Tool for Developing RN Specialty Practices: Transitioning from Special Nursing Procedures/Transfer of Medical Function to RN Specialty Practices January 13, 2016 1 | Page

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Tool for Developing RN Specialty Practices:
Transitioning from Special Nursing Procedures/Transfer of Medical Function to RN Specialty Practices
January 13, 2016
1 | P a g e

Transitioning from Special Nursing Procedures/Transfer of Medical Function to RN Specialty Practices
Transition in policy takes time and resources. This tool has been developed to provide you with a starting point for navigating the transition from Special Nursing Procedures/Transfer of Medical Function to RN Specialty Practices. The current Standards for RN Specialty Practices provide the information you will need to ensure policies are in place to support your RNs in meeting their professional standards in this area. Some key activities for this transition include (but are not limited to):
1. Understanding the two processes that make up RN Specialty Practices - RN Procedures and RN Clinical Protocols (refer to pages 11-17).
2. Reviewing current policies that are classified as Special Nursing Procedures or Transfer of Medical Function and conduct an assessment to determine if each activity is appropriate to RN practice and will require either a RN Procedure or RN Clinical Protocol (refer to page 17 and Appendix F on page 41).
3. Connecting with others in your health region or provincially who are doing the same work. The SRNA has a distribution list of known contacts for those working on developing RN Specialty Practices policy. Please email Anita Nivala at [email protected] if you are interested in having your name added to that list. There are a couple of examples of policies included in this document, however other health regions have also developed/are developing policies. Saskatoon Health Region has their policies available online at https://www.saskatoonhealthregion.ca/about/Pages/Policies-and-Procedures.aspx
4. Developing an overarching policy for RN Specialty Practices (refer to page 18).5. Ensuring policies contain the required information for RN Procedures (refer to page 19).6. Ensuring policies contain the required standard content for RN Clinical Protocols (refer to page
38).7. Working through the Developing RN Clinical Protocols flow sheet to ensure all steps have
been covered (refer to page 44).8. Ensuring the RNs in your workplace are familiar with the changes in policy and are aware of
the standards and responsibilities for implementing RN Specialty Practices (refer to pages 7-9).
2 | P a g e

3 | P a g e
Foundations in RN nursing education program requiring additional employer based eduction
RN Procedures
IV push medications
Health Condition in an EmergencyRN Clinical
ProtocolAnaphylaxis
Health Service/ProgramRN Clinical
ProtocolImmunization
Advanced RN InterventionRN Clinical
ProtocolVentilator adjustment
Special Nursing Procedures
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.

4 | P a g e
Foundations in RN nursing education program requiring additional employer based eduction
RN Procedures
IV push medications
Health Condition in an EmergencyRN Clinical
ProtocolAnaphylaxis
Health Service/ProgramRN Clinical
ProtocolImmunization
Advanced RN InterventionRN Clinical
ProtocolVentilator adjustment
Transfer of Medical Function
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.

Assessment for RN Specialty Practices
The following steps provide a method for assessing and determining whether it is appropriate to introduce a RN specialty practice into RN practice. This is not a comprehensive list of assessment questions and when required, others should be added.
Step 1 Assessment Using evidence-informed research, information from an expert health care organization and/or expert opinion, begin by reviewing whether the specialty practice is reasonable and appropriate to introduce into RN practice.
Determine whether the RN specialty practice fits within the SRNA’s interpretation of the RN scope of practice and is safe for clients. Questions to consider include:
Yes/No Action items
Is there literature to support that RNs are safely performing the activity in a similar practice setting?
Is there value for a client population to receive this care from a RN?
Have the benefits, risks, and potential complications of the activity been considered?
Are the symptoms for the health condition appropriate for a RN to identify?
Does the client’s health condition or the Advanced RN Intervention occur often enough for RNs to maintain their competence and proficiency to perform the required care?
Is there a need for a risk management assessment?
Is there a need to consult with the SRNA Practice Advisors?
Determine if the appropriate resources (e.g. personnel, equipment) are available to deliver and support safe client care? Questions to consider include:
Yes/No Action items
5 | P a g e
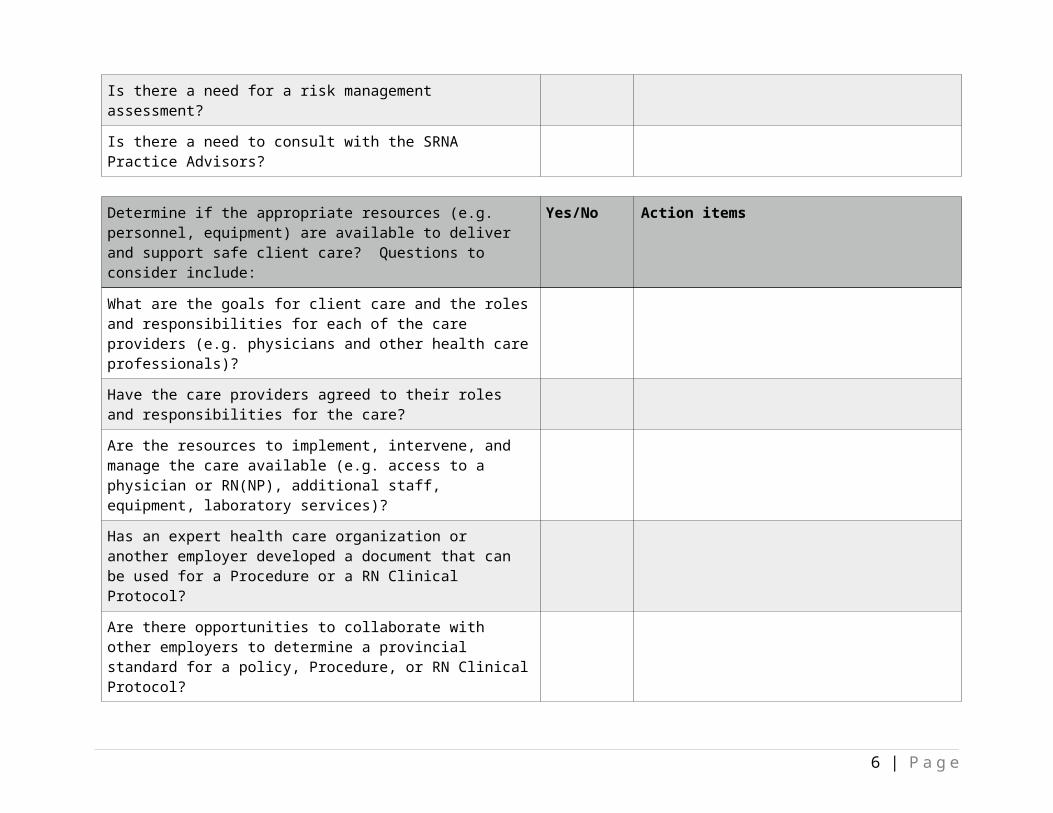
What are the goals for client care and the roles and responsibilities for each of the care providers (e.g. physicians and other health care professionals)?
Have the care providers agreed to their roles and responsibilities for the care?
Are the resources to implement, intervene, and manage the care available (e.g. access to a physician or RN(NP), additional staff, equipment, laboratory services)?
Has an expert health care organization or another employer developed a document that can be used for a Procedure or a RN Clinical Protocol?
Are there opportunities to collaborate with other employers to determine a provincial standard for a policy, Procedure, or RN Clinical Protocol?
Determine whether the specialized competencies and the education for a RN specialty practice is available and can be acquired by a RN. Questions to consider include:
Yes/No Action items
What are the specialized competencies that are required to safely perform the RN specialty practice and to manage any intended or unintended outcomes?
Are the required specialized competencies reasonable to obtain from an education course?
Is there a method to certify that a RN has attained the specialized competencies?
Has an expert health care organization developed specialized competencies and an education course that can be used or is the employer required to develop one?
Has the frequency for performing the activity in the practice setting been determined?
6 | P a g e

Are there qualified professionals/ mentors available to teach the RN specialty practice and supervise practicum if required?
Are there opportunities for a RN to maintain their specialized competencies with case reviews, practice, on-line learning etc.?
If the responses to the above questions are deemed to be appropriate, reasonable, and consistent with professional RN practice, then proceed to implementing the RN specialty practice.
Step 2 Implementation
The safe implementation of a RN specialty practice entails a number of considerations. Questions to consider include:
Yes/No Action items
Has an employer policy that supports a RN specialty practice been developed and the involved health care professionals have provided their support?
Has a Procedure or a RN Clinical Protocol been approved?
Have the RNs who will be implementing the RN specialty practice attained the specialized competencies from an appropriate education course?
Are appropriate resources (e.g. personnel, equipment, or other) in place?
Are there opportunities to collaborate with other employers to determine a provincial standard for a policy, Procedure, or RN Clinical Protocol?
Following the implementation of the RN specialty practice, it is necessary to proceed to an evaluation.Step 3 Evaluation
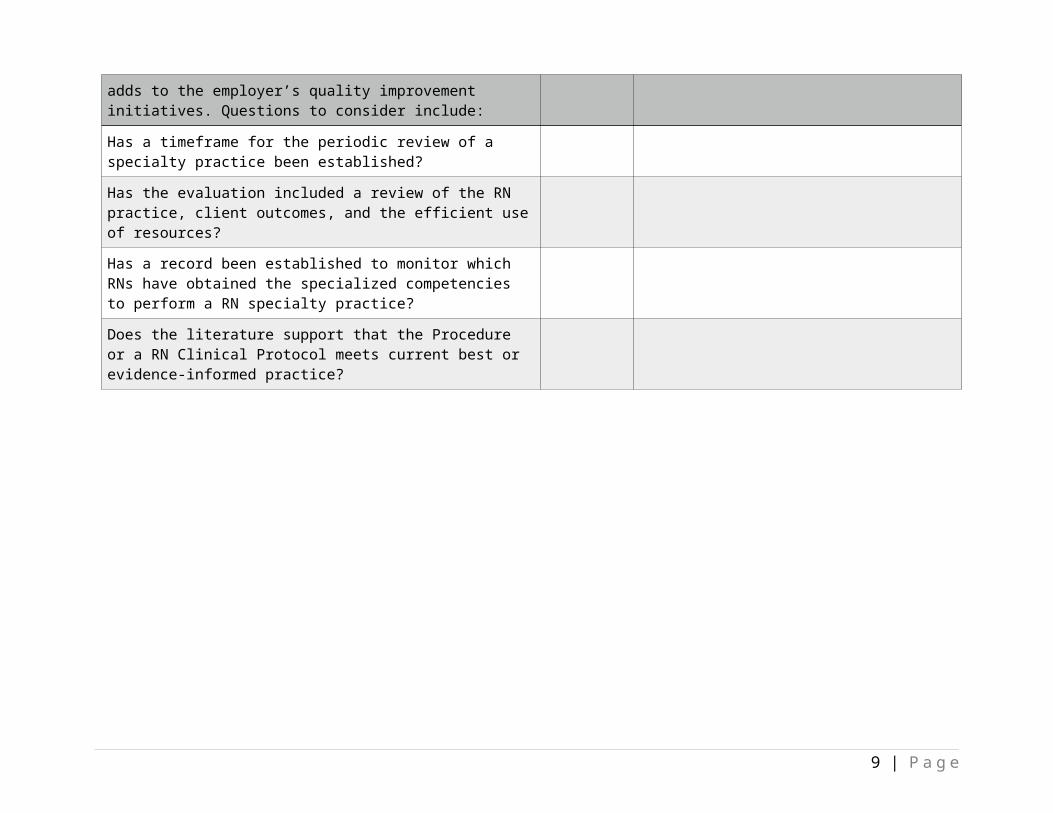
Evaluation provides for a regular review of the RN’s performance of a RN specialty practice and adds to the employer’s quality improvement initiatives. Questions to consider include:
Yes/No Action items
7 | P a g e

Has a timeframe for the periodic review of a specialty practice been established?
Has the evaluation included a review of the RN practice, client outcomes, and the efficient use of resources?
Has a record been established to monitor which RNs have obtained the specialized competencies to perform a RN specialty practice?
Does the literature support that the Procedure or a RN Clinical Protocol meets current best or evidence-informed practice?
Developing a RN Clinical Protocol
Yes No Actions needed to move to next step (if applicable)
1. Would clients with a specific health condition benefit from a RN performing a RN Clinical Protocol in a specific practice setting (Public
Go to 2 STOPReview for
8 | P a g e
Yes No Actions needed to move to next step (if applicable)
Health)? options
2. Is the performance of the RN Clinical Protocol consistent with safe client care as defined in RN scope of practice, SRNA practice documents, and current evidence-informed research?
Go to 3 STOPReview for options
3. Within the RN scope of practice, can a RN manage the potential complications (unintended outcomes) when implementing the RN Clinical Protocol?
Go to 4 STOPReview for options
4. Does the employer have the resources (e.g. appropriate personnel, equipment) to support the RN Clinical Protocol in the practice setting?
Go to 5 STOPReview for options
5. Can the specialized competencies be identified that will enable a RN to safely and competently perform the RN Clinical Protocol?
Go to 6 STOPReview for options
6. Is there an evidence-informed education course, delivered by a qualified professional, available for a RN to take or is the employer required to develop one?
Go to 7 STOPReview for options
7. Is it possible to achieve a collaborative agreement between the employer, RNs, and the physicians for the shared responsibility and clarity of roles and responsibilities for the safe delivery of care?
Go to 8 STOPReview for options
8. Has an employer policy been developed and approved? Go to 9 STOPReview for options
9. Has a review date for the policy, the RN Clinical Protocol, and the education been established?
Go to 10 STOPReview for options
10. Answering “YES” to all of the above questions determines that is possible to develop a RN Clinical Protocol.
9 | P a g e

Example 1 - RN Specialty Practices Policy – courtesy of Sunrise Health Region
Subject: RN (Registered Nurse) Specialty Practices
Number: 870.001
Distribution: Acute & Emergency Manual All Sunrise Health Region sites and the following affiliates: St. Anthony’s Hospital
St. Paul Lutheran HomeSt. Peter’s Hospital
Approval: Vice President of Integrated Health Services
Original Signed by Roberta Wiwcharuk Developed by:
Professional Practice
Implementation Date: July 15, 2015
Revision # :
Review: (mmyy)
Initial
POLICY Registered Nurses (RNs) in Sunrise Health Region may be required to learn specialized competencies in order to provide the client care that is unique to their practice settings. Specialized competencies, which are beyond the foundational competencies obtained in an entry to practice RN education program, enable performance of specialty practices including skills, treatments, and interventions. RN Specialty Practices replaces the previous Transfer of Medical Function category.
For complete details refer to the SRNA Standards for RN Specialty Practices document.
DEFINITIONS:
Specialty Practices
Procedures RN Clinical Protocols
A health condition in an emergency (without a client specific order)
A health service program (without a client specific
order)
An advanced RN intervention (with a client specific
order)

Specialty Practices: Skills, treatments and interventions within the RN scope of practice that have specialized competencies obtained beyond the entry to practice RN education program.
Procedure: Set of steps or a detailed way of performing an activity that has a desired outcome (Lippincott, Williams & Wilkins, 2007).
General RN Procedures: General registered nursing procedures that are part of the curriculum of a basic entry level education program are not included as specialty practices.
Examples of General RN Procedures are: urethral catheterization, intravenous initiation, wound care, medication administration.
It is an employer’s discretion to create policy and procedure documents for General RN Procedures.
Specialty Practice Procedures: The education for a Specialty Practice Procedure builds upon the foundational competencies. Examples of Specialty Practice Procedures include, but are not limited to, the: administration of specialized antineoplastic agents; observing and interpreting Central Venous Pressure (CVP) manometers; conducting specific skills with hemodialysis catheters; and performing venipuncture.
RN Clinical Protocol: A series of registered nursing activities including interventions, services and treatments implemented in pre‐determined situations to provide highly specialized client care. The purpose of a RN Clinical Protocol is to allow RNs to work collaboratively with physicians on an agreed upon practice for the clinical management of a client care situation where their scopes of practice overlap. RN Clinical Protocols contribute to timely, quality, and efficient client care and provide a standardized process for the safe implementation of client care. A RN shall not delegate or assign the client care required for a RN Clinical Protocol to a non‐RN.
Advanced RN Intervention: A skill that is complex in its knowledge requirement and application, may require the performance of minor invasive actions, and has an increased potential for unintentional outcomes that a RN must manage appropriately and safely. An Advanced RN Intervention must be written in a RN Clinical Protocol.
Medical Directive: A Medical Directive allows a RN to carry out activities that cannot be performed within the general RN scope of practice (e.g., order diagnostic tests, order immunizations, or provide a client with a preliminary medical diagnosis). A Medical Directive is a client care order that is written in advance by a physician and can be implemented by a RN for a specific client population.
RESPONSIBILITIES REGARDING IMPLEMENTATION OF SPECIALTY PRACTICES:

1. The RN is responsible for:1.1. Ensuring his/her practice is consistent with legislation, SRNA bylaws, the scope and
standards of practice, and pertinent SRNA documents including the most current version of the following:
1) SRNA Standards and Foundation Competencies for the Practice of Registered Nurses;
2) Canadian Nurses Association, Code of Ethics for Registered Nurses;3) Standards for RN Specialty Practices; and4) The Joint Statement on RN Clinical Protocols between the College of Physicians
and Surgeons of Saskatchewan (CPSS) and the Saskatchewan Registered Nurses’ Association (SRNA).
1.2. Acting in a professional manner, being accountable for his/her own practice, and maintaining conduct, competence (knowledge, skill, and judgment) and proficiency in all aspects of his/her nursing practice including the competence required to conduct a specialty practice.
1.3. Obtaining and maintaining the appropriate specialized competencies, proficiency, and education for any specialty practice he/she must perform.
1.4. Being aware of his/her competence, and not performing any Specialty Practice until he/she has obtained the appropriate education and received certification of approval to perform it from a qualified educator.
1.5. Adhering to Sunrise Health Region policy for a Specialty Practice Procedure or a RN Clinical Protocol.
1.6. Identifying the appropriate situation when a RN Clinical Protocol can be implemented independently and when a client‐specific order is required. A RN Clinical Protocol may be implemented in three situations:
1) Immediate management of a Health Condition in an Emergency without a client‐specific order (e.g., defibrillation).
2) Provision of care in a Health Service Program without a client specific order (e.g., RN Diabetes Educator adjusting insulin doses).
3) Implementation of an Advanced RN Intervention with a client specific order (e.g., intraosseous device insertion).
1.7. Being responsible and accountable when implementing a RN Clinical Protocol by:
1) Adhering to the written RN Clinical Protocol document.2) Completing an assessment of the client (including health history and presenting
state of health).3) Using sound clinical judgment to determine:
a) A nursing diagnosis derived from the assessment;b) The available options for the client’s care needs;c) The risks and benefits of each option (e.g., the client’s care warrants
implementation of a RN Clinical Protocol, the consequences to the client if the RN Clinical Protocol is not implemented); and
d) The ability to manage both intentional and unintentional outcomes until client‐specific orders are obtained.

4) Obtaining written consent (when required) for an Advanced RN Intervention (e.g., pap‐smears, suturing a simple laceration, application of a back slab cast for a simple bone fracture).
5) Communicating with the physician in a timely manner to obtain client‐specific orders when:
a) After the initial stabilization of care or at the point in the RN Clinical Protocol where it states that a physician must be contacted;
b) The RN does not have the competence to manage the intentional or unintentional care outcome(s);
c) The RN Clinical Protocol does not specify the client’s health condition or their presenting signs and symptoms;
d) The RN Clinical Protocol specifies that a physician must provide a client‐specific order before the care is provided;
e) After the RN Clinical Protocol is started there is an acute change in the client’s situation;
f) The laboratory findings, client assessment, or other information is inconsistent with the data in the RN Clinical Protocol; or
g) Other unexpected circumstances occur.6) Documenting on the client’s health record (e.g., chart):
a) Name of the RN Clinical Protocol that was provided;b) Time it was provided;c) Client care that was provided;d) Client’s response to the care;e) Time the physician was contacted and client‐specific orders were
received;f) Education that was provided to the client and his/her family; andg) Other information as appropriate.
1.8. Not delegating or assigning the client care required for a RN Clinical Protocol to a non‐RN.
1) A Graduate Nurse shall not accept sole responsibility for a client care assignment that requires the use of a RN Clinical Protocol. A Graduate Nurse may contribute to the client’s care in this situation by working under the direct supervision of a RN.
2. Sunrise Health Region is responsible for:2.1. Providing the essential resources (e.g., education, personnel, equipment) required by
the RN to safely perform the specialty practice ensuring his/her practice is consistent with legislation, SRNA bylaws, the scope and standards of practice, and pertinent SRNA documents including the most current version of the following:1) SRNA Standards and Foundation Competencies for the Practice of Registered
Nurses;2) The Canadian Nurses Association, Code of Ethics for Registered Nurses;3) Standards for RN Specialty Practices; and4) The Joint Statement on RN Clinical Protocols between the College of Physicians
and Surgeons of Saskatchewan (CPSS) and the Saskatchewan Registered Nurses’ Association (SRNA).
2.2. Ensuring policies, Specialty Practice Procedures, RN Clinical Protocols, and job descriptions support RNs who are required to perform a Specialty Practice. A job

description cannot expand the legislated scope of RN practice as interpreted by the SRNA.
2.3. Working with physicians and RNs to identify potential RN Clinical Protocols and providing organizational approval for their use.
2.4. Ensuring any consent requirements for an advanced RN intervention are included within the RN Clinical Protocol (e.g., consent for a pap smear, suturing a simple laceration, or applying a back slab cast).
2.5. Ensuring all RNs who are performing Specialty Practices receive the education required to attain the necessary specialized competencies and proficiency and maintain their competence in the Specialty Practice.
2.6. Maintaining a current record of the RNs who are approved to perform each Specialty Practice in the specific practice setting.
3. Shared Expectations with RN Clinical Protocols:3.1. A RN Clinical Protocol is an agreed upon document between physicians and RNs for
the clinical management of a client care situation. To enable clear roles and responsibilities between care providers and maintain safe client care, there are shared expectations between the: individual RN adhering to the RN standards of practice, the employer, and physician(s).
4. The physician is responsible for:4.1. Providing the medical diagnosis, treatment, prescribing and monitoring of the client’s
health and/or their medical disease or disorder.4.2. Participating in the development and written approval of a document and policy for the
RN Clinical Protocol. A medical representative (e.g., medical health officer, chair of a medical advisory committee, department head) may approve a policy on behalf of a group of physicians.
4.3. Assuming the ongoing medical management of the client’s care and providing client‐specific orders once he/she has been notified by a RN that a RN Clinical Protocol has been implemented.
EDUCATION FOR SPECIALTY PRACTICES:1. For a Specialty Practice Procedure, the RN clinical experts [e.g., RN Clinical Nurse
Educators, RN Clinical Nurse Specialists, RN(NP)s] must determine the appropriate education by assessing evidence‐informed research. When available, the educational content that has been developed by an expert health care organization should be utilized.
2. For a RN Clinical Protocol, the following criteria apply:2.1. To determine the appropriate education, the employer must consult with RNs (e.g.,
point‐of‐care RNs, RN(NP)s, Clinical Instructors, Clinical Nurse Specialists) and, when required, other health care professionals (e.g., physicians, pharmacists).
2.2. When available, education courses developed by an expert health care organization or a formal educational institution must be utilized. Examples of expert developed education include:

1) Heart and Stroke Foundation of Canada Life Support ‐ Advanced Cardiovascular Life Support (ACLS) or Pediatric Advanced Life Support (PALS).
2) Sugar & Safe Care, Temperature, Airway, Blood Pressure, Laboratory Work and Emotional Support (S.T.A.B.L.E).
3) Trauma Nursing Core Course (TNCC)2.3. The education for an Advanced RN Intervention (e.g., pap tests, pelvic
examinations, suturing a simple laceration, application of back slab cast) must be obtained from the curriculum of a formal educational institution (e.g., University of Saskatchewan Continuing Education and Development for Nurses; Saskatchewan Polytechnic).
REFERENCES:1. SRNA Standards for RN Specialty Practices (DRAFT, Feb. 10, 2015).

Example 2 - RN Clinical Protocols Policy – courtesy of Sunrise Health Region
Date effective: August 18, 2014
Date to be reviewed: August 18, 2016
Issuing authority(s): Vice President of Integrated Health ServicesVice President of Medical Services
(RN CLINICAL PROTOCOL- DEFIBRILLATION)
DEFINITION Defibrillation – The application of electrical shock through externally placed
pads, to stun the heart and briefly terminate all electrical activity, including ventricular fibrillation (VF) and pulseless ventricular tachycardia (VT). If the heart is still viable its normal pacemakers may eventually resume electrical activity that ultimately results in a perfusing rhythm.
Rapid response is required, so defibrillation shall be done without a client specific order immediately on recognition of pulseless VT of VF. ACLS/PALS algorithms are to be followed while waiting for a physician to arrive and provide client-specific orders.
ETIOLOGY VF can be the result of several alterations in the electrical system of the
myocardium including:o a result of chaotic electrical activity in the ventricleso several small simultaneous re-entry mechanismso a series of rapid discharges from multiple foci within the ventricular myocardium.
VT is generally from a re-entry mechanism that causes the ventricle to fire at a rate greater than 100. Without prompt intervention this can result in a loss of cardiac output, and likely will degenerate in to VF and ultimately death.
Both rhythms are ultimately the result of alterations in the electrical system, so rapid defibrillation is recommended to disrupt the activity and allow the opportunity for the myocardium to resume normal activity and cause a return of spontaneous circulation (ROSC).
HIGH ALERT The discovery of the absence of vital signs should be followed by
immediate assessment of cardiac rhythm for ventricular tachycardia or ventricular fibrillation. These rhythms require immediate intervention, so the physician should be contacted simultaneously with treatment initiation to increase client chance of survival.

OBJECTIVE To provide rapid defibrillation to Sunrise Health Region clients presenting or
exhibiting pulseless VT or VF to improve their chance of survival.
ASSESSMENT Assess level of consciousness; an unresponsive client likely indicates poor cerebral
perfusion. Quick assessment of the airway, breathing and circulation as per ACLS guidelines.
Absence of normal respirations or pulse is an indication to initiate the cardiac arrest algorithm.
Attach to a cardiac monitor with the capabilities of providing electrical intervention (i.e. defibrillation) and interpret the rhythm seen.
NURSING DIAGNOSIS AND THERAPEUTIC ACTIONS Nursing diagnosis:
o Inadequate cardiac output for tissue/organ perfusion due to cardiac arrhythmia.o Decreased cardiac output related to inadequate ventricular filling associated with
rapid tachycardia. Therapeutic Actions:
o Follow ACLS/PALS Algorithms included below for Cardiac Arrest.o Initiate Cardiopulmonary Resuscitation (CPR) immediately upon discovery of the
absence or loss of pulse. Ensure the physician is made aware of the situation and knows to respond immediately.
o Place self adhesive defibrillation pads on the client’s chest (if not on already) in the anterolateral positions depicted on the pads themselves. Alternatively the pads may be placed in the anterior/posterior position. Do NOT interrupt CPR for pad placement.
oo In
t erpre t
cardiac rhythm on monitor and without delay identify if rhythm is VT or VF. If VT or VF charge to the appropriate level depending on client and as per ACLS/PALS protocol. Continue CPR while the machine is charging.
o Once the defibrillator is charged, ensure the environment is safe by visually identifying all members are clear of the client as well as stating “you’re clear, I’m clear, we’re all clear”.
o Deliver the charge and immediately resume CPR.o Continue for another 2 minute cycle of CPR and then begin again with a pulse
check and then as per ACLS/PALS protocols until physician arrives to provide client-specific orders. .
INTENDED AND UNINTENDED OUTCOMES Intended Outcome: Client has ROSC and follow up care is provided as directed by
the physician. Unintended Outcomes:

o Client remains in an unstable rhythm and requires further intervention according to ACLS/PALS algorithms until physician arrives to provide client-specific orders.
o Client deteriorates or actions are ineffective and resuscitation efforts are ceased by the physician.
COMMUNICATION The physician should be contacted immediately on recognition of pulseless VT or
VF. Information should be relayed utilizing the SBAR format with emphasis on urgent response required.
Client-specific orders should be received as soon as the physician arrives and assesses the situation.
EDUCATION The option for family to be present during resuscitation should be provided. All
efforts to share information with the client and family should be made in a timely fashion after immediate client care is provided.
DOCUMENTATION Documentation shall be done on the Code Blue Record and placed into the client
chart. The RN should document:o the time the physician was contacted and any orders receivedo the RN Clinical Protocol-Defibrillation was usedo the time defibrillation was providedo the client response to defibrillationo Any further interventions requiredo Any education/information provided to client or family
REFERENCESCanadian Association of Critical Care Nurses (2005). Family Presence During
Resuscitation. Retrieved from http://www.caccn.ca/en/publications/position_statements/family_presence_during_resuscitation_2005.html
Heart and Stroke Foundation of Canada. (2011). ACLS Cardiac Arrest, Arrhythmias, and their
treatment. Medtronic (2012). Physio-control Quick-Combo Pacing/Defibrillation/ECG electrodes. Neumar, R., Otto, C., Link, M., Kronick, S., Shuster, M., Callaway,C., Kudenchuk, P., Ornato,
P., McNally, B., Silvers, S., Passman, R., White, R., Hess, E., Tang, W., Davis, D., Sinz, E., & Morrison, L. (2010). 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science. Part 8: Adult Advanced Cardiovascular Life Support. Circulation, 122, p. S729-S767. doi: 10.1161/CIRCULATIONAHA.110.970988
SRNA (2014). Standards for RN Specialty Practices DRAFT May 16, 2014. Urden, L., Stacy, K., Lough, M. (2014). Critical Care Nursing 7th Ed. Elsevier Mosby: St.

Louis Missouri.
A RN clinical protocol outlines a series of registered nursing actions that are implemented in pre-determined situations to provide specialized client care in Saskatchewan. A RN who implements a RN clinical protocol must meet the criteria as outlined in the SRNA document, Standards for RN Specialty Practices (2014). This RN clinical protocol contains evidenced-informed content that is used in conjunction with a RNs critical thinking and clinical judgment to determine when it is appropriate for it to be implemented according to the client’s presenting health situation.


Related Documents











