-DPIS
Model is the women sensitization,
mobilization campaign. Women and
children are most vulnerable when their
families and communities are torn apart by
violence. There is prevalent, pervasive
violence against women and girls,
including gender-based and domestic
violence, the killing of women by
members of their families; abductions,
forced marriages and torture of women
and girls in conflict and humanitarian
crises in various nations in Europe, Asia
and Africa; United States, Canada and
others nations across the globe. In spite of
increasing deployment of military and
police personnel to combat violence and
dismantle human trafficking/ drug/arms/
terrorist/militant/criminal networks and
infrastructure, violence persists in various
countries across the globe. Gross human
rights abuses and breeches of International
Humanitarian Laws (IHL) by security and
intervention forces, including violation of
national and local laws and norms that
regulate what is acceptable use of force,
are also being recorded by national and
international human rights monitoring
groups (Igboegwu, 2019; Muller, 2015).
Research evidence also shows that
individuals with (vs. without) PTSD have
more violent marriages and are at a higher
risk of violence towards and by their
partners (Jordan, Marmar, Fairbank,
Sclenger, Kulka, Hough & Weiss, 1992).
These highlighted issues expose the
vulnerability of women in times of
conflict and humanitarian crises. Women’s
safety, emotions, bodily health and bodily
integrity are threatened and jeopardized by
the violent treatment they receive around
the world and during times of conflict. In
or out of war, women are handicapped in
society and subjected to sexual assault at a
larger rate than men partially due to their
lack of autonomy in society and power
within their families. Much of women’s
rights in society depends on the place they
are given within the family as they are the
basis for society’s structure. The power a
woman holds in society affects everything
from the family’s social class to whether
the children are sent to school or pressured
into work. The immense potentials that lie
in woman have not yet been fully
recognized, developed and utilized in the
development and general upliftment of
society, just as the immense powers that
lie in the environment have not been fully
appreciated and utilized in development of
the world.
Violence against women and girls is
perpetuated by gaps in knowledge,
policies, institutional capacities and
consequent neglect of the psychological
dimension of social and criminal justice,
public safety, security and development,
including education, health, women,
children and youth development sectors,
in the policy agenda, at all levels. An
important component of the 3-DPIS
Model is therefore the “Women Go On!”
mobilization campaign. It is aimed to
inspire and sensitize women and girls to
recognize their fundamental mission in
society, as guardians of the flame of
longing and enthusiasm in the hearts of
their people for uplifting, enduring values
that serve as building blocks of peace and
nation building. It is aimed to empower
women and girls through psychological

Igboegwu, C.I. (2020). Psychological Intervention to Break the Cycle of Violence and Accelerate
Public Safety, Security and Development (With Special Reference to Africa),
International Journal for Psychotherapy in Africa 5(1):11-21
19
science, art and culture to know their role
and enhance their skills in politics,
leadership and general upliftment of the
society, in order to facilitate the 3-DPIS
transformation project to break the cycle
of violence in the society.
Women and girls are most
vulnerable when their families and
communities are torn apart by violence.
Thus, the Women Go On! campaign
component of the 3-DPIS is aimed to
inspire, sensitize and mobilize women and
girls, world-wide, as the bedrock of their
communities and nations, and instruments
for social change, to facilitate
mainstreaming of the psychological
dimension of the highlighted sectors, as a
priority agenda, in order to transform and
empower their communities and
institutions to break the cycle of violence
and lay a firm foundation for the reign of
peace in our hitherto troubled world.
Conclusion
Countries and communities are destroyed
by violence. Images and accounts of
violence pervade the media; it is on the
streets, homes, schools, workplaces and
institutions. It has become a universal
scourge that tears at the fabric of society,
threatening the lives of women and
children, present day survival and
collective future of the people, world-
wide.
The 3-DPIS theory shows how
violence is perpetuated in society. It also
explains how gaps in knowledge, policies
and institutional capacities of
stakeholders, due to neglect of the
psychological dimension of social and
criminal justice, internal security, public
safety and development, including health,
education, women, children and youth
development, as a priority agenda,
produce weak institutions and diverse
categories of psychologically disoriented,
destabilized and disillusioned populations
that perpetuate violence in society. The 3-
DPIS aims to mobilize national, regional
and international cooperation to bridge the
highlighted gaps, transform and empower
communities and institutions at all levels,
to break the cycle of violence and
accelerate public safety, security and
development in the society. This
intervention has become a most
compelling need, in view of COVID-19
pandemic, which is bound to exacerbate
the mental health crisis and cycle of
violence being perpetuated by the
highlighted neglect. In facilitation of the
agenda to break this vicious circle,
women and girls are to play a key role in
inspiring and uplifting their land and
people, recognizing their fundamental,
natural role and inherent abilities as the
guardians of the flame of longing and
enthusiasm for the values that serve as
building blocks of peace and nation
building.
Women and children are most
vulnerable, when their families and
communities are torn apart by violence.
How the mother hen weaves her
protective, loving wings over her chicks to
protect them from the evil eye of
predatory hawks, is how a truly conscious,
genuine woman envelops and shields her
children, community and nation through
her inspiring, protective, caring, loving
thoughts, words and actions, so that they
survive the harsh, evil, challenging, visible
and invisible influences of the world and
actualize their potential. Thus, the woman
creates a bridge to the life-giving,
sustaining power of God in creation, thus,

International Journal for Psychotherapy in Africa (5:1)
20
laying the hitherto neglected firm
foundation for a sustainable, global
civilization. When peaceful, safe, secure
communities and nations are created
through the bridging of gaps in
knowledge, policies and institutional
capacities of stakeholders, mainstreaming
of the psychological dimension as a
priority agenda in the social and criminal
justice, public safety, security and
development, including health, education,
women, children and youth development,
communities and institutions, at all levels,
will be transformed and empowered to
break the cycle of violence. Women,
children, youths, the elderly, all categories
of the people in all their diversities will,
then, be able to live, work, flourish and
actualize their potentials in peaceful, safe,
secure, developed communities and
nations.
The 3-DPIS Model will guide the
mainstreaming of the psychological
dimension, as a priority agenda, in the
social and criminal justice, public safety,
internal security and development sectors
in Nigeria, other nations in Africa and
world-wide. It should be integrated into
the agenda for conflict prevention,
management and post conflict
reconstruction, as well as COVID-19
pandemic prevention, recovery and
restoration of health. It will address the
vulnerabilities that perpetuate violence, as
well as restore, heal and rehabilitate
psychological consequences of trauma,
including the adverse mental health impact
of armed conflict and COVID-19
pandemic Africa and other regions of the
world. The 3-DPIS, also, provides the
guiding light for teachers, in researchers,
clinicians in the traumatic stress field and,
indeed, all stakeholders to make more
effective and sustainable impact through
their services in the society for the
enthronement of peace in our hitherto
troubled world.
The 3-DPIS Model integrates
psychological science, art and culture in
psychotherapy and provides a holistic
intervention to address the mental health
crisis of PTSD and co-morbidities, such as
depression, which perpetuate violence in
the society. It will facilitate pro-social
engagement with all diverse categories of
the population, mobilizing their
cooperation at the community level,
national, regional and international levels,
including the dissemination of evidence-
based data, to bridge the gaps in
knowledge, policies and institutional
capacities in the highlighted sectors within
which violence thrives. It will transform
and empower communities and
institutions, at all levels, to mainstream the
psychological dimension of social and
criminal justice, public safety, security and
development sectors, including health,
education, women, children and youth
development, as a priority agenda, in order
to break the cycle of violence, accelerate
public safety, security, and development
for the reign of peace in our hitherto
troubled world.
References
American Psychiatric Association (2013).
Diagnostic and statistical manual of
mental disorder (5th ed.), Arlington,
VA: American Psychiatric
Association
Brady, K. T. (1997). Post-traumatic stress
disorder and co-morbidity:
Recognizing the many faces of
PTSD. Journal of Clinical
Psychiatry, 58 (9), 12 -15.
Igboegwu, C.I. (2020). Psychological Intervention to Break the Cycle of Violence and Accelerate
Public Safety, Security and Development (With Special Reference to Africa),
International Journal for Psychotherapy in Africa 5(1):11-21
21
Burnam, M. A., Stein, J. A., Golding, J.
M., Siegel, J. M., Sorenson,
S.B., Forsythe, A. B. & Telles, C.A.
(1988). Sexual assault and mental
disorders in a community
population. Journal Consulting
Clinical Psychology. 56(6):843-50.
Foa, E.B.; Ehlers, A.; Clark, D. M.; Tolin,
D. F. & Orsillo, S. M. (1999). The
post-traumatic cognitions inventory
(PTCI): Development and
validation. Psychological
Assessment. 11:303–314.
Garbarino, J. (2002). Forward: Pathways
from childhood trauma to adolescent
violence and delinquency. Journal
of Aggression, Maltreatment, and
Trauma, 6(1), xxvxxxi. Gibson, L.
E., Holt, J. C., Fondacaro, K. M., T
Igboegwu, C. I. (2006). Security, Peace
and Development Strategies in
Africa: Bridging the Gaps. Abuja,
Nigeria, Yaliam Press Ltd.
Igboegwu, C. I. (2006). The 3-
Dimensional psychological
intervention strategy diagram
illustration, theory and model for
transformation and empowerment of
African communities and institutions
for sustainable peace, security and
development in the new millennium
(pp.40) In C. I. Igboegwu (2006).
Security, Peace and Development
Strategies in Africa: Bridging the
Gaps. Abuja, Nigeria, Yaliam Press
Ltd.
Igboegwu, C. I. (2013). Adverse mental
health impact of armed conflict in
Africa. Unpublished paper presented
at the Seminar held by the
Department of Psychology,
Nasarawa State University, Keffi,
Nigeria
Igboegwu, C. I. (2018). Prevalence and
predictors of post-traumatic stress
disorder and depression among
Nigeria police personnel.
(Unpublished doctoral thesis).
Nasarawa State University, Keffi,
Nasarawa, State, Keffi, Nigeria
Igboegwu C. I. (2019, November). The
Co-morbidity of post-traumatic
stress disorder and depression in
personnel of Nigeria Police Force.
Poster presented at the 35th
Conference of the International
Society for traumatic Stress Studies,
held in Boston, Massachusetts, #
245
Jordan, K. B.; Marmar, C. R. &Weiss, D.
S. (1992). Problems in families of
male Vietnam veterans with
posttraumatic stress disorder.
Journal of Consulting Clinical
Psychology. 60(6):916-26.
Lansford, J.E., Miller-Johnson, S. &
Berlin, l.J. (2007). Early Physical
Abuse and Later Violent
Delinquency: A Prospective
Longitudinal Study. Journal of
Child Maltreatment. 12: 3, 233-245
Muller, R. T. (2015, November, 2012).
Officers with PTSD at Greater Risk
for Police Brutality. Psychology
Today. New York City
Neller, D. J.; Denney, R. L.; Pietz, C. A.
& Thomlinson, R. Paul (2006). The
Relationship between Trauma and
Violence in a Jail Inmate Sample.
Journal of Interpersonal Violence,
21: 9, 1234-1241.
World Health Organisation (2014). Global
status report on violence prevention.
World Health report. Geneva. World
Health Organization.
https://www.ncbi.nlm.nih.gov/pubmed/?term=Sorenson%20SB%5BAuthor%5D&cauthor=true&cauthor_uid=3264558
https://www.ncbi.nlm.nih.gov/pubmed/?term=Sorenson%20SB%5BAuthor%5D&cauthor=true&cauthor_uid=3264558
International Journal for Psychotherapy in Africa (5:1)
22
The Relevance Of Acceptance And Commitment
Therapy (ACT) In The Treatment Of Emotional
Numbing Among The Adolescents:
A Narrative Review
Uchenna E. Enem
Educational Foundations, Veritas University, Abuja
Bahago Samaila
Educational Foundations, Veritas University, Abuja
Abstract The issue of emotional numbing is a serious emotional challenge among the adolescents
and which is greatly impacting on them negatively and sometimes goes unnoticed until
the damage is done. The study explored the concept of emotional numbing, its symptoms
and the causes for a clear understanding of the phenomenon. It also examined the
Acceptance and Commitment therapy (ACT), its core processes as a suitable therapeutic
property to resolve the emotional problem of the adolescents who go through such pain.
The ACT is a process and mindfulness model which promotes psychological flexibility
through fostering openness, awareness and engagement as illustrated in its six core
processes. It was observed that the ACT promotes emotional awareness through the
functions of the six core processes of the ACT model and as a result, could be adopted to
manage the challenges of emotional numbing among the adolescents. The researchers
therefore recommend that the therapists identify such adolescents in the schools and
address their issues with the ACT model.
Key words: Adolescents, Emotional Numbing, Psychological flexibility/inflexibility and
Acceptance and Commitment Therapy (ACT).
Introduction
Emotion is a very important aspect of
human life which determines how we
function in life. Emotions manifest in
cognitive, behavioural and physiological
properties of man and as a result
influences human behaviour. Daniel
(2011) has observed that emotions are
state of feelings that result in physical and
psychological changes that influence our
behaviour. Emotions are multifaceted
phenomenon that involves changes in
subjective experience, behaviour and
physiology (Gross, 2014).This explains
that emotion is behaviourial, we behave in
a certain way due to our emotions; people
who can readily express their emotions
behave differently from people who
conceal their emotions. Emotions are also
instrumental to our motivation in life, be it

Enem, U.E. & Samaila, B. (2020). The Relevance of Acceptance and Commitment Therapy (ACT)
in the Treatment of Emotional Numbing among the Adolescents: A Narrative Review,
International Journal for Psychotherapy in Africa 5(1):22-34
23
positive or negative (Gaulin et al, 2003).
Though emotion is not a causal force but
comprises of components such as anger,
mood, motivation, temperament,
disposition etc.
The study of emotion is a necessary
outcome in the life of the adolescents
because they spend quite amount of time
learning in the classroom and interacting
actively which involves a lot of emotions.
Emotions also predict important learning
outcome as well as future career choices
(Valiente et al., 2012). These researchers
have juxtaposed students’ emotion with
their academic achievement, asserting that
the former influences the latter.
Studying emotions within a group of
adolescents lends support to Emotional
Contagion which is a situation of one
person’s emotions and related behavior
reflecting a similar emotions and
behaviour on other people. Emotional
contagion was observed to influence
significantly the individual level attitude
and group processes (Barsade, 2002). In
his study on group emotional contagion,
positive emotional contagion members
experienced improved co-operation,
decreased conflict, and increased
perceived task performance. Evidently,
maintaining positive emotions or
emotional stability among our adolescents
is a way of improving the quality of their
achievement; be it academics, social life,
and their future career choices. Albeit, it is
a fact that emotions generally are not well
addressed in researches, in the words of
Zembylas (2003), he pointed out that
emotion was an elusive construct that
could not easily be measured and regarded
a feminine issue and not a worthwhile
research topic.
The adolescence is a formative
period in the life of the adolescents, during
which they experience emotional changes
as well as other changes. Heller et al
(2016) defined adolescence as a time of
transition from childhood to adulthood
when individuals experience significant
changes in cognitive capabilities, physical
maturity, biological functioning, social
environment and family and peer
relationships. Though some of them may
go through these challenges successfully,
there is need to understand and maintain
their emotional development and habit, to
promote their well-being, improve their
interpersonal relationships, adopt effective
academic standard which could foster their
career development and assist them to
integrate properly in the society.
Researchers like Rojas et al (2015) have
related the adolescents’ poor
psychological outcome such as anxiety,
suicidal thought etc to a range of
emotional intensity. They described the
emotions as; high frequency and intensity
of positive emotions, low frequency and
intensity of negative emotions, instability
of positive and negative emotions, and low
emotional clarity.
Maintaining emotional stability
requires training, counselling and
psychotherapy depending on the intensity
and the trigger of the emotional instability.
Emotional numbing is a type of emotion
that one may have without being aware of
it and may exacerbate the adolescents’
activities, development and productivity if
it prolongs.
Emotional Numbing
Emotional numbing is an aspect of
emotion that has not received much
attention probably because it is overtly a
situation of shutting off negative feelings.
Litz and Gray (2002) posited that
emotional numbing entails a deficit in
International Journal for Psychotherapy in Africa (5:1)
24
responsiveness to positive emotional
stimuli but not to negative emotional
stimuli. A person may decide to shut out
feelings and certainly not feel anything.
Shutting out feelings may make one feel
he/she is in control but it comes with
underlying effect on the individual
especially when the numbness lasts for a
long time. It manifests as feelings of
emptiness, confusion, exhaustion and in
diminished responsiveness to emotional
stimuli. Mendez (2019) described
emotional numbing as a mental and
emotional process of shutting out feelings
and may be experienced as deficits of
emotional response or reactivity. She also
explained that “while emotional numbing
blocks or shuts down negative feelings
and experiences, it also shuts down the
ability to experience pleasure, engage in
positive interactions and social activities,
and interferes with openness of intimacy,
social interests, and problem-solving.
Emotional numbing obviously affects
one’s feelings, his/her actions and social
relationship.
Emotional numbing is a diminished
interest or pleasure in important activities:
feelings of detachment or estrangement
from people: and a restricted range of
emotion (APA, 2000). Emotional numbing
makes one feel;
isolated from and superficial to
reality,
invisible to and detached from other
people and activities,
numb to people’s reactions and
opinions,
loss of interest in important
activities one used to enjoy,
flat in both physical and emotional
situations
inability to participate in life,
difficulty in expressing positive
feelings like joy, happiness, and love
confusion and lack of
communication
sleep walking through the day time
altered sense of sight, feelings and
sounds,
The foregoing explains why
Diagnostic and Statistical Manual–v
(DSM-5) (2013) classified emotional
numbing as Depersonalization-de-
realization disorder (DD) (Huizen, 2017).
Researchers have stressed the
semblance between emotional numbing
and posttraumatic stress disorder saying
that the people who suffer PTSD
experience emotional numbing- a deficit
to express or experience emotion (Tull,
2003). According to Kerig et al (2016),
emotional numbing has implications for
maladaptive outcomes in adolescence such
as delinquent behaviour. Delinquent
behaviors may include the addiction to,
use and abuse of substances, sexual related
offences, truancy, stealing, pilfering,
aggressions, violence and the like. He
drew attention to the symptom of
emotional numbing in posttraumatic stress
disorder (PTSD) in his study by
investigating whether numbing of positive
emotions was associated with PTSD
symptoms above and beyond numbing of
negative emotions, general emotional
numbing or depressive symptoms among
at-risk adolescents. The result in
hierarchical multiple regression evinced
that general emotional numbing and
numbing of anger accounted for
significant variance with PTSD symptoms
while numbing of sadness and positive
emotions were correlates of depressive
symptoms.

Enem, U.E. & Samaila, B. (2020). The Relevance of Acceptance and Commitment Therapy (ACT)
in the Treatment of Emotional Numbing among the Adolescents: A Narrative Review,
International Journal for Psychotherapy in Africa 5(1):22-34
25
In an attempt to underpin the
emotional numbing symptoms associated
with PTSD, Tull et al. (2003) discovered
that hyperarousal symptoms predicted
emotional numbing above and beyond
experiential avoidance and other
symptoms of PTSD. Foa et al (1992)
expressed that emotional numbing
symptoms are the distinctive feature of
PTSD from other anxiety disorder.
Researchers for example Huizen
(2017) identified some causes of
emotional numbing to include:
1. Trauma and Stress: Individuals who
are exposed to continual stress may
develop emotional numbness as a
coping mechanism to avoid the
experience. Huizen (2017) listed
some examples of stress as; loss of
close one, traumatic experiences like
car crash, bombing, physical abuse,
exposure to violence, emotional
abuse or neglect, impairment,
interpersonal conflict and financial
crisis.
2. Medications: The anti-anxiety drugs
and Anti-depressant medications
have been found to have side effect
of emotional numbing on the young
children who took them.
3. Other common causes of temporary
emotional numbness include:
seizure, drug abuse, panic attacks,
severe depression, severe anxiety
and posttraumatic stress disorder.
Clients in this category, experience a
lot of pain which include psychological
and physical pain. HeShuchang et al
(2011) found in their study that scores of
emotional distressed pain patients
(Chronic backache) were higher than the
control group, explaining that emotional
distress could lead to chronic pain. The
professionals who treat emotional
distressed pain find it difficult to provide a
soothing solution to their problems.
Medical intervention, in most cases may
cause further problems in terms of chronic
pain, though might be helpful with acute
pain (Van Tulder et al (2000).
Based on the researchers’
experience, emotional numbing is a
serious problem which the adolescents
experience all the time. The temporary
emotional numbing might not be
dangerous but its persistence impacts on
their academic achievement. An
adolescent who is experiencing emotional
numbing as a result of trauma, shock or
other forms of stressors may feel alienated
or act in alienation to things around him
for instance he/she may forget
examination time or to write his or her
name and matriculation number on the
answer script and when confronted may
look aloof to the situation. Sometimes they
are encountered wandering hopelessly in
the compound, at times talking to
themselves, appearing tattered, not placing
value and committed to their goals,
playing truancy to class work and dwell
much on the pain and seeking for
immediate relieve from it. Such search for
relieve from emotional discomfort is
destructive, a situation known as
psychological inflexibility. Therapists
need to identify the cause of the numbing
and help resolve the pain clinically.
Given the situation, emotional
numbing among the adolescents could be
treated with Acceptance and commitment
therapy for its efficacy in chronic pain.
ACT has also adapted an assessment
measure for the pain adolescence, Chronic
Pain Acceptance Questionnaire,
Adolescent Version (CPAQ-A)

International Journal for Psychotherapy in Africa (5:1)
26
Description of Acceptance and
Commitment Therapy (ACT)
Acceptance and Commitment Therapy
(ACT) is a psychotherapy of learning to
accept change in circumstance but try as
much as possible to make the best of the
situation without trying to change your
perception of the outcome (Chalk, 2019).
This therapy is essential to coping with
chronic pain from long-term conditions.
Emotional numbing if lasts longer can
trigger a condition of chronic pain as
reported above. As a result, the processes
and methods incorporated in the ACT will
have a far reaching effect in treating
emotional numbing.
ACT according to Eccleston et al
(2009) emanated as a call to improve the
standard of psychotherapy by focusing
adequate attention on therapeutic
processes through selection of processes
and methods known to produce
improvement. In line with the
consideration, ACT was one of the
approaches within Cognitive Behaviour
therapy (CBT) that met the challenge.
ACT is an acceptance and mindfulness
based-approach that can be applied to
many emotional problems and disorders. It
is also a process-based, third wave,
cognitive behavioural therapy (CBT). It
has been reported to solve a broad set of
psychological problems (Ruiz, 2010&
Bach and Hayes, 2002). ACT approaches
psychological problem in a dynamic
manner manifesting in verbal, social,
emotional and direct sensory influences on
behaviour with emphasis on how suffering
emerges with human abilities in language
and thought. People who are in pain
exhibit psychological inflexibility or
destructive experiential avoidance, a
constant behaviour pattern geared towards
searching for immediate relieve of
minimizing physical and emotional
discomfort (Hayes, 1999). They spend
great effort in fighting against their
experiences of pain; which includes
physical sensations, emotions, memories,
images and thoughts about the pain. They
normally indulge in reducing their
physical activities, avoiding thoughts of
pain or by engaging in excessive thoughts
of pain, avoiding people, ruminating about
the causes of their pain, asking
overwhelming questions about their pain
or seeking a second opinion to their
medications. ACT emphasizes observing
thoughts and feelings as they are, without
trying to change them and behaving in
ways consistent with valued goals and life
direction. Its goal mainly, is to reduce the
dominance of pains in someone’s life and
improve daily functioning (McCracken,
2011) through increased psychological
flexibility rather than increased
psychological inflexibility or destructive
experiential avoidance. Psychological
inflexibility or experiential avoidance can
only reduce pain tolerance and increase
the enormity of the pain (Gilbert et al,
2004).Psychological flexibility on the
other hand is the ability to persist or to
change behaviour, being conscious in the
midst of discomfort and other
discouraging experiences guided by goals
and values (Hayes, 2000). This implies
having the ability to accept pain, or any
form of discomfort in manner to reduce
the dominance of such pains in ones’ life.
A patient who is experiencing emotional
numbing as a result of trauma, one has to
develop the capability to accept the pain
and other devastating experiences through
reduction of dominance of the pain. The
basic understanding of ACT in respect to
chronic pain is that in as much as the pain
hurts, it is the struggle with the pain that
Enem, U.E. & Samaila, B. (2020). The Relevance of Acceptance and Commitment Therapy (ACT)
in the Treatment of Emotional Numbing among the Adolescents: A Narrative Review,
International Journal for Psychotherapy in Africa 5(1):22-34
27
causes suffering or more pain. In the case
of the chronic pain, the causal and the
maintaining factors may be uncertain and
the struggle to reduce or remove the pain
may not be successful. Be it the case,
McCracken et al (2004) posited that the
continuing attempts to control the pain (a
situation Hayes, 2000 termed
psychological inflexibility) may be
maladaptive especially if the pain control
measures cause unwanted side effects or
lack of involvement in valued activities
like family relationships, dedication to
work, community roles.
ACT emphases is on seeing that
patients’ responses toward the symptom of
pain is more successful in relation to their
own goal through the increase of
psychological flexibility. Patients
experiencing emotional numbing in ACT
will realize that turning away from pain
and distress simultaneously result to
turning away from their values and goals.
Psychological flexibility comprises of six
therapeutic processes which are organized
into a structure known as hexaflex, which
are; Acceptance, Cognitive defusion,
Flexible present-focused attention, Self-as
context, Values and Committed action
(Hayes, 1999). Taking a look at the
processes, Feliu-Soler et al (2018)
described them thus: Acceptance is
described as the ability to embrace or
accept the unwanted experiences (pain,
thoughts, feelings, memories etc) in
connection to one’s goals. Cognitive
defusion is the ability to differentiate
between the thoughts and the experiences
which the thoughts relate. It means
experiencing thoughts as thoughts without
getting entangled in the literal meaning of
thoughts. Therefore it is the process of
learning to notice the process of thought
rather than getting caught up in the
content. They described flexible present-
focused attention as being able to connect
with the present moment and track
moment to moment experiences. Self-as a
context is the distinction between the
observed thoughts /feelings and the person
who observes. They saw values as freely
chosen directions connected with desired
aims and goals that guide actions. Lastly,
committed action is related with choosing
a course of action guided by value, and
then persisting in this choice, or changing
one’s direction if need be.
The hexaflex is the key model of
Acceptance and Commitment Therapy
(ACT) framework encompassing the
structure of the six core processes (as
mentioned above) and the treatment guide.
When the clients work through the key
areas, they identify areas of entanglement
and are able to remove themselves from
such entanglement. The psychological
flexibility is at the centre of the ACT
model. The six core processes relate to
one another as well foster psychological
flexibility. The six core processes are in
three components; Open (acceptance and
cognitive defusion), Aware (Contact with
the present and self-as a context) and
Engaged (values and committed action) as
illustrated below
Figure 1: The hexaflex model of ACT for
psychological flexibility and
inflexibility
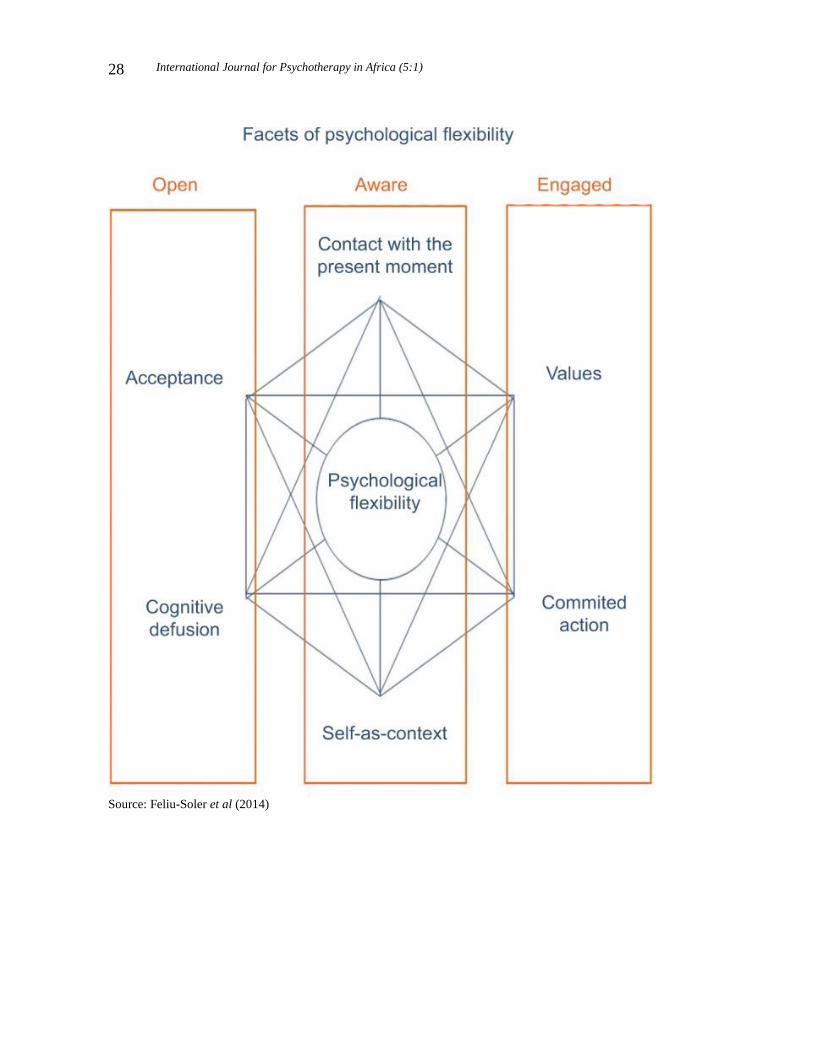
International Journal for Psychotherapy in Africa (5:1)
28
Source: Feliu-Soler et al (2014)

Enem, U.E. & Samaila, B. (2020). The Relevance of Acceptance and Commitment Therapy (ACT)
in the Treatment of Emotional Numbing among the Adolescents: A Narrative Review,
International Journal for Psychotherapy in Africa 5(1):22-34
29
Measuring the six core processes of
ACT in relation to Emotional Numbing
(1). Acceptance: The most widely
used assessment measures in pain context
for acceptance is a 20-item Chronic Pain
Acceptance Questionnaire (CPAQ)
developed by McCracken et al (2004).
The scale has emphasized on two major
aspects of pain assessment:
(a) Achieving acceptance is the
willingness to experience pain, it reflects
the absence of attempts to control or
reduce pain. Ones’ thoughts and feelings
about pain must change before one can
take important steps in my life. Achieving
acceptance for the emotional numbing
adolescents depends on their being able to
open up fully to the reality of the pain or
discomfort they are experiencing and
accepting both the positive and negative of
the new situation. Focusing only on the
negative side will lead to self-defeatism,
and depression while a focus on the reality
and the worst possible outcome will assist
them achieve genuine acceptance and gain
productive life while experiencing
discomfort.
(b) Activity engagement entails
engaging in valuable activities in the
presence of pain, living a good life
irrespective of pain or discomfort. Pain
acceptance in ACT was correlated with
lower self-rated pain intensity, less self-
rated depression and pain-related anxiety,
greater physical and social ability, less
pain avoidance and better work status.
This scale will afford the therapist the
level of acceptance of pain by the
adolescents. An adolescent suffering
emotional numbing, the cause of the pain,
be it stress or trauma, should be accepted
and they should not struggle with attempts
to remove the pain. The therapists should
provide activities that the adolescents
could engage in as to move on with their
life endeavours rather than focus on the
pain which could generate more
devastating issues.
The CPAQ was validated by Wicksell et
al (2009) among other researchers, they
compared CPAQ with the Tampa scale of
Kinesiophobia in the treatment of pain in
an empirical study. The study investigated
the psychometric properties of the
instrument and compared its relation to
another pain assessment scale-Tampa
Scale of kinesiophobia. The result
indicated that CPAQ explained more
variance than Tampa Scale of
kinesiophobia in pain intensity, disability,
life satisfaction, and depression.
(2). Cognitive Defusion. The widely
used measure for cognitive defusion is the
Cognitive Fusion Questionnaire (CFQ). It
is a seven item scale with all the items
keyed towards cognitive fusion. In ACT,
cognitive defusion intervention tries to
detach thoughts from actions and create
psychological distance between the person
and their thoughts, memories, beliefs and
self-stories. This suggests that how we
react to mental occurrences is basically
essential. For instance, ones’ thought
should not cause one emotional pain or
distress. The adolescents should be
thought decentering, to step outside of
their mental events towards objective
stance in life. Evidence has lend support
on the reliability and validity of the CFQ
for use among people with chronic pain
(Gillanders et al, 2014)
(3). Flexible present-focused
attention: This aspect of the process is
mostly measured by questionnaires that

International Journal for Psychotherapy in Africa (5:1)
30
measure mindfulness. According to Feliu-
soler et al (2018), the most commonly
used is the Mindful Attention Awareness
Scale (MAAS). The scale is a 15-item one
that measures the general tendency to be
attentive to one’s experiences in daily life
ie. The level of one’s mindfulness or
mindlessness to moment-to-moment
activities. Abilities in trait mindfulness
improves psychological and physical well-
being, manifesting in autonomy, vitality
and satisfaction. The authors of this scale
have ascertained its validity and reliability
across cultures and ages in patients with
chronic pain. The adolescent of emotional
numbing should be discouraged against
dwelling in the past. They should pre-
occupy themselves with the present issues
instead of the past or even future events or
occurrences. Some of them may not be
aware of what they doing until they fall
into great problems. For instance, an
adolescent in a counselling session who
was recovering from a shock in an
accident has maintained that he did know
how his car got into the gutter. He was
neither hit by another car nor did his car
developed a fault. The scale will help
determine how the adolescents are focused
in what they are doing.
(4). Self-as a context: The Self-
Experience Questionnaire (SEQ) is the
mostly widely used assessment measure
for self in people with chronic pain. SEQ’s
validity and reliability was ascertained for
measure of self as defined within the
psychological flexibility model Yul et al
(2017). It is a 15-item questionnaire for
investigating “Self” in chronic pain. The
adolescents through the response to the
items, elucidate their level of self -
separateness from thoughts, emotions and
sensations. Self-as a context entails an
experience of taking a perspective from
which to observe one’s psychological
experience, a sense of separation from of
containing one’s psychological
experiences. Be it the case, the adolescents
should learn to a distinction between their
experiences and Self through which they
could improve their psychological
flexibility.
(5). Value: The ACT model
emphasizes on values-based action for the
treatment of chronic pain. It developed a
measure for value known as Chronic Pain
Value Inventory (CPVI), a 12-item
measure. The respondents rate the
importance of the value they hold for in
six domains of live functionalities: family,
friends, work, intimate/close interpersonal
relationships, health, and growth or
learning and their success in at living
according to them on a 5point scale.
Evidently, the greater success scores are
associated with better future functioning
(McCracken et al, 2014). The adolescents
based on their rating are expected to rate
high on the domains for vitality and
productivity irrespective of pain. If reverse
is the case they need to be drilled to place
values on the things that matter in their
lives.
(6). Committed Action: Finally the
measure for committed action. The most
widely measure on this aspect is the
Committed Action Questionnaire (CAQ).
Its reliability and validity for the treatment
of chronic pain was ascertained. It has a
version of 18 items and a version of 8-
items (CAQ-8). It assesses the construct of
committed action drawn from the
psychological flexibility model of ACT.
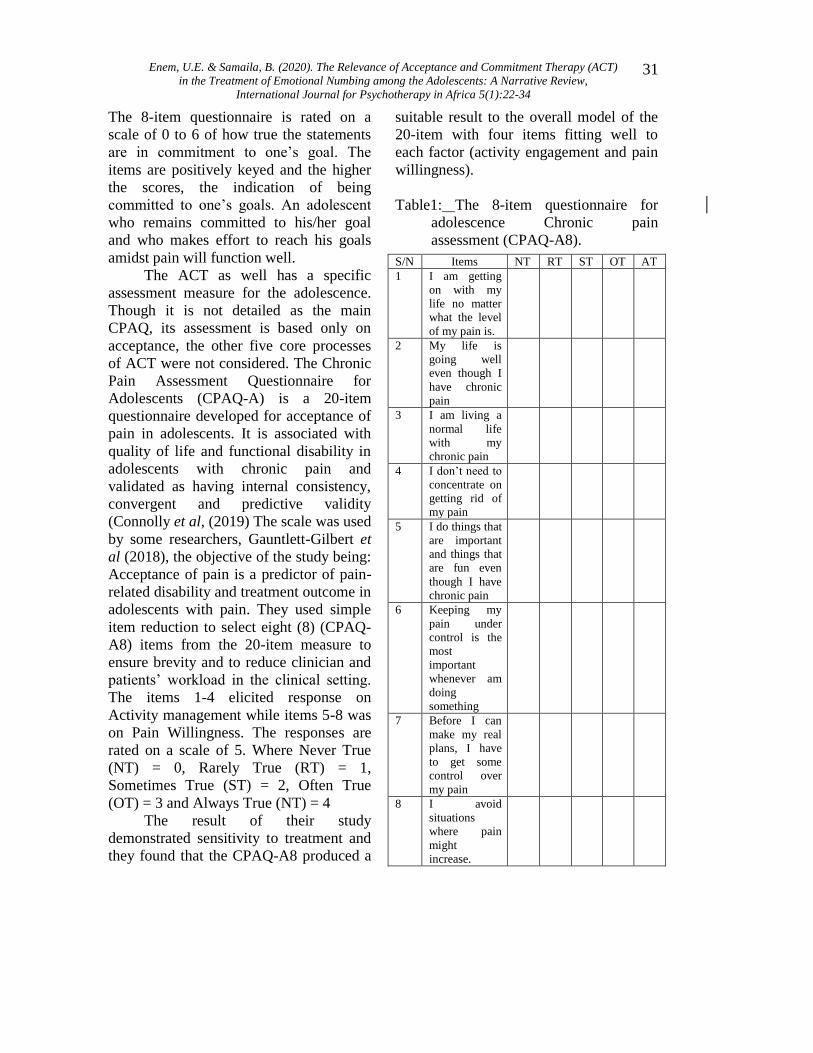
Enem, U.E. & Samaila, B. (2020). The Relevance of Acceptance and Commitment Therapy (ACT)
in the Treatment of Emotional Numbing among the Adolescents: A Narrative Review,
International Journal for Psychotherapy in Africa 5(1):22-34
31
The 8-item questionnaire is rated on a
scale of 0 to 6 of how true the statements
are in commitment to one’s goal. The
items are positively keyed and the higher
the scores, the indication of being
committed to one’s goals. An adolescent
who remains committed to his/her goal
and who makes effort to reach his goals
amidst pain will function well.
The ACT as well has a specific
assessment measure for the adolescence.
Though it is not detailed as the main
CPAQ, its assessment is based only on
acceptance, the other five core processes
of ACT were not considered. The Chronic
Pain Assessment Questionnaire for
Adolescents (CPAQ-A) is a 20-item
questionnaire developed for acceptance of
pain in adolescents. It is associated with
quality of life and functional disability in
adolescents with chronic pain and
validated as having internal consistency,
convergent and predictive validity
(Connolly et al, (2019) The scale was used
by some researchers, Gauntlett-Gilbert et
al (2018), the objective of the study being:
Acceptance of pain is a predictor of pain-
related disability and treatment outcome in
adolescents with pain. They used simple
item reduction to select eight (8) (CPAQ-
A8) items from the 20-item measure to
ensure brevity and to reduce clinician and
patients’ workload in the clinical setting.
The items 1-4 elicited response on
Activity management while items 5-8 was
on Pain Willingness. The responses are
rated on a scale of 5. Where Never True
(NT) = 0, Rarely True (RT) = 1,
Sometimes True (ST) = 2, Often True
(OT) = 3 and Always True (NT) = 4
The result of their study
demonstrated sensitivity to treatment and
they found that the CPAQ-A8 produced a
suitable result to the overall model of the
20-item with four items fitting well to
each factor (activity engagement and pain
willingness).
Table1: The 8-item questionnaire for
adolescence Chronic pain
assessment (CPAQ-A8).
S/N Items NT RT ST OT AT
1 I am getting
on with my
life no matter
what the level
of my pain is.
2 My life is
going well
even though I
have chronic
pain
3 I am living a
normal life
with my
chronic pain
4 I don’t need to
concentrate on
getting rid of
my pain
5 I do things that
are important
and things that
are fun even
though I have
chronic pain
6 Keeping my
pain under
control is the
most
important
whenever am
doing
something
7 Before I can
make my real
plans, I have
to get some
control over
my pain
8 I avoid
situations
where pain
might
increase.

International Journal for Psychotherapy in Africa (5:1)
32
The scale will assist identify the chronic
pain adolescents who are engaging
actively in other activities irrespective of
the pains because activity engagement will
improve and foster their psychological
flexibility which aids their functionality in
life. On the other the adolescents who are
not engaging well in activities would get
some professional help to enable them
adjust. The last four items will indicate the
chronic pain adolescents who have
accepted and who have not accepted the
pain situation willingly. The latter will get
help to improve their psychological
flexibility.
Discussions
ACT is a mindfulness- process based
approach to treating emotional pain and it
has showcased that pain is unavoidable in
humans but can be accepted. Accepting
pain and engaging in activities that will
help one establish sense of self. A sense of
self that is greater than one’s thoughts and
feelings. The ACT teaches the individual
to develop observed-self which facilitates
cognitive defusion, a situation where the
clients learn neither to believe nor be
controlled by thoughts. For instance, Dahl
et al (2014) expressed that any pain-
related thoughts that tell the client to avoid
particular situation or activities can be
seen for what they are (thoughts), rather
than what they say they are (truth or
reality).ACT helps clients to create and
maintain awareness of the present
moment, identify personal and deeply
important valued life direction that will
provide natural positive reinforcement.
In ACT, struggling to avoid pain causes
more suffering to the client because it
indicates non-acceptance to what is
already there, the intensity of (the
suffering) which depends on the extent of
the clients’ fusion with thoughts and
feelings associated with the pain (Feliu-
Soler et al, (2014)).
Efficacy of ACT in the treatment of
emotional pain of adolescents which
manifests in form of emotional numbing is
not in doubt because emotional numbing
is evidence of poor emotional awareness.
Most of the sufferers use destructive
experiential avoidance and psychological
inflexibility for discomforting experiences
which worsens the situation. Teaching
them processes that promote
psychological flexibility will enhance their
well-being.
Conclusion
Emotional numbing is a serious emotional
problem that has been in the cog of the
adolescents’ development and has not
received much attention in the area of
research. Its manifestations may result
from exposure to trauma, shock, attack or
exposure to violent situations. Kerig et al
(2016) noted that emotional numbing has
implication for maladaptive outcomes in
adolescence such as delinquent behaviour.
Emotional numbing (avoidance,
detachment) blocks the adolescents’
capacity from confronting, processing and
managing emotions and experiences. The
Acceptance and Commitment Therapy
(ACT) as a psychotherapy creates positive
awareness in them through the exposure to
core processes of ACT and which will
predispose them to psychological
flexibility and in turn aids them to
function properly in the society and
improve their interpersonal relationships.
Enem, U.E. & Samaila, B. (2020). The Relevance of Acceptance and Commitment Therapy (ACT)
in the Treatment of Emotional Numbing among the Adolescents: A Narrative Review,
International Journal for Psychotherapy in Africa 5(1):22-34
33
Recommendations
The researchers make the following
recommendations based on the study
1. That therapists should identify
emotional numbing among the
adolescents and use the ACT model
to resolve their problems
2. That psychologists should make
further researches on emotional
numbing
3. That the in-school adolescents
should be constantly educated on
emotional awareness
References
Bach, P. & Hayes, S.C. (2002). The use of
Acceptance and Commitment
Therapy to prevent the re-
hospitalization of psychotic patients:
a randomized controlled trial.
Journal of Consulting and Clinical
Psychology. 70(5), 1129-1139
Barsade, S.G. (2002). The ripple effect:
Emotional Contagion and its
influence on group behaviour.
Administrative Science Quarterly.
47(4), 644-675
Connolly, S. & DeAmicis, L. (2019).
Further validation of chronic pain
acceptance questionnaire for
adolescents in a broader paediatric
context. Journal of Contextual
Behavioural Science. 12, 314-321.
Daniel, L. (2011). Psychology. New York.
Worth Press
Eccleston, C., Williams A.C., & Morley,
S. (2009).Psychological therapies
for the management of chronic pain
(excluding headache) in adults.
Cochrane Database of Systematic
Reviews. Retrieved on 20th march
2020 from
http;//www.pubmed.ncbi.nlm.gov/23
15224.
Feliu-Soler, A., Montesinos, F., Gutierrez-
Martinez, O., Scott, W., McCracken,
L.M. & Luciano, J. V.
(2018).Current status of acceptance
and commitment Therapy for
chronic pain: A narrative Review
Gaulin, Steven, J.C. & Donald,H. (2003).
Evolutionary Psychology. New
Jersey. Prentice Hall
Gillanders, D.T., Bolderston, H. & Bond,
F.W. (2014). The development and
initial validation of the cognitive
Fusion Questionnaire. Behavioural
Therapy. 45(1), 83-101
Goubert, L., Crombez, G., Eccleston, C. &
Devulder, J. (2004).Distraction from
Chronic pain during a pain inducing
activity associated with greater pain
activity pain. Pain. 110(1), 220-227
Gross, J.J. (2014). Emotional regulation:
Conceptual and empirical
foundations. In J.J. Gross (Ed).
Handbook of emotion regulation
(pp. 3-20). NewYork, NY Guilford
Press.
Hayes, S.C., Strosahl, K. & Wilson, K.G.
(1999). Acceptance and
Commitment Therapy: An
experiential approach to behaviour
change. New York, Guilford Press.
Hayes, S.C. (2000). Acceptance and
Commitment Therapy in the
treatment of experiential avoidance
disorders. Clinician’s Research
Digest: Supplemental Bulletin
22(June), 1-2.
Heller, A.S. & Casey, B.J. (2016). The
neurodynamics of emotion:
Delineating typical and atypical
emotional processes during
International Journal for Psychotherapy in Africa (5:1)
34
adolescence. Developmental
Science. 19(1), 3-18.
HeShuchang, M.D., HeMingwei, & Opler,
G.A. (2011). Emotional and neuro-
ehavioural status in chronic pain
patients. Retrieved on 19-03-2020
from http://www.ncbi.nlm.nih.gov
Huizen, J. (2017). Feeling numb: What
you need to know. Medical News
Today. November 17, 2017.
Kerig, P.K., Bennet, D.C., Caplo, S.D.
(2016). Numbing of positive,
negative, and general emotions:
Associations with trauma exposure,
posttraumatic stress, and depressive
symptoms among justice-involved
youth. Journal of Traumatic
Stress. 29(2). Retrieved on 19-03-
2020 from
https://onlinelibrary.wiley.com/doi/a
bs/10.1002/jts.22087
McCracken, L.M., Vowles, K., &
Eccleston, C. (2004). Acceptance of
chronic pain: Component analysis
and a revised assessment method.
Pain. 107(1-2), 159-166
McCracken, L.M., Martinez, G. (2011).
Processes of change in
psychological flexibility in an
interdisciplinary group-based
treatment for chronic pain based on
acceptance and commitment.
Behaviour Research and Therapy.
49(4), 267-274
Rojas, S.M., Leen-Feldner, F.W.,
Blumenthal, H., Lewis, S.F., &
Feldner, M.T. (2015). Risk for
suicide among treatment seeking
adolescents: The role of positive and
negative affect intensity. Cognitive
Therapy and Research. 39(2), 145-
169.
Ruiz, F.J. (2010). A review of Acceptance
and Commitment Therapy (ACT)
empirical evidence, correlational,
experimental psychopathology
component and outcome studies.
International Journal Psychol.
10,125-162.
Tull, M.T. & Roemer, L. (2003).
Alternative explanations of
emotional numbing of
Posttraumatic Stress Disorder: An
examination Hyperarousal and
experiential avoidance. Journal of
Psychopathology and Behaviour
Assessment. 25, 147-154
Valiente, C., Swanson, J., & Eisenberg, N.
(2012). Linking students’ emotions
and academic achievement: when
and why emotions matter. Child
Development Perspectives 6(2),129-
135.
Wallace, D.P. et al (2011). Adolescent
acceptance of pain: Confirmatory
Factor Analysis and Further
Validation of the Chronic Pain
Acceptance. Journal of Pain.
Retrieved from
https://pubmed.ncbi.nim.nih.gov/214
29810/ on 19-03-2020
Wicksell, R.K., Olsson, G.L. & Melin L.
(2009). The chronic pain acceptance
questionnaire- Further validation
including a confirmatory factor
analysis as a comparison with the
Tampa Scale of Kinesiophobia.
European Journal of Pain.
13(7),760-768.
Zembylas, M. (2003). Caring for teacher
emotion: Reflections on teacher self-
Development. Studies in Philosophy
and Education. 22(2), 103-125.
Sigida, S.T. & Masola, N.J. (2020). Diagnosis And Treatment Of Mental Illness By Vhavenda Traditional
Healers In Vhembe District, South Africa, International Journal for Psychotherapy in Africa 5(1):35-43
35
Diagnosis And Treatment Of Mental Illness By
Vhavenda Traditional Healers In Vhembe District,
South Africa
Salome Thilivhali Sigida
Nare Judy Masola
Department of Psychology, University of Limpopo,
South Africa
Abstract In rural African communities, traditional healers hold an esteemed and powerful position
in the diagnosis and treatment of various illnesses. They assume a significant role in
addressing the mental health care needs of individuals by offering cultural appropriate
treatment and they are easily accessible. This was a qualitative study, and specifically,
the case study method was utilised. Ten traditional healers were chosen through
purposive and snowball sampling to participate in the study. Data was collected through
semi-structured interviews and analysed using the thematic analysis method. The findings
revealed that several procedures (like throwing of bones and direct observation of
patient’s behaviours) are used to diagnose mental illness. The findings also revealed that
mental illness can be treated through the use of traditional remedies and practices (like
rituals). From the findings of the study, it can be suggested that both traditional medical
interventions and some culturally relevant psychological procedures are used to treat
mental illness. Increased cooperation between western oriented psychotherapists and
African traditional healers is therefore highly recommended.
Key words: South African traditional healers, traditional remedies, treatment, diagnosis,
mental illness.
Introduction
In different societies around the world,
culture plays an important role in
understanding how different groups
construct health and illness (Zungu, 2013).
In addition to this, every society develops
its cultural way of managing illness
(Mokgobi, 2014). In this regard, it has
been indicated by Brandt and Rozin (2013,
p.148) that, how society responds to
disease reveals its deepest cultural, social
and morals. It is, therefore worth noting
that because the attainment of good health
is intrinsically desirable; people in
different parts of the world, more
specifically people living in sub-Saharan

International Journal for Psychotherapy in Africa (5:1)
36
Africa utilise traditional healers for their
healthcare needs, including mental health
(James, Wardle, Steel, & Adams, 2018;
Madu, Baguma & Pritz, 1997). Moreover,
literature has shown that traditional
healers play an important role in health
care for the majority of South Africans.
Interestingly, efforts towards achieving
optimum health are as diverse as the
social, cultural, economic, mental,
spiritual, physical, and even political
circumstances of the particular individual
at any point in time (Zuma, Wight, Rochat
& Moshabela, 2016).
In South Africa, especially in
indigenous societies, it is estimated that
between 60% and 80% of South African
consult traditional healers and that these
healers are frequently consulted for mental
illness when compared to western-trained
counterparts (Puckree, Mkhize, Mgobhozi
& Lin, 2002; Truter, 2007). Thus
traditional healer’s beliefs and medicine
play an important role in the treatment of
illness, this also includes the treatment of
mental illness (Tomita, Burns, King,
Baumgartner, Davis, Mtshemla, & Susser,
2015). Interestingly, traditional healers are
geographically accessible and offer
treatment that is similar to the culture of
their patients (Burns, 2011; Tomita et al,
2015). They are the entry point for care in
many African communities (Richter,
2003; Zungu, 2013). Ross (2010), also
pointed out that the treatment of
traditional healers is also used along with
western treatment.
The various ways in which
individuals conceptualize social
circumstances reflect their fundamental
belief and perspective on the world that
gives their lives direction and motivation.
In an unforeseen manner, perception is the
source of reason for the way things are on
the planet, including speculations about
mental illness, death, misery, how human
suffering is (Nwoye, 2011). Taking into
account the assorted varieties in the
human direction across social orders and
societies, musings, thinking and methods
for knowing about individuals inside these
social orders likewise contrast from
various perspectives, particularly from the
predominant Western idea and thinking
(Yidana, 2014). It is important to note that
decisions about mental health and
wellbeing and the possible interventions
during illness episodes are often managed
by the people's belief structures (Berger &
Luckmann, 1967). In this regard,
individual and collective response to
mental illness varies and reflects pertinent
information, culture, and knowledge of
aetiology, including the accessibility of
treatment alternatives.
In some of the indigenous societies,
knowledge and thoughts on issues relating
to psychological wellbeing are supported,
taking into account mending professionals'
capacity to develop and reproduce culture
with the progression of time (Wuthnow,
James, Albert, & Edith, 1984). As
indicated by Thomas (1999), since illness
is socio-culturally constructed, the ways
people express their mental sicknesses
gives knowledge into how they see the
world just as sourcing potential
mediations. As the training proceeds, the
perspective stays genuine in abstract
credibility as it is affirmed and
reconfirmed without anyone else
comparable to the social others (Berger &
Luckmann, 1967).
Even though literature shows the
popularity of traditional healers, their roles
and competencies are often criticized and
belittle (Zuma et al., 2016). There is
abundant evidence showing that in Africa,

Sigida, S.T. & Masola, N.J. (2020). Diagnosis And Treatment Of Mental Illness By Vhavenda Traditional
Healers In Vhembe District, South Africa, International Journal for Psychotherapy in Africa 5(1):35-43
37
"illness representations are commonly
constructed to emphasize external and
uncontrollable supernatural factors"
(Bogart, Wagner, Galvan & Banks et al.,
2010, p.182). The importance of
recognising cultural belief systems and
practices in dealing with mental health has
been highlighted (Kubeka, 2016). In most
African cultures a core belief is that
diseases are due to a violation of cultural
taboos or witchcraft (Mufamadi & Sodi,
2010). Whilst there is evidence to suggest
that most people in rural communities
consult with traditional healers for illness,
including mental illness, there appears to
be very little research that has been done
to understand how traditional healers
diagnose and treat mental illness. Based
on the relatively fewer studies that have
been conducted on this particular subject,
the current study seeks to understand how
traditional healers diagnose and treat
mental illness at Vhembe District in
Limpopo Province, South Africa.
Traditional healers as Spiritual and
healing Specialists
An African traditional healer is
characterized by the World Health
Organization as an "individual who is perceived by
the community in which he or
she lives as competent to provide
health care by using vegetable,
animal and mineral substances
and other methods based on the
social, cultural and religious
background, as well as on the
knowledge, attitude and beliefs
that are prevalent in the
community regarding physical,
mental and social well-being and
the causation of disease and
disability" (WHO, 2002).
Thus, traditional healing is an effort to
increase comprehension or vision into an
inquiry or circumstance in a given
network of sick individuals. It is a
methodical procedure of sorting out what
gives off an impression of being
disengaged aspects of presence with the
end goal that they give understanding into
an issue close by and an answer thereof
(Sambe, Abanyam, & Lorkyaa, 2013).
Besides, this recuperating alludes to a lot
of methodologies including the specialty
of utilising custom or service to procure
data from the soul world to anticipate the
future and mend the psychological sick
person. In some indigenous networks, this
training is the principle methods for
spotting purportedly profound issues and
endorsing cures (Azongo & Abdulai,
2014). Customary healers who are thought
to have otherworldly powers can
recognize the ills influencing individuals
and society and recommend cures from
the gods and imperceptible world.
In situations where afflictions manifest
individually, useful separation gets
worrying because of the arrangement of
causal spirits as per the external
manifestation of afflictions. In this
manner, depending on the society and the
current community, different meanings
may be added to the same condition. As a
result, diagnosis and course of action in
such situations are often decided through
divination. Subsequently, finding and
strategy in such circumstances are
frequently chosen through divination.
While clinical specialists use machines to
decide the reason for sickness, traditional
healers utilize divination to decide the
reason for tribulations and decide the
treatment. In the cosmology of the nearby
individuals, divination assumes a focal job
in lay meetings to decide the correct
International Journal for Psychotherapy in Africa (5:1)
38
treatment or referral for therapy (Azongo
& Abdulai, 2014).
Overseeing mental illnesses of this
nature concerning healers and the
tormented exposes two significant
perceptions drawn from the recuperating
rehearses. The primary issue includes
dependence on soothsayers to figure out
which soul is liable for a specific issue.
Under this condition, an assortment of
otherworldly elements might be tended to
thus use the profound lab to decide the
soul liable for the pain (Sambe, Abanyam,
& Lorkyaa, 2013). Per the cosmological
set up of the individuals, this is the main
way they can give the correct antitoxin.
The subsequent perception includes the
demonstration of distinguishing proof of
the reason for the sickness and the
mediations to be attempted. Although
individuals would frequently contend that
the training establishes a post hoc
appraisal in that it is simply after an
improvement in the state of the patient that
a connection between what was at first
hypothesized can be certified, one needs to
endure at the top of the priority list that the
training is a piece of their believability
structure and its proceeded with training
makes it genuine.
Research Methods
Study design: A qualitative research
approach was best suited for this study as
the focus was on understanding the
diagnosis and treatment of mental illness
by Vhavenda traditional healers.
Setting: The sample was recruited from
Vhembe District in Limpopo Province
South Africa.
Study population and sampling
strategy: In total 10 participants (8 males
and 2 females), aged between 35 years and
60 years were selected through purposive
and snowball sampling to participate in
the study
Data collection: Data for this study was
collected through the use of in-depth semi-
structured one-to-one interviews. The
interviews were conducted in Tshivenda a
predominant language used by the
participants. An interview guide was used
to guide the discussions.
Data analysis: Data was analysed through
thematic data analysis.
Ethical considerations: Before
conducting the study, ethical clearance
was requested from The University of
Limpopo's Research Ethics Committee
and also from the Vhembe Traditional
Healers Association. After obtaining
ethical approval and permission, the
researchers commenced with data
collection. The participants were assured
of privacy and confidentiality.
Results and Discussion
From the findings of the study two themes
emerged from data analysis; those are, (a)
the diagnosis of mental illness and (b) the
treatment of mental illness. The two
themes are presented and discussed below
in line with the previous findings.
Diagnosis of mental illness
Traditional healers use several procedures
to diagnose mental illness. For example,
the use of mufuvha or ṱhangu (divination
bones) are common procedures that the
traditional healers use to diagnose mental
illness.
"…when we talk about mental illness to us
as ṅanga (traditional healers), it is when
Sigida, S.T. & Masola, N.J. (2020). Diagnosis And Treatment Of Mental Illness By Vhavenda Traditional
Healers In Vhembe District, South Africa, International Journal for Psychotherapy in Africa 5(1):35-43
39
we observe in this manner, firstly we
throw bones and determine if it is related
to mental illness" [Participant 3]
"As ṅanga (traditional healers), we see
through our bones that a person has a
mental illness and what caused that
mental illness."[Participant 6]
These findings are consistent with the
findings of Buhrmann (1984) and
Ngubane (1977), they reported that
divination bones are used in other parts of
Africa to diagnose illnesses. It was further
pointed out by traditional healers in this
study that mufuvha and thangu (divination
bones) not only help to diagnose mental
illness, they also help to inform traditional
healers what caused the mental illness and
the type of mental illness the patient might
have.
"So we take mufuvha or ṱhangu
[divination bones] and throw them down
and see what kind of mental illness the
person has."[Participant 9]
Participants also mentioned that they can
see that the person has mental illness
through their behaviour, they further
pointed out that the behaviour of the
person with mental illness is different
from the behaviour of other people. The
following extracts express this notion:
"We can also see that a person has mental
illness by his/her behaviour"[Participant
6] "Ehh…that is why I mentioned that why I
mentioned that sometimes you will see by
action…."[Participant 8]
"Mental illness is when a person is
behaving unusually. These things
that…ehh…things that a normal person
cannot do". [Participant 6]
"Maybe when we know that a person must
live or think or his behaviour is different
from other people"[Participant 7]
It could be suggested that mental illness is
understood by participants as a condition
that has some behavioural manifestations
that are not considered normal within their
social context. In other words, mental
illness is understood and described in the
context of the socio-cultural context of the
individual affected. The participants went
further and reported some of the
behaviours that are not considered to be
normal. These findings are supported by
Mufamadi (2001), Mzimkulu and Simbayi
(2006), Robertson (2006), who indicated
that in many parts of Africa, mental illness
is understood to be present when an
individual shows behavioural signs and
symptoms that are perceived to deviate
from social norms. The participants also
described some of the behaviours that are
not considered normal:
“mental illness is…eh...like when you see
a person playing with their fingers,
pointing here and there, laughing alone,
and also collecting dirty
things"[Participant 8]
"From there the person will start talking
alone or calling someone's name, or
saying "I'm coming now", or "I didn't take
everything" or "I will come tomorrow"
then you will know that that person has a
mental illness"[Participant 7]
The description of mental illness
according to traditional healers
interviewed in the study can be said to be
linked to how mental illness is
conceptualised in the academic literature.
The American Psychiatric Association
(2013) in particular, conceptualises mental
illness as being a manifestation of a

International Journal for Psychotherapy in Africa (5:1)
40
behavioural, psychological or biological
dysfunction in the individual.
Treatment of mental illness
Participants considered mental illness to
be a condition that can be treated through
traditional remedies and practices. The
following extracts further express this
understanding:
"Yes, they can be cured by u aravhedziwa
dzi tsemo (steaming) and those things will
come out and they will live a normal life
just like everyone."[Participant 1]
"That person will be given some remedy to
inhale and will be given some soft
porridge and he will eat and be
healed"[Participant 6]
Previous studies reported that traditional
healers use different herbs to treat illness
(Dlamini, 2006). It is estimated that there
are over 300 medicinal plants that are used
by traditional healers to treat illness
(Rankoana, 2016; Truter, 2007). These
findings are similar to Hadebe (1986) who
reported that some traditional healers'
intervention strategies include the use of
namesis, anema, steaming, taking
medicine nasally and vaccination. Dlamini
(2006) also reported that herbal medicine
is the most commonly used treatment
method by traditional healers. Besides
giving herbs to patients for the treatment
of mental illness, it was also reported by
the participants that certain curative rituals
are performed to treat mental illness.
"So when a person has been done such
things…it means that we must make some
herbs and a wristlet and some water and
he will go and call his ancestors under a
big tree. And tell them to stay with him
and those things that were cast to him to
remain there. After that, he must bath his
body and that means those things are
gone." [Participant 4]
The above extract indicates that traditional
healing not only aims at achieving
physical treatment purposes but also the
psycho-spiritual treatment (United Nations
Joint Programme on HIV/AIDS, 2006).
One participant reported that traditional
healers acknowledge and recognise the
role that can be played by other role
players in mental health promotion as
reflected in the extract below:
"But if such a person seeks help from
people who can counsel him, people like
pastors and fellow Christians such person
can improve without any need for
medicine."[Participant 3]
This means when traditional healers can
see that they are unable to assist the
patient in seeking the treatment they then
refer or advise their patients to go
religious healers such as pastors.
Therefore, there is a need for closer
cooperation between indigenous healers
and other role players such as western
trained health care practitioners and
spiritual/faith healers.
Conclusion
In conclusion, the results of the study
show that traditional healers occupy
multiple roles, that is the role they play
goes beyond healing using herbs. They
also perform other healing practice such as
the performance of curative rituals. Both
traditional medical interventions and some
culturally relevant psychological
procedures are used to treat mental illness
by traditional healers. This suggests that
traditional healers play an important role
Sigida, S.T. & Masola, N.J. (2020). Diagnosis And Treatment Of Mental Illness By Vhavenda Traditional
Healers In Vhembe District, South Africa, International Journal for Psychotherapy in Africa 5(1):35-43
41
in medicine and psychotherapy at the
same time in their communities. The
authors therefore recommend increased
cooperation between western oriented
psychotherapists and African traditional
healers.
References American Psychiatric Association. (2013).
Diagnostic and Statistical Manual of
Mental Disorders. Arlington:
American Psychiatric Association.
Azongo, T. B., & Abubakari, A. (2014).
Complementary or Contradictory?
Role of diviners in healthcare
delivery in Ghana: Implications and
consequences. International Journal
of Research in Health Sociology,
2(4):999-1008.
Berger, P., & Luckmann, T. (1967). The
Social Construction of Reality: A
treatise in the Sociology of
Knowledge Anchor Books: USA.
Bogart, L. M., Wagner, G., Galvan, F. H.,
& Banks, D. (2010). Conspiracy
beliefs about HIV are related to
antiretroviral treatment non-
adherence among African American
men with HIV. Journal of acquired
immune deficiency syndromes
(1999), 53(5), 648.
Burns, J. K. (2011). The mental health gap
in South Africa: A human rights
issue. The Equal Rights
Review, 6(99), 99-113.
Bührmann, M. V. (1987). The feminine in
witchcraft: Part II. Journal of
Analytical Psychology, 32(3), 257-
277.
Brandt, A. M., & Rozin, P.
(2013). Morality and health.
Routledge.
Dlamini, B.P. (2006). African indigenous
methods of health promotion and
HIV/AIDS prevention (Unpublished
doctoral thesis), University of
Zululand, South Africa
James, P. B., Wardle, J., Steel, A., &
Adams, J. (2018). Traditional,
complementary and alternative
medicine use in Sub-Saharan Africa:
a systematic review. BMJ Global
Health, 3(5), e000895.
Hadebe, J. M. B. (1986). An African view
of psychopathology: A
blueprint. Journal of Psychology:
University of Zululand, 2(2), 1-26.
Kubeka, N. P. (2016). The psychological
perspective on Zulu ancestral
calling: A phenomenological
study (Masters Dissertation)
University of Pretoria, Pretoria,
South Africa.
Madu, S. N., Baguma, P. & Pritz, A.
(eds.) (1997). African traditional
healing: Psychotherapeutic
investigations. Vienna: Facultas
Universitaetsverlag.
Mokgobi, M. G. (2014). Understanding
traditional African healing. African
Journal for Physical Health
Education, Recreation, and
Dance, 20(Suppl 2), 24.
Mufamadi, J. (2001). A group of
traditional healers ‘perceptions of
and approaches to the treatment of
mental illness. In Indigenous
Knowledge Conference (p. 88).
University of Saskatchewan. May
(28-30)
Mufamadi, J., & Sodi, T. (2010). Notions
of mental illness by Vhavenda
traditional healers in Limpopo
Province, South Africa. Indilinga
African Journal of Indigenous
Knowledge Systems, 9(2), 253-264.
Mzimkulu, K. G., & Simbayi, L. C.
(2006). Perspectives and practices of
International Journal for Psychotherapy in Africa (5:1)
42
Xhosa speaking African traditional
healers when managing
psychosis. International Journal of
Disability, Development and
Education, 53(4), 417-431.
Nwoye, C. M. (2011). Igbo cultural and
religious worldview: An insider’s
perspective. International Journal of
Sociology and Anthropology, 3(9),
304-317.
Ngubane, B. S. (1997). Awakening
southern giant. Cargo Systems
International, 24 (1), 53-54
Puckree, T., Mkhize, M., Mgobhozi, Z., &
Lin, J. (2002). African traditional
healers: what health care
professionals need to
know. International Journal of
Rehabilitation Research, 25(4), 247-
251.
Joint United Nations Programme on
HIV/AIDS, & UNAIDS.
(2006). Collaborating with
traditional healers for HIV
prevention and care in sub-Saharan
Africa: Suggestions for programme
managers and field workers. New
York: World Health Organization.
Rankoana, S. A. (2016). Curative care
through administration of plant-
derived medicines in Sekhukhune
District Municipality of Limpopo
province, South Africa. African
Journal of Traditional,
Complementary and Alternative
Medicines, 13(2), 47-51.
Richter, M. (2003). Traditional medicines
and traditional healers in South
Africa. Treatment Action Campaign
and AIDS Law Project, 17, 4-29.
Robertson, B. A. (2006). Does the
evidence support collaboration
between psychiatry and traditional
healers? Findings from three South
African studies. African Journal of
Psychiatry, 9(2), 87-90.
Ross, E. (2010). Inaugural lecture: African
spirituality, ethics and traditional
healing–implications for indigenous
South African social work education
and practice. South African Journal
of Bioethics and Law, 3(1), 44-51.
Sambe, N., Abanyam, N. L., & Iorkyaa, P.
(2013). The role of divination in
treatment of disease in Kwande
Local Government Area of Benue
State, Nigeria. Int J Humanit Soc Sci
Invent, 2, 21-9.
Tomita, A., Burns, J. K., King, H.,
Baumgartner, J. N., Davis, G. P.,
Mtshemla, S., ... & Susser, E.
(2015). Duration of untreated
psychosis and the pathway to care in
KwaZulu-Natal, South Africa. The
Journal of Nervous and Mental
Disease, 203(3), 222.
Thomas, L. E. (1999). Under the canopy:
Ritual process and spiritual
resilience in South Africa.
Columbia, Univ of South Carolina
Press
Truter, I. (2007). African traditional
healers: Cultural and religious
beliefs intertwined in a holistic
way. South African Pharmaceutical
Journal, 74(8), 56-60.
World Health Organization. (2002).
Traditional medicine strategy 2002-
2005. Retrieved from
http://www.who.int/h
/booktraditional_medicine-
strategy.pdf. 12 September2019
Wuthnow, R., Bergesen, A. J., &
Kurzweil, E. (2010). Cultural
Analysis: The Work of Peter L.
Berger, Mary Douglas, Michel
Foucault and Jürgen

Sigida, S.T. & Masola, N.J. (2020). Diagnosis And Treatment Of Mental Illness By Vhavenda Traditional
Healers In Vhembe District, South Africa, International Journal for Psychotherapy in Africa 5(1):35-43
43
Habermas (Vol. 5). London:
Routledge.
Yidana, A. (2014). Socio-religious factors
influencing the increasing
plausibility of faith healing in
Ghana. American Journal of
Sociological Research, 4(1): 1-10.
Zungu, N. (2013). Social representations
of AIDS and narratives of risk
among Xhosa men. Unpublished
Doctoral dissertation). University of
Cape Town, Cape Town, South
Africa.
Zuma, T., Wight, D., Rochat, T., &
Moshabela, M. (2016). The role of
traditional health practitioners in
Rural KwaZulu-Natal, South Africa:
generic or mode specific? BMC
Complementary and Alternative
Medicine, 16(1), 304.
International Journal for Psychotherapy in Africa (5:1)
44
Psychotherapy Training In Africa South Of Sahara
Prof. Sylvester Ntomchukwu Madu (D.Sc. Psych., Innsbruck)
Department of Psychology,
Chukwuemeka Odumegwu Ojukwu University, Nigeria.
Abstract The scarcity of properly trained psychotherapists in Africa south of Sahara on the one
hand, and the increasing incidence of emotional problems resulting from poverty and
underdevelopment, child abuse and neglect, trauma resulting from different forms of
crime and abuse of human dignity, insecurity problems like terrorism, insurgency,
kidnapping and hijacking, increasing stress-provoking lifestyles, tribal and national wars
and conflicts, westernization and globalisation, and the HIV/AIDS pandemic, different
forms of cancer, and all sorts of abuse of human dignity on the other hand, call for
urgent need for establishment of institutions for formal psychotherapy training in Africa.
This paper highlights not only the above lacuna but also describes the important aspects
of psychotherapy training in the Western world. It went further to describe current efforts
being made (with Nigeria as an example) to establish a world-class tertiary institution,
the School of Psychotherapy and Health Sciences (SPHS), which takes it lead from
modern psychotherapy training programmes in Austria. The SPHS in Nigeria is affiliated
to Sigmund Freud University, Vienna, Austria. Students from SPHS are trained by
qualified staff from Nigeria and from Austria, and they are properly equipped with
psychotherapeutic skills that will enable them to address the emotional problems of
Africans, in which ever work-setting they find themselves. They are also registerable with
the World Council for Psychotherapy and with other psychotherapy organisations world-
wide.
Key words: Psychotherapy Training, Africa, South of Sahara
Introduction
The World Council for Psychotherapy
African Chapter (WCP-AC) was
inaugurated at its first Conference in
Kampala, Uganda in 1997. The second
WCP-AC Conference took place in
Polokwane, South /Africa, in 1998. The
third, fourth, and fifth Conferences also
took place in Polokwane (RSA) in 2000,
2004, and 2008 respectively. The sixth
one took place in Kampala, Uganda in
2010. In 2014, we hosted the seventh
World Congress in Durban, South Africa.
The seventh WCP-AC Conference is now
taking place in 2020 in Johannesburg,
South Africa.
Our focus during the conferences were:
1. To make Awareness campaign about
psychotherapy.

Madu, S.N. (2020). Psychotherapy Training in Africa South of Sahara,
International Journal for Psychotherapy in Africa 5(1):44-53
45
2. To sensitize African on the need for
Psychotherapy.
3. To establish a platform for
discussion among African
Psychotherapists, including national
associations.
4. To publish books in the area of
psychotherapy in Africa; and so far,
we published 8 books in the area of
Psychotherapy in Africa.
As successful as the conferences and
publications were, there is still a vacuum
we need to fill, and they are:
• Formal Training of Professional
Psychotherapists in Africa.
• Formal Training in Psychotherapy
Science.
• Establishment of Scientific Journals
for Psychotherapy in Africa.
In most black African countries south of
Sahara, the challenges posed by poverty
and underdevelopment, child abuse and
neglect, trauma resulting from different
forms of crime and abuse of human
dignity, insecurity problems like terrorism,
insurgency, militancy, kidnapping and
hijacking, increasing stress-provoking
lifestyles, tribal and national wars and
conflicts, westernization and globalisation,
and the HIV/AIDS pandemic, different
forms of cancer, are enormous (Madu,
2009; Madu, Baguma & Pritz, 1996;
Madu, 2003). The emotional aspects of
those problems need to be addressed by
well-trained psychotherapists, using
appropriate psychotherapeutic methods
that would appeal to the African clients.
One may consider psychotherapy to be
that process that enables people to express
their feelings in a protected environment,
to a person well-trained to listen with
understanding and compassion. The
process helps people reconnect with – and
honour – their roots, affirm their identity,
and develop healthy ways of being in the
world (Pritz, Kuriansky, Nemeth,
Mulcahy, Walsh & Madu, 2005). By
restoring an individual's human dignity,
and personal and cultural identity through
psychotherapy, the person can regain
emotional resilience and achieve
sustainable mental health to overcome fear
and deal effectively with personal
suffering and trauma in the world.
Surely, we have the likes of Sigmund
Freud and Carl Rogers in Africa, but often
we run short of African-originated and
integrated forms of psychotherapy to be
used to address our emotional problems. It
is a challenge for us to know exactly how
to adapt the different western forms of
psychotherapy to our African situations.
Some African traditional and religious
faith healers, have been said to be
managing many of the physical as well as
emotional problems of our people (Ebigbo
& Tyodzua, 1982; Madu, 1989; Madu &
Adebayo, 1996; Madu et al. 1997; Madu
& Ohaeri, 1989; Peltzer, 1995). In spite of
that, how we (the western-oriented
African psychotherapists) should relate to
them professionally, is still a matter of
debate (Madu, Baguma & Pritz, 1998,
1999, 2000; Madu & Govender, 2005).
The above are some of the challenges that
have generated intensive dialogue among
African psychologists and
psychotherapists.
Types of African psychotherapy clients:
According to Ebigbo and Ihezue (1981),
there are three types of clients (in black
Africa) - the traditional, the mixed, and

International Journal for Psychotherapy in Africa (5:1)
46
the western oriented types. The
traditional type grew up and spent most
of his or her formative years in rural areas.
Some of them move to the townships at a
later stage in their lives. Their world
image is analogical, magical and pictorial.
They always go to traditional healers
when they have health problems
(including emotional problems).
The intermediate mixed type was either
born and bred in the rural areas but moved
to a city to work and live as an adult or
grew up in a city but continued to have a
very strong tie to the rural areas and their
customs. This type is a compendium of
two cultural systems (the traditional and
the western-oriented), because he or she
has the tendency of making use of the two
methods of healing (traditional and
western) at the same time (concurrently).
Some of them also consult the religious
faith healers. It is worth noting here that
the majority (about 80%) of the black
African population today would fall
(within either the traditional or) the mixed
types (compare also with Peltzer, 1991;
Pennymon, 2004). African well-trained
psychotherapists would be particularly
relevant to this group of clients (the mixed
type).
Most of the western-oriented type of
clients were born and bred in the
townships. They are educated, mostly
Christians or Moslems, they come from
monogamous families and their parents
are also educated. From childhood, they
have always been treated in hospitals and
have never thought of going to a
traditional healer for treatment. The
western forms of psychotherapy would
appeal to this group of clients.
The above complexity in types of clients
found in Africa makes it imperative that
special training programmes need to be
organised for psychotherapists in Africa.
The psychotherapists trained in Africa
should be well-equipped to attend to any
of the types of clients found in Africa.
Some African-Originated Forms of
Psychotherapy
The problems psychotherapists are
encountering in trying to apply western
oriented psychotherapy in an African
culture have also been extensively
reported (Madu, 1991; Hanneke, 1989;
Oladimeji, 1988). Happily, some of the
western trained psychotherapists have
gone a step further in trying to develop
some Africa-based forms of
psychotherapy. Three examples of such
forms of psychotherapy are the Ubuntu
therapy (Nefale& van Dyk, 2003; Louw &
Madu, 2004), the "Meseron” Therapy
(Awaritefe, 1995, 1997, 2004; Ofovwe,
2005), the "Harmony Restoration
Therapy" (Ebigbo, Oluka, Ezenwa,
Obidigbo, Okwaraji, 1995) and the
Culture-Centred Psychotherapy (CCP)
(Madu, 2013). Each of these forms of
therapy has some aspects of the African
cultures, values, and belief systems as its
take-off-base.
It is however an unfortunate reality that no
full training programme has been
developed for any of the African-
originated forms of psychotherapy. Also,
no formal full training programme for any
form of psychotherapy (whether western
or African) is available in most countries
of Africa South of Sahara. The few
psychotherapists who were trained
overseas who came back and settle in
Africa, are overwhelmed with work as

Madu, S.N. (2020). Psychotherapy Training in Africa South of Sahara,
International Journal for Psychotherapy in Africa 5(1):44-53
47
lecturers teaching clinical, counselling, or
other branches of psychology in
institutions of higher learning. Those
psychology post-graduate programmes
offer students only a few modules in
psychotherapy. Clinical psychology
students, for example, therefore graduate
being experts in psychopathology and
psycho-diagnostics; but become
handicapped when it comes to
psychotherapy. When it comes to
treatment, cure or management of
psychological problems, they become
helpless-helpers. The enormous need for
fully trained psychotherapists who would
be at the grass-root addressing the
emotional problems associated with
poverty and underdevelopment, child
abuse and neglect, trauma resulting from
different forms of crime and abuse of
human dignity, insecurity problems like
terrorism, insurgency, kidnapping and
hijacking, increasing stress-provoking
lifestyles, tribal and national wars and
conflicts, westernization and globalisation,
and the HIV/AIDS pandemic, different
forms of cancer, remains far-fetched. This
paper therefore throws some light on a
way forward from this dilemma by
highlighting some efforts being made, in
collaboration with some of our colleagues
overseas, to set up a training institution for
psychotherapy, using Nigeria as an
example.
Psychotherapy training in the Western
world
In Europe and America, psychotherapy
training is a rigorous training that lasts for
many years. It is often organised by the
respective professional bodies in charge of
licensing the graduants from the different
schools of psychotherapy (Psychoanalysis,
Behaviour therapy, Client-Centred
Psychotherapy, Gestalt therapy, Logo
therapy, to mention but only a few). To
qualify to be admitted into any of the
schools of thought, in most cases, one
must have acquired a master’s degree in a
relevant field of study (e.g., clinical
psychology, counselling psychology).
Each psychotherapy training is often
divided into three segments/phases: 1.
Theoretical phase. 2. Phase of Self-
experience of psychotherapy
(Eigentherapie Phase). 3. Practical phase.
During the theoretical part, the trainee is
exposed to many theories and publications
in the specific psychotherapy school of
thought. Thus, the trainee acquaints
him/herself with the thoughts of the
father-founders of the school of thought as
well as with the research findings of
modern psychotherapists in the same
school of thought. Series of seminars and
workshops are organised for the trainees
to ensure proper internalisation of the
school of thought. During the second stage
of the training, the trainees are meant to
experience themselves psychotherapy
sessions as clients. They are to go to an
approved renowned psychotherapist of the
same school of thought as clients for
psychotherapy. The reason behind this
(compulsory) experience of psychotherapy
as clients is to ensure that they do not later
become helpless helpers. This self-
experience of psychotherapy offers the
trainees the opportunity to deal with and
properly address shackles of
psychopathology in them which may later
be a hindrance, an intervening variable, or
a source of counter-transference, when
they start to practice as therapists. Even,
not having a problem can be a problem.
Until the candidate is certified by the
psychotherapist that he/she has successful

International Journal for Psychotherapy in Africa (5:1)
48
gone through this phase, he/she may not
move on to the next phase which is real
practical training phase. The therapy
period may last for between 6 months and
many years. During the third phase, the
candidate is then allowed under close
mentoring and supervision to handle real
clients. The sessions conducted are tape-
recorded or video-taped and supervised by
his/her trainers. Many hours of successful
sessions of psychotherapy must be
demonstrated before the candidate is
certified as a psychotherapist of the
respective school of thought.
The whole process of going through the
three phases of training takes years (e.g.
minimum of 4 years for Client-centred
therapy, minimum of 5 years for
Behaviour therapy, and minimum of 6
years for Psychoanalysis). Moreover, it is
very cost-intensive. In addition to the
training, one may still have to undergo
certain forms of application and scrutiny
before he/she is given the license to
practice as a “Psychotherapist” in the
country/continent/world. For example, the
World Council for Psychotherapy which is
based in Vienna, Austria, demands such
before one is given a certificate as a
“World Psychotherapist”.
Some of the founders of the World
Council for Psychotherapy (WCP) have
taken the training of psychotherapists a
new direction. Before the 1990s, most of
the training of psychotherapists were
organised by the different professional
bodies and outside the university system.
All forms of psychotherapy training had
three phases: the theoretical phase, the
self-experience phase, and the practical
phase. But in the mid-1990s, motivated by
the need to make psychotherapy more
scientific, and thereby also research based,
a university was established in Austria,
with a mandate to train students in
Psychotherapy Science and related
disciplines. Since then, one could study
psychotherapy science at Diploma, B.Sc.,
M.Sc., and PhD levels in Austria. These
training programmes brought a 4th
component to the training of
psychotherapist: the Research Component.
Following this model, a trainee in
Psychotherapy Science must now go
through relevant theories, self-experience
of psychotherapy, practicals, and research,
thereby also widening their score for
future profession.
Psychotherapy training in Africa South
of Sahara, using Nigeria as an example
As already indicated above, to date, no full
formal psychotherapy training programme
exist in most part of Africa South of
Sahara (including Nigeria) (to the
knowledge of the author) (see also Peltzer
et al, 1989). Therefore, in collaboration
with the founders of the World Council for
Psychotherapy and the Sigmund Freud
University, Vienna, Austria, efforts are
being made to establish a training
institution in Nigeria which will have
Psychotherapy Science as a niche area.

Madu, S.N. (2020). Psychotherapy Training in Africa South of Sahara,
International Journal for Psychotherapy in Africa 5(1):44-53
49
SCHOOL OF PSYCHOTHERAPY AND HEALTH SCIENCES, OKIJA, NIGERIA
Web address: www.sphs.com.ng; Email: [email protected];
[email protected]. Mobil: +234-9063927862.
The School for Psychotherapy and Health
Sciences (SPHS) started with Internship,
Certificate, Diploma, and post-graduate
programmes in the area of psychotherapy
Science. These programmes took to the
model that ensures well-grounding in
relevant theories, self-experience of
psychotherapy, practicals, and research.
The school also gives the trainees the
opportunity of choosing to be trained with
emphasis on any of the major western
psychotherapy schools of thought (e.g.
Client-Centred therapy, Psychoanalysis,
Behaviour therapy, Logo therapy, etc.), or
on any of the afore-mentioned African
originated forms of psychotherapy (e.g.,
Harmony Restoration therapy, Meseron
Therapy, Ubuntu Therapy, or Culture-
Centred Psychotherapy).
The Brand of Psychotherapy
The School for Psychotherapy and Health
Sciences (SPHS) started in 2016 with
Internship and Certificate programmes for
post-graduate students. These programmes
took to the model that ensures well-
grounding in relevant theories, self-
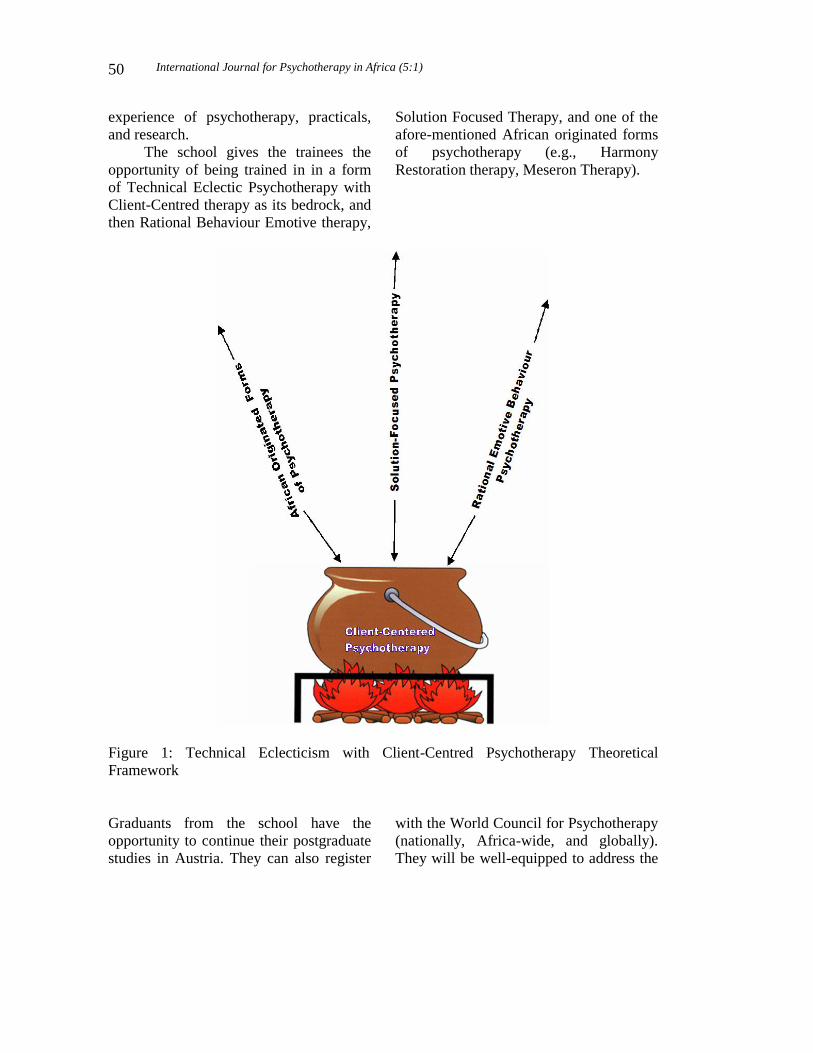
International Journal for Psychotherapy in Africa (5:1)
50
experience of psychotherapy, practicals,
and research.
The school gives the trainees the
opportunity of being trained in in a form
of Technical Eclectic Psychotherapy with
Client-Centred therapy as its bedrock, and
then Rational Behaviour Emotive therapy,
Solution Focused Therapy, and one of the
afore-mentioned African originated forms
of psychotherapy (e.g., Harmony
Restoration therapy, Meseron Therapy).
Figure 1: Technical Eclecticism with Client-Centred Psychotherapy Theoretical
Framework
Graduants from the school have the
opportunity to continue their postgraduate
studies in Austria. They can also register
with the World Council for Psychotherapy
(nationally, Africa-wide, and globally).
They will be well-equipped to address the
Madu, S.N. (2020). Psychotherapy Training in Africa South of Sahara,
International Journal for Psychotherapy in Africa 5(1):44-53
51
emotional problems of our people, no
matter the type of client that comes for
psychotherapy, and no matter whether the
clients are in hospitals/clinics, refugee
camps, rehabilitation centres, or in a
setting of private practice.
So far, the School of Psychotherapy and
Health Sciences, Nigeria has:
– Trained about 33 students in
different programmes of
psychotherapy.
– Organised 4 National Conferences in
the area of Psychotherapy.
– Published 4 volumes of the
International Journal for
Psychotherapy in Africa.
Conclusion
Haven shown that there is scarcity of
properly trained psychotherapists in Africa
South of Sahara on the one hand, and that
there is increasing incidence of emotional
problems resulting from insurgency,
terrorism, westernisation, urbanisation,
stress-provoking life-styles, criminality
and all sorts of abuse of human dignity on
the other hand, we hereby call for call for
urgent need to establishment of
institutions for formal psychotherapy
training in Africa. The establishment of
the School of Psychotherapy and Health
Sciences (SPHS), which takes it lead from
modern psychotherapy training
programmes in Austria, is a move in the
right direction. Students from the
institutions should be properly equipped
with psychotherapeutic skills that will
enable them to address the emotional
problems of Africans, in whichever work-
setting they find themselves. After
completing a stage of study, they should
also have the opportunity of continuing
their training in Austria.
Recommendations
Based on the success experience at SPHS,
I recommend the following:
1. Establishment of more institutions
that focus on training Africans in
the area of psychotherapy is key to
development of psychotherapy in
Africa.
2. Organisation of Psychotherapy
Conferences is also crucial. We
need to tell our own story by
ourselves.
3. Publishing of more journals that
focus on psychotherapy in Arica
would give us for cross-pollination
of ideas in the area of
psychotherapy in Africa.
References
Awaritefe A. (1995). Meseron therapy. A
paper presented at the first national
conference on the practice of
psychotherapy in Nigeria held at the
Nigerian Institute for International
Affairs, Victoria island, Lagos, 6th –
9th November.
Awaritefe A. (1997). Meseron therapy in
the treatment of depression. A paper
presented at the National
Conference/Workshop of the
Nigerian Society for psychotherapy,
University of Calabar teaching
Hospital, Calabar, Nigeria.
Awaritefe A. (2004): Meseron therapy in
the management of Anorexia
Nervosa. Nigeria Journal of
Clinical and Counseling Psychology,
vol. 10(1), 29-36.
Ebigbo, P.O. and Ihezeu, U.H. (1981) The
"ogbanje" phenomenon and its
International Journal for Psychotherapy in Africa (5:1)
52
meaning for psychotherapy in
Nigeria.
ZeitschriftfürPsychosomatischeMedi
zin und Psychoanalyse, 27,84-91.
Ebigbo, P.O. and Tyodzua, W. (1982).
Healing methods of a prayer house
in Enugu, Nigeria. In: Erinosho O.
A. and Bell, N. W. (eds.) Mental
Health in Africa (pp. 192-195).
Ibadan: University of Ibadan Press.
Ebigbo, P. O., Oluka, J., Ezenwa, M.,
Obidigbo, G. and Okwaraji, F. (eds.)
(1995). The practice of
psychotherapy in Africa. Lagos:
International Federation for
Psychotherapy, Nigeria.
Hanneke B. (1989). Psychoanalytic
psychotherapy in Africa: Kenyan
experiences (pp. 575-585). In:
Peltzer, K. and Ebigbo, P.O. (eds.)
Clinical Psychology in Africa.
Enugu: Chuka.
Louw, D. & Madu, S. N. (2004). The
Unifying aspects of the Ubuntu
Culture. In S.E. Idemudia (Eds)
Culture, Psychosocial disorder and
Mental Health: An African
perspective-The Unifying aspects of
Cultures (pp. 10-18).Vienna: Trans-
Studienzurveränderung der Welt.
Madu, S.N. (1989).
KlientenzentriertePschotherapievaria
blen in der
Behandlungsmethodeeinesnigerianis
chenMedizinmannes.
Personzentriert, 1, 48-54.
Madu, S. N. (ed.) (2009). Trauma and
Psychotherapy in Africa.
Polokwane: World Council for
Psychotherapy.
Madu, S.N. & Adebayo, E.O. (1996).
Psychological healing processes of a
prayer house in Ibadan, and some
ideas for African psychotherapy. In:
Madu, Baguma and Pritz (eds.)
Psychotherapy in Africa, first
Investigations (pp. 129-133).
Vienna: World Council for
Psychotherapy.
Madu, S.N. &Adejumo, O. (1996).
Psychological techniques used by
five Yoruba traditional birth
attendants during normal delivery in
Nigeria. In: Madu, Baguma and
Pritz (eds.) Psychotherapy in Africa,
first Investigations (pp. 88-96).
Vienna: World Council for
Psychotherapy.
Madu, S.N., Baguma, P.K. & Pritz, A.
(eds.) (1996). Psychotherapy in
Africa, first Investigations. Vienna:
World Council for Psychotherapy.
Madu, S. N. (1991). Problems of
"western" psychotherapy practice in
Nigeria: An experience made in
Ibadan. Journal of Integrative and
Eclectic Psychotherapy, 10, 1, 68-
75.
Madu, S.N. and Ohaeri, J.U. (1989).
Nigerian traditional healers method
of treatment of obsessional neurosis.
Tropical and Geographical
Medicine. 41,4,383-387.
Madu, S. N., Baguma, P. &Pritz, A.
(eds.)(1997). African traditional
healing: Psychotherapeutic
investigations. Vienna:
FacultasUniversitaetsverlag.
Madu, S. N., Baguma, P. & Pritz, A.
(eds.)(1998). In quest for
psychotherapy for modern Africa.
Pietersburg: UNIN Press.
Madu, S. N., Baguma, P. &Pritz, A.
(eds.)(1999). Cross-cultural
Dialogue on Psychotherapy in
Africa. Pietersburg: UNIN Press.
Madu, S.N. (2020). Psychotherapy Training in Africa South of Sahara,
International Journal for Psychotherapy in Africa 5(1):44-53
53
Madu, S. N., Baguma, P. &Pritz, A. (eds.)
(2000). Psychotherapy and African
Reality. Pietersburg: UNIN Press.
Madu, S. N. (Ed.) (2003). Contributions to
psychotherapy in Africa. Polokwane:
UNIN Press.
Madu, S. N. & Govender, S. (eds.) (2005).
Mental health and psychotherapy in
Africa. Polokwane (Pietersburg):
University of Limpopo Press.
Madu, S. N. (2013). Psychotherapy: Unity
in diversity. Ife Psychologia: An
International Journal of Psychology
in Africa, 21(3), 1-16.
Nefale, M. C. & Van Dyk, G. A. J. (2003).
Ubuntu therapy - A
psychotherapeutic model for the
African client. In S. N. Madu (ed.).
Contributions to psychotherapy in
Africa (pp. 7-20). Polokwane: UNIN
Press.
Ofovwe, C. E. (2005). African originated
psychotherapy: Meseron – an
antidote for stress. In S. N. Madu
and S. Govender (eds.) Mental
health and psychotherapy in Africa
(pp. 164-171). Polokwane:
University of Limpopo Press.
Oladimeji, B.Y. (1988) Applications of
behaviour therapy in Nigeria. In:
Peltzer, K. and Ebigbo, P.O. (eds.)
Clinical psychology in Africa (pp.
612-619). Enugu: Chuka.
Peltzer, K. (1991) Cross-cultural
psychotherapy in an African context.
Journal of Integrative and Eclectic
Psychotherapy, 10, 1: 75-80.
Peltzer, K. (1995) Psychology and Health
in Africa, Examples of
Ethnopsychotherapy practice.
Frankfurt: IKO-Verlag.
Peltzer, K., Ebigbo, P.O. Stubbe, H. and
Madu, S.N. (1989) Training in
clinical psychology at masters level.
In: Peltzer, K. and Ebigbo P.O.
(eds.) Clinical Psychology in Africa
(pp. 500-511). Enugu: Chuka.
Pennymon, W. (2004). Multicultural
Competency: A Practitioner’s
Perspective. A paper presented at
the 4th African Conference on
Psychotherapy, University of the
North, South Africa, 30 June to 2
July 2004.
Pritz, A., Kuriansky, J., Nemeth, D. G.,
Mulcahy, G., Walsh, N. & Madu, S.
N. (2005). Introducing a holistic and
practical vision of human rights
from different perspectives: The
psychotherapy perspective. A World
Council for Psychotherapy (WCP)
position paper presented at the
United Nations Annual Conference
in New York,7 September 2005.
International Journal for Psychotherapy in Africa (5:1)
54
Post-Traumatic Stress Disorder And Depression In
Personnel Of Nigeria Police Force:
Implications For Psychotherapy
Chioma Ihuoma Igboegwu
18011 Pomelo Lane, Pflugerville, Texas 78660, USA.
Abstract Psychological disorders associated with combat operations among active duty military
and police personnel have become one of the most serious issues compelling the
increasing attention of scholars in traumatic stress studies, psychology, psychiatry,
contemporary medicine, human development, military and police administrators. Most of
the research investigation on this insidious mental health crisis has, however, been
reported in military populations more than in police personnel. In addition, very few
studies have examined the prevalence of post-traumatic stress disorder and depression in
Nigeria and the role of combat deployment on the manifestation of PTSD symptoms
among personnel of the Nigeria Police Force. The purpose of the current article is to
summarize and discuss the current empirical research on the prevalence of PTSD and
depression in personnel of Nigeria Police Force, using cohorts from Federal Capital
Territory, Abuja (FCT-Abuja); Abia, Benue and Lagos states, Nigeria, who returned
from counter terrorism, insurgency operations and other combat duties, and the impact
of combat deployment on PTSD symptoms manifestation in the cohort. The article, also,
highlights implications of the research findings for psychotherapy as well as recommends
a holistic psychological model, the Three-Dimensional Psychological Intervention
Strategy (3-DPIS) Model, integrating psychological science, art and culture in
psychotherapy, to address the identified mental health crisis.
Key words: Post-traumatic stress disorder, depression, police, psychotherapy, Nigeria.
Introduction Pervasive and unrelenting violence,
including terrorism, insurgency and
banditry, threatens the safety and security
of the people of Nigeria, their present-day
survival and collective future. This tragic
crisis has become one of the most serious
issues compelling the increasing attention
of scholars in traumatic stress studies,
psychology, psychiatry, contemporary
medicine, human development, military
and police administrators. The unrelenting
violence and multiple critical incident
stressors are being unleashed in various
communities, farms and forests in Nigeria
by armed herds men, and Boko Haram, a
jihadist militant organization and Islamic
State’s West Africa Province affiliated to

Igboegwu, C.I. (2020). Post-Traumatic Stress Disorder and Depression in Personnel of Nigeria Police
Force: Implications for Psychotherapy, International Journal for Psychotherapy in Africa 5(1):54-69
55
Islamic State of Iraq and the Levant (ISIL)
and ALQEIDA in the Middle East. Their
atrocities include the beheading of
Christians and security agents, abduction
and forced recruitment of under-age boys;
large-scale murders, conquests of territory,
bombing of churches, and mosques they
consider deficient in their type of Islamic
ideology; unexpected violet attacks of
villages, military, prison and police
facilities during the day and at night, mass
execution of villagers, abduction, rape and
enslavement of women and girls.
This has led to the increasing
deployment of personnel of Nigeria Police
Force to arrest the crisis being unleashed
in the various locations by the terrorists,
insurgents and criminal groups. Policing is
associated with exposure to traumatic,
violent and horrific events with an
increased risk for an insidious mental
health crisis, such as post-traumatic stress
disorder (PTSD) and co-morbidity of
depression (Marchard, Boyer, Nadeau &
Martin, 2013). McCafferty, Godofredo,
Domingo, and McCafferety (1990) also
explained that police personnel experience
similar levels of stress as people engaged
in military combat and therefore suffer the
adverse mental health impact of armed
conflict. Exposure to traumatic events in
combat operations may account for as
many as 50 percent of the casualties in
armed conflict-torn environment and
subsequent lead to the development of
PTSD (Mareth & Brooker, 1985). There
are multiple critical incident stressors
associated with policing present-day
Nigeria.
Overwhelming research evidence
shows that the prevalence rate for PTSD
and co-occurring disorders, such as
depression, among trauma survivors is
higher among those “at risk” due to their
history of traumatic incident exposure
(Ameh, Kazeem, Abdulkarim & Olasupo
(2014 ). The level of traumatic stress
connected with defeating criminal and
terrorist networks, and being involved in
war and violent conflicts can be alarming,
socially, morally destructive and
damaging to physical and mental
wellbeing (Dietz, 2004).
The psychological burden associated
with combat exposure is therefore a major
concern to military and police authorities
because of the considerable disability and
co-morbidity of depression associated
with PTSD (Kessler, 2000). The insidious
mental health crisis has adverse
implications both for the police personnel
affected, for the employer, and for society
in general. PTSD and depression in police
and military populations predispose them
to excessive use of force, alcoholism,
substance abuse, divorce, domestic
violence, violations of human rights and
international humanitarian laws, including
mass executions and torture (Amnesty
international, 2008; Marchard, Boyer,
Nadeau & Martin, 2013). It also has
adverse implications for public safety and
the security for police personnel,
communities into which they are
deployed, their families and the
psychological development of their
children (Igboegwu, 2019; Marchard,
Boyer, Nadeau & Martin, 2013; Van der
Kolk, Spinazzola & Pelcovitz, 2005;).
Chae and Boyle (2013) also linked the
increasing incidents of suicidal behavior in
the police population to those who suffer
from PTSD. While O’Hara, Violanti,
Levenson, and Clark (2013) points out that
suicide in the police population is not
openly discussed in police culture because
police officers perceive police suicide as
dishonorable to the profession. Patients
International Journal for Psychotherapy in Africa (5:1)
56
with diagnosed PTSD may also have co-
morbid psychological disorders, such as
depression (MDD), substance abuse and
addictions (Javidi & Yadollahie, 2012).
Koenen, Harley, Lyons, Wolfe, Simpson
and Goldberg (2002) explained that MDD
increases the vulnerability for the later
development of PTSD. While Breslau,
Davis, Peterson and Schultz, (2000)
revealed that PTSD was a risk factor for
later depression.
According to World Bank (2018), 22
per cent of Nigerians suffer from chronic
depression. Duckers, Alisic and Brewin
(2016) however observed the dearth of
information on PTSD in Nigeria, due to
the wide spread stigma and discrimination
associated with mental illness in the
country. Ohaeri and Jegede (1991) also
revealed that depression tends to mask
itself in somatic symptoms among
Africans, which may explain why it is also
under-diagnosed or under- recognized in
Nigeria. Depression has been found to be
the strongest single risk factor for
attempted or completed suicides (WHO,
2017). Depression and PTSD are
predictive of violence and suicides (WHO,
2017).
Despite adverse health and
security impact (Pacella, Hruska, &
Delahanty, 2013; WHO, 2017), very few
studies have examined co-morbidity of
PTSD and depression, especially in
Nigeria (Alisic & Brewin (2016). Only
prevalence rates of the disorders have
been reported with little information on
their predictors in police population. Thus,
the urgent need for theoretical models for
the understanding of PTSD and depression
in active duty personnel of Nigeria Police
Force in order to bridge the research gap
and respond to their mental health needs.
The present study therefore examined the
prevalence of PTSD and depression
among Nigeria police personnel in Federal
Capital Territory, Abuja (FCT-Abuja);
Abia, Benue and Lagos states, Nigeria,
who returned from counter terrorism,
insurgency operations and other combat
duties, and the impact of combat
deployment on PTSD symptoms
manifestation in the cohort, and its
implications for psychotherapy in Nigeria.
Research Questions
The following research questions were
raised:
1. What are the patterns of
Posttraumatic Stress Disorder
(PTSD) and Depression symptoms
among personnel of the Nigeria
Police Force?
2. How would combat deployment
bring about PTSD symptoms among
personnel of the Nigeria Police
Force?
Specific Objectives of the Study
1. To assess the prevalence of PTSD
and Depression among personnel of
the Nigeria Police Force
2. To examine the role of combat
deployment in the manifestation of
PTSD symptoms among personnel
of the Nigeria Police Force.
Relevance of the Study
It is anticipated that the outcomes of the
study will:
1. Provide information on the
prevalence of PTSD and Depression
among personnel of the Nigeria
Police Force
2. Enable authorities of the Nigeria
Police Force to identify the mental
health needs of its personnel who are
exposed to combat operations
Igboegwu, C.I. (2020). Post-Traumatic Stress Disorder and Depression in Personnel of Nigeria Police
Force: Implications for Psychotherapy, International Journal for Psychotherapy in Africa 5(1):54-69
57
3. Provide indicators for policy
formulation on psychological and
mental health services for personnel
of Nigeria Police Force.
4. Throw light on the implications of
the findings on psychotherapy in
Nigeria.
In the research study, the following
hypotheses were stated
1. There will be a higher prevalence of
PTSD and Depression symptoms
among junior than senior rank
personnel of the Nigeria Police
Force
2. There will be a relationship between
duration of combat duty deployment
and the prevalence of Post-traumatic
Stress Disorder
Scope of the Study The study was restricted to the Counter
Terrorism Unit, K9 (Dog) Unit, Special
Protection Unit (SPU), and Mobile Police
Force (MPF) at the Nigeria Police Force
Headquarters, Abuja; Benue, Abia and
Lagos states, Nigeria. The locations were
selected because pre deployment briefing
and training of police personnel for
combat assignment duties are held at the
Police Headquarters, Abuja, Nigeria. The
selection of research participants was
specific to returnees from counter
insurgency, terrorism, militancy
operations and mediation in election
violence in trouble spots across the
country.
Method
The research was a prospective study of
180 police personnel with age range 25-59
years from the Counter Terrorism, Police
Mobile Force, Special Protection and Dog
Units of the Nigeria Police Force. 70.7%
of the research participants had Senior
Secondary Eduction (SSCE) level, while
28.3% of them had tertiary level of
education; 73.9% of the cohort were junior
rank, while 26.1% of them were senior
rank; 30.6% of them had Boko Haram
violent attacks, while 22.8% of them had
militants violent attacks, among other
forms of critical incident exposure. Their
period of combat deployment ranged from
1-3 months, 4-6 months, and 7 months and
above.
Prior to the research study, the
validation of the Posttraumatic Stress
Disorder Checklist-Military Version
(PCL-M) was undertaken. The Beck
Depression Inventory (BDI) is already
being used in research in Nigeria. I chose
to validate the PCL-M to enable me screen
for PTSD in the Nigeria Police population.
The PCL-M was found reliable with
Cronbach’s Alpha reliability Coefficient
of .833. Once validated the PCL-M was
adapted for use in the Nigeria police
personnel with a new name, Post-
traumatic Stress Disorder Checklist,
Military and Police Version (PCL-MP).
Ethical approval was given by
Nigerian Psychological Association
(NPA) to justify seeking permission from
the Inspector-General of Police, Nigeria.
When approval was granted, I commenced
the selection of research participants in the
various police formations, namely, the
Nigeria Police Headquarters (NPQ),
Abuja, Benue, Abia and Lagos States to
select participants. Voluntary informed
consent was sought and given.
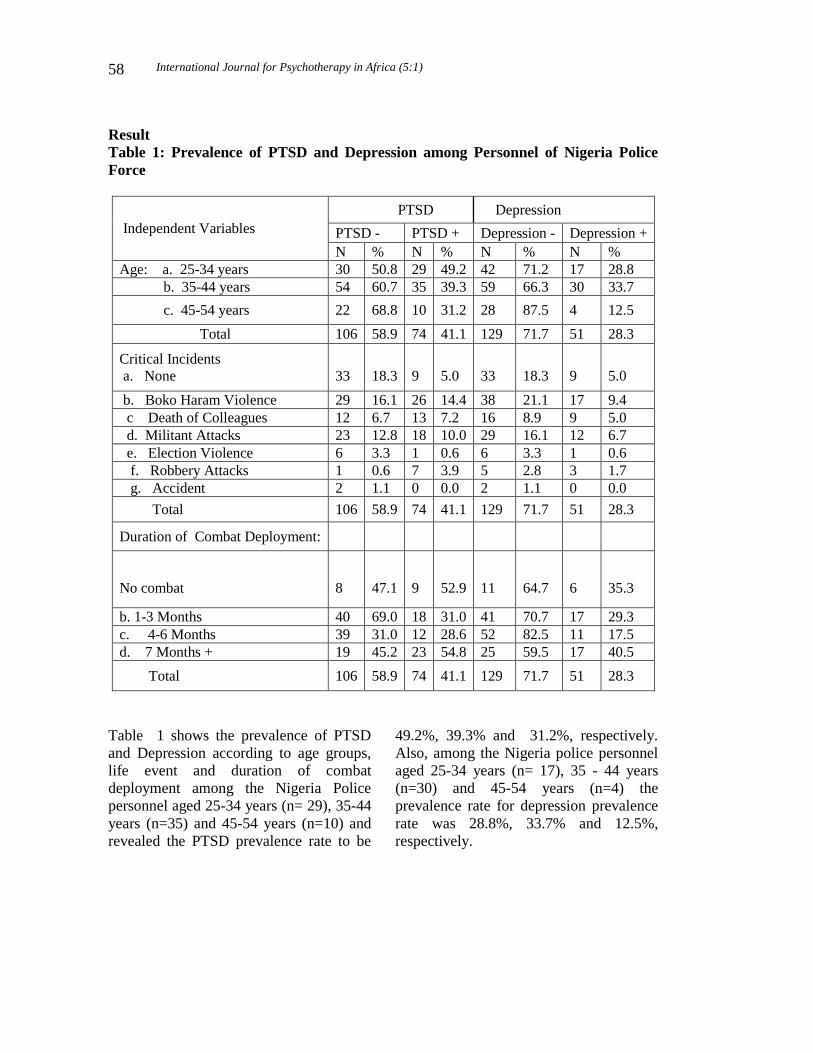
International Journal for Psychotherapy in Africa (5:1)
58
Result
Table 1: Prevalence of PTSD and Depression among Personnel of Nigeria Police
Force
Independent Variables
PTSD Depression
PTSD - PTSD + Depression - Depression +
N % N % N % N %
Age: a. 25-34 years 30 50.8 29 49.2 42 71.2 17 28.8
b. 35-44 years 54 60.7 35 39.3 59 66.3 30 33.7
c. 45-54 years 22 68.8 10 31.2 28 87.5 4 12.5
Total 106 58.9 74 41.1 129 71.7 51 28.3
Critical Incidents
a. None
33
18.3
9
5.0
33
18.3
9
5.0
b. Boko Haram Violence 29 16.1 26 14.4 38 21.1 17 9.4
c Death of Colleagues 12 6.7 13 7.2 16 8.9 9 5.0
d. Militant Attacks 23 12.8 18 10.0 29 16.1 12 6.7
e. Election Violence 6 3.3 1 0.6 6 3.3 1 0.6
f. Robbery Attacks 1 0.6 7 3.9 5 2.8 3 1.7
g. Accident 2 1.1 0 0.0 2 1.1 0 0.0
Total 106 58.9 74 41.1 129 71.7 51 28.3
Duration of Combat Deployment:
No combat
8
47.1
9
52.9
11
64.7
6
35.3
b. 1-3 Months 40 69.0 18 31.0 41 70.7 17 29.3
c. 4-6 Months 39 31.0 12 28.6 52 82.5 11 17.5
d. 7 Months + 19 45.2 23 54.8 25 59.5 17 40.5
Total 106 58.9 74 41.1 129 71.7 51 28.3
Table 1 shows the prevalence of PTSD
and Depression according to age groups,
life event and duration of combat
deployment among the Nigeria Police
personnel aged 25-34 years (n= 29), 35-44
years (n=35) and 45-54 years (n=10) and
revealed the PTSD prevalence rate to be
49.2%, 39.3% and 31.2%, respectively.
Also, among the Nigeria police personnel
aged 25-34 years (n= 17), 35 - 44 years
(n=30) and 45-54 years (n=4) the
prevalence rate for depression prevalence
rate was 28.8%, 33.7% and 12.5%,
respectively.
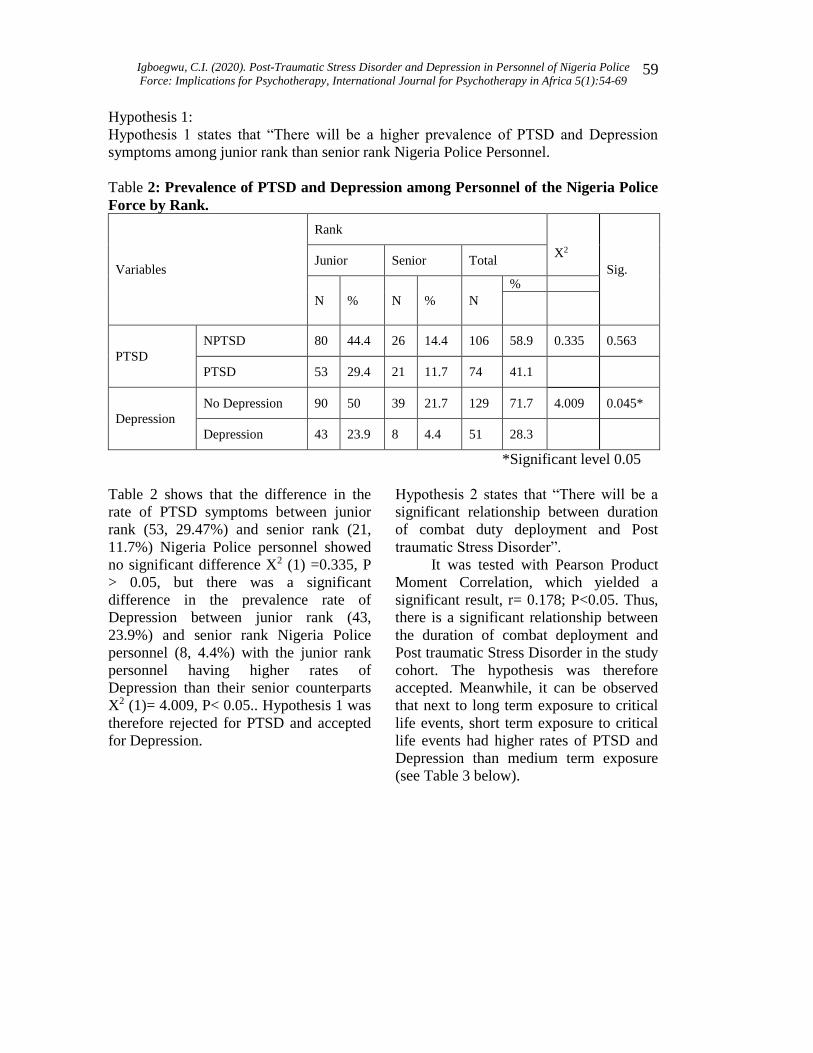
Igboegwu, C.I. (2020). Post-Traumatic Stress Disorder and Depression in Personnel of Nigeria Police
Force: Implications for Psychotherapy, International Journal for Psychotherapy in Africa 5(1):54-69
59
Hypothesis 1:
Hypothesis 1 states that “There will be a higher prevalence of PTSD and Depression
symptoms among junior rank than senior rank Nigeria Police Personnel.
Table 2: Prevalence of PTSD and Depression among Personnel of the Nigeria Police
Force by Rank.
Variables
Rank
Sig. Junior Senior Total
X2
N % N % N
%
PTSD
NPTSD 80 44.4 26 14.4 106 58.9 0.335 0.563
PTSD 53 29.4 21 11.7 74 41.1
Depression
No Depression 90 50 39 21.7 129 71.7 4.009 0.045*
Depression 43 23.9 8 4.4 51 28.3
*Significant level 0.05
Table 2 shows that the difference in the
rate of PTSD symptoms between junior
rank (53, 29.47%) and senior rank (21,
11.7%) Nigeria Police personnel showed
no significant difference X2 (1) =0.335, P
> 0.05, but there was a significant
difference in the prevalence rate of
Depression between junior rank (43,
23.9%) and senior rank Nigeria Police
personnel (8, 4.4%) with the junior rank
personnel having higher rates of
Depression than their senior counterparts
X2 (1)= 4.009, P< 0.05.. Hypothesis 1 was
therefore rejected for PTSD and accepted
for Depression.
Hypothesis 2 states that “There will be a
significant relationship between duration
of combat duty deployment and Post
traumatic Stress Disorder”.
It was tested with Pearson Product
Moment Correlation, which yielded a
significant result, r= 0.178; P<0.05. Thus,
there is a significant relationship between
the duration of combat deployment and
Post traumatic Stress Disorder in the study
cohort. The hypothesis was therefore
accepted. Meanwhile, it can be observed
that next to long term exposure to critical
life events, short term exposure to critical
life events had higher rates of PTSD and
Depression than medium term exposure
(see Table 3 below).
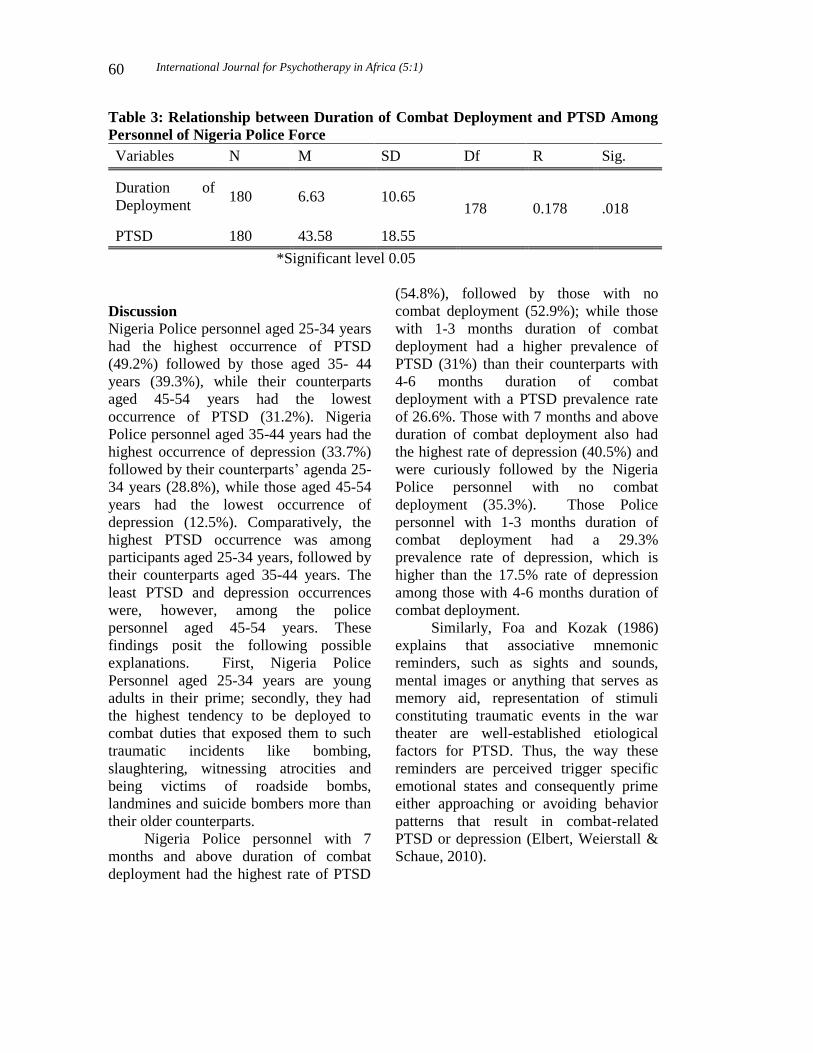
International Journal for Psychotherapy in Africa (5:1)
60
Table 3: Relationship between Duration of Combat Deployment and PTSD Among
Personnel of Nigeria Police Force
Variables N M SD Df R Sig.
Duration of
Deployment 180 6.63 10.65
178 0.178 .018
PTSD 180 43.58 18.55
*Significant level 0.05
Discussion
Nigeria Police personnel aged 25-34 years
had the highest occurrence of PTSD
(49.2%) followed by those aged 35- 44
years (39.3%), while their counterparts
aged 45-54 years had the lowest
occurrence of PTSD (31.2%). Nigeria
Police personnel aged 35-44 years had the
highest occurrence of depression (33.7%)
followed by their counterparts’ agenda 25-
34 years (28.8%), while those aged 45-54
years had the lowest occurrence of
depression (12.5%). Comparatively, the
highest PTSD occurrence was among
participants aged 25-34 years, followed by
their counterparts aged 35-44 years. The
least PTSD and depression occurrences
were, however, among the police
personnel aged 45-54 years. These
findings posit the following possible
explanations. First, Nigeria Police
Personnel aged 25-34 years are young
adults in their prime; secondly, they had
the highest tendency to be deployed to
combat duties that exposed them to such
traumatic incidents like bombing,
slaughtering, witnessing atrocities and
being victims of roadside bombs,
landmines and suicide bombers more than
their older counterparts.
Nigeria Police personnel with 7
months and above duration of combat
deployment had the highest rate of PTSD
(54.8%), followed by those with no
combat deployment (52.9%); while those
with 1-3 months duration of combat
deployment had a higher prevalence of
PTSD (31%) than their counterparts with
4-6 months duration of combat
deployment with a PTSD prevalence rate
of 26.6%. Those with 7 months and above
duration of combat deployment also had
the highest rate of depression (40.5%) and
were curiously followed by the Nigeria
Police personnel with no combat
deployment (35.3%). Those Police
personnel with 1-3 months duration of
combat deployment had a 29.3%
prevalence rate of depression, which is
higher than the 17.5% rate of depression
among those with 4-6 months duration of
combat deployment.
Similarly, Foa and Kozak (1986)
explains that associative mnemonic
reminders, such as sights and sounds,
mental images or anything that serves as
memory aid, representation of stimuli
constituting traumatic events in the war
theater are well-established etiological
factors for PTSD. Thus, the way these
reminders are perceived trigger specific
emotional states and consequently prime
either approaching or avoiding behavior
patterns that result in combat-related
PTSD or depression (Elbert, Weierstall &
Schaue, 2010).

Igboegwu, C.I. (2020). Post-Traumatic Stress Disorder and Depression in Personnel of Nigeria Police
Force: Implications for Psychotherapy, International Journal for Psychotherapy in Africa 5(1):54-69
61
Police personnel and members of the
Armed Forces, who are often deployed to
combat zones are of younger age group,
except for those who joined at the officer
cadre. This means that police personnel of
younger age group, who are deployed to
combat zones, are at the receiving end of
the command chain which limits their
choices to avoid or escape traumatic
incidents. One notes, also, that the highest
depression prevalence was among the
police personnel aged 35-44 years. The
least PTSD and depression prevalence was
among the police personnel aged 45-54
years. This suggests that the rate of
depression in the cohort was differential.
This is indicated by the 33.7% prevalence
of depression among Nigeria Police
personnel aged 33-44 years, which is
followed by the 28.8% rate of depression
among the Nigeria Police personnel aged
25-34 years. Those aged 45-54 years had
the lowest prevalence of depression and
PTSD, implying that in the face of
adversity, people respond differently.
While some people experience PTSD,
others experience depression. These
findings therefore suggest that more
elderly Nigeria Police personnel may be at
command positions. Accordingly, the
trauma they experience might be vicarious
and not as manifest as those of the
younger age groups because they identify
with the predicament of the “rank and
file”.
The discovery that Nigeria Police
personnel that experienced Boko Haram
and militancy related violence have the
highest occurrence of PTSD corroborates
the findings of Hoge (2004) and Gao
(2006) that PTSD and depression are
significantly linked to combat trauma
exposure. PTSD and depression are not
only linked to combat exposure, but also
to participating in or witnessing atrocities.
It is interesting to note that violence
related to elections, robbery, accidents and
the bereavement of colleagues did not
generate high rates of PTSD and
depression. This outcome confirms that
violent extremism, such as terrorism,
militancy and insurgency, which trigger
high levels of stress, have adverse mental
health consequences, such as heightened
rates of PTSD and depression.
Another outcome of the study was
that Nigeria Police personnel with 7
months and above duration of combat
deployment had the highest occurrence of
PTSD (54.8%), followed by Nigeria
Police personnel with no combat
deployment (52.9%). While the Nigeria
Police personnel with 1-3 months duration
of combat deployment had a higher
prevalence of PTSD (31.0%) than the
Nigeria Police personnel with 4-6 months
duration of combat deployment, with a
PTSD prevalence rate of 28.6%. The
Nigeria Police personnel with 7 months
and above duration of combat deployment
had the highest rate of depression (40.5%)
and were curiously followed by the
Nigeria Police personnel with no combat
deployment (35.3%).In addition, the
Nigeria Police personnel with 1-3 months
duration of combat deployment had a
29.3% prevalence of depression, which is
higher than the 17.5% rate of depression
among Nigeria Police personnel with 4-6
months duration of combat deployment. A
possible explanation for these is that
cumulative stressful impact of combat
exposure and exhaustion of coping
resources of the Nigeria Police personnel
are responsible.
But the unusual result of high rates
of PTSD and depression among personnel
of the Nigeria Police Force, who were

International Journal for Psychotherapy in Africa (5:1)
62
never deployed to combat operation,
suggests that combat operations are not
the only stressors capable of inducing
PTSD and depression among human
populations. The contribution of other life
events that were not anticipated by the
study could have been significant. For
example, Heim and Nemeroff (2008)
revealed that exposure to traumatic
incidents in childhood increases the risk of
adult psychopathology, because of the
same processes of sensitization of
traumatic memories. Cannabis and alcohol
abuse/dependence can also induce PTSD
and Depression (Raimo & Schuckit,
1998). Therefore, genetic predisposition,
exposure to adverse life events, such as
gender-based and domestic violence
(GBDV) tends to place any victim at risk
to PTSD and depression (Jessor & Jessor,
1977).
One observes, also, that Nigeria
Police personnel with 1-3 months duration
of combat exposure had a higher
prevalence of depression and PTSD than
the personnel with 4-6 months duration of
combat exposure. This could be due to
“shock” at the onset of combat after which
coping efforts led to “adaptation”. While
the least rate of PTSD and depression
associated with 4-6 months duration of
combat deployment may be indicative of
the positive use of coping efforts by
personnel of the Nigeria Police Force.
This outcome conforms with Selye’s
proposition of the Generalised Adaptation
Syndrome (GAS), whereby the initial
response to stress is accompanied by vivid
physiological arousal followed by a period
of resilience characterized by the fight or
flee response the failure, which leads to
learned helplessness, frustration and
exhaustion (Selye, 1975.)
The study revealed that PTSD and
depression symptoms increase as duration
of combat deployment increases, which is
consistent with Hoge (2004) and Gao
(2006). The discovery that Nigeria Police
personnel that experienced Boko Haram
and militancy related violence have the
highest occurrence of PTSD also
corroborates the findings of Hoge (2004)
and Gao (2006) that PTSD and depression
are significantly linked to trauma
exposure. PTSD and depression are not
only linked to combat exposure, but also
to participating in or witnessing atrocities.
A major part of the symptomatology
of PTSD is the remembering of the painful
recollection in the mind which has both
features of psycho-physiological
reactivation and psychological pain. A
distinctive part of this condition is the
continuous reactivation of the traumatic
memory and the associated stress response
related to the persistent aggravation
rekindling of the reactivity of the
individual (McFarlane, Yehuda & Clark,
2002). Thus, PTSD symptoms have been
explained as the failure of the retention
and extinction of conditioned fear (Milad,
Orr, Lasko, Chang, Rauch & Pitman,
2008). Another important point to note is
that the recollection of painful, distressful
incidents in the mind are a key component
of man’s phenomenological reaction to
distressing life events. Freud emphasized
the importance of recollection of painful
incidents in the mind in his first lecture
with Breuer, signifying that that these
were the prime causes or forces that
mainly bring about symptom onset and
maintenance (Freud, 2001). Wessa and
Flor (2007) explained that these
recollection of painful, distressful
incidents in the mind are activated by a
fear conditioning mechanisms, which

Igboegwu, C.I. (2020). Post-Traumatic Stress Disorder and Depression in Personnel of Nigeria Police
Force: Implications for Psychotherapy, International Journal for Psychotherapy in Africa 5(1):54-69
63
maintain and ignite the increased arousal
that is central to the symptoms of PTSD,
in the presence of adverse environmental
conditions. Scholars, who specialize in
PTSD and depression research, also
believe that the predisposition to develop
both PTSD and depression most likely
indicates a joint vulnerability with regard
to trauma exposure (McFarlane, Yehuda
& Clark, 2002).
It is important to note that combat-
related psychological disorders, such as
PTSD and depression among personnel of
the Nigeria Police Force do not only affect
the Police personnel, but their families,
Nigerian communities and the general
public. PTSD and depression can also lead
to poor decision-making, disciplinary
problems, excessive use of sick leave,
severe difficulty in regulating affect,
which can impact negatively on the
quality of life as well as the relationships
of the police personnel. There are also
attention difficulties that can undermine
learning and employment and thus
complicate reintegration of police
returnees with their families and
communities. There can also be negligent,
accidental bullet discharge, alcohol/drug
dependence, explosive anger,
interpersonal violence, including gender-
based and domestic violence (GBDV),
murder and suicide.
Implications for Psychotherapy
Psychotherapists in Nigeria should take
the above findings into consideration
when treating clients from the Nigeria
Police Force. The preponderance of
available scientific evidence has
established that psychological
interventions, particularly cognitive-
behavioral therapies (CBTs), are usually
as effective or more effective than
medications in the treatment of
depression, even if severe, for both
vegetative and social adjustment
symptoms, especially when patient-rate
measures and long-term follow-up are
examined (Antonuccio, 1995). A meta-
analysis by Wexler and Cicchetti, (1992)
also stated that pharmacotherapy alone is
substantially worse than psychotherapy,
alone. The relapse rate is higher among
depressives treated with combined
treatment than with, just psychotherapy.
Psychotherapy is more effective than
medication in the long-term and is more
enduring than medication. While Grohol,
(2019) also asserts that psychotherapy is
more cost-effective, and leads to fewer
relapses of anxiety and mild to moderate
depression than medication use alone.
Depression can be effectively treated with
six to eight sessions of psychotherapy,
particularly cognitive behavioral therapy
and problem-solving therapy.
Psychotherapy is provided in active
collaboration between therapist and client.
Increased interdisciplinary collaboration
between psychotherapists in Nigeria, other
mental health disciplines and public health
is recommended to develop, enact, and
evaluate multi-level preventive
interventions aimed at decreasing the
population health burden of major
depression.
According to APA (2013), the main
treatments for people with PTSD are
psychotherapy, medications, or both.
Psychological treatments are however
considered first-line treatment for PTSD.
They have been confirmed to have larger
effect sizes in Randomised Clinical Trials
(RCTs) than pharmacotherapy. Cognitive
behaviour therapy (CBT), prolonged
exposure, and eye movement
desensitization and reprocessing therapy

International Journal for Psychotherapy in Africa (5:1)
64
have had multiple RCTs that showed large
reductions in PTSD symptoms (Foa,
Rothbaum, & Furr, 2003). Therapy
involves an active collaboration between
therapist and client.
To monitor progress in treatment,
brief self-report measures of symptoms of
PTSD should be routinely used. The 17-
item PTSD Checklist, such as the
Posttraumatic Stress Disorder Checklist,
Military and Police Version (PCL-MP),
Posttraumatic Stress Disorder Checklist,
Civilian Version (PCL-C) and Beck
Depression Inventory (BDI) should be
commonly used scales for monitoring
PTSD symptoms and Depression among
personnel of Nigeria Police Force.
Conclusion
In the present study, prevalence of PTSD
and depression among personnel of the
Nigeria Police Force were examined;
study result analysis revealed highest
PTSD occurrence among Nigeria Police
personnel aged 25-34 years, while the
highest depression occurrence was among
the police personnel aged 35-44 years. The
least PTSD and depression occurrences
were however, among the police personnel
aged 45-54 years; age, critical incident
exposure and duration of combat
deployment were predictors of PTSD in
the Nigeria police personnel. More
attention should be given to these factors
in guiding policy and procedures for both
pre and post deployment psychological
evaluation and psychotherapeutic
intervention services for active duty police
personnel of the Nigeria Police Force.
Recommendations
Most active duty Nigeria Police personnel
are in their prime age range placing them
at risk for the onset of PTSD and
depression. There is therefore the need for
psychotherapeutic services programme
development, implementation, evaluation
and monitoring for young Police personnel
and their family members. This will be of
great benefit to the Nigeria Police Force
and the Nigerian society and will help
Nigeria Police personnel to recognize
signs and symptoms of stress, PTSD and
depression symptoms in themselves and
others as well as decrease the stigma of
seeking assistance.
Findings from the study also call for
the bridging of gaps in knowledge,
policies and institutional capacities of
stakeholders, in order to mainstream the
psychological dimension of social and
criminal justice, public safety, security and
development sectors, including health,
education, women, children and youth
development, in the policy agenda, at the
community level, national, regional and
international levels, using the Three-
Dimensional Psychological Intervention
Strategy (3-DPIS) Model, which has been
developed by Igboegwu (Igboegwu,
2006). This will empower the Police and
Armed Forces with evidence-based data,
including relevant information, for
decision making for the balancing of
priorities of changing combat mission
requirements with preservation of long-
term mental health and psychological
well-being of active duty Military and
Police Forces.
The 3-DPIS Model, integrating
psychological science, art and culture in
psychotherapy, will provide a holistic
intervention to address the identified
mental health crisis. It will facilitate pro-
social engagement with all diverse
categories of the population, mobilization
of their cooperation at the community
level, national, regional and international
Igboegwu, C.I. (2020). Post-Traumatic Stress Disorder and Depression in Personnel of Nigeria Police
Force: Implications for Psychotherapy, International Journal for Psychotherapy in Africa 5(1):54-69
65
levels, including the dissemination of
evidence-based data, to bridge the gaps in
knowledge, policies and institutional
capacities in the highlighted sectors within
which violence thrives. It will transform
and empower communities and
institutions, at all levels, to mainstream the
psychological dimension of social and
criminal justice, public safety, security and
development sectors, including health,
education, women, children and youth
development, as a priority agenda, in order
to break the cycle of violence, accelerate
public safety, security and development in
the society.
References
Adebayo, D. O. (1996). The relationship
between job expectation, self
esteem, perceived controllability and
unemployment: Induced general
depression. Issues in Health
Psychology, 3 (2), 22-27
Al-Turkait, F. A., & Ohaeri, J. U. (2008).
Psychopathological status, behavior
problems, and family
adjustment of Kuwaiti children
whose fathers were involved in the
first Gulf war. Child and
Adolescent Psychiatry and Mental
Health, 2(1), 12.
Ameh, A.S.1, Kazeem, O.T., Abdulkarim,
I.B., & Olasupo. S. (2014). Post-
traumatic stress disorder among
Nigerian Military Personnel-
Findings from post-deployment
survey. Projournal of Humanities
and Social Science, 2 (1), 56-6.
American Psychiatric Association (2013).
Diagnostic and statistical manual of
mental disorders, (5th ed.),
Arlington, VA: American
Psychiatric Publishing.
Amnesty international (May, 2008).
Nigeria: “Pragmatic policing”
through extra-judicial executions
and torture. AI Index: AFR
44/006/2008 Correlates and
consequences of exposure to video
game violence: hostile personality,
empathy, and aggressive
behavior. Personality and Social
Psychology Bulletin, 31(11), 1573-
1586.
Antonucccio, David (1995).
Psychotherapy for depression: No
stronger medicine. American
Psychologists Journal. 50(6):450-
4522.
Breslau, N., Kessler, R. C., Chilcoat, H.
D., Schultz, L. R., Davis, G. &
Andreski P. (1998). Trauma and
post-traumatic stress disorder in the
community: The 1996 Detroit area
survey of trauma. Archive of
General Psychiatry. 55: 626–632.
Callanan & Rosenberger (2011). The
Influence of Media on Penal
Attitudes, Criminal Justice Review.
36: 4, 435-455
Chae, M., & Boyle, D. (2013). Police
Suicide: Prevalence, Risk, and
Protective Factors. Policing: An
International Journal of Police
Strategies & Management, 36, 91-
118.
Dietz, M. (2014). Explaining Combat
Related Posttraumatic Stress
Disorder: An Integrated Mental
Illness and Military Process Model.
Doctorate Degree Dissertation East
Tennessee State (USA)
Ehlers, A. & Clark, D. M. (2000). A
cognitive model of posttraumatic
stress disorder. Behaviour Research
and Therapy. 38, 319-345
International Journal for Psychotherapy in Africa (5:1)
66
Freud, S. (2001). Beyond the Pleasure
Principle. The Standard Edition of
the Complete Works of Sigmund
Freud (Vol. XVIII). London:
Vintage.
Foa, E.B., & Kozak, M.J. (1986).
Emotional processing of fear:
exposure to corrective information.
Psychological Bulletin, 99, 20-35.
Foa, E. B., & Rothbaum, B. O. (1998).
Treating the trauma of rape:
Cognitive-behavioral therapy for
PTSD. New York: The Guilford
Press.
GAO (2006). VA Health Care: Spending
for Mental Health Strategic Plan
Initiatives was substantially less
than planned. GAO-07-66
Washington, DC: GAO.
Green, B.L., Saunders, P.A., Power, E.,
Dass-Brailsford, P., Bhat Schelbert,
P., Giller, E., Wissow, L., Hurtado-
de-Mendoza, A. & Mete, M.
(2016). “Trauma-Informed Medical
Care: Patient response to a primary
care provider communication
training.” Journal of Loss and
Trauma. 21, 147-159.
Greene-Shortridge, T. M., Britt, T. W.,
and Castro, C. A. (2007). The stigma
of mental health problems in the
military. Military Medicine, 172
(2)157
Grohol, J. (2018). Depression Treatment:
Psychotherapy, Medication or
Both? Psych Central. Retrieved on
April 17, 2020, from
https://psychcentral.com/lib/depressi
on-treatment-Psychotherapy-
medication-or both
Heim, C. & Nemeroff, C. B. (2001). The
role of childhood trauma in the
neurobiology of mood and anxiety
disorders: preclinical and clinical
studies. Biological Psychiatry.
49(12):1023-
39.
Hoge, C., Castro, C., Messer, S., McGurk,
D., Cotting, D., & Koffman, R.
(2004). Combat duty (s) in Iraq and
Afghanistan, mental health
problems, and barriers to care. New
England Journal of Medicine, 351,
13-22.
Igboegwu, C. I. (2016). Adverse mental
health impact of armed conflict in
Africa. Unpublished paper presented
at the Seminar held by the
Department of Psychology,
Nasarawa State University, Keffi,
Nigeria
Javidi, H., &Yadollahie, M. (2012). Post-
traumatic Stress Disorder. The
International Journal of
Occupational and Environmental
Medicine, 3, 1.
Jessor, R., & Jessor, S. L. (1977). Problem
Behaviour and Psychological
Development Longitudinal Study of
Youth. New York: Academic Press.
John G. S, David A. P. & John R. S.
(1984). Post-Traumatic Stress: Study
of Police Officers Involved in
Shootings. Psychological Reports:
55(1): 127-131.
John, G. Stratton, David, A. Parker, John
R. Snibbe (1984, August). Post-
Traumatic Stress: Study of Police
Officers Involved in Shootings.
Psychological Report. 55(1),127.
Jordan B.K., Marmar C.R., Fairbank J.A.,
Schlenger W.E., Kulka R.A., Hough
R.L., Weiss D.S. (92) Problems in
families of male Vietnam veterans
with posttraumatic stress disorder
Journal of Consulting and Clinical
Psychology, 60(6), 916–926.
Igboegwu, C.I. (2020). Post-Traumatic Stress Disorder and Depression in Personnel of Nigeria Police
Force: Implications for Psychotherapy, International Journal for Psychotherapy in Africa 5(1):54-69
67
McFarlane, A. C., Yehuda, R. & Clark, C.
R. (2002). Biologic models of
traumatic memories and post-
traumatic stress disorder: The role of
neural networks. Psychiatric Clinics
of North America Special Issue:
Recent Advances in the Study of
Biological Alterations in Post-
Traumatic Stress Disorder. 25:253–
270
McCafferty, F. L., Domingo, G. D., &
McCafferty, E. A. (1990).
Posttraumatic stress disorder in the
police officer: paradigm of
occupational stress. Southern
Medical Journal, 83(5), 543-547.
Marchand, A., Nadeau, C. Nadeau, C,
Beaulieu-Prévost, D. Boyer., B. &
Martin. M. (2015). Predictors of
Posttraumatic Stress Disorders,
Psychological Trauma: A
prospective study, theory, research,
practice, and policy. American
Psychological Association. 7(3)
212–221
Milad, M. R.; Orr, S. P.; Lasko, N. B.;
Chang, Y.; Rauch, S. L. &
Pitman, R. K. (2008). Presence and
acquired origin of reduced recall for
fear extinction in PTSD: results of a
twin study. Journal of Psychiatric
Research. 2008; 42(7):515-
20Mareth, T.R., & Brooker, A.E.
(1985). Combat stress reaction: a
concept in evolution. Military
Medicine, 150, 4: 186 - 190.
Kessler, R. C. (2000). Posttraumatic stress
disorder: the burden to the
individual and to society. Journal of
Clinical Psychiatry, 61(5), 4-12.
Kessler, R. C. & Bromet, E. J. (2013). The
epidemiology of depression across
cultures. Annual Review on Public
Health, 34: 119–138.
Kessler, R. C.; Sonnega, A. Bromet, E.
Hughes, M. & Nelson, C. B. (1995).
Posttraumatic stress disorder in the
national comorbidity survey.
Archives of General Psychiatry, 52,
1048-106
Kessler, R. C.; Chiu, W.T.; Demler O.;
Merikangas, K.R, ; Walters, E.
E.(2005). Prevalence, severity, and
comorbidity of 12-month DSM- IV
disorders in the National
Comorbidity Survey Replication
Archive of General Psychiatry.
62(6):617-627
Koenen, K. C., Harley, R., Lyons, M. J.,
Wolfe, J., Simpson, J. C., &
Goldberg, J. (2002). A twin registry
study of familial and individual risk
factors for trauma exposure and
posttraumatic stress disorder. The
Journal of Nervous and Mental
Disease. 190: 209– 218
Keane, Zimmering & Candesen (1985). A
behavior formulation of PTSD in
Vietnam veterans. The Behaviour
Therapist. 8, 9-12
Koenen, K. C., Harley, R., Lyons, M. J.,
Wolfe, J., Simpson, J. C., &
Goldberg, J. (2002) A twin registry
study of familial and individual risk
factors for trauma exposure and
posttraumatic stress . The Journal of
Nervous and Mental Disease. 190:
209-218
Koenen K. C., Stellman, S. D., Sommer, J.
F. & Stellman, J. M. (2008).
Persisting posttraumatic stress
disorder symptoms and their
relationship to functioning in
Vietnam veterans: a 14-year follow-
up. Journal of Trauma Stress.
2008;21(1):49–57.
Kulka, R.A., Schlenger, W.E., Fairbank,
J.A., Hough, R.L., Jordan, B. K.,
https://www.ncbi.nlm.nih.gov/pubmed/?term=Kessler%20RC%5BAuthor%5D&cauthor=true&cauthor_uid=15939839
https://www.ncbi.nlm.nih.gov/pubmed/?term=Walters%20EE%5BAuthor%5D&cauthor=true&cauthor_uid=15939839
International Journal for Psychotherapy in Africa (5:1)
68
Marmar, C.R., & Weiss, D.S.
(1990). Trauma and the Vietnam
war generation: Report of findings
from the national Vietnam veterans
readjustment Study. New York:
Brunner/Mazel.
McCafferty, F. L., Domingo, G. D., &
McCafferty, E. A. (1990).
Posttraumatic stress disorder in the
police officer: paradigm of
occupational stress. Southern
Medical Journal, 83(5), 543-547.
Marchand, A., Nadeau, C. Nadeau, C,
Beaulieu-Prévost, D. Boyer., B. &
Martin.., M. (2015). Predictors of
Posttraumatic Stress Disorders,
Psychological Trauma: A
prospective study, theory, research,
practice, and policy. American
Psychological Association. 7, 3,
212–221
Maguen, Shira, Li Ren, Jeane O. Bosch,
Charles R. Marmar, and Karen
H. Seal, “Gender Differences in
Mental Health Diagnoses Among
Iraq and Afghanistan Veterans
Enrolled in Veterans Affairs Health
Care,” American Journal of Public
Health, Vol. 100, 12, 2010, pp.
2450–2456.
Mareth, T.R., & Brooker, A.E. (1985).
Combat stress reaction: a concept in
evolution. Military Medicine, 150, 4:
186 - 190.
Muller, R. T. (2015, November, 2012).
Officers with PTSD at Greater Risk
for Police Brutality. Psychology
Today. New York City
National Center for Post-Traumatic Stress
Disorder (2004). Iraq war clinical
guide. National center for PTSD and
the department veterans affairs.
Retrieved from
http://www.ptsd.va.gov
Nel, J. A. (1994). A contextual approach
to post-shooting trauma in the South
African Police services.
Unpublished paper presentation at a
police psychology conference,
Pretoria (South Africa).
Ohaeri, J. U. & Jegede, R. O. (1991).
Depression and the general medical
practitioner in Nigeria. Medicare 6
(7), 11-3.
O'Hara, A. F., Violanti, J. M., Levenson,
R. L., & Clark, R. G. S. (2013).
National police suicide estimates:
Web surveillance study III.
(Website, Date of Access????)
Selye, H. (1975). Stress and Distress.
Comprehensive Therapy. 1(8): 9-13.
Shalev, A. Y., Freedman, S., Peri,
T., Brande, D., Sahar, T., Orr, S.P.
& Pitman, R. K. (1998). Prospective
study of posttraumatic stress
disorder and depression following
trauma. American Journal of
Psychiatry. 155(5):630-7
Van der Kolk, B. A.; Spinazzola J.;
Pelcovitz, D.; Sunday, Roth, S.
(2005). Disorders of Extreme Stress:
The Empirical Foundation of a
Complex Adaptation to Trauma.
Journal of Traumatic Stress.
18(5), 389–399
Wessa, M., & Flor, H. (2007). Failure of
Extinction of Fear Responses in
Posttraumatic Stress Disorder:
Evidence from Second-Order
Conditioning. American Journal of
Psychiatry. 164:1684–1692).Wexler,
B.E., & Cicchetti, D.V. (1992). The
outpatient treatment of depression:
Implications of outcome research for
clinical practice. The Journal of
Igboegwu, C.I. (2020). Post-Traumatic Stress Disorder and Depression in Personnel of Nigeria Police
Force: Implications for Psychotherapy, International Journal for Psychotherapy in Africa 5(1):54-69
69
Nervous and Mental Disease,
180(5), 277-286.
World Bank. (2018). Nigeria - Depression
Brief. Mind body behavior
development brief. Washington,
D.C.: World Bank Group. http:
documents.worldbank.org/curated/e/
607301516882442320/Nigeria-
Depression-Brief.

International Journal for Psychotherapy in Africa (5:1)
70
Personality Trait, Drug use and Abuse as Predictors
of Suicidal Intention Among Youths:
A Focus for Psychotherapy
Charity Justin Takyun,
Department of Psychology, Faculty of Social Sciences,
Federal University of Lafia, Nasarawa State, Nigeria
Okwoli Matthew James
Department of Psychology, Faculty of Social Sciences,
Federal University of Lafia, Nasarawa State, Nigeria
Maryam Abubakar
Benue State University, Makurdi, Nigeria
Abstract The rate at which youths commit suicide and the number who attempt suicide is on the
increase every day. Every suicide is a tragedy that affects families, communities and
entire countries and has long-lasting effects on the people left behind. This study
investigates Personality Trait and Drug use and Abuse as predictors of suicidal ideation
among adolescents in Makurdi Metropolis in Benue State, Nigeria, and makes
suggestions for effective psychotherapeutic treatment of suicidal ideation among the
youth. The study employed survey research design where 325 participants were
randomly drawn from Makurdi Metropolis in Benue State through Stratified,
Convenience and Simple Random Sampling Methods. Personality Trait Scale, Drug use
and Abuse Scale, Bio data and Suicidal Ideation Scale were used for data collection.
Three hypotheses were tested using multiple regression and simple regression analyses.
The result revealed a positive relationship between Personality Trait and suicidal
intention among adolescents. Drug use and Abuse also shows significant influence on
suicidal intention among the youths. There was a significant interactive influence of
Personality Trait and Drug use and Abuse on suicide ideations among the adolescents.
Based on these findings, it was concluded that Personality Trait and Drug use and Abuse
are predictors of suicidal ideation among youths in Makurdi Metropolis in Benue State,
Nigeria. It is recommended that understanding personality traits of youths, type of
substance used and abused can further help Clinicians during psychotherapeutic
sessions with youths in solving problems of suicidal ideation. Parents and caregivers
should be enlightened on the behavioral and attitudinal signs to watch out for when their
wards are abusing drugs and also the danger of the use and abuse of drugs.
Key words: Personality Traits, Substance Use and Abuse, Suicidal Ideation, and
psychotherapy.

Takyun, C.J.; Okwoli, M.J. & Abubakar, M. (2020). Personality Trait, Drug use and Abuse as
Predictors of Suicidal Intention Among Youths: A Focus for Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):70-83
71
Introduction The rate at which youths commit suicide
and the numbers who attempt suicide
increase daily. Every suicide is a tragedy
that affects families, communities and
entire countries and has long-lasting
effects on the people left behind. The
major tragedy of suicide is not the victim
but the people left behind. Many families
have been forced into single parenting and
poverty as result of suicide.
Youth is the period in life
characterized by movement, changes and
transitions from one state into another in
several domains at the same time. Youths
sometimes address new challenges with
regard to building their own identity,
developing self-esteem, acquiring
increasing independence and
responsibility and building new intimate
relationships, etc. In the meantime, they
are subject to ongoing, changing
psychological and physical processes
themselves. Youths are often confronted
with high expectations; sometimes too
high from significant relatives and peers.
Such situations inevitably provoke a
certain degree of helplessness, insecurity,
stress and a sense of losing control which
may lead to suicidal ideation (Patton,
Sawyer, Santelli, Ross, Afifi&Allen,
2016). To address these challenges and to
reduce the rates of suicide in the country,
the risk factors of this disorder need to be
identified for proper solution.
Suicide is a fatal self-injurious act
with some evidence of intent to die.
Suicidal thoughts are thinking about,
considering, or planning suicide
(Shneidman, 1985). The range of suicidal
ideation varies from fleeting thoughts, to
extensive thoughts, to detailed planning.
Most people who have suicidal thoughts
do not go on to make suicide attempts, but
suicidal thoughts are considered a risk
factor. Suicidal ideation does not just
occur, but comes as a result of some
factors; life events and family events, all
of which may increase the risk (Crosby,
Alex; Beth & Han 2011).
Suicide is the act of taking one's
own life (Uddin; Burton; Maple; Khan;
Khan, 2019). Suicide is different from
attempted suicide or non-fatal suicidal
behavior which is self-injury with at least
some desire to end one's life that does not
result in death (Turecki& Brent, 2016).
Assisted suicide is when one individual
helps another bring about their own death
indirectly via providing either advice or
the means to the end. This is in contrast to
euthanasia, where another person takes a
more active role in bringing about a
person's death (Lester & David, 2009).
Suicidal ideation is thoughts of ending
one's life but not taking any active efforts
to do so.It may or may not involve exact
planning or intent (Lester & David, 2009).
Those who have previously
attempted suicide may be at a higher risk
for future attempts (Ajdacic-Gross, Weiss,
Ring, Hepp, Bopp, Gutzwiller&Rössler,
2008).The most commonly used method
of suicide is partly related to the
availability of effective means. Common
methods of suicide include hanging,
pesticide poisoning, and firearms (Nock,
Borges, Bromet, Alonso &Angermeyer,
2008). For a successful therapeutic
sessions with youths, Clinicians must
understand that a number of factors may
increase the risk of suicide among youths.
These factors include among others
personality traits and substance use and
abuse.

International Journal for Psychotherapy in Africa (5:1)
72
Suicidal ideation may depend on the
individual personality traits. This
difference is as a result of individual
unique characteristic. The Big Five
personality traits also known as the five-
factor model (FFM) and the OCEAN
model, is taxonomy for personality traits.
It is the unique characteristic that
differentiates people. The OCEAN is an
acrimony for; openness, consciousness,
Extraversion, Agreeableness and
Neuroticism.
Individuals with openness
experience are generally very active, have
a tremendous inclination towards
creativity and aesthetics and listen to their
heart i.e. follow their inner feelings. Such
individuals are generally open to new
learning, skill sets and experiences.
(Poropat, 2009).The Conscientiousness
personality trait listens to their conscience
and act accordingly. Such individuals are
extremely cautious and self disciplined.
They never perform any task in haste but
think twice before acting. (Marshall &
Georgiades, 2005).
Extraversion refers to a state where
individuals show more concern towards
what is happening outside. Such
individuals love interacting with people
around and are generally talkative. They
do not like spending time alone but love
being the centre of attraction of parties and
social gatherings. Such individuals love
going out, partying, meeting people and
often get bored when they are all by
themselves (Ambridge, 2014).
Agreeableness is a personality trait which
teaches individuals to be adjusting in
almost all situations. Such individuals do
not crib and face changes with a smile.
They accommodate themselves to all
situations and are friendly and kind
hearted. People (Marshall & Georgiades,
2005). Neuroticism is a trait where
individuals are prone to negative thoughts
such as anxiety, anger, envy, guilt and so
on. Such individuals are often in a state of
depression and do not how to enjoy life.
Substance misuse may also be a risk
factor for suicide. The use of psychoactive
substances constitutes one of most
important public health problems among
youth worldwide (Oshodi, Aina&Onajole,
2010). Recent studies in African countries
have shown that the phenomenon of drug
use is also common in the continent and is
becoming one of the most disturbing
health-related problems among youths
(Olawole-saac, Ogundipe, Amoo &
Adeloye, 2015) needing a quick
intervention of clinicians and other health
workers for psychotherapy.
Psychotherapy is the use of
psychological methods to help an
individual change his or her behavior in
order to overcome problems in a desired
way. In order to have successful
therapeutic sessions with clients and
restore their well being and mental health,
therapists must understand client’s
personality profile, the use and misuse of
psychoactive drugs among other things.
Statement of the Problem Suicidal ideation can lead to suicide itself.
Experiencing the suicide of a relative can
have a significant impact on family
members' emotional health. Youths’
suicide may have negative implication on
physical health of family members. People
bereaved by suicide may be at increased
risk of negative physical outcomes,
including hypertension, diabetes and
pancreatic cancer. This avoidance of grief-
related emotions may prevent relatives
from engaging in meaningful life task
whereby they assimilate the death of their
Takyun, C.J.; Okwoli, M.J. & Abubakar, M. (2020). Personality Trait, Drug use and Abuse as
Predictors of Suicidal Intention Among Youths: A Focus for Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):70-83
73
loved one into their new reality making
recovery difficult. There is need therefore
for a therapist to have in-depth
understanding of other predisposing
factors to suicide such as personality traits
and substance use and abuse. Therefore
this study intends to fill this gap in
literature.
Aim and Objectives of the Study
The aim of this study is to determine the
role of personality traits and substance use
and abuse as predictors of suicidal
ideation among youths in Makurdi
Metropolis. The specific objectives of the
study are to; i. Investigate the relationship between
personality traits and suicidal
ideation among youths in Makurdi
Metropolis.
ii. Investigate the relationship between
substance use and abuse and
suicidal ideation among youths in
Makurdi Metropolis.
iii. Investigate the joint influence of
personality traits and substance use
and abuse on suicidal ideation
among youths in Makurdi
Metropolis.
iv. Make recommendations for
effective treatment of suicidal
ideation among youth.
Research Questions
The following research questions were
raised to guide the study:
i. What is the relationship between
personality traits and suicidal
ideation among youths in Makurdi
Metropolis?
ii. What is the relationship between
substance use and abuse and
suicidal ideation among youths in
Makurdi Metropolis?
iii. To what extend will personality
traits and substance use and abuse
jointly predict suicidal ideation
among youths in Makurdi
Metropolis?
Conceptual Review
Personality Traits Gordon (1937) described two major ways
to study personality: the nomothetic and
the idiographic. Nomothetic psychology
seeks general laws that can be applied to
many different people, such as the
principle of self-actualization or the trait
of extraversion. Idiographic psychology is
an attempt to understand the unique
aspects of a particular individual.
Psychoactive Drugs
Bronstein, Spyker, Cantilena, Green,
Rumack and Dart (2010) defines “misuse”
as a use of the substance that does not
follow medical indications or prescribed
dosing which bears similarity to certain
abuse definitions. In some, although not
all definitions, misuse is specifically
restricted to prescription or over-the-
counter medications. Two definitions
propose that misuse occurs only when a
drug is taken with a therapeutic intent (ie,
the use does not involve seeking
psychotropic or euphoric effects) in a
manner other than as prescribed.
National Center on Addiction and
Substance Abuse at Columbia University
(2012) defines drug abuse as an
Intentional improper or incorrect use of a

International Journal for Psychotherapy in Africa (5:1)
74
substance where the victim was likely
attempting to achieve a euphoric or
psychotropic effect. All recreational use of
substances for any reason is included. It
also means the use of drug to get high; use
in combination with other drugs to get
high; use as a substitute for other drugs of
abuse.
Suicide
Vocabulary.com (2019) views the word
suicide to have breaks down into the Latin
words sui and caedere, which together
translate to “kill oneself.” However, not
all suicides are about the final end of life.
For example, a righteous politician can
commit political suicide by speaking
publicly about an unpopular topic. We call
a person who has killed himself a suicide,
and a police report might tell how many
suicides happen in a city each year.
Theoretical Review
Interpersonal Theory of Suicide
The interpersonal theory of suicide
attempts to explain why individuals
engage in suicidal behaviour and to
identify individuals who are at risk. It was
developed by Joiner (2005) and focuses
on why people commit suicide. The theory
consists of three components that together
lead to suicide attempts. According to this
theory, the simultaneous presence of
thwarted belongingness and perceived
burdensomeness produce suicidal ideation.
While the desire for suicide is necessary, it
alone cannot result to suicide. Rather,
Joiner (2005) asserts that one must also
have acquired capability (that is, the
acquired ability to overcome one's natural
fear of death). They must have wiped
away all possible fear and consequences
of death.
Belongingness which is the feeling
of acceptance is believed to be a
fundamental need, something that is
essential for an individual's psychological
health and well-being. Increased social
connectedness is a construct related to
belongingness that has been shown to
lower risk for suicide. More specifically,
being married, having children, and
having more friends are associated with a
lower risk of suicidal behavior (Joiner,
Hollar& Van Orden, 2007). Additionally,
working together with others has been
shown to have a preventive effect (Joiner,
Hollar& Van Orden, 2007. According to
this theory, personality traits may also
contribute to this phenomenal. This is
because some of the personality traits like
introversion that prefers to be only
concerned with their own life and nothing
else. Such individuals do not bother about
others and are seldom interested in what is
happening around. They prefer staying
back at home rather than going out and
spending time with friends. Such
individuals speak less and enjoy their own
company. Such person would never be
fine in meetings, clubs, parties or social
get-togethers. They generally do not have
many friends and tend to rely on few
trusted ones (Marshall & Georgiades,
2005).
Interpersonal theory of suicide also
tries to explain the importance of
perceived burdensomeness. Perceived
burdensomeness is the belief that one is a
burden on others or society. Joiner (2005)
describes perceived burdensomeness as
the belief that "my death is worth more
than my life". Unemployment, medical or
health problems and incarceration are
examples of situations in which a person
may feel like they are a burden to others
(Joiner, 2005). It is important to note that

Takyun, C.J.; Okwoli, M.J. & Abubakar, M. (2020). Personality Trait, Drug use and Abuse as
Predictors of Suicidal Intention Among Youths: A Focus for Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):70-83
75
the burdensomeness is "perceived", and is
often a false belief. According to the
theory, thwarted belongingness and
perceived burdensomeness together
constitute the desire for suicide.
Sometimes, these people may decide to
use drugs as the way out of their problems,
which may in turn open ways of taking
their own lives since they will feel little
fear about death due to drugs influence.
Interpersonal theory of suicide tries to
explain the importance of acquired
capability in suicidal ideation. Joiner
(2005) terms this "acquired" capability
because it is not an ability with which
humans are born with. Rather, this ability
to engage in suicidal behaviors is only
acquired through life experiences. Fear of
death is a natural and powerful instinct.
According to the theory, one's fear of
death is weakened when one is exposed to
physical pain or provocative life
experiences as these experiences often
lead to fearlessness and pain insensitivity.
These experiences could include
childhood trauma, witnessing a traumatic
event, suffering from a severe illness, or
engaging in self-harm behaviors such as
drugs.
These behaviors are thought to result
in the desensitization to painful stimuli
and to increase one's ability to engage in
suicidal behaviors. This component is
important in identifying individuals who
are likely to attempt or die by suicide. For
example, youths are exposed to physical
pain or provocative experiences in the
process of making it in life. More
specifically, youths with a history of
unemployment have likely been exposed
to grave poverty, witnessing the death of
others trying to make it in life, and are
habituated to fear of painful experiences
(Joiner, 2010). This is consistent with data
indicating an increased rate of suicide in
youths.
Empirical Review
Personality Traits and Suicidal Ideation
Marc, Alessandra, Alessandra and Kerstin
(2018) investigated the function of
personality traits on suicidal ideation. The
Interpersonal-Psychological Theory of
Suicide (IPTS) has been increasingly
studied over the last years, responding to
the demand for a valid framework
addressing suicide. Yet, only a few studies
have explored the function of personality
in the IPTS and none with clinical
patients. They aimed to contribute to fill
this gap in investigating the relationship
between personality as conceptualized by
the Five-Factor Model, the IPTS
constructs, and a dimensional measure of
current suicidal ideation correlation,
multiple linear regression, and path
analyses based on a trait-interpersonal
framework in a sample of 201 individuals
visiting the psychiatric emergency room of
a general hospital with current suicidal
ideation. Neuroticism (positively) and
openness (negatively) predicted perceived
burdensomeness, while neuroticism
(positively) and extraversion (negatively)
predicted thwarted belongingness. Higher
conscientiousness and lower extraversion
were both predictors of the acquired
capability for suicide. However, none of
the models involving path analyses with
IPTS variables as mediators of the
relationship between personality traits and
suicidal ideation was adequately adjusted
to the data. Thus, it appears that
personality plays a significant albeit
modest role in suicide when considered
from an IPTS perspective. As personality
is frequently assessed in the clinical

International Journal for Psychotherapy in Africa (5:1)
76
routine, health professionals should
consider it as complementary to detect
individuals at risk of or presenting suicidal
ideation.
Substance Use and Abuse and Suicidal
Ideation
Pompili, Serafini, Innamorati (2010)
conducted research on substance use and
suicide and concluded that substance use
independently increases the risk of
suicidal behavior. According to their
result, acute and chronic drug abuse
impairs judgment, weaken impulse
control, and interrupt neurotransmitter
pathways, leading to suicidal tendencies
through disinhibition. Additionally,
physiological and metabolic stress
resulting from drug abuse can lead to
neurotoxic damage and other severe
medical complications.
Bohnert, Ilgen and Louzon (2017)
conducted a research and concluded that
almost all substance use disorders are
associated with an increase in suicide risk.
Their result shows that the suicide hazard
ratio is 1.35 for cocaine use, 2.10 for
psychostimulant use, 3.83 for
benzodiazepine use, 3.89 for cannabis use,
and 11.36 for sedative use. Additionally,
marijuana use, cocaine use, alcohol use
and cigarette smoking were all found to be
independently related to suicide, even
after controls for socio-demographic
factors. Tobacco use and smoking appear
to contribute to deaths by suicide. Current
smokers are at the highest risk of suicidal
ideation, plans, and attempts, followed by
past smokers, with nonsmokers carrying
the lowest risk. Genetic vulnerabilities in
the serotonergic system may predispose a
smoker to suicide, although the exact
mechanisms have yet to be elucidated.
Hypotheses i. Personality traits will significantly
predict suicidal ideation among
youths in Makurdi Metropolis.
ii. Substance use and abuse will
significantly predict suicidal
ideation among youths in Makurdi
Metropolis.
iii. Personality traits and substance will
significantly and jointly predict
suicidal ideation among youths in
Makurdi Metropolis
METHOD
Design
Survey design was used for the study. This
design enabled the researcher to find the
relationship between personality traits and
suicidal ideation and psychoactive drugs
used and suicidal ideation among youths
in Makurdi metropolis in Benue state. This
is a survey study that tried to seek the
opinion of youths with the use of
questionnaires on suicidal ideation.
Participants
The populations for this study were
strictly youths in Makurdi Metropolis in
Benue State. The study involved 300
youths, 142 male which is 71 % and
female 57 which is 29 % randomly
selected to participate in the study. The
participants were asked to fill their bio-
data and to respond to the option that best
fit them.
Instruments
Three set of instruments were used for the
study. The instruments are (1) personality
traits (lBS) Scale, (2) Alcohol, Smoking

Takyun, C.J.; Okwoli, M.J. & Abubakar, M. (2020). Personality Trait, Drug use and Abuse as
Predictors of Suicidal Intention Among Youths: A Focus for Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):70-83
77
and Substance Involvement Scale
(ASSIST) and (3) suicidal ideation scale.
The Big five inventory: the big five
inventory (BFI) by John and Srivastava
(1999) is a 44-iteminstrument that assesses
the big five personality factors
(neuroticism, extraversion, openness,
agreeableness, and conscientiousness).
Items are scored using a 5- point, Likert
scale that ranges from disagree strongly to
agree strongly. BFI scales include 8–10
items each, and have demonstrated
moderate to high internal consistency
reliability (alpha range = .79 to .88;
median = .82) as well as substantial
convergent/ discriminant relations with
other big five instruments,
Alcohol, Smoking and Substance
Involvement Scale (ASSIST) is a
standardize scale that measure drug
involvement and the rate of use. The
strong overall results in the reliability and
validity studies suggest that the ASSIST is
a valid screening test for international use.
ASSIST is score ranging from Never=0
Once Twice=2, Monthly= 3, Weekly=4,
Daily=6 or Almost Daily=7
Suicide ideation was assessed with
the Geriatric Suicide Ideation Scale
(GSIS), a 31-item measure of suicide
ideation designed for use with older
adults. This multidimensional measure
assesses Suicide Ideation (e.g., “I want to
end my life”), Death Ideation (e.g., “I long
for the peaceful slumber of death”), Loss
of Personal and Social Worth (e.g., “I
generally feel pretty worthless”), and
Perceived Meaning in Life (e.g., “I feel
that my life is meaningful”; reverse-
scored). GSIS items are rated on a 5-point
Likert format scale (1 = strongly disagree,
5 = strongly agree) and yield total scores
ranging from 31 to 155, with higher scores
indicating greater intensity of suicide
ideation. Acceptable internal consistency
has been demonstrated for GSIS total
scores (Cronbach’s α = 0.90) and the four
subscales (Cronbach’s α = 0.74 – 0.86).59
In the present study, Cronbach’s α = .91
and .94 for GSIS total scores at time 3 and
4, respectively.
Procedures
The procedure for the study involved
moving from street to street engaging the
youths. The participants were asked to fill
the bio-data and to respond to the option
that best fit them. 320 questionnaires were
distributed. It was only the 300
questionnaires that were filled completely
that were used for the study. The
researcher waited and collected the
questionnaires after they were filled. Some
of the illiterate participants that may find it
difficult to read were assisted by the
researcher and assistant that helped to read
and interpret for the illiterate participants.
Method of Data Analysis The statistical methods for this study were
Simple and Multiple Regressions
Analysis. The simple regression tested the
relationship between personality traits and
suicidal ideation, psychoactive drug used
abuse on suicidal ideation. Multiple
regression was used to determine a
statistically significance joint relationship
as well as personality traits and
psychoactive drug use and abuse on
suicidal ideation.
RESULTS
Hypotheses Testing
Hypotheses 1
This hypothesis states that personality
traits will significantly predict suicide
ideations among adolescents.

International Journal for Psychotherapy in Africa (5:1)
78
This hypothesis was tested using Multiple
Regression Analysis and the results are
tabulated and interpreted as shown below.
Table 1: Multiple Regression
Analysis showing the
influence of Personality
on Suicide Ideation
among Adolescents Variables R R2 F ß t p
Constant .770 .593 96.551
.022
.178
.369
-.079
.325
2.727
0.591
2.260
4.558
0.876
3.270
.007
.555
.024
.000
.382
.001
Agreeableness
Conscientiousness
Openness to Exp.
Extroversion
Neuroticism
Dependent Variable: Suicide Ideation
The results presented in Table 1 showed
that personality traits have significantly
and jointly predicted suicide ideations
among adolescents (R = .591 = R2 = .593
(F (5, 331) = 96.551, t = 2.720, p< .05).
This means that all the five dimensions of
personality traits had jointly contributed to
59.3% changes observed in the level of
suicide ideations among adolescents. In
considering the individual personality
traits, the results clearly showed that
agreeableness has no significant influence
on suicide ideations (ß = .022, p>.05),
when the variance explained by the other
four factors are controlled. This means
that adolescents who are predominantly
agreeable are less likely to contemplate
suicide. This implies that adolescents who
are dominant on agreeableness have only
2.2% chances for suicide ideation. Thus,
they are insulated from suicide ideations.
On the contrary, conscientiousness has
significantly made the unique positive
contribution to suicide ideations (ß = .178,
p<.05). This means that adolescents who
are dominant on conscientiousness have
17.8% chances of contemplating suicide.
Similarly, openness to experience has a
significant positive influence on suicide
ideations (ß = -.369, p<.05). This means
that adolescents who are predominant on
openness to experience are highly (36.9%)
preoccupied with suicide ideations.
Furthermore, neuroticism has a significant
positive influence on suicide ideations (ß
= .325, p<.05). This means that
adolescents who are predominant on
neurotic personality trait are highly
(32.5%) preoccupied with suicide
ideations. Lastly, the results showed that
extroversion has no significant influence
on suicide ideations (ß = -.079, p>.05),
when the variance explained by the other
four factors are controlled. This means
that adolescents who are extroverts are
7.9% less likely to contemplate suicide.
Therefore, the hypothesis that personality
traits will significantly predict suicide
ideations among adolescents has been
confirmed for conscientiousness, openness
to experience and neuroticism but not for
agreeableness and extroversion.
Hypotheses II
This hypothesis states that drug use/abuse
will significantly predict suicide ideations
among adolescents.
This hypothesis was tested using Simple
Regression Analysis and the results are
tabulated and interpreted as shown below.
Table 2: Regression analysis showing
the influence of drug use/abuse on
suicide ideations Variables R R2 F ß t Sig
Constant .756 .571 99.746
.756
3.512
21.160
.001
.000 Drug
Use/Abuse
Criterion variable: Suicide Ideations
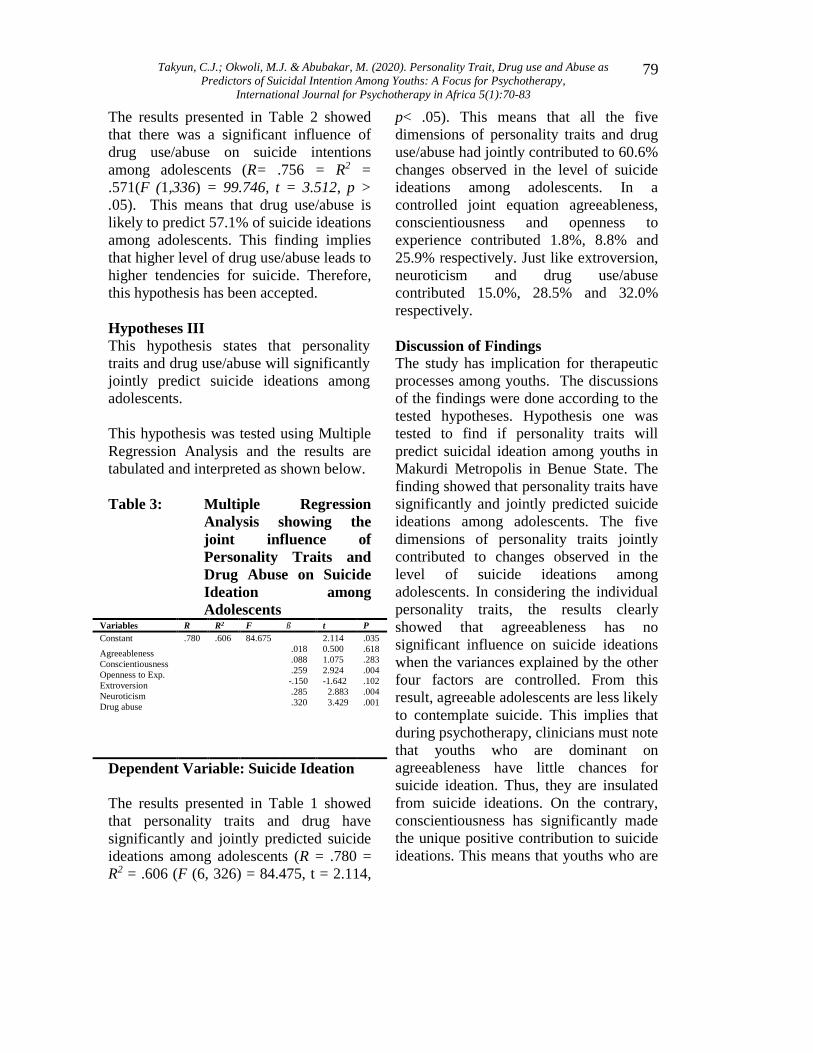
Takyun, C.J.; Okwoli, M.J. & Abubakar, M. (2020). Personality Trait, Drug use and Abuse as
Predictors of Suicidal Intention Among Youths: A Focus for Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):70-83
79
The results presented in Table 2 showed
that there was a significant influence of
drug use/abuse on suicide intentions
among adolescents (R= .756 = R2 =
.571(F (1,336) = 99.746, t = 3.512, p >
.05). This means that drug use/abuse is
likely to predict 57.1% of suicide ideations
among adolescents. This finding implies
that higher level of drug use/abuse leads to
higher tendencies for suicide. Therefore,
this hypothesis has been accepted.
Hypotheses III
This hypothesis states that personality
traits and drug use/abuse will significantly
jointly predict suicide ideations among
adolescents.
This hypothesis was tested using Multiple
Regression Analysis and the results are
tabulated and interpreted as shown below.
Table 3: Multiple Regression
Analysis showing the
joint influence of
Personality Traits and
Drug Abuse on Suicide
Ideation among
Adolescents Variables R R2 F ß t P
Constant .780 .606 84.675
.018
.088
.259
-.150
.285
.320
2.114
0.500
1.075
2.924
-1.642
2.883
3.429
.035
.618
.283
.004
.102
.004
.001
Agreeableness
Conscientiousness
Openness to Exp.
Extroversion
Neuroticism
Drug abuse
Dependent Variable: Suicide Ideation
The results presented in Table 1 showed
that personality traits and drug have
significantly and jointly predicted suicide
ideations among adolescents (R = .780 =
R2 = .606 (F (6, 326) = 84.475, t = 2.114,
p< .05). This means that all the five
dimensions of personality traits and drug
use/abuse had jointly contributed to 60.6%
changes observed in the level of suicide
ideations among adolescents. In a
controlled joint equation agreeableness,
conscientiousness and openness to
experience contributed 1.8%, 8.8% and
25.9% respectively. Just like extroversion,
neuroticism and drug use/abuse
contributed 15.0%, 28.5% and 32.0%
respectively.
Discussion of Findings
The study has implication for therapeutic
processes among youths. The discussions
of the findings were done according to the
tested hypotheses. Hypothesis one was
tested to find if personality traits will
predict suicidal ideation among youths in
Makurdi Metropolis in Benue State. The
finding showed that personality traits have
significantly and jointly predicted suicide
ideations among adolescents. The five
dimensions of personality traits jointly
contributed to changes observed in the
level of suicide ideations among
adolescents. In considering the individual
personality traits, the results clearly
showed that agreeableness has no
significant influence on suicide ideations
when the variances explained by the other
four factors are controlled. From this
result, agreeable adolescents are less likely
to contemplate suicide. This implies that
during psychotherapy, clinicians must note
that youths who are dominant on
agreeableness have little chances for
suicide ideation. Thus, they are insulated
from suicide ideations. On the contrary,
conscientiousness has significantly made
the unique positive contribution to suicide
ideations. This means that youths who are

International Journal for Psychotherapy in Africa (5:1)
80
dominant on conscientiousness have
higher chances of contemplating suicide.
Similarly, openness has a significant
positive influence on suicide ideations.
This means that youths who are
predominant on openness are highly
preoccupied with suicide ideations.
Furthermore, neuroticism has a significant
positive influence on suicide ideations.
The youths that are predominant on
neurotic personality trait are highly
preoccupied with suicide ideations. Lastly,
the results showed that extroversion has
no significant influence on suicide
ideations when the variances explained by
the other four factors are controlled. That
is to say that, youths that are extroverts are
less likely to contemplate suicide.
Therefore, the hypothesis that stated that
personality traits will significantly predict
suicide ideations among adolescents has
been confirmed for conscientiousness,
openness to experience and neuroticism
but not for agreeableness and
extroversion.
These findings are in line with those
of Winnie, Jan, Adrian, Thomas and Peter
(2018) that assessed associations between
suicide ideation and personality
characteristics in a sample of community-
residing adults 65 years of age and older.
Within the sample of older adults, more
severe suicide ideations was significantly
associated with lower Extraversion and
greater Neuroticism and Socially
Prescribed Perfectionism, controlling for
age, sex, and depression symptom
severity. Although findings concerning
Neuroticism were not consistent across
measures, Extraversion and Socially
Prescribed Perfectionism appear to have
particularly robust associations with
suicide ideation.
Hypothesis two stated that drug use/abuse
will significantly predict suicidal ideation.
The result showed that there was a
significant influence of drug use/abuse on
suicide intentions among adolescents.
This means that drug use and abuse is a
strong predictor of suicide ideations
among adolescents. This finding implies
that higher level of drug use/abuse among
youths leads to higher tendencies for
suicide. Therefore, this hypothesis has
been accepted.
This finding is also in line with a
survey conducted by the Substance Abuse
and Mental Health Services
Administration in (2015) which showed
those 9.8 million people ≥18 years old
seriously considered suicide in the past 12
months, with 1.4 million making nonfatal
suicide attempts. Young adults aged 18–
25 were also more likely to have serious
thoughts of suicide or suicide attempts due
to drug abuse.
This finding is also in line with Wilcox,
Conner and Caine, et al. (2004) conducted
research on substance abuse and suicide
and concluded that the rates increased to
72.2% for synthetic opioids and were
20.6% for heroin. A meta-analysis the
researchers showed that heroin use
increased the risk of suicide by 13.5 times
compared with the 10-fold increase with
alcohol use disorder. Another study
investigating the association between
prescription opioid use and suicide among
patients with chronic non-cancer pain
revealed that an increased opioid dose was
related to an increased risk of suicide,
even after controlling for demographic and
clinical factors.
The hypothesis three states that
personality traits and drug abuse will
significantly and jointly predict suicidal
ideation among youths in Makurdi
Takyun, C.J.; Okwoli, M.J. & Abubakar, M. (2020). Personality Trait, Drug use and Abuse as
Predictors of Suicidal Intention Among Youths: A Focus for Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):70-83
81
metropolis. The result showed that
personality traits and drug have
significantly and jointly predicted suicide
ideations among youths. This means that
all the five dimensions of personality traits
and drug use/abuse had jointly contributed
to changes observed in the level of suicide
ideations among adolescents. In a
controlled joint equation agreeableness,
conscientiousness and openness to
contributed to suicidal ideation
respectively. Just like extroversion,
neuroticism and drug use/abuse
contributed also contributed respectively.
Conclusion/Recommendations
In a bid to conclude that personality traits
and drug use/abuse as predictors of
suicidal ideation among youths in Makurdi
metropolis in Benue State, theories were
reviewed, data were collected and the
hypotheses were tested. Based on the
result, it was concluded that:
i. Personality traits predicted suicidal
ideation among youths in Makurdi
metropolis in Benue State. ii. Drug use/abuse predicted suicidal
ideation among youths in Makurdi
mertopolis in Benue State.
iii. There is an interactive influence of
personality traits and drug use/abuse
on suicidal ideation among
adolescents in Makurdi metopolis in
Benue State.
We therefore recommend that: i. Communication skills, listening
exercises, emotional expression,
and conflict resolution are also
important parts of treatment which
therapists must not neglect during
the psychotherapeutic sessions
i. Therapists should encouraged
patients through creating of rapport
to communicate their feelings, their
fears and desires during therapy.
ii. Therapist should help patients to
examine and change any beliefs
about suicide. Some of these
mistaken beliefs are widely shared
in the society and can result from
past traumatic events, family
attitudes, or cultural ideas.
iii. Government should discourage the
use of drugs in the society if there is
a true need to control the high level
of suicide in the country.
iv. Parents and care givers should
educate, monitor their children cum
wards to know their mood and
recommend psychotherapy, as this
can help in suicide prevention
among youths
Limitations of the Study
Having contributed immensely to
knowledge; however, the study is limited
in some aspects:
Youths demonstrated some level of fear
and shame when filling the questionnaires
since it involves their private life. They
felt that the information given might be
used in discussing them. So the researcher
could not guarantee the degree of their
responses.
The study was only limited to two
independent variables; personality traits
and drug use and abuse. The study was
only limited to adolescents in the study
area.
International Journal for Psychotherapy in Africa (5:1)
82
The study was limited to specific
population group which is Markudi
Metropolis.
References
Ajdacic-Gross. V, Weiss. M.G, Ring. M,
Hepp. U, Bopp. M, Gutzwiller. F,
&Rössler. W (2008)."Methods of
suicide: international suicide
patterns derived from the WHO
mortality database" Bulletin of the
World Health Organization. 86 (9):
726–32.
Bohnert KM, Ilgen MA, Louzon S, et al.
(2017): Substance use disorders and
the risk of suicide mortality among
men and women in the US Veterans
Health Administration. Addiction;
112:1193–1201
Crosby, Alex; Beth, Han (2011)."Suicidal
Thoughts and Behaviors Among
Adults Aged ≥18 Years --- United
States, 2008-2009" Morbidity and
Mortality Weekly Report (MMWR).
60 (13). 3.
Joiner, Jr., T.E., Hollar, D., & Van Orden,
K.A. (2007). "On Buckeyes, Gators,
Super Bowl Sunday, and the Miracle
on Ice: 'Pulling together' is
associated with lower suicide rates".
Journal of Social and Clinical
Psychology, 25, 180–196.
Joiner, T. E. (2005).Why People Die By
Suicide. Cambridge, MA: Harvard
University Press
Joiner, T. E. (2010)."Overcoming the fear
of lethal injury: Evaluating suicidal
behavior in the military through the
lens of the interpersonal–
psychological theory of suicide".
Clinical Psychology Review. 30(3),
298-307.
Lester, David (2009). "Extended suicide".
In Wasserman, Danuta; Wasserman,
Camilla (eds.). Oxford textbook of
suicidology. Oxford: Oxford
University Press. pp. 134–36
Marc B, Alessandra C, Alessandra C,
&Kerstin W, (2018).The Function of
Personality in Suicidal Ideation from
the Perspective of the Interpersonal-
Psychological Theory of Suicide.
International Journal of
Environmental Research in Public
Health; 15(4): 636.
National Center on Addiction and
Substance Abuse at Columbia
University (2012). Substance Use
and Abuse; Columbia University.
Patton. G.C, Sawyer.S.M, Santelli. J.S,
Ross. D.A, Afifi. R, Allen. N.B, et
al. (2016) .Our future: a Lancet
commission on adolescent health
and wellbeing. Lancet, 387:2423–
78.
Olawole-Isaac, O Ogundipe, E O Amoo,
D Adeloye (2018). Substance use
among adolescents in sub-Saharan
Africa: A systematic review and
meta-analysis. South African
Journal of Child Health;12(2b): 79-
83.
Pompili. M, Serafini. G, Innamorati. M, et
al. (2010): Suicidal behavior and
alcohol abuse. International Journal
of Environ Res Public Health;
7:1392–1431
Routledge; (2013).Orbach I. Suicide
prevention for adolescents. In: King
R, Apter A, editors. editors. Suicide
in Children and Adolescents.
Cambridge: Cambridge University
Press; (2006), pp.1–40.
Shneidman, E. S. (1985). Definition of
suicide. New York, NY: Wiley.
Shneidman, E. S. (1993). Suicide as
psychache: A clinical approach to
Takyun, C.J.; Okwoli, M.J. & Abubakar, M. (2020). Personality Trait, Drug use and Abuse as
Predictors of Suicidal Intention Among Youths: A Focus for Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):70-83
83
self-destructive behavior. Northfield,
NJ: Jason Aronson.
Stedman's Medical Dictionary (28th ed.)
MaryLand: Lippincott Williams &
Wilkins (LWW).
Turecki. G, Brent DA (March
2016).Suicide and suicidal
behaviour. Lancet.387 (10024):
1227–39.
Winnie. S. C, Jan. S, Adrian. L, Thomas.
M & Peter. A, (2018).The
Relationship between Personality
Traits with Depressive Symptoms
and Suicidal Ideation among
Medical Students: A Cross-Sectional
Study at One Medical School in
Germany; International Journal of
Environment Research in Public
Health.; 15(7): 1462
Allport, G. W. (1937). Personality: A
psychological interpretation. New
York: Holt.

International Journal for Psychotherapy in Africa (5:1)
84
Posttraumatic Stress Disorder Among Trafficked
Victims, Role Of Self-Esteem, Demographic Factors
And Relevance Of Psychotherapy
Ezeakor Adolphus I.
Psychology Department,
Chukwuemeka Odumegwu Ojukwu University, Igbariam
Okpala Michael O.
Psychology Department,
Nnamdi Azikiwe University, Awka
Abstract Objective: Experiences of traumatic exposure of trafficked victims keep tormenting them
after they are rescued. Trafficked victims at rehabilitation centers of National Agency for
Prohibition of Trafficking in Persons and Other Related Matters (NAPTIP) at Southern
Zones have been found to present with posttraumatic stress disorder. This finding made it
necessary that improving their mental health should include efforts to identify factors
likely to predispose, maintain, or perpetuate PTSD presentation among trafficked
victims. Current study thereby examined posttraumatic stress disorder among trafficked
victims: the role of self-esteem and demographic factors. Method: 55 participants
selected through total population sampling technique from the rehabilitation centers of
NAPTIP in their South-East, South-South, and South-West zonal offices, participated.
Their age ranged between 14 to 25 years, with a mean age of 19.89 and a standard
deviation of 2.87. The instruments administered on them were Posttraumatic Stress
Disorder Keane Scale (PKS) (Keane, Malloy & Fairbanks, 1984) and Index of Self –
Esteem (ISE) (Hudson, 1982). Mental State Examination of some of the clients was also
done. The study used ex-post-facto design and Independent t-test was used to test the
hypotheses. Result: This revealed that hypotheses two to seven on demographic factors
were rejected. It also showed that only hypothesis one on self-esteem was accepted,
t(53)=-3.26, p <.05. Conclusion: The relevance of psychotherapy will establish the
linkage through trafficked victims at rehabilitation centers of NAPTIP in her zonal
offices in the southern parts of Nigeria, and determine self-esteem factor likely to
influence PTSD presentation.
Key words: Demographic Factors, Posttraumatic Stress Disorder, Self-esteem,
Trafficked Victims and Psychotherapy

Ezeakor, A.I & Okpala, M.O. (2020). Posttraumatic Stress Disorder among Trafficked Victims,
Role of Self-Esteem, Demographic Factors and Relevance of Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):84-97
85
Introduction Traumatic event is an unpleasant or
disturbing experience that causes physical,
emotional, psychological distress or harm
and is perceived and experienced as a
threat to one’s safety or to the stability of
one’s world (Medline Plus, 2004). World
Health Organization (WHO), International
Classification of Diseases, Tenth Edition
(ICD-10), (1992), defines traumatic
stressor as events or situations that are
exceptionally threatening or catastrophic
in nature, which are likely to cause
pervasive distress in almost anyone.
American Psychiatry association (APA),
Diagnostic and Statistical Manual of
Mental Disorders, Fifth Edition (DSM –
V) (2013), on the other hand, defines
traumatic stressors as events that involve
life endangerment, death, or serious injury
or threat and are accompanied by feelings
of intense fear, horror or helplessness.
Human trafficking or trafficking in
persons (TIP) is a traumatic event
(Carling, 2005) and experiences of
Nigerian trafficked victims could best be
referred to as traumatic. International
Organization for Migration (2001)
estimates that trafficking in human beings
is a huge billion industry worldwide.
Scholars (Sita, 2003; Morka, 2009) noted
that this trend has degenerated to a level to
warrant its description as becoming the
order of the day in Nigeria, being an
organized crime, which has lawyers,
herbalists, corrupt immigration and police
officers and relatives or friends “as
participants”. Certainly, as these
unscrupulous persons pursue their
business interest, they perpetuate the
traumatic exposure of the trafficked
victims. European Race Audit Bulletin
(1997) revealed that after being recruited,
the victims are conveyed through long and
tortuous land routes mainly through the
Sahara Desert to European counties. Once
they arrive the victims are forced to work
as sex hawkers (especially the girls). The
victims often undergo a process of
initiation or ritual, which involves
collection of underwear, pubic hair and
other personal items deemed fit by the
baronesses. This is aimed at instilling fear
in the victims in order to prevent them
from revealing anything that could lead to
the arrest of the baronesses. These ugly
exposures made victims to directly have
traumatic experiences, witness traumatic
events as they happen to other victims, or
leant of one that had happened to the
person they know. It is these negative
experiences that make them vulnerable to
posttraumatic stress disorder (PTSD).
According to ICD-10, traumatic
experiences are characterized as being
outside the range of usual human
experience and have been implicated in
the aetiology of certain specified
psychiatric disorders, like PTSD. PTSD is
the most common psychological disorder
following traumatic experiences (Caffo &
Belaise, 2003). Gelder, Harrison and
Cowen, (2006) noted that the clinical
features of PTSD can be divided into three
groups. The symptoms of the first group
are related to hyperarousal and include
persistent anxiety, irritability, insomnia,
and poor concentration. The second group
of symptoms centers on intrusion,
involving intense intrusive imagery of the
events, sudden flashback, and recurrent
distressing dreams. The third group of
symptoms is concerned with avoidance
and includes difficulty in recalling
stressful events at will, avoidance of
reminders to the events, a feeling of
detachment, inability to feel emotion
(‘numbing’), and diminished interest in
International Journal for Psychotherapy in Africa (5:1)
86
activities. Gelder et al., (2006) noted that
the most characteristic symptoms are
flashbacks, night mares, and intrusive
images, sometimes known collectively as
re-experiencing symptoms.
While not all trafficked victims die
as a result of terror unleashed on them in
the course of their trafficking, it is
perceived that the traumatic experiences
trafficked victims had could precipitate
PTSD. After some traumatic events,
survivors feel forced into a painful
reconsideration of their beliefs about the
meaning and purpose of life (Janoff-
Bulman, 1985). However, not all survivors
of traumatic events develop posttraumatic
stress reactions (Sadruddin, Walter &
Hidalgo, 2005). Certainly, some are more
susceptible. Self-esteem and demographic
factors may stand the chance to influence
the presentation of PTSD among
trafficked victims.
Self-esteem refers to a person’s
overall evaluation or appraisal of his or
her own worth. Baumeister (2008) defined
self-esteem as how favourably someone
evaluates himself or herself. Human
trafficking experiences can cause major
change in a victim’s life leading to grave
change in self-concept as the victim
experiences difficulty in adjusting to the
new image he/she has of himself/herself
(Carson & Arnold, 1996). This could
predispose trafficked victims to PTSD.
Similarly, a wide range of factors,
ranging from demographic characteristics
to personal psychological factors have
been associated with PTSD onset after
disasters. Gender (female) has consistently
been shown to be at risk factor for the
onset of PTSD after disasters (Grieger,
Fullerton & Ursano, 2003; Pulcino, Galea
& Alern, 2003). Moreso, Fitzpatrick and
Boldizar (1993) stated that whereas boys
were reported to experience more
traumatic events, girls have a higher rate
of PTSD.
Personal psychological factors such
as guilt and anger (Hull, Alexander &
Klein, 2002), external locus of control
(North, Spitznagel, & Smith, 2001),
weaker coping ability (Stewart, Mitchell
& Wright, 2004) and low social support
(Johnson, North & Smith, 2002), have
been associated with PTSD onset after
traumatic events. Accordingly, the general
objective of this study is to examine the
influence of self-esteem and demographic
factors on PTSD among trafficked
victims. It is from this general purpose
that the following specific purposes arose:
1. To know if there will be a
significant difference between
victims with low self-esteem and
victims with high self-esteem on
PTSD.
2. To know if there will be a
significant difference between minor
and adult victims of human
trafficking on PTSD.
3. To know if there will be a
significant difference between the
victims from monogamous family
setting and those from polygamous
family setting on PTSD.
4. To know if there will be a
significant difference between
victims who attended school and
those who do not on PTSD.
5. To know if there will be a
significant difference between
victims trafficked outside Nigeria
and those trafficked within Nigeria
on PTSD.
6. To know if there will be a
significant difference between
victims trafficked for sexual

Ezeakor, A.I & Okpala, M.O. (2020). Posttraumatic Stress Disorder among Trafficked Victims,
Role of Self-Esteem, Demographic Factors and Relevance of Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):84-97
87
exploitation and those trafficked for
non-sexual exploitation on PTSD.
Literature Review
Literature review for this article is carried
out under the following sub-headings: a)
Psychological theories of PTSD; b) Self-
esteem and PTSD; and c) Demographic
Factors and PTSD
a. Psychological Theories of PTSD
Learning theorists assume that PTSD
arises from a classical conditioning of fear
(Fairbank & Brown, 1987; Keane,
Zimerine, & Caddell, 1985). A trafficked
victim who has been raped may fear
walking in a certain place (conditioned
stimulus (CS) because of memories of
having been raped in a similar
environment (UCS). Based on this
classically conditioned fear, avoidance is
built up, and victims are negatively
reinforced by the reduction of fear that
comes from not being in the presence of
the CS. PTSD is a prime example of the
two-factor theory of avoidance learning,
proposed years ago by Mowrer (1947).
Psychodynamic theories emphasize
the role of emotional development in
determining individual variations in the
response to severely stressful events
(Gelder et al., 2006). A psychodynamic
theory proposed by Horowitz (1986,1990)
posits that memories of the traumatic
event occur constantly in the person’s
mind and are so painful that they are either
consciously suppressed (by distraction, for
example) or repressed. The person is
believed according to Davison and Neale
(2001) to engage in a kind of internal
struggle to integrate the trauma into his or
her existing beliefs about himself and the
world to make some sense out of it.
Cognitive theories suggest that
PTSD arises when the normal processing
of emotionally charged information is
overwhelmed, so that memories persist in
an unprocessed form in which they can
intrude into conscious awareness (Gelder
et al., 2006). In support of this idea,
patients with PTSD tend to have
incomplete and disorganized recall of the
traumatic events (Ehlers, Mayou, &
Bryant, 1998). Individual differences in
response to the same traumatic events are
explained as due to differences in the
appraisal of the trauma and of its effects
(Ehlers et al., 1998). Similarly, difference
in the appraisal of the early symptoms
may explain why these symptoms persist
longer in some people. Negative
interpretations of intrusive thoughts (for
example, “I am going mad”) after road
accidents predict the continuing presence
of PTSD after one year (Ehlers et al.,
1998).
In an international study of
trafficked prostituted children and adults,
including male prostitutes in five
countries, it was found that almost three-
fourths of the victims met the diagnostic
criteria for PTSD (Farley, Barel, Kiremire,
& Sezquin, 1998; Silbert & Pines, 1981).
Again, a multi-country report published in
2003 found that nearly 70% of women
trafficked for prostitution that was studied
met the criteria for PTSD (Farley &
Melissa, 2003). In a study of female
survivors of human trafficking in Nepal,
PSTD was found to be higher in sex
workers group (29.6%) than in the non-sex
workers group (7.5%) (Tsutsumi, Izutsu,
Poudyal, Kato, & Marui, 2008). Also, in
Israel, about 17% of trafficked women
(the majority of which were from
Moldevia, Ukraine, Russia, and Central
Asian Republics of Soviet Union), who

International Journal for Psychotherapy in Africa (5:1)
88
had worked as sex workers scored over the
cut-off point of measurement for PTSD
(Tsutsumi et al., 2008).
b. Self-esteem and PTSD
Self-discrepancy theory developed by
Higgins (1989) posits that self-
discrepancy serves to introduce
accessibility of the various ways people
construe the world. According to Higgins
(1989), one’s self-esteem is defined by the
match between how one sees oneself and
how one want to be seen by others, and he
argues that any likely discrepancy will
occur between these three dimensions of
self: one’s actual self, one’s ought self and
one’s ideal self. If the discrepancy is
between one’s actual self and ought
selves, he/she may feel guilty, ashamed
and resentful; if there is discrepancy
between one’s actual and ideal selves, one
will feel disappointed, frustrated, sad and
unfulfilled (Strauman, 1992).
According to Higgins (1989), one’s
self-esteem level based on these three
dimensions depends on a number of
factors, that included the amount of
discrepancy, the importance of the
discrepancy to the self and the extent to
which one focuses on one’s self
discrepancies. The most focused, the
greater the harm. From this perspective,
the major source of low self-esteem is the
guilt and shame that some victims feel
when they do not experience idealized
emotions that follow with returning home
with money made abroad through
prostitution and becoming role model to
the vulnerable ones in the society.
Study by Hershberger and D’Augelli
(1995) found self-esteem to be negatively
correlated with mental health variables
such as measure of psychiatric symptoms;
suicidal ideation and suicide attempts,
among victimized youths. Bradley,
Schwartz and Kaslow, (2005) reported a
finding showing that low self- esteem was
related to high mental health difficulties.
Salami (2010) reported that the
relationship between exposure to violence
and PTSD was moderated by resilience,
self-esteem and social support.
Consequently, self-esteem is suspected to
be a variable likely to influence PTSD
presentation among trafficked victims.
c. Demographic Factors and PTSD
Population of developing countries
appears to create favourable market for
victims to be trafficked. Such population
creates avenues for criminal activities like
human trafficking to be thriving, perhaps,
due to poverty. The study by Inocencio
(2011) carried out at the University of
Roehampton in London using quantitative
analyses of secondary data to identify risk
factors associated with trafficking hotspots
in Nigeria and Indonesia, used content
analysis to identify ‘hotspot’ areas for
human trafficking. The hotspot refers to
locations that were more developed, had
higher populations, and a record of more
crime. Such could engender clandestine
operation of trafficking business.
Good number of epidemiological
studies on gender and PTSD revealed that
PTSD is twice as common in women as in
men. According to Yehuda (2007), some
of these differences are clearly societal
and non-biologically based. Findings from
some studies suggest that whether
traumatic experience will lead to PTSD is
dependent on the type of trauma and the
gender involved. According to Spitzberg
(1999), rape in both men and women,
carries one of the highest risks for
producing PTSD that approximately 0.7%
of men in the United States reported being
Ezeakor, A.I & Okpala, M.O. (2020). Posttraumatic Stress Disorder among Trafficked Victims,
Role of Self-Esteem, Demographic Factors and Relevance of Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):84-97
89
raped as compared with 9.2% of women
who develop PTSD.
Hypotheses
1. There would be a significant
difference between victims with low
self-esteem and victims with high
self-esteem on PTSD.
2. There would be a significant
difference between minor and adult
victims of human trafficking on
PTSD.
3. There would be a significant
difference between victims from
monogamous family setting and
those from polygamous family
setting on PTSD.
4. There would be a significant
difference between victims who
attended school and those who do
not on PTSD.
5. There would be a significant
difference between victims
trafficked outside Nigeria and those
trafficked within Nigeria on PTSD.
6. There would be a significant
difference between victims
trafficked for sexual exploitation and
those trafficked for non-sexual
exploitation on PTSD.
Method
A sample of 55 participants selected
through total population sampling
technique, participated. They were
employed from the rehabilitation centers
of National Agency for Prohibition of
Trafficking in Persons and Other Related
Matters (NAPTIP) in their South-East,
South-South, and South-West zonal
offices. Their age ranged between 14 to 25
years, with a mean age of 19.89 and a
standard deviation of 2.87.
Instruments
Two standardized instruments used for
data collection were Posttraumatic Stress
Disorder Keane Scale (PKS) (Keane,
Malloy & Fairbanks, 1984) and Index of
Self-Esteem (ISE) (Hudson, 1982). The
demographic factors of the participants
were collected using the section for
demographic factors added to the
instruments by the researchers. The
instruments were pilot tested using
twenty-three (23) trafficked victims
elicited from these zones. A Cronbach co-
efficient alpha reliability method was used
to determine the reliability estimates for
the instruments and .90 and .88 were
obtained for PKS and ISE, respectively.
The trafficked victims involved in the
pilot test were however, not used in the
main study. Moreover, mental state
examination of each participant from
South-South zone (where access to victims
was granted) was undertaken to generate
qualitative data peculiar to trafficked
victims, the nature of which the
instruments used did not capture.
Procedure
A letter seeking for permission to embark
on this study was sent to each Zonal
Director of the three zones used. On
obtaining their oral approval through the
Head of Research Unit of the concerned
zones, different dates were chosen for the
administration of the instruments on the
participants. With the assistance of a
NAPTIP staff in Counseling and
Rehabilitation Unit in the zone, the
instruments were administered on the
participants. Importantly, only trafficked
victims who have been in the
rehabilitation center for a month and
above, can read and understand English
Language, and willing to participate
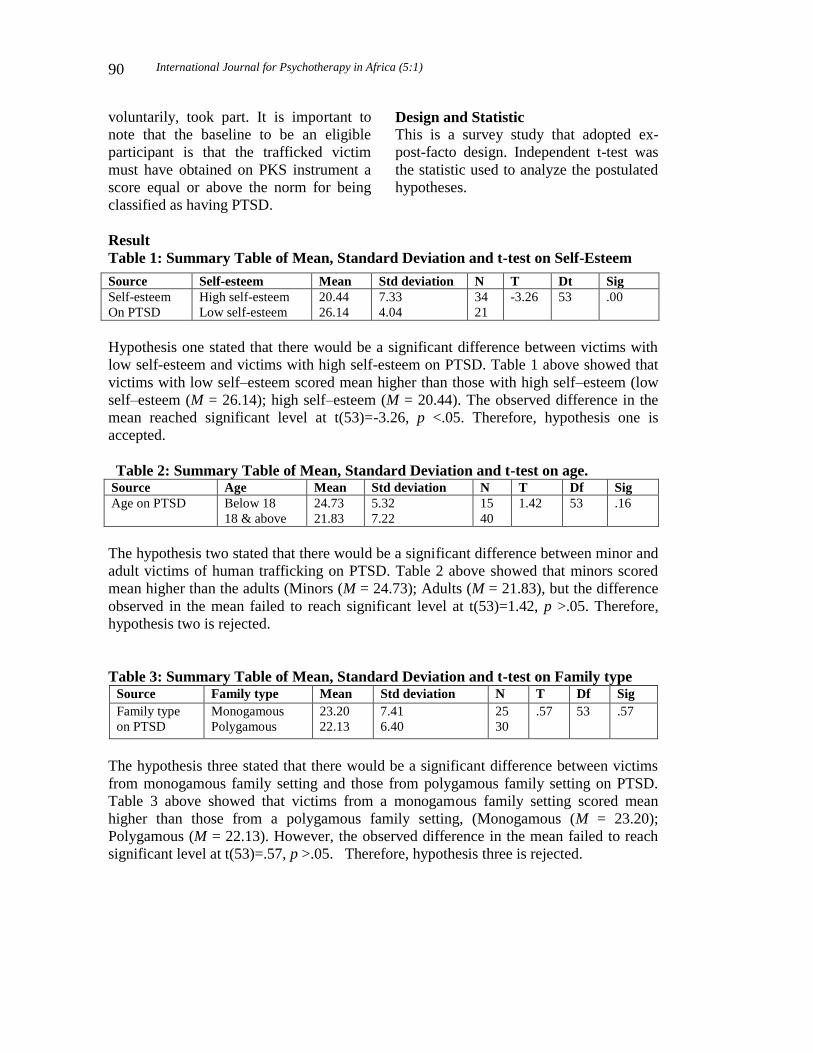
International Journal for Psychotherapy in Africa (5:1)
90
voluntarily, took part. It is important to
note that the baseline to be an eligible
participant is that the trafficked victim
must have obtained on PKS instrument a
score equal or above the norm for being
classified as having PTSD.
Design and Statistic
This is a survey study that adopted ex-
post-facto design. Independent t-test was
the statistic used to analyze the postulated
hypotheses.
Result
Table 1: Summary Table of Mean, Standard Deviation and t-test on Self-Esteem
Hypothesis one stated that there would be a significant difference between victims with
low self-esteem and victims with high self-esteem on PTSD. Table 1 above showed that
victims with low self–esteem scored mean higher than those with high self–esteem (low
self–esteem (M = 26.14); high self–esteem (M = 20.44). The observed difference in the
mean reached significant level at t(53)=-3.26, p <.05. Therefore, hypothesis one is
accepted.
Table 2: Summary Table of Mean, Standard Deviation and t-test on age. Source Age Mean Std deviation N T Df Sig
Age on PTSD Below 18
18 & above
24.73
21.83
5.32
7.22
15
40
1.42 53 .16
The hypothesis two stated that there would be a significant difference between minor and
adult victims of human trafficking on PTSD. Table 2 above showed that minors scored
mean higher than the adults (Minors (M = 24.73); Adults (M = 21.83), but the difference
observed in the mean failed to reach significant level at t(53)=1.42, p >.05. Therefore,
hypothesis two is rejected.
Table 3: Summary Table of Mean, Standard Deviation and t-test on Family type Source Family type Mean Std deviation N T Df Sig
Family type
on PTSD
Monogamous
Polygamous
23.20
22.13
7.41
6.40
25
30
.57 53 .57
The hypothesis three stated that there would be a significant difference between victims
from monogamous family setting and those from polygamous family setting on PTSD.
Table 3 above showed that victims from a monogamous family setting scored mean
higher than those from a polygamous family setting, (Monogamous (M = 23.20);
Polygamous (M = 22.13). However, the observed difference in the mean failed to reach
significant level at t(53)=.57, p >.05. Therefore, hypothesis three is rejected.
Source Self-esteem Mean Std deviation N T Dt Sig
Self-esteem
On PTSD
High self-esteem
Low self-esteem
20.44
26.14
7.33
4.04
34
21
-3.26 53 .00
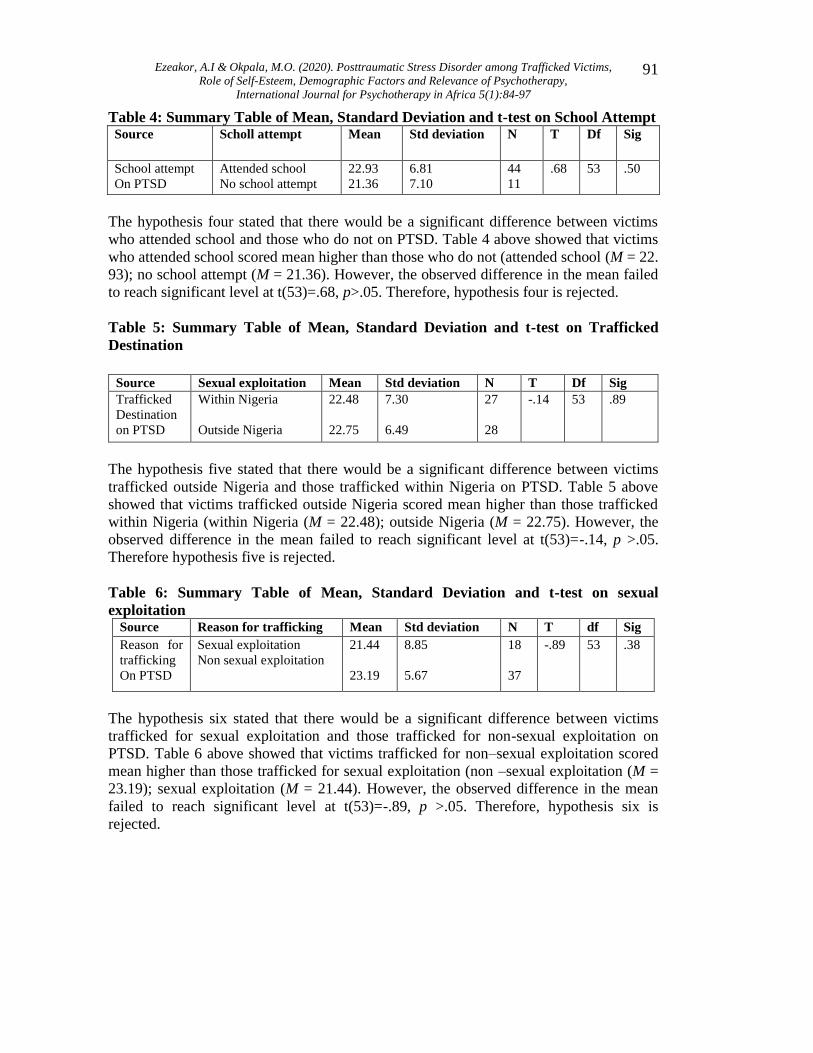
Ezeakor, A.I & Okpala, M.O. (2020). Posttraumatic Stress Disorder among Trafficked Victims,
Role of Self-Esteem, Demographic Factors and Relevance of Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):84-97
91
Table 4: Summary Table of Mean, Standard Deviation and t-test on School Attempt Source Scholl attempt Mean Std deviation N T Df Sig
School attempt
On PTSD
Attended school
No school attempt
22.93
21.36
6.81
7.10
44
11
.68 53 .50
The hypothesis four stated that there would be a significant difference between victims
who attended school and those who do not on PTSD. Table 4 above showed that victims
who attended school scored mean higher than those who do not (attended school (M = 22.
93); no school attempt (M = 21.36). However, the observed difference in the mean failed
to reach significant level at t(53)=.68, p>.05. Therefore, hypothesis four is rejected.
Table 5: Summary Table of Mean, Standard Deviation and t-test on Trafficked
Destination
The hypothesis five stated that there would be a significant difference between victims
trafficked outside Nigeria and those trafficked within Nigeria on PTSD. Table 5 above
showed that victims trafficked outside Nigeria scored mean higher than those trafficked
within Nigeria (within Nigeria (M = 22.48); outside Nigeria (M = 22.75). However, the
observed difference in the mean failed to reach significant level at t(53)=-.14, p >.05.
Therefore hypothesis five is rejected.
Table 6: Summary Table of Mean, Standard Deviation and t-test on sexual
exploitation Source Reason for trafficking Mean Std deviation N T df Sig
Reason for
trafficking
On PTSD
Sexual exploitation
Non sexual exploitation
21.44
23.19
8.85
5.67
18
37
-.89 53 .38
The hypothesis six stated that there would be a significant difference between victims
trafficked for sexual exploitation and those trafficked for non-sexual exploitation on
PTSD. Table 6 above showed that victims trafficked for non–sexual exploitation scored
mean higher than those trafficked for sexual exploitation (non –sexual exploitation (M =
23.19); sexual exploitation (M = 21.44). However, the observed difference in the mean
failed to reach significant level at t(53)=-.89, p >.05. Therefore, hypothesis six is
rejected.
Source Sexual exploitation Mean Std deviation N T Df Sig
Trafficked
Destination
on PTSD
Within Nigeria
Outside Nigeria
22.48
22.75
7.30
6.49
27
28
-.14 53 .89
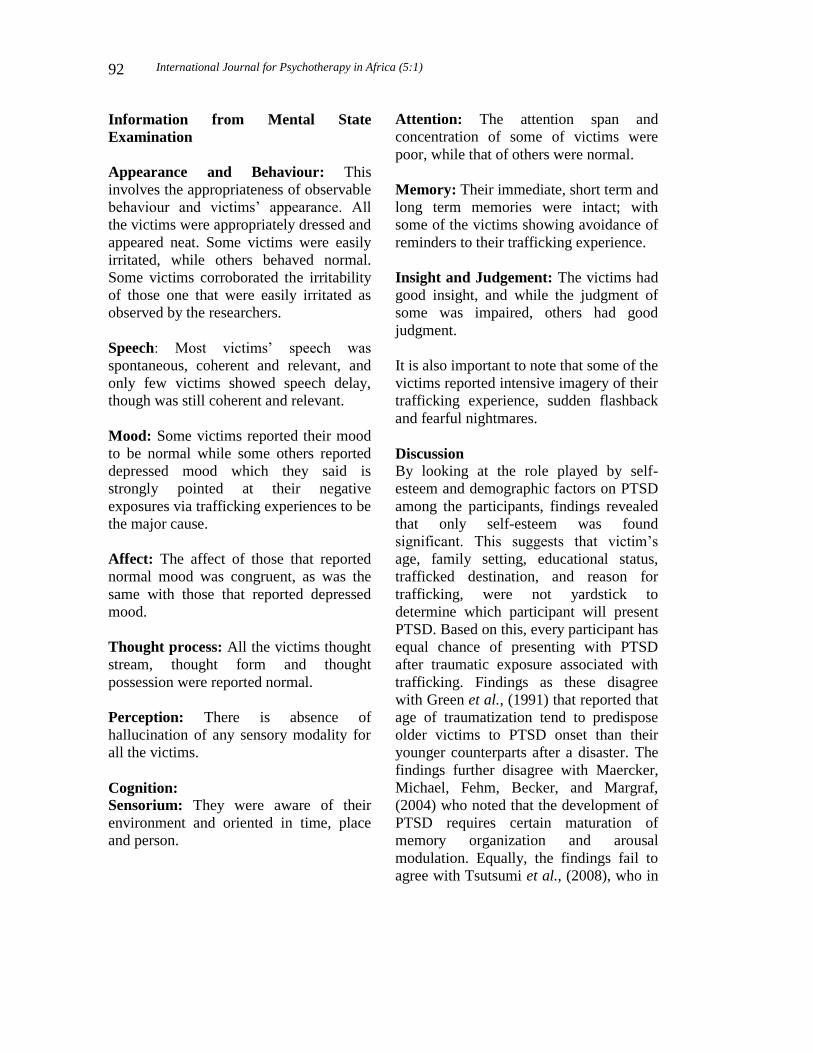
International Journal for Psychotherapy in Africa (5:1)
92
Information from Mental State
Examination
Appearance and Behaviour: This
involves the appropriateness of observable
behaviour and victims’ appearance. All
the victims were appropriately dressed and
appeared neat. Some victims were easily
irritated, while others behaved normal.
Some victims corroborated the irritability
of those one that were easily irritated as
observed by the researchers.
Speech: Most victims’ speech was
spontaneous, coherent and relevant, and
only few victims showed speech delay,
though was still coherent and relevant.
Mood: Some victims reported their mood
to be normal while some others reported
depressed mood which they said is
strongly pointed at their negative
exposures via trafficking experiences to be
the major cause.
Affect: The affect of those that reported
normal mood was congruent, as was the
same with those that reported depressed
mood.
Thought process: All the victims thought
stream, thought form and thought
possession were reported normal.
Perception: There is absence of
hallucination of any sensory modality for
all the victims.
Cognition:
Sensorium: They were aware of their
environment and oriented in time, place
and person.
Attention: The attention span and
concentration of some of victims were
poor, while that of others were normal.
Memory: Their immediate, short term and
long term memories were intact; with
some of the victims showing avoidance of
reminders to their trafficking experience.
Insight and Judgement: The victims had
good insight, and while the judgment of
some was impaired, others had good
judgment.
It is also important to note that some of the
victims reported intensive imagery of their
trafficking experience, sudden flashback
and fearful nightmares.
Discussion
By looking at the role played by self-
esteem and demographic factors on PTSD
among the participants, findings revealed
that only self-esteem was found
significant. This suggests that victim’s
age, family setting, educational status,
trafficked destination, and reason for
trafficking, were not yardstick to
determine which participant will present
PTSD. Based on this, every participant has
equal chance of presenting with PTSD
after traumatic exposure associated with
trafficking. Findings as these disagree
with Green et al., (1991) that reported that
age of traumatization tend to predispose
older victims to PTSD onset than their
younger counterparts after a disaster. The
findings further disagree with Maercker,
Michael, Fehm, Becker, and Margraf,
(2004) who noted that the development of
PTSD requires certain maturation of
memory organization and arousal
modulation. Equally, the findings fail to
agree with Tsutsumi et al., (2008), who in

Ezeakor, A.I & Okpala, M.O. (2020). Posttraumatic Stress Disorder among Trafficked Victims,
Role of Self-Esteem, Demographic Factors and Relevance of Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):84-97
93
a study of female survivors of human
trafficking in Nepal, reported that PTSD
was found to be higher in sex workers
group than in the non sex workers group.
Findings as this did not support the view
of Anaeto (2008) that those trafficked for
sexual exploitation are at greater risk of
developing psychological disorders
following their being at greater risk of
violence and abuse.
Besides, obtaining a significant
difference between low and high self-
esteem level among trafficked victims on
PTSD indicates that the two variables can
associate. It could be that the victims with
low self-esteem had low self-esteem
before being trafficked and their traumatic
exposure exacerbated it or that the
trafficking experiences lowered their self-
esteem. It could as well be that those with
high self-esteem before being trafficked
had the exploits (e.g. income) they made
from the trafficking increase their self-
esteem or that their self-esteem increased
for the first time following the gains they
recorded from the trafficking. It is
suspected that trafficked victims that
consciously made themselves available to
be trafficked could have such goal
attainment increase their self-esteem.
Current study finding agrees with Bradley
et al., (2005) who reported that low self-
esteem was related to high mental health
difficulties, as well as with Salami (2010)
who reported that self-esteem moderated
presentation of PTSD.
Relevance of Psychotherapy Psychotherapy is an activity that enables
people to develop understanding about
themselves and make changes in their
lives. Grand (1997) cites that
psychotherapy takes into account the
socio-cultural and socio-political context
in which the client lives and how these
factors affect the client’s present problem.
The relevance of psychotherapy to the
handling of PTSD in Trafficked victims at
rehabilitation centers at NAPTIP’s
southern zonal offices cannot be
overemphasized. Psychotherapy may
involve working with current problems,
immediate crisis, and long-term
difficulties that Trafficked victims
experience in presentations of their
problems. It also involves maintaining the
PTSD that underlies:
1. Overwhelming feelings of sadness
or helplessness
2. An inability to cope with everyday
problems
3. Drinking problems, being
aggressive to an extent that is
harming themselves or others
4. Feeling constantly on edge or
worrying unnecessarily
In addition, one cannot treat a
persons’ illnesses unless one knows why
they are ill and how it happened. This
statement illustrates how psychotherapy
helps people gain insight in dealing with
their PTSD cases. Psychotherapy targets
to improve therapeutic support to
influence people’s behavior with the
myriads of the available therapies such as
Cognitive Behavioural Therapy (CBT),
Behavioural Therapy (BT), Rational
Emotive Behavioural Therapy (REBT),
Aversion Therapy, to mention but few.
Madu (2003) supports this view that
psychotherapy is a basic need for the
human, irrespective of gender, colour, or
race. He explains that psychotherapy in
the past, present and future targets
people’s health and wellness.
Psychotherapy refers to a sum total of
knowledge, representing generation of

International Journal for Psychotherapy in Africa (5:1)
94
experiences, careful observations and try-
and-error experiments which
psychotherapists in a particular ethnic
group possess, and which enable them to
handle both social and health problems
affecting people in their respective
communities. As a clinicians, one of the
authors realized the illustration of Madu
here while working with Trauma Network
United Kingdom. Based on author’s
(Ezeakor) scientific knowledge and
research, he observed that psychotherapy
improves a lot with PTSD trauma victims
to regain their self-esteem in the society.
With PTSD Trafficked victims, the
authors have seen things that stay quite a
long time with them while working with
people that are shattered with emotional
difficulties. In the presentations of their
stories, we observed that prolonged
trauma is a targeted lesson for us to see
what people pass through in their lives and
also the possible behavioural indicators
such as:
1. Reluctant to disclosure of trauma
due to shame and guilt
2. The stigma associated with abuse,
torture and power relations
3. Inability to seek help as a result of
low self-esteem
4. Hyper arousal or symptoms of
anger, fearfulness, irritability,
temper tantrums and regressive or
clinging behaviour
Remarkable presentations of
peoples’ PTSD with multiple experiences
of abuses and despair challenged our
practice to look at how psychotherapy is
structured to improve support for PTSD
Trafficked victims to regain their self-
esteem with the instrument of the modern
technology.
Conclusion Of the factors examined in the present
study, only victims’ self-esteem level was
found to be a factor likely to determine
who is to present PTSD. Inferring from
this, one can assert that victims’
evaluation of their worth is an important
aspect of their mental health and ability to
cope with associated negative experiences
of trafficking. Psychotherapy facilitates
improved mental state of individual(s)
who are unable to successfully process
and handle the inundating psycho-
emotional presentations.
Psychotherapy on treatment
modalities with PTSD Trafficked victims
explains the basic need for the human
interventions. The intensifying efforts in
psychotherapy need promotion of co-
operation and a favourable atmosphere for
cross-pollination of ideas between the
western-oriented psychotherapists and
their African colleagues. It will create
opportunities for training, especially in the
School of Psychotherapy and Health
Sciences Okija Nigeria, where
psychotherapy knowledge facilitates
professional development on PTSD
related crisis and trauma. Enriching in
more information services and problem-
solving strategies, the relevance of
psychotherapy will continue to be a basic
human need for PTSD Trafficked victims
to regain their self-esteem in Africa.
References
American Psychiatric Association (2013).
Diagnostic and statistical manual of
mental disorders, fifth edition.
Washington, D.C.: APA.
Anaeto, J. (2008). Handbook on access to
justice for victims of Trafficking in
Nigeria, for the validation workshop
on the handbook on access to justice
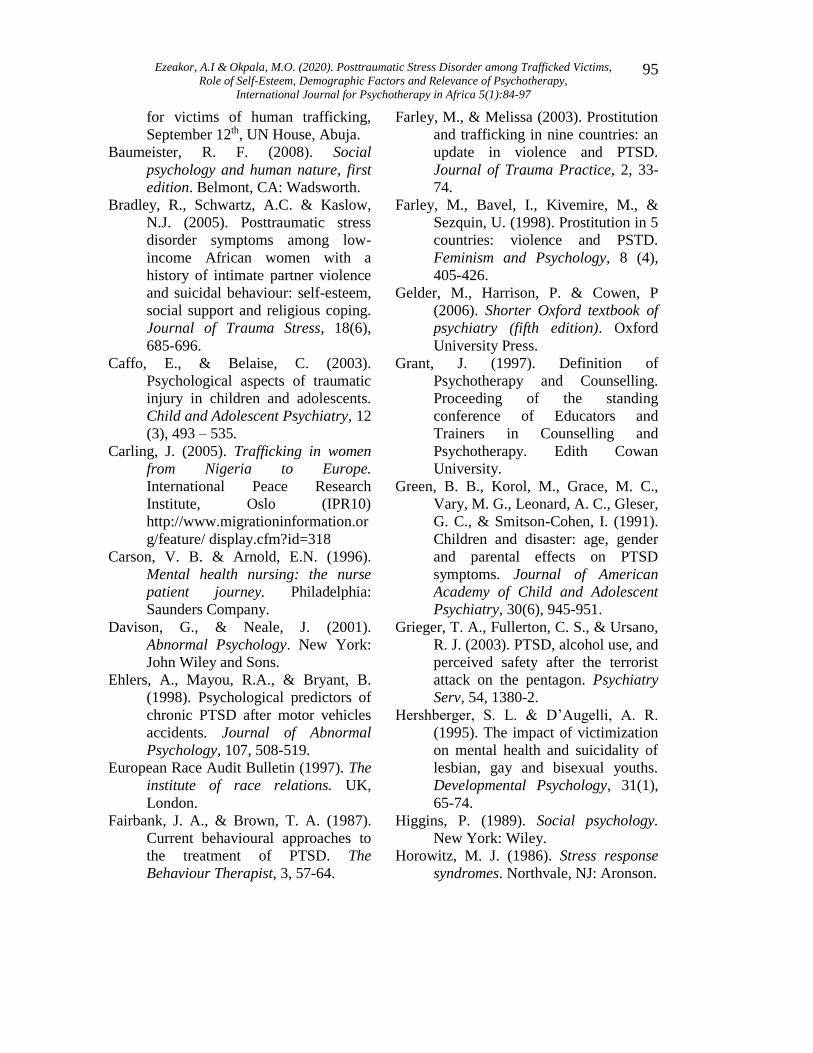
Ezeakor, A.I & Okpala, M.O. (2020). Posttraumatic Stress Disorder among Trafficked Victims,
Role of Self-Esteem, Demographic Factors and Relevance of Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):84-97
95
for victims of human trafficking,
September 12th, UN House, Abuja.
Baumeister, R. F. (2008). Social
psychology and human nature, first
edition. Belmont, CA: Wadsworth.
Bradley, R., Schwartz, A.C. & Kaslow,
N.J. (2005). Posttraumatic stress
disorder symptoms among low-
income African women with a
history of intimate partner violence
and suicidal behaviour: self-esteem,
social support and religious coping.
Journal of Trauma Stress, 18(6),
685-696.
Caffo, E., & Belaise, C. (2003).
Psychological aspects of traumatic
injury in children and adolescents.
Child and Adolescent Psychiatry, 12
(3), 493 – 535.
Carling, J. (2005). Trafficking in women
from Nigeria to Europe.
International Peace Research
Institute, Oslo (IPR10)
http://www.migrationinformation.or
g/feature/ display.cfm?id=318
Carson, V. B. & Arnold, E.N. (1996).
Mental health nursing: the nurse
patient journey. Philadelphia:
Saunders Company.
Davison, G., & Neale, J. (2001).
Abnormal Psychology. New York:
John Wiley and Sons.
Ehlers, A., Mayou, R.A., & Bryant, B.
(1998). Psychological predictors of
chronic PTSD after motor vehicles
accidents. Journal of Abnormal
Psychology, 107, 508-519.
European Race Audit Bulletin (1997). The
institute of race relations. UK,
London.
Fairbank, J. A., & Brown, T. A. (1987).
Current behavioural approaches to
the treatment of PTSD. The
Behaviour Therapist, 3, 57-64.
Farley, M., & Melissa (2003). Prostitution
and trafficking in nine countries: an
update in violence and PTSD.
Journal of Trauma Practice, 2, 33-
74.
Farley, M., Bavel, I., Kivemire, M., &
Sezquin, U. (1998). Prostitution in 5
countries: violence and PSTD.
Feminism and Psychology, 8 (4),
405-426.
Gelder, M., Harrison, P. & Cowen, P
(2006). Shorter Oxford textbook of
psychiatry (fifth edition). Oxford
University Press.
Grant, J. (1997). Definition of
Psychotherapy and Counselling.
Proceeding of the standing
conference of Educators and
Trainers in Counselling and
Psychotherapy. Edith Cowan
University.
Green, B. B., Korol, M., Grace, M. C.,
Vary, M. G., Leonard, A. C., Gleser,
G. C., & Smitson-Cohen, I. (1991).
Children and disaster: age, gender
and parental effects on PTSD
symptoms. Journal of American
Academy of Child and Adolescent
Psychiatry, 30(6), 945-951.
Grieger, T. A., Fullerton, C. S., & Ursano,
R. J. (2003). PTSD, alcohol use, and
perceived safety after the terrorist
attack on the pentagon. Psychiatry
Serv, 54, 1380-2.
Hershberger, S. L. & D’Augelli, A. R.
(1995). The impact of victimization
on mental health and suicidality of
lesbian, gay and bisexual youths.
Developmental Psychology, 31(1),
65-74.
Higgins, P. (1989). Social psychology.
New York: Wiley.
Horowitz, M. J. (1986). Stress response
syndromes. Northvale, NJ: Aronson.
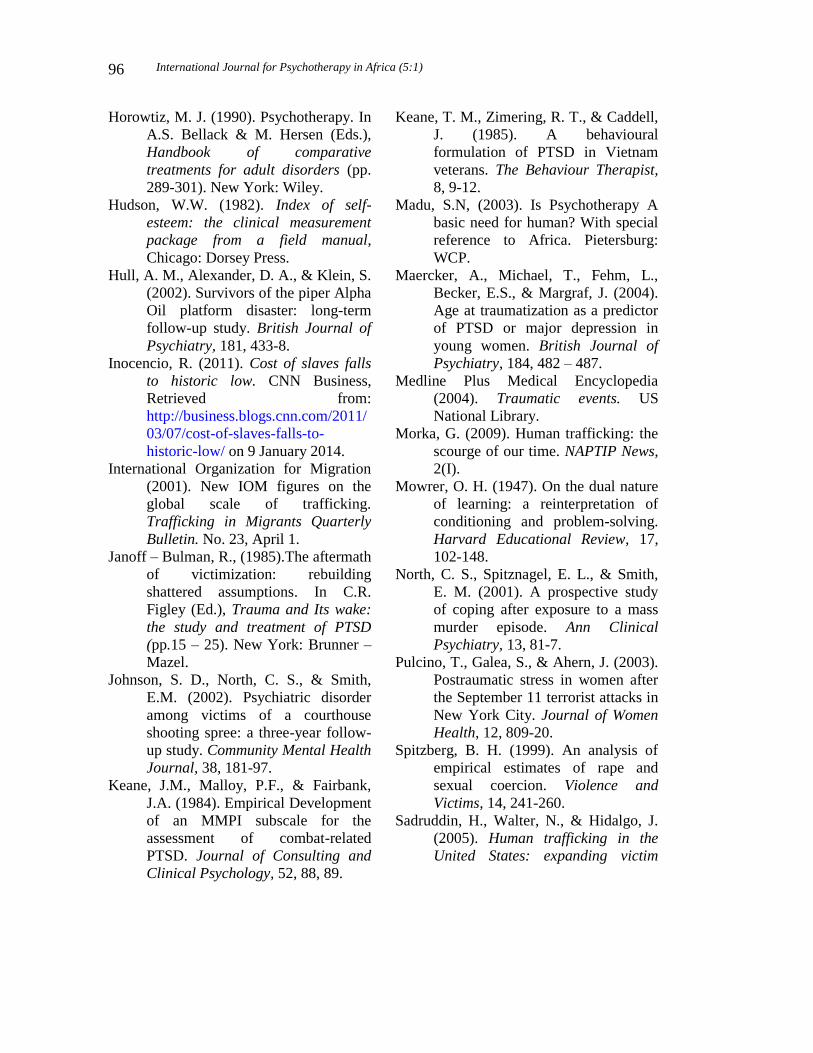
International Journal for Psychotherapy in Africa (5:1)
96
Horowtiz, M. J. (1990). Psychotherapy. In
A.S. Bellack & M. Hersen (Eds.),
Handbook of comparative
treatments for adult disorders (pp.
289-301). New York: Wiley.
Hudson, W.W. (1982). Index of self-
esteem: the clinical measurement
package from a field manual,
Chicago: Dorsey Press.
Hull, A. M., Alexander, D. A., & Klein, S.
(2002). Survivors of the piper Alpha
Oil platform disaster: long-term
follow-up study. British Journal of
Psychiatry, 181, 433-8.
Inocencio, R. (2011). Cost of slaves falls
to historic low. CNN Business,
Retrieved from:
http://business.blogs.cnn.com/2011/
03/07/cost-of-slaves-falls-to-
historic-low/ on 9 January 2014.
International Organization for Migration
(2001). New IOM figures on the
global scale of trafficking.
Trafficking in Migrants Quarterly
Bulletin. No. 23, April 1.
Janoff – Bulman, R., (1985).The aftermath
of victimization: rebuilding
shattered assumptions. In C.R.
Figley (Ed.), Trauma and Its wake:
the study and treatment of PTSD
(pp.15 – 25). New York: Brunner –
Mazel.
Johnson, S. D., North, C. S., & Smith,
E.M. (2002). Psychiatric disorder
among victims of a courthouse
shooting spree: a three-year follow-
up study. Community Mental Health
Journal, 38, 181-97.
Keane, J.M., Malloy, P.F., & Fairbank,
J.A. (1984). Empirical Development
of an MMPI subscale for the
assessment of combat-related
PTSD. Journal of Consulting and
Clinical Psychology, 52, 88, 89.
Keane, T. M., Zimering, R. T., & Caddell,
J. (1985). A behavioural
formulation of PTSD in Vietnam
veterans. The Behaviour Therapist,
8, 9-12.
Madu, S.N, (2003). Is Psychotherapy A
basic need for human? With special
reference to Africa. Pietersburg:
WCP.
Maercker, A., Michael, T., Fehm, L.,
Becker, E.S., & Margraf, J. (2004).
Age at traumatization as a predictor
of PTSD or major depression in
young women. British Journal of
Psychiatry, 184, 482 – 487.
Medline Plus Medical Encyclopedia
(2004). Traumatic events. US
National Library.
Morka, G. (2009). Human trafficking: the
scourge of our time. NAPTIP News,
2(I).
Mowrer, O. H. (1947). On the dual nature
of learning: a reinterpretation of
conditioning and problem-solving.
Harvard Educational Review, 17,
102-148.
North, C. S., Spitznagel, E. L., & Smith,
E. M. (2001). A prospective study
of coping after exposure to a mass
murder episode. Ann Clinical
Psychiatry, 13, 81-7.
Pulcino, T., Galea, S., & Ahern, J. (2003).
Postraumatic stress in women after
the September 11 terrorist attacks in
New York City. Journal of Women
Health, 12, 809-20.
Spitzberg, B. H. (1999). An analysis of
empirical estimates of rape and
sexual coercion. Violence and
Victims, 14, 241-260.
Sadruddin, H., Walter, N., & Hidalgo, J.
(2005). Human trafficking in the
United States: expanding victim
Ezeakor, A.I & Okpala, M.O. (2020). Posttraumatic Stress Disorder among Trafficked Victims,
Role of Self-Esteem, Demographic Factors and Relevance of Psychotherapy,
International Journal for Psychotherapy in Africa 5(1):84-97
97
protection beyond prosecution
witnesses. New York: Free.
Salami, S. O. (2010). Moderating effects
of resilience, self-esteem and social
support on adolescents’ reactions to
violence. Asian Social Science,
6(12), 101-110.
Silbert, M., & Pines, A. (1981).
Occupational hazards of street
prostitutes. Criminal Justice and
Behaviours, 8 (4), 395-399.
Sita, N. M. (2003). Trafficking in women
and children situation and some
trends in African countries. Paper
delivered by Director UNAFRI.
Stewart, S. H., Mitchell, T. L., & Wright,
K. D. (2004). The relations of PTSD
symptoms to alcohol use and coping
drinking in volunteers who
responded to the Swissair flight III
airline disaster. Journal of Anxiety
Disorder, 18, 57 – 68.
Strauman, T. J. (1992). Self-guides,
autobiographical memory, anxiety
and dysphoria: towards a cognitive
model of vulnerability emotional
distress. Journal of Abnormal
Psychology, 101, 87-95.
Tsutsumi, A., Izutsu, T., Poudyal, A. K.,
Kato, S. & Marui, E. (2008).
Survivors of human trafficking in
Nepal. Social Science Medicine, 66
(8), 1841-7.
World Health Organization (1992). The
international classification of
diseases, tenth edition. Geneva:
World Health Organization.
Yehuda, R., Engel, S. M., Brand, S. R.,
Seckl, J., Marcus, S. M., &
Berkowitz, G. S. (2005).
Transgenerational effects of PTSD
in babies of mothers exposed to the
World Trade Center attacks during
pregnancy. Journal of Clinical
Endocrinology & Metabolism, 90,
4115–4118.
International Journal for Psychotherapy in Africa (5:1)
98
Integration Of Spirituality Into Psychotherapy –
A Potential Model For Nigeria
Richard Uwakwe
Department of Mental Health, Faculty of Medicine
Nnamdi Azikiwe University, Awka, Nigeria.
[email protected]; [email protected]
Abstract Although Sigmund Freud, reputed to be the father of psychoanalysis was not favourably
disposed to religion, recent developments indicate that interest in religion and mental
health and psychotherapy has grown. Most clients that come to psychotherapy are likely
to have a religious orientation and will benefit from integrating spirituality into therapy.
Psychotherapists need to learn the techniques and skills of how this integration can best
be achieved especially in Nigeria where religion is a very sensitive issue.
Key words: Religion, psychotherapy, Nigeria.
Introduction
Long before the development of modern
psychological treatments, it has been
known that giving psychological and
social assistance to people in distress was
helpful. The psychosocial assistance may
sometimes involve religious approaches
such as prayers. Traditionally, Sigmund
Freud is often credited as the father of
formal psychoanalysis. Freud’s views
about religion have been a matter of
academic debate. Freud is said to have
regarded religion as an illusion on one
hand and as having originated from the
father figure in the Oedipus complex
(Ahmed 2012; Okon 2012). Freud saw
belief in God as an attempt to reconcile
humankind with its embeddedness into
nature that is mostly experienced as
traumatic. He interpreted the formation of
religions in terms of their function in this
conflict between nature and culture, or
between the ego and the drive.
In recent times, although skepticism
remains, there seems to have been a flood
of interest in spirituality, in respect of
people’s health, mental health and
psychotherapy. A myriad of issues
surround this subject.
In this paper, the author will attempt
to briefly examine the potential
opportunities for integrating spirituality
into psychotherapy in Nigeria.
Religion and Spirituality
Susanto and Idris (2017) in reviewing
Freudian view of religion, opined that
Freud theorized that religion was a tool to
make people believe in the existence of
God or Gods and that the gods function as
a medium to overcome the threat of
nature, to make people accept the cruelty
of their fate and promise rewards for the
suffering and the frustration demanded of
human beings. In other words, through
religion, men merely attempt to protect

Uwakwe, R. (2020). Integration of Spirituality into Psychotherapy –
A Potential Model For Nigeria, International Journal for Psychotherapy in Africa 5(1):98-107
99
themselves against all kinds of threats and
suffering. This protection is said to be
only an illusion: gods do not really
protect human beings, but are only
imagined to have protected them.
This line of thought thus dismisses
religion more or less as a psychological
defence mechanism.
While many Christian writers
present Carl Jung as being non-religious,
or in fact anti-religious, especially with
respect to Christianity, those who ascribe
the initial thoughts or ideas leading to the
formation of alcoholic anonymous regard
Jung as deeply religious (James, 2016).
In fact the tones of the steps of the
alcoholic anonymous look very spiritual.
The first of the twelve steps is particularly
remarkable, indicating that the client has
reached the point of human limit and
requires a Higher Power, which is a very
spiritual laden position.
The famed Psychiatrist, Jerome
Frank is often generally quoted to have
averred that psychotherapy is not
primarily an applied science but rather that
in some ways it more resembles a religion
(Dow 1986; James 2016).
In themselves, the two concepts of
religion and spirituality have been difficult
to define universally.
According to Dew et al (2008),
religion is an “organized system of beliefs,
rituals, practices, and community, oriented
toward the sacred”. It is said that religion
tends to focus on formal organizations
with specifically defined and widely
accepted beliefs, practices, and traditions.
Spirituality, in contrast, can be thought of
as a “search for the sacred, a process
through which people seek to discover,
hold on to, and, when necessary, transform
whatever they hold sacred in their lives”
(Hill & Pargament, 2008). Unlike religion
which is practiced in communities of
individuals, spirituality can be a very
private experience and need not be part of
experiences in organized religion.
Authorities in the field have argued that it
is possible for someone to be religious but
not spiritual, spiritual but not religious,
neither religious nor spiritual, or both
spiritual and religious (Worthington et al
1996). Different people from all walks of
life fall into these various groups of
religious orientations. In most parts of the
world there is no doubt that quite a
number of people are religious.
Although the distinction has been
made between religion and spirituality yet
at the same time, the concepts may be
seen as just terms and words. Some, [for
example Nolan and Crawford (1997)]
argue that spirituality is subsumed by
religion while others see religion as one
dimension of spirituality (Hill et al.,
2000). People who are spiritual may be
involved in establishing religion
organizations. Therefore spirituality and
religion may be interchangeable. In this
paper, any expression of personal or
communal belief or practice about God
will be taken as spirituality or religion.
Therefore throughout this paper, the two
terms will be used interchangeably.
Psychotherapy and Religion
Psychotherapy has many definitions but
Meltzoff and Kornreich (1970) provided
a classical conceptualization. They defined
Psychotherapy as the informed and
planned application of techniques derived
from established psychological principles,
by persons qualified through training and
experience to understand these principles
and to apply these techniques with the
intention of assisting individuals to modify
such personal characteristics as feelings,

International Journal for Psychotherapy in Africa (5:1)
100
values, attitudes, and behaviors which are
judged by the therapist to be maladaptive
or maladjustive. (p. 6). This is the
definition adopted in this paper. The
psychotherapy may involve simple talk
between the therapist and the client or any
other technique used to produce a change
in the feeling, thinking or behaviour of the
client.
Perhaps for political and other
reasons, there does not seem to be an
official documentation of the religious
orientation of Nigerians, distributed across
the main stream faiths of Christianity and
Islam. There is no official documentation
by the National Population Commission as
to how many Nigerians belong to which
religion. However, in general, most
people believe that Nigeria is a very
religious country and that most of its
citizens belong to one or another religious
faith. In many western and non-western
countries many people are to a large extent
religious.
Pew Research (2008) reported that
more than nine-in-ten Americans (92%)
believe in the existence of God or a
universal spirit, sixty three percent of
American women and 44% of American
men say that religion is very important to
their lives and Americans are nearly
unanimous in accepting a belief in God
and religion (92%), and large majorities
believe in life after death (74%) and
believe that the Scripture is the word of
God (63%).
According to the same report, more
than half of the studied American
population (54%) claim that they attend
religious services fairly regularly (at least
once or twice per month), with about four-
in-ten (39%) saying they attend worship
services every week. The report indicates
that Americans also engage in a wide
variety of private devotional activities.
Nearly six-in-ten (58%), for instance,
profess that they pray every day. The
report states that some people who are not
affiliated with a particular religious
tradition do not necessarily lack religious
beliefs or practices. In fact, a large portion
(41%) of the unaffiliated population
admits that religion is at least somewhat
important in their lives, seven-in-ten
accept that they believe in God, and more
than a quarter (27%) claim that they
attend religious services at least a few
times a year (Pew Research, 2008).
From these findings, the authors
think that it is safe to assume that religion
and spirituality are of relevance to the
lives of a large portion of American clients
every psychotherapist will come in contact
with. This is most likely the case in
Nigeria and perhaps a huge number of
countries throughout the world.
While religious and spiritual issues
may not be a primary focus of treatment,
they are likely to be relevant aspects of
each client’s life, helping to define their
values, beliefs, lifestyle choices, and
decision making. The authors of the
American religious survey hitherto
referred to; contend that many people find
spirituality and religiosity extremely
comforting. Some people may consult
psychotherapists when there is something
wrong in their lives that their faith does
not help them with. Feelings of
depression, existentiality, anxiety, etc
affect people of all faiths.
Most religious faiths have rules,
regulations and prohibitions against such
things as masturbation, pre-marital sex,
extra marital sex, or, sex during a
woman’s menstrual cycle, stealing,
forgiveness, generosity, etc. These may

Uwakwe, R. (2020). Integration of Spirituality into Psychotherapy –
A Potential Model For Nigeria, International Journal for Psychotherapy in Africa 5(1):98-107
101
become areas of conflict for some people
for which psychotherapy may be needed.
There are other areas of life where
religious faith can become a complicating
problem for many people. These problems
include such things as homosexuality,
divorce, abortion, inter faith marriage,
depression and many heterosexual
practices. Religious and spiritual issues
may be relevant to the underlying issues
that prompt clients to seek treatment.
These can include conflicts over religious
values, crises of faith, feelings of
alienation from one’s religion, and
distortion of religious beliefs and
practices, among others.
On the other hand, the client’s
religious and spiritual beliefs and faith
community may be sources of strength
and support that may be accessed in the
course of psychotherapy to assist clients to
achieve their treatment goals. Yet it has
been reported that many psychotherapists
do not enquire about the religious and
spiritual aspects of their clients (Frazer &
Hansen, 2009; Hathaway, Scott & Garver,
2004).
Post and Wade (2009) contend that
the recent resurgence of interest within
the mental health professions to
understand and address the sacred is
probably attributed to the following
developments: research showing a positive
relationship between religion and health;
the majority of the general public in the
United States identifying as religious or
spiritual; and the ascendancy of
multicultural counseling encouraging
sensitivity to cultural diversity, which
includes the religious and spiritual (Hage,
Hopson, Siefel, Payton, & DeFanti, 2006).
The authors cited the study by Delaney,
Miller, and Bisono (2007) who surveyed
the religiosity and spirituality of some
members of the American Psychological
Association (APA) to make comparisons
to both a sample of psychologists
surveyed in 1985 and reported that the
psychologists remain much less religious
than the population they serve.
Post and Wade (2009) were of the
view that psychologists as a group tend to
embrace spirituality more commonly
today than they did in the mid-1980s.
Psychologists today, they argue, are more
likely to describe themselves as ‘‘spiritual
but not religious’’ than the population they
serve (Delaney et al., 2007).
Still, it seems that most
psychologists view the religiosity of their
clients positively.
The widespread nature of religious
orientation among a great number of
people in the world implies that the
majority of people who come for
psychotherapy are likely to belong to one
or another religion. The question is
whether these clients can be treated
without any reference to their spirituality
or if it is possible to integrate their religion
with their psychotherapeutic treatment.
Integration of Spirituality in
Psychotherapy
Some have advocated the integration of
spirituality in psychotherapy when
appropriate and if the therapists have the
competence to do so. According to Plante
(2016) mindfulness, a method that
originated from Buddhist tradition has
been found to be commonly used in
psychotherapy in recent times. This is also
true of yoga, prayer, meditation from other
traditions etc. Hodge (2006) in a review
of the then extant literature demonstrated
that incorporating spirituality into
cognitive therapy for depressive disorders
was effective.

International Journal for Psychotherapy in Africa (5:1)
102
More recently, Pearce et al (2015) have
developed a manualized psychotherapeutic
approach, Religiously Integrated
Cognitive Behavioral Therapy (RCBT)
which is designed to assist persons with
depressive disorders to develop
depression-reducing thoughts and
behaviors informed by their own religious
beliefs, practices, and resources. The
treatment approach has been developed for
five major world religions (Christianity,
Judaism, Islam, Buddhism, and
Hinduism), making it useful for ill
individuals from a variety of religious
backgrounds. Kennedy, Macnab and Ross
(2015) reviewed published literature from
2010, and reported that spirituality has
been found useful in psychotherapy when
dealing with a number of psychosocial
conditions including anxiety, depression,
schizophrenia and coping with physical
illness.
Peres, Smao and Nasello (2007)
regard religious beliefs and practices as
constituting an important part of culture
and principles which clients use to shape
judgments and process information.
Therefore, it is said that Psychotherapists
may use knowledge of these belief
systems and appreciation of their potential
to leverage client adherence and achieve
better outcomes. The humanistic
psychotherapies believe that humans have
the innate tendency to grow and self-
actualize. These potentialities can be
harnessed in clients when their religious
beliefs and practices are taken into
account in therapy. In doing this, a key
issue is the maintenance of neutrality and
ethical standard.
Challenges and Suggestions
Integration of spirituality into
psychotherapy poses a number of
challenges, not only because most
therapists have neither the training nor the
experience in the area but also because
religion and spirituality can be highly
personal and it can be an exceedingly
great challenge for professionals to
separate their personal beliefs (or lack of
beliefs) and practices from their
professional ones (Plante, 2006).
In Nigeria the challenge can be quite
huge and more complicated, not only
because of the likely nature of the training
and experience of therapists but because
of the sensitive nature of religion in the
country. In both Islam and Christendom,
the beliefs are not homogenous and
denominational/ sectarian conflicts are not
uncommon. How can religion be
integrated into psychotherapy with an
acceptable coherent marriage that does not
evoke bias, prejudice, and unwitting overt
or covert conflict?
Plante (2016) provided some
suggestions on the principles that should
guide the integration of spirituality into
psychotherapy. The author argues that
spirituality and religion should be treated
as a multicultural and diversity issue
demonstrating respect for and attention to
multiculturalism that includes religion and
spirituality on par with race, ethnicity,
gender, sexual orientation, and so forth
(American Psychological Association,
2002).
In the helping professions such as
education, medicine, social works etc,
clients and therapists come from mixed
different backgrounds –both cultural and
religious. Once there is mutual respect
and understanding, Jews, Shintoists,
Buddhists, Muslims, Jainists, Animists etc
could be attended to by Christians,
Confuciusnists, vice versa.Plante (2006)
states that other principles to consider in
Uwakwe, R. (2020). Integration of Spirituality into Psychotherapy –
A Potential Model For Nigeria, International Journal for Psychotherapy in Africa 5(1):98-107
103
integration of religion into psychotherapy
include keeping biases in check, staying
within one’s own area of expertise,
referring to experts including clerics,
being aware of best practices and evidence
based assessments and interventions, and
using resources where available. A
psychotherapist must be ethical and
mature and avoid imposing his or her
religious disposition on the client while
attempting to integrate religion into
psychotherapy. The overriding issue will
be what the client believes in. There is
need for extra caution in cases where the
client and the therapist do not share the
same beliefs. Barnett and Johnson (2011)
recommend that in taking such an
integrative decision, the therapist must
carefully consider and do the following:
i. Respectfully assess the client’s
religious or spiritual beliefs and
preferences.
ii. ii. Carefully assess any connection
between the presenting problem and
religious or spiritual beliefs and
commitments:
iii. Weave results of assessment into
the informed consent process.
iv. Honestly consider the therapist’s
counter- transference to the client’s
religiousness.
v. Honestly evaluate the therapist’s
competence in any given case.
vi. Consult with experts in the area of
religion and psychotherapy.
vi. If appropriate, clinically indicated,
and client gives consent, consult
with client’s own clergy or other
religious professional.
vii. Take a decision about treating the
client or making a referral.
viii. Assess outcomes and adjust plan
accordingly.
In the same vein, the American Psychiatric
Association, 2006 (as cited by Peres Smao
and Nasello, 2007) recommend that
psychotherapists working with the
question of spirituality and religiousness
should do the following:
i. Determine whether religious and
spiritual variables are clinical
characteristics relevant to the
complaints and symptoms
presented.
ii. Examine the role of religion and
spirituality in the belief system.
iii. See whether religious idealizations
and representations of God are
relevant and approach this
idealization clinically.
iv. Demonstrate the use of religious and
spiritual resources in psychological
treatment.
v. Use interview procedures to access
history and involvement of religion
and spirituality.
vi. Get trained in appropriate
interventions for religious and
spiritual subjects and update
knowledge of ethics in relation to
religious and spiritual themes in
clinical practice.
It has been suggested that psychotherapists
can learn how to integrate spirituality in
their session by learning from the
experience of those who already know
how to do it and also by becoming more
self-aware to enhance their work with
religious/spiritual clients (Bartoli, 2007).
Being aware of one’s own beliefs and
biases regarding religion/spirituality for
example by exploring one’s own spiritual
ideas and values through writing a
spiritual autobiography is thought to help
therapists avoid imposing their own values
on their clients. (Wiggins, 2008). Peres,
International Journal for Psychotherapy in Africa (5:1)
104
Smao and Nasello (2007) opine that
religious belief is an important part of
culture, principles and values used by
clients to shape judgments and process
information. The authors argue that
confirming clients’ beliefs and perceptive
leanings may boost the ability to organize
or comprehend painful, chaotic, or
unexpected events. The authors further
state that to be successful in integrating
spirituality into psychotherapy, it will be
helpful for therapists to be versed in some
of the basic tenets of their clients’
religions but not necessarily for therapists
to be experts in comparative religion.
Instead, approaching religious/spiritual
clients with an openness and willingness
to engage the religious/ spiritual
conversation will help clients to feel
comfortable expressing their needs.
Post and Wade (2009) gave the
following summary:
Psychotherapists can
routinely assess clients’
treatment preferences for
including or not including
spirituality. Therapists should
routinely assess for religious/
spiritual history and
concerns. Empirical evidence
suggests that
religious/spiritual
interventions are often
effective.
Consequently, integrated psychoreligious
interventions can be delivered effectively
by therapists of all religious/spiritual
beliefs.
In one study in south western
Nigeria, Adegoke (2007) concluded that
many Nigerians use spiritual healing
homes to solve their various problems,
with great influence of education and
economic factors associated with such
religious use. Before they reach formal
psychiatric care, up to 80% of Nigerians
would have contacted a spiritual guide
(Toftegaard et al 2015). More recent
studies indicate that for both physical and
psychological illnesses, Nigerians
copiously use religious therapeutic
approach (Amadi et al 2016; Busari &
Muftau M. A. 2017).
Therefore Nigerians are already used
to religiously delivered therapy.
The questions to consider are: to what
extent is psychotherapy taught and
practised in Nigeria? In view of the
multicultural and multi-religious nature of
Nigeria, with a very sensitive
ethnoreligious characteristic, what
practical steps are necessary in integrating
spirituality into formal psychotherapy in
Nigeria? How can the only school of
psychotherapy in Nigeria (School of
Psychotherapy and Health Sciences;
www.sphs.com.ng), especially at its early
phase, establish the culture of integrating
spirituality in psychotherapy training?
There are no available records to
show the level of psychotherapy practice
in Nigeria. It is also not clear to what
extent Nigerian practising
psychotherapists and clinical
psychologists weave spirituality into
psychotherapy in their local practice.
These issues need to be properly studied to
permit an assessment of what may already
be in place.
Conclusion
It is likely, given the very religious nature
of Nigerians, that bringing spirituality into
psychotherapy would be a potentially
useful model. It has been reported that
therapy seems more effective when the
therapist and the client have common
Uwakwe, R. (2020). Integration of Spirituality into Psychotherapy –
A Potential Model For Nigeria, International Journal for Psychotherapy in Africa 5(1):98-107
105
cultural heritage ((Hayes, McAleavey,
Castonguay, & Locke 2016). Religion in
itself is a culture (Cohen and Hill 2007).
It can therefore be speculated that the
results of treatment may be more effective
if religious Nigerian clients and therapists
adopt spirituality in therapy.
Although there are no available
research reports to show how religious
Nigerian clinical psychologists and
psychotherapists are, nevertheless, one can
speculate that the majority of these
Nigerian professionals are doubtless
religious in view of the religiocultural
milieu of the country. Given that many
Nigerians are already religiously inclined
with respect to their mental health,
Psychotherapists in this environment will
need to seriously consider and attune
themselves to incorporate religion into
psychotherapy. Religious healers should
not be seen as competitors but
complementers and psychotherapists
should be ready and willing to synergize
with them in resolving clients
psychosocial problems (Uwakwe &
Otakpor 2014). In other words, while
adopting religion integration into
psychotherapy, therapists should feel free
to refer clients to religious guides when
and if necessary. Taking into account the
suggestions and experiences of therapists
in other climes, there is need for home
grown local studies to guide the way to
proceed in integrating religion into
psychotherapy in Nigeria.
Religion is part and parcel of the
psychological fabric of human beings and
cannot be separated from their mental
health. Research evidence shows that
religiousness has been associated with
positive outcomes in many investigated
psychosocial and physical problems. If
psychotherapists maintain good ethical
and professional standards and learn the
art and skill of integrating religion into
psychotherapy, the process can be
successful. This will be useful in Nigeria
where religion matters much to most
people.
References
Adegoke T.G. (2007). Sociocultural
factors influencing the use of
spiritual healing churches in Ibadan
Metropolis, Nigeria. Anthropologist
(9) 3: 225-232.
Ahmed, S. (2012). Sigmund Freud’s
psychoanalytic theory: Oedipus
complex: a critical study with
reference to D.H. Lawrence’s “sons
and lovers”. International Journal
of English and literature. 3 (3): 60-
70.
Amadi, K.U; Uwakwe, R; Odinka,
P.C; Ndukuba, A.C; Muomah,
C.R; Ohaeri, J. (2016). Religion,
coping and outcome in outpatients
with depression and diabetes. Acta
Psychiatrica Scandinavica, 133 (6):
489-496.
American Psychological Association
(2002). Ethical principles of
psychologists and code of conduct.
American Psychologist, 57, 1060-
1073.
American Psychological Association
(2003). Guidelines on multicultural
education, training, research,
practice, and organizational change
for psychologists. American
Psychologist, 58, 377-402.
Barnett, J. E., & Johnson, W. B. (2011).
Integrating spirituality and religion
into psychotherapy: Persistent
dilemmas, ethical issues, and a
proposed decision-making
International Journal for Psychotherapy in Africa (5:1)
106
process. Ethics & Behavior, 21(2),
147-164.
Buckley, D. (2008). Where the waters
meet: convergence and
complementarity in therapy and
theology. Karnac books. 2008.
London.
Busari, A. A; Muftau M. A. (2017).
High prevalence of complimentary
and alternative medicine use among
patients with sickle cell disease in a
tertiary hospital in Lagos, South
West Nigeria. Biomed Central
Complementary and Alternative
Medicine, 17: 299.
Cohen, A.B; Hill, P.C. (2007). Religion
as culture: Religious Individualism
and Collectivism among American
Catholics, Jews and Protestants.
Journal of Personality, 75: 4.
Delaney, H.D., Miller, W.R., & Bisono´,
A.M. (2007). Religiosity and
spirituality among psychologists: A
survey of clinician members of the
American Psychological association.
Research and Practice, 38, 538–546
Dew, R. E., Daniel, S. S., Armstrong, T.
D., Goldston, D. B., Triplett, M. F.,
& Koenig, G. (2008).
Religion/spirituality and adolescent
psychiatric symptoms: A
review. Child Psychiatry and
Human Development, 39(4), 381–
398.
Dow J. Universal Aspects of Symbolic
Healing: A Theoretical Synthesis.
American anthropologist 1986, 88
(1): 56-69.
Frazier, R. E., & Hansen, N. D. (2009).
Religious/spiritual psychotherapy
behaviors: Do we do what we
believe to be important?
Professional Psychology: Research
and Practice, 40, 81–87.
Hathaway, W. L., Scott, S. Y., & Garver,
S. A. (2004). Assessing
religious/spiritual functioning: A
neglected domain in clinical
practice? Professional Psychology:
Research and Practice, 35, 97–104.
Hayes, J.A; McAleavey A.A; Castonguay
L.G; Locke B.D. (2016).
Psychotherapists’s Outcomes with
White and Racial/Ethnic Minority
Clients: First, The Good News.
Journal of Consulting Psychology,
63 (3): 261-2681.
Hill, P.C.; Pargament, K.I.; Hood, R.W.;
McCullough, J.P.; Swyers, D.B.;
Larson, D.B.; Zinnbauer, B.J.
(2000). Conceptualizing Religion
and Spirituality: Points
Commonality, Points of Departure.
Journal for the Theory of Social
Behaviour. 30: 51-77.
Hill, P. C., & Pargament, K. I. (2008).
Advances in the conceptualization
and measurement of religion and
spirituality: Implications for
physical and mental health
research. Psychology of Religion
and Spirituality, S (1), 3–17.
Hodge, D.R. (2006). Spiritually modified
cognitive therapy – a review of the
literature. Social Work. 51 (2): 157-
166.
James, L (2016). Carl Jung and alcoholic
anonymous: is a Theistic
psychopathology feasible? Acta
psychopathologica. 2 (1): 7.
Kennedy, G. A., Macnab, F. A. & Ross, J.
J. (2015), The effectiveness of
spiritual/religious interventions in
psychotherapy and Counselling: a
review of the recent literature.
Melbourne: PACFA.
Meltzoff, J; Kornreich, M. (1970).
Research in psychotherapy. New
Uwakwe, R. (2020). Integration of Spirituality into Psychotherapy –
A Potential Model For Nigeria, International Journal for Psychotherapy in Africa 5(1):98-107
107
York: Atherton, 1 Nolan, P.;
Crawford. P. (1997). Towards a
rhetoric of spirituality in mental
health care. Journal of Advanced
Nursing, 26: 289-294.
Okon, E. E. (2012). Critical reflections on
Freudian theory of religion.
Research on humanities and social
sciences. 2 (10): 103- 109.
Pearce, J., Koenig, H. G.; Robins, C. J.;
Nelson, B.; Shaw, S. F.; Cohen, H.
J.; King, M. B. (2015). Religiously
integrated cognitive behavioral
therapy: A new method of treatment
for major depression in patients with
chronic medical illness.
Psychotherapy, 52(1): 56-66.
Peres, J.F.P, Smao J.P, Nasello A. G.
(2007). Spirituality, religiousness
and psychotherapy. Archives of
clinical psychiatry. 34
(Supplementary). 1: 136-145.
Pew Research. (2008). Pew forum on
religion and public life: Religion and
public life project. Available
at http://www.pewforum.org/2008/0
6/01/u-s-religious-landscape-survey-
religious-beliefs-and-practices/
Plante, T. G. (2016). Principles of
incorporating spirituality into
Professional clinical practice.
Principles of incorporating
spirituality into professional clinical
practice. Practice Innovations. 1 (4):
276-281.
Post, B. C, Wade, N. G. (2009). Religion
and Spirituality in Psychotherapy: A
Practice-Friendly Review of
Research Article. Journal of Clinical
Psychology. 65: 131-146.
Susanto, S. & Idris, S. (2017). Ar-Ramiry
International Journal of Islamic
studies, 4 (1): 55-70.
Toftegaard, K. L; Gustafsson, L.N;
Uwakwe, R; Andersen, U. A;
Becker, T; Bickel, G. G ; Bork,
B; Cordes, J; Frasch, K; Jacobsen ,
B. A; Kilian, R; Larsen, J. I;
Lauber, C; Mogensen, B; Rössler,
W; Tsuchiya, K.J; Munk-Jørgensen,
P. (2015). Where are patients who
have co-occurring mental and
physical diseases located?
International Journal of Social
Psychiatry, 61 (5): 456- 464.
Uwakwe, R; Otakpor A. N. (2014). Public
Mental Health- Using the Mental
Health Action Program to put all
hands to the pumps. Frontiers in
Public Health, 2: 33.
Worthington Jr. E.L., Kurusu, T.A.,
McCullough, M.E., & Sandage, S.J.
(1996). Empirical research on
religion in counseling: A 10-year
review and research prospectus.
Psychological Bulletin. 119: 448–
487.
Acknowledgments: I thank Prof. S.N.
Madu, Ven. Dr. G.O Madubuike and Rev.
Sr. Dr. C. Ekwe for their critique of the
initial draft.
Richard.

International Journal for Psychotherapy in Africa (5:1)
108
English Language Students And Their Coping Styles
During Lockdown As A Result Of The Novel
Coronavirus 2019 (Covid-19) Global Pandemic
Bridget Ngozi Madu
Department of English,
Chukwuemeka Odumegwu Ojukwu University,
P.M.B 6059 Igbariam Campus, Nigeria.
Abstract The author examined the effective and ineffective coping mechanisms of English
language undergraduate students during the total lockdown in Nigeria as a result of the
Corona Virus (COVID-19) global pandemic. The participants in the study were twenty
undergraduate students of English language in a state university. The students were
interviewed on telephone on their coping styles during lockdown as a result of the
COVID-19 global pandemic. Their responses were recorded on the phone, transcribed,
and thematically analysed using qualitative methods. Results show that they used such
effective coping mechanisms as having a positive attitude towards the lockdown, and
therefore used the opportunity for reading novels, writing poems, playing and dancing
music at home, and painting/drawing. Other effective coping activities reported were:
Having quiet moments for meditation and prayers, home physical exercises and aerobic,
sleeping/resting, watching television and movies, gardening/farming, family
bonding/reunion, and expected/desired pregnancy. Some of them also reported some
ineffective ways of coping, such as denial of reality of COVID-19, feeling anxious,
boredom/loneliness, weight gained, substance abuse/use, domestic violence, unwanted
pregnancy, longing for intimate sexual partner, being angry with the governments
because of food-shortage/starvation, and obsessive-compulsive behaviour. The author
concludes that the effective coping mechanisms would enhance their proficiency in
English language, and should be encouraged; while the ineffective ways of coping would
definitely be detrimental to their future professions and life in general, and should be
discouraged.
Key words: English language students, Lockdown, COVID-19, Coping strategies,
Nigeria.
Introduction
The corona virus (COVID-19) which
started in China in December 2019
quickly spread over the whole world
within a few months, infecting and killing
thousands of people in many parts of the
world (Africa CDC, April 13, 2020;
Nigerian Centre for Disease
Control/NCDC, 2020). In order to control
the spread of the deadly virus, most
countries of the world embarked on total
lockdown. In Nigeria, the total lockdown

Madu, B.N. (2020). English Language Students and their Coping Styles During Lockdown as a
Result of the Novel Coronavirus 2019 (Covid-19) Global Pandemic,
International Journal for Psychotherapy in Africa 5(1):108-115
109
was enforced on 30th March 2020. Like in
most countries of the world, all schools,
churches, mosques, airlines, businesses
(except for food and vegetable sellers)
were closed. There were no inter-country,
inter-state, or inter-town movements. In
many cases, people were not even allowed
to come out of their homes or flats (except
for those on essential duties like nurses,
medical doctors, and police). People were
compelled to stay at home for months,
depending on when the country declared
its own total lockdown. This unexpected
lockdown was never experienced before
by most living citizens of the world.
Students in secondary and tertiary
institutions, who were mostly teenagers or
young adults, must have experienced the
lockdown in a special way. For young
people who are full of life and energy, and
some with mood swings, all of a sudden to
sit at home without knowing when the
lockdown will end, can be devastating.
This made the author to investigate the
coping strategies of English language
students during the lockdown. The author,
being a lecturer of English language in a
university, had telephone contacts of some
of her students; thus she decided to limit
her investigation to English language
students.
The aim of the study therefore was
to investigate the experiences of English
language students during the COVID-19
total lockdown in Nigeria and their coping
mechanisms.
Lahey (2009: 456-459) grouped
coping with stress into two: Effective
coping and Ineffective coping. Under
effective coping are removing or reducing
the source of stress, cognitive or attitude
change, and managing stress reactions.
While ineffective coping strategies are
withdrawal from the society or
environment (social isolation), aggression
(like domestic violence), self-medication
(like using drugs to forget the stressful
situation), and defense mechanisms like
denial of reality (as suggested by Freud,
1949). Lahey’s view on coping with stress
is the theoretical framework adopted for
this work.
Literature review shows that many
authors from different parts of the world
have reported the experiences of
university students and the general public
during lockdown as a result of the
COVID-19 pandemic. Some of the authors
reported that their respondents felt more
worried, depressed, were preoccupied with
the idea of contracting the virus, had sleep
disturbances, and felt their existence was
being threatened (Chakraborty &
Chatterjee, 2020). Spanish Arts,
Humanities, and Social Science students
also expressed higher levels of anxiety,
depression, and stress more than
Engineering and Architecture students
(Odriozola-Gonzalez, Plachuelo-Gomez,
Irurtia, & de Luis-Garcia (2020). See also
similar report about Veterinary students in
England Yiannouli, 2020). In the U.S.,
Schildkraut, Nickerson and Ristoff (2020)
reported of fear and anxiety among
students. Similar to reports from other
authors, Mucci, Mucci, Diolaiuti (2020)
reported feeling of uncertainty, fear,
despair, stress, sleep disturbances,
depressive symptoms and suicidal ideation
among their participants in Italy. Also, in
Italy, Galle, Sabella, Da Molin, De Giglio,
et al. (2020) reported complaints of
decreased physical activities among Life
Science Degree Students; and Cellini,
Canale, and Mioni (2020) reported of
sleep difficulties (lower sleep quality),
depression, anxiety, and stress symptoms
International Journal for Psychotherapy in Africa (5:1)
110
among their participants. None of the
above studies were conducted in Nigeria,
and none of them focused on English
language students.
The author therefore set out for the
study with the following two objectives: 1. To find out the effective ways the
English language students are using
to cope with the unusual mandatory
lockdown.
2. To find out the ineffective ways the
English language students are using
to cope with the unusual mandatory
lockdown.
Method
This study used the qualitative research
method where 20 key informants (English
language students) are interviewed
through telephone call and their responses
analysed using thematic method of data
analysis (De Vos, Strydom, Fouche, &
Delport, 2002).
The participants (key informants)
interviewed were 20 English language
students of a State University in Nigeria.
There was no distance learning or online
education system in the university.
Because of the lockdown as a result of the
COVID-19 pandemic, the students had to
be interviewed on telephone. The
interview took place between 29th and 30th
April 2020 (that is, one month after the
total lockdown was enforced in Nigeria).
The author, using the Departmental record
selected 5 students at each undergraduate
level (100-400 levels) and contacted them.
The method of selection was simple
random sampling.
The researcher first of all called each
student using a cell-phone (handset),
explained the nature and purpose of the
research to him/her, assured him/her of
confidentiality and anonymity, and sought
oral consent from him/her to participate in
the study. Any student who did not agree
to participate in the study would have been
left out, but all of them agreed to
participate.
A topic guide which has the
following question was used for the
interview: “How are you coping with the
total lockdown due to the corona virus
pandemic?” Their responses were
recorded on the phone. The recorded
responses were transcribed and
thematically analysed, to find out their
effective, as well as, ineffective ways of
coping with the situation.
Result
The following themes emerged as a result
of the thematic analysis of the transcribed
interviews responses: a) Effective coping mechanisms:
1. Change of perception and
attitude towards the lockdown.
Many of the students saw the
lockdown as a necessity to
save their lives and that of
others. One of the students
said “Doc, it is better for us to
sit at home and be alive than to
go to school and die”.
2. Opportunity for reading
novels: Some of the students
used the period to read novels
which they did not have time
to read before because the
hectic nature of their
university activities. One
student said “I have even
Madu, B.N. (2020). English Language Students and their Coping Styles During Lockdown as a
Result of the Novel Coronavirus 2019 (Covid-19) Global Pandemic,
International Journal for Psychotherapy in Africa 5(1):108-115
111
finished reading one novel I
have been wishing to read”.
3. Writing poems: One boy said
“I am good in writing poems,
so I have written some during
this lockdown”.
4. Playing and dancing music at
home. One student said “I
have been playing and dancing
rock music everyday”.
5. Painting/drawing: Two
students said they are good in
painting and drawing; so they
are keeping themselves busy
with paintings and drawings.
6. Having quiet moments for
meditation and prayers. One
girl said “It has been a good
opportunity for me to have
quiet moments and pray to my
God”.
7. Home physical exercises and
aerobic. Another girl said “I
am enjoying having time for
my physical exercises at home
and aerobic. I also at times
walk around our compound”.
8. Sleeping and resting: One girl
said: “I sleep, sleep and sleep.
I have not had such a rest in a
long time. The last time I had
siesta was in my boarding
(secondary) school”.
9. Watching Television and
movies: Many students said
they often watch TV and
movies. One student said, “I
am enjoying my African
Magic day and night”.
10. Gardening/farming: Some
students said that this is
farming season, so they are
helping their parents in
farming/gardening. “We
cultivate cassava” a student
said.
11. Family bonding/reunion: One
girl said “This is the first time
all my brothers and sisters are
staying at home chatting and
playing with each other. We
get to know each other better”.
12. Expected/desired pregnancy:
One lady said “I have been
married and living in the same
house with my husband for
four years and I am a day-
student, but I could not
conceive a child. Now, during
this lockdown, I don’t know
how it happened. I am
pregnant”.
b) Ineffective coping mechanisms:
Some students however reported the
following ineffective ways of coping with
the lockdown:
1. Denial of reality: Some boys
do not believe that the corona
virus is a reality. One boy said:
“It is all about politics! They
(the government) are all
deceiving us! They want to
make money with this issue. It
is not real”.
International Journal for Psychotherapy in Africa (5:1)
112
2. Feeling anxious: One girl said,
“I am always feeling anxious
and suspicious of everybody
because I do not know who is
carrying this virus and who is
not. I can’t even sleep well
again”.
3. Boredom: Some students
experienced the period as very
boring. One student said “The
thing (lockdown) is just boring
me”.
4. Weight gained: One girl said
“I eat and eat and eat. I have
even gained a lot of weight”.
5. Substance abuse/use: One boy
said “I am now smoking and
drinking (alcohol) more than
before”.
6. Domestic violence: Some
ladies said: “It is like we are
quarrelling everyday at home.
I want this thing (lockdown) to
end so that we go our different
ways again”.
7. Unwanted pregnancy: One
lady said “I already have three
children and I did not want
more. But now the lockdown
has made me to be pregnant
again”.
8. Longing for intimate sexual
partner: One boy said, “My
girlfriend is living in another
State and I cannot meet her
(for sex) due to the lockdown.
This thing (lockdown) should
stop so that I go and meet her.”
9. Angry with the governments
because of food shortage/
starvation: Some students are
angry with the governments
for forcing their parents who
are business men/women to sit
at home and do nothing; while
they (the governments) did not
provide enough palliatives to
cushion the effect of the
lockdown. One student said:
“Look at America and other
countries; they provide enough
food and drinks to people
every day. They bring them to
their door-steps. Watch your
TV and see what I am saying.”
10. Obsessive-compulsive
behaviour: One girl said, “I am
always washing my hands for
fear of contacting the virus. I
wash my hands almost every
five minutes, even though I am
at home. I cannot stop doing it.
It’s too bad.”
Discussion
As English language students, it is a
desired finding to see that the participants
in this study used such effective coping
mechanisms (Lahey, 2009) as having a
positive attitude towards the lockdown,
and therefore used the opportunity for
reading novels, writing poems, playing
and dancing music at home, and
painting/drawing. These activities would
enhance their proficiency in English
language. None of the literature reviewed
reported of any effective coping activity
among students.

Madu, B.N. (2020). English Language Students and their Coping Styles During Lockdown as a
Result of the Novel Coronavirus 2019 (Covid-19) Global Pandemic,
International Journal for Psychotherapy in Africa 5(1):108-115
113
Other effective coping activities
engaged by participants in this study are:
having quiet moments for meditation and
prayers, home physical exercises and
aerobic, sleeping/resting, watching
Television and movies, gardening/
farming, family bonding/reunion, and
expected/desired pregnancy. These are
desirable coping style which may not be
unique to English language students.
Again, none of the literature reviewed
mentioned any of the coping mechanisms.
Besides the above-mentioned
effective coping mechanisms used by the
English language students who
participated in this study, some of them
also reported some ineffective ways of
coping (Lahey, 2009), such as denial of
reality of COVID-19, feeling anxious,
boredom/loneliness, weight gained,
substance use/abuse, domestic violence,
unwanted pregnancy, longing for intimate
sexual partner, being angry with the
governments because of food shortage/
starvation, and obsessive-compulsive
behaviour. Freud (1949) referred to denial
of reality as a form of defense mechanism
with which the Ego protects itself from a
form perceived threat. Current literature
search also shows that many authors have
also reported similar ineffective coping
mechanisms among their participants.
Some of them reported that their
respondents felt more worried, depressed,
were preoccupied with the idea of
contracting the virus, had sleep
disturbances, and felt their existence was
being threatened (Chakraborty &
Chatterjee, 2020). Spanish Arts,
Humanities, and Social Science students
also expressed higher levels of anxiety,
depression, and stress more than
Engineering and Architecture students
(Odriozola-Gonzalez, Plachuelo-Gomez,
Irurtia, & de Luis-Garcia, 2020;
Yiannouli, 2020). In the U.S., Schildkraut,
Nickerson and Ristoff (2020) also reported
of fear and anxiety among students.
Mucci, Mucci, and Diolaiuti (2020)
reported feeling of uncertainty, fear,
despair, stress, sleep disturbances,
depressive symptoms and suicidal ideation
among their participants in Italy; Galle,
Sabella, Da Molin, De Giglio, et al. (2020)
reported complaints of decreased physical
activities among Life Science Degree
Students; and Cellini, Canale, and Mioni
(2020) reported of sleep difficulties (lower
sleep quality), depression, anxiety, and
stress symptoms among their participants.
The above ineffective ways of coping with
the lockdown are not good for anybody,
not to talk of students who are still young
and growing. The ineffective ways of
coping will definitely be a setback in their
future profession and life in general.
Conclusion
It is concluded that English language
students who participated in this study
used such effective ways of coping with
COVID-19 pandemic such as having a
positive attitude towards the lockdown,
and therefore read novels, wrote poems,
played and danced music at home, and
painted/drew pictures. These activities
must have enhanced their proficiency in
English language. The students also
reported some ineffective ways of coping
such as denial of reality of COVID-19,
feeling anxious, boredom/loneliness,
weight gained, substance abuse/use,
domestic violence, unwanted pregnancy,
longing for intimate sexual partner, being
angry with the governments because of
food shortage/starvation, and obsessive-
compulsive behaviour. The ineffective
ways of coping will definitely be a setback
International Journal for Psychotherapy in Africa (5:1)
114
in their future profession and life in
general.
Recommendation
While we wish that such a total lockdown
due to COVID-19 pandemic would not
repeat itself in our lifetime, it is
recommended that English language
students (in Nigeria) are made aware of
the desired effective ways of coping with
such lockdowns in the future. They should
also be discouraged from using the
ineffective ways as reported by many
authors.
Future studies should use English
language students from many other
universities as participants. That would
increase the external validity of the
findings. A comparison of the coping
styles of English language students and
that of other students would be interesting.
Also, a study design that triangulates both
quantitative and qualitative methods is to
be encouraged.
References
Africa Centre for Disease Control and
Prevention (Africa CDC) (2020).
COVID-19 case update, 13th April
2020. Addis Ababa, Ethiopia: Africa
CDC.
Cellini, N., Canale, N. & Mioni, G.
(2020). Changes in sleep pattern,
sense of time and digital media use
duringCOVID-19 lockdown in Italy.
Journal of Sleep Research.
Electronic publication, May15,
2020, e13074.
Chakraborty, K. & Chatterjee, M (2020).
Psychological impact of COVID-19
pandemic on general population in
West Bengal: A Cross-sectional
study. Indian Journal of Psychiatry,
62, 3, 266-272.
De Vos, A.S., Strydom, H., Fouche, C.B.
& Delport, C.S.L. (2002). Research
at grass roots: For social science
and human service professions.
Pretoria: Van Schaik.
Freud, S. (1949). A general introduction to
psychoanalysis. New York: Garden
City Publishing.
Galle, F., Sabella, E.A., Da Molin, G., De
Giglio, O., Caggiano, G., Di
Onofrio, V., Ferracuti, S.,
Montagna, M. T., Liguori, G. Orsi,
G. B. & Napoli, C. (2020).
International Journal of
Environmental Research and Public
Health, 17(10), Electronic
publication, May 16, 2020.
Lahey, B. B. (2009). Psychology: An
introduction. Boston: Mc Graw Hill.
Mucci, F., Mucci, N. & Diolaiuti, F.
(2020). Lockdown and isolation:
Psychological aspects of COVID-19
pandemic in the general population.
Clinical Neuropsychiatry, 17(2), 63-
64.
Nigerian Centre for Disease Control
(NCDC) (2020). COVID-19 case
update (11.50pm, 19/04/20).
Twitter/Facebook:@NCDCgov/Covi
d19.NCDC.gov.ng. Accessed
19/04/20.
Odriozola-Gonzalez, P., Plachuelo-
Gomez, A., Irurtia, M.J. & de Luis-
Garcia, R. (2020). Psychological
effects of COVID-19 outbreak and
lockdown among students and
workers of a Spanish university.
Psychiatry Research, 290, 113-128.
Schildkraut, J., Nickerson, A.B. &
Ristoff, T. (2020). Locks, lights, out
of sight: Assessing students’
perceptions of emergency
preparedness across multiple

Madu, B.N. (2020). English Language Students and their Coping Styles During Lockdown as a
Result of the Novel Coronavirus 2019 (Covid-19) Global Pandemic,
International Journal for Psychotherapy in Africa 5(1):108-115
115
lockdown drills. Journal of School
Violence, 19(1), 93-106.
Yiannouli, A. (2020). How is the
lockdown affecting Vet students?
The Veterinary Record, 186(16), e5.

International Journal for Psychotherapy in Africa (5:1)
116
Genuineness In Client Centered Psychotherapy:
It’s Relevance To The Nigerian Society During
The Convid-19 Global Pandemic
Promise Chinedu Uwakwe
Department of Psychology,
Imo State University, Owerri, Nigeria.
Abstract In this paper, the concept of genuineness, as expressed by Carl Rogers in Client-
Centered Psychotherapy, is the platform on which efforts of some Nigerian citizens and
governments to curb the spread of corona virus (COVID-19) is discussed. The
genuineness in seeing COVID-19 as real, the political goodwill, the sincerity in
administering the COVID-19 funds, in carrying out the internationally mapped out
measures to contain the virus, and in the distribution of the palliatives to cushion the
adverse effects of the lockdown, are questioned. A call for attitudinal change on the part
of the concerned citizenry and the governments are therefore made.
Key words: Genuineness, Client-Centered Psychotherapy, Corona Virus (COVID-19),
Nigeria.
Introduction
Genuineness remains an important
condition for a good insight into the
authenticity of life variability, especially
regarding psychological well-being.
Changeability is one oblivious reality of
life and most times fundamental to the
incongruence faced by many (Crowell,
2016). As humans grow and develop in
the biological and psychological domain,
lots of challenges are experienced
consequent to the inherent changes
accompanying these developments.
Genuineness is a vital ingredient applied
in creating an enabling atmosphere for
individuals to gain superior insights into
their challenges in a psychotherapeutic
engagement. In problem solving, it can be
said that clear insights into the indices of
human challenges are essential to the
effective management and/or helpful in
sorting life predicaments or changes
successfully. Genuineness is perceived as
the unadulterated and congruent external
display of an individual’s actual internally
recognized values, beliefs, emotions, and
other perceptions of themselves including
the world they exist in (Crowell, 2016).
In psychotherapy, assiduous efforts
are made through the application of
psychological methods that helps a person
change behavior and overcome problems
in desired ways (APA, 2016).When
individuals enter therapy, they are in a
state of incongruence, meaning there is a
difference between how they see

Uwakwe, P.C. (2020). Genuineness In Client Centered Psychotherapy:
It’s Relevance To The Nigerian Society During The Convid-19 Global Pandemic,
International Journal for Psychotherapy in Africa 5(1):116-121
117
themselves and reality (Lietaer, 2001). But
through the reflection of genuineness by
the therapist, the individual tends to find
reasons to be genuine to his or herself and
by extension other persons around.
Psychotherapy aims to improve an
individual's well-being and mental health,
to resolve or mitigate troublesome
behaviors, beliefs, compulsions, thoughts,
or emotions, and to improve relationships
and social skills (Grafanaki, & McLeod,
2002).
As a behavioral healing principle or
condition, genuineness should be prized
highly, cultured and promoted at all cost
and by any well-meaning government or
institution with the goal of behavioral
harmony. This highlights the necessity of
creating enabling environment for such
social services as psychotherapy to thrive,
since it is bound to eliciting genuineness
from individuals and society.
It is therefore unarguable that
genuineness is a useful tool for survival in
the face of the current Corona Virus
(Covid-19) pandemic, where many
persons have become confused,
traumatized, anxious, fearful, and many
other emotionally disturbing conditions
experienced by many in the Nigerian
society. Thus, psychotherapy, principled
in genuineness, has been shown to be
helpful in reaching the etiology of the
individual’s emotional and behavioral
challenges and key to positive thinking
(Karlsson, 2011).
In Nigeria, the imposition of total
lockdown across the country, as measure
to inhibit the spread of the Corona virus
(Covid-19) pandemichas forced millions
of people to stay at home, restricting their
mobility and pushing them to increase
screen time (Adebajo, 2020).
Corona virus is a spherical or
pleomorphic, single stranded, enveloped
RNA and covered with club shaped
glycoprotein. Corona viruses are of four
sub- types such as Alpha, Beta, Gamma
and Delta Corona virus. Each of the sub-
types of Corona viruses have many
serotypes. Some of them affect human
while others affect animals such as pigs,
birds, cats, mice and dogs (ICTV, 2020).
The adverse situation created by
Covid-19 has led many to call on Nigerian
and African leaders to adapt their Corona
virus response measures to the realities on
the ground (Adebajo, 2020). But the
measures applied by the Nigerian
government seem to lack sensitivity and
sincerity and seem not to be truly survival
oriented. As these measures such as:
shutdown of economy without proven
palliatives, sensitization of the masses,
payment of wages/salaries in some part of
the country, establishment of Covid-19
intervention team/committee without strict
follow-up on their actions and activities,
setting up of Covid-19 quarantine centers
with no sensitization program involving
mental health workers to work against
phobia and stigmatization (BBC News,
2020), tend to reflect the proven survival
narrative of a typical Nigerian society in
the face of outbreaks. This situation can be
described as lacking genuineness in
content and intent.
However, this work expresses the
need for the Nigerian society to adopt and
domesticate her own model for the fight
against Corona virus to the unique
Nigerian personality, culture, social
construct, belief system etc, as it attempts
to reflect the relevance of genuineness in
the Nigeria society in the ongoing global
covid-19 pandemic.

International Journal for Psychotherapy in Africa (5:1)
118
Since the first index confirmed case
relating to the COVID-19
pandemic in Nigeria on 27 February 2020
when an Italian citizen in Lagos tested
positive for the virus, caused by SARS-
CoV-2 (Olurounbi, 2020 ), the Nigeria
society has continued to be in panic and
confusion as the pandemic expresses itself
in bereavement for those who have lost
their dear ones to the virus and phobia for
socialization as the government tries to
clamp down on social gathering in other to
foster social distancing as prescribed by
World Health Organization. As
precautionary measures adopted against
the spread of the virus are being
implemented, there has been increase in
assaults and molestations by Covid-19 law
enforcement agents across many
settlements in Nigeria. According to
health ministry data, Covid-19 law
enforcers have killed 18 people in Nigeria
since lockdowns began on 30 March 2020
(BBC News, 2020). Another overt impact
of the Covid-19 pandemic in Nigeria is
hunger and starvation. Unlike many other
countries going through the shock of
Covid-19 pandemic, the Nigerian society
seems not to have an accurate data of
palliatives intervention to help masses
cushion the terrible effects of the
pandemic (Adebajo, 2020). Consequently,
many persons have become financially
bankrupt, since meeting survival needs
like food, health care, accommodation
bills (house rent, water supply bill,
electricity bill has become a problem. This
asks the question of sincerity and
genuineness in the attitude of the Nigerian
government towards properly addressing
the problem of Covid-19 pandemic.
Background to the concept of
Genuineness
The person-centered approach was
developed from the concepts of
humanistic psychology. The humanistic
approach “views people as capable and
autonomous, with the ability to resolve
their difficulties, realize their potential,
and change their lives in positive ways”
(Seligman, 2006). Rogers (1942),
advanced an approach to psychotherapy
and counseling that, at the time (1940s–
1960s), was considered extremely radical
if not revolutionary. Carl Rogers
emphasized the humanistic perspective as
well as ensuring therapeutic relationships
with clients promote self-esteem, and
actualization in their life, and help them to
use their strengths (Seligman, 2006).
The theory is described as non-
directive. This concept moved away from
the idea that the therapist was the expert
and towards a theory that trusted the
innate tendency of human beings to find
fulfillment of their personal potentials. An
important part of this theory is that, in a
particular psychological environment, the
fulfillment of personal potentials includes
sociability, the need to be with other
human beings and a desire to know and be
known by other people. It also includes
being open to experience, being trusting
and trustworthy, being curious about the
world, being creative and compassionate.
The psychological environment described
by Rogers was one where a person felt
free from threat, both physically and
psychologically. This environment could
be achieved when being in a relationship
with a person who was deeply
understanding (empathic), accepting
(having unconditional positive regard) and
genuine (congruent) (Wendera, et al
2008).

Uwakwe, P.C. (2020). Genuineness In Client Centered Psychotherapy:
It’s Relevance To The Nigerian Society During The Convid-19 Global Pandemic,
International Journal for Psychotherapy in Africa 5(1):116-121
119
The psychotherapists in this approach
works to understand an individual’s
experience from their point of view. The
psychotherapist must positively value the
client as a person in all aspects of their
humanity, while aiming to be open and
genuine as another human being. This is
vital to helping an individual feel accepted
and better understands their own feelings,
essentially helping them to reconnect with
their inner values and sense of self-worth.
This connection with their inner resources
enables them to find their own way to
move forward. The work of the therapist,
therefore, is to facilitate this by creating an
enabling environment for client to find the
solution to his or her problems. The
therapist does not try directing the client
or offering solutions. Roger’s proposition
was that, any relationship possessing the
conditions, would produce psychological
change within the client, irrespective of
whichever psychological approach was
employed.
Genuineness or Congruence requires
the therapist to be transparent about his or
her feelings and thoughts. He or she does
not present an aloof professional facade,
but is present and transparent to the client
in the sense that, he or she expresses
feelings and thoughts that he or she
actually experiences rather than those he
or she thinks. This will help the client
open up. In this regard, the therapist may,
sometimes, share his or her personal
experiences with the client. The aim of
this is to make the client comfortable
enough to become genuine and fully
express him or herself (Rogers, 1959).
Genuineness and its relevance to the
Nigerian society amidst the Covid-19
global pandemic
Many people in some Nigerian societies
are said not to be genuine. They are
fraudulent, untruthful, deceitful,
untrustworthy and unreliable. What of the
so called “419” people, the scammers,
fraudsters etc. Even in this period of
Covid-19 pandemic, the Nigerian society
can be said to witnessing manifold levels
and forms of insincerity.
Many individuals and even some
church leaders are denying the reality of
Covid-19 (Adebayo, 2020; Jideonuo,
2020). They are not genuinely spreading
the news that putting on face mask,
washing/sanitizing hands often, and
maintaining social/physical distancing
would assist in curing the spread of the
virus.
However, with all these opposing
trait to genuineness, it can be said that
many religious leaders in Nigeria have
need to review their value system by
adopting the principle of genuineness in
modifying their cognition and personality
so as to front more sincere and helpful
paradigm that can enable the government
and masses survive the Covid-19
pandemic or any other pandemic in later
times.
Similarly, some Nigerian political
activities point to traces of insensitivity,
insincerity, manipulations,
unaccountability, dishonesty, greed, fraud
and other manner of spurious behavioral
tendencies to lack in genuineness and fair
play for everyone. Some evidence to lack
of genuineness in the political
activities/system during the pandemic
includes: 1. Non-transparent records on the of
Covid-19 funds.
International Journal for Psychotherapy in Africa (5:1)
120
2. Insincerity in the disbursement of
Covid-19 funds by the Federal and
state governments.
3. Inconsistent/conflicting information
on the causes (etiology and
precursor) of Convid-19 pandemic.
4. Inconsistent/conflicting information
on the outbreak statistic/update.
5. Compromises on the mapped out
measures to curb the spread of
Covid-19.
6. Dissatisfaction of the masses in
quantity, quality, and manner of
palliatives distributed to cushion the
adverse effects of the lockdown on
poor people.
7. Disbelieves in figures of infected
individuals as posited by Nigeria
Centre for Diseases Control
(NCDC).
Finally, an observation on attitude of
masses to the covid-19 pandemic in the
Nigerian, especial with regards to
commitment and adherence to
precautionary measures setup by the
governments, reveals huge dishonesty and
lack of corporation. In as much as the
governments make some efforts to
orientate and enlighten the masses on the
alarming dangers implicated with the
pandemic, it is noticed that many persons
seem to show little or no commitment to
the directives of the governments against
the spread of the virus. This is made
visible by the large scale of poor
commitment by many individuals in
adherence to wearing of face mask, the
stay at home bill, regular washing of
hands, and social distancing. This
predisposition can be classified as
dishonest in the sense that many of these
individuals who decline government
directives, do so merely to frustrate the
efforts of the government; and not
necessarily because they doubt the
information projected by the government
about the pandemic.
However, it has been established
with all these traits of insincerity,
selfishness, dishonesty, fraud /scamming
found in some Nigerians during the
pandemic, that there is huge lack of
genuineness found many Nigerians with
respect to curbing the spread of Cov0d-19
pandemic. When genuineness is a seldom
character within the government of a
given society, the citizens see that as a
model. When one is not genuine to
him/herself, he/she cannot be genuine to
the environment. Not being genuine leads
to many psychological problems. Durđa
(2017) posits that genuineness
(authenticity) is closely connected to
mental health and significantly contributes
to it. Therefore, genuineness in Client
Centered Therapy has vital a role to play
among such societies that are said to be
fraudulent, corrupt, inconsiderate
especially, during a pandemic situation
like the Covid-19.
Conclusion
Genuineness, as used in Client Centered
Psychotherapy, provided a platform on
which to question and discuss genuineness
of the part of some Nigerian citizens and
governments with respect to controlling
the spread of Covid-19 global pandemic.
The genuineness and sincerity in seeing
the virus as real; the genuine goodwill in
political, in social and financial efforts in
controlling the virus are questioned.
Attitudinal change in the entire populace
both on the part of some citizenry and
Uwakwe, P.C. (2020). Genuineness In Client Centered Psychotherapy:
It’s Relevance To The Nigerian Society During The Convid-19 Global Pandemic,
International Journal for Psychotherapy in Africa 5(1):116-121
121
some government in Nigeria are therefore
called for.
References
Adebajo K. (2020). COVID-19: Infodemic
Challenges the War Against The
Pandemic in Nigeria. Newsletters of
humble angle.online news feed.
APA (American Psychological
Association) (2016). Client centered
therapy. Retrieved from http://
apa.com, May 10, 2020.
BBC News (2020). BbcNews May 2020.
Retrieved from http:// bbcnews
.com.
Crowell, S. (2016). Existentialism. In E.
N. Zalta, (Ed.), The Stanford
encyclopedia of philosophy.
Retrieved from
http://plato.stanford.edu/archives/sp
r2016/entries/existentialism.
Durđa G. (2017). Authenticity as a
predictor of mental health. Research
Gate Journal 10.21465/2017-kp-1-
2-0002.
Grafanaki, S., & McLeod, J. (2002).
Experiential congruence: A
qualitative analysis of client and
counsellor narrative accounts of
significant events in time-
limited person-centred therapy.
Counselling and Psychotherapy
Research, 2(1), 20-33.
International Committee on Taxonomy of
Viruses (ICTV 2020).Taxonomy
history: Orthocoronavirinae.
Retrieved 24 January 2020.
Jideonwo C. Covid-19: There’s One Thing
Nigeria’s Religious Rockstars Can
Do To Help. Publication of African
Arguments.
Karlsson, H. How Psychotherapy changes
the Brain. Psychiatric Times. 2011
Lietaer, G. (2001). Being genuine as a
therapist: Congruence and
transparency. In G. Wyatt (ed.),
Rogers’ therapeutic conditions:
Evolution, theory and practice. Vol.
1.Congruence (pp. 36-54). Ross-on-
Wye, UK: PCCS Books.
Olurounbi R. (2020), Coronavirus: Nigeria
goes home for funds out of fear on
COVID-19 Impact. The Africa
Report Newsletter.
Rogers, C. (1959). A Theory of Therapy,
Personality and Interpersonal
Relationships as Developed in the
Client-centered Framework. In (ed.)
S. Koch, Psychology: A Study of a
Science. Vol. 3: Formulations of the
Person and the Social Context. New
York: McGraw Hill.
Rogers, Carl R. (1942). Counseling and
psychotherapy. Cambridge, MA:
Riverside Press. ISBN 978-
1406760873.
Wandera, J. (2008). Persons centered
therapy. Oxford University Press.
East Africa Ltd.

International Journal for Psychotherapy in Africa (5:1)
122
Gender Differences In Attitude To The Skin Disease-
Atopic Dermatitis Among Adolescents:
The Role Of Cognitive Behavioral Therapy
Charity Justin Takyun
Department of Psychology, Faculty of Social Sciences,
Federal University of Lafia, Nasarawa State, Nigeria.
Aleksandra Surenovich Kocharyan
Department of Counseling and Psychotherapy
Faculty of Psychology,
V.N. Karazin Kharkiv National University, Ukraine
Abstract This paper examines gender differences in attitude to the skin disease-atopic dermatitis
among adolescents: The role of Cognitive- Behavioural Therapy. 83 adolescents aged
between 13 and 15 and diagnosed with moderate (43) to grave (40) atopic dermatitis
took part in the study. The groups were divided according to gender; group 1 was made
up of 38 adolescent boys, and group 2 was made up of 45 adolescent girls. The control
group included 80 adolescents (40 girls and 40 boys) matched for age. The
psychodiagnostic complex used in the study were: Method for establishing the disease
attitude type (DAT) and Male and Female Painting projective test. Data were analyzed
using correlation and student’s t-test. The comparison of data yielded results that
indicate gender-specific types of attitude to the disease among adolescents diagnosed
with atopic dermatitis. A statistically significant difference between the groups was found
in the anosognosic disease attitude type that is more typical of adolescent boys. This
disease attitude type is characterized by active rejection of thoughts about the disease
and its consequences which is explained by boy’s bravado, by their wish to demonstrate
invulnerability and confidence, which is in effect an attempt to compensate for low self-
appraisal.
Key words: Atopic dermatitis among Adolescents, Gender differences, attitude to
Disease, CBT.
Introduction
The skin has many functions among which
are protection, thermoregulation, water-
salt exchange, excretion, blood pooling, as
well as endocrine, metabolic, receptor, and
immune functions. In addition to the
above physiological skin functions, it also
plays a psychological role – the skin is an
expression and self-presentation organ.
Skin diseases are therefore characterized
by their external noticeability and
concomitant skin itch. This characteristic

Takyun, C.J. & Kockaryan, A.S. (2020). Gender Differences in Attitude to the Skin Disease-Atopic
Dermatitis among Adolescents: The Role of Cognitive Behavioral Therapy,
International Journal for Psychotherapy in Africa 5(1):122-135
123
of skin diseases arises as a result of
psychic problems which in turn adversely
impact on the mental state of the patient,
thus leading to a vicious circle. Atopic
dermatitis is one of the most wide-spread
skin diseases occurring in different age
groups in both males and females in all
countries. According to the WHO, the
prevalence rate of atopic dermatitis is
constantly rising and is 6% to 25% in
different countries. It occurs significantly
more frequently in women. Atopic
dermatitis is more prevalent among the
citizens of large cities than amongrural
population. Usually manifesting itself at
an early age, atopic dermatitis soon
acquires a chronic recurrent course. The
discomfort related to severe itching leads
to the disruption of sleep, every-day life
and social activity which in turn requires
the application of psychological
intervention in order to change negative
and unrealistic faulty emotional
disturbances.
The adolescent stage of atopic
dermatitis is diagnosed in children above
13 years of age. It affects the face and
upper body parts and has a chronic
recurrent course (Smirnova, 2006).
Adolescence is usually characterized as a
critical and transitional age. It is regarded
as the most important and the most
difficult period of life characterized by
abrupt, rapid and critical events.
Adolescence is perceived as the second
birth, resulting in the emergence of a new
“self” (Averin, 2003; Cle, 1997;
Obukhova, 2003, & Polivanova, 1996).
Adolescence is accounted for by the
presence of a major need to be “satisfied
with one’s own appearance. (Mendelevich
& Solovyeva, 2002). Accordingly, the
adolescent thinks that other people are
equally concerned with their appearance
and behavior. This very belief was termed
in Reana (2003) as "imaginary audience",
and it is viewed as one of the main
manifestations of egocentricity in
adolescence. Adolescents persistently
attempt to predict others’ reactions to
themselves. However, these predictions
depend on adolescents’ self-attitude. In
their view, other people will treat them the
same way they treat themselves. Due to
these reasons, adolescents constantly
construct the "imaginary audience" with
themselves in the spotlight of attention.
The affect often experienced by
adolescents is “shame” as a reaction to
constant attention on the part of the
"imaginary audience". He or she view
acceptance by others as very important.
The acceptance of one’s own body
acquires a major interest. In the
adolescent’s view, “being attractive”
means having successful personal
relationships. Thus, the body becomes a
hostage of romantic relationships rather
than a value in itself. Sexual maturation
increases inner tension. Bodily appearance
and feelings become even more important
enhancing the possibility of intimate
relationship with a partner. Therefore,
when an adolescent evaluates his or her
body and detects physical defect, a
conclusion is drawn about his/her own
social inferiority. A desire may also arise
to compensate drawbacks in another field
or to try and improve them. Discomfort or
insults by people around regarding the
peculiarity of appearance can cause
violent affect and pervert the behavior of
the adolescent thereby causing traumatic
experiences.

International Journal for Psychotherapy in Africa (5:1)
124
The Role of Cognitive- Behavioral
Therapy (CBT) In Changing Thought
Pattern
As opined in Takyun, (2009), the major
challenge for mental health community is
to learn how best to help people who are
suffering from all forms of traumatic
experiences including emotional trauma.
Foa et al (1995), developed Brief
Cognitive-Behavioural Treatments which
include various forms of relaxation
therapy and education. Cognitive
restructuring is applied in CBT which
involves techniques for replacing
catastrophic, self-defeating thought
patterns with more adaptive, self-
reassuring statements. What sustains an
individual through the disease process is
the therapeutic alliance. Therapeutic
interventions attempts to restore not only
an individuals somatic and social balance
but also the sense of coherence. The use of
Cognitive Behavioral Therapy (CBT) is
aimed at changing negative and unrealistic
faulty reasoning because thinking
determines feelings, emotions and
behaviors.
Attitude to disease The reflection of a disease in a person’s
emotion is commonly called the internal
disease pattern (IDP). This term
encompasses everything “a patient feels
and experiences, all the multitude of
his/her feelings, the general sense of well-
being, self-observation, ideas about the
disease and its causes – the patient’s entire
huge world consisting of complex
combinations of perceptions and feelings,
emotions, affects, conflicts, psychic
experiences and traumas”. (Yeresko,
Isurina, & Koydanovskaya 1994; Amon,
2000). The term was first introduced by
the physician- Luria (1977) and is now
broadly used in medical psychology. As a
complex structural unit, the internal
disease pattern consists of several levels:
sensitive, emotional, intellectual,
volitional, and rational.
The IDP is determined not only by
the nosology, but also by the patient’s
personality, it is as individual and dynamic
as our internal world. There are a number
of studies describing how the patient
experiences his/her condition (Nikolaeva,
1987).
Mendelevich, (2005) states that the
type of reaction to a particular disease is
determined by two characteristics:
objective gravity of the disease (defined
by the mortality rate and disability
likelihood) and its subjective gravity (the
patient’s assessment of his/her condition).
Subjective gravity depends on social
and constitutional features including the
individual’s sex, age, and profession. Each
age group has a distinct disease gravity
register – a classification of diseases by
their socio-psychological significance and
gravity (Karvasarsky, 2002; Mendelevich,
2005). Thus, the most serious
psychological reaction in adolescence may
be caused by diseases that change the
adolescent’s appearance making him/her
unattractive. It is accounted for by the
presence of a major need to be “satisfied
with their own appearance” in
adolescents’ consciousness (Mendelevich,
2005).
The typology of disease reactions
includes 13 types of psychological disease
reactions distinguished based on three
factors: the nature of somatic condition,
the type of personality with the character
accentuation type being of major
importance, and disease attitude in the
referent (significant) group (Lichko, &
Ivanov, 1980):
Takyun, C.J. & Kockaryan, A.S. (2020). Gender Differences in Attitude to the Skin Disease-Atopic
Dermatitis among Adolescents: The Role of Cognitive Behavioral Therapy,
International Journal for Psychotherapy in Africa 5(1):122-135
125
1. Harmonic type: This reaction type
is characterized by sober evaluation
of one’s condition without the
inclination to overstate one’s
burden, but also without
underestimating the disease gravity.
The patient is willing to actively
contribute to the treatment. He or
she does not want to burden others
with the need for care. In case of an
unfavorable disability forecast the
individual shifts to the domains of
life that remain available. In case of
an unfavorable prognosis, attention,
care and interests are centered on
close relatives’ life and the patient’s
own business.
2. Ergopathic type. This reaction type
is characterized by “withdrawal
from “disease to work”. Excessively
responsible, sometimes obsessive,
volitional attitude to work is typical,
which is sometimes more
pronounced than attitude to the
disease. Selective attitude to
treatment caused by the desire to
continue work in spite of the disease
gravity. The desire to maintain
professional status and to continue
work in the current position by any
means.
3. Anosognosic type. This type is
characterized by active rejection of
thoughts about the disease, its
potential consequences, denial of
obvious disease signs, attributing
them to random events or other
transient conditions. Refusal of
medical examinations and
treatment, desire to do with one’s
own means.
4. Anxious type. This reaction type is
characterized by constant
nervousness and distrust to
unfavorable disease outcome,
possible complication treatment
inefficiency .The search for new
treatment methods, craving for
additional information about the
disease, possible complications and
treatment methods.
5. Hypochondriac type. This type is
characterized by an excessive focus
on subjective disease-related and
other negative feelings. An
inclination to always share them
with doctors, medical staff and
people around. Exaggeration of the
existing disease and the search for
non-existent diseases and sufferings.
Exaggeration of unpleasant
sensations associated with side
effects and diagnostic procedures.
The combination of willingness to
be treated and the disbelief in
treatment success. Constant demand
for thorough examination by
superior specialists. Fear of the pain
of procedures and possible harmful
effects,
6. Neurasthenic type. This type is
characterized by an “irritable
weakness” behavior. Outbursts of
irritation, especially when in pain
orin case of painful sensations,
treatment failures or unfavorable
examination findings. Irritation
often hits the nearest person and
often ends in remorse and tears.
Intolerance of pain sensations. Lack
of general tolerance. Inability to
wait for relief. Later, the feeling of
International Journal for Psychotherapy in Africa (5:1)
126
remorse for inconveniences and lack
of restraint.
7. Melancholic type. This type is
characterized by the feeling of
depression because of the disease,
disbelief in recovery, possible
improvement, or treatment effect.
Active depressive statements to
suicidal thoughts. Pessimistic view
of everything around, disbelief in
the therapeutic success even in spite
of positive evidence.
8. Apathetic type. This type is
characterized by complete
indifference to one’s fate, disease
outcome, and treatment results.
Passive compliance with procedures
and treatment when insistently
induced from outside. Loss of
interest to life and everything that
arouse interest before. Inertness and
apathy in behavior, activities and
interpersonal relationships.
9. Sensitive type. This type is
characterized by excessive concern
with possible ‘negative impression
and information about the disease.
Concerns that people around will
start avoiding and considering
inferior the person, treat with
contempt or apprehension, spread
gossip or unfavorable information
about the causes and nature of the
disease. Fear of becoming
burdensome to relatives and
resulting unfriendly relationships.
10. Egocentric type. This type is
characterized by "withdrawal into
disease", demonstration of the
feeling of suffering to relatives and
people around in order to capture
their attention. The demand for
exclusive care: everybody must
forget and leave everything just to
take care of the patient. Other
people’s conversations are quickly
turned to oneself. They require care
and attention from others, they only
see competitors and treat them in a
hostile manner. Constant desire to
show their particular condition and
uniqueness of the disease.
11. Paranoid type. This type is
characterized by the confidence that
the disease is a result of somebody’s
evil intention. Extreme
suspiciousness towards drugs and
procedures. Propensity to attribute
possible complications and side
effects of treatment to incompetence
or evil intention of doctors and
medical staff. Accusations and
demand of punishment in this
respect.
12. Dysphoric type. This attitude type is
dominated by angry, dismal, and
sullen mood and constantly gloomy
and dissatisfied appearance. Envy
and hatred towards the healthy,
including friends and relatives. Fits
of anger with an inclination to blame
the disease on others. Demand for
particular attention and
suspiciousness against procedures
and the therapy. Aggressive,
sometimes despotic attitude to
relatives, demand that everybody
should please them.
13. Obsessive-phobic type. This type is
characterized by fears that concern
unreal, unlikely disease

Takyun, C.J. & Kockaryan, A.S. (2020). Gender Differences in Attitude to the Skin Disease-Atopic
Dermatitis among Adolescents: The Role of Cognitive Behavioral Therapy,
International Journal for Psychotherapy in Africa 5(1):122-135
127
complications, treatment failures,
disease-related difficulties in life,
work or family; objects (talismans)
and rituals become protection from
phobias.
Dubrovina, (2008) investigated
disease attitude types in adolescents with
neurodermatitis. The disease duration was
between 10 and 17 years. The harmonic
type of disease attitude was absent in this
population, the euphoric type was
observed in 40.7% of cases, sensitive type
in 26.9%, anosognosic type also in 26.9%,
and mixed psychological reaction was
found in 51,9% of cases. Severe atopic
dermatitis characterized by deteriorated of
general condition, activity and mood,
increased personal anxiety and
intrapsychic behavioral patterns of mainly
anxious type, in authors’ opinion, this
demonstrate “withdrawal into disease”
among adolescents with atopic dermatitis.
Gender Differences in adolescents
It is at early school age that children start
interpreting contacts between girls and
boys as romantic and sexual (Isaev &
Kagan, 1979; Kagan, 1990, 1991). The
emergence of sexuality in relationships
between girls and boys is manifested
under conditions of sexual segregation.
Children of different genders have
different attitudes to sex and related
issues. Bendas, (2007) opined that, as a
result of conversations with children of
different sexes, it revealed gender
differences in attitudes to sex. Girls talked
willingly, used verbal constructions with
multiple details, demonstrated serious
reflection, whereas boys used short
phrases, jargons, and sexual slangs. Girls
draw information about sexual life from
the family, while the source of sexual
information for boys is their friends and
the mass media. Girls were more
interested in sexual relations between
people; they are afraid of psychic pain
from potential loss of a child and fear
early pregnancy. Boys were more
interested in the issues of contraception,
abortions, sexual intercourses, and
childbirth. Girls were more realistic
concerning career and family, they were
aware of the risks of alcohol consumption,
drug abuse and violence, whereas boys
demonstrated fearlessness and a humorous
attitude to sex and violence.
When sexual maturation begins in
adolescence, sexual segregation is ruined,
and the same happens to gender
confrontation. Boys and girls start
building new relations (Ilyin 2002). Man’s
role is traditionally instrumental and
action-oriented, and the woman’s role is
expressive and communicative. This is
evidenced by experimental data showing
that the masculine style is solution-
oriented, whereas women have either
expressive or mixed style. Mendelevich
(2005) and Kocharyan (2010) point to
women’s better tolerance of pain, long-
lasting movement limitation or
immobilization. In contrast to Bendas,
(2007) with data on better pain tolerance
in men and higher pain sensitivity in
women. Studies dealing with individual
diseases often contrast gender differences
in the mental course of the disease.
However, there is no comprehensive
systematization or classification of gender
differences in psychic reaction to a disease
as of present. At the same time, there is a
great amount of research dealing with
gender differences and its analysis
provides a solid foundation for studying
and analyzing gender differences in
disease reaction among adolescents

International Journal for Psychotherapy in Africa (5:1)
128
diagnosed with atopic dermatitis
(Golovneval, 2006; Kleitsina, 2004;
Vorontsov, 2008). Thus, literature
provides data on gender differences in
visual system development registered in
school age and adolescence. Males
outperform females in spatial perception
and chronometric indicators; females
develop earlier visual acuity and visual
estimation with the right eye. Attention
studies also demonstrate gender
differences. Thus, females outperform
males in voluntary attention. Females
focus more on the speed and males more
on the precision of the task, Males are
better at working with novel tasks and
females with patterns; females also outdo
males in communicative attention. Male’s
general intelligence has a clear structure
with predominant non-verbal component,
whereas female’s intelligence is poorly
integrated.
Females are more emotional than
males. It is evidenced by the following
empirical facts: Females are more anxious;
the link of emotions to interpersonal
relations is more significant for girls and
women than for boys and men; females
more often talk about negative emotions,
and positive emotions are experienced
more vividly; females are more prone to
depression; females are more sensitive to
negative events experienced by their
friends or relatives than male; females are
not a shame of demonstrating their
emotional reactions; females are more
precise about the non-verbal expression of
emotions; females are better at
recognizing emotional signals from other
people (Bendas, 2007; Heibrun, 1976;
Ilyin, 2002).
Greater emotionality in females is
evident by data about lower emotionality
in males: males do not like to show their
emotions, especially negative ones. They
are emotionally reserved even with same-
sex friends and are subject to strict social
regulations with regard to emotionality
demonstration. There are also male and
female emotions. It is anger for males and
sorrow and fear for females (Bendas,
2007)
Males show an advantage in terms
of the masculine aspect of self-evaluation,
whereas females in terms of the feminine
aspect. The shift of self-evaluation
towards narcissism in female is associated
with keenness on their appearance, and
with physical conditions and social status
in male. Females have less stable self-
evaluation than males. These differences
are influenced by the level of openness in
relations, reaction to the feedback, stress
caused by relations with relatives, and
protective mechanisms (Ilyin, 2002). Boys
and men outdo girls and women in open
physical aggression, whereas girls and
women are more prone to often resort to
hidden verbal aggression (Bendas, 2007).
The aim of this article is therefore to
assess gender differences in attitude to
disease among adolescents diagnosed with
the skin disease -Atopic Dermatitis and to
explore the role of Cognitive Behavioral
Therapy in changing thought pattern of
individuals experiencing emotional
disturbances.
METHOD
Participant’s characteristics
Participant’s characteristics include 83
adolescents aged between 13 and 15 and
diagnosed with moderate (43) to grave
(40) atopic dermatitis took part in the
study. The groups were divided according
to gender – group one (1) included 45
adolescent girls, and 38 adolescent boys

Takyun, C.J. & Kockaryan, A.S. (2020). Gender Differences in Attitude to the Skin Disease-Atopic
Dermatitis among Adolescents: The Role of Cognitive Behavioral Therapy,
International Journal for Psychotherapy in Africa 5(1):122-135
129
were in group two (2). The control group
included 80 adolescents (40 girls and 40
boys) matched for age. The participants
did not have complaints about the
psychological condition. However, the
patients showed irritability,
aggressiveness, tearfulness, low mood,
sub-depressive conditions, increased
anxiety, feeling of inferiority, disbelief in
treatment success, suspiciousness, sleep
disorders, asthenic conditions,
unwillingness to meet with peers; on the
contrary, they prefer to retreat into
themselves or a close circle of people.
These conditions did not reach a clinical
level so adolescent patients were not
examined by a psychiatrist.
Instruments & Procedure
The psychodiagnostic complex used
include the following methods:
Method for establishing the disease
attitude type (DAT) Male and Female
Painting projective test.
Method for establishing the disease
attitude type (DAT) (Wassermann L.I. et al
(2003) was developed at the Laboratory of
Clinical Psychology at V.M. Bekhterev
Institute. The method distinguishes
between 12 types of disease attitudes
grouped into 3 blocks. There were two
blocking criteria: “adaptivity-
disadaptation” (influence of disease
attitude on personality adaptation) and
“intrapsychic orientation” of disadaptation
(in case of disadaptive relationships). This
technique took the form of a questionnaire
consisting of 12 tables with sets of
statements each containing from 10 to 16
statements. The patient is asked to select
two most suitable statements. In addition
to “Yes” and “No” answers, each table
with statements also had the “Not
applicable” option, which allows for more
precise classification of disease attitudes.
Male and Female Painting projective test
by Romanova N.M. (2004).The Male and
Female Painting (MFP) studies personal
gender attitudes. The author of the method
defines gender attitudes as a certain
gestalt, a figure against the background of
a person’s individual gender concept.
Gender attitudes point to the person’s
main socio-sexual dominance.
The participant is supposed to paint male
and female figures. The analysis of the
painting (size of the figure, their mutual
positioning, graphic features of same-sex
and opposite-sex figures, completeness of
the painting) help determine the nature of
relationship between man and woman,
single out gender attitudes reflecting the
main aspects of gender identity.
The author of the method
distinguishes between the following types
of gender: - mindsets: support, isolation,
cooperation, independence,
attraction, indifference;
- attitudes: super valuable object,
blame object, romantic object,
functional object, object of
contempt, sexual object, dangerous
object, incomprehensible object,
low-value object.
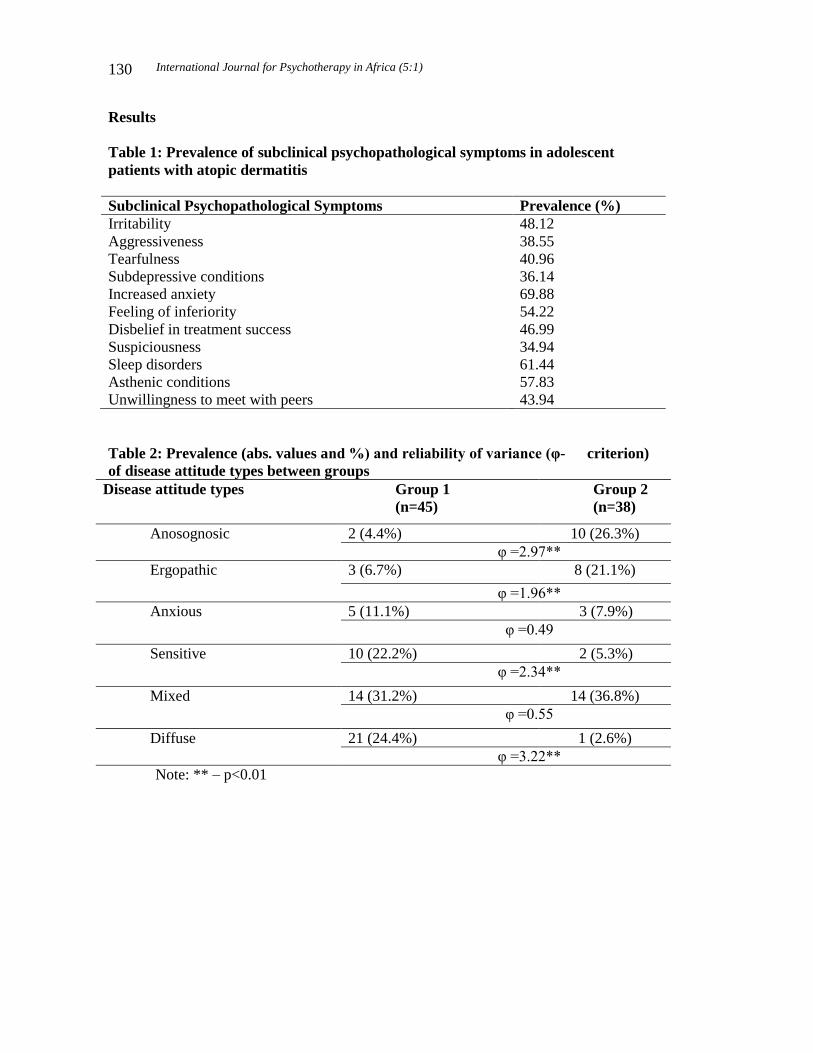
International Journal for Psychotherapy in Africa (5:1)
130
Results
Table 1: Prevalence of subclinical psychopathological symptoms in adolescent
patients with atopic dermatitis
Subclinical Psychopathological Symptoms Prevalence (%)
Irritability 48.12
Aggressiveness 38.55
Tearfulness 40.96
Subdepressive conditions 36.14
Increased anxiety 69.88
Feeling of inferiority 54.22
Disbelief in treatment success 46.99
Suspiciousness 34.94
Sleep disorders 61.44
Asthenic conditions 57.83
Unwillingness to meet with peers 43.94
Table 2: Prevalence (abs. values and %) and reliability of variance (φ- criterion)
of disease attitude types between groups
Disease attitude types Group 1
(n=45)
Group 2
(n=38)
Anosognosic 2 (4.4%) 10 (26.3%)
φ =2.97**
Ergopathic 3 (6.7%) 8 (21.1%)
φ =1.96**
Anxious 5 (11.1%) 3 (7.9%)
φ =0.49
Sensitive 10 (22.2%) 2 (5.3%)
φ =2.34**
Mixed 14 (31.2%) 14 (36.8%)
φ =0.55
Diffuse 21 (24.4%) 1 (2.6%)
φ =3.22**
Note: ** – p<0.01

Takyun, C.J. & Kockaryan, A.S. (2020). Gender Differences in Attitude to the Skin Disease-Atopic
Dermatitis among Adolescents: The Role of Cognitive Behavioral Therapy,
International Journal for Psychotherapy in Africa 5(1):122-135
131
Discussion of findings
Table 1 shows the prevalence of the
conditions in the group of adolescent
patients suffering from atopic dermatitis.
The fact that more than 60% of
adolescents with atopic dermatitis reported
sleep disorders caused by itching and
unpleasant thoughts is the basis for
asthenic manifestations.
Table 2 shows comparison of data
obtained in two samples yielded results
that indicate gender-specific types of
disease attitudes in adolescents diagnosed
with atopic dermatitis.
A statistically significant difference
between the groups was found in the
anosognosic disease attitude type that is
more typical of adolescent boys. This
disease attitude type is characterized by
active rejection of thoughts about the
disease and its consequences.
Male adolescents have unreasonably
uplifted spirits, are light-minded about the
disease, they try to ignore the disease and
tend to break the regime and not to abide
by recommendations. Lack of this disease
attitude type among females can be
explained by boys’ bravado, by their wish
to demonstrate their invulnerability and
confidence, which is in effect an attempt
to compensate for low self-appraisal.
Boys tend to maintain the existing
gender stereotypes attributed to males,
such as power and stamina, whereas they
think that the recognition of problems,
fears and anxiety is a sign of weakness.
It was noted by Bendas, (2007) that
boys and men have to resort to a more
powerful protection of their self-esteem
than women, i.e. this disease attitude type
works as a falsifier and amplifier of self-
esteem. Besides, it should be noted that
boys are more reserved than girls: the
latter more readily share their experiences
and trust adults. This gender difference
may also mean that, when giving answers,
boys are more inclined to stay reserved
and to demonstrate their invulnerability.
Girls, who are “allowed” to be weak,
uncertain, and expressive, do not resort to
this self-description of the disease because
they do not have to employ such self-
protection methods.
Boys also differ from girls in terms
of the ergopathic disease attitude type,
which is characterized by a “retreat into
studies”, preoccupation with their
activities, over-responsibility, and
volitional attitude; despite the disease,
boys try to maintain their status at school
and remain active. This gender difference
may be explained by the fact that boys
have more pronounced motivation to be a
success in the fields that suggest activity,
encouragement or discouragement (Ilyin,
2002). Purposefulness and result-
orientedness, which is characteristic of
males, make boys determined and firm in
their hard work and the desire to overcome
obstacles posed by the disease. The
achievement of goals is very important for
males because it is in this way that they
can prove their success and not fall in their
own eyes. Many authors Averin (2003)
emphasize that females prioritize
interpersonal relations which is evidenced
by greater significance of communication
for women. Males are more task-oriented
so the men’s style is described as
analytical and manipulative.
The sensitive disease attitude type is
typical of teenage girls. This type is
characterized by interpsychic personal
reactions, which explains girls’ social
maladaptation. Girls’ major concern in

International Journal for Psychotherapy in Africa (5:1)
132
relation to the disease is the unfavorable
impression that the disease symptoms may
produce on people around, and this makes
girls overly vulnerable and shy. It leads to
a restricted behavior and the narrowing of
the range of interpersonal contacts. Mood
fluctuations are influenced by
interpersonal contacts that are more
significant for girls than for boys. Girls are
more oriented towards relationships that
are disrupted as a result of the disease,
whereas boys are more task-oriented.
Boys and girls are motivated by different
needs: the need for affiliation is more
important for girls than the need for
achievements, which is more important for
males. In addition to the affiliative vector
of females’ motivation accounting for the
sensitive disease attitude, another factor is
the females’ attitude to their appearance.
Attractive appearance is one of the central
life values; it is females that tend to be
highly dissatisfied with their appearance
(Rumsey, 2009). Attractive appearance is
of great social value, it raises female’s
self-appraisal and value for people around.
The symptoms of atopic dermatitis
negatively affect the appearance of a
teenage girl, which is a reason for the
sensitive disease attitude. Females are
under a greater social and cultural
influence related to the appearance, and
the teenagers’ environment is a “merciless
appearance judge”, which is evidenced by
the phenomenon of lookism –
discrimination by looks.
The diffuse disease attitude type is
also characteristic of adolescent girls with
atopic dermatitis. Non-differentiation
indicates the vagueness of the disease
pattern, which apparently seizes the whole
personality leaving no zones free from
conflict. It should be noted that an
indispensable part of the undifferentiated
disease attitude type in girls is its
sensitized component (100%). Lower
pronouncedness of the diffuse disease
attitude in boys may be explained by
lower vulnerability of males to this disease
and greater vulnerability and involvement
of females.
Irrespective of gender, the mixed
disease attitude of intra- and inter-psychic
type is the most common disease attitude
type. Thus, ergopathic disease attitude
type is more common among boys. It is
characterized by absorption into an
activity, ethnicity, and general activity.
Sensitive and diffuse disease attitude types
are more common among girls. Their
major concern in relation to the disease is
the unfavorable impression that the
disease symptoms may produce on people
around, and this makes girls overly
vulnerable and shy. It leads to a restricted
behavior and the narrowing of the range of
interpersonal contacts. Mood fluctuations
are influenced by interpersonal contacts
that are more significant for girls than for
boys. Girls are more oriented towards
relationships that are disrupted as a result
of the disease. The symptoms of atopic
dermatitis negatively affect the appearance
of a teenage girl, which is a reason for the
sensitive disease attitude. People around
are treated as condemning and
discriminating based on appearance.
Diffuse disease attitude type is a
combination of types into two blocks:
1) intrapsychic, including anxious,
hypochondriac, neurasthenic, melancholic,
and apathetic types; 2) interpsychic,
including sensitive, dysphoric, and
paranoid types. The diffuseness means
that the disease pattern is unshaped,
underarticulated and vague.

Takyun, C.J. & Kockaryan, A.S. (2020). Gender Differences in Attitude to the Skin Disease-Atopic
Dermatitis among Adolescents: The Role of Cognitive Behavioral Therapy,
International Journal for Psychotherapy in Africa 5(1):122-135
133
Male-specific disease attitude types
among adolescents with atopic dermatitis
are the types that do not considerable
disrupt social adaptation (ergopathic,
anosognosic). Female-specific disease
attitude types among adolescents with
atopic dermatitis are the types (sensitive,
diffuse) that disrupt psychic adaptation,
mainly of interpsychic orientation. The
adaptivity-disadaptivity poles are set by
gender mechanisms: in boys, it is “false
self-evaluation” and task-orientedness
(adaptation pole), while in girls it is
motivation of affiliation and high
significance of appearance for females
(disadaptivity pole).Irrespective of gender
the most common disease attitude type is
the mixed disease attitude of intra- and
inter-psychic type. Harmonic disease
attitude type was not diagnosed. The study
has serious implication for youths In
Africa most especially where families
have been undermined, truncated and
displaced due to multi-faceted and
complex issues exposing them to all kinds
of skin diseases. Youths who are most
passionate about their look are often the
most vulnerable;emotionally, physically
and psychological. As stated earlier, the
most serious psychological reaction in
adolescence may be caused by diseases
that change the adolescent’s appearance,
making him or her feel unattractive
thereby the need for Cognitive Behavioral
treatment that changes the adolescents
thought pattern from maladaptive to
adaptive.
Conclusion & Suggestions
The quality of life in girls with atopic
dermatitis is significantly decreased – the
disease influences all spheres of their life
and does not leave any “lucid windows”.
The most significant component disrupted
among the girls is the sphere of personal
relationships. The decrease in the life
quality of males with atopic dermatitis is
due to two factors: 1) disturbance of the
general sense of well-being, which affects
adolescents’ day-to-day activity and
learning; 2) “disrupted leisure”, which is
related to the limitation of personal
relationships and the need to follow the
therapeutic regimen.
Adolescents with atopic dermatitis
have decreased self-esteem. Boys have
higher self-esteem than girls. In the
subjective world image of the girls with
AD, “attractive appearance ensures
success and is the basis for self-
confidence”; girls with atopic dermatitis
demonstrate the “phenomenon of scissors”
– a large gap between the system of actual
self-evaluation and demands (ideal images
of the self), which creates inner tension
and incongruence which inform the need
for behavioral treatment.
Suggestions for further studies
include the investigation of adolescent’s
personal traits that account for the
predisposition to certain disease attitude
types and to determine how the
adolescence crisis affects the shaping of
the disease attitude type.
References
Averin, V.A. (2003). Human psychology
from birth to death. Childhood,
Adolescence, Maturity, Old age: A
full course of developmental
psychology. Olma-Press
Amon, G. (2000). Psychosomatic therapy.
SPb. Rech pp 237.
Bendas, T.V. (2007). Gender psychology.
SPb. Piter, pp 300.
Cle, M. (1997). Adolescence psychology.
A reader. pp 103-140.
International Journal for Psychotherapy in Africa (5:1)
134
Foa, E.B., and Gershuny,B. (1995).
Arousal, Numbing and Intrusions;
Syptom Structure of PTSD
Following Assault. American
Journal of Psychiatry.
Golovneval, V. (2006). Gender
identity.Tendencies of changes.
Kharkov. NUA.
Ilyin, Y.P. (2002). Deferential
psychophysiology of men and
women. SPb. Piter.
Isaev, D.N. & Kagan, V.Y. (1979). Sexual
education and psycho hygiene.
Kagan, V.Y. (1990). Psychosexual
education of children and
adolescents. Fiction Literature.
Kocharyan, A. S. (2010). A person’s
gender role space.
http://www.pca.kh.ua/2010.
Klertsina, I. S. (2004). Psychology of
gender relations. Theory and
practices. SPb. Aleteya.
Lichko, N. and Ivanov (1980). Medical
and psychological examination of
patients.
Journal of Neuropathology and Psychiatry
(8) 1195-1198.
Mendelevich V. D. Clinical and Medical
Psychology: A handbook. Med
Press, 2005.
Mendelevich, V.D. and Solovyeva, S.L.
(2002), Neurosology and
psychosomatic Medicine. MED-
Press.
Nikolaeva, V.N. (1987). Influence of a
chronic disease on the psyche.
Obukhova I.F. (2003). Age psychology.
Russian Pedagogic Association.
Romanova, (2004). The male and Female
painting test. Journal of applied
psychology, (3) 38-44.
Smirnova, G.I. (2006) The modern
concept of treating atopic dermatitis
in children. Vol. 8(1) 32-38.
Takyun, C.J. (2009). Exploring Cognitive
Behavioral Therapy for the Survival
and rehabilitation of rape victims.
Nigerian Journal of Social
Research, 1 (5), 30-37.
Wasserman, L.I et al (2003). Medical
psychodiagnostics: Theory, practice
and training. Faculty of Philosophy.
Academic Publishing Center pg 736.
Related Documents











