Innovative Solutions Using Zygoma Implants Paul P. Binon, DDS, MSD, FAO Private Practice, Roseville, CA The article is associated with the American College of Prosthodontists’ journal-based continuing education program. It is accompanied by an online continuing education activity worth 1 credit. Please visit www.wileyhealthlearning.com/jopr to complete the activity and earn credit. Keywords Remote implant support; zygoma implants; severe resorption; edentulous maxilla. Correspondence Paul P. Binon, 1158 Cirby Way, Roseville, CA 95661. E-mail: [email protected]. The author denies any conflicts of interest. Accepted April 15, 2016 doi: 10.1111/jopr.12504 Abstract The severely resorbed edentulous maxilla presents significant treatment challenges. The introduction of remote implant support using zygoma implants has provided a plethora of treatment possibilities for many patients. This article presents four very different sets of circumstances successfully treated using this protocol. Treatment of the severely resorbed edentulous maxilla presents a set of unique and challenging problems. 1,2 Early efforts to augment the deficient maxilla varied from hydroxyapatite (HA) buildups, rib and hip bone sandwich grafts, and sinus augmenta- tion using a variety of material combinations. Currently several different augmentation protocols can be used to build up the internal vertical height of the sinus floor so that implants can be placed. 3-6 This is a viable protocol that requires two surgeries. After the initial surgery, a waiting period of 4 to 6 months is necessary to permit graft maturation. At that time the implants can be placed in the grafted sites, and another 6 months are necessary for the implants to securely integrate in the grafted bone. During this staged sequence, the patient typically wears a complete denture with a soft liner. Total treatment time will range from 12 to 15 months or more. Most often this protocol requires 6 to 8 implants and typically results in a bar-retained overdenture (Fig 1). 7-9 In an effort to reduce the number of surgeries and allow for the immediate use of the implants, Dr. P-I Branemark devel- oped the concept of remote implant support, 10-13 which essen- tially involves making a window into the lateral sinus wall, raising the Schneiderian membrane and gaining direct visual- ization of the base of the zygomatic arch. A series of special long drills are used to prepare an osteotomy in the medial wall of the zygomatic arch until it exits at the outer cortex. Im- plant lengths and corresponding drills range from 35 to 52.5 mm long. The implants have a unique design with an implant body from 4 to 5 mm in diameter. The coronal end has a 45° external hex connection, allowing it to be positioned perpen- dicular to the palate. In the classic approach, 2 to 4 anterior im- plants are placed in the premaxilla for optimal load distribution (Fig 2). Universal abutments are placed on the implants along with temporary cylinders, and a previously made complete den- ture is transitioned into a fixed palate-less interim prosthesis. If there is no bone for anchorage in the premaxilla, the quad zygoma approach can be used. It involves the placement of two zygoma implants on each side of the dental arch. The zygoma implant can also be used unilaterally in cases where there is sufficient bone for conventional implant place- ment on one side of the arch and a serious deficiency on the other. It can also be used in conjunction with the “All-on-4” approach when additional posterior support is necessary. The major advantages of this protocol is that it significantly reduces the treatment time line from 12/15 months to 6/7 months, eliminates extensive grafting surgery, and immediately results in a fixed prosthesis. There is ample long-term documen- tation in the literature with 97%+ long-term success rates. 14-16 In addition, it allows the prosthodontist innovative options to solve exceptionally challenging circumstances. Four such chal- lenging cases are presented that highlight the flexibility of the zygoma protocol. The typical prosthetic protocol requires the following steps once the patient has decided on treatment. If the existing den- ture fits reasonably well it can be used. If not, an immediate denture is made in advance of the surgery date. On completion of the surgery, the abutment locations are indexed with bite registration paste. Access holes to allow direct pick-up of the temporary cylinders are created in the denture. With the tem- porary cylinders seated on the abutments, the denture is seated. The cylinders are then bonded to the denture using the brush bead technique with fast-cure resin (Qyk-Set; Holmes Dental Co., Hatboro, PA). This is sequentially completed until all the temporary cylinders are firmly attached to the denture. The den- ture is then removed from the mouth. The palate, the flanges, and excess tube length of the temporary cylinders are removed and adjusted. It is reinserted in the mouth, and the occlusion is 244 Journal of Prosthodontics 26 (2017) 244–251 C 2016 by the American College of Prosthodontists

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Innovative Solutions Using Zygoma ImplantsPaul P. Binon, DDS, MSD, FAO
Private Practice, Roseville, CA
The article is associated with the American College of Prosthodontists’ journal-based continuing education program. It is accompanied
by an online continuing education activity worth 1 credit. Please visit www.wileyhealthlearning.com/jopr to complete the activity and
earn credit.
Keywords
Remote implant support; zygoma implants;severe resorption; edentulous maxilla.
Correspondence
Paul P. Binon, 1158 Cirby Way, Roseville, CA95661. E-mail: [email protected].
The author denies any conflicts of interest.
Accepted April 15, 2016
doi: 10.1111/jopr.12504
AbstractThe severely resorbed edentulous maxilla presents significant treatment challenges.The introduction of remote implant support using zygoma implants has provided aplethora of treatment possibilities for many patients. This article presents four verydifferent sets of circumstances successfully treated using this protocol.
Treatment of the severely resorbed edentulous maxilla presentsa set of unique and challenging problems.1,2 Early efforts toaugment the deficient maxilla varied from hydroxyapatite (HA)buildups, rib and hip bone sandwich grafts, and sinus augmenta-tion using a variety of material combinations. Currently severaldifferent augmentation protocols can be used to build up theinternal vertical height of the sinus floor so that implants can beplaced.3-6 This is a viable protocol that requires two surgeries.After the initial surgery, a waiting period of 4 to 6 months isnecessary to permit graft maturation. At that time the implantscan be placed in the grafted sites, and another 6 months arenecessary for the implants to securely integrate in the graftedbone. During this staged sequence, the patient typically wearsa complete denture with a soft liner. Total treatment time willrange from 12 to 15 months or more. Most often this protocolrequires 6 to 8 implants and typically results in a bar-retainedoverdenture (Fig 1).7-9
In an effort to reduce the number of surgeries and allow forthe immediate use of the implants, Dr. P-I Branemark devel-oped the concept of remote implant support,10-13 which essen-tially involves making a window into the lateral sinus wall,raising the Schneiderian membrane and gaining direct visual-ization of the base of the zygomatic arch. A series of speciallong drills are used to prepare an osteotomy in the medial wallof the zygomatic arch until it exits at the outer cortex. Im-plant lengths and corresponding drills range from 35 to 52.5mm long. The implants have a unique design with an implantbody from 4 to 5 mm in diameter. The coronal end has a 45°external hex connection, allowing it to be positioned perpen-dicular to the palate. In the classic approach, 2 to 4 anterior im-plants are placed in the premaxilla for optimal load distribution(Fig 2). Universal abutments are placed on the implants alongwith temporary cylinders, and a previously made complete den-
ture is transitioned into a fixed palate-less interim prosthesis.If there is no bone for anchorage in the premaxilla, the quadzygoma approach can be used. It involves the placement of twozygoma implants on each side of the dental arch.
The zygoma implant can also be used unilaterally in caseswhere there is sufficient bone for conventional implant place-ment on one side of the arch and a serious deficiency on theother. It can also be used in conjunction with the “All-on-4”approach when additional posterior support is necessary.
The major advantages of this protocol is that it significantlyreduces the treatment time line from 12/15 months to 6/7months, eliminates extensive grafting surgery, and immediatelyresults in a fixed prosthesis. There is ample long-term documen-tation in the literature with 97%+ long-term success rates.14-16
In addition, it allows the prosthodontist innovative options tosolve exceptionally challenging circumstances. Four such chal-lenging cases are presented that highlight the flexibility of thezygoma protocol.
The typical prosthetic protocol requires the following stepsonce the patient has decided on treatment. If the existing den-ture fits reasonably well it can be used. If not, an immediatedenture is made in advance of the surgery date. On completionof the surgery, the abutment locations are indexed with biteregistration paste. Access holes to allow direct pick-up of thetemporary cylinders are created in the denture. With the tem-porary cylinders seated on the abutments, the denture is seated.The cylinders are then bonded to the denture using the brushbead technique with fast-cure resin (Qyk-Set; Holmes DentalCo., Hatboro, PA). This is sequentially completed until all thetemporary cylinders are firmly attached to the denture. The den-ture is then removed from the mouth. The palate, the flanges,and excess tube length of the temporary cylinders are removedand adjusted. It is reinserted in the mouth, and the occlusion is
244 Journal of Prosthodontics 26 (2017) 244–251 C© 2016 by the American College of Prosthodontists

Binon Zygoma Implants
carefully checked and adjusted. Six months later the temporaryhybrid denture is removed from the mouth, the implants arechecked for stability, and an impression is taken. At the nextappointment a cast verification jig is used to verify the accuracyof the master cast. A framework is then constructed out of tita-nium, bite relationship records are obtained, and denture teethare set on the framework. The setup is tried in the mouth for thenormal prosthetic evaluations of vertical dimension, phonetics,occlusion, and esthetics. On patient approval, the prosthesis isprocessed and inserted at the next appointment. Post-insertioninstructions are given, and the patient is monitored closely forthe first 3 months.
Clinical case #1: the rescue concept
A 60-year-old woman presented with a primary complaint thather maxillary implants were painful, the gum tissue chroni-cally bled, and was “growing” over her tissue bar. Her dentalhistory showed a maxillary subperiosteal implant followed byseveral blade implants placed in the early 1980s. Subsequentto failure, she had a ridge graft with hipbone, bilateral sinusaugmentations, and the placement of six HA-coated implantsin 1997.
Figure 3 illustrates the condition of the soft tissues. Periodon-tal evaluation indicated generalized pocket depths in excess of7 mm around the six implants. Intake radiographs verified sig-nificant cratering and bone loss around all implants (Fig 4).Treatment plans were presented that included (1) removal ofthe implants and grafting of the ridge defects and a conven-tional denture, (2) removal of the implants, bilateral sinus graftsfollowed in 6 months with the placement of six implants anda new, more-hygienic bar, (3) removal of the failing implants,grafting of the ridge defects, and the placement of two conven-tional implants in the premaxilla and bilateral zygoma implants.The implants would be loaded immediately if insertion torquespermitted. The patient decided on the zygoma immediate loadtreatment plan.
At the time of surgery the loss of the HA coating on the failedimplants and the advanced cratering and bone loss was veri-fied (Fig 5). Two conventional and two zygoma implants werepurchased from Nobel Biocare Holding AG, Kloten, Switzer-land. Four implants were placed, the denture was indexed,and temporary cylinders were picked up in the denture. Thedenture was then appropriately modified, the occlusion ad-justed, and inserted in the mouth (Fig 6). Healing was un-eventful, and 6 months later (Fig 7) an impression was madeand sent to the laboratory. A titanium milled bar (Cagenix Inc.,Memphis, TN) was made and tested in the mouth for passivefit. The denture sequence was completed, and the definitiveprosthesis inserted (Fig 8). The patient transitioned from a fail-ing, six HA-coated, implant-supported bar to a fixed prosthesisin 7 months (Fig 9). A postoperative radiograph showed well-integrated implants (Fig 10).
Clinical case #2: the acquired defectsolution
A 45-year old female patient presented in 2002 with a needto restore the upper arch following ablative surgery of a mu-
coepidermoid tumor. The surgery resulted in a large palatal de-fect (6×6×2.5 mm) (Fig 11). A pretreatment CT scan showedthe extent of the palatal defect (Fig 12). The patient was aheavy smoker with advanced periodontal disease. The remain-ing maxillary dentition had a hopeless prognosis. Alternativesto a complete maxillary denture were evaluated. Following ini-tial periodontal efforts to retain selected teeth, the patient se-lected a zygoma implant-based fixed prosthesis treatment plan.The maxillary teeth were removed, and two anterior implantsand two zygoma implants (Nobel Biocare Holding AG) wereplaced. The maxillary denture made in advance of surgery wasconverted to a fixed interim hybrid denture (Fig 13). A tem-porary obturator bulb was made and relined with soft dentureliner (Visco-gel; Dentsply, York, PA). Subsequently a more sta-ble and retentive temporary obturator was constructed (Fig 14).Healing was uneventful, and at 6 months a definitive impres-sion of the maxilla was made (Fig 15). Following the usualprotocol, a titanium retention bar (Cagenix Inc.) was designedwith lingual wings in the bicuspid area to incorporate bilateralLocator retentive elements (Zest Anchors LLC., Escondido,CA.) to retain the removable obturator portion of the prosthesis(Fig 16). After completion of a wax try-in, the fixed hybrid wasprocessed. In addition, a cobalt chrome palatal strap that incor-porated Locator retention cups to retain the obturator portionwas made (Fig 17). This permitted fixed restoration for functionand esthetics (Fig 18) that is easily accessible for hygiene witha removable and stable obturator prosthesis. A postoperativeradiograph taken in 2015 after more than 5 years of functionshows excellent osseous stability (Fig 19).
Clinical case #3: a congenital defectsolution
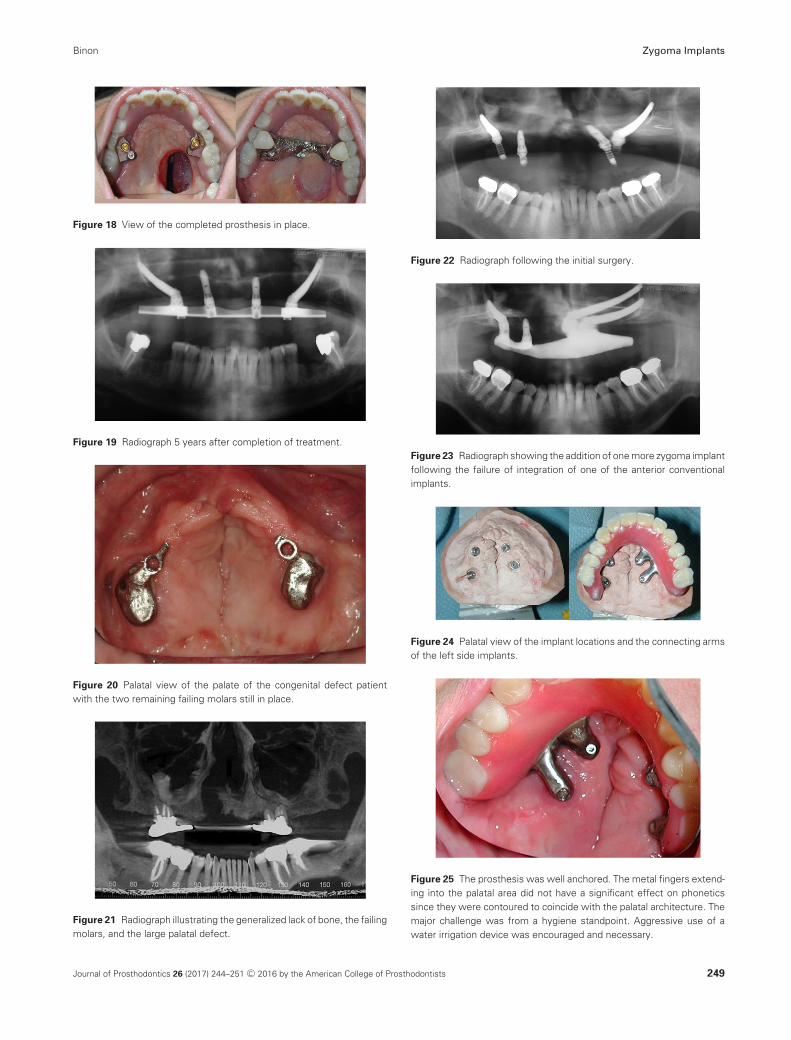
A male patient of record since 1984 had a history of right sidecleft palate and lip surgically repaired. The maxilla was con-tracted with a longitudinal fistula and no bony union. Therewas a pharyngeal flap with a narrow pedicle. Initially therewere four teeth remaining that helped secure his prosthesis.Because of advanced periodontal disease, two of the four teethwere removed, and the remaining two molars (#3 and 14) wererestored with gold sub-crowns and a bar interconnected withtwo ERA attachments (Sterngold Dental LLC., Attleboro, MA)(Fig 20). This arrangement functioned for 22 years. The barwas removed at that time to limit anterior/posterior loading.The teeth were fibrous encapsulated and demonstrated plus 3mobility. The patient’s palate was flat with anterior areas ofeasily compressed mobile tissue (Fig 21). Limited alternativesto a complete denture were available. The patient opted fora zygoma-assisted (Nobel Biocare Holding AG) fixed hybridprosthesis. Locating anterior bone for support proved challeng-ing. Two small islands of bone were located, and the surgerywas completed uneventfully (Fig 22). The temporary prosthesiswas secure and functional following surgery. After 3 monthsthe left anterior conventional implant failed. A second zygomaimplant was then inserted, and the temporary prosthesis wasmodified to accept an additional temporary coping (Fig 23).Six months from insertion of the second zygoma implant, theimplants were tested, and a final impression was obtained. Thecast was verified, and a milled titanium bar was made. The
Journal of Prosthodontics 26 (2017) 244–251 C© 2016 by the American College of Prosthodontists 245
Zygoma Implants Binon
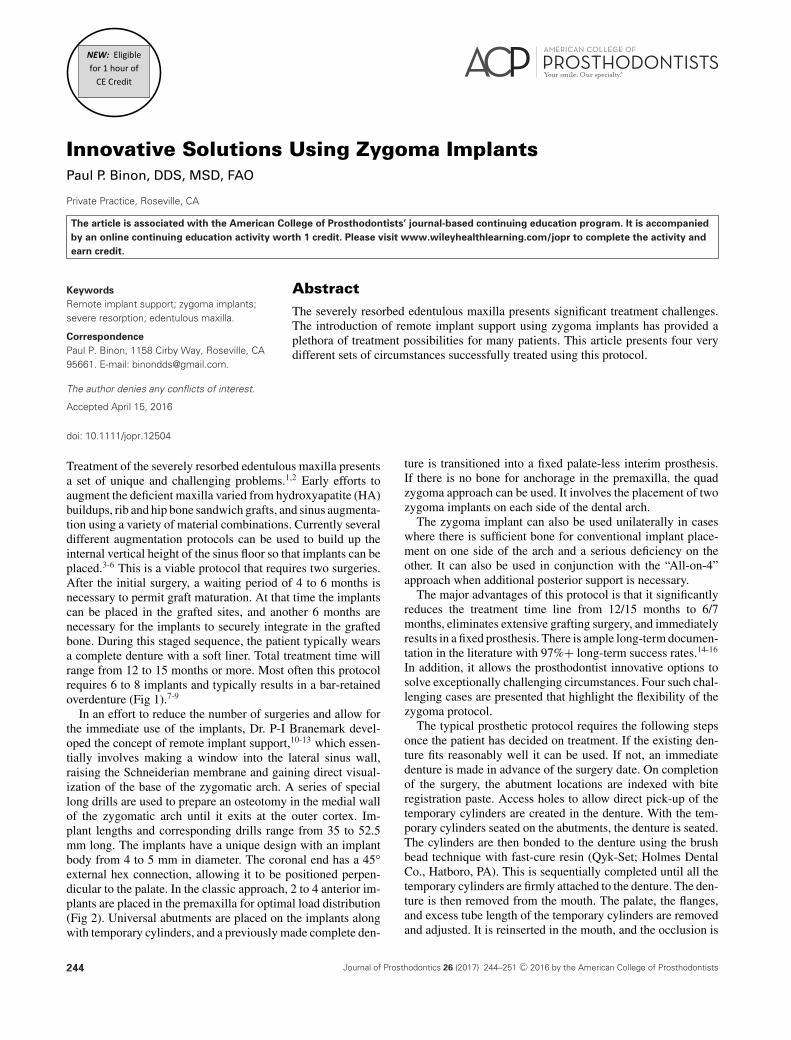
Figure 1 Example of typical conventional restorative treatment protocolfollowing bilateral sinus augmentation using 6 to 8 implants with a bar-retained overdenture.
Figure 2 Surgery planning imagery indicating the location of the pro-jected implants in the zygoma as well as the anterior maxilla for a typicalzygoma case.
Figure 3 Pretreatment condition of the soft tissues.
challenge with cases with minimal palatal bone is that the exitpoint of the head of the zygoma implant is typically locatedcloser to the midline. This is true because the zygoma implant
Figure 4 Intake radiograph indicating extensive bone loss and crateringaround existing implants.
Figure 5 With the palatal tissues reflected, the condition of the failedHA surgical coated implants is quite obvious.
Figure 6 Following placement of bilateral zygoma implants and twoconventional anterior implants, the modified provisional denture was at-tached to the implant abutments, and the patient left with an immediateload fixed prosthesis.
246 Journal of Prosthodontics 26 (2017) 244–251 C© 2016 by the American College of Prosthodontists
Binon Zygoma Implants
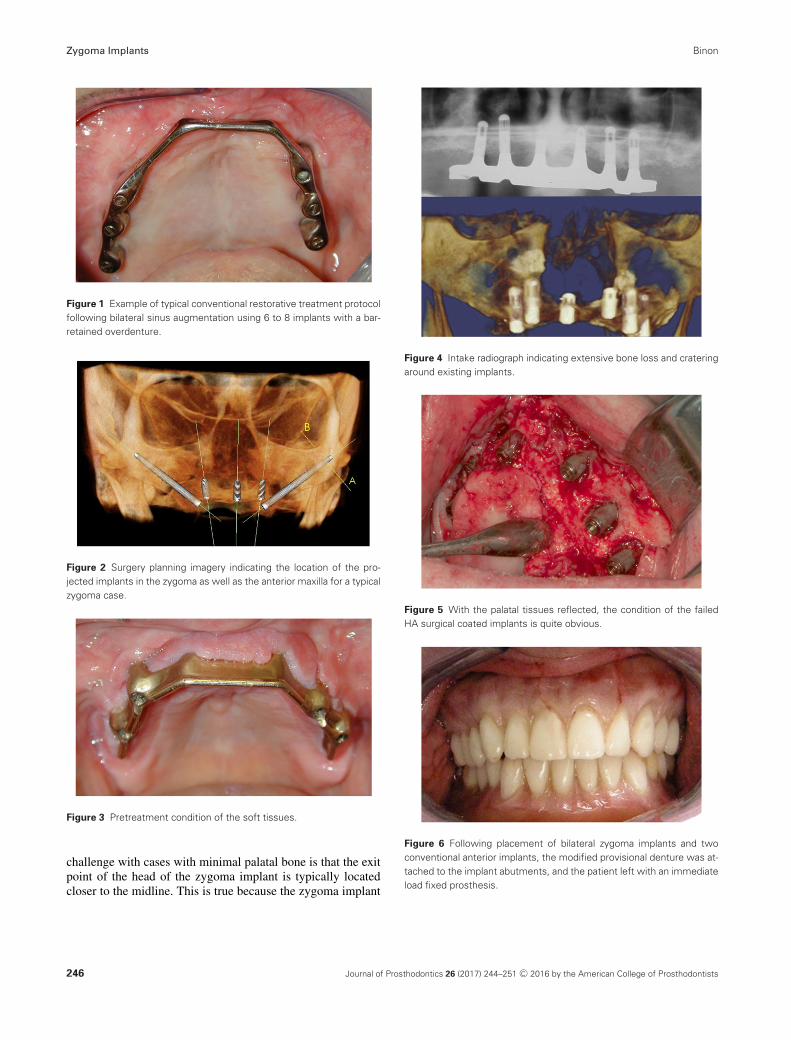
Figure 7 Appearance of the tissues at 6 months, following removal ofthe interim fixed prosthesis. Impression copings are in place immediatelyprior to taking the impression for the definitive restoration.
Figure 8 Anterior view of the completed definitive restoration in place.
Figure 9 Palatal view of the completed fixed implant-supported hybrid.
lies almost flat due to the minimal difference in angulation be-tween the zygoma and the residual hard palate. This is amplifiedfurther in cleft palate patients due to the contracted shape of themaxillary arch (Fig 24). It results in horizontal extension fromthe body of the prosthesis to engage the abutment locations(Fig 25). The prosthesis has successfully functioned for morethan 9 years.
Figure 10 Post-insertion radiograph.
Figure 11 Second patient documenting the results of ablative surgeryand the active advanced periodontal disease.
Clinical case #4: the untreatable maxilla
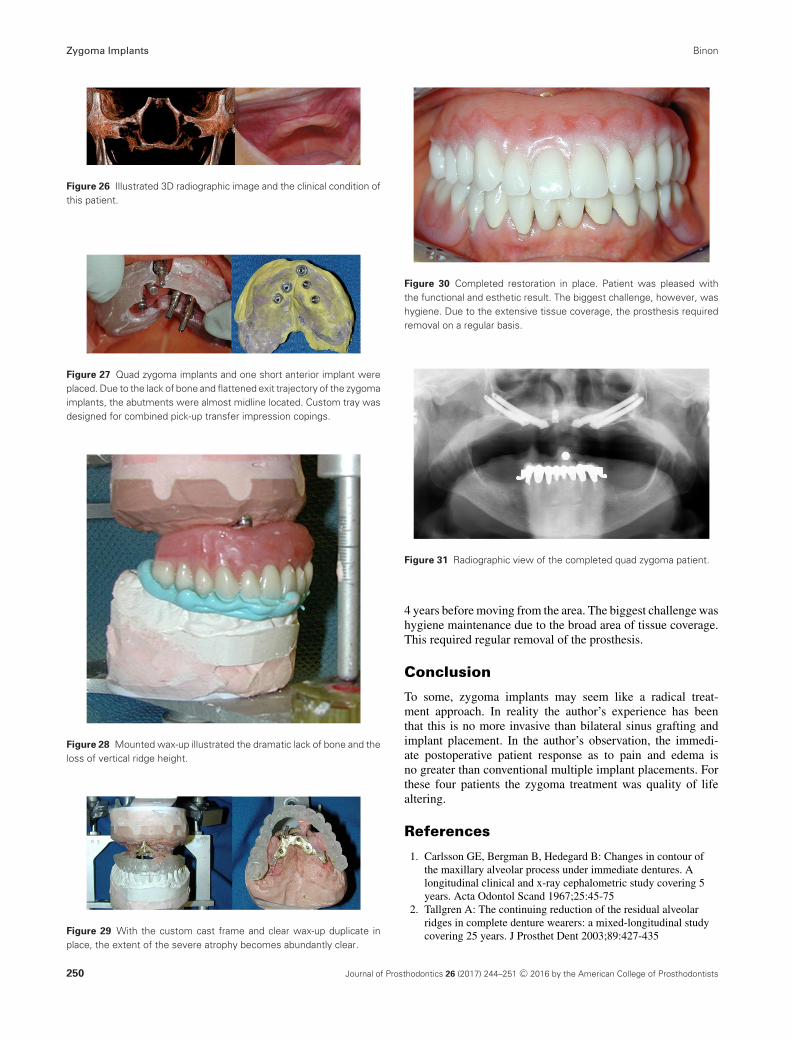
In 2004 a 79-year-old female Asian patient presented witha primary complaint that she could not wear a denture. Sheused considerable adhesive and still there was no retention,stability, function, or comfort. She related that she had a ribgraft augmentation that completely resorbed in short order, fol-lowed by an HA particulate augmentation that also failed ina short time. Examination indicated advanced atrophy, a mo-bile and easily compressed soft tissue roll, and the presenceof no vestibule. CT images verified the dramatic lack of bone(Fig 26). Due to previous surgical experiences with limitedresults, sinus augmentation was ruled out, leaving only re-construction with a hybrid fixed prosthesis supported by thequad zygoma approach. The implants were placed, and thedenture was converted to a fixed prosthesis following the stan-dard protocol. Healing was uneventful. Six months later animpression was made of the maxilla (Fig 27). Occlusal recordswere obtained, the casts mounted, and a wax-up was completed(Fig 28). Note the severe vertical and horizontal bone defi-ciency present (Fig 29). To minimize intrusion of the palatalarea, a custom cast frame was designed and cast. Once thepassive fit was confirmed, the prosthesis was processed and in-serted. Esthetically and functionally this was a successful result(Fig 30, 31). The patient functioned with the prosthesis for
Journal of Prosthodontics 26 (2017) 244–251 C© 2016 by the American College of Prosthodontists 247
Zygoma Implants Binon
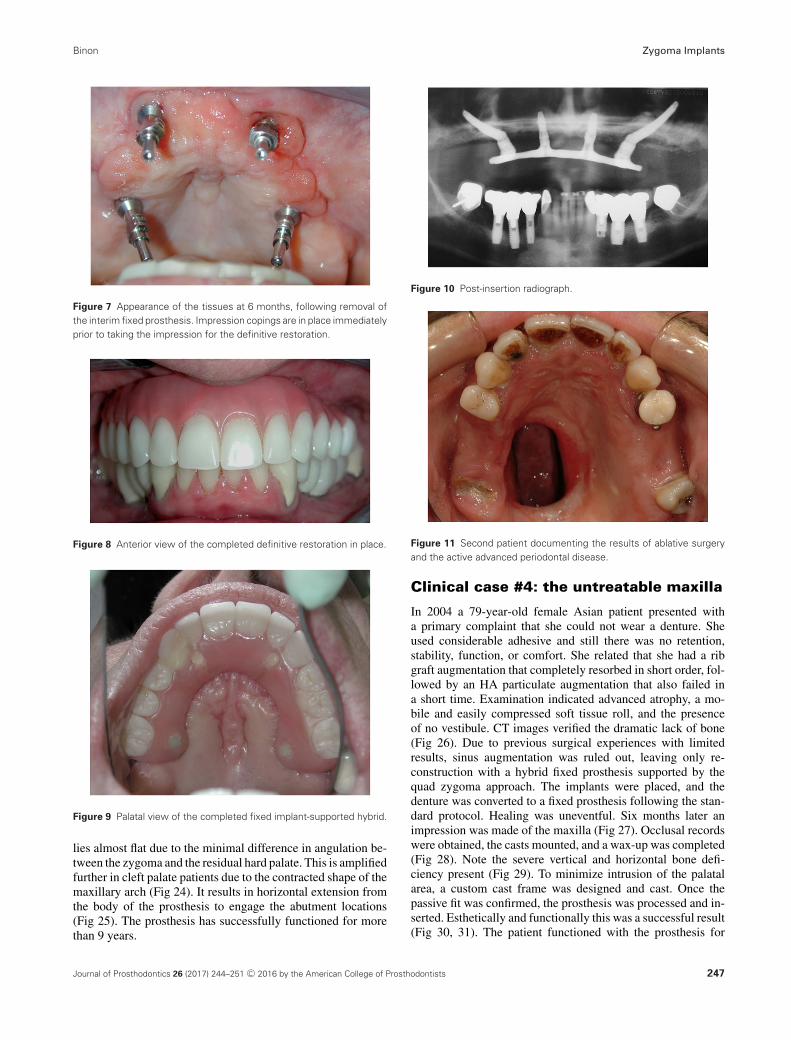
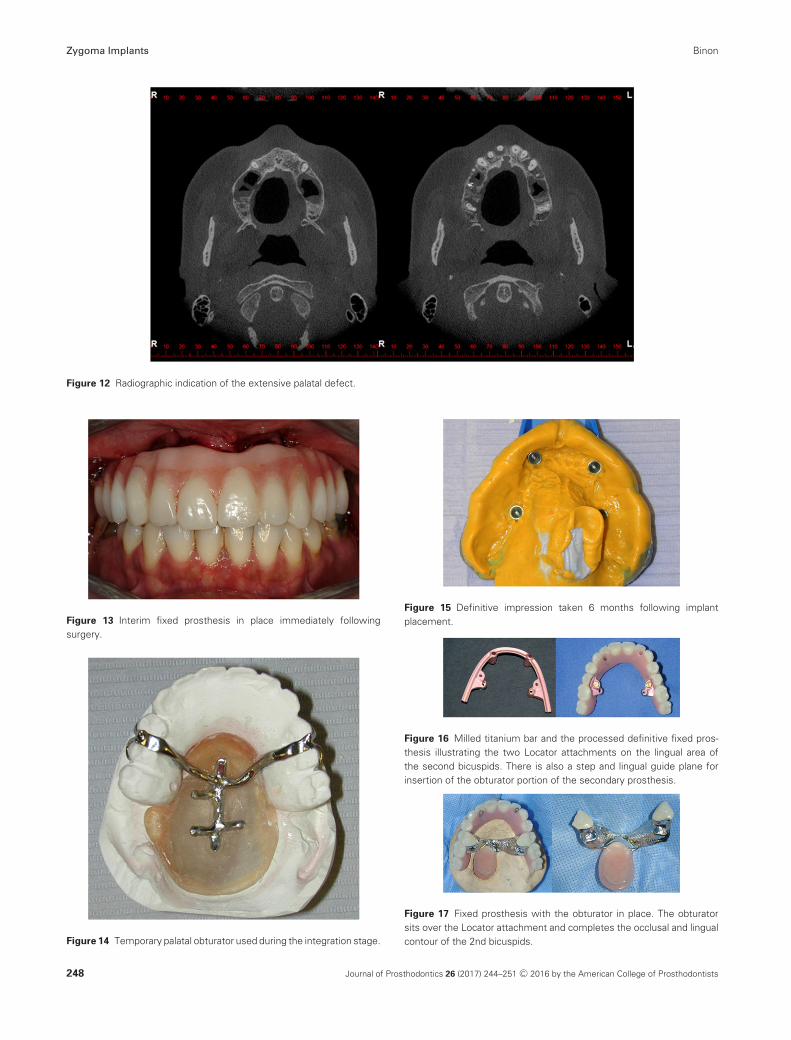
Figure 12 Radiographic indication of the extensive palatal defect.
Figure 13 Interim fixed prosthesis in place immediately followingsurgery.
Figure 14 Temporary palatal obturator used during the integration stage.
Figure 15 Definitive impression taken 6 months following implantplacement.
Figure 16 Milled titanium bar and the processed definitive fixed pros-thesis illustrating the two Locator attachments on the lingual area ofthe second bicuspids. There is also a step and lingual guide plane forinsertion of the obturator portion of the secondary prosthesis.
Figure 17 Fixed prosthesis with the obturator in place. The obturatorsits over the Locator attachment and completes the occlusal and lingualcontour of the 2nd bicuspids.
248 Journal of Prosthodontics 26 (2017) 244–251 C© 2016 by the American College of Prosthodontists
Binon Zygoma Implants
Figure 18 View of the completed prosthesis in place.
Figure 19 Radiograph 5 years after completion of treatment.
Figure 20 Palatal view of the palate of the congenital defect patientwith the two remaining failing molars still in place.
Figure 21 Radiograph illustrating the generalized lack of bone, the failingmolars, and the large palatal defect.
Figure 22 Radiograph following the initial surgery.
Figure 23 Radiograph showing the addition of one more zygoma implantfollowing the failure of integration of one of the anterior conventionalimplants.
Figure 24 Palatal view of the implant locations and the connecting armsof the left side implants.
Figure 25 The prosthesis was well anchored. The metal fingers extend-ing into the palatal area did not have a significant effect on phoneticssince they were contoured to coincide with the palatal architecture. Themajor challenge was from a hygiene standpoint. Aggressive use of awater irrigation device was encouraged and necessary.
Journal of Prosthodontics 26 (2017) 244–251 C© 2016 by the American College of Prosthodontists 249
Zygoma Implants Binon
Figure 26 Illustrated 3D radiographic image and the clinical condition ofthis patient.
Figure 27 Quad zygoma implants and one short anterior implant wereplaced. Due to the lack of bone and flattened exit trajectory of the zygomaimplants, the abutments were almost midline located. Custom tray wasdesigned for combined pick-up transfer impression copings.
Figure 28 Mounted wax-up illustrated the dramatic lack of bone and theloss of vertical ridge height.
Figure 29 With the custom cast frame and clear wax-up duplicate inplace, the extent of the severe atrophy becomes abundantly clear.
Figure 30 Completed restoration in place. Patient was pleased withthe functional and esthetic result. The biggest challenge, however, washygiene. Due to the extensive tissue coverage, the prosthesis requiredremoval on a regular basis.
Figure 31 Radiographic view of the completed quad zygoma patient.
4 years before moving from the area. The biggest challenge washygiene maintenance due to the broad area of tissue coverage.This required regular removal of the prosthesis.
Conclusion
To some, zygoma implants may seem like a radical treat-ment approach. In reality the author’s experience has beenthat this is no more invasive than bilateral sinus grafting andimplant placement. In the author’s observation, the immedi-ate postoperative patient response as to pain and edema isno greater than conventional multiple implant placements. Forthese four patients the zygoma treatment was quality of lifealtering.
References
1. Carlsson GE, Bergman B, Hedegard B: Changes in contour ofthe maxillary alveolar process under immediate dentures. Alongitudinal clinical and x-ray cephalometric study covering 5years. Acta Odontol Scand 1967;25:45-75
2. Tallgren A: The continuing reduction of the residual alveolarridges in complete denture wearers: a mixed-longitudinal studycovering 25 years. J Prosthet Dent 2003;89:427-435
250 Journal of Prosthodontics 26 (2017) 244–251 C© 2016 by the American College of Prosthodontists

Binon Zygoma Implants
3. Desjardins R: Prosthesis design for osseointegrated implants inthe edentulous maxilla. Int J Oral Maxillofac Implants1992;7:311-320
4. Jemt T: Fixed implant-supported prosthesis in the edentulousmaxilla. Clin Oral Implants Res 1994;5:142-147
5. Lewis S, Sharma A, Nishimura R: Treatment of edentulousmaxillae with osseointegrated implants. J Prosthet Dent1992;68:503-508
6. Taylor T: Fixed implant rehabilitation for the edentulous maxilla.Int J Oral Maxillofac Implants 1991;6:329-337
7. Sadowsky SJ: The implant-supported prosthesis for theedentulous arch: design considerations. J Prosthet Dent1997;78:28-33
8. Henry PJ: A review of guidelines for implant rehabilitation of theedentulous maxilla. J Prosthet Dent 2002;87:281-288
9. Zitzman NU, Marinello CP: Fixed or Removableimplant-supported restorations in the edentulous maxilla:Literature review. Pract Periodontics Aesthet Dent2000;12:599-608
10. Branemark PI, Grondahl K, Ohrnell LO, et al: Zygoma fixture inthe management of advanced atrophy of the maxilla: techniqueand long term results. Scand J Plast Reconstr Surg Hand Surg2004;38:70-85
11. Bedrossian E, Stumpel LJ, Beckeley ML, et al: The zygomaticimplant; preliminary data on treatment of severely resorbedmaxillae. A clinical report. Int J Oral Maxillofac Implants2002;17:861-865
12. Bedrossian E, Stumpel LJ: Immediate stabilization at stage II ofzygomatic implants: rational and technique. J Prosthet Dent2001;1:10-14
13. Bedrossian E, Rangert B, Stumpel LJ, et al: Immediate functionwith the zygomatic implant: a graftless solution for patients withmild to advanced atrophy of the maxilla. Int J Oral MaxillofacImplants 2006;21:937-942
14. Malevez C, Abarca M, Durdu F, et al: Clinical outcome of 103consecutive zygomatic implants: a 6-48 months follow-up study.Clin Oral Implants Res 2004;15:18-22
15. Aparicio C, Ouazzani W, Garcia R, et al: A prospective clinicalstudy on titanium implants in the zygomatic arch for prostheticrehabilitation of the atrophic edentulous maxilla with a follow-upof 6 months to 5 years. Clin Implant Dent Relat Res2006;8:114-122
16. Aparicio C, Ouazzani W, Aparicio A, et al: Immediate/Earlyloading of zygomatic implants: clinical experiences after 2 to 5years of follow-up. Clin Implant Dent Relat Res 2010;12 Suppl1:e77-82
Journal of Prosthodontics 26 (2017) 244–251 C© 2016 by the American College of Prosthodontists 251
Related Documents











