Interceptive Orthodontics Professor Dr. Sun Sun Win Professor & Head Children’s Dentistry & Orthodontics Department University of Dental Medicine,Yangon

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 1/39
Interceptive Orthodontics
Professor Dr. Sun Sun WinProfessor & Head
Children’s Dentistry & Orthodontics Department University of Dental Medicine,Yangon

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 2/39
Interceptive Orthodontics
• Certain malocclusion need correction at an earlier stage
in order to facilitate normal development of the
occlusion or to reduce the severity of malocclusion.
• This kind of early intervention is called interceptive
orthodontics.
( Not all malocclusions can be prevented )
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 3/39
Common malocclusions which need early intervention are
1. Early loss of primary teeth.
2. Retained primary teeth.
3. Anterior cross-bite (with displacement).4. Posterior cross-bite with displacement
5. Median Diastema
6. Harmful Para-functional habits
7. Supernumerary teeth

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 4/39
1. Early loss of primary teeth.
Unilateral loss centreline shift.
- Delayed eruption of permanent tooth.
- Centre line shift.
- Localised crowding.
- Including loss of space due to inter - proximal caries
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 5/39
Management
To prevent early loss of primary teeth.
• Use of fissure sealants.
• Restore carious teeth.
• Dietary advice.
• Use of fluoride

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 6/39
2. Retained Primary teeth
- cross-bite
- median diastema
- displacement of the permanent teeth.
- rotation
Treatment remove the retained primary teeth.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 7/39
3. Anterior Crossbite
One or more upper incisors occlude lingual to the
corresponding lower incisors.
Causes
Class III skeletal pattern
Crowding
Retained primary teeth
Presence of supernumerary teeth.
Trauma.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 8/39
Management
- Remove etiological factors.
- Differentiate skeletal problems from others.
(a) Tongue blade correction.
(b) Lower inclined bite plane.
(c) Removable appliance with either cantilever spring or
screw.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 9/39
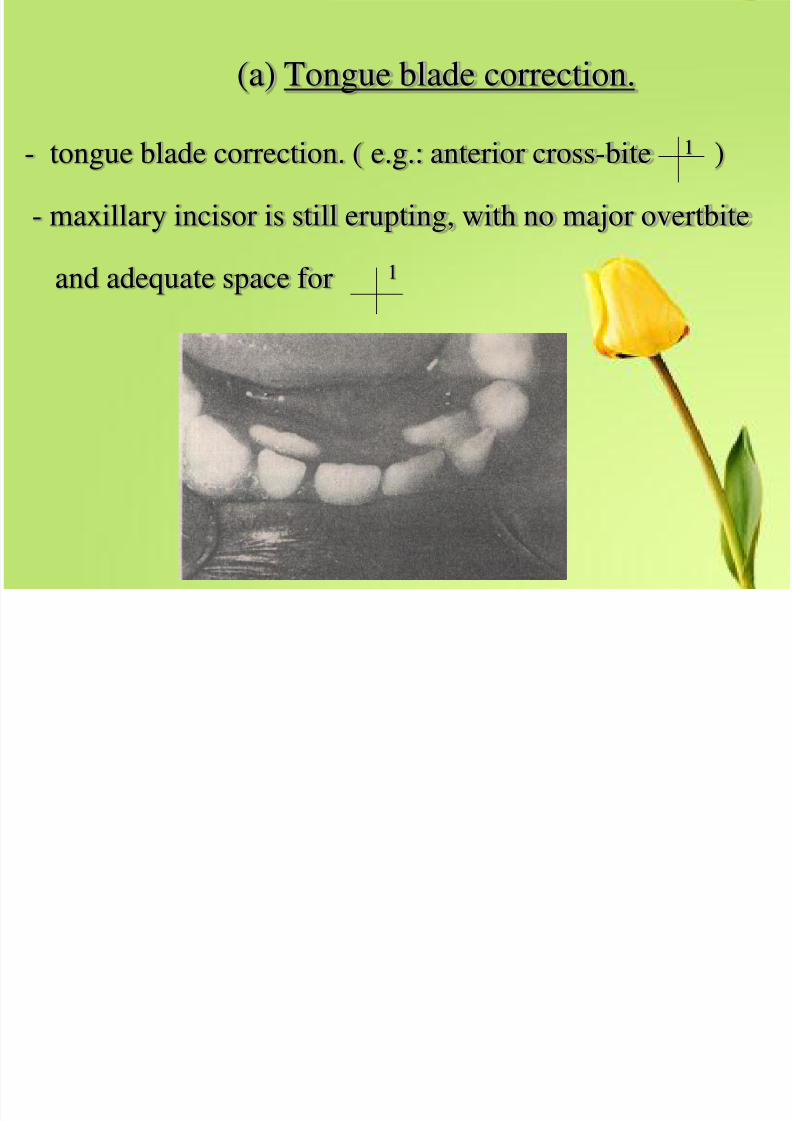
(a) Tongue blade correction.
- tongue blade correction. ( e.g.: anterior cross-bite 1 )
- maxillary incisor is still erupting, with no major overtbite
and adequate space for 1

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 10/39
The patient is instructed to insert the tongue blade at an
angle between the teeth and bite firmly, maintaining
the pressure for 5 sec, then interrupt and repeat for 25
times.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 11/39
• 3 times a day.
• if the tongue blade exercise is not
successful after 2 wks (or)
• if tooth eruption is too advanced, a bite
plane is more satisfactory.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 12/39
(b). Lower inclined bite plane.
• have sufficient inclination to produce a definite
forward sliding
• motion of the maxillary incisor on closure.
• should not impinge on soft tissue of the
mandibular teeth.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 13/39
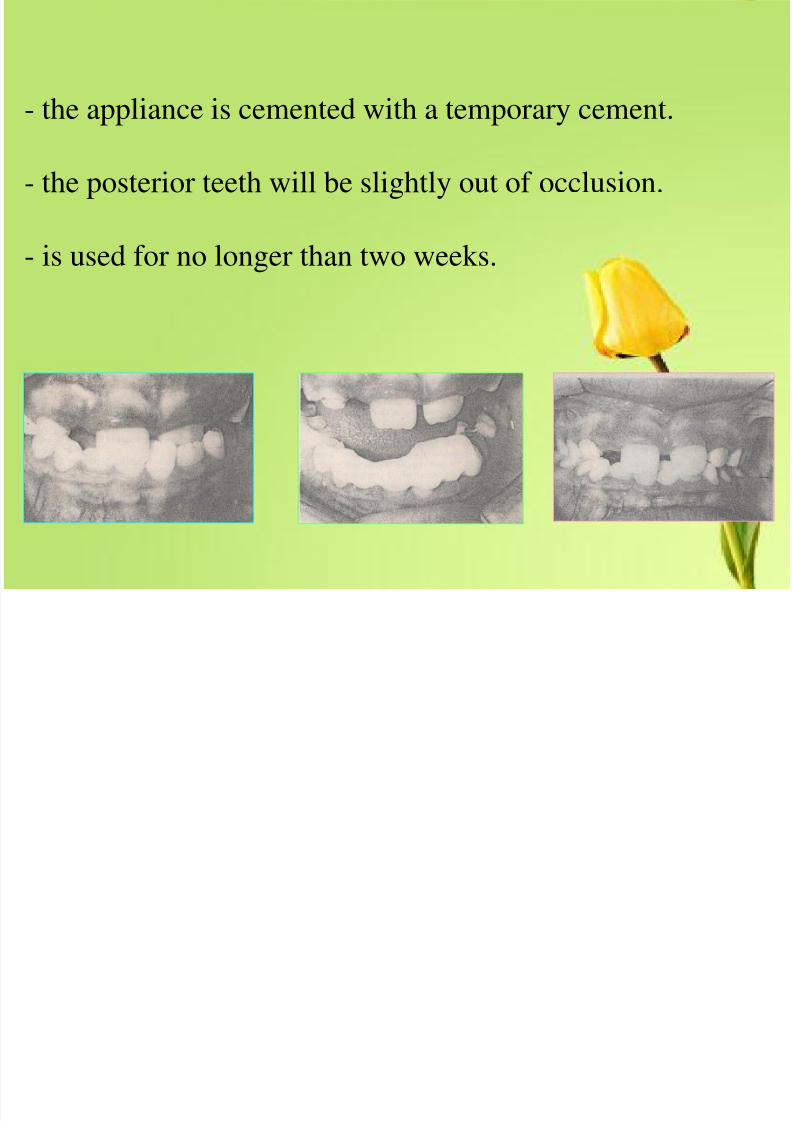
- the appliance is cemented with a temporary cement.
- the posterior teeth will be slightly out of occlusion.
- is used for no longer than two weeks.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 14/39
(C) Removable appliance with either cantilever
spring or screw
• single tooth – single or double cantilever spring.
• of more teeth are in cross bite – crossed
cantilever or a screw.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 15/39
• E.g. : instructions to the technician on applianceconstruction.
• Appliance design for a case with incisor cross-bite
on a child in a mixed dentition.
• Adam’s clasps on6 6
+D D
orE E
• Double cantilever spring ( Z spring) on 1
• Posterior bite plane half molar capping withadequate thickness.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 16/39
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 17/39
4. Posterior crossbite with displacement
- A unilateral posterior crossbite with displacement is
easily corrected during the mixed dentition,
- But one without an associated displacement is
probably skeletal in origin and correction should
not be attempted.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 18/39
Possible causes
• Narrow maxilla
• Deviated path of eruption of maxillary first
permanent molar.
Clinical features
• Cross-bite involving one or more posterior teeth
• Lateral displacement of the mandible.

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 19/39
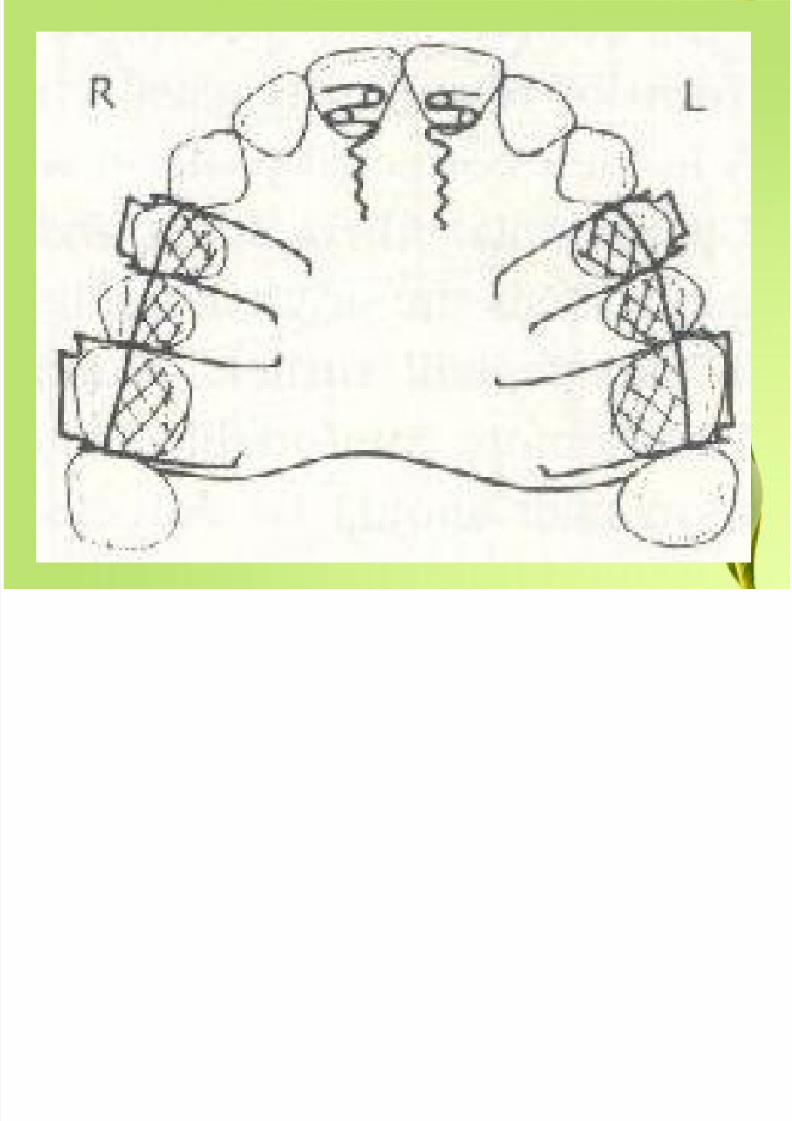
Design of the appliance
- Adams Clasps on 6D / D6
- Mid line expansion screw
- Half molar capping sufficiently thick to relieve
occlusal interference.

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 20/39
5. Median Diastema
Median Diastema spacing between
1 1
Common Causes
a. Physiological diastema
b. Retained primary teeth
c. Supernumerary teeth
d. Missing Lateral incisore. Fibrous frenum
f. microdontia 2 2
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 21/39

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 22/39
(a). Physiological diastema
• The diastema which develops between two
permanent central incisor is transient abnormality.
• Permanent incisors erupt into a more forward and
proclined position than their predecessors.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 23/39
- Normally this space closes spontaneously as the lateralincisors erupt, but may persist even after the lateral
incisors have erupted, particularly if the primary canines
have been lost and upper incisor become flared to the
labial.
( ugly duckling stage of development ).- No need of early correction and close spontaneously

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 24/39
(b). Retained primary teeth
• Remove the primary tooth and observe spontaneous
space closure.
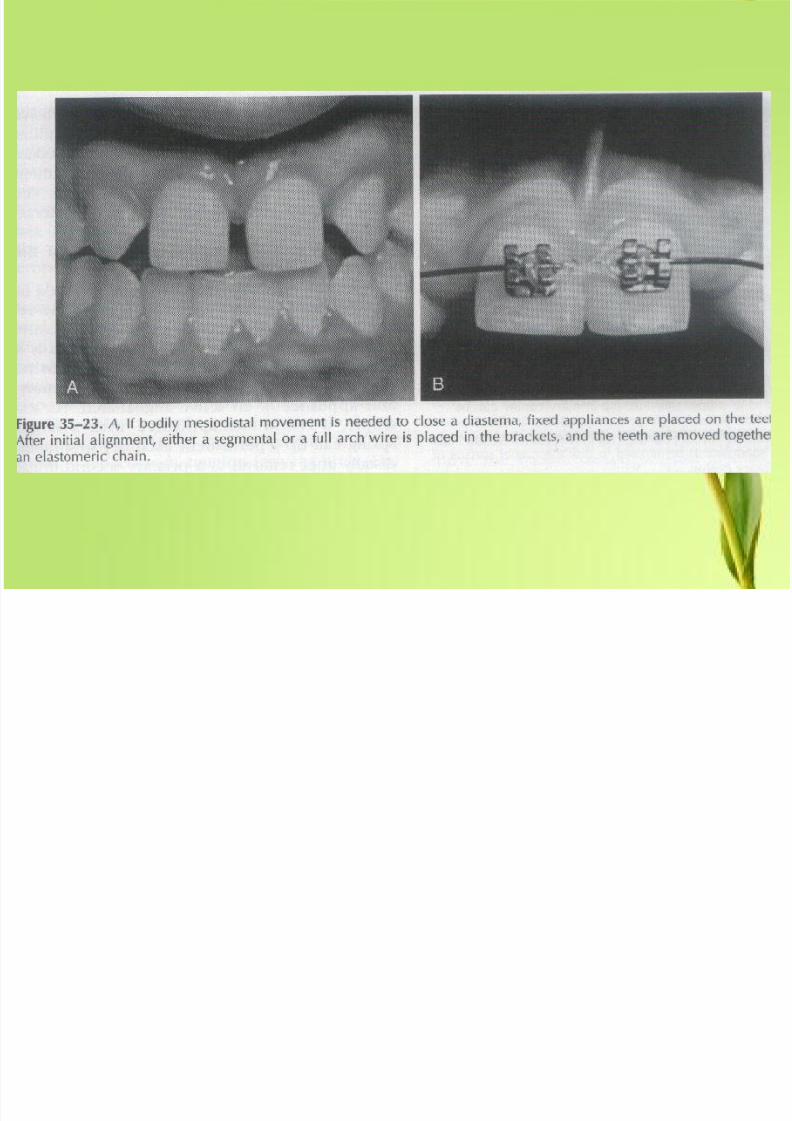
• If the space is not closing, close the diastema using
an appliance.
(c). Supernumerary teeth
• Management of Supernumerary teeth
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 25/39
(d). Missing Lateral incisor
Space closure between 1 1
Replacement (prosthesis) for missing lateral incisor.
(e). Fibrous frenum
Due to high frenum attachment ( Presence of
fibrous frenum extending from the incisive papilla to the
inner surface of the upper lip
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 26/39
(X-ray – inverted V shaped notch between central incisor
where the fibrous tissue of the frenum is attached.
Frenectomy after eruption of 3 3 and space
closure,
(f). Microdontia
Peg shaped lateral incisor 2 2
Space closure, crown build-up of 2 2 up to
normal form and size.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 27/39
Choice of the appliance
• Choice of the appliance depend on the width of the
diastema and the inclination of the incisor teeth.
• If the space is less than 2 mm or teeth are distally inclined
simple tipping movement with a removable
appliance can move the teeth into a normal
alignment.

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 28/39
6. Harmful Parafunctional habits
(a). Thumb sucking
(b). Finger sucking
(c). Nail biting
(d). Dummy sucking
(e) Lip sucking
(f). Prolonged bottle feeding
(g). Tongue thrust and mouth breathing habits

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 29/39
- The presence of an oral habit in the 3 to 6 year old
child is an important finding during clinical
examination.
- 6 year - is not usually present> 6 year – effect on eruption of permanent teeth
and occlusion.
Thus – should be eliminated before the permanent
incisors erupt.

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 30/39
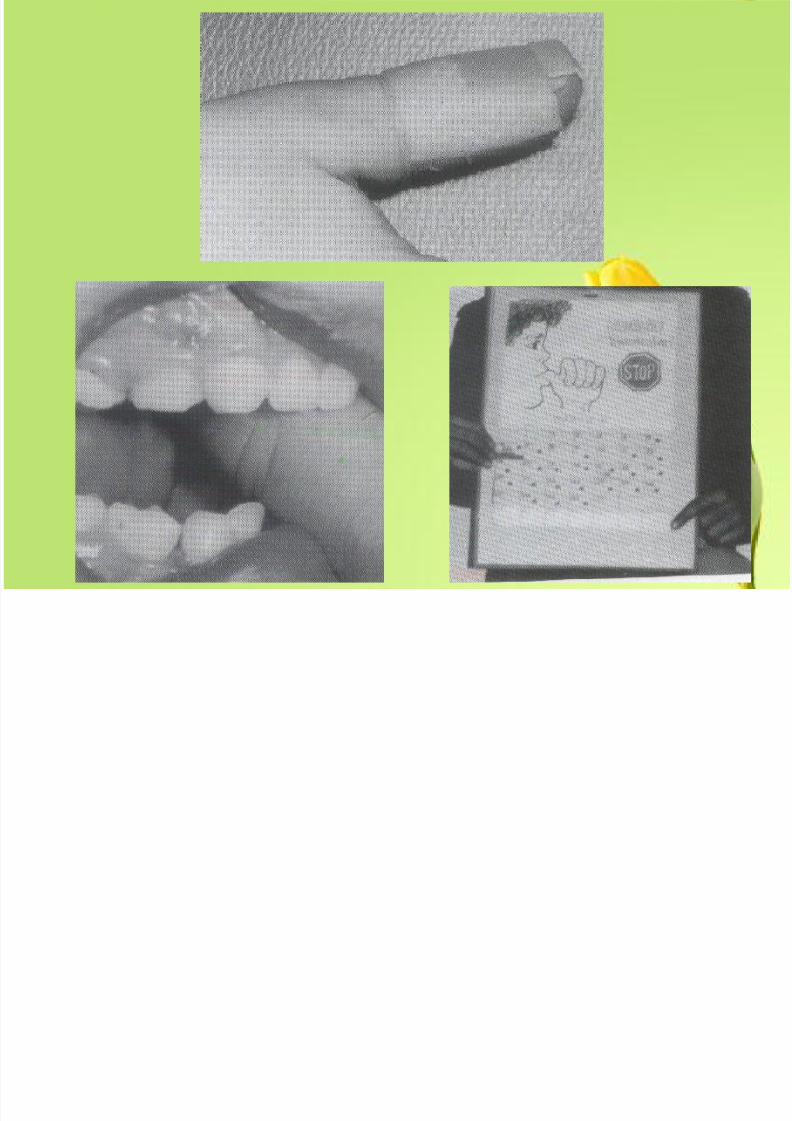
Thumb and Finger Habits
-Highly specified cause – and – effect relationship.-Types of dental changes vary with intensity,
duration and frequency of the habit as well as the
manner in which position of the digit in the mouth.
- 4 to 6 hrs of force per day are probably the minimum
necessary to cause the movement.-A child who sucks continuously ( > 6 hrs ) can
cause significant dental changes.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 31/39
Features of malocclusion
1. proclination of upper incisor2.retroclination of lower incisor
3.retardation of eruption of upper and lower teeth
4.asymmetric anterior open bite depending on the
side where the finger is held
5. adaptive tongue thrust
6. maxillary constriction – posterior cross bite.

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 32/39
Management
-Persuade the child to stop the habit
-Identify the child who is willing to stop the habit but
unable to do so at night
-Fit habit breaking appliance
-Correct adaptive tongue thrust using a tongue guard.
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 33/39
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 34/39
Dummy sucking ( Pacifier Habits )
-similar to changes created by thumb habits
-but ended before 5 years of age
-easy to stop this habits
-then start sucking a digit
-elimination of the subsequent finger habit maybecome necessary
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 35/39
Lip Habits ( Lip sucking )
-most lip habits do not cause
dental problems
-can maintain an existing malocclusion
-result is
a proclination of the maxillary incisorsa retroclination of the mandibular incisors
an increased overjet

8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 36/39
• Nail Biting
-no evidence it can cause malocclusion
or dental change
-other than minor enamel fracture
-some reported incisor rotation
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 37/39
Tongue Thrust and Mouth Breathing Habits
-tongue thrust is characteristic of the infantile
swallowing
-no simple cause – and – effect relationship
-may be able to sustain and open bite but not create one
( Proffit and Mason, 1975 )
-should be considered a finding and not a problem to be
treated
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 38/39
Mouth Breathers
-because of mandibular posture or incompetent lips or
a suspected nasal airway obstruction
-a weak relationship between mouth breathing and
malocclusion characterized by a long lower face and
maxillary constriction
8/3/2019 Interceptive Prof)
http://slidepdf.com/reader/full/interceptive-prof 39/39
End
Related Documents











