ORIGINAL ARTICLE Heart Vessels (2009) 24:271–276 © Springer 2009 DOI 10.1007/s00380-008-1111-4 B. Jug (*) · N. Vene · M. Šebeštjen · M. Šabovič · I. Keber Department of Vascular Diseases, Clinic of Internal Medicine, University Clinical Center Ljubljana, Zaloška 7/VI, SI-1000 Ljubljana, Slovenia Tel. +386-41-811-830; Fax +386-1-522-8070 e-mail: [email protected] B.G. Salobir Clinic of Nuclear Medicine, University Clinical Center, Ljubljana, Slovenia Borut Jug · Barbara Gužič Salobir · Nina Vene Miran Šebeštjen · Mišo Šabovič · Irena Keber Interleukin-6 is a stronger prognostic predictor than high-sensitive C-reactive protein in patients with chronic stable heart failure Abstract Heart failure is characterized by activation of the immune system which is strongly associated with disease severity and outcome. We sought to compare the prognostic impact of two established inflammatory markers – interleukin-6 (IL-6) and high-sensitivity C-reactive protein (hsCRP) – in patients with chronic heart failure. In stable, optimally managed outpatients with chronic heart failure, baseline levels of hsCRP and IL-6 were determined. Clini- cal follow-up was obtained and the rate of events (heart failure related deaths or hospitalizations) were recorded. We included 201 patients (32.7% female, NYHA class II [66.2%] or III [33.8%], mean age 70 years). During a median follow up of 614 (367–761) days, 64 (30.9%) patients expe- rienced an event; those with an event had higher levels of hsCRP (median 2.93 [interquartile range 2.36–8.92] vs 2.23 [1.32–5.77] mmol/l) and IL-6 (7.8 [4.7–10.3] vs 4.3 [2.6–7.9] pg/ml). However, on Cox multivariate analysis, IL-6 but not hsCRP emerged as an independent predictor of prognosis (hazard ratio HR adjusted 2.74, 95% confidence interval 1.17– 6.43; P = 0.020). Our findings suggest that IL-6 is a better prognostic predictor than hsCRP in patients with chronic stable heart failure. Key words Congestive heart failure · Prognosis · Inflam- mation · C-reactive protein · High-sensitivity C-reactive protein Introduction Heart failure carries an unfavorable prognosis. However, several interventions known to improve survival in heart failure have been introduced in everyday clinical practice, while most risk-stratification strategies still rely on prognos- tic factors that have been identified and validated before current management strategies. 1,2 Therefore, management of patients with chronic heart failure calls for a sustained identification of novel and validation of established prog- nostic factors. Heart failure is characterized by activation of the immune system. 3 Several proinflammatory cytokines have been associated with heart failure severity, progression, and unfavorable outcomes. 4–6 Ample interest has been espe- cially devoted to the prognostic role of interleukin-6 (IL- 6) 7–9 and high-sensitivity C-reactive protein (hsCRP) 10–12 – both markers of systemic inflammation and prognostic factors in advanced heart failure. Interleukin-6 levels are related to the severity of left ventricular dysfunction and the degrees of activation of the sympathetic and rennin– angiotensin systemsand have emerged as one of the most important predictors of long-term survival in patients with chronic heart failure. 13,14 Similarly, hsCRP is associated with an increased rate of major cardiovascular events and adds incremental prognostic information to that provided by BNP alone. 15 However, previous studies mostly focused on single prognostic markers in patients with advanced heart failure (usually awaiting heart transplantation), and no direct com- parison of the prognostic impact of IL-6 and hsCRP has been carried out in patients with stable chronic heart failure. Therefore, we sought to evaluate and compare these two prognostic markers in patients with stable and optimally managed chronic heart failure. Patients and methods Patients Patients were recruited from the Heart Failure Clinic of the University Clinical Center in Ljubljana. Patients had to meet the following criteria: signs and/or symptoms of heart Received: December 7, 2007 / Accepted: August 28, 2008

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ORIGINAL ARTICLE
Heart Vessels (2009) 24:271–276 © Springer 2009DOI 10.1007/s00380-008-1111-4
B. Jug (*) · N. Vene · M. Šebeštjen · M. Šabovič · I. KeberDepartment of Vascular Diseases, Clinic of Internal Medicine, University Clinical Center Ljubljana, Zaloška 7/VI, SI-1000 Ljubljana, SloveniaTel. +386-41-811-830; Fax +386-1-522-8070e-mail: [email protected]
B.G. SalobirClinic of Nuclear Medicine, University Clinical Center, Ljubljana, Slovenia
Borut Jug · Barbara Gužič Salobir · Nina Vene Miran Šebeštjen · Mišo Šabovič · Irena Keber
Interleukin-6 is a stronger prognostic predictor than high-sensitive C-reactive protein in patients with chronic stable heart failure
Abstract Heart failure is characterized by activation of the immune system which is strongly associated with disease severity and outcome. We sought to compare the prognostic impact of two established infl ammatory markers – interleukin-6 (IL-6) and high-sensitivity C-reactive protein (hsCRP) – in patients with chronic heart failure. In stable, optimally managed outpatients with chronic heart failure, baseline levels of hsCRP and IL-6 were determined. Clini-cal follow-up was obtained and the rate of events (heart failure related deaths or hospitalizations) were recorded. We included 201 patients (32.7% female, NYHA class II [66.2%] or III [33.8%], mean age 70 years). During a median follow up of 614 (367–761) days, 64 (30.9%) patients expe-rienced an event; those with an event had higher levels of hsCRP (median 2.93 [interquartile range 2.36–8.92] vs 2.23 [1.32–5.77] mmol/l) and IL-6 (7.8 [4.7–10.3] vs 4.3 [2.6–7.9] pg/ml). However, on Cox multivariate analysis, IL-6 but not hsCRP emerged as an independent predictor of prognosis (hazard ratio HRadjusted 2.74, 95% confi dence interval 1.17–6.43; P = 0.020). Our fi ndings suggest that IL-6 is a better prognostic predictor than hsCRP in patients with chronic stable heart failure.
Key words Congestive heart failure · Prognosis · Infl am-mation · C-reactive protein · High-sensitivity C-reactive protein
Introduction
Heart failure carries an unfavorable prognosis. However, several interventions known to improve survival in heart
failure have been introduced in everyday clinical practice, while most risk-stratifi cation strategies still rely on prognos-tic factors that have been identifi ed and validated before current management strategies.1,2 Therefore, management of patients with chronic heart failure calls for a sustained identifi cation of novel and validation of established prog-nostic factors.
Heart failure is characterized by activation of the immune system.3 Several proinfl ammatory cytokines have been associated with heart failure severity, progression, and unfavorable outcomes.4–6 Ample interest has been espe-cially devoted to the prognostic role of interleukin-6 (IL-6)7–9 and high-sensitivity C-reactive protein (hsCRP)10–12 – both markers of systemic infl ammation and prognostic factors in advanced heart failure. Interleukin-6 levels are related to the severity of left ventricular dysfunction and the degrees of activation of the sympathetic and rennin–angiotensin systemsand have emerged as one of the most important predictors of long-term survival in patients with chronic heart failure.13,14 Similarly, hsCRP is associated with an increased rate of major cardiovascular events and adds incremental prognostic information to that provided by BNP alone.15
However, previous studies mostly focused on single prognostic markers in patients with advanced heart failure (usually awaiting heart transplantation), and no direct com-parison of the prognostic impact of IL-6 and hsCRP has been carried out in patients with stable chronic heart failure. Therefore, we sought to evaluate and compare these two prognostic markers in patients with stable and optimally managed chronic heart failure.
Patients and methods
Patients
Patients were recruited from the Heart Failure Clinic of the University Clinical Center in Ljubljana. Patients had to meet the following criteria: signs and/or symptoms of heart
Received: December 7, 2007 / Accepted: August 28, 2008

272
failure at inclusion, and echographic evidence of left ven-tricular dysfunction – i.e., impaired systolic function (left ventricular ejection fraction [LVEF] <0.50 measured by Simpson biplane method) or impaired diastolic function (defi ned as LVEF > 0.50 and either: an E/E′ ratio on tissue Doppler recordings at the mitral ring >15 or an E/E′ ratio >8 plus one of the following: (a) atrial fi brillation, (b) elevated natriuretic peptides, or (c) echographic indices of diastolic dysfunction on transmitral and pulmonary veins fl ow pattern). Patients were in New York Heart Association (NYHA) functional class II or III, optimally managed according to current guidelines and stable for at least 3 months prior to inclusion.
We excluded patients with recent (<3 months) myo-cardial infarction, stroke, or thromboembolism, with sig-nifi cant liver (enzymes >3-times the upper reference limit) or renal dysfunction (creatinine level >250 μg/l), and patients with chronic autoimmune or infl ammatory diseases and malignancies. Informed consent was obtained from all participants according to a protocol approved by the National Committee for Medical Ethics and Biomedical Investigation.
Study design and follow-up
At inclusion, patients underwent thorough clinical exami-nation, echographic assessment, and had their blood drawn. We planned a minimum follow-up of 12 months at regular 3-month intervals. If the patient missed a follow-up appoint-ment, telephone contacts with next of kin and/or the general practitioner were carried out and pertinent medical records were examined in order to assess changes in health status.
The predefi ned primary outcome was a composite of cardiovascular death (pump failure, fatal myocardial infarc-tion, or sudden cardiac death) or unplanned hospital admis-sion for management of worsening heart failure (confi rmed by two independent cardiologists blinded for baseline measurements).
Biochemical analysis
All patients had venous blood samples (ethylenediamine-tetraacetic acid) taken after 30 min of rest in the supine position from the cubital vein. Samples were centrifuged at 3000 rpm for 10 min at 0°C and separated immediately afterwards.
Interleukin-6 levels were measured by quantitative sand-wich enzyme immunoassay technique (R&D Systems, Min-neapolis, MN, USA). The intra- and interassay coeffi cient variations were 11.1% and 16.0%, respectively.
High-sensitivity CRP levels were determined by a modifi cation of laser nephelometric technique (Behring Diagnostics, Rarburg, Germany). The intra- and interassay coeffi cient variations were 5.5% and 10.5%, respectively.
Statistical analysis
Sample size was calculated to detect a hazard ratio of 2.0 with the following assumptions: proportional hazards, β = 0.80 and α = 0.05, median survival time 24 months, accrual (recruitment) time 12 months, follow-up time after end of recruitment 12 months.16 Normal distribution was assessed by the Kolmogorov–Smirnov test. Baseline characteristics were summarized by mean (standard deviation) for nor-mally and by median (inter-quartile range) for non-normally distributed continuous variables, and by frequency (percentage) for categorical variables. Between-group dif-ferences were tested by the Student t-test for normally and by the Mann–Whitney U-test for non-normally distributed variables, and proportions were compared using the chi-square test.
The estimated hazard (risk) ratios were adjusted for major univariate predictors of morbidity and mortality using a multivariate Cox proportional hazard regression model. For analysis purposes, variables were dichotomized by medians used as cutoffs. A two-tailed P value of less than 0.05 was considered statistically signifi cant.
Results
A total of 201 patients were included. One third of patients were female, mean age was 70 years (inter-quartile range 61–77). One hundred and thirty-one (65%) patients were in NYHA class II, and 70 (34.8%) were in NYHA class III. The majority (148 patients, 73.6%) had heart failure with impaired left ventricular ejection fraction (LVEF) and 53 (26.4%) had heart failure with preserved LVEF. Mean duration of heart failure at inclusion was 26 months, and etiology was ischemic in 45%, hypertensive in 21%, isch-emic and hypertensive in 10%, idiopathic dilatational in 16%, and other in 8% of patients.
Of the 201 patients with heart failure, 64 patients (31.8%) experienced an event (19 patients died and 45 were ho spitalized) after 6–668 days (median 307 days). Median follow-up period in survivors was 711 days (range 580–838) days. Cumulative event rate for all patients was 9.9% at 6 months, 16.3% at 12 months, and 31.8% at 24 months.
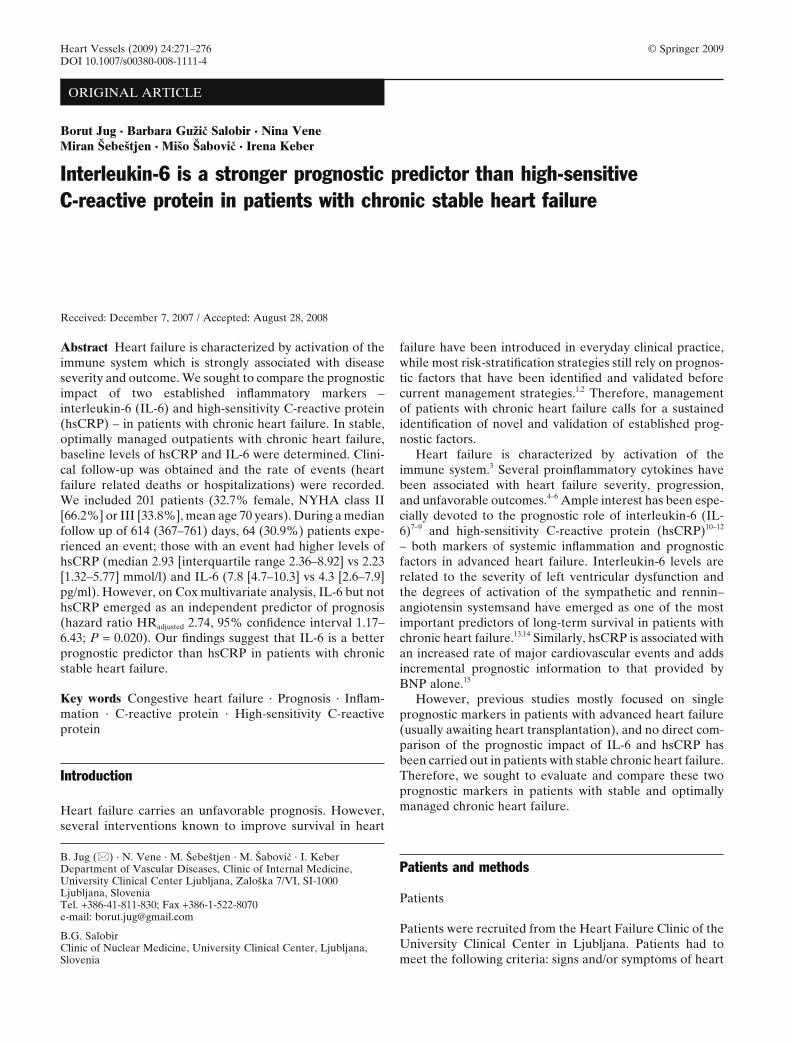
Patients who experienced an event (heart failure-related death or hospitalization) had increased levels of hsCRP and IL-6, they more often had diabetes mellitus, coronary artery disease, lower systolic blood pressure, worse performance on the 6-min walking test, lower LVEF, and higher uric acid levels; they also were more often prescribed a loop diuretic and less often a beta blocker (Table 1).
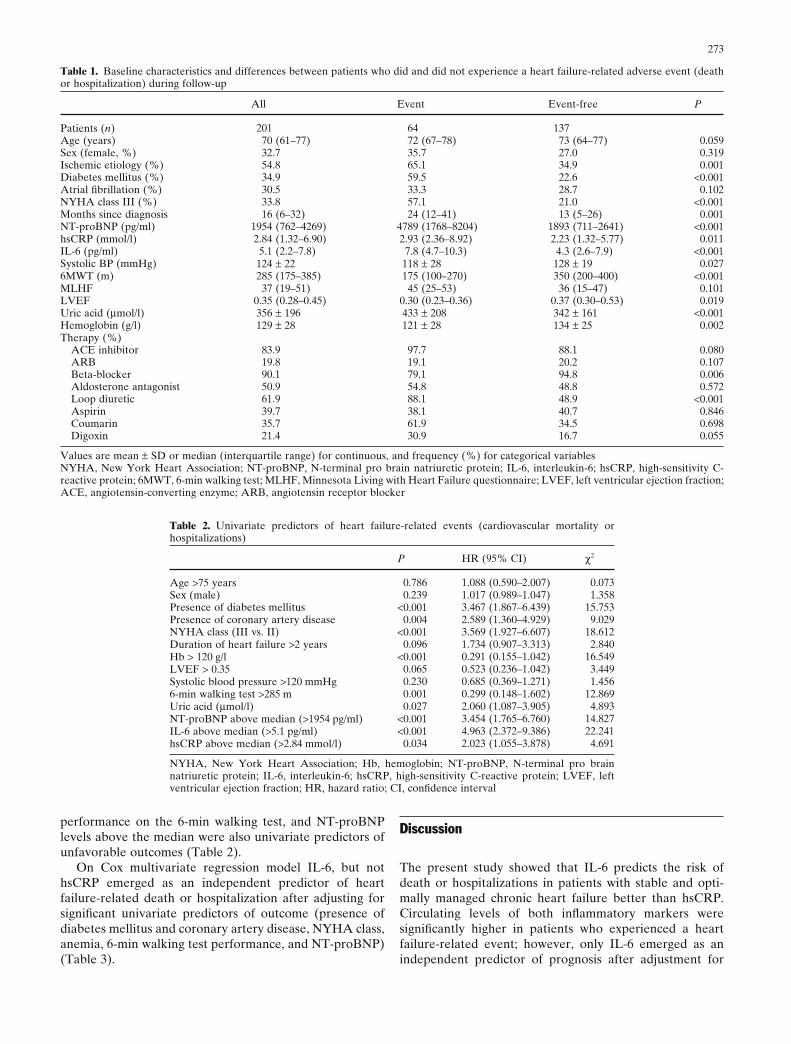
Levels of hsCRP and IL-6 above the respective medians were univariate predictors of an increased rate of heart failure related deaths or hospitalizations; however the asso-ciation between hsCRP and heart failure-related events was restricted to patients with coronary heart disease (Fig. 1). Presence of diabetes or coronary artery disease, NYHA class III, duration of heart failure >2 years, anemia (hemo-globin < 120 g/l), poor systolic function (LVEF < 0.35), poor
273
performance on the 6-min walking test, and NT-proBNP levels above the median were also univariate predictors of unfavorable outcomes (Table 2).
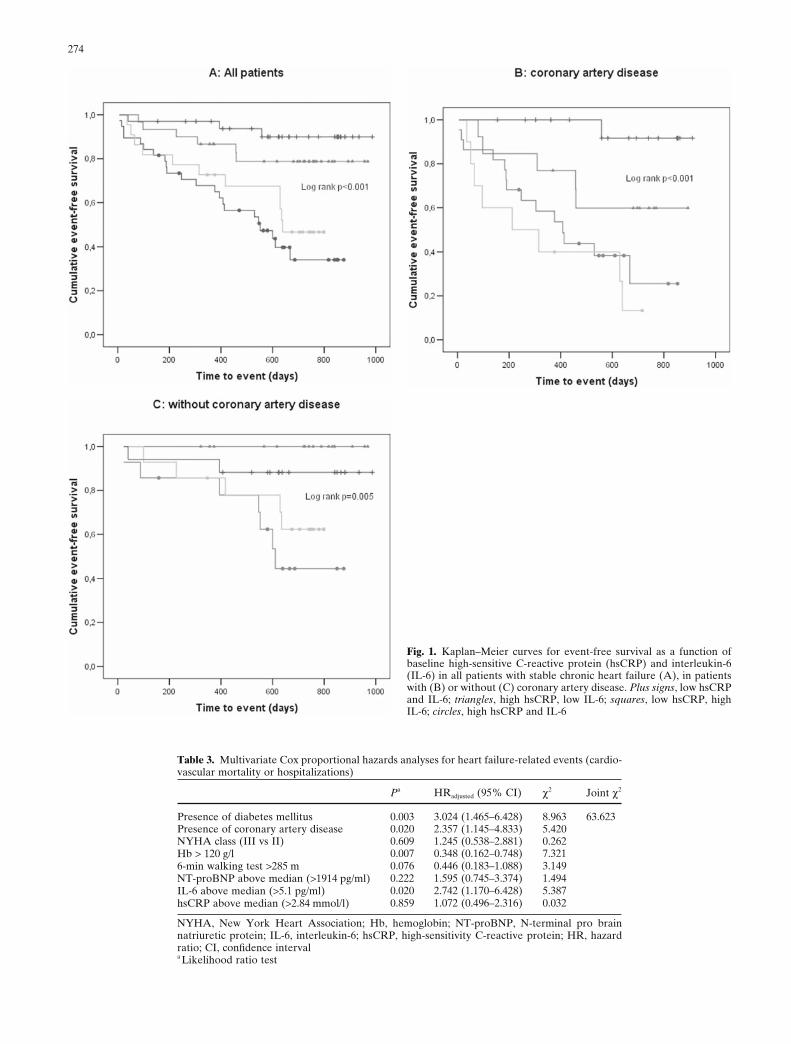
On Cox multivariate regression model IL-6, but not hsCRP emerged as an independent predictor of heart failure-related death or hospitalization after adjusting for signifi cant univariate predictors of outcome (presence of diabetes mellitus and coronary artery disease, NYHA class, anemia, 6-min walking test performance, and NT-proBNP) (Table 3).
Discussion
The present study showed that IL-6 predicts the risk of death or hospitalizations in patients with stable and opti-mally managed chronic heart failure better than hsCRP. Circulating levels of both infl ammatory markers were signifi cantly higher in patients who experienced a heart failure-related event; however, only IL-6 emerged as an independent predictor of prognosis after adjustment for
Table 1. Baseline characteristics and differences between patients who did and did not experience a heart failure-related adverse event (death or hospitalization) during follow-up
All Event Event-free P
Patients (n) 201 64 137Age (years) 70 (61–77) 72 (67–78) 73 (64–77) 0.059Sex (female, %) 32.7 35.7 27.0 0.319Ischemic etiology (%) 54.8 65.1 34.9 0.001Diabetes mellitus (%) 34.9 59.5 22.6 <0.001Atrial fi brillation (%) 30.5 33.3 28.7 0.102NYHA class III (%) 33.8 57.1 21.0 <0.001Months since diagnosis 16 (6–32) 24 (12–41) 13 (5–26) 0.001NT-proBNP (pg/ml) 1954 (762–4269) 4789 (1768–8204) 1893 (711–2641) <0.001hsCRP (mmol/l) 2.84 (1.32–6.90) 2.93 (2.36–8.92) 2.23 (1.32–5.77) 0.011IL-6 (pg/ml) 5.1 (2.2–7.8) 7.8 (4.7–10.3) 4.3 (2.6–7.9) <0.001Systolic BP (mmHg) 124 ± 22 118 ± 28 128 ± 19 0.0276MWT (m) 285 (175–385) 175 (100–270) 350 (200–400) <0.001MLHF 37 (19–51) 45 (25–53) 36 (15–47) 0.101LVEF 0.35 (0.28–0.45) 0.30 (0.23–0.36) 0.37 (0.30–0.53) 0.019Uric acid (μmol/l) 356 ± 196 433 ± 208 342 ± 161 <0.001Hemoglobin (g/l) 129 ± 28 121 ± 28 134 ± 25 0.002Therapy (%) ACE inhibitor 83.9 97.7 88.1 0.080 ARB 19.8 19.1 20.2 0.107 Beta-blocker 90.1 79.1 94.8 0.006 Aldosterone antagonist 50.9 54.8 48.8 0.572 Loop diuretic 61.9 88.1 48.9 <0.001 Aspirin 39.7 38.1 40.7 0.846 Coumarin 35.7 61.9 34.5 0.698 Digoxin 21.4 30.9 16.7 0.055
Values are mean ± SD or median (interquartile range) for continuous, and frequency (%) for categorical variablesNYHA, New York Heart Association; NT-proBNP, N-terminal pro brain natriuretic protein; IL-6, interleukin-6; hsCRP, high-sensitivity C-reactive protein; 6MWT, 6-min walking test; MLHF, Minnesota Living with Heart Failure questionnaire; LVEF, left ventricular ejection fraction; ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker
Table 2. Univariate predictors of heart failure-related events (cardiovascular mortality or hospitalizations)
P HR (95% CI) χ2
Age >75 years 0.786 1.088 (0.590–2.007) 0.073Sex (male) 0.239 1.017 (0.989–1.047) 1.358Presence of diabetes mellitus <0.001 3.467 (1.867–6.439) 15.753Presence of coronary artery disease 0.004 2.589 (1.360–4.929) 9.029NYHA class (III vs. II) <0.001 3.569 (1.927–6.607) 18.612Duration of heart failure >2 years 0.096 1.734 (0.907–3.313) 2.840Hb > 120 g/l <0.001 0.291 (0.155–1.042) 16.549LVEF > 0.35 0.065 0.523 (0.236–1.042) 3.449Systolic blood pressure >120 mmHg 0.230 0.685 (0.369–1.271) 1.4566-min walking test >285 m 0.001 0.299 (0.148–1.602) 12.869Uric acid (μmol/l) 0.027 2.060 (1.087–3.905) 4.893NT-proBNP above median (>1954 pg/ml) <0.001 3.454 (1.765–6.760) 14.827IL-6 above median (>5.1 pg/ml) <0.001 4.963 (2.372–9.386) 22.241hsCRP above median (>2.84 mmol/l) 0.034 2.023 (1.055–3.878) 4.691
NYHA, New York Heart Association; Hb, hemoglobin; NT-proBNP, N-terminal pro brain natriuretic protein; IL-6, interleukin-6; hsCRP, high-sensitivity C-reactive protein; LVEF, left ventricular ejection fraction; HR, hazard ratio; CI, confi dence interval
274
Table 3. Multivariate Cox proportional hazards analyses for heart failure-related events (cardio-vascular mortality or hospitalizations)
Pa HRadjusted (95% CI) χ2 Joint χ2
Presence of diabetes mellitus 0.003 3.024 (1.465–6.428) 8.963 63.623Presence of coronary artery disease 0.020 2.357 (1.145–4.833) 5.420NYHA class (III vs II) 0.609 1.245 (0.538–2.881) 0.262Hb > 120 g/l 0.007 0.348 (0.162–0.748) 7.3216-min walking test >285 m 0.076 0.446 (0.183–1.088) 3.149NT-proBNP above median (>1914 pg/ml) 0.222 1.595 (0.745–3.374) 1.494IL-6 above median (>5.1 pg/ml) 0.020 2.742 (1.170–6.428) 5.387hsCRP above median (>2.84 mmol/l) 0.859 1.072 (0.496–2.316) 0.032
NYHA, New York Heart Association; Hb, hemoglobin; NT-proBNP, N-terminal pro brain natriuretic protein; IL-6, interleukin-6; hsCRP, high-sensitivity C-reactive protein; HR, hazard ratio; CI, confi dence intervala Likelihood ratio test
Fig. 1. Kaplan–Meier curves for event-free survival as a function of baseline high-sensitive C-reactive protein (hsCRP) and interleukin-6 (IL-6) in all patients with stable chronic heart failure (A), in patients with (B) or without (C) coronary artery disease. Plus signs, low hsCRP and IL-6; triangles, high hsCRP, low IL-6; squares, low hsCRP, high IL-6; circles, high hsCRP and IL-6

275
usual prognostic factors, in particular for the presence of diabetes mellitus and coronary artery disease, anemia, NT-proBNP, and NYHA class.
Heart failure is characterized by derangements of the immune system. Chronic heart failure promotes T-lymphocyte activation (as measured by an increase in HLA-DR and CD40L antigen expression17 and by an increased number of interferon-gamma producing CD4+ T lympho-cytes),18 resulting in an overproduction of infl ammatory chemokines. Cytokine overproduction and spill-over into the bloodstream have been attributed to a cross-talk between neurohormones and cytokines and are therefore directly related to heart failure severity.4,19,20 Moreover, animal models have proposed that proinfl ammatory cyto-kines directly infl uence cardiac function and heart failure progression by inducing myocardiocyte hypertrophy, dis-rupting the extracellular matrix and endothelial function, infl uencing myocardial contractility, and promoting myo-cardiocyte apoptosis21–25 – all of which ultimately lead to cardiac remodeling and heart failure progression.
Infl ammatory cytokines are associated with heart failure severity and progression. Previous studies have confi rmed that tumor necrosis factor alpha (TNF-α), its soluble recep-tors 1 and 2, carbohydrate antigen 125, IL-1, IL-2, and IL-6, and hsCRP predict heart failure progression and adverse cardiovascular outcomes.5,6,15,26–31 However, comparisons between the prognostic role of different cytokines have yielded inconclusive results. For instance, IL-6 has emerged as an independent predictor of prognosis after adjusting for big endothelin, IL-1, IL-10, and IL-12, TNF-α, CD40, and even NT-proBNP,9,32 but not for soluble TNF-α receptor 1.33 Differences in the studied populations as well as a high short-term variability of IL-6 concentrations and different methods of assessing IL-6 plasma concentrations further complicate comparisons between studies. Moreover, patho-physiologic roles and interactions between different cyto-kines are complex and the prognostic role of a specifi c cytokine may thus vary with disease stage and severity.34
In our study, IL-6 emerged as a stronger prognostic pre-dictor in chronic heart failure compared to hsCRP. Both hsCRP and IL-6 are markers of infl ammation; however, hsCRP seems to provide less specifi c information about the extent of infl ammation directly related to heart failure and its severity. Firstly, hsCRP is an acute-phase reactant released into the bloodstream in response to various non-specifi c stimuli – one of them being IL-6 itself.6,35 Secondly, hsCRP may refl ect cytokine activation in the context of heart failure but may also indicate vascular risk. The present study confi rmed previous reports11 that the deleterious impact of an elevated hsCRP is restricted to patients with coronary heart disease. In this regard, elevated levels of hsCRP may also be an epiphenomenon that is not directly related to heart failure progression; in fact, the recent CORONA study showed that lowering hsCRP levels with statin therapy in patients with ischemic heart failure does not translate into a reduction of cardiovascular events.36
Despite providing evidence that IL-6 is a stronger pre-dictor of heart failure related death or hospitalization than hsCRP, our study has some limitations that need to be
taken into account. Firstly, the modest number of parti-cipants allowed us to focus on the primary aim of the study – a comparison of the prognostic role of IL-6 and hsCRP. Thus, it provides additional insight into the infl ammatory processes and derangements in chronic heart failure, but larger cohorts should validate clinical applicability of our fi ndings. Secondly, the prognostic impact of infl ammatory markers still needs a mechanistic explanation which further studies are called upon to provide. Thirdly, our conclusions cannot be generalized to all heart failure patients as we only included optimally managed ambulatory patients with stable chronic heart failure.
In conclusion, our fi ndings demonstrate that IL-6 is a stronger predictor of outcome in patients with stable chronic heart failure than hsCRP. Interleukin-6 levels were associ-ated with an increased risk of heart failure-related death or hospitalizations even after allowing for known prognostic factors, particularly NT-proBNP, LVEF, and NYHA class. Nevertheless, larger cohort studies need to confi rm our fi ndings, as well as to address and compare other infl amma-tory markers of prognosis.
References
1. Butler J, Khadim G, Paul KM, Davis SF, Kronenberg MW, Chomsky DB, Pierson RN, Wilson JR (2004) Selection of patients for heart transplantation in the current era of heart failure therapy. J Am Coll Cardiol 43:787–793
2. Zugck C, Haunstetter A, Krüger C, Kell R, Schellberg D, Kübler W, Haass M (2002) Impact of beta-blocker treatment on the prog-nostic value of currently used risk predictors in congestive heart failure. J Am Coll Cardiol 39:1615–1622
3. Mann D, Young J (1994) Basic mechanism in congestive heart failure: recognizing the role of proinfl ammatory cytokines. Chest 105:897–904
4. Anker S, Von Haehling S (2004) Infl ammatory mediators in chronic heart failure: an overview. Heart 90:464–470
5. Sharma R, Rauchhaus M, Ponikowski PP, Varney S, Poole-Wilson, PA, Mann DL, Coats AJS, Anker SD (2000) The relationship of the erythrocyte sedimentation rate to infl ammatory cytokines and survival in patients with chronic heart failure treated wit angiotensin-converting enzyme inhibitors. J Am Coll Cardiol 36:523–528
6. Deswal A, Petersen NJ, Feldman AM, Young JB, White BG, Mann DL (2001) Cytokines and cytokine receptors in advanced heart failure: an analysis of the cytokine database from the Vesna-rinone trial (VEST). Circulation 103:2055–2059.
7. Papanicolaou D, Wilder R, Monolagas S, Chrosos GP (1998) The pathophysiologic roles of interleukin-6 in human disease. Ann Intern Med 128:127–137
8. Kanada T, Takahashi T (2004) Interleukin-6 and cardiovascular disease. Jpn Heart J 45:183–193
9. Kell R, Haunstetter A, Dengler T, Zugck C, Kubler W, Haass M (2002) Do cytokines enable risk stratifi cation to be improved in NYHA functional class III patients? Comparison with other poten-tial predictors of prognosis. Eur Heart J 23:70–78
10. Shah SJ, Marcus GM, Gerber IL, McKeown BH, Vessey JC, Jordan MV, Huddleston M, Foster E, Chatterjee K, Michaels AD (2006) High-sensitivity C-reactive protein and parameters of left ventricular dysfunction. J Card Fail 12:61–65
11. Lamblin N, Mouquet F, Hennache B, Dagorn J, Susen S, Bauters C, de Groote P (2005) High-sensitive C-reactive protein: potential adjunct for risk stratifi cation in patients with stable congestive heart failure. Eur Heart J 26:2245–2250
12. Kistorp C, Raymond I, Pedersen F, Gustafsson F, Faber J, Hildebrandt P (2005) N-terminal pro-brain natriuretic peptide, C-reactive protein, and urinary albumin levels as predictors of mor-
276
tality and cardiovascular events in older adults. JAMA 293:1609–1616
13. Maeda K, Tsutamoto T, Wada A, Mabuchi N, Hayashi M, Tsutsui T, Ohnishi M, Sawaki M, Fujii M, Matsumoto T, Kinoshita M (2000) High levels of plasma brain natriuretic peptide and interleukin-6 after optimized treatment for heart failure are inde-pendent risk factors for morbidity and mortality in patients with congestive heart failure. J Am Coll Cardiol 36:1587–1593
14. Tsutamoto T, Hisanaga T, Wada A, Maeda K, Ohnishi M, Fukai D, Mabuchi N, Sawaki M, Kinoshita M (1998) Interleukin-6 spill-over in the peripheral circulation increase with the severity of heart failure and high plasma level of interleukin-6 is an important prog-nostic predictor in patients with congestive heart failure. J Am Coll Cardiol 31:391–398
15. Anand IS, Latini R, Florea VG, Kuskowski MA, Rector T, Masson S, Signorini S, Mocarelli P, Hester A, Glazer R, Cohn JN, for the Val-HeFT Investigators (2005) C-reactive protein in heart failure: Prognostic value and the effect of valsartan. Circulation 112:1428–1434
16. Dupont W, Plummer W (1990) Power and sample size calculations: a review and computer program. Controlled Clin Trials 11:116–128
17. Ueno A, Murasaki K, Hagiwara N, Kasanuki H (2007) Increases in circulating T lymphocytes expressing HLA-DR and CD40 ligand in patients with dilated cardiomyopathy. Heart Vessels 22:316–321
18. Fukunaga T, Soejima H, Irie A, Sugamura K, Oe Y, Tanaka T, Kojima S, Sakamoto T, Yoshimura M, Nishimura Y, Ogawa H (2007) Expression of interferon-gamma and interleukin-4 produc-tion in CD4(+) T cells in patients with chronic heart failure. Heart Vessels 22:178–183
19. Burger A, Benicke M, Deten A, Zimmer H-G (2001) Catechol-amines stimulate interleukin-6 synthesis in rat cardiac fi broblasts. J Am Physiol Heart Circ Physiol 201:H14–H21
20. Lee DL, Sturgis LC, Labazi H, Osborne JB, Fleming C, Pollock JS, Manhiani M, Imig JD, Brands MW (2005) Angiotensin II hypertension is attenuated in interleukin-6 knockout mice. Am J Physiol Heart Circ Physiol 290:H935–H940
21. Arstall MA, Sawyer DB, Fukuzawa R, Kell R (1999) Cytokine-mediated apoptosis in cardiac myocytes: the role of inducible nitric oxide synthase induction and peroxisome generation. Circ Res 85:829–840
22. Blum A, Miller H (2001) Pathophysiological role of cytokines in congestive heart failure. Ann Rev Med 52:15–27
23. Franchimont N, Rydziel S, Delany A, Canalis E (1997) Interleukin-6 and its soluble receptor cause a marked induction of collagenase 3 expression in rat osteoblast cultures. J Biol Chem 272:12144–12150
24. Janssen SP, Gayan-Ramirez G, Van Den Bergh A, Herijgers P, Maes K, Verbeken E, Decramer M (2005) Interleukin-6 causes
myocardial failure and skeletal muscle atrophy in rats. Circulation 111:996–1005
25. Hirota H, Yoshida K, Kaishimoto T, Taga T (1995) Continuous activation of gp139, a signal transducing receptor component for interleukin-6-related cytokines, causes myocardial hypertrophy. Proc Natl Acad Sci USA 92:4862–4866
26. Varol E, Ozaydin M, Altinbas A, Aslan SM, Dogan A, Dede O (2007) Elevated carbohydrate antigen 125 levels in hypertrophic cardiomyopathy patients with heart failure. Heart Vessels 22:30–33
27. Ferrari R, Bachetti T, Confortini R (1995) Tumor necrosis factor soluble receptors in patients with various degrees of congestive heart failure. Circulation 92:1479–1486
28. Torre-Amione G, Kapadia S, Benedict C, Oral H, Young J, Mann DL (1996) Proinfl ammatory cytokine levels in patients with depressed left ventricular ejection fraction: a report from the Studies of Left Ventricular Dysfunction (SOLVD). J Am Coll Cardiol 31:391–398
29. Yin WH, Chen JW, Jen HL, Chiang MG, Huang WP, Feng AN, Shing Young M, Lin SJ (2004) Independent prognostic value of elevated high-sensitive C-reactive protein in chronic heart failure. Am Heart J 146:931–938
30. Bozkurt B (2000) Activation of cytokines as a mechanism of disease progression in heart failure. Ann Rheum Dis 59:90–93
31. Munger M, Johnson B, Amber I, Callahan K, Gilbert E (1996) Circulating concentrations of proinfl ammatory cytokines in mild or moderate heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am J Cardiol 77:723–727
32. Tsutamoto T, Asai S, Tanaka T, Sakai H, Nishiyama K, Fujii M, Yamamoto T, Ohnishi M, Wada A, Saito Y, Horie M (2007) Plasma level of cardiotrophin-1 as a prognostic predictor in patients with chronic heart failure. Eur J Heart Fail 9:1032–1037
33. Rauchhaus M, Doehner W, Francis D (2000) Plasma cytokine parameters and mortality in patients with chronic heart failure. Circulation 102:3060–3067
34. Ferrari R (2002) Interleukin-6: a neurohumoral predictor of prog-nosis in patients with heart failure: light and shadow (editorial). Eur Heart J 23:9–10
35. Gonway D, Buggins P, Hughes E, Lip GYH (2004) Relationship of interleukin-6 and C-reactive protein to the prothrombotic state in atrial fi brillation. J Am Coll Cardiol 43:2075–2082.
36. Kjekshus J, Apetrei E, Barrios V, Böhm M, Cleland JG, Cornel JH, Dunselman P, Fonseca C, Goudev A, Grande P, Gullestad L, Hjalmarson A, Hradec J, Jánosi A, Kamenský G, Komajda M, Korewicki J, Kuusi T, Mach F, Mareev V, McMurray JJ, Ranjith N, Schaufelberger M, Vanhaecke J, van Veldhuisen DJ, Waagstein F, Wedel H, Wikstrand J, for the CORONA Group (2007) Rosu-vastatin in older patients with heart failure. N Engl J Med 357:2248–2261
Related Documents