Patient disposition • The study was completed on May 27, 2020 (last patient last visit), with 61 patients in phase 1b and 100 patients in phase 2 • Out of the 161 patients who discontinued from treatment phase, 130 patients (80.7%) entered the survival follow-up and 31 patients (19.3%) discontinued from study (Table 1) – Four patients alive at the end of the study and 1 patient was transferred into a rollover clinical study • Most common reason for discontinuation of study treatment was disease progression (123 patients, 76.4%), followed by adverse events (AEs, 19 patients, 11.8%) Table 1: Patient Disposition Characteristic All patients (N=161) n (%) Treatment phase Completed 6 cycles of treatment 70 (43.5) Discontinued from treatment phase 161 (100) Entered survival follow-up 130 (80.7) Discontinued from study 31 (19.3) Primary reason for discontinuation from treatment Progressive disease 123 (76.4) Adverse event 19 (11.8) Subject/guardian decision 8 (5.0) Death 7 (4.3) Non-compliance with study treatment 1 (0.6) Physician decision 1 (0.6) Protocol deviation 1 (0.6) Study terminated by sponsor 1 (0.6) Baseline characteristics • The majority of patients were Asian (81.4%) and <65 years of age (67.1%) (Table 2) • The overall median age (range) was 60 years (32-78 years) • Most patients had a baseline ECOG performance status of 1 (78.3%) – 6 patients (3.7%) reported an ECOG performance status of 2 Table 2: Baseline characteristics Demographic variable Phase 1b N=61 Phase 2 N=100 Median age (range), years 58.0 (36-77) 61.0 (32-78) Sex, n (%) Female Male 36 (59.0) 25 (41.0) 52 (52.0) 48 (48.0) Race, n (%) Asian Caucasian 53 (86.9) 8 (13.1) 78 (78.0) 22 (22.0) ECOG performance status, n (%) 0 1 2 12 (19.7) 45 (73.8) 4 (6.6) 17 (17.0) 81 (81.0) 2 (2.0) ECOG, Eastern Cooperative Oncology Group Overall survival • Median follow-up time (range) was 12.2 (0.9-70.2) months • The overall median OS (95% CI) was 13.9 (11.6-15.7) months (Table 3) Table 3: Overall survival Phase 2 N=100 No of events/N (%) 82/100 (82) Median overall survival (95% CI), months 13.9 (11.6 - 15.7) % Event-free probability (95% CI) 12 months 24 months 36 months 48 months 58.4 (47.7 - 67.7) 22.9 (14.7 - 32.2) 12.1 (6.2 - 20.0) 10.7 (5.2 - 18.4) Figure 1: Kaplan-Meier plot of overall survival (Phase 2) Probability of survival Time (months) 0 100 4 84 8 66 12 52 16 33 20 24 24 19 28 16 32 11 36 10 40 9 44 8 48 6 52 3 56 3 60 2 64 1 68 1 72 0 All Patients Number of patients at risk Time (months) 1.0 0.8 0.6 0.4 0.2 0.0 0 Censoring Times Kaplan-Meier medians [95% CI] (months) All Patients: 13.93 [11.60; 15.67] No of events/N = 82/100 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 Safety • Median duration of exposure (range): – Phase 1b: 16 (0.4-209.7) weeks – Phase 2: 18.5 (0.4-268.0) weeks • 15 patients (9.3%) had died on-treatment – The majority of deaths (10 patients, 6.2%) were attributed to the study indication, NSCLC – Two patients (1.2%) died due to pneumonia and 1 patient each (0.6%) died due to dyspnea, myocardial infarction and cerebrovascular accident • Approximately one-third of patients had serious AEs (54 patients, 33.5%) – The most frequent serious AEs (reported in ≥ 2.0% patients) were pneumonia, dyspnea (7 patients, 4.3%), and pulmonary embolism (5 patients, 3.1%) • Almost all patients (159 patients, 98.8%) experienced at least one AE; most being suspected to be related to study treatment (140 patients, 87.0%) • The most frequent AEs of any grade (reported in ≥25% of patients, regardless of causality) were nausea (36%), decreased appetite (32.9%), peripheral edema (32.3%), hypoalbuminemia (29.8%), vomiting (27.3%), and rash (25.5%) Table 4: Treatment-related adverse events (reported in at least 10% of all patients) Preferred term All patients N=161 All grades n (%) Grade 3/4 n (%) Total 140 (87.0) 51 (31.7) Nausea 45 (28.0) 5 (3.1) Peripheral oedema 37 (23.0) 8 (5.0) Rash 35 (21.7) 2 (1.2) Decreased appetite 34 (21.1) 3 (1.9) Diarrhea 30 (18.6) 1 (0.6) Paronychia 29 (18.0) 1 (0.6) Vomiting 29 (18.0) 4 (2.5) Increased amylase 25 (15.5) 10 (6.2) Fatigue 23 (14.3) 4 (2.5) Increased alanine aminotransferase 19 (11.8) 3 (1.9) Lipase increased 18 (11.2) 10 (6.2) Phase 1b/2 study of capmatinib plus gefitinib in patients with EGFR-mutated, MET-dysregulated non-small cell lung cancer who received prior therapy: Final overall survival and safety Yi-Long Wu 1 , Li Zhang 2 , Dong-Wan Kim 3 , Xiaoqing Liu 4 , Dae Ho Lee 5 , James CH Yang 6 , Myung-Ju Ahn 7 , Johan F. Vansteenkiste 8 , Wu-Chou Su 9 , Enriqueta Felip 10 , Mariana Cabini 11 , Sabine Glaser 11 , Oezlem Tanriverdi 11 , Andrea Chassot Agostinho 11 , Daniel SW Tan 12 1 Guangdong General Hospital and Guangdong Academy of Medical Sciences, Guangdong, China; 2 Sun Yat-sen University Cancer Center, Guangdong, China; 3 Seoul National University Hospital, Seoul, Republic of Korea; 4 Affiliated Hospital of the Chinese Academy of Military Medical Sciences, Beijing, China; 5 University of Ulsan College of Medicine, Seoul, Republic of Korea; 6 National Taiwan University Hospital, Taipei, Taiwan; 7 Samsung Medical Center, Seoul, Republic of Korea; 8 University Hospital KU Leuven, Leuven, Belgium; 9 National Cheng Kung University Hospital, Tainan, Taiwan; 10 Vall d’Hebron University Hospital, Barcelona, Spain; 11 Novartis Pharma AG, Basel, Switzerland; 12 National Cancer Centre Singapore, Singapore Poster presented at the 2021 ASCO Annual Meeting, held virtually on 4–8 June 2021 This study is sponsored by Novartis Pharma AG Poster 9048 KEY FINDINGS AND CONCLUSIONS Scan to obtain: • Poster https://www.medicalcongress. novartisoncology.com/ASCO/Lung_Cancer/ lung_cancer.html#WuYL90488409 Copies of this poster obtained throughQuick Response (QR) code are for personal use onlyand may not be reproduced without permissionof the authors INTRODUCTION • Capmatinib is a highly selective MET inhibitor approved for the treatment of adult patients with MET exon 14 skipping (METex14)-mutated, advanced non-small cell lung cancer (NSCLC) based on results from the global phase 2 GEOMETRY mono-1 study (NCT02414139) 1 • In the phase 1b/2 NCT01610336 study, we investigated the combination of capmatinib with an epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI), gefitinib in patients with EGFR-mutated and MET-dysregulated NSCLC who failed previous EGFR TKI therapy 2 – The recommended phase 2 dose (RP2D) was capmatinib 400 mg twice-daily (bid) and gefitinib 250 mg once-daily (qd) – An objective response rate (ORR) of 29% was reported in phase 2, regardless of MET status in the primary analysis 3 – The ORR was 47% in patients with high MET-amplified tumors (MET gene copy number ≥6) 3,4 • Here, we report final overall survival (OS) and safety data from the study RESULTS Acknowledgements • We thank the patients, their families and caregivers, and the investigators who participated in the study • This study was sponsored by Novartis Pharmaceuticals Corporation • Medical writing and editorial assistance was provided by Aarti Kamaraj (Novartis Healthcare Pvt Ltd) and Varunkumar Pandey (Novartis Healthcare Pvt Ltd) • Capmatinib 400 mg bid in combination with gefitinib 250 mg qd showed encouraging clinical activity in patients with EGFR- mutant and MET-dysregulated NSCLC – Median OS (95% CI) was 13.9 (11.6-15.7) months • The combination was well tolerated • The most frequent AEs of any grade (reported in ≥25% of patients, regardless of causality) were nausea (36%), decreased appetite (32.9%), peripheral edema (32.3%), hypoalbuminemia (29.8%), vomiting (27.3%), and rash (25.5%) • The data suggests that combining MET inhibitor capmatinib with an EGFR-TKI may be a promising treatment option for EGFR-mutated, MET -dysregulated NSCLC, particularly for patients with MET amplified tumors Presenting Author: Dr. Yi-Long Wu [email protected] METHODS • This was an open-label, multicenter study, which was composed of a phase 1b dose escalation part and a phase 2 dose expansion part DOR, duration of response; ECOG PS, Eastern Cooperative Oncology Group Performance Status; EGFR, epidermal growth factor receptor; FISH, Fluorescence In Situ Hybridization; IHC, Immunohistochemistry; MET, mesenchymal epithelial transition factor; MTD, maximum tolerated dose; NSCLC, non-small cell lung cancer; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; RECIST, Response evaluation criteria in solid tumors; RP2D, recommended phase 2 dose; TKI, tyrosine kinase inhibitor Key eligibility criteria: • Locally advanced or metastatic NSCLC harboring EGFR mutation (exon 19 deletion or L858R) • Clinical benefit with prior single-agent EGFR TKI before progression • Dysregulated MET pathway post-progression on EGFR TKIs a • ECOG PS ≤2 • ≥1 measurable lesion according to RECIST v1.1 (phase 2) STUDY DESIGN 2 Phase 1b capmatinib + gefitinib 250 mg Phase 2 capmatinib + gefitinib 250 mg Endpoints: Primary: • ORR per RECIST v1.1 Secondary: • OS, DOR, PFS • Safety and tolerability • Pharmacokinetic profile Initial expansion group b in approximately 40 patients Determine MTD or RP2D At least 18 patients MET dysregulation group in approximately 90 patients a High MET expression was defined as ≥50% of tumor cells with IHC 3+, MET gene amplification was defined as gene copy number ≥4 by FISH b Enrollment of patients in the initial expansion group had stopped at the time when protocol Amendment 3 was approved by the Health Authority/Institutional Review Board at the study site. References 1. N Engl J Med 2020; 383: 944-957 2. https://clinicaltrials.gov/ct2/show/NCT01610336 accessed on Apr 8, 2021 3. J Clin Oncol. 2018; 36(31): 3101-3109 4. J Clin Oncol. 2019; 37(3): 261 Disclosures (Dr Yi-Long Wu) Dr Yi-Long Wu reports personal fees from AstraZeneca (advisory board and speaker), Eli Lilly (speaker), Merck (advisory board and speaker), Pfizer (speaker), and Sanofi (speaker) outside the submitted work; grants and personal fees from Roche (advisory board and speaker) and Boehringer Ingelheim (advisory board and speaker) outside the submitted work

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Patient disposition• The study was completed on May 27, 2020 (last patient last visit), with 61 patients in phase 1b and 100
patients in phase 2
• Out of the 161 patients who discontinued from treatment phase, 130 patients (80.7%) entered thesurvival follow-up and 31 patients (19.3%) discontinued from study (Table 1)
– Four patients alive at the end of the study and 1 patient was transferred into a rollover clinical study
• Most common reason for discontinuation of study treatment was disease progression (123 patients,76.4%), followed by adverse events (AEs, 19 patients, 11.8%)
Table 1: Patient Disposition
CharacteristicAll patients
(N=161)n (%)
Treatment phase
Completed 6 cycles of treatment 70 (43.5)
Discontinued from treatment phase 161 (100)
Entered survival follow-up 130 (80.7)
Discontinued from study 31 (19.3)
Primary reason for discontinuation from treatment
Progressive disease 123 (76.4)
Adverse event 19 (11.8)
Subject/guardian decision 8 (5.0)
Death 7 (4.3)
Non-compliance with study treatment 1 (0.6)
Physician decision 1 (0.6)
Protocol deviation 1 (0.6)
Study terminated by sponsor 1 (0.6)
Baseline characteristics• The majority of patients were Asian (81.4%) and <65 years of age (67.1%) (Table 2)
• The overall median age (range) was 60 years (32-78 years)
• Most patients had a baseline ECOG performance status of 1 (78.3%)
– 6 patients (3.7%) reported an ECOG performance status of 2
Table 2: Baseline characteristics
Demographic variable Phase 1bN=61
Phase 2N=100
Median age (range), years 58.0 (36-77) 61.0 (32-78)Sex, n (%)
FemaleMale
36 (59.0)25 (41.0)
52 (52.0)48 (48.0)
Race, n (%)AsianCaucasian
53 (86.9)8 (13.1)
78 (78.0)22 (22.0)
ECOG performance status, n (%)012
12 (19.7)45 (73.8)
4 (6.6)
17 (17.0)81 (81.0)
2 (2.0)ECOG, Eastern Cooperative Oncology Group
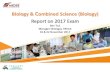
Overall survival• Median follow-up time (range) was 12.2 (0.9-70.2) months
• The overall median OS (95% CI) was 13.9 (11.6-15.7) months (Table 3)
Table 3: Overall survivalPhase 2N=100
No of events/N (%) 82/100 (82)Median overall survival (95% CI), months 13.9 (11.6 - 15.7)
% Event-free probability (95% CI)12 months24 months36 months48 months
58.4 (47.7 - 67.7)22.9 (14.7 - 32.2)12.1 (6.2 - 20.0)10.7 (5.2 - 18.4)
Figure 1: Kaplan-Meier plot of overall survival (Phase 2)
Prob
abili
ty o
f sur
viva
l
Time (months) 0100
484
866
1252
1633
2024
2419
2816
3211
3610
409
448
486
523
563
602
641
681
720All Patients
Number of patients at riskTime (months)
1.0
0.8
0.6
0.4
0.2
0.0
0
Censoring Times
Kaplan-Meier medians [95% CI] (months)All Patients: 13.93 [11.60; 15.67]
No of events/N = 82/100
4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72
Safety• Median duration of exposure (range):
– Phase 1b: 16 (0.4-209.7) weeks
– Phase 2: 18.5 (0.4-268.0) weeks
• 15 patients (9.3%) had died on-treatment
– The majority of deaths (10 patients, 6.2%) were attributed to the study indication, NSCLC
– Two patients (1.2%) died due to pneumonia and 1 patient each (0.6%) died due to dyspnea, myocardialinfarction and cerebrovascular accident
• Approximately one-third of patients had serious AEs (54 patients, 33.5%)
– The most frequent serious AEs (reported in ≥ 2.0% patients) were pneumonia, dyspnea (7 patients,4.3%), and pulmonary embolism (5 patients, 3.1%)
• Almost all patients (159 patients, 98.8%) experienced at least one AE; most being suspected to berelated to study treatment (140 patients, 87.0%)
• The most frequent AEs of any grade (reported in ≥25% of patients, regardless of causality) were nausea(36%), decreased appetite (32.9%), peripheral edema (32.3%), hypoalbuminemia (29.8%), vomiting(27.3%), and rash (25.5%)
Table 4: Treatment-related adverse events (reported in at least 10% of all patients)
Preferred term All patientsN=161
All grades n (%) Grade 3/4 n (%)
Total 140 (87.0) 51 (31.7)
Nausea 45 (28.0) 5 (3.1)
Peripheral oedema 37 (23.0) 8 (5.0)
Rash 35 (21.7) 2 (1.2)
Decreased appetite 34 (21.1) 3 (1.9)
Diarrhea 30 (18.6) 1 (0.6)
Paronychia 29 (18.0) 1 (0.6)
Vomiting 29 (18.0) 4 (2.5)
Increased amylase 25 (15.5) 10 (6.2)
Fatigue 23 (14.3) 4 (2.5)
Increased alanine aminotransferase 19 (11.8) 3 (1.9)
Lipase increased 18 (11.2) 10 (6.2)
Phase 1b/2 study of capmatinib plus gefitinib in patients with EGFR-mutated, MET-dysregulated non-small cell lung cancer who received prior therapy: Final overall survival and safetyYi-Long Wu1, Li Zhang2, Dong-Wan Kim3, Xiaoqing Liu4, Dae Ho Lee5, James CH Yang6, Myung-Ju Ahn7, Johan F. Vansteenkiste8, Wu-Chou Su9, Enriqueta Felip10, Mariana Cabini11, Sabine Glaser11, Oezlem Tanriverdi11, Andrea Chassot Agostinho11, Daniel SW Tan12
1Guangdong General Hospital and Guangdong Academy of Medical Sciences, Guangdong, China; 2Sun Yat-sen University Cancer Center, Guangdong, China; 3Seoul National University Hospital, Seoul, Republic of Korea; 4Affiliated Hospital of the Chinese Academy of Military Medical Sciences, Beijing, China; 5University of Ulsan College of Medicine, Seoul, Republic of Korea; 6National Taiwan University Hospital, Taipei, Taiwan; 7Samsung Medical Center, Seoul, Republic of Korea; 8University Hospital KU Leuven, Leuven, Belgium; 9National Cheng Kung University Hospital, Tainan, Taiwan; 10Vall d’Hebron University Hospital, Barcelona, Spain; 11Novartis Pharma AG, Basel, Switzerland; 12National Cancer Centre Singapore, Singapore
Poster presented at the 2021 ASCO Annual Meeting, held virtually on 4–8 June 2021This study is sponsored by Novartis Pharma AG
Poster 9048
KEY FINDINGS AND CONCLUSIONS
Scan to obtain:• Poster
https://www.medicalcongress.novartisoncology.com/ASCO/Lung_Cancer/lung_cancer.html#WuYL90488409Copies of this poster obtained throughQuick Response (QR) code are for personal use onlyand may not be reproduced without permissionof the authors
INTRODUCTION• Capmatinib is a highly selective MET inhibitor approved for the treatment of adult patients with MET exon 14 skipping (METex14)-mutated,
advanced non-small cell lung cancer (NSCLC) based on results from the global phase 2 GEOMETRY mono-1 study (NCT02414139)1
• In the phase 1b/2 NCT01610336 study, we investigated the combination of capmatinib with an epidermal growth factor receptor (EGFR)tyrosine kinase inhibitor (TKI), gefitinib in patients with EGFR-mutated and MET-dysregulated NSCLC who failed previous EGFR TKI therapy2
– The recommended phase 2 dose (RP2D) was capmatinib 400 mg twice-daily (bid) and gefitinib 250 mg once-daily (qd)– An objective response rate (ORR) of 29% was reported in phase 2, regardless of MET status in the primary analysis3
– The ORR was 47% in patients with high MET-amplified tumors (MET gene copy number ≥6)3,4
• Here, we report final overall survival (OS) and safety data from the study
RESULTS
Acknowledgements• We thank the patients, their families and caregivers, and the investigators who participated in the study• This study was sponsored by Novartis Pharmaceuticals Corporation• Medical writing and editorial assistance was provided by Aarti Kamaraj (Novartis Healthcare Pvt Ltd) and Varunkumar Pandey (Novartis Healthcare Pvt Ltd)
• Capmatinib 400 mg bid in combination with gefitinib 250 mg qd showed encouraging clinical activity in patients with EGFR-mutant and MET-dysregulated NSCLC– Median OS (95% CI) was 13.9 (11.6-15.7) months
• The combination was well tolerated• The most frequent AEs of any grade (reported in ≥25% of patients,
regardless of causality) were nausea (36%), decreased appetite (32.9%), peripheral edema (32.3%), hypoalbuminemia (29.8%), vomiting (27.3%), and rash (25.5%)
• The data suggests that combining MET inhibitor capmatinib with an EGFR-TKI may be a promising treatment option forEGFR-mutated, MET-dysregulated NSCLC, particularly for patients with MET amplified tumors
Presenting Author: Dr. Yi-Long [email protected]
METHODS• This was an open-label, multicenter study, which
was composed of a phase 1b dose escalation partand a phase 2 dose expansion part
DOR, duration of response; ECOG PS, Eastern Cooperative Oncology Group Performance Status; EGFR, epidermal growth factor receptor; FISH, Fluorescence In Situ Hybridization; IHC, Immunohistochemistry; MET, mesenchymal epithelial transition factor; MTD, maximum tolerated dose; NSCLC, non-small cell lung cancer; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; RECIST, Response evaluation criteria in solid tumors; RP2D, recommended phase 2 dose; TKI, tyrosine kinase inhibitor
Key eligibility criteria:• Locally advanced or metastatic NSCLC harboring
EGFR mutation (exon 19 deletion or L858R)• Clinical benefit with prior single-agent EGFR TKI
before progression• Dysregulated MET pathway post-progression on
EGFR TKIsa
• ECOG PS ≤2• ≥1 measurable lesion according to RECIST v1.1
(phase 2)
STUDY DESIGN2
Phase 1bcapmatinib + ge�tinib 250 mg
Phase 2capmatinib + ge�tinib 250 mg
Endpoints:
Primary: • ORR per RECIST v1.1
Secondary:• OS, DOR, PFS• Safety and tolerability• Pharmacokinetic profile
Initial expansion groupb in approximately 40 patientsDetermine
MTD or RP2D At least
18 patients MET dysregulation group in approximately 90 patients
aHigh MET expression was defined as ≥50% of tumor cells with IHC 3+, MET gene amplification was defined as gene copy number ≥4 by FISHbEnrollment of patients in the initial expansion group had stopped at the time when protocol Amendment 3 was approved by the Health Authority/Institutional Review Board at the study site.
References1. N Engl J Med 2020; 383: 944-9572. https://clinicaltrials.gov/ct2/show/NCT01610336 accessed on Apr 8, 20213. J Clin Oncol. 2018; 36(31): 3101-31094. J Clin Oncol. 2019; 37(3): 261
Disclosures (Dr Yi-Long Wu)Dr Yi-Long Wu reports personal fees from AstraZeneca (advisory board and speaker), Eli Lilly (speaker), Merck (advisory board and speaker), Pfizer (speaker), and Sanofi (speaker) outside the submitted work; grants and personal fees from Roche (advisory board and speaker) and Boehringer Ingelheim (advisory board and speaker) outside the submitted work

PHASE 1B/2 STUDY OF CAPMATINIB PLUS GEFITINIB IN PATIENTS WITH EGFR-MUTATED, MET-DYSREGULATED NON-SMALL CELL LUNG CANCER WHO RECEIVED PRIOR THERAPY: FINAL OVERALL SURVIVAL AND SAFETY
Dr Yi-Long Wu
Guangdong General Hospital and Guangdong Academy of Medical Sciences, Guangdong, China

Dr Yi-Long Wu
Introduction
• Capmatinib is a highly selective MET inhibitor approved for the treatment of adult patients with MET exon 14
skipping (METex14)-mutated, advanced non-small cell lung cancer (NSCLC) based on results from the global
phase 2 GEOMETRY mono-1 study (NCT02414139)1
• In the phase 1b/2 NCT01610336 study, we investigated the combination of capmatinib with an epidermal
growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI), gefitinib in patients with EGFR-mutated and
MET-dysregulated NSCLC who failed previous EGFR TKI therapy2
• The recommended phase 2 dose (RP2D) was capmatinib 400 mg twice-daily (bid) and gefitinib 250 mg once-daily (qd)
• An objective response rate (ORR) of 29% was reported in phase 2, regardless of MET status in the primary analysis3
• The ORR was 47% in patients with high MET-amplified tumors (MET gene copy number ≥6)3,4
• Here, we report final overall survival (OS) and safety data from the study
1. N Engl J Med 2020; 383:944-957
2. https://clinicaltrials.gov/ct2/show/NCT01610336 accessed on Apr 8, 2021
3. J Clin Oncol. 2018;36(31):3101-3109.
4. J Clin Oncol. 2019;37(3):261

Dr Yi-Long Wu
Methods
• This was an open-label, multicenter study, which was composed of a phase 1b dose escalation part and a
phase 2 dose expansion part
1. https://clinicaltrials.gov/ct2/show/NCT01610336 accessed on Apr 8, 2021
Key eligibility criteria:
• Locally advanced or metastatic
NSCLC harboring EGFR mutation
(exon 19 deletion or L858R)
• Clinical benefit with prior single-agent
EGFR TKI before progression
• Dysregulated MET pathway post-
progression on EGFR TKIsa
• ECOG PS ≤2
• ≥1 measurable lesion according to
RECIST v1.1 (phase 2)
Determine
MTD or
RP2D
At least 18
patients
Initial expansion groupb in
approximately 40 patients
MET dysregulation group in
approximately 90 patients
Phase 2
capmatinib + gefitinib 250 mgPhase 1b
capmatinib + gefitinib 250 mg
aHigh MET expression was defined as ≥50% of tumor cells with IHC 3+, MET gene amplification was defined as gene copy number ≥4 by FISHbEnrollment of patients in the initial expansion group had stopped at the time when protocol Amendment 3 was approved by the Health Authority/Institutional Review Board at the study site.
DOR, duration of response; ECOG PS, Eastern Cooperative Oncology Group Performance Status; EGFR, epidermal growth factor receptor; FISH, Fluorescence In Situ Hybridization; IHC,
Immunohistochemistry; MET, mesenchymal epithelial transition factor; MTD, maximum tolerated dose; NSCLC, non-small cell lung cancer; ORR, overall response rate; OS, overall survival;
PFS, progression-free survival; RECIST, Response evaluation criteria in solid tumors; RP2D, recommended phase 2 dose; TKI, tyrosine kinase inhibitor
STUDY DESIGN1
Endpoints:
Primary:
• ORR per RECIST
v1.1
Secondary:
• OS, DOR, PFS
• Safety and tolerability
• Pharmacokinetic
profile

Results
Patient disposition• The study was completed on May 27, 2020
(last patient last visit), with 61 patients in
phase 1b and 100 patients in phase 2
• Out of the 161 patients who discontinued
from treatment phase, 130 patients (80.7%)
entered the survival follow-up and 31
patients (19.3%) discontinued from study
• Four patients alive at the end of the study
and 1 patient was transferred into a rollover
clinical study
• Most common reason for discontinuation of
study treatment was disease progression
(123 patients, 76.4%), followed by adverse
events (AEs, 19 patients, 11.8%)
Dr Yi-Long Wu
All patients
(N=161)
n (%)
Treatment phase
Completed 6 cycles of treatment
Discontinued from treatment phase
Entered survival follow-up
Discontinued from study
70 (43.5)
161 (100)
130 (80.7)
31 (19.3)
Primary reason for discontinuation from
treatment
Progressive disease
Adverse event
Subject/guardian decision
Death
Non-compliance with study treatment
Physician decision
Protocol deviation
Study terminated by sponsor
123 (76.4)
19 (11.8)
8 (5.0)
7 (4.3)
1 (0.6)
1 (0.6)
1 (0.6)
1 (0.6)

Results
Baseline characteristics• The majority of patients were Asian (81.4%)
and <65 years of age (67.1%)
• The overall median age (range) was 60
years (32-78 years)
• Most patients had a baseline ECOG
performance status of 1 (78.3%)
• 6 patients (3.7%) reported an ECOG
performance status of 2
Dr Yi-Long Wu
Demographic variablePhase 1b
N=61
Phase 2
N=100
Median age (range), years 58.0 (36-77) 61.0 (32-78)
Sex, n (%)
Female
Male
36 (59.0)
25 (41.0)
52 (52.0)
48 (48.0)
Race, n (%)
Asian
Caucasian
53 (86.9)
8 (13.1)
78 (78.0)
22 (22.0)
ECOG performance status, n
(%)
0
1
2
12 (19.7)
45 (73.8)
4 (6.6)
17 (17.0)
81 (81.0)
2 (2.0)

Results
Overall survival• Median follow-up time (range) was 12.2 (0.9-
70.2) months
• The overall median OS (95% CI) was 13.9
(11.6-15.7) months
Dr Yi-Long Wu
Phase 2
N=100
No of events/N (%) 82/100 (82)
Median overall survival (95% CI), months 13.9 (11.6 - 15.7)
% Event-free probability (95% CI)
12 months
24 months
36 months
48 months
58.4 (47.7 - 67.7)
22.9 (14.7 - 32.2)
12.1 (6.2 - 20.0)
10.7 (5.2 - 18.4)

Results
Kaplan-Meier plot of overall survival (Phase 2)
Dr Yi-Long Wu

Results
Safety
• Median duration of exposure (range):
• Phase 1b: 16 (0.4-209.7) weeks
• Phase 2: 18.5 (0.4-268.0) weeks
• 15 patients (9.3%) had died on-treatment
• The majority of deaths (10 patients, 6.2%) were attributed to the study indication, NSCLC
• Two patients (1.2%) died due to pneumonia and 1 patient each (0.6%) died due to dyspnea, myocardial infarction and
cerebrovascular accident.
• Approximately one-third of patients had serious AEs (54 patients, 33.5%).
• The most frequent serious AEs (reported in ≥ 2.0% patients) were pneumonia, dyspnea (7 patients, 4.3%), and pulmonary
embolism (5 patients, 3.1%).
Dr Yi-Long Wu

Results
Safety
• Almost all patients (159 patients, 98.8%)
experienced at least one AE; most being
suspected to be related to study treatment
(140 patients, 87.0%)
• The most frequent AEs of any grade
(reported in ≥25% of patients, regardless of
causality) were nausea (36%), decreased
appetite (32.9%), peripheral edema (32.3%),
hypoalbuminemia (29.8%), vomiting (27.3%),
and rash (25.5%)
Dr Yi-Long Wu
Preferred term
All patients
N=161
All grades n (%) Grade 3/4 n (%)
Total 140 (87.0) 51 (31.7)
Nausea 45 (28.0) 5 (3.1)
Peripheral oedema 37 (23.0) 8 (5.0)
Rash 35 (21.7) 2 (1.2)
Decreased appetite 34 (21.1) 3 (1.9)
Diarrhea 30 (18.6) 1 (0.6)
Paronychia 29 (18.0) 1 (0.6)
Vomiting 29 (18.0) 4 (2.5)
Amylase increased 25 (15.5) 10 (6.2)
Fatigue 23 (14.3) 4 (2.5)
Increased alanine aminotransferase 19 (11.8) 3 (1.9)
Lipase increased 18 (11.2) 10 (6.2)
Treatment-related adverse events (reported in at least 10% of all patients)

Key findings and conclusions
• Capmatinib 400 mg bid in combination with gefitinib 250 mg qd showed encouraging clinical activity in
patients with EGFR-mutant and MET-dysregulated NSCLC
• Median OS (95% CI) was 13.9 (11.6-15.7) months
• The combination was well tolerated
• The most frequent AEs of any grade (reported in ≥25% of patients, regardless of causality) were nausea
(36%), decreased appetite (32.9%), peripheral edema (32.3%), hypoalbuminemia (29.8%), vomiting (27.3%),
and rash (25.5%)
• The data suggests that combining MET inhibitor capmatinib with an EGFR-TKI may be a promising treatment
option for EGFR-mutated, MET-dysregulated NSCLC, particularly for patients with MET amplified tumors
Dr Yi-Long Wu
Related Documents