http://informahealthcare.com/drt ISSN: 1061-186X (print), 1029-2330 (electronic) J Drug Target, 2014; 22(9): 769–789 ! 2014 Informa UK Ltd. DOI: 10.3109/1061186X.2014.929138 REVIEW ARTICLE Insights into drug delivery across the nail plate barrier Manish V. Saner, Abhijeet D. Kulkarni, and Chandrakantsing V. Pardeshi Department of Pharmaceutics, R. C. Patel Institute of Pharmaceutical Education and Research, Shirpur, North Maharshtra University, Maharashtra, India Abstract Topical therapy is at the forefront in treating nail ailments (especially onychomycosis and nail psoriasis) due to its local effects, which circumvents systemic adverse events, improves patient compliance and reduces treatment cost. However, the success of topical therapy has been hindered due to poor penetration of topical therapeutics across densely keratinized nail plate barrier. For effective topical therapy across nail plate, ungual drug permeation must be enhanced. Present review is designed to provide an insight into prime aspects of transungual drug delivery viz. nail structure and physiology, various onychopathies, techniques of nail permeation enhancement and in vitro models for trans-nail drug permeation studies. Updated list of drug molecules studied across the nail plate and key commercial products have been furnished with sufficient depth. Patents pertinent to, and current clinical status of transungual drug delivery have also been comprehensively reviewed. This is the first systematic critique encompassing the detailed aspects of transungual drug delivery. In our opinion, transungual drug delivery is a promising avenue for researchers to develop novel formulations, augmenting pharmaceutical industries to commercialize the products for nail disorders. Keywords Nail permeation, nail plate, onychomycosis, penetration enhancement, topical therapy, transungual drug delivery History Received 3 April 2014 Revised 9 May 2014 Accepted 25 May 2014 Published online 25 June 2014 Introduction Humans and animals alike are commonly plagued by the infiltration of microorganisms beneath the nail [1]. Topical therapeutics are desirable in the treatment of nail ailments like onychomycosis, a fungal nail infection, and nail psoriasis. These nail ailments are widely spread in the population, among elderly and immunocompromised patients. The topical treatment is an attractive option owing to its non-invasiveness, drug targeting to the site of action, elimination of adverse effects associated with systemic therapy, thereby raising the patient compliance and cutting back the treatment costs. However, topical therapy had limited success, primarily due to poor permeability of the nail plates to the topically applied therapeutics. For effective topical therapy across nail plate, ungual drug permeation must be enhanced [2]. Certainly, enhancement of ungual drug permeation can be accomplished by physical techniques (iontophoresis, acid etching, carbon dioxide laser, hydration and occlusion, electroporation, UV-light, photodynamic therapy, sonophor- esis/phonophoresis), mechanical methods (nail avulsion and nail abrasion) or by use of various chemical penetration enhancers (sulfites, mercaptans, hydrogen peroxides, urea, water, keratolytic agents, keratinolytic enzymes). In the past decade or so, several findings have been reported for transungual delivery of ticonazole [3], econazole [4], oxiconazole [5], ketoconazole [6,7], sertaconazole [8], miconazole [9], terbinafine [10–12], ciclopirox [13], and so on. The increased attention of researchers in this particular area may be ascribable to the infancy in the field, launch and success of several commercial topical antifungal nail lacquers like Loceryl Õ , Penlac Õ , Curanil Õ , and the obvious opportu- nities for research and development of new products in this previously neglected area. There are but few reports highlighting the crucial aspects of ungual and transungual drug delivery and associated limitations. Present review is a state-of-the-art collection of prominent facets that embodies the anatomy of nail apparatus, factors affecting drug transport into and through the nail plate, various diseases of nails, in vitro models to study transungual drug permeation and methods of nail penetration enhance- ment. Furthermore, various drug formulations studied, till date, across the nail plate and key commercial products marketed for nail disorders also contributes to the outline of this review. List of chemical enhancers has been updated to the most recent one. Patents pertaining to transungual drug delivery have also been listed systematically, for the first time. No literature available at present stating the current clinical perspectives on transungual drug delivery and our efforts are first endeavor in this direction. The prime objective behind designing of this manuscript is to present these latest updates before the scientific community. Address for correspondence: Chandrakantsing V. Pardeshi, Assistant Professor, Department of Pharmaceutics, R. C. Patel Institute of Pharmaceutical Education and Research, Shirpur (425405), Dist.- Dhule, Maharashtra, India. Tel: +91 2563 255189. Fax: +91 2563 251808. E-mail: [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

http://informahealthcare.com/drtISSN: 1061-186X (print), 1029-2330 (electronic)
J Drug Target, 2014; 22(9): 769–789! 2014 Informa UK Ltd. DOI: 10.3109/1061186X.2014.929138
REVIEW ARTICLE
Insights into drug delivery across the nail plate barrier
Manish V. Saner, Abhijeet D. Kulkarni, and Chandrakantsing V. Pardeshi
Department of Pharmaceutics, R. C. Patel Institute of Pharmaceutical Education and Research, Shirpur, North Maharshtra University,
Maharashtra, India
Abstract
Topical therapy is at the forefront in treating nail ailments (especially onychomycosis and nailpsoriasis) due to its local effects, which circumvents systemic adverse events, improves patientcompliance and reduces treatment cost. However, the success of topical therapy has beenhindered due to poor penetration of topical therapeutics across densely keratinized nail platebarrier. For effective topical therapy across nail plate, ungual drug permeation must beenhanced. Present review is designed to provide an insight into prime aspects of transungualdrug delivery viz. nail structure and physiology, various onychopathies, techniques of nailpermeation enhancement and in vitro models for trans-nail drug permeation studies. Updatedlist of drug molecules studied across the nail plate and key commercial products have beenfurnished with sufficient depth. Patents pertinent to, and current clinical status of transungualdrug delivery have also been comprehensively reviewed. This is the first systematic critiqueencompassing the detailed aspects of transungual drug delivery. In our opinion, transungualdrug delivery is a promising avenue for researchers to develop novel formulations, augmentingpharmaceutical industries to commercialize the products for nail disorders.
Keywords
Nail permeation, nail plate, onychomycosis,penetration enhancement, topical therapy,transungual drug delivery
History
Received 3 April 2014Revised 9 May 2014Accepted 25 May 2014Published online 25 June 2014
Introduction
Humans and animals alike are commonly plagued by the
infiltration of microorganisms beneath the nail [1]. Topical
therapeutics are desirable in the treatment of nail ailments like
onychomycosis, a fungal nail infection, and nail psoriasis.
These nail ailments are widely spread in the population,
among elderly and immunocompromised patients. The topical
treatment is an attractive option owing to its non-invasiveness,
drug targeting to the site of action, elimination of adverse
effects associated with systemic therapy, thereby raising the
patient compliance and cutting back the treatment costs.
However, topical therapy had limited success, primarily due
to poor permeability of the nail plates to the topically applied
therapeutics. For effective topical therapy across nail plate,
ungual drug permeation must be enhanced [2].
Certainly, enhancement of ungual drug permeation can be
accomplished by physical techniques (iontophoresis, acid
etching, carbon dioxide laser, hydration and occlusion,
electroporation, UV-light, photodynamic therapy, sonophor-
esis/phonophoresis), mechanical methods (nail avulsion and
nail abrasion) or by use of various chemical penetration
enhancers (sulfites, mercaptans, hydrogen peroxides, urea,
water, keratolytic agents, keratinolytic enzymes). In the past
decade or so, several findings have been reported for
transungual delivery of ticonazole [3], econazole [4],
oxiconazole [5], ketoconazole [6,7], sertaconazole [8],
miconazole [9], terbinafine [10–12], ciclopirox [13], and so
on. The increased attention of researchers in this particular
area may be ascribable to the infancy in the field, launch and
success of several commercial topical antifungal nail lacquers
like Loceryl�, Penlac�, Curanil�, and the obvious opportu-
nities for research and development of new products in this
previously neglected area.
There are but few reports highlighting the crucial aspects
of ungual and transungual drug delivery and associated
limitations. Present review is a state-of-the-art collection of
prominent facets that embodies the anatomy of nail apparatus,
factors affecting drug transport into and through the nail plate,
various diseases of nails, in vitro models to study transungual
drug permeation and methods of nail penetration enhance-
ment. Furthermore, various drug formulations studied, till
date, across the nail plate and key commercial products
marketed for nail disorders also contributes to the outline of
this review. List of chemical enhancers has been updated to
the most recent one. Patents pertaining to transungual drug
delivery have also been listed systematically, for the first time.
No literature available at present stating the current clinical
perspectives on transungual drug delivery and our efforts are
first endeavor in this direction. The prime objective behind
designing of this manuscript is to present these latest updates
before the scientific community.
Address for correspondence: Chandrakantsing V. Pardeshi, AssistantProfessor, Department of Pharmaceutics, R. C. Patel Institute ofPharmaceutical Education and Research, Shirpur (425405), Dist.-Dhule, Maharashtra, India. Tel: +91 2563 255189. Fax: +91 2563251808. E-mail: [email protected]

To reach to a valid conclusion, authors desires to mention
here that the field of transungual drug delivery is relatively
young, and vibrant and is a promising avenue for researchers
to develop novel topical formulations for transungual drug
delivery, augmenting pharmaceutical industries to commer-
cialize the products for topical therapy of nail disorders.
The human nail apparatus: structure and physiology
The nail apparatus, as illustrated in Figure 1, is composed of
the proximal nail fold (PNF), nail matrix, nail bed, and the
hyponychium, which altogether formulates the nail plate. The
nail plate (corpus unguis), produced mainly by the matrix,
emerges via PNF and is held in place by lateral nail folds.
It covers the nail bed and detaches from the latter at
hyponychium (skin under the free edge of the nail plate)
[14]. The nail plate is a thin (0.25–1 mm), hard, slightly elastic,
translucent, convex-shaped structure and is made up of
approximately 80–90 layers of dead, keratinized, flattened
cells which are tightly bound to one another via numerous
intercellular links, membrane-coating granules, and desmo-
somes. Based on the differential ultrasound transmission, the
nail plate can be divided into three macroscopic layers, namely
dorsal, intermediate and ventral. The dorsal layer is few cells
thick, while intermediate layer is softer, more flexible and
represents the thickest layer of the nail plate. The ventral layer
is very thin (consists of only 1–2 cells thick), and it connects the
nail plate to the underlying nail blade [14,15]. Often within the
proximal aspect of the nail plate, most notably on thumbs, are
the white crescent-shaped areas, called lanulae. Rich vascular
network of the underlying nail bed imparts visibly pink color to
the dorsal surface of nail unit [16]. According to Kobayashi
et al. [17], the thickness ratio of nail plate layers (dorsal,
intermediate, and ventral) is 3:5:2, respectively. On average,
the dimensions of the flattened corneocytes in the upper nail
layer are 34� 60� 2.2 mm, while those in the lower nail layer
are thicker, at 40� 53� 5.5 mm.
The chemical composition of the nail plate is depicted in
Table 1 [1]. Chemically, nail plate consists mainly of the
fibrous proteins, keratins, 80% of which are of ‘‘hard’’ hair
type keratin while the remainder is of ‘‘soft’’ skin type keratin
[18]. The hair-type keratin filaments are only concentrated in
intermediate nail layers, whereas skin-type keratin filaments
are found in the dorsal and ventral layers [19]. The keratin
filaments are thought to be held together by globular,
cysteine-rich proteins, whose disulfide links act as ‘‘glue’’
and responsible for the toughness and barrier properties of
nails [20]. The nail plate contains 7–12% of water under
normal conditions while the water content can rise up to 35%
at a relative humidity of 100%. Water content is important for
elasticity, flexibility, and opacity of the nail [21,22]. The nail
plate also contains very small amounts of lipids (0.1–1%),
Figure 1. The schematic illustration of nail apparatus. Reprinted from [16], with kind permission of the copyright holder, Elsevier, Amsterdam.
Table 1. Chemical composition and other characteristicsof nail plate [data from 1].
Characteristics Normal values
Water content 9–35%Lipid content 0.1–1%Disulfide linkage 10.60%Thickness 50–1000mMaximum swelling capacity 25%Water loss rate 1.94 mg/cm2/h
770 M. V. Saner et al. J Drug Target, 2014; 22(9): 769–789

which are organized as bilayers, oriented parallel to the nail
surface and concentrated in the dorsal and ventral nail layers
[23,24].
The nail matrix (matrix unguis) (a highly proliferative
epidermal tissue), along with minor contribution from the nail
bed, forms the entire length of the nail plate (Figure 2). It is
likewise called the nail root and lies beneath the PNF. Cell
division of nail matrix results in continuous development of
onychocytes (nail plate cells), which grows throughout the
life [25]. The nail matrix also contains melanocytes, which
pigment surrounding keratinocytes and appears as longitu-
dinal bands across the nail plate, which are often easily visible
in dark-skinned individuals [26].
The PNF has a dorsal and a ventral epithelial surface. It is a
continuation of the skin of each digit (the dorsal surface) that
folds underneath itself, resting above the nail matrix
(the ventral surface) as shown in Figure 1. At the junction
between dorsal and ventral surfaces, there exists the
eponychium (cuticle), which serves to seal off the potential
space between the PNF and the nail plate, shielding the matrix
from environmental damage [26].
The nail bed (area underneath the nail plate) is a thin, soft
and non-cornified epithelium that extends from the lanulae to
the eponychium. The nail bed serves as a holder and slide for the
growing nail plate and plays a predominant role in forming
deeper layers of the nail plate. In relation to other nail
structures, there is a noticeable decrease in cell division among
the keratinocytes within the epidermis of the nail bed [27]. Rich
vascular network of the underlying nail bed imparts visibly pink
color to the dorsal surface of the nail unit. In addition, the nail
bed is well perfused with lymphatic vessels [28].
The hyponychium is situated underneath the free edge of
the nail plate. Anatomically, it indicates the transition of the
nail bed to the normal epidermis of the fingers and toes.
A component of the hyponychium, that reflects onto the
ventral surface of the nail plate called ‘‘onychodermal band’’.
This band serves to protect the nail parenchyma from the
outside environment by providing a barrier to chemical agents
and infectious organisms.
The growth rate of nails is highly variable from individual
to individual. The average growth rate is 3 mm per month for
fingernail and 1 mm per month for toenail. A fingernail grows
out completely in around 6 months while a normal toenail in
12–18 months [20]. The growth rate of nails is highly
influenced by various factors viz. age (ageing slows the rate),
gender (growth rate is higher in males), climate (slower in
cold climate), dominant hand (growth rate is faster), preg-
nancy (faster), diseased condition (the rate may be increased
or decreased; rate is faster in psoriasis, slower in fever),
malnutrition (slower), drug administration (may increase or
decrease the rate) [14].
Physiologically, human nails have been developed to grasp
and manipulate objects. It protects the terminal phalanx and
fingertip from traumatic injury. Nails also provide enhance-
ment of fine touch and fine digital movements and also aid in
scratching and grooming. Nails are often modified or
decorated to become a cosmetic accessory. Nails are also
capable of conveying information about individual’s social
standing [29].
Disease targets for transungual drug delivery
Nails can suffer from a very wide array of diseases which can
range from relatively harmless conditions like pigmentation as
in case of heavy smokers to more painful, and devastating
conditions characterized by dystrophied, hypertrophied,
inflamed or infected nails [28]. Most commonly occurring
nail diseases and their description have been presented in Table
2 [26,30]. The two most common infectious diseases affecting
the nail apparatus are onychomycosis (a fungal infection of the
nail plate and/or nail bed) and nail psoriasis.
Onychomycosis
Onychomycosis (Tinea unguium) is a fungal nail infection,
which accounts for about 50% of nail disorders. It affects
approximately 5% of the population worldwide [31,32]. The
principal pathogens are dermatophyte fungi (Trichophyton
rubrum, T. interdigitale, and T. mentagrophyte,
Figure 2. Schematic representation of subdivisions of nail matrix and their contribution to different layers of the nail plate. The dorsal section (a) of thenail matrix contributes to the most superficial layers of the nail plate whereas the intermediate region (b) of the nail matrix forms the deeper layers.The ventral subdivision (c) is the most distal part of the nail matrix and it is contributed by the nail bed. Reprinted from [16], with kind permission ofthe copyright holder, Elsevier, Amsterdam.
DOI: 10.3109/1061186X.2014.929138 Drug delivery across the nail plate barrier 771

Epidermophyton floccosum), the non-dermatophyte molds
(Scopulariopsis brevicaulis and Scytalidium dimidiatum), and
yeasts (Candica albicans) [33]. Majority (90–95%) of the
infections are caused by dermatophytes, while the rest being
caused by yeast and molds. Toenails are affected more than
fingernails [34]. Onychomycosis is found to be more preva-
lent in elderly patients and diabetics [35]. The other risk
factor associated with onychomycosis are immunosupression,
as in Human Immunodeficiency Virus (HIV) infection and
cancer, and atopic disorders. Therefore, the incidence of
onychomycosis seems to increase due to rising elderly
population, extensive use of immunosuppressant in infections
with HIV. Current lifestyle factors such as wearing of tight-
fitting clothings, use of communal recreational facilities and
health clubs have too led to the increased prevalence of
onychomycosis [36–39].
Clinically, onychomycosis can be categorized into four
types depending on the site of infection and pathophysiology:
namely (i) distal and lateral subungual onychomycosis: fungal
infection begins at hyponychium and distal or lateral nail bed,
(ii) superficial white onychomycosis: fungal infection begins
at nail plate and white chalky patches appears on the nail
plate, (iii) proximal subungual onychomycosis: fungal infec-
tion invades via PNF and penetrate the nail plate, producing
white discoloration in the lanulae, (iv) total dystrophic
onychomycosis: entire nail plate and nail bed are attacked
by the fungus and this is the endpoint of all forms of
onychomycosis [40].
Clinical diagnosis of onychomycosis is based on the
patient’s history, physical examination, direct microscopy,
and culture of nail specimens. Direct microscopy serves
only as a screening technique for the presence or absence
of fungi; culture can actually assist in differentiating among
the pathogens and identifying the etiological agents [32].
Onychomycosis is difficult to treat since it is chronic, hard
to eradicate and tends to relapse. In the past, surgical avulsion
was the only treatment option for onychomycosis. Surgical
avulsion, is, however, extremely traumatic and painful [41].
Treatment of onychomycosis is known to be challenging;
failure to achieve ‘‘disease-free nail’’ is fairly common with
one course of therapy [42] and a high relapse rate (22.2%) is
reported by Tosti et al. [43]. Such treatment failure has been
attributed to a possible lack of diagnostic accuracy, incorrect
antifungal or delivery strategy, presence of dormant spores
(not killed by antifungals, thereby acting as a reservoir of
fungus and germinate to relapse the infection, after
the conclusion of the treatment), concentrated zones of
fungi (into which drug diffusion is inadequate) or resistant
fungi [44]. Currently, the pharmacotherapy for onychomy-
cosis involve the use of systemic (terbinafine, itraconazole,
fluconazole, griseofulvin, etc.) and topical (amorolfine,
ciclopirox, tioconazole, etc.) antifungal agents, either alone
or in combinations, depending on the severity of the
condition. Mechanical treatments (surgical/mechanical nail
avulsion or debridement) are also on current treatment
strategy options. Topical treatment avoids problems asso-
ciated with systemic therapy. However, in case of former,
drug diffusion into highly keratinized nail plate is poor
and duration of treatment is long. Currently, topical therapy
is recommended only in early stages of the disease and
when only a few nails are affected, due to its limited success
rate [2].
Table 2. Most commonly occurring nail diseases and their description [26,30].
Disease/disorder Description
Onychomycosis It is a fungal nail infection caused by dermatophytes, yeasts or non-dermatophyte molds. The prevalence rate ofonychomycosis is determined by age, occupation, social class, climate and living environment.
Nail psoriasis It is characterized by pitting (presence of small shallow holes in the nail plate), nail fragility, crumbling and nail loss.It may also result in onycholysis (separation of the nail plate from the nail bed), subungual hyperkeratosis, splinterhemorrhages and paronychia (inflamed and swollen nail folds).
Nail patella syndrome It is also known as HOOD (hereditary onycho-osteodysplasia) syndrome. It is a genetic disorder and the majorhallmarks of this syndrome are poorly developed fingernails and toenails. The lack of growth or complete absence offingernails results from the mutations in the LMX1B gene.
Subungual hematoma It is a collection of blood underneath a fingernail or toenail. It is sometimes known as runner’s toe or tennis toe. It maybe caused by horizontal separation of the nail plate from the nail bed. It is characterized, clinically, by reddish-blackdiscoloration of the nails. The nail plate may also get more compact and more brittle as a consequence of the injury(onychochauxis).
Beau’s lines Beau’s lines are deep grooved horizontal lines of darkened cells that run from side to side on the fingernail. It may beinduced by injury, illness, malnutrition or major metabolic condition or due to chemotherapy. It may be the result ofany interruption in the protein formation of the nail plate.
Pterygium unguis It is also known as dorsal Pterygium. It is the inward advance of skin over the nail plate usually the result of trauma tothe matrix due to a surgical procedure or by a deep cut to the nail plate. It results in the loss of nail plate due to thedevelopment of scar tissue.
Onychatrophia Onychatrophia is a scarring process. It is an atrophy or wasting away of the nail plate which causes it to lose its luster,shrinks and falls off. Once it is damaged, the nail won’t recover.
Onychogryposis It is also known as ram’s horn nails. It is a hypertrophy that may produce nails resembling claws or ran’s horn. It ischaracterized by thickened nail plate and often a result of trauma. It represents the inward curved nail plate, pinchingthe nail bed.
Obychorrhexis Onychorrhexis are also known as brittle nails, in which nail plate often split vertically, peel and/or have vertical ridges.It may be hereditary or may result from excessive use of strong soaps, water exposure or nail polish remover.
Leuconychia It is characterized by white lines or spots in the nail plate. The most common cause is the injury to the nail matrix.It may be caused by entrapment of tiny air bubbles in the nail plate layers due to trauma or it may be hereditary.
Melanonychia It is characterized by vertical black or brown pigmented bands, often termed as ‘‘nail moles’’, which usually form in thenail matrix. It may be a result of trauma.
772 M. V. Saner et al. J Drug Target, 2014; 22(9): 769–789
Nail psoriasis
Nail psoriasis is the second most important disease target for
the development of topical nail products as it is alleged to be
prevalent in 80–90% of patients with skin psoriasis and affects
about 1–3% of the entire population. The disease can affect
the nail plate, nail matrix, nail bed, nail folds and the
surrounding soft tissues. The psoriatic nail matrix results in
pitting (presence of small shallow holes in nail plate), nail
fragility, crumbling or nail loss. Nail bed involvement causes
onycholysis (separation of the nail plate from the nail bed),
subungual hyperkeratosis (deposition and collection of cells
under the nail plate) and splinter hemorrhages (as a result of
trauma). Psoriatic nail folds results in paronychia (inflamed
and swollen nail folds) which leads to transverse ridging of
the nail plate [45].
Nail psoriasis tends to be persistent and refractory to
treatment and hence, it is understandable that a standardized
therapeutic regimen does not currently exist. Although,
intralesional injections of cortisone into the nail fold,
topical application of corticosteroids, vitamin D3 analogs,
5-fluorouracil (5-FU), anthralin, tazarotene, phototherapy and
photochemotherapy, systemic administration of immunosup-
pressants, combination therapies and biological therapies have
shown some success [16,46]. Diseased nails may also be
chemically extracted using urea ointment. Urea ointment
(40%) upon application softens the diseased nail plate and,
after 5–10 d, the entire nail plate may be lifted off the nail bed
and trimmed behind the PNF. A disease-free nail may then
grow back [14,47].
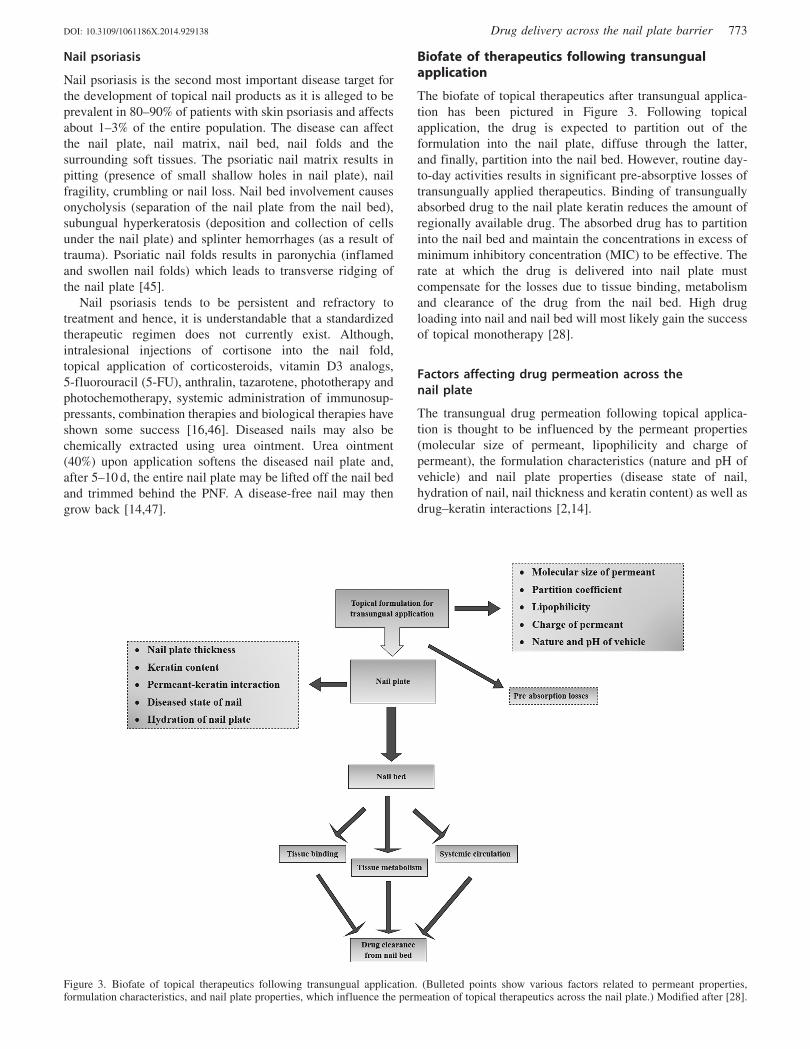
Biofate of therapeutics following transungualapplication
The biofate of topical therapeutics after transungual applica-
tion has been pictured in Figure 3. Following topical
application, the drug is expected to partition out of the
formulation into the nail plate, diffuse through the latter,
and finally, partition into the nail bed. However, routine day-
to-day activities results in significant pre-absorptive losses of
transungually applied therapeutics. Binding of transungually
absorbed drug to the nail plate keratin reduces the amount of
regionally available drug. The absorbed drug has to partition
into the nail bed and maintain the concentrations in excess of
minimum inhibitory concentration (MIC) to be effective. The
rate at which the drug is delivered into nail plate must
compensate for the losses due to tissue binding, metabolism
and clearance of the drug from the nail bed. High drug
loading into nail and nail bed will most likely gain the success
of topical monotherapy [28].
Factors affecting drug permeation across thenail plate
The transungual drug permeation following topical applica-
tion is thought to be influenced by the permeant properties
(molecular size of permeant, lipophilicity and charge of
permeant), the formulation characteristics (nature and pH of
vehicle) and nail plate properties (disease state of nail,
hydration of nail, nail thickness and keratin content) as well as
drug–keratin interactions [2,14].
Figure 3. Biofate of topical therapeutics following transungual application. (Bulleted points show various factors related to permeant properties,formulation characteristics, and nail plate properties, which influence the permeation of topical therapeutics across the nail plate.) Modified after [28].
DOI: 10.3109/1061186X.2014.929138 Drug delivery across the nail plate barrier 773

Permeant properties
The most significant permeant property that has marked
influence on the permeation of diffusing molecules is the
molecular weight. As likely, molecular weight has an inverse
relationship with the drug permeation into nail plate. Higher
the molecular weight, harder it is for permeating molecule to
diffuse through the keratin network, and lower is the
permeation [48]. Kobayashi et al. [49] reported that the
dense keratin network of nail is found to increase the path
length of diffusing molecules by virtue of its greater pore
tortuosity. The permeation rate was found to decrease, on
account of increased friction between diffusing molecules and
the keratin network, as the molecular size of permeant
increased. Permeation of larger molecules through the pores
in the close-meshed keratin network of the nail plate is
obviously more difficult than the permeation of smaller
molecules. There exists an inverse relationship between
the permeability coefficient of several ionic and non-ionic
model drugs across human nail plate and their molecular
weight.
The permeability of diffusing molecules through nail plate
is influenced by the permeability coefficient of the permeant.
In most instances, the permeation rate was found to decrease
with an increase in carbon-chain length or lipophilicity of the
permeant. The decrease in permeability coefficient with
increase in lipophilicity of permeant was attributed to
hydrophilic nature of the nail plate [14,28]. Walters et al.
[50] studied the permeation of a series of homologous
alcohols (C1–C12), diluted in saline, through avulsed human
nail plates. Increasing chain length from single carbon to
eight carbon atoms resulted in decreased permeability coef-
ficient, after which, increasing chain length (up to C12)
resulted in an increased permeability coefficient. The nail
plate seems to be a hydrophilic gel membrane when the
permeation of lower alcohols (5C8) is considered. The
authors have concluded that the nail plate behaves like a
concentrated hydrogel and this indicates a facilitating role of
water towards the diffusion of alcohol molecules. It is
possible that when an aqueous formulation is applied, nails
swell due to water uptake into the nail plate. Consequently,
the keratin network expands, leading to the formation of
larger pores through which diffusing molecules can permeate
more easily. Still, the increase in permeation of higher
alcohols (C10–C12) with increasing lipophilicity was sug-
gested to take place through a lipidic pathway. Despite the
lower lipid content (0.1–1%) in the nail plate, this lipidic
pathway appears to be important rate-controlling barrier to
the passage of highly hydrophobic permeant.
A surface charge of permeant seems to be a key
consideration for passive diffusion of molecules through the
nail plate. Regardless of the nature of the charge, non-ionic
permeants were found to have approximately 10-fold greater
permeability as compared to their ionic counterparts [49]. The
low permeability of the charged species was thought to be
caused by a small increase in molecular size due to the
hydration of the charged species. Reduced permeation of
the charged species was attributed to the ‘‘Donnan effect’’,
i.e. electrostatic repulsion between the charged keratin
membrane and like-charged diffusing molecule [51,52].
The nail keratin has an isoelectric point (pI) of 5.0 [53],
thus carries a net negative charge at pH 7.4 while net positive
charge at pH 2.0. At pH 7.4, the negatively charged benzoate
ion is repelled by the negatively charged keratin, resulting
in decreased diffusion of the solute through the nail
plate and thereby lowered permeability coefficient. This
reduced permeability was attributed to the decreased keratin
swelling due to charge inversion of keratin, when the
environment was altered from an acidic to a neutral or basic
one [54]. Similarly, at pH 2.0, the positively charged
pyridinium ion is repelled by the positively charged keratin,
resulting in lower permeability coefficient of the pyridinium
cation [14].
Formulation characteristics
Water plays a facilitating role in enhancing the diffusion of
water soluble permeants through the nail plate. The perme-
ability coefficients of alcohols diluted in saline through nail
plates was 5 times greater than the permeability coefficient of
neat alcohols [55]. Water hydrates the nail plate, resulting in
subsequent swelling. Considering the nail plate to be a
hydrogel, swelling results in expansion of keratin network,
leading to the formation of larger pores. Permeant molecules
can diffuse through these pores easily resulting in increased
permeability coefficient. Replacing water with non-polar
solvent, which does not hydrate the nail plate, is therefore
expected to reduce the drug permeability into nail plate. This
was demonstrated by Walters et al. [55], whose results
suggested that the addition of non-polar co-solvent such as
dimethyl sulfoxide (DMSO) and isopropanol decreased the
transungual permeation of hexanol. In short, increasing
concentration of co-solvent or decreasing concentration of
water in the medium results in decreasing permeability
coefficient of hexanol. The precise mechanism behind this has
not been well documented.
The molecules in soluble form and unionized state, in
general, have good permeation across nail plate. The pH of
the aqueous vehicle governs the extent of ionization, aqueous
solubility of the permeant and its interaction with nail plate
keratin fibers. The extent of ionization is influenced by pKa
value of the permeant and the pH of the vehicle. As a general
rule, acidic drugs are unionized at lower pH values while
basic drugs remain unionized at higher pH values. Thus, it is
estimated that acidic drugs are well permeated at low pH
values while basic drugs exhibit better permeation at higher
pH values. Soong [56] studied the permeation of benzoic acid
through a human nail plate at different pH. The donor
compartment contained a saturated solution of permeant
and receptor compartment contained permeation medium of
the same pH as of the donor. It was observed that, as the
pH of the medium increased from 2.0 to 8.5, the permeability
coefficient of benzoic acid decreased by 95.5%. This
was attributed to greater permeation of uncharged molecules
(at pH 2.0) through the nail plate compared to charged
molecules (at pH 8.5). Further, Mertin and Lippold
(1997b) [54], also observed the greater permeation of
undissociated benzoic acid at pH 2.0 across the bovine
hoof membrane compared to dissociated benzoate ion at
higher pH.
774 M. V. Saner et al. J Drug Target, 2014; 22(9): 769–789

Nail plate properties
The various nail plate properties which have significant
influence on the permeation of drug across the nail plate
includes the nail plate’s diseased state, hydration, thickness,
keratin content and permeant–keratin interactions. The nail
plate’s diseased state is expected to have an enormous
influence on nail permeability. Kobayashi et al. [49] demon-
strated comparable permeation of 5-FU in healthy nail plates
and in nail plates with mild fungal infection. Nail plate with
heavy fungal infections were not used due to their uneven
thickness and as such plates ‘‘collapsed’’ when placed in
water. However, the diseased nail plate may be heavily
thickened, which increases the distance the drug has to
permeate through the nail plate before reaching the nail bed;
this would have a negative influence on the success of topical
therapy. Also, presence of dermatophytoma (a dense focus of
fungi with thick shortened hyphae) in onychomycotic nails is
likely to change the drug diffusion through nail plate; thereby
is thought to melt off the success of topical therapy. Diseased
nail plates may also be more ‘‘crumbly’’, which could
increase the nail porosity and thereby increase the nail
permeability. The diseased nail plate can also detach from the
nail bed, and such detachment presents a huge barrier to drug
movement into the nail bed if the detachment is surrounded
by ‘‘non-detached’’ nail areas. On the other hand, if
onycholysis occurs at the proximal edge of the nail plate,
drug formulation can be applied within the detached space,
which would facilitate drug delivery into the nail bed [2].
Hydration of nail plate increases the ungual permeability
of polar compounds as the nail plate is thought to behave like
a concentrated hydrogel and the mechanism behind this fact
has already been discussed earlier [55]. De Berker et al. [57]
observed the increased toenail thickness along the nail. Mean
nail plate thickness increased progressively along the entire
length of the nail ranging between 590mm and 1080 mm. This
high thickness poses the difficulty for the permeant to
penetrate the nail structure.
Binding of permeant to keratin within the nail also
contribute to disappointing topical efficacy in nail diseases.
Binding to keratin reduces the availability of permeant,
weakens the concentration gradient and thereby limits the
deep penetration [58].
Enhancement of drug permeation into nails
Nail disorders can be successfully treated only when applied
topical therapeutics are able to permeate through the dense
keratinized nail plate and reach the deeper layers of nail
apparatus at amounts above the MIC. This can be made
practically possible using different techniques of ungual
penetration enhancement viz. physical, chemical and mech-
anical methods (Figure 4). However, effective penetration
remains challenging as the nail is thought to be made of
approximately 80–90 layers of tightly bound keratinized cells,
100-folds thicker than the stratum corneum (SC) [59].
Therefore, high nail thickness, poor drug permeation and
prolonged transport lag time contribute to unsatisfactory
outcomes in ungual topical therapy. Physical, chemical and
mechanical modes of penetration enhancement may improve
topical efficacy.
Mechanical methods of nail penetration enhancement
Mechanical methods of nail penetration enhancement
(nail abrasion and avulsion), although invasive and extremely
painful, have been used by dermatologists and podiatric
physicians since long time. Thus, current research focuses on
less invasive physical and chemical modes of nail penetration
enhancement.
Nail abrasion
Out of three layers of nail (dorsal, intermediate and ventral,
that vary in thickness in the proportion of 3:5:2, respectively),
the dorsal layer is found to be the major barrier for permeation
of drug into the nail plate. One of the methods employed to
mechanically enhance the transungual drug delivery is filing
the surface of the nail plate using an abrasive. Filing removes
the dorsal layer of nail plate, thus reduces the barrier that
drugs have to permeate through to reach the deeper nail
layers. Filing has shown to double the permeability
coefficient of 5-FU and flurbiprofen through the nail plate
in vitro [17]. In clinical trials, filing the nail plate prior to the
application/re-application of drug-loaded formulations were
found to be indispensable for the success of topical therapy
[60,61]. Nail abrasion, sometimes, involves sanding of the
nail plate to thin out its thickness or destroy it completely.
Depending on the required intensity, sandpaper number 150
or 180 can be utilized for sanding purpose. The sanding must
be performed on nail edges and should not cause discomfort.
An efficient instrument for sanding is a high-speed
(350 000 rpm) sanding hand piece. Nail abrasion, using
sandpaper nail files, prior to antifungal nail lacquer treatment
may reduce the critical fungal mass and thereby aids in
effective penetration [62,63].
More aggressive abrasion of dorsal surface of nail plate
using electrical equipment or nail drilling using dentist’s drill
has proved to be beneficial in clinics for improving the
efficacy of topical antifungal treatment [63–66]. Sumikawa
et al. [67] performed the drilling to reduce nail thickness to
1–2 mm in thickened nail areas and studied the influence of
foot care intervention on topical therapy of distal-lateral
subungual onychomycosis in diabetic patients.
Nail avulsion
Total nail avulsion (surgical removal of entire nail plate) or
partial nail avulsion (partial removal of the affected nail plate)
is usually carried out under local anesthesia. Keratolytic
agents (urea or a combination of urea and salicylic acid),
which softens the nail plate, have been utilized for non-
surgical nail avulsion in clinical studies, prior to topical
treatment of onychomycosis [68].
Physical methods of nail penetration enhancement
Iontophoresis
The application of electric current (electromotive force) has
proved to enhance the diffusion of charged molecules through
the hydrated keratin network of a nail and found to cause a
large increase in ungual drug flux compared to passive
transport [58,69]. Transungual transport of uncharged per-
meants depends on electroosmosis while that of ionic
DOI: 10.3109/1061186X.2014.929138 Drug delivery across the nail plate barrier 775

permeants relies on electrophoresis, with a small contribution
from electroosmosis. Influence of electric current on nails are
reversible in vitro; nail plates return to their normal after
iontophoretic treatment [59]. Several factors responsible for
enhancement of iontophoretic drug flux includes: electro-
phoresis/electrorepulsion (interaction between electric field
and charge of ionic permeant), electroosmosis (convective
solvent flow in preexisting and newly charged pathways),
permeabilization/electroporation and electric-field induced
pore induction [58,59].
Murthy et al. (2007a) was the first to demonstrate the
feasibility of transungual iontophoresis. The authors system-
atically studied in vitro transport of salicylic acid (SA) across
the human nail plate using specifically-designed diffusion
cells [58]. Iontophoresis significantly enhanced drug flux
through the nail compared to passive transport. Iontophoretic
trans-nail flux improved with higher SA concentration
(up to 2 mg/ml), higher current density (up to 0.5 mA/cm2),
higher buffer ionic strength (50–100 mM) and higher pH.
Findings of Murthy et al. (2007b) stated increased
transungual glucose and griseofulvin flux with higher pH
(pH45) in anodal iontophoresis [69]. Cathodal iontophoresis
followed the opposite trend for pH-dependent transport
(i.e. increased drug flux at lower pH). SA flux was enhanced
�16-fold while of griseofulvin �8-fold with iontophoresis
[58,69].
Hao and Li (2008a) accomplished in vitro iontophoresis
experiments on human nails with neutral and charged
molecules. Anodal iontophoresis at 0.3 mA enhanced manni-
tol (MA) and urea (UR) transport compared to passive
transport. Also, findings suggested only a marginal contribu-
tion of electroosmosis in anodal iontophoretic transport
of MA and UR at low electric currents (�0.3 mA). The
contribution of electroosmosis increased with permeant’s
molecular size and current strength [59]. For a positively
charged permeant, tetraethylammonium ion (TEA), pene-
tration was significantly enhanced �29-fold with anodal
iontophoresis at only 0.1 mA. Moreover, the contribution
of electroosmosis was less than 10% of electrophoresis in
TEA [59].
Figure 4. Illustrative representation of the various techniques of nail penetration enhancement.
776 M. V. Saner et al. J Drug Target, 2014; 22(9): 769–789

Hao and Li (2008b) [70] also examined the influence of
pH and ionic strength on the electro-osmotic transungual
transport of neutral molecules. When pH was below pI
(pH55), the nail plates were positively charged and electro-
osmotic flow occurred from cathode to anode. On the
contrary, when pH was above pI (pH 45), the nail plates
were negatively charged and electro-osmotic flow occurred
from anode to cathode. In addition, electroosmosis improved
significantly from pH 7.4 to 9.0 in anodal iontophoretic
transport. As discussed earlier, electro-osmosis contribution
was greater in MA than UR due to increased molecular size.
Furthermore, the significant electro-osmotic enhancement
was seen only in MA, not UR, with pH changes (anodal
transport at pH 7.4 and 9.0 and cathodal transport at pH 3.0).
Electroosmosis correlated inversely with ionic strength,
decreasing former by four times when the solution ionic
strength increased from 0.04 to 0.7 M.
Manda et al. [71] investigated the plausibility of ionto-
phoretic delivery of terbinafine hydrochloride (TH) to the nail
matrix via PNF. In vitro drug permeation studies were
performed in Franz diffusion cell across folded porcine
epidermis as a model for PNF. A custom-designed foam-pad-
type patch system was used for iontophoresis across excised
cadaver toenails. The amount of drug delivered into the nail
matrix following iontophoresis for 3 h at 0.5 mA/cm2 was
significantly higher than the MIC of TH. The study concluded
that the iontophoresis across the PNF could be developed as a
potential method to target drugs to nail matrix.
Acid etching
Application of surface-modifying chemical etchants (10%
phosphoric acid gel or 20% tartaric acid solution) onto the
dorsal surface of nail clippings was used in vitro to modify the
nail plate surface, resulting in formation of profuse micro-
porosities, prior to application of topical formulations, such as
adhesive polymeric films [7,72]. These microporosities
increases the wettability and surface area and decreases the
contact angle; thereby provide an ideal surface for bonding
materials. They improve interpenetration and bonding of a
polymeric delivery system and facilitate interdiffusion of
topical therapeutics [7]. Atomic force microscopy (AFM)
revealed that application of abovementioned etchants
increased the mean surface roughness by 1.3 and 1.7 times,
respectively. Etching the nail plate surface with phosphoric
acid gel also increased the adhesion of drug-loaded polymeric
films onto the nail plate surface and drug diffusion
(the latter by �6-fold) through the nail plate. Improved
bioadhesion and drug permeation were thought to be
attributed to the increased nail plate surface area, providing
‘‘greater opportunity for the polymer chains (of therapeutic
films) to bond with the nail plate and for drug diffusion’’. The
latter also benefited from a decreased membrane thickness of
the etched nail plate, as studied on hot-melt extruded (HME)
hydroxypropyl cellulose (HPC) films loaded with ketocon-
azole as a model drug, across human nails in vitro [72,73].
Pulsed laser/carbon dioxide (CO2) laser
Natural barriers that limits the permeation of topical
therapeutics have been abandoned by pulsed laser systems.
Following topical application, laser energy would be
absorbed by the keratin network in the nail plate and
scattered heat lead to vaporization and thus, removal of nail
layers.
Laser application on the nail plate in vitro resulted in the
formation of craters whose shape, size and other properties,
such as crater wall smoothness, the presence of cracks and of
melted and re-solidified tissue depended on the nature of laser
system employed. The effect of different laser systems on nail
plate ablation rates, ablation efficiencies and subsequent
crater morphologies has been studied by Neev et al. [74].
Among four laser systems studied, the ultrashort pulsed laser
system was found to display best ablation efficiencies without
cracks or thermal damage to the nail plate. However, the
efficacy of laser on transungual drug permeation in vivo is yet
to be established [74].
CO2 laser treatment may produce positive, but unpredict-
able, results. One method involves avulsion of diseased nail
portion followed by laser treatment at a density of 5000 W/
cm2. Thus, underlying tissue is exposed to direct laser
therapy. Penetrating the nail plate with CO2 laser beam
followed by daily topical antifungal treatment, penetrating
laser-induced puncture holes is another method of nail
penetration enhancement based on CO2 laser-treated ablation
of nail plate [75].
Microporation
PathFormer is an FDA-approved hand-held microcutting
(nail trephination) device (developed by Path Scientific,
Carlisle, USA) used to drill a hole (microconduite) of specific
depth in the nail plate without affecting the nail bed in order
to drain subungual hematomas [76]. Figure 5 depicts the
PathFormer device, its components and the microconduites
drilled in toenail using PathFormer [77]. This device uses
the electrical resistance of the nail bed as a feedback to stop
and retract the drill when it has penetrated through the nail
plate. Besides, it eliminated the need for anesthesia. The nail
plate is drilled using a 400-mm diameter tissue cutter in a
hand-held device driven by two small electrical motors.
The depth of the hole created by the device is said to be
precisely controlled by the electrical resistance; the electrical
resistance of the highly keratinized nail plate decreases upon
microcutting from 5 MX (undrilled) to 10–20 kX (upon
reaching the nail bed) as each successive layer of nail tissue
is removed [78]. Microconduites of varying depths corres-
ponding to the electrical resistances ranging from 90 to 25 kXwere drilled to assess the tolerability of the technique
in healthy adult subjects. The procedure was well tolerated,
with regard to pain and pressure felt by the volunteers,
when five microconduites (of diameter 400 mm and depths
corresponding to electrical resistance of 90–25 kX) were
drilled in each patient’s toenail, without penetrating the
nail bed.
Boker and co-workers employed the same device in their
clinical studies to drill microconduites prior to application of
terbinafine cream and placebo cream. Though transungual
permeation of terbinafine was increased, the number of
microconduites drilled and the extent of enhancement
obtained is not revealed [79].
DOI: 10.3109/1061186X.2014.929138 Drug delivery across the nail plate barrier 777

Low-frequency ultrasound
The potential of low frequency ultrasound as a physical nail
penetration enhancement technique has been evaluated on
whole nail plates and on bovine hoof membranes [80,81].
Torkar and co-workers applied a low frequency ultrasound
(20 kHz) to the hoof membranes using a 13-mm ultrasound
probe held at a distance of 13 mm from the surface through a
liquid coupling medium and employed a 50% intensity level
as a pretreatment procedure for 1 min in a pulsatile fashion.
Their findings suggested an enhanced drug permeation
through hoof membrane and it was attributed to the
ultrasound-induced disruption of the hoof membrane [81].
Although the mechanism of membrane disruption has not
yet been clearly interpreted, it is possible that inertial
cavitation or pit formation is involved, as has been proposed
for low frequency ultrasound-assisted transdermal drug
delivery [82,83]. Cavitation (formation and collapse of gas
bubbles) occurs when low frequency ultrasound waves are
applied in a liquid. Cavitation may be stable (periodic bubble
growth and oscillations) or inertial (violent growth and
collapse). The violent collapse of a very large number of gas
bubbles in the liquid medium generates shock waves, which
travel through the membrane and impact on the membrane
(Figure 6a). This results in asymmetrical pressure and the
formation of liquid microjects which impact on (Figure 6b)
and penetrate through the membrane (Figure 6c). This leads
to the formation of pits on the membrane surface, which could
act as conduites or microconduites for ungual drug flux.
Hydration and occlusion
Hydration may increase the pore size of nail matrix, thereby
enhances the transungual penetration. Again, hydrated nails
are more elastic and permeable. Hydration aids in enhanced
iontophoretic transungual drug delivery [59], whereas solu-
tion pH and ionic strength have no significant influence on
nail hydration [70].
Human nails can retain water �25% of its weight, twice of
its normal water content (10–15%), and has a pronounced
effect on drug penetration in the region of high water content
(RH480%) [84]. Gunt and Kasting reported that increasing
ambient relative humidity (RH) from 15% to 100% enhanced
permeation of [3H]-ketoconazole by �3-folds in vitro, as
studied on excised human nail plates. Flux increased from
0.175 mg/cm2/h at 15% RH to 0.527 mg/cm2/h at 100% RH [85].
Figure 5. Diagram demonstrates: (a) the PathFormer (nail trephination) device, consisting of power supply circuite, foot of PathFormer, and sensingelectrodes. (b) Application of PathFormer on a fingernail: The sensing electrodes are attached to the skin prior to the procedure. The circuite verifiesthat the electrodes are in good contact with the skin. The foot of the PathFormer stabilizes the device during 3–5 s procedure. (c) Close up view of thePathFormer’s foot (shown in inset). The electrically conducting foot encloses, but does not contact the cutter. The cutter is held tightly by the chuck.The blue switch on the top activates the device, and (d) a row of five openings (microconduites) drilled in toenail with PathFormer. Each opening is0.4 mm in diameter, and created in less than 3 s. Reproduced from [77], with kind permission from PathScientific, Carlisle, MA.
778 M. V. Saner et al. J Drug Target, 2014; 22(9): 769–789

Susilo et al. revealed in their in vivo experiments
examining sertaconazole-loaded nail patches, a remarkable
enhanced nail penetration (40–50%) with mean sertaconazole
concentrations above the MIC at 2, 4 and 6 weeks [8].
Transonychial water loss, decrease in ceramide concentration
and water binding capacity may result from onychomycosis.
Occlusion may resolve these changes via reconstitution of
water and lipid homeostasis in dystrophic nails. In addition,
sertaconazole was able to amass in substantial subungual
concentrations under occlusion [8].
Miscellaneous methods
A patent has been filed on ONYCHOLASER� – a micro-
surgical laser unit which is used to make holes in tissues,
especially fingernails and toenails [86]. Antifungals are then
topically applied to these holes for the treatment of
onychomycosis.
A recent patent on the application of heat and/or UV light
to fingernails or toenails that are afflicted by onychomycosis,
discusses the different devices and methodologies which may
effectively provide exposure. It involves heating the nail,
exposing it to UV light and subsequently treating with topical
antifungal therapy [87].
5-Aminolevulinic acid-mediated photodynamic therapy
(ALA-PDT) is a medical treatment based on a combination
of a sensitizing drug and a visible light used together for
destruction of cells. Donnelly et al. [88] developed a
novel bioadhesive patch containing ALA and conducted
in vitro penetration studies across the human nail. Their
findings suggested that, if sufficient concentrations of ALA
could be achieved within the nail matrix and at the nail
bed, PDT may open the new vistas for treatment of
onychomycosis.
Chemical methods of nail penetration enhancement
Many chemical permeation enhancers that facilitate
transdermal penetration have not been effective in enhancing
the transungual drug permeability. As earlier mentioned
in ‘‘The nail apparatus’’, the lipid content of the nail plate is
0.1–1%. This very low lipid levels explain why transdermal
enhancers, many of which are known to act by fluidizing
the skin lipids, have been unsuccessful as transungual
penetration enhancers. Chemical enhancement of nail
plate permeability has therefore been focused on the cleavage
of chemical and physical bonds that maintain the integrity
of nail plate keratin. The disulfide, peptide, hydrogen and
polar bonds were identified as potential targets for
ungual chemical penetration enhancers. The chemical
enhancer may be applied to the nail plate prior to or
concomitantly with the drug formulation. The various
chemical enhancers exploited till date have been quoted in
Table 3.
Figure 6. Proposed mechanism of transungual penetration enhancement by low-frequency ultrasound. Cavitation of gas bubbles in the liquid mediumresults in generation of shockwaves which impact on the membrane (a), while gas bubbles collapse near the membrane results in the formation of liquidmicrojets which impact on membrane (b), and even penetrate through the membrane (c). Reprinted from [83] after slight modifications, with kindpermission of the copyright holder, Elsevier, Amsterdam.
Table 3. Chemical enhancement of ungual drug permeation (Modified after [2]).
Chemical enhancer Permeant Methodology Ref
Sodium sulfite 5,6-Carboxyfluoresceine Diffusion cells [2]2-n-Nonyl-1,3-dioxolane Econazole EcoNail� lacquer [4]N-acetylcysteine (15%) Oxiconazole Drug applied on human nail
plates for 6 weeks[5]
N-(2-mercaptopropionyl) glycine (MPG, 10%) Water Diffusion cells [89]Mercaptoethanol (3%) Tolnaftate; 5-FU Diffusion cells [90]N-acetylcysteine (3%) 5-FU, Tolnaftate Diffusion cells [90]Thioglycolic acid & Urea- H2O2 Caffeine, Methylparaben, Terbinafine ————— [91]Cysteine Mannitol Diffusion cells [93]Thioglycolic acid (5%) Caffeine, Mannitol Diffusion cells [93]H2O2 (35%) Mannitol Diffusion cells [93]Keratinolytic agents (Keratinase) Metformin HCl Diffusion cells [97]Keratolytic agents (Papain, Urea & salicylic acid) Ketoconazole, Miconazole, Itraconazole Diffusion cells [98]N-acetylcysteine (5%) Itraconazole Nail immersed in drug solution [99]
DOI: 10.3109/1061186X.2014.929138 Drug delivery across the nail plate barrier 779

Reducing agents that cleaves the nail disulfide bond
Thiols
Thiols, compounds containing sulfhydryl groups (-SH), are
the agents that reduce the disulfide linkage in the keratin
matrix of the nail [89], as exhibited below:
Nail�S�S�Nailþ2R�SH$ 2Nail�SHþR�S�S�R
Where, R–SH represents a thiol. The thiols which have been
used as transungual penetration enhancers include N-
acetylcysteine, mercaptoethanol, N-(2-mercaptopropionyl)
glycine (MPG), pyrithone and thioglycolic acid (TGA) [89].
Once cleaved, disulfide bonds are unlikely to be reformed in
the dead nail plate. Thus, nail plates may be pretreated with
the enhancer prior to drug application (rather than being used
in drug formulation). Pretreatment with the enhancer would
resolve drug-enhancer compatibility problems, if any, and
enable higher drug and enhancer concentrations to be
employed.
Hoogdalem et al. evaluated the penetration-enhancing
properties of N-acetylcysteine in vivo and revealed an
enhanced retention of antifungal agent oxiconazole in upper
nail layers [5]. Kobayashi et al. demonstrated that
N-acetylcysteine and 2-mercaptoethanol enhanced the per-
meability of antifungal drug tolnaftate in upper layers of nail
clippings, attributed to swelling and softening of nail plate
[90]. TGA is known to increase the transungual drug flux and
reduce the lag time of compounds with varied polarity.
TGA-mediated redox reaction involving nail disulfide linkage
overcome the barrier integrity of the nail, facilitating the drug
flux [91].
Sulfites
Incubation of proteins and peptides containing disulfide bond
with sodium sulfite is known to cleave disulfide bond to
produce thiols and thiosulfates, as depicted in following
reaction:
R� S� S� Rþ Na2SO3 ! R� S� Hþ R� S� SO3H
Thus, it was hypothesized that incubation of nail plates
with sodium sulfite could reduce the nail plate’s barrier
properties and enhance ungual drug flux [2]. Certainly, the
penetration of 5,6-carboxyfluoresceine (as a model drug)
through nail clippings from a healthy volunteer was found
to be significantly enhanced in the presence of sodium
sulfite [92]. It was found to enhance the transungual
permeation on pretreatment and on co-application as well.
Oxidizing agent that cleaves the nail disulfide bond
Much less attention has been given on the use of oxidizing
agents for cleavage of nail disulfide bonds and to enhance
transungual drug permeability. Hydrogen peroxide has been
used alone or in combination with urea, as urea hydrogen
peroxide (UHP), to enhance transungual drug flux.
Pretreatment of nails with hydrogen peroxide (35% wt in
water) alone for 20 h increased mannitol permeation �3-fold
following a 120 h permeant application [93]. MedNail�
technology consists of pretreatment of nails with reducing
agent TGA, followed by oxidizing agent UHP.
Nail pretreatment with MedNail increased ungual drug flux
of terbinafine �18-fold, with concomitant increased fungal
eradication by Penlac and Loceryl [94].
Water
The pivotal role of water as a transungual permeation
enhancer for alkanols is well documented in the literature
[55]. Nail hydration and swelling, on contact with water, have
been thought to be a probable mechanism for the higher drug
flux from aqueous vehicle. The permeability coefficient of
C2-C10 n-alkanols (but not methanol) from a saline solution
through the nail was �5 times greater than from neat alcohols
[50]. The role of water in the donor medium was confirmed
when its replacement with an organic solvent (isopropanol or
DMSO) reduced the permeability of hexanol (but not
methanol) in a concentration-dependent manner [55].
Kobayashi et al. revealed higher drug flux of the hydro-
philic 5-FU from aqueous drug formulation (compared
with lipophilic) drug-saturated formulations containing
N-acetylcysteine and mercaptoethanol [90]. Gunt and
Kasting reported that increasing ambient RH from 15% to
100% enhanced permeation of [3H]-ketoconazole by �3-folds
in vitro, as studied on excised human nail plates and the
diffusivity of water increased by more than 400-folds. This is
attributed to increase in nail plate hydration by nail incubation
in environments of increasing RH [85,95]. An increase in
ungual flux of hydrophilic drugs from aqueous vehicles is
associated with an increase in nail weight. The flux of
hydrophilic drugs was found to be higher from aqueous
vehicle compared to their lipophilic counterparts.
However, increased nail swelling and enhanced drug flux
do not always occur together, as in case of resorcinol [93] and
urea [89], which caused nail swelling but failed to signifi-
cantly enhance the flux of mannitol. On the contrary,
enhanced flux of tolnaftate has not been associated with
nail swelling owing to the lipophilic nature of the vehicle
used [90]. Therefore, nail hydration and swelling by a
formulation cannot always be considered as an indication
for the enhanced transungual drug permeation.
Keratinolytic enzymes
Keratinolytic enzymes are known to hydrolyze the keratin
matrix of nail plate, thereby altering its barrier properties and
subsequently enhancing the transungual permeation [96].
Mohorcic et al. conducted permeation studies using modified
Franz diffusion cells and found keratinase to markedly
enhance the permeation (more than double) of metformin
HCl (model drug) through bovine hoof membranes (model
nail plate). Indeed, the keratinase intensely affected the
surface of human nail clippings (on incubation for 48 h),
acting on the intercellular cement that holds the nail
corneocytes together. This resulted in the separation of
corneocytes on the dorsal surface of the nail and ‘‘lifted
off’’ the nail plate (Figure 7A). The surface of the corneocytes
was corroded as well, as revealed by scanning electron
microscopy (SEM) (Figure 7B), suggesting enzyme action on
the interfilamentous matrix [97].
Papain, an endopeptidase that contains a highly reactive
sulfhydryl group, has also shown some promising action as a
780 M. V. Saner et al. J Drug Target, 2014; 22(9): 769–789

transungual penetration enhancer [98]. Incubation of nail in
papain solution (15% w/v) for 1 d, followed by soaking
salicylic acid solution (20% w/v) for 10 d enabled the
permeation of antifungals, miconazole, ketoconazole and
itraconazole. The aggressive pretreatment regime fractured
the nail surface and possibly created pathways (pores) for
ungual drug penetration, as revealed by SEM analysis.
Keratolytic enhancers
The Guirrero et al. demonstrated the influence of keratolytic
agents (papain, urea and salicylic acid) on the permeability of
three imidazole antifungals (miconazole, ketoconazole and
itraconazole). In the absence of keratolytic agents, no
transungual antifungal permeation was detected over a
period of 60 d [98]. Urea and salicylic acid are known to
soften and hydrate the nail plate [90]. The swelling and
hydration of nail plate would enhance the drug permeation as
a consequence of the formation of a less dense structure with
large pores. Keratolytic agents were found to damage and
fracture the nail plate surface [98]. The drug load in nail was
found to increase on incubation with drug solution containing
urea, but failed to enhance ungual drug flux when used alone
in many cases. In fact, it has been found to reduce the ungual
flux of 5-FU. This is due to an alteration in pH of the solution
(from pH 4.7 to 7.2) upon inclusion of urea, which resulted in
ionization of the acidic 5-FU (pKa¼ 8.0, 13.0) into negatively
charged species and repulsion between the like-charged drug
and the nail (which also carries a negative charge above pH
5.0 due to its pKa of �5) [90].
Urea has a synergistic effect on ungual drug flux when
used in combination with other penetration enhancers [89].
Sun et al. reported that itraconazole concentration in nail
plates in the presence of both N-acetylcysteine and urea
was 94 times higher than that of the control (no enhancer),
compared to 20 times in the presence of urea only and
49 times in the presence of N-acetylcysteine only [99].
Interestingly, the beneficial effect of combining urea with
proven transungual enhancers was observed even when urea
did not enhance the ungual drug permeation alone; transun-
gual flux of water being enhanced by 3.5-fold in the presence
of urea and MPG, compared with an increase of 2.5-fold in
the presence of MPG only [89].
Urea is a keratolytic agent that acts by unfolding,
solubilizing and denaturing the nail keratin. The process of
keratin unfolding by urea (probably via interaction with their
hydrogen bonds) would facilitate the cleavage of disulfide
bonds. The dismantling of disulfide bonds promote the
disruption of the nail plate barrier and subsequently enhance
the ungual drug permeation. Thus, urea has been included in
nail lacquers [100]. Urea has been employed at high
concentrations (40%) to chemically avulse the diseased nail
plates [47,101].
2-n-nonyl-1,3-dioxolane (SEPA�)
2-n-nonyl-1,3-dioxolane (a skin penetration enhancer) is as
well known as SEPA (Soft enhancement of percutaneous
absorption), which has proven to be efficient in increasing
transdermal drug delivery [101–103]. Hui et al. examined the
delivery of econazole across human nail from a lacquer
formulation (EcoNail�) with a penetration enhancer,
2-n-nonyl-1,3-dioxolane. Findings of Hui et al. suggested
that the addition of 2-n-nonyl-1,3-dioxolane (18%) to
econazole nail lacquer (test group) delivered six times more
drug through human nail than an identical lacquer formulation
without enhancer (control group). Concentrations of econa-
zole in the deep nail layer and nail bed were significantly
higher in the ‘‘test group’’ than in ’’control group’’.
Moreover, the concentration of econazole in the deep nail
layer in the test group was 14 000 times higher than the MIC
necessary to inhibit the fungal growth [4].
Miscellaneous enhancers
N-methyl-2-pyrrolidone, polypropylene glycol 400, DMSO,
Labrasol, mercaptoethanol, Transcutol are found to increase
the ungual drug permeation through the bovine hoof mem-
brane. Inorganic salts such as sodium metabisulphite, sodium
citrate, potassium phosphate and ammonium carbonate were
found to increase the drug load as well as the drug uptake rate
of terbinafine HCl. Additionally, sodium dodecyl sulfate and
Figure 7. SEM photomicrographs showing influence of keratinase solution on nail plate. (A) Nail corneocytes ‘‘lift off’’ the nail plate, owing toenzyme action on the intercellular cement after incubation of nail clippings in a keratinase solution. (B) Keratinase seems to ‘‘corrode’’ the surface ofindividual corneocytes, possibly due to the action of keratinase on the interfilamentous matrix. Reprinted from [97], with kind permission of thecopyright holder, Elsevier, Amsterdam.
DOI: 10.3109/1061186X.2014.929138 Drug delivery across the nail plate barrier 781

polyethylene glycols were identified as potential transungual
enhancers. Sodium phosphate was found to be the most
effective inorganic salt to enhance the transungual permeation
of terbinafine HCl, due to increased hydration of the nail plate
and higher thermodynamic activity of the drug in the presence
of inorganic salt [104].
Murthy and co-workers [105] assessed the influence of
polyethylene glycols (PEGs) on the in vitro transungual
permeation of terbinafine by passive and iontophoretic
processes using gel formulations containing different molecu-
lar weight PEGs (30% w/w). Passive delivery using low
molecular weight (LMW) PEGs (200 and 400 MW) indicated
moderate enhancement of drug permeation and drug load in
the nail plate whereas iontophoresis delivery significantly
enhanced the drug permeation and drug load into the nail
plate. Little or no effect on drug permeation and was observed
with high molecular weight PEGs (1000–3350 MW) in
passive or iontophoretic processes. This study concluded
that the enhancement in drug permeation by LMW PEGs is
likely due to their ability to lead to greater water uptake and
swelling of nail and LMW PEGs are indeed a promising
transungual permeation enhancer.
TranScreen-N�: Method for rapid screening oftransungual penetration enhancers
Topical monotherapy of nail diseases (onychomycosis and
nail psoriasis) has been abandoned due to poor permeability
of the human nail plate to topical therapeutics. Chemical
enhancers are likely to improve the drug delivery across
the nail plate. Selecting the most effective chemical
enhancer for the given drug and formulation is highly
crucial in determining the efficacy of topical therapy of nail
diseases [106].
Nail swelling alone cannot always be considered as an index
for the increased transungual permeation since, many transun-
gual penetration enhancers are not likely to promote the
swelling of the nail plate. Besides, most of the screening
methods cannot be used to predict the extent of permeation
from lipophilic systems, which may fail to hydrate or swell the
nail plate. Screening the big pool of enhancers using currently
followed diffusion cell experiments would be tedious and
expensive. In this context, TranScreen-N was devised as a high
throughput method of screening transungual penetration
enhancers. It is a rapid microwell plate-based technique
which involves two different procedures; the simultaneous
exposure treatment and sequential exposure treatment [107].
Murthy and co-workers (2009c) screened several chemical
enhancers using TranScreen-N employing diffusion studies
using Franz diffusion cell. In TranScreen-N technique, the
enhancers can be categorized according to whether they need
to be applied before or concomitantly with drugs (or by either
procedure) to enhance the transungual drug delivery.
TranScreen-N technique can significantly reduce the cost
and duration required to screen transungual drug delivery
enhancers. The treatment procedures adopted by Murthy and
co-workers for screening of chemical enhancers is presented
in Figure 8 [106].
Vaka et al. [108] studied the effect of pretreatment using
five different chemical etchants on the delivery of TH and
5-FU into and across the human cadaver fingernail plates
using TranScreen-N technique. The dorsal surface of nail
plate was pretreated with these chemical etchants in gel
formulation for a period of 60 s and evaluated for drug load
and in vitro permeation. Of the five chemical etchants – lactic
acid (LA), tartaric acid (TTA), glycolic acid (GA), citric acid
(CA) and phosphoric acid (PA) – evaluated, PA was identified
as the most potent transungual etchant while LA did not
demonstrated any etching properties. Optical microscopy and
AFM revealed that the PA enhanced the transungual drug
delivery by decreasing the keratin density of the dorsal layer
of the nail plate and by microstructural alterations. The study
demonstrated that pretreatment of the nail plate with PA
(1% or 10% w/w) for short duration could be a potential
method of improving the efficiency of topical monotherapy in
treatment of nail disorders.
In vitro models to study transungual drug permeation
Nail is considered to be a stringent barrier to the permeation
of topical therapeutics owing to its thickness, chemical
composition, and relatively compact nature. In spite of this,
good number of experiments exhibit permeability of drugs
through the keratinized nail plate. Several models have been
developed and evaluated to predict the permeation of drug
through and across the human nail plate, some of which are
conferred below:
Animal hoof membranes
Animal hooves and human nail plate are reported to possess
analogous properties in regard to the content of keratin and
the release of soluble protein on incubation with keratinase,
and thus offer an alternative to human nails in permeation
studies [109]. Therefore, bovine [110], porcine [111] and
horse [93] hooves have been used by many researchers as
in vitro models to assess the nail permeability of topical
therapeutics.
Khengar et al. compared the swelling behavior of human
nail and horse’s hooves as a consequence of solvent uptake in
presence of penetration enhancers. When immersed in control
solution, an increase in weight by hooves was 40 ± 9%
compared to 27 ± 3% weight increase by human nails. Results
of Khengar suggested that the mammalian hoof is capable of
taking up and retaining more water than human nail, as
animal hoof keratin is thought to be less dense than human
nail plate (provides support to the findings of Mertin &
Lippold, 1997a) [48,93].
Animal hoof is more permeable than the human nail plate.
Hoof proteins have a significantly less disulfide linkage
compared to human nail plate [21]. As a result, the hoof may
be less susceptible to transungual permeation enhancers that
cleaves disulfide linkages. In such cases, enhancement of
perungual absorption in the hoof may be less than the
enhancement that could be achieved in human nail plate.
These findings may indicate that animal hooves do not
necessarily provide a representative model in which diffusion
through the nail can be evaluated.
Predominantly, hydrophilic gel membrane property of
human nail plate is similar to that of bovine hoof membrane,
which indeed made bovine hoof membrane a more suit-
able in vitro model for transungual permeation studies. Mertin
and Lippold (1997a) evaluated the in vitro permeability of
782 M. V. Saner et al. J Drug Target, 2014; 22(9): 769–789

several antifungals through bovine hoof membranes using
diffusion cell. The relationship between permeability coeffi-
cients through human nail plate for the screened antifungals
was predicted and reported (r¼ 0.971) on the basis of their
permeation rates through the hoof membranes and their water
solubilities using the following equation:
log PN ¼ 3:723þ 1:751 log PH
where PN is the nail plate permeability coefficient and PH is
the permeability coefficient through the bovine hoof mem-
brane obtained experimentally [48].
Nail clippings
Nail clippings from fingers and toe nails of healthy human
volunteers are widely used as in vitro models to evaluate the
transungual formulations. Nail clippings can be hydrated by
soaking in water or other media prior to experimentations.
Permeation studies are carried out by mounting the hydrated
nail clippings on a nail adaptor, which is then sandwiched
between the donor and receiver compartments of diffusion
cell. Kobayashi et al. have established a relationship between
physicochemical properties and permeability of several
therapeutics across nail clippings [49]. Physical penetration
enhancement techniques such as iontophoresis were also
studied by several researchers using nail clippings as a
permeation barrier [58,69,112]. However, nail clipping is
short of the nail bed, so it might not be the best in vitro model
for ungual permeation studies.
Cadaver nail plates
A human finger and toe nail plates are, not surprisingly the
model considered to simulate, very closely, the in vivo
conditions. Hence, cadaver nail plate samples were used very
frequently to evaluate several topical antifungal formulations
containing transungual enhancers [89]. Physical enhancement
techniques were also being investigated using human cadaver
nail plates [11].
Murthy et al. (2009b) have revealed an improvement in the
permeation of terbinafine HCl when sodium sulfite and other
inorganic salts were used as penetration enhancers. Permeation
studies were performed across human cadaver nail plates
mounted on the nail adapter in the vertical Franz diffusion cell.
They observed that permeation was enhanced by�3–5-folds in
the presence of salts [104].
Figure 8. Schematic representation of sequence of procedures in TranScreen-N. It is micro-well plate-based technique of screening transungualpermeation enhancers. This involved ‘‘simultaneous exposure’’ and ‘‘sequential exposure’’ procedures run in parallel for screening of chemicalenhancers. Reprinted from [106] after slight modifications, with kind permission of copyright holder, John Willey and Sons Ltd., Hoboken, NJ.
DOI: 10.3109/1061186X.2014.929138 Drug delivery across the nail plate barrier 783

Recently, Vejnovic et al. performed the permeation studies
across human cadaver nail plates using specially designed
modified Franz diffusion cell. Hydrophobins were used as
permeation enhancers and caffeine was employed as model
permeant. The permeability coefficient of caffeine was found
to increase by �3.6-folds in the presence of salts [113].
Hao and Li (2008a) studied the passive and the
iontophoretic transport of model permeants such as mannitol,
urea and tetraethylammonium ion across fully hydrated,
excised human cadaver nail plates with respect to location
(fingernail or toenail) and concluded that there is large
individual variability in nail permeation [59].
Nair et al. [114] evaluated the effect of iontophoresis on
the transungual delivery of TH using two ex vivo models viz.
nail on agarose model with human cadaver toe nails and a
surrounding ‘‘skin-like’’ barrier membrane and separately
with intact cadaver toe model. The drug was loaded into two
different applicator (nail-only and nail-and-skin applicator).
In the nail on agarose model, the amount of TH permeated
through the nail or nail and skin increased linearly with an
increase in the electrical dose for both the applicators, with
higher permeation observed using the nail-and-skin applicator
because of the increased skin delivery. The study concluded
that the iontophoresis improved TH permeation through and
load into the nail, and achieved levels above the MIC of TH
for dermatophytes. This may offer a novel treatment option
for onychomycosis.
Intact toes
Murthy et al. (2009a) have used excised toe as a model for
in vivo transungual permeation studies [11]. However, the
drug clearance from the nail bed and the nail matrix is lacking
in this model. Nonetheless, the cadaver toes simulate the
in vivo in many aspects and is one of the most appropriate
model for transungual drug delivery experimentations [28].
Opto-thermal transient emission radiometry(OTTER): Tool for estimation of solvent diffusioninto nails in vivo
Xiao et al. first described an infrared remote sensing
technique, Opto-Thermal Transient Emission Radiometry
(OTTER), to probe the extent to which solvents permeate
through the human nail plate in vivo. They examined the
efficiency of OTTER using decanol, glycerol and butyl
acetate as model solvents. Preliminary experiments have been
conducted on human volunteers using OTTER to examine the
uptake of the solvents that could potentially be used to deliver
active ingredients across the nail plate. Their findings
demonstrated the potential of OTTER as a tool to investigate
and optimize excipients to target drugs to the human nail
tissues in vivo [115].
Drug formulations studied across nail plate
A plenty of literature supports the investigational studies
being undertaken by scientists working particularly on
transungual drug delivery systems. The prime objective
might be the treatment of major onychopathies, in particular,
onychomycosis and nail psoriasis. Table 4 highlights a current
outlook on the role of various pilot molecules loaded in a
variety of topical formulations applied across the nail plate as
investigated in different research laboratories around the
globe.
Key commercial products available on market fornail disorders
A wide range of formulations has been developed for ungual
and transungual applications. In Table 5, authors have tried to
present a comprehensive coverage of all key commercial
products available on market for addressing the treatment of
nail disorders. Promising success to the development of
topical nail formulations and a good response to such
products in the pharmaceutical market enrolled these on the
list of pharmaceutical industries which have been looking for
further development to bring better therapeutic outcomes in
topical therapies.
Patents pertaining to transungual drug delivery
Despite the fact that many of them have not reached the
pharmaceutical market so far, a good number of patents have
been received on transungual drug delivery. Due to the
challenge of poor permeation across nail plate, only few
patents have been transferred into commercial marketed
products. However, there are some patents on the methods
Table 4. Drug formulations studied across nail plate as investigated indifferent research laboratories (Modified after [28]).
Pilot molecule Formulation/s Ref
Tioconazole Topical nail solution [3]Econazole Nail lacquer [4]Oxiconazole Nail lacquer [5]Ketoconazole Gel [6]Ketoconazole Films [6,7]Sertaconazole Nail patch [8]Miconazole Powder [9]Terbinafine Combination of oral &
topical solution[10]
Terbinafine Aqueous solution [11]Terbinafine HCl Topical gel [11]Terbinafine HCl Bilayered nail lacquer [12]Ciclopirox Topical gel [13]Chloramphenicol Nail lacquer [48]5-aminolevulinic acid Nail patch [88]Clobetasol-17-ropionate Nail lacquer [101]Caffeine Solution [113]Tioconazole & Griseofulvin Topical nail solution [116]Dimethyl sulfoxide Topical nail solution [117]Panthenol Non-lacquer film &
nail solution[118]
Glutaraldehyde Topical nail solution [119]Amorolfine/Ciclopirox Nail lacquer [120–123]Naftifine HCl Gel [124]Clotrimoxazole Cream [124]Ketoconazole/Ciclopirox Cream [125]Juglans regia
(Walnut hulls extract)Cream [126]
Voriconazole Nail lacquer [127]Keratin Thick film [128]Ketoconazole Nail lacquer [129]Triamcinolone &
Ciclopirox olamineAqueous nail lacquer [130]
Terbinafine HCl Liposome gel,Ethosome gel
[131]
Geraniol & Nerol Gel [132]
784 M. V. Saner et al. J Drug Target, 2014; 22(9): 769–789

and devices employed to enhance the transungual permeabil-
ity and they would, no doubt, handover new formulations, in
the near future with major nail ailments at their crux. Selected
patents related to transungual drug delivery systems are
briefly outlined in Table 6.
Clinical status of transungual drug delivery
Substantial advancement has been built in this expanse of
research at the clinical level and some topical formulations
have been approved by FDA for clinical purpose. Table 7 lists
the transungually applied therapeutics that are either clinically
approved or in advanced phases of clinical trials [149].
Concluding remarks and future directions
Transungual drug delivery is indeed a reality, but its
therapeutic value is still under question. The permeability of
the dense, highly keratinized nail plate to topical therapeutics is
quite poor as such. This demonstrates poor delivery of
permeant molecules into the nail bed, which is believed to be
a primary site for many onychopathies (more often onycho-
mycosis and nail psoriasis). The permeant molecule must have
low molecular weight and remain undissociated in order to
permeate through the nail plate. However, there have been
contradictory findings and conflicting reports in the literature
about the influence of other variables relevant to permeant
(size, surface charge and hydrophilicity/hydrophobicity) and
formulation (nature and pH of the vehicle) on the transungual
drug permeation. This may be due to inadequate exploration of
factors affecting, and mechanisms involved in transungual
permeation. Under these circumstances, nail plate permeabil-
ity is modulated by an array of permeation enhancement
techniques that overcome the relatively impermeable nail plate
barrier and improve the therapeutic potential of topical cargos.
Table 5. Key commercial products available on market for transungual drug delivery.
Pilot molecule Formulation Brand name Manufacturer
Ciclopiroxamine (8%) Topical solution Onylac Cipla (Mumbai, India)Ciclopiroxamine (8%) Topical solution; Nail lacquer Penlac� Dermik Laboratories (Mississauga, Canada)Ciclopirox Nail lacquer Loprox� Aventis Pharma. Ltd. (Mumbai, India)Ciclopirox Gel (0.77%), Cream (0.77%), Solution (8%),
Topical suspension (0.77%)Loprox� Medicis Pharmaceutical Corp. (Scottsdale, AZ)
Ciclopirox Cream (1%) Loprox� Sanofi-Aventis (Paris, France)Ciclopirox olamine Cream (0.77%) Fougera� Fougera Pharmaceutical Inc. (Melville, NY)Ciclopirox Topical solution (8%) Rejuvenail� Menarini (Florence, Australia)Ciclopirox (8%) Nail lacquer Ciclopoli� Polichem SA (Pazzallo, Switzerland)Amorolfine (5%) Nail lacquer Loceryl� Roche Laboratories (Basel, Australia)Amorolfine (5%) Nail lacquer Curanil� Galderma (Lausanne, Switzerland)Econazole (5%) Nail lacquer EcoNail� Macrochem Corp. (Lexington, MA)Urea (40%) Nail film Umecta� Jsj Pharmaceuticals (Charleston, SC)Sertaconazole nitrate Nail patch Zalain� Labtec GmbH (Langenfeld, Germany)Sertaconazole nitrate (2%) Cream Ertaczo� OrthoNeutorgena (Los Angeles, CA)Tazarotene (0.1%) Gel Tazorac� Allergan Inc. (Irvine, CA)Tazarotene (0.05% & 0.1%) Topical gel Zorac� Allergan Inc. (Irvine, CA)Tazarotene Cream Avage� Allergan Inc. (Irvine, CA)Ticonazole Topical solution Trosyl� Pfizer Ltd. (Tadworth, UK)Salicylic acid Nail paint Phytex� Pharmax Healthcare Ltd. (Bexley, UK)Methyl undecenoate Nail paint Monphytol� LAB (UK)
Table 6. Patents pertaining to ungual and transungual drug delivery systems.
Drug Therapeutic application Drug delivery system Patent no. Ref
Griseofulvin Onychomycosis Nail lacquer US 005487776 A (1996) [133]Ciclopirox olamine Onychomycosis Topical solution US 005840283 A (1998) [134]Butenafine HCl Onychomycosis Gel US 006143794 A (2000) [135]Fluconazole NS Nail lacquer, Solution US 006585963 B1 (2003) [136]Antifungal topical agents Onychomycosis Topical gel & cream US 006846837 B2 (2005) [137]Antimycotic agents Onychoschizia Nail lacquer US 0134039 A1 (2006) [138]Benzalkonium chloride NS Lotion, ointment, nail polish US 7198794 B1 (2007) [139]Clotrimazole, Amorolfine, Terbinafine NS Topical solution & Cream US 0166249 A1 (2007) [140]Terbinafine HCl Onychomycosis Dual action nail coat US 7462362 B2 (2008) [141]Antifungal agents Onychomicosis Solution, Solid/semisolid implants,
Microparticles & crystalsUS 0132442 A1 (2008) [142]
Terbinafine HCl, Fluconazole Onychomicosis Gel (Iontophoresis) US 0319371 A1 (2008) [143]Terbinafine Nail psoriasis Hydrogel US 0175945 A1 (2009) [144]Antifungal agents Onychomicosis NS US 0215888 A1 (2009) [145]Terbinafine Onychomicosis NS US 7820720 B2 (2010) [146]Hydrogen peroxide Onychomicosis Gel US 0098645 A1 (2010) [1]Terbinafine HCl, Clotrimazole Onychomicosis Cream US 0083692 A1 (2011) [147]Antifungal agents Onychomicosis,
Nail psoriasisThermogel US 0010227 A1 (2012) [148]
NS, not specified.
DOI: 10.3109/1061186X.2014.929138 Drug delivery across the nail plate barrier 785
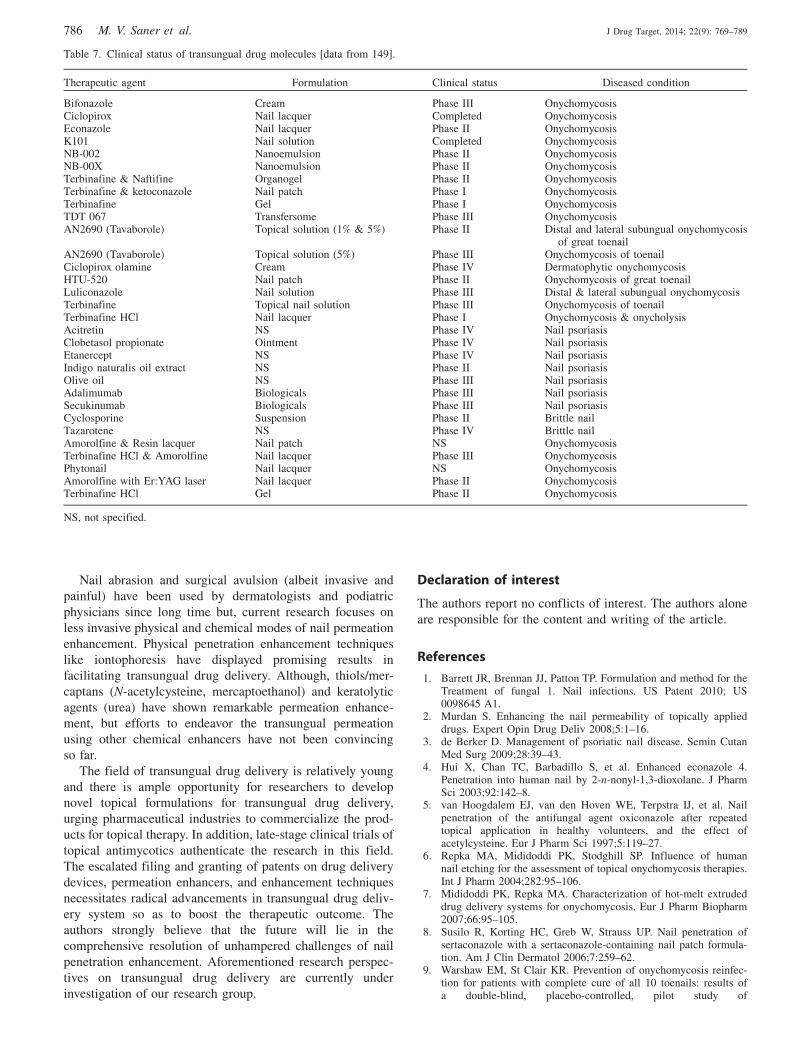
Nail abrasion and surgical avulsion (albeit invasive and
painful) have been used by dermatologists and podiatric
physicians since long time but, current research focuses on
less invasive physical and chemical modes of nail permeation
enhancement. Physical penetration enhancement techniques
like iontophoresis have displayed promising results in
facilitating transungual drug delivery. Although, thiols/mer-
captans (N-acetylcysteine, mercaptoethanol) and keratolytic
agents (urea) have shown remarkable permeation enhance-
ment, but efforts to endeavor the transungual permeation
using other chemical enhancers have not been convincing
so far.
The field of transungual drug delivery is relatively young
and there is ample opportunity for researchers to develop
novel topical formulations for transungual drug delivery,
urging pharmaceutical industries to commercialize the prod-
ucts for topical therapy. In addition, late-stage clinical trials of
topical antimycotics authenticate the research in this field.
The escalated filing and granting of patents on drug delivery
devices, permeation enhancers, and enhancement techniques
necessitates radical advancements in transungual drug deliv-
ery system so as to boost the therapeutic outcome. The
authors strongly believe that the future will lie in the
comprehensive resolution of unhampered challenges of nail
penetration enhancement. Aforementioned research perspec-
tives on transungual drug delivery are currently under
investigation of our research group.
Declaration of interest
The authors report no conflicts of interest. The authors alone
are responsible for the content and writing of the article.
References
1. Barrett JR, Brennan JJ, Patton TP. Formulation and method for theTreatment of fungal 1. Nail infections. US Patent 2010; US0098645 A1.
2. Murdan S. Enhancing the nail permeability of topically applieddrugs. Expert Opin Drug Deliv 2008;5:1–16.
3. de Berker D. Management of psoriatic nail disease. Semin CutanMed Surg 2009;28:39–43.
4. Hui X, Chan TC, Barbadillo S, et al. Enhanced econazole 4.Penetration into human nail by 2-n-nonyl-1,3-dioxolane. J PharmSci 2003;92:142–8.
5. van Hoogdalem EJ, van den Hoven WE, Terpstra IJ, et al. Nailpenetration of the antifungal agent oxiconazole after repeatedtopical application in healthy volunteers, and the effect ofacetylcysteine. Eur J Pharm Sci 1997;5:119–27.
6. Repka MA, Mididoddi PK, Stodghill SP. Influence of humannail etching for the assessment of topical onychomycosis therapies.Int J Pharm 2004;282:95–106.
7. Mididoddi PK, Repka MA. Characterization of hot-melt extrudeddrug delivery systems for onychomycosis. Eur J Pharm Biopharm2007;66:95–105.
8. Susilo R, Korting HC, Greb W, Strauss UP. Nail penetration ofsertaconazole with a sertaconazole-containing nail patch formula-tion. Am J Clin Dermatol 2006;7:259–62.
9. Warshaw EM, St Clair KR. Prevention of onychomycosis reinfec-tion for patients with complete cure of all 10 toenails: results ofa double-blind, placebo-controlled, pilot study of
Table 7. Clinical status of transungual drug molecules [data from 149].
Therapeutic agent Formulation Clinical status Diseased condition
Bifonazole Cream Phase III OnychomycosisCiclopirox Nail lacquer Completed OnychomycosisEconazole Nail lacquer Phase II OnychomycosisK101 Nail solution Completed OnychomycosisNB-002 Nanoemulsion Phase II OnychomycosisNB-00X Nanoemulsion Phase II OnychomycosisTerbinafine & Naftifine Organogel Phase II OnychomycosisTerbinafine & ketoconazole Nail patch Phase I OnychomycosisTerbinafine Gel Phase I OnychomycosisTDT 067 Transfersome Phase III OnychomycosisAN2690 (Tavaborole) Topical solution (1% & 5%) Phase II Distal and lateral subungual onychomycosis
of great toenailAN2690 (Tavaborole) Topical solution (5%) Phase III Onychomycosis of toenailCiclopirox olamine Cream Phase IV Dermatophytic onychomycosisHTU-520 Nail patch Phase II Onychomycosis of great toenailLuliconazole Nail solution Phase III Distal & lateral subungual onychomycosisTerbinafine Topical nail solution Phase III Onychomycosis of toenailTerbinafine HCl Nail lacquer Phase I Onychomycosis & onycholysisAcitretin NS Phase IV Nail psoriasisClobetasol propionate Ointment Phase IV Nail psoriasisEtanercept NS Phase IV Nail psoriasisIndigo naturalis oil extract NS Phase II Nail psoriasisOlive oil NS Phase III Nail psoriasisAdalimumab Biologicals Phase III Nail psoriasisSecukinumab Biologicals Phase III Nail psoriasisCyclosporine Suspension Phase II Brittle nailTazarotene NS Phase IV Brittle nailAmorolfine & Resin lacquer Nail patch NS OnychomycosisTerbinafine HCl & Amorolfine Nail lacquer Phase III OnychomycosisPhytonail Nail lacquer NS OnychomycosisAmorolfine with Er:YAG laser Nail lacquer Phase II OnychomycosisTerbinafine HCl Gel Phase II Onychomycosis
NS, not specified.
786 M. V. Saner et al. J Drug Target, 2014; 22(9): 769–789

prophylactic miconazole powder 2%. J Am Acad Dermatol 2005;53:717–20.
10. Avner S, Nir N, Henri T. Combination of oral terbinafine andtopical ciclopirox compared to oral terbinafine for the treatment ofonychomycosis. J Dermatolog Treat 2005;16:327–30.
11. Nair AB, Kim HD, Davis SP, et al. An ex vivo toe model used toassess applicators for the iontophoretic ungual delivery of terbina-fine. Pharm Res 2009;26:2194–201.
12. Shivakumar HN, Vaka SRK, Madhav NV, et al. Bilayered naillacquer of terbinafine hydrochloride for treatment of onychomy-cosis. J Pharm Sci 2010;99:4267–76.
13. Hui X, Wester RC, Barbadillo S, et al. Ciclopirox delivery into thehuman nail plate. J Pharm Sci 2004;93:2545–8.
14. Murdan S. Drug delivery to the nail following topical application.Int J Pharm 2002;236:1–26.
15. Achten G, Andre J, Laporte M. Nails in light and electronmicroscopy. Semin Dermatol 1991;10:54–64.
16. Jiaravuthisan MM, Sasseville D, Vender RB, et al. Psoriasis of thenail: anatomy, pathology, clinical presentation, and a review of theliterature on therapy. J Am Acad Dermatol 2007;57:1–27.
17. Kobayashi Y, Miyamoto M, Sugibayashi K, Morimoto Y. Drugpermeation through the three layers of the human nail plate.J Pharm Pharmacol 1999;51:271–8.
18. Lynch MH, O’Guin WM, Hardy C, et al. Acidic and basic hair/nail(‘‘hard’’) keratins: their colocalization in upper cortical and cuticlecells of the human hair follicle and their relationship to ‘‘soft’’keratins. J Cell Biol 1986;103:2593–606.
19. Garson JC, Baltenneck F, Leroy F, Riekel C, Muller M.Histological structure of human nail as studied by synchrotronX-ray microdiffraction. Cell Mol Biol 2000;46:1025–34.
20. Fleckman P. Basic science of the nail unit. In: Scher RK, Daniel IIICR, eds. Nails: therapy, diagnosis, surgery, 2nd ed. Philadelphia(PA): WB Saunders; 1997.
21. Baden HP, Goldsmith LA, Fleming B. A comparative study of thephysicochemical properties of human keratinized tissues. BiochimBiophys Acta 1973;322:269–78.
22. Forslind B. Biophysical studies of the normal nail. Acta DermVenereol 1970;50:161–8.
23. Gniadecka M, Nielsen OF, Christensen DH, Wulf HC. Structure ofwater, proteins, and lipids in intact human skin, hair and nail.J Invest Dermatol 1998;110:393–8.
24. Walters KA, Flynn GL. Permeability characteristics of the humannail plate. Int J Cosmet Sci 1983;5:231–46.
25. Zaias N. The nail in health and disease, 2nd ed. New York (NY):Spectrum publications Inc.; 1989.
26. Baran R, de Berker DAR, Holzberg M, Thomas L. Baran andDawber’s diseases of the nail and their management, 4th ed.Chichester, UK: Wiley-Blackwell, John Wiley and Son’s, Ltd;2012.
27. Achten G, Parent D. The normal and pathologic nail. Int J Dermatol1983;22:556–65.
28. Shivakumar HN, Juluri A, Desai BG, Murthy SN. Ungualand Transungual drug delivery. Drug Dev Ind Pharm 2012;38:901–11.
29. Alam G, Singh MP, Singh A, et al. Transungual drug transport:advancement and challenges. J Pharm Res 2012;5:2574–9.
30. Nail Diseases and Disorders. Available from: www.hooked-on-nails.com/naildisorders.html [last accessed 25 Dec 2013].
31. Ghannoum MA, Hajjeh RA, Scher R, et al. A large-scale NorthAmerican study of fungal isolates from nails: the frequency ofonychomycosis, fungal distribution, and antifungal susceptibilitypatterns. J Am Acad Dermatol 2000;43:641–8.
32. Kaur R, Kashyap B, Bhalla P. Onychomycosis-epidemiology,diagnosis and management. Ind J Med Micobiol 2008;26:108–16.
33. de Berker D. Nails and hairs. Medicine 2009;37:286–90.34. Midgley G, Moore MK, Cook JC, Phan QG. Mycology of nail
disorders. J Am Acad Dermatol 1994;31:S68–74.35. Sigurgeirsson B, Steingrimsson O. Risk factors associated with
onychomycosis. J Eur Acad Dermatol Venereol 2004;18:48–51.36. Cohen PR, Scher RK. Topical and surgical treatment of
onychomycosis. J Am Acad Dermatol 1994;31:S74–7.37. Daniel III CR. The diagnosis of nail fungal infection. Arch
Dermatol 1991;127:1566–7.38. Gupta AK, Shear NH. Onychomycosis. Going for cure. Can Fam
Physician 1997;43:299–305.
39. Scher RK. Onychomycosis: a significant medical disorder. J AmAcad Dermatol 1996;35:S2–5.
40. Elewski BE, Charif MA, Daniel III CR. Onychomycosis. In: ScherRK, Daniel CR, eds. Nails: therapy, diagnosis, surgery, 3rd ed.Philadelphia (PA): WB Saunders; 2010.
41. Niewerth M, Korting HC. Management of onychomycoses. Drugs1999;58:283–96.
42. Baran R, Gupta AK, Pierard GE. Pharmacotherapy of onychomy-cosis. Expert Opin Pharmacother 2005;6:609–24.
43. Tosti A, Piraccini BM, Stinchi C, Colombo MD. Relapses ofonychomycosis after successful treatment with systemic antifun-gals: a three-year follow-up. Dermatology 1998;197:162–6.
44. Arrese JE, Pierard GE. Treatment failures and relapses inonychomycosis: a stubborn clinical problem. Dermatology 2003;207:255–60.
45. Tosti A, Piraccini BM. Dermatological diseases. In: Scher RK,Daniel III CR, eds. Nails: therapy, diagnosis, surgery, 3d ed.Philadelphia (PA): WB Saunders; 2005.
46. Lawry M. Biological therapy and nail psoriasis. Dermatol Ther2007;20:60–7.
47. Farber EM, South DA. Urea ointment in the non-surgical avulsionof nail dystrophies. Cutis 1978;22:689–92.
48. Mertin D, Lippold BC. In-vitro permeability of the human nail andof a keratin membrane from bovine hooves: prediction of thepenetration rate of antimycotics through the nail plate and theirefficacy. J Pharm Pharmacol 1997;49:866–72.
49. Kobayashi Y, Komatsu T, Sumi M, et al. In vitro permeation ofseveral drugs through the human nail plate: relationship betweenphysicochemical properties and nail permeability of drugs. Eur JPharm Sci 2004;21:471–7.
50. Walters KA, Flynn GL, Marvel JR. Physicochemical characterisa-tion of the human nail: permeation pattern for water and thehomologous alcohols and differences with respect to the stratumcorneum. J Pharm Pharmacol 1983;35:28–33.
51. Higa M, Tanioka A, Miyasaka K. A study of ion permeationacross a charged membrane in multicomponent ion systems asa function of membrane charge density. J Memb Sci 1990;49:145–69.
52. Higa M, Tanioka A, Miyasaka K. An experimental study of ionpermeation in multicomponent ion systems as a function ofmembrane charge density. J Memb Sci 1991;64:255–62.
53. Marshall RC. Characterisation of the proteins of human hair andnail by electrophoresis. J Invest Dermatol 1983;80:519–24.
54. Mertin D, Lippold BC. In vitro permeability of the human nail andof a keratin membrane from bovine hooves: influence of thepartition coefficient octanol/water and the water solubility of drugson their permeability and maximum flux. J Pharm Pharmacol 1997;49:30–4.
55. Walters KA, Flynn GL, Marvel JR. Physicochemical characterisa-tion of the human nail: solvent effects on the permeation ofhomologous alcohols. J Pharm Pharmacol 1985;37:771–5.
56. Soong MH. Transport properties of drugs and model compoundsacross the human nail. [PhD dissertation], University of Minnesota;1991.
57. de Berker D, Mawhinney B, Sviland L. Quantification of regionalmatrix nail production. Br J Dermatol 1996;134:1083–6.
58. Murthy SN, Wiskirchen DE, Bowers CP. Iontophoretic drugdelivery across human nail. J Pharm Sci 2007;96:305–11.
59. Hao J, Li SK. Transungual iontophoretic transport of polar neutraland positively charged model permeants: effects of electrophoresisand electroosmosis. J Pharm Sci 2008;97:893–905.
60. Pittrof F, Gerhards J, Erni W, Klecak G. Loceryl nail lacquer-realisation of a new galenical approach to onychomycosis therapy.Clin Exp Dermatol 1992;17:26–8.
61. Lauharanta J. Comparative efficacy and safety of amorolfine naillacquer 2-percent versus 5-percent once weekly. Clin Exp Dermatol1992;17:41–3.
62. Baran R, Hay RJ, Garduno JI. Review of antifungal therapy and theseverity index for assessing onychomycosis: Part I. J DermatologTreat 2008;19:72–81.
63. Di Chiacchio N, Kadunc BV, de Almeida AR, Madeira CL.Nail abrasion. J Cosmet Dermatol 2003;2:150–2.
64. Fukuda T, Shiohara T. Topical treatment of onychomycosis with anelectrically driven high speed grinder. Jpn J Dermatol 2001;111:37–42.
DOI: 10.3109/1061186X.2014.929138 Drug delivery across the nail plate barrier 787

65. Hargreaves GK. The treatment of onychomycosis with griseofulvin.Br J Dermatol 1960;72:358–64.
66. Kishimoto K. Evaluation of a nail grinding system using anelectronic high-speed dental teeth grinder in patients withonychomycosis. Jpn J Dermatol 2005;115:1035–40.
67. Sumikawa M, Egawa T, Honda I, et al. Effects of foot careintervention including nail drilling combined with topical anti-fungal application in diabetic patients with onychomycosis.J Dermatol 2007;34:456–64.
68. Hettinger DF, Valinsky MS. Treatment of onychomycosis with nailavulsion and topical ketoconazole. J Am Podiatr Med Assoc 1991;81:28–32.
69. Murthy SN, Waddell DC, Shivakumar HN, et al. Iontophoreticpermselective property of human nail. J Dermatol Sci 2007;46:150–2.
70. Hao J, Li SK. Mechanistic study of electroosmotic transport acrosshydrated nail plates: effects of pH and ionic strength. J Pharm Sci2008;97:5186–97.
71. Manda P, Sammeta SM, Repka MA, Murthy SN. Iontophoresisacross the proximal nail fold to target drugs to the nail matrix.J Pharm Sci 2012;101:2391–97.
72. Repka MA, O’haver J, See CH, et al. Nail morphology studies asassessments for onychomycosis treatment modalities. Int J Pharm2002;245:25–36.
73. Mididoddi PK, Prodduturi S, Repka MA. Influence of tartaric acidon the bioadhesion and mechanical properties of hot-melt extrudedhydroxypropyl cellulose films for the human nail. Drug Dev IndPharm 2006;32:1059–66.
74. Neev J, Nelson JS, Critelli M, et al. Ablation of human nail bypulsed lasers. Lasers Surg Med 1997;21:186–92.
75. Rothermel E, Apfelberg DB. Carbon dioxide laser use for certaindiseases of the toenails. Clin Podiatr Med Surg 1987;4:809–21.
76. Salter SA, Ciocon DH, Gowrishankar TR, Kimball AB. Controllednail trephination for subungual hematoma. Am J Emerg Med 2006;24:875–7.
77. Platform technology for minimally invasive medical devices.Available from: www.pathscientific.com [last accessed 12 Jan2014].
78. Ciocon D, Gowrishankar TR, Herndon T, Kimball AB. How lowshould you go: novel device for nail trephination. Dermatol Surg2006;32:828–33.
79. Boker A, Ciocon D, Kimbell A. A randomized, double-blindplacebo-controlled, pilot study of 1% terbinafine cream appliedtwice daily and delivered via nail plate microporation for thetreatment of subungual toenail trephination. J Am Acad Dermatol2007;56:AB114.
80. Mididoddi P, Upadhye S, Raymond C, et al. Influence of etchingand ultrasound on the permeability of ciclopirox through the humannail. AAPS J 2006;8:R6114.
81. Torkar A, Kristl J, Murdan S. Low-frequency ultrasound to enhancetopical drug delivery to the nail. AAPS J 2007;9:T3221.
82. Mitragotri S, Kost J. Low-frequency sonophoresis – a review. AdvDrug Del Rev 2004;56:589–601.
83. Azagury A, Khoury L, Enden G, Kost J. Ultrasound mediatedtransdermal drug delivery. Adv Drug Del Rev 2014;72:127–43.
84. Gunt H, Kasting GB. Hydration effect on human nail permeability.J Cosmet Sci 2006;57:183–4.
85. Gunt HB, Kasting GB. Effect of hydration on the permeation ofketoconazole through human nail plate in vitro. Eur J Pharm Sci2007;32:254–60.
86. Karell ML. Laser apparatus for making holes and etchings. USPatent 1999, US 005947956A.
87. Maltezos G, Scherer A. Treatment of toenail fungus. US Patent2007, US 0104664A1.
88. Donnelly RF, McCarron PA, Lightowler JM, Woolfson AD.Bioadhesive patch-based delivery of 5-aminolevulinic acid to thenail for photodynamic therapy of onychomycosis. J Control Release2005;103:381–92.
89. Malhotra GG, Zatz JL. Investigation of nail permeation enhance-ment by chemical modification using water as a probe. J Pharm Sci2002;91:312–23.
90. Kobayashi Y, Miyamoto M, Sugibayashi K, Morimoto Y.Enhancing effect of N-acetyl-l-cysteine or 2-mercaptoethanol on
the in vitro permeation of 5-fluorouracil or tolnaftate through thehuman nail plate. Chem Pharm Bull 1998;46:1797–802.
91. Brown MB, Khengar RH, Turner RB, et al. Overcoming the nailbarrier: a systematic investigation of ungual chemical penetrationenhancement. Int J Pharm 2009;370:61–7.
92. Ng Y, Mohorcic M, Torkar A, et al. Sodium sulphite – a potentialonycheal enhancer to increase the topical drug delivery to the nail.AAPS J 2007;9:T3181.
93. Khengar RH, Jones SA, Turner RB, et al. Nail swelling as a pre-formulation screen for the selection and optimisation of ungualpenetration enhancers. Pharm Res 2007;24:2207–12.
94. Khengar RH, Jones SA, Brown MB. The use of a novel ungualpenetration enhancing technology, MedNail to demonstrate thatdisulphide bond disruption in the nail increases the permeabilityof three antifungal agents. Proceedings Skin Forum; 2008 Jun 25–26; London.
95. Gunt HB, Miller MA, Kasting GB. Water diffusivity in human nailplate. J Pharm Sci 2007;96:3352–62.
96. Gradisar H, Friedrich J, Krizaj I, Jerala R. Similarities andspecificities of fungal keratinolytic proteases: comparison ofkeratinases of Paecilomyces marquandii and Doratomyces micro-sporus to some known proteases. Appl Environ Microbiol 2005;71:3420–6.
97. Mohorcic M, Torkar A, Friedrich J, Kristl J, Murdan S. Aninvestigation into keratinolytic enzymes to enhance ungual drugdelivery. Int J Pharm 2007;332:196–201.
98. Quintanar-Guerrero D, Ganem-Quintanar A, Tapia-Olguı́n P, et al.The effect of keratolytic agents on the permeability of threeimidazole antimycotic drugs through the human nail. Drug DevInd Pharm 1998;24:685–90.
99. Sun Y, Liu J, Wang JCT, De Doncker P. Nail penetration.In: Bronaugh RL, Maibach HI, eds. Percutaneous absorption:drugs-cosmetics-mechanisms-methodology, 3rd ed. New York(NY): Marcel Dekker Inc.; 1999.
100. Baran R, Coquard F. Combination of fluconazole and urea in anail lacquer for treating onychomycosis. J Dermatolog Treat 2005;16:52–5.
101. Baran R, Tosti A. Chemical avulsion with urea nail lacquer.J Dermatolog Treat 2002;13:161–4.
102. Morganti F, Bramanti E, Solaro R, et al. Thermal and spectro-scopic characterization of interactions between 2-nonyl-1,3-dioxolane and stratum corneum components. J BioactiveCompatible Polym 1999;14:162–7.
103. Samour CM, Donaruma LG, Daskalakis S, et al. SEPAs, a newclass of percutaneous absorption enhancers. Proct Int SympControlled Rel Bioact Mat 1989;16:183–4.
104. Nair AB, Sammeta SM, Vaka SRK, Murthy SN. A study on theeffect of inorganic salts in transungual drug delivery of terbina-fine. J Pharm Pharmacol 2009;61:431–7.
105. Nair AB, Chakraborty C, Murthy SN. Effect of polyethyleneglycols on the trans-ungual delivery of terbinafine. Curr DrugDeliv 2010;7:407–14.
106. Murthy SN, Vaka SRK, Sammeta SM, Nair AB. TranScreen-N:method for rapid screening of trans-ungual drug delivery enhan-cers. J Pharm Sci 2009;98:4264–71.
107. Murthy SN, Maibach HI. (2012). Topical nail products and ungualdrug delivery. Boca Raton (FL): CRC press.
108. Vaka SRK, Murthy SN, O’Haver JH, Repka MA. A platform forpredicting and enhancing model drug delivery across the humannail plate. Drug Dev Ind Pharm 2011;37:72–9.
109. Vignardet C, Guillaume YC, Friedrich J, Millet J. A first orderexperimental design to assess soluble proteins released by a newkeratinase from Doratomyces microsporus on human substrates.Int J Pharm 1999;191:95–102.
110. Monti D, Saccomani L, Chetoni P, et al. In vitro transungualpermeation of ciclopirox from a hydroxypropyl chitosan-based,water soluble nail lacquer. Drug Dev Ind Pharm 2005;31:11–17.
111. Myoung Y, Choi HK. Permeation of ciclopirox across porcinehoof membrane: effect of pressure sensitive adhesives andvehicles. Eur J Pharm Sci 2003;20:319–25.
112. Smith KA, Hao L, Li SK. Effects of ionic strength on passive andiontophoretic transport of cationic permeant across human nail.Pharm Res 2009;26:1446–55.
788 M. V. Saner et al. J Drug Target, 2014; 22(9): 769–789

113. Vejnovic I, Simmler L, Betz G. Investigation of differentformulations for drug delivery through the nail plate. Int JPharm 2010;386:185–94.
114. Nair AB, Kim H, Friden P, et al. Transungual iontophoresis ofterbinafine for onychomycosis: ex vivo evaluation. J Am AcadDermatol 2009;60:AB115.
115. Xiao P, Zheng X, Imhof RE, et al. Opto-thermal transient emissionradiometry (OTTER) to image diffusion in nails in vivo. Int JPharm 2011;406:111–13.
116. Hay RJ, Clayton YM, Moore MK. A comparison of tioconazole28% nail solution versus base as an adjunct to oral griseofulvin inpatients with onychomycosis. Clin Exp Dermatol 1987;12:175–7.
117. Hui X, Shainhouse Z, Tanojo H, et al. Enhanced human nail drugdelivery: nail inner drug content assayed by new unique method.J Pharm Sci 2002;91:189–95.
118. Hui X, Baker SJ, Wester RC, et al. In Vitro penetration of a noveloxaborole antifungal (AN2690) into the human nail plate. J PharmSci 2007;96:2622–31.
119. Suringa DW. Treatment of superficial onychomycosis withtopically applied glutaraldehyde. A preliminary study. ArchDermatol 1970;102:163–7.
120. Marty JL. Amorolfine nail lacquer: a novel formulation. J EurAcad of Dermatol Venereol 1995;4:S17–21.
121. Franz TJ. Absorption of amorolfine through human nail.Dermatology 1992;184:18–20.
122. Gupta AK, Fleckman P, Baran R. Ciclopirox nail lacquer topicalsolution 8% in the treatment of toenail onychomycosis. J Am AcadDermatol 2000;43:S70–80.
123. Polak A. Amorolfine: a review of its mode of action and in vitroand in vivo antifungal activity. J Am Med Assoc South East Asia1993;9:11–18.
124. Obadiah J, Scher R. Nail disorders: unapproved treatments. ClinDermatol 2002;20:643–8.
125. Baden HP. Treatment of distal onychomycosis with avulsion andtopical antifungal agents under occlusion. Arch Dermatol 1994;130:558–9.
126. Bindra RL, Singh AK, Shawl AS, Kumar S. Anti-fungal herbalformulation for treatment of human nails fungus and processthereof. US Patent 2001; US 6296838 B1.
127. Tandel A, Agrawal S, Wankhede S. Transungual permeation of theVoriconazole nail lacquer against Trichophyton rubrum. J DrugDeliv Ther 2012;2:25–33.
128. Lusiana, Reichl S, Muller-Goymann CC. Infected nail plate modelmade of human hair keratin for evaluating the efficacy of differenttopical antifungal formulations against Trichophyton rubrum invitro. Eur J Pharm Biopharm 2013;84:599–605.
129. Hafeez F, Hui X, Chiang A, et al. Transungual delivery ofketoconazole using novel lacquer formulation. Int J Pharm 2013;456:357–61.
130. Nogueiras-Nieto L, Delgado-Charro MB, Otero-Espinar FJ.Thermogelling hydrogels of cyclodextrin/poloxamer polypseudor-otaxanes as aqueous-based nail lacquers: application to thedelivery of triamcinolone acetonide and ciclopirox olamine. EurJ Pharm Biopharm 2013;83:370–7.
131. Tanrıverdi ST, Ozer O. Novel topical formulations of Terbinafine-HCl for treatment of onychomycosis. Eur J Pharm Sci 2013;48:628–36.
132. Miron D, Cornelio R, Troleis J, et al. Influence of penetrationenhancers and molecular weight in antifungals permeationthrough bovine hoof membranes and prediction of efficacy inhuman nails. Eur J Pharm Sci 2014;51:20–5.
133. Nimni M. Anti-fungal nail lacquer and method therefor. US Patent1996; US 005487776 A.
134. Sorenson JL, Petersen RV. Composition and method for treatingdiseased nail. US Patent 1998; US 005840283 A.
135. Chaudhari B, Chim MF, Bucks D. Topical formulations for thetreatment of nail fungal 135. diseases. US Patent 2000; US006143794 A.
136. Quan D, Ruiz A. Nail compositions and methods for administeringsame. US Patent 2003; US 006585963 B1.
137. Maibach HI, Luo EC, Hsu T. Topical administration of basicantifungal compositions to treat fungal infections of the nails. USPatent 2005; US 006846837 B2.
138. Mailland F. Nail restructuring compositions for topical applica-tion. US Patent 2006; US 0134039 A1.
139. Riley L. Topical formulation for treating fingernails and toenails.US Patent 2007; US 007198794 B1.
140. Meyer H. Pharmaceutical and cosmetic formulations for treatingfingernails. US Patent 2007; US 0166249 A1.
141. Kepka SW, Mo J, Wang H, et al. Antifungal nail coat and methodof use. US Patent 2008; US 7462362 B2.
142. Kochinke FM, Bright C. Compositions and methods for treatingconditions of the nail unit. US Patent 2008; US 0132442 A1.
143. Etheredge RW, Goldberg DI, Davis SP, et al. Method and systemfor treating of onychomycosis with an applicator having gelmedicament layer. US Patent 2008; US 0319371 A1.
144. Zhang J, Warner KS, Kumar P, Aliyar H. Systems, methods, andformulations for topically treating nail fungal infections and nailpsoriasis. US Patent 2009; US 0175945 A1.
145. Singh J, Dan M. Topical nail formulation. US Patent 2009; US0215888 A1.
146. Cevc G, Vierl U. Topical terbinafine formulations and methods ofadministering same for the treatment of fungal infections. USPatent 2010; US 7820720 B2.
147. Bailey C. Method and apparatus for improving the appearance ofnails affected by onychomycosis through the topical application ofhighly concentrated or supersaturated boric acid. US Patent 2011;US 0083692 A1.
148. Lusiana, Muller-Goymann C. Formulation for nail and nail beddiseases. US Patent 2012; US 0010227 A1.
149. Available from www.clinicaltrials.gov [last accessed 07 May2014].
150. Dutet J, Delgado-Charro MB. Electroosmotic transport of man-nitol across human nail during constant current iontophoresis.J Pharm Pharmacol 2010;62:721–9.
151. Dutet J, Delgado-Charro MB. Transungual iontophoresis oflithium and sodium: effect of pH and co-ion competition oncationic transport numbers. J Control Release 2010;144:168–74.
152. Dutet J, Delgado-Charro MB. In vivo transungual iontophoresis:effect of DC current application on ionic transport and onTransonychial water loss. J Control Release 2009;140:117–25.
153. Nogueiras Nieto L, Gomez Amoza JL, Delgado Charro MB,Otero-Espinar FJ. Hydration and N-acetyl-l-cysteine alter themicrostructure of human nail and bovine hoof: implications fordrug delivery. J Control Release 2011;156:337–44.
154. Smith KA, Hao J, Li SK. Influence of pH on transungual passiveand iontophoretic transport. J Pharm Sci 2010;99:1955–67.
155. Hao J, Smith KA, Li SK. Iontophoretically enhanced ciclopiroxdelivery into and across human nail plate. J Pharm Sci 2009;98:3608–16.
156. Hao J, Smith KA, Li SK. Chemical method to enhancetransungual transport and iontophoresis efficiency. Int J Pharm2008;357:61–9.
157. Hao J, Smith KA, Li SK. Time-dependent electrical properties ofhuman nail upon hydration in vivo. J Pharm Sci 2010;99:107–18.
158. Smith KA, Hao J, Li SK. Effect of organic solvents on the barrierproperties of human nail. J Pharm Sci 2011;100:4244–57.
DOI: 10.3109/1061186X.2014.929138 Drug delivery across the nail plate barrier 789
Related Documents











