
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Joseph Priestly – discovers N2O in 1773
Crawford W. Long – 1842. Country Dr. in Georgia first used ether for neck surgery. Did not publicize.Tried to claim credit after Morton’s demonstration but…Important lesson learned – if you don’t publish it, it didn’t happen.
Sir Humphrey Davy – experimented with N2O, reported loss of pain, euphoria
Horace Wells 1844. Demonstrated N2O for tooth extraction –deemed a failure because patient “reacted”.
History of Anesthesia

WORLD ANAESTHESIA DAY
16TH OCT 1846
W.T.G.MORTON
John Collin Warren
Gilbert Abortt
How do Inhalational Anesthetics Work?
Surprisingly, the mechanism of action is still largely unknown.
"Anesthetics have been used for 160 years, and how they work is one of the great mysteries of neuroscience," James Sonner, M.D. (UCSF)
Lipid Theory
Membrane Stabilization Theory
Promiscuous Receptor Agonist Theory:
Anesthetics may act at GABA receptors, NMDA receptors, other receptors
Modifying functions of ION CHANNELS (opening of
inhibitory ion channels (Cl- or K+) and closing of excitatory ion channels (Na+)
Speed(extremely rapid action and fast changes in level of anesthesia)
Faster turnover/recovery times
Route of administration- lungs (get 100% of cardiac output)
Margin of safety

The main target of inhalation anesthetics is the brain.
Goal
To develop and maintain a satisfactory
partial pressure or tension of anesthetic at
the site of anesthetic action in brain.
Alveolar concentration of anesthetic gas is
indirectly reflects brain concentration.
PA PB
Vaporizer
Breathing Circuit
Alveoli (lungs)
Arterial Blood
Tissues (VRG [brain], MUS,FAT)
Venous blood (coming back to lungs)
Alveoli (lungs, again)
Breathing Circuit (to be rebreathed)

Time constant
Uptake and distribution of anestheticgases
FI
FA
FD
MAC
Brain Partial pressure
drives depth of
anesthesia
Equilibrates
Ventilation
λB/G
CO
PA - PV
λT/BTissue blood flow
[Parterial - PTissue]
12
FA/FI
Concentration and
second gas effects
Time constant
VRG

The absorption phase is usually called -
uptake
The metabolic phase is usually called -
biotransformation
The excretion phase is usually called –
elimination.
lowering of drug concentration in one compartment by delivery into another compartment is called
redistribution
Partial Pressure-the pressure a gas exerts- proportional
its fractional mass
AdditivePatm = PO2 + PN2
=160mmHg + 600mmHg
= 760mmHg
Ptotal= Pgas1+ Pgas2+ ….+Pgas N
(Dalton’s law)
Same pressure each gas would have if
IT ALONE occupied the same volume

Pressure- gas phase
Concentration – amount of gas
dissolved in a solution.
Solubility = volume of gas
volume of liquid
(at standard temperature)
What is “ PARTIAL PRESSURE OF GAS” in
solution?
Reflects a “force” of gas to escape
out of solution ( think of CO2 in a bottle
of soda)
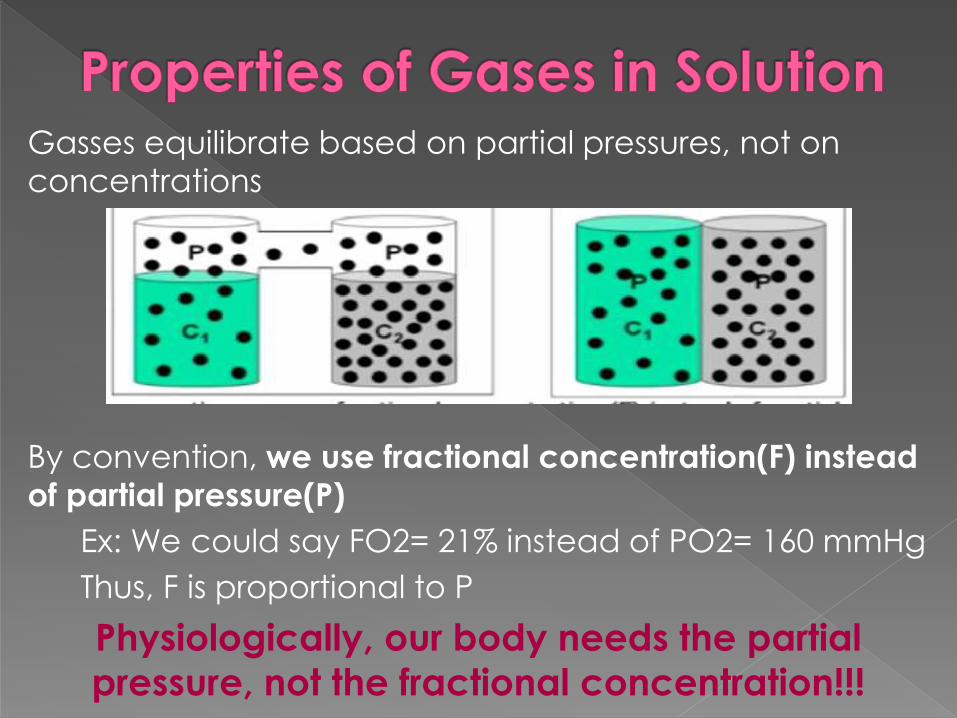
Gasses equilibrate based on partial pressures, not on
concentrations
By convention, we use fractional concentration(F) instead
of partial pressure(P)
Ex: We could say FO2= 21% instead of PO2= 160 mmHg
Thus, F is proportional to P
Physiologically, our body needs the partial
pressure, not the fractional concentration!!!
Henry”s law: Cg = k Pg
Cg - is concentration of gas in solution
k - is a solubility constant
Pg - is the partial pressure of the gas
Physiologically,
Anesthetic gases work based on partial
pressure in the brain, not fractional
concentration
Anesthetic gases work based on partial
pressure in the brain, not fractional
concentration !
The vaporizers are calibrated to deliver a set
partial pressure, NOT a set fractional
concentration!SEVO vaporizer only delivers 1% sevoflurane
when P atm= 760mmHg.
But it will always deliver(appr) the correct partial
pressure of sevoflurane at any altitude.
True for ALL vaporizers EXCEPT DESFLURANE

Getting agent from the anesthesia
machine into the brain so the patient goes to sleep!!!
Goal: achieve “steady state” of anesthetic partial pressures throughout the system
Vaporizer adds agent to the fresh gas flow at a fixed concentration
Fresh gas mixes with circuit gas (bag, tubing canister, piping), dilutes concentration of agent
Compartments equilibrate and concentration of agent in the circuit rises

Fractional concentration of agent leaving the
circuit is Fi (fraction inspired)
Fractional concentration of agent in the lungs is FA (fraction alveolar)
Initially, FA/Fi = 0 because Fa is a 0
No agent in the lungs yet
These compartments will also equilibrate over time
You will be at EQ when FA=Fi, or FA/Fi=1
Fast induction is defined as FA/Fi → 1 quickly

ANAESTHESIC
MACHINE BREATHING
CIRCUIT
LUNGS
ARTERIAL
BLOOD
VENOUS
BLOOD
BRAIN
FGF
FI
FA
Fa
Path of anesthetic

FFGO -is the fraction of inspired
anesthetic in the gas leaving the fresh
gas outlet.
T - is time.
τ - is a time constant.
The time constant is simply the
volume or “capacity” of the circuit
(VC) divided by the fresh gas flow (FGF) or τ = VC/FGF.
Concentration in the circuit (FI) will
rise according to first-order kinetics:

Concentration of (FA) will rise
analogous to Fi
FA -is the alveolar concentration
T - is time.
τ -is a time constant.
The time constant for raise of FA
concentration and equals FRC/VA
FRC-functional residual capacity
VA- minute ventilation
The time required for flow through a
container to equal the capacity of the
container.
TC is volume (capacity)/flow.
The time constant for the lungs is
FRC/Valveolar.
The time constant for the anesthesia circuit
is circuit capacity/FGF.
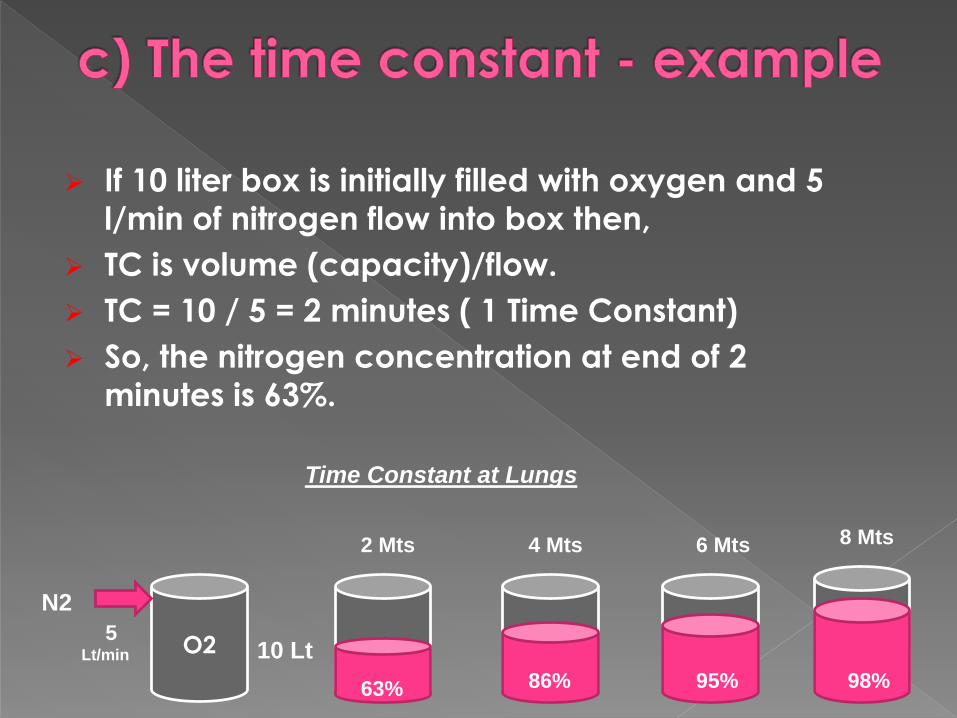
If 10 liter box is initially filled with oxygen and 5
l/min of nitrogen flow into box then,
TC is volume (capacity)/flow.
TC = 10 / 5 = 2 minutes ( 1 Time Constant)
So, the nitrogen concentration at end of 2
minutes is 63%.
O2 10 Lt5
Lt/min
2 Mts 4 Mts 6 Mts 8 Mts
63% 86% 95% 98%
N2
Time Constant at Lungs
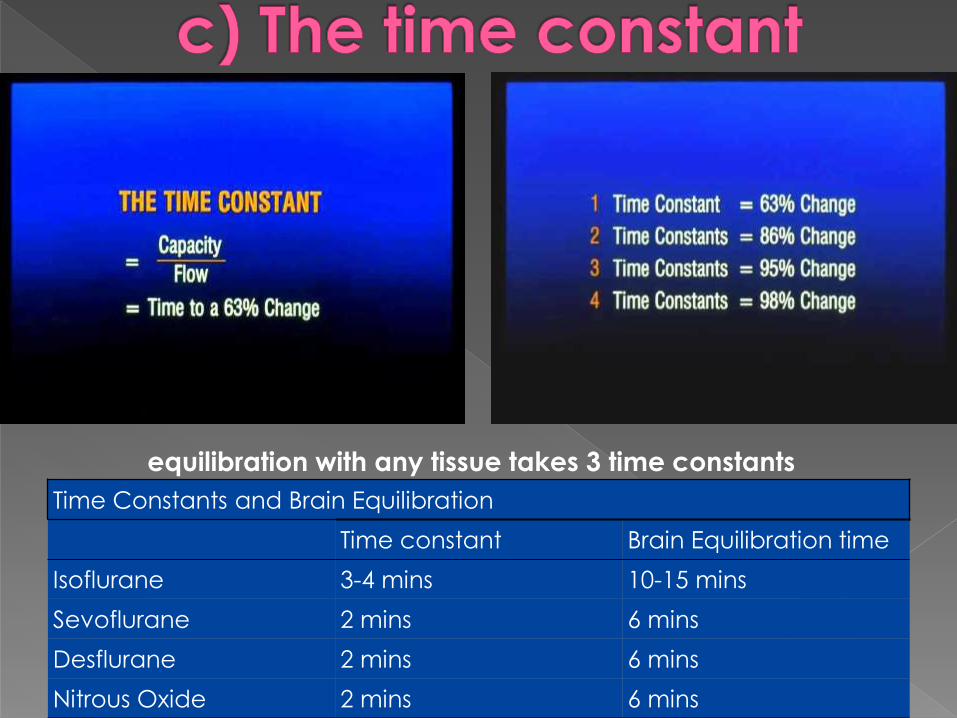
Time Constants and Brain Equilibration
Time constant Brain Equilibration time
Isoflurane 3-4 mins 10-15 mins
Sevoflurane 2 mins 6 mins
Desflurane 2 mins 6 mins
Nitrous Oxide 2 mins 6 mins
equilibration with any tissue takes 3 time constants

a) The inspired concentration (FI)Inspired concentration - FA/FI
b) The alveolar ventilation (Valveolar)- Minute alveolar ventilation - FA/FI
- Larger the FRC - slows raise of alveolar concentration
c) The time constant
d) Anesthetic uptake by the blood
e) The concentration and second gas effects

1) Fresh Gas Flow rate:↑ FGF → ↑ speed of induction & recovery.
2) Volume of breathing circuit (apparatus dead space): incr. ↑volume → slower induction (dilution of anesthetic gases.)
3) Absorption by the breathing circuit: rubber tubing absorbs ˃plastic & silicon.

Increase in
Minute alveolar ventilation
Increases FA/FI
The change is greatest for
more soluble anesthetics
methoxyflurane - increases by 75%
isoflurane - by 18%
desflurane - by only 6%.
negative feedback that results
from respiratory depression
high ventilation → rapid
induction → hypoventilation

Increase FA/FI Decrease FA/FIComment
Low blood solubility High blood solubility
As the blood solubility
decreases, the rate of rise in
FA/FI increases.
Low cardiac output High cardiac output The lower the cardiac
output, the faster the rate of
rise in FA/FI
High minute ventilation Low minute ventilation The higher the minute
ventilation, the faster the
rate of rise in FA/FI
Factors that Increase or Decrease the Rate of Rise of FA/FI
Uptake from the lung = Blood solubility x Cardiac Output x [PA-PV]
Bar. pressure
50%O2
50%N2O2Lt
2Lt
4Lt
33%N2O
66%O2
3Lt
2Lt
1Lt
Uptake of half
of the N2O
38%N2O
62%O2
1Lt of N2O
1 Lt
50%O2 + 50%N2O
Ventilation Effect Inspired Gas
1.5Lt
4Lt
2.5Lt
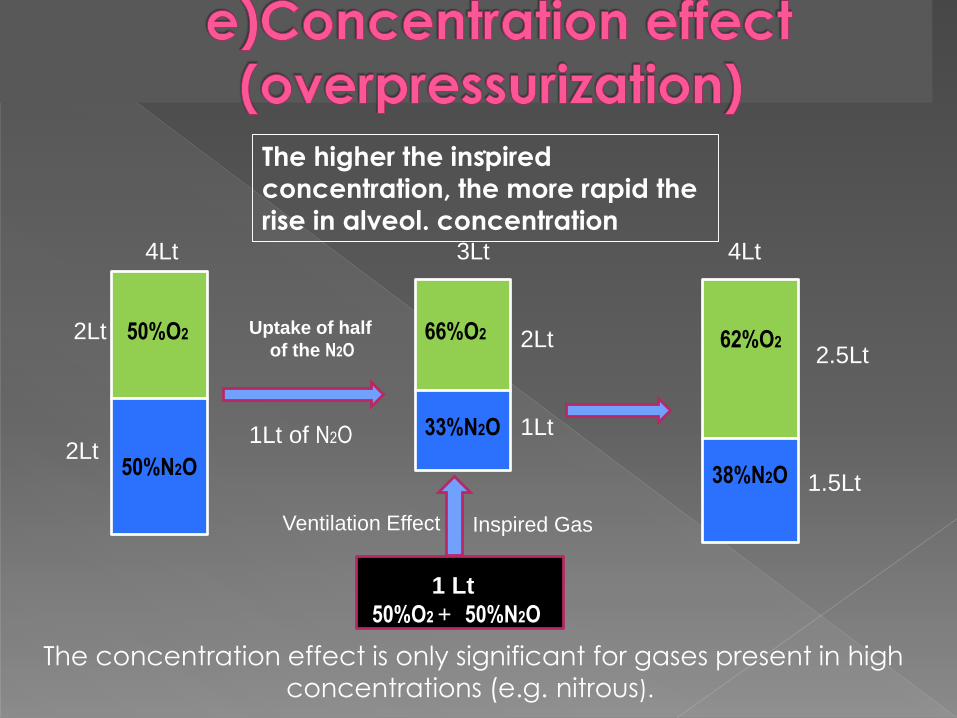
The higher the inspired
concentration, the more rapid the
rise in alveol. concentration
.
The concentration effect is only significant for gases present in high
concentrations (e.g. nitrous).

.
Two components:
1.the concentrating effect 2.an augmented gas inflow effect

Administration of 70% nitrous oxide produces a more rapid rise in the
FA/FI ratio of nitrous oxide than
administration of 10% nitrous oxide
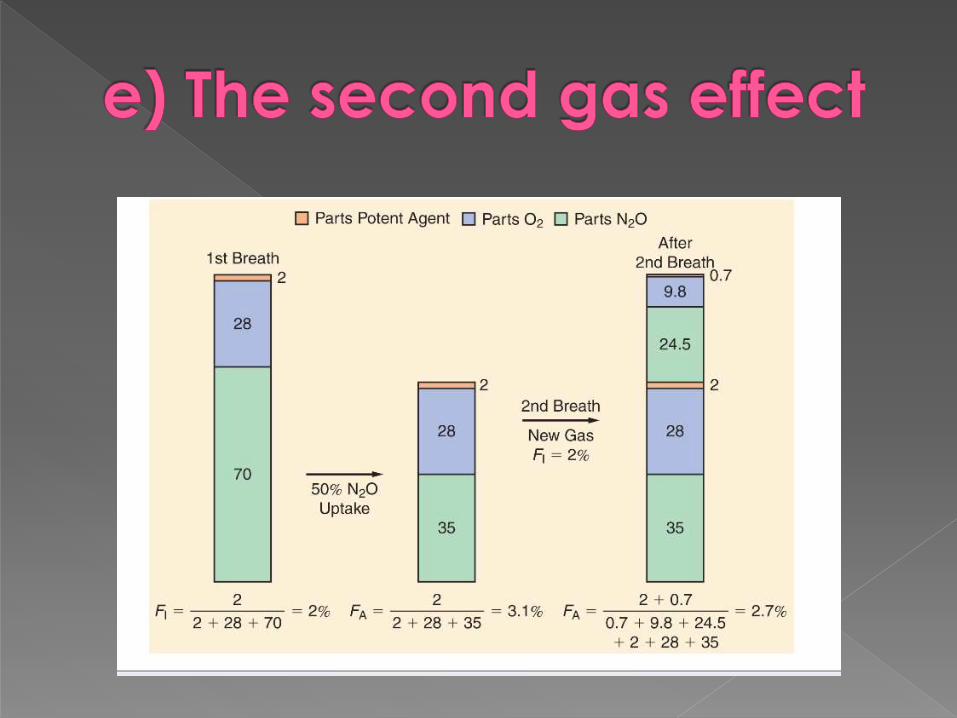
The FA/FI ratio for 0.5% halothane rises more rapidly when given with
70% nitrous oxide than when given with 10% nitrous oxide.
Concentration effect
Second gas effect

Factors raising the alveolar concentration (FA/FI )
a) The inspired concentration (FI)
b) The alveolar ventilation (Valveolar)
c) The time constant
d) Anesthetic uptake by the blood
e) The concentration and second gas effects

Factors determining uptake by blood
A. Solubility in blood
B. Cardiac Output
C. The mixed venous anesthetic concentration
d. Tissue uptake of anesthetic

Uptake from the lung = Blood solubility x Cardiac Output x [PA-PV]
Barometric pressure
U Lung = λB/G x Q x ((PA-Pvenous)
Barometric pressure
Fick equation
λB/G - blood:gas partition coefficient
Q - cardiac output
PA - alveolar partial pressure of anesthetic
Pv - mixed venous partial pressure of anesthetic
PB is barometric pressure.
Solubility is defined in terms of the partition coefficient
Partition coefficient is the ratio of the
amount of substance present in one phase compared with another, the two phases
being of equal volume and in equilibrium
[λB/G = CB ]
CG

Gas
Blood
Partition Coefficient = Ratio of Concentration
Concentrations Equilibirates
Partial pressure Equalize
CG =CB
PG = PB
Halothane
λB/G = CB = 2.5 = 2.5
CG 1
Equal volume
Partial pressures are equal but concentrations are not !!!

Blood has 50 balls of halothane/ml Gas has 20 balls of halothane / ml
Halothane blood / gas partition coefficient = 2.5
No net diffusion when
partial pressures are
equal.

Blood has 8 balls / ml desflurane Gaseous desflurane has 20 balls /ml
Desflurane blood / gas partition coefficient = 0.42
No net diffusion when
partial pressures are
equal.

Higher solubility (λB/G>1)= more agent in the blood and less in the gas phase.
A lower solubility (λB/G<1)= less agent in the blood and more in the gas phase.
Other partition coefficients:
-Brain:Blood, Muscle:Blood, Fat:Blood(describe movement of gas from one
environment to another)
Blood-GasBrain-
Blood
Liver-
Blood
Kidney-
Blood
Muscle-
Blood
Fat-
Blood
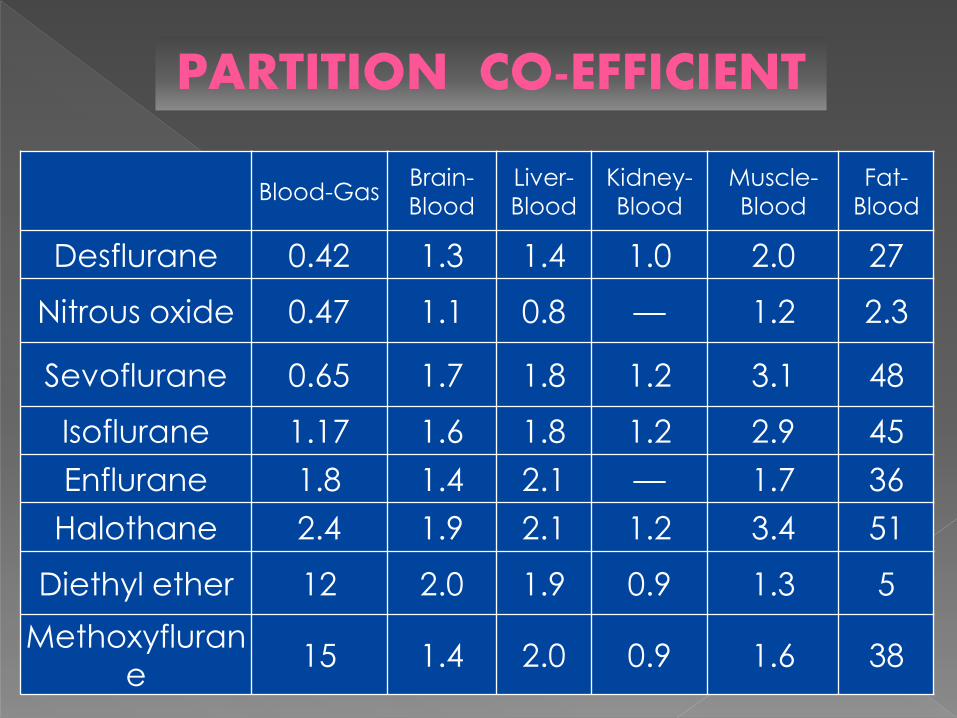
Desflurane 0.42 1.3 1.4 1.0 2.0 27
Nitrous oxide 0.47 1.1 0.8 — 1.2 2.3
Sevoflurane 0.65 1.7 1.8 1.2 3.1 48
Isoflurane 1.17 1.6 1.8 1.2 2.9 45
Enflurane 1.8 1.4 2.1 — 1.7 36
Halothane 2.4 1.9 2.1 1.2 3.4 51
Diethyl ether 12 2.0 1.9 0.9 1.3 5
Methoxyfluran
e15 1.4 2.0 0.9 1.6 38
PARTITION CO-EFFICIENT
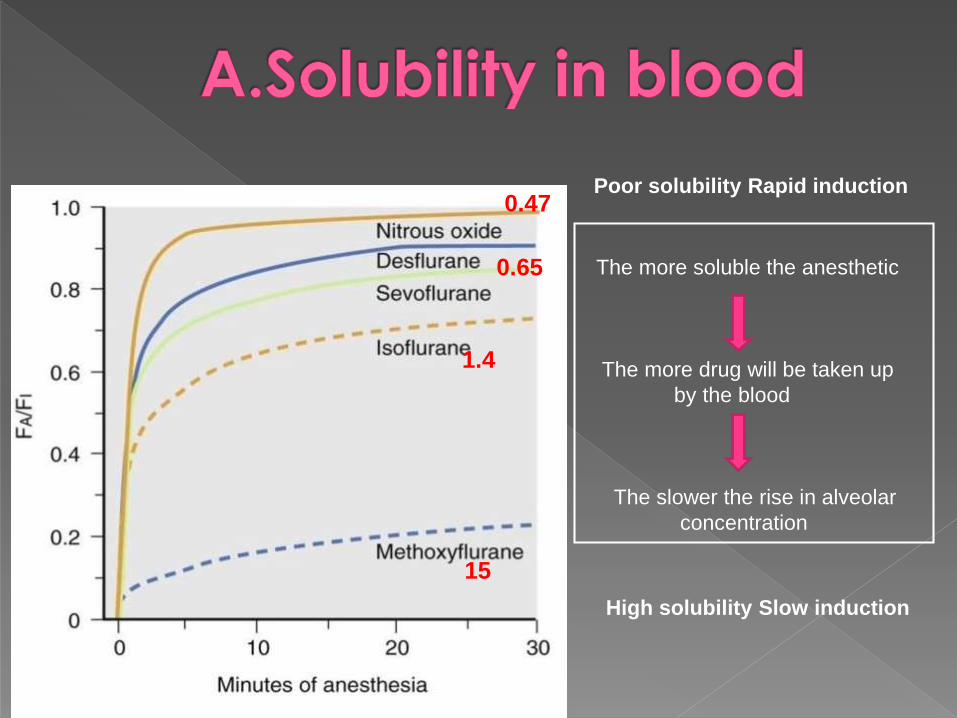
The more soluble the anesthetic
The more drug will be taken up
by the blood
The slower the rise in alveolar
concentration
15
1.4
0.65
0.47Poor solubility Rapid induction
High solubility Slow induction
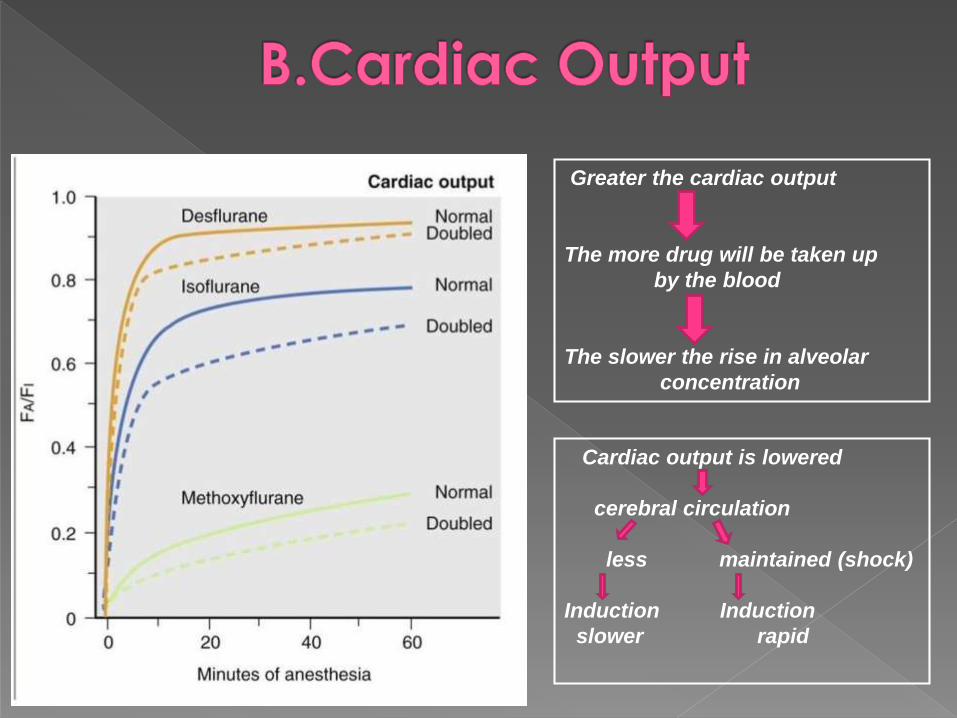
Greater the cardiac output
The more drug will be taken up
by the blood
The slower the rise in alveolar
concentration
Cardiac output is lowered
cerebral circulation
less maintained (shock)
Induction Induction
slower rapid

An increase in CO from 2 to 18 L/min
will decrease the alveolar anesthetic
concentration by augmenting
uptake, thereby slowing the rise of the FA/FI ratio.
B.Cardiac Output(Perfusion Effects)
More soluble anesthetics (halothane)
- effect is more prominent
Positive feedback - as inspired
concentration increases, greater cardiovascular depression reduces
anesthetic uptake and actually
increases the rate of rise of FA/FI.
The difference between partial pressure in the alveoli and that in venous blood
Partial pressure in venous blood depends on tissue uptake of anesthetic
At equilibrium, (no tissue uptake)
The venous partial pressure = arterial partial pressure = alveolar partial pressure
PA – PV = 0
Rate of rise of the mixed venous concentration depends on the tissue uptake of the anesthetic

AT EQUILIBRIUM
No
tis
sue
up
tak
e
PA
PV
PA – PV = 0
PA = PV
FA/FI
FAT
VRG
MG
4-8mts
2-6Hrs
3-4 days
1. The tissue/blood partition coefficient (tissue solubility)
2. The tissue blood flow.
3. The tissue anesthetic concentration
Tissue Uptake = Tissue solubility x Tissue blood flow x [Parterial - PTissue]
Atmospheric pressure

Gas
BloodTissue
Concentrations Equilibirates
Partial pressure Equalize
CG =CB = CT
PG = PB = PT
Equal volume
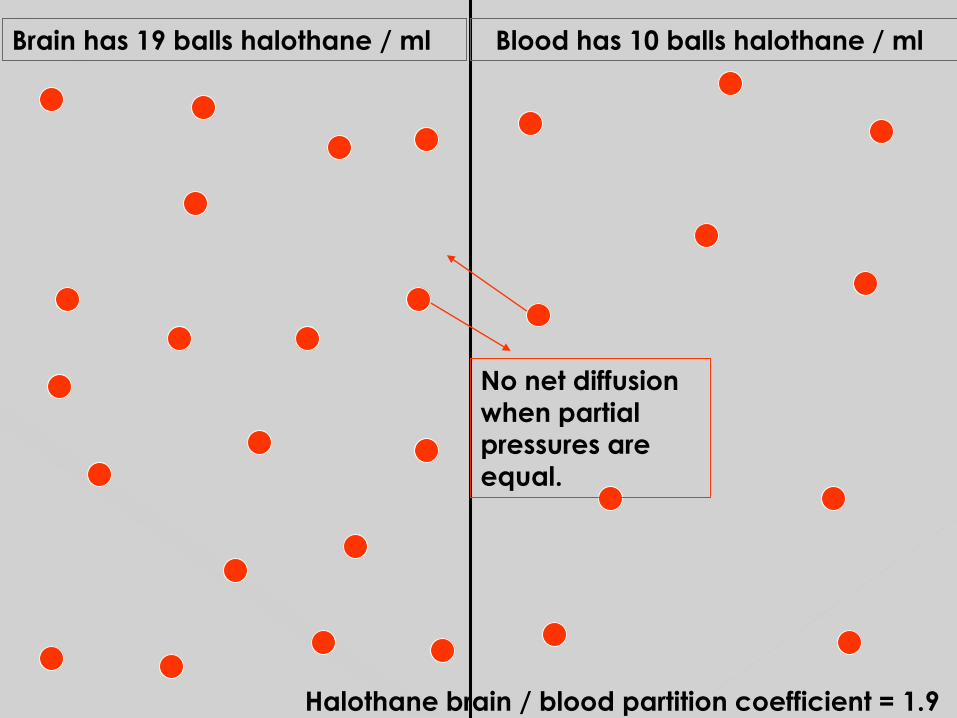
Brain has 19 balls halothane / ml Blood has 10 balls halothane / ml
Halothane brain / blood partition coefficient = 1.9
No net diffusion
when partial
pressures are
equal.

Brain has 11 balls N2O / ml Blood has 10 balls N2O / ml
N2O brain / blood partition coefficient = 1.1
No net diffusion
when partial
pressures are
equal.
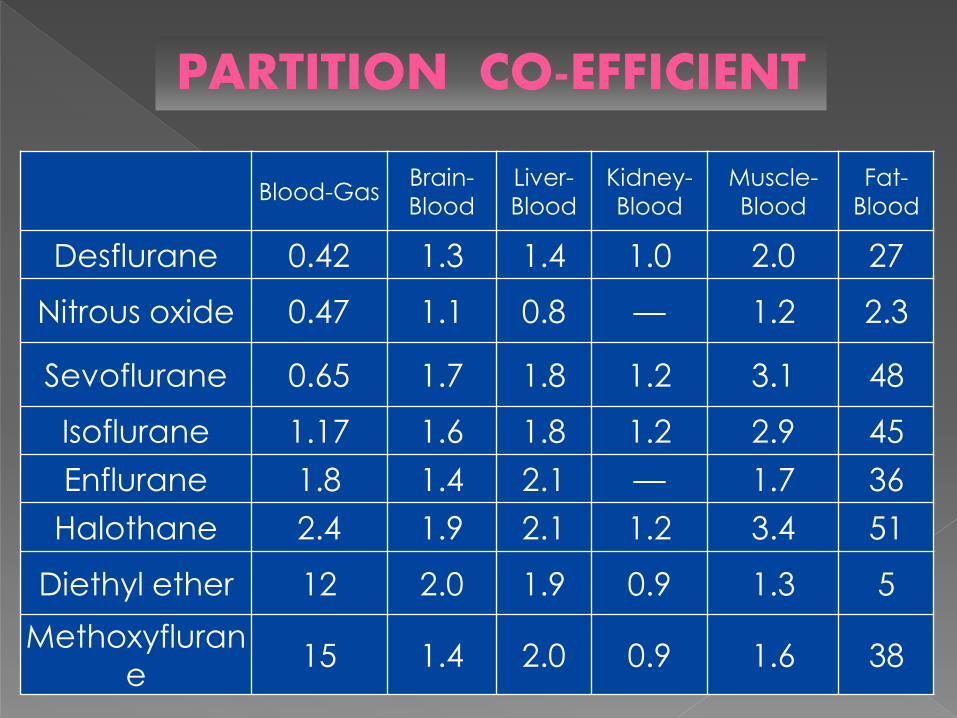
Blood-GasBrain-
Blood
Liver-
Blood
Kidney-
Blood
Muscle-
Blood
Fat-
Blood
Desflurane 0.42 1.3 1.4 1.0 2.0 27
Nitrous oxide 0.47 1.1 0.8 — 1.2 2.3
Sevoflurane 0.65 1.7 1.8 1.2 3.1 48
Isoflurane 1.17 1.6 1.8 1.2 2.9 45
Enflurane 1.8 1.4 2.1 — 1.7 36
Halothane 2.4 1.9 2.1 1.2 3.4 51
Diethyl ether 12 2.0 1.9 0.9 1.3 5
Methoxyfluran
e15 1.4 2.0 0.9 1.6 38
PARTITION CO-EFFICIENT

The rate of rise in tissue anesthetic concentration is
proportional to tissue blood flow and inversely
proportional to the tissue capacity.
The tissue capacity = tissue solubility х tissue volume
Just as discussed for the lungs, the tissues have a time
constant too:
Time Constant = Tissue solubility x Volume
Flow


Equilibration of
the VRG complete
in 4 to 8 minutes
After 8 minutes,
the Muscle group
(MG) determines
most of uptake.
Once MG
equilibration is
complete Fat
group (FG)
determines the
uptake
Two important characteristics of
Inhalational anesthetics which govern
the anesthesia are :
Solubility in the blood(blood : gas partition co-efficient)
Solubility in the fat
(oil : gas partition co-efficient)
It indicates the amount of gas that is
soluble in oil phase.
It is a measure of lipid solubility of
anesthetic.
It is a measure of anesthetic potency
Higher the lipid solubility – potent anesthetic.
(e.g., halothane)

Meyer – Overton Rule
Anesthetic potency
correlates with lipid
solubility
Holds true across species
Because inhalation agents act through the lipid-rich
CNS cells, anesthetic potency increases with
lipid solubility.

OIL GAS PARTITION CO-EFFICIENT
Higher the Oil: Gas Partition
Co-efficient lower the MAC .
E.g., Halothane
1.4 220
0.8
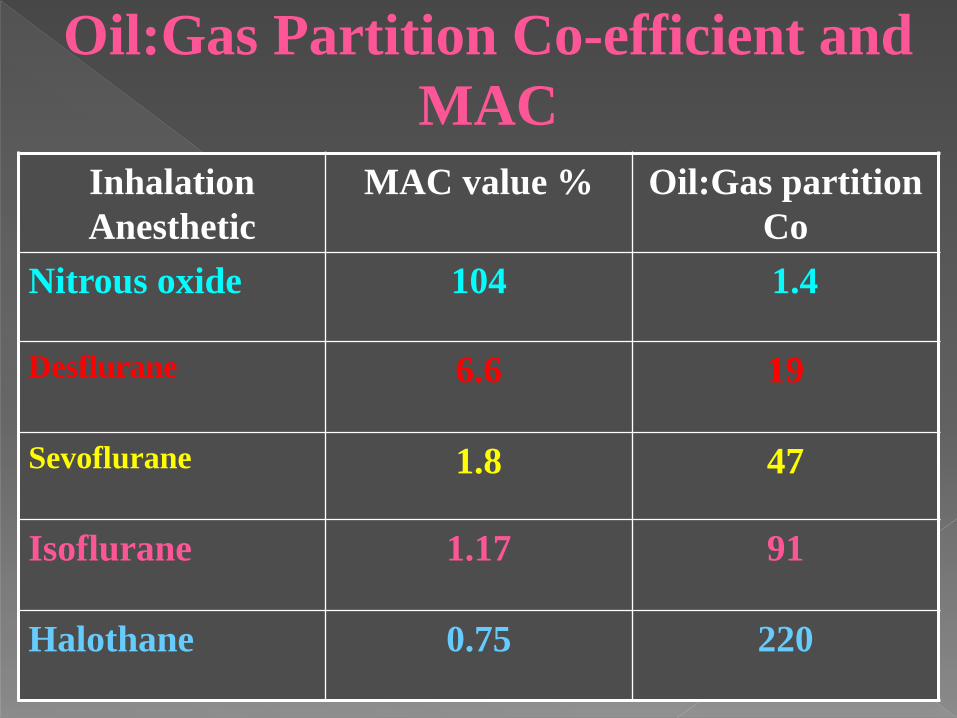
Inhalation
Anesthetic
MAC value % Oil:Gas partition
Co
Nitrous oxide 104 1.4
Desflurane 6.6 19
Sevoflurane 1.8 47
Isoflurane 1.17 91
Halothane 0.75 220
Oil:Gas Partition Co-efficient and
MAC
At EQ:PA(alveoli)= Pblood =PCNS
Rapid transfer of gases:
alveoli > blood > CNS
F is proportional to P, so
1% SEV in the alveoli = 1% SEV in the CNS
At EQ, if you know PA of a gas, then
you know PCNS

Recovery from anesthesia, like induction, depends on:
anesthetic solubility- is the primary determinant of the rate of fall of FA
cardiac output
minute ventilation
Loss of inhaled anesthetics via skin, gastrointestinal viscera and the pleura are insignificant

The greater the solubility of inhaled anesthetic, the
larger the capacity for absorption in the bloodstream
and tissues.

The “reservoir” of anesthetic in the body at
the end of administration depends on:
1. Tissue solubility (which determines the capacity)
2. The dose
3. Duration of anesthetic (which determine how
much of that capacity is filled).
Low solubility→Rapid recoveryDesflurane>Sevoflurane>Isoflurane
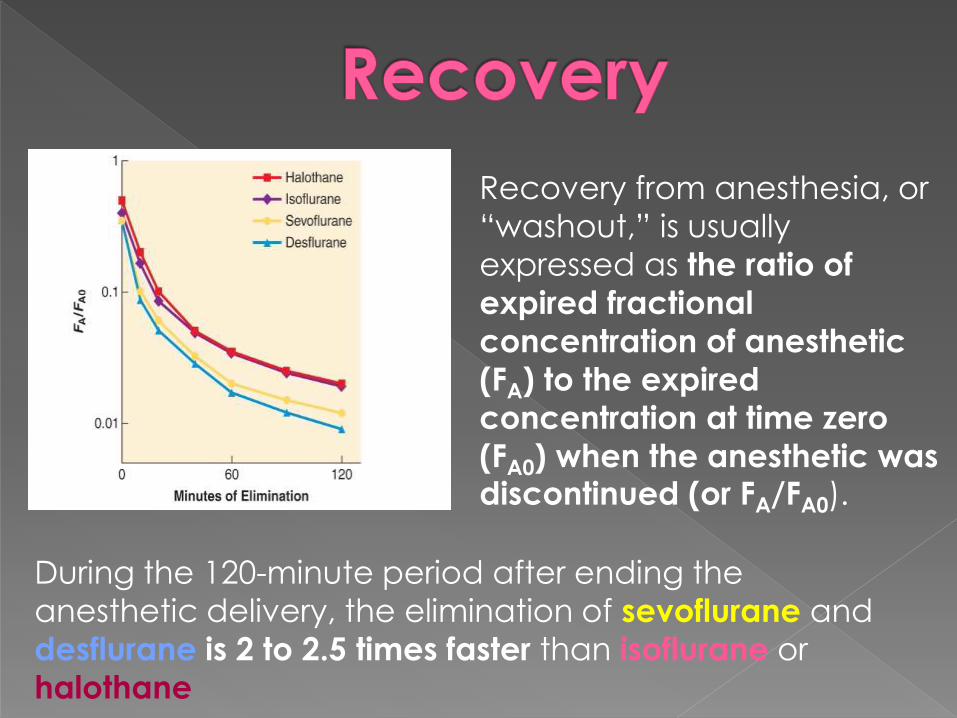
Recovery from anesthesia, or
“washout,” is usually
expressed as the ratio of
expired fractional
concentration of anesthetic
(FA) to the expired
concentration at time zero
(FA0) when the anesthetic was discontinued (or FA/FA0).
During the 120-minute period after ending the
anesthetic delivery, the elimination of sevoflurane and
desflurane is 2 to 2.5 times faster than isoflurane or
halothane

The longer the duration of a highly soluble anesthetic, the greater
the reservoir of anesthetic in the body, and the higher the curve
seen in the right half( slow recovery)
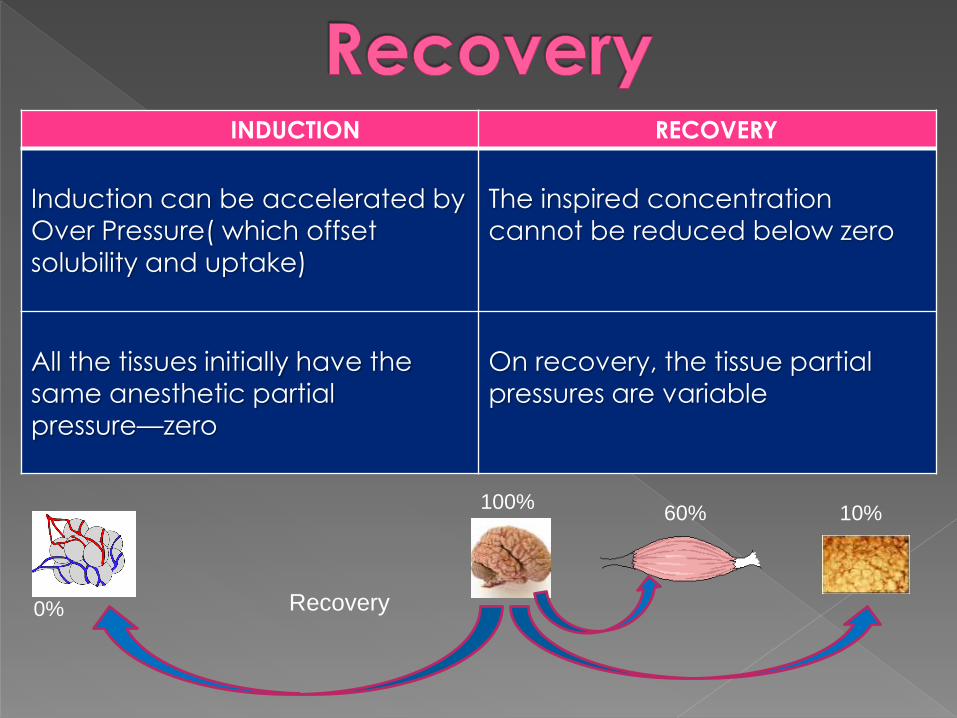
INDUCTION RECOVERY
Induction can be accelerated by
Over Pressure( which offset solubility and uptake)
The inspired concentration
cannot be reduced below zero
All the tissues initially have the
same anesthetic partial
pressure—zero
On recovery, the tissue partial
pressures are variable
100%60% 10%
0% Recovery
As long as an arterial-to-tissue partial pressure gradient exists, muscle and fat will absorb anesthetic(especially fat).
After discontinuation of anesthesia, muscle and fat may continue to absorb anesthetic, even hours later.
The redistribution continues until blood/alveolar anesthetic partial pressure falls below tissue partial pressure.
1. Increased solubility slows recovery
2. Increasing ventilation may help the recovery
from potent agents
3. Prolonged anesthesia delays recovery
4. There is no concentration effect on
emergence
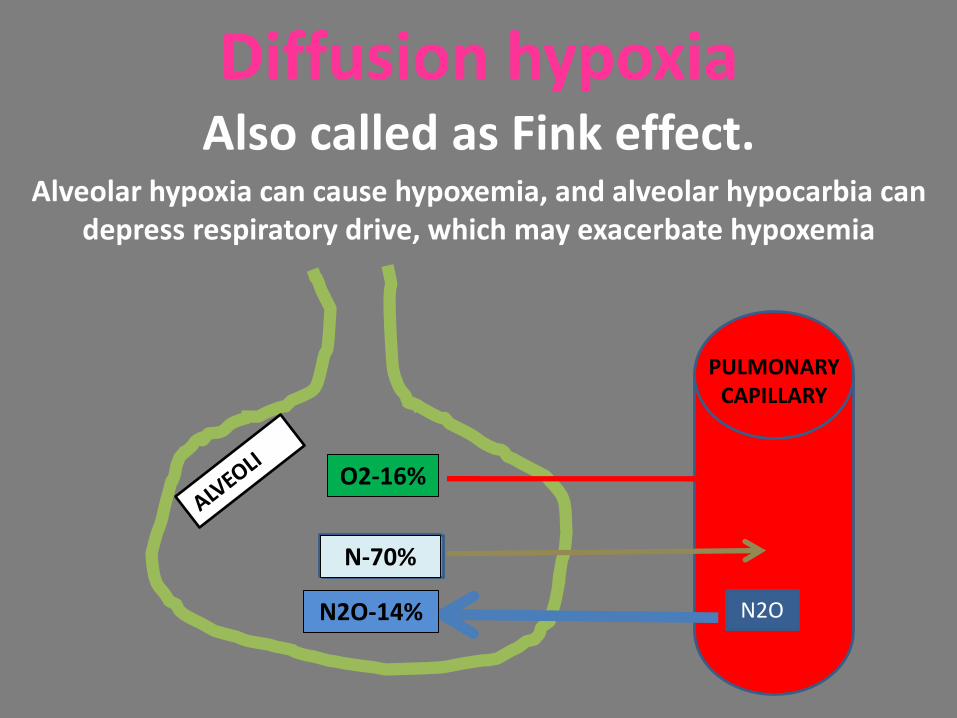
Diffusion hypoxiaAlso called as Fink effect.
Alveolar hypoxia can cause hypoxemia, and alveolar hypocarbia can depress respiratory drive, which may exacerbate hypoxemia
N2O
N- 79%
O2-21%O2-21%
N- 79%
N2O
O2-16%
N-70%
N2O-14%
PULMONARY CAPILLARY

MAC - is the alveolar concentration of
an anesthetic at 1 atm that prevents
movement in response to a surgical
stimulus in 50% of patients.
Analogous to the ED50 expressed for
intravenous drugs.
MAC value is a measure of inhalational
anesthetic potency.

AGENT MAC POTENCY
Methoxy-flurane 0.16% Most potent
Halothane 0.74%
Isoflurane 1.17%
Enflurane 1.7%
Sevoflurane 2.05%
Desflurane 6.0%
Nitrous oxide 104% Least potent
The lower the MAC– the more potent the agent!
Standard MAC values are roughly additive !!!
Administering 0.5 MAC of a potent
agent and 0.5 MAC of nitrous
oxide is equivalent to 1 MAC of
potent agent.
MAC effects for other response parameters are
not necessarily additive !!!
Combining 0.6 MAC of nitrous
oxide with 0.6 MAC of isoflurane
produces less hypotension than
1.2 MAC of isoflurane alone.

MAC awake: MAC allowing voluntary response tocommand in 50% of patients(0.15 – 0.5 MAC)
MAC 95%: MAC that prevents movement in 95 % ofpatients (1.2-1.3 MAC or +25% of MAC)
MAC intubation: MAC that allows intubation withoutmuscle relaxant, coughing or bucking in 50% ofpatients.
MAC-BAR (1.7-2.MAC or +50% of stand. MAC), whichis the concentration required to block autonomicreflexes to nociceptive stimuli.

MAC in Subjects Ages 30 to 60
Inhaled
Anesthetics
In O2 60%-70%
N2O
MACAWAKE MAC BAR
Desflurane 6.6% 2.83% 2.42% 1.45 MAC
Sevoflurane 1.8% 0.66% 0.61% 2.24 MAC
Isoflurane 1.17% 0.56% 0.39% 1.30 MAC
Halothane 0.75% 0.29% 0.41% 1.30 MAC


MAC decreases with
age - 6% per decade
(similar between agents)
MAC- is maximum at 6
months

Duration of inhaled anesth. administration
Gender
Type of surgical stimulation
Thyroid function
Hypo- or hypercarbia
Metabolic alkalosis
Hyperkalemia
And magnesium levels
Red-haired females have a 19% increase in MAC compared with dark-haired females. These data suggest involvement of mutations
of the MCIR(melanocyte stimulating hormone receptor) allele.

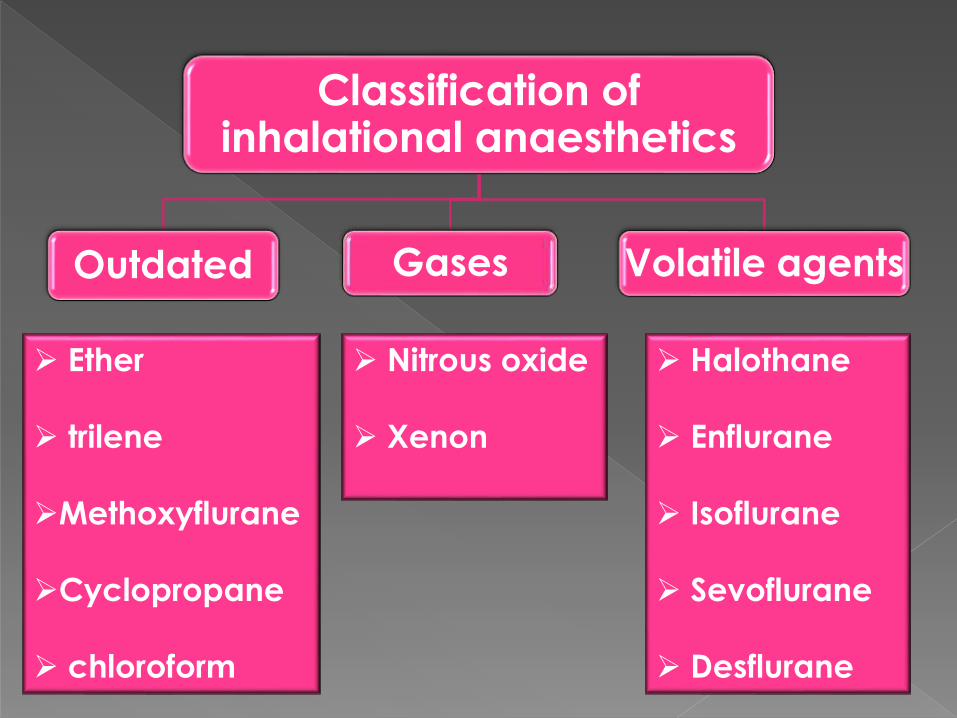
Classification of inhalational anaesthetics
Outdated Gases Volatile agents
Ether
trilene
Methoxyflurane
Cyclopropane
chloroform
Nitrous oxide
Xenon
Halothane
Enflurane
Isoflurane
Sevoflurane
Desflurane
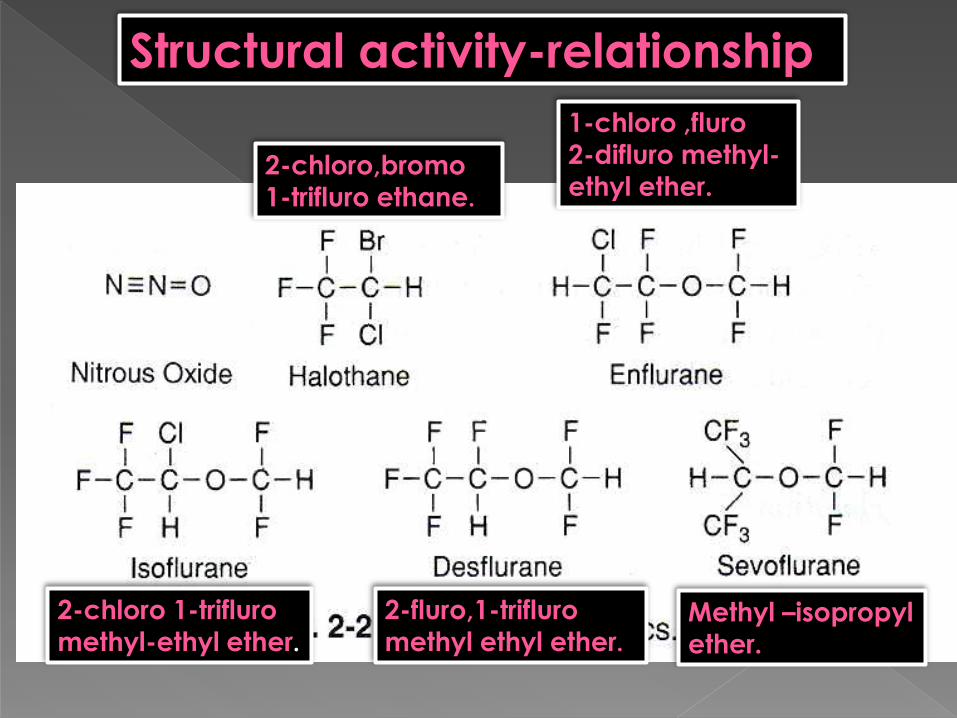
Structural activity-relationship
2-chloro,bromo
1-trifluro ethane.
Methyl –isopropyl
ether.
2-fluro,1-trifluro
methyl ethyl ether.
2-chloro 1-trifluro
methyl-ethyl ether.
1-chloro ,fluro
2-difluro methyl-
ethyl ether.

All agents cause CBF, causing ICP(especially Halothane) and impair autoregulation of vascular tone( least with sefoflurane at<1MAC)
Volatile agents cerebral metabolic rate, N2O may
Desflurane and isoflurane at < 1 MAC can suppress status epilepticus while sevoflurane concentrations associated whith epileptiform EEG.
All agents SEP/MEP signals.(sensory-evoked potentials and motor-evoked potentials (MEPs).
All agents decreases CMRO2 :
Desflurane=Isoflurane=Sevoflurane>Halothane
Cerebral Metabolic Rate and Electroencephalogram
EEG an isoelectric-no further decreases in CMR are
generate, however:
Desflurane-induced isoelectric EEG reverts to
continuous activity with time, despite an unchanging
MAC, a property unique to Desflurane
All of the potent agents depress CMR to
varying degrees !!!
Isoflurane abolishes EEG activity at doses
used clinically, while Sevoflurane and
Desflurane at 2 MAC
Desflurane and Isoflurane at < 1 MAC
can suppress status epilepticus while
Sevoflurane concentrations associated whith
epileptiform EEG.

All of the potent agents increase CBF in a time-
dependent as well as dose-dependent manner !!!
Desflurane=Isoflurane=Sevoflurane<Halothane
The increase in CBF with increasing dose caused by the
potent agents occurs despite decreases in CMR -
cerebral uncoupling .
↓CMR→ vasoconstrictia (physiologicly), with VA
vasodilatory effect
Because the volatile anesthetics are direct
vasodilators, all are considered to diminish
autoregulation in a dose-dependent fashion.
Sevoflurane preserves autoregulation up to approx.1MAC.
At 1.5 MAC sevoflurane preserves better than isoflurane(This
may be a result of less of a direct vasodilator effect of
sevoflurane).
0.5 MAC desflurane reduced autoregulation and
isoflurane did not. At 1.5 MAC, both anesthetics
substantially reduced autoregulation.
Significant hypercapnia is associated with
dramatic increases in CBF whether or not
volatile anesthetics are administered.
Hypocapnia can blunt or abolish volatile
anesthetic-induced increases in CBF
depending on when the hypocapnia is
produced.

The increase in CBF→ ↑ICP
Isoflurane, sevoflurane and desflurane >1 MAC
produce mild increases in ICP, paralleling their mild increases in CBF.
All three potent agents may be used at appropriate
doses, especially with adjunctive and compensatory
therapies, in just about any neurosurgical procedure.
Isoflurane does not appear to alter CSF production, but may increase, decrease, or leave unchanged the resistance to resorption depending on dose.
Sevoflurane at 1 MAC depresses CSF production up to 40%.
Desflurane at 1 MAC leaves CSF production unchanged or increased.
In general, anesthetic effects on ICP via changes in CSF dynamics are clinically far less important than
anesthetic effects on CBF.

A common effect of the potent
volatile anesthetics has been a dose-related decrease in arterial
blood pressure
Primary mechanism to decrease
blood pressure with increasing dose
is lowering regional and systemic
vascular resistance.
Sevoflurane up to about 1 MAC results in minimal, if any, changes in
steady-state heart rate while
enflurane, isoflurane, and
desflurane increase it 5 to 10% from
baseline
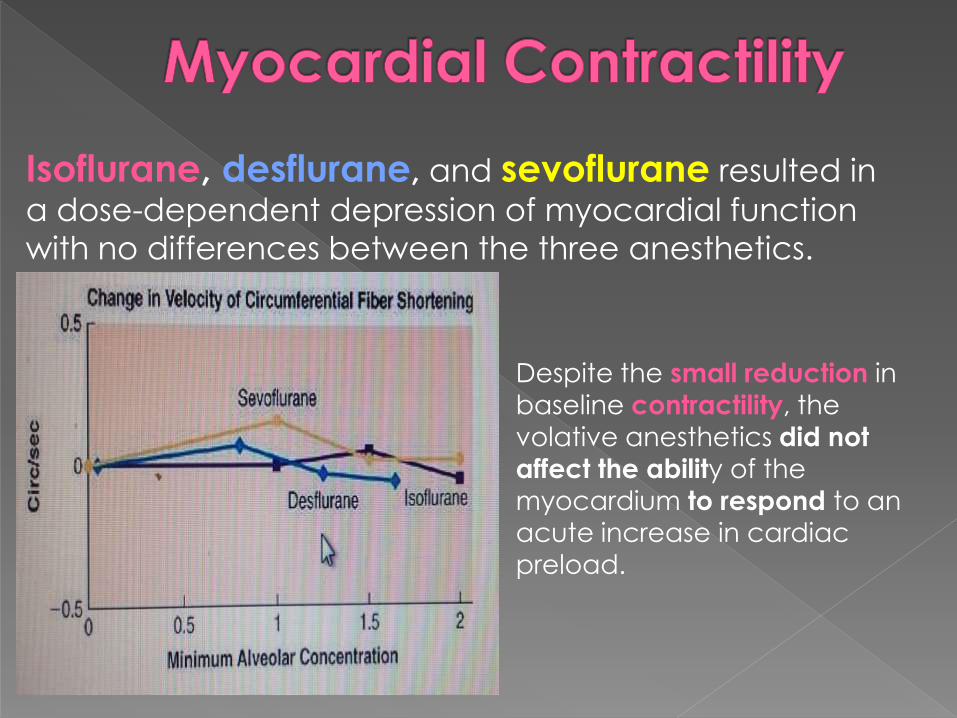
Isoflurane, desflurane, and sevoflurane resulted in
a dose-dependent depression of myocardial function
with no differences between the three anesthetics.
Despite the small reduction in
baseline contractility, the
volative anesthetics did not
affect the ability of the
myocardium to respond to an
acute increase in cardiac preload.

Most of the volatile anesthetics have been studied
during both controlled and spontaneous ventilation.
Spontaneous ventilation(SV) reduces the high
intrathoracic pressures from positive pressure
ventilation.
The negative intrathoracic pressure during the
inspiratory phase of spontaneous ventilation augments
venous return and cardiac filling and improves cardiac
output and, hence, blood pressure.
SV is associated with higher PaCO2, causing cerebral
and systemic vascular relaxation. This contributes to an
improved cardiac output via afterload reduction.
It has been suggested that spontaneous ventilation
might improve the safety of inhaled anesthetic
administration because:
Concentration of a VA that produces
cardiovascular collapse > the conc. that
results in apnea.
Oxygen consumption is decreased approximately 10 to 15% during general anesthesia.
The distribution of cardiac output also is altered by anesthesia. Blood flow to liver, kidneys, and gut is decreased, particularly at deep levels of anesthesia.
- In contrast, blood flow to the brain, muscle, and skin is increased or not changed.
Sinoatrial node discharge rate is slowed by the volatile anesthetics. Conduction in the His-Purkinje system also is prolonged by the volatile anesthetics.

Isoflurane (and most other potent volatile anesthetics)
increases coronary blood flow many times beyond
that of the myocardial oxygen demand, thereby
creating potential for “steal.”
Steal is the diversion of blood from a myocardial bed
with limited or inadequate perfusion to a bed with
more adequate perfusion.
Neither isoflurane, sevoflurane, or desflurane at
concentrations up to 1.5 MAC cause steal effect.
There are only minor effects on decreasing minute ventilation.
The ventilatory effects are dose-dependent.
Their net effect of a gradual decrease in minute ventilation has been associated with increasing resting Paco2.
All volatile anesthetics decrease tidal volume
↓(TV) and increase respiratory rate ↑(RR)

Isoflurane does not
increase respiratory rate
above 1 MAC.
N2O increases respiratory
rate as much or more than
the inhaled anesthetics.
Desflurane results in the
greatest increase in
Paco2 .

In awake humans, changes in arterial CO2 such that
minute ventilation increases 3 L/min per a 10-mm Hg
increase in Paco2.
All inhaled anesthetics produce a dose-dependent depression of the ventilatory
response to hypercarbia!
The threshold at which
breathing stops, called the
apneic threshold.
It is generally 4 to 5 mm Hg below
the prevailing resting Paco2

Ing.Anesth., including nitrous oxide, produce a dose-
dependent attenuation of the ventilatory response to
hypoxia.
Has important clinical implications.
The short-acting sevoflurane and
desflurane may prove
advantageous - more rapid
washout and their minimal effect
on hypoxic sensitivity at
subanesthetic concentrations.

Bronchoconstriction under anesthesia occur:
direct stimulation of the laryngeal and tracheal areas
administration of adjuvant drugs that cause histamine
release
noxious stimuli activating vagal afferent nerves
The reflex response to these stimuli may be enhanced :
- in lightly anesthetized patients
- in patients with known reactive airway disease
including those requiring bronchodilator therapy
- chronic smoking histories.
Bronchoconstriction - via M2 and M3 muscarinic
receptors, which initiate increases in intracellular
cyclic guanosine monophosphate(cGMP).
Bronchiolar muscle relaxation – adrenergic β2-
receptors → an increase in intracellular cyclic
adenosine monophosphate(cAMP).
The volatile anesthetics relax airway smooth muscle primarily by directly depressing smooth muscle
contractility and indirectly inhibiting the reflex
neural pathway!
Volatile anesthetics have been used effectively to treat
status asthmaticus when other conventional treatments
have failed!
Sevoflurane may be a better choice.

Smokers have impaired mucociliary function compared
with nonsmokers.
and the combination of a volatile anesthetic in a smoker
who is mechanically ventilated sets up a scenario for
inadequate clearing of secretions, mucus plugging,
atelectasis, and hypoxemia.
Volatile anesthetics and nitrous oxide reduce ciliary movement and alter the characteristics
of mucus.

Inadequate hepatocyte oxygenation (oxygen supplyrelative to oxygen demand) is the principal mechanismresponsible for hepatic dysfunction following anesthesiaand surgery.
The liver has two blood supplies:
1 Hepatic artery(well-oxygenated).
2 Portal vein( poorly oxygenated).
Postoperative liver dysfunction has been associated with
most volatile anesthetics, with halothane receiving the
most attention.

HBF-Desflurane=Isoflurane=Sevoflurane<Halothane
The ether-based anesthetics
(isoflurane, sevoflurane, desflurane)
maintain or increase hepatic artery
blood flow while decreasing (or not changing) portal vein blood flow.
Halothane decreases in both
portal vein and hepatic artery
blood flow, thereby significantly compromising total hepatic artery
blood flow.
Altered liver function tests have been used as an
index of hepatic injury during anesthesia.
ALT, AST, GST
Increases in the ALT or AST are not uniquely
specific to the liver.
The centrilobular area of the liver is most
susceptible to hypoxia.
A more sensitive measure GST(α-glutathione S-
transferase), since it is distributed primarily in the
centrilobular hepatocytes.

The inhaled anesthetics have two important actions on neuromuscular function:
1. Directly relax skeletal muscle(nitrous oxide does not).
2. Potentiate the action of neuromuscular blocking drugs.
All of the potent volatile anesthetics serve as triggers for malignant
hyperthermia (MH)!!!
While N2O is considered safe in MH-susceptible
patients!!!

Uterine smooth muscle tone is diminished by volatile
anesthetics.
There is a dose-dependent decrease in spontaneous
myometrial contractility.
Uterine relaxation/atony can become problematic at
concentrations of volatile anesthesia >1 MAC, and
might delay the onset time of newborn respiration.
Consequently, a common technique used to provide
GA for urgent CS is to administer low concentrations of the VA, such as 0.5 to 0.75 MAC, combined with N20

Volatile anesthetics produce similar dose-related
decreases in renal blood flow, glomerular
filtration rate, and urine output.
These changes most likely reflect the effects of
volatile anesthetics on systemic blood pressure and
cardiac output.
Preoperative hydration attenuates or abolishes many
of the changes in renal function associated with
volatile anesthetics.
Physical properties: It is a laughing gas,colorless and odorless
It is only inorganic anesthetic gas in clinical use.
Non Explosive and Non Inflammable
Gas at room temperature and can be kept as a liquid under pressure.
It is relatively inexpensive.
low potency (MAC = 104%) and is relatively insoluble in blood
Nitrous oxide does not produce significant skeletal muscle relaxation, but it does have analgesic effects.
Elimination: almost 100% exhalation.
It causes post operative Nausea and Vomiting

Oxidizes Co atom in vitamin B12, inactivates
methinoine synthetase Affects myelin formation →peripheral neuropathies,
neurotoxicity.
Homocysteine accumulation
Inhibits thymidylate syntetase(DNA
syntesis)→teratogenicity.
Bone marrow depression-megaloblastic anemia

Air embolism
Pneumothorax
Acute Intestinal Obstruction
Tension Pneumocephalus
Tympanic membrane grafting
75% nitrous oxide can expand a pneumo-
thorax to double or triple its size in 10 and
30 minutes!!!
Physical Properties:
It is halogenated alkene.
Sweet, non-pungent.
Non Inflammable and Non explosive.
Least expensive .
CV: myocardial depression
- ↓BP and CO by up to 50%
- causes slowing of SA node conduction resulting in bradycardia
Resp: ↑RR, ↓↓TV, ↓MV, ↓↓hypercapnic drive, potent bronchodilator.
CEREBRAL:
It increases cerebral blood flow.
NEUROMUSCULAR:
Relaxes skelatal muscle and potentiates Non depolarizing neuro-muscular blocking agents.
RENAL:
Reduces renal blood flow, glomerular filtration rate and urinary output.
Hepatic
↓hepatic blood flow: impaired hepatic drug clearance.
-Liver oxidation→trifluoroacetic acid(TFA)
- 20% metabolised
- 1in 5 adults hepatotoxicity(lethargy, nausea,fever)
likely related to changes in HBF.
-”Halothane hepatitis”(rare): massive hepatic necrosis.
likely immune mechanism(eosinophilia, rash, fever)
Contraindications:
Unexplained liver dysfunction.
Intra-cranial mass lesions.
Hypovolemic patient with severe cardiac diseases

Isoflurane is a halogenated methyl ethyl ether
Clear, nonflammable liquid at room temperature.
Has a high degree of pungency.
It has become the “gold standard” anesthetic since its
introduction in the 1970s
Contraindications:
No such contraindication.
Patient with severe hypovolemia may not tolorate its
vasodilating effects.
It is the most potent of the volatile
anesthetics in clinical use.

Sevoflurane is a sweet-smelling, completely fluorinated methyl isopropyl ether
Non-pungent, low solubility- exellent for inhalation induction
+muscle relaxation(enough for peds intubation) potentiates NMBA.
Elimination:
-5%-liver metabolism
BaOH, soda lime- Compound A
-nephrotoxic in rats
-but has not been associated with renal injury in human volunteers or patients, with or without renal impairment, even when fresh gas flows are 1 L/min or less.

Very similar to Isoflurane in structure but much less
soluble, less potent.
Very high vapor pressure - requires special vaporizer.
- can boil at normal OR temperature.
- special vaporizer heats it to a gas and then blends it
with the FGF.
Desflurane is the most pungent
of the VA !!!
and if administered via the face mask results in:
coughing,salivation,breath holding,and laryngospasm.
Desflurane has the lowest blood:gas
solubility of the potent VA

Is an inert gas, difficult to obtain, and hence extremely expensive.
It has many characteristics approaching those of an “ideal” inhaled anesthetic.
Nonexplosive, nonpungent, and odorless, and thus can be inhaled with ease.
Its blood:gas partition coefficient is 0.14, and unlike the other potent VA , xenon provides some degree of analgesia.
Does not produce significant myocardial depression.
Because of its scarcity and high cost, new anesthetic systems need to be developed to provide for recycling of xenon.
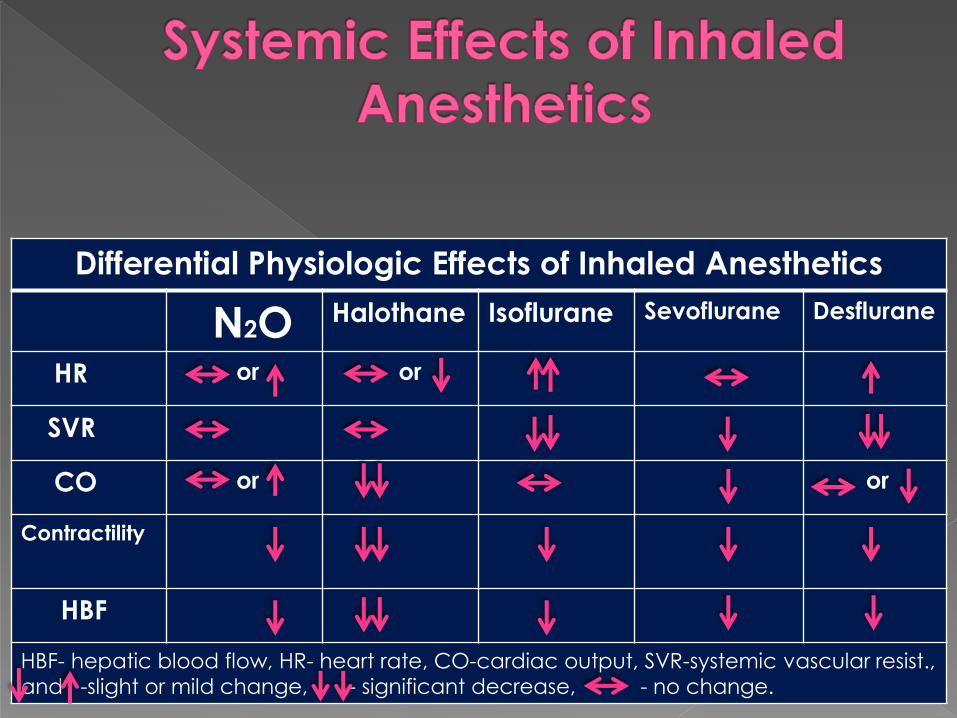
Differential Physiologic Effects of Inhaled Anesthetics
N2O Halothane Isoflurane Sevoflurane Desflurane
HR or or
SVR
CO or or
Contractility
HBF
HBF- hepatic blood flow, HR- heart rate, CO-cardiac output, SVR-systemic vascular resist.,
and -slight or mild change, - significant decrease, - no change.
Related Documents











