Systemic Response to Systemic Response to Injury & Metabolic Injury & Metabolic Support Support a review of Schwartz’s Principles of a review of Schwartz’s Principles of Surgery- Chapter 1 Surgery- Chapter 1 L. Coughlin, M.D. L. Coughlin, M.D. July 7, 2008 July 7, 2008

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Systemic Response to Systemic Response to Injury & Metabolic Injury & Metabolic
SupportSupporta review of Schwartz’s Principles of a review of Schwartz’s Principles of
Surgery- Chapter 1Surgery- Chapter 1
L. Coughlin, M.D.L. Coughlin, M.D.July 7, 2008July 7, 2008

IntroductionIntroduction
Inflammatory response to injuryInflammatory response to injury to restore tissue functionto restore tissue function Eradicate invading microorganismsEradicate invading microorganisms
Local- limited duration, restores Local- limited duration, restores functionfunction
MajorMajor overwhelming inflammatory responseoverwhelming inflammatory response Potential multi-organ failurePotential multi-organ failure Adversely impacts patient survivalAdversely impacts patient survival

Clinical Spectrum of Clinical Spectrum of SIRSSIRS
InfectionInfection Identifiable source of Identifiable source of
microbial insultmicrobial insult
SIRS = 2 or more:SIRS = 2 or more: Temp ≥38˚C or ≤36˚CTemp ≥38˚C or ≤36˚C HR ≥ 90 bpmHR ≥ 90 bpm RR ≥ 20 breaths/min or RR ≥ 20 breaths/min or
PaCO2 ≤ 32 mmHg or PaCO2 ≤ 32 mmHg or mechanical ventilationmechanical ventilation
WBC ≥ 12,000/µL or ≤ WBC ≥ 12,000/µL or ≤ 4000/µL or ≥ 10% band 4000/µL or ≥ 10% band formsforms
SepsisSepsis Infection + SIRSInfection + SIRS
Severe SepsisSevere Sepsis Sepsis + Organ Sepsis + Organ
DysfunctionDysfunction
Septic ShockSeptic Shock Sepsis + Cardiovascular Sepsis + Cardiovascular
Collapse (requires Collapse (requires vasopressors)vasopressors)

SignalingSignaling
Humoral – inflammatory mediators in the Humoral – inflammatory mediators in the circulation can induce fever and anorexia i.e. circulation can induce fever and anorexia i.e. TNF-TNF-αα
Neural – parasympathetic vagal stimulation Neural – parasympathetic vagal stimulation attenuates the inflammatory response via Ach attenuates the inflammatory response via Ach releaserelease Reduces HR, increases gut motility, dilates Reduces HR, increases gut motility, dilates
arterioles, constricts pupils, and decreases arterioles, constricts pupils, and decreases inflammationinflammation
Reduces macrophage activationReduces macrophage activation Reduces macrophage release of pro-inflammatory Reduces macrophage release of pro-inflammatory
mediators (TNF-mediators (TNF-αα, IL-1, IL-18), IL-1, IL-18)

Hormone SignalingHormone Signaling
Hormone classifications Hormone classifications polypeptide polypeptide (cytokine, insulin)(cytokine, insulin)
amino acid amino acid (epinephrine, serotonin, or histamine(epinephrine, serotonin, or histamine)) fatty acid fatty acid (cortisol, leukotrienes)(cortisol, leukotrienes)
PathwaysPathways Receptor Kinases Receptor Kinases – insulin– insulin
Guanine nucleotide binding (G-protein) Guanine nucleotide binding (G-protein) - - prostaglandinsprostaglandins
Ligand Gated ion channels Ligand Gated ion channels

Adrenocorticotropic Adrenocorticotropic HormoneHormone
Synthesized anterior pituitarySynthesized anterior pituitary Regulated by circadian signalsRegulated by circadian signals Pattern is dramatically altered in injured Pattern is dramatically altered in injured
patientspatients Elevation is proportional to injury severityElevation is proportional to injury severity Released by: pain, anxiety, vasopressin, Released by: pain, anxiety, vasopressin,
angiotensin II, cholecystokinin, angiotensin II, cholecystokinin, catecholamines, and pro-inflammatory catecholamines, and pro-inflammatory cytokinescytokines
ACTH signals increase glucocorticoid ACTH signals increase glucocorticoid productionproduction

GlucocorticoidsGlucocorticoids
Cortisol – elevated following injury, Cortisol – elevated following injury, duration of elevation depends on severity of duration of elevation depends on severity of
injuryinjury Potentiates hyperglycemiaPotentiates hyperglycemia
Hepatic gluconeogenesisHepatic gluconeogenesis Muscle and adipose tissue –> induces insulin Muscle and adipose tissue –> induces insulin
resistanceresistance Skeletal m.–> protein degradation, lactate Skeletal m.–> protein degradation, lactate
releaserelease Adipose -> reduces release of TG, FFA, glycerolAdipose -> reduces release of TG, FFA, glycerol

Exogenous Exogenous administrationadministration
Adrenal suppression in the acutely illAdrenal suppression in the acutely ill Acute Adrenal InsufficiencyAcute Adrenal Insufficiency Atrophy of the adrenal glandsAtrophy of the adrenal glands Weakness, n/v, fever, hypotensionWeakness, n/v, fever, hypotension Hypoglycemia, hyponatremia, hyperkalemiaHypoglycemia, hyponatremia, hyperkalemia
ImmunosuppressionImmunosuppression Thymic involution, decreased T-killer and NK fcn, Thymic involution, decreased T-killer and NK fcn,
graft vs host rxns, delayed hypersensitivity graft vs host rxns, delayed hypersensitivity responses, inability of monocyte intracellular responses, inability of monocyte intracellular killing, inhibition of superoxide reactivity and killing, inhibition of superoxide reactivity and chemotaxis in neutrophilschemotaxis in neutrophils
Down regulates pro-inflammatory cytokine Down regulates pro-inflammatory cytokine production (TNF-production (TNF-αα, IL-1, IL-6), IL-1, IL-6)
Increases anti-inflammatory mediator IL-10Increases anti-inflammatory mediator IL-10 Useful in septic shock, surgical trauma, and CABGUseful in septic shock, surgical trauma, and CABG

Macrophage Inhibitory Macrophage Inhibitory FactorFactor
Glucocorticoid antagonist Glucocorticoid antagonist produced by anterior pituitary & T-produced by anterior pituitary & T-
lymphocyteslymphocytes Reverses immunosuppressive effects Reverses immunosuppressive effects
of glucocorticoidsof glucocorticoids Potentiates G- and G+ septic shockPotentiates G- and G+ septic shock Experimentally improves survivalExperimentally improves survival

Growth HormoneGrowth Hormone
During stress -> protein synth, fat During stress -> protein synth, fat mobilization, and skeletal cartilage growthmobilization, and skeletal cartilage growth
2˚ to release of insulin-like growth factor 2˚ to release of insulin-like growth factor (IGF1)(IGF1)
Injury reduces IGF1 levelsInjury reduces IGF1 levels IGF1 inhibited by pro-inflammatory IGF1 inhibited by pro-inflammatory
cytokinescytokines TNF-TNF-αα, IL-1, IL-1αα, IL-6, IL-6
GH admin to pediatric burn patients shows GH admin to pediatric burn patients shows improvement in their clinical courseimprovement in their clinical course

CatecholaminesCatecholamines Severe injury activates the adrenergic Severe injury activates the adrenergic
systemsystem Norepi and Epi immed. increase 3-4 fold Norepi and Epi immed. increase 3-4 fold
and remain elevated 24-48hrs after injuryand remain elevated 24-48hrs after injury EpinephrineEpinephrine
hepatic glycogenolysis, gluconeogenesis, hepatic glycogenolysis, gluconeogenesis, lipolysis, and ketogenesislipolysis, and ketogenesis
Decreases insulin and glucagon secretionDecreases insulin and glucagon secretion Peripheral- lipolysis, insulin resistance in Peripheral- lipolysis, insulin resistance in
skeletal m.skeletal m. = stress induced hyperglycemia= stress induced hyperglycemia

Epinephrine – other Epinephrine – other effectseffects
Increase secretion of T3, T4, and Increase secretion of T3, T4, and reninrenin
Reduces release of aldosteroneReduces release of aldosterone Enhances leukocyte demargination Enhances leukocyte demargination
and lymphocytosisand lymphocytosis

AldosteroneAldosterone
Synthesized, stored, released from the Synthesized, stored, released from the adrenal zona glomerulosaadrenal zona glomerulosa
Maintains intravascular volumeMaintains intravascular volume Conserves sodiumConserves sodium Eliminates potassium and hydrogen ionsEliminates potassium and hydrogen ions Acts on the early distal convoluted tubulesActs on the early distal convoluted tubules
Deficiency- hypotension, hyperkalemiaDeficiency- hypotension, hyperkalemia Excess- edema, HTN, hypokalemia, Excess- edema, HTN, hypokalemia,
metab alkalosismetab alkalosis

InsulinInsulin Stress inhibited release + peripheral Stress inhibited release + peripheral
insulin resistance = hyperglycemiainsulin resistance = hyperglycemia Injury has 2 phases of insulin releaseInjury has 2 phases of insulin release
Within hours- release is suppressedWithin hours- release is suppressed Later- normal/xs insulin production with Later- normal/xs insulin production with
peripheral insulin resistanceperipheral insulin resistance Activated lymphocytes have insulin Activated lymphocytes have insulin
receptors -> enhanced Tcell proliferation receptors -> enhanced Tcell proliferation and cytotoxicityand cytotoxicity
Tight control of glucose levels esp. in Tight control of glucose levels esp. in diabetics significantly reduces mortality diabetics significantly reduces mortality after injuryafter injury

Acute Phase ProteinsAcute Phase Proteins
Nonspecific markersNonspecific markers Produced by hepatocytesProduced by hepatocytes Response to injury, infection, inflammationResponse to injury, infection, inflammation Induced by IL-6Induced by IL-6 C-reactive protein best reflects C-reactive protein best reflects
inflammationinflammation No diurnal variation, not affected by feedingNo diurnal variation, not affected by feeding Affected only by preexisting hepatic failureAffected only by preexisting hepatic failure Accuracy surpasses that of ESRAccuracy surpasses that of ESR

Inflammatory MediatorsInflammatory Mediators
Heat Shock ProteinsHeat Shock Proteins Reactive Oxygen MetabolitesReactive Oxygen Metabolites EicosanoidsEicosanoids Fatty Acid MetabolitesFatty Acid Metabolites Kallikrein-Kinin SystemKallikrein-Kinin System SerotoninSerotonin HistamineHistamine CytokinesCytokines

Heat Shock ProteinsHeat Shock Proteins
Induced by hypoxia, trauma, heavy Induced by hypoxia, trauma, heavy metals, and hemorrhagemetals, and hemorrhage
Intracellularly modify and transport Intracellularly modify and transport proteinsproteins SteroidsSteroids
Requires gene induction by a Requires gene induction by a transcription factortranscription factor
ACTH sensitiveACTH sensitive Production seems to decline with ageProduction seems to decline with age

Reactive Oxygen Reactive Oxygen MetabolitesMetabolites
Short-livedShort-lived Cause tissue injury by oxidation of Cause tissue injury by oxidation of
unsaturated fatty acids within cell unsaturated fatty acids within cell membranesmembranes
Produced by anaerobic glucose oxidation Produced by anaerobic glucose oxidation and reduction to superoxide anion in and reduction to superoxide anion in leukocytesleukocytes
Further metabolized to hydrogen peroxide Further metabolized to hydrogen peroxide and hydroxyl radicalsand hydroxyl radicals
Cells are protected by oxygen scavengers – Cells are protected by oxygen scavengers – glutathione and catalasesglutathione and catalases
In ischemia- production of oxygen In ischemia- production of oxygen metabolites are activated but nonfunctional metabolites are activated but nonfunctional due to no oxygen supply. After reperfusion, due to no oxygen supply. After reperfusion, large amounts are produced causing injurylarge amounts are produced causing injury

EicosanoidsEicosanoids
Phospholipids
Arachadonic Acid
Cyclic endoperoxidases(PGG2, PGH2)
Hydroperoxyeicosatetraenoic acid(HPETE)
ProstaglandinsPGD2, PGE2, PGF2α, PGI2
ThromboxaneTXA2
Hydroxyeicosatetraenoic Acid HETE
Leukotrienes
Cyclooxygenase 1 & 2 Lipoxygenase
Phospholipase A2 CorticosteroidsGlucocorticoids(Cortisol)

EicosanoidsEicosanoids Secreted by nucleated cells (not lymphocytes)Secreted by nucleated cells (not lymphocytes) Induced by hypoxic injury, direct tissue Induced by hypoxic injury, direct tissue
injury, endotoxin, norepinephrine, injury, endotoxin, norepinephrine, vasopressin, ang II, bradykinin, serotonin, vasopressin, ang II, bradykinin, serotonin, ACh, cytokines, histamineACh, cytokines, histamine
Diverse systemic effectsDiverse systemic effects Adverse effects include acute lung injury, Adverse effects include acute lung injury,
pancreatitis, renal failurepancreatitis, renal failure NSAIDs acetylate COX which reduce NSAIDs acetylate COX which reduce
prostaglandin levelsprostaglandin levels

Eicosanoid EffectsEicosanoid Effects Pancreas – glucagon Pancreas – glucagon
secretion- PGD2, PGE2secretion- PGD2, PGE2 Liver – glucagon stimulated Liver – glucagon stimulated
glucose production- PGE2glucose production- PGE2 Adipose – lipolysis- PGE2Adipose – lipolysis- PGE2 Bone – resorption- PGE2, Bone – resorption- PGE2,
PGF2PGF2αα, PGI2, PGI2 Parathyroid – PTH Parathyroid – PTH
secretion- PGE2secretion- PGE2 Pulmonary – Pulmonary –
Bronchoconstriction- Bronchoconstriction- PGF2PGF2αα, TXA2, LTC4, LTD4, , TXA2, LTC4, LTD4, LTE4LTE4
Immune – suppress Immune – suppress lymphocytes- PGE2lymphocytes- PGE2
Hematologic Hematologic platelet aggregation- TXA2platelet aggregation- TXA2 Capillary leakage- PGE2, Capillary leakage- PGE2,
LTLT PMN adherence and PMN adherence and
activation- LTactivation- LT Pituitary Pituitary
Prolactin- PGE1Prolactin- PGE1 LH- PGE1, PGE2, 5-HETELH- PGE1, PGE2, 5-HETE TSH- PGA1, PGB1, PGE1, TSH- PGA1, PGB1, PGE1,
PGE1PGE1αα GH- PGE1 GH- PGE1
Renal – renin secretion- Renal – renin secretion- PGE2, PGI2PGE2, PGI2
GI – cytoprotective- PGE2GI – cytoprotective- PGE2

Fatty Acid MetabolitesFatty Acid Metabolites Omega 6 FA – precursors of inflammatory Omega 6 FA – precursors of inflammatory
mediators (LT, PG, platelet activating, factor)mediators (LT, PG, platelet activating, factor) found in enteral nutrition formulasfound in enteral nutrition formulas
Substituting Omega 3 FA attenuate the Substituting Omega 3 FA attenuate the inflammatory responseinflammatory response Reduces TNFReduces TNFαα, IL6, PGE2, IL6, PGE2 Reduces the metabolic rater, normalizes glucose Reduces the metabolic rater, normalizes glucose
metabolism, attenuates weight loss, improves metabolism, attenuates weight loss, improves nitrogen balance, reduces endotoxin induced nitrogen balance, reduces endotoxin induced acute lung injury, minimizes reperfusion injury to acute lung injury, minimizes reperfusion injury to the myocardium, small intestine, and skeletal the myocardium, small intestine, and skeletal muscles.muscles.

Kallikrein-Kinin SystemKallikrein-Kinin System
Bradykinins are potent vasodilatorsBradykinins are potent vasodilators Stimulated by hypoxic and ischemic injuryStimulated by hypoxic and ischemic injury
Hemorrhage, sepsis, endotoxemia, tissue injuryHemorrhage, sepsis, endotoxemia, tissue injury Magnitude proportional to severity of injuryMagnitude proportional to severity of injury
Produced by kininogen degradation by Produced by kininogen degradation by kallikreinkallikrein
Kinins increase capillary permeability Kinins increase capillary permeability (edema), pain, inhibit gluconeogenesis, renal (edema), pain, inhibit gluconeogenesis, renal vasodilation, incr bronchoconstrictionvasodilation, incr bronchoconstriction
In clinical trials, bradykinin antagonists help In clinical trials, bradykinin antagonists help reverse G- sepsis, but do not improve survivalreverse G- sepsis, but do not improve survival

SerotoninSerotonin
Present in intestinal chromaffin cells Present in intestinal chromaffin cells & platelets& platelets
Vasoconstriction, Vasoconstriction, bronchoconstriction, platelet bronchoconstriction, platelet aggregationaggregation
Myocardial chronotrope and Myocardial chronotrope and ionotropeionotrope
Unclear role in inflammationUnclear role in inflammation

HistamineHistamine
Stored in neurons, skin, gastric mucosa, Stored in neurons, skin, gastric mucosa, mast cells, basophils, and plateletsmast cells, basophils, and platelets
H1 – bronchoconstriction, increases H1 – bronchoconstriction, increases intestinal motility and myocardial intestinal motility and myocardial contractilitycontractility
H2 – inhibits histamine releaseH2 – inhibits histamine release H1/H2 – hypotension, decreased venous H1/H2 – hypotension, decreased venous
return/peripheral blood pooling, return/peripheral blood pooling, increased capillary permeability, increased capillary permeability, myocardial failure.myocardial failure.

CytokinesCytokines
Most potent mediators of inflammationMost potent mediators of inflammation Local- eradicate microorganisms, promote Local- eradicate microorganisms, promote
wound healingwound healing Overwhelming response- hemodynamic Overwhelming response- hemodynamic
instability (septic shock) or metabolic instability (septic shock) or metabolic derangements (muscle wasting)derangements (muscle wasting)
Uncontrolled- end-organ failure, deathUncontrolled- end-organ failure, death Self-regulatory production of anti-Self-regulatory production of anti-
inflammatory cytokines, but inappropriate inflammatory cytokines, but inappropriate release may render the patient release may render the patient immunocompromised and susceptible to immunocompromised and susceptible to infectioninfection

Tumor Necrosis Factor Tumor Necrosis Factor αα Secreted from monocytes, macrophages, Secreted from monocytes, macrophages,
TcellsTcells Responds early, T ½ < 20minResponds early, T ½ < 20min Potent evocation of cytokine cascadePotent evocation of cytokine cascade Induces muscle catabolism/cachexia, Induces muscle catabolism/cachexia,
coagulation, PGE2, PAF, glucocorticoids, coagulation, PGE2, PAF, glucocorticoids, eicosanoidseicosanoids
Circulating TNF receptors compete with Circulating TNF receptors compete with cellular receptors and may act as a cellular receptors and may act as a counter regulatory system to prevent counter regulatory system to prevent excessive TNF-excessive TNF-αα activity activity

Interleukin-1Interleukin-1
Released by activated macrophages, Released by activated macrophages, endothelial cellsendothelial cells
IL1IL1αα- cell membrane associated- cell membrane associated IL1IL1ββ- circulation- circulation Synergistic with TNF- Synergistic with TNF- αα T ½ = 6 minT ½ = 6 min Induces febrile response by stimulating PG Induces febrile response by stimulating PG
activity in the anterior hypothalamusactivity in the anterior hypothalamus Release of Release of ββ-endorphins after surgery reduce -endorphins after surgery reduce
perception of painperception of pain

Interleukin-2Interleukin-2
Promotes T-lymphocyte proliferation, Promotes T-lymphocyte proliferation, Ig production, gut barrier integrityIg production, gut barrier integrity
T ½ < 10 minT ½ < 10 min Major injury or perioperative blood Major injury or perioperative blood
transfusions reduce IL-2 activity transfusions reduce IL-2 activity leading to a transient leading to a transient immunocompromised stateimmunocompromised state
Regulates lymphocyte apoptosisRegulates lymphocyte apoptosis

Interleukin-4Interleukin-4 Produced by type 2 T Helper lymphocytesProduced by type 2 T Helper lymphocytes Important in antibody-mediated switching Important in antibody-mediated switching
and antigen presentationand antigen presentation Induces class switching to promote IgE & Induces class switching to promote IgE &
IgG4IgG4 Important in allergic and antihelmintic responsesImportant in allergic and antihelmintic responses
Anti-inflammatory- downregulates IL-1, TNF-Anti-inflammatory- downregulates IL-1, TNF-αα, IL-6, IL-8 and oxygen radical production, IL-6, IL-8 and oxygen radical production
Increases macrophage susceptibility to anti-Increases macrophage susceptibility to anti-inflammatory effects of glucocorticoidsinflammatory effects of glucocorticoids

Interleukin-5Interleukin-5
Released from T lymphocytes, Released from T lymphocytes, eosinophils, mast cells and basophilseosinophils, mast cells and basophils
Promotes eosinophil proliferation Promotes eosinophil proliferation and airway inflammationand airway inflammation

Interleukin-6Interleukin-6 Induced by IL-1 and TNF-Induced by IL-1 and TNF-αα Levels are detectable within 60 min of injury, Levels are detectable within 60 min of injury,
peak 4-6 hours, and persist up to 10 dayspeak 4-6 hours, and persist up to 10 days Levels are proportional to extent of tissue Levels are proportional to extent of tissue
injuryinjury Pro-inflammatoryPro-inflammatory
Mediates hepatic acute phase response during Mediates hepatic acute phase response during injury and convalescence injury and convalescence
Induces and prolongs neutrophil activityInduces and prolongs neutrophil activity Anti-inflammatoryAnti-inflammatory
Attenuate TNF-Attenuate TNF-αα and IL-1 activity and IL-1 activity Promote release of circulating TNF- Promote release of circulating TNF- αα receptors & receptors &
IL-1 antagonistsIL-1 antagonists

Interleukin-8Interleukin-8
Released from monocytes, Released from monocytes, macrophages, T lymphocytesmacrophages, T lymphocytes
Activity similar to IL-6Activity similar to IL-6 Chemoattractant for PMNs, Chemoattractant for PMNs,
basophils, eosinophils, and basophils, eosinophils, and lymphocytes, activates PMNslymphocytes, activates PMNs
Proposed biomarker for risk of Proposed biomarker for risk of multiple organ failuremultiple organ failure

Interleukin-10Interleukin-10
Anti-inflammatoryAnti-inflammatory Released from T lymphocytesReleased from T lymphocytes Down-regulates TNF-Down-regulates TNF-αα activity activity Also attenuates IL-18 mRNA in Also attenuates IL-18 mRNA in
monocytesmonocytes Studies in animal sepsis and ARDS Studies in animal sepsis and ARDS
models suggest induced IL-10 models suggest induced IL-10 decreases the systemic inflammatory decreases the systemic inflammatory response and reduces mortalityresponse and reduces mortality

Interleukin-12Interleukin-12
Promotes differentiation of type 1 T Promotes differentiation of type 1 T Helper cellsHelper cells
Promotes PMN and coagulation activationPromotes PMN and coagulation activation In primate studies, IL-12 induces In primate studies, IL-12 induces
inflammatory responses independent of inflammatory responses independent of TNF-TNF-αα and IL-1 and IL-1
In animal studies of fecal peritonitis and In animal studies of fecal peritonitis and burns, IL-12 administration increases burns, IL-12 administration increases survival, whereas IL-12 neutralization survival, whereas IL-12 neutralization increases mortalityincreases mortality

Interleukin-13Interleukin-13
Similar to IL-4, overall anti-Similar to IL-4, overall anti-inflammatoryinflammatory
Modulates macrophage functionModulates macrophage function Unlike IL-4, has no effect on T Unlike IL-4, has no effect on T
lymphocyteslymphocytes Inhibits NO production Inhibits NO production Inhibits pro-inflammatory cytokinesInhibits pro-inflammatory cytokines Attenuates leukocyte interaction with Attenuates leukocyte interaction with
activated endothelial surfacesactivated endothelial surfaces

Interleukin-15Interleukin-15
Derived from macrophagesDerived from macrophages Shares receptor components with IL-Shares receptor components with IL-
2, and shares promoting lymphocyte 2, and shares promoting lymphocyte activation/prolif.activation/prolif.
In neutrophils, it induces IL-8 and In neutrophils, it induces IL-8 and nuclear factor nuclear factor ккB -> enhanced B -> enhanced phagocytosis against fungal phagocytosis against fungal infectionsinfections

Interleukin-18Interleukin-18
Formerly IFN-Formerly IFN-γγ-inducing factor-inducing factor Produced by macrophagesProduced by macrophages Pro-inflammatory, similar to IL-12Pro-inflammatory, similar to IL-12 Increased levels are pronounced Increased levels are pronounced
(especially in G- sepsis) and can last (especially in G- sepsis) and can last up to 21 daysup to 21 days

Interferon-Interferon-γγ
Helper T lymphocytes activated by bacterial Helper T lymphocytes activated by bacterial antigens, IL-2, IL-12, or IL-18 produce IFN-antigens, IL-2, IL-12, or IL-18 produce IFN-γγ
IFN-IFN-γγ can induce IL-2, IL-12, or IL-18 can induce IL-2, IL-12, or IL-18 Detectable in circulation by 6 hrs and Detectable in circulation by 6 hrs and
remain elevated for up to 8 daysremain elevated for up to 8 days Activate circulating and tissue macrophagesActivate circulating and tissue macrophages Induces acute lung inflammation by Induces acute lung inflammation by
activating alveolar macrophages after activating alveolar macrophages after surgery or traumasurgery or trauma

Granulocyte-Macrophage Granulocyte-Macrophage Colony-Stimulating FactorColony-Stimulating Factor
Delays apoptosis of macrophages and PMNsDelays apoptosis of macrophages and PMNs Promotes the maturation and recruitment of Promotes the maturation and recruitment of
PMNs in inflammation and perhaps wound PMNs in inflammation and perhaps wound healinghealing
May contribute to organ injury such as May contribute to organ injury such as ARDSARDS
Peri-operative GM-CSF undergoing major Peri-operative GM-CSF undergoing major oncologic procedures and burn patients oncologic procedures and burn patients demonstrate enhances neutrophil counts demonstrate enhances neutrophil counts and fcnand fcn

High Mobility Group Box High Mobility Group Box 11
DNA transcription factorDNA transcription factor Expressed 24-48 hrs after injuryExpressed 24-48 hrs after injury Associated with weight loss, food Associated with weight loss, food
aversion, shock, SIRS and Sepsisaversion, shock, SIRS and Sepsis Peak levels are associated with Peak levels are associated with
ARDS and deathARDS and death

Cell Signaling PathwaysCell Signaling Pathways
Heat Shock ProteinsHeat Shock Proteins produced in response to ischemia/injuryproduced in response to ischemia/injury HS Factors are activated upon injury, undergo HS Factors are activated upon injury, undergo
conformational changes, translocate into the conformational changes, translocate into the nucleus, and bind HSP promoter regionsnucleus, and bind HSP promoter regions
Attenuate inflammatory responseAttenuate inflammatory response Ligand Gated Ion ChannelsLigand Gated Ion Channels
When activated by a ligand, a rapid influx of When activated by a ligand, a rapid influx of ions cross the cell membrane. i.e. ions cross the cell membrane. i.e. neurotransmittersneurotransmitters

Cell Signaling PathwaysCell Signaling Pathways G-protein receptorsG-protein receptors
Largest family of signaling receptorsLargest family of signaling receptors Adjacent effector protein activated receptorAdjacent effector protein activated receptor Second messengers – cAMP or calciumSecond messengers – cAMP or calcium Can result in gene transcription or activation of Can result in gene transcription or activation of
phospholipase Cphospholipase C Tyrosine KinasesTyrosine Kinases
When activated, receptors dimerize, When activated, receptors dimerize, phosphorylate, and recruit secondary signaling phosphorylate, and recruit secondary signaling molecules molecules
Used in gene transcription and cell proliferationUsed in gene transcription and cell proliferation i.e. insulin, PGDF, IGF-1i.e. insulin, PGDF, IGF-1

Cell Signaling PathwaysCell Signaling Pathways
Janus Kinase/Signal Transduction and Janus Kinase/Signal Transduction and Activator of Transcription (JAK-STAT)Activator of Transcription (JAK-STAT) IL-6, IL-10, IL-12, IL-13, IFN-IL-6, IL-10, IL-12, IL-13, IFN-γγ Ligand binds to the receptor, receptor dimerizes, Ligand binds to the receptor, receptor dimerizes,
enzymatic activation via phosphorylation enzymatic activation via phosphorylation propagates through the JAK domain and recruits propagates through the JAK domain and recruits STAT to the cytosolic receptor portion. STAT to the cytosolic receptor portion.
STAT dimerizes and translocates into the nucleus STAT dimerizes and translocates into the nucleus as a transcription factoras a transcription factor
Suppressors of cytokine signaling (SOCS) block Suppressors of cytokine signaling (SOCS) block JAK-STATJAK-STAT

Tumor Necrosis FactorTumor Necrosis Factor
Apoptosis - normal fcn of cellular disposal Apoptosis - normal fcn of cellular disposal w/o activating the immune/inflammatory w/o activating the immune/inflammatory systemsystem
2 receptors2 receptors TNFR-1 : inflammation, apoptosis, circulatory TNFR-1 : inflammation, apoptosis, circulatory
shockshock TNFR-2 : no inflammation or shockTNFR-2 : no inflammation or shock
CD95 (Fas) receptor similar structure to CD95 (Fas) receptor similar structure to TNFR-1TNFR-1 Initiates apoptosisInitiates apoptosis

Cell Mediated Cell Mediated InflammationInflammation
PlateletsPlatelets Source of eicosanoids and vasoactive Source of eicosanoids and vasoactive
mediatorsmediators Clot is a chemoattractant for PMNs/monocytesClot is a chemoattractant for PMNs/monocytes Modulate PMN endothelium adherenceModulate PMN endothelium adherence Migration occurs within 3 hrs of injury Migration occurs within 3 hrs of injury
Mediated by serotonin, PAF, PGE2Mediated by serotonin, PAF, PGE2 EosinophilsEosinophils
Migrate to parasitic infection and allergen Migrate to parasitic infection and allergen challenge to release cytotoxic granuleschallenge to release cytotoxic granules
Reside in the GI, lung, and GU tissuesReside in the GI, lung, and GU tissues Activated by IL-3, GM-CSF, IL-5, PAF, and Activated by IL-3, GM-CSF, IL-5, PAF, and
anaphylatoxins C3a and C5aanaphylatoxins C3a and C5a

Cell Mediated Cell Mediated InflammationInflammation
LymphocytesLymphocytes T-helpers produce IL-3, TNF-T-helpers produce IL-3, TNF-αα, GM-CSF , GM-CSF
TH1: IFN-TH1: IFN-γγ, IL-2, IL-12, IL-2, IL-12 TH2: IL-4, IL-5, IL-6, IL-9, IL-10, IL-13TH2: IL-4, IL-5, IL-6, IL-9, IL-10, IL-13 Severe infection – shift toward more TH2Severe infection – shift toward more TH2
Mast CellsMast Cells First responders to injuryFirst responders to injury Produce histamine, cytokines, eicosanoids, Produce histamine, cytokines, eicosanoids,
proteases, chemokines, TNF-proteases, chemokines, TNF-αα (stored in granules) (stored in granules) Cause vasodilation, capillary leakage, and recruit Cause vasodilation, capillary leakage, and recruit
immunocytesimmunocytes

Cell Mediated Cell Mediated InflammationInflammation
MonocytesMonocytes Downregulation of receptor TNFR is clinically Downregulation of receptor TNFR is clinically
and experimentally correlated with CHF, and experimentally correlated with CHF, nonsurvival in sepsisnonsurvival in sepsis
NeutrophilsNeutrophils Modulate acute inflammationModulate acute inflammation Maturation is stimulated by G-CSFMaturation is stimulated by G-CSF Rolling (L-selectin (fast), P-selectin (slow)Rolling (L-selectin (fast), P-selectin (slow) Adhesion/transmigration – ICAM 1, 2, PECAM Adhesion/transmigration – ICAM 1, 2, PECAM
1, VCAM 1, CD181, VCAM 1, CD18

Endothelium-Mediated Endothelium-Mediated InjuryInjury
Neutrophil-Endothelium InteractionNeutrophil-Endothelium Interaction Increased vascular permeability – facilitate Increased vascular permeability – facilitate
oxygen delivery and immunocyte migrationoxygen delivery and immunocyte migration Accumulation of neutrophils at injury sites Accumulation of neutrophils at injury sites
can cause cytotoxicity to vital organscan cause cytotoxicity to vital organs Ischemia-reperfusion injury potentiates Ischemia-reperfusion injury potentiates
this response by releasing oxygen this response by releasing oxygen metabolites and lysosomal enz.metabolites and lysosomal enz.
Neutrophils – rolling 10-20min (p-selectin), Neutrophils – rolling 10-20min (p-selectin), >20min>20min

Nitric OxideNitric Oxide
Derived from endothelial surfaces Derived from endothelial surfaces responding to Ach, hypoxia, endotoxin, responding to Ach, hypoxia, endotoxin, cellular injury, or shear stresses of cellular injury, or shear stresses of circulating bloodcirculating blood
T ½ = secondsT ½ = seconds Reduces microthrombosis, mediates Reduces microthrombosis, mediates
protein synthesis in hepatocytesprotein synthesis in hepatocytes Formed from oxidation of L-arginine Formed from oxidation of L-arginine
via NOS (+calmodulin, Ca2+, NADPH)via NOS (+calmodulin, Ca2+, NADPH)

Prostacyclin (PGI2)Prostacyclin (PGI2)
Endothelium derived in response to Endothelium derived in response to shear stress and hypoxiashear stress and hypoxia
VasodilatorVasodilator Platelet deactivation (increases Platelet deactivation (increases
cAMP)cAMP) Clinically used to reduce pulmonary Clinically used to reduce pulmonary
hypertension (especially pediatric)hypertension (especially pediatric)

EndothelinsEndothelins
Produced as a response to a variety Produced as a response to a variety of factors – injury, anoxia, thrombin, of factors – injury, anoxia, thrombin, IL-1, vasopressin IL-1, vasopressin
ET-1 is a potent vasoconstrictor, 10x ET-1 is a potent vasoconstrictor, 10x more potent than angiotensin IImore potent than angiotensin II

Platelet Activating Platelet Activating FactorFactor
Phospholipid component of cell Phospholipid component of cell membranes, constitutively expressed at membranes, constitutively expressed at low levelslow levels
Released by PMNs, platelets, mast cells, Released by PMNs, platelets, mast cells, monocytes during acute inflammationmonocytes during acute inflammation
Further activates PMNs and plateletsFurther activates PMNs and platelets Increases vascular permeabilityIncreases vascular permeability PAF antagonists reduce PAF antagonists reduce
ischemia/reperfusion injuryischemia/reperfusion injury

Metabolism During Metabolism During FastingFasting
Comparable to changes Comparable to changes seen in acute injuryseen in acute injury
Requires 25-40 Requires 25-40 kcal/kg/day of carbs, kcal/kg/day of carbs, protein, fatprotein, fat
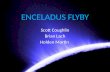
Normal adult body Normal adult body contains 300-400g contains 300-400g carbs (glycogen) – 75-carbs (glycogen) – 75-100g hepatic, 200-250g 100g hepatic, 200-250g muscle (not available muscle (not available systemically due to systemically due to deficiency of G6P)deficiency of G6P)
Mass Mass (kg)(kg)
Energy Energy (Kcal)(Kcal)
Days Days AvailabAvailablele
WaterWater 4949 00 00
ProteinProtein 66 24,00024,000 1313
GlycogGlycogenen
0.20.2 800800 0.40.4
FatFat 1515 140,00140,0000
7878
TotalTotal 70.270.2 164,80164,8000
91.491.4

Metabolism During Metabolism During FastingFasting
A healthy 70kg adult will use 180 g /d A healthy 70kg adult will use 180 g /d of glucose to support obligate of glucose to support obligate glycolytic cells (neurons, RBCs, PMNs, glycolytic cells (neurons, RBCs, PMNs, renal medulla, skeletal m.)renal medulla, skeletal m.)
Glucagon, Norepi, vasopressin, AngII Glucagon, Norepi, vasopressin, AngII promote utilization of glycogen stores promote utilization of glycogen stores
Glucagon, Epi, and cortisol promote Glucagon, Epi, and cortisol promote gluconeogenesisgluconeogenesis
Precursors include lactate (sk.m., rbc, Precursors include lactate (sk.m., rbc, pmn), glycerol, and aa (ala, glutamine)pmn), glycerol, and aa (ala, glutamine)

Metabolism of Simple Metabolism of Simple StarvationStarvation
Lactate is not sufficient for glucose Lactate is not sufficient for glucose demandsdemands
Protein must be degraded (75 g/d) Protein must be degraded (75 g/d) for hepatic gluconeogenesisfor hepatic gluconeogenesis
Proteolysis from decreased insulin Proteolysis from decreased insulin and increased cortisoland increased cortisol
Elevated urinary nitrogen (7 -> 30 Elevated urinary nitrogen (7 -> 30 g/d)g/d)

Metabolism of Prolonged Metabolism of Prolonged StarvationStarvation
Proteolysis is reduced to 20g/d and Proteolysis is reduced to 20g/d and urinary nitrogen excretion stabilizes to 2-urinary nitrogen excretion stabilizes to 2-5g/d5g/d
Organs (myocardium, brain, renal cortex, Organs (myocardium, brain, renal cortex, sk.m) adapt to ketone bodies in 2-24 dayssk.m) adapt to ketone bodies in 2-24 days
Kidneys utilize glutamine and glutamate Kidneys utilize glutamine and glutamate in gluconeogenesisin gluconeogenesis
Adipose stores provide up to 40% calories Adipose stores provide up to 40% calories (approx 160 g FFA and glycerol)(approx 160 g FFA and glycerol) Stimulated by reduced insulin and increased Stimulated by reduced insulin and increased
glucagon and catecholaminesglucagon and catecholamines

Metabolism Following Metabolism Following InjuryInjury
Magnitude of expenditure is Magnitude of expenditure is proportional to the severity of injuryproportional to the severity of injury
Changes in Changes in Lipid AbsorptionLipid Absorption Lipid OxidationLipid Oxidation Carbohydrate metabolismCarbohydrate metabolism

Lipid AbsorptionLipid Absorption Oxidation of 1g fat = 9 kcal energyOxidation of 1g fat = 9 kcal energy Dietary lipids require pancreatic lipase and Dietary lipids require pancreatic lipase and
phospholipase to hydrolyze TG into FFA and phospholipase to hydrolyze TG into FFA and monoglycerides within the duodenummonoglycerides within the duodenum
After gut absorption, enterocytes resynthesize TG After gut absorption, enterocytes resynthesize TG from monoglycerides + fatty acyl-CoAfrom monoglycerides + fatty acyl-CoA
Long chain TG (>12 carbons) enter the circulation Long chain TG (>12 carbons) enter the circulation as chylomicrons. Shorter FA chains directly enter as chylomicrons. Shorter FA chains directly enter portal circulation and are transported via albuminportal circulation and are transported via albumin
Under stress, hepatocytes utilize FFA as fuelUnder stress, hepatocytes utilize FFA as fuel Systemically TG and chylomicrons are used from Systemically TG and chylomicrons are used from
hydrolysis with lipoprotein lipase (suppressed by hydrolysis with lipoprotein lipase (suppressed by trauma and sepsis)trauma and sepsis)

Fatty Acid OxidationFatty Acid Oxidation FFA + acyl-CoA = LCT are transported FFA + acyl-CoA = LCT are transported
across the mitochondrial inner membrane across the mitochondrial inner membrane via the carnitine shuttlevia the carnitine shuttle
Medium-chain TG (MCT) 6-12 carbons Medium-chain TG (MCT) 6-12 carbons long, freely cross the mitochondrial long, freely cross the mitochondrial membranemembrane
Fatty acyl-CoA undergoes Fatty acyl-CoA undergoes ββ-oxidation to -oxidation to acetyl-CoA to enter TCA cycle for acetyl-CoA to enter TCA cycle for oxidation to ATP, CO2, and wateroxidation to ATP, CO2, and water
Excess acetyl-CoA is used for ketogenesisExcess acetyl-CoA is used for ketogenesis

Carbohydrate Carbohydrate MetabolismMetabolism
Carbohydrates + pancreatic intestinal Carbohydrates + pancreatic intestinal enzymes yield dimeric units (sucrase, enzymes yield dimeric units (sucrase, lactase, maltase)lactase, maltase)
Intestinal brush border disaccharidases Intestinal brush border disaccharidases break them into simple hexose units which break them into simple hexose units which are transported into the intestinal mucosaare transported into the intestinal mucosa
Glucose and galactose are absorbed via a Glucose and galactose are absorbed via a sodium dependent active transport pumpsodium dependent active transport pump
Fructose absorption via facilitated diffusionFructose absorption via facilitated diffusion

Carbohydrate Carbohydrate MetabolismMetabolism
1g carbohydrate = 4 kcal energy1g carbohydrate = 4 kcal energy IV/parenteral nutrition 3.4 kcal/g IV/parenteral nutrition 3.4 kcal/g
dextrosedextrose In surgical patients dextrose In surgical patients dextrose
administration is to minimize muscle administration is to minimize muscle wastingwasting
Glucose can be utilized in a variety of Glucose can be utilized in a variety of pathways – phosphorylation to G6P then pathways – phosphorylation to G6P then glycogenesis or glycogenolysis, pyruvic glycogenesis or glycogenolysis, pyruvic acid pathway, or pentose shuntacid pathway, or pentose shunt

Protein and Amino Acid Protein and Amino Acid MetabolismMetabolism
Average adult protein intake 80-120 Average adult protein intake 80-120 g/dayg/day every 6 g protein yields 1 g nitrogenevery 6 g protein yields 1 g nitrogen 1g protein = 4 kcal energy1g protein = 4 kcal energy
Following injury, glucocorticoids Following injury, glucocorticoids increase urinary nitrogen excretion increase urinary nitrogen excretion (>30g/d), peak at 7d, persist 3-7 (>30g/d), peak at 7d, persist 3-7 wkswks

Nutrition in the Surgical Nutrition in the Surgical PatientPatient
Nutritional assessment to determine the Nutritional assessment to determine the severity of deficiencies/excessseverity of deficiencies/excess
Wt loss, chronic illnesses, dietary habits, Wt loss, chronic illnesses, dietary habits, quality/quantity of food, social habits, quality/quantity of food, social habits, medsmeds
Physical exam – loss of muscle/adipose Physical exam – loss of muscle/adipose tissue, organ dysfunctiontissue, organ dysfunction
Biochemical – Cr excretion, albumin, Biochemical – Cr excretion, albumin, prealbumin, total lymphocyte count, prealbumin, total lymphocyte count, transferrintransferrin

Surgical NutritionSurgical Nutrition
Support the requirements for protein synthesisSupport the requirements for protein synthesis Nonprotein calorie : nitrogen ratio = 150:1Nonprotein calorie : nitrogen ratio = 150:1 A lower rate of 80-100:1 may be beneficial in A lower rate of 80-100:1 may be beneficial in
some critically ill or hypermetabolic patients some critically ill or hypermetabolic patients
Basal Energy Expenditure (BEE):Basal Energy Expenditure (BEE):men = 66.47 + 13.75(W) + 5(H) – 6.76(A) kcal/dmen = 66.47 + 13.75(W) + 5(H) – 6.76(A) kcal/d
women = 655.1 + 9.56(W) + 1.85(H) – 4.68 (A) kcal/dwomen = 655.1 + 9.56(W) + 1.85(H) – 4.68 (A) kcal/d
W= wt in kg, H= Ht in cm, A= age W= wt in kg, H= Ht in cm, A= age in yearsin years

Enteral FeedingEnteral Feeding
Less expensive and risks than parenteralLess expensive and risks than parenteral Reduced intestinal atrophyReduced intestinal atrophy 44% reduction in infections over 44% reduction in infections over
parenteral in the critically illparenteral in the critically ill Healthy patients without malnutrition Healthy patients without malnutrition
undergoing uncomplicated surgery can undergoing uncomplicated surgery can tolerate 10 d of maintenance IV fluids tolerate 10 d of maintenance IV fluids only before significant protein catabolism only before significant protein catabolism beginsbegins

Initiation of Enteral Initiation of Enteral FeedingFeeding
Immediately after adequate fluid Immediately after adequate fluid resuscitation (UOP)resuscitation (UOP)
Not absolute prerequisites: presence Not absolute prerequisites: presence of bowel sounds, passage of flatus or of bowel sounds, passage of flatus or stoolstool
Gastric residuals of >200ml in 4-6 Gastric residuals of >200ml in 4-6 hrs or abdominal distention requires hrs or abdominal distention requires cessation/lowering the ratecessation/lowering the rate

Enteral FormulasEnteral Formulas
Low-residue isotonic Low-residue isotonic caloric density 1.0kcal/ml, 1500-1800 ml/daycaloric density 1.0kcal/ml, 1500-1800 ml/day Provide carbs, protein, lytes, water, fat, water Provide carbs, protein, lytes, water, fat, water
sol vitamins, calorie:Nitrogen of 150:1.sol vitamins, calorie:Nitrogen of 150:1. No fiber bulk = minimum residueNo fiber bulk = minimum residue Standard for stable patients with an intact GI Standard for stable patients with an intact GI
tracttract Isotonic with fiberIsotonic with fiber
Soluble and insoluble fiber (soy)Soluble and insoluble fiber (soy) Delay GI transit time and reduce diarrheaDelay GI transit time and reduce diarrhea Not contraindicated in the critically illNot contraindicated in the critically ill

Enteral FormulasEnteral Formulas Immune-EnhancingImmune-Enhancing
Glutamine, argenine, omega-3 FA, nucleotides, beta-Glutamine, argenine, omega-3 FA, nucleotides, beta-carotene.carotene.
Benefits not consistent in trialsBenefits not consistent in trials ExpensiveExpensive
Calorie-DenseCalorie-Dense 1.5-2 kcal/ml, higher osmolality (ok for intragastric 1.5-2 kcal/ml, higher osmolality (ok for intragastric
feeding)feeding) for fluid restriction/inability to tolerate larger for fluid restriction/inability to tolerate larger
volumesvolumes High-ProteinHigh-Protein
Isotonic and nonisotonic availableIsotonic and nonisotonic available calorie:Nitrogen ratio of 80-120:1calorie:Nitrogen ratio of 80-120:1

Enteral FormulasEnteral Formulas ElementalElemental
Contain predigested nutrients, small peptidesContain predigested nutrients, small peptides Limited complex carbs and fat (long/med Limited complex carbs and fat (long/med
chains)chains) Easily absorbed, but limited long term useEasily absorbed, but limited long term use High osmolality = slow infusion or dilutedHigh osmolality = slow infusion or diluted Expensive Expensive
Renal-FailureRenal-Failure Lower fluid volume, K, phos, and MgLower fluid volume, K, phos, and Mg Essential aa, high calorie : nitrogen ratio, no Essential aa, high calorie : nitrogen ratio, no
vitaminsvitamins

Enteral FormulasEnteral Formulas
Pulmonary-FailurePulmonary-Failure Fat content is increased to 50% of total Fat content is increased to 50% of total
caloriescalories Reduces CO2 production and ventilation Reduces CO2 production and ventilation
burdenburden Hepatic-FailureHepatic-Failure
50% of aa are branched chains (Leu, Ile, 50% of aa are branched chains (Leu, Ile, Val)Val)
Potentially reverses encephalopathyPotentially reverses encephalopathy Controversial, no clear benefits in trialsControversial, no clear benefits in trials

Enteral AccessEnteral Access Nasogastric Tube - requires intact mental status Nasogastric Tube - requires intact mental status
and laryngeal reflexes to reduce aspirationand laryngeal reflexes to reduce aspiration Difficult to place, requires radiographic confirmationDifficult to place, requires radiographic confirmation If required >30 d, convert to PEGIf required >30 d, convert to PEG Problems: clogging, kinking, inadvertent removalProblems: clogging, kinking, inadvertent removal
Percutaneous Endoscopic Gastrostomy – Percutaneous Endoscopic Gastrostomy – Impaired swallowing/obstruction, major facial trauma Impaired swallowing/obstruction, major facial trauma Contraindications: ascites, coagulophathy, gastric Contraindications: ascites, coagulophathy, gastric
varices, gastric neoplasm, lack of suitable locationvarices, gastric neoplasm, lack of suitable location Tubes can be use for 12-24 mosTubes can be use for 12-24 mos Requires endoscopic transillumination of abdominal wall Requires endoscopic transillumination of abdominal wall
and passage of catheter into an insufflated stomachand passage of catheter into an insufflated stomach Complications in 3% of cases: infection, peritonitis, Complications in 3% of cases: infection, peritonitis,
aspiration/pneumonia, leaks, dislodgement, bowel aspiration/pneumonia, leaks, dislodgement, bowel perforation, enteric fistulas, bleedingperforation, enteric fistulas, bleeding

Percutaneous Endoscopic Percutaneous Endoscopic Gastrostomy-JejunostomyGastrostomy-Jejunostomy
Feeding administered past the pylorusFeeding administered past the pylorus Cannot tolerate gastric feedings/signif Cannot tolerate gastric feedings/signif
aspirationaspiration Passes a catheter through an existing Passes a catheter through an existing
PEG past the pylorus into the PEG past the pylorus into the duodenumduodenum
Long term malfunction >50% due to Long term malfunction >50% due to retrograde tube migration into the retrograde tube migration into the stomach, kinking, cloggingstomach, kinking, clogging

Direct Percutaneous Direct Percutaneous Endoscopic JejunostomyEndoscopic Jejunostomy
Same technique as PEG placement Same technique as PEG placement but requires an but requires an enteroscope/colonscope to reach the enteroscope/colonscope to reach the jejunumjejunum
Less malfunction than PEG-J Less malfunction than PEG-J Kinking/clogging reduced by placing Kinking/clogging reduced by placing
larger caliber catheterslarger caliber catheters

Surgical Gastrostomy and Surgical Gastrostomy and JejunostomyJejunostomy
With complex abdominal With complex abdominal trauma/laparatomy there may be an trauma/laparatomy there may be an opportunity for placementopportunity for placement
Contraindication: distal obstruction, Contraindication: distal obstruction, severe intestinal wall edema, radiation severe intestinal wall edema, radiation enteritis, inflammatory bowel disease, enteritis, inflammatory bowel disease, ascites, severe immunodeficiency, bowel ascites, severe immunodeficiency, bowel ischemiaischemia
Adverse effects: abdominal/bowel Adverse effects: abdominal/bowel distention, cramps, pneumotosis distention, cramps, pneumotosis intestinalis, small bowel necrosisintestinalis, small bowel necrosis

Parenteral NutritionParenteral Nutrition
Continuous infusion of hyperosmolar Continuous infusion of hyperosmolar carbs, proteins, fats and other nutrients carbs, proteins, fats and other nutrients through a catheter into the SVCthrough a catheter into the SVC
Optimal > 100-150 kcal/g nitrogens Optimal > 100-150 kcal/g nitrogens Higher rates of infection compared to Higher rates of infection compared to
enteralenteral Studies with parenteral nutrition and Studies with parenteral nutrition and
complete bowel rest results in increased complete bowel rest results in increased stress hormone and inflammatory stress hormone and inflammatory responsesresponses

Parenteral Nutrition Parenteral Nutrition RationaleRationale
Seriously ill patients with malnutrition, Seriously ill patients with malnutrition, sepsis or surgery/trauma when use of sepsis or surgery/trauma when use of the GI tract for feeding is not possiblethe GI tract for feeding is not possible Short bowel syndrome after massive Short bowel syndrome after massive
resectionresection Prolonged paralytic ileus (>7 days)Prolonged paralytic ileus (>7 days) Severe intestinal malabsorptionSevere intestinal malabsorption Functional GI disorders – esophageal Functional GI disorders – esophageal
dyskinesiadyskinesia Etc.Etc.

Total Parenteral Total Parenteral NutritionNutrition
Central parenteral nutrition, aka Central parenteral nutrition, aka TPNTPN
Requires access to a large diameter Requires access to a large diameter veinvein
Dextrose content is high (15-25%)Dextrose content is high (15-25%)

Peripheral Parenteral Peripheral Parenteral NutritionNutrition
Lower osmolalityLower osmolality Reduced dextrose (5-10%)Reduced dextrose (5-10%) Protein (3%)Protein (3%) Not appropriate for severe Not appropriate for severe
malnutrition due to need for larger malnutrition due to need for larger volumes of some nutrientsvolumes of some nutrients
Shorter periods, < 2 wksShorter periods, < 2 wks

Parenteral NutritionParenteral Nutrition
Dextose 15-25%Dextose 15-25% Amino acids 3-5%Amino acids 3-5% Vitamins (Vit K is not included)Vitamins (Vit K is not included) Lipid emulsions to prevent essential FA Lipid emulsions to prevent essential FA
deficiency (10-15% of calories)deficiency (10-15% of calories) Prepared by the pharmacy from Prepared by the pharmacy from
commercially available kitscommercially available kits If prolonged – supplement trace If prolonged – supplement trace
mineralsminerals Zinc (eczematous rash), copper (microcytic Zinc (eczematous rash), copper (microcytic
anemia), chromium (glucose intolerance)anemia), chromium (glucose intolerance)

Parenteral NutritionParenteral Nutrition
Insulin supplement to insure glucose Insulin supplement to insure glucose tolerancetolerance
IV fluids/electrolytes if high fluid IV fluids/electrolytes if high fluid losseslosses
Freq. monitor fluid status, vital Freq. monitor fluid status, vital signs, UOP, electrolytes, BUN, and signs, UOP, electrolytes, BUN, and LFTs. Glucose q6hLFTs. Glucose q6h

ComplicationsComplications Hyperglycemia – pt with impaired glc tolerance or Hyperglycemia – pt with impaired glc tolerance or
high infusion ratehigh infusion rate Tx- volume replacement, correct electrolytes, insulinTx- volume replacement, correct electrolytes, insulin Avoid by monitoring daily fluid balance, glc, & lytesAvoid by monitoring daily fluid balance, glc, & lytes
Overfeeding – results in CO2 retention and Overfeeding – results in CO2 retention and respiratory insufficiencyrespiratory insufficiency
Hepatic steatosisHepatic steatosis Cholestasis and gallstonesCholestasis and gallstones Hepatic abnormalities – serum transaminase, alk Hepatic abnormalities – serum transaminase, alk
phos and bilirubinphos and bilirubin Intestinal - atrophy from disuse, bacterial Intestinal - atrophy from disuse, bacterial
overgrowth, reduced lymphoid tissue and IgA overgrowth, reduced lymphoid tissue and IgA production, impaired gut immunityproduction, impaired gut immunity

Special FormulationsSpecial Formulations Glutamine and ArginineGlutamine and Arginine
Glutamine – nonessential aa, comprises 66% of free Glutamine – nonessential aa, comprises 66% of free amino acidsamino acids
During stress glu is depleted and shunted as a fuel During stress glu is depleted and shunted as a fuel source to visceral organs and tumorssource to visceral organs and tumors
Inconclusive data for benefits of increased Inconclusive data for benefits of increased supplementationsupplementation
Arginine – nonessential aa, promotes net nitrogen Arginine – nonessential aa, promotes net nitrogen retention and protein synthesis in the critically retention and protein synthesis in the critically ill/injured. Benefits still under investigation.ill/injured. Benefits still under investigation.
Omega-3 Fatty AcidsOmega-3 Fatty Acids Canola or fish oil. Displaces omega-6 FAs, Canola or fish oil. Displaces omega-6 FAs,
theoretically reducing pro-inflammatory responsestheoretically reducing pro-inflammatory responses NucleotidesNucleotides
? Increase cell proliferation, DNA synthesis, T Helper ? Increase cell proliferation, DNA synthesis, T Helper cell functioncell function

ReferencesReferences
The material in this presentation was The material in this presentation was directly adapted from:directly adapted from:
E. Lin, S. E. Calvano, and S. F. Lowry. E. Lin, S. E. Calvano, and S. F. Lowry. Chapter 1. Systemic Response to Injury Chapter 1. Systemic Response to Injury and Metabolic Support. In Schwartz's and Metabolic Support. In Schwartz's Principles of Surgery, 8Principles of Surgery, 8thth ed. ed. F. C. Brunicardi, D. K. Andersen , T. R. Billiar, D. L. Dunn, J. G. Hunter, R. E. Pollock, eds. McGraw-Hill Professional, 2004.eds. McGraw-Hill Professional, 2004.
Related Documents