1 Integrated Medium Term Plan 2015/16 – 2017/18 Summary Document Bwrdd Iechyd Prifysgol Aneurin Bevan yw enw gweithredol Bwrdd Iechyd Lleol Prifysgol Aneurin Bevan Aneurin Bevan University Health Board is the operational name of Aneurin Bevan University Local Health Board

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Integrated Medium Term Plan
2015/16 – 2017/18
Summary Document
Bwrdd Iechyd Prifysgol Aneurin Bevan yw enw gweithredol Bwrdd Iechyd Lleol Prifysgol Aneurin Bevan Aneurin Bevan University Health Board is the operational name of Aneurin Bevan University Local Health Board
2
The Integrated Medium Term Plan
1. Introduction
This Integrated Medium Term Plan (IMTP) provides the Health Board with a process and vehicle to review and articulate the organisation’s values, future strategy, key
priorities and delivery actions for the period 2015/16 to 2017/18. It reiterates and reflects our values and commitment to engage and collaborate with partners, patients, communities and staff to deliver safe and high quality services. The plan reflects
current pressures and priorities and outlines the service and system change required to deliver the strategic future we set out in our Clinical Futures Strategy.
The plan highlights key priorities, actions and outcomes for delivering more patient centred services within local communities wherever possible. Those priorities have to
be set within a financial framework that is affordable and supported by workforce strategies for delivery and improvement. Priorities have been developed through
engagement processes with key partners and Divisions to provide the foundation for achieving delivery and also reflect national strategies and policy requirements.
The plan has focused on clarifying key priorities supported by actions, likely timescales and the expected benefits. This reflects significant progress compared to
the 2014/15 IMTP and we will continue to strengthen these through the delivery process. Effective alignment and connecting the outcomes of individual plans is critical to achieve more ambitious service and system change. There will be particular focus
on developing services which have a greater primary care focus to provide alternatives which are more accessible for patients. This will require developing the
necessary infrastructure and investment to support this shift to local delivery. The development of more appropriate services will require the Health Board to adapt
and modernise processes and health systems to make sure services are effective, safe, accessible and timely. This requires greater integration of services within
primary, community and secondary care services and with Social Care and third sector organisations.
The IMTP provides a comprehensive overview of Health Board plans. This document provides a synopsis of the planning process, service priorities, workforce implications
and financial plans and is supported by a detailed technical document. The technical document complies with Welsh Government Planning guidance.
We will robustly monitor and scrutinise the delivery of our plans, ensuring that benefits are realised by our citizens and key enablers to support change are
optimised.
3
2. Health Board’s Values and Mission
The Health Board strives for excellence in our collective efforts to deliver effective health care and encourages a culture of support, respect, integrity and teamwork.
This is balanced with always assessing and challenging services to strive for improvement to match and exceed national standards, learning from success and
identifying where improvements are required. This ambition must be driven by a commitment to work collaboratively and effective engagement with patients, communities, staff, partner organisations and government.
We believe in putting the patient first, staff taking personal responsibility to safeguard
patients, fostering a strong passion for improvement in delivery of services, and making sure that promoting pride in service delivery promotes improvements in patient experience.
Our mission and ambition is that by 2019:
Everyone is able to live longer healthier lives at home or in a homely setting. The
will be an integrated health and social care system, which includes housing and the third sector, built around Neighbourhood Care Networks focusing on prevention, anticipation and supported self management delivering reductions in health
inequalities in the most deprived communities.
Development of cohesive services for children, older and vulnerable people will be available to all the distinct communities served including an agreed suite of care pathways delivering care which is safe, local, citizen centred, clinically and cost
effective.
Sustainable 24/7 primary care services are in place to ensure that urgent and planned primary care is locally accessible to enable patients to receive their care close to home.
A more equal relationship between patients and professionals (using co-production
approaches), based on openness and sharing information ensuring that the intensity of testing and treatment is consistent with the seriousness of the illness and the individual patient goals.
Shift the balance of services to primary care by increasing the number of specialist
services currently provided in hospitals to primary care settings with more seamless collaboration between practitioners across the whole system. This will necessitate some services working very differently to support patients in primary care, through
direct patient contact, indirect support to practice teams and remote monitoring of patients.
Technological opportunities will be maximised with an integrated electronic health
and social care record system that allows clinicians and social care practitioners to
share information about patients that enables new workflows (for example virtual clinics, booking systems, advice lines) across the health and social care system,
which will also enable patients and carers to access appropriate, timely and relevant information. All our independent contractors will be part of the NHS network so that patients will have a single record that will facilitate shared care and
patient management across all settings.
4
All local services will be configured within the 12 Neighbourhood Care Networks and
designed to meet the health and social care needs of their communities. This will require a professional and managerial accountability structure to ensure the delivery of safe, effective, efficient services to meet the health and social care
needs of the communities they serve.
When hospital treatment is required, and cannot be provided in a community setting, day case and ambulatory care treatment will be the norm. There will be 24/7 access to consultant led hyper-acute and specialist care, facilitated by
consolidating these service in the newly opened Specialist and Critical Care Centre at Llanfrechfa Grange in 2019. Whatever the setting, care will be provided to the
highest standards of quality and safety, with the citizen at the centre of all decisions. At all times, in every part of the system, we will strive to be “best in
class”, pushing the boundaries of efficiency, effectiveness and proportional interventions in accordance with prudent healthcare. There will be a focus on ensuring that people are supported in their home or community environment as
soon as appropriate.
This will be supported by a reduction in health inequalities in the most deprived communities and a reduction in premature deaths in key conditions such as cancers, heart attacks and strokes. Our health service will be regarded as a caring and
improving health system built on a model where integration, partnership working, prudence and public participation are all paramount.
The delivery of these challenging and ambitious aspirations will require a significant refocusing on achieving major changes to align investment and improvements in
public health, facilitating more patient services being delivered within primary care and community services closer to patients’ homes, and sustainable secondary care
services which provide timely access for appropriate patients. Our values and plans have always had a strong focus on delivering safe and high
quality services and national targets in spite of challenges associated with increasing demands on health services, capacity pressures and the impact of challenges
associated with financial austerity. There is a collective determination to ensure that the values developed over recent years are sustained and that leadership continues to be based on fundamental standards, openness and transparency, candour with
patients, effective engagement with communities, patients, staff, and partners in planning and delivery of services in an effective manner.
5
3. Key Drivers Feedback from Engagement
Our commitment to improving service quality, patient safety and experience and the delivery of timely services for patients, not only focuses on delivery of key targets but
also ensuring that we are developing effective plans with communities and partner organisations to reduce the impact of health inequalities and promoting people to take more responsibility for their own health. The engagement process has identified key
issues where we must develop improved service:
Timely access to primary care, in particular General Practice Reliability and responsiveness of ambulance services Delays and queues in emergency departments
Knowledge of locally available services, understanding when and how to use them Concern that the Specialist and Critical Care Centre has not yet opened
Sustainability of the current system of care Increasing and persistent pressure on the health system
Maintaining focus on quality and patient care The necessity for change within healthcare systems and delivering key
improvements
Health Needs Assessment
The Health Board covers diverse geographical areas and covers a mix of rural, urban and valley communities. Many of these areas experience high levels of social deprivation, including low incomes, poor housing stock and high unemployment
resulting in many challenges:
Smoking is a major risk factor for heart disease and remains a significant public health concern with 24 per cent of the adult population being active smokers with the subsequent impact on quality of health and life expectancy.
A quarter of adults are obese (BMI ≥30) with rates in Blaenau Gwent, Torfaen and Caerphilly significantly higher than the Wales average.
Low participation of local residents undertaking physical exercise on a regular basis. Poor dietary habits illustrated with a survey in 2009/10 demonstrating the
proportion of adults in the Health Board who had consumed at least five portions of
fruit and vegetable in the previous day was 32 per cent. Alcohol misuse with around 43 per cent of adults reported drinking above
recommended limits in the previous week. In relation to patterns of alcohol misuse around 131,118 residents report binge drinking.
Deprivation is higher than the Welsh average, ill health more prevalent and life
expectancy is 10 years lower for residents in the most deprived areas of Gwent then in the least deprived areas.
Four of the Local Authority areas a high percentage of children are living in poverty Children living in a deprived area in Gwent are less likely to be breast fed and more
likely to have dental caries which is an indicator of a poor diet.
The latest projections indicate that if current trends continue, the number of persons
aged 65 and over will increase from one in five residents in 2015 (108,500 people) to one in four by 2030 (153,000 people). The proportion aged 75 and over is projected to increase from 10% to 19%, the sharpest increases being in Monmouthshire and
Torfaen. By 2030 8% of our citizens will be 85, more than double the proportion in
6
2015. The increase in the number of older people is likely to be associated with a rise in long-term conditions whose prevalence is strongly age-related, such as circulatory
and respiratory diseases, cancers and dementia.
We face major challenges linked to health inequalities and the consequent impact in demand for services particularly associated with cancers, cardio vascular diseases and dementia. Working collaboratively with partners to support people to adjust lifestyles
improves health status, reduce or delay the onset chronic conditions and improve life expectancy and quality of life in older years is of a critical component of any strategy
to deliver a sustainable health care system.
Legacy Issues from the 2014/15 Plan Significant progress has been made in improving performance on many issues during
the past 12 months including: Major improvement in the care of Stroke patients with the ring fencing beds
improving performance against Bundle 2 of the Stroke pathway. Sustaining improvements in reducing C Diff rates and numbers with a reduction of
46% on the previous year. Sustaining the lowest level of MRSA rates in Wales for several years.
Significant reduction in the backlog of Outpatient follow up patients and plans in place to deliver further improvement.
Reduction in the Health Board’s RAMI to 94 (lowest in Wales) in June 14 compared
to the Welsh average of 103. Sustaining good compliance with patient safety solutions for alerts and rapid
response notices together with comparatively low number of serious incidents. Continued to ensure good access for patients to GP and Dental services. Major changes to the Minor Oral Surgery and Glaucoma pathways to reduce
demand to secondary care and develop more sustainable services. Progress achieved in improving outpatient services in Neurology, Diabetes,
Orthopaedics and Nephrology. Published the second Annual Quality Statement outlining the positive progress
being actioned.
Positive progress with the digitisation of medical records with over 60,000 patients now having their records available in a digitised format.
Progress achieved in recovering cancer performance during late 2014. Developed plans for delivery of the Prudent Healthcare agenda. Developed an approach for convergence of WCP and the local Health Board clinical
portal to further promote the National IT Programme. Good progress in implementing Nursing Principles although recruitment difficulties
may be a risk to delivery. Investment in Public Health to target improvements in population health prioritising
smoking cessation, immunisations and obesity.
Agreed plans and investment to improve compliance with the Mental Health Measure requirements without losing the well regarded service model.
Achieving more progress in integrating services in primary, secondary and community care, including care of the elderly and frail and development of integrated pathways for minor oral surgery and ophthalmology.
Increasing healthcare improvement and R&D activity reflecting the benefits of University Health Board status and building our partnership with Cardiff University
on pioneering applied mathematical modelling in UK health care through our ABCi. Rolled out the Values and Behaviour framework across the Health Board.
7
Improved levels of medical appraisals with sustainable plans going forward. Progressed work to deliver the SCCC and participated fully in the ongoing work of
the South Wales Programme.
There have been major challenges in key delivery areas during 2014/15, particularly
with waiting times for treatment; cancer waits in some specialties; and in keeping pace with unscheduled care demand. These pressures are not unique to Gwent, but
experienced throughout the United Kingdom. Locally, much of this increased demand is generated by our system’s inability to adequately care for the growing number of elderly frail patients. The impacts on our ability to manage flow for all our patients
(planned and unscheduled care needs) across the system are significant. Some of the key areas to focus on in 2015/16 to recover a more timely access to services include:
Reducing the number of patients waiting for long periods of time in Accident and
Emergency departments. Working with ambulance services to make sure patients are directed to the best
place to meet their needs to reduce delays for ambulances at hospitals.
Reducing waiting times for patients requiring outpatient assessment, diagnostic investigation or planned surgery.
Reducing variation in cancer waiting times by resolving some key workforce issues in Breast services.
Reducing the number of patients waiting for outpatient follow up.
These challenges illustrate that current service models need to evolve to meet
changing needs for health services, particularly reviewing traditional systems and approaches. These changes range from using key skills available in the primary care contractor professions such as Pharmacists, Optometrists, Dentists and Podiatrists,
bespoke community models of care for elderly and frail patients and the application of prudent principles in supporting patients in accessing effective treatment. It also
illustrates the need to modernise some services to make sure that patients can be seen by staff with the skills to deal with their issues safely and in a timely manner.
Key Challenges arising from Demographic Changes Health Services are facing unprecedented challenges from demographic changes
which are already resulting in increased demands on services. There has been a significant increase in age and lifestyle related chronic conditions which require the development of more integrated service models across primary care and hospital
services.
Demands on community services which extends to nursing home provision and funded nursing care (FNC) are similarly increasing, resulting in major capacity and financial challenges. Community services play an important role by providing more appropriate
services releasing hospitals to provide acute and rehabilitation services in a timelier manner.
Risks to Service Sustainability Our services need to adapt and develop to reflect the wider requirements of the health
service nationally and locally. In addition to demographic changes there are also regulatory pressures, including the changing arrangements for junior medical training
which will require investment and different solutions impacting on services with the immediate challenge being in Paediatrics, Obstetrics and General Surgery.
8
4. The Health Board’s Strategic Direction Our Clinical Futures Strategy sets out the strategic direction for modernising clinical services. A central theme is the creation of “networks” that bring care as close to the
patient as possible through progressive working practices within Neighbourhood Care Networks (NCNs), a new relationship with patients as experts in their own health, the use of new technology, and our maturing NCNs as the vehicle through which local
services are organised and delivered. They are already becoming the fundamental building blocks that bind together the work of all partners in health and care in a
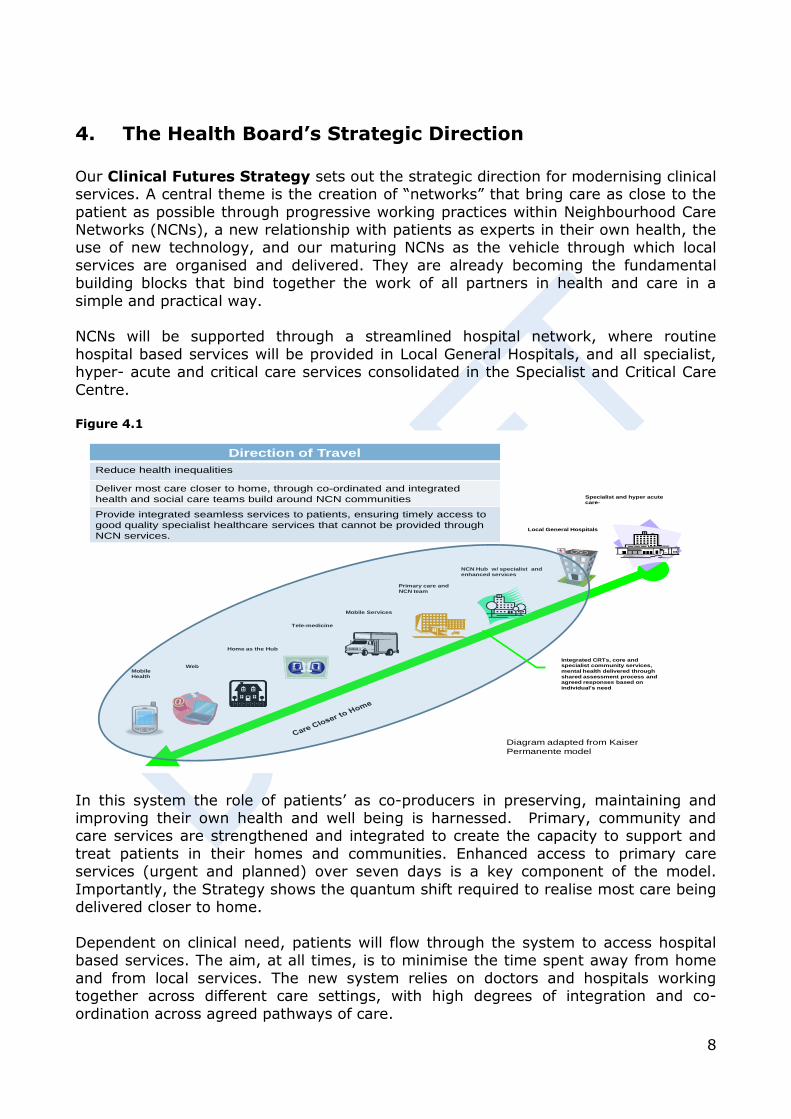
simple and practical way. NCNs will be supported through a streamlined hospital network, where routine
hospital based services will be provided in Local General Hospitals, and all specialist, hyper- acute and critical care services consolidated in the Specialist and Critical Care
Centre. Figure 4.1
In this system the role of patients’ as co-producers in preserving, maintaining and improving their own health and well being is harnessed. Primary, community and care services are strengthened and integrated to create the capacity to support and
treat patients in their homes and communities. Enhanced access to primary care services (urgent and planned) over seven days is a key component of the model.
Importantly, the Strategy shows the quantum shift required to realise most care being delivered closer to home.
Dependent on clinical need, patients will flow through the system to access hospital based services. The aim, at all times, is to minimise the time spent away from home
and from local services. The new system relies on doctors and hospitals working together across different care settings, with high degrees of integration and co-
ordination across agreed pathways of care.
2
Mobile Services
NCN Hub w/ specialist and enhanced services
Primary care and NCN team
Web
Tele-medicine
Local General Hospitals
Specialist and hyper acute care-
Home as the Hub
Mobile Health
Integrated CRTs, core and specialist community services,
mental health delivered through
shared assessment process and agreed responses based on
individual’s need
Direction of Travel
Reduce health inequalities
Deliver most care closer to home, through co-ordinated and integrated
health and social care teams build around NCN communities
Provide integrated seamless services to patients, ensuring timely access to
good quality specialist healthcare services that cannot be provided through
NCN services.
Diagram adapted from Kaiser
Permanente model
9
The Welsh Government has set out the national strategic direction for Health Boards and
Trusts within the overarching ‘Programme for Government’ and the NHS Wales Strategy ‘Together for Health’, underpinned by more detailed strategies and delivery plans based on key service areas or population groups and linked to the seven strategic
themes of ‘Together for Health’, namely:
Service modernisation, including more care closer to home and specialist centres of excellence
Addressing health inequalities
Better IT systems and an information strategy ensuring improved care for patients Improving quality of care
Workforce development Instigating a “compact with the public” and
A changed financial regime
We support these themes and feels that they are fully reflected in our local strategic
plans. Our Clinical Futures Strategy has to make sure that the health system works effectively with partners to manage increasing demand for services, delivering
effective, safe and sustainable services within the context of considerable workforce and social change.
We will continue to work collaboratively with other Health organisations. The South Wales Programme focused on the optimum, sustainable configuration for some
specialist hospital based services (consultant-led maternity and neo-natal care, paediatrics and emergency medicine). Specifically it considered those services where seriously ill and/or injured patients who need to be in hospital will have better and faster access to
care from senior and expert doctors and their teams, which will have an immediate and direct effect on their recovery.
The Acute Care Alliances (ACAs) were established in 2014 as the mechanism through which the outcome of the South Wales Programme (SWP) would be
implemented, monitored and reviewed. For the UHB, the outcome was the reconfiguration of services in line with the Board’s Clinical Futures Strategy, with the
Specialist and Critical Care Centre (SCCC) an essential development in enabling change. We are part of the South East ACA, with the Clinical Futures Board the structure supporting local planning, with representation from Powys Health Board. We
work closely with neighbouring ACAs and Health Boards on a number of service issues, notably where there are potential changes to patient flows e.g. with the Heads
of the Valleys population. Our Board recognises its role as the decision making body of matters related to ACAs and retains full accountability.
10
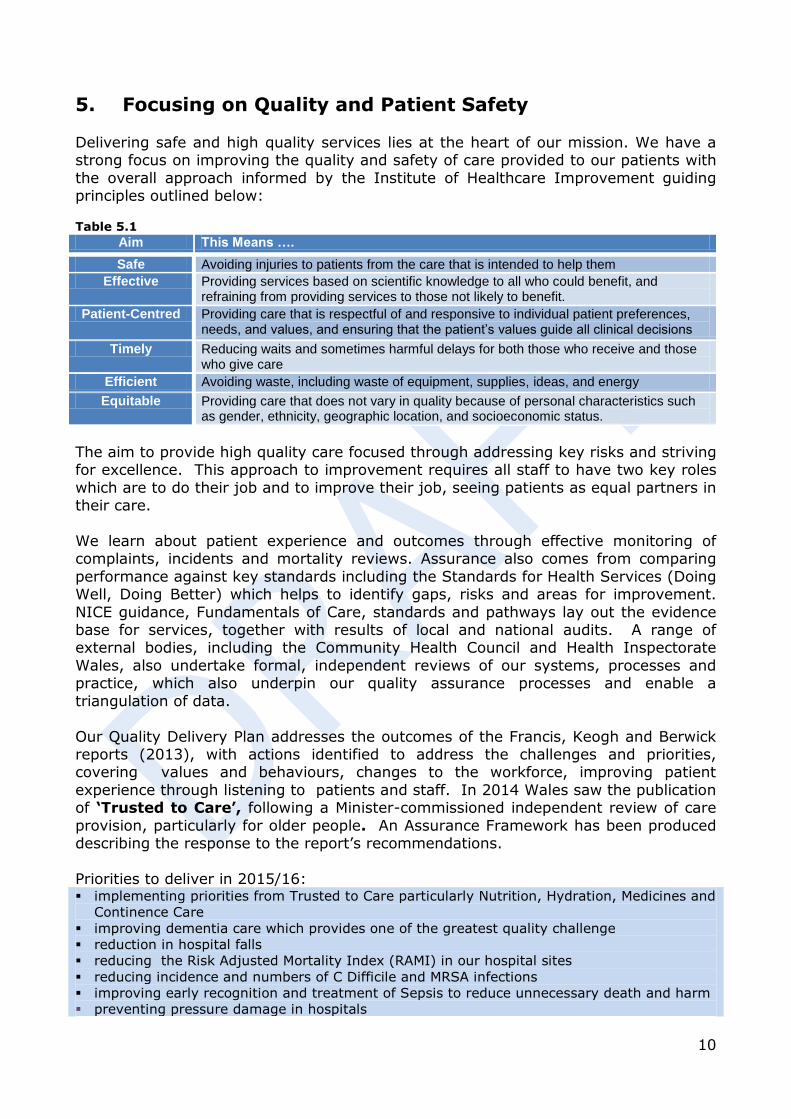
5. Focusing on Quality and Patient Safety Delivering safe and high quality services lies at the heart of our mission. We have a strong focus on improving the quality and safety of care provided to our patients with
the overall approach informed by the Institute of Healthcare Improvement guiding principles outlined below: Table 5.1
Aim This Means ….
Safe Avoiding injuries to patients from the care that is intended to help them
Effective Providing services based on scientific knowledge to all who could benefit, and refraining from providing services to those not likely to benefit.
Patient-Centred Providing care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that the patient’s values guide all clinical decisions
Timely Reducing waits and sometimes harmful delays for both those who receive and those who give care
Efficient Avoiding waste, including waste of equipment, supplies, ideas, and energy
Equitable Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status.
The aim to provide high quality care focused through addressing key risks and striving for excellence. This approach to improvement requires all staff to have two key roles
which are to do their job and to improve their job, seeing patients as equal partners in their care.
We learn about patient experience and outcomes through effective monitoring of complaints, incidents and mortality reviews. Assurance also comes from comparing
performance against key standards including the Standards for Health Services (Doing Well, Doing Better) which helps to identify gaps, risks and areas for improvement.
NICE guidance, Fundamentals of Care, standards and pathways lay out the evidence base for services, together with results of local and national audits. A range of external bodies, including the Community Health Council and Health Inspectorate
Wales, also undertake formal, independent reviews of our systems, processes and practice, which also underpin our quality assurance processes and enable a
triangulation of data.
Our Quality Delivery Plan addresses the outcomes of the Francis, Keogh and Berwick reports (2013), with actions identified to address the challenges and priorities, covering values and behaviours, changes to the workforce, improving patient
experience through listening to patients and staff. In 2014 Wales saw the publication of ‘Trusted to Care’, following a Minister-commissioned independent review of care
provision, particularly for older people. An Assurance Framework has been produced describing the response to the report’s recommendations.
Priorities to deliver in 2015/16: implementing priorities from Trusted to Care particularly Nutrition, Hydration, Medicines and
Continence Care
improving dementia care which provides one of the greatest quality challenge
reduction in hospital falls
reducing the Risk Adjusted Mortality Index (RAMI) in our hospital sites
reducing incidence and numbers of C Difficile and MRSA infections
improving early recognition and treatment of Sepsis to reduce unnecessary death and harm
preventing pressure damage in hospitals
11
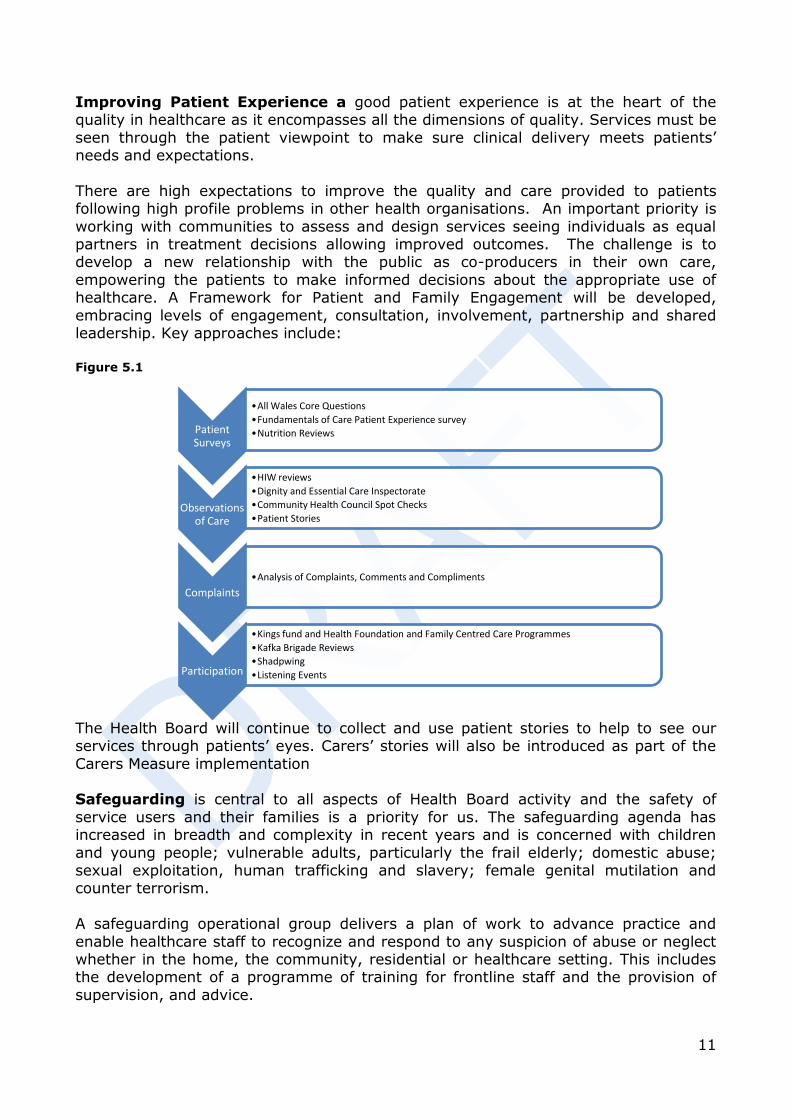
Improving Patient Experience a good patient experience is at the heart of the quality in healthcare as it encompasses all the dimensions of quality. Services must be
seen through the patient viewpoint to make sure clinical delivery meets patients’ needs and expectations.
There are high expectations to improve the quality and care provided to patients following high profile problems in other health organisations. An important priority is
working with communities to assess and design services seeing individuals as equal partners in treatment decisions allowing improved outcomes. The challenge is to develop a new relationship with the public as co-producers in their own care,
empowering the patients to make informed decisions about the appropriate use of healthcare. A Framework for Patient and Family Engagement will be developed,
embracing levels of engagement, consultation, involvement, partnership and shared leadership. Key approaches include:
Figure 5.1
The Health Board will continue to collect and use patient stories to help to see our services through patients’ eyes. Carers’ stories will also be introduced as part of the
Carers Measure implementation Safeguarding is central to all aspects of Health Board activity and the safety of
service users and their families is a priority for us. The safeguarding agenda has increased in breadth and complexity in recent years and is concerned with children
and young people; vulnerable adults, particularly the frail elderly; domestic abuse; sexual exploitation, human trafficking and slavery; female genital mutilation and counter terrorism.
A safeguarding operational group delivers a plan of work to advance practice and
enable healthcare staff to recognize and respond to any suspicion of abuse or neglect whether in the home, the community, residential or healthcare setting. This includes the development of a programme of training for frontline staff and the provision of
supervision, and advice.
Patient Surveys
•All Wales Core Questions
•Fundamentals of Care Patient Experience survey
•Nutrition Reviews
Observations of Care
•HIW reviews
•Dignity and Essential Care Inspectorate
•Community Health Council Spot Checks
•Patient Stories
Complaints
•Analysis of Complaints, Comments and Compliments
Participation
•Kings fund and Health Foundation and Family Centred Care Programmes
•Kafka Brigade Reviews
•Shadpwing
•Listening Events
12
A Safeguarding Committee, chaired by an Independent Member, provides the strategic lead and reports to the Quality and Patient Safety Committee. Senior
representation on the regional Children’s Safeguarding Board, Adult Safeguarding Board and Multi- Agency Public Protection Strategic Management Board supports close inter-agency working and in the scrutiny of inter-agency practice to identify where
improvements can be made. Over the coming year the Health Board will be working with partner agencies to further strengthen safeguarding processes and practice in
meeting the requirements for the implementation of the Social Services and Well-being (Wales) Act 2014 and the Gender-based Violence, Domestic Abuse and Sexual Violence (Wales) bill, introduced in June 2014.
13
6. Mechanism to deliver our Strategic Direction and
address challenges
The previous sections identified some of the key challenges that need to be addressed if we are to advance our goals of improving access, quality and sustainability through
an increasingly prudent healthcare system. If we are to realise our vision, as set out in our Clinical Futures Strategy, we must take action to:
Increase focus on helping people and communities stay healthy Meet the needs of a growing ageing population and people with chronic disease
Address disparities in low socioeconomic populations Provide care in the most appropriate setting and in a timely manner Improve access to a range of services delivered through Neighbourhood Care
Network teams and improve patient flow across the system Develop a workforce that will meet future needs and provide a flexible, challenging,
safe and satisfying work environment Realise the benefits of our integrated health system by adopting quality clinical
practices including standardising pathways of care, anticipating needs, fostering
innovation and promoting better outcomes. Improve information and measurement systems to support decision making and
delivery.
This list is not exhaustive but illustrates the multifaceted and co-ordinated work required to address current challenges and to truly transform the health system. Transformation is not an instant process and requires careful consideration of
priorities, appropriately phased actions and appropriate alignment of resources to achieve the best outcomes, now and in the future.
As we develop our service strategies, the UHB will organise these changes around two fundamentally important and interlinked relationships. These are:
How services are shaped with communities
and other partners to best improve health and prevent early onset of illness and injury. This requires focus on specific
improvement goals tailored to these communities and groups, developing cross
cutting public sector supports and enabling local ownership of this improvement.
How services are organised to meet the patients’ need for quality, accessibility and
sustainable care, from initial assessment through to treatment and discharge or ongoing care. This means designing our system along
key pathways of care – describing the life events when health-care needs arise from birth
to death and when treatment is needed. We will design these pathways based on best evidence, driven by prudent healthcare principles and
quality and measure the improvement.
Figure 6.1 - Integrating Service Response

14
As a further step toward this vision of integration and improvement, we are concentrating our change efforts into the delivery of preventative activities with
neighbourhood care networks as the primary mechanism for delivering care, access to the right service, flow through the system and service sustainability. Our priority plans have been aligned and organised around 10 service change plans. These are:
Table 6.1
SCP Title SCP Title
1 Reducing Health Inequalities 6 Continuing Health Care
2 Prevention and Improving Population Health 7 Service Sustainability
3 Primary Care and Provider Services 8 Mental Health and Learning Disability
4 Integration – Bringing Care Closer to Home 9 Urgent and Emergency Care
5 Chronic Conditions Management 10 Planned Care
Figure 6.2 below illustrates how these programmes align and the intended outcomes or contribution they make to deliver our vision. Figure 6.2
There will be a shift in the balance of services to Neighbourhood Care Networks, by increasing the range of hospital based services that will be delivered in primary and
community care settings and there will be seamless collaboration between practitioners across the whole system. This will necessitate working very differently to focus on supporting patients in a primary care setting, through direct patient contact,
indirect support to NCN teams and remote monitoring for patients.
Significant enabling plans related to finance, infrastructure, workforce, delivery and information technology are being developed and aligned with the priorities and outcome targets identified in each of the Service Change Plans. Table x summarises
plans that require additional investment, together with applicable funding streams.
Improve Health and Prevent Early Onset of Illness/Injury
Service Change Plans 1 and 2
Reduce health inequalities and lessen demand for healthcare
Building a Neighbourhood Care Network Foundation for Delivery of Care
Service Change Plans 3,4,5, and 8
Provide majority of care through integrated teams organised around our 12 NCN Communities
Improving Access; Flow and Reducing Waits
Service Change Plans 9 and 10
Robust needs assemments, demand/capacity alignment that minimises coversion from NCNs to secondary care and maximise timely provision of
care when required
Service Sustainability
Service Change Plans 6 and 7
Ensuring services that are clinically or financially vulnerable are stablised and maintained for our citizens , and where relevant, across
South Wales

15
Summary table
No. UHB plans Funding stream
1 Living Well, Living Longer programme to reduce health inequalities in most deprived areas
Pathfinders/Once for Wales
2 Increase access to Smoking cessation services in primary care to reduce burden of disease
Primary Care
3 To reduce referrals to secondary care through introduction community
MSK & OA knee programme
Primary Care
4 To develop a multi-professional Primary Care support and improvement team to support practices in difficulty, test out new service models and enable service improvement
Primary Care
6 To optimising GP access and agree health Board standards that build on 5As for Access
Primary Care
7 To improve support to Care Homes through effective medicines
management and anticipatory care planning to reduce secondary care admissions
Primary Care
8 To realign district nursing services to NCNs and increase capacity to meet primary and secondary care demand
Primary Care
9 To transform prison healthcare services Primary Care
10 To transform the minor oral surgery pathway Primary Care
11 To transform ophthalmic provision through development of a primary care based Ophthalmology Diagnostic Treatment Centres
Primary Care
12 To support NCN development Primary Care
13 To implement a number of Local Authority schemes to Intermediate Care Fund
14 To strengthen community cardiac failure services to improve patient
care and reduce admissions
Primary Care
15 To transform the respiratory pathway Primary Care
16 To transform the diabetes pathway, transformation Primary Care
17 To strengthen patient support and education within Primary Care Primary Care
18 To improve outcomes and reduce length of stay through implementation of a community neuro-rehabilitation service
Primary Care
19 To redesign the stroke service to improve outcomes Intermediate Care Fund
20 To strengthen CAMHS services to meet demand and improve access Primary Care
21 To strengthen Primary Care Mental Health Teams to improve access
and reduce waiting times
Primary Care
22 To use the RAID programme to improve patient care and reduce demand on secondary care
Intermediate Care Fund
23 With the third sector, to extend care co-ordination across Gwent to
maintain independent living and reduce demand on secondary care
Primary Care
24 To improve pharmacy support to NCNs to improve both access and patient care
Primary Care
25 To strengthen frailty services to maintain care of patients in the community
Primary Care
26 To improve the care of elderly patients through the creation of Elderly Frail Units
Primary Care
28 To implement patient flow technologies to improve patient flow Technologies fund
29 To improve access to physiotherapy and occupational therapy through
7 day working
Primary Care
30 To expand telemedicine to provide support to primary care and shift balance of care
Technologies fund
31 To extend the role of Community Resource Teams to support Out Of Hours GP services
Primary Care

16
7. Improving Health and Preventing Early Onset of Illness and Injury
The health of individuals and our population as a whole is affected by several factors;
the socioeconomic environment; where we live and work; genetic makeup; the presence of risks to health; individual lifestyle choices; and access to health and supports. Taken together, these factors determine how healthy we are as individuals
and as residents of Gwent.
Major health disparities exist in Gwent that are differentially distributed among populations by gender, education, income and other indicators of disadvantage. Not only are the consequences of disparities avoidable, they are costly. Evidence suggests
that, as well as the burden of ill health for individuals, health inequalities cost the economy around £31-£33 billion each year in loss of productivity and £20 - £32 billion
in lost taxes and welfare payments. Treatment of the disease outcomes of these health inequalities consumes 1/3rd of the NHS budget, with direct treatment costs in England amounting to £5.5 billion per year. Reducing the current rate of heart
disease, stroke, cancer, diabetes and liver disease for the most deprived fifth of the population to nearer the rate for the least deprived fifth would make a significant
contribution towards the UHBs ability to create a sustainable healthcare system for Gwent.
A co-ordinated effort is required to promote and protect the health of our citizens and to address health inequalities.
Service Change Plan 1 – Reducing Health Inequalities is a systematic,
population scale programme, to increase the prevention, early identification and optimal primary care management of heart disease, stroke, diabetes, cancer and liver disease in our most deprived communities, where the rates of these diseases are
highest.
Reducing health inequalities across the UHB matters because, on average, there is nearly a 10 year difference in the average life expectancy at birth between men in the very least and very most deprived fifths of the population and around a 20 year
difference in healthy life expectancy. A similar pattern is true for women too. Inequalities are particularly evident in cancer incidence, mortality and survival.
Emergency hospital admissions rate is twice as high for people living in the most deprived areas compared with rates for the least.
Of the patients living in the most deprived fifth areas of
Wales, around 66% were registered within the catchment area of five of
our Neighbourhood Care Networks.
Graph 7.1 - % of patients living in most deprived fifth of areas in Wales, NCN clusters in ABUHB 2013
17
The Living Well, Living Longer programme has been designed to have population
impact on inequalities in health over a five year time period. The programme will address inequalities in access to primary care; develop a sustainable primary care system for identification and management of chronic cardiovascular disease and
cancers in the highest areas of need. This programme is a core component of our delivery plans for heart disease, stroke, diabetes and liver disease. It focuses on:
Identification and reduction of risk of cardiovascular disease. Reducing inequalities in cancer incidence and stage of presentation.
Reducing inequalities in health expectancy due to lifestyle risk factors.
The programme will co-produce with communities a network of support for people to make healthy changes to their lifestyle, building on local assets such as Communities
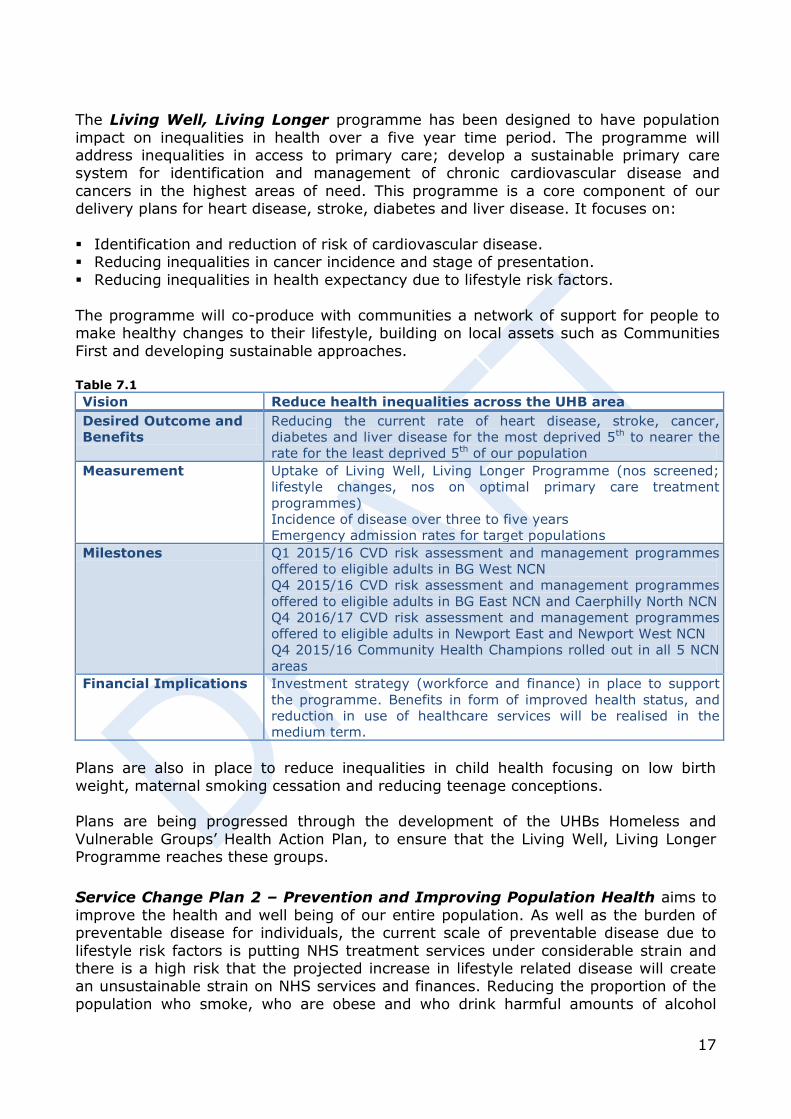
First and developing sustainable approaches. Table 7.1
Vision Reduce health inequalities across the UHB area
Desired Outcome and
Benefits
Reducing the current rate of heart disease, stroke, cancer,
diabetes and liver disease for the most deprived 5th to nearer the
rate for the least deprived 5th of our population
Measurement Uptake of Living Well, Living Longer Programme (nos screened;
lifestyle changes, nos on optimal primary care treatment
programmes)
Incidence of disease over three to five years
Emergency admission rates for target populations
Milestones Q1 2015/16 CVD risk assessment and management programmes
offered to eligible adults in BG West NCN
Q4 2015/16 CVD risk assessment and management programmes
offered to eligible adults in BG East NCN and Caerphilly North NCN
Q4 2016/17 CVD risk assessment and management programmes
offered to eligible adults in Newport East and Newport West NCN
Q4 2015/16 Community Health Champions rolled out in all 5 NCN
areas
Financial Implications Investment strategy (workforce and finance) in place to support
the programme. Benefits in form of improved health status, and
reduction in use of healthcare services will be realised in the
medium term.
Plans are also in place to reduce inequalities in child health focusing on low birth
weight, maternal smoking cessation and reducing teenage conceptions. Plans are being progressed through the development of the UHBs Homeless and
Vulnerable Groups’ Health Action Plan, to ensure that the Living Well, Living Longer Programme reaches these groups.
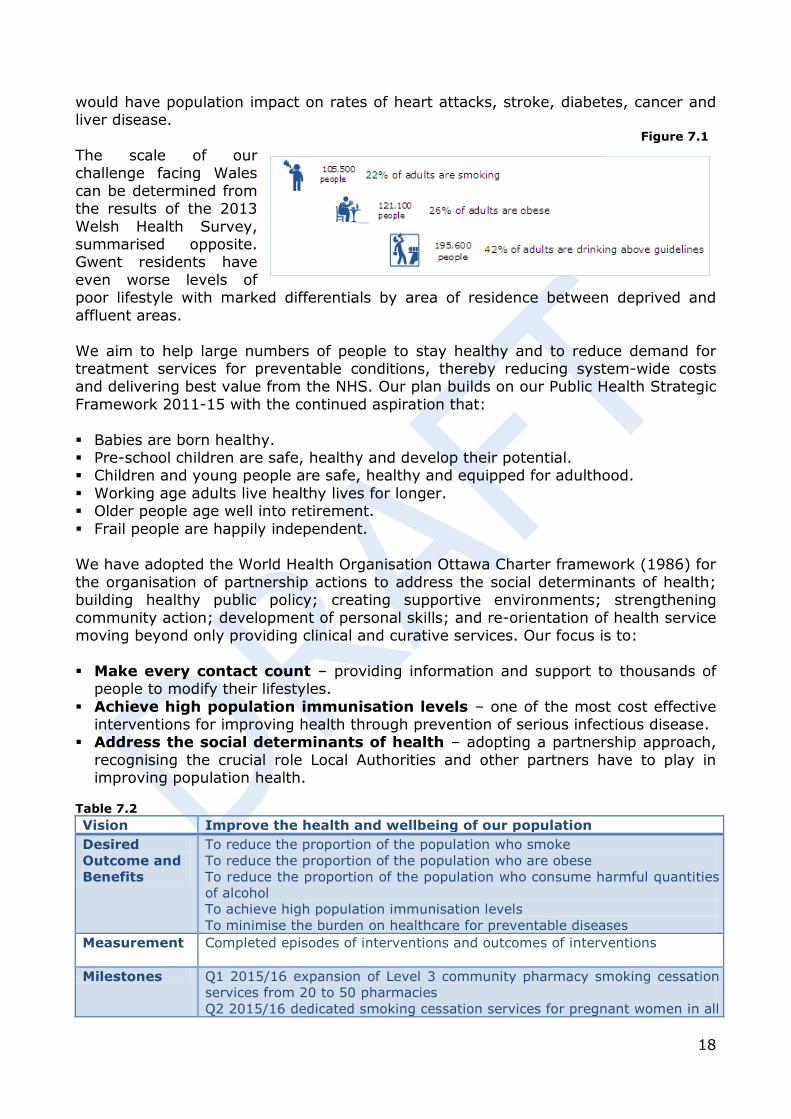
Service Change Plan 2 – Prevention and Improving Population Health aims to
improve the health and well being of our entire population. As well as the burden of preventable disease for individuals, the current scale of preventable disease due to
lifestyle risk factors is putting NHS treatment services under considerable strain and there is a high risk that the projected increase in lifestyle related disease will create an unsustainable strain on NHS services and finances. Reducing the proportion of the
population who smoke, who are obese and who drink harmful amounts of alcohol
18
would have population impact on rates of heart attacks, stroke, diabetes, cancer and liver disease.
The scale of our challenge facing Wales
can be determined from the results of the 2013
Welsh Health Survey, summarised opposite. Gwent residents have
even worse levels of poor lifestyle with marked differentials by area of residence between deprived and
affluent areas.
We aim to help large numbers of people to stay healthy and to reduce demand for treatment services for preventable conditions, thereby reducing system-wide costs and delivering best value from the NHS. Our plan builds on our Public Health Strategic
Framework 2011-15 with the continued aspiration that:
Babies are born healthy. Pre-school children are safe, healthy and develop their potential. Children and young people are safe, healthy and equipped for adulthood.
Working age adults live healthy lives for longer. Older people age well into retirement.
Frail people are happily independent. We have adopted the World Health Organisation Ottawa Charter framework (1986) for
the organisation of partnership actions to address the social determinants of health; building healthy public policy; creating supportive environments; strengthening
community action; development of personal skills; and re-orientation of health service moving beyond only providing clinical and curative services. Our focus is to:
Make every contact count – providing information and support to thousands of people to modify their lifestyles.
Achieve high population immunisation levels – one of the most cost effective interventions for improving health through prevention of serious infectious disease.
Address the social determinants of health – adopting a partnership approach,
recognising the crucial role Local Authorities and other partners have to play in improving population health.
Table 7.2
Vision Improve the health and wellbeing of our population
Desired
Outcome and
Benefits
To reduce the proportion of the population who smoke
To reduce the proportion of the population who are obese
To reduce the proportion of the population who consume harmful quantities
of alcohol
To achieve high population immunisation levels
To minimise the burden on healthcare for preventable diseases
Measurement Completed episodes of interventions and outcomes of interventions
Milestones Q1 2015/16 expansion of Level 3 community pharmacy smoking cessation
services from 20 to 50 pharmacies
Q2 2015/16 dedicated smoking cessation services for pregnant women in all
Figure 7.1
19
Vision Improve the health and wellbeing of our population
5 Local Authority areas
Q4 2015/16 Child Obesity Action Plan agreed by all agencies
Q4 2016/17 achieve UNICEF Baby Friendly Accreditation and increase
numbers of mothers breastfeeding at 6 weeks
Q1 2015/16 Adult Weight Management Service extended to include routine
referrals of patients presenting with knee pain who are obese
Q1 2015/16 Child Weight Management Service Treatment Pathway agreed
Q4 2015/16 Alcohol Harm Reduction Pathway develop and agreed with
partners
Q4 2015/16 delivery of immunisation and vaccination programmes
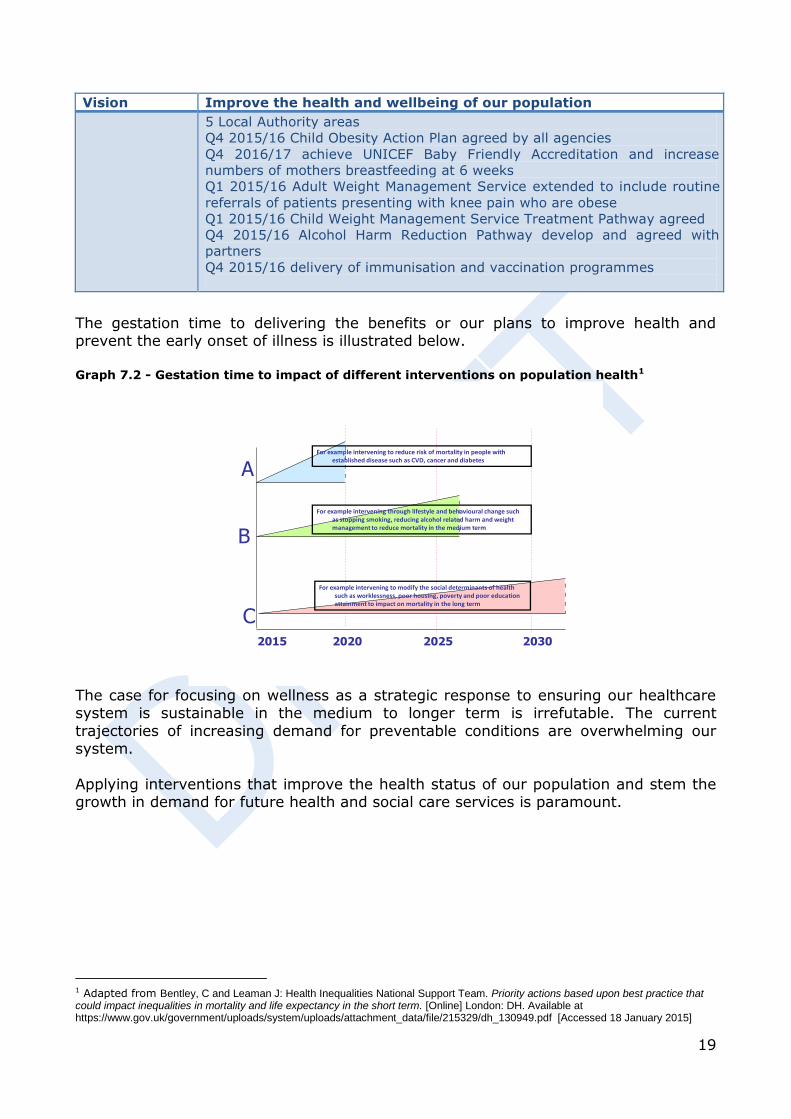
The gestation time to delivering the benefits or our plans to improve health and prevent the early onset of illness is illustrated below.
Graph 7.2 - Gestation time to impact of different interventions on population health1
2015 2020 2025 2030
A
B
C
For example intervening to reduce risk of mortality in people with established disease such as CVD, cancer and diabetes
For example intervening through lifestyle and behavioural change such as stopping smoking, reducing alcohol related harm and weight management to reduce mortality in the medium term
For example intervening to modify the social determinants of health such as worklessness, poor housing, poverty and poor education attainment to impact on mortality in the long term
The case for focusing on wellness as a strategic response to ensuring our healthcare system is sustainable in the medium to longer term is irrefutable. The current
trajectories of increasing demand for preventable conditions are overwhelming our system.
Applying interventions that improve the health status of our population and stem the growth in demand for future health and social care services is paramount.
1 Adapted from Bentley, C and Leaman J: Health Inequalities National Support Team. Priority actions based upon best practice that could impact inequalities in mortality and life expectancy in the short term. [Online] London: DH. Available at https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/215329/dh_130949.pdf [Accessed 18 January 2015]
20
8. Building a Neighbourhood Care Network Foundation for
Delivery of Care
Care at home, or in the patient’s community, with the most appropriate person, with the right skills delivering care at the right time, is the unequivocal aim of our future
vision. Strengthening Primary and Community Care services is therefore our top priority and the central tenet of our Clinical Futures Strategy and a key component of the Social Service and Wellbeing Act.
In 2011 we established 12 Neighbourhood Care
Networks (NCN), each comprising of primary care, health and social care, housing and third sector community providers operating within the boundaries
of the neighbourhood. The original role was facilitative and enabling, responding to local need and national
priorities across health and social care and has resulted in increased uptake of influenza immunisations, smoking cessation and the
development of the Living Well, Living Longer programme.
Our decision to actively adopt this broader integrated
network approach (as opposed to clusters of General Practitioners) places our NCHs in a strong position to capitalise at pace, on the opportunities presented by the national Primary Care Plan and the Social Service and Wellbeing Act implementation and
crucially the direction of travel set by the Health Board.
Creating the capacity to deliver care closer to home will be achieved through the integration of treatment and care for our NCN communities. Our plans bind together the work of all partners in health and social care in a simple and practical
way. Our twelve NCNs will become the focus for the communities they service, building multidisciplinary teams supporting local people with physical, psychological
and social care needs. It is essential that the priorities for primary and community services as articulated through the five Single Integrated Plans, developed at a Local Authority level, are reflected and delivered through our NCNs. Over the next
three years NCNs will become the main vehicle that drives the implementation of our key priorities, including our response to the Social Services and Wellbeing Act.
Our clinically led NCNs create annual plans which are focused on discrete communities of 30 to 50,000 people. These plans reflect the needs of their neighbourhood
population and underpin the key role that NCNs play in determining future models for integrated service design and delivery. NCNs are in a unique position to:
Reduce Health inequalities through the Living Well, Living Longer programme and
supporting lifestyle changes.
Actively involve of the public, patients and their carers in decisions about their care and wellbeing.
Deliver improvements in access and quality of care. Enable and support the provision of more care closer to home, where appropriate
and reducing any unnecessary attendance in hospital settings.
Figure 8.1
21
Refocus the balance of care through adopting co-ordinated care models where generalists work closely with specialists and wider support in the community to
prevent ill health, reduce dependency and effectively treat illness. Ensure all services and clinical pathways comply with prudent healthcare principles. Directly support the development of the Specialist and Critical Care Centre, and the
Clinical Futures Hospital network – ensuring that we deliver a truly integrated system of care.
Our vision is to deliver most care closer to home (System change) by re-engineering the whole pathway of care with the express intention of providing most of
the pathway closer to home. These pathways will play a crucial role in simplifying our system of care and improving flow at the interface points to minimise fragmentation
and avoidable delay in the patient journey. They will assist both health and social care staff and patients understand and achieve the best approaches for care which is safe,
person centred, clinically and cost effective. We recognise that the combination of targeted action within primary care services and informing and empowering the individual with a condition will improve their sense of wellbeing and avoid repeated
admission to hospital.
Four separate but interconnected Service Change Plans - SCP 3 (Independent Contractor Services, 4 (Integration and NCN development), 5 (Chronic Conditions) and 8 (Mental Health) - have been developed to progress our ambition to create a
Primary Care led NHS. They are designed strengthen universal primary care services, and to create the capacity to integrate care for frail older people and people with
chronic conditions. Our ambition is to attain the scale of service transformation that has been achieved in mental health services over recent decades (i.e. reducing the need for hospital based care through developing pro-active, robust, integrated, multi-
disciplinary and multi-agency teams in our communities).
Our plans for Mental Health and Learning Disability (SCP 8) services make a significant contribution to the delivery of care closer to home.
Service Change Plan 3 – Primary Care Services (Independent Contractors) sets out the unique role of primary care in co-ordinating care for people to the wide range
of services delivered by our healthcare system. Primary Care is a crucial component of the strategic solution for sustainable healthcare. Whilst we have had success in using General Dental Practitioners and Community Optometrists to provide minor oral
surgery and glaucoma assessment services in a primary care setting, which would have traditionally been provided in a hospital setting, we recognise the opportunities
that exist in working collaboratively to provide more care closer to home. We have plans to develop Primary Care Ophthalmic Diagnostic and Treatment Centres to treat glaucoma initially with the potential to manage Wet AMD.
There are significant challenges in recruitment and retention of GPs across the UK
mirrored withnin the Health Board. Consequently, our plan is predicated on planning for a more sustainable GP workforce whose role will increasingly be to provide overarching leadership of a range of health care professionals.
Improving Access to (Contractor) universal services by developing sustainable
primary care services (urgent and planned care) over 7 days. This includes innovative service and staffing models to ensure that citizens have reliable access to primary
22
care clinicians that offer a better alternative than attending Emergency Departments or relying on Out of Hours Services such as 7 day minor illness centres.
Optimising access to primary care also helps improve quality, patient experience and over reliance on secondary care services. Our focus is based on:
Matching demand and capacity (for core and enhanced services).
Reducing variation across contractor services that cannot be explained on the basis of illness, medical evidence or patient preference.
Extending range of services provided through primary care contractor services
(General Dental Services, Primary Care Eye Services and Community Pharmacies). Sustainable workforce (for core and 7 day General Medical Service provision).
IM&T capability to provide timely access to shared information necessary to co-ordinate and manages care.
Supporting the development of the general practice infrastructure of estate and I M & T.
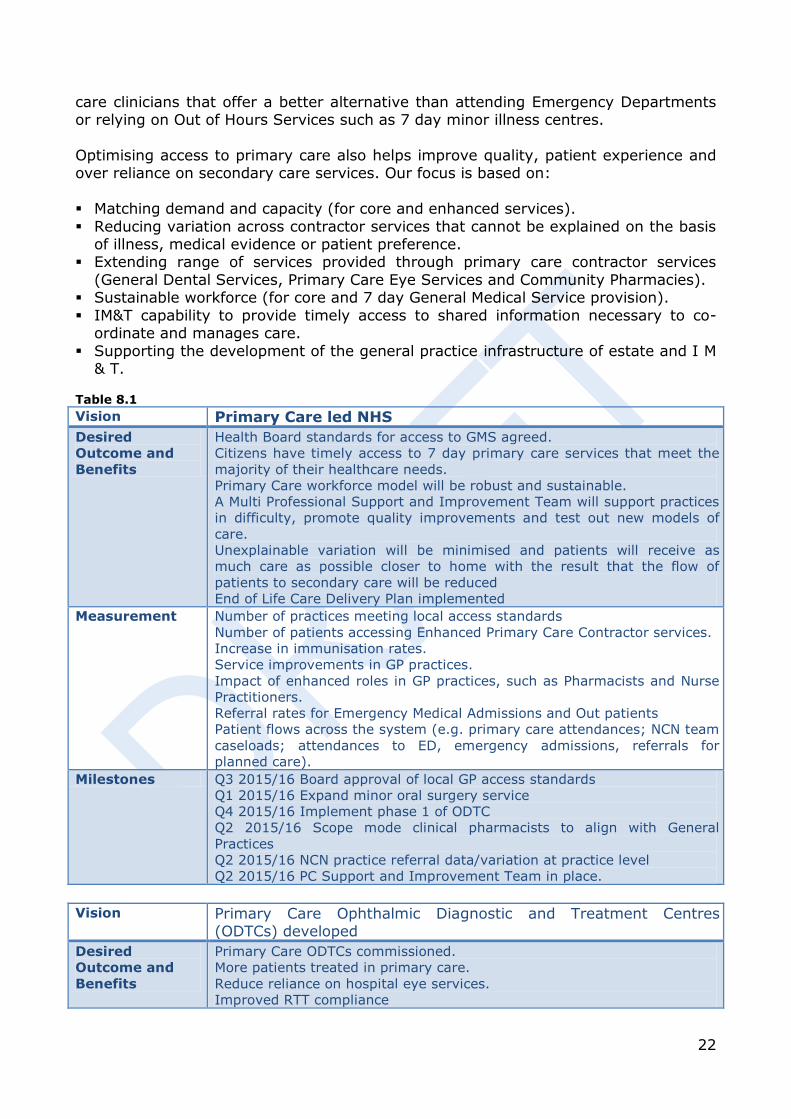
Table 8.1
Vision Primary Care led NHS
Desired
Outcome and
Benefits
Health Board standards for access to GMS agreed.
Citizens have timely access to 7 day primary care services that meet the
majority of their healthcare needs.
Primary Care workforce model will be robust and sustainable.
A Multi Professional Support and Improvement Team will support practices
in difficulty, promote quality improvements and test out new models of
care.
Unexplainable variation will be minimised and patients will receive as
much care as possible closer to home with the result that the flow of
patients to secondary care will be reduced
End of Life Care Delivery Plan implemented
Measurement Number of practices meeting local access standards
Number of patients accessing Enhanced Primary Care Contractor services.
Increase in immunisation rates.
Service improvements in GP practices.
Impact of enhanced roles in GP practices, such as Pharmacists and Nurse
Practitioners.
Referral rates for Emergency Medical Admissions and Out patients
Patient flows across the system (e.g. primary care attendances; NCN team
caseloads; attendances to ED, emergency admissions, referrals for
planned care).
Milestones Q3 2015/16 Board approval of local GP access standards
Q1 2015/16 Expand minor oral surgery service
Q4 2015/16 Implement phase 1 of ODTC
Q2 2015/16 Scope mode clinical pharmacists to align with General
Practices
Q2 2015/16 NCN practice referral data/variation at practice level
Q2 2015/16 PC Support and Improvement Team in place.
Vision Primary Care Ophthalmic Diagnostic and Treatment Centres (ODTCs) developed
Desired
Outcome and
Benefits
Primary Care ODTCs commissioned.
More patients treated in primary care.
Reduce reliance on hospital eye services.
Improved RTT compliance
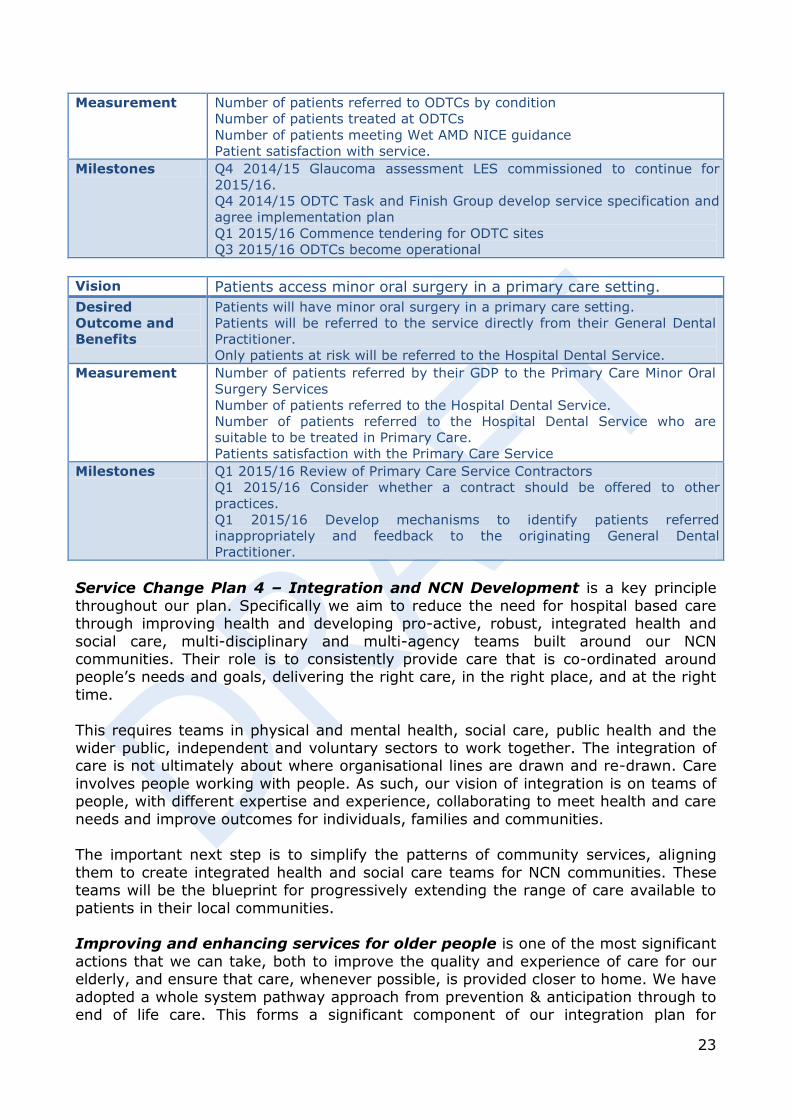
23
Measurement Number of patients referred to ODTCs by condition
Number of patients treated at ODTCs
Number of patients meeting Wet AMD NICE guidance
Patient satisfaction with service.
Milestones Q4 2014/15 Glaucoma assessment LES commissioned to continue for
2015/16.
Q4 2014/15 ODTC Task and Finish Group develop service specification and
agree implementation plan
Q1 2015/16 Commence tendering for ODTC sites
Q3 2015/16 ODTCs become operational
Vision Patients access minor oral surgery in a primary care setting.
Desired
Outcome and
Benefits
Patients will have minor oral surgery in a primary care setting.
Patients will be referred to the service directly from their General Dental
Practitioner.
Only patients at risk will be referred to the Hospital Dental Service.
Measurement Number of patients referred by their GDP to the Primary Care Minor Oral
Surgery Services
Number of patients referred to the Hospital Dental Service.
Number of patients referred to the Hospital Dental Service who are
suitable to be treated in Primary Care.
Patients satisfaction with the Primary Care Service
Milestones Q1 2015/16 Review of Primary Care Service Contractors
Q1 2015/16 Consider whether a contract should be offered to other
practices.
Q1 2015/16 Develop mechanisms to identify patients referred
inappropriately and feedback to the originating General Dental
Practitioner.
Service Change Plan 4 – Integration and NCN Development is a key principle
throughout our plan. Specifically we aim to reduce the need for hospital based care through improving health and developing pro-active, robust, integrated health and
social care, multi-disciplinary and multi-agency teams built around our NCN communities. Their role is to consistently provide care that is co-ordinated around people’s needs and goals, delivering the right care, in the right place, and at the right
time.
This requires teams in physical and mental health, social care, public health and the wider public, independent and voluntary sectors to work together. The integration of care is not ultimately about where organisational lines are drawn and re-drawn. Care
involves people working with people. As such, our vision of integration is on teams of people, with different expertise and experience, collaborating to meet health and care
needs and improve outcomes for individuals, families and communities. The important next step is to simplify the patterns of community services, aligning
them to create integrated health and social care teams for NCN communities. These teams will be the blueprint for progressively extending the range of care available to
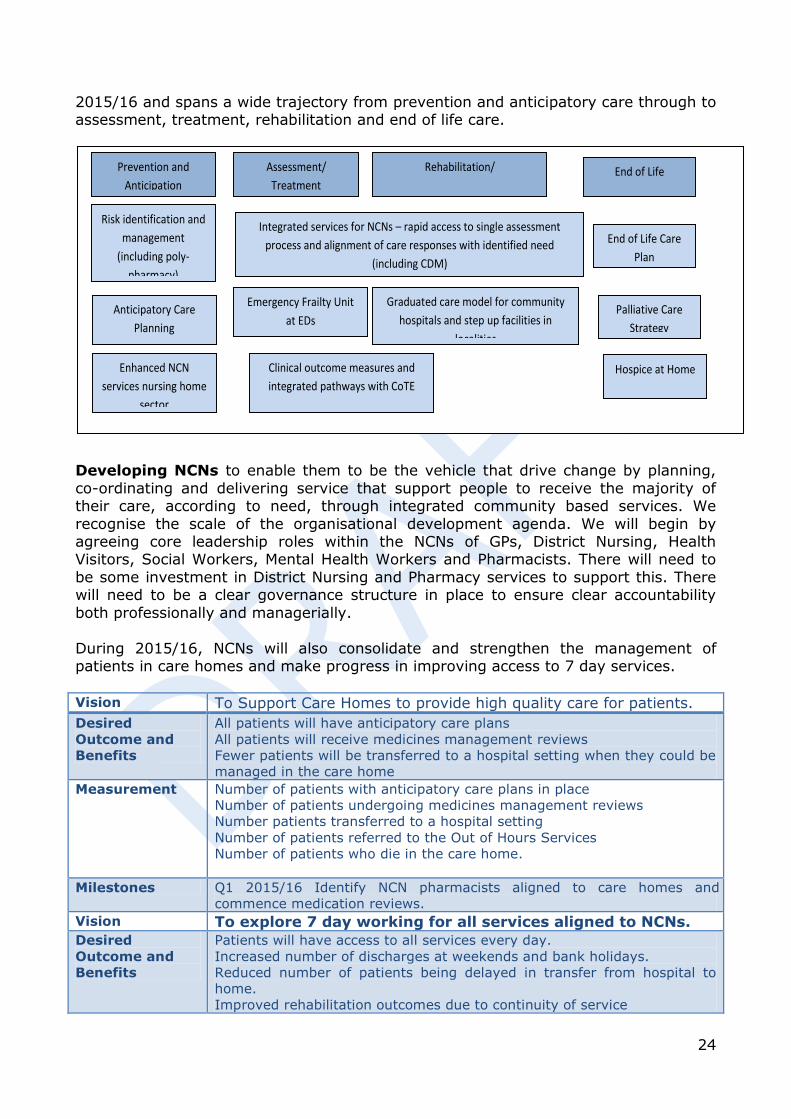
patients in their local communities. Improving and enhancing services for older people is one of the most significant
actions that we can take, both to improve the quality and experience of care for our elderly, and ensure that care, whenever possible, is provided closer to home. We have
adopted a whole system pathway approach from prevention & anticipation through to end of life care. This forms a significant component of our integration plan for
24
2015/16 and spans a wide trajectory from prevention and anticipatory care through to assessment, treatment, rehabilitation and end of life care.
Developing NCNs to enable them to be the vehicle that drive change by planning,
co-ordinating and delivering service that support people to receive the majority of their care, according to need, through integrated community based services. We
recognise the scale of the organisational development agenda. We will begin by agreeing core leadership roles within the NCNs of GPs, District Nursing, Health Visitors, Social Workers, Mental Health Workers and Pharmacists. There will need to
be some investment in District Nursing and Pharmacy services to support this. There will need to be a clear governance structure in place to ensure clear accountability
both professionally and managerially.
During 2015/16, NCNs will also consolidate and strengthen the management of patients in care homes and make progress in improving access to 7 day services.
Vision To Support Care Homes to provide high quality care for patients.
Desired
Outcome and
Benefits
All patients will have anticipatory care plans
All patients will receive medicines management reviews
Fewer patients will be transferred to a hospital setting when they could be
managed in the care home
Measurement Number of patients with anticipatory care plans in place
Number of patients undergoing medicines management reviews
Number patients transferred to a hospital setting
Number of patients referred to the Out of Hours Services
Number of patients who die in the care home.
Milestones Q1 2015/16 Identify NCN pharmacists aligned to care homes and
commence medication reviews.
Vision To explore 7 day working for all services aligned to NCNs.
Desired
Outcome and
Benefits
Patients will have access to all services every day.
Increased number of discharges at weekends and bank holidays.
Reduced number of patients being delayed in transfer from hospital to
home.
Improved rehabilitation outcomes due to continuity of service
Assessment/
Treatment
Prevention and
Anticipation End of Life Rehabilitation/
Recovery/ Maintenance
Risk identification and
management
(including poly-
pharmacy)
Integrated services for NCNs – rapid access to single assessment
process and alignment of care responses with identified need
(including CDM)
Anticipatory Care
Planning
Emergency Frailty Unit
at EDs
Dementia Pathway (including RAID – see SCP 8)
End of Life Care
Plan
Enhanced NCN
services nursing home
sector
Graduated care model for community
hospitals and step up facilities in
localities
Clinical outcome measures and
integrated pathways with CoTE
Palliative Care
Strategy
Hospice at Home
25
Measurement No of patients accessing services at weekends and bank holidays
No of discharges at weekends.
Number of patients referred to out of hours with exacerbations of chronic
conditions.
Number of patients attending hospitals with exacerbations of chronic
conditions.
Milestones Q1 2015/16 Identify additional capacity required to enable 7 day working
Q2 2015/16 Additional staff in place
Prison healthcare – we are responsible for healthcare provision at HMP Usk and Prescoed Prison, with a prisoner population of 520. Prisoners should be able to receive
the same access to healthcare as the general population, this is currently compromised by a reliance on hospital based services, where the prison capacity to comply with prisoner escort arrangements cannot meet demand. Our plan sets out to
develop and implement in-reach services, maximise virtual services and reduce inequalities in access to physical and mental healthcare services.
Vision Prisoners in the secure estate will receive the same standard of care as people living in the community.
Desired
Outcome and
Benefits
Prisoners will be supported to make positive lifestyle changes
Prisoners will be supported to stop smoking in preparation for the Prison
Smoking ban being enforced.
Prisoners will have access to a range of Independent Contractors.
Prisoners will have as much care as possible within the secure setting.
Measurement General medical Services Quality and Outcomes Framework data.
Reductions in number of prisoners smoking
Increase in immunisation uptake
Increase in prisoners screened for Blood Bourne Viruses.
Increase in number of in reach services for mental health support
Increase in patients accessing General Dental Services and Optometry
Services
Milestones Q1 2015/16 Smoking cessation across both sites
Q1 2015/16 All patients to undergo timely chronic conditions management
reviews
Q2 2015/16 Establish in reach sexual health clinics
Q4 2015/16 Prepared for impact of Social Services and Well Being Act
implementation
Q4 2015/16 Improve uptake of blood bourne virus screening
Service Change Plan 5 – Chronic Conditions there is a strong link between
deprivation and the numbers of people with poor health including chronic health conditions, for example the incidence of diabetes in Wales is almost doubled in areas
of high deprivation compared to areas of least deprivation. The burden of chronic conditions for our population is significant as illustrated in Figure x.

26
While our plans to reduce the burden of ill-health through reducing health inequalities
(SCP1) and prevention and improving population health (SCP2) will deliver benefits in the medium/long term, supporting our citizens who currently live with one or more
long term conditions is a key priority. Managing patients with chronic conditions is a core component of General Medical Services and the plans set out in SCP 3 and 4 are fundamental to optimising outcomes for our citizens with chronic conditions.
A holistic approach to care frames evidence based practice for each chronic condition,
and we are adopting a whole system pathway approach for diabetes, chronic respiratory disease and arthritic knee. Co-production is central to all our interactions with patients.
Patient activation and learning to self manage their condition has not been promoted
and supported as extensively as it needs to be. This has led to a dependency relationship with health services, which needs to be altered and the balance of responsibility focused on enabling patients to be active and central participants in
managing their condition. There are several education and rehabilitation programmes available, although these do not meet demand and are not always well attended, with
only a small number of people completing the full programmes. We are working with Colleges of Further Education to develop modular programmes that are more accessible to patients and their carers.
Our plans are based on the principle of prudent healthcare, supporting people to be
full participants in their care, providing information, advice and support to make appropriate lifestyle choices and changes, maintaining psychological and emotional wellbeing, improving early detection and optimal management of their chronic
conditions, predominantly in primary and community care settings. Our approach is illustrated through the work we are progressing on the management of diabetes.
Figure 8.3 - WHS results - ABUHB residents by LA, health board and Wales for selected
conditions
0
10
20
30
40
50
60
High Bp Arthritis Heart condition
Respiratory Condition
Diabetes Mental Illness
Caer BG Tor Mon Npt ABUHB Wales

27
The prevalence of Type 2 Diabetes in our local population is 27% higher than the UK average with 37,311 residents being cared for predominantly by local primary care
(85%) supported by specialist secondary care diabetes services. 90% of patients have Type 2 diabetes, and the numbers of people who develop Type 2 diabetes is expected to rise sharply over the next 10 years. 30% of our adult population are at significant
risk of developing the condition and any actions we can take to improve health and prevent the early onset of diabetes form a central plank of our approach to developing
sustainable services. To deliver the highest possible level of care for the increasing number of citizens with
diabetes we are moving from the current two stream service to one where we have a fully integrated diabetic pathway spanning patient education/participation, primary
care and specialist inpatient and ambulatory care. Figure x below illustrates the integrated pathway and highlights the key changes that will be progressed through
this service change plan.
Table 8.3
Vision An integrated diabetes pathway, focused on supporting each person with
diabetes to self manage by delivering care and support centred and co-
ordinated around their needs.
This integrated pathway ensures that all parts of the system work together to
deliver all the components of the care pathway with clear protocols for who
does what and what services are provided and where.
Desired
Outcome and
Benefits
Improved patient experience and competence to self manage
Improved clinical outcomes
Improved governance
Increased capacity for delivery of care close to home
Increased capacity to provide specialist diabetic care
Reduction in referrals to outpatient specialist services
Reduction in unplanned admissions
Measurement Patient satisfaction surveys
Figure 8.4 - Integrated pathway for diabetic care
Key Changes
Patient participation and support groups (NCNs)
Learning and Activation capacity/
access to programmes
Planned, robust interface with diabetes specialists and primary care to ensure equitable access to high quality generalist care
Initiation of injectable therapy
Integrated specialist nursing team directing delivery of care within
community settings, in reach to hospital diabetic services
Focus specialist care “Super Six” Improved and equitable access to diabetic care for patients admitted to hospital
28
Numbers of newly diagnosed patients accessing education and training
Compliance with annual review measures
Numbers of diabetic population with poorly controlled diabetes
Reduction in procedures resulting from diabetes (amputations,
ophthalmology)
Referrals to specialist services
Admissions
Milestones Q1 2015/16 – establish integrated Diabetic Specialist Nursing service
Q2 2015/16 – eliminate specialist follow-up outpatient backlog
Q4 2015/16 –patient participation groups established in all NCNs
Q4 2015/16 – consultant mentoring and advice in primary care settings
established
Q4 2015/16 – Insulin initiation and supervision enhanced primary care
services
Workforce Integrated DSN team 6 wte
Finance 2015/16 - £260,000 (integrated DSN team)
2015/16 - £ ……. (insulin initiation and supervision)
Service Change Plan 8 – Mental Health and Learning Disability around 100,000 people in Gwent experience mental health symptoms at any one time. Of our 240,000 children and young people, around 1 in 10 will have a mental health or behavioural
disorder, and many of these go on to experience mental health problems in adulthood. Our older adult population is set to increase by 27% by 2030 with a
predicted 39% increase in the numbers of older people with dementia. A predicted 2.3% increase in the prevalence of people with a learning disability by
2020 will impact on the capacity of our service to meet the increasingly complex physical and learning needs of this population. This may place additional pressure on
demand for Continuing Healthcare Services. In order to meet future demand in a sustainable way mental health needs to become everybody’s business, care should be delivered close to home, and efforts to reduce health inequalities that impact on
emotional health and wellbeing. Our service change plan identifies the following service transformation priorities.
Primary Care Mental Health Support Services improving access to assessment and
therapeutic interventions in primacy care and community settings. 13 work streams testing a range of new and innovative approaches including the use of “Super-Groups” (large scale therapeutic group interventions to develop community capacity to
enhance community resilience), computerised Cognitive Behaviour Therapy. Table 8.4 Vision To improve the emotional and psychological well-being and mental health of
the population via the provision of enhanced Primary Care MH support
Desired
Outcome and
Benefits
Improved clinical outcomes and patient experience via timely access to
mental health assessments and evidence based interventions within primary
care.
Achievement of PCMHSS Tier 1 targets.
Further integration within Primary Care supporting the development of
extended Primary Care teams.
Measurement Monitoring of performance trajectory for Tier 1 targets for PCMHSS
assessment and intervention. (Predicted to meet July ‘15). Service user,
carer and GP satisfaction undertaken by CHC. Aggregation of patient clinical
outcome measures.
Milestones Nov 2014 – Nov 2015: 12 month SCF programme implemented
29
Re-designing the Third Sector Service Model in order to ensure equity of access for
patients and maximise the contribution of the third sector to the care pathway. Table 8.5 Vision All service users will have access to the same range of recovery focused
services regardless of where they live in Gwent
Desired
Outcome and
Benefits
Equitable access to a range of third sector support across Gwent.
Measurement Resource distribution across Gwent is in line with need.
Outcome framework is in place and monitored for all third sector providers.
Milestones Feb - April: Consultation on proposed service model
April - May: Final service model agreed
Feb - March: Further consideration of mechanism for commissioning final
service model
April: Commissioning plan and timescales agreed
Older Adult Mental Health Liaison (RAID), early identification of patients, joint working and up skilling non-mental health professionals to care of patients in acute hospital
settings. Table 8.6 Vision To improve outcomes and the experience of older people with mental
health difficulties within secondary physical healthcare settings
Desired
Outcome and
Benefits
Improve clinical outcomes and patient experience.
Improve patient flow and reduction in bed usage at RGH, STW and one
other site
Reduction in demand on social care via increased number of individual
returning to original residence
Improved integrated working and skill within physical and mental health
workforce
Measurement Length of stay
Numbers of admissions
Patient/Carer experience
Staff experience
Milestones Jan: Interim Pilot Evaluation Report
March - April: Final Pilot Evaluation Report
February - March: Pursue funding options to continue service for a further
12 months
Plans are also being progressed to develop a Low Secure Unit to bring care closer to home and reduce reliance on independent sector providers.
Collectively these service change plans will create
capacity to deliver more care to patients’ in their
homes, or through their local NCN team.
30
9. Improving Access, Flow and Reducing Waits Timely and appropriate access supports good clinical outcomes. Deterioration of health is reduced, unnecessary duplication of investigations is avoided and the burden
to patients, families, communities and other support services is minimised as much as possible.
Over the past 10 to 15 years access to planned and emergency services has becoming increasingly difficult due to a number of factors, including disease complexity, system
expansion, ageing population, public expectation and workforce changes. We recognise the need to address each of those components in order to achieve optimal
health outcomes for our patients. We need to make immediate improvements against locally and nationally agreed
standards including the maintenance of the 95% 4 hour transit time ED target, elimination of 12 hour waits and achieving Referral to Treatment Time targets. To
achieve this we need to reduce demand, improve patient flow across the system, reduce delayed discharges and increase direct and timely admissions for those who
require inpatient care. SCP 9 and SCP 10 set out the significant actions that need to be progressed in the
short to medium term for Urgent & Emergency Care and Planned Care respectively. These service change plans do not stand alone; they are integrally linked to areas for
improvement in: Primary care assess
Reduction in variation (including clear pathways and thresholds for accessing secondary care)
Diabetes, Respiratory and Stroke Pathways Creating capacity in our neighbourhood care network teams to provide high quality,
person centred, anticipatory, effective and efficient care to provide more care in the
community Improving health and preventing early onset of illness and injury
Collectively these programmes are designed to “cool” the system down, smooth demand, reduce inefficiencies and support the system to deliver optimal care for our
patients.
Service Change Plan 9 – Urgent and Emergency Care there are significant pressures on urgent and emergency care services across the Health Board that require an improved whole system approach which maximises the contribution of
every service with the aim of caring for patients in the right place, at the right time and by the right care team.
This past winter has highlighted continuing capacity pressures on our current system resulting from a higher proportion of “majors” presenting at our Emergency
Departments, stubbornly high ambulance conveyance rates (30% of patients arrive by ambulance) that results in ambulance clustering which further exacerbates our efforts
to improve patient flow and an increasing ration of patients with complex care needs admitted to hospital.
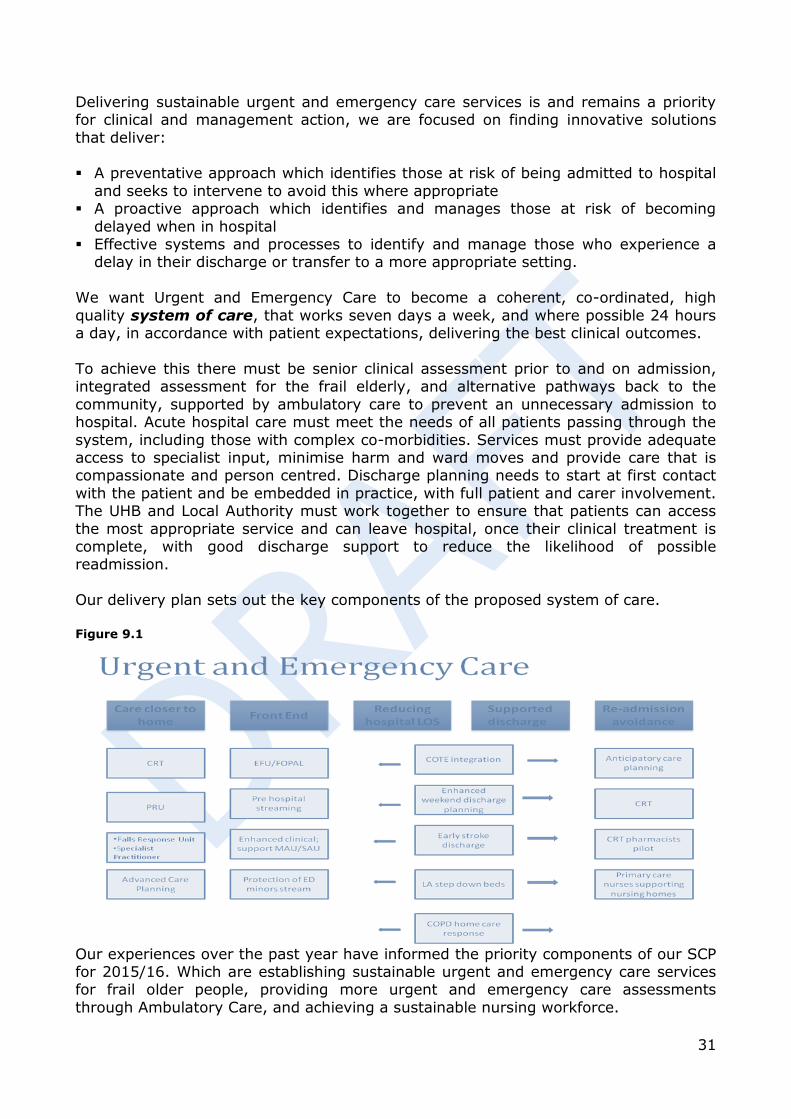
31
Delivering sustainable urgent and emergency care services is and remains a priority for clinical and management action, we are focused on finding innovative solutions
that deliver: A preventative approach which identifies those at risk of being admitted to hospital
and seeks to intervene to avoid this where appropriate A proactive approach which identifies and manages those at risk of becoming
delayed when in hospital Effective systems and processes to identify and manage those who experience a
delay in their discharge or transfer to a more appropriate setting.
We want Urgent and Emergency Care to become a coherent, co-ordinated, high
quality system of care, that works seven days a week, and where possible 24 hours a day, in accordance with patient expectations, delivering the best clinical outcomes.
To achieve this there must be senior clinical assessment prior to and on admission, integrated assessment for the frail elderly, and alternative pathways back to the
community, supported by ambulatory care to prevent an unnecessary admission to hospital. Acute hospital care must meet the needs of all patients passing through the
system, including those with complex co-morbidities. Services must provide adequate access to specialist input, minimise harm and ward moves and provide care that is compassionate and person centred. Discharge planning needs to start at first contact
with the patient and be embedded in practice, with full patient and carer involvement. The UHB and Local Authority must work together to ensure that patients can access
the most appropriate service and can leave hospital, once their clinical treatment is complete, with good discharge support to reduce the likelihood of possible readmission.
Our delivery plan sets out the key components of the proposed system of care.
Figure 9.1
Our experiences over the past year have informed the priority components of our SCP for 2015/16. Which are establishing sustainable urgent and emergency care services for frail older people, providing more urgent and emergency care assessments
through Ambulatory Care, and achieving a sustainable nursing workforce.
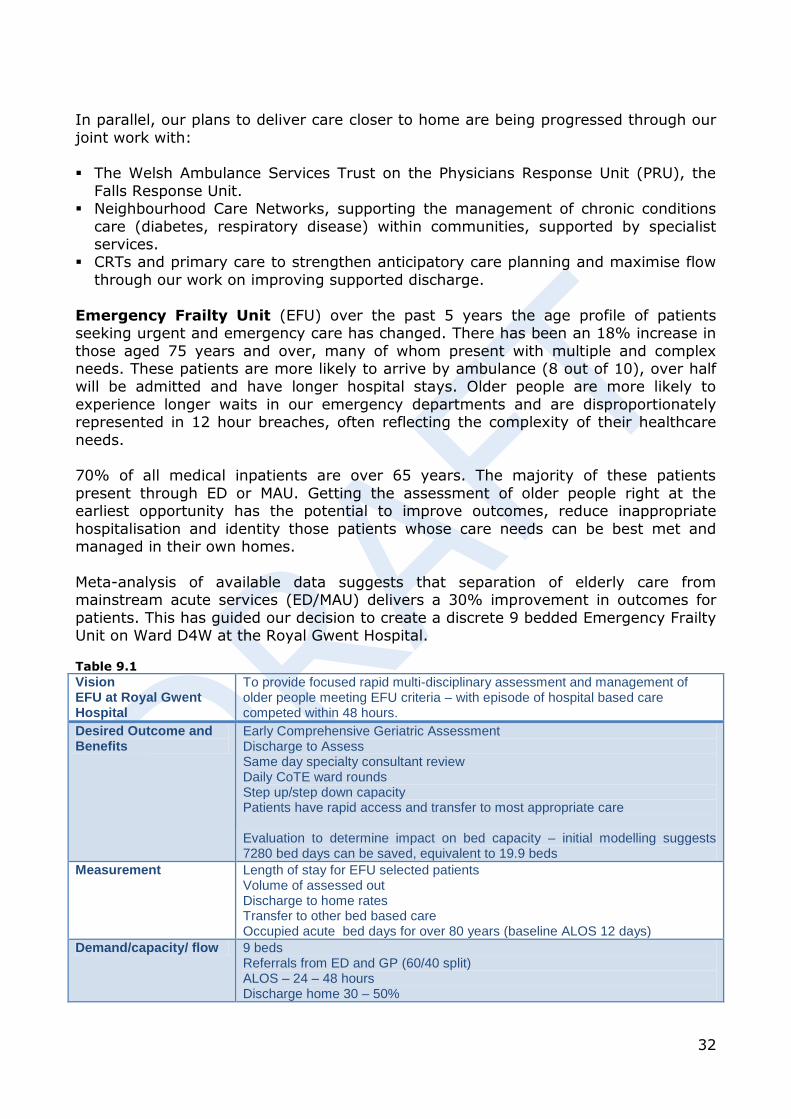
32
In parallel, our plans to deliver care closer to home are being progressed through our
joint work with: The Welsh Ambulance Services Trust on the Physicians Response Unit (PRU), the
Falls Response Unit. Neighbourhood Care Networks, supporting the management of chronic conditions
care (diabetes, respiratory disease) within communities, supported by specialist services.
CRTs and primary care to strengthen anticipatory care planning and maximise flow
through our work on improving supported discharge.
Emergency Frailty Unit (EFU) over the past 5 years the age profile of patients seeking urgent and emergency care has changed. There has been an 18% increase in
those aged 75 years and over, many of whom present with multiple and complex needs. These patients are more likely to arrive by ambulance (8 out of 10), over half will be admitted and have longer hospital stays. Older people are more likely to
experience longer waits in our emergency departments and are disproportionately represented in 12 hour breaches, often reflecting the complexity of their healthcare
needs. 70% of all medical inpatients are over 65 years. The majority of these patients
present through ED or MAU. Getting the assessment of older people right at the earliest opportunity has the potential to improve outcomes, reduce inappropriate
hospitalisation and identity those patients whose care needs can be best met and managed in their own homes.
Meta-analysis of available data suggests that separation of elderly care from mainstream acute services (ED/MAU) delivers a 30% improvement in outcomes for
patients. This has guided our decision to create a discrete 9 bedded Emergency Frailty Unit on Ward D4W at the Royal Gwent Hospital.
Table 9.1 Vision EFU at Royal Gwent Hospital
To provide focused rapid multi-disciplinary assessment and management of older people meeting EFU criteria – with episode of hospital based care competed within 48 hours.
Desired Outcome and Benefits
Early Comprehensive Geriatric Assessment Discharge to Assess Same day specialty consultant review Daily CoTE ward rounds Step up/step down capacity Patients have rapid access and transfer to most appropriate care Evaluation to determine impact on bed capacity – initial modelling suggests 7280 bed days can be saved, equivalent to 19.9 beds
Measurement Length of stay for EFU selected patients Volume of assessed out Discharge to home rates Transfer to other bed based care Occupied acute bed days for over 80 years (baseline ALOS 12 days)
Demand/capacity/ flow 9 beds Referrals from ED and GP (60/40 split) ALOS – 24 – 48 hours Discharge home 30 – 50%
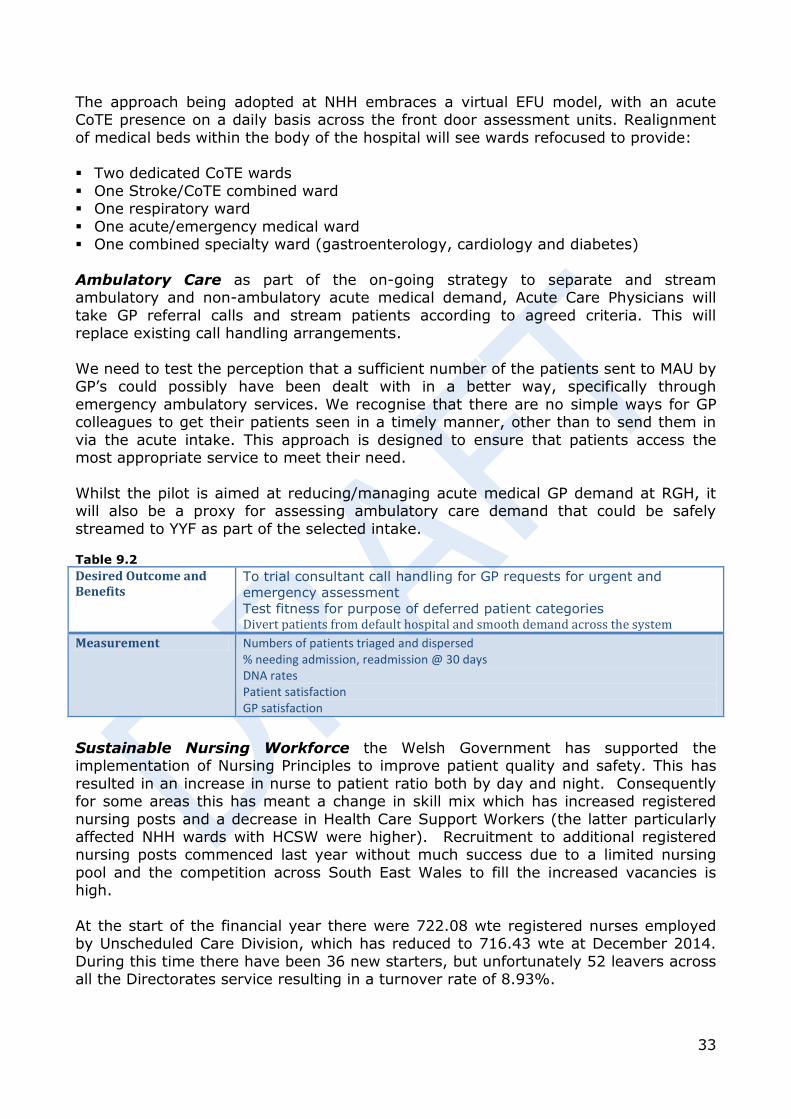
33
The approach being adopted at NHH embraces a virtual EFU model, with an acute CoTE presence on a daily basis across the front door assessment units. Realignment
of medical beds within the body of the hospital will see wards refocused to provide: Two dedicated CoTE wards
One Stroke/CoTE combined ward One respiratory ward
One acute/emergency medical ward One combined specialty ward (gastroenterology, cardiology and diabetes)
Ambulatory Care as part of the on-going strategy to separate and stream ambulatory and non-ambulatory acute medical demand, Acute Care Physicians will
take GP referral calls and stream patients according to agreed criteria. This will replace existing call handling arrangements.
We need to test the perception that a sufficient number of the patients sent to MAU by GP’s could possibly have been dealt with in a better way, specifically through
emergency ambulatory services. We recognise that there are no simple ways for GP colleagues to get their patients seen in a timely manner, other than to send them in
via the acute intake. This approach is designed to ensure that patients access the most appropriate service to meet their need.
Whilst the pilot is aimed at reducing/managing acute medical GP demand at RGH, it will also be a proxy for assessing ambulatory care demand that could be safely
streamed to YYF as part of the selected intake. Table 9.2 Desired Outcome and Benefits
To trial consultant call handling for GP requests for urgent and
emergency assessment
Test fitness for purpose of deferred patient categories Divert patients from default hospital and smooth demand across the system
Measurement Numbers of patients triaged and dispersed % needing admission, readmission @ 30 days DNA rates Patient satisfaction GP satisfaction
Sustainable Nursing Workforce the Welsh Government has supported the implementation of Nursing Principles to improve patient quality and safety. This has
resulted in an increase in nurse to patient ratio both by day and night. Consequently for some areas this has meant a change in skill mix which has increased registered
nursing posts and a decrease in Health Care Support Workers (the latter particularly affected NHH wards with HCSW were higher). Recruitment to additional registered nursing posts commenced last year without much success due to a limited nursing
pool and the competition across South East Wales to fill the increased vacancies is high.
At the start of the financial year there were 722.08 wte registered nurses employed by Unscheduled Care Division, which has reduced to 716.43 wte at December 2014.
During this time there have been 36 new starters, but unfortunately 52 leavers across all the Directorates service resulting in a turnover rate of 8.93%.
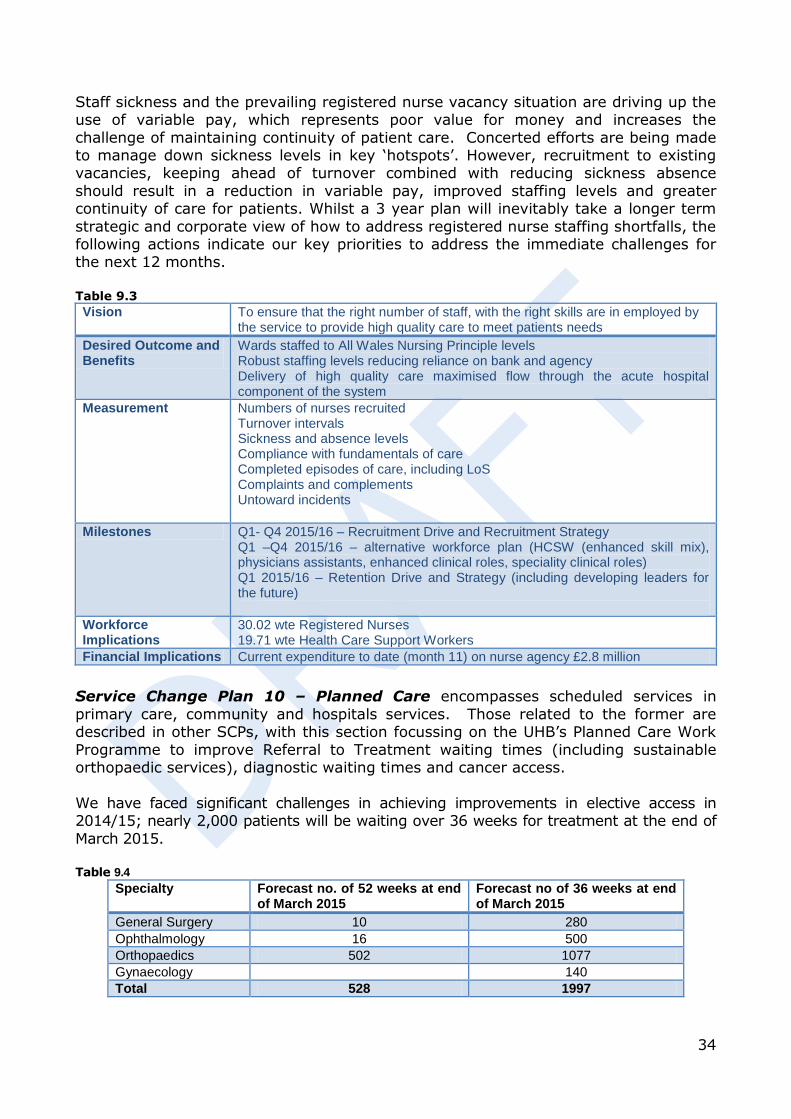
34
Staff sickness and the prevailing registered nurse vacancy situation are driving up the use of variable pay, which represents poor value for money and increases the
challenge of maintaining continuity of patient care. Concerted efforts are being made to manage down sickness levels in key ‘hotspots’. However, recruitment to existing vacancies, keeping ahead of turnover combined with reducing sickness absence
should result in a reduction in variable pay, improved staffing levels and greater continuity of care for patients. Whilst a 3 year plan will inevitably take a longer term
strategic and corporate view of how to address registered nurse staffing shortfalls, the following actions indicate our key priorities to address the immediate challenges for the next 12 months.
Table 9.3 Vision To ensure that the right number of staff, with the right skills are in employed by
the service to provide high quality care to meet patients needs
Desired Outcome and Benefits
Wards staffed to All Wales Nursing Principle levels Robust staffing levels reducing reliance on bank and agency Delivery of high quality care maximised flow through the acute hospital component of the system
Measurement Numbers of nurses recruited Turnover intervals Sickness and absence levels Compliance with fundamentals of care Completed episodes of care, including LoS Complaints and complements Untoward incidents
Milestones Q1- Q4 2015/16 – Recruitment Drive and Recruitment Strategy Q1 –Q4 2015/16 – alternative workforce plan (HCSW (enhanced skill mix), physicians assistants, enhanced clinical roles, speciality clinical roles) Q1 2015/16 – Retention Drive and Strategy (including developing leaders for the future)
Workforce Implications
30.02 wte Registered Nurses 19.71 wte Health Care Support Workers
Financial Implications Current expenditure to date (month 11) on nurse agency £2.8 million
Service Change Plan 10 – Planned Care encompasses scheduled services in
primary care, community and hospitals services. Those related to the former are described in other SCPs, with this section focussing on the UHB’s Planned Care Work
Programme to improve Referral to Treatment waiting times (including sustainable orthopaedic services), diagnostic waiting times and cancer access.
We have faced significant challenges in achieving improvements in elective access in 2014/15; nearly 2,000 patients will be waiting over 36 weeks for treatment at the end of
March 2015. Table 9.4
Specialty Forecast no. of 52 weeks at end of March 2015
Forecast no of 36 weeks at end of March 2015
General Surgery 10 280
Ophthalmology 16 500
Orthopaedics 502 1077
Gynaecology 140
Total 528 1997

35
Our aim is to deliver Best in Class performance for planned care, to improve timely access to elective services, and delivering RTT targets. Our system wide Planned Care
Programme (see Figure x) essentially adopts a two prong approach, focusing on reducing demand across our population and optimising capacity.
Demand and capacity assessment for key specialities has been undertaken, with details
included in the supporting technical plan. The recurrent demand/capacity gap sets out the scale of the sustainability challenge where demand for service outstrips capacity to deliver care locally. This results in outpatient and treatment backlogs with the consequent delays
for patients on some surgical pathways. Figure 9.2
Planned Care Programme
DemandPrudent Healthcare
Capacity
Orthopaedic sustainability plan
Co-productionOutpatient
Transformation
Lifestyle
Patient education
Theatre modernisation
Expand primary care services
Best in Class & benchmarking
7 day services Separation of elective and emergency
streamsAlternative
interventions
Post Op Care Assessment
Unit
Clinicalthresholds
INNU
Pathwaydevelopment
Referral rateanalysis
Our analysis of demand and capacity gaps has identified the need for specific actions
in two specialities: Orthopaedics and Ophthalmology and these delivery plans are summarised below: Table 9.5 Vision
Orthopaedic
Services
To provide a sustainable orthopaedic service by:
Managing demand through prudent healthcare
Optimising capacity
Rebalancing activity between secondary and primary care
Eliminating backlogs and providing sustainable services
Demand/capa
city/ flow
Treatment demand is calculated to be 10.797, which includes both the 52
week and 36 week backlogs.
Treatment capacity is assessed at 10,319, which includes a contribution
from prudent healthcare and the UHB will use external capacity to provide
greater resilience in its delivery plan. The local plans include a range of
initiatives including backfilling, weekend working, consultant expansion
and high productivity lists.
The protection of elective orthopaedic access, which has been
compromised in recent years, is an essential.
Desired
Outcome and
Benefits
52 week clearance by end of November 2015, with 478 breaches of 36
weeks at end of March 2016.
Elimination of 36 week waits in 2016/17.
Workforce
and financial
impacts
The workforce and financial impacts of the orthopaedic delivery plan are
included in the respective sections of the plan.
Supporting
information
Detailed delivery plans and supporting profiles are included in the supporting
technical plan and annexes.
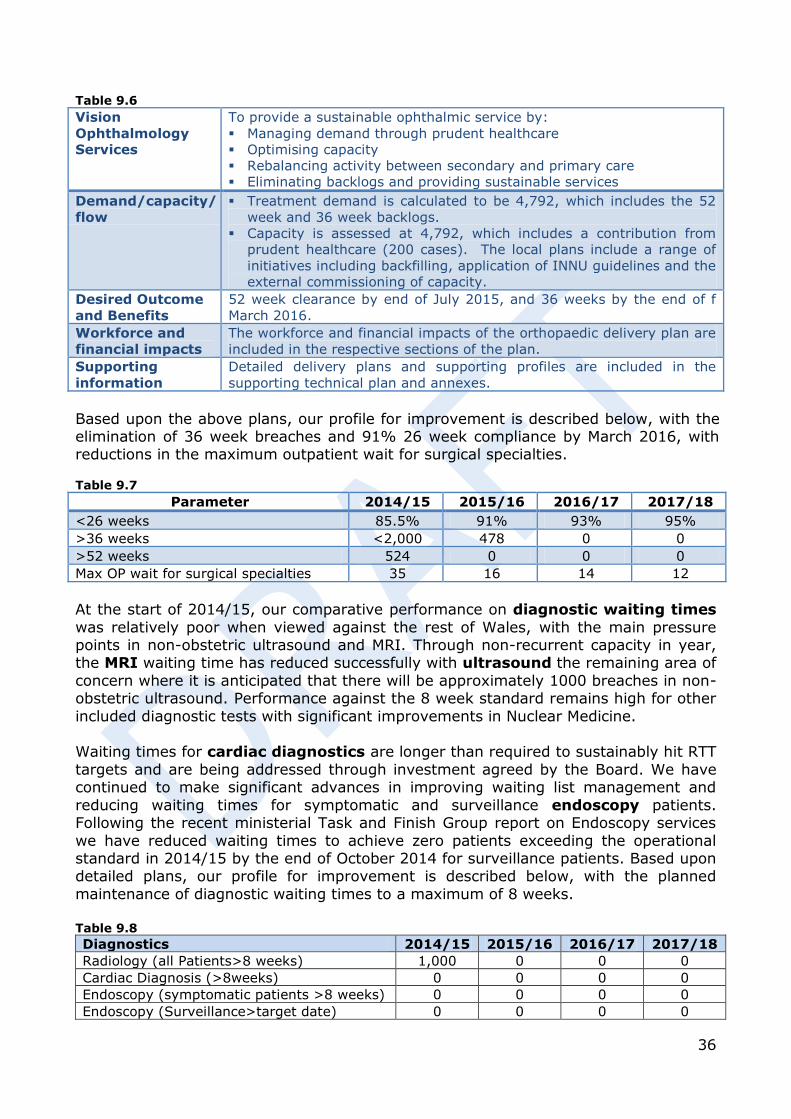
36
Table 9.6 Vision
Ophthalmology
Services
To provide a sustainable ophthalmic service by:
Managing demand through prudent healthcare
Optimising capacity
Rebalancing activity between secondary and primary care
Eliminating backlogs and providing sustainable services
Demand/capacity/
flow
Treatment demand is calculated to be 4,792, which includes the 52
week and 36 week backlogs.
Capacity is assessed at 4,792, which includes a contribution from
prudent healthcare (200 cases). The local plans include a range of
initiatives including backfilling, application of INNU guidelines and the
external commissioning of capacity.
Desired Outcome
and Benefits
52 week clearance by end of July 2015, and 36 weeks by the end of f
March 2016.
Workforce and
financial impacts
The workforce and financial impacts of the orthopaedic delivery plan are
included in the respective sections of the plan.
Supporting
information
Detailed delivery plans and supporting profiles are included in the
supporting technical plan and annexes.
Based upon the above plans, our profile for improvement is described below, with the elimination of 36 week breaches and 91% 26 week compliance by March 2016, with reductions in the maximum outpatient wait for surgical specialties. Table 9.7
Parameter 2014/15 2015/16 2016/17 2017/18
<26 weeks 85.5% 91% 93% 95%
>36 weeks <2,000 478 0 0
>52 weeks 524 0 0 0
Max OP wait for surgical specialties 35 16 14 12
At the start of 2014/15, our comparative performance on diagnostic waiting times
was relatively poor when viewed against the rest of Wales, with the main pressure points in non-obstetric ultrasound and MRI. Through non-recurrent capacity in year, the MRI waiting time has reduced successfully with ultrasound the remaining area of
concern where it is anticipated that there will be approximately 1000 breaches in non-obstetric ultrasound. Performance against the 8 week standard remains high for other
included diagnostic tests with significant improvements in Nuclear Medicine. Waiting times for cardiac diagnostics are longer than required to sustainably hit RTT
targets and are being addressed through investment agreed by the Board. We have continued to make significant advances in improving waiting list management and
reducing waiting times for symptomatic and surveillance endoscopy patients. Following the recent ministerial Task and Finish Group report on Endoscopy services
we have reduced waiting times to achieve zero patients exceeding the operational standard in 2014/15 by the end of October 2014 for surveillance patients. Based upon detailed plans, our profile for improvement is described below, with the planned
maintenance of diagnostic waiting times to a maximum of 8 weeks. Table 9.8 Diagnostics 2014/15 2015/16 2016/17 2017/18
Radiology (all Patients>8 weeks) 1,000 0 0 0
Cardiac Diagnosis (>8weeks) 0 0 0 0
Endoscopy (symptomatic patients >8 weeks) 0 0 0 0
Endoscopy (Surveillance>target date) 0 0 0 0
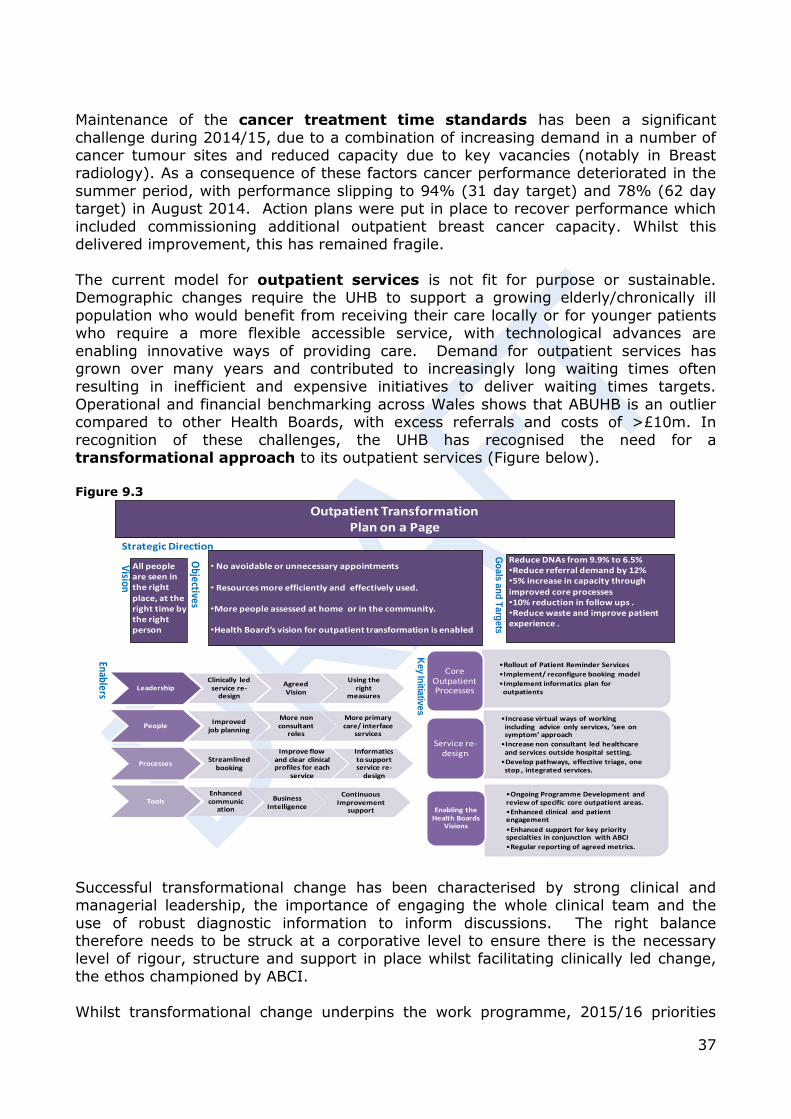
37
Maintenance of the cancer treatment time standards has been a significant
challenge during 2014/15, due to a combination of increasing demand in a number of cancer tumour sites and reduced capacity due to key vacancies (notably in Breast radiology). As a consequence of these factors cancer performance deteriorated in the
summer period, with performance slipping to 94% (31 day target) and 78% (62 day target) in August 2014. Action plans were put in place to recover performance which
included commissioning additional outpatient breast cancer capacity. Whilst this delivered improvement, this has remained fragile.
The current model for outpatient services is not fit for purpose or sustainable. Demographic changes require the UHB to support a growing elderly/chronically ill
population who would benefit from receiving their care locally or for younger patients who require a more flexible accessible service, with technological advances are
enabling innovative ways of providing care. Demand for outpatient services has grown over many years and contributed to increasingly long waiting times often resulting in inefficient and expensive initiatives to deliver waiting times targets.
Operational and financial benchmarking across Wales shows that ABUHB is an outlier compared to other Health Boards, with excess referrals and costs of >£10m. In
recognition of these challenges, the UHB has recognised the need for a transformational approach to its outpatient services (Figure below). Figure 9.3
Successful transformational change has been characterised by strong clinical and managerial leadership, the importance of engaging the whole clinical team and the
use of robust diagnostic information to inform discussions. The right balance therefore needs to be struck at a corporative level to ensure there is the necessary level of rigour, structure and support in place whilst facilitating clinically led change,
the ethos championed by ABCI.
Whilst transformational change underpins the work programme, 2015/16 priorities
Outpatient TransformationPlan on a Page
Strategic Direction
Vision
All people are seen in the right place, at the right time by the right person
Objectives
• No avoidable or unnecessary appointments
• Resources more efficiently and effectively used.
•More people assessed at home or in the community.
•Health Board’s vision for outpatient transformation is enabled
Go
als
an
d T
arg
ets
Reduce DNAs from 9.9% to 6.5%•Reduce referral demand by 12%•5% increase in capacity through improved core processes•10% reduction in follow ups .•Reduce waste and improve patient experience .
Enablers LeadershipClinically led
service re-design
Agreed Vision
Using the right
measures
PeopleImproved
job planning
More non consultant
roles
More primary care/ interface
services
ProcessesStreamlined
booking
Improve flow and clear clinical profiles for each
service
Informatics to support service re-
design
ToolsEnhanced communic
ation
Business Intelligence
Continuous Improvement
support
Ke
y In
itiativ
es
•Rollout of Patient Reminder Services
•Implement/ reconfigure booking model
•Implement informatics plan for outpatients
Core Outpatient Processes
•Increase virtual ways of working including advice only services, ’see on symptom’ approach
•Increase non consultant led healthcare and services outside hospital setting.
•Develop pathways, effective triage, one stop , integrated services.
Service re-design
•Ongoing Programme Development and review of specific core outpatient areas.
•Enhanced clinical and patient engagement
•Enhanced support for key priority specialties in conjunction with ABCI
•Regular reporting of agreed metrics.
Enabling the Health Boards
Visions
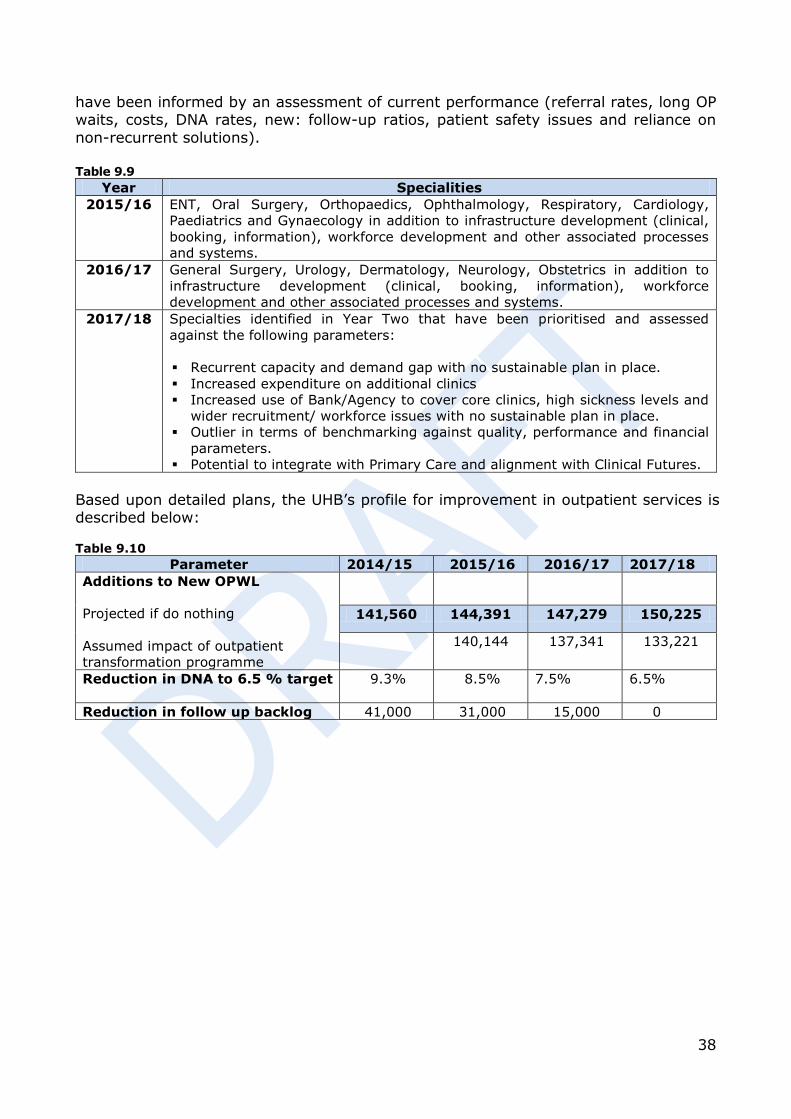
38
have been informed by an assessment of current performance (referral rates, long OP waits, costs, DNA rates, new: follow-up ratios, patient safety issues and reliance on
non-recurrent solutions). Table 9.9
Year Specialities
2015/16
ENT, Oral Surgery, Orthopaedics, Ophthalmology, Respiratory, Cardiology,
Paediatrics and Gynaecology in addition to infrastructure development (clinical,
booking, information), workforce development and other associated processes
and systems.
2016/17 General Surgery, Urology, Dermatology, Neurology, Obstetrics in addition to
infrastructure development (clinical, booking, information), workforce
development and other associated processes and systems.
2017/18 Specialties identified in Year Two that have been prioritised and assessed
against the following parameters:
Recurrent capacity and demand gap with no sustainable plan in place.
Increased expenditure on additional clinics
Increased use of Bank/Agency to cover core clinics, high sickness levels and
wider recruitment/ workforce issues with no sustainable plan in place.
Outlier in terms of benchmarking against quality, performance and financial
parameters.
Potential to integrate with Primary Care and alignment with Clinical Futures.
Based upon detailed plans, the UHB’s profile for improvement in outpatient services is described below: Table 9.10
Parameter 2014/15 2015/16 2016/17 2017/18
Additions to New OPWL
Projected if do nothing
Assumed impact of outpatient
transformation programme
141,560 144,391 147,279 150,225
140,144 137,341 133,221
Reduction in DNA to 6.5 % target
9.3% 8.5% 7.5% 6.5%
Reduction in follow up backlog 41,000 31,000 15,000 0
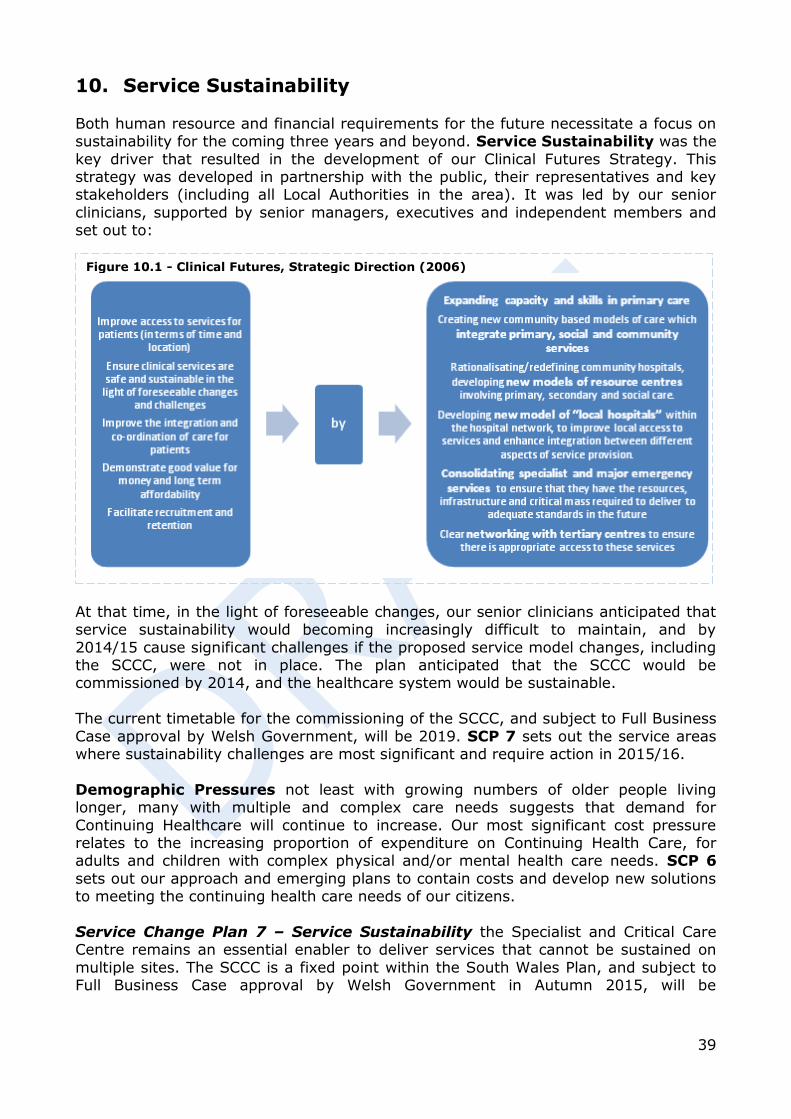
39
10. Service Sustainability
Both human resource and financial requirements for the future necessitate a focus on sustainability for the coming three years and beyond. Service Sustainability was the
key driver that resulted in the development of our Clinical Futures Strategy. This strategy was developed in partnership with the public, their representatives and key stakeholders (including all Local Authorities in the area). It was led by our senior
clinicians, supported by senior managers, executives and independent members and set out to:
At that time, in the light of foreseeable changes, our senior clinicians anticipated that service sustainability would becoming increasingly difficult to maintain, and by
2014/15 cause significant challenges if the proposed service model changes, including the SCCC, were not in place. The plan anticipated that the SCCC would be commissioned by 2014, and the healthcare system would be sustainable.
The current timetable for the commissioning of the SCCC, and subject to Full Business
Case approval by Welsh Government, will be 2019. SCP 7 sets out the service areas where sustainability challenges are most significant and require action in 2015/16.
Demographic Pressures not least with growing numbers of older people living longer, many with multiple and complex care needs suggests that demand for
Continuing Healthcare will continue to increase. Our most significant cost pressure relates to the increasing proportion of expenditure on Continuing Health Care, for adults and children with complex physical and/or mental health care needs. SCP 6
sets out our approach and emerging plans to contain costs and develop new solutions to meeting the continuing health care needs of our citizens.
Service Change Plan 7 – Service Sustainability the Specialist and Critical Care Centre remains an essential enabler to deliver services that cannot be sustained on
multiple sites. The SCCC is a fixed point within the South Wales Plan, and subject to Full Business Case approval by Welsh Government in Autumn 2015, will be
Figure 10.1 - Clinical Futures, Strategic Direction (2006)
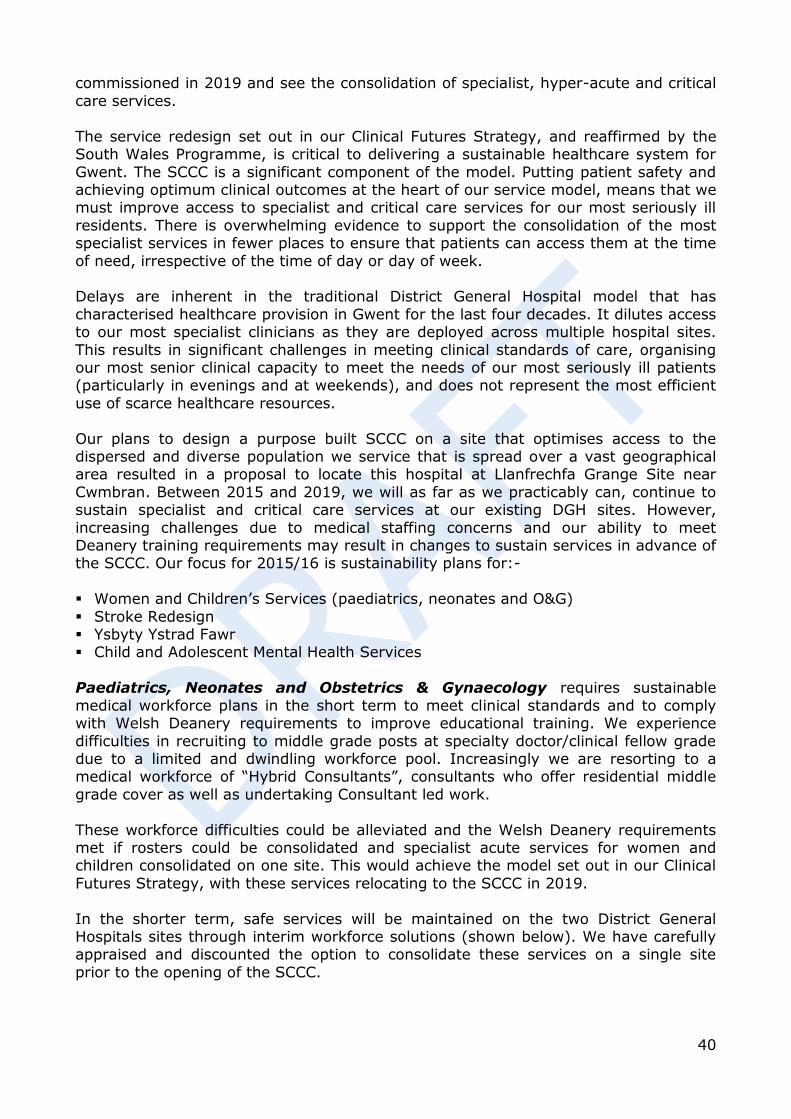
40
commissioned in 2019 and see the consolidation of specialist, hyper-acute and critical
care services.
The service redesign set out in our Clinical Futures Strategy, and reaffirmed by the South Wales Programme, is critical to delivering a sustainable healthcare system for
Gwent. The SCCC is a significant component of the model. Putting patient safety and achieving optimum clinical outcomes at the heart of our service model, means that we must improve access to specialist and critical care services for our most seriously ill
residents. There is overwhelming evidence to support the consolidation of the most specialist services in fewer places to ensure that patients can access them at the time
of need, irrespective of the time of day or day of week. Delays are inherent in the traditional District General Hospital model that has
characterised healthcare provision in Gwent for the last four decades. It dilutes access to our most specialist clinicians as they are deployed across multiple hospital sites.
This results in significant challenges in meeting clinical standards of care, organising our most senior clinical capacity to meet the needs of our most seriously ill patients (particularly in evenings and at weekends), and does not represent the most efficient
use of scarce healthcare resources.
Our plans to design a purpose built SCCC on a site that optimises access to the dispersed and diverse population we service that is spread over a vast geographical area resulted in a proposal to locate this hospital at Llanfrechfa Grange Site near
Cwmbran. Between 2015 and 2019, we will as far as we practicably can, continue to sustain specialist and critical care services at our existing DGH sites. However,
increasing challenges due to medical staffing concerns and our ability to meet Deanery training requirements may result in changes to sustain services in advance of the SCCC. Our focus for 2015/16 is sustainability plans for:-
Women and Children’s Services (paediatrics, neonates and O&G)
Stroke Redesign Ysbyty Ystrad Fawr Child and Adolescent Mental Health Services
Paediatrics, Neonates and Obstetrics & Gynaecology requires sustainable
medical workforce plans in the short term to meet clinical standards and to comply with Welsh Deanery requirements to improve educational training. We experience
difficulties in recruiting to middle grade posts at specialty doctor/clinical fellow grade due to a limited and dwindling workforce pool. Increasingly we are resorting to a medical workforce of “Hybrid Consultants”, consultants who offer residential middle
grade cover as well as undertaking Consultant led work.
These workforce difficulties could be alleviated and the Welsh Deanery requirements met if rosters could be consolidated and specialist acute services for women and children consolidated on one site. This would achieve the model set out in our Clinical
Futures Strategy, with these services relocating to the SCCC in 2019.
In the shorter term, safe services will be maintained on the two District General Hospitals sites through interim workforce solutions (shown below). We have carefully appraised and discounted the option to consolidate these services on a single site
prior to the opening of the SCCC.
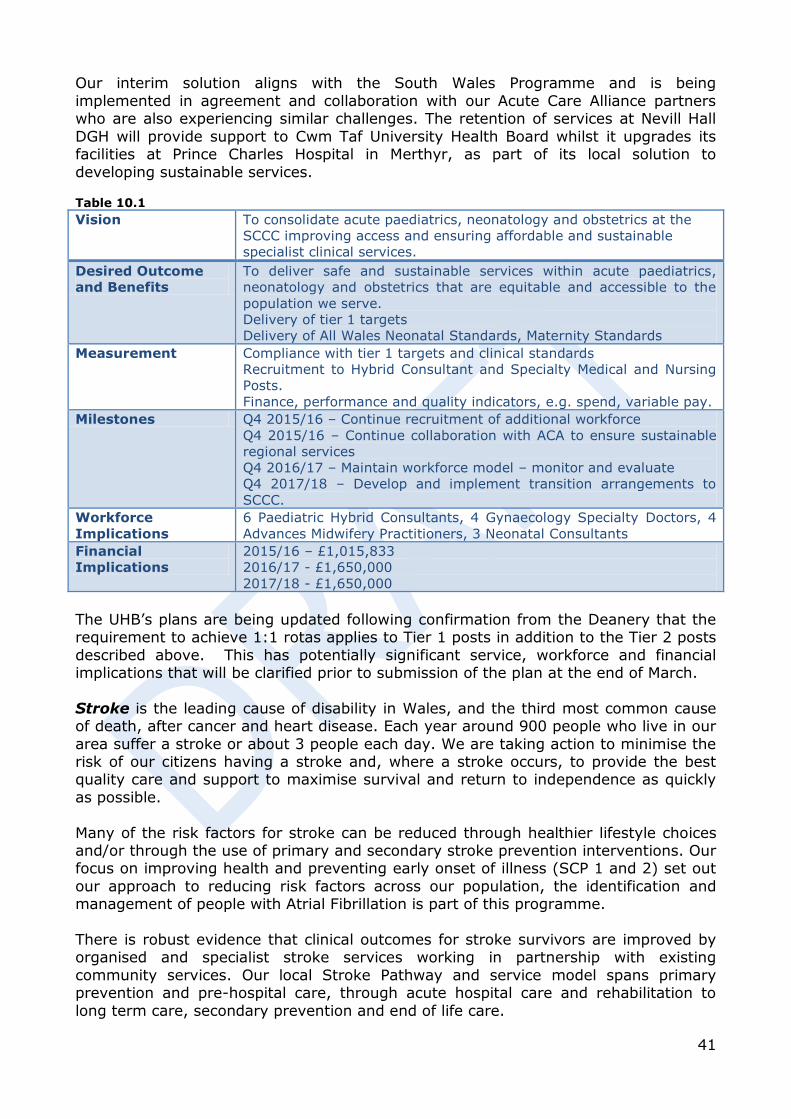
41
Our interim solution aligns with the South Wales Programme and is being
implemented in agreement and collaboration with our Acute Care Alliance partners who are also experiencing similar challenges. The retention of services at Nevill Hall
DGH will provide support to Cwm Taf University Health Board whilst it upgrades its facilities at Prince Charles Hospital in Merthyr, as part of its local solution to
developing sustainable services. Table 10.1 Vision To consolidate acute paediatrics, neonatology and obstetrics at the
SCCC improving access and ensuring affordable and sustainable
specialist clinical services.
Desired Outcome
and Benefits
To deliver safe and sustainable services within acute paediatrics,
neonatology and obstetrics that are equitable and accessible to the
population we serve.
Delivery of tier 1 targets
Delivery of All Wales Neonatal Standards, Maternity Standards
Measurement Compliance with tier 1 targets and clinical standards
Recruitment to Hybrid Consultant and Specialty Medical and Nursing
Posts.
Finance, performance and quality indicators, e.g. spend, variable pay.
Milestones Q4 2015/16 – Continue recruitment of additional workforce
Q4 2015/16 – Continue collaboration with ACA to ensure sustainable
regional services
Q4 2016/17 – Maintain workforce model – monitor and evaluate
Q4 2017/18 – Develop and implement transition arrangements to
SCCC.
Workforce
Implications
6 Paediatric Hybrid Consultants, 4 Gynaecology Specialty Doctors, 4
Advances Midwifery Practitioners, 3 Neonatal Consultants
Financial
Implications
2015/16 – £1,015,833
2016/17 - £1,650,000
2017/18 - £1,650,000
The UHB’s plans are being updated following confirmation from the Deanery that the requirement to achieve 1:1 rotas applies to Tier 1 posts in addition to the Tier 2 posts
described above. This has potentially significant service, workforce and financial implications that will be clarified prior to submission of the plan at the end of March.
Stroke is the leading cause of disability in Wales, and the third most common cause of death, after cancer and heart disease. Each year around 900 people who live in our
area suffer a stroke or about 3 people each day. We are taking action to minimise the risk of our citizens having a stroke and, where a stroke occurs, to provide the best quality care and support to maximise survival and return to independence as quickly
as possible.
Many of the risk factors for stroke can be reduced through healthier lifestyle choices and/or through the use of primary and secondary stroke prevention interventions. Our focus on improving health and preventing early onset of illness (SCP 1 and 2) set out
our approach to reducing risk factors across our population, the identification and management of people with Atrial Fibrillation is part of this programme.
There is robust evidence that clinical outcomes for stroke survivors are improved by organised and specialist stroke services working in partnership with existing
community services. Our local Stroke Pathway and service model spans primary prevention and pre-hospital care, through acute hospital care and rehabilitation to
long term care, secondary prevention and end of life care.
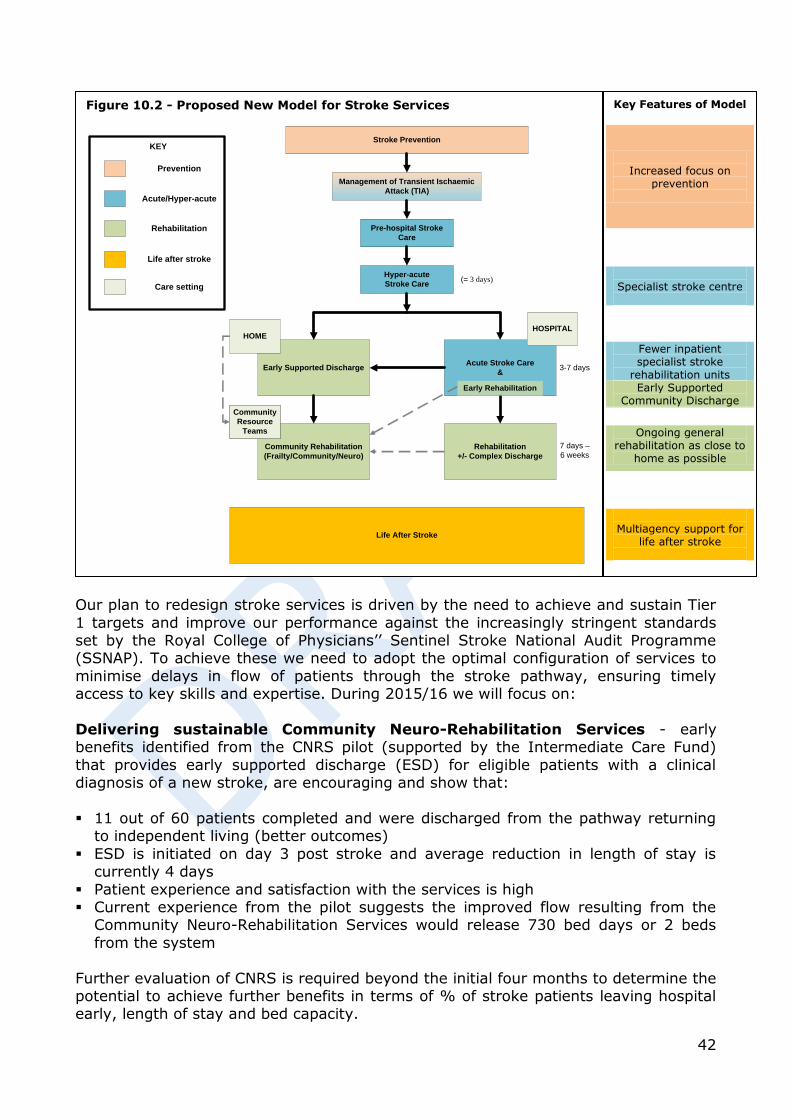
42
Our plan to redesign stroke services is driven by the need to achieve and sustain Tier
1 targets and improve our performance against the increasingly stringent standards set by the Royal College of Physicians’’ Sentinel Stroke National Audit Programme (SSNAP). To achieve these we need to adopt the optimal configuration of services to
minimise delays in flow of patients through the stroke pathway, ensuring timely access to key skills and expertise. During 2015/16 we will focus on:
Delivering sustainable Community Neuro-Rehabilitation Services - early benefits identified from the CNRS pilot (supported by the Intermediate Care Fund)
that provides early supported discharge (ESD) for eligible patients with a clinical diagnosis of a new stroke, are encouraging and show that:
11 out of 60 patients completed and were discharged from the pathway returning
to independent living (better outcomes)
ESD is initiated on day 3 post stroke and average reduction in length of stay is currently 4 days
Patient experience and satisfaction with the services is high Current experience from the pilot suggests the improved flow resulting from the
Community Neuro-Rehabilitation Services would release 730 bed days or 2 beds
from the system
Further evaluation of CNRS is required beyond the initial four months to determine the potential to achieve further benefits in terms of % of stroke patients leaving hospital early, length of stay and bed capacity.
Figure 10.2 - Proposed New Model for Stroke Services
Hyper-acute
Stroke Care
Early Supported DischargeAcute Stroke Care
&
Community Rehabilitation
(Frailty/Community/Neuro)
Rehabilitation
+/- Complex Discharge
Life After Stroke
Community
Resource
Teams
Management of Transient Ischaemic
Attack (TIA)
Pre-hospital Stroke
Care
(= 3 days)
3-7 days
7 days –
6 weeks
Stroke Prevention
Community
Resource
Teams
HOMEHOSPITAL
Early Rehabilitation
Prevention
Acute/Hyper-acute
Rehabilitation
Life after stroke
KEY
Care setting
Key Features of Model
Increased focus on
prevention
Specialist stroke centre
Fewer inpatient specialist stroke
rehabilitation units Early Supported
Community Discharge
Ongoing general rehabilitation as close to
home as possible
Multiagency support for
life after stroke
43
Hyper-acute Stroke Unit (HASU) – strong clinical evidence suggests that stroke patients have better outcomes when they are admitted to a specialist stroke unit and
then returned home as quickly as possible.
In August 2014, we ring fenced beds in RGH for acute strokes. This enabled the service to deliver and sustain delivery of Tier 1 stroke targets. The redesigned stroke service will need to deliver against more stringent targets that Welsh Government will
introduce this year including shorter times to thrombolysis treatment and admission of all stroke patients to a stroke ward within 4 hours.
Establishing a single Hyper Acute Stroke Unit for Gwent will improve timely access to stroke specialists. It will rely on efficient flow of patients to and from HASU as any
patient in our catchment area with a suspected stroke will be directed to this unit.
Extensive modelling using demand/capacity techniques with mathematical scenarios are being undertaken to ensure that the clinical and physical infrastructure required to support the stroke pathway is understood and in place.
This will include consideration of the optimal configuration of inpatient based stroke
rehabilitation. Table 10.2 Milestones Q4 2014/15 – continued stakeholder engagement
Q4 2014/15 – Demand management analysis and initial evaluation of
CNRS pilot
Q1 2015/16 – formal consultation on new model of stroke care
Q1 2015/16 – Blueprint for implementation
Q2 2015/16 – Implement centralised HASU; reconfigure acute stroke and
rehabilitation services
Q 3 2015/16 – Sustainable CNRS workforce model
Financial
Implications
tbc
Sustainable Clinical Model Ysbyty Ystrad Fawr
Ysbyty Ystrad Fawr (YYF) opened in November 2011; it is the first of a new generation of enhanced Local Hospitals originally conceived in our Clinical Futures Strategy. It
plays a pivotal role in providing hospital based healthcare (excluding high dependency services) to the local population as part of the local health and social care system.
The site has 269 beds, 146 of which accommodate medical patients with a further 10 assessment trolleys in the Medical Assessment Unit. The hospital also provides
excellent diagnostic services. In 2014 the Wales Postgraduate Deanery issued a directive in respect of Core Medical
Training (CMT) Doctors, out of hours on call training has to be provided in a busier District General Hospital and seven day Consultant present at YYF is required to retain
trainees on site between 9am and 9pm. This has presented two distinct and significant challenges, namely:
Removal of 9 junior doctors (up to registrar level trainees) from on-call rota.
44
Insufficient consultant resource to sustain on-call rota, provide 7 day presence and
develop/deliver new service models for ambulatory care and emergency frailty services.
In order to maintain the safety of patients and deliver sustainable enhanced services
at YYF, we are redesigning the overnight service model and investing in additional consultant cover.
The Hospital at Night (H@N) approach is being adopted with two Advanced Nurse Practitioners and one Registrar level doctor on site overnight. The ANP and Registrar
are the first responders to any cardiac arrest or acute incident (core skills for these roles include Advanced Life Support). This revised model will limit the role that YYF can play in our hospital network; specifically admissions will not be possible between
8pm and 8am. In addition the threshold for transferring a deteriorating patient to a DGH will be lowered, because the Registrar will not be available to accompany any
patient transfer. Additional Consultant Capacity is also required to provide seven day consultant
presence and develop ambulatory care and emergency frailty services as set out in table x. Table 10.3
Current Capacity Shortfall
Sustain the on-call rota 6 consultants covering 1:8 rota 2 sessions
8am – 8pm on site consultant presence
13 consultant sessions
8 sessions
Emergency Frailty Unit
Ambulatory Care Service
2 sessions
3 sessions
Table 10.4 Vision
To develop a sustainable clinical model for patients with urgent and
unscheduled care needs, optimising the provision of care closer to
home
Desired Outcome
and Benefits
Deliver safe and sustainable services at YYF
Meet the requirements of the Deanery, ensuring the Health Board
maintains its postgraduate medical training commitments
Comprehensive 7 day Emergency Services for Frail Elderly –
improving flow and reducing the need for and length of hospital
stays
Robust emergency/urgent ambulatory care service
Measurement Compliance with Tier 1 targets
Number of patients assessed by EFU and their disposition (admitted,
CRT, home)
Number of patient transfers (deteriorating patient)
Number and timeliness of repatriation of Caerphilly residents
admitted overnight (RGH) back to YYF
Deanery review of junior doctor training
Milestones Q4 2014/15 – Recruit and embed H@N model
Q1 2015/16 – Recruit consultants
Q2 2015/16 – Maintain workforce and service model – monitor and
evaluate
Workforce
Implications
3 Consultants, 2.6 Advanced Nurse Practitioners, 2 Administration
and Clerical
Financial
Implications
2014/15 - £70,000
2015/16 – £588,000
45
Child and Adolescent Mental Health Services (CAHMS) there are concerns about
the sustainability of CAMHS across the United Kingdom, including Welsh Government and amongst the public. Meeting the psychological, emotional and mental health
needs of our children and young people has been identified by the Minister for Health and Social Care as a priority.
Locally demand for service had doubled over the past two years, and the proportion of referrals designated as urgent increased fourfold. We need to develop a sustainable
and functioning secondary care CAHMS service, that reflects the changing demand and presentation of mental health difficulties and suggest models by which services
can be provided. We need to capitalise on the opportunity offered to children and young people in primary care settings through Local Primary Care Mental Health Support Services, ensuring that early intervention and assessment services are
accessible. Our focus is on developing sustainable NHS Specialist CAHMS services for children and young people who:
misuse substances; are in the youth justice system;
are looked after by Local Authorities; have sensory impairments;
learning disabled children. An increasing number of children will have a formal Care & Treatment Plan (CTP)
through the mental health measure, or statutory social care or education requirements. Involvement of social care staff in the care programme is a key
component of the service. The model of care provided will provide a range of services, delivering a continuity of involvement, from specialist consultation through to intensive, evidence based, and direct therapy.
The structural arrangement of these core specialist CAMHS services will be in the form
of three multidisciplinary community teams equitably covering the ABUHB population, tier 3 services offering intense assessments and appropriate interventions, and a crisis outreach team who will work with emergency presentations and link closely with the
nationally commissioned South Wales inpatient unit, in order to minimise length of admission and improve clinical outcomes.
Within the specialist CAMHS directorate are specific resources for children and
adolescents with learning disability (CALDS), youth offending services (YOTS) specialist nurses, young person’s substance misuse services, virtual Tier 3 forensic service, and continuing care. Table 10.5 Vision
To develop a sustainable and functioning secondary CAMHS
Desired Outcome
and Benefits
Reduction of children admitted to adult MH wards
Equitable CAMHS service in Gwent
Patient receiving care in own homes / community where possible
Measurement Service performance measures will be based on clear expectations of
capacity and activity (based on benchmarking data and resource
allocated) but primarily focus on achievement of patient outcomes
and patient feedback, audit of governance performance (e.g. DNA
rates, risk assessments, complaints, compliments, staff wellbeing,
training and development) and regular multiagency, peer review of
services.
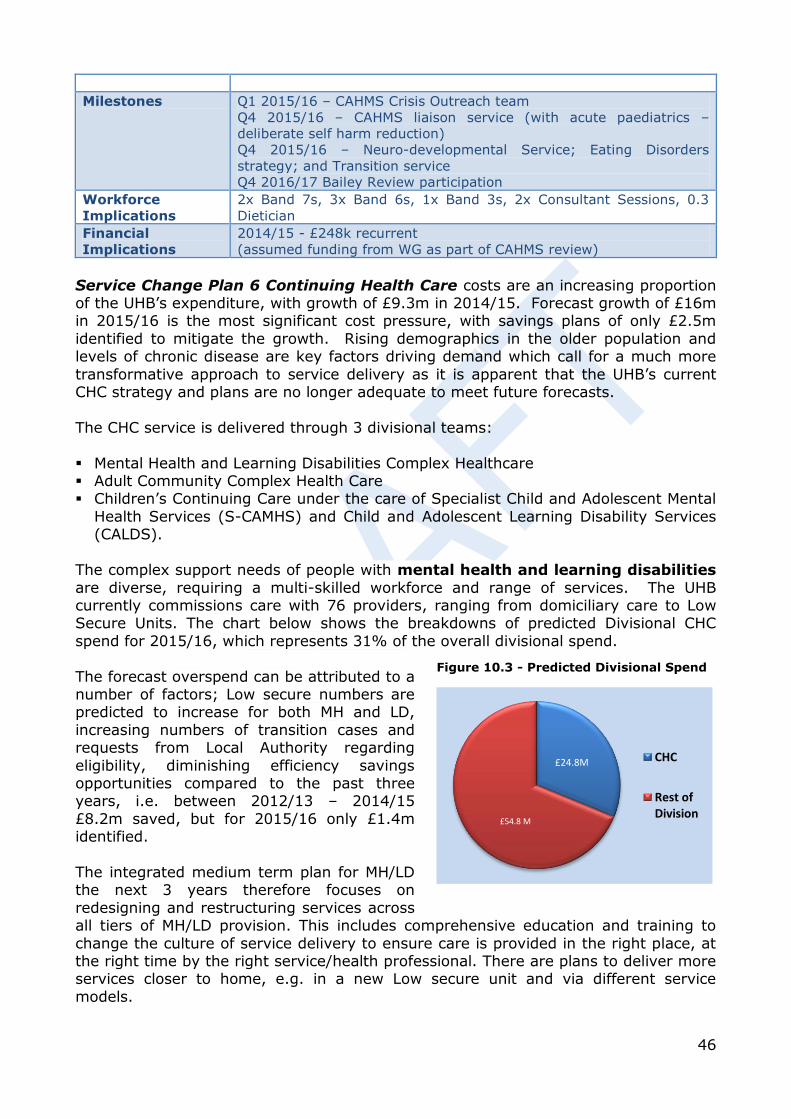
46
Milestones Q1 2015/16 – CAHMS Crisis Outreach team
Q4 2015/16 – CAHMS liaison service (with acute paediatrics –
deliberate self harm reduction)
Q4 2015/16 – Neuro-developmental Service; Eating Disorders
strategy; and Transition service
Q4 2016/17 Bailey Review participation
Workforce
Implications
2x Band 7s, 3x Band 6s, 1x Band 3s, 2x Consultant Sessions, 0.3
Dietician
Financial
Implications
2014/15 - £248k recurrent
(assumed funding from WG as part of CAHMS review)
Service Change Plan 6 Continuing Health Care costs are an increasing proportion of the UHB’s expenditure, with growth of £9.3m in 2014/15. Forecast growth of £16m in 2015/16 is the most significant cost pressure, with savings plans of only £2.5m
identified to mitigate the growth. Rising demographics in the older population and levels of chronic disease are key factors driving demand which call for a much more
transformative approach to service delivery as it is apparent that the UHB’s current CHC strategy and plans are no longer adequate to meet future forecasts.
The CHC service is delivered through 3 divisional teams:
Mental Health and Learning Disabilities Complex Healthcare Adult Community Complex Health Care Children’s Continuing Care under the care of Specialist Child and Adolescent Mental
Health Services (S-CAMHS) and Child and Adolescent Learning Disability Services (CALDS).
The complex support needs of people with mental health and learning disabilities
are diverse, requiring a multi-skilled workforce and range of services. The UHB currently commissions care with 76 providers, ranging from domiciliary care to Low Secure Units. The chart below shows the breakdowns of predicted Divisional CHC
spend for 2015/16, which represents 31% of the overall divisional spend.
The forecast overspend can be attributed to a number of factors; Low secure numbers are predicted to increase for both MH and LD,
increasing numbers of transition cases and requests from Local Authority regarding
eligibility, diminishing efficiency savings opportunities compared to the past three years, i.e. between 2012/13 – 2014/15
£8.2m saved, but for 2015/16 only £1.4m identified.
The integrated medium term plan for MH/LD the next 3 years therefore focuses on
redesigning and restructuring services across all tiers of MH/LD provision. This includes comprehensive education and training to
change the culture of service delivery to ensure care is provided in the right place, at the right time by the right service/health professional. There are plans to deliver more services closer to home, e.g. in a new Low secure unit and via different service
models.
Figure 10.3 - Predicted Divisional Spend
£24.8M
£54.8 M
CHC
Rest of Division

47
Adult Community Complex Healthcare (CHC) service sits within Community
Services Division and operates across 5 Localities in Gwent. Its aims are to ensure people with complex care needs receive safe and high quality nursing care packages
at home or in placements in the care home sector, that support independence and prevent deterioration. It monitors, commissions and supports the provision of funded
nursing care (FNC) and case manages patients with Huntingdon’s Disease and Acquired Brian Injury (ABI). It also provides a Complex Care Occupational Health service and has a key role in safeguarding, escalating concerns, contracting and
governance and the business administration function.
ABUHB’s Complex HC team currently commissions care with nursing homes, specialist (YPD) and domiciliary care providers alongside its own in-house services.
Care packages are provided to people with a wide range of needs that arise from complex conditions such as degenerative disorders, acquired brain injuries, dementia
and palliative care. As eligibility for CHC is based on need and arises from such a wide range of disorders, it is difficult to record or categorise packages of care to facilitate service model redesign or to accurately predict CHC growth. The current growth
forecasts are based on historical data. However the most significant areas of growth contributing to the forecast overspending are EMI, which has grown by over 62%
(£5.1million) over the past two years and adults, which has grown by almost 16% (£3.4million) over the past 2 years.
Children’s Continuing Care (CALDS and CAMHS) sits within the Family and Therapies Division and is responsible for the assessment and placement of young
people eligible for CHC funding. The service commissions and provides for young people requiring placement funded through Continuing Care, or WHSSC commissioned services, young people with complex Learning Disabilities and associated co-
morbidities and it manages transition arrangements of young people with late presentation developing serious mental health issues.
While there have been significant improvements in communication between adult and young people’s services within health, there remains significant room for improving
early notification of potential transition between agencies, particularly in relation to young people placed out of county by education/social services. The lack of alternative
forms of accommodation is currently a limiting factor for early engagement with local health (CAMHS/CALDS) services that could drive alternative strategies for
management of CHC in the future. Current demand for CHC placement for CALDS/CAMHS placements is stable at present with an average of two new cases per annum.
The Children’s Community Continuing Care service is responsible for delivering a
range of complex care packages within the community. This service continues to experience steadily increasing demand with a major challenge in relation to recruitment of qualified nurses.
The development of Young Peoples services requires a multi-agency approach to
developing a range of alternative community based service provision including more therapeutic community placements as an alternative to secure care and also as a step down from secure placement. There are opportunities, including the ending of
Tripartite funding arrangement which should reduce expenditure in 2015/16 and potential changes in local in-patient and secure/ low secure children’s services is likely
48
to reduce demand for out of county placements and more opportunities for community
supported placements.
Desired Future State while this SCP currently focuses on a range of measures to improve current operational efficiency and effectiveness, the longer term plan is to
undertake a system wide review of the patient pathways that lead to high cost and long term packages of care. The projected growth in demand for adult health and social care means that there needs to be a fundamental change in strategy across the
whole system in future.
Our strategy for the next 3-5 years is being developed by a CHC Strategic Planning Task & Finish Group that has been established since February 2015 it addresses:
ABUHB’s financial position compared with other Health Boards across Wales; ABUHB’s growth assumptions and make recommendations on how to forecast more
accurately for the future; Recommendations on UK best practice models and future management of CHC Options for savings/cost avoidance over the next three years;
Options for improving joint working with Local Authorities and other partners including collaborative commissioning proposals;
Workforce and organisational development implications of proposed changes. This strategic approach will enable us to:
Develop a shared vision for future adult health and social care with partner
agencies recognising the need to reduce future demand and resource intensity of current models of care.
Develop alternative models of care across the system that impact on demand and outcomes.
Develop a shared approach to commissioning, through working with partners, to
more effectively manage the market, including strategically shaping independent
sector developments to meet predicted local needs and where appropriate to progress shared/pooled budgets across partner organisations. This recognises the
considerable scope to provide more cost effective care and more capacity for future demand through more innovative Procurement Options, e.g:
□ Work with the care home sector and residential social landlords to develop
alternative service models – e.g. In One Place model and social enterprises.
□ Reviewing existing high cost packages of care to ensure alignment in meeting the patient’s/client’s needs and optimising value for money.
□ Regular review of care packages and agreed changes. □ Align closely with NCNs and Local Authorities to support care closer to home. □ Participation in the Collaborative Commissioning national project (CCAP) and
early adoption of opportunities identified.
Develop greater intelligence to identify opportunities to intervene more proactively at earlier stages of the patient’s pathway through care delivery redesign, in order to change the trajectory of disease progression or loss of function (fig x).
In the short term this SCP will implement solutions that can be put in place to take
advantage of operational efficiencies. The task and finish group charged with
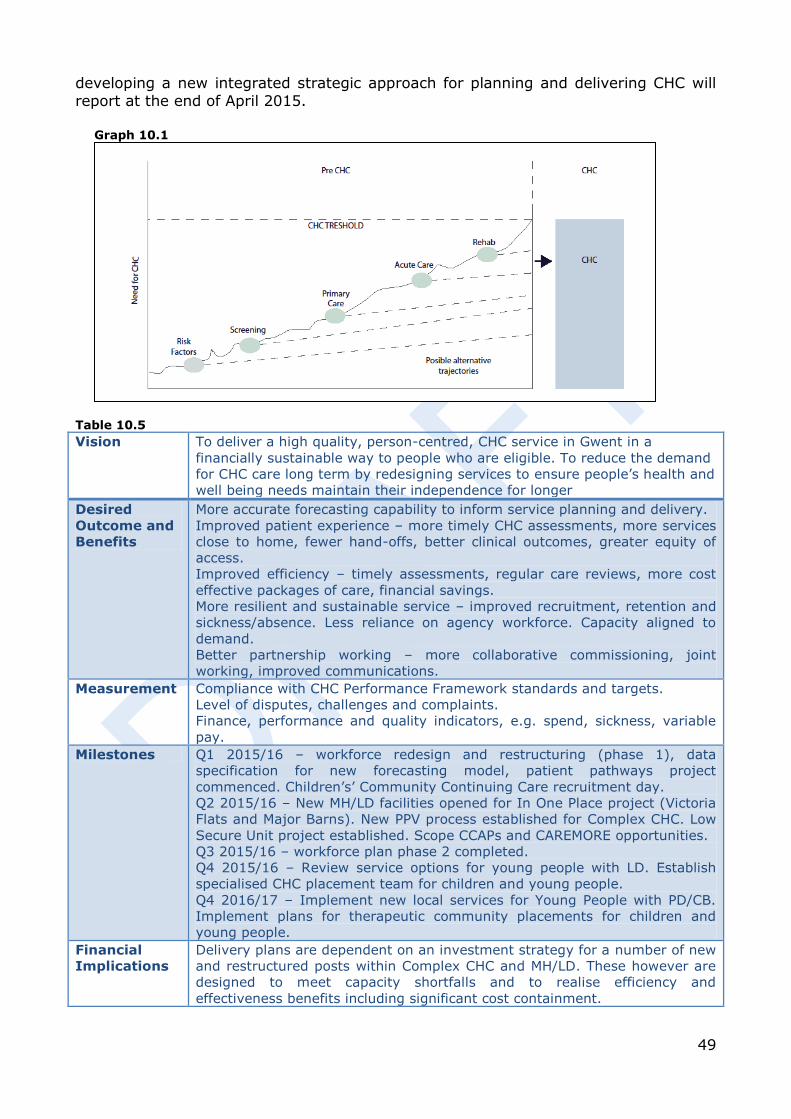
49
developing a new integrated strategic approach for planning and delivering CHC will
report at the end of April 2015. Graph 10.1
Table 10.5 Vision To deliver a high quality, person-centred, CHC service in Gwent in a
financially sustainable way to people who are eligible. To reduce the demand
for CHC care long term by redesigning services to ensure people’s health and
well being needs maintain their independence for longer
Desired
Outcome and
Benefits
More accurate forecasting capability to inform service planning and delivery.
Improved patient experience – more timely CHC assessments, more services
close to home, fewer hand-offs, better clinical outcomes, greater equity of
access.
Improved efficiency – timely assessments, regular care reviews, more cost
effective packages of care, financial savings.
More resilient and sustainable service – improved recruitment, retention and
sickness/absence. Less reliance on agency workforce. Capacity aligned to
demand.
Better partnership working – more collaborative commissioning, joint
working, improved communications.
Measurement Compliance with CHC Performance Framework standards and targets.
Level of disputes, challenges and complaints.
Finance, performance and quality indicators, e.g. spend, sickness, variable
pay.
Milestones Q1 2015/16 – workforce redesign and restructuring (phase 1), data
specification for new forecasting model, patient pathways project
commenced. Children’s’ Community Continuing Care recruitment day.
Q2 2015/16 – New MH/LD facilities opened for In One Place project (Victoria
Flats and Major Barns). New PPV process established for Complex CHC. Low
Secure Unit project established. Scope CCAPs and CAREMORE opportunities.
Q3 2015/16 – workforce plan phase 2 completed.
Q4 2015/16 – Review service options for young people with LD. Establish
specialised CHC placement team for children and young people.
Q4 2016/17 – Implement new local services for Young People with PD/CB.
Implement plans for therapeutic community placements for children and
young people.
Financial
Implications
Delivery plans are dependent on an investment strategy for a number of new
and restructured posts within Complex CHC and MH/LD. These however are
designed to meet capacity shortfalls and to realise efficiency and
effectiveness benefits including significant cost containment.

50
11. Workforce & Organisational Development Challenges The performance of local services is directly related to the workforce who provides
care and services to local people. We are facing major workforce challenges in many areas including:
Recruitment of medical staff, General Practitioners and in some specialist service
including radiology and psychiatry. Changes to junior doctor training impacting on service sustainability. Managing the “survival curve” to achieve optimum staffing levels in nursing to
comply with the Nursing Principle Standards and developing enhanced roles within nursing and Allied Health Professionals to improve recruitment (above average
turnover rates) and retention Escalating variable pay costs due to nursing shortages - these costs are in the
region of £1.1m per month and developing effective plans to reduce and contain
costs. Shortages in the workforce and other factors are impacting on the health of the
workforce with sickness absence rates higher than normal at an average of 5.51% (591 WTE’s).
National shortages creating recruitment challenges in key areas e.g. sonographers.
Future service changes potentially changing career paths for staff Using staffing as efficiently and effectively as possible when services are under
pressure and when change is required to improve services. Staffing 7 day services within current resources and recruitment challenges.
Delivery We must employ an effective Organisational Development approach which prepares
and supports the organisation to achieving successful change. Our OD strategy will be finalised by July 2015 and will provide approaches to deliver:
Nurse Recruitment Strategy, compliant with Nursing principles by Quarter 1 Year 1 Developing short term interventions to enable the UHB to survive the recruitment
curve to bridge nursing vacancies. Improving compliance of staff receiving Performance and Development reviews
from 60% to 85% during 2015/16.
Sickness Absence Reduction with the potential of ½% year on year to push towards the Welsh Government (WG) target and maximising performance and reliance on
variable pay through: maximising attendance at work and Health at Work initiatives; management of sickness absence in line with the organisational plan
submitted to WG; effective full roll out of E-Rostering by year 3;
roll out of electronic bank system by Quarter 2 year 1. Slick Recruitment tactics by refocusing the Bank Office to become a Resourcing
Function structured to deliver an effective recruitment pipeline (Quarter 2 year 1). Effective up to date Job Plans for all medical staff which are aligned to
organisational and service objectives to reduce Waiting List Initiatives (WLI) by
25% by Quarter 4 Year 1. Efficient and effective deployment of staff utilising the principles of Prudent
Healthcare. This will include implementing skill mix changes such as development of the graduated care model for patients going through the Healthcare system, the
51
development of roles to support this include the introduction of Rehabilitation
Health Care Support Worker (Quarter 1 Year 1) to support effective basic level therapeutic and care interventions throughout the week in rehabilitation settings,
the development of Band 4 Support Worker roles in a community setting by Quarter 4 Year 1. Additionally, the development and deployment of Physician Assistants to
support shortage areas and avoid medical locum costs within Year 2. Continue to monitor workforce performance - working with managers to maximise
business intelligence to support the effective management of staff.
Delivering systems to underpin the development of good leadership, management and accountability at all levels in the UHB.
Become a socially responsible organisation e.g. through use of alternative employment schemes, apprenticeships, and the achievement of the corporate platinum standard.
Develop systems to identify and grow talent within the organisation and across the NHS and public sector in Wales to ensure effective succession planning system is in
place by Quarter 3 Year 1. Building on the Workforce Benchmarking highlighted by PWC and Iview information
on comparative workforce costs, to identify and address areas of potential savings.
Working with the Neighbourhood Care Networks to develop effective workforce models and plans. This will enable the effective shift of staff from a secondary
setting to primary and community setting. Increase workforce planning capacity within the organisation.
The UHB will ensure that there is a sufficient supply of graduates undertaken through the yearly educational commissioning process. To meet the needs of the nursing
workforce within the UHB and local labour markets, the organisation will increase its graduate nursing training numbers to reflect both the ageing demographics of this staff group and also the requirement for new and extended roles. Likewise, figures will
need to increase for other staff groups such as radiographers and therapies to meet changing service models, 7 day services and extension of roles.
Workforce Impact and Outcomes To date a number of workforce changes and efficiencies have been identified. Some
of these will not equate to WTE reductions but cost reductions due to changes in the skill, which is similarly applicable to areas where additional payments such as WLIs,
agency costs or reductions in additional sessions for the medical workforce. This cannot be correlated with a reduction in WTE but these workforce savings will be
offset against variable pay usage. Investment opportunities are linked to numerous schemes and the impact of these is
shown in the table below. A significant number of the WTE staff increases are aligned to sustainability plans and plans to meet performance targets (RTT) and include
requirements for additional consultants, advanced practitioners and other support staff groups across a variety of specialities. The development of primary care services will increase the number of pharmacists and specialists nurses to deliver care closer to
home.
The following savings in WTE by staff group have been identified by the Divisions:
Staff Group Investment Opportunities WTE Workforce Savings WTE
Additional Professional 5.1
Management and Administration 7.48
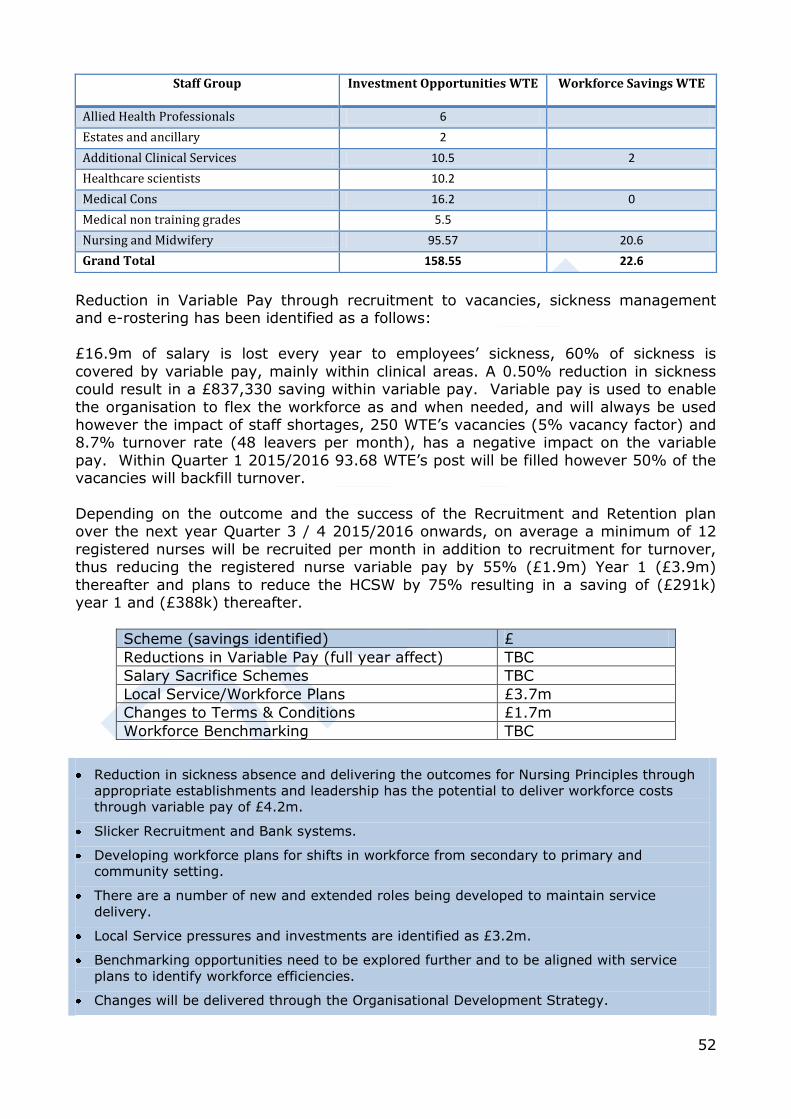
52
Staff Group Investment Opportunities WTE Workforce Savings WTE
Allied Health Professionals 6
Estates and ancillary 2
Additional Clinical Services 10.5 2
Healthcare scientists 10.2
Medical Cons 16.2 0
Medical non training grades 5.5
Nursing and Midwifery 95.57 20.6
Grand Total 158.55 22.6
Reduction in Variable Pay through recruitment to vacancies, sickness management and e-rostering has been identified as a follows:
£16.9m of salary is lost every year to employees’ sickness, 60% of sickness is
covered by variable pay, mainly within clinical areas. A 0.50% reduction in sickness could result in a £837,330 saving within variable pay. Variable pay is used to enable
the organisation to flex the workforce as and when needed, and will always be used however the impact of staff shortages, 250 WTE’s vacancies (5% vacancy factor) and 8.7% turnover rate (48 leavers per month), has a negative impact on the variable
pay. Within Quarter 1 2015/2016 93.68 WTE’s post will be filled however 50% of the vacancies will backfill turnover.
Depending on the outcome and the success of the Recruitment and Retention plan over the next year Quarter 3 / 4 2015/2016 onwards, on average a minimum of 12
registered nurses will be recruited per month in addition to recruitment for turnover, thus reducing the registered nurse variable pay by 55% (£1.9m) Year 1 (£3.9m)
thereafter and plans to reduce the HCSW by 75% resulting in a saving of (£291k) year 1 and (£388k) thereafter.
Scheme (savings identified) £
Reductions in Variable Pay (full year affect) TBC
Salary Sacrifice Schemes TBC
Local Service/Workforce Plans £3.7m
Changes to Terms & Conditions £1.7m
Workforce Benchmarking TBC
Reduction in sickness absence and delivering the outcomes for Nursing Principles through
appropriate establishments and leadership has the potential to deliver workforce costs
through variable pay of £4.2m.
Slicker Recruitment and Bank systems.
Developing workforce plans for shifts in workforce from secondary to primary and
community setting.
There are a number of new and extended roles being developed to maintain service
delivery.
Local Service pressures and investments are identified as £3.2m.
Benchmarking opportunities need to be explored further and to be aligned with service
plans to identify workforce efficiencies.
Changes will be delivered through the Organisational Development Strategy.
53
12. Finance Health services are facing increasing demands, medical advancements, higher
expectation from the public and the impact from financial austerity within the general economy. The Nuffield Trust in 2014 published ‘A Decade of Austerity in Wales’ highlights the financial pressures facing Wales. This report re-emphasized the funding
pressures facing health service whilst demand for service was increasing. This would result in increasing pressures to be met with a reduced budget in real terms requiring
efficiency savings on an annual basis of possibly 3.7% per year. The scope for traditional general efficiency savings still exists but on a reduced scale
compared to previously. This requires greater emphasis on wider system changes through major service change and modernisation and adopting the principles of
Prudent Healthcare across the NHS system. Furthermore, the Health Board faces a greater challenge with a funding and spend per
head baseline that is below the Welsh average based on population and need. A financial strategy of continuing to seek greater efficiencies on its own from existing
service models is unlikely to succeed in the medium term.
An assessment has been undertaken which models the future financial outlook based
on existing service and workforce plans against key funding assumptions for the next three years. Some of the key funding assumptions include:
Funding increases for the next three years based on the Allocation Letter for 15/16
and experience from previous years.
Full funding of National pay pressures and pension changes each year in line with cost impact
Full funding of capital charges across the three years Based on previous trends an additional 2.5% uplift in the recurrent allocation for
16/17 and 17/18
An additional £16m from Welsh forecast in 15/16 based on a fair share of the £80m to support innovation and developments in primary and integrated care on a
recurrent basis. The Health Board has undertaken a robust analysis of other major cost drivers
including Primary and Secondary Care Prescribing, NICE pressures, the impact of Continuing Health Care and Funded Nursing Care, externally commissioned services
including specialised services, external contracts and the Welsh Risk Pool.
The Health Board has also assessed key areas requiring recurrent investment that supports:
the ambitions of the national plan for a primary care service in Wales delivers integration between health and social care through the Intermediate
Care Fund the ambitions of the Health Board to deliver efficiencies through technology the priorities of the National Delivery plan programmes.
The Health Board welcomes the additional £80m funding earmarked for these
priorities and ABUHB is assuming it receives its fair share to facilitate delivery of the strategic change agenda over the next three years.
54
In addition, further costs are anticipated for 2015/16 and beyond to support:
Local sustainability issues specifically medical staffing and junior doctor issues Additional investment to improve delivery of Tier 1 targets
Improving flow across Unscheduled Care Supporting enabling investment to support the service change agenda Reflecting the impact of increasing demand and demographics
Each investment will be considered in terms of its costs and the assessment of
expected benefits and outcomes and aligned to the key organisational objectives and Service Change Plans.
The requirements from the detailed financial modelling going forward suggests that financial sustainability will only be achieved through a combination of delivering
improved operational efficiency, mitigating potential cost growth and robust outcome based service change plans. The IMTP has identified modest cash-releasing saving opportunities to the value of £28m across the three year period. The savings
identified equate to 1.8% of controllable expenditure in 15/16 reducing to 1% in 16/17 and 0.6% in 17/18. Further work will continue to identify improvements in
efficiency and cost mitigation and more significantly the impact of the Service Change Plans.
Operational efficiency improvement will target the following opportunities:
Improving length of stay further and to support existing capacity constraints Reducing outpatient costs through reviewing referral rates and reduced follow ups Procurement and price savings in partnership with shared services
Reducing variable pay across the system through improved recruitment and sickness management
Better rostering through e-rostering Improved productivity through medical job planning External provider efficiency
Further cost mitigation is being pursued in the following areas:
CHC is a key area being reviewed as a result of significant levels of growth being
forecast. This work is being progressed through new project arrangements and the development of a clear action plan
The anticipated growth associated with External Contracts and WHSSC is under
review through the commissioning process and aims to identify the opportunities and choices that could mitigate some of these increasing costs.
Primary care prescribing growth and NICE costs continue to be key issues and is currently only partially being offset through opportunities to mitigate cost with further work being pursued through the Health Board’s Medicines Management
work stream. Further changes to national terms and conditions led by Welsh Government would
also help mitigate increasing annual workforce costs. Further consideration of the cost benefit analysis of local pressures and priorities.
Service Change Plans require further work to identify the opportunities and this will be an iterative process as they are further developed and the impact assessment
completed.
55
The financial plan does have some key risks associated with both planning assumptions and delivery including:
Risk of Key Planning Assumptions
The planned increases in the allocation over the next three years in terms of general growth pay and pensions funding and targeted allocations are fundamental to the delivery of the plan and any reductions in this funding will have a direct
impact on the scale of challenge facing the UHB. The assessment of growth is based on known information at this stage and will be
reviewed and updated continuously throughout the ongoing planning cycle. However any major changes in the modelled cost increases will impact on the financial plan.
Increases in the demand for services across the sectors above those assumed in the plan could jeopardise the service plans and assumed savings.
Increases in WHSSC and the Welsh Risk Pool costs above the current provision. Changes in delivery assumptions of Tier 1 targets during the three years. CHC levels of growth and the potential impact of the national framework above
current assumptions.
Delivery Risks The most significant risk is the development and ambition of Service Change Plans
to deliver the scale of savings required to achieve a balanced plan in 2015/16.
The ability to deliver cost reductions through operational efficiency and not just improved productivity.
Improving flow in unscheduled care system is key to delivering other components of the plan.
Ability to develop and implement recruitment plans to deliver more sustainable
services and improve efficiency. Risk of further costs associated with medical staff rotas and deanery requirements.
Management capacity and capability given the scale of the agenda Ability to deliver the scale of change needed in years 2 and 3 if year 1 is unable to
deliver service and financial balance.
The Health Board needs to respond to the local and national challenges and modernise
how health services are delivered. The IMTP attempts to critically evaluate the service and system changes required including critically evaluating the value of services in
terms of cost and outcome, sustaining the focus on quality and patient safety, pursuing the agreed local strategic plans and ensure that the service change plans are delivered.
A summary of the main points in the financial plan is as follows:
The plan is based upon the UHB provisional year-end out-turn for 2014-15 of breakeven and an underlying deficit of £3.2m going into 2015/16.
The plan assumes 2.5% general growth in funding for the following two years
and full funding of capital charges and the national pay and pension changes across all three years.
Service Demand and other inflation cost growth has been modelled based on local and national evidence and suggests potential increases in cost across the system of between £30m - £40m per annum.
The plan assumes the UHB will receive £16m in 2015/16 to support delivery of
56
its primary care and integration service agenda in addition to innovative technologies and national delivery plans.
Further local service pressures and investments of £13m suggested by divisions
for year one and £10m per annum thereafter to primarily support improvements in access targets, improving flow across the unscheduled care
system and service sustainability. These will require further consideration in the context of the overall plan.
Cash-releasing opportunities of £13m have been identified to date for 2015/16. A level of high value opportunities that exist across the system need to be further targeted and realised to improve operational efficiency. Further work is
also ongoing to mitigate costs in terms of growth and consideration of local priorities which is assumed to deliver a further reduction of £6m in 2015/16.
Despite the above, the service and workforce plans are not affordable within the available funding by £19.7m in 2015/16 and the Service Change Plans need to be escalated to enable the priority schemes to be translated into a sustainable
delivery plan. The scale of progress made in year 1 will have a significant impact on the
outlook for years 2 and 3. The risk assessment of the current plan based on planning and delivery
assumptions identifies a risk range of over £100m across the three year period.
The current IMTPs at divisional level require further work to enable the Board to fully prioritise and allocate resources for the 2015/16 financial year. Therefore,
it is proposed that the Board initially delegates budgets based on those commitments
which have previously been approved plus pay and pensions costs for 2015/16, on the
basis that robust plans – supported by appropriate business cases – are developed quickly for the Board to consider.

57
13. Key Enablers
The delivery of the IMTP is dependent on ensuring that the Health Board has established and takes advantage of the opportunities provided by key enablers. This
is important to build the necessary capacity and capability for delivery and removing key problems which may inhibit progress.
Organisational Development will be a key enabler to support the Health Board in delivering a challenging agenda. The future focus for 2015/16 will be to build and
continue to respond to individual and organisational needs through the PADR process and a range of other interventions including:
Continued opportunities for development for aspiring leaders and managers through the Core Skills for Managers and Supervisors Programme, Enhanced
Leadership and Management Programme and Leading for Quality and Improvement Programme.
Encouragement of staff to participate in national programmes that develop clinical
and leadership talent such as Academi Wales Summer School and Senior Leadership Experience.
The key priorities for delivery are:
Identify key staff groups where talent and succession management will further support the organisation. This will be achieved through a review of provision for
groups such as Administration & Clerical and Directorate Management roles by September 2015.
Articulate the responsibilities and accountabilities of all managers in the effective
line management of their staff. This will continue to form a key part of the PADR process for 2015/16 for managers.
Ensure all managers have demonstrated the relevant skills and knowledge to enable them to discharge their responsibilities and this is monitored via the PADR process.
Ensure the organisational behaviours and values are embedded and underpin all our actions and interactions as an organisation. This is a developmental process
which will be formally reviewed by June 2015. The sustainability of the workforce organisational infrastructure and organisational
cultures and values will be an important focus as the demographic changes in the workforce begin to impact. The organisation will continue to support programmes such
as the Senior Leadership Experience nationally and the local infrastructure to feed these programmes, thus ensuring the work started by leaders and managers within
the UHB today can be carried forward into the Clinical Futures strategy and its ultimate delivery in 2018.
The accountability of managers for people management in the delivery of patient care, financial sustainability and quality improvements will continue to remain a priority.
The Employee Engagement Framework has been developed based on the priorities identified from the 2013 Staff Survey results. However, a whole systems approach to
improve engagement of staff continues to be necessary if the culture required to deliver the strategy of the UHB is to be achieved. This transformational approach
requires small transactional steps encouraging staff to raise and discuss issues at the point at which they are identified. To support this, we have:

58
Engaged with the Investors in People Framework to improve all aspects of employee engagement.
Agreed standards of engagement across the UHB with identified metrics to enable review and monitoring.
Identified methods to assess staff feedback in terms of progress made against the issues identified within the Staff Survey.
Continued to improve communication between individuals and managers through
the implementation of standards for engagement enabling staff to feel empowered to raise concerns, and that managers support the actions necessary to bring about
the improvement required. The success of this action will be monitored by the next Staff Survey in 2016.
Prudent Healthcare principles encourage NHS staff to consider carefully the actions taken in caring for patients, ensuring that there is no harm, carry out the minimum
appropriate intervention and share information with patients about treatment options. There must be a collaborative approach between clinical decision makers, patients, managers and finance teams to ensure that resources are used most effectively to
deliver the highest quality of care and to decrease costs through inadequate management and clinical capacity, waste, harm and variation that do not contribute to
a positive outcome for the patient. This includes treatments which have no, or limited evidence base and tests which may lead to over diagnosis and over treatment with the associated harms.
There needs to be a greater focus to prevent people from becoming ill by providing
them with skills and incentives to take greater responsibility for their own health and wellbeing and that of others. Public Health improvement needs to be at the forefront to raise awareness of the importance of self management. Early diagnosis and
prevention, and efficient and effective care must be provided to ensure waste and duplication is eliminated and primary and community care is strengthened.
The benefits and outcomes anticipated include:
Improved patient outcomes. Reduction in the number of inappropriate cases being referred to secondary care
services. Care provided closer to home in a community setting.
Co-production and self management. Opportunities realised ensuring greater clinical benefit.
Reduction in harm from antibiotic prescribing.
Increased capacity in radiology with a reduction in harm associated with over diagnosis.
Overall increase in capacity for secondary care services thus ensuring compliance with RTT.
Predicated on outcome measures including patient reported outcome measures
which will be monitored and reported to directorates and NCNs. Reduction in medicines cost of >£550k.
The Prudent Healthcare agenda will be used as an opportunity to focus on interventions that are of low or limited clinical value. It will aim to support
transformational change across the health system and ensure co-production to make sure healthcare provided fits the needs and circumstances of the patient whilst
actively avoiding waste and harm. This will be (in some areas) a resourceful approach
59
to prudent healthcare in order to achieve an evidence based shift of resource into
primary and community care.
Key priorities for delivery in 2015/16 include:
Renal Transplants Immunosuppressant Drugs Repatriation – Work with WHSSC, the Cardiff & Vale Renal Centre and Primary Care colleagues to manage the repatriation of patients to the C&V Renal Centre and deliver significant drug costs procurement
savings. Cardiac Surgery – Further develop Cardiac Surgery Commissioning arrangements
with WHSSC including a review of current demand & capacity profiles and performance against benchmarks.
NICU – Review of current capacity and commissioning/contracting arrangements in
conjunction with the Neonatal Network. Immunology - Development of a Contracting Framework and Service Specification
for the Cardiff & Vale service. Implementation of ABUHB CAMHS CITT Team – Work with the Family & Therapies
Division and WHSSC to implement a local CITT team to work alongside and reduce
the reliance on existing CAMHS Tier 4 Inpatient Services. Homecare Drugs – Work with Velindre to identify savings opportunities through
implementing a wider homecare drugs initiative. Blood Products Procurement - Work with WHSSC to identify and implement savings
opportunities arising from the improved procurement of blood products.
ALAS – Work with WHSSC to review the current contracting framework and investment with a view to improving current performance levels and identifying
likely future need/pressures. WHSSC Prioritisation – Identify opportunities for ABUHB including the impact on
core services.
Transfer of Services – Work with WHSSC to develop arrangements for the transfer of the commissioning of non-specialised services back to Health Boards.
Paediatric Endocrinology – Agree regional service model requirements with WHSSC. Enzyme Replacement Therapies – Implement opportunities for drug procurement
savings.
Risk Sharing - Review current risk share principles and the current differential between Health Boards utilisation and contribution towards WHSSC services.
CAMHS Procurement – Identify potential savings opportunities in regard to the future commissioning of CAMHS placements.
WAST – work with other Health Boards and WHSSC as part of the collaborative commissioning arrangements to develop new commissioning arrangements for Emergency Ambulance Services.
? Orthopaedic work ? Vascular services work
? Radiology review Prudent Healthcare will be used as a key enabler to evaluate future plans and changes
in service provision to make sure that patient benefits and value for money is assured.
External Contracting Opportunities 2015/16 Onwards, we contract with other Health organisations for services to local patients which cannot be provided locally. Specific priorities for delivery in 15\16 beyond the ongoing, monthly/annual
commissioning & contracting arrangements:
60
YYF Repatriation – opportunity to pursue higher level of delivery against targets if
deemed a strategic priority for the UHB. Also pursue higher marginal rate of recovery from C&V and Cwm Taf, this depends on the final LTA agreed for 2014/15
plus consideration of wider baseline adjustment opportunities and the optimal benefit.
Outsourcing – key piece of work in 2014/15 to support ABUHB delivery of RTT, local capacity pressures likely to necessitate ongoing arrangements into 2015/16 and potentially 2016/17. Potential for service profile to alter/expand.
South Wales Collaborative – from a commissioning and contracting perspective, ongoing work with NHS Wales colleagues to consider and implement the impact of
new patient flows, for example: ▫ Vascular Surgery – Clinical model review has determined a hub and spoke model
for the region, C&V the likely hub. The patient flow impact and associated detail
to be worked through, additional costs at C&V expected with the potential release of some marginal costs for the Directorate.
▫ SCCC – impact of service centralisation to be worked through from an AB provider LTA perspective, primarily for Powys patients. To date the centralisation of Paeds services at RGH has been considered.
University Status, Medical Education and Research & Development our
philosophy is to foster a strong culture of Research and Innovation which will feed into policy and practice. Embracing this philosophy over the coming years will ensure growth in the research portfolio and develop a culture where research is a core
activity that is offered to patients as part of their routine clinical care. There has already been notable progress and it is hoped to further build upon:
Increased number of portfolio studies and Principal Investigators. Investment in Mental Health research resulted in ABUHB being the highest recruiter
in Wales to the National Centre for Mental Health study last year. 229 patients were recruited and this year the recruitment figures are already higher.
Investment in pathology to ensure patients are able to access clinical trials in Velindre.
Investment in ITU where the research portfolio is growing; last year 635
participants were recruited into the FREE study (Family Reported Experiences Evaluation).
In order to grow the R and D as a key aspect of University Status, a commitment has been made that a minimum of 45 Consultant SPA sessions will be allocated to
research from April 2015, with named individuals to take the work forward. The ABUHB conference attracted over 300 delegates which enabled the
organisation to showcase research excellence and encourage new researchers to
come forward. Significant increase in number of patients recruited to clinical trials.
Mathematical modelling work with Masters and PhD students contributing to the work of ABCi.
ABCi development work in healthcare improvement methodologies and training
throughout the Health Board divisions.
The focus and benefits from innovation will be a key strategic driver going forward. Collaborations and Partnerships planning and delivery of our services, in the
context of established partnerships and multiagency mechanisms, underpins the UHB strategic approach to sustainable service improvement and change. While the current
and projected financial difficulties facing public sector organisations present significant
61
challenges, they also offer opportunities for greater innovation in the pooling of
resources and expertise, enabling continued development of services which address identified need.
The five Single Integrated Plans (SIPs) are based on comprehensive needs
assessments of the Local Authority area, using an outcomes based methodology. They address the needs of the whole population in the area with a specific focus on the disadvantaged, vulnerable or at risk of becoming vulnerable. The structures that
have been developed to support Neighbourhood Care Networks (NCNs) and local partnerships form the delivery element of the Local Service Board (LSB) partnership
structures. Implementation of the Social Services and Well-Being Act and changes heralded by
the Well-Being of Future Generations (Wales) Bill, in supporting wider public service reform, puts greater emphasis on the role of collaborative solutions in anticipating
future service demand and preventing the preventable. Implementation of Public Service Boards and Well-being Plans, replacing the current LSBs and SIPs, will enable the UHB, with its partners, to build on the successes of existing collaborative
approaches in addressing the diversity of citizen needs.
In recognition of the variation in levels of deprivation and health and well being challenges across our catchment population, as identified within the Needs Assessment, the twelve multiagency NCNs are implementing Development Plans
which target health and well being priorities within the communities they serve. The NCNs are pivotal delivery units, enabling the planning and delivery of services to their
50,000 – 60,000 catchment population based on a pathway approach which puts greater emphasis on care delivered closer to home.
Work is underway to reflect the requirements of the Primary Care Plan “Our Plan for a Primary Care Service for Wales up to March 2018”, enabling a more joined up
approach to the identification of need and the development of service solutions, widening the role of our partners including housing and the Independent and Third Sectors.
Underpinning these key partnership structures is work to embed co-production
principles within service planning and delivery, recognising in particular that:
Patients are ‘experts’ in their own circumstances and capable of making decisions (examples of work in this area include the development of the diabetes, COPD and stroke pathways). The responsibility that individuals have, in both improving and
maintaining their own health and well being, are a further important aspect of this approach.
Clinicians need to move away from being purely ‘fixers’ to also being ‘facilitators’ of a patient’s treatment and care based on greater equalisation of the clinician; patient relationship.
In acknowledging the key role of our communities and wider stakeholders in
highlighting and informing necessary service improvement and change, the UHB is implementing a corporately driven approach to engagement which is underpinned by the principles of coproduction and which builds on effective engagement mechanisms
implemented at Local Service Board (LSB) and Neighbourhood Care Network (NCN) levels. The UHB Engagement and Communication framework facilitates continual
engagement with our communities, based on a ‘You said – we did’ approach to
62
engagement and feedback, and an equal partnership and shared responsibility for
health outcomes, between patients and professionals. The aim is to ensure timely input of wider opinion to the improvement and development of our services.
We have also undertaken a stakeholder analysis in recognition of the fact that within
overall stakeholder groups there are “subgroups” that may have more or less interest and direct impact on the role and function of the UHB, in terms of their power and influence. It is anticipated that the UHB will become more mature in its approach to
stakeholder management with further refinement of this analysis to enable better targeting of engagement activities.
In relation to existing engagement mechanisms at a local authority and LSB level, there will be occasions when the UHB needs to engage jointly with partners on issues
that affect wider stakeholder groups, for example public health and well being matters, and occasions when the UHB needs to engage unilaterally, for example in
gathering feedback on services and undertaking coproduction approaches to proposed service change.
This coordinated approach to communication and engagement will also enable more effective mechanisms for the gathering of patient experience and stakeholder
feedback, complaint based intelligence and opinion on proposed service change in informing delivery and developing the Health Board’s future plans.
ICT we continue to work in partnership with NHS Wales Information Service (NWIS) to develop and implement national information solutions and merge and integrate
local systems or their functions with national technologies and frameworks in support of the national strategy. Some of the key roles of Informatics include:
Developing and managing the local infrastructure to allow clinicians and others to access applications and technology service in order to support patient care and
communications. Developing and implementing new systems and enhancing current functionality,
including training and support for users.
Integrating data to support business and clinical analysis at local and Welsh level. Facilitating engagement with clinicians and others to develop more effective designs
and implementation of information systems. Developing the technical aspects of TeleHealth as a facilitator to service
improvement and delivery benefits to patients and the service. Undertaking the above in conjunction with partners in NHS Wales, Social Care,
voluntary and commercial healthcare sectors.
Some of the key priorities for delivery in 2015/16 include:
Continue the roll out of the Digitised Health Board including the introduction of
bookmarking functionality and eforms.
Commence implementation of convergence plans between the Welsh Clinical Portal and CWS.
Complete the implementation of the National Laboratory Information System (LIMS).
Replace the current ORMIS Theatre Information System with the TOMS system.
Transition the current Symphony A&E system to the national EDCIMS system. Replace the Nevill Hall Hospital telephone system.
63
Develop a business case for a Patient Flow Management system and proceed to
procurement subject to approval. Develop a new digital dictation system to include voice recognition.
Develop greater mobility for using technology for clinical staff.
We have more detailed plans for 15/16 and beyond as part of the technical document. This highlights the importance of establishing close links with the national programme but without losing the benefits of local innovation.
Aneurin Bevan Centre for Improvement (ABCi) provides a systematic approach
to innovation, service improvement and leadership. ABCi supports the development of an organisational culture which supports staff to develop creative and innovative solutions to service pressures. This drive for service improvement and delivery is
supported by the development of programmes to promote leadership skills, teamwork and focus on quality.
ABCi has been instrumental in promoting and supporting the implementation of the ‘Improving Quality Together’ programme. This has been used as a positive process to
build capacity, capability and confidence by supporting teams and individuals by developing improvement skills and a spirit of empowerment. A key focus has been
developing local, national and international links to promote learning and research to improve collaborative working and leadership capacity. ABCi specifically has strong links with Cardiff University which has resulted in the appointment of a Mathematician
with expert skills in operational research to support improvement in key services.
ABCi will be a key resource to develop greater capacity and capability for delivery in 15/16 and will also provide resource to support improvement in key elements of Service Change Plans. Some examples include:
Development of a community nursing e-rostering tool.
Reviewing demand capacity for Breast Services. Supporting the National Patient Flow Programme in Unscheduled Care. Studying the complex demand and pathways for Cardiology Services.
Supporting the major work to review Continuing Health Care Services.
ABCi will be utilised to support delivery of key priorities within the Health Board’s Service Change Plans.
Capital Plans more services are being provided in the community and in ways which differ from the traditional models of care focused on acute hospitals. However there is
a continued reliance upon a range of healthcare premises to ensure appropriate care is provided safely as close to the patient as possible. The availability of capital
investment allows the Health Board to ensure compliance to best practice and facilitate change to service provision.
The Health Board has a large estate portfolio exceeding 50 premises (hospitals and clinics) together with a number of commercial leases in place to provide
accommodation for various staff groups and services. This size of estate does not fully portray the scale of the estate when the spread of specific sites and the number of premises contained within a site are also considered. The estate has a large number
of premises, of varying ages, state and utilisation to manage in a way that supports service delivery.

64
The current forecast for Health Board capital funding inclusive of projected SCCC
investment is outlined below:
Table 13.1
The All Wales Capital Programme is funding the Specialist Critical Care Centre (SCCC) over the next 5 years. The only other approved source of capital currently available
to the UHB over the next three years is Discretionary Capital and it has been assumed for planning purposes that funding will continue at the 2014-2015 level, i.e. £7.2M per annum, over this period.
The Outline Business Case for the SCCC was formally approved by the Minister for
Health and Social Services in October 2013. This represents a significant step forward and reinforces the principles identified within the Clinical Futures Strategy and the South Wales Programme.
The IMTP process and corresponding work to identify and address service, estate and
equipment risk has identified a number of priorities for capital investment which cannot be accommodated from the Health Board’s available discretionary capital
funding. These are therefore put forward for potential funding from the Welsh Government Strategic Capital Programme and are outlined in the Technical document.
We are also developing further potential proposals for capital investment to resolve current service pressures, provide more sustainable services, improve quality of
services and make better use of resources. Examples include: Resolving the capacity, flow and environment in the Emergency Department at the
Royal Gwent and St Woolos hospitals. Providing more local and cost effective mental health low secure accommodation.
Cath Lab replacement at the Royal Gwent Hospital to ensure service continuity. Resolving regulatory issue with the reprovision of the Endoscopy Unit at the Royal
Gwent Hospital.
Developing plans to deal with Estate infrastructure risks at Nevill Hall and Royal Gwent hospitals.
Upgrade Pharmacy Aspetic Suites. Implementing the Health Board’s Primary Care Estate Strategy. Invest to Save Accommodation Strategy.
Options to improve car parking.
It is estimated that the organisation’s demand for Capital is estimated to be in excess of £77m over the period 2015-2016 to 2019-2020 with Discretionary Capital funding anticipated to be circa £7.2m per annum. It is also assumed that in most areas there
will be further unforeseen capital requirements resulting in the need for a contingency to cover future requirements.
2015/16 2016/17 2017/18 2018/19 2019/20
£000 £000 £000 £000 £000
All Wales Approved Schemes
SCCC 7,553 106,842 92,610 62,369 19,161
Source
Funding in CRL 7,209 7,209 7,209 7,209 7,209
Property Disposals 50
Total Discretionary 7,209 7,259 7,209 7,209 7,209
Total Funding 14,762 114,101 99,819 69,578 26,370
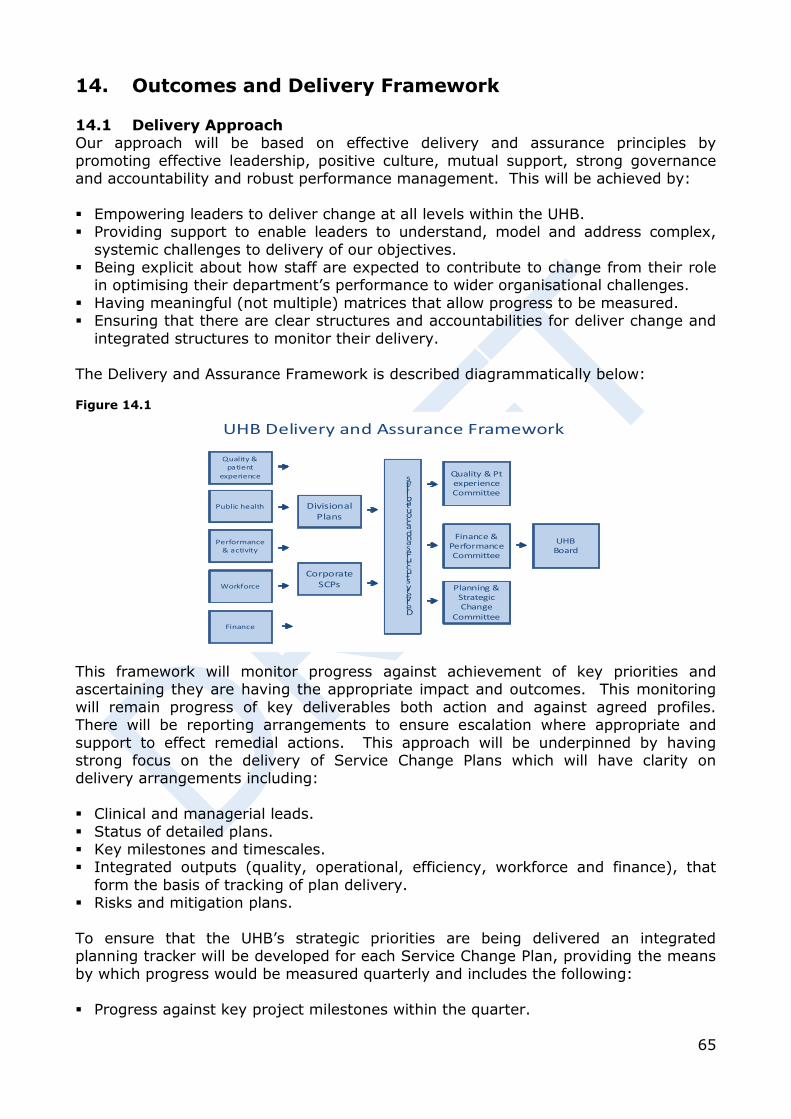
65
14. Outcomes and Delivery Framework 14.1 Delivery Approach Our approach will be based on effective delivery and assurance principles by
promoting effective leadership, positive culture, mutual support, strong governance and accountability and robust performance management. This will be achieved by:
Empowering leaders to deliver change at all levels within the UHB. Providing support to enable leaders to understand, model and address complex,
systemic challenges to delivery of our objectives. Being explicit about how staff are expected to contribute to change from their role
in optimising their department’s performance to wider organisational challenges.
Having meaningful (not multiple) matrices that allow progress to be measured. Ensuring that there are clear structures and accountabilities for deliver change and
integrated structures to monitor their delivery. The Delivery and Assurance Framework is described diagrammatically below: Figure 14.1
This framework will monitor progress against achievement of key priorities and ascertaining they are having the appropriate impact and outcomes. This monitoring
will remain progress of key deliverables both action and against agreed profiles. There will be reporting arrangements to ensure escalation where appropriate and
support to effect remedial actions. This approach will be underpinned by having strong focus on the delivery of Service Change Plans which will have clarity on delivery arrangements including:
Clinical and managerial leads.
Status of detailed plans. Key milestones and timescales. Integrated outputs (quality, operational, efficiency, workforce and finance), that
form the basis of tracking of plan delivery. Risks and mitigation plans.
To ensure that the UHB’s strategic priorities are being delivered an integrated planning tracker will be developed for each Service Change Plan, providing the means
by which progress would be measured quarterly and includes the following:
Progress against key project milestones within the quarter.
UHB Delivery and Assurance Framework
Quality & patient
experience
Public health
Performance & activity
Workforce
Finance
DivisionalPlans
CorporateSCPs
Finance & PerformanceCommittee
Planning & Strategic Change
Committee
UHBBoard
Delivery structures and accoutabilities Quality & Pt
experienceCommittee
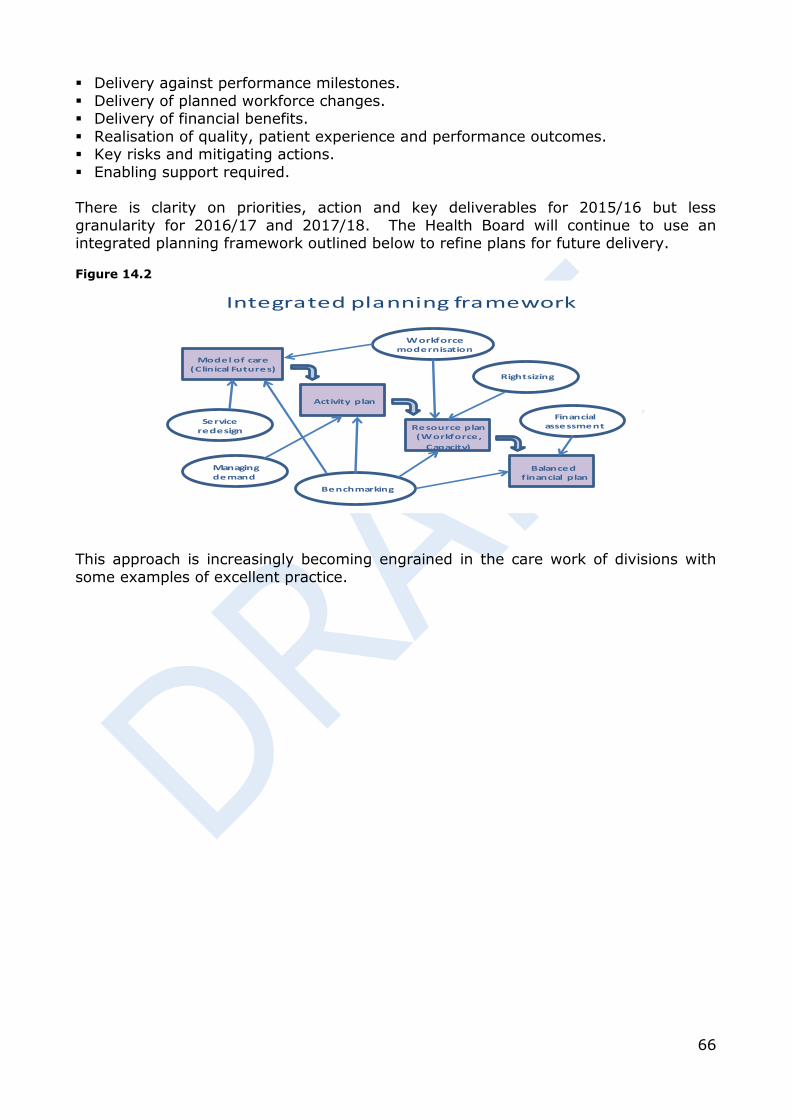
66
Delivery against performance milestones.
Delivery of planned workforce changes. Delivery of financial benefits.
Realisation of quality, patient experience and performance outcomes. Key risks and mitigating actions.
Enabling support required. There is clarity on priorities, action and key deliverables for 2015/16 but less
granularity for 2016/17 and 2017/18. The Health Board will continue to use an integrated planning framework outlined below to refine plans for future delivery. Figure 14.2
Integrated planning framework
Activity plan
Model of care(Clinical Futures)
Resource plan(Workforce,
Capacity)
Balanced financial plan
Managing demand
Financial assessment
Benchmarking
Rightsizing
Service redesign
Workforcemodernisation
This approach is increasingly becoming engrained in the care work of divisions with
some examples of excellent practice.
Related Documents











