INNOVATIONS IN LUNG CANCER TREATMENT JAMES JETT, MD EDWARD KIM, MD DAVID SPIGEL, MD KEVIN OEFFINGER, MD (FACILITATOR) JANUARY 17, 2019 9:00 AM ET

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

INNOVATIONS IN LUNG CANCER TREATMENTJAMES JETT, MD
EDWARD KIM, MD
DAVID SPIGEL, MD
KEVIN OEFFINGER, MD (FACILITATOR)
JANUARY 17, 2019
9:00 AM ET

TODAY’S AGENDA
2
*Sessions will be recorded.*Please mute phones when not speaking. Mute cell phones and try to reduce extraneous noise. *Remember to e-mail Octavia Vogel by 1/21 if you are requesting CME/CEU credit.
Time Presentation Presenter (s)
9:00-9:10 Welcome, roll call, housekeeping Dr. Oeffinger
9:10-9:45 Didactic Presentation:
Part 1: 20 minutes <Title>
Part 2: 15 minutes <Title>
Dr. Kim
Dr. Jett
9:45-10:00 Q & A/Discussion Dr. Oeffinger
10:00-10:15 Program/Case Presentation: Dr. Spigel
10:15-10:25 Q & A/Discussion Dr. Oeffinger
10:25-10:30 Conclusion/Next session Dr. Oeffinger
Dawn Wiatrek, Ph.D.
Octavia Vogel, MPH

DISCLOSURE
UNM CME policy, in compliance with the ACCME Standards of
Commercial Support, requires that anyone who is in a position
to control the content of an activity disclose all relevant financial
relationships they have had within the last 12 months with a
commercial interest related to the content of this activity.
The following planners and faculty disclose that they have no
financial relationships with any commercial interest: (next slide)
3

FACILITATOR & PRESENTERS
Lead Facilitator: Kevin OeffingerDirector, Duke Center for Onco-Primary Care Director, Duke Supportive Care and Survivorship Center Duke Cancer Institute
Presenters: James R. Jett, MD Professor of Medicine, Emeritus National Jewish Health Chief Medical Officer, Oncimmune Ltd Nottingham, United Kingdom.
Edward S. Kim, MD Chair of Solid Tumor Oncology and Investigational TherapeuticsDonald S. Kim Distinguished Chair for Cancer Research Levine Cancer InstituteCarolinas Health Care System, Charlotte, NC
Case Presenter: David Spigel, MDChief Scientific OfficerDirector, Lung Cancer Research ProgramSarah Cannon Health System
4

LEARNING OBJECTIVES
This session will provide information on innovations in lung
cancer treatment including:1. Molecular assessment and targeted therapies
2. Immune checkpoint inhibitors
3. Long term survival rates
4. Implications for treatment decision making
5

Molecular Assessment and Targeted Therapy of Lung Cancer Patients in 2019
Edward S. Kim, M.D., FACP
Chair, Solid Tumor Oncology and Investigational Therapeutics
Medical Director, Clinical Trials Office
Levine Cancer Institute, Atrium Health, Charlotte, NC

L E V I N E C A N C E R I N S T I T U T E
Disclosures
• Consulting
– AstraZeneca
– Boehringer-Ingelheim
– Pfizer
– Roche/Genentech
– Takeda
– Celltrion

L E V I N E C A N C E R I N S T I T U T E
The Era of Precision Medicine
• Genomic Testing– Tissue and blood
• Novel Therapeutics– Small molecules, Immunotherapy
• Less Chemotherapy
• More choices
• People living longer with cancer

L E V I N E C A N C E R I N S T I T U T E
Importance of Clinical Trials
L E V I N E C A N C E R I N S T I T U T E
Must Allow More Patients to Participate

L E V I N E C A N C E R I N S T I T U T E

L E V I N E C A N C E R I N S T I T U T E
NSCLC: A Major Public Health Problem
• Estimated 1.6 million deaths each year worldwide from lung cancer
• In 2015:
• Estimated 221,200 new cases of lung cancer expected to be diagnosed in US
• 158,000 Americans expected to die from lung cancer
• Leading cause of cancer-related deaths in US men and women
• More deaths from lung cancer than breast, prostate, colon, liver, melanoma, and kidney cancers combined
• Need for better thought out, patient-driven studies
Torre LA, et al. CA Cancer J Clin. 2015;65(2):87-108.Siegel RL, et al. CA Cancer J Clin. 2015;65(1):5-29.

L E V I N E C A N C E R I N S T I T U T E
Lung Cancer Treatment 2000:
ECOG 1594 Comparison of 4 First-Line Doublet
Regimens in Advanced NSCLC
• Nonsquamous and squamous histologies
• No differences
• Efficacy not so encouraging
• Easy for providers to “take home a message”
• “Treat with any doublet you would like”
Schiller JH, et al. N Engl J Med. 2002;346:92-98.
Pro
ba
bil
ity o
f S
urv
iva
l

L E V I N E C A N C E R I N S T I T U T E
BATTLE Trial

Erlotinib SorafenibVandetanib Erlotinib + Bexarotene
Randomization:Equal Adaptive
Primary end point: 8 week Disease Control (DC)
Umbrella Protocol
BATTLE Trial Schema
EGFR KRAS/BRAF VEGF RXR/CyclinD1
Core Biopsy
Biomarker Profile
ES Kim et al. Cancer Discovery 2011

The Changing Landscape of Lung Cancer: 200580 of 100 patients eligible for chemotherapy
Only 15-20% of tumors had a partial
response

Molecular subsets: EGFR MutationsThe Changing Landscape of Lung Cancer: 2019

Molecular subsets: ALK
The Changing Landscape of Lung Cancer: 2019

Molecular subsets: ROS1
The Changing Landscape of Lung Cancer: 2019
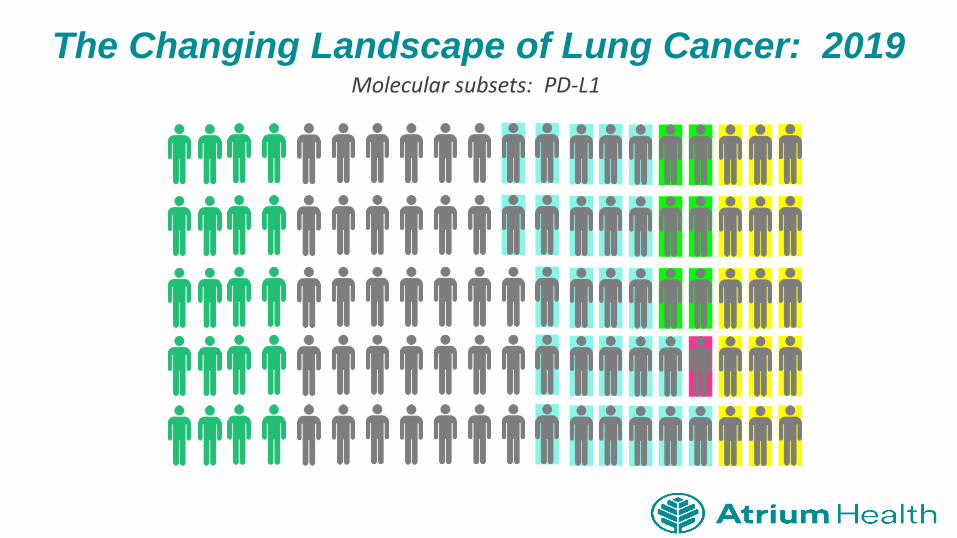
Molecular subsets: PD-L1
The Changing Landscape of Lung Cancer: 2019

Molecular subsets: BRAFv600E
The Changing Landscape of Lung Cancer: 2019

Molecular subsets: 50% of patients candidates for targeted therapy
The Changing Landscape of Lung Cancer: 2019

L E V I N E C A N C E R I N S T I T U T E
NSCLC Drug Approvals/Indications:
2015 - Present• Alectinib
• Necitumumab
• Nivolumab
• Osimertinib
• Gefitinib
• Ramucirumab
• Atezolizumab
• Ceritinib
• Brigatinib
• Dacomitinib
• Pembrolizumab
– PD-L1 + (1st, 2nd line)
– MSI-H or dMMR solid tumors
– NSCLC (Carboplatin + Pemetrexed)
• Crizotinib (ROS1)
• Lorlatinib
• Dabrafenib, Trametinib
• Durvalumab

L E V I N E C A N C E R I N S T I T U T E
Targeted Therapy in 2019
EGFR (10%)
ALK(4%)
ROS1(1%)
BRAF (2%)
2010: Erlotinib2013: Afatinib2015: Gefitinib2015: Osimertinib2018: Dacomitinib201?: Poziotinib
2011: Crizotinib2014: Ceritinib2015: Alectinib2017: Brigatinib2018: Lorlatinib
2015: Crizotinib2018: Lorlatinib201?: Entrectinib
2017:Dabrafenib and Trametinib

L E V I N E C A N C E R I N S T I T U T E

L E V I N E C A N C E R I N S T I T U T E
Osimertinib vs. Pemetrexed Platinum in T790M
Positive EGFR mutant NSCLC

L E V I N E C A N C E R I N S T I T U T E
Osimertinib vs. Pemetrexed Platinum in
T790M Positive EGFR mutant NSCLC

L E V I N E C A N C E R I N S T I T U T E
First-line Osimertinib vs SoC for
EGFR Mutant Advanced NSCLC
(FLAURA)
• Primary endpoint: PFS
• Secondary endpoints including: ORR, DoR, OS, safety
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.
Treatment-naive pts with
advanced NSCLC
adenocarcinoma with an
EGFR exon 19 or 21
mutation,
WHO PS 0/1,
stable CNS mets
permitted
(N = 556)
Osimertinib 80 mg PO daily
(n = 279)
Erlotinib 150 mg or Gefitinib 250 mg
PO daily
(n = 277)
Until disease progression
or unacceptabl
e toxicity
EGFR mutation (del19 vs L858R) and race (Asian vs non-Asian)

L E V I N E C A N C E R I N S T I T U T E
FLAURA: PFS
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.
PF
S (
%)
MosPts at Risk, n
Osimertinib
SoC
100806040200
0 6 9 2112 18 24 27
279277
262239
233197
210152
13978
7137
2610
00
153
178107
42
Osimertinib(n = 279)
SoC(n = 277)
Median PFS, mos 18.9 10.2
HR (95% CI) 0.46 (0.37-0.57); P < .0001

L E V I N E C A N C E R I N S T I T U T E
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.
FLAURA: Overall Survival Interim Analysis

L E V I N E C A N C E R I N S T I T U T E
PFS in Patients w/ & w/out CNS Metastases
Ramalingam S, et al. ESMO 2017. Abstract LBA2_PR.

L E V I N E C A N C E R I N S T I T U T E
Uncommon Mutations: Afatinib
• 3 patients in group 1 achieved complete response
– 1 each with G719X, K739_1744dup6, and L858R+Q709G/V
-100
-80
-60
-40
-20
0
20
40
60
80
100
120
Max
imu
mch
ange
fro
m b
ase
line
(%)
Group 2 (n=14): de novo T790M mutationsT790M alone, T790M+Del19, T790M+L858R, T790M+G719X, T790M+L858R+G719X
Group 1 (n=33): point mutations or duplications in exons 18-21L861Q, G719X, G719X+S768I, G719X+L861Q, E709G or V+L858R, S768I+L858R,
S768I, L861P, P848L, R776H+L858R, L861Q+Del19, K739_1744dup6
Group 3 (n=20): exon 20 insertions

L E V I N E C A N C E R I N S T I T U T E
Alectinib vs crizotinib in treatment-naïve advanced ALK+ NSCLC: primary results of the global phase III ALEX study (LBA9008)
Presented By Alice Shaw at 2017 ASCO Annual Meeting

L E V I N E C A N C E R I N S T I T U T E
Primary endpoint: PFS, investigator-assessed
Presented By Alice Shaw at 2017 ASCO Annual Meeting

L E V I N E C A N C E R I N S T I T U T E
Leptomeningeal carcinomatosis responded to alectinib
Pre-alectinib 6 weeks on alectinib
Pre-alectinib
CSF cytology
Ou, S et al., WCLC 2013

L E V I N E C A N C E R I N S T I T U T E
ROS1+ NSCLC treated with Crizotinib

L E V I N E C A N C E R I N S T I T U T E
BRAF V600E: Dabrafenib and Trametinib
L E V I N E C A N C E R I N S T I T U T E
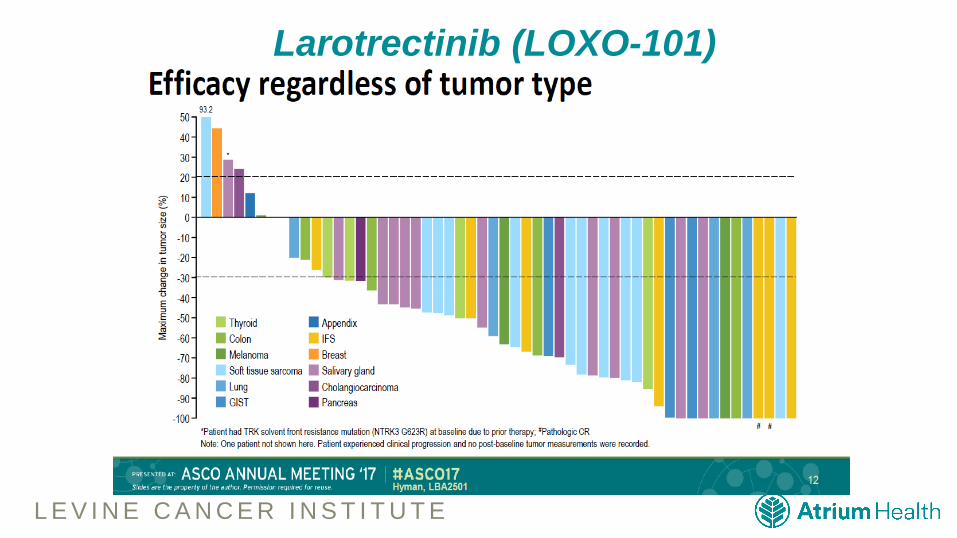
Larotrectinib (LOXO-101)

L E V I N E C A N C E R I N S T I T U T E
Biomarker Recommendations:
Practical Applications
• EGFR
• BRAF
• ALK
• ROS1
• PD-L1
• EGFR T790M (post EGFR-TKI therapy)
• TRK fusions
Biomarkers performed at baseline

L E V I N E C A N C E R I N S T I T U T E
Targeted Agent and Profiling Utilization
Registry (TAPUR) Study
• Pragmatic phase 2 study with FDA-approved, targeted agents
• 60-70% match rates
• Incorporates general and drug-specific eligibility criteria
• Adopted ASCO-Friends Eligibility Criteria

L E V I N E C A N C E R I N S T I T U T E
Drugs Available in TAPUR
Pharmaceutical Company(Number of Drugs)
Drug(s) Provided for TAPUR Study
AstraZeneca (1) Olaparib
Bayer (1) Regorafenib
Bristol-Meyers Squibb (3) Dasatinib, Nivolumab + Ipilimumab
Eli Lilly (1) Cetuximab
Genentech (4) Trastuzumab + Pertuzumab, Vemurafenib + Cobimetinib
Merck (1) Pembrolizumab
Pfizer (6)Axitinib, Bosutinib, Crizotinib, Palbociclib, Sunitinib, Temsirolimus

L E V I N E C A N C E R I N S T I T U T E
HER2 and Breast Cancer Patients
• Would you ever treat a patient with breast cancer without knowing the HER2 status?

L E V I N E C A N C E R I N S T I T U T E
Conclusions: Delivering Precision Medicine
• Must practice Precision Medicine now
• Molecularly-base clinical medicine
– Genomic testing at appropriate points of care
– Reflex biomarker testing, Molecular tumor board
• Blood-based marker testing and collection system-wide
• Cutting-Edge Clinical trials
– ASCO TAPUR, Phase I sites

L E V I N E C A N C E R I N S T I T U T E
The Fight Against Lung Cancer:
Thank you for your attention
ECHO-ACSJanuary 17, 2019
James R. Jett, M.D.
Professor of Medicine, Emeritus
National Jewish Health
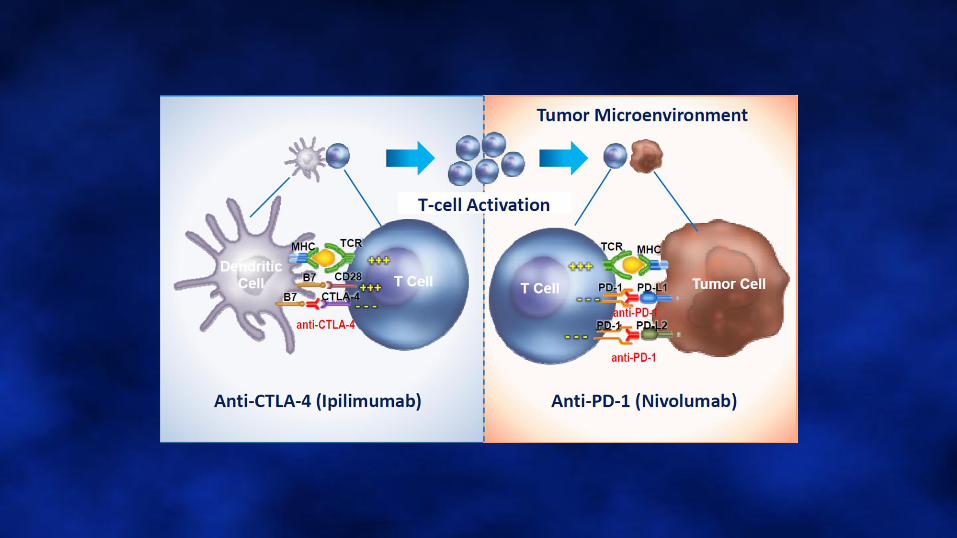

Immune Checkpoint Inhibitors
•Anti PD-1
•Nivolumab*
•Pembrolizumab*
•Anti PD-L1
•Atezolizumab*
•Durvalumab*
•Avelumab
•* FDA approved for NSCLC
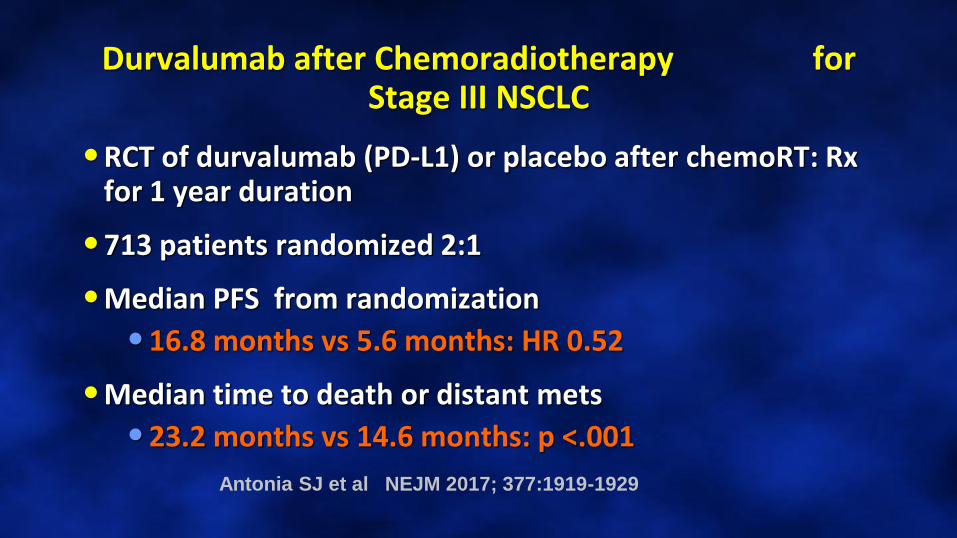
Durvalumab after Chemoradiotherapy for Stage III NSCLC
•RCT of durvalumab (PD-L1) or placebo after chemoRT: Rx for 1 year duration
•713 patients randomized 2:1
•Median PFS from randomization
•16.8 months vs 5.6 months: HR 0.52
•Median time to death or distant mets
•23.2 months vs 14.6 months: p <.001
Antonia SJ et al NEJM 2017; 377:1919-1929

Antonia SJ et al NEJM 2017; 377:1919-1929
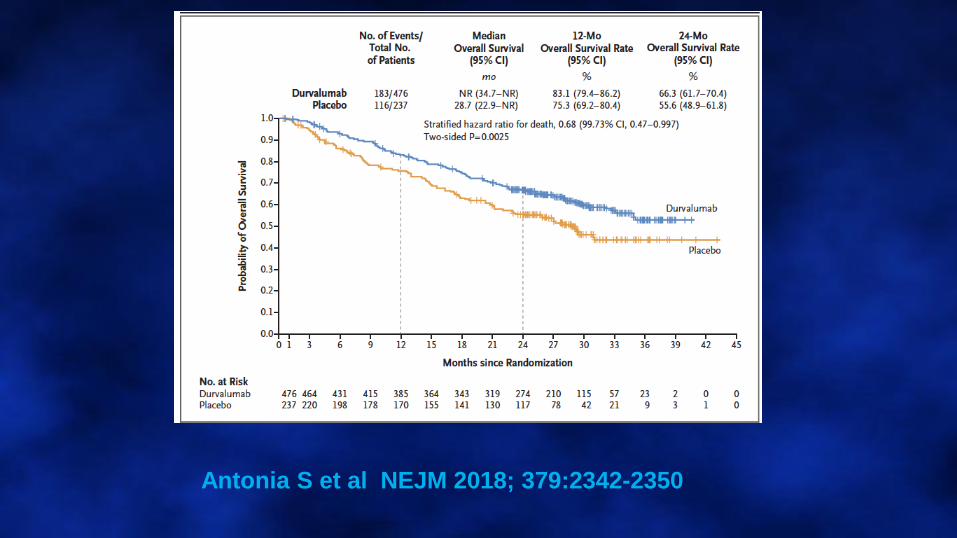
Antonia S et al NEJM 2018; 379:2342-2350

Pembrolizumab in Untreated NSCLC
•Phase III trial of 305 patients with untreated stage IV NSCLC (>50% PD-L1)
•Fixed dose 200mg IV q 3 weeks
•RCT of pembro vs platinum doublet CT
•No EGFR or ALK mutations
•PFS of 10.3 vs 6.0 months ( HR=0.50)
•6 month survival 80 vs 72% (HR 0.60)
Reck et al NEJM 2016; 375:1823-33

Reck et al NEJM 2016; 375:1823-33

Pembrolizumab in Untreated NSCLC
•Response rate: 44.8 vs 27.8%
•Median duration of response
•Not reached (1.9-14.1) vs 6.3 months
•Grade 3+ toxicity: 26.6% vs 53.3%
FDA approved pembrolizumab for frontline treatment in stage IV NSCLC with 50%+ staining of PD-L1 of tumor cells
Reck et al NEJM 2016; 375:1823-33

Reck et al NEJM 2016; 375:1823-33

Gandhi L et al NEJM 2018; 378:2078-2092

Pembro plus Chemotherapy in Nonsquamous NSCLC: KEYNOTE 189
•Phase III trial of pemetrexed and a platinum with or without pembrolizumab
•PFS 8.8 vs 4.9 mos
•Survival at 1-year 69% vs 49%
• Improvement in survival seen in all PD-L1 categories
Gandhi L et al NEJM 2018; 378:2078-2092

Gandhi L et al NEJM 2018; 378:2078-2092

Pembro plus Chemotherapy for Squamous Cell Lung: KEYNOTE 407
Paz-Ares L et al NEJM 2018; 379:2040-2051

Squamous Cell: KEYNOTE 407
Paz-Ares L et al NEJM 2018; 379:2040-2051

Horn L et al NEJM 2018; 379:2220-2229

Atezo in Frontline ED Small Cell
Horn L et al NEJM 2018; 379:2220-2229
Long Term Survival with Stage IV Non-Small Cell Lung Cancer

Five Year Survival in EGFR Mutant Lung Adenocarcinoma Treated with TKIs
•137 patients with metastatic adenoca
•PFS was 12.1 months
•Overall median survival of 30.9 months
•Five year survival of 14.6%
•95% CI of 9.7-21.9%
Lin JJ et al J Thorac Oncol 2016; 11:556-565

Solomon B et al J Clin Oncol pub online May 16, 2018

HR 0.76
HR 0.35
(85%
crossover
)
4 yr
survival
(57 vs 49%)
Solomon B et al J Clin Oncol pub online May 16, 2018

Pembrolizumab and Long Term Survival in Stage IV NSCLC
•KEYNOTE trials with pembrolizumab in second or greater line therapy
•Eval with long term survival models
•Estimated survival beyond 5 years at 21% and 25% in two trials
•With docetaxel long term survival 5%
Hellman MD et al ASCO-SITC Clin Immuno-
Oncology symposium abst #77, 2017

Five Year Survival in NSCLC Responders to Immunotherapy
•F/U of a Phase Ib dose ranging study of advanced NSCLC treated with nivolumab
•Dose excalating study of 129 pts
•Dose cohorts 1mg, 3mg, 10mg/kg
•At 5 years the overall survival was 16%
•5 year survival on docetaxel was 4%
Gettinger S et al J Clin Oncol 2018; 36:1675-1684

In Summary
CASE PRESENTATION
DAVID SPIGEL, MD
69
CASE EXAMPLE
70

CASE RELATED QUESTIONS FOR GROUP DISCUSSION
71

JOIN US FOR LUNG CANCER PATIENT SUPPORT ECHO:
MULTIDISCIPLINARY TEAMS AND CARE COORDINATION IN LUNG
CANCER PATIENT CARE
JANUARY 31, 2019
9:00 AM ET
72
Presenters:Thomas Asfeldt, RN, MAN, MBA
Director, Outpatient Cancer Services & Radiation Oncology, Sanford Health
ACCC Advisory Board Member for the
Optimal Care Coordination Model for Medicaid Patients with Lung Cancer
Peter Mazzone, M.D., MPH
Pulmonologist
Director, Lung Cancer Program
Respiratory Institute, Cleveland Clinic
Wendi Waugh Administrative Director of Cancer Services/Community Health and Wellness
Southern Ohio Medical Center
Pilot site director for the ACCC Optimal Care Coordination Model Pilot Study
Related Documents











