INFRARED THERMOMETER HEALTH TECHNOLOGY ASSESSMENT SECTION MEDICAL DEVELOPMENT DIVISION MINISTRY OF HEALTH MALAYSIA 012/2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
i
INFRARED
THERMOMETER
HEALTH TECHNOLOGY ASSESSMENT SECTION
MEDICAL DEVELOPMENT DIVISION
MINISTRY OF HEALTH MALAYSIA
012/2012

ii
DISCLAIMER Technology review is a brief report, prepared on an urgent basis, which draws on restricted reviews from analysis of pertinent literature, on expert opinion and / or regulatory status where appropriate. It has not been subjected to an external review process. While effort has been made to do so, this document may not fully reflect all scientific research available. Additionally, other relevant scientific findings may have been reported since completion of this review. Please contact: [email protected], if you would like further information.
Health Technology Assessment Section (MaHTAS) Medical Development Division Ministry of Health Malaysia Level 4, Block E1, Precinct 1 Government Office Complex 62590 Putrajaya Tel: 603 88831246 Fax: 603 8883 1230 Available at the following website: http://www.moh.gov.my
iii
Prepared by Madam Sin Lian Thye Nurse/ Information Specialist Health Technology Assessment Section (MaHTAS) Ministry of Health Malaysia Dr. Junainah Sabirin Principal Assistance Director Health Technology Assessment Section (MaHTAS) Ministry of Health Malaysia Reviewed by: Datin Dr. Rugayah Bakri Public Health Physician & Deputy Director Health Technology Assessment Section (MaHTAS) Ministry of Health Malaysia DISCLOSURE The author of this report has no competing interest in this subject and the preparation of this report is totally funded by the Ministry of Health, Malaysia.
iv
EXECUTIVE SUMMARY Introduction Evaluation of body temperature is one of the oldest known diagnostic methods and is still an important sign of health and disease, both in everyday life and in medical care. Accurate temperature measurement is critically important, particularly in neonates and immune compromised children whom suspicion of infection could result in investigations, treatment and even hospitalization. Consequently, inaccurate body temperature measurement may result in patients remain undiagnosed and untreated, or receiving unnecessary or inappropriate intervention.
Pulmonary artery temperature is considered the “gold standard” for measuring core body temperature. The distal esophagus and nasopharynx are considered acceptable alternatives. Other methods for measuring core body temperature include rectal and bladder measurement. However, all these methods are considered invasive procedures. Clinically, oral and rectal temperatures are the most reliable indicators of core body temperature.
This review was requested by the Senior Principle Assistant Director, Medical Services Development Section, following a product demonstration by a Company.
Objective/aim The objective of this systematic review was to assess the safety, efficacy/effectiveness and cost-effectiveness of Infrared thermometer for fever detection in a hospital or primary care setting.
Results and conclusions Infrared tympanic thermometer in children One systematic review and four diagnostic accuracy studies showed that infrared tympanic thermometer temperature measurement better reflect the core body temperature than axilla thermometer temperature measurement. It also showed that the Infrared tympanic thermometer sensitivity and specificity was moderate. However, the sensitivity and specificity increased with higher cut of point of temperature defined as fever. Infrared tympanic thermometer in adult With respect to its use in adult population, there was fair level of evidence involving four diagnostic accuracy studies that showed that infrared tympanic thermometer was less accurate to reflect core body temperature than pulmonary artery catheter or mercury in glass oral thermometer. Non- contact infrared thermometer Four studies were retrieved on the effectiveness of non-contact infrared thermometer in children. The evidence found was inconclusive whereby two studies reported good correlation of non-contact infrared thermometer with rectal/ mercury in glass axilla thermometer but the other two studies did not show good correlation.
v
Cost - effectiveness/Cost The evidence showed that the infrared tympanic thermometer with lowest purchase price has higher overall cost compared to the highest purchase price, This was because of the increased cost of consumables (nearly double the price in the cheaper infrared tympanic thermometer) that contributed to the total cost. In contrast, the cost of covers of the expensive infrared tympanic thermometer was found to be cheaper. Safety There was no retrievable evidence reporting any adverse events related to the use of the infrared thermometer. Methods Electronic databases were searched from inception: MEDLINE including MEDLINE In-Process & Other Non-Indexed Citations (Ovid); PubMed; EBM Reviews, Cochrane database of systematic; EBM Reviews - Health Technology Assessment; NHS economic evaluation database. Searches were also run in Horizon Scanning database- National Horizon Scanning Centre, Australia and New Zealand Horizon Scanning Network, National Horizon Scanning Birmingham, EuroScan; FDA; MHRA. In addition to the database searches, articles were identified from reviewing the bibliographies of retrieved articles and hand searching of journals.
A combination of both controlled vocabulary, such as the National Library of Medicine‟s MeSH (Medical Subject Headings), and keywords free text. The search strategies used in MEDLINE were adapted for use in other databases. The search was limited by including search filters for „human studies‟.
1
INFRARED THERMOMETER 1. INTRODUCTION
Evaluation of body temperature is one of the oldest known diagnostic methods and is still an important sign of health and disease, both in everyday life and in medical care.1,2 Accurate temperature measurement is critically important, particularly in neonates and immune compromised children whom suspicion of infection could result in investigations, treatment and even hospitalization.3,4 Consequently, inaccurate temperature measurement may result in patients remain undiagnosed and untreated, or receiving unnecessary or inappropriate intervention.5,6 In health centres and hospitals, nurses are responsible for measuring body temperature accurately and it is important to take into account the kind of thermometer and the sites of the body used for taking the measurement.7 Pulmonary artery temperature is considered the “gold standard” for measuring core body temperature,8 as mixed venous blood temperature reflects thermoregulation by the hypothalamus. The distal esophagus and nasopharynx are considered acceptable alternatives to the pulmonary artery catheter and commonly used intra-operatively.9, 10 However, like the pulmonary artery catheter, these instruments are invasive and thus are generally inappropriate outside the peri-anesthesia, peri-operative and critical care setting. Other invasive methods include rectal and bladder measurement. Clinically, oral and rectal temperatures are the most reliable indicators of core body temperature.11,12 Children younger than four years have difficulty keeping an oral thermometer under their tongues, making reliable temperature measurements difficult. At present, rectal thermometer has traditionally been considered the gold standard for temperature measurement in young children because it correlates highly with core body temperature.11,12,13 However, when the core temperature increases or decreases abruptly, rectal temperature changes more slowly and can be substantially different from the core temperature. In addition without proper sterilization techniques, rectal thermometer has the capacity to spread contaminants that are commonly found in stool. Rectal thermometers are very stressful for infants, are time-dependent and require certain level of practice. These characteristics make it an undesirable procedure for infants, health workers and parents.14 Mercury in glass thermometer was the traditional type of thermometer used to measure body temperature. However, mercury thermometers are gradually being phased out. This is because of concerns regarding the toxic environmental effect of mercury, namely toxicity from the absorption due to breakage and risk of infection.15,1 Thus, they are no longer recommended for use in infants and young children.16,17 Furthermore, The UK Health and Safety Regulations requires that mercury containing
2
medical devices should not be used whenever a suitable alternative exists.18
Electronic thermometers are widely used by healthcare professionals as alternative methods to mercury thermometers. This thermometer is supposedly accurate and very quick to use but they are often complex and quite expensive. Recently, cheaper compact electronic thermometers have been produced and available for use by the public, as well as healthcare professionals. Other types of thermometer available in the market is the chemical phase change thermometers which uses a combination of chemicals that change colour in response to variations in temperature. This type of thermometer is either chemical dot thermometers where the chemicals are contained in cells on a plastic stick, or chemical forehead thermometers which consists of a patch of chemicals in a plastic pouch that is placed on the forehead. Chemical dot thermometers are usually designed for single use but reusable types are also available. In recent years, infrared thermometers have been more frequently used. This type of thermometer determines the temperature of infrared emission from a source rather than absorbing heat from the tissue and reaching thermal equilibrium with it. Temperatures can typically be obtained in less than five seconds. Most thermometers of this type measure temperature at the ear drum (infrared tympanic thermometers) but temporal artery thermometers are now available where temperature is
measured on the scalp.15 Researchers have found a difference of 0.5 C between the tympanic thermometer and the mercury-in-glass thermometer.6, 19, 20 This review was requested by the Senior Principle Assistant Director, Medical Services Development Section, following a product demonstration by a company.
2. OBJECTIVE/AIM
The objective of this systematic review was to assess the safety, efficacy/effectiveness and cost-effectiveness of Infrared thermometer for fever detection in a hospital or primary care setting.
3. TECHNICAL FEATURES 3.1 Infrared ear thermometer 3.1.1 Mechanism of action
Infrared thermometers, also called tympanic thermometers, detect infrared energy emanating from the ear canal and tympanic membrane. Often a large number of measurements are performed rapidly to calculate the

3
temperature in the auditory canal. The tympanic membrane was initially adopted as a measurement site because its blood supply from the internal carotid artery was thought to reflect the temperature at the hypothalamus, which regulates body temperature. However, the blood supply is more complex than this, as the external carotid artery also supplies the tympanic membrane. Further, the mechanism by which temperature is controlled is not necessarily related to the temperature of the hypothalamus.21 The thermometer probe, which is not in contact with the tympanic membrane, contains optical sensors, usually thermopiles (electronic devices that convert thermal energy into electrical energy) that can detect infrared emissions. The received energy is converted into a temperature reading.17 Infrared tympanic thermometers are licensed for use in people of all ages, including babies and young children.
3.1.2 Technique for measurement
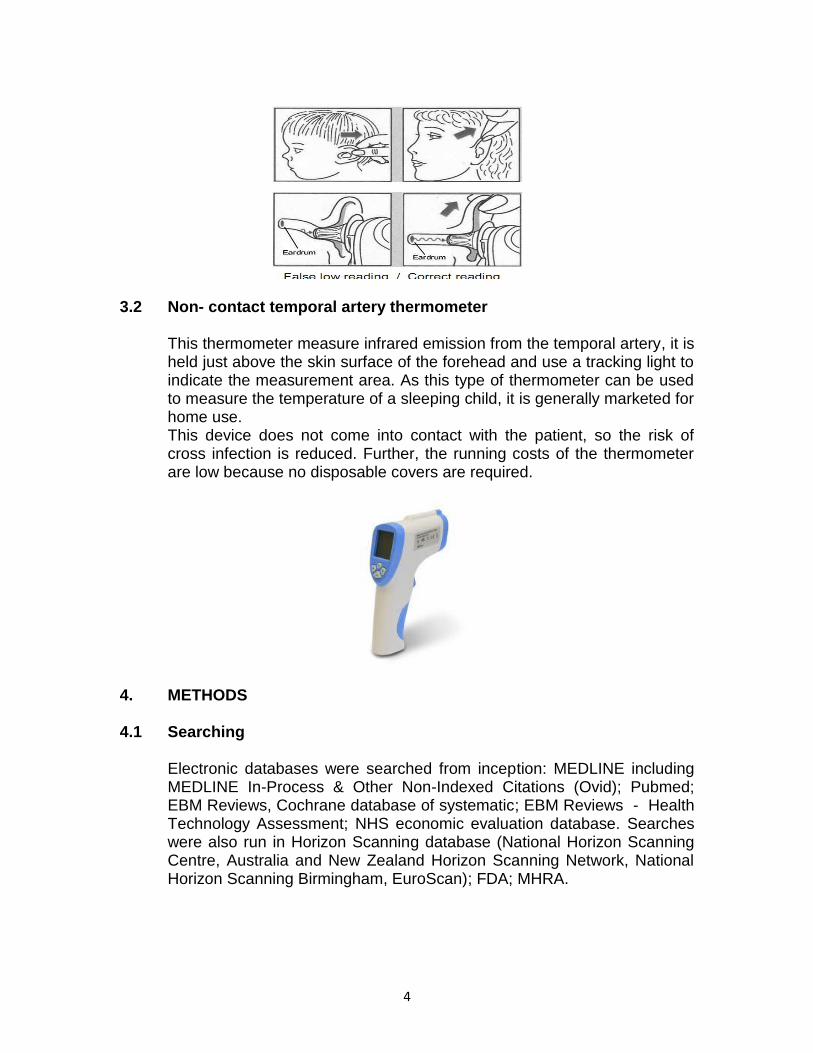
An appropriate disposable probe cover should be used. The nurse should inspect the cover to ensure that it has been fitted correctly and that there are no wrinkles over the tip end. This will ensure the most accurate reading possible is achieved. The cover is also used to help keep the probe tip clean and for infection control purposes. The temperature of ear
canal may be 2 C lower than the eardrum, therefore incorrect placing can give falsely low temperature readings. The heat energy received by the thermometer probe depends on the anatomy of the ear, the design of the thermometer probe and where the probe is placed. The thermometer calculates the patient‟s temperature from the infra-red energy received. Some models apply an offset to the ear measurement to indicate the temperature at a different site on the body, such as the oral site reading. Correct measurement technique is very important to ensure reliable temperature readings. With some patients and gentle but firm pull on the ear may be required to straighten the ear canal. Alternatively, the tragus may be gently retracted. The probe should be placed gently in the ear canal ensuring a snug fit and aimed at the eardrum as shown in the picture below.
4
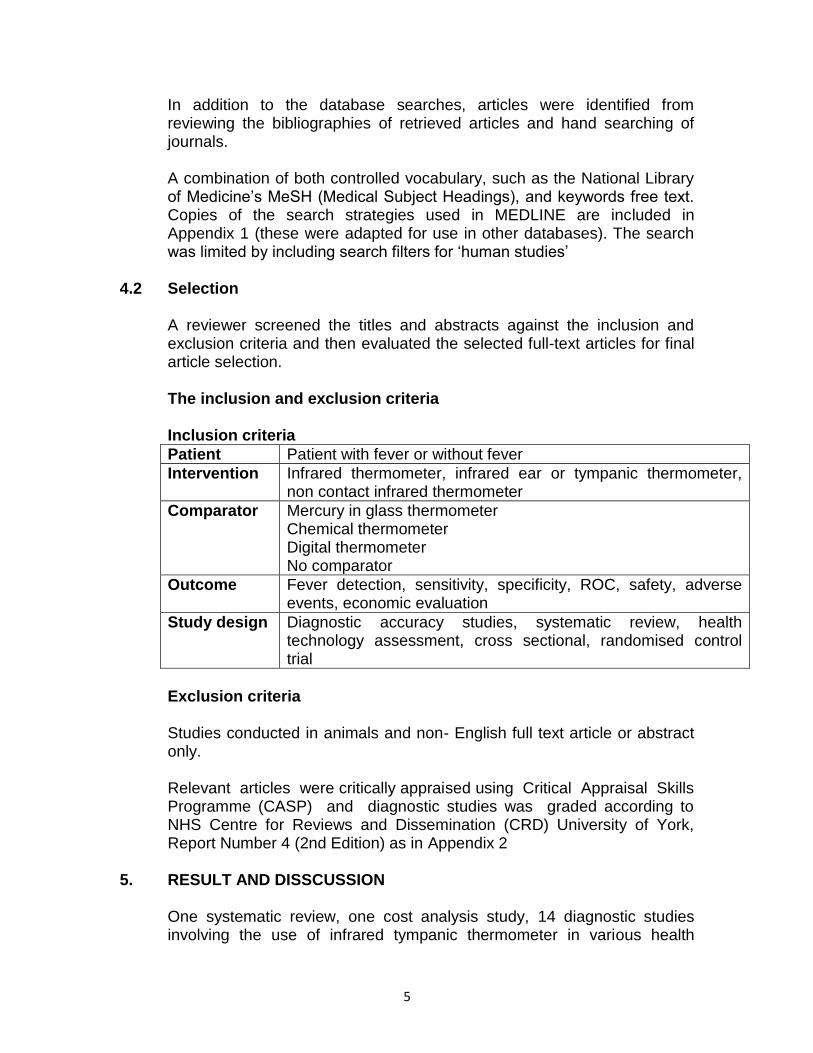
3.2 Non- contact temporal artery thermometer
This thermometer measure infrared emission from the temporal artery, it is held just above the skin surface of the forehead and use a tracking light to indicate the measurement area. As this type of thermometer can be used to measure the temperature of a sleeping child, it is generally marketed for home use. This device does not come into contact with the patient, so the risk of cross infection is reduced. Further, the running costs of the thermometer are low because no disposable covers are required.
4. METHODS 4.1 Searching
Electronic databases were searched from inception: MEDLINE including MEDLINE In-Process & Other Non-Indexed Citations (Ovid); Pubmed; EBM Reviews, Cochrane database of systematic; EBM Reviews - Health Technology Assessment; NHS economic evaluation database. Searches were also run in Horizon Scanning database (National Horizon Scanning Centre, Australia and New Zealand Horizon Scanning Network, National Horizon Scanning Birmingham, EuroScan); FDA; MHRA.
5
In addition to the database searches, articles were identified from reviewing the bibliographies of retrieved articles and hand searching of journals. A combination of both controlled vocabulary, such as the National Library of Medicine‟s MeSH (Medical Subject Headings), and keywords free text. Copies of the search strategies used in MEDLINE are included in Appendix 1 (these were adapted for use in other databases). The search was limited by including search filters for „human studies‟
4.2 Selection
A reviewer screened the titles and abstracts against the inclusion and exclusion criteria and then evaluated the selected full-text articles for final article selection. The inclusion and exclusion criteria Inclusion criteria
Patient Patient with fever or without fever
Intervention Infrared thermometer, infrared ear or tympanic thermometer, non contact infrared thermometer
Comparator Mercury in glass thermometer Chemical thermometer Digital thermometer No comparator
Outcome Fever detection, sensitivity, specificity, ROC, safety, adverse events, economic evaluation
Study design Diagnostic accuracy studies, systematic review, health technology assessment, cross sectional, randomised control trial
Exclusion criteria Studies conducted in animals and non- English full text article or abstract only. Relevant articles were critically appraised using Critical Appraisal Skills Programme (CASP) and diagnostic studies was graded according to NHS Centre for Reviews and Dissemination (CRD) University of York, Report Number 4 (2nd Edition) as in Appendix 2
5. RESULT AND DISSCUSSION
One systematic review, one cost analysis study, 14 diagnostic studies involving the use of infrared tympanic thermometer in various health
6
service environments ranging from primary care to intensive care were identified. Out of these 14 studies, four studies involved adults and 10 studies involved children. Six diagnostic studies were identified for the use of non-contact infrared thermometer in hospital.
5.1 Safety
There was no retrievable evidence on the adverse events related to the use of infrared tympanic or non-contact infrared thermometer. Based on the document submitted by the company, this infrared tympanic thermometer or non-contact infrared had received TUV certification in Taiwan and it is a class II b device.
5.2 Efficacy/Effectiveness 5.2.1 Infrared tympanic thermometer in children
Dodd et al performed a systematic review that evaluated diagnostic accuracy by examining the sensitivity and specificity of the infrared tympanic thermometer. Twenty three studies were included (n = 4,098 children), majority of the studies used 38°C as cut-off point for fever for both rectal and tympanic temperatures. The pooled estimates 95% confidence interval for sensitivity and specificity of infrared thermometer were 63.7% (95% CI 55.6% to 71.8%) and 95.2% (95% CI 93.5% to 96.9%), respectively. Thus, infrared tympanic thermometer would fail to diagnose three to four fever in every 10 febrile children (with fever defined
by a rectal temperature of 38 C or above).22, Level 2
Nimah et al conducted a study on 36 children (mean age = 20 months) admitted to paediatric and cardiac intensive care units at Cincinnati Children‟s Hospital Medical Center. Infrared tympanic, forehead sensor, indwelling rectal probe and axilla digital thermometer temperature measurement were compared with indwelling Foley Catheter bladder Thermometer with sensor temperature measurement as reference standard. It was found that tympanic temperature measurement was more closely agreed with bladder temperature when using cut off point of
100.4 F (38 C) defined as fever, the mean difference of infrared
tympanic measurement was - 0.03 (1.43) F; sensitivity = 80%, specificity = 81% as compared to rectal temperatures with mean difference of - 0.62 (1.44)°F, sensitivity = 67%, specificity = 93%; but forehead temperature
revealed a mean difference of - 0.56 (±1.81) F, sensitivity = 57%; specificity was 87%, while the mean difference of axillary temperatures was -1.25 (±1.73)°F, sensitivity = 40%, specificity = 98%. The authors discouraged the use of axilla thermometer in critically ill children and stated that infrared tympanic thermometer was accurate, reliable, practical and a less invasive substitute for bladder or rectal thermometer.23, level 2
7
El-Radhi and Patel conducted a study among 106 infants attending an accident and emergency department comparing tympanic temperature measure by infrared tympanic thermometer and axilla temperature electronic thermometer to those temperature measures by rectal thermometer (device no stated). The study result found that the agreement between rectal and tympanic temperatures appeared greater in both afebrile children with the mean difference of 0.38°C (range 0.25°C to 0.50°C) and febrile children with the mean difference of 0.42°C (range 0.27°to 0.58°C). For infants with rectal temperature of 38°C to 38.9°C, the sensitivity of infrared tympanic thermometer was 76%, while the sensitivity of axilla electronic thermometer was 24%. Similarly, for infants with a rectal temperature greater than 38.9°C, the sensitivity of infrared tympanic thermometer was 100% and sensitivity for axilla electronic thermometer was 89%. The authors concluded that infrared tympanic thermometer was more accurate than axilla electronic thermometer and offered additional practical benefits. 6, level 2
Musumba et al conducted study to compare infrared tympanic thermometer and electronic axilla thermometer to rectal electronic thermometer in 145 children with median age of 40 months admitted to a Kilifi District Hospital with severe malaria. They found that 95% limit of agreement mean difference for tympanic temperature measured by infrared tympanic thermometer was 0.42°C (95% LOA -1.6°C to 2.44°C) and axilla temperature measure by electronic thermometer was 0.74°C (95% LOA -0.85°C to 2.33°C). The authors concluded that in children with severe malaria, tympanic thermometer showed more accurate reflection of the body temperatures at admission and it‟s should be preferably used where available. 24,level 2
Sehgal et al study compared rectal and tympanic temperature in children with signs and symptoms of meningitis at Emergency Division of Kalawati
Saran Children‟s Hospital. The found that the mean difference was 0.8 C
(sd = 0.5 C), p=0.001 in 60 children with signs and symptoms of meningitis. While 60 children without signs and symptoms of meningitis,
the mean difference was 0.1 C (sd = 0.1 C), p>0.05). When examining a range of rectal temperature of 38°C to 40°C as cut off point of fever, temperature measurement by tympanic thermometer had a sensitivity of
100% throughout and specificity peaked at 89% when using 39.5 C as a cut of point. The authors concluded that tympanic thermometer can reliably predict core temperature over a wide range of readings.25, level 2
Study carried out by van Staaij et al compare between both left and right ear temperature using infrared tympanic thermometer with rectal digital thermometer among 41 children (with mean age of 5.9 years) admitted to a general paediatric ward of a children hospital in Netherland. An analysis
8
of variance revealed no statistically significant differences between right tympanic, left tympanic or rectal temperatures. Right tympanic and rectal temperature differed by more than 0.5°C in 10 children with the maximum difference being 1.78°C. When fever was defined as a rectal temperature of 38°C or greater, sensitivity and specificity were 93.3% and 92% respectively. The authors concluded that infrared tympanic thermometer was accurately reflects rectal temperature and validly assessed the presence of fever in children.26, level 2 Jean-Mary et al conducted study among 198 children with mean age of 1.3 years attending a hospital-based primary care practice in Boston for “well child” visits or acute illness to compare infrared tympanic and infrared axilla thermometer temperature measurement with digital rectal thermometer temperature measurement. The mean rectal temperature was 100.2°F (range, 96.9°- 105.1°F). Sixty-three patients were considered febrile, as defined by a rectal temperature ≥100.4° F, and 135 were
considered afebrile. When rectal fever defined as ≥ 100.4 F or greater, the sensitivity and specificity for infrared axilla thermometer was 63.5% and 92.6% respectively (diagnostic accuracy was 83.3%); and infrared tympanic thermometer was 68.3% and 94.8% respectively (diagnostic accuracy was 86.4%). The authors concluded that for a healthcare visit in the outpatient setting, the use of either of these devices was an appropriate screening tool, but if the history or physical examinations raised concerns for possible febrile illness, the rectal value should be used for the purpose of clinical accuracy.27, level 2
Paes et al evaluated the accuracy of temperature measure by infrared tympanic thermometer with digital rectal thermometer temperature measurement in 100 children with mean age of 3.24 years admitted to pediatric ward of Spaarne Hospital in The Netherlands. The mean difference tympanic temperature reading was found to be 0.271°C (SD ± 0.573°C), and the Pearson correlation coefficient (R) were 0.827, there was a strong correlation between rectal and tympanic correlation. When rectal temperature used 38.0°C as cut-off point for fever defined, the sensitivity and specificity for tympanic temperature measurement was 80% and 97% respectively; and positive predictive value was 91% and negative predictive value 94%. The data suggested that the tympanic thermometer is accurate in predicting rectal temperature. The SD of differences between rectal temperature and temperature measured with tympanic temperature was large. This indicates that the tympanic thermometer is not able to predict rectal measurement.28, level 2
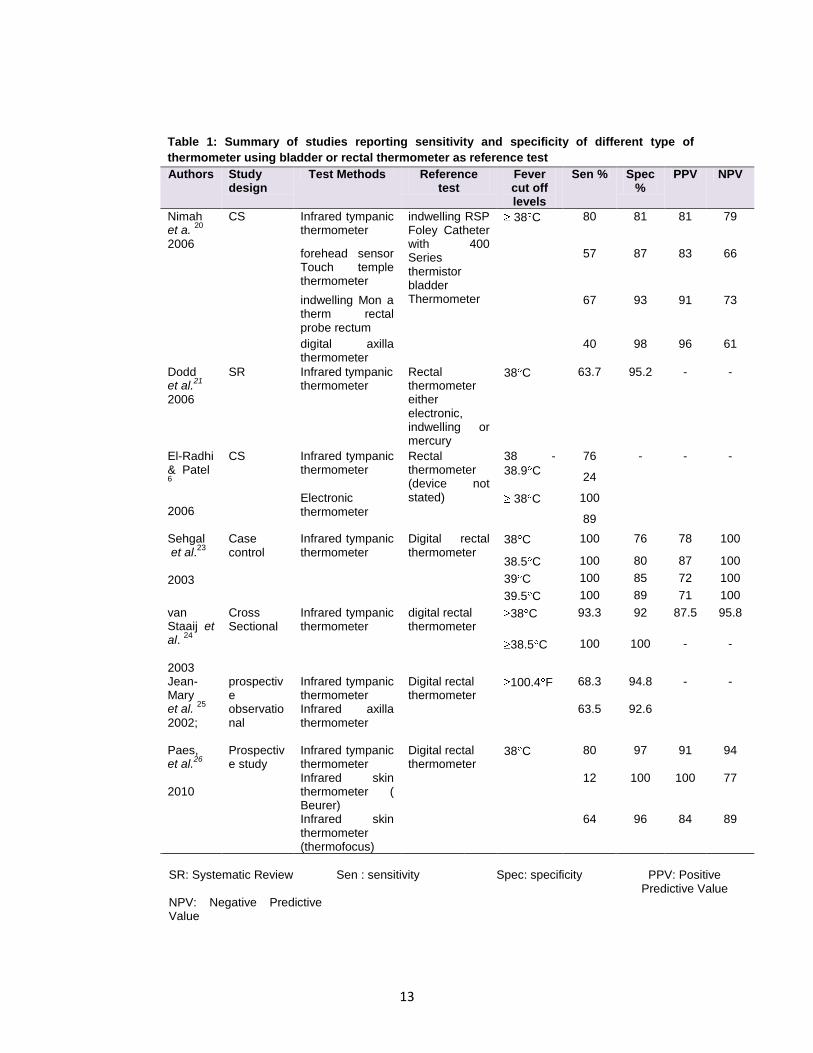
The above studies were summaries in table 1. Devrim et al compared two different type of infrared tympanic thermometer (home and clinical) to measure body temperature with axilla temperature
9
using mercury in glass thermometer among 102 children admitted to general pediatric ward and neonatal intensive care unit in the Hacettepe University Ihsan Dog ˘ramacı Children‟s Hospital. When axillary temperatures used cut of point of >38.3°C as defined fever, the mean temperature difference of clinical tympanic temperature measurement was - 0.74°C (95% LOA, 1.75°C to 0.27°C), the sensitivity and specificity was 95% and 96% respectively. While, for home tympanic temperature measurement, the mean temperature difference was - 0.14°C (95% LOA -1.27°C, 0.98°C), sensitivity and specificity was 69%, and 85% respectively. The authors concluded that home tympanic thermometer could be used for screening but not to decide patient follow-up.29,level 2
Hay et al study compared between body temperature measured by infrared tympanic thermometer and axilla temperature measure by mercury in glass thermometer among 16 preschool children with acute cough presenting to primary care. The mean differences between the axillary and tympanic measures was 1.18°C (95% LOA - 0.73 to 3.09).
When used axilla temperature with cut of point of 37 C or greater, the sensitivity and specificity were 15% and 98.6% respectively. The authors concluded that the mean difference was too large for the evaluated infrared tympanic thermometer to replace the axilla mercury in glass thermometer in normal clinical practice and that infrared tympanic thermometer was poorly in detecting febrile children.30, level 2
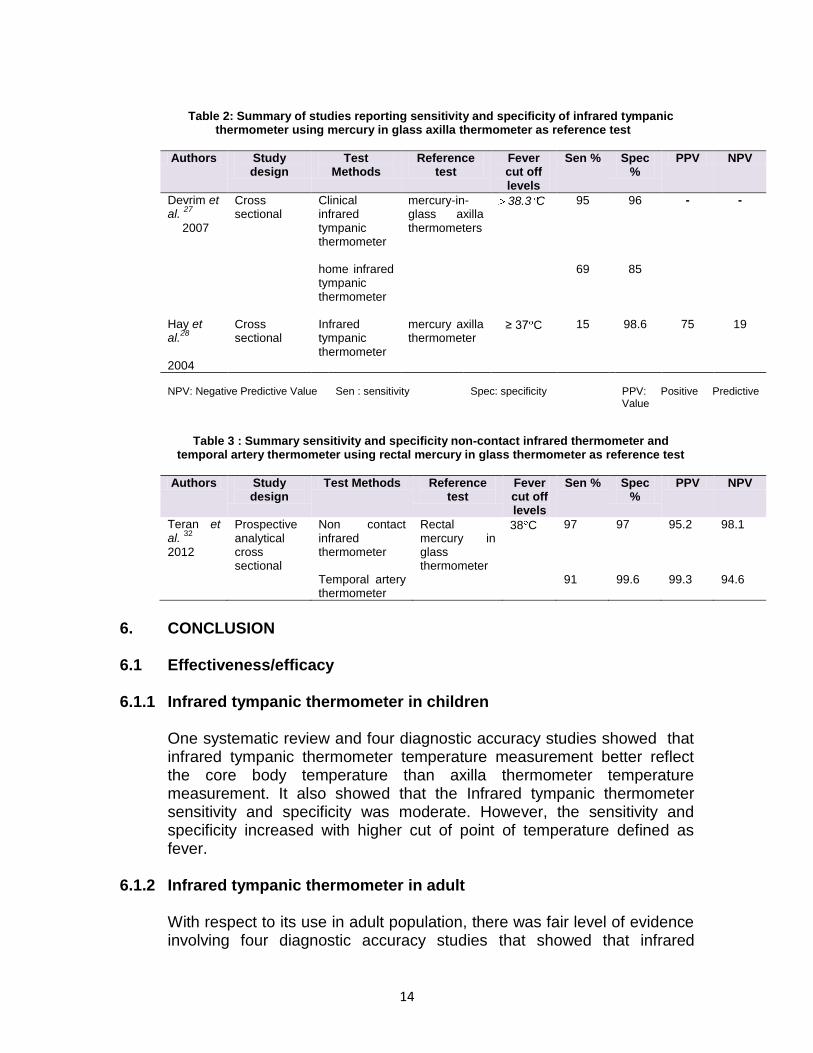
The above studies were summaries in table 2.
5.2.2 Infrared tympanic thermometer in adults
Moran et al conducted study among 110 patients admitted to intensive care unit a tertiary referral, university affiliated hospital in Australia, with the aim to compare body temperature measured by infrared tympanic thermometer and axilla temperature using mercury in glass thermometer to pulmonary artery catheter temperature measurement. They found that pulmonary artery temperatures were more consistent with axilla mercury-in-glass thermometer with the mean difference of 0.295 (95% LOA - 0.424°C to 1.014°C) than infrared tympanic thermometer with the mean difference of 0.358°C (95% LOA -0.560°C to 1.276°C). They concluded that infrared tympanic thermometer could not be used as accurate measures of core body temperature in the critically ill.31, level 2
In another smaller study of 25 intensive care unit patients conducted by Farnell et al comparing chemical and tympanic temperature measurements against the „gold standard‟ Pulmonary Artery Catheter (PAC). They found that the mean temperature differences between the PAC were 0.2 °C(p<0.0001, SD = 0.34) for chemical and 0.0 °C (p=0.39,
10
SD = 0.59) for tympanic temperatures and the mean temperature differences ranged from -1.3 to 0.9°C and -2.3 to1.0 °C respectively. Both the chemical and tympanic thermometers were significantly correlated with temperatures derived from the PAC (r = 0.81, p<0.0001 and r = 0.59, p<0.0001). The Bland–Altman plot of difference suggests that 95% of the
chemical thermometer readings were within a -0.5 to0.9 C range of the PAC. In contrast, 95% of the tympanic thermometer readings were within
a much wider range (-1.2 to 1.2 C).5, level 2 Rajee and Sultana compared temperature measure using infrared tympanic thermometer with oral temperature measure using mercury in glass thermometer among 200 emergency room attendees Freemasons Hospital, East Melbourne, Victoria, Australia. They found the tympanic thermometer agreed with the mercury thermometer within −1.0 to 1.1°C.). When fever defined as a oral temperature of 38°C or greater, the sensitivity and specificity of tympanic thermometer was 60% and 97% respectively.32, level 2
However, in another study conducted in Hong Kong by Lo et al in 100 adult surgical patients compare between temperature measured using infrared tympanic thermometer with oral temperature by mercury in glass thermometer. They found greater agreement between tympanic and oral temperatures measurement in afebrile patients, the mean difference was 0.018°C (95%LOA -0.52°C to 0.56°C) than febrile patients with the mean difference of 0.24°C (95%LOA -0.43°C, 0.9°C). The authors concluded that oral mercury-in-glass thermometer should not be replaced with infrared tympanic thermometer.33, level 2
5.2.3 Non-Contact infrared forehead/skin thermometer in children
A prospective, analytical, cross-sectional study was designed by Teran et al in order to assess the effectiveness of the infrared non-contact thermometer and temporal artery thermometer with rectal mercury in glass thermometer in 434 children aged 1 to 48 months in the emergency room and inpatient unit from the Pediatric Hospital Albina R. de Patiño. They found that both temperature measurements were strongly correlated with the rectal temperature measurements r=0.950 for temporal artery thermometer and r=0.952 for non-contact infrared thermometer. The mean difference in temperature between the rectal mercury in glass
thermometer and the non-contact thermometer was 0.029 0.01°C (p<0.001), while the mean difference between the temporal artery
thermometer and the rectal mercury in glass thermometer was - 0.20 0.27°C (p<0.001). When fever was defined as a temperature equal to or higher than 38°C, the sensitivity and specificity for the non-contact thermometer was 97%. While the sensitivity was 91% and specificity was
11
99.6% for temporal artery thermometer. The authors concluded that the non-contact infrared thermometer is a reliable, comfortable and accurate method of measurement of temperature and is a very useful tool to screen for fever in the paediatric population.34, level 2
The above study was summaries in table 3. Similarly, De Curtis et al evaluated accuracy temperature measured using infrared skin thermometer compared to temperature measure using rectal mercury in glass thermometer as reference test, in 107 newborn admitted to the newborn nursery or neonatal intensive care unit at University of Rome. They found that the mean difference temperature reading of non-contact infrared thermometer taken immediately after the mercury in glass
rectal thermometer measurement was -0.052 C (95% CI, -0.112 to
0.008 C). The LOA was -0.682 to 0.578. The authors concluded that infrared skin thermometer cannot act as a substitute for rectal mercury in glass thermometer in all cases; however, the differences between the two measurements were modest and this is encouraging for the use of infrared skin thermometer in monitoring body temperature in newborns.12, level 2
However, another study done by Fortune et al evaluated the accuracy of a non-contact infrared thermometer compared with a rectal electronic thermometer in two hundred patients with the mean age of 1.4 years presenting to a tertiary pediatric emergency department. The study result revealed a linear relationship between rectal electronic and non-contact infrared thermometer was observed; however, the coefficient of determination value between the two measurement was r2=0.48 (p<0.01). They also found that non-contact infrared thermometer tend to overestimate the temperature of afebrile children and underestimate the temperature in febrile patients with r2=0.149 (p<0.01). The author concluded that on-contact infrared thermometer did not sufficiently agree with rectal electronic thermometer to indicate its routine use.35, level 2 Chiappini et al conducted a study to assess the diagnostic accuracy of non-contact infrared thermometer compared with axilla mercury in glass thermometer for detecting fever in 251 children admitted to pediatric emergency department or pediatric clinic in five Italian cities. They found that the mean body temperature obtained by mercury-in-glass
thermometer and non-contact infrared thermometer was 37.18 C (SD
0.96 C) and 37.30 C (SD = 0.92 C), respectively (p=0.153). Non-contact
infrared thermometer clinical repeatability was 0.108 C (SD 0.095 C),
similar to that of the mercury-in-glass thermometer 0.11 C (SD 0.1 C; p=0.517). A significant correlation between temperature values obtained with the two procedures was observed (r2
=0.84; p<0.0001). The limits of agreement, by the Bland and Altman method, were - 0.62 (95%CI: - 0.47 to - 0.67) and 0.76 (95%CI: 0.61 to 0.91). When fever defined as axillary

12
temperature > 38 C; the sensitivity was 89 % and specificity was 90% respectively. The Non Contact Infrared Thermometer showed a good performance. 36, level 2
5.3 Cost effectiveness/Cost
Tympanic measurement can be provided by infrared sensing thermometer only, so there was no comparative analysis by different types of thermometer, thus only the least and most expensive type of infrared sensing model. The cost analysis calculated on total cost of using exclusively the least costly model and the most expensive model of infrared sensing thermometer was conducted. The result showed that the tympanic thermometer with the lowest purchase price has a higher overall cost compare to the tympanic thermometer with highest purchase priced. This is because of the increased cost of consumables (nearly double the price) that contribute to the total cost. In contrast, the cost of covers is lower in the most expensive model. The recurring costs per year (consumables and staff) are more than £ 50,000 (RM 246,824.00) more per year for the cheaper model, which outweighs the higher initial purchase price of the most expensive model. The result also indicate that time for reading is not important cost driver for tympanic measurement because it take only two second to make a temperature reading. The (discounted) cost over 10 years including staff costs is range from £ 732, 000 (RM 3,613,504.00) to £ 1,064,000 (RM 5,252,416.00).15 level 1
5.4 Limitations
Several imitation need to be address when interpreting the above studies, there were lack of information regarding thermometer calibration, temperature methods such as depth of penetration, placement time, mode used or “ear tug use”, and whether measurement were concurrent or sequential and the time to complete all measurement, lack of information on blinding across temperature measurement sites and during repeated measurement at the same site, small sample size i.e. less than 50 patient.
In additional, the selection was done by one reviewer. Although there was no limit apply on language during the search but only English articles were included in this report.
13
Table 1: Summary of studies reporting sensitivity and specificity of different type of
thermometer using bladder or rectal thermometer as reference test
Authors Study design
Test Methods Reference test
Fever cut off levels
Sen % Spec %
PPV NPV
Nimah et a.
20
2006
CS Infrared tympanic thermometer
indwelling RSP Foley Catheter with 400 Series thermistor bladder Thermometer
38 C 80 81 81 79
forehead sensor Touch temple thermometer
57 87 83 66
indwelling Mon a therm rectal probe rectum
67 93 91 73
digital axilla thermometer
40 98 96 61
Dodd et al.
21
2006
SR
Infrared tympanic thermometer
Rectal thermometer either electronic, indwelling or mercury
38 C 63.7 95.2 - -
El-Radhi & Patel 6
2006
CS Infrared tympanic thermometer
Rectal thermometer (device not stated)
38 -
38.9 C
76 - - -
24
Electronic thermometer
38 C 100
89
Sehgal et al.
23
2003
Case control
Infrared tympanic thermometer
Digital rectal thermometer
38 C 100 76 78 100
38.5 C 100 80 87 100
39 C 100 85 72 100
39.5 C 100 89 71 100
van Staaij et al.
24
2003
Cross Sectional
Infrared tympanic thermometer
digital rectal thermometer
38 C 93.3 92 87.5 95.8
38.5 C 100 100 - -
Jean-Mary et al.
25
2002;
prospective observational
Infrared tympanic thermometer
Digital rectal thermometer
100.4 F 68.3 94.8 - -
Infrared axilla thermometer
63.5 92.6
Paes, et al.
26
2010
Prospective study
Infrared tympanic thermometer
Digital rectal thermometer
38 C 80 97 91 94
Infrared skin thermometer ( Beurer)
12 100 100 77
Infrared skin thermometer (thermofocus)
64 96 84 89
SR: Systematic Review NPV: Negative Predictive Value
Sen : sensitivity
Spec: specificity
PPV: Positive
Predictive Value
14
Table 2: Summary of studies reporting sensitivity and specificity of infrared tympanic
thermometer using mercury in glass axilla thermometer as reference test
Authors Study design
Test Methods
Reference test
Fever cut off levels
Sen % Spec %
PPV NPV
Devrim et al.
27
2007
Cross sectional
Clinical infrared tympanic thermometer
mercury-in-glass axilla thermometers
38.3 C
95 96 - -
home infrared tympanic thermometer
69 85
Hay et al.
28
2004
Cross sectional
Infrared tympanic thermometer
mercury axilla thermometer
≥ 37 C 15 98.6 75 19
NPV: Negative Predictive Value
Sen : sensitivity
Spec: specificity
PPV: Positive Predictive Value
Table 3 : Summary sensitivity and specificity non-contact infrared thermometer and temporal artery thermometer using rectal mercury in glass thermometer as reference test
Authors Study design
Test Methods Reference test
Fever cut off levels
Sen % Spec %
PPV NPV
Teran et al.
32
2012
Prospective analytical cross sectional
Non contact infrared thermometer
Rectal mercury in glass thermometer
38 C 97 97 95.2 98.1
Temporal artery thermometer
91 99.6 99.3 94.6
6. CONCLUSION 6.1 Effectiveness/efficacy 6.1.1 Infrared tympanic thermometer in children
One systematic review and four diagnostic accuracy studies showed that infrared tympanic thermometer temperature measurement better reflect the core body temperature than axilla thermometer temperature measurement. It also showed that the Infrared tympanic thermometer sensitivity and specificity was moderate. However, the sensitivity and specificity increased with higher cut of point of temperature defined as fever.
6.1.2 Infrared tympanic thermometer in adult With respect to its use in adult population, there was fair level of evidence involving four diagnostic accuracy studies that showed that infrared
15
tympanic thermometer was less accurate to reflect core body temperature than pulmonary artery catheter or mercury in glass oral thermometer.
6.1.2 Non- contact infrared thermometer
Four studies were retrieved on the effectiveness non-contact infrared thermometer in children. The evidence found was inconclusive whereby two studies reported good correlation of non- contact infrared thermometer with rectal/axilla mercury in glass but the other two studies did not show good correlation
6.2 Cost - effectiveness/Cost
The evidence showed that the infrared tympanic thermometer with lowest purchase price has higher overall cost compared to the highest purchase price, This was because of the increased cost of consumables (nearly double the price in the cheaper infrared tympanic thermometer) that contributed to the total cost. In contrast, the cost of covers of the expensive infrared tympanic thermometer was found to be cheaper.
6.3 Safety
There was no retrievable evidence reporting any adverse events related to the use of the infrared thermometer.
16
REFERENCES 1. Sund-Levander M, & Grodzinsky, E. Time for a change to assess and evaluate body temperature in clinical practice. Int J Nurs Pract. 2009;15(4):241- 9. 2. Lu SH, Dai YT. Normal body temperature and the effects of age, sex, ambient temperature and body mass index on normal oral temperature: a prospective, comparative study. Int J Nurs Stud. 2009;46(5):661-8. 3. Craig J.V., Lancaster G.A., Taylor S., et al. Infrared ear thermometry compared with rectal thermometry in children: a systematic review. Lancet. 2002;360(9333):603-9. 4. Robinson J.L, Jou H., Spady DW. Accuracy of parents in measuring body temperature with a tympanic thermometer. BMC Fam Pract. 2005;6(1):3. 5. Farnell S, Maxwel lL, Tan S, et al. Temperature measurement: comparison of non-invasive methods used in adult critical care. J Clin Nurs. 2005;14(5):632-9. 6. Jensen B, Jensen F, Madsen S, et al. Accuracy of digital tympanic, oral, axillary
and rectal thermometers compared with standard rectal mercury thermometers. Eur J Surg. 2000;166:848-51.
7. Khorshid L, Eser I, Zaybak A, et al. Comparing mercury-in glass, tympanic and disposable thermometers in measuring body temperature in healthy young people. J of Clin Nurs. 2005;14 (4):496-500. 8. Fulbrook P. core temperature measurement in adults : a literature review. J Adv Nurs.1993;18(9):1451-60. 9. Hooper VD, Andrews, J.O. Accuracy of noninvasive core temperature
measurement in acutely ill adults: The state of the science. Biol Res Nurs. 2006;8(1):24-34.
10. Moran DS, Mendal, L. Core temperature measurement: methods and current insights. Sports Med. 2002;32(14):879-85. 11. Ishimine PF. Fever without source in children 0-36 months of age. Pediatr Clin North Am. 2006;53:167-94. 12. De Curtis M, Calzolari F, Marciano A, et al. Comparison between rectal and infrared skin temperature in the newborn. Arch Dis Child. 2008;93:F55 - F7. 13. McCarthy PL. Fever. Pediatr Rev.1998;19:401-8. 14. El-Radhi AS, Barry W. Thermometry in paediatric practice. Arch Dis Child. 2006;91(4):351-6. 15. National Collaborating Centre for Women's and Children's Health [Clinical
guideline]. Feverish illness in children: assessment and initial management in children younger than 5 years. London: Royal College of Obstetricians and Gynaecologists, Available: http://guidance.nice.org.uk/CG47/guidance/pdf/English (accessed on 10 July 2012)2007.
16. Canadian Paediatric Society. Temperature measurement in paediatrics. Ottawa: The Society; 2007. Reference No. CP00-01. Available: http://www.cps.ca/english/statements/CP/cp00-01.htm (accessed on 1 July 2012).
17. Crawford DC, Hicks B, Thompson MJ. Which thermometer? Factors influencing best choice for intermittent clinical temperature assessment. J Med Eng Technol. 2006;30 (4):199-211.
18. Health and Safety Executive. Control of Substances Hazardous to Health. 2007, http://www.sholland.gov.uk/NR/rdonlyres/9DABB32F-884D-46B5-9A30- C7EEFC071ECF/0/coshh.pdf access on 25 July 2012.
17
19. Kocooglu H, Goksu S, Isık M, et al. Infrared tympanic thermometer can accurately measure the body temperature in children in an emergency. Int J Pediatr Otorhinolaryngol. 2002;65:39-43. 20. Prentice D, Mereland J. A comparison of infrared ear thermometry with electronic predictive thermometry in a geriatric setting. Geriatr Nurs.1999;20:314-7. 21. Bratincsák A, Palkovits, M. Evidence that peripheral rather than intracranial thermal signals induce thermoregulation. Neuroscience. 2005;135(2):525-32. 22. Dodd SR, Lancaster GA, Craig JV, et al. In a systematic review, infrared ear
thermometry for fever diagnosis in children finds poor sensitivity. J Clin Epidemiol. 2006;59(4):354-7.
23. Nimah MM, Bshesh K, Callahan JD, et al. Infrared tympanic thermometry in comparison with other temperature measurement techniques in febrile children. Pediatr Crit Care Med. 2006;7(1):48-55.
24. Musumba CO, Griffiths KL, Ross A, et al. Comparison of axillary, rectal and tympanic temperature measurements in children admitted with malaria. J Trop Pediatr. 2005;51(4):242-4.
25. Sehgal A, Dubey NK, Jyothi MC, et al. Comparison of tympanic and rectal temperature in febrile patients. Ind J Pediatr. 2002 Apr;69(4):305-8.
26. van Staaij BK, Rovers MM, Schilder AG, et al. Accuracy and feasibility of daily infrared tympanic membrane temperature measurements in the identification of fever in children. Int J Pediatr Otorhinolaryngol. 2003;67(10):1091-7.
27. Jean-Mary MB, Dicanzio J, Shaw J, et al. Limited accuracy and reliability of infrared axillary and aural thermometers in a pediatric outpatient population. J Pediatr. 2002;141(5):671-6. 28. Paes BF, Vermeulen K, Brohet RM, et al. Accuracy of tympanic and infrared skin thermometers in children. Arch Dis Child. 2010;95(12):974-8. 29. Devrim I, Kara A, Ceyhan M, et al. Measurement accuracy of fever by tympanic
and axillary thermometry. Pediatr Emerg Care. 2007;23(1):16-9. 30. Hay AD, Peters T.J., Wilson A, et al. The use of infrared thermometry for the
detection of fever. Br J Gen Pract. 2004;54(503):448-50. 31. Moran JL, Peter JV, Solomon PJ, et al. Tympanic temperature measurements:
are they reliable in the critically ill? A clinical study of measures of agreement. Crit Care Med. 2007;35(1):155-64.
32. Rajee M, Sultana RV. NexTemp thermometer can be used interchangeably with tympanic or mercury thermometers for emergency department use. Emerg Med Australas.2006;18(3):245-51.
33. Lo S, Lau, L., Law, I., Yip, A. Should we replace the mercury in glass thermometer with the tympanic thermometer? Ann Coll Surg Hong Kong. 2003; 7(1):18-22.
34. Teran CG, Torrez-Llanos J, Teran-Miranda TE, et al. Clinical accuracy of a non-contact infrared skin thermometer in paediatric practice. Child Care Health Dev. 2011 Jun 8 (38):471-473
35. Fortuna EL, Carney MM, Macy M, et al. Accuracy of non-contact infrared thermometry versus rectal thermometry in young children evaluated in the emergency department for fever. JEmerg Nurs. 2010, Mar;36(2):101-4.
36. Chiappini E, Sollai S, Longhi R, et al. Performance of non-contact infrared thermometer for detecting febrile children in hospital and ambulatory settings. J Clin Nurs. 2011 May; 20(9-10):1311-8.
18
9. APPENDIX 9.1. Appendix 1: LITERATURE SEARCH STRATEGY
Ovid MEDLINE® In-process & other Non-Indexed citations and OvidMEDLINE® 1948 to present
1. Fever/ 2. fever*.tw. 3. hyperthermia*.tw. 4. pyrexia*.tw. 5. 1 or 2 or 3 or 4 6. Thermometers/ 7. Thermometer*.tw. 8. Body Temperature/ 9. (body adj1 temperature*).tw. 10. Thermography/ 11. thermograph*.tw. 12. 6 or 7 or 8 or 9 or 10 or 11 13. 5 and 12
OTHER DATABASES
EBM Reviews - Cochrane database of systematic reviews
Same MeSH, keywords, limits used as per MEDLINE search
EBM Reviews - Health Technology Assessment
PubMed
NHS economic evaluation database
FDA Non contact infrared thermometer
MHRA
TUV
Euroscan
Australia and New Zealand Horizon Scanning Network (ANZHSN)
NHSC
19
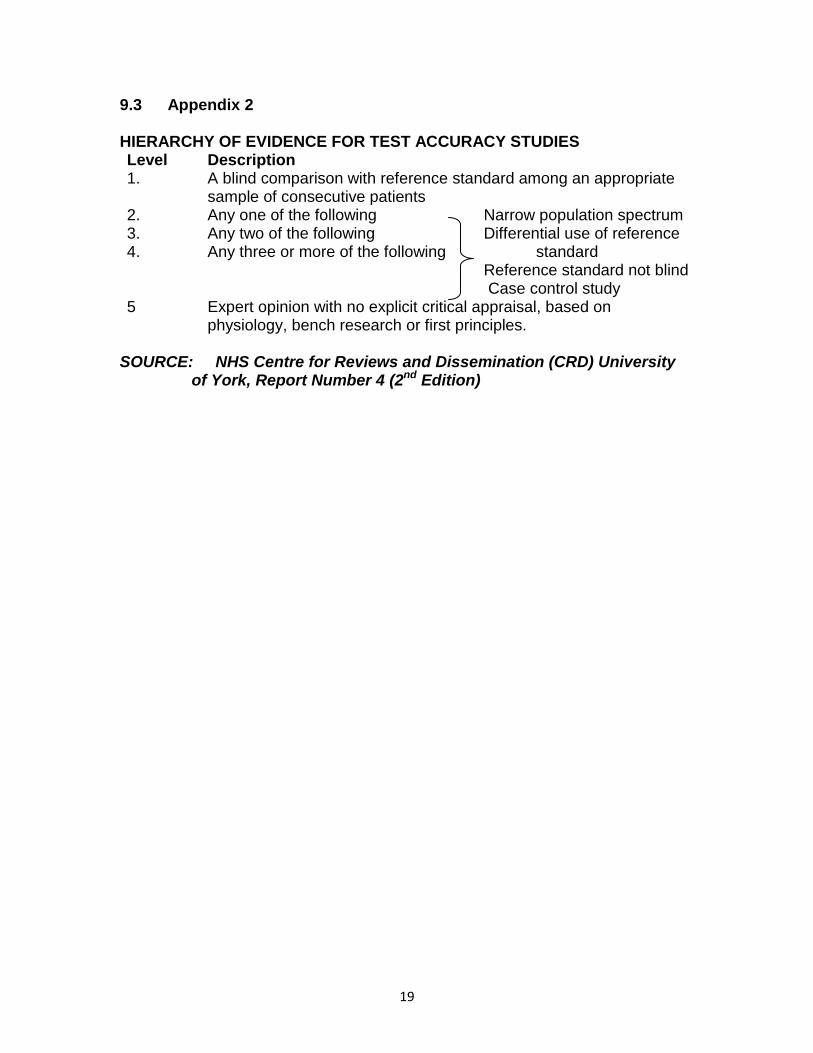
9.3 Appendix 2 HIERARCHY OF EVIDENCE FOR TEST ACCURACY STUDIES Level Description 1. A blind comparison with reference standard among an appropriate
sample of consecutive patients 2. Any one of the following Narrow population spectrum
Differential use of reference standard Reference standard not blind Case control study
3. Any two of the following 4. Any three or more of the following
5 Expert opinion with no explicit critical appraisal, based on physiology, bench research or first principles.
SOURCE: NHS Centre for Reviews and Dissemination (CRD) University
of York, Report Number 4 (2nd Edition)
Related Documents











