Law and Human Behavior, Vol. 12, No. 4, 1988 Information Disclosure, Subject Understanding, and Informed Consent in Psychiatric Research* Paul R. Benson,~" Loren H. Roth,$ Paul S. Appelbaum,w Charles W. Lidz,~ and William J. Winslade Investigator information disclosure and subject understanding are examined in four psychiatric studies using data drawn from observation of 88 consent sessions. In an attempt to determine if subjects" understanding of research can be improved, three experimental methods of information giving (in- cluding the use of independent subject educators) are compared to standard investigator disclosure. Findings indicate that the use of experimental techniques generally increases the quality of informa- tion delivered to prospective subjects, with disclosures by subject educators generating the most complete information. Subject understanding was also found to be significantly associated with the quality of information provided. Diagnosis and level of psychopathology, however, were found to be the most important predictors of subject understanding, with schizophrenics and the highly impaired most likely to demonstrate poor comprehension. These results suggest that the degree of improvement in understanding obtainable for severely disordered subjects is substantially lower than it is for others. The implications of these findings for informed consent, the regulation of medical research, and the protection of human subjects are discussed. INTRODUCTION Periodic exposes of the misuse of human subjects in medical research has led to the development of numerous ethical codes, and since 1966, to increasingly corn- ? Department of Sociology, University of Massachusetts, Boston. $ Program in Law and Psychiatry, Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine. w Program in Medicine and the Law, Department of Psychiatry, University of Massachusetts Medical Center, Worcester. Department of Medical Humanities, University of Texas Medical Branch, Galveston. * Supported by the Foundations Fund for Research in Psychiatry. The authors thank Florence Cohen, Mary Scott Dewire, Mary Hagman, Janice Holden, and Michael Malkin, all of whom assisted in carrying out this study. We also wish to thank Charles Brody, Gray Cavender, Gene Fisher, Nancy Jurik, and Joseph Sheley for their valuable comments on earlier drafts of this article. Jane Tamae Kuroda ably prepared the manuscript. 455 0147-7307/88/1200-0455506.00/0 1988 Plenum Publishing Corporation

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Law and Human Behavior, Vol. 12, No. 4, 1988
Information Disclosure, Subject Understanding, and Informed Consent in Psychiatric Research*
Paul R. Benson,~" Loren H. Roth,$ Paul S. Appelbaum,w Charles W. Lidz,~ and William J. Winslade�82
Investigator information disclosure and subject understanding are examined in four psychiatric studies using data drawn from observation of 88 consent sessions. In an attempt to determine if subjects" understanding of research can be improved, three experimental methods of information giving (in- cluding the use of independent subject educators) are compared to standard investigator disclosure. Findings indicate that the use of experimental techniques generally increases the quality of informa- tion delivered to prospective subjects, with disclosures by subject educators generating the most complete information. Subject understanding was also found to be significantly associated with the quality of information provided. Diagnosis and level of psychopathology, however, were found to be the most important predictors of subject understanding, with schizophrenics and the highly impaired most likely to demonstrate poor comprehension. These results suggest that the degree of improvement in understanding obtainable for severely disordered subjects is substantially lower than it is for others. The implications of these findings for informed consent, the regulation of medical research, and the protection of human subjects are discussed.
INTRODUCTION
Periodic exposes of the misuse of human subjects in medical research has led to the development of numerous ethical codes, and since 1966, to increasingly corn-
? Department of Sociology, University of Massachusetts, Boston. $ Program in Law and Psychiatry, Western Psychiatric Institute and Clinic, University of Pittsburgh
School of Medicine. w Program in Medicine and the Law, Department of Psychiatry, University of Massachusetts Medical
Center, Worcester. �82 Department of Medical Humanities, University of Texas Medical Branch, Galveston. * Supported by the Foundations Fund for Research in Psychiatry. The authors thank Florence Cohen,
Mary Scott Dewire, Mary Hagman, Janice Holden, and Michael Malkin, all of whom assisted in carrying out this study. We also wish to thank Charles Brody, Gray Cavender, Gene Fisher, Nancy Jurik, and Joseph Sheley for their valuable comments on earlier drafts of this article. Jane Tamae Kuroda ably prepared the manuscript.
455
0147-7307/88/1200-0455506.00/0 �9 1988 Plenum Publishing Corporation
456 BENSON ET AL.
plex federal regulations in the U.S. (Benson and Roth, in press; Capron, 1986; Swazey, 1978). Informed consent has emerged as a major element of these codes and regulations (Annas, Glantz, & Katz, 1977; Greenwald, Ryan, & Mulvihill, 1982). Succinctly stated, the informed consent doctrine requires that prospective subjects be apprised of important elements of the research project so they can make rational and autonomous decisions regarding study participation (Appel- baum, Lidz, & Meisel, 1987; Faden & Beauchamp, 1986). Some observers, par- ticularly in law and bioethics, have embraced the doctrine, viewing it as essential for ensuring both the autonomy and protection of prospective research subjects (Fried, 1974; Glass, 1970; President's Commission, 1982; Ramsey, 1970). Others, however, have been far less laudatory, maintaining that it is unrealistic to expect laypersons to comprehend enough of a research project's rationale and proce- dures to render "truly informed" consent (Chayet, 1976; Inglefinger, 1972; Ham- ilton, 1983; Laforet, 1976).
The application of informed consent to research utilizing the mentally ill has been especially controversial (Stanley & Stanley, 1981; Macklin, 1982). Experts have frequently questioned the viability of informed consent obtained from indi- viduals whose mental condition and reliance on caregivers may adversely affect their decision-making capacity (Dyer, 1982; Garham, 1975; Ketai et al., 1981). However, many informed consent advocates view psychiatric patients as a proto- typal "population at risk" urgently in need of the protections afforded by the doctrine (Goldstein, 1979; Plotkin, 1977; Singer, 1977). Moreover, some have suggested that the mentally disordered are, in fact, no less competent to consent to research than are the medically ill or others (Stanley et al., 1981).
RESEARCH PROBLEM
Given the doctrine's import, surprisingly few social scientific studies of in- formed consent have been undertaken in medical research settings. Important exceptions, however, should be noted, including the work of Barber (1980; Barber et al., 1973), Gray (1975; 1978), and Lidz (Lidz and Roth, 1981; Lidz et al., 1984). In an influential study conducted in the early 1970s, Gray (1975) inter- viewed 52 female participants in a labor-induction study conducted at a major university medical center. Of these 52 subjects, all of whom had signed a docu- ment formally consenting to the study, 20 (39%) were discovered by Gray to be unaware of their research involvement. Moreover, even those aware of their in- volvement frequently misunderstood important aspects of the research and their participation in it. Unfortunately, as in most informed consent research (Pryce, 1978; Howard, DeMets, & the BHAT Research Group, t981; Riecken & Ravich, 1982), Gray did n o t directly observe medical investigators' disclosure of research information to prospective subjects. For this reason, he was unable to determine if subjects' low level of understanding was due to poor comprehension, misunder- standing, forgetfulness, or simply because they were never informed. Lidz and his co-workers (1984), in a study employing ethnographic techniques, found that investigators often confused the concepts of research, treatment, and diagnostic

INFORMATION DISCLOSURE 457
testing in their discussions with subjects. In turn, subjects seldom perceived the procedures they were undergoing strictly as "research," seeing them instead largely as an effort by clinicians to "understand them better" and thus improve their treatment. Clearly, the style and content of investigators' communication of information affects prospective subjects' understanding of research. Few studies of informed consent have examined these communications and this fact has hin- dered the development of sound research in the area (Meisel & Roth, 1983).
A second problem of informed consent research, particularly from the stand- point of public policy, is its inattention to the possibility that subject under- standing can be improved through modifications in the consent process. In her review of the research literature, Stanley (1981) notes that, across informed con- sent studies, increased instruction appears to be associated with greater subject understanding. Several methods of improving information disclosure have been proposed, including the use of videotaped presentations (Barbour & Blumen- krantz, 1978) and structured "tests" that prospective subjects must pass prior to their enrollment in research (Miller & Willner, 1974). The use of independent "subject advocates" has also been advanced (McGrath & Briscoe, 1981), most controversially in the late 1970s by proposed (but never adopted) U.S. federal regulations governing research on the mentally ill (Department of Health, Educa- tion, and Welfare, 1978). 1 While each of these proposed consent process modifi- cations is intriguing, it is unknown if they can be implemented effectively in clin- ical studies or if their use can actually improve the disclosure of information to prospective subjects and increase their understanding of research.
This investigation examines informed consent in four psychiatric studies. In view of the deficiencies of past informed consent research, our study incorpo- rates close observation of investigator-subject communication with a detailed assessment of subjects' research understanding. In addition, within each psychi- atric study, four different methods of information disclosure are utilized and com- pared. Employing this quasiexperimental design, we examine whether and to what extent, compared to routine disclosures, innovative disclosure techniques increase the amount and quality of information given to prospective subjects. Finally, using multivariate analyses, we examine what factors (including quality of disclosed information, psychopathology, and subject sociodemographic char- acteristics) best explain variation in subjects' understanding of research.
METHODS
Study Design As noted above, study data are taken from a multimethod investigation of
informed consent carried out in four psychiatric research studies. In an attempt to
In late 1986, the use of subject advocates similar to that envisioned by the proposed DHEW regula- tions was advanced in a discussion draft of revised human subject research guidelines drafted by the Medical Research Council of Canada. The recommendation to employ subject advocates is highly controversial and it is unclear whether it will be retained in the final version of the revised Canadian guidelines (see Benson and Roth, in press).
458 BENSON ET AL.
determine whether information delivery and subject understanding can be im- proved, four different disclosure techniques were utilized sequentially within each study:
1. Unassisted disclosure. In this base-line group, subject consents were ob- tained in the psychiatric researcher's customary manner.
2. Unassisted disclosure with videotape. In this second group, subjects re- ceived routine investigator disclosures and viewed an instructional video- tape prepared by the psychiatric researcher.
Following these first two sets of disclosures, members of our research team met separately with investigators from each psychiatric study, provided them with feedback concerning subjects' research understanding to that point in the study, and suggested possible ways of improving their delivery of research information. Following these meetings with investigators, two final disclosure methods were utilized:
3. Assisted disclosure with "improved" videotape. A second instructional videotape was prepared and shown to subjects in this third group; in addi- tion, subjects received whatever additional information the investigator deemed appropriate to disclose.
4. Neutral educator. In this final disclosure group, a "neutral educator" (af- filiated with our study) and the psychiatric investigator independently provided information to prospective research subjects, z
Study Descriptions Two of the psychiatric studies examined in our informed consent research
were conducted at a major university medical center, the other two at a govern- ment psychiatric facility located in another section of the U.S. While space limi- tations prohibit full discussion of each project (see Benson et al., 1987 for more detail3), the four studies can be briefly described as follows:
The Depression Study. The purpose of this study was to compare the thera- peutic action and side effects of two antidepressant medications in elderly pa- tients. Subjects diagnosed with a major depression were randomly placed on one of the two drugs and treated in a double-blind fashion for a period of 10 weeks.
The Schizophrenia Study. The goal of this research project was to determine the optimal minimal dose of antipsychotic medication for different groups of com- munity-based chronic schizophrenics. The study's double-blind design called for
z Three individuals served as neutral educators across the four psychiatric studies. In the schizo- phrenia study, the neutral educator was a doctoral student in psychology. In the depression study, the neutral educator was an attorney. In the social skills and borderline personality disorder studies, the neutral educator was a psychiatric nurse. All three neutral educators were white females in their early thirties.
3 Detailed descriptions of each psychiatric study, including specific risks and benefits, are available from the senior author on request.

INFORMATION DISCLOSURE 459
subjects to be randomly treated for several years with either a low or moderate dose of antipsychotic medication.
The Social Skills Study. This study was designed to investigate the efficacy of social skills training with chronic schizophrenic outpatients. Subjects were randomly assigned to one of three possible treatment conditions: a control group, which received normal day hospital treatment, and two experimental groups re- ceiving different forms of social skills training. 4
The Borderline Personality Disorder Study. This final study compared the effectiveness of two different psychotropic drugs versus placebo in the treatment of borderline personality disorder. The study utilized a randomized, double-blind research design and lasted 6 weeks.
Data Collection Procedures
Overall, 88 disclosure sessions between psychiatric researchers and prospec- tive subjects were observed across the four psychiatric studies, 24 each in the depression and schizophrenia projects and 20 each in the social skills and border- line personality disorder studies. 5 Systematic observations of disclosure sessions were carried out in each study using video and audiotape. Standardized interac- tional rating forms were also completed by observers following all disclosure ses- sions. 6 Immediately following each disclosure, subjects were questioned re- garding their understanding of the psychiatric research project using a semistruc- tured interview. Subjects were also queried about the consent process itself and the requirements of their prospective role as a psychiatric study participant. Sub- jects ' levels of psychiatric impairment were assessed using Gorham and Overall's (1962) Brief Psychiatric Rating Scale [BPRS], as well as several other standard scales. 7 Finally, subjects were evaluated in two followup interviews, one com-
4 As noted in the text, the initial intent of the social skills study was the comparison of three forms of psychiatric treatment, two social skills training methods and day-hospital treatment. However, midway into our study (beginning with subject 14, observed in the third cell in our four-group, 20-subject protocol), the design of the social skills study was altered by the psychiatric investigators: subject randomization into the three treatment groups was discontinued and thereafter all subjects received social skills training. Following this unexpected change in the social skills study, five items assessing disclosure of now-irrelevant methodological or procedural issues were deleted (see foot- note 10). In addition, three items assessing subjects' understanding of moot methodological issues (use of different treatments, randomization, and use of a control group) were deleted for subjects 14 and 15. For subjects 16-20, these three items were replaced with similar items reflecting new study procedures (see footnote 12).
s Our initial research design called for the observation of 24 disclosure sessions per psychiatric re- search project, with each of the four disclosure method groups including a total of six subjects, Severe delays in subject recruitment in the social skills and borderline personality disorder studies, however, forced us to reduce our total observations in these two studies to 20. Disclosure groups in each of these two studies were thus reduced to five subjects, while disclosure groups in the depres- sion and schizophrenia projects employed the originally planned six subjects.
6 Copies of study instruments are available on request from the senior author. 7 The BPRS is a standardized rating scale widely employed in psychiatric research. The scale is sub-
divided into 19 subscales, each of which assesses a specific element of patient behavior (including anxiety, hostility, suspiciousness, hallucinations, grandiosity, conceptual disorganization, blunted
460 BENSON ET AL.
pleted in approximately two weeks, and another 2-6 months following the initial disclosure (the present analysis utilizes only the first set of interviews).
Subjects were recruited into our study as they were identified as prospective research participants by psychiatric investigators. Following their agreement to take part in our study, subjects were placed sequentially in one of the four disclo- sure groups; thus subject assignment to disclosure method was contingent upon the point in our protocol at which they were recruited. Because research has suggested that patient education and social class (Boreham & Gibson, 1978; Cartwright , 1964; Matthews, 1983), race (Adebimpe, 1981), sex (Wallen, Waitzkin, & Stoeckle, 1979; West, 1986), and age (Stanley et al., 1986) may affect physician-patient communication, data from the four psychiatric studies were pooled and the possibility of nonrandom subject assignment to disclosure groups on these sociodemographic variables were investigated using oneway ANOVA. No statistically significant (p < .05) differences were uncovered. Psychopa- thology may also influence clinicians' information disclosure (Benson, 1983). In order to check for potential nonrandom subject assignment to disclosure groups on this factor, an additional ANOVA was performed, using the BPRS as an indi- cator of psychopathology. Again, no statistically significant differences were noted, suggesting that approximately random assignment of subjects across dis- closure groups was achieved.
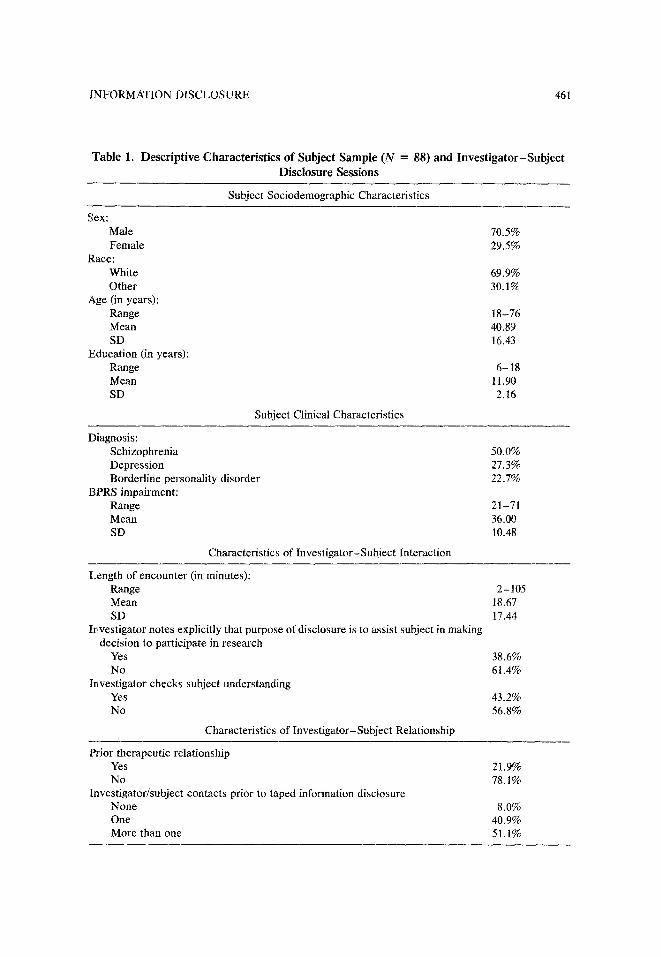
In addition to the 88 subjects taking part in our informed consent study, 12 individuals (one each from the depression and schizophrenia studies, 7 from the social skills study, and 3 from the borderline personality study) declined to partic- ipate, largely because they did not wish to be videotaped, s Table i presents de- scriptive data on the subject sample, disclosure sessions, and investigator-sub- ject relations observed across the four psychiatric studies.
Dependent Variables Two aspects of informed consent are examined in this paper. The first is the
quality of research information verbally disclosed to prospective psychiatric sub-
affect, and emotional withdrawal, among others). Each behavior is scored by an examining psychia- trist on a scale of 1 (not present) to 7 (extremely severe). The total BPRS score is the sum of these 19 subscale scores. Subject BPRS scores for this study were assessed by psychiatrists affiliated with our project.
8 Prior to participating in our research, all subjects were informed of the purpose and methods of the informed consent study. In most cases, subjects were told that the purpose of the project was " to study how people are told about research and what they understand." Subjects were also informed that the results of the study might be used to suggest changes in the way people are told about research. Prospective subjects were verbally informed of specific research procedures (videotaping and interviews), study risks and benefits, and that their participation was voluntary. Subjects were also given a written form with this information, which they were asked to sign if they agreed to participate in the study. Clearly, the process of obtaining our own subject consents, in and of itself, was a complex process and one that, at least to some extent, confounded our findings. Some sub- jects, particularIy those who were highly impaired, evidenced considerable confusion and were un- able to clearly differentiate between the informed consent and psychiatric studies. It is ironic that our informed consent study might have been methodologically sounder if we had not obtained sub- ject consent. It is also ironic that subjects' understanding of our study appeared at times to be as deficient as their understanding of the psychiatric study in which they were concurrently involved. These findings will be more closely examined in future reports.
INFORMATION DISCLOSURE 461
Table 1. Descriptive Characterist ics of Subject Sample (N = 88) and Inves t iga tor -Subjec t Disclosure Sessions
Subject Sociodemographic Characteristics
Sex: Male 70.5% Female 29.5%
Race: White 69.9% Other 30.1%
Age (in years): Range 18 - 76 Mean 40.89 SD 16.43
Education (in years): Range 6-18 Mean 11.90 SD 2.16
Subject Clinical Characteristics
Diagnosis: Schizophrenia 50.0% Depression 27.3% Borderline personality disorder 22.7%
BPRS impairment: Range 21-71 Mean 36.00 SD 10.48
Characteristics of Investigator-Subject Interaction
Length of encounter (in minutes): Range 2 - t 05 Mean 18.67 SD 17.44
Investigator notes explicitly that purpose of disclosure is to assist subject in making decision to participate in research
Yes 38.6% No 61.4%
Investigator checks subject understanding Yes 43.2% No 56.8%
Characteristics of Investigator-Subject Relationship
Prior therapeutic relationship Yes 21.9% No 78.1%
Investigator/subject contacts prior to taped information disclosure None 8.0% One 40.9% More than one 51.1%
462 BENSON ET AL.
jects. As noted above, disclosure sessions between prospective subjects and psy- chiatric investigators were observed and taped. Following each disclosure, the level of completeness of communicated information items was rated by study observers on a four-point scale utilizing the psychiatric study's written consent form as a standard reference point. Scores on the information disclosure scale ranged from a low of 0 (no disclosure of information) to a high of 3 (disclosure of information superior to the written consent form). For each study, a total of 12-22 items of research information were assessed and grouped into six informa- tion subcategories (study purposes, procedures, risks, benefits, alternatives, and methodology). Subcategory scores were constructed by summing relevant item scores for each subject and dividing that total by the number of items employed in each study for that specific subcategory. 9 Information subcategory scores thus range from 0 to 3. A global information quality score was produced by adding subcategory scores, dividing that sum by the number of relevant subcategories, and multiplying by 10.10 Possible scores on the resulting index range from 0 to 30. The alpha coefficient of reliability for the final information quality index is 0.84.
The second dependent variable, subject research understanding, was con- structed using items taken from subject interviews completed following each dis- closure session. Fifteen items (covering largely the same areas as the information disclosure items) were used to produce the composite subject understanding mea- sure. Responses to each item were assessed on a three-point scale, indicating "poor" (scored 0), "fair" (scored 1), or "good" (scored 2) subject under- standing. 11 The subject understanding index was constructed by summing item
9 In the depression study, for example, three specific risks were outlined as being associated with study participation, all of them related to the use of antidepressant medication (cardiovascular ef- fects, bowel and digestive problems, and fatigue). The disclosure of each of these risks was assessed by observers on a three-point scale. A "risk subcategory score" was then produced for each de- pression study subject by summing separate risk disclosure scores and dividing that total by 3.
10 Because of modifications in the social skills study, five disclosure items were deleted for the final seven subjects in this research project (see footnote 4). Deleted measures included all three items assessing disclosure of study methodology, one item assessing disclosure of study risks, and one item assessing disclosure of study procedures. Global information quality indices for subjects 1-13 were produced by summing across all six disclosure subcategories, While indices for subjects 14-20 were produced by summing across the five subcategories now relevant to the modified study (risks, benefits, alternatives, procedures, and purpose; methodology is excluded). Index scores across the two sets of subjects were standardized by dividing individual score totals by the number of relevant subcategories for that subject, six for subjects 1-13, five for subjects 14-20. All results were then multiplied by 10.
11 A score of 0 (poor understanding) was given for an unacceptable subject response, one that was factually wrong, irrelevant to the question, or delusional. A score of 1 (fair understanding) was given for a partially correct response, one that was incomplete, or held with marked uncertainty. A score of 2 (good understanding) was given for an acceptable (although not necessarily fully com- plete) response. A subject's understanding of study risks, for example, would be scored 0 if a subject gave no response or if a completely incorrect, delusional, or incoherent response to the interview question. If the subject could recall one study risk (e.g., a drug side-effect), a score of 1 would be given. If the subject could recall two or more risks, a score of 2 would be given. Interrater reliability in the scoring of subject understanding exceeded 0.90 (Kendall tau coefficients) in all four p~,ychiatric studies.

INFORMATION DISCLOSURE 463
scores for each subject.lz Possible scores on the understanding index range from 0 to 30; the alpha coefficient for the measure is 0.81.
RESULTS
The Impact of Disclosure Method on Information Quality
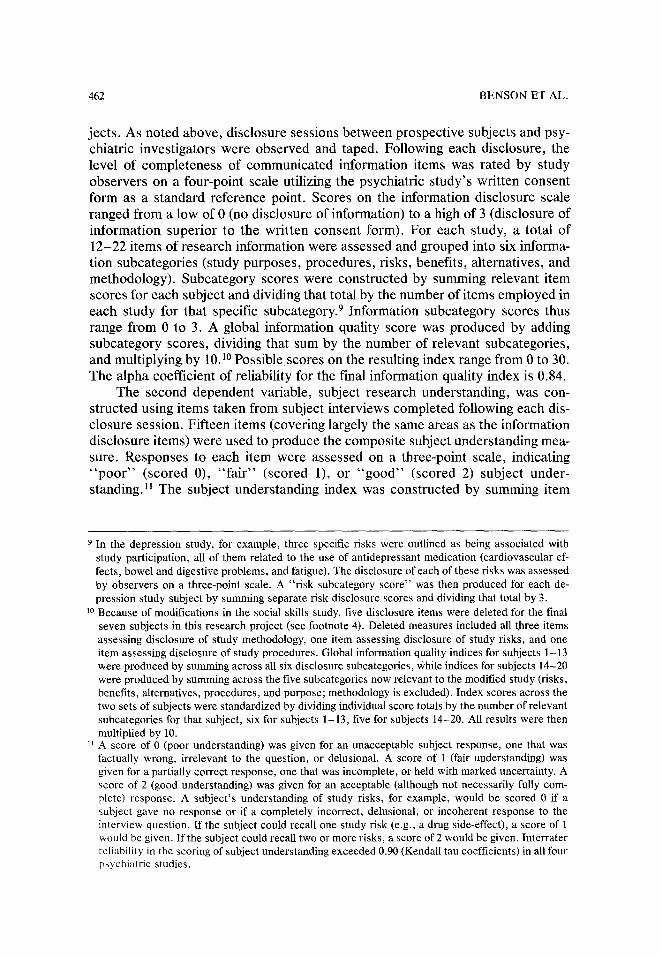
We first examine the effect of disclosure method on the quality of research information communicated to prospective psychiatric subjects. Table 2 presents data on the six information subcategories (risks, benefits, alternatives, purposes, procedures, and methods), as well as several other aspects of informed consent, cross-tabulated by disclosure method.
Prior informed consent studies (Gray, 1975; Lidz et al., 1984) have noted that subjects at times believe they have little choice but to consent to research, espe- cially when the study is conducted by physicians to whom they feel an obligation as a patient. This suggests that investigators need to clearly inform prospective subjects that they have the fight to accept or reject research participation. As Table 2 shows, only 27% of subjects in the unassisted disclosure group and 36% in the unassisted videotape group were explicitly informed of their right to choose. Marked improvement in the disclosure of this information, however, was noted in the assisted videotape and neutral educator disclosure groups, where 73% and 91%, respectively, were so informed.
Perusal of the written consent form by prospective subjects is also necessary for adequate informed consent. Nevertheless, across the first three disclosure methods, a substantial percentage of patients were not encouraged to read the consent document, 36% in the unassisted disclosure group, 50% in the unassisted videotape group, and 46% in the assisted videotape group. However, the per- centage of subjects so encouraged rose to 100% in the neutral educator group. Similarly, assessment of subject understanding during disclosure was often not observed using the first three disclosure methods, but occurred in all disclosures employing a neutral educator.
Significant differences by disclosure method were also found in mean infor- mation subcategory scores. Comparing the first experimental method (unassisted disclosure with videotape) to the base-line method (unassisted disclosure), a sig- nificant increase in the quality of communicated information was noted for the latter in only one subcategory, research purposes. In contrast, when compared to the base-line method, all subcategories (except research risks) showed significant improvement using the second experimental method, assisted disclosure with videotape. The disclosure of all information subcategories was significantly ira-
x2 Because of modifications in the social skills study, three items dealing with study methodology and procedures were deleted from initial understanding interviews with subjects 14 and 15. For subjects 16-20, substituted items appropriate to the modified study design were employed (see footnote 4). Composite understanding scores for subjects 14-15 were derived by assigning each deleted item that subject's mean score on all remaining understanding items.
464 B E N S O N E T A L .
proved utilizing the neutral educator method. Overall, the largest improvements in information disclosure were found using the neutral educator method, with the greatest subcategory gains occurring in the communication of research alterna- tives and methods. Finally, compared to base-line disclosures, global information quality was significantly improved using the assisted videotape and neutral edu- cator techniques.
The above analyses suggest that the use of innovative methods of informa- tion delivery (particularly the use of neutral educators) can improve the quality of research information communicated to prospective psychiatric subjects. How- ever, these analyses do not take differences by research study into account, nor do they test for statistical interaction between psychiatric study and disclosure method. Lastly, it is possible that factors inadequately controlled for by the study design may bias these bivariate results.
In order to expand our analysis of information disclosure, as well as increase its precision through the control of potentially confounding factors, a series of multivariate models were estimated employing ordinary least-squares (OLS) mul- tiple regression. Two major explanatory variables were employed in the regres- sions: (a) psychiatric research study (comprising three effects-coded nominal cat- egories), and (b) information disclosure method (represented by three dummy-
T a b l e 2 . C o n s e n t D i s c l o s u r e C o m p l e t e n e s s by I n f o r m a t i o n D i s c l o s u r e M e t h o d ,
A l l P s y c h i a t r i c S tu d ie s ~
Unassis ted Assisted Neutral Unassisted video video educator Total disclosures disclosures disclosures disclosures disclosures
(n = 22) (n = 22) (n = 22) (n = 22) (N - 88)
Subject's right to choose emphasized or noted during disclosure 27% 36% 73% 91% 57% b
Subject encouraged to read consent form 64% 50% 54% 100% 67% b Subject understanding of research
checked during disclosure 50% 45% 36% 100% 58% b Mean Information Disclosure
Scores (range 0-3) : Research risks 1.38 1.58 2.03 2.55 c 1.89 b
(1422) (1.19) (0.69) (0.49) (1.04) Research benefits 1463 1.72 2.35 c 2.39 r 2.02 b
(1,20) (0.79) (0f.60) (0.66) (0.90) Research purposes 1,64 2.32 c 2.42 c 2.70 c 1.89 b
(1.07) (0.68) (0.69) (0.43) (0.84) Research alternatives 1.03 1.28 1.99 c 2.46 ~ 1.69 b
(0.95) (0.86) (1.14) (0.51) (1.05) Research procedures 1.80 2.13 2.49 ~ 2.57 ~ 2.25 ~
(0.95) (0.67) (0.22) (0,38) (0.68) Research methods 1.49 1.98 2.55 c,a 2.91 c,e 2.23 b:
(1.21) (1.16) (0.98) (0.14) (1.12) Mean global information quality
(Range 0 -30) 14.95 18.34 22.80 ~ 25.49 ~ 20.49 b
a Note: Percentages may not sum to 100 owing to rounding. Standard deviations are parenthesized. b Percentage (or mean) differences between disclosure method groups statistically significant at p < .01 level: chi-
square (or one-way ANOVA), l-tail test. A posteriori contrast of disclosure group mean with unassisted (base-line) group mean significant at p < .05 level: Tukey's Honestly Significant Difference test.
d Group n reduced to 20 owing to design modifications in social skills study (see footnotes 4 and l0 of text). e Group n reduced to 17 owing to changes in social skills study. : Total subject N reduced to 81 owing to changes in social skills study.

1N FORMATION DISCLOSURE 465
coded categories, with "unassisted disclosures" the omitted reference category). 13 Two additional independent variables were also included as statis- tical controls: whether the prospective subject had a prior therapeutic relation- ship with the investigator, and (e) the extent of investigator-subject discussion occurring prior to the taped disclosure session.14 The former control variable is a dichotomy; the latter was divided into three categories and dummy-coded (with "no discussion" the omitted category).
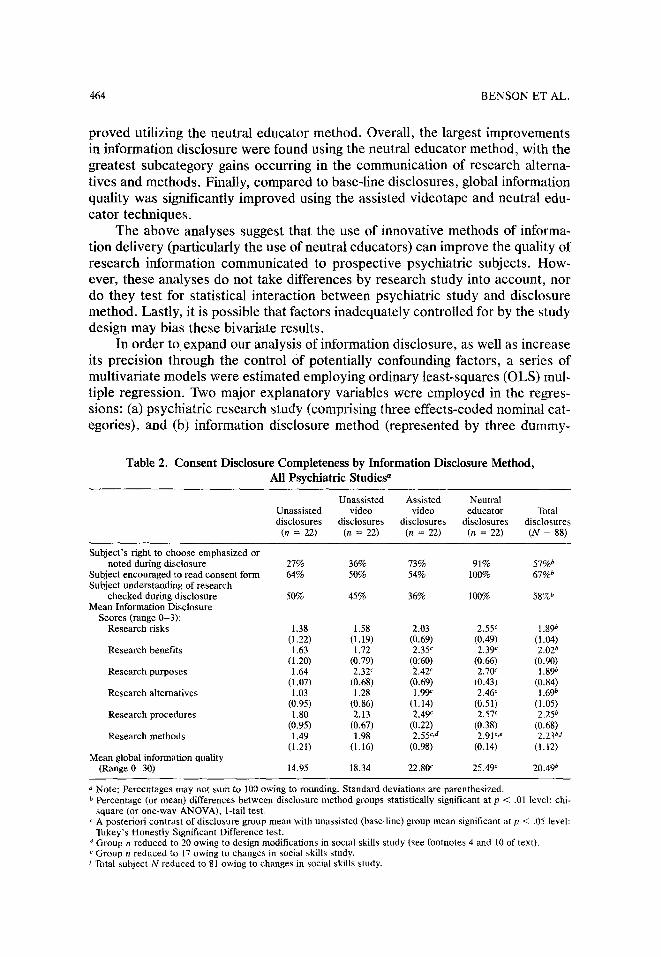
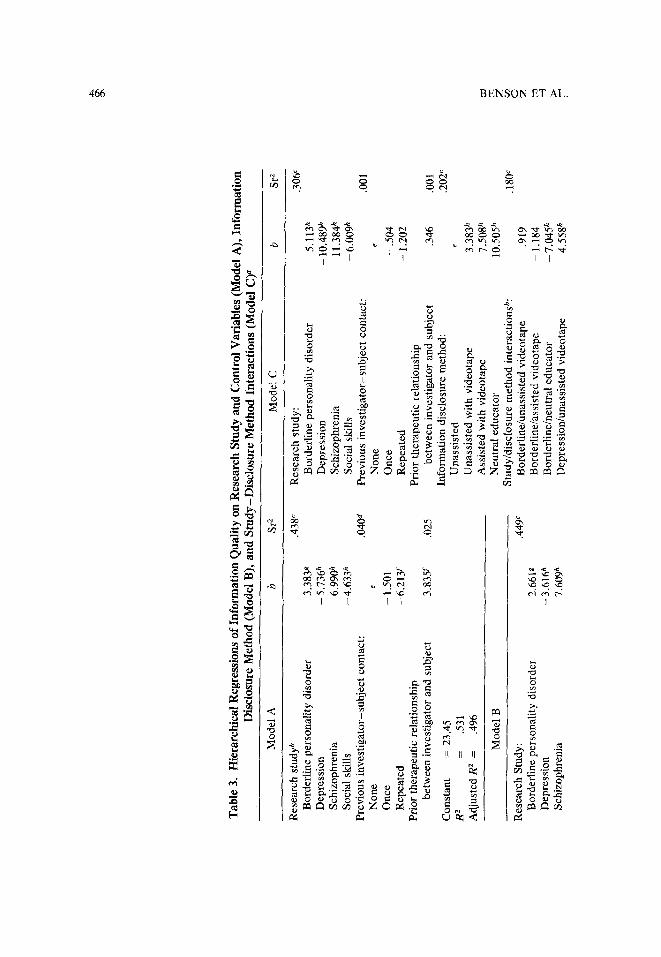
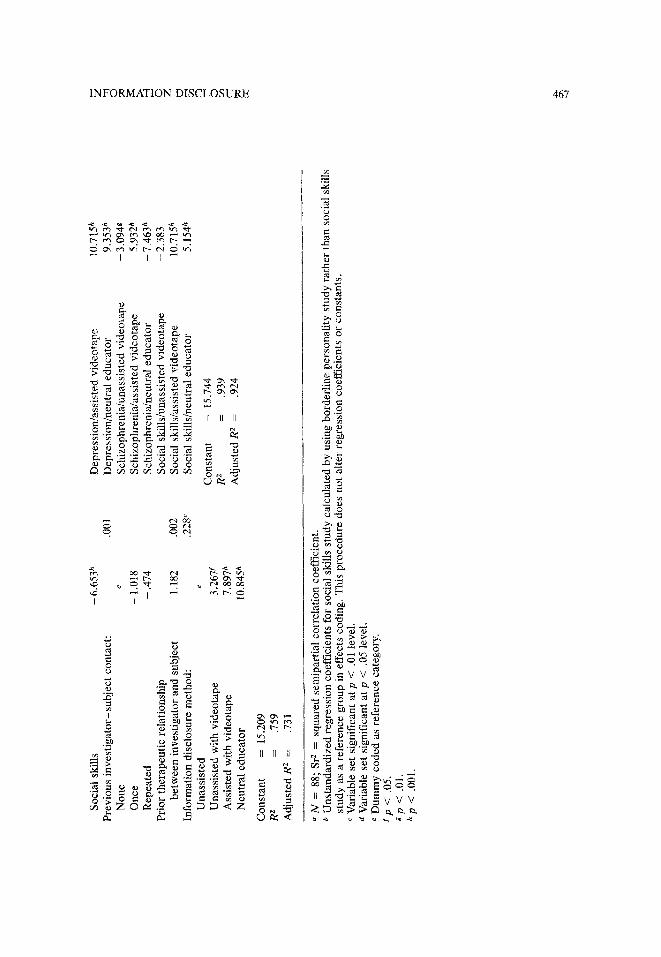
In order to clearly assess the main and interactive effects of the major ex- planatory variables on information quality, a series of three hierarchical regres- sion equations were estimated (Cohen and Cohen, 1975). The first equation (Model A) estimates the regression of information quality on research study and the control variables. The second equation (Model B) adds disclosure method to this initial model, while the third equation (Model C) adds disclosure method and a series of multiplicative study-disclosure method interaction terms. The results of the three regressions are presented in Table 3.
Estimation of the Model A equation shows research study to be a highly significant predictor of information quality, accounting uniquely for 82% of the model's explained variance (R 2) of 0.531. Within the variable set, the schizo- phrenia study generates the highest level of information quality, followed by the borderline personality disorder study. Much poorer in their oral communication of research information are the social skills and depression studies. Both control variables are also significant in the initial equation, indicating that previous inves- tigator-subject discussion concerning the psychiatric study decreases informa- tion communicated during the taped disclosure, while the existence of a prior treatment relationship between investigator and subject increases these commu- nications.
Model B adds a set of three dummy-coded contrasts representing disclosure method to the initial regression equation. As suggested in the bivariate results, the multivariate analysis shows disclosure method to be a highly significant de- terminant of information quality, with each experimental disclosure technique in- troduced into the protocol having a progressively greater impact on the depen-
13 In effects-coding, the unstandardized regression coefficients represent the difference between the category mean and the unweighted mean of all category means, rather than the difference between a category mean and the reference group mean, as in dummy-coding (Cohen & Cohen, 1975). Ef- fects-coding was used to represent research study in the regressions presented in Table 3 because no one study could be selected as a more appropriate reference group titan any other.
14 As noted, it has been suggested that subjects may uncritically consent to research participation when the study investigator is also their treating physician. Because a substantial percentage (22%) of our observed subjects had been treated therapeutically by their study investigator at some point, a dummy-coded variable was included in the regression analyses to take this factor into account. In addition, in most cases, some discussion regarding the psychiatric research took place between subject and investigator prior to the taped disclosures that serve as the basis for our analysis of subject-researcher communication. In most cases, these discussions were minimal, but in some cases (particularly in the borderline personality disorder study), subjects received consideraNe in- formation prior to the taped disclosure session. A second variable was employed in the multivariate analyses in an attempt to control statistically for these occurrences.
Tab
le 3
. H
iera
rchi
cal R
egre
ssio
ns o
f In
form
atio
n Q
ualit
y on
Res
earc
h St
udy
and
Con
trol
Var
iabl
es (
Mod
el A
), I
nfor
mat
ion
Dis
clos
ure
Met
hod
(Mod
el B
), a
nd S
tudy
-Dis
clos
ure
Met
hod
Inte
ract
ions
(M
odel
C) a
Mo
del
A
b S
r 2
Mo
del
C
b S
r z
Res
earc
h s
tud
y b
.438
~
Res
earc
h s
tud
y:
.306
~
Bo
rder
lin
e p
erso
nal
ity
dis
ord
er
3.38
3g
Bo
rder
lin
e p
erso
nal
ity
dis
ord
er
5.11
3 h
Dep
ress
ion
-
5.73
6 h
Dep
ress
ion
-
10,4
89 h
S
chiz
op
hre
nia
6.
99ff
' S
chiz
op
hre
nia
11
.384
h
So
cial
ski
lls
- 4.
633
h S
oci
al s
kill
s -
6.00
9 h
Pre
vio
us
inv
esti
gat
or-
sub
ject
co
nta
ct:
.040
~
Pre
vio
us
inv
esti
gat
or-
sub
ject
co
nta
ct:
.001
N
on
e e
No
ne
e
On
ce
- 1.
501
On
ce
-.5
04
R
epea
ted
-
6.21
3 f
Rep
eate
d
- 1.
202
Pri
or
ther
apeu
tic
rela
tio
nsh
ip
Pri
or
ther
apeu
tic
rela
tio
nsh
ip
bet
wee
n i
nv
esti
gat
or
and
su
bje
ct
3,83
5~
.025
b
etw
een
in
ves
tig
ato
r an
d s
ub
ject
.3
46
.001
Co
nst
ant
=
23.4
5 In
form
atio
n d
iscl
osu
re m
eth
od
: .2
02 c
R z
=
.5
31
Un
assi
sted
e
Ad
just
ed R
2 =
.4
96
Un
assi
sted
wit
h v
ideo
tap
e 3.
383
h A
ssis
ted
wit
h v
ideo
tap
e 7.
508
h M
od
el B
N
eutr
al e
du
cato
r 10
.505
h
Stu
dy
/dis
clo
sure
met
ho
d i
nte
ract
ion
sb:
.180
c R
esea
rch
Stu
dy
: .4
49 ~
B
ord
erli
ne/
un
assi
sted
vid
eota
pe
.919
B
ord
erli
ne
per
son
alit
y d
iso
rder
2.
661g
B
ord
erli
ne/
assi
sted
vid
eota
pe
- 1.
184
Dep
ress
ion
-
3-61
6h
Bo
rder
lin
e/n
eutr
al e
du
cato
r -
7.04
5 h
Sch
izo
ph
ren
ia
7"60
9h
Dep
ress
ion
/un
assi
sted
vid
eota
pe
4.55
8 h
�9
So
cial
ski
lls
-6.6
53
h
Dep
ress
ion
/ass
iste
d v
ideo
tap
e 10
.715
h
Pre
vio
us
inv
esti
gat
or-
sub
ject
co
nta
ct:
.00
1
Dep
ress
ion
/neu
tral
ed
uca
tor
9.35
3 h
No
ne
e S
chiz
op
hre
nia
/un
assi
sted
vid
eota
pe
- 3.
0943
O
nce
-
1.01
8 S
chiz
op
hre
nia
/ass
iste
d v
ideo
tap
e -
5.93
2 h
Rep
eate
d
- .4
74
Sch
izo
ph
ren
ia/n
eutr
al e
du
cato
r -
7.46
3 h
Pri
or
ther
apeu
tic
rela
tio
nsh
ip
So
cial
sk
ills
/un
assi
sted
vid
eota
pe
-2.3
83
b
etw
een
in
ves
tig
ato
r an
d s
ub
ject
1.
182
.002
S
oci
al s
kil
ls/a
ssis
ted
vid
eota
pe
10.7
15 h
In
form
atio
n d
iscl
osu
re m
eth
od
: .2
28 c
S
oci
al s
kil
ls/n
eutr
al e
du
cato
r 5.
154
h U
nas
sist
ed
e
Co
nst
ant
=
15.7
44
Un
assi
sted
wit
h v
ideo
tap
e 3.
267f
R
2
=
.939
A
ssis
ted
wit
h v
ideo
tap
e 7.
897
h N
eutr
al e
du
cato
r 10
.845
h
Ad
just
ed R
z
=
.924
Co
nst
ant
=
15.2
09
R 2
=
.7
59
Ad
just
ed R
z
=
,731
�9
7~
:g
�9
"N
=
88;
Sr 2
=
squ
ared
sem
ipar
tial
co
rrel
atio
n c
oef
fici
ent.
b
Un
stan
dar
diz
ed r
egre
ssio
n c
oef
fici
ents
fo
r so
cial
ski
lls
stu
dy
cal
cula
ted
by
usi
ng
bo
rder
lin
e p
erso
nal
ity
stu
dy
rat
her
th
an s
oci
al s
kill
s st
ud
y a
s a
refe
ren
ce g
rou
p i
n ef
fect
s co
din
g,
Th
is p
roce
du
re d
oes
no
t al
ter
reg
ress
ion
co
effi
cien
ts o
r co
nst
ants
. c
Var
iabl
e se
t si
gn
ific
ant
at p
<
.0
1 le
vel.
a
Var
iabl
e se
t si
gn
ific
ant
at p
<
.0
5 le
vel,
e
Du
mm
y c
od
ed a
s re
fere
nce
cat
ego
ry.
Yp
<
.05.
g
p <
.0
1.
h p
<
.001
.
"-4
468 B E N S O N E T A L .
dent variable. As a set, disclosure method uniquely accounts for 30% of the vari- ance explained by the second model (0.759).
Model C was estimated to check for variation in the impact of disclosure method across the four psychiatric research studies. The results of this third re- gression clearly indicate that such a statistical interaction exists between study and disclosure method, accounting uniquely for 19% of the final model R 2 of 0.939. Examination of interaction term coefficients indicates that, when com- pared to unassisted base-line communications, the effect of each experimental disclosure method on information quality varies by research study in the fol- lowing manner:
1. In the borderline personality disorder study: the neutral educator method is significantly less effective than it is in general (averaged over all studies);
2. In the schizophrenia study: each experimental method is significantly less effective than it is in general (averaged over all studies);
3. In the depression study: each experimental method is significantly more effective than it is in general (averaged over all studies);
4. In the social skills study: the assisted videotape and the neutral educator method are each significantly more effective than in general (averaged over all studies).
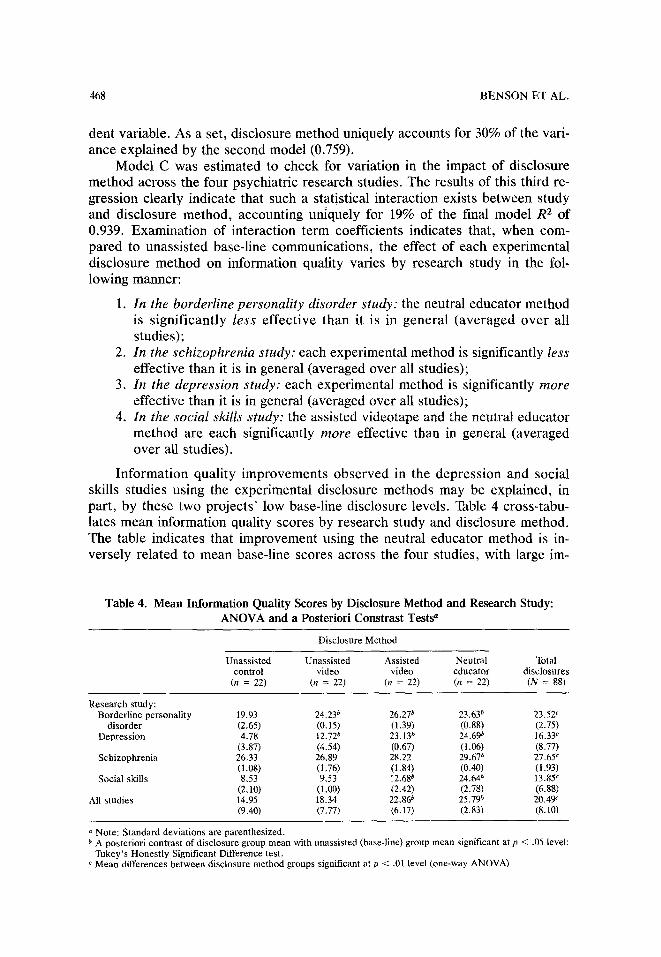
Information quality improvements observed in the depression and social skills studies using the experimental disclosure methods may be explained, in part, by these two projects' low base-line disclosure levels. Table 4 cross-tabu- lates mean information quality scores by research study and disclosure method. The table indicates that improvement using the neutral educator method is in- versely related to mean base-line scores across the four studies, with large im-
Table 4. M e a n I n f o r m a t i o n Qua l i ty Scores by D i s c l o s u r e M e t h o d a n d R e s e a r c h Study: A N O V A a n d a Poster ior i Cons tras t Tes t s a
Disclosure Method
Unassisted Unassisted Assisted Neutral Total control video video educator disclosures
(n = 22) (n = 22) (n = 22) (n = 22) (N = 88)
Research study: Borderline personality
disorder Depression
Schizophrenia
Social skills
All studies
19.93 24.23 b 26.27 b 23.63 b 23.52 c (2,65) (0.15) (1.39) (0.88) (2.75) 4.78 12.72 b 23.13 b 24.69 b 16-33 c
(3.87) (4,54) (0.67) (1.06) (8.77) 26.33 26,89 28.22 29.67 b 27.65 c (1.08) (1.76) (1.84) (0.40) (1.93) 8.53 9,53 12.68 b 24.64 ~ 13.85 c
(2.10) (1.00) (2.42) (2.78) (6.88) 14.95 18.34 22.86 b 25.79 ~ 20.49 ~ (9,40) (7.77) (6.17) (2.83) (8.10)
Note: Standard deviations are parenthesized. b A posteriori contrast of disclosure group mean with unassisted (base-line) group mean significant at p <
Tukey's Honestly Significant Difference test. c Mean differences between disclosure method groups significant at p < .01 level (one-way ANOVA).
.05 level:

INFORMATION DISCLOSURE 469
provement using neutral educators evident in the depression and social skills studies (where mean base-line scores are low) and small improvement in the bor- derline and schizophrenia projects (where mean baseline scores are relatively high).
In summary, our findings thus far indicate that modifications in the consent process can significantly improve the quality of information communicated to prospective research subjects. Moreover, results suggest that consent interven- tions are most effective where they are most needed: in research studies where, under normal circumstances, little information is communicated to prospective subjects.
Disclosed Information and Subject Understanding
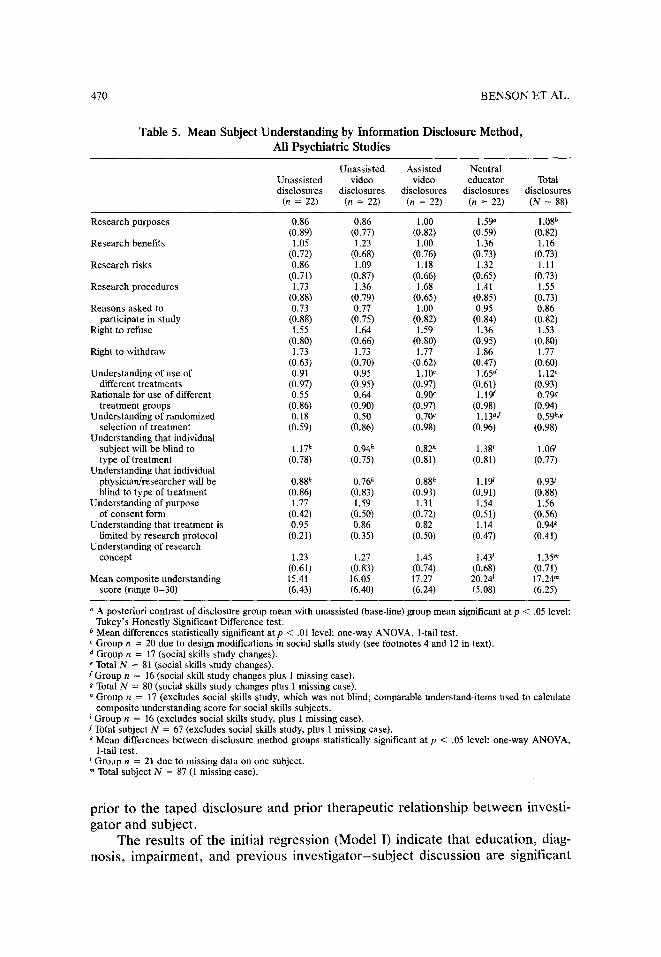
A second question remains: does improved information disclosure result in greater subject understanding? Table 5 presents the 15 specific items comprising the composite understanding index cross-tabulated by disclosure method. While prospective research subjects generally demonstrated good understanding of the purpose of the written consent form and their right to refuse or withdraw from the study, they evidenced much lower understanding of other areas. For example, they frequently did not understand the psychiatric research project's purpose or why they had been asked to participate in it. Subjects also often demonstrated poor understanding of important methodological aspects of the study, including the randomized and double-blind treatment assignment.
Compared to earlier improvements in information disclosure, subject under- standing also appears to be less affected by modifications in information disclo- sure method. Table 5 indicates that, when compared to subjects informed with the base-line disclosure method, the understanding of subjects informed by a neutral educator improves significantly on only two items (research purposes and ran- domized selection of treatment). It should be noted, however, that while not ob- taining statistical significance, several other areas of subject understanding (in- cluding study risks and benefits, understanding of and rationale for different treatment groups, understanding of investigator blindness, and treatment limita- tions) evidence substantive improvement using the neutral educator method. In addition, mean differences in overall subject understanding by disclosure method nearly reach statistical significance (p = .054).
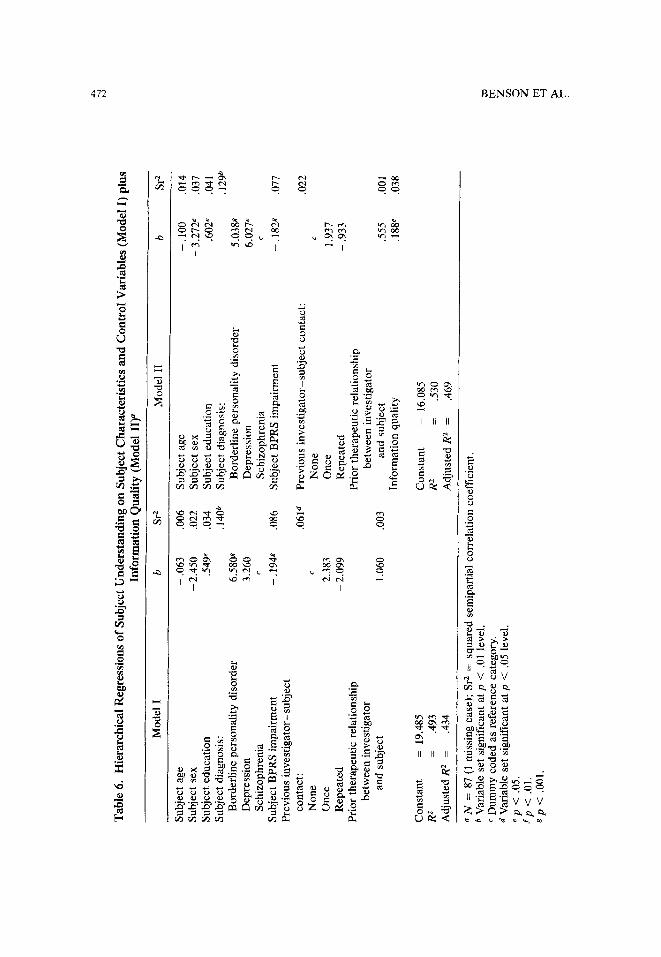
To what extent does improved information disclosure actually translate into increased subject understanding and to what degree is improvement in under- standing limited by subject psychopathology and other subject characteristics? In order to address these questions, two final hierarchical regression equations were estimated, using subject understanding as the dependent variable. The results of these regressions are presented in Table 6. The independent variables employed in the first of these two regressions (Model I) include subject sex and age, educa- tional attainment (measured in years), diagnosis (dummy-coded with schizo- phrenia serving as the omitted reference category), and psychiatric impairment (indicated by BPRS score). As in the previous regressions, two additional control variables were also included in the equations: investigator-subject discussions
470 B E N S O N E T A L .
Table 5. Mean Subject Understanding by Information Disclosure Method, All Psychiatric Studies
Unassisted Assisted Neutral Unassisted video video educator Total disclosures disclosures disclosures disclosures disclosures
(n = 22) (n = 22) (n = 22) (n = 22) (N = 88)
Research purposes
Research benefits
Research risks
Research procedures
Reasons asked to participate in study
Right to refuse
Right to withdraw
0.86 0.86 1.00 1.59 ~ 1.08 b (0.89) (0,77) (0.82) (0.59) (0.82) 1.05 1.23 1.00 1.36 1.16
(0.72) (0,68) (0.76) (0.73) (0.73) 0.86 1,09 1.18 1.32 1.11
(0.71) (0.87) (0.66) (0.65) (0.73) 1.73 1.36 1.68 1.41 1.55
(0.88) (0.79) (0.65) (0.85) (0.73) 0.73 0.77 1.00 0.95 0.86
(0.88) (0.75) (0.82) (0,84) (0.82) 1.55 1.64 1.59 1.36 1.53
(0.80) (0.66) (0.80) (0.95) (0.80) 1.73 1.73 1.77 1.86 1.77
(0.63) (0.70) (0.62) (0.47) (0.60) Understanding of use of 0.91 0.95 1.10 c 1.65 d 1.12*
different treatments (0.97) (0.95) (0.97) (0.61) (0.93) Rationale for use of different 0.55 0.64 0.90 c 1.19 t" 0.79e
treatment groups (0.86) (0.90) (0.97) (0.98) (0.94) Understanding of randomized 0.18 0.50 0.70 c 1.13 ad 0.59 b,g
selection of treatment (0.59) (0.86) (0.98) (0.96) (0.98) Understanding that individual
subject will be blind to 1.17 h 0.94 h 0.82 h 1.38 i 1.06/ type of treatment (0.78) (0.75) (0.81) (0.81) (0.77)
Understanding that individual physician/researcher will be 0.88 h 0.76 h 0.88 h 1.19 i 0.93/ blind to type of treatment (0.86) (0.83) (0.93) (0.91) (0.88)
Understanding of purpose 1.77 1.59 1.31 1.54 1.56 of consent form (0.42) (0.50) (0.72) (0.51) (0.56)
Understanding that treatment is 0.95 0.86 0.82 1.14 0.94 k limited by research protocol (0.21) (0.35) (0.50) (0.47) (0.41)
Understanding of research concept 1.23 1.27 1.45 1.43 t 1.35"
(0.61 ) (0.83) (0.74) (0.68) (0.71 ) Mean composite understanding 15.41 16.05 17.27 20.24 t 17.24 m
score (range 0-30) (6.43) (6.40) (6.24) (5.08) (6.25)
A posteriori contrast of disclosure group mean with unassisted (base-line) group mean significant at p < .05 level: Tukey's Honestly Significant Difference test.
b Mean differences statistically significant at p < .01 level: one-way ANOVA, 1-tail test. c Group n = 20 due to design modifications in social skills study (see footnotes 4 and 12 in text). d Group n = 17 (social skills study changes). e Total N = 81 (social skills study changes). S Group n = 16 (social skill study changes plus 1 missing case). g Total N = 80 (social skills study changes plus 1 missing case). h Group n = 17 (excludes social skills study, which was not blind; comparable understand-items used to calculate
composite understanding score for social skills subjects. i Group n = 16 (excludes social skills study, plus 1 missing case). J Total subject N = 67 (excludes social skills study, plus 1 missing case). k Mean differences between disclosure method groups statistically significant at p < .05 level: one-way ANOVA,
l-tail test. Group n = 21 due to missing data on one subject.
" Total subject N = 87 (1 missing case).
prior to the taped disclosure and prior therapeutic relationship between investi- gator and subject.
The results of the initial regression (Model I) indicate that education, diag- nosis, impairment, and previous investigator-subject discussion are significant

INFORMATION DISCLOSURE 471
predictors of subject understanding, accounting jointly for 49% of the variance of the dependent variable. Examination of the squared semipartial correlation coef- ficients associated with each variable shows diagnosis and psychiatric impair- ment as the two most significant determinants of subject understanding, ac- counting, respectively, for 29% and 17% of the model's explained variance. Schizophrenics and highly impaired subjects were found most likely to demon- strate low research understanding, while the less impaired and those diagnosed with borderline personality disorder evidenced the highest levels of under- standing.
Model II reestimates the previous equation adding information quality as an independent variable. While a significant predictor of subject understanding, in- formation quality uniquely accounts for only a modest 7% of the total R 2 ac- counted for by Model II. In comparison, subject sociodemographic character- istics (age, sex, and education) uniquely account for 14%, and subject clinical characteristics (diagnosis and impairment) for 48% of the explained variance in this final model.
DISCUSSION AND CONCLUSION
The results of the present study support a number of earlier findings flowing from informed consent investigations conducted in medical research settings. As in previous studies, we found prospective subjects' understanding of research and research participation to be problematic in many areas. In particular, subjects demonstrated poor understanding of scientific rationale and procedures and fre- quently perceived research participation in therapeutic and personalized terms-- for example, noting that "research means finding out what works best for me" or "research means doing special tests on my condition." The tendency of subjects to view research participation in clinical terms has been described by us else- where as "the therapeutic misconception" (Appelbaum, Roth, & Lidz, 1983; Ap- pelbaum et al., 1987).
A number of factors were significantly related to subject understanding. Subjects' educational level was positively associated with research under- standing. Clinical characteristics, such as psychiatric diagnosis and level of im- pairment, were also highly important predictors of research understanding, with schizophrenic and highly impaired subjects significantly more likely than others to display poor comprehension.
An important, but seldom examined, influence on understanding is the amount and quality of information communicated to prospective subjects during the consent process. Our investigation indicated that information disclosures by psychiatric researchers (particularly when unassisted) frequently lacked or mis- communicated key information on study risks, benefits, alternative treatments, study procedures, and methodology. In particular, investigators often down- played scientific and methodological aspects of their research, while, at the same time, emphasizing its therapeutic elements (one investigator, for example, rou- tinely refused to describe his project as "research" in discussions with prospec-
Tab
le 6
, H
iera
rch
ical
Reg
ress
ion
s o
f S
ub
ject
Un
der
stan
din
g
on
Su
bje
ct C
har
acte
rist
ics
and
C
on
tro
l V
aria
ble
s (M
od
el I
) p
lus
Info
rmat
ion
Q
ual
ity
(M
od
el
II) a
4~
-,,d
tO
Mod
el I
b
Sr 2
M
od
el I
I b
Sr 2
Sub
ject
age
S
ubje
ct s
ex
Sub
ject
ed
uca
tio
n
Sub
ject
dia
gnos
is:
Bor
derl
ine
per
son
alit
y d
iso
rder
D
epre
ssio
n
Sch
izo
ph
ren
ia
Sub
ject
BP
RS
im
pai
rmen
t P
rev
iou
s in
ves
tig
ato
r-su
bje
ct
cont
act:
N
on
e O
nce
R
epea
ted
P
rior
the
rape
utic
rel
atio
nshi
p b
etw
een
inv
esti
gato
r an
d s
ubje
ct
Co
nst
ant
= 19
.485
R
z
= .4
93
Ad
just
ed R
z
= .4
34
- .0
63
.006
S
ubje
ct a
ge
-. 1
00
,014
-
2.45
0 .0
22
Sub
ject
sex
-
3.27
2 e
,037
.5
49 *
.034
S
ubje
ct e
du
cati
on
.6
02 e
.041
,1
40 b
Sub
ject
dia
gnos
is:
.129
0 6.
580e
B
orde
rlin
e p
erso
nal
ity
dis
ord
er
5,03
8g
3.26
0 D
epre
ssio
n
6,02
7 e
Sch
izo
ph
ren
ia
c -.
19
4g
.0
86
Sub
ject
BP
RS
im
pai
rmen
t -.
18
2e
.077
.061
d P
revi
ous
inv
esti
gat
or-
sub
ject
con
tact
: .0
22
c N
on
e c
2.38
3 O
nce
1.
937
- 2.
099
Rep
eate
d
- .9
33
Pri
or t
her
apeu
tic
rela
tion
ship
b
etw
een
inv
esti
gato
r 1.
060
.003
an
d s
ubje
ct
.555
.0
01
Info
rmat
ion
qua
lity
.1
88 e
.038
Co
nst
ant
= 16
.085
R
~
= .5
30
Ad
just
ed R
2
= .4
69
a N
=
87 (
1 m
issi
ng c
ase)
; S
r 2 =
sq
uar
ed s
emip
arti
al c
orre
lati
on c
oeff
icie
nt.
b V
aria
ble
set
sign
ific
ant
at p
<
.01
leve
l,
c D
um
my
cod
ed a
s re
fere
nce
cat
egor
y.
a V
aria
ble
set
sign
ific
ant
at p
<
.05
leve
l.
ep
< ,0
5,
ep
< .0
1.
gp
<
.001
.
r~
,..]
>

INFORMATION DISCLOSURE 473
tive subjects). Incomplete and, in some cases, misleading investigator communi- cations clearly contributed to poor understanding by subjects in some instances (for additional descriptive findings and discussion on this issue, see Benson, Roth, & Winslade, 1985; Benson et al., 1987).
Given these deficiencies in investigator information disclosure and subject understanding, can informed consent processes be improved? Our findings sug- gest they can. Innovative methods of information delivery, employing third-party investigator and subject education, were generally superior to unassisted investi- gator disclosures in transmitting high-quality research information to prospective subjects. However, our research also indicates that the impact of increased infor- mation on subject understanding may vary substantially across studies using dif- ferent patient populations. By increasing the amount and quality of disclosed in- formation, some improvement in understanding appears possible for most psychi- atric subjects. However, the degree of improvement may be substantially lower for schizophrenics and the highly impaired than it is for others. Further research is needed to better assess the limitations imposed by psychopathology and other clinical factors on subject comprehension.
Because of the relatively small size of our subject sample, the results of this study should be viewed as preliminary and in need of replication. Its findings, nevertheless, strongly suggest that the current system of eliciting informed con- sent in psychiatric research is not working as well as it could. Improvement in this regard, however, is at least partially contingent upon the willingness of clin- ical researchers to give up their unilateral control of medical information--and thus some measure of professional and interpersonal dominance vis-a-vis their subjects (Freidson, 1970; Katz, 1984; Waitzkin, 1986). However, as we have ob- served elsewhere (Appelbaum et al., 1987), it is often n o t in researchers' best interest to equalize relations with subjects by sharing information, uncertainty, and decision making with them. For this reason, modifications in the consent process would probably need to be implemented by independent third parties, such as local institutional review boards (Robertson, 1982). Such intervention into the traditionally dyadic investigator-subject relationship would undoubtedly create problems for medical researchers, including potential study delays and the probability that some prospective subjects would decide not to participate as a result of increased educational efforts. In the end, the question of how much weight to give to informed consent is a matter of values and societal priorities. It is a question that social scientific research may enlighten, but cannot resolve.
R E F E R E N C E S
Adebimpe, V. R. (1981). White norms and psychiatric diagnosis of black patients. American Journal of Psychiatry, 138, 279-285.
Annas, G. J., Glantz, L. H., & Katz, B. E (1977). Informed consent to human experimentation. Cambridge, Massachusetts: Batlinger.
Appelbaum, E S., Lidz, C. W., & Meisel, A. (1987). Informed consent: legal theory and clinical practice. New York: Oxford University Press.
474 BENSON ET AL.
Appelbaum, P. S., Roth, L. H., & Lidz, C. W. (1983). The therapeutic misconception: Informed con- sent in psychiatric research. International Journal of Law and Psychiatry, 5, 319-329.
Appelbaum, P. S., Roth, L. H., Lidz, C. W., Benson, E, & Winslade, W. (1987). False hopes and best data: Consent to research and the therapeutic misconception. Hastings Center Report, 17, 20-24.
Barber, B. (1980). Informed consent in medical therapy and research. New Brunswick, New Jersey: Rutgers University Press.
Barber, B., Lally, J., Makarushka, J. L., & Sullivan, D. (1973). Research on human subjects: Problems of social control in medical experimentation. New York: Russell Sage Foundation.
Barbour, G. L., & Blumenkrantz, M. J. (1978). Videotape aids informed consent decision. Journal of the American Medical Association, 240, 2741-2742.
Benson, E R. (1983). Informed consent: Drug information disclosed to patients prescribed antipsy- chotic medication. Journal of Nervous and Mental Disease, 172, 642-652.
Benson, E R., & Roth, L. H. (in press). Trends in the social control of medical and psychiatric re- search. In D. N. Weisstub (Ed.), Mental health and law: International perspectives, Vol. 3, New York: Pergamon.
Benson, E R., Roth, L. H., & Winslade, W. J. (1985). Informed consent in psychiatric research: Preliminary findings from an ongoing investigation. Social Science and Medicine, 20, 1331-1341.
Benson, E R., Roth, L. H., Appelbaum, E S., Lidz, C. W., & Winslade, W. J. (1987). Informed con- sent and the regulation of psychiatric research. In J. L. Miller & M. Lewis (Eds.), Research in Social Problems and Public Policy, Vol. 5 (pp. 151-192), New York: JAI Press.
Boreham, E, & Gibson, D. (1978). The informative process in private medical consultations: A pre- liminary investigation. Social Science and Medicine, 12(5A), 409-416.
Capron, A. M. (1986). Human experimentation. In J. E Childress, E A. King, K. H. Rothenberg, & W. J. Wadlington, (Eds.), BioLaw: A legal and ethical reporter on medicine, health care, and bioengineering (pp. 217-252). Frederick, Maryland: University Press of America.
Cartwright, A. (1964). Human relations and hospital care. London: Routledge and Kegan Paul. Chayet, N. L. (1976). Informed consent of the mentally disabled: A failing fiction. Psychiatric Annals,
6, 295-299. Cohen, J., & Cohen, E (1975). Applied regression~correlation analysis for the behavioral sciences.
Hillsdale, New York: Lawrence Erlbaum Associates. Department of Health, Education and Welfare. (1978). Protection of human subjects. Research in-
volving those institutionalized as mentally infirm: Report and recommendations for public com- ment. Federal Register 43 (March 17). Washington, D.C.: U.S. Government Printing Office.
Dyer, A. R. (1982). Informed consent and the nonautonomous person. IRB: A Review of Human Subjects Research, 4, 1-4.
Faden, R. R., and Beauchamp, T. L. (1986). A history and theory of informed consent. New York: Oxford University Press.
Freidson, E. (1970). The profession of medicine. New York: Dodd, Mead, and Co. Fried, C. (1974). Medical experimentation: Personal integrity and social policy. Amsterdam: Elsevier. Garham, J. C. (1975). Some observations on informed consent in non-therapeutic research. Journal of
Medical Ethics 1, 135-145. Glass, E. S. (1970). Restructuring informed consent: Legal therapy for the doctor-patient relation-
ship. Yale Law Journal, 79, 1533. Goidstein, J. (1978). On the right of the institutionalized mentally infirm to consent to or to refuse to
participate as subjects in biomedical or behavioral research. In National Commission for the Protection of Human Subjects in Biomedical and Behavioral Research, Appendix: Research In- volving Those Institutionalized as Mentally Infirm. DHEW Publication No. (OS) 78-0007. Wash- ington, D.C.: U.S. Government Printing Office.
Gorham, R., & Overall, J. (1962). The brief psychiatric rating scale. Psychological Reports, I0, 799-812.
Gray, B. H. (1975). Human subjects in medical experimentation. New York: Wiley-Interscience. Gray, B. H. (1978). Complexities of informed consent. Annals of the American Academy of Political
and Social Science, 437, 37-48. Greenwald, R. A., Ryan, M. K., & Mulvihill, J. E. (Eds.). (1982). Human subjects research: A hand-
book.for institutional review boards. New York: Plenum.
INFORMATION DISCLOSURE 475
Hamilton, M. (1983). On informed consent. British Journal of Psychiatry, 143, 416. Howard, J. M., DeMets, D., & the BHAT Research Group (1981). How informed is informed con-
sent? The BHAT experience. Controlled Clinical Trials, 2, 287-303. tnglefinger, E J. (1972). Informed (but uneducated) consent. New England Journal of Medicine, 288,
465-466. Katz, J. (1984). The silent world of doctor and patient. New York: Free Press. Ketai, R., Minter, R. E., Brandwin, M. A., & Brode, M. (1981). Family influence in the recruitment
of schizophrenic research subjects. American Journal of Psychiatry, 138, 351-354. Laforet, E. G. (1976). The fiction of informed consent. Journal of the American Medical Association,
235, 1579-1585. Lidz, C. W., & Roth, L. H. (1981). The signed form: Informed consent? In J. E Boruch and J. S.
Cecil (Eds.), Solutions to ethical and legal issues in social research. New York: Academic Press. Lidz, C. W., Meisel, A., Zerubavel, E., Carter, M., Sestak, R. M., & Roth, L. H. (1984). Informed
consent: A study of decisionmaking in psychiatry. New York: Guilford Press. Mackin, R. (1982). Some problems in gaining informed consent from psychiatric patients. Emory Law
Journal, 31, 345-374. Matthews, J. J. (1983). The communication process in clinical settings. Social Science and Medicine,
17, 1371-1378. Meisel, A., & Roth, L. H. (1983). Toward an informed discussion of informed consent: A review and
critique of the empirical studies. Arizona Law Review, 25, 265-346. McGrath, K., & Briscoe, R. J. (1981). The role of subject advocate in a community-based medical
research facility. IRB: A Review of Human Subjects Research, 3, 6-7. Miller, R., & WiUner, H. S. (1974). The two-part consent form; A suggestion for promoting free and
informed consent. New England Journal of Medicine, 290, 964-966. Plotkin, R. (1977). Limiting the therapeutic orgy: Mental patients' right to refuse treatment~ North-
western University Law Review, 72, 461-525. President's Commission for the Study of Ethical Problems in Medicine & Biomedical & Behavioral
Research. (1982). Making health care decisions: The ethical and legal implications of informed consent in the patient-practitioner relationship. Vol. 1: Report. Washington, D.C.: U.S. Govern- ment Printing Office.
Pryce, I. G. (1978). Clinical research upon mentally ill subjects who cannot give informed consent. British Journal of Psychiatry, 132, 366-369.
Ramsey, P. (1970). The Patient as Person. New Haven, Connecticut: Yale University Press. Riecken, H. W., & Ravich, R. (1982). Informed consent to biomedical research in Veterans Adminis-
tration hospitals. Journal of the American Medical Association, 248, 344-348. Robertson, J. A. (1982). Taking consent seriously: IRB intervention in the consent process. IRB: A
Review of Human Subjects Research, 4, 1-5. Singer, R. (1977). Consent of the unfree: Medical experimentation and behavior modification in the
closed institution, Part II. Law and Human Behavior, 1, 105-122. Stanley, B. (1981, January). Informed consent & competence: A review of empirical research. Un-
published paper presented at a NIMH workshop, "Empirical Research on Informed Consent with Subjects of Uncertain Competence". Rockville, Maryland.
Stanley, B., & Stanley, M. (1981). Psychiatric research with psychiatric patients: Protecting their autonomy. Comprehensive Psychiatry, 22, 420-425.
Stanley, B., Stanley, M., Lautin, A., Kane, J., & Schwartz, N. (1981). Informed consent and compe- tency in psychiatric research. American Journal of Psychiatry, 138, 669-671.
Stanley, B., Guido, J., Stanley, M., & Shortell, D. (1986). The elderly patient and informed consent: Empirical findings. Journal of the American Medical Association, 246, 1302-1306.
Swazey, J. A. (1978). Protecting the "animal of necessity": Limits to inquiry in clinical investigation. Daedulus, 107, 129-145.
Related Documents