Influence of Baseline Global Longitudinal Strain Measurements on Left Ventricular Functional Outcomes in Children Treated with Anthracycline Chemotherapy by Daniel Yunwen Wang A thesis submitted in conformity with the requirements for the degree of Master of Science Institute of Medical Science University of Toronto © Copyright by Daniel Yunwen Wang 2020

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Influence of Baseline Global Longitudinal Strain Measurements on Left Ventricular Functional Outcomes in
Children Treated with Anthracycline Chemotherapy
by
Daniel Yunwen Wang
A thesis submitted in conformity with the requirements for the degree of Master of Science
Institute of Medical Science University of Toronto
© Copyright by Daniel Yunwen Wang 2020
ii
Influence of Baseline Global Longitudinal Strain Measurements on
Left Ventricular Functional Outcomes in Children Treated with Anthracycline Chemotherapy
by
Daniel Yunwen Wang
Master of Science
Institute of Medical Science University of Toronto
2020
Abstract
Pediatric cancer patients who receive anthracycline chemotherapy are at risk for developing
cardiac dysfunction during and after treatment. Global longitudinal strain (GLS) has been
proposed as a sensitive marker of early myocardial changes in adults. We examined the
significance of a lower baseline GLS in children with cancer. Echocardiograms were performed
at baseline, before each subsequent dose of anthracycline, and 12 months after treatment
completion. A total of 176 pediatric cancer patients were included in our analyses. Patients who
presented with a lower baseline GLS (17.2 ± 1.5%) had improved GLS at 12-months post-
treatment (19.6 ± 2.6%), p=0.004. Overall, no difference in left ventricular systolic function was
observed during and after anthracycline treatment between patients with a lower baseline GLS
compared with age- and cancer diagnosis-matched patients who had higher baseline GLS. These
suggest that lower baseline GLS values should not preclude pediatric cancer patients from
receiving anthracycline chemotherapy.
iii
Acknowledgments
The completion of this thesis would not have been possible without the support and assistance
from many individuals.
First and foremost, I would like to express my sincere gratitude to my supervisor, Dr. Luc
Mertens. Thank you very much for your continuous support of my M.Sc. study over the past two
year. Your immense knowledge in the field of echocardiography was invaluable for the
formulation of my research topic and study objectives. I have learned a great deal through my
project about the applications of echocardiography in the context of cardio-oncology. You have
always been patient with me and your dedication, as well as willingness to support me even
during your busiest times are what motivated me and made this project possible. I would also
like to thank you for sponsoring my conference trip to Chicago to attend the 2018 American
Heart Association Scientific Sessions. It was a truly wonderful learning and networking
experience, a luxury that not many graduate students can have. Additionally, I cannot thank you
enough for taking such a genuine interest in my degree and in my future. To say that you have
inspired me is an understatement. Once again, thank you for accepting me as your graduate
student and providing this truly incredible learning opportunity.
I would also like thank the rest of my thesis committee: Dr. Paul Nathan and Dr. Cedric
Manlhiot. Thank you for the guidance you have provided not just during our PAC meetings but
also through emails and countless hours of discussion. Your insightful comments and
encouragement are what propelled me through my thesis project. Your enthusiasm and
knowledge have significantly contributed to my development as a clinical researcher. Thank you,
Dr. Nathan, for your expertise in childhood cancer and the support you have offered throughout
the past two year. I remember to this day the guidance and suggestions you gave me when I first
started my M.Sc. degree. Thank you, Dr. Manlhiot, for your expertise in biostatistics, which
greatly enhanced my statistical knowledge and improved the overall quality of my project.
My sincere thanks also go to Dr. Steve Fan, who had dedicated countless hours since the
beginning of my project to help me structure and optimize my statistical analyses. Your
willingness to patiently work alongside me and support me through my analyses was more than I
could have asked for. Without your precious support, it would not have been possible to conduct
iv
this research. Likewise, thank you, Emily Somerset, for your expertise and dedication. Several
aspects of this project would not have been possible without your support.
To the PCS2 project managers, Emily Lam, Anne Christie, and Rosemary Wagner, thank you all
for the support, feedback, and encouragement that you have provided throughout the past two
years. Your knowledge of the PCS2 study and its database was an immense asset to my thesis
project. The sole reason as to why I had a dataset to work with for my project was because of
your dedication in coordinating and maintaining the large amount of data collected by the PCS2
investigators.
To Nita Choonsingh and Michela Barbieri, thank you for the many hours you have dedicated, the
countless emails you have answered, and the numerous meetings you have scheduled for me
over the past two years. Nita, I wish you all the happiness with your new family!
I thank everyone on the PCS2 team for their commitment to the project. In particular, I thank Dr.
Jacqueline Wheatley, Dr. Maryam Esmaeilzadeh, Dr. Cameron Slorach, Dr. Wei Hui, Dr. Paul
Kantor, Dr. Seema Mital and Dr. Peter Liu for your input on my conference abstract and
manuscript, as well as your willingness to support and share your knowledge outside of my
thesis committee. Over the past two years, I have learned a lot and acquired many skills, and I
have all of you to thank for that.
Thank you, Canadian Institutes of Health Research, SickKids Research Institute, and Enbridge
for the scholarships that enabled me to perform my graduate research.
Lastly, I would like to extend my profound gratitude to everyone outside of this project that
supported me throughout my M.Sc. journey. I thank my parents for their unfailing support and
continuous encouragement throughout my years of study. I am extremely grateful to my friends
for always being understanding and believing in me, even when I was at my worst. I thank all the
echo fellows that I have met over the past two years for their unparalleled support and
encouragement. I have grown as an individual throughout this experience and am very fortunate
to have had you all by my side during this process. This accomplishment would not have been
achievable without every one of you.
Once again, thank you all for being a part of this chapter of my life.
v
Statement of Contributions
Dr. Luc Mertens contributed immensely to the study design, data analysis plans, and critical
revision of the thesis. In addition, Dr. Mertens’s expertise in the field of echocardiography, as
well as his knowledge of cardiovascular outcomes in cancer patients were indispensable for the
interpretation of the findings. Dr. Mertens’s contributions were unquestionably essential for the
completion of this thesis.
Dr. Paul Nathan offered significant contributions to the design of the study, interpretation of the
data collected, and revision of the thesis. As an oncologist, Dr. Nathan also provided the context
and clinical significance of the study outcomes and findings from an oncological perspective.
Moreover, his expertise with pediatric cancer survivorship was a huge asset for the project.
Dr. Cedric Manlhiot shared his expertise in data analytics and provided invaluable guidance on
cohort selection, statistical analysis, and data interpretation. Dr. Manlhiot also ensured that
adequate statistical tests and models were used to analyze data within the thesis.
Dr. Steve Fan and Emily Somerset, with their expertise in biostatistics, dedicated many hours to
help structure and optimize the statistical models used for the project. Additionally, both Dr. Fan
and Emily S. provided guidance with R coding. Their support was instrumental in addressing
analysis-related challenges as well as successfully meeting the thesis objectives.
Emily Lam, Anne Christie, and Rosemary Wagner assisted with data collection and the
extraction of relevant patient data for the project. In addition, their expertise with the PCS2 study
and database greatly helped with the conception of my Master’s project.
Lastly, funding for this project was generously provided by the Canadian Institutes of Health
Research, SickKids Research Institute, and Enbridge. Thank you.
vi
Table of Contents ACKNOWLEDGMENTS .......................................................................................................... III
STATEMENT OF CONTRIBUTIONS ..................................................................................... V
TABLE OF CONTENTS ........................................................................................................... VI
LIST OF ABBREVIATIONS .................................................................................................... IX
LIST OF FIGURES ..................................................................................................................... X
LIST OF TABLES ...................................................................................................................... XI
LIST OF APPENDICES .......................................................................................................... XII
INTRODUCTION ................................................................................................................ 1
1.1 CHILDHOOD CANCER IN CANADA ................................................................................. 1
1.2 LATE EFFECTS OF CHILDHOOD CANCER SURVIVORSHIP ............................................. 2
1.3 CARDIOVASCULAR OUTCOMES IN CHILDREN WITH CANCER ...................................... 6
1.4 ANTHRACYCLINE CHEMOTHERAPY AND CARDIOTOXICITY ........................................ 9
1.4.1 Pathophysiology of Anthracycline Cardiotoxicity .................................................... 11
1.4.2 Risk Factors for Anthracycline Cardiotoxicity ......................................................... 13
1.4.3 Prevention of Anthracycline Cardiotoxicity ............................................................. 15
1.5 DETECTION OF ANTHRACYCLINE CARDIOTOXICITY .................................................. 17
1.5.1 Current Clinical Practice Guidelines ....................................................................... 17
1.5.2 Definition of Cardiotoxicity ...................................................................................... 18
1.5.3 Global Longitudinal Strain for the Early Detection of Cardiotoxicity ..................... 19
1.5.4 Baseline Global Longitudinal Strain ........................................................................ 22
1.5.5 Other Measures of Cardiotoxicity ............................................................................ 24
1.6 BIOMARKERS FOR THE EARLY DETECTION OF CARDIOTOXICITY ............................. 26
STUDY RATIONALE, OBJECTIVES, AND HYPOTHESES ...................................... 29
2.1 STUDY RATIONALE ....................................................................................................... 29
2.2 STUDY OBJECTIVES ...................................................................................................... 29
2.3 SPECIFIC AIMS .............................................................................................................. 30
vii
2.4 HYPOTHESES ................................................................................................................ 31
METHODOLOGY ............................................................................................................. 33
3.1 STUDY DESIGN OVERVIEW .......................................................................................... 33
3.2 PREVENTING CARDIAC SEQUELAE IN PEDIATRIC CANCER SURVIVORS (PCS2) STUDY
34
3.3 STUDY POPULATION ..................................................................................................... 46
3.4 ECHOCARDIOGRAPHIC STRAIN ASSESSMENT ............................................................. 48
3.5 CARDIAC BIOMARKERS ASSESSMENT ......................................................................... 52
3.6 STATISTICAL ANALYSIS ............................................................................................... 56
RESULTS ............................................................................................................................ 62
4.1 BASELINE CHARACTERISTICS ...................................................................................... 62
4.2 BASELINE GLS IN PEDIATRIC CANCER PATIENTS ...................................................... 69
4.3 BASELINE CARDIAC BIOMARKERS .............................................................................. 81
DISCUSSION ...................................................................................................................... 97
5.1 BASELINE CARDIAC STRAIN IN PEDIATRIC CANCER PATIENTS (OBJECTIVE 1) .......... 99
5.2 CARDIAC OUTCOMES IN PEDIATRIC CANCER PATIENTS WITH LOWER BASELINE GLS
(OBJECTIVE 2) ........................................................................................................................ 102
5.3 CARDIAC BIOMARKERS AND CARDIAC FUNCTION IN PEDIATRIC CANCER PATIENTS
(OBJECTIVE 3) ........................................................................................................................ 106
5.4 STRENGTHS AND LIMITATIONS OF THE STUDY ......................................................... 112
5.5 CONCLUSION .............................................................................................................. 114
5.6 FUTURE DIRECTIONS .................................................................................................. 115
REFERENCES .......................................................................................................................... 117
APPENDICES ........................................................................................................................... 138
APPENDIX I: GUIDELINES FOR CARDIOMYOPATHY SURVEILLANCE .................................... 138
APPENDIX II: ECHOCARDIOGRAPHIC PROTOCOL ................................................................ 141
APPENDIX III: CAUSE OF DEATH ........................................................................................... 143
APPENDIX IV: CORRELATION ANALYSES: BASELINE – END-TREATMENT .......................... 145
APPENDIX V: FIXED EFFECT MODEL ANALYSES .................................................................. 147
APPENDIX VI: CHANGES IN CARDIAC FUNCTION: BASELINE – END-TREATMENT ............. 149
APPENDIX VII: CARDIAC BIOMARKERS REGRESSION ANALYSES ....................................... 152

viii
APPENDIX VIII: GAMLSS Z-SCORE MODEL OUTPUTS ...................................................... 156
ix
List of Abbreviations
ANOVA Analysis of variance
ATP Adenosine triphosphate
BNP Brain natriuretic peptide
CALIPER Canadian Laboratory Initiative on Pediatric Reference Intervals
CBR3 Carbonyl reductase 3
CI Confidence interval
CMR Cardiac magnetic resonance
COG Children’s Oncology Group
CS Circumferential strain
ELISA Enzyme-linked immunosorbent assay
GAMLSS Generalized Additive Models for Location Scale and Shape
GLS Global longitudinal strain
HAS3 Hyaluronan synthase 3
hs-TnT High-sensitivity troponin T
IGF-BP7 Insulin-like growth factor binding protein 7
IQR Interquartile range
LV Left ventricular
LVEDD Left ventricular end-diastolic diameter
LVEF Left ventricular ejection fraction
LVPWT Left ventricular posterior wall thickness
MPO Myeloperoxidase
NT-proBNP N-terminal pro-Brain natriuretic peptide
PCS2 Preventing Cardiac Sequelae in Pediatric Cancer Survivors
ROS Reactive oxygen species
SD Standard deviation
SIGN Scottish Intercollegiate Guidelines Network
SNP Single nucleotide polymorphism
TDR Thickness to dimension ratio
TnT Troponin T
us-TnI Ultrasensitive troponin I
x
List of Figures Figure 1 Timeline of data and specimen acquisition from the Acute Cohort...................... 37 Figure 2 Timeline of data and specimen acquisition from the Survivor Cohort................. 40 Figure 3 Flow chart of patient selection for echocardiographic strain assessment............. 51 Figure 4 Flow chart of patient selection for NT-proBNP assessment................................. 54 Figure 5 Flow chart of patient selection for hs-TnT assessment......................................... 55 Figure 6 Comparison of baseline GLS and CS between patients and healthy controls...... 66 Figure 7 Correlation between GLS at baseline and LVEF/CS at baseline.......................... 70 Figure 8 Correlation between baseline GLS and GLS/LVEF/CS at 12-month follow-up.. 71 Figure 9 Change in cardiac function from baseline to 12-month follow-up....................... 78 Figure 10 Difference of change over time for GLS, LVEF, and CS..................................... 79 Figure 11 Scatterplot of baseline NT-proBNP concentration by age.................................... 83 Figure 12 NT-proBNP levels in CALIPER controls versus patients at baseline and 12-month
follow-up............................................................................................................... 86 Figure 13 Correlation between baseline NT-proBNP and echocardiographic parameters.... 87 Figure 14 Scatterplot of baseline hs-TnT concentration by age............................................ 90 Figure 15 hs-TnT levels in CALIPER controls versus patients at baseline and 12-month
follow-up............................................................................................................... 92 Figure 16 Correlation between baseline hs-TnT and echocardiographic parameters............ 93 Figure 17 Cardiac biomarker z-score values in CALIPER controls versus patients at baseline
and 12-month follow-up........................................................................................ 96
xi
List of Tables Table 1 Eligibility criteria for the Acute Cohort................................................................ 36
Table 2 Eligibility criteria for the Survivor Cohort............................................................ 39 Table 3 Continuous distribution models implemented in the GAMLSS software
package.................................................................................................................. 59 Table 4 Continuous distribution models used for z-score modeling.................................. 61 Table 5 Clinical and echocardiographic characteristics of the study population at
baseline.................................................................................................................. 64 Table 6 Comparison of baseline strain parameters between patients and healthy
controls.................................................................................................................. 65 Table 7 Comparison of baseline cardiac function between cancer diagnosis groups and
healthy controls..................................................................................................... 67 Table 8 Comparison of baseline clinical and echocardiographic characteristics between
included and excluded patients............................................................................. 68 Table 9 Association between baseline GLS and follow-up echocardiographic
parameters............................................................................................................. 73 Table 10 Breakdown of baseline GLS measurements in the low GLS group with
corresponding LVEF and CS for each GLS group............................................... 74 Table 11 Comparison of clinical characteristics in patients with lower GLS (<19%) and
patients with higher GLS (>20%) at baseline....................................................... 75 Table 12 Comparison of echocardiographic characteristics between the low GLS group and
the high GLS group at baseline, end-treatment, and 12-month follow-up............ 77 Table 13 Clinical characteristics of the five patients in the low GLS group who remained
with a reduced GLS at 12-month follow-up.......................................................... 77 Table 14 Difference of change over time (from baseline to 12-month follow-up).............. 79 Table 15 Comparison of clinical characteristics and NT-proBNP levels between patients
with cardiac biomarker data and healthy CALIPER controls............................... 84 Table 16 Number of CALIPER controls and patients at baseline and 12-month follow-up
with abnormal NT-proBNP by age group............................................................. 85 Table 17 Comparison of clinical characteristics and hs-TnT levels between patients (>1
year old) and healthy CALIPER controls (>1 year old)........................................ 91 Table 18 Summary of p values pertaining to correlation analyses between baseline cardiac
biomarker z-scores and echocardiographic parameters of cardiac function......... 96
xii
List of Appendices Appendix I Guidelines for Cardiomyopathy Surveillance......................................... 138 Appendix II Echocardiographic Protocol.................................................................... 141 Appendix III Cause of Death........................................................................................ 143 Appendix IV Correlation Analyses: Baseline – End-Treatment................................... 145 Appendix V Fixed Effect Model Analyses.................................................................. 147 Appendix VI Changes in Cardiac Function: Baseline – End-Treatment...................... 149 Appendix VII Cardiac Biomarkers Regression Analyses.............................................. 152 Appendix VIII GAMLSS Z-Score Model Outputs......................................................... 156
1
Introduction
1.1 Childhood Cancer in Canada
In Canada, childhood cancer represents the leading disease-related cause of death in children past
infancy and is second only to unintentional accidents in overall mortality (Statistics Canada
2019; Ellison and Janz 2015). Each year, close to 910 children between the ages of 0 to 14 years
are diagnosed with cancer and an average of 125 deaths in the pediatric population are related to
malignant neoplasms (Statistics Canada 2019; Ellison and Janz 2015). The highest incidence of
childhood cancer is observed among the youngest infants under one year of age, and nearly half
(47.4%) of all cancer cases in children are diagnosed within the first five years of life (Xie,
Onysko, and Morrison 2018). Males are 20% more likely to be diagnosed with cancer during
their childhood than females, and of all Canadian provinces, Ontario has the highest average
annual age-standardized incidence rate of approximately 170 cases per million children (Xie,
Onysko, and Morrison 2018; Ellison and Janz 2015). Overall, the incidence of childhood cancer
in Canada has been steadily increasing by an average rate of 0.4% per year, a change partially
explained by the increased use of more advanced diagnostic technology and improved cancer
reporting (Xie, Onysko, and Morrison 2018).
Leukemia is the most common type of cancer that occurs in children and accounts for
approximately 32% of all new cancer diagnoses each year in Canada. Tumors originating in the
central nervous system and lymphomas follow in incidence, constituting 19% and 11% of all
new cancer cases respectively (Xie, Onysko, and Morrison 2018). The remainder is comprised of
neuroblastoma (7.8%), soft tissue sarcoma (6.5%), renal tumors (5.2%), and other less common
types of cancer (Xie, Onysko, and Morrison 2018). Altogether, childhood cancer is undeniably
rare, accounting for only less than 1% of the total annual cancer incidence in the Canadian
population (Xie, Onysko, and Morrison 2018). Nevertheless, diagnosis of cancer in children
often has a tremendous lifelong health, psychosocial, and financial impact on both the child and
their family (Canadian Cancer Society/National Cancer Institute of Canada 2008). Special
attention for this distinctive population is warranted to address their unique and complex needs,
as well as to develop and optimize strategies for their long-term care.
2
1.2 Late Effects of Childhood Cancer Survivorship
With the continuous advancements in treatment strategies and supportive care, cancer-specific
mortality rates in children have steadily declined over the last three decades by an average of
2.0% per year (Ellison and Janz 2015). At present, it is estimated that over 83% of all children
diagnosed with cancer will live five or more years beyond their cancer diagnosis and become
long-term survivors (Noone et al. 2018; Nathan, Amir, and Abdel-Qadir 2016). The population
of long-term childhood cancer survivors in the United States in 2013 was in excess of 370,000,
and is expected to approach 500,000 by 2020 (Robison and Hudson 2014). In Canada, there are
currently around 40,000 individuals who have survived beyond five years from their primary
childhood cancer diagnosis (Nathan, Amir, and Abdel-Qadir 2016). Despite the progresses made
to date, there is growing evidence that cancer survivorship does not necessarily translate into full
restoration of health. Instead, a large proportion of childhood cancer survivors is expected to
remain at an increased, lifelong risk for serious adverse complications, secondary to their cancer
or their exposure to curative cancer therapy during childhood (Reulen et al. 2010; Hudson et al.
2013; Robison et al. 2005; Mertens et al. 2001). Such complications that arise as a result of the
disease process, the treatment, or both are broadly referred to as “late effects”, and a myriad of
late effects have been recognized by the medical community. For example, some may be directly
observable due to their impact on physical appearance (e.g. surgical amputation) or because of
their influence on vital physiological functions (e.g. neurocognitive impairment) (Kadan-Lottick
et al. 2010; Y. T. Cheung et al. 2018). There are also other less obvious late effects such as
infertility (Kadan-Lottick et al. 2010; Y. T. Cheung et al. 2018), hypothyroidism (Çağlar et al.
2014), and osteopenia (M. J. Kang and Lim 2013; Nagarajan et al. 2010) where more advanced
medical screening or imaging tests are required to uncover the irregularities.
Treatment-related late effects are extremely common and of particular concern in survivors of
childhood cancer (Robison et al. 2005; Hudson et al. 2013). Among adult survivors of childhood
cancer who had prior exposure to cancer therapy, it is estimated that 95.5% (95% confidence
interval [CI]: 94.8 – 98.6%) will develop at least one chronic health condition by the age of 45
years (Hudson et al. 2013), and 73.4% (95% CI: 69.0 – 77.9%) within 30 years from their cancer
diagnosis (Oeffinger et al. 2006). These late effects of cancer therapy may be comprised of
cardiovascular, pulmonary, renal, or reproductive dysfunction, endocrinopathies, metabolic
disorders, musculoskeletal complications, neurocognitive or neurosensory impairments, or the
3
development of second or subsequent cancers (Armstrong, Stovall, and Robison 2010; Hudson et
al. 2013; Bhakta et al. 2016; Kooijmans et al. 2019). Additionally, 80.5% (95% CI: 73.0 -
86.6%) of all childhood cancer survivors are predicted to develop a severe, disabling, or life-
threatening chronic condition by 45 years of age (Hudson et al. 2013); 42.4% (95% CI: 33.7 –
51.2%) by 30 years following cancer diagnosis (Oeffinger et al. 2006).
Coinciding with the high prevalence of late health effects in childhood cancer survivors is a
greater lifetime risk for hospitalization (Kenborg et al. 2019; Sorensen et al. 2019; Sieswerda et
al. 2016; Brewster et al. 2014; Kirchhoff et al. 2014). In a population-based cohort study that
pooled data from both the Utah Cancer Registry and the Utah Population Database, 2,571
survivors of childhood and adolescent cancer were identified alongside a comparison cohort
consisting of 7,713 age- and sex-matched subjects who did not have cancer (Kirchhoff et al.
2014). During an average follow-up duration of 14 years, the hazard for any hospitalization was
found to be 1.52-times (95% CI: 1.31 – 1.66) higher in the survivor group relative to the
comparison cohort. Survivors were also shown to have a 1.67-fold (95% CI: 1.58 – 1.77)
increase in hospital admission rate. In another longitudinal follow-up study using medical record
linkage, childhood cancer survivors were found to have a 2.2-times (95% CI: 1.9 – 2.5) higher
hospitalization rate relative to the general population (Sieswerda et al. 2016). The increased
hospitalization rates among survivors persisted up to at least 30 years after their initial cancer
diagnosis, with the highest rates observed in survivors who were 5-10 and 20-30 years from their
primary diagnosis. Likewise, the largest inter-Nordic cohort study of childhood cancer survivors
to date, known as the Adult Life after Childhood Cancer in Scandinavia study, identified 4,003
five-year survivors of childhood leukemia, among which 1,490 (37.2%) had experienced at least
one hospitalization during a median follow-up duration of 16 years (range: 5 – 42 years). The
standardized hospitalization rate ratio was determined to be 2.08 (95% CI: 1.96 – 2.20) in
comparison to the general population, and leukemia survivors were shown to have an elevated
risk of hospitalization even at >20 years past their cancer diagnosis (Sorensen et al. 2019).
Findings from a Canadian study of 1157 survivors of childhood cancer further confirmed the
elevated risk of hospitalization in this patient population (Bradley et al. 2010). In that study,
survivors were found to be 4.4-times (95% CI: 3.7 – 5.2) more likely to be admitted to the
hospital at least once. Survivors also had a higher average number of hospital admissions relative
to the general population in British Columbia. Moreover, a detailed examination of
hospitalization records from the same cohort uncovered that the duration of hospital stay is close
4
to 40% longer for childhood cancer survivors compared to those who did not have cancer during
their childhood (Kirchhoff et al. 2014; Bradley et al. 2010).
The burden of childhood cancer survivorship is further highlighted in studies of premature
mortality following cancer therapy. The Childhood Cancer Survivor Study, established in 1994,
represents the largest and most comprehensively characterized epidemiological research cohort
of childhood cancer survivors to date in North America (Robison et al. 2002). It is a self-reported
questionnaire-based interdisciplinary retrospective cohort study by design, and constitutes a total
of 25,664 childhood cancer survivors who received their cancer diagnosis and treatment between
January 1, 1970 and December 31, 1999, alongside 5,059 siblings as comparative controls
(Robison et al. 2009; Childhood Cancer Survivor Study 2017). Early findings from the study
group indicated that survivors of childhood cancer have a 10.8-fold (95% CI: 10.3 – 11.3) excess
in overall mortality risk when compared to the general population (Mertens et al. 2001). Relapse
of the original cancer accounted for the majority (67.4%) of deaths whereas 21.3% were related
to the exposure to cancer treatment (Mertens et al. 2001). More recently, Yeh et al. estimated the
conditional life expectancy of childhood cancer survivors to be only 50.6 years, which translated
to a loss of 10.4 years (17.1%) in lifespan when compared to the general population (Yeh et al.
2010). The risk of excess premature mortality was shown to be especially high amongst
survivors of brain and bone tumors, where the life expectancy was reduced by as much as 17.8
years (28.2%) relative to age-matched populations (Yeh et al. 2010). Additionally, a report from
the National Cancer Institute indicated that on average, 69.3 years of life would be expected to
be lost when a child dies of cancer, compared to only 15.1 life years for adult cancer patients
(National Cancer Institute 2001).
Given the high prevalence and increased awareness of late effects in survivors of childhood
cancer, several clinical practice guidelines, including the “Long-Term Follow-Up Guidelines for
Survivors of Childhood, Adolescent, and Young Adult Cancers” by the Children’s Oncology
Group (COG) (Children’s Oncology Group 2018) and the “Long-term follow-up of survivors of
childhood cancer (SIGN Clinical Guideline 132)” by the Scottish Intercollegiate Guidelines
Network (SIGN) (Gan and Spoudeas 2014) have been published to aid the prevention, early
detection, diagnosis, treatment, follow-up, survivorship, and palliative care of childhood cancer.
A number of multi-disciplinary, multi-center collaborative research projects have also been
established worldwide to facilitate the understanding and prevention of late effects in childhood
5
cancer survivors through the use of real-world evidence. Notable research groups include the
following:
(1) Childhood Cancer Survivor Study – North America (Robison et al. 2002)
(2) St Jude Lifetime Cohort Study – United States (Bhakta et al. 2017)
(3) Childhood, Adolescent, and Young Adult Cancer Survivors Research Program – Canada
(McBride et al. 2010)
(4) British Childhood Cancer Survivor Study – United Kingdom (Fidler, Reulen et al. 2017)
(5) Swiss Childhood Cancer Survivor Study – Switzerland (Kuehni et al. 2011)
(6) Adult Life after Childhood Cancer in Scandinavia Study – Nordic countries (Asdahl et al.
2015)
(7) PanCare Childhood and Adolescent Cancer Survivor Care and Follow-Up Studies –
Across 12 European nations (Grabow et al. 2018)
Altogether, improvement in childhood cancer survival has resulted in a growing need for
research and strategies specifically designed to address the unique late effects experienced by
this distinctive population. Ongoing, systematic follow-up studies of larger cohorts of childhood
cancer survivors well into their adulthood will help elucidate the full spectrum of damage
associated with curative cancer therapy and devise possible interventions that may be integrated
into follow-up plans to mitigate potential late effects. Researchers and primary care providers
alike, play an important role in balancing survival with late effects; all to ensure the best possible
quality of life for long-term survivors of childhood cancer.
6
1.3 Cardiovascular Outcomes in Children with Cancer
Cardiovascular disease including congestive heart failure, cardiomyopathy, coronary artery
disease, stroke, pericardial disease, arrhythmias, valvular disease, and vascular dysfunction,
represents one of the most significant late effects in survivors of childhood cancer. In fact, it is
the leading non-cancer cause of serious morbidity and mortality in long-term survivors of
childhood cancer; third when cancer-related factors such as cancer relapse and second malignant
neoplasms are taken into consideration (Mertens et al. 2001, 2008; Lipshultz, Jacob, et al. 2013;
Nathan, Amir, and Abdel-Qadir 2016; Armenian et al. 2018). Compared to the general
population, childhood cancer survivors experience a seven to ten-fold increase in risk of
premature death from their underlying cardiovascular complications (van der Pal et al. 2012;
Lipshultz, Jacob, et al. 2013; Armenian et al. 2015; Mulrooney et al. 2016; Scholz-Kreisel et al.
2017). In comparison to age-matched controls, survivors are up to 15-times more likely to
develop congestive heart failure, 6-times more likely to develop pericardial disease, and 5-times
more likely to develop myocardial infarction or valvular abnormalities (Oeffinger et al. 2006;
Mulrooney et al. 2009). A preliminary analysis of the European PanCareSurFup cohort of 83,333
five-year survivors of childhood cancer yielded a cardiac late effect incidence rate of 2.6%, given
a median observation time of 16 years (Grabow et al. 2018). The Dutch Childhood Oncology
Group followed 6,615 five-year survivors of childhood cancer and reported a 4.4% (95% CI:
3.4% – 5.5%) cumulative incidence of developing heart failure by 40 years after diagnosis
((Lieke) et al. 2019). In a systematic review on cardiovascular late sequalae in long-term
survivors of childhood cancer, the prevalence of cardiac late effects was found to range from
0.1% to 54% for congestive heart failure, 0.5% to 17.0% for coronary diseases, 0.0% to 19.3%
for stroke, 0.7% to 4.0% for pericardial disease, 0.3% to 12.5% for disorders of the cardiac
conduction system, and 1.2% to 50.0% for valvular dysfunction during a follow-up period of 2.3
to 65.0 years (Scholz-Kreisel et al. 2017). The wide variation in prevalence is a direct result of
the heterogeneity in study design and population used for the 64 publications examined in the
systematic review.
From the Childhood Cancer Survivor Study, the cumulative incidence of reported adverse
cardiac events was found to remain elevated in survivors even after 25 years from their initial
cancer diagnosis (Armstrong et al. 2014; Mulrooney et al. 2009). Cardiovascular risk in general
was shown to be persistent as well as progressive in their cohort of childhood cancer survivors.
7
In the case of congestive heart failure, the risk was shown to gradually escalate over time,
reaching an 11.4-fold (95% CI: 4.7 – 27.3) increased risk relative to sibling controls by the age
of 35 years (Mulrooney et al. 2016; Armstrong et al. 2014). Mertens et al. also showed that the
relative risk of mortality due to cardiovascular complications increases with time (Mertens et al.
2008; Nathan, Amir, and Abdel-Qadir 2016). In specific, by 30 years after cancer diagnosis,
causes other than cancer recurrence (e.g. second malignant neoplasms and cardiovascular
disease) overtake cancer relapse and end up as the main determinants of quality of life as well as
premature mortality in long-term survivors of childhood cancer (Mertens et al. 2008; Armstrong
et al. 2009; Carver et al. 2007). Accordingly, a substantial proportion of childhood cancer
survivors are at risk for late-onset cardiac complications. Unfortunately, cardiac alterations may
also occur during or shortly after completion of cancer treatment, and disease presentation can
vary from minor subclinical abnormalities to fatal ventricular arrhythmias or heart failure
(Bloom et al. 2016; Lipshultz, Jacob, et al. 2013).
There is evidence that suggests cancer itself may be a risk factor and predispose cancer patients
to adverse cardiovascular complications (Giza et al. 2017; Demers et al. 2012). For instance, it is
well known that neoplastic cells are capable of creating inflammatory microenvironments
through the production of pro-inflammatory cytokines and chemokines such as tumor necrosis
factor-α and interleukin-6 (Demers et al. 2012; Chechlinska, Kowalewska, and Nowak 2010).
Such inflammatory microenvironments can damage endothelial linings and promote
microvascular permeability and leakage of pro-coagulating factors as well as low-density lipo-
protein cholesterol particles into the extravascular space and vascular intima respectively (Giza
et al. 2017). The entire inflammatory process can then translate into a pro-atherosclerotic state
and thereby, increasing the risk of coronary artery disease in cancer patients. Additionally,
symptoms of stable angina may also appear due to the restriction of systematic blood flow
caused by the formation of plaques within the vessel lumen. Furthermore, newly formed plaques
from the inflammatory process are generally at high risk of rupture and atherothrombosis, which
altogether, further increase the vulnerability of cancer patients to developing myocardial
infarction (Giza et al. 2017).
More often however, cardiovascular morbidity and mortality in cancer patients are attributed to
cardiotoxic side effects of chemotherapeutic agents or radiation therapies, which were once used
to cure their cancer. The incidence of adverse events affecting the cardiovascular system varies
widely with the class of cancer therapy used and the intensity at which the treatment was given
8
(Giza et al. 2017). Additionally, the route of administration, the interval between cancer
treatments, the cumulative dosage, and the age of the patient during treatment are all important
contributors to the development of cardiac toxicity (Reinbolt et al. 2016). Of the various types of
cancer treatments available today, anthracycline chemotherapy in particular, continues to evoke
considerable interest in both the basic and clinical sciences due to its widespread use in the
oncology setting despite being among the most notorious chemotherapeutic agents that cause
cardiotoxicity in both adult and childhood malignancies (McGowan et al. 2017). Although
observed frequencies differ between studies, it is estimated that as many as 65% of all childhood
cancer survivors who had prior exposure to anthracycline chemotherapy will develop at least
some form of subclinical cardiovascular abnormality within 10 years after treatment (Lipshultz et
al. 1991; Kremer et al. 2002; McGowan et al. 2017).
9
1.4 Anthracycline Chemotherapy and Cardiotoxicity
Anthracyclines, first isolated in the 1960s from Streptomyces peucetius, are among the most
efficacious chemotherapeutic agents available for treating both hematological malignancies and
solid tumors in children and adults. At present, nearly 60% of all pediatric cancer patients are
still treated with anthracycline chemotherapy (Lipshultz, Alvarez, and Scully 2008). Doxorubicin
and daunorubicin were the first anthracyclines to be employed in the treatment of cancer and
remain by far, the most commonly administered variants of anthracyclines in clinical practice
(McGowan et al. 2017). There are also newer analogues such as epirubicin, idarubicin, and
mitoxantrone that have been approved for clinical use. Each analogue has distinct advantages
over doxorubicin or daunorubicin in terms of the volume of distribution, half-life duration, or
lipophilicity, and all have become invaluable alternatives to their forerunners for certain patient
groups and indications (McGowan et al. 2017; Simunek et al. 2009).
Despite its extensive use and excellent anti-tumor efficacy, one major drawback of anthracycline
chemotherapy is its dose-dependent cardiotoxic profile, which has the potential to progress into
dilated cardiomyopathy and systolic heart failure (Lipshultz, Jacob, et al. 2013). A cross-
sectional study from the St Jude Lifetime Cohort of 1,853 adult survivors of childhood cancer
found the risk of developing cardiomyopathy to be 2.7-times (95% CI: 1.1 – 6.9) higher among
patients who had received a cumulative anthracycline dose of greater than 250 mg/m2 than those
who had no exposure to anthracycline treatment (Mulrooney et al. 2016). In a retrospective
examination of 4,018 patient records, the cumulative incidence of heart failure was determined to
be 3%, 7%, and 18% in patients who received a cumulative anthracycline dose of 400, 550, and
700 mg/m2 respectively (Von Hoff et al. 1979). Steinherz et al. evaluated echocardiograms from
201 survivors of pediatric malignancies and reported subclinical cardiac dysfunction in 11% of
patients who received cumulative anthracycline doses of <400 mg/m2, increasing to 23% at 400
to 599 mg/m2, 47% at 600 to 799 mg/m2, and to 100% at ³800 mg/m2 (Steinherz et al. 1991).
Similarly, in a long-term follow-up study of cardiac function in 601 five-year survivors of
childhood cancer, those who received 151 to 300 mg/m2, 301 to 450 mg/m2, and >450 mg/m2 of
anthracycline were found to have a 7.0 (95% CI: 1.5 – 10.0), 7.8 (95% CI: 2.8 – 21.3), and 10.6
(95% CI: 3.3 – 33.4) fold increase in risk of reduced systolic function respectively, relative to
children who only received 1 to 150 mg/m2 of anthracycline chemotherapy (van der Pal et al.
10
2010b). Furthermore, in another retrospective analysis of three trials comprising of 630 patients
with breast and lung cancer who were treated with doxorubicin, the incidence of clinical heart
failure increased exponentially from 5% among those who received a cumulative dose of 400
mg/m2 to 48% for patients who received 700 mg/m2 (Swain, Whaley, and Ewer 2003).
Interestingly, data from the Childhood Cancer Survivor Study had described a trend towards an
increased risk of asymptomatic cardiac abnormalities even among pediatric cancer patients who
were exposed to as little as 100 mg/m2 of doxorubicin (Hudson et al. 2007). This finding was
supported by a more recent cross-sectional study of 91 childhood cancer survivors, where 25
(27.5%) patients developed subclinical abnormalities in left ventricular (LV) structure, despite
being treated with very low doses of anthracycline chemotherapy (mean cumulative dose: 59 ±
13 mg/m2) (Leger et al. 2015). Similarly, in a multi-center study of over 3,000 adult breast
cancer patients, symptomatic heart failure occurred in 1.7% to 2.1% of five-year survivors who
had received reportedly safe sub-threshold cumulative doses of anthracycline between 240 and
360 mg/m2 (Trudeau et al. 2005). Likewise, in a cohort study of lymphoma patients previously
treated with doxorubicin, 4% of patients who received moderate anthracycline doses of 500 to
550 mg/m2 later developed congestive heart failure. Occult ventricular dysfunctions were also
evident in patients who received lower doses of anthracyclines (Hequet et al. 2004). Thus, based
on these observations, it is currently believed that no completely safe dose of anthracyclines
exists, whether it be in children or the adult population.
Anthracycline cardiotoxicity is generally categorized into three distinct types based on the timing
of onset of signs or symptoms following treatment exposure: acute, early-onset, or late-onset
(Lipshultz, Jacob, et al. 2013; Adams and Lipshultz 2005). Acute forms of cardiac toxicity
appear within the first week after anthracycline administration and are often temporary as well as
reversible upon discontinuation of treatment. Less than 1% of children treated with anthracycline
chemotherapy are estimated to develop this type of cardiotoxicity. Toxicities may present as a
transient depression of myocardial contractility or some form of electrophysiological
abnormality. In rare circumstances, they may also result in fatal arrhythmias, a pericarditis-
myocarditis syndrome, or fatal acute left ventricular dysfunction (Lipshultz et al. 2015). Despite
being relatively uncommon, patients who are diagnosed with cardiac abnormalities during or
shortly after completion of chemotherapy are often at greatest risk for subsequent long-term
cardiotoxicity (Lipshultz et al. 2015; Lipshultz, Jacob, et al. 2013).
11
Early-onset cardiotoxicity refers to cardiac abnormalities that appear after one week and within
one year of completing anthracycline chemotherapy. Depression in contractility and dilated
cardiomyopathy are examples of this type of cardiotoxicity. Unlike acute cardiotoxicity, early-
onset cardiotoxicity may persist even after the discontinuation of anthracycline treatment. In
some cases, it may also be progressive and lead to pericardial effusion or overt heart failure
(Loar et al. 2018; Adams and Lipshultz 2005). The incidence of early-onset cardiotoxicity is
slightly higher than that of acute cardiotoxicity. In a cohort study of 115 children with acute
lymphoblastic leukemia, congestive heart failure was diagnosed in 11 patients (9.6%), all of
whom developed within one year of treatment with doxorubicin (Lipshultz et al. 1991). More
recently, Cardinale et al. assessed anthracycline-related cardiotoxicity in terms of left ventricular
ejection fraction (LVEF) and reported an incidence of cardiotoxicity of 9%, with 98% of cases
displaying abnormal changes in cardiac function within the first year after chemotherapy
(Cardinale et al. 2015). The median time from the last cycle of anthracycline chemotherapy to
the development of early-onset cardiotoxicity was determined to be 3.5 months.
Late-onset cardiotoxicity refers to cardiac complications that appear after one year post-
anthracycline chemotherapy completion. The incidence ranges widely from 5% to 65% and can
remain asymptomatic for more than two decades after treatment completion (Mulrooney et al.
2009; Pein et al. 2004; Steinherz et al. 1991; Moke et al. 2018). It is progressive in nature where
a continuing loss of functional cardiomyocytes leads to an increase in LV afterload alongside a
reduction in LV systolic function. With further cardiac deterioration, this type of cardiotoxicity
may also result in heart failure or death (Lipshultz et al. 2015). The prognosis is generally poor
in children who develop heart failure after anthracycline exposure, with five-year overall
survival rates dropping below 50% (Felker et al. 2000; Ehrhardt, Fulbright, and Armenian 2016).
1.4.1 Pathophysiology of Anthracycline Cardiotoxicity
Cardiotoxicity associated with anthracycline exposure is often characterized by phenotypical and
functional changes in key cardiac cells such as cardiomyocytes, endothelial cells, and fibroblasts,
as well as cardiac and endothelial progenitor cells (Nebigil and Désaubry 2018). Early in the
natural history of anthracycline-induced cardiotoxicity, myocardial biopsy specimens collected
12
from cancer patients treated with anthracyclines frequently reveal an acute loss of myocytes
(Trachtenberg et al. 2011). Rat studies of cardiac responses to anthracycline exposure have
similarly shown markedly increased expressions of several apoptotic markers shortly after
infusion of low doses of doxorubicin (Arola et al. 2000; Bulten et al. 2019). At the same time,
myofibrillar disarray and mitochondrial deterioration may be observed in heart tissues shortly
after exposure to anthracycline chemotherapy (Nebigil and Désaubry 2018). The continuing loss
of functional myocytes eventually leads to progressive myocardial wall thinning and increased
wall stress. Several compensatory pathways including the activation of adrenergic pathways and
release of growth factors are employed to counter these subclinical cardiac alterations; however,
the consequences often include progressive cardiac remodeling, dilatation, as well as fibrosis.
Late cardiac dysfunction including overt systolic dysfunction and congestive heart failure ensue
when the reserve capacity for compensatory activity in the heart is exceeded.
To date, the exact molecular mechanism by which cardiotoxicity arises from anthracycline
exposure remains inconclusive, though several interconnected modes of action have been
proposed (McGowan et al. 2017). The former hypothesis involves the production of reactive
oxygen species (ROS) and consequent oxidative stress as major contributors to myocardial injury
(Tokarska-Schlattner et al. 2006). Anthracyclines possess a quinone moiety that is prone to
univalent reduction by cellular oxido-reductases (McGowan et al. 2017). Given the high oxygen
metabolism in myocardial cells, anthracyclines can readily undergo repeated cycles of redox
reactions in the mitochondria and generate ROS in the form of superoxide anions during the
process (Simunek et al. 2009). In addition, anthracyclines can complex with cellular iron and
catalyze a Fenton reaction, which further increases the amount of ROS within the cardiomyocyte
(Link et al. 1996). It is believed that cardiomyocytes are particularly susceptible to ROS in part
due to the low concentration of free radical scavenger molecules within heart tissues (Kwok and
Richardson 2000). Accumulation of ROS within cardiomyocytes causes oxidative stress through
lipid peroxidation and alteration of mitochondrial membrane permeability as well as function.
Increased oxidative damage can ultimately trigger the activation of caspase 9 and caspase 3,
leading to the release of cytochrome c into the cytosol (Volkova and Russell 3rd 2011). It can
also stimulate the mitogen-activated protein kinase pathway and the stress-activated protein
kinase pathway, both of which are involved in the modulation of myocyte apoptosis (Senkus and
Jassem 2011).
13
Several studies have suggested that the interference with DNA topoisomerase II may also be a
possible mechanism by which anthracycline-mediated cardiotoxicity occurs (Mordente et al.
2017). DNA topoisomerases play an important role during normal DNA transcription and
replication by inducing temporary single or double-stranded breaks to regulate the over- or
underwinding of DNA strands (McGowan et al. 2017). Two isozymes of topoisomerase exist:
topoisomerase 2α, which is widely expressed in rapidly dividing cells and topoisomerase 2β, a
variant more abundant in quiescent cells like cardiomyocytes (Vejpongsa and Yeh 2014). In
cardiomyocytes following anthracycline exposure, anthracyclines can intercalate DNA and form
stable ternary complexes with topoisomerase 2β. These complexes interfere with the normal
function of topoisomerase 2β, induce permanent double-stranded breaks in DNA strands, inhibit
normal DNA replication and thereby, trigger myocyte apoptosis (Tewey et al. 1984). In addition,
anthracycline combined with topoisomerase 2β may suppress peroxisome proliferator-activated
receptor activity, leading to dysregulation of oxidative metabolism and mitochondrial
dysfunction, and ultimately increased myocardial cell apoptosis (Finck and Kelly 2007). In
support of this proposed mechanism, in vitro studies have proven that topoisomerase 2β is
essential for the binding of doxorubicin to DNA (Tewey et al. 1984). Topoisomerase 2β-
knockout mice have also been shown to be protected against DNA damage following
doxorubicin administration (Lyu et al. 2007).
Other proposed mechanisms of anthracycline-induced cardiotoxicity include transcriptional
changes in intracellular adenosine triphosphate (ATP) (Lipshultz, Jacob, et al. 2013),
interference with the signaling cascade of growth factor neuregulin-1 and its associated tyrosine
kinase receptors ErbB2 and ErbB4 (Wadugu and Kuhn 2012), and disruption of the sarcomeric
protein, titin, leading to myofibril instability and diastolic dysfunction (Crone et al. 2002).
1.4.2 Risk Factors for Anthracycline Cardiotoxicity
Cumulative anthracycline dose is by far, the strongest predictor of subsequent heart failure risk
(Von Hoff et al. 1979; Steinherz et al. 1991; Swain, Whaley, and Ewer 2003). Several other
factors that increase the risk of cardiotoxicity following anthracycline chemotherapy have been
identified and are summarized by a number of review articles (Nathan, Amir, and Abdel-Qadir
2016; Lipshultz et al. 2015; Franco and Lipshultz 2015). In brief, female sex (Lipshultz et al.
14
1995), younger age (<1 year old) at treatment (van der Pal et al. 2010a), longer follow-up
duration after treatment (Lipshultz et al. 2005), African American ancestry (Krischer et al. 1997),
and trisomy 21 (Krischer et al. 1997) are all associated with an increased risk of cardiac toxicity
during or after anthracycline treatment (Nathan, Amir, and Abdel-Qadir 2016; Lipshultz et al.
2015). Concomitant radiation therapy is also a significant risk factor, where a cumulative
radiation dose of >30 Gy directed at the heart can increase the risk of cardiovascular disease and
mortality by as much as 37 folds (van der Pal et al. 2010a; Travis et al. 2012). Concomitant
treatment with cyclophosphamide, cytarabine, cisplatin, and ifosfamide may be associated with a
greater risk of cardiotoxicity (Lipshultz, Jacob, et al. 2013). Additionally, the presence of pre-
existing cardiovascular risk factors and comorbidities such as hypertension, hyperlipidemia,
diabetes, and renal dysfunction have been linked to an increased cardiovascular risk following
anthracycline treatment, though the same comorbidities are seldom observed in pediatric cancer
patients (Lipshultz et al. 2015). Furthermore, traditional cardiovascular risk factors including
smoking, consumption of alcohol, and physical inactivity have been implicated as important risk
factors in the context of anthracycline cardiotoxicity (Lipshultz et al. 2015; Landy et al. 2012).
Certain genetic factors may also confer individual susceptibility to cardiotoxicity following
anthracycline chemotherapy. For instance, children who are homozygous for the G allele at the
V244M position of the carbonyl reductase 3 (CBR3) gene have been found to be at a 5.5-fold
(95% CI: 1.8 – 16.6) increased risk of cardiomyopathy, following exposure to <250 mg/m2
cumulative anthracycline doses (Blanco et al. 2012). Similarly, Wang et al. discovered the
hyaluronan synthase 3 (HAS3) rs2232228 AA genotype to be associated with an 8.9-fold (95%
CI: 2.1 – 37.5) increased risk of cardiomyopathy in anthracycline-treated individuals, relative to
those with the GG genotype (Wang et al. 2014). Furthermore, a significant association between
the development of cardiotoxicity and the presence of the rs10836235 CC homozygous variant
of the catalase gene has been reported (Rajic et al. 2009). A coding variant in RARG (rs2229774,
p.Ser427Leu) has also been linked to a 4.7-fold (95% CI: 2.7 – 8.3) increase in anthracycline-
induced cardiotoxicity in children with cancer (Aminkeng et al. 2015). On the basis of evidence
supporting the involvement of anthracycline-iron complexes in the pathophysiology of
anthracycline-induced cardiotoxicity, conditions that interfere with tissue iron metabolism were
also anticipated to predispose cancer patients to cardiovascular abnormalities. Indeed, in a study
of 184 patients with high-risk acute lymphoblastic leukemia, Lipshultz et al. found that
mutations in the hemochromatosis gene, HFE, were associated with doxorubicin-induced
myocardial injury (Lipshultz, Lipsitz, et al. 2013). In specific, carriers of the HFE C282Y gene
15
mutation were 9.2-times (95% CI: 1.1 – 76.5) more likely to develop cardiotoxicity relative to
noncarriers. Overall, there are numerous studies that suggest a genetic predisposition in the risk
of anthracycline-related cardiotoxicity. However, the contribution of these genetic factors to risk
susceptibility in pediatric cancer patients ultimately remains inconclusive as conflicting findings
are published in the current literature (Reinbolt et al. 2016; Blanco et al. 2008).
1.4.3 Prevention of Anthracycline Cardiotoxicity
Dexrazoxane is an iron chelator and an important cardioprotectant in the context of anthracycline
cardiotoxicity. It acts by reducing the formation of anthracycline-iron complexes and thereby
limiting ROS production and consequent tissue damage (Lipshultz 1996). The cardioprotective
effects of dexrazoxane have been investigated by various groups. In one study by the Dana-
Farber Cancer Institute Acute Lymphoblastic Leukemia Consortium, the effectiveness of
dexrazoxane as a cardioprotectant was assessed in 206 children with acute lymphoblastic
leukemia (Lipshultz 1996). Elevation of cardiac troponin T, an accurate surrogate for acute
myocardial damage in children, following doxorubicin treatment was detected in fewer patients
(21%) who received concomitant dexrazoxane compared to 50% of patients who were treated
with doxorubicin alone (p<0.001). A long-term follow-up study of 134 of the 206 children
revealed a long-lasting cardioprotective effect of dexrazoxane, with no detectable compromise in
overall doxorubicin efficacy (Lipshultz et al. 2010). Choi et al. similarly reported significantly
fewer cardiac events (27.7% versus 52.4%) and cases of severe congestive heart failure (6.4%
versus 14.3%) in children with solid tumors who received dexrazoxane than those who did not
(Choi et al. 2010). Dexrazoxane also improved the five-year cardiac event free survival rate
(69.2% versus 45.8%, p=0.04). In a systematic review of 26 publications on the risk of
cardiotoxicity associated with dexrazoxane in children treated with anthracycline chemotherapy,
dexrazoxane use was associated with improvements in echocardiographic measures of cardiac
function such as ejection fraction, shortening fraction z-score, and left ventricular thickness-to-
dimension ratio. The risk of clinical or subclinical cardiotoxicity was also found to be reduced by
approximately 60% in children who received concomitant dexrazoxane treatment (Shaikh et al.
2016).
16
Infusion protocols may influence subsequent cardiotoxicity. The use of lower cumulative doses
of anthracyclines is expectedly, protective against subsequent anthracycline cardiotoxicity
(Lipshultz et al. 2015). In adult cancer patients, continuous infusion of anthracycline is preferred
over bolus administration. An early study of 51 adult cancer patients who received anthracycline
chemotherapy on different infusion schedules demonstrated lower levels of cardiac injury from
cardiac biopsy among patients who were given a continuous infusion compared to those who
received the standard bolus dose (Legha et al. 1982). This finding was supported by a recent in
vivo study where healthy rats were injected intraperitoneally with epirubicin, either as a bolus
dose or slowly infused via micro osmotic pumps (Yang et al. 2017). Histopathology revealed less
eosinophilic enhancement, interstitial hemorrhage, and necrotizing muscle atrophy, and thereby,
less cardiotoxicity in the slow infusion group versus the bolus group, without any compromise to
the overall antitumor efficacy of epirubicin. Nevertheless, the same has not been demonstrated in
the pediatric population. In a multi-center randomized trial of 204 children with high-risk acute
lymphoblastic leukemia, continuous infusion of doxorubicin did not improve the ten-year event-
free survival (83% versus 78%, p=0.24), nor did it offer additional cardioprotection over bolus
infusion (Lipshultz, Miller, Lipsitz, et al. 2012). Due to the lack of conclusive evidence, some
researchers even oppose the continuous infusion of anthracycline in children as it may actually
increase the risk of thromboembolic events and mucositis, despite offering negligible benefits in
terms of cardioprotection (Lipshultz et al. 2015).
The use of β-blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers,
and statins have also been investigated as potential options for the prophylaxis and treatment of
anthracycline cardiotoxicity (Gulati et al. 2016; Kaya et al. 2013; Kalay et al. 2006; Henriksen
2018). However, the full extent of protection offered by these treatments remain to be
determined, especially in the pediatric population. Ongoing randomized trials including the
ICOS-ONE study (NCT01968200), PROACT study (NCT03265574), and the Cardiac CARE
study (ISRCTN24439460) aim to address this gap in knowledge in the near future.
17
1.5 Detection of Anthracycline Cardiotoxicity
Echocardiography serves as the modality of choice for detecting and monitoring cardiotoxicity in
survivors of childhood cancer because of its widespread availability, non-invasive nature and
cost-effectiveness (Rosa et al. 2016; Armenian et al. 2015). It also offers the advantage of not
exposing patients to unnecessary radiation as with radionuclide multigated blood pool imaging
scans (Henriksen 2018). Assessment of cardiac function using echocardiography enables
clinicians to gain insight into not only the structural abnormalities of the heart, but also regional
as well as global malfunctions that may occur in survivors as a result of their exposure to
cardiotoxic chemotherapy. Early detection of subclinical ventricular dysfunction by means of
echocardiography can help aid the identification of at-risk pediatric patients and allow for pre-
emptive modification of cancer therapy to mitigate further cardiac injury as well as reduce the
risk of developing late cardiac events.
1.5.1 Current Clinical Practice Guidelines
A recent consensus report from the International Late Effects of Childhood Cancer Guideline
Harmonization Group strongly recommended the use of detailed two-dimensional
echocardiography as the primary surveillance modality for monitoring cardiac function in
survivors of childhood cancer who had exposure to anthracycline chemotherapy (Armenian et al.
2015). Appendix I presents a summary of the guideline recommendations. In brief, pediatric
patients who received high doses of anthracycline (³250 mg/m2) are recommended to have an
echocardiogram performed within 2 years after completion of treatment, 5 years after cancer
diagnosis, and every 5 years thereafter. The frequency of surveillance are modified according to
several factors including the cumulative anthracycline dose received, concomitant exposure to
mediastinal radiation therapy, or pregnancy (Armenian et al. 2015). A European Society of
Cardiology 2016 Position Paper along with the 2016 American Society of Clinical Oncology
Clinical Practice Guideline both advised the use of echocardiography to monitor heart function
in cancer patients before, during, and after anthracycline treatment to facilitate the early
detection of changes in cardiac function (Zamorano et al. 2016). The Children’s Oncology Group
18
long-term follow-up guidelines recently modified their guidelines and eliminated the need for a
one-year post-treatment screening echocardiogram in high-risk patients following anthracycline
chemotherapy (Children’s Oncology Group 2013, 2018). Instead, all patients who received ³250
mg/m2 of anthracycline are advised to undergo echocardiographic screening every two years
after treatment. Those who were treated with less than 250 mg/m2 of anthracycline are advised to
be screened every two years if they also received ³15 Gy of chest radiation; every five years
otherwise (Children’s Oncology Group 2018). At present, there are no published, or agreed-
upon, guidelines for the frequency of echocardiographic screening to be performed in pediatric
cancer patients during their chemotherapy treatment.
1.5.2 Definition of Cardiotoxicity
Cardiac toxicity is traditionally described based on the clinical development of congestive heart
failure or on the evidence of a serial decline in left ventricular ejection fraction (LVEF) (Biasillo,
Cipolla, and Cardinale 2017). A reduction in LVEF by more than 10% from baseline to a final
value of less than 55% was once regarded as the most widely accepted definition of
chemotherapy-related cardiac toxicity (Khouri et al. 2012). Currently, an Expert Consensus
Statement from the American Society of Echocardiography, in collaboration with the European
Association of Cardiovascular Imaging defines cardiotoxicity in adult patients during and after
cancer therapy as a >10% reduction in LVEF from baseline to a value of less than 53% (Plana et
al. 2014). A definition for cardiotoxicity specific to the pediatric cancer population has not been
proposed. Rather, the same values from the adult data are often extended to the pediatric
population to define cardiotoxicity.
Despite the given definitions, the use of LVEF as the sole determinant of cardiotoxicity in cancer
patients is increasingly being recognized as inadequate. There are several inherent limitations to
monitoring cardiac function based on LVEF assessment alone. First, the measurement of LVEF
is load dependent and influenced by changes in both preload and afterload (Cikes and Solomon
2015). This is especially problematic in cancer patients as they may receive treatments (e.g.
cyclophosphamide) or experience side effects (e.g. vomiting or diarrhea), all of which may
significantly affect loading conditions (Biasillo, Cipolla, and Cardinale 2017). Second, poor
19
image quality and inadequate operator expertise can hinder the proper manual delineation of
endocardial borders, resulting in a considerable loss of reproducibility. In a study of 56 adult
patients with breast cancer, the minimum detectable change in LVEF by the same observer was
found to be 10% (Thavendiranathan et al. 2013). Between different observers who followed the
same procedures for measuring LVEF, the lower limit of detectable change in LVEF increased
up to 13%. Consequently, LVEF assessment may lack the specificity to detect subtle changes
(<10%) in left ventricular function, representing a significant limitation for cancer patients as
small changes in ventricular function may have important implications on their subsequent
treatment approaches. Third, subclinical myocardial impairments including myocyte loss and
interstitial fibrosis frequently occur in the presence of a preserved LVEF (Ewer et al. 1984).
Therefore, a reduction in LVEF is likely reflective of late-stage cardiac dysfunction, at which a
substantial amount of cardiac reserve has been exhausted and the potential for the heart to fully
recover from the underlying cardiac damage has been diminished.
1.5.3 Global Longitudinal Strain for the Early Detection of Cardiotoxicity
In light of the shortcomings of LVEF assessment, there is growing interest in the use of
myocardial strain imaging by two-dimensional speckle tracking echocardiography for the early
detection of subclinical myocardial dysfunction (Cheng et al. 2013). This method directly
evaluates the deformation of myocardial segments during systole and thus, is minimally affected
by changes in ventricular loading conditions (Çetin et al. 2018). It is also independent on the
angle of insonation and exhibits high reproducibility (Loar et al. 2018). An examination of
myocardial strain indices in 25 pediatric patients who received anthracycline chemotherapy
found the intra- and interobserver variability for strain measures to be less than 5% (Pignatelli et
al. 2015). Likewise, in a prospective cohort study of 86 patients who underwent anthracycline
chemotherapy, the intra-class coefficient and the corresponding inter-observer intraclass
coefficient for strain measurements were determined to be 0.96 (95% CI: 0.95 – 0.97) and 0.93
(95% CI: 0.91 – 0.94) respectively, representing an excellent agreement within and between
observers (Charbonnel et al. 2017). One key limitation of strain imaging is the intervendor
variability (Amzulescu et al. 2019). Therefore, consistency in investigatory procedures becomes
20
especially important when performing longitudinal evaluations in patients using strain
parameters.
In adults, a reduction in global longitudinal strain (GLS) has been shown to be a significant,
independent predictor of subsequent cardiac mortality and morbidity (Biering-Sørensen et al.
2017). Additionally, GLS have been proposed as a more sensitive marker for subtle, early
abnormalities in LV myocardial performance compared to the conventional LVEF, in adult
cancer patients who undergo chemotherapy (Kalam, Otahal, and Marwick 2014; Laufer-Perl et
al. 2018).
An early two-dimensional myocardial strain imaging study of 52 women (age: 49 ± 9 years) with
histologically confirmed breast cancer reported a significant reduction in absolute GLS from
17.8 ± 2.1% at baseline to 16.3 ± 2.0% one week after completion of anthracycline
chemotherapy, p<0.01 (Stoodley et al. 2011). Close to 50% of those patients displayed a
reduction in GLS of >10% from baseline, while no subject had a clinically significant reduction
in LVEF of ³10% after treatment. Kang et al. obtained echocardiograms at baseline and 1 day
after completion of chemotherapy in 67 patients with large B-cell non-Hodgkin lymphoma and
found a significant reduction in GLS (18.3 ± 1.9% to 16.2 ± 1.9%, p<0.01) despite normal LVEF
at both time points (Y. Kang et al. 2013). Similarly, in a study where cardiac function was
assessed by three-dimensional strain imaging before, and at 12 and 36 weeks after anthracycline
chemotherapy, a significant decrease (10.1% ± 6.3%) in GLS from baseline was detected at 12-
week follow-up (Mornos et al. 2014). No concurrent deterioration in LVEF was observed. In a
multiple logistic regression analysis, the change in GLS from baseline to 12-week follow-up was
indicated as the only independent predictor of future anthracycline-related cardiac toxicity (odds
ratio: 1.09, 95% CI: 0.06 – 2.25). Furthermore, the predictive value of GLS was confirmed by
Sawaya et al. in 43 HER-2-overexpressing breast cancer patients treated with anthracyclines or
trastuzumab (Sawaya et al. 2011). A >10% decrease in longitudinal strain between baseline and
3 months post-treatment was found to be predictive of subsequent declines in LVEF. The same
group also reported in a study of 81 women with breast cancer, treated with anthracyclines
followed by taxanes and trastuzumab, that 53% of patients with a GLS of <19% at anthracycline
treatment completion developed cardiotoxicity during follow-up (Sawaya et al. 2012). In
contrast, only 13% of patients who had GLS ≥19% developed subsequent cardiotoxicity. A 10%
decrease in GLS from baseline to end of anthracycline treatment, along with GLS measured at
treatment completion were found to be strong independent predictor of later-onset cardiotoxicity
21
defined by a reduction in LVEF (both p<0.05). Likewise, Negishi et al. reported that a relative
reduction in GLS by 11% between baseline and 6 months after trastuzumab treatment was
strongly associated with a >10% decrease in LVEF at the 12-month follow-up study visit
(Negishi et al. 2013). More recently, in a prospective, observational study conducted by Gripp et
al., cardiac function was monitored every three months in a cohort of 49 women diagnosed with
breast cancer who underwent anthracycline and/or trastuzumab therapy (Gripp et al. 2018). Five
patients (10%) developed cardiotoxicity during follow-up and GLS obtained during the third
month of follow-up was the only parameter independently associated with the event (Hazard
Ratio: 2.77, 95% CI: 1.39 – 5.54, p=0.004). Further analysis revealed an absolute GLS value of
16.6% to have predictive value for subsequent cardiotoxicity with a sensitivity of 80% and a
specificity of 95%. A 14% reduction in GLS was also shown to predict future cardiotoxicity with
a sensitivity and specific of 80% and 99% respectively. In another study of 61 female breast
cancer patients, 18 patients (29.5%) developed cardiomyopathy during a follow-up period of 12
months (El-Sherbeny, Sabry, and Sharbay 2019). A significant difference in GLS between those
who developed cardiomyopathy and those who did not was detected at the 3-month follow-up
study visit, whereas significant changes in LVEF were not observed until the 6-month follow-up.
In a receiver operating characteristic curve analysis, an absolute GLS value of 18% at 3 months
after trastuzumab treatment was found to be an optimal cut-off for the prediction of subsequent
cardiotoxicity. Given the growing evidence provided above, current guidelines by the American
Society of Echocardiography, the European Association of Cardiovascular Imaging, and the
American Society of Clinical Oncology all endorse the use of GLS in adult cancer patients to
facilitate the detection of subclinical cardiac dysfunction (Plana et al. 2014; Armenian et al.
2017).
In contrast, recommendations pertaining to the use of GLS in the pediatric cancer population is
lacking, although similar changes in GLS preceding subsequent declines in LVEF have also been
reported. For instance, in a prospective study of 19 children receiving anthracycline
chemotherapy, a significant decrease in GLS from baseline was detected 4 months later, whereas
changes in LVEF were not observed until 8 months post-baseline (Poterucha et al. 2012).
Findings from the St. Jude Lifetime Cohort study similarly showed that during a median follow-
up of 23 years, one third of survivors presented with abnormal GLS while only 5.8% had
evidence of reduced LVEF (Armstrong et al. 2015). Yu et al. performed two-dimensional
speckle tracking echocardiography in 134 adult survivors of childhood, adolescent, and young
adult cancer treated with anthracycline and reported abnormal GLS of ≤16% in 31 patients
22
(21.3%), a significantly higher prevalence than those who had abnormal LVEF <55% (n=8,
6.0%) (Yu et al. 2016). In a Norwegian population-based study, GLS in long-term adult
survivors of childhood lymphoma and acute lymphoblastic leukemia was examined and
compared to controls without known hypertension, diabetes, or cardiovascular disease
(Christiansen et al. 2016). Absolute GLS was significantly lower in survivors than in controls
(19.0 ± 2.2% versus 21.4 ± 2.0%, p<0.001) and impaired LV systolic function by GLS was
demonstrated in 53 survivors (28%) who all had normal LVEF. Reduction in GLS was also
found to be associated with high cumulative anthracycline doses. Çetin et al. compared cardiac
function between 45 childhood cancer survivors treated with anthracycline and 38 healthy
controls and found a significantly reduced GLS in the patient group (21.3 ± 3.2% versus 23.9 ±
2.9%, p=0.012) (Çetin et al. 2018). LVEF was normal in both groups. Altogether, several studies
suggest that GLS is also a robust and sensitive parameter for the early detection of subtle
abnormalities in LV myocardial performance in children. However, the prognostic value of
abnormal GLS among pediatric cancer patients ultimately remains undetermined.
Based on a systematic review on the use of myocardial strain imaging in cancer patients during
and after chemotherapy, a 10% to 15% decrease in peak LV systolic GLS during therapy relative
to baseline is currently considered to be of clinical significance and have a high prognostic value
for predicting future major adverse cardiac events prior to the decline in global LVEF
(Thavendiranathan et al. 2014). A meta-analysis of 28 datasets also suggested that a GLS of
19.7% (95% CI: 18.9% – 20.4%) is normal in adults (Yingchoncharoen et al. 2013). In children,
a systematic review and meta-analysis of 43 data sets concluded that a normal GLS is around
20.3% (95% CI: 19.4% – 21.1%) when a GE equipment is used; 20.5% (95% CI: 20.1% –
21.8%) when Philips equipment and software are used (Levy et al. 2016). Another meta-analysis
of 28 pediatric studies reported a similar mean GLS reference value of 20.5% (95% CI: 20.0% –
21.0%) (Jashari et al. 2015).
1.5.4 Baseline Global Longitudinal Strain
Recently, some investigators have suggested that baseline GLS measured prior to chemotherapy
exposure may help with the early identification of cancer patients with preserved LVEF who are
23
at increased risk of developing adverse cardiovascular events following cancer treatment (Rhea
et al. 2015; Mousavi et al. 2015; Hatazawa et al. 2018; Tanaka 2019). In a retrospective study of
158 patients (age: 53 ± 15 years) with a baseline LVEF of 50% to 59% and treated with
anthracycline chemotherapy, 12 patients (8%) were identified to have later developed major
adverse cardiac events such as congestive heart failure, cardiac arrest, or cardiac death (Mousavi
et al. 2015). Baseline LVEF was comparable between patients who developed cardiac events and
those who did not (53 ± 3% versus 54 ± 3%, p=0.27), but baseline GLS was significantly lower
in the former group (16.0 ± 2.5% versus 17.8 ± 2.5%, p=0.015). Additionally, baseline LVEF did
not predict the occurrence of cardiac events, whereas a baseline GLS of ≤16% was associated
with a 4.7-fold (95% CI: 1.5 – 16.0) increase in major cardiac events relative to patients with a
baseline GLS of >16%. This significance remained even after adjusting for age (p=0.033).
Moreover, no difference in baseline LVEF was observed between patients who presented with
a baseline GLS of ≤16% and those who had baseline GLS >16% (both 54%, p=0.11). Another
retrospective study by Ali et al. similarly reported that patients (age: 59 ± 18 years) who
developed symptomatic heart failure or cardiac death after anthracycline chemotherapy had
lower GLS at baseline compared to those who did not (15.0 ± 2.8% versus 19.7 ± 2.7%,
p<0.0001) (Ali et al. 2016). Lower baseline GLS was associated with a 1.47-fold (95% CI:
1.35 – 1.59) increase in hazard of subsequent cardiac events and the association remained
significant even among patients with normal LVEF at baseline, as well as in a multivariate
analysis adjusting for age and clinical factors. Furthermore, a receiver operating characteristic
curve analysis identified a baseline GLS value of less than 17.5% to be the optimal cut-off for
prediction of future cardiac events.
In a recent retrospective single-center study conducted by Hatazawa et al., baseline clinical and
echocardiographic parameters were examined in 73 lymphoma patients with preserved LVEF
who underwent anthracycline chemotherapy (Hatazawa et al. 2018). The average age of the
cohort was 64 ± 15 years and the cumulative anthracycline dose was 265 ± 107 mg/m2. The
mean LVEF and GLS at baseline were 65 ± 5% and 21.1 ± 2.7% respectively. Of the 73 patients,
10 (14%) developed LV dysfunction during the 50-months follow-up period. Those ten patients
were found to have had lower LVEF (60 ± 7% versus 65 ± 5%, p<0.01) and GLS (18.5 ± 3.4%
versus 21.6 ± 2.4%, p<0.001) at baseline compared to the patients who did not develop
cardiotoxicity. A multivariate logistic regression analysis identified a reduced baseline GLS to be
the only independent predictor of LV dysfunction following anthracycline chemotherapy (odds
ratio: 0.65, 95% CI 0.49 – 0.87, p=0.004). The authors also compared characteristics between
24
patients who had baseline GLS ≤19% (n=14) and those who had GLS >19% (n=59) at baseline.
No difference was observed between the two groups in terms of clinical characteristics such as
age, sex, and cumulative anthracycline dose. Baseline LVEF was lower in patients with reduced
baseline GLS relative to those with higher baseline GLS (60 ± 5% versus 66 ± 5%, p<0.001).
Interestingly, Tadic et al. demonstrated in a retrospective study that despite having preserved
LVEF, patients with solid tumors (age: 56 ± 9 years) had significantly reduced GLS compared
to controls (17.8 ± 3.5% versus 19.1 ± 2.1%, p=0.022) even before the administration of any
cancer treatment (Tadic et al. 2018). Assuncao et al. in a retrospective study of 76 adult acute
leukemia patients also found pre-existing abnormalities in GLS prior to them receiving any
anthracycline chemotherapy (Assuncao et al. 2017). In specific, patients had lower GLS
relative to matched controls who did not have cancer nor cardiac disease (19.3 ± 2.7% versus
20.9 ± 1.9%, p<0.001) at baseline. However, no difference in LVEF was observed between the
two groups. The authors concluded that the diagnosis of acute leukemia itself may predispose
patients to cardiac alterations prior to cancer treatment exposure.
These findings require further investigation in children with cancer. A better understanding of
the potential impact of pre-treatment myocardial strain abnormalities in pediatric cancer patients
as well as their predictive value for post-chemotherapy changes in left ventricular systolic
function is also warranted.
1.5.5 Other Measures of Cardiotoxicity
Cardiac remodeling occurs as a compensatory mechanism following anthracycline exposure and
accordingly, remodeling parameters may have a role in the detection of anthracycline-induced
cardiac damage. In a longitudinal cohort study of 115 doxorubicin-treated long-term survivors of
childhood acute lymphoblastic leukemia, left ventricular posterior wall thickness (LVPWT) and
left ventricular thickness to dimension ratio (TDR) were significantly reduced within 3 years of
diagnosis (Lipshultz et al. 2005). In contrast, substantial changes in LV contractility and
shortening fraction were not documented until 5 to 9 years post-diagnosis. LVPWT defines the
degree of myocardial damage and fibrosis in the inferolateral wall segments, while TDR is used
as a surrogate for the overall cardiac remodeling process. In another multi-center, prospective
25
randomized trial involving dexrazoxane, LVPWT and TDR were shown to be the only two
parameters that significantly differed between the treatment arm (the group receiving
dexrazoxane) and the dexrazoxane-naïve control group at 5 years after completion of
anthracycline treatment (Lipshultz et al. 2010). A consensus paper from an International Forum
on Cardiac Remodeling had proposed that in adults with cardiomyopathy or post myocardial
infarction, early evidence of cardiac remodeling is predictive of long-term outcomes (Cohn,
Ferrari, and Sharpe 2000).
Other strain parameters such as circumferential strain (CS) have also been subject to analysis in
the context of anthracycline cardiotoxicity. To date, studies have demonstrated that a change in
CS between 11% and 16.7% is suggestive of future adverse clinical outcomes (Loonen et al.
2012; Plana et al. 2014; Pignatelli et al. 2015; Narayan et al. 2016, 2017). The proposed
reference range for CS is 20.9% to 27.8% for adults (Yingchoncharoen et al. 2013) and 19.9% to
24.6% for children (Jashari et al. 2015; Levy et al. 2016; Tuzovic et al. 2018). Nonetheless,
longitudinal, confirmatory studies have been lacking in regard to CS and cardiotoxicity and thus,
the prognostic value of CS for adverse cardiac outcomes remains inconclusive.
26
1.6 Biomarkers for the Early Detection of Cardiotoxicity
Cardiac biomarkers are increasingly being explored as new tools for the early identification,
assessment, and monitoring of cardiac damage associated with cancer treatment in pediatric
cancer patients. This biomarkers approach presents with various advantages. It is minimally
invasive, more economical than conventional imaging techniques, and the interpretation of
laboratory results often has a low interobserver variability (Cardinale et al. 2017). At present, the
majority of studies in the cardio-oncological field focuses on two families of cardiac biomarkers:
natriuretic peptides and troponins.
Brain natriuretic peptide (BNP) is a hormone released by the myocardium in response to
increased wall strain and pressure overload (Cardinale et al. 2017). Its prohormone, proBNP, is
cleaved into two peptides upon activation, generating a C-terminal biologically active BNP
peptide alongside a biologically inactive N-terminal proBNP (NT-proBNP) peptide. BNP plays a
critical role in the maintenance of cardiovascular homeostasis through the modulation of the
glomerular filtration rate and stimulation of vasodilation (Cardinale et al. 2015). It also inhibits
the renin-angiotensin-aldosterone system and prevents unfavorable myocardial remodeling
(Michel, Rassaf, and Totzeck 2018). Currently, both American Heart Association (L. et al. 2017)
and European Society of Cardiology (Ponikowski et al. 2016) guidelines acknowledge the
elevation of natriuretic peptides in various cardiac disease and endorse the use of BNP and NT-
proBNP for the diagnosis as well as management of heart failure.
In pediatric cancer patients receiving chemotherapy, findings have been inconsistent in terms of
the association between serum BNP/NT-proBNP levels and the subsequent development of
cardiac dysfunction. In one randomized controlled study of 205 children with high-risk acute
lymphoblastic leukemia treated with either doxorubicin alone or doxorubicin with dexrazoxane,
NT-proBNP levels were increased in 89% and 92% of the former and latter group respectively,
before exposure to treatment (Lipshultz, Miller, Scully, et al. 2012). Following treatment, the
percentages dropped to 48% and 20% respectively, but increased NT-proBNP levels detected
within the first 90 days of treatment were significantly associated with an abnormal LV TDR 4
years later. The investigators concluded that early increases in NT-proBNP levels may be
predictive of future cardiac stress. Their findings also suggest that early elevations in NT-
proBNP levels may help identify a population of patients that is more vulnerable to
27
chemotherapy induced cardiac injury. The same conclusion was not attained in a study
conducted by Ekstein et al., in which NT-proBNP levels and cardiac function were assessed
before, during, and after anthracycline treatment in 25 children newly diagnosed with cancer
(Ekstein et al. 2007). Prior to the first dose of anthracycline, the average level of NT-proBNP
was 151 ± 112 pg/mL, a concentration comparable to healthy age-matched controls (p=0.13).
After the first anthracycline treatment, the concentration of NT-proBNP increased significantly
and remained elevated throughout the entire treatment compared to baseline as well as controls.
In 14 (61%) patients, the highest NT-proBNP level was in fact, observed during or after the first
cycle of anthracycline treatment. No associations between increased NT-proBNP levels and age,
sex, or cancer diagnosis were detected. Despite the observed changes in NT-proBNP levels, no
abnormalities in echocardiographic measures of cardiac function were detected both at the
beginning of treatment and at the end of the follow-up period.
Cardiac troponins, involved in the contractile apparatus of cardiomyocytes, directly reflect
cardiomyocyte integrity and represent the biomarkers of choice for the assessment of
cardiomyocyte injury in a variety of cardiovascular pathologies (Cardinale et al. 2017). In the
pediatric cardio-oncological setting, an elevation in cardiac troponin T (TnT) levels has been
reported after initial doxorubicin treatment and was predictive of LV dilatation as well as wall
thinning 9 months later in a group of high-risk acute lymphoblastic leukemia patients (Lipshultz
et al. 1997). A long-term follow-up study of the same population revealed that children who had
at least one elevation in cardiac TnT levels during doxorubicin treatment had significantly lower
LV end-diastolic posterior wall thickness (p=0.005) and LV end-diastolic TDR (p=0.004) five
years after treatment completion compared to those who did not display any raised
concentrations (Lipshultz et al. 2010). The finding validated the use of cardiac TnT as a
surrogate endpoint for LV health in long-term survivors of childhood acute lymphoblastic
leukemia.
Recent advancements in assay technology have led to the development of new high-sensitivity
troponin assays that are capable of detecting very small elevations in serum troponin levels with
negligible variability (Cardinale et al. 2017). The use of such high-sensitivity troponin measures
in the field of cardiotoxicity was first evaluated by Sawaya et al. in a multi-center study of 81
women with breast cancer, treated with anthracyclines followed by taxanes and trastuzumab
(Sawaya et al. 2012). Ultrasensitive troponin I (us-TnI), alongside echocardiograms were
obtained and examined at baseline and 3, 6, 9, 12 and 15 months during chemotherapy. An
28
elevated us-TnI concentration (≥30 pg/mL) at completion of anthracycline therapy was found to
be predictive of subsequent LV dysfunction (p=0.04). In a cross-sectional study of 100 adult
survivors of childhood leukemia who were treated with anthracycline chemotherapy, elevated
high-sensitivity troponin T (hs-TnT) levels were detected in 19 subjects (Y. Cheung et al. 2013).
Those subjects had received significantly higher cumulative doses of anthracycline than patients
who had normal hs-TnT (288 ± 126 versus 201 ± 83 mg/m2, p<0.001) and longitudinal systolic
strain rate at study investigation was lower as well (-0.86 ± 0.14 versus -0.95 ± 0.18 /s, p=0.049).
However, no differences in LVEF, GLS and CS were found between survivors with and without
elevated hs-TnT concentrations. Another study measured hs-TnT levels in 64 long-term
survivors of childhood cancer treated with anthracyclines and found normal levels in all patients,
despite 7 survivors having had a mildly decreased LVEF of 48% to 55% (Pourier et al. 2015).
Overall, very few studies to date, have examined hs-TnT levels in cancer patients. Longitudinal
data on hs-TnT are also lacking. As such, further research is required to fully understand the
utility of hs-TnT as an early marker of future cardiotoxicity in pediatric cancer patients.
29
Study Rationale, Objectives, and Hypotheses
2.1 Study Rationale
Cardiac toxicity remains a major limitation of anthracycline chemotherapy, strongly impacting
the quality of life and overall survival in children with cancer. Emphasis in the field of cardio-
oncology has been on the early detection of subclinical ventricular dysfunction to mitigate the
degree of cardiac injury. GLS measured by speckle tracking echocardiography is increasing used
in adult cancer patients who undergo chemotherapy, to detect subtle, early abnormalities in LV
myocardial performance prior to changes in LVEF. However, the importance of GLS among
pediatric cancer patients treated with anthracycline chemotherapy is less well defined. Moreover,
some studies in adult cancer patients have demonstrated that baseline GLS measured prior to
chemotherapy exposure may be abnormal, and such abnormalities were powerful tools for the
screening of patients who may be at an excessive risk for subsequent anthracycline-related
cardiotoxicity. These findings warrant investigation in the pediatric population. Furthermore,
findings have either been inconsistent or non-existent in regard to NT-proBNP and hs-TnT levels
in pediatric cancer patients treated with anthracycline. By using longitudinal data collected by a
multi-center cohort study, this study aims to address the gaps in the literature and elucidate
whether baseline myocardial strain influences cardiac outcomes one year after completion of
anthracycline chemotherapy.
2.2 Study Objectives
To assess the baseline cardiac function in pediatric cancer patients prior to anthracycline
exposure
To examine whether a lower GLS at baseline impacts the cardiac response to anthracycline
chemotherapy in pediatric cancer patients
30
To explore the relationship between baseline cardiac biomarkers and echocardiographic
parameters in pediatric cancer patients before, during, and after receiving anthracycline
treatment
2.3 Specific Aims
To assess the baseline cardiac function in terms of LVEF and strain measurements
(GLS and CS) in pediatric cancer patients prior to anthracycline exposure
To examine whether there are differences in cardiac strain measurements between
healthy controls and pediatric cancer patients prior to administration of anthracycline
chemotherapy
To determine whether there is a subgroup of patients with GLS at the lower limit of
normal or in the abnormal range, prior to anthracycline administration and if so,
uncover its associated demographic, disease, and treatment factors
To examine the impact of a lower GLS at baseline on LVEF and strain parameters (GLS
and CS) during anthracycline treatment
To examine the impact of a lower GLS at baseline on LVEF and strain parameters (GLS
and CS) 12 months after completion of anthracycline treatment
To elucidate the profiles of specific cardiac biomarkers (NT-proBNP and hs-TnT) in
pediatric cancer patients prior to and after receiving anthracycline chemotherapy
To compare cardiac biomarkers (NT-proBNP and hs-TnT) measurements between
healthy controls and pediatric cancer patients
To explore the relation between cardiac biomarkers (NT-proBNP and hs-TnT) levels at
baseline and LVEF, GLS, and CS measurements at baseline
To explore the relation between cardiac biomarkers (NT-proBNP and hs-TnT) levels at
baseline and LVEF, GLS, and CS measurements during anthracycline treatment
31
To explore the relation between cardiac biomarkers (NT-proBNP and hs-TnT) levels at
baseline and LVEF, GLS, and CS measurements at 12 months after completion of
anthracycline treatment
2.4 Hypotheses
Objective 1
• There will be differences in cardiac strain measurements between pediatric cancer
patients prior to receiving anthracycline chemotherapy and healthy controls
Objective 2
2.1.1 Pediatric cancer patients who present with a lower GLS at baseline will have worse
LVEF, GLS, and CS during anthracycline chemotherapy than those who start with a
higher baseline GLS, even when adjusting for patient demographics and cancer
diagnosis
2.1.2 Pediatric cancer patients who present with a lower GLS at baseline will have worse
LVEF, GLS, and CS 12 months after completion of anthracycline chemotherapy than
those who start with a higher baseline GLS, even when adjusting for patient
demographics and cancer diagnosis
Objective 3
3.1.1 Pediatric cancer patients will have higher levels of both NT-proBNP and hs-TnT prior
to anthracycline administration compared to healthy controls
32
3.1.2 Elevated NT-proBNP and hs-TnT levels at baseline in pediatric cancer patients will be
associated with worse echocardiographic measurements of cardiac function at baseline
3.1.3 Elevated NT-proBNP and hs-TnT levels at baseline in pediatric cancer patients will be
associated with worse echocardiographic measurements of cardiac function during
anthracycline treatment
3.1.4 Elevated NT-proBNP and hs-TnT levels at baseline in pediatric cancer patients will be
associated with worse echocardiographic measurements of cardiac function at 12
months after completion of anthracycline chemotherapy
33
Methodology
3.1 Study Design Overview
A retrospective analysis of prospectively captured data was conducted to examine whether
baseline cardiac function in pediatric cancer patients influences cardiac outcomes in response to
anthracycline chemotherapy exposure. The study was approved by research ethics boards at each
participating study site and written informed consent was obtained from each participant or their
legal guardian.
Using the data collected in the context of the Preventing Cardiac Sequelae in Pediatric Cancer
Survivors (PCS2) study, we identified 176 pediatric patients (age: <18 years) newly diagnosed
with cancer who had echocardiographic measurements from both the baseline echocardiogram
(performed before the first dose of anthracycline) and at 12-months after completion of
anthracycline chemotherapy. Baseline cardiac function in terms of LVEF and strain parameters
(GLS and CS) were examined and compared against a control cohort comprised of children aged
4 to 18 years, without heart disease. The patient cohort was then dichotomized based on their
baseline GLS measurement. Clinical characteristics and cardiac function measured at baseline,
end-treatment, and 12-month follow-up were compared between the ‘low GLS group’ (baseline
GLS <19%) and the ‘high GLS group’ (baseline GLS >20%), as well as within each respective
group.
A sub-analysis of cardiac biomarkers was also performed. In total, 95 baseline NT-proBNP and
57 baseline hs-TnT serum samples from consenting PCS2 patients were assayed. Baseline
cardiac biomarker levels were compared against the reference Canadian Laboratory Initiative on
Pediatric Reference Intervals (CALIPER) cohort. We explored whether there are any
relationships between cardiac biomarkers measured prior to anthracycline exposure and
echocardiographic parameters of cardiac function, including LVEF, GLS, CS and LV end-
diastolic diameter (LVEDD) assessed before, during, and after anthracycline chemotherapy.
34
3.2 Preventing Cardiac Sequelae in Pediatric Cancer Survivors (PCS2) Study
The Preventing Cardiac Sequelae in Pediatric Cancer Survivors (PCS2) study is a prospective,
multi-center, observational cohort study designed to use novel echocardiographic parameters of
cardiac function, combined with genetic and biological markers to identify patients with
childhood cancer who are at risk of developing acute or progressive, late-onset cardiac
dysfunction following anthracycline chemotherapy (Skitch et al. 2017). The overarching aim of
the PCS2 study was to develop a risk prediction algorithm specific to childhood cancer survivors
who are at risk of cardiac disease following anthracycline treatment. There are five collaborating
centers in Canada and on in the United States: The Hospital for Sick Children (Toronto, Ontario,
Canada), Princess Margaret Hospital (Toronto, Ontario, Canada), McMaster Children’s Hospital
(Hamilton, Ontario, Canada), London Health Sciences Centre (London, Ontario, Canada), The
Children’s Hospital of Eastern Ontario (Ottawa, Ontario, Canada), and The Children’s Hospital
of Orange County (Orange County, California, United States). Altogether, the five Canadian
sites account for 97% of cancers treated in pediatric hospitals in the province of Ontario and
approximately 45% of all childhood cancers diagnosed throughout Canada.
Two patient cohorts have been recruited for the long-term assessment of anthracycline-induced
cardiotoxicity: Acute Cohort and Survivor Cohort.
3.2.1 Acute Cohort
The Acute Cohort was comprised of a prospective cohort of children under 18 years of age at the
time of cancer diagnosis, who had cancer treatment plans that involved at least one dose of any
of the following anthracycline agents: doxorubicin, daunorubicin, epirubicin, idarubicin, and/or
mitoxantrone (n = 303). Eligibility criteria are summarized in Table 1. Echocardiographic
parameters of acute cardiac dysfunction, genetic variants related to anthracycline susceptibility,
and biological markers of early cardiac damage were systematically examined to identify
patients who were at risk of progressive cardiac damage at one year from their last cycle of
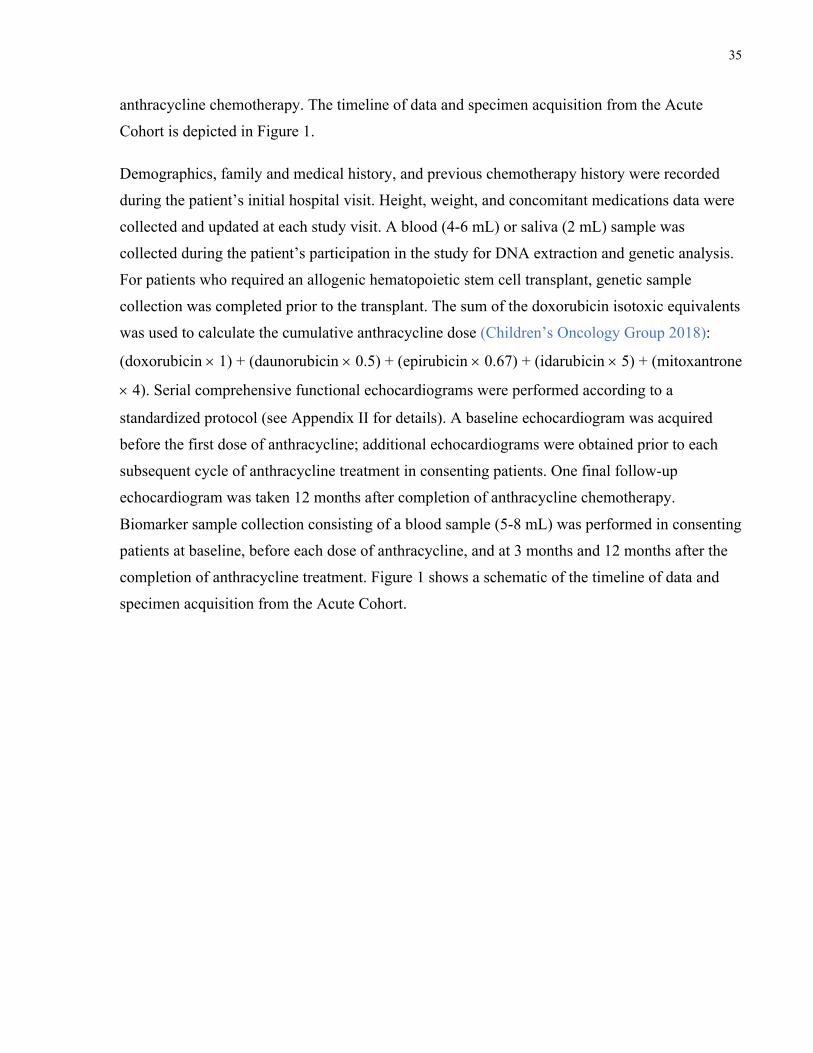
35
anthracycline chemotherapy. The timeline of data and specimen acquisition from the Acute
Cohort is depicted in Figure 1.
Demographics, family and medical history, and previous chemotherapy history were recorded
during the patient’s initial hospital visit. Height, weight, and concomitant medications data were
collected and updated at each study visit. A blood (4-6 mL) or saliva (2 mL) sample was
collected during the patient’s participation in the study for DNA extraction and genetic analysis.
For patients who required an allogenic hematopoietic stem cell transplant, genetic sample
collection was completed prior to the transplant. The sum of the doxorubicin isotoxic equivalents
was used to calculate the cumulative anthracycline dose (Children’s Oncology Group 2018):
(doxorubicin ´ 1) + (daunorubicin ´ 0.5) + (epirubicin ´ 0.67) + (idarubicin ´ 5) + (mitoxantrone
´ 4). Serial comprehensive functional echocardiograms were performed according to a
standardized protocol (see Appendix II for details). A baseline echocardiogram was acquired
before the first dose of anthracycline; additional echocardiograms were obtained prior to each
subsequent cycle of anthracycline treatment in consenting patients. One final follow-up
echocardiogram was taken 12 months after completion of anthracycline chemotherapy.
Biomarker sample collection consisting of a blood sample (5-8 mL) was performed in consenting
patients at baseline, before each dose of anthracycline, and at 3 months and 12 months after the
completion of anthracycline treatment. Figure 1 shows a schematic of the timeline of data and
specimen acquisition from the Acute Cohort.
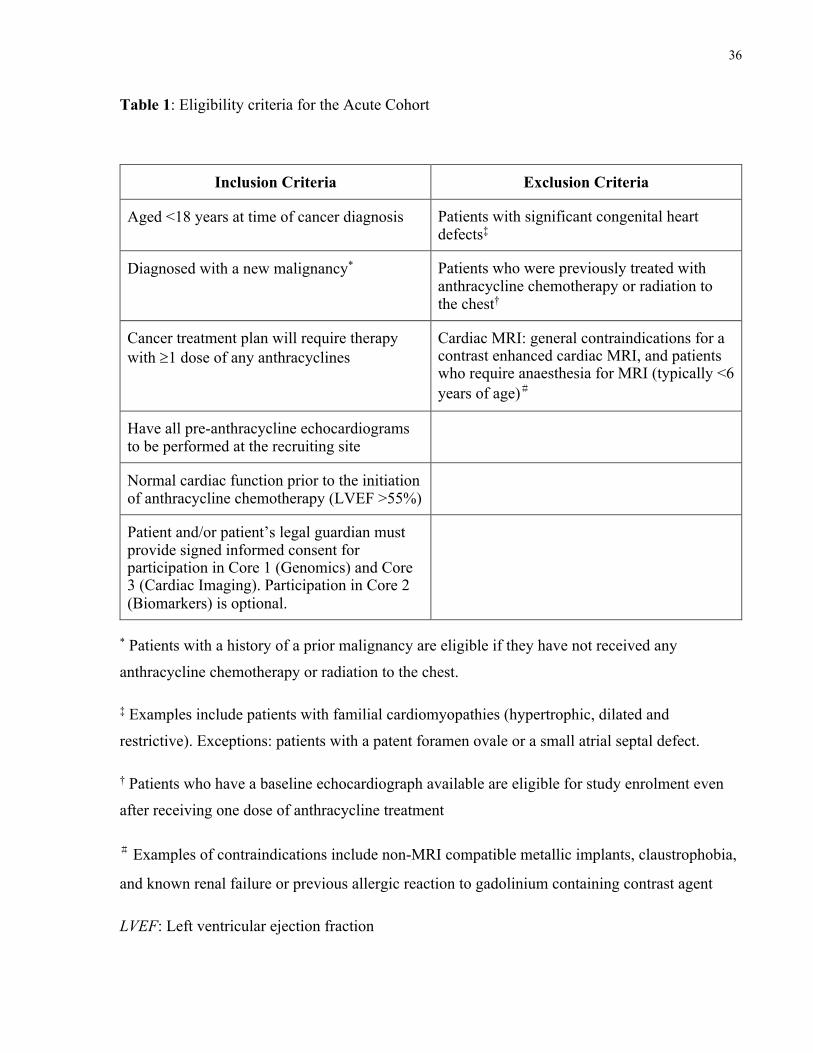
36
Table 1: Eligibility criteria for the Acute Cohort
Inclusion Criteria Exclusion Criteria
Aged <18 years at time of cancer diagnosis Patients with significant congenital heart defects‡
Diagnosed with a new malignancy* Patients who were previously treated with anthracycline chemotherapy or radiation to the chest†
Cancer treatment plan will require therapy with ³1 dose of any anthracyclines
Cardiac MRI: general contraindications for a contrast enhanced cardiac MRI, and patients who require anaesthesia for MRI (typically <6 years of age)#
Have all pre-anthracycline echocardiograms to be performed at the recruiting site
Normal cardiac function prior to the initiation of anthracycline chemotherapy (LVEF >55%)
Patient and/or patient’s legal guardian must provide signed informed consent for participation in Core 1 (Genomics) and Core 3 (Cardiac Imaging). Participation in Core 2 (Biomarkers) is optional.
* Patients with a history of a prior malignancy are eligible if they have not received any
anthracycline chemotherapy or radiation to the chest.
‡ Examples include patients with familial cardiomyopathies (hypertrophic, dilated and
restrictive). Exceptions: patients with a patent foramen ovale or a small atrial septal defect.
† Patients who have a baseline echocardiograph available are eligible for study enrolment even
after receiving one dose of anthracycline treatment
# Examples of contraindications include non-MRI compatible metallic implants, claustrophobia,
and known renal failure or previous allergic reaction to gadolinium containing contrast agent
LVEF: Left ventricular ejection fraction
37
Figure 1: Timeline of data and specimen acquisition from the Acute Cohort.
BIOMKR: Serum collection for biomarker analyses; CLIN: Gather clinical data; DNA: Blood or
saliva sample collection for DNA analyses; ECHO: Echocardiogram acquisition
1 st dose 2 nd dose 3 rd dose Baseline 3 month F/U 1 year F/U
CLIN
DNA
ECHO ECHO ECHO ECHO ECHO
BIOMKR BIOMKR BIOMKR BIOMKR
Final dose ……….
BIOMKR BIOMKR BIOMKR
ECHO
38
3.2.2 Survivor Cohort
The Survivor Cohort consisted of a prospective cohort of childhood cancer survivors who had
completed their last cycle of anthracycline chemotherapy 3 or more years prior to study
enrolment (n = 818). Survivors who attended a specialized provincial network of childhood
cancer survivor clinics at the six participating centres were approached for study recruitment and
were followed for a study duration of two years. Table 2 indicates the eligibility criteria for this
cohort. The trajectory of changes in novel echocardiographic parameters of ongoing cardiac
stress, injury, and remodeling were examined. In addition, the study group aimed to identify
predictors of genetic susceptibility to anthracycline-induced cardiotoxicity as well as biomarker
indicators of cardiac damage and remodeling. The timeline of data and specimen acquisition
from the Survivor Cohort is depicted in Figure 2.
Height and weight were assessed, and demographics, family and medical history, as well as
cancer therapy history, including the last date of chemotherapy were recorded at the baseline
study visit. Updates on concomitant medication data were obtained at each study visit. In
consenting patients, samples for genomic analysis were collected in the form of either a blood (4-
6 mL) or saliva (2 mL) sample at study enrolment. Serial echocardiograms to comprehensively
assess cardiac function were performed according to a standardized protocol at baseline, and at
12 months and 24 months after the initial study visit (see Appendix II for details). Additional
blood samples (5-8 mL) were collected at each echocardiogram time point for biomarker
analysis from patients who had provided consent. Finally, cardiac MRI was performed either
within 6 months of study enrolment or the 12 or 24-month study visit, or within 6 months of a
subsequent standard clinical follow-up echocardiogram. Participation in this cardiac MRI
component of the study was optional. A diagram showing the timeline of data and specimen
acquisition from the Survivor Cohort is shown in Figure 2.
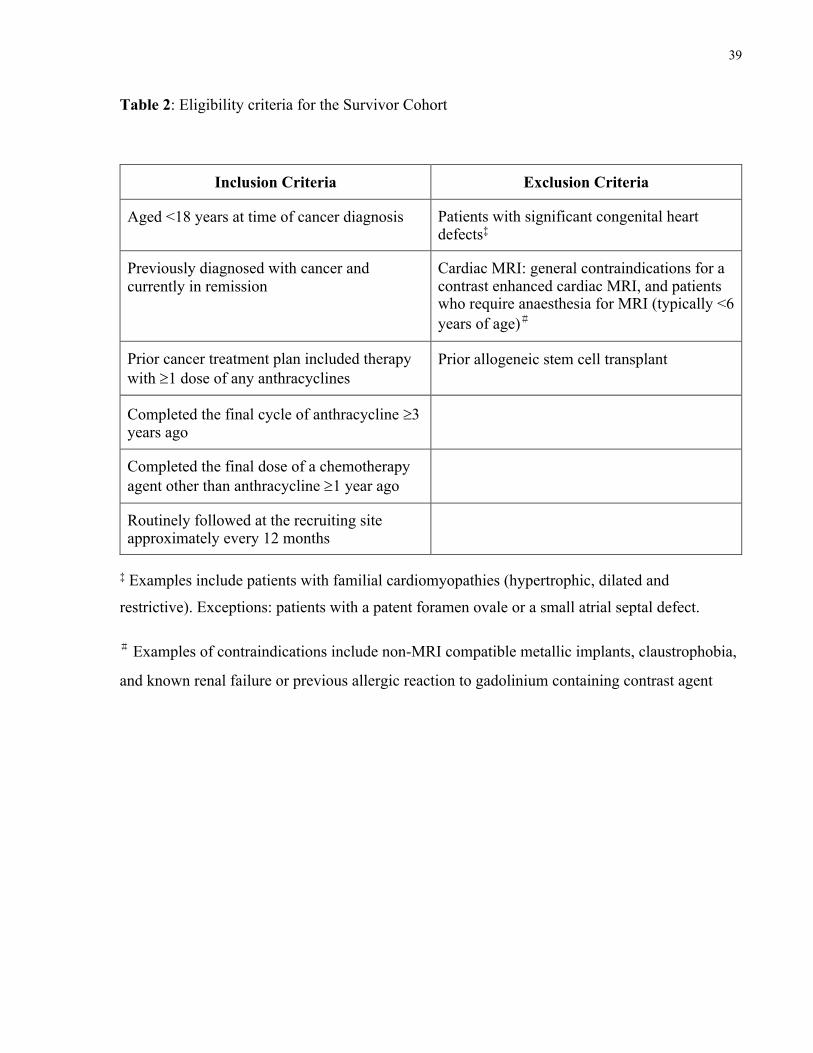
39
Table 2: Eligibility criteria for the Survivor Cohort
Inclusion Criteria Exclusion Criteria
Aged <18 years at time of cancer diagnosis Patients with significant congenital heart defects‡
Previously diagnosed with cancer and currently in remission
Cardiac MRI: general contraindications for a contrast enhanced cardiac MRI, and patients who require anaesthesia for MRI (typically <6 years of age)#
Prior cancer treatment plan included therapy with ³1 dose of any anthracyclines
Prior allogeneic stem cell transplant
Completed the final cycle of anthracycline ³3 years ago
Completed the final dose of a chemotherapy agent other than anthracycline ³1 year ago
Routinely followed at the recruiting site approximately every 12 months
‡ Examples include patients with familial cardiomyopathies (hypertrophic, dilated and
restrictive). Exceptions: patients with a patent foramen ovale or a small atrial septal defect.
# Examples of contraindications include non-MRI compatible metallic implants, claustrophobia,
and known renal failure or previous allergic reaction to gadolinium containing contrast agent
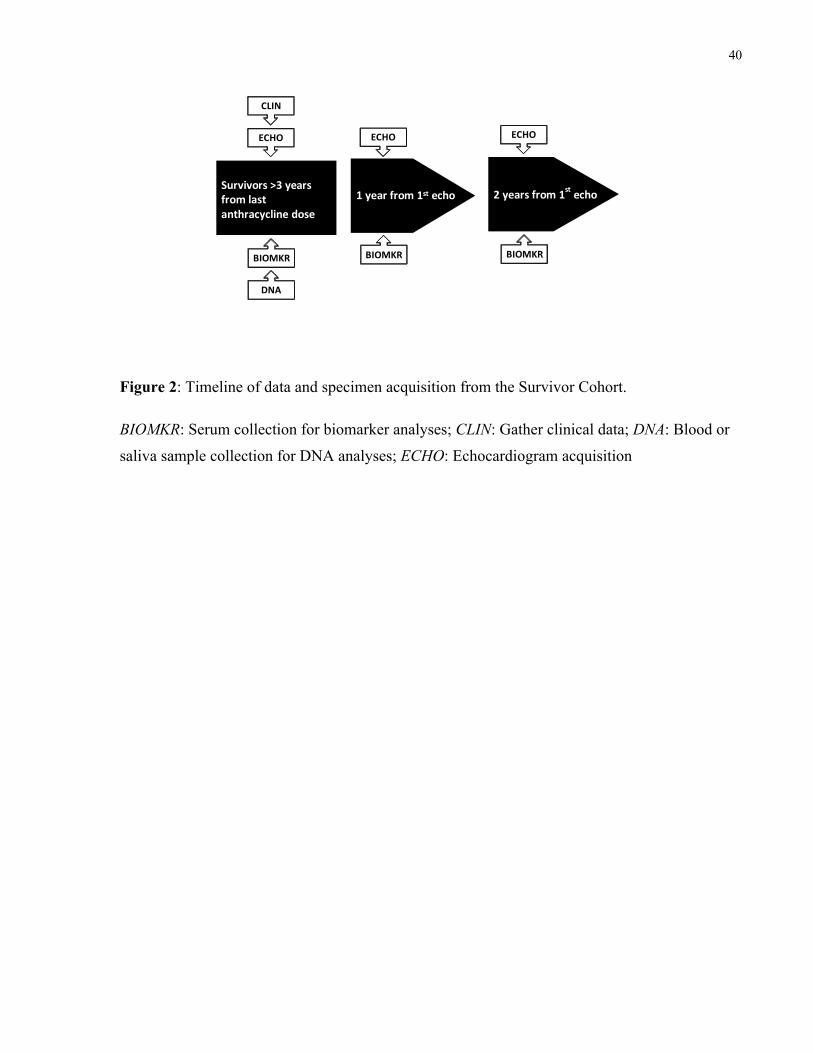
40
Figure 2: Timeline of data and specimen acquisition from the Survivor Cohort.
BIOMKR: Serum collection for biomarker analyses; CLIN: Gather clinical data; DNA: Blood or
saliva sample collection for DNA analyses; ECHO: Echocardiogram acquisition
Survivors >3 years from last anthracycline dose
1 year from 1st echo
Open label study
CLIN
BIOMKR
ECHO
DNA
ECHO ECHO
BIOMKR BIOMKR
2 years from 1st echo
41
3.2.3 PCS2 Study Objectives
The primary objective of the the PCS2 study was to identify patients with childhood cancer who
were at risk of developing acute or progressive, late-onset cardiac dysfunction following
anthracycline chemotherapy through the use of novel echocardiographic parameters of cardiac
function, alongside genetic and biological markers. There were four collaborative cores that
underlay the PCS2 study: Core 1 (Genomics), Core 2 (Biomarkers), Core 3 (Cardiac imaging),
and Core 4 (Registry).
Core 1: Genomics
The Genomics Core was responsible for conducting comprehensive genome-wide single
nucleotide polymorphism (SNP) genotyping to identify genetic variants that predispose children
with cancer to cardiac dysfunction following anthracycline exposure. Genes in pathways related
to anthracycline absorption, distribution, metabolism, and excretion were prioritized for
examination and analysis, in addition to those that were involved in pathways known to be
important in the cardiac response to injury. Whole exome sequencing or targeted exome capture
were also performed in patients with extreme phenotypes to identify additional rare variants that
conferred susceptibility to anthracycline cardiotoxicity. Conversely, genetic profiles of patients
who presented with preserved cardiac function despite having received high doses of
anthracycline treatment were also examined to identify genetic variants that might potentially be
protective against anthracycline cardiotoxicity.
Core 2: Biomarkers
The Biomarkers Core focused on both the discovery of novel biomarkers and the evaluation of
existing biomarker predictors of acute and chronic cardiac toxicity in children treated with
42
anthracycline chemotherapy. The team first examined candidate biomarkers that were detectable
before, during, and 1 year after anthracycline exposure, and evaluated their association with early
cardiac remodeling and injury in a small subgroup of children enrolled in the Acute Cohort at the
Hospital for Sick Children (Discovery Cohort). The findings were then validated in similarly
recruited Acute Cohort patients from the Hamilton, London, and Ottawa sites (Validation
Cohort).
Two main biomarkers chosen for investigation were N-terminal pro B-type natriuretic peptide
(NT-proBNP) and high sensitivity troponin T (hs-TnT). When possible, other candidate
biomarkers such as myeloperoxidase (MPO) and insulin-like growth factor binding protein 7
(IGF-BP7) were also assessed. Serial serum samples (5-8 mL) from consenting patients were
collected at the time points specified in Figure 1. Using quality-controlled enzyme-linked
immunosorbent assays (ELISA) on the most appropriate platforms, individual biomarker levels
at each collection time point were analyzed and patterns of change over time were evaluated
against the primary outcomes (reduced LVEF, development of heart failure, or cardiac
remodeling). All biomarker samples were assayed in replicates with appropriate procedural
controls. Once the best candidate biomarkers were identified from the Discovery Cohort, the
same biomarkers were examined in the Validation Cohort to determine the reproducibility and
cross population validity of the marker performance.
In the Survivor Cohort, the primary aim of the Biomarkers Core was to determine the relation
between candidate biomarkers levels and imaging parameters of cardiac remodeling or sub-
clinical dysfunction in childhood cancer survivors who had exposure to anthracycline
chemotherapy. The same panel of candidate biomarkers from the Acute Cohort was assessed.
Following additional consent, serum samples (5-8 mL) were collected concurrent with study
echocardiograms performed at baseline, and at 12 months and 24 months after the initial study
visit. The same standardized methodology as the Acute Cohort was used to assay the samples.
The Biomarker Core further used a cardiac differentiated human stem cell platform to uncover
novel candidate biomarkers that are responsive to cardiac injury following anthracycline
exposure. Myocyte, endothelial, and myofibroblast lineages that resemble a child’s myocardium
were derived from differentiated human cardiac stem cells and exposed to increasing doses of
doxorubicin (10-300 ng/mL) in solution for up to 72 hours. Cellular responses such as cell death
and activation of free radical scavenging systems were assessed, along with the extent of DNA
43
damage that occurred following anthracycline treatment. Protein expression was then compared
against control cell samples. Candidate biomarkers were identified through a mixture of
regression modeling and a customized biomarker priority filter that considered the following
characteristics: consistency and degree of change, small molecular size, detectability in
peripheral blood, stability in a hydrophilic environment, co-regulation with high risk genetic
SNPs, and low background levels in the untreated population. Finally, the resulting best novel
candidate markers were evaluated in both the Acute and Survivor Cohorts using antibodies or
multiple reaction monitoring on mass spectrometry.
Core 3: Cardiac Imaging
The Cardiac Imaging Core explored the utility of novel echocardiographic parameters of early
ventricular dysfunction and cardiac magnetic resonance (CMR) imaging as predictors of
progressive cardiac deterioration after anthracycline exposure in children with cancer. In
specific, the Cardiac Imaging team investigated in the Acute Cohort, whether a reduction in
regional myocardial function (as measured by longitudinal and circumferential strain) occurred
early after anthracycline exposure and determined whether these fluctuations influenced the
trajectory of change in cardiac function from baseline to 12 months after anthracycline
chemotherapy.
Patients in the Acute Cohort all completed a baseline echocardiogram prior to commencing
anthracycline chemotherapy, and additional echocardiograms were performed according to the
schedule outlined in Figure 1. A standardized functional protocol was followed and is described
in Appendix II. All echocardiographic examinations were performed using a Vivid 7 or Vivid E9
ultrasound system (GE Healthcare, Wauwatosa, WI). Details pertaining to the procedures for
echocardiographic image acquisition and offline echocardiographic analyses have been
previously published (Dallaire et al. 2016). In brief, study participants were instructed to be in
the left lateral decubitus position during the examination and all images were acquired during
sinus rhythm and spontaneous breathing. Sedation was not applied to any participants for the
echocardiographic studies and transducers were changed accordingly for optimal image
acquisition. Strain measurement by speckle tracking echocardiography was performed in
44
accordance to procedures previously outlined by Koopman et al. (Koopman et al. 2011).
Longitudinal strain was assessed based on standard apical four, three and two chamber view
images. Mean circumferential strain was determined through parasternal short-axis images that
were acquired at the basal, mid, and apical ventricular levels. Determination of systolic LV
function and quantification of cardiac chamber size were performed in accordance to
methodology recommendations proposed by the Pediatric Measurement Writing Group of the
American Society of Echocardiography Pediatric and Congenital Heart Disease Council (Lopez
et al. 2010).
Offline echocardiographic analyses were performed using the EchoPAC software version
110.1.3 (GE Healthcare, Wauwatosa, WI). To limit interobserver variability, one single
experienced research sonographer completed all aspects of image quantification. The Teichholz
formula was applied for the calculation of ejection fraction (Wandt et al. 1999). For strain
measurements, the endocardial border was first traced manually, tracking was automatically
performed, and satisfactory analyses were acquired when the software indicated adequate
tracking. When the software indicates otherwise, manual adjustments were made to the tracking
points throughout the cardiac cycle. Only image acquisitions with a minimum of four
appropriately tracking segments were approved for further analysis. Mean values of 6 segments
were averaged to calculate the mean circumferential strain and longitudinal strain. Global
longitudinal strain described the average longitudinal strain from the 3 apical views. Secondary
imaging parameters including diastolic function parameters, tissue Doppler measurements and
other myocardial deformation measurements were additionally obtained. Analyses of these
measurements may help identify novel echocardiographic parameters predictive of early
myocardial dysfunction.
The main responsibility of the Cardiac Imaging core in the Survivor Cohort was to identify and
examine cardiac remodeling parameters in a subgroup of long-term childhood cancer survivors
who present with early signs of myocardial dysfunction. This subgroup was followed over time
to elucidate the trajectory of change in cardiac function and remodeling. By doing so, a cardiac
phenotype of early damage could be defined, which could help inform future intervention
studies.
At each of the echocardiogram time points depicted in Figure 2, patients in the Survivor Cohort
had their longitudinal and circumferential strain measured, as well as LVPWT and TDR. Based
45
on current clinical evidence, a mean longitudinal strain of > -18% and a mean circumferential
strain measurement of > -15% at the basal level of the heart were defined a priori as subclinical
cardiac dysfunction. Likewise, a LVPWT and TDR z-score of < -2.0 defined a clinically
significant cardiac remodeling. The proportion of survivors that develop subclinical dysfunction
(as measured by strain), global dysfunction (defined as LVEF <55% or development of heart
failure), or remodeling (in terms of LVPWT and TDR) was recorded and the rate of change in
each of the aforementioned parameters was studied over time. Additionally, the relationship
between strain parameters and remodeling parameters were explored.
Lastly, in a pre-selected group of patients from both the Acute and Survivor Cohorts, the Cardiac
Imaging team used T1 mapping CMR to explore the association between echocardiographic
parameters of cardiac dysfunction and fibrosis, as well as other biomarkers of collagen
metabolism.
Core 4: Registry
The Registry Core aimed to re-enroll former PCS2 participants in a new longitudinal
observational cohort registry after the PCS2 study duration and follow them well into their
adulthood to better understand the long-term cardiac sequelae in cancer patients. All living PCS2
participants who were treated for their cancer at The Hospital for Sick Children, Princess
Margaret Hospital, and McMaster Children’s Hospital were approached and would be followed
by the registry for as long as they remain alive. Participants included in the registry have the
right to withdraw from the registry at any given time. For completeness of data, patients who
died prior to the establishment of the registry also had their vital status included in the registry. A
review of medical charts would be performed annually by research staff members, and
information pertaining to the following would be collected and updated: echocardiogram reports,
raw echocardiogram data (when available), changes in medical status, height, weight,
concomitant medication, full details on any cancer treatments, and results of any clinical tests
related to cardiac or cancer health. Participants would also be given an optional annual
questionnaire to elaborate upon their cardiac and cancer health.
46
3.2.4 PCS2 Study Outcomes
The primary outcomes of the PCS2 study were defined as follows:
• A reduced LVEF (<55%) or a drop in LVEF of ³10% over serial echocardiograms
• Development of symptomatic heart failure, graded using New York Heart Association
(NYHA) classification (or Ross heart failure class 2 in infants <2 years old)
• Cardiac remodeling defined as an LVPWT or TDR z-score < -2.0 (or a reduction in
LVPWT or TDR z-score by ³1 standard deviation compared to baseline in the Acute
group)
The occurrence of any one or more of the above in study participants at 12 months after
anthracycline treatment (Acute Cohort), or at any study visit (Survivor Cohort) was indicative of
anthracycline-related cardiotoxicity.
3.3 Study Population
For the present study, we examined serial echocardiographic data from patients enrolled in the
Acute Cohort of the PCS2 study. Eligibility criteria for the Acute Cohort and details on study
procedures are described in Section 3.2. All serial functional echocardiograms were performed
according to a standardized protocol (Appendix II).
The control cohort consisted of children aged 4 to 18 years, without heart disease, who were
prospectively recruited from local schools as volunteers and from a selection of patients
attending the cardiac clinic at The Hospital for Sick Children. With the exception of a
physiological murmur, all controls had normal results on physical examination and
inconspicuous medical histories. Full anatomic and functional echocardiography were performed
to further identify and exclude any children who had abnormal echocardiographic findings,
including minor defects such as small atrial septal defect and patent ductus arteriosus. This same
47
cohort had been previously incorporated into studies by our group that determined reference
values for LV systolic strain (Dallaire et al. 2016), as well as for pulse wave Doppler and tissue
Doppler imaging (Dallaire et al. 2015).
Data pertaining to cardiac biomarkers were also extracted and examined for Acute Cohort
patients enrolled at The Hospital for Sick Children who consented to participate in the
Biomarkers Core of the PCS2 study. The time points at which serum samples were collected for
biomarker analysis are shown in Figure 1.
Normal pediatric reference values for cardiac biomarkers of interest were derived from previous
publications (Albers et al. 2006; Abiko et al. 2018), as well as from the database developed by
the Canadian Laboratory Initiative on Pediatric Reference Intervals (CALIPER) project (Schnabl
et al. 2008).
3.3.1 The Canadian Laboratory Initiative on Pediatric Reference Intervals
(CALIPER) Project
The CALIPER project is a national research initiative launched in 2008 to develop a
comprehensive database of pediatric reference intervals for both traditional and emerging novel
biomarkers of pediatric disease (Schnabl et al. 2008). Healthy children and adolescents from
birth to 18 years of age formed the basis of the project and were recruited from schools,
churches, community programs, as well as hospital outpatient clinics. Those who had a history of
chronic illness or metabolic disease, or an acute illness within the previous month were ineligible
for CALIPER enrolment. Exclusion criteria also included those who were pregnant and those
who had used prescribed medications in the two weeks prior to study enrolment.
In order for the CALIPER project to derive comprehensive age- and sex-specific reference
intervals that encompass the major ethnic groups of Canada’s diverse population, participants or
their legal guardian first completed a short health questionnaire following written informed
consent. Information collected by the health questionnaire included demographic data such as
sex, ethnicity, family and medical history, diet, exercise status, and anthropometric
measurements including height, weight, and waist circumference. Participants were also
48
encouraged to complete an optional self-report on Tanner stage, which is a measure of sexual
maturity (Marshall and Tanner 1969, 1970). Such data would help the CALIPER project
establish accurate and reliable reference intervals, defined as the central 95% of test results
expected in a healthy population, for various pediatric biochemistry tests based on a child’s age,
sex, and ethnicity in clinical diagnosis.
Following consent and the health questionnaire, participants would then visit a participating
CALIPER site to provide a one-time small blood sample. The amount of blood to be drawn
varied depending on the participant’s age where those aged 0 to <1 year provided 3.5 mL, 1 to
<11 years provided 7.0 mL, and 11 to <19 years provided 10.5 mL in total. All blood samples
were collected using serum separator tubes (SSTTM; BD), stored at -80°C until testing, and
analyzed using the Cobas® e 411 analyzer (Roche Diagnostics, Mannheim, Germany). Prior to
running the samples, CalSet and PreciControl sets from the same manufacturer were used to
ensure proper calibration of the assays. As of 2014, over 8400 children and adolescents had been
recruited for the CALIPER project, and pediatric reference intervals for more than 70 common
biochemical markers, proteins, lipids and enzymes, as well as endocrine markers and fertility
hormones have been published by the CALIPER group (Schnabl et al. 2008; Adeli 2014).
3.4 Echocardiographic Strain Assessment
Serial echocardiographic data from patients enrolled in the Acute Cohort (total n = 303) of the
PCS2 study were examined. Of particular interest for the present study was the relative cardiac
function assessed at the following three time points: baseline, end-treatment, and 12-month
follow-up. The ‘baseline’ echocardiogram refers to the echocardiographic study performed
before the first dose of anthracycline treatment, but not necessarily before the administration of
any chemotherapy (i.e. some participants had received other non-anthracycline chemotherapy
prior to PCS2 study enrollment). As depicted in Figure 1, additional echocardiographic studies
were completed prior to each subsequent dose of anthracycline chemotherapy. The ‘end-
treatment’ echocardiogram refers to the echocardiographic study conducted before the last cycle
of anthracycline treatment. Any echocardiograms performed between 0 to 45 days before the
administration of the last dose of anthracycline were included for analysis, which essentially
49
corresponded to 90% of all end-treatment echocardiograms that were performed. The final
‘follow-up’ echocardiogram was completed approximately 12 months after the last dose of
anthracycline chemotherapy. We allowed the 12-month follow-up window to be within 10 to 17
months post-anthracycline treatment completion in order to have a comparable set of
echocardiographic measurements. Any echocardiographic studies that were completed outside of
this 10 to 17-month window were excluded from analyses (n = 40).
Given our primary study objective of evaluating whether a lower GLS at baseline impacts the
cardiac response to anthracycline chemotherapy in pediatric cancer patients, we excluded 51
patients who had echocardiograms performed at baseline but did not have a measurable GLS due
to quality issues with the scans. Furthermore, we excluded 76 patients who did not have a
follow-up echocardiogram performed within the time frame of 10 to 17 months post-
anthracycline completion. Of these 76 cases, 40 had echocardiograms completed outside of the
prespecified time frame as previously mentioned, 19 were due to the death of the patient during
the study period (none of which were due to cardiovascular issues – Appendix III), and 4 patients
were lost to follow-up. Accordingly, the study cohort that formed the basis for our analyses
consisted of 176 pediatric cancer patients in the Acute Cohort who had relevant
echocardiographic measurements from both the baseline echocardiogram and the 12-month
follow-up echocardiogram. The identification process for the study cohort is summarized in
Figure 3.
To address the first objective of our study, the baseline cardiac function in terms of LVEF and
strain parameters (GLS and CS) were assessed in the 176 pediatric cancer patients. Cardiac strain
measurements between these patients and a pediatric cohort of healthy controls were also
compared to examine whether there are differences in strain parameters between the two groups.
Details on this control cohort have been previously described in Section 3.3. To account for the
possible influence of age on cardiac strain parameters (Abou et al. 2017), the two cohorts were
divided into quartiles based on age for comparison of strain measurements.
The 176 patients selected for echocardiographic strain assessment were then dichotomized based
on their GLS measurement at baseline. The ‘low GLS group’ included subjects with a lower
GLS (absolute value <19%) at baseline, whereas the ‘high GLS group’ comprised of those with a
higher GLS (absolute value >20%) at baseline. Patients who presented with a baseline GLS of
³19% to ≤20% were excluded to allow for a more distinct separation in terms of GLS between

50
the two comparison groups. Each patient in the low GLS group was matched to two subjects
from the high GLS group based on age group (0 – 5 years old, 5 – 10 years old, 10 – 15 years
old, or 15+ years old) and cancer diagnosis (leukemia, lymphoma, bone/soft tissue sarcoma, or
other embryonal tumors). LVEF and strain parameters, including GLS and CS, measured at
baseline, end-treatment, and 12-month follow-up were compared within each group, as well as
between the two patient groups.
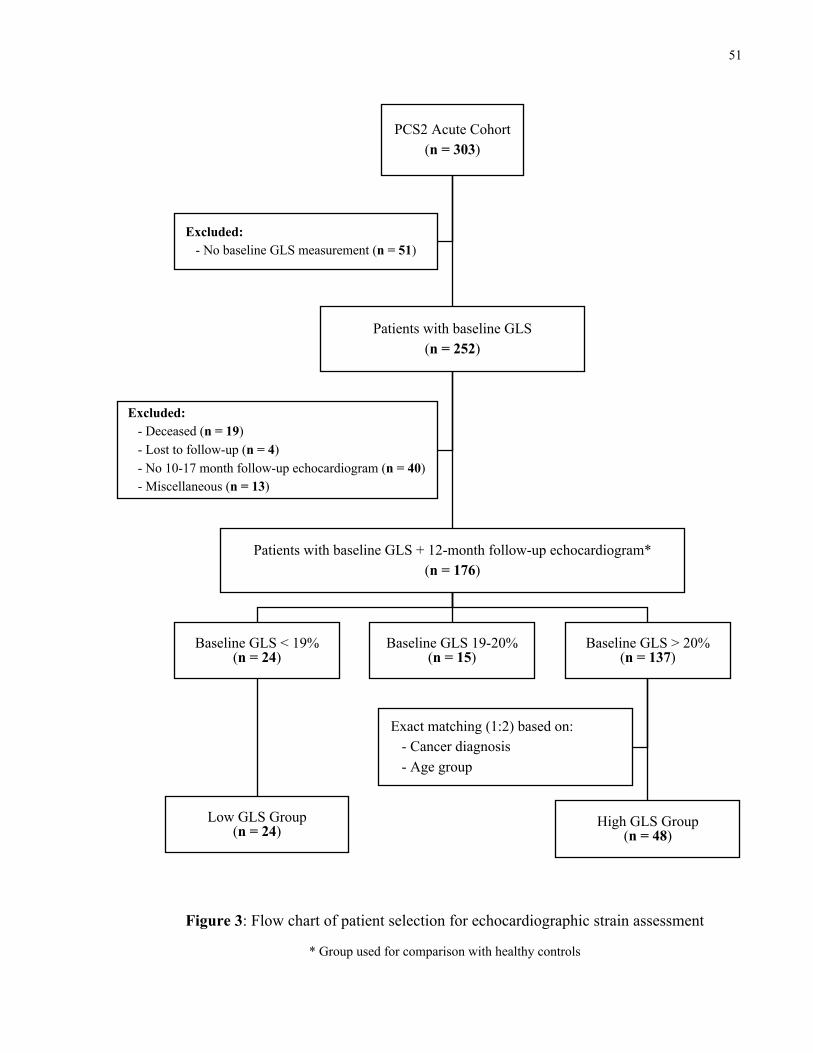
51
PCS2 Acute Cohort (n = 303)
Patients with baseline GLS(n = 252)
Patients with baseline GLS + 12-month follow-up echocardiogram*(n = 176)
Baseline GLS < 19%(n = 24)
Low GLS Group(n = 24)
a
Baseline GLS 19-20%(n = 15)
Baseline GLS > 20%(n = 137)
High GLS Group(n = 48)
a
Exact matching (1:2) based on:- Cancer diagnosis- Age group
Excluded:- Deceased (n = 19)- Lost to follow-up (n = 4)- No 10-17 month follow-up echocardiogram (n = 40) - Miscellaneous (n = 13)
Excluded:- No baseline GLS measurement (n = 51)
Figure 3: Flow chart of patient selection for echocardiographic strain assessment
* Group used for comparison with healthy controls
52
3.5 Cardiac Biomarkers Assessment
As a sub-analysis, we explored whether there are any relationships between cardiac biomarkers
measured prior to anthracycline exposure and echocardiographic parameters assessed before,
during, and after anthracycline chemotherapy in pediatric cancer patients. The two biomarkers
selected for investigation in the present study were N-terminal pro B-type natriuretic peptide
(NT-proBNP) and high sensitivity troponin T (hs-TnT). Serum samples (5-8 mL) were collected
at baseline and other pre-specified time points from consenting patients (Figure 1), and stored at
-80°C until assay testing. Analyses of individual biomarker levels were carried out using
appropriate ELISA assays, in accordance to the standardized procedures set out by the
Biomarkers Core of the PCS2 study (see Section 3.2.3). The NT-proBNP assay (Roche
Diagnostics) employed for analysis has a detection range of 5 to 35,000 pg/mL (Roche
Diagnostics 2019b). The hs-TnT assay (Roche Diagnostics) used has a detection limit of 3
pg/mL, a 99th percentile upper reference limit of 14 pg/mL, and a 10% coefficient of variation
precision of 13 pg/mL (Roche Diagnostics 2019a).
Patient selection for the NT-proBNP and hs-TnT analyses is illustrated in Figure 4 and Figure 5
respectively. Of the 255 Acute Cohort patients enrolled at The Hospital for Sick Children, 173
(67.8%) had consented and provided serum samples for our biomarker studies. A total of 95
biospecimen samples have been analyzed to date.
NT-proBNP Assessment
Of the 95 serum samples assayed, four patient samples were excluded due to missing NT-
proBNP measurements. Consequently, we had a total of 91 baseline NT-proBNP measurements
that were obtained from patient serum samples collected prior to the first dose of anthracycline
chemotherapy. NT-proBNP concentrations at baseline were compared across cancer diagnosis
groups in the Acute Cohort and against the reference CALIPER cohort (described in Section
3.3.1). In order to examine how NT-proBNP levels change after exposure to anthracycline
chemotherapy, we further identified patients who had provided serum samples for biomarker
53
analysis at both the baseline and the 12-month follow-up study visits (n = 54). NT-proBNP
concentrations were compared between the two time points.
To address whether abnormalities in NT-proBNP levels prior to anthracycline administration can
predict echocardiographic findings of sub-clinical cardiac dysfunction after anthracycline
exposure in pediatric cancer patients, we also assessed the relation between NT-proBNP levels at
baseline and echocardiographic parameters of cardiac function including LVEF, GLS, and CS,
measured at baseline, end-treatment, and 12 months post-anthracycline treatment. There were 68
patients who had both a baseline NT-proBNP measurement and a 12-month follow-up
echocardiogram performed. Similarly, 64 patients with baseline NT-proBNP values had an end-
treatment echocardiogram completed within 0 to 45 days prior to the last dose of anthracycline
chemotherapy (Figure 4).
Hs-TnT Assessment
Baseline hs-TnT measurements were obtained from a total of 57 patient serum samples (Figure
5). Assessment of hs-TnT levels followed the same analysis plan as described above for NT-
proBNP. Baseline hs-TnT concentrations were first compared across cancer diagnosis groups
among Acute Cohort patients, and then compared against CALIPER patients. The trajectory of
change in hs-TnT concentration after anthracycline chemotherapy was also examined. Finally,
the association between baseline hs-TnT levels and cardiac function assessed before, during, and
after anthracycline treatment was explored.
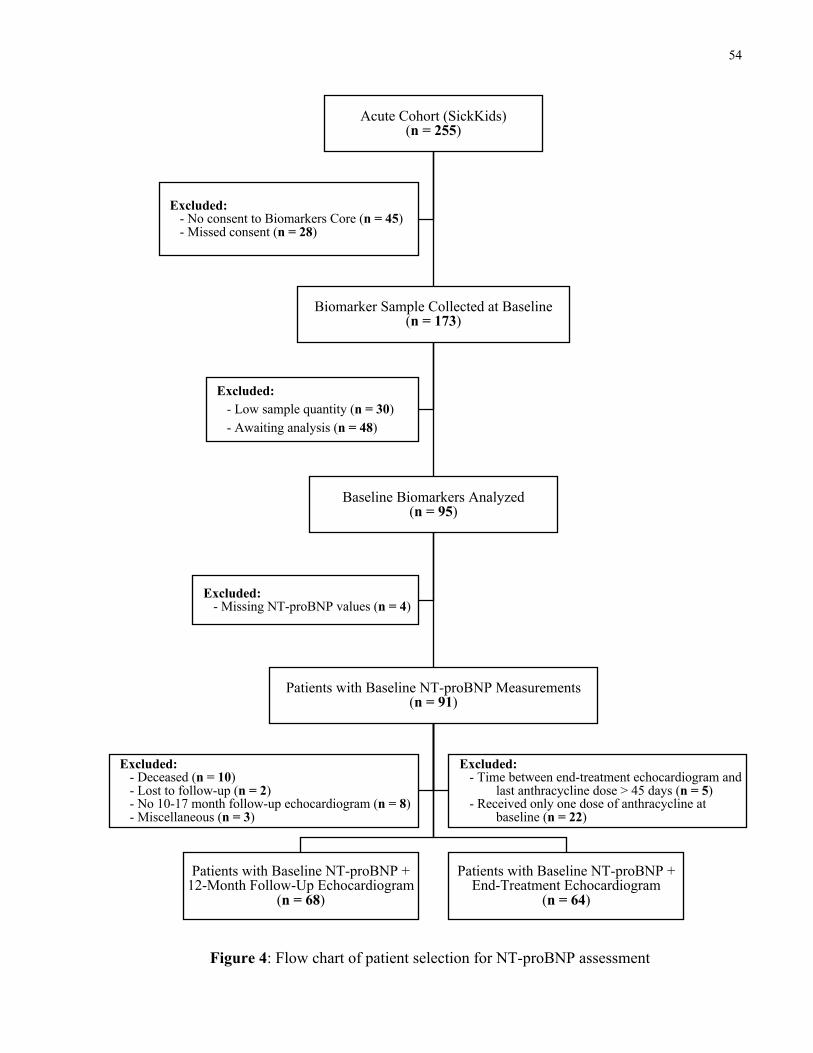
54
Figure 4: Flow chart of patient selection for NT-proBNP assessment
Acute Cohort (SickKids)(n = 255)
Biomarker Sample Collected at Baseline(n = 173)
Baseline Biomarkers Analyzed(n = 95)
Patients with Baseline NT-proBNP Measurements(n = 91)
Patients with Baseline NT-proBNP + 12-Month Follow-Up Echocardiogram
(n = 68)
Patients with Baseline NT-proBNP + End-Treatment Echocardiogram
(n = 64)
Excluded:- Deceased (n = 10)- Lost to follow-up (n = 2)- No 10-17 month follow-up echocardiogram (n = 8)- Miscellaneous (n = 3)
Excluded:- Time between end-treatment echocardiogram and
last anthracycline dose > 45 days (n = 5)- Received only one dose of anthracycline at
baseline (n = 22)
Excluded:- Missing NT-proBNP values (n = 4)
Excluded: - Low sample quantity (n = 30)- Awaiting analysis (n = 48)
Excluded:- No consent to Biomarkers Core (n = 45)- Missed consent (n = 28)
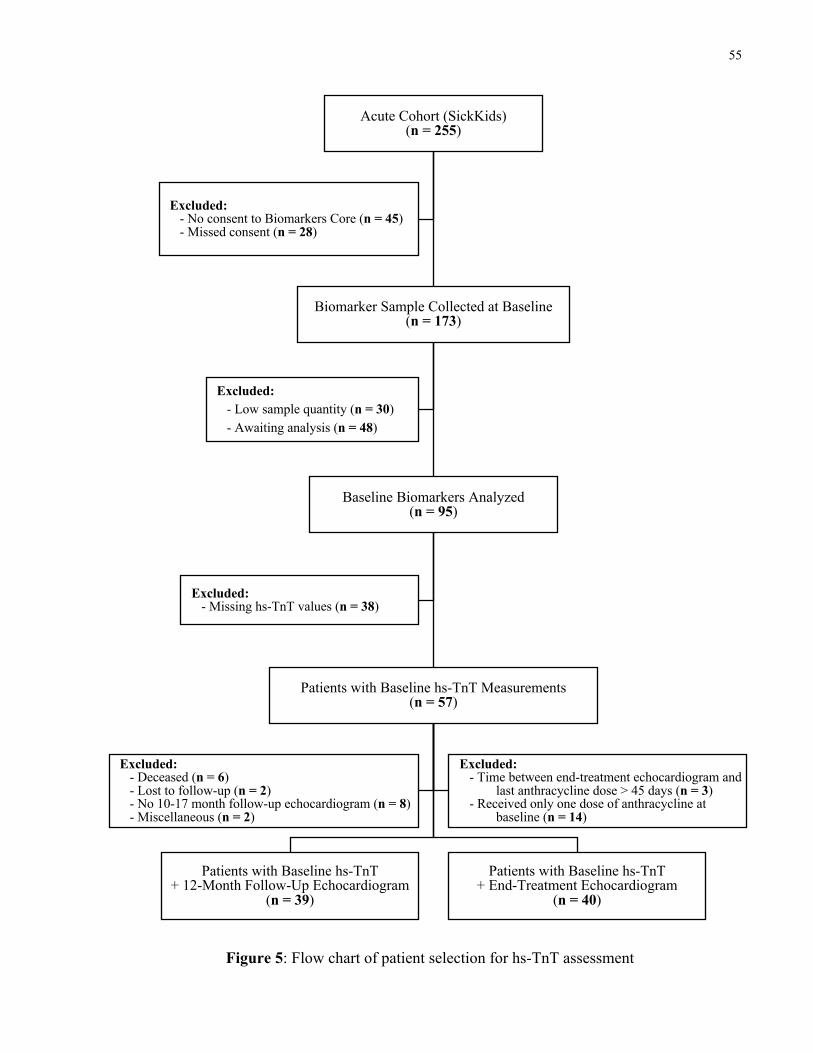
55
Acute Cohort (SickKids)(n = 255)
Biomarker Sample Collected at Baseline(n = 173)
Baseline Biomarkers Analyzed(n = 95)
Patients with Baseline hs-TnT Measurements(n = 57)
Patients with Baseline hs-TnT+ 12-Month Follow-Up Echocardiogram
(n = 39)
Patients with Baseline hs-TnT+ End-Treatment Echocardiogram
(n = 40)
Excluded:- Deceased (n = 6)- Lost to follow-up (n = 2)- No 10-17 month follow-up echocardiogram (n = 8)- Miscellaneous (n = 2)
Excluded:- Time between end-treatment echocardiogram and
last anthracycline dose > 45 days (n = 3)- Received only one dose of anthracycline at
baseline (n = 14)
Excluded:- Missing hs-TnT values (n = 38)
Excluded: - Low sample quantity (n = 30)- Awaiting analysis (n = 48)
Excluded:- No consent to Biomarkers Core (n = 45)- Missed consent (n = 28)
Figure 5: Flow chart of patient selection for hs-TnT assessment
56
3.6 Statistical Analysis
All data were analyzed using R version 3.4.2. The mean and standard deviation were reported for
continuous variables with normal distributions. Median values with their corresponding
interquartile ranges (IQRs) were reported for continuous variables with non-normal distributions.
Differences in demographics and clinical characteristics were assessed using chi-squared tests or
Fisher’s exact tests for categorical variables. Continuous variables were analyzed using t-tests,
analysis of variance (ANOVA) tests, Mann-Whitney U tests, and Kruskal Wallis tests. Where
applicable, post-hoc analyses were conducted in variables with more than two groups to discern
comparisons that were statistically significant. Matched-pair analyses were used for comparisons
between matched pairs. Additionally, spearman’s rank correlation was used to evaluate the
association between functional parameters, strain measurements, and cardiac biomarker levels.
Univariate and multivariate regressions, as well as spline regressions (Mulla 2007) were also
performed to further explore the association between various echocardiographic parameters as
well as candidate cardiac biomarkers. Spline regression is a statistical modeling technique where
a combination of linear or polynomial functions are used to fit a given dataset. In spline
regression, the dataset is first divided into multiple bins and a separate model is fitted for each
individual bin. All polynomials are then pieced together and smoothed to generate a continuous
polynomial regression line for the given dataset. This technique has the advantage of creating a
model with a better fit for the data than ordinary linear or polynomial regression lines while also
avoiding over-fitting, which is a common drawback of polynomial regressions. Beta coefficients
and their respective 95% confidence intervals (95% CI) were reported for each regression
analysis. R-squared (R2) values were also reported to show the percentage of the response
variable that was explained by a given linear model. Missing values were excluded from
analysis. A p value of less than 0.05 was considered to be statistically significant.
57
Development of Age and Sex-Adjusted z-score Models for Cardiac Biomarker
Assessment
At present, there are only age-specific reference ranges for NT-proBNP in the pediatric
population (Albers et al. 2006), and none that also take into consideration the sex of the child. As
previously described, several studies have demonstrated sex differences in the prognostic value
of NT-proBNP (Leosdottir et al. 2011; Kim et al. 2017). Therefore, it becomes important to
account for both age and sex while evaluating serum biomarker levels and their predictive value.
To address this shortcoming, we developed age and sex-adjusted z-score models for each of the
two cardiac biomarkers using data from the CALIPER cohort. Based on the healthy reference
data from the CALIPER project, z-score models were generated using the Generalized Additive
Models for Location Scale and Shape (GAMLSS) R package developed by Rigby and
Stasinopoulos (Rigby and Stasinopoulos 2005).
The GAMLSS framework is a flexible statistical modeling technique that is capable of fitting a
variety of different distributions based on a given response variable (Y) (Rigby et al. 2017). For a
given random continuous variable Y, its range can be denoted as RY and can vary anywhere
between -∞ to ∞. The theoretical probability density function used by the GAMLSS method is
denoted as f (y | q), where the parameter vector q denotes a family of parameters. Often, up to
four parameters are included in the GAMLSS family of distributions, and are denoted as qT = (µ,
s, n, t). The µ, s, n, and t parameters describe the location, scale, skewness and kurtosis of the
distribution respectively, and together, the parameters determine the overall shape of the model
distributions. A location parameter (µ) represents the ‘center’ of the distribution and can refer to
the mean, median, or mode in the probability density function. A scale parameter (s) describes
the spread of the distribution. A skewness parameter (n) is related to the measure of asymmetry
in a distribution where distributions with a longer tail to the right than the left are considered to
be positively skewed, while ones with a longer tail to the left are considered to be negatively
skewed. A symmetrical distribution is considered to have zero skewness. A kurtosis (t)
parameter is a measure of how ‘heavy’ or ‘wide’ the distribution tails are relative to a normal
distribution. For example, a distribution with wider tails than a normal distribution is considered
to have high kurtosis, whereas those with thinner tails generally have low kurtosis.
58
Given the RY and the family of distribution (qT), the GAMLSS framework can devise a
regression model along with a z score equation that are most appropriate for a given dataset. A
large number of explicit continuous distributions are available for implementation in the
GAMLSS software package and are listed in Table 3 (Rigby et al. 2017). The GAMLSS family
of distributions used to develop our z-score models are summarized in Table 4. Once the final z-
score models were generated, the biomarker data from our Acute Cohort patients were inputted
to obtain age- and sex-adjusted z-score values for both NT-proBNP and hs-TnT. The exact same
analyses described in Section 3.5 were repeated using z-score values.
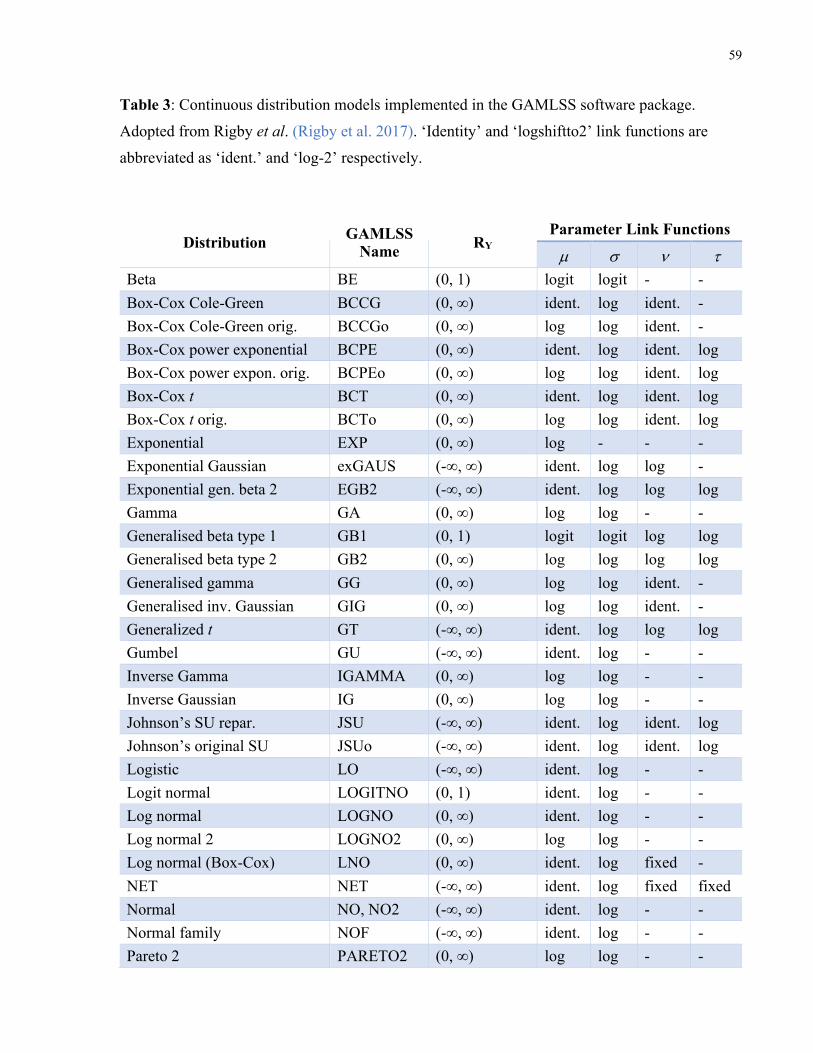
59
Table 3: Continuous distribution models implemented in the GAMLSS software package.
Adopted from Rigby et al. (Rigby et al. 2017). ‘Identity’ and ‘logshiftto2’ link functions are
abbreviated as ‘ident.’ and ‘log-2’ respectively.
Distribution GAMLSS Name RY
Parameter Link Functions
µ s n t Beta BE (0, 1) logit logit - - Box-Cox Cole-Green BCCG (0, ∞) ident. log ident. - Box-Cox Cole-Green orig. BCCGo (0, ∞) log log ident. - Box-Cox power exponential BCPE (0, ∞) ident. log ident. log Box-Cox power expon. orig. BCPEo (0, ∞) log log ident. log Box-Cox t BCT (0, ∞) ident. log ident. log Box-Cox t orig. BCTo (0, ∞) log log ident. log Exponential EXP (0, ∞) log - - - Exponential Gaussian exGAUS (-∞, ∞) ident. log log - Exponential gen. beta 2 EGB2 (-∞, ∞) ident. log log log Gamma GA (0, ∞) log log - - Generalised beta type 1 GB1 (0, 1) logit logit log log Generalised beta type 2 GB2 (0, ∞) log log log log Generalised gamma GG (0, ∞) log log ident. - Generalised inv. Gaussian GIG (0, ∞) log log ident. - Generalized t GT (-∞, ∞) ident. log log log Gumbel GU (-∞, ∞) ident. log - - Inverse Gamma IGAMMA (0, ∞) log log - - Inverse Gaussian IG (0, ∞) log log - - Johnson’s SU repar. JSU (-∞, ∞) ident. log ident. log Johnson’s original SU JSUo (-∞, ∞) ident. log ident. log Logistic LO (-∞, ∞) ident. log - - Logit normal LOGITNO (0, 1) ident. log - - Log normal LOGNO (0, ∞) ident. log - - Log normal 2 LOGNO2 (0, ∞) log log - - Log normal (Box-Cox) LNO (0, ∞) ident. log fixed - NET NET (-∞, ∞) ident. log fixed fixed Normal NO, NO2 (-∞, ∞) ident. log - - Normal family NOF (-∞, ∞) ident. log - - Pareto 2 PARETO2 (0, ∞) log log - -
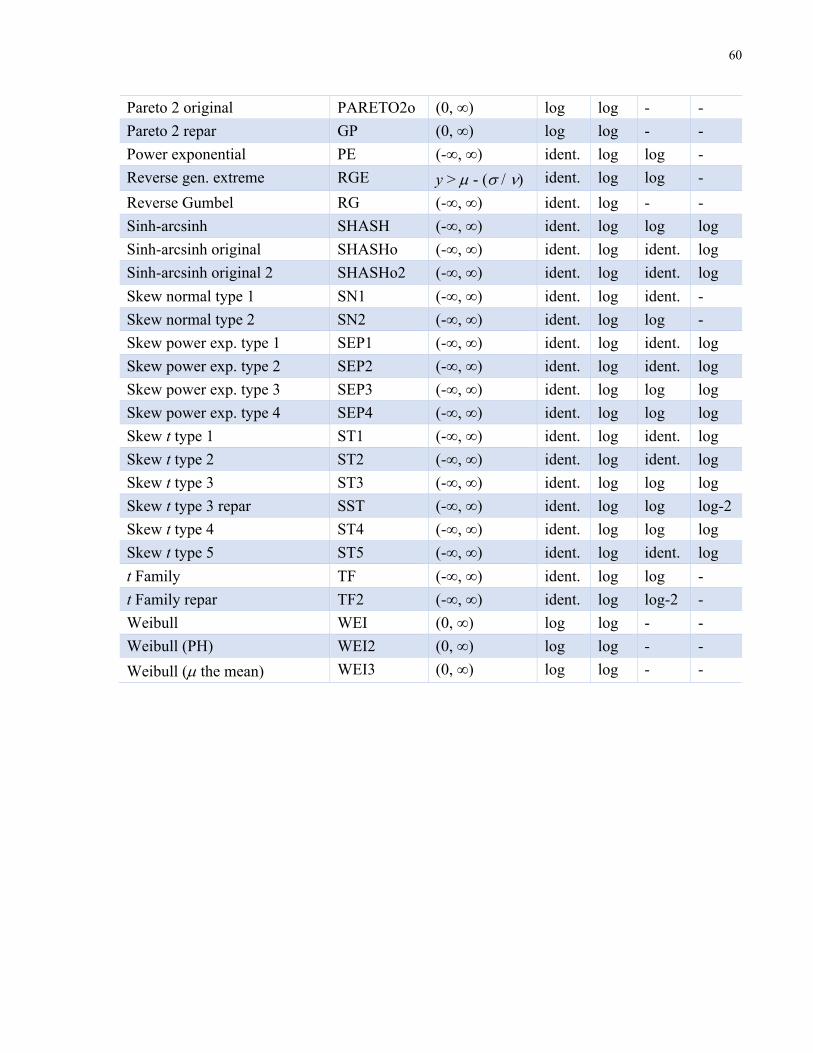
60
Pareto 2 original PARETO2o (0, ∞) log log - - Pareto 2 repar GP (0, ∞) log log - - Power exponential PE (-∞, ∞) ident. log log - Reverse gen. extreme RGE y > µ - (s / n) ident. log log - Reverse Gumbel RG (-∞, ∞) ident. log - - Sinh-arcsinh SHASH (-∞, ∞) ident. log log log Sinh-arcsinh original SHASHo (-∞, ∞) ident. log ident. log Sinh-arcsinh original 2 SHASHo2 (-∞, ∞) ident. log ident. log Skew normal type 1 SN1 (-∞, ∞) ident. log ident. - Skew normal type 2 SN2 (-∞, ∞) ident. log log - Skew power exp. type 1 SEP1 (-∞, ∞) ident. log ident. log Skew power exp. type 2 SEP2 (-∞, ∞) ident. log ident. log Skew power exp. type 3 SEP3 (-∞, ∞) ident. log log log Skew power exp. type 4 SEP4 (-∞, ∞) ident. log log log Skew t type 1 ST1 (-∞, ∞) ident. log ident. log Skew t type 2 ST2 (-∞, ∞) ident. log ident. log Skew t type 3 ST3 (-∞, ∞) ident. log log log Skew t type 3 repar SST (-∞, ∞) ident. log log log-2 Skew t type 4 ST4 (-∞, ∞) ident. log log log Skew t type 5 ST5 (-∞, ∞) ident. log ident. log t Family TF (-∞, ∞) ident. log log - t Family repar TF2 (-∞, ∞) ident. log log-2 - Weibull WEI (0, ∞) log log - - Weibull (PH) WEI2 (0, ∞) log log - - Weibull (µ the mean) WEI3 (0, ∞) log log - -
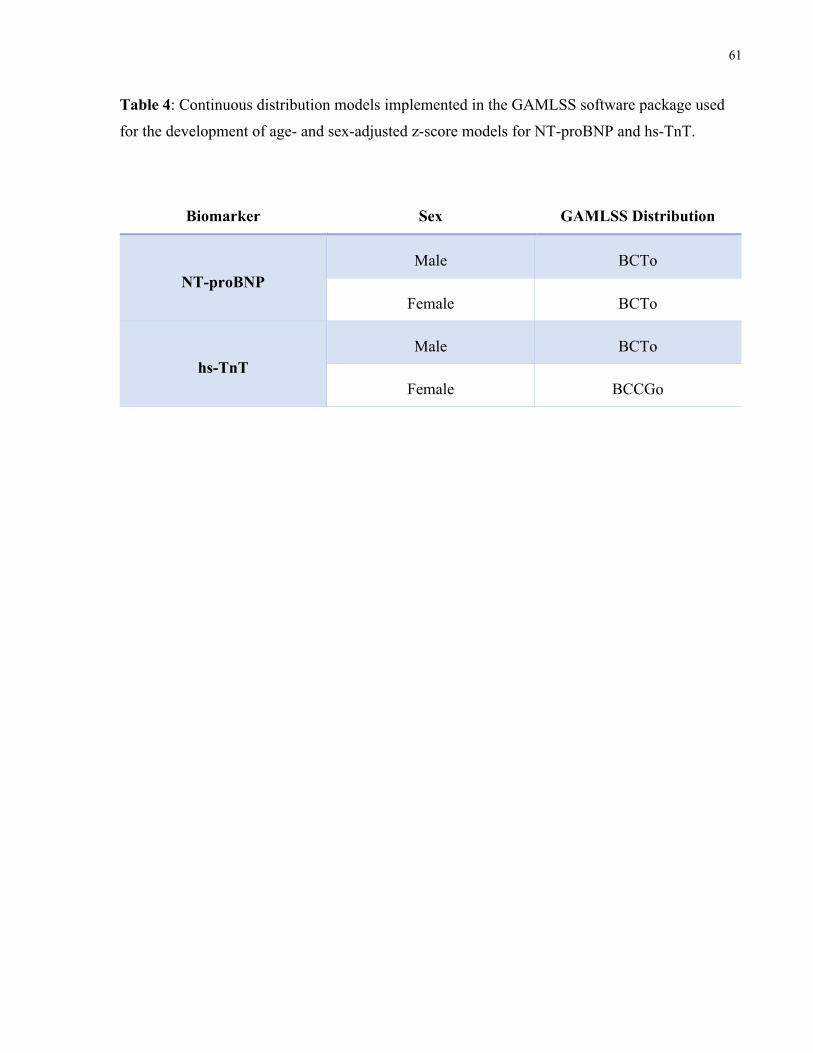
61
Table 4: Continuous distribution models implemented in the GAMLSS software package used
for the development of age- and sex-adjusted z-score models for NT-proBNP and hs-TnT.
Biomarker Sex GAMLSS Distribution
NT-proBNP Male BCTo
Female BCTo
hs-TnT Male BCTo
Female BCCGo
62
Results
4.1 Baseline Characteristics
Baseline clinical and echocardiographic characteristics of the study cohort are summarized in
Table 5. The median age at baseline was 9.0 years (IQR: 4.5 – 14.1) and 73 subjects (41.5%)
were female. The majority of patients had leukemia (n = 78, 44.3%), 51 (29.0%) had lymphoma,
28 (15.9%) had bone or soft tissue sarcoma, and 19 (10.8%) had other embryonal tumors such as
neuroblastoma, hepatoblastoma, and Wilms tumor. A total of 50 patients (28.4%) had a history
of other non-anthracycline chemotherapy. Echocardiographic parameters of cardiac function
were normal at baseline, with mean LVEF, GLS, and CS measurements of 64.0 ± 5.7%, 22.1 ±
2.8%, and 20.0 ± 3.2% respectively. Patients proceeded to receive a median cumulative
anthracycline dose of 149 mg/m2 (IQR: 75 – 202) and 32 patients (18.2%) received concomitant
dexrazoxane during their anthracycline treatment.
A total of 151 healthy pediatric controls without heart disease were recruited and included in the
present study. In comparison to the controls, the patient cohort was younger (9.0 [IQR: 4.5 –
14.1] versus 12.3 [IQR: 6.1 – 15.1] years, p=0.004) at baseline (Table 6). Overall, no significant
differences were detected for both GLS and CS between patients and controls. Even when age
was taken into consideration, no difference in strain measurements was observed across all age
quartiles (Figure 6), with the exception of CS being lower in patients of the youngest age quartile
compared to the controls (19.5 ± 2.6% versus 21.9 ± 2.3%, p=0.001).
When baseline cardiac function was compared between the four cancer diagnosis groups
alongside the controls, statistically significant differences were observed in all echocardiographic
measurements including LVEF, GLS, and CS (Table 7a). Post-hoc analysis using the Tukey
method (Table 7b) revealed lymphoma patients to have lower LVEF at baseline than leukemia
patients (62.1 ± 5.8% versus 65.2 ± 5.5%, p=0.012). Similarly, lymphoma and bone/soft tissue
sarcoma patients had lower baseline GLS than leukemia patients. GLS was also lower in the
control cohort compared to leukemia patients (21.8 ± 2.1% versus 23.1 ± 2.4%, p=0.002). In
contrast, healthy controls had a higher CS relative to lymphoma patients at baseline (20.6 ± 2.6%
63
versus 19.2 ± 3.6%, p=0.039), while no other statistically significant differences in CS were
observed between the four cancer diagnosis groups.
To ensure that the 176 patients included in our study were representative of the entire Acute
Cohort of the PCS2 study in terms of baseline characteristics, we also compared the baseline
clinical and echocardiographic characteristics between those included for analyses and the 127
Acute Cohort patients who were excluded due to aforementioned reasons (see Section 3.4 for
details). The results are depicted in Table 8. Patients who were included in the present study
were older than those who were excluded (9.0 [IQR: 4.5 – 14.1] versus 5.9 [IQR: 3.1 – 13.4]
years), but the age difference between the two groups did not achieve statistical significance
(p=0.051). The distribution of sex and cancer diagnoses were similar between the two groups, as
well as the cumulative anthracycline dose received by the two groups (all p > 0.05). Furthermore,
no difference in terms of baseline cardiac function was detected between the two groups.
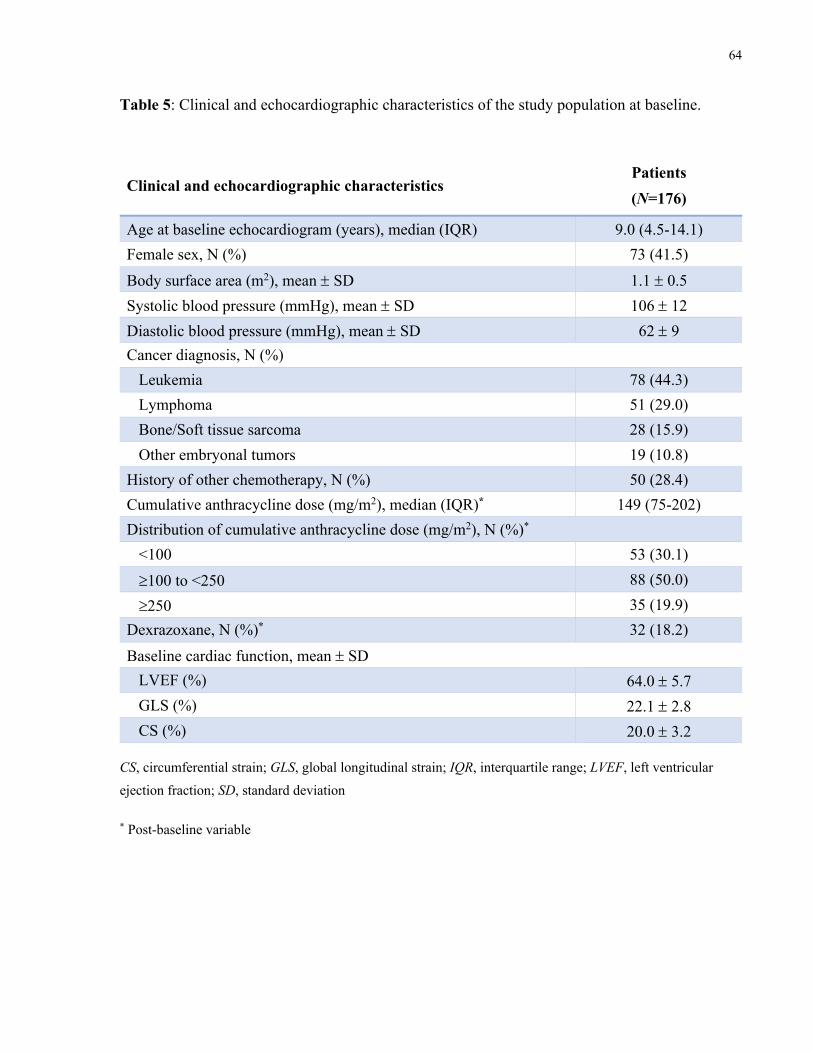
64
Table 5: Clinical and echocardiographic characteristics of the study population at baseline.
Clinical and echocardiographic characteristics Patients (N=176)
Age at baseline echocardiogram (years), median (IQR) 9.0 (4.5-14.1) Female sex, N (%) 73 (41.5) Body surface area (m2), mean ± SD 1.1 ± 0.5 Systolic blood pressure (mmHg), mean ± SD 106 ± 12 Diastolic blood pressure (mmHg), mean ± SD 62 ± 9 Cancer diagnosis, N (%) Leukemia 78 (44.3) Lymphoma 51 (29.0) Bone/Soft tissue sarcoma 28 (15.9) Other embryonal tumors 19 (10.8) History of other chemotherapy, N (%) 50 (28.4) Cumulative anthracycline dose (mg/m2), median (IQR)* 149 (75-202) Distribution of cumulative anthracycline dose (mg/m2), N (%)* <100 53 (30.1) ³100 to <250 88 (50.0) ³250 35 (19.9) Dexrazoxane, N (%)* 32 (18.2) Baseline cardiac function, mean ± SD LVEF (%) 64.0 ± 5.7 GLS (%) 22.1 ± 2.8 CS (%) 20.0 ± 3.2
CS, circumferential strain; GLS, global longitudinal strain; IQR, interquartile range; LVEF, left ventricular ejection fraction; SD, standard deviation
* Post-baseline variable
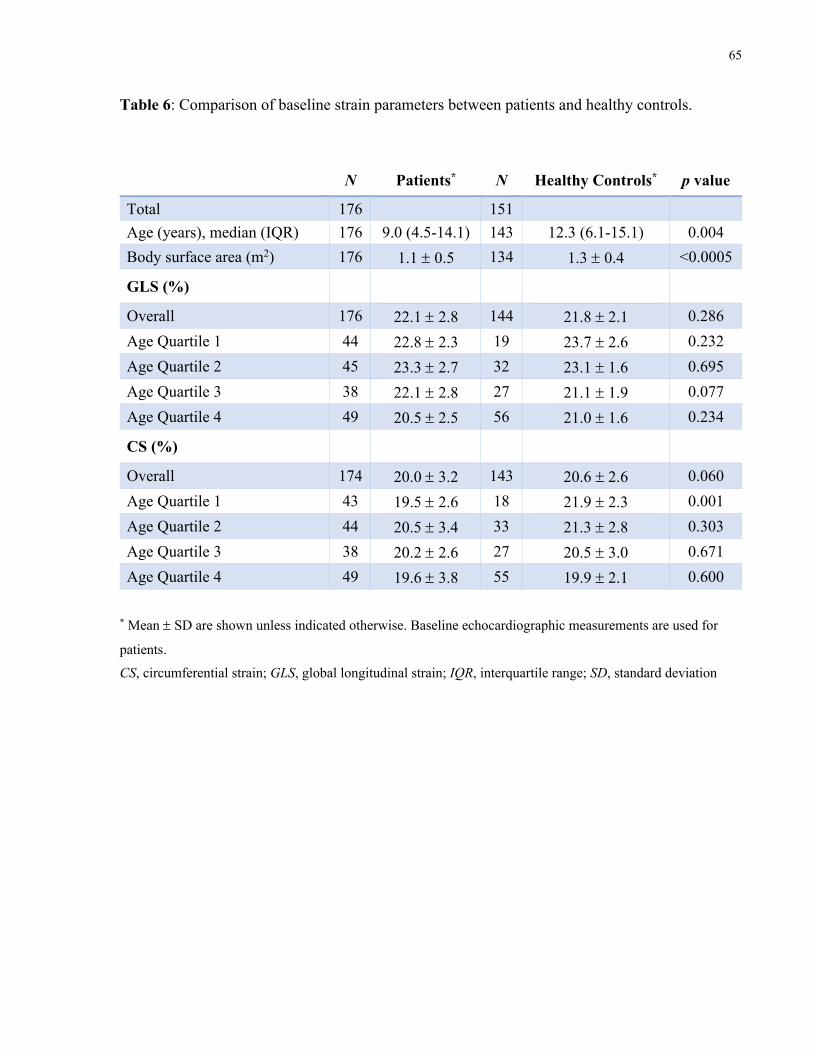
65
Table 6: Comparison of baseline strain parameters between patients and healthy controls.
N Patients* N Healthy Controls* p value
Total 176 151 Age (years), median (IQR) 176 9.0 (4.5-14.1) 143 12.3 (6.1-15.1) 0.004 Body surface area (m2) 176 1.1 ± 0.5 134 1.3 ± 0.4 <0.0005
GLS (%)
Overall 176 22.1 ± 2.8 144 21.8 ± 2.1 0.286 Age Quartile 1 44 22.8 ± 2.3 19 23.7 ± 2.6 0.232 Age Quartile 2 45 23.3 ± 2.7 32 23.1 ± 1.6 0.695 Age Quartile 3 38 22.1 ± 2.8 27 21.1 ± 1.9 0.077 Age Quartile 4 49 20.5 ± 2.5 56 21.0 ± 1.6 0.234
CS (%)
Overall 174 20.0 ± 3.2 143 20.6 ± 2.6 0.060 Age Quartile 1 43 19.5 ± 2.6 18 21.9 ± 2.3 0.001 Age Quartile 2 44 20.5 ± 3.4 33 21.3 ± 2.8 0.303 Age Quartile 3 38 20.2 ± 2.6 27 20.5 ± 3.0 0.671 Age Quartile 4 49 19.6 ± 3.8 55 19.9 ± 2.1 0.600
* Mean ± SD are shown unless indicated otherwise. Baseline echocardiographic measurements are used for
patients.
CS, circumferential strain; GLS, global longitudinal strain; IQR, interquartile range; SD, standard deviation
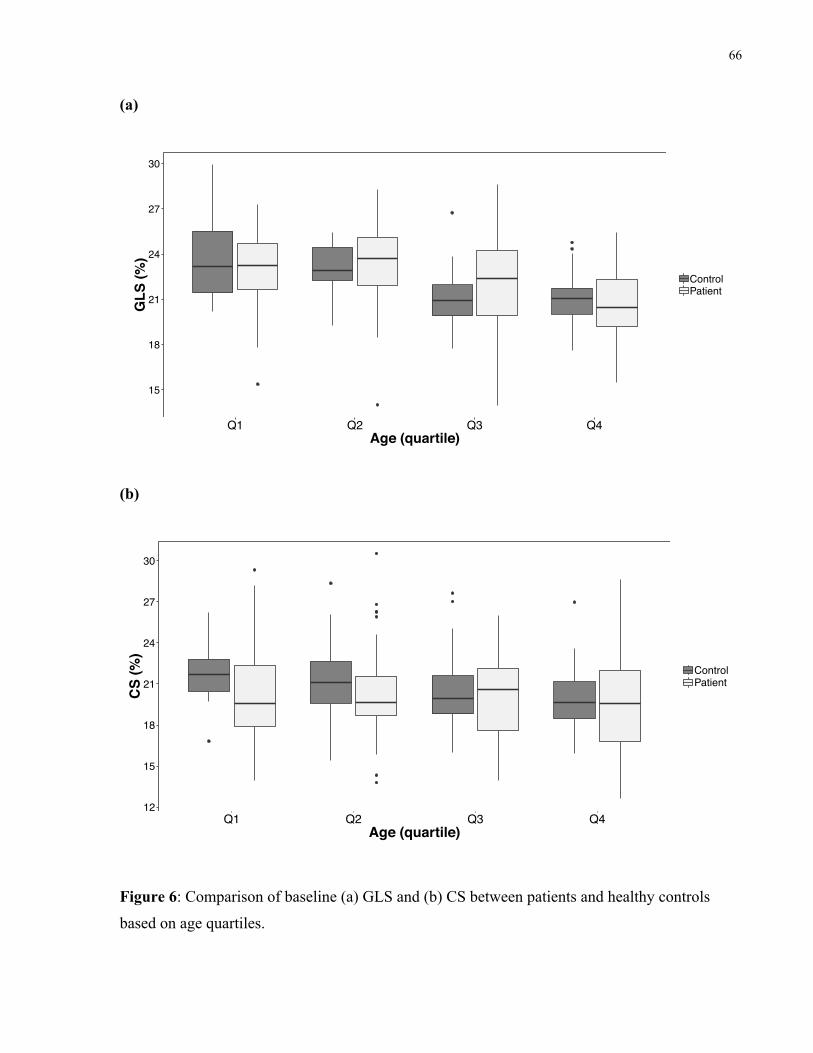
66
(a)
(b)
Figure 6: Comparison of baseline (a) GLS and (b) CS between patients and healthy controls
based on age quartiles.
15
18
21
24
27
30
Q1 Q2 Q3 Q4Age (quartile)
GLS
(%)
ControlPatient
12
15
18
21
24
27
30
Q1 Q2 Q3 Q4Age (quartile)
CS
(%)
ControlPatient
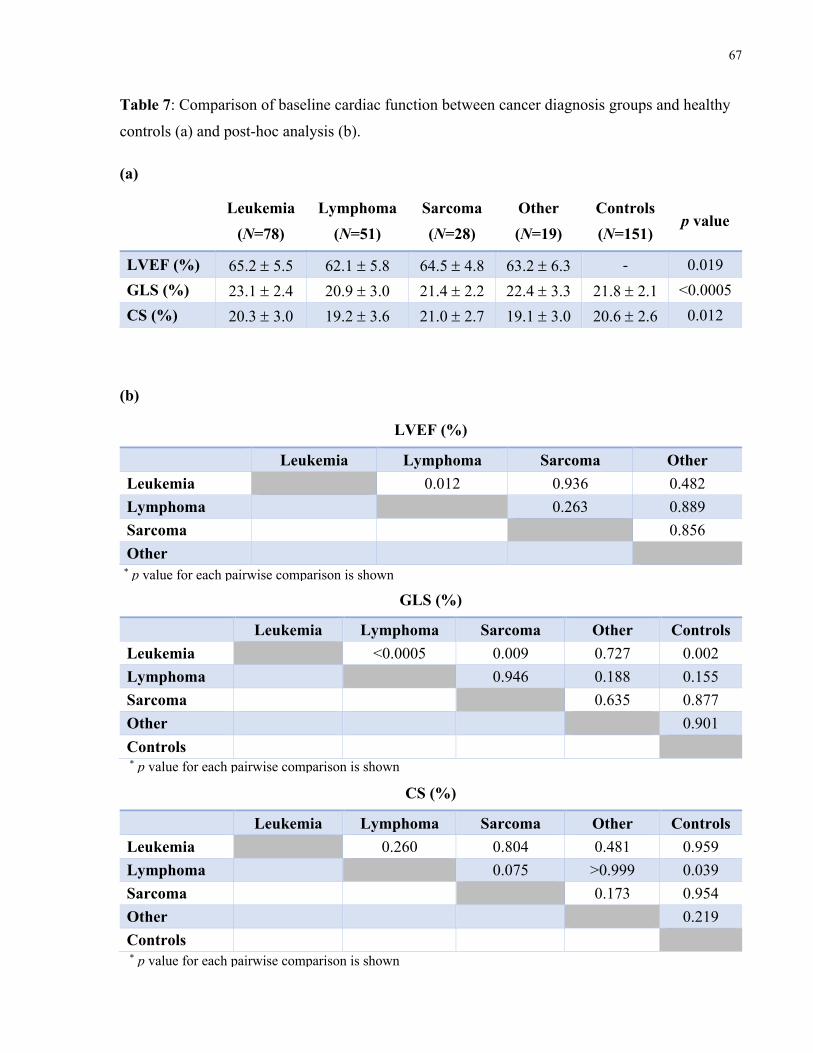
67
Table 7: Comparison of baseline cardiac function between cancer diagnosis groups and healthy
controls (a) and post-hoc analysis (b).
(a)
Leukemia
(N=78) Lymphoma
(N=51) Sarcoma (N=28)
Other (N=19)
Controls (N=151)
p value
LVEF (%) 65.2 ± 5.5 62.1 ± 5.8 64.5 ± 4.8 63.2 ± 6.3 - 0.019 GLS (%) 23.1 ± 2.4 20.9 ± 3.0 21.4 ± 2.2 22.4 ± 3.3 21.8 ± 2.1 <0.0005 CS (%) 20.3 ± 3.0 19.2 ± 3.6 21.0 ± 2.7 19.1 ± 3.0 20.6 ± 2.6 0.012
(b)
LVEF (%)
Leukemia Lymphoma Sarcoma Other Leukemia 0.012 0.936 0.482 Lymphoma 0.263 0.889 Sarcoma 0.856 Other
GLS (%)
Leukemia Lymphoma Sarcoma Other Controls Leukemia <0.0005 0.009 0.727 0.002 Lymphoma 0.946 0.188 0.155 Sarcoma 0.635 0.877 Other 0.901 Controls
CS (%)
Leukemia Lymphoma Sarcoma Other Controls Leukemia 0.260 0.804 0.481 0.959 Lymphoma 0.075 >0.999 0.039 Sarcoma 0.173 0.954 Other 0.219 Controls
* p value for each pairwise comparison is shown
* p value for each pairwise comparison is shown
* p value for each pairwise comparison is shown
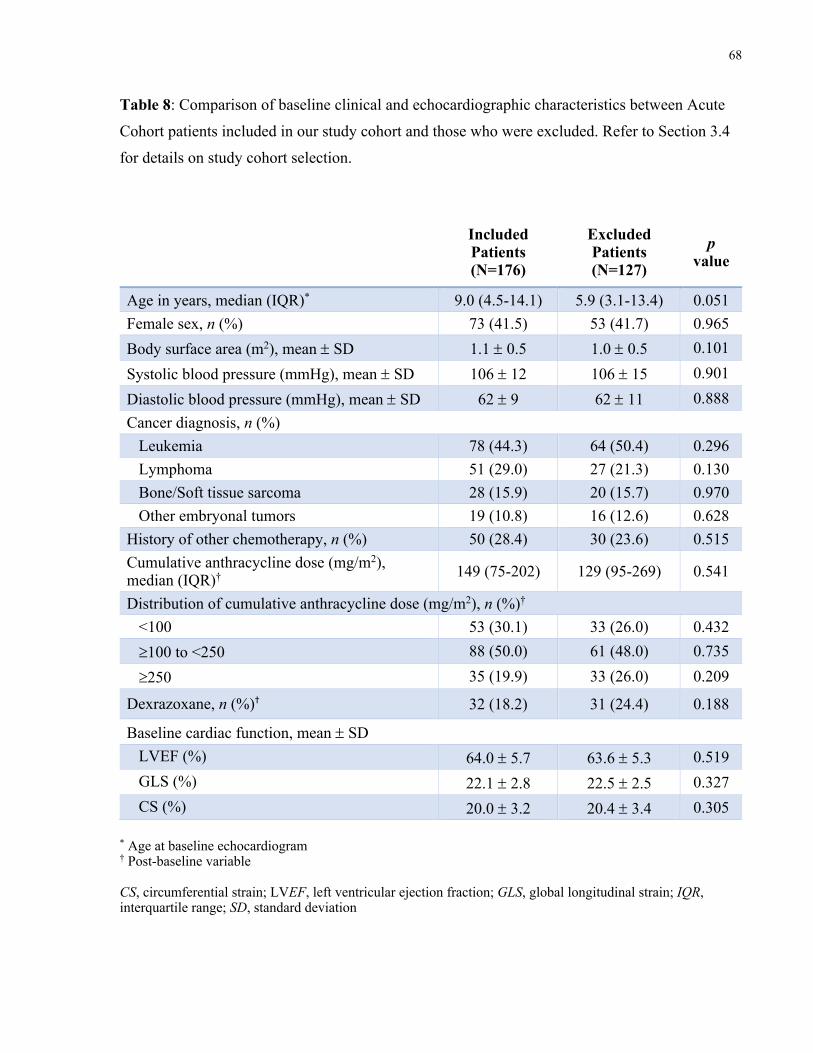
68
Table 8: Comparison of baseline clinical and echocardiographic characteristics between Acute
Cohort patients included in our study cohort and those who were excluded. Refer to Section 3.4
for details on study cohort selection.
Included Patients (N=176)
Excluded Patients (N=127)
p value
Age in years, median (IQR)* 9.0 (4.5-14.1) 5.9 (3.1-13.4) 0.051 Female sex, n (%) 73 (41.5) 53 (41.7) 0.965 Body surface area (m2), mean ± SD 1.1 ± 0.5 1.0 ± 0.5 0.101 Systolic blood pressure (mmHg), mean ± SD 106 ± 12 106 ± 15 0.901 Diastolic blood pressure (mmHg), mean ± SD 62 ± 9 62 ± 11 0.888 Cancer diagnosis, n (%) Leukemia 78 (44.3) 64 (50.4) 0.296 Lymphoma 51 (29.0) 27 (21.3) 0.130 Bone/Soft tissue sarcoma 28 (15.9) 20 (15.7) 0.970 Other embryonal tumors 19 (10.8) 16 (12.6) 0.628 History of other chemotherapy, n (%) 50 (28.4) 30 (23.6) 0.515 Cumulative anthracycline dose (mg/m2), median (IQR)† 149 (75-202) 129 (95-269) 0.541
Distribution of cumulative anthracycline dose (mg/m2), n (%)† <100 53 (30.1) 33 (26.0) 0.432 ³100 to <250 88 (50.0) 61 (48.0) 0.735 ³250 35 (19.9) 33 (26.0) 0.209
Dexrazoxane, n (%)† 32 (18.2) 31 (24.4) 0.188
Baseline cardiac function, mean ± SD LVEF (%) 64.0 ± 5.7 63.6 ± 5.3 0.519 GLS (%) 22.1 ± 2.8 22.5 ± 2.5 0.327 CS (%) 20.0 ± 3.2 20.4 ± 3.4 0.305
* Age at baseline echocardiogram † Post-baseline variable CS, circumferential strain; LVEF, left ventricular ejection fraction; GLS, global longitudinal strain; IQR, interquartile range; SD, standard deviation
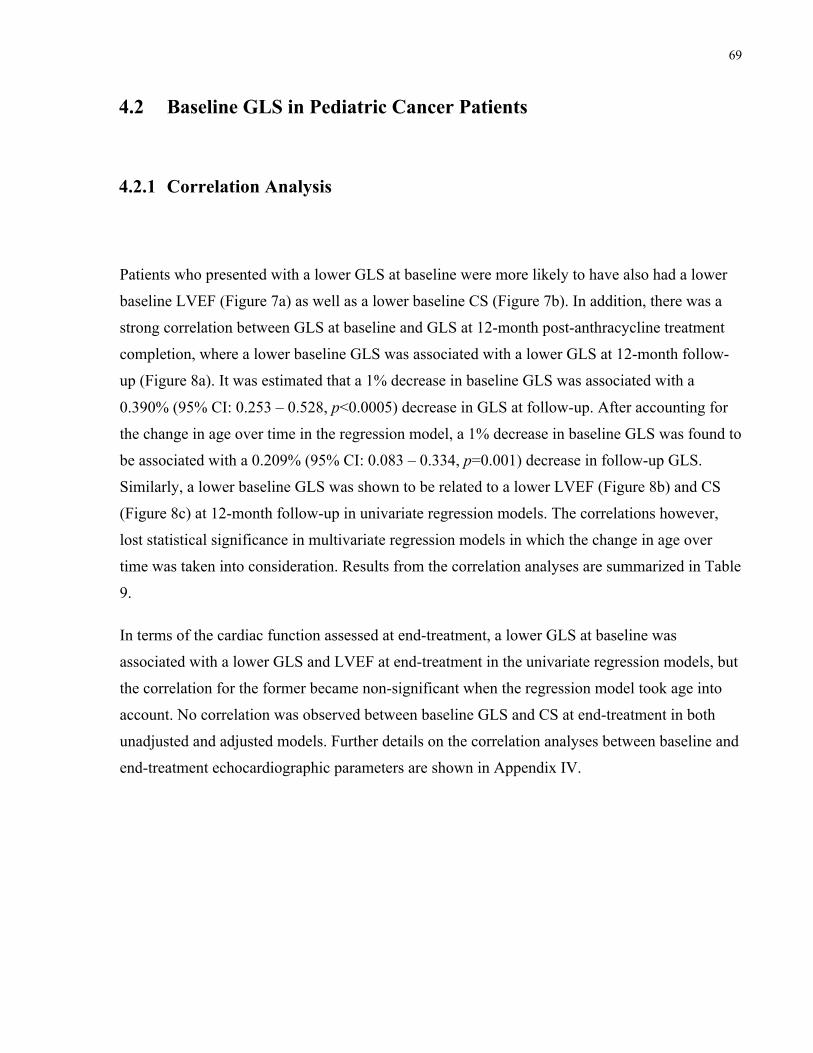
69
4.2 Baseline GLS in Pediatric Cancer Patients
4.2.1 Correlation Analysis
Patients who presented with a lower GLS at baseline were more likely to have also had a lower
baseline LVEF (Figure 7a) as well as a lower baseline CS (Figure 7b). In addition, there was a
strong correlation between GLS at baseline and GLS at 12-month post-anthracycline treatment
completion, where a lower baseline GLS was associated with a lower GLS at 12-month follow-
up (Figure 8a). It was estimated that a 1% decrease in baseline GLS was associated with a
0.390% (95% CI: 0.253 – 0.528, p<0.0005) decrease in GLS at follow-up. After accounting for
the change in age over time in the regression model, a 1% decrease in baseline GLS was found to
be associated with a 0.209% (95% CI: 0.083 – 0.334, p=0.001) decrease in follow-up GLS.
Similarly, a lower baseline GLS was shown to be related to a lower LVEF (Figure 8b) and CS
(Figure 8c) at 12-month follow-up in univariate regression models. The correlations however,
lost statistical significance in multivariate regression models in which the change in age over
time was taken into consideration. Results from the correlation analyses are summarized in Table
9.
In terms of the cardiac function assessed at end-treatment, a lower GLS at baseline was
associated with a lower GLS and LVEF at end-treatment in the univariate regression models, but
the correlation for the former became non-significant when the regression model took age into
account. No correlation was observed between baseline GLS and CS at end-treatment in both
unadjusted and adjusted models. Further details on the correlation analyses between baseline and
end-treatment echocardiographic parameters are shown in Appendix IV.
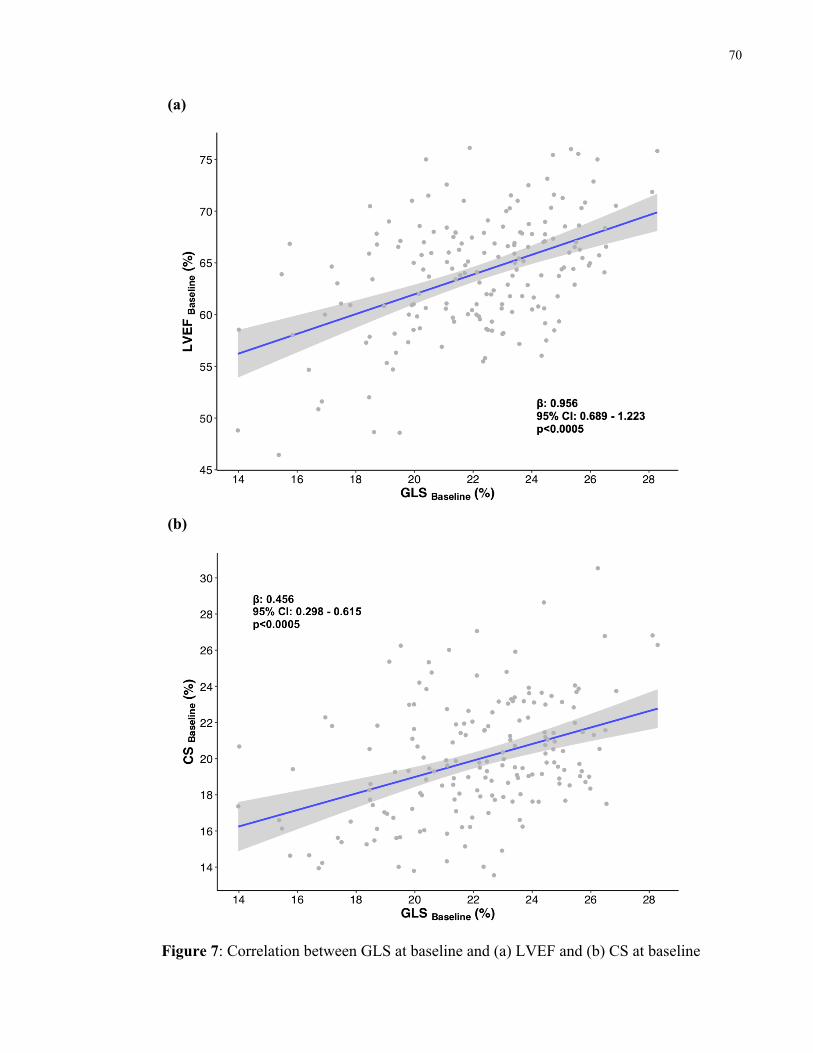
70
(a)
(b)
Figure 7: Correlation between GLS at baseline and (a) LVEF and (b) CS at baseline
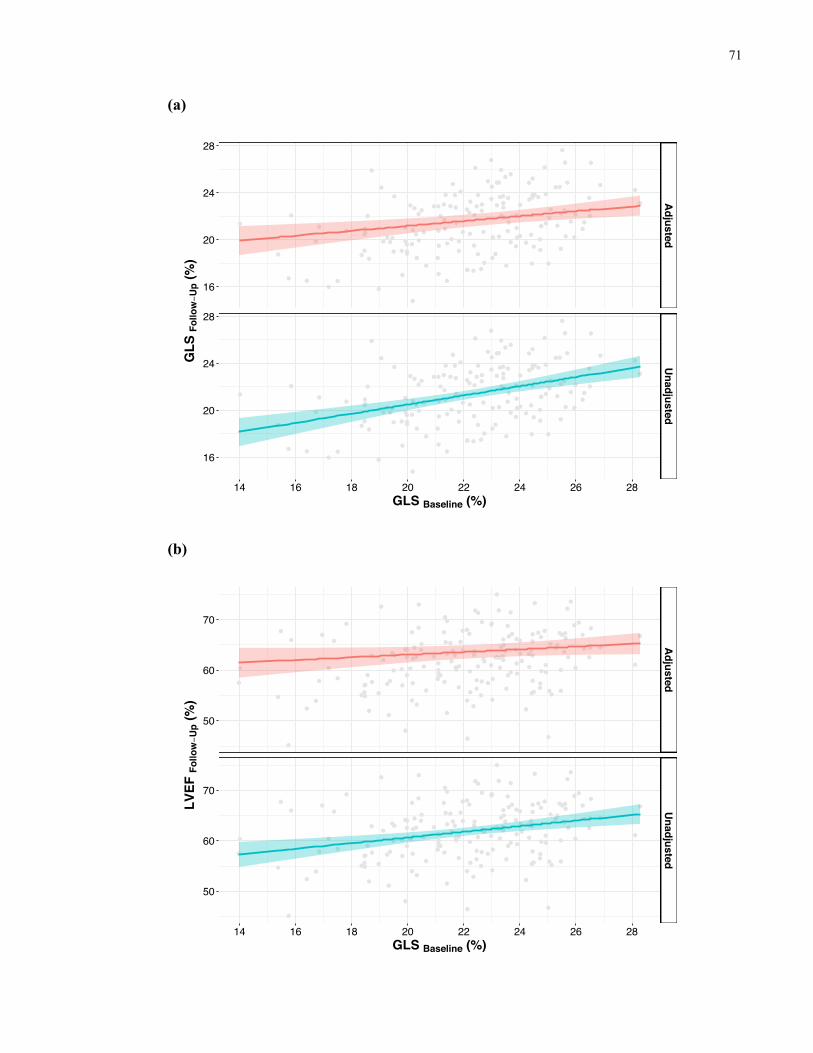
71
(a)
(b)
Adjusted
Unadjusted
14 16 18 20 22 24 26 28
16
20
24
28
16
20
24
28
GLS Baseline (%)
GLS
Fol
low−U
p (%
)
Adjusted
Unadjusted
14 16 18 20 22 24 26 28
50
60
70
50
60
70
GLS Baseline (%)
LVEF
Fol
low−U
p (%
)
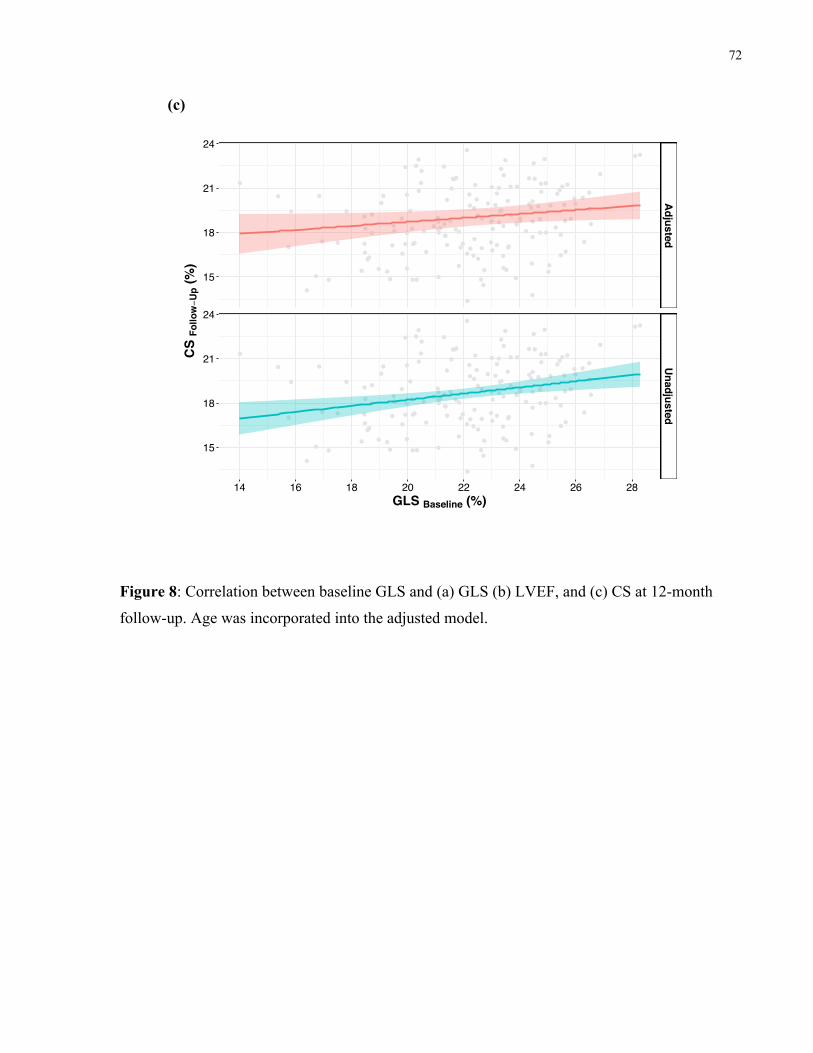
72
(c)
Figure 8: Correlation between baseline GLS and (a) GLS (b) LVEF, and (c) CS at 12-month
follow-up. Age was incorporated into the adjusted model.
Adjusted
Unadjusted
14 16 18 20 22 24 26 28
15
18
21
24
15
18
21
24
GLS Baseline (%)
CS
Follo
w−U
p (%
)
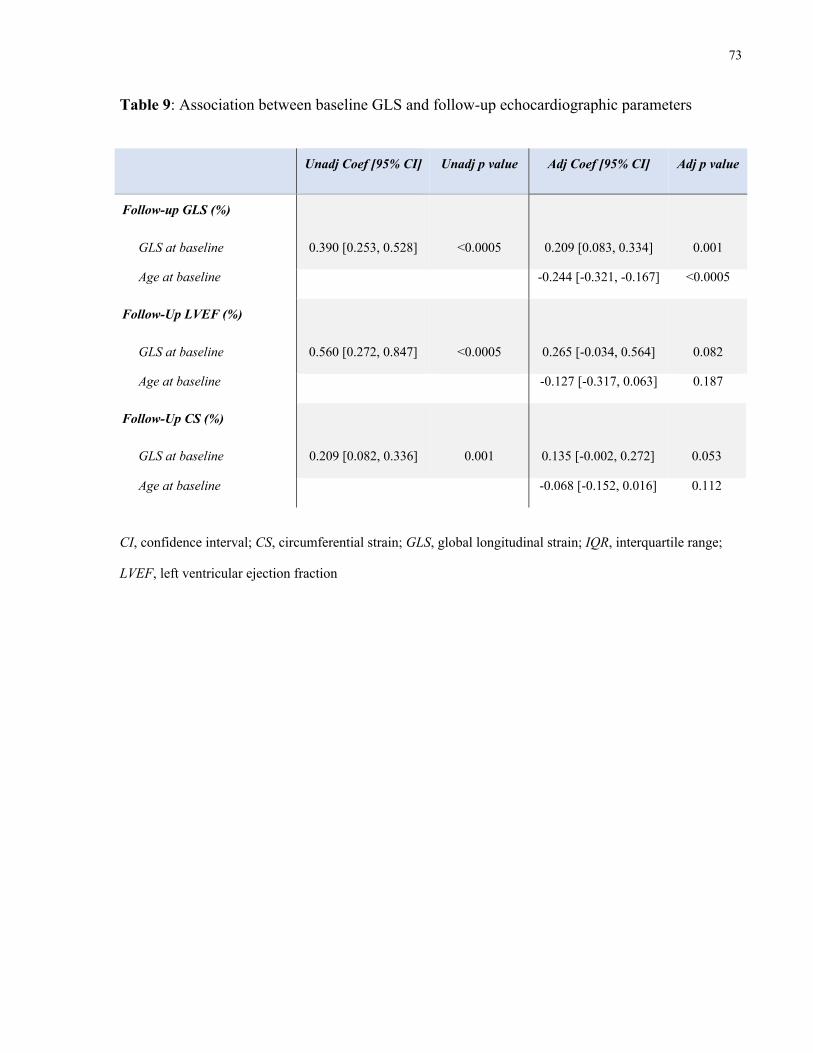
73
Table 9: Association between baseline GLS and follow-up echocardiographic parameters
Unadj Coef [95% CI] Unadj p value Adj Coef [95% CI] Adj p value
Follow-up GLS (%)
GLS at baseline 0.390 [0.253, 0.528] <0.0005 0.209 [0.083, 0.334] 0.001
Age at baseline -0.244 [-0.321, -0.167] <0.0005
Follow-Up LVEF (%)
GLS at baseline 0.560 [0.272, 0.847] <0.0005 0.265 [-0.034, 0.564] 0.082
Age at baseline -0.127 [-0.317, 0.063] 0.187
Follow-Up CS (%)
GLS at baseline 0.209 [0.082, 0.336] 0.001 0.135 [-0.002, 0.272] 0.053
Age at baseline -0.068 [-0.152, 0.016] 0.112
CI, confidence interval; CS, circumferential strain; GLS, global longitudinal strain; IQR, interquartile range;
LVEF, left ventricular ejection fraction
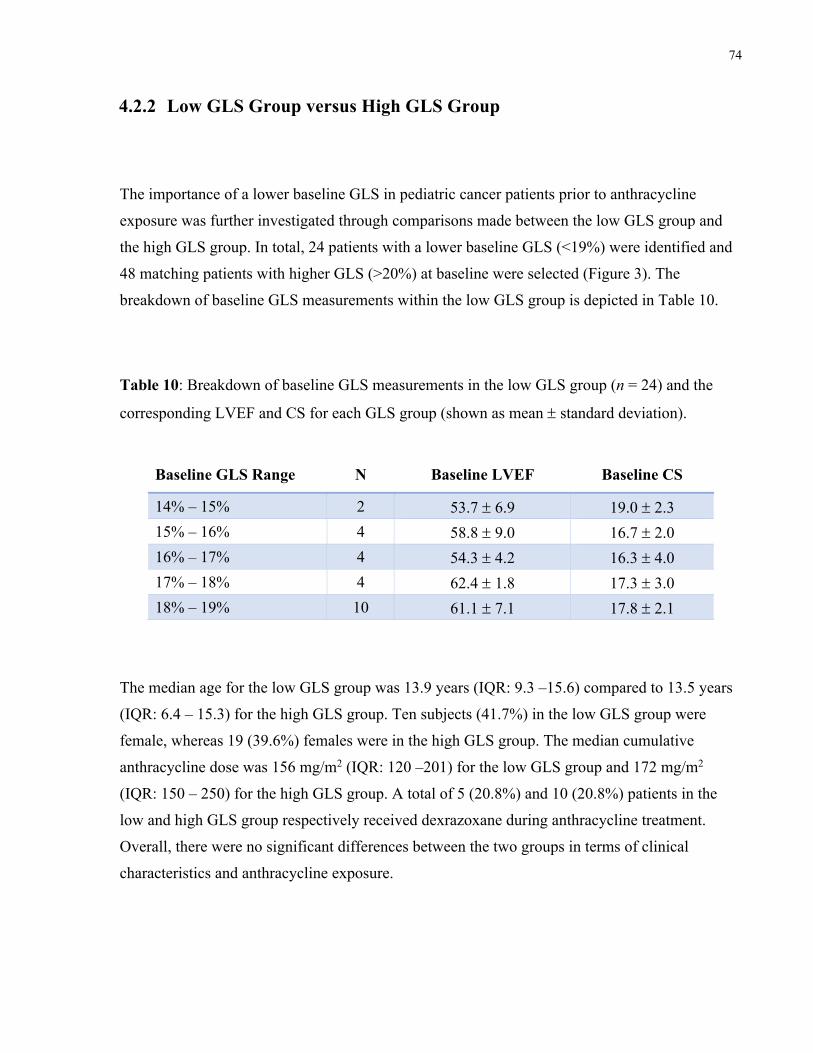
74
4.2.2 Low GLS Group versus High GLS Group
The importance of a lower baseline GLS in pediatric cancer patients prior to anthracycline
exposure was further investigated through comparisons made between the low GLS group and
the high GLS group. In total, 24 patients with a lower baseline GLS (<19%) were identified and
48 matching patients with higher GLS (>20%) at baseline were selected (Figure 3). The
breakdown of baseline GLS measurements within the low GLS group is depicted in Table 10.
Table 10: Breakdown of baseline GLS measurements in the low GLS group (n = 24) and the
corresponding LVEF and CS for each GLS group (shown as mean ± standard deviation).
Baseline GLS Range N Baseline LVEF Baseline CS
14% – 15% 2 53.7 ± 6.9 19.0 ± 2.3 15% – 16% 4 58.8 ± 9.0 16.7 ± 2.0 16% – 17% 4 54.3 ± 4.2 16.3 ± 4.0 17% – 18% 4 62.4 ± 1.8 17.3 ± 3.0 18% – 19% 10 61.1 ± 7.1 17.8 ± 2.1
The median age for the low GLS group was 13.9 years (IQR: 9.3 –15.6) compared to 13.5 years
(IQR: 6.4 – 15.3) for the high GLS group. Ten subjects (41.7%) in the low GLS group were
female, whereas 19 (39.6%) females were in the high GLS group. The median cumulative
anthracycline dose was 156 mg/m2 (IQR: 120 –201) for the low GLS group and 172 mg/m2
(IQR: 150 – 250) for the high GLS group. A total of 5 (20.8%) and 10 (20.8%) patients in the
low and high GLS group respectively received dexrazoxane during anthracycline treatment.
Overall, there were no significant differences between the two groups in terms of clinical
characteristics and anthracycline exposure.
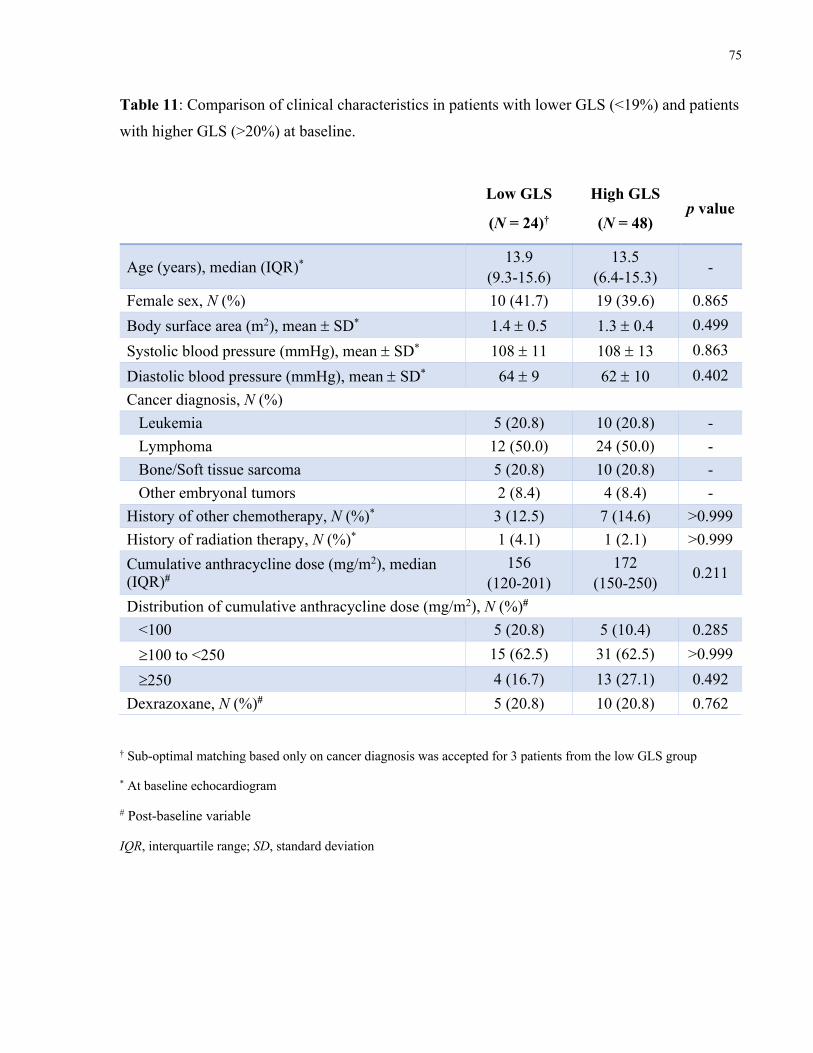
75
Table 11: Comparison of clinical characteristics in patients with lower GLS (<19%) and patients
with higher GLS (>20%) at baseline.
Low GLS
(N = 24)†
High GLS
(N = 48) p value
Age (years), median (IQR)* 13.9 (9.3-15.6)
13.5 (6.4-15.3) -
Female sex, N (%) 10 (41.7) 19 (39.6) 0.865 Body surface area (m2), mean ± SD* 1.4 ± 0.5 1.3 ± 0.4 0.499 Systolic blood pressure (mmHg), mean ± SD* 108 ± 11 108 ± 13 0.863 Diastolic blood pressure (mmHg), mean ± SD* 64 ± 9 62 ± 10 0.402 Cancer diagnosis, N (%) Leukemia 5 (20.8) 10 (20.8) - Lymphoma 12 (50.0) 24 (50.0) - Bone/Soft tissue sarcoma 5 (20.8) 10 (20.8) - Other embryonal tumors 2 (8.4) 4 (8.4) - History of other chemotherapy, N (%)* 3 (12.5) 7 (14.6) >0.999 History of radiation therapy, N (%)* 1 (4.1) 1 (2.1) >0.999 Cumulative anthracycline dose (mg/m2), median (IQR)#
156 (120-201)
172 (150-250) 0.211
Distribution of cumulative anthracycline dose (mg/m2), N (%)# <100 5 (20.8) 5 (10.4) 0.285 ³100 to <250 15 (62.5) 31 (62.5) >0.999 ³250 4 (16.7) 13 (27.1) 0.492 Dexrazoxane, N (%)# 5 (20.8) 10 (20.8) 0.762
† Sub-optimal matching based only on cancer diagnosis was accepted for 3 patients from the low GLS group
* At baseline echocardiogram
# Post-baseline variable
IQR, interquartile range; SD, standard deviation
76
At baseline, the low GLS group had a mean GLS of 17.2 ± 1.5% while the high GLS group had a
mean GLS of 22.5 ± 1.6% (Table 12). Both mean LVEF (59.2 ± 6.7% versus 64.8 ± 4.3%,
p=0.001) and CS (17.4 ± 2.5% versus 20.8 ± 3.4%, p<0.0005) at baseline were lower in the low
GLS group relative to the high GLS group. Twelve months after completion of anthracycline
chemotherapy, GLS had improved to 19.6 ± 2.6% in the low GLS group as a whole (p=0.004),
but of the 24 patients in the low GLS group, four patients remained with a reduced GLS of 16%
to 17%, and one patient had a follow-up GLS of 14.8%. Basic clinical characteristics of these
five patients are summarized in Table 13. Changes in both LVEF (58.5 ± 5.7%) and CS (17.6 ±
2.0%) from baseline to follow-up were insignificant (Figure 9a).
In contrast, subjects in the high GLS group showed a decline in all three echocardiographic
parameters from baseline to the follow-up 12 months after anthracycline treatment (Figure 9b):
GLS had decreased to 20.4 ± 2.2%, LVEF to 60.3 ± 5.5%, and CS to 18.1 ± 2.3%, all p<0.0005.
Twelve patients ended up with a GLS of <18% at the 12-month follow-up, one of which had a
reduced GLS of <15%. This one subject was male, 12.8 years old at the time of leukemia
diagnosis, and had received a cumulative anthracycline dose of 298 mg/m2. Table 14 presents the
difference of change over time between the two patient groups and results were confirmed using
fixed effect model analyses (Appendix V).
Identical patterns of changes in cardiac function were observed for both patient groups between
baseline measurements and measurements obtained at end-treatment (Appendix VI). Overall, as
depicted in Table 12 and Figure 10, despite the difference in GLS at baseline, the two patient
groups displayed clinically insignificant difference in LVEF, GLS, as well as CS after
anthracycline exposure at both end-treatment and 12-month follow-up.
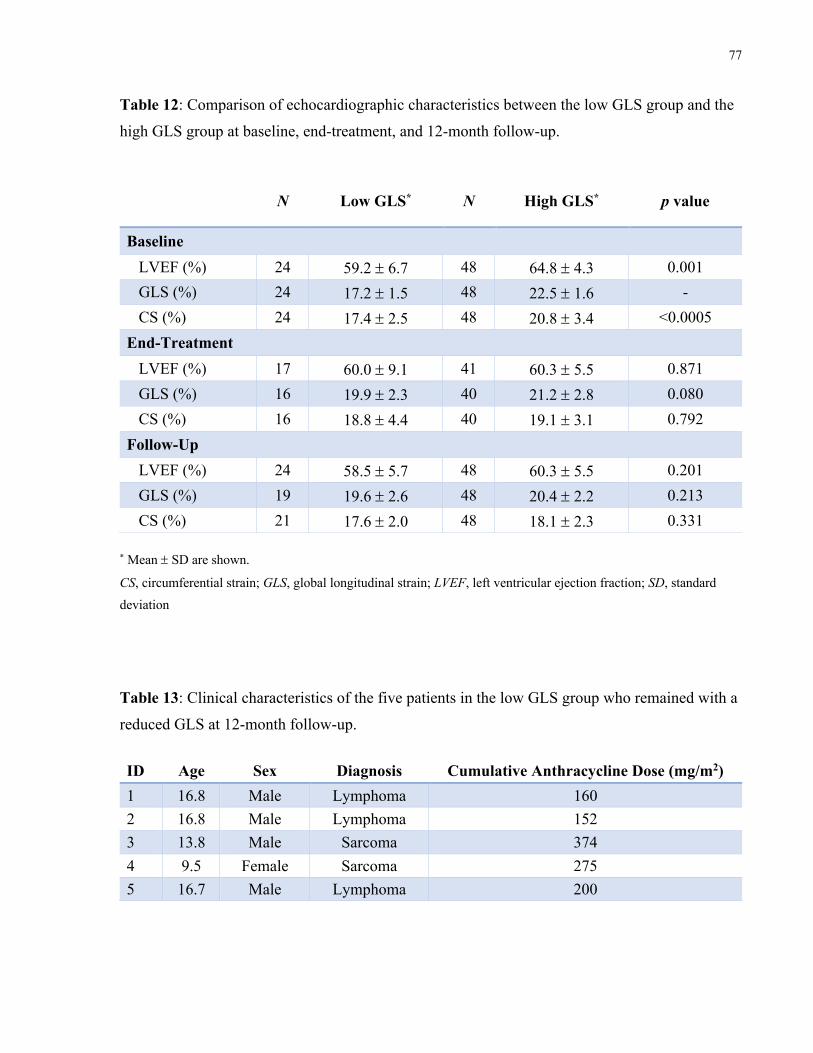
77
Table 12: Comparison of echocardiographic characteristics between the low GLS group and the
high GLS group at baseline, end-treatment, and 12-month follow-up.
N Low GLS* N High GLS* p value
Baseline LVEF (%) 24 59.2 ± 6.7 48 64.8 ± 4.3 0.001 GLS (%) 24 17.2 ± 1.5 48 22.5 ± 1.6 - CS (%) 24 17.4 ± 2.5 48 20.8 ± 3.4 <0.0005 End-Treatment LVEF (%) 17 60.0 ± 9.1 41 60.3 ± 5.5 0.871 GLS (%) 16 19.9 ± 2.3 40 21.2 ± 2.8 0.080 CS (%) 16 18.8 ± 4.4 40 19.1 ± 3.1 0.792 Follow-Up LVEF (%) 24 58.5 ± 5.7 48 60.3 ± 5.5 0.201 GLS (%) 19 19.6 ± 2.6 48 20.4 ± 2.2 0.213 CS (%) 21 17.6 ± 2.0 48 18.1 ± 2.3 0.331
* Mean ± SD are shown.
CS, circumferential strain; GLS, global longitudinal strain; LVEF, left ventricular ejection fraction; SD, standard deviation
Table 13: Clinical characteristics of the five patients in the low GLS group who remained with a
reduced GLS at 12-month follow-up. ID Age Sex Diagnosis Cumulative Anthracycline Dose (mg/m2) 1 16.8 Male Lymphoma 160 2 16.8 Male Lymphoma 152 3 13.8 Male Sarcoma 374 4 9.5 Female Sarcoma 275 5 16.7 Male Lymphoma 200
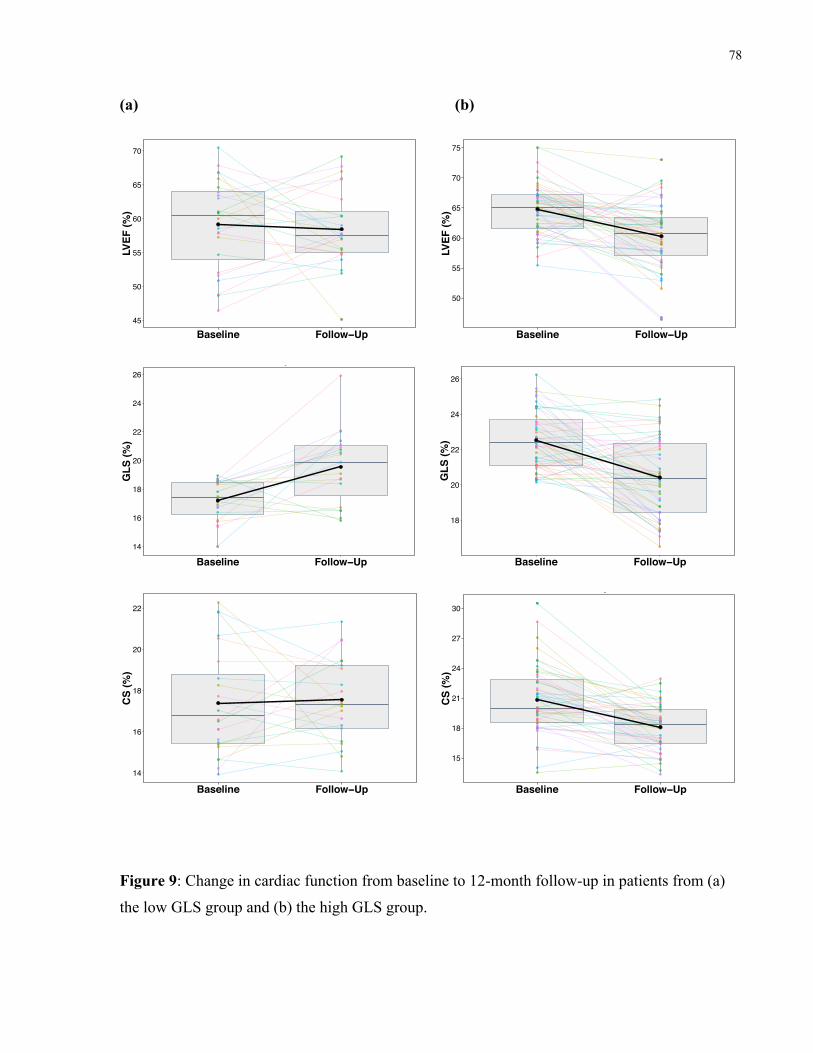
78
(a) (b)
Figure 9: Change in cardiac function from baseline to 12-month follow-up in patients from (a)
the low GLS group and (b) the high GLS group.
45
50
55
60
65
70
Baseline Follow−Up
LVEF
(%)
Group 1
50
55
60
65
70
75
Baseline Follow−Up
LVEF
(%)
Group 2
14
16
18
20
22
24
26
Baseline Follow−Up
GLS
(%)
Group 1
18
20
22
24
26
Baseline Follow−Up
GLS
(%)
Group 2
14
16
18
20
22
Baseline Follow−Up
CS
(%)
Group 1
15
18
21
24
27
30
Baseline Follow−Up
CS
(%)
Group 2
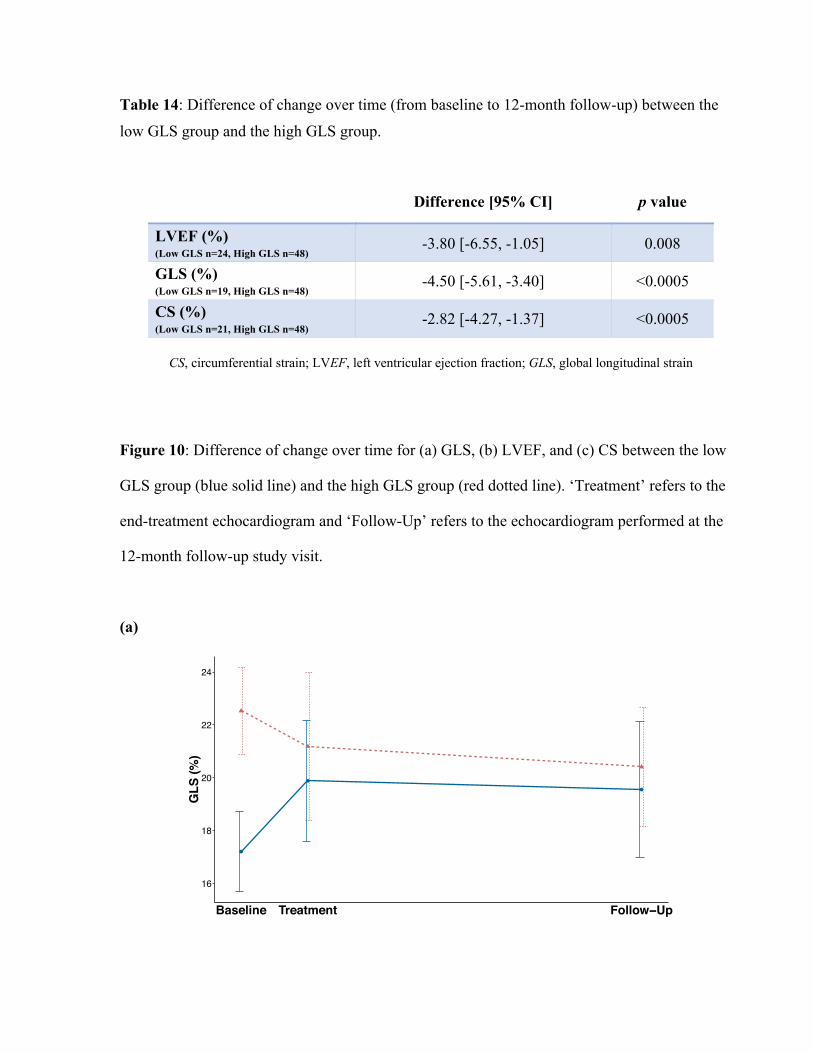
Table 14: Difference of change over time (from baseline to 12-month follow-up) between the
low GLS group and the high GLS group.
Difference [95% CI] p value
LVEF (%) (Low GLS n=24, High GLS n=48) -3.80 [-6.55, -1.05] 0.008
GLS (%) (Low GLS n=19, High GLS n=48) -4.50 [-5.61, -3.40] <0.0005
CS (%) (Low GLS n=21, High GLS n=48) -2.82 [-4.27, -1.37] <0.0005
CS, circumferential strain; LVEF, left ventricular ejection fraction; GLS, global longitudinal strain
Figure 10: Difference of change over time for (a) GLS, (b) LVEF, and (c) CS between the low
GLS group (blue solid line) and the high GLS group (red dotted line). ‘Treatment’ refers to the
end-treatment echocardiogram and ‘Follow-Up’ refers to the echocardiogram performed at the
12-month follow-up study visit.
(a)
16
18
20
22
24
Baseline Treatment Follow−Up
GLS
(%)
GroupGroup 1
Group 2
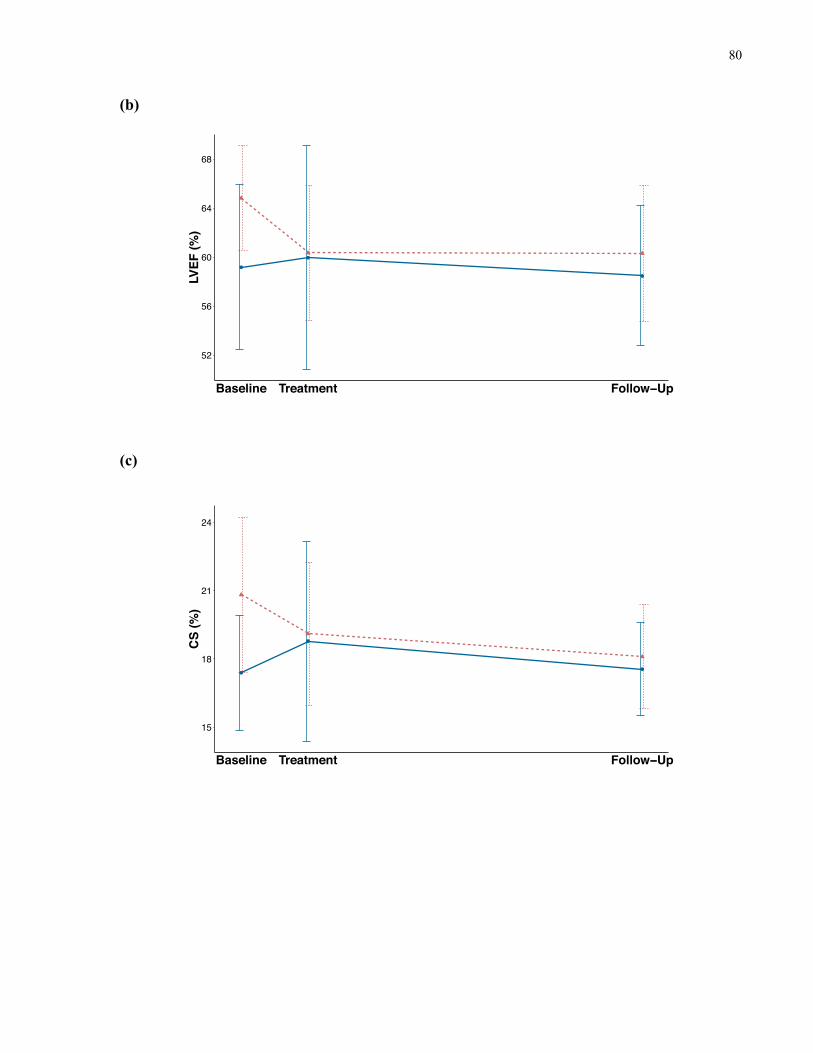
80
(b)
(c)
52
56
60
64
68
Baseline Treatment Follow−Up
LVEF
(%)
GroupGroup 1
Group 2
15
18
21
24
Baseline Treatment Follow−Up
CS
(%)
GroupGroup 1
Group 2
81
4.3 Baseline Cardiac Biomarkers
4.3.1 N-terminal pro-B-type natriuretic peptide (NT-proBNP)
In total, 91 patients in our study cohort had a baseline NT-proBNP measurement and 479
CALIPER controls with NT-proBNP data were identified (Figure 4). NT-proBNP concentrations
ranged from 11 pg/mL to 4,046 pg/mL in patients and 5 pg/mL to 5,756 pg/mL in CALIPER
controls, with the highest NT-proBNP values observed in the youngest patients (Figure 11). The
median age was 6.9 years (IQR: 4.0 – 13.8) in patients at baseline compared to 2.5 years (IQR:
0.4 – 13.2) in CALIPER controls, p<0.0005. However, given that 210 (43.8%) of CALIPER
controls were below 1 year of age compared to only 2 (2.2%) in the patient cohort, in addition to
the large variability in NT-proBNP concentrations, especially evident in CALIPER controls,
under the age of 1 year, subjects < 1 year old were excluded from further analyses to allow for
more accurate and robust comparisons between the two groups. Accordingly, NT-proBNP
measurements from 89 patients and 269 CALIPER controls who were over 1 year of age were
examined.
Table 15 presents the clinical characteristics between the two groups of children over 1 year of
age. The patient group was younger at baseline than CALIPER controls (8.3 [IQR: 4.0 – 13.9]
versus 12.3 [IQR: 6.8 – 14.7] years, p=0.011). Median NT-proBNP levels were shown to be
significantly higher in patients compared to CALIPER controls (107.1 [IQR: 50.3 – 276.6]
versus 43.7 [IQR: 23.8 – 74.1] mg/m2, p<0.0005). Based on the age-dependent reference values
(97.5th percentile) published by Albers et al. (Albers et al. 2006), 21 patients (23.6%) were found
to have abnormal NT-proBNP levels at baseline whereas only 6 (2.2%) children had abnormal
levels in the CALIPER cohort (Table 16). A significant correlation between baseline NT-
proBNP levels and age was demonstrated for both the patient group (p=0.006) and the CALIPER
cohort (p<0.0005), where younger children had higher baseline NT-proBNP levels. In addition,
having a history of chemotherapy prior to receiving anthracycline chemotherapy did not affect
NT-proBNP levels that were assessed at baseline – the median baseline NT-proBNP
concentration was 89.7 pg/mL (IQR: 56.8 – 169.5) in patients who had a history of other
chemotherapy versus 125.9 pg/mL (IQR: 47.0 – 399.6) in those who did not, p=0.393.

82
At the 12-month follow-up study visit, NT-proBNP measurements were obtained from a total of
118 patient serum samples, 52 (44.1%) of which were from patients who also had a NT-proBNP
measurement at baseline. A higher NT-proBNP at baseline was associated with a higher NT-
proBNP at follow-up (p=0.004). A paired analysis of the NT-proBNP levels in these 52 patients
revealed that the median NT-proBNP concentration decreased from 97.5 pg/mL (IQR: 40.0 –
410.3) at baseline to 59.3 pg/mL (IQR: 27.8 – 104.0) at follow-up (p=0.006). Post-hoc analysis
using the Dunn Test for multiple comparisons showed that both baseline and follow-up NT-
proBNP values in patients were significantly higher than that of the CALIPER cohort. A
graphical representation of the NT-proBNP levels in patients at baseline and 12-month follow-
up, as well as in CALIPER controls is presented in Figure 12. Eleven patients (9.3%) had
abnormal NT-proBNP levels (Table 16). Between the four cancer diagnosis groups, no
difference in baseline NT-proBNP concentration was observed: leukemia (138.1 pg/mL, IQR:
58.6 – 502.6), lymphoma (73.8 pg/mL, IQR: 28.5 – 386.0), bone/soft tissue sarcoma (105.8
pg/mL, IQR: 67.4 – 263.6), and other embryonal tumors (90.2 pg/mL, IQR: 55.1 – 169.5),
p=0.590.
When the relationship between baseline NT-proBNP levels and cardiac function was examined
(Figure 13), no significant correlations were found for any of the echocardiographic parameters
(LVEF, GLS, and CS) assessed at baseline, end-treatment, and 12-month follow-up. Baseline
NT-proBNP levels also showed no correlation with LV end-diastolic diameter (LVEDD),
measured at each of the three time points. No correlation was detected between follow-up NT-
proBNP measurements and echocardiographic parameters at follow-up.
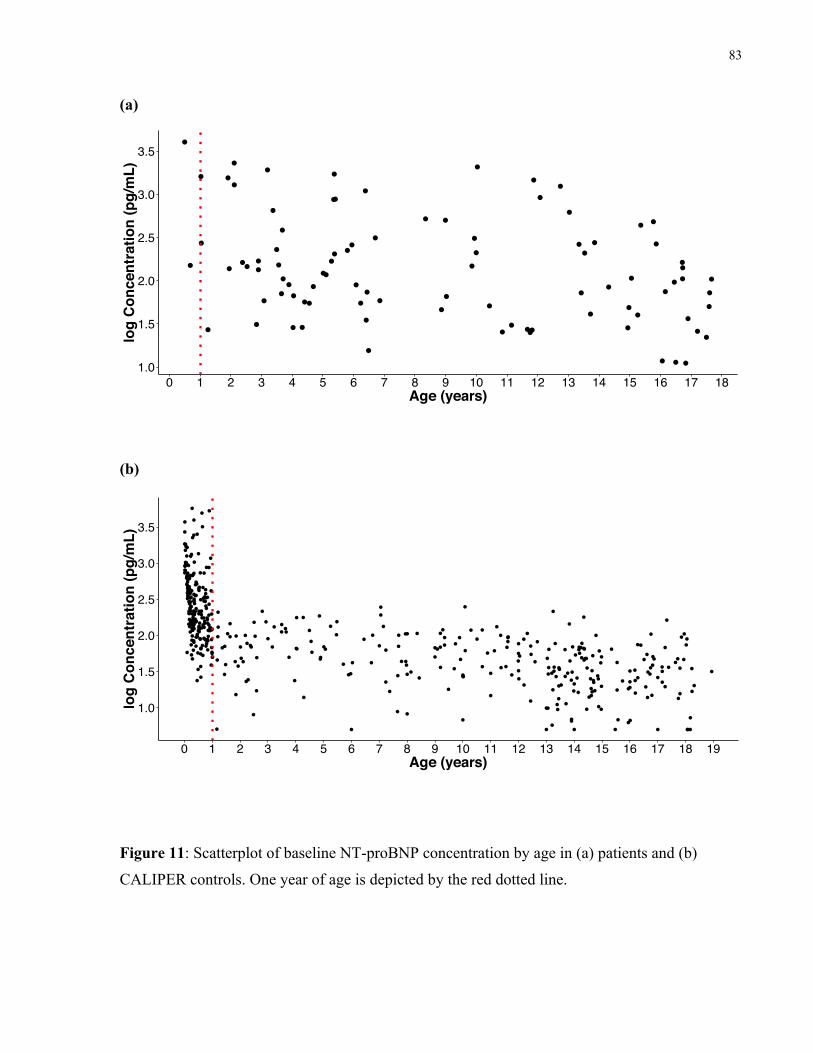
83
(a)
(b)
Figure 11: Scatterplot of baseline NT-proBNP concentration by age in (a) patients and (b)
CALIPER controls. One year of age is depicted by the red dotted line.
1.0
1.5
2.0
2.5
3.0
3.5
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18Age (years)
log
Con
cent
ratio
n (p
g/m
L)N−Terminal Pro B−Type Natriuretic Peptide
(NT−proBNP)
1.0
1.5
2.0
2.5
3.0
3.5
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19Age (years)
log
Con
cent
ratio
n (p
g/m
L)
N−Terminal Pro B−Type Natriuretic Peptide (NT−proBNP)
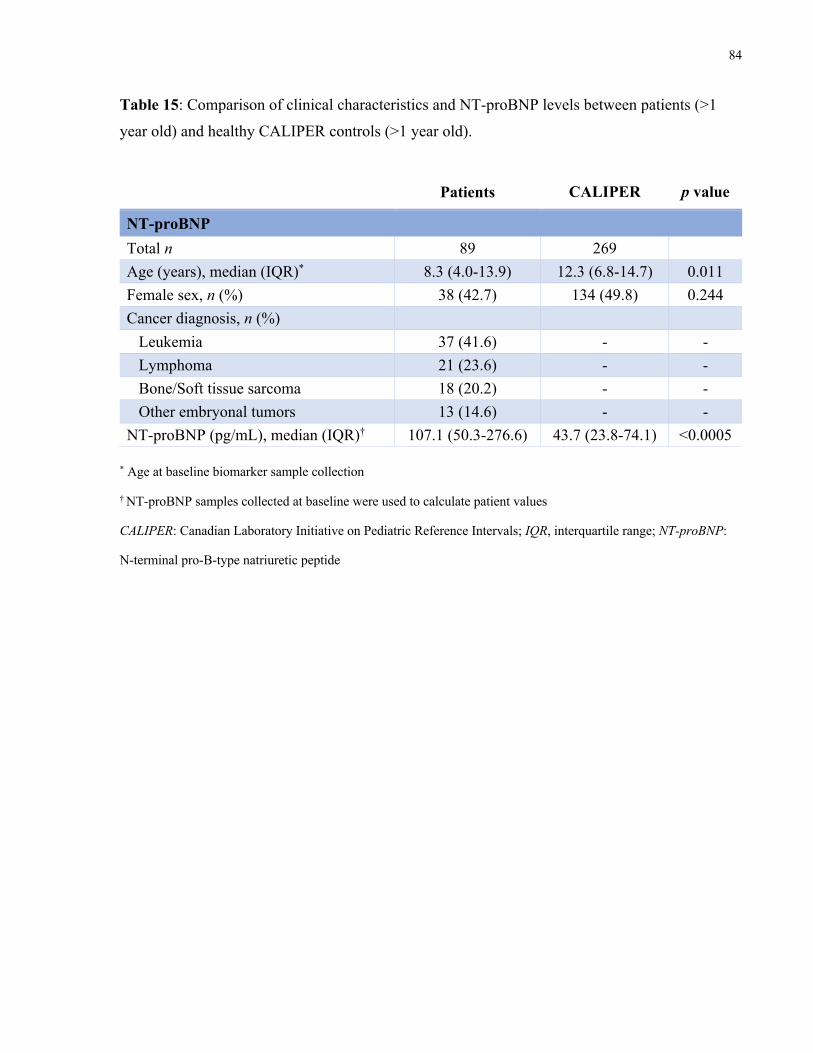
84
Table 15: Comparison of clinical characteristics and NT-proBNP levels between patients (>1
year old) and healthy CALIPER controls (>1 year old).
Patients CALIPER p value
NT-proBNP Total n 89 269 Age (years), median (IQR)* 8.3 (4.0-13.9) 12.3 (6.8-14.7) 0.011 Female sex, n (%) 38 (42.7) 134 (49.8) 0.244 Cancer diagnosis, n (%) Leukemia 37 (41.6) - - Lymphoma 21 (23.6) - - Bone/Soft tissue sarcoma 18 (20.2) - - Other embryonal tumors 13 (14.6) - - NT-proBNP (pg/mL), median (IQR)† 107.1 (50.3-276.6) 43.7 (23.8-74.1) <0.0005
* Age at baseline biomarker sample collection
† NT-proBNP samples collected at baseline were used to calculate patient values
CALIPER: Canadian Laboratory Initiative on Pediatric Reference Intervals; IQR, interquartile range; NT-proBNP:
N-terminal pro-B-type natriuretic peptide
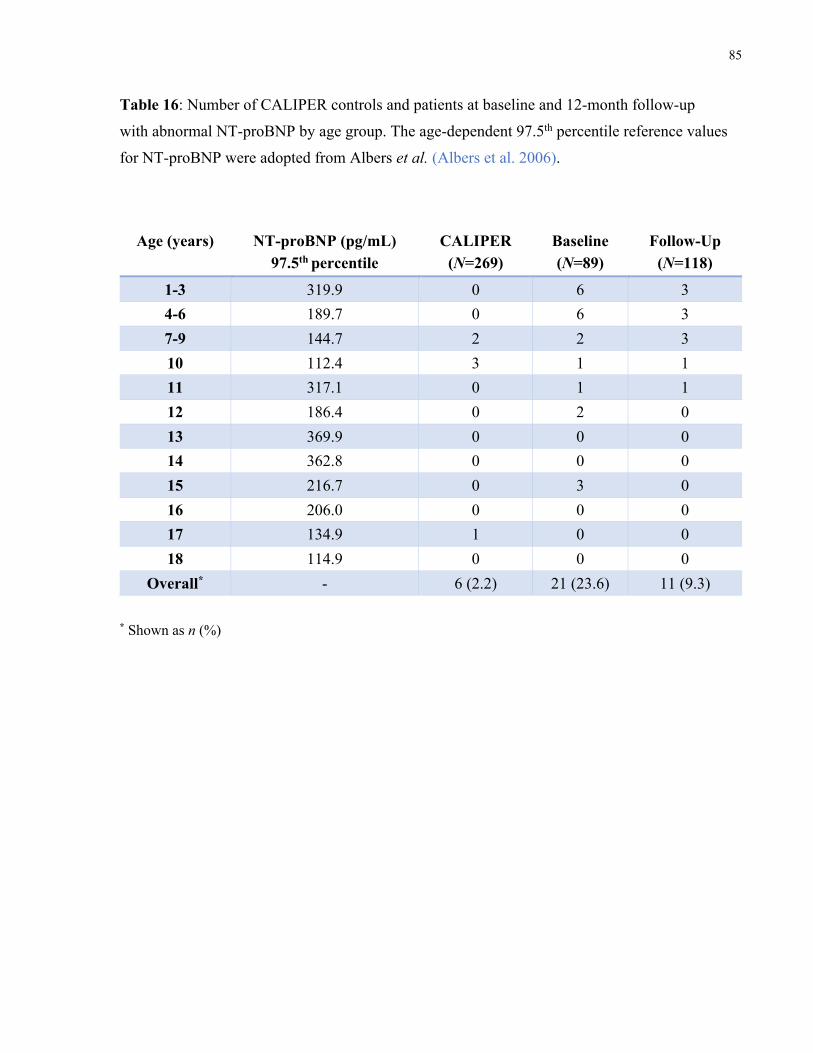
85
Table 16: Number of CALIPER controls and patients at baseline and 12-month follow-up
with abnormal NT-proBNP by age group. The age-dependent 97.5th percentile reference values
for NT-proBNP were adopted from Albers et al. (Albers et al. 2006).
Age (years) NT-proBNP (pg/mL) 97.5th percentile
CALIPER (N=269)
Baseline (N=89)
Follow-Up (N=118)
1-3 319.9 0 6 3 4-6 189.7 0 6 3 7-9 144.7 2 2 3 10 112.4 3 1 1 11 317.1 0 1 1 12 186.4 0 2 0 13 369.9 0 0 0 14 362.8 0 0 0 15 216.7 0 3 0 16 206.0 0 0 0 17 134.9 1 0 0 18 114.9 0 0 0
Overall* - 6 (2.2) 21 (23.6) 11 (9.3) * Shown as n (%)
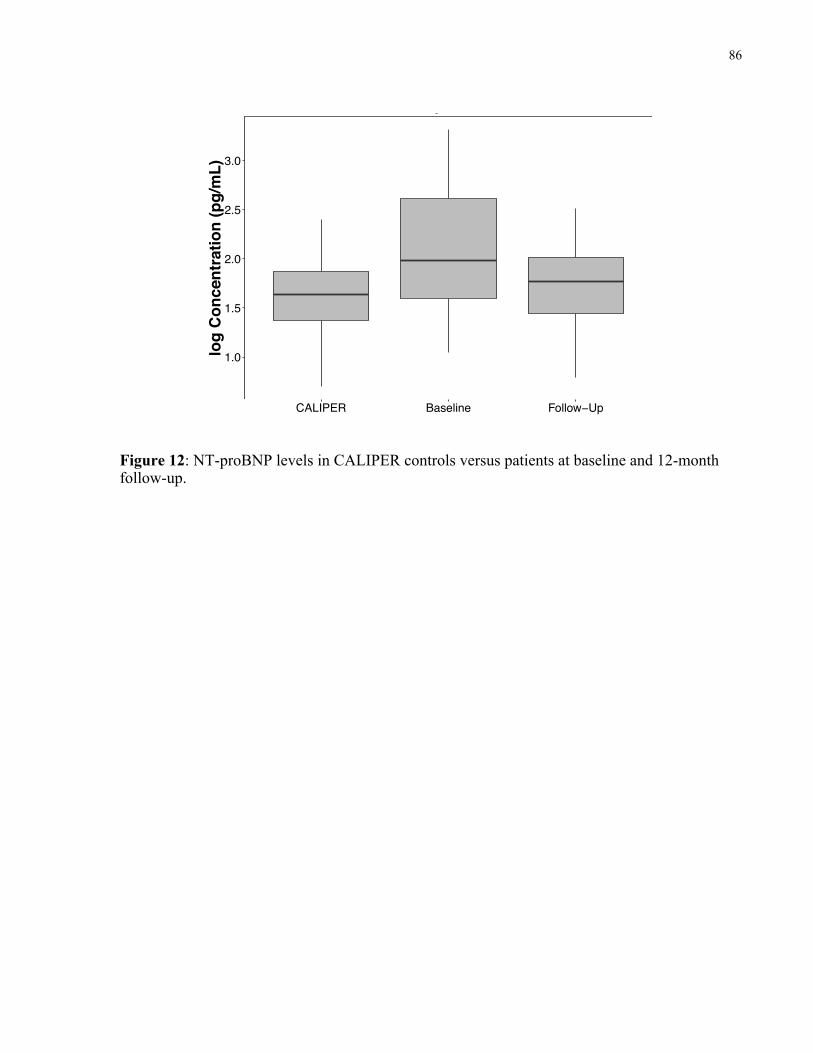
86
Figure 12: NT-proBNP levels in CALIPER controls versus patients at baseline and 12-month follow-up.
1.0
1.5
2.0
2.5
3.0
CALIPER Baseline Follow−Up
log
Con
cent
ratio
n (p
g/m
L)
NT−proBNP
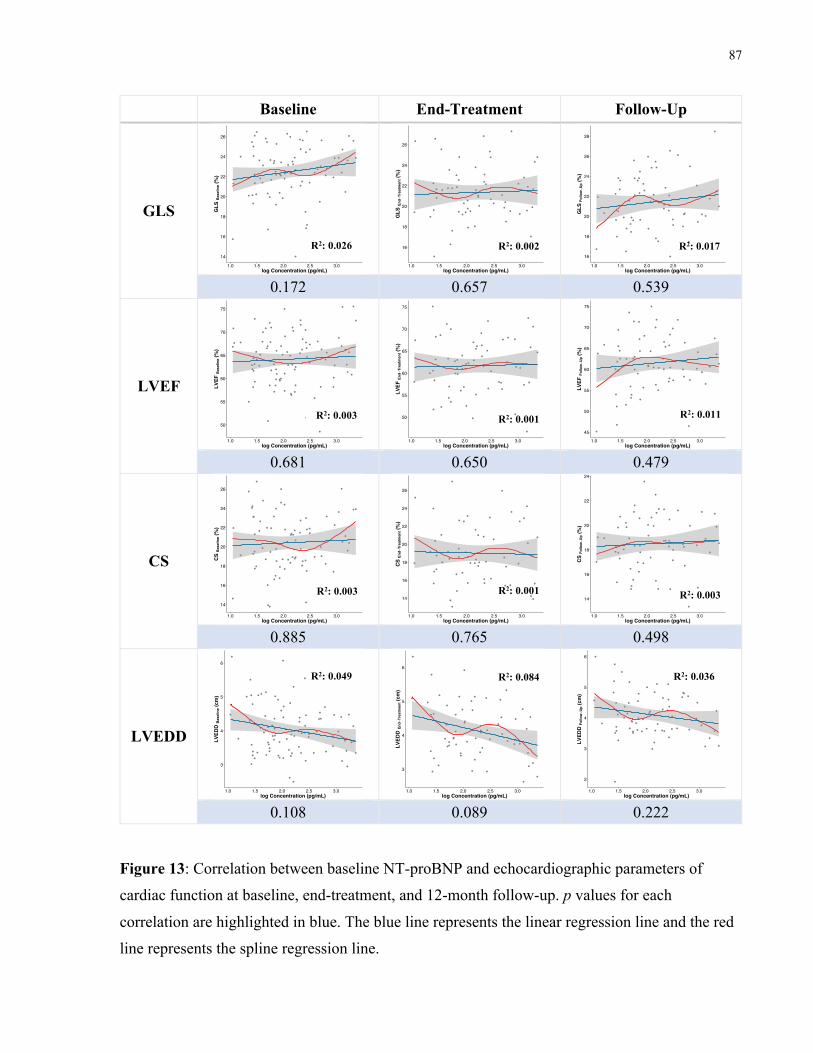
87
Baseline End-Treatment Follow-Up
GLS
0.172 0.657 0.539
LVEF
0.681 0.650 0.479
CS
0.885 0.765 0.498
LVEDD
0.108 0.089 0.222
Figure 13: Correlation between baseline NT-proBNP and echocardiographic parameters of
cardiac function at baseline, end-treatment, and 12-month follow-up. p values for each
correlation are highlighted in blue. The blue line represents the linear regression line and the red
line represents the spline regression line.
14
16
18
20
22
24
26
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
GLS
Bas
elin
e (%
)
16
18
20
22
24
26
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
GLS
End
−Tre
atm
ent (
%)
16
18
20
22
24
26
28
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
GLS
Follo
w−U
p (%
)
50
55
60
65
70
75
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
LVEF
Bas
elin
e (%
)
50
55
60
65
70
75
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
LVEF
End
−Tre
atm
ent (
%)
45
50
55
60
65
70
75
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
LVEF
Follo
w−U
p (%
)
14
16
18
20
22
24
26
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
CS
Bas
elin
e (%
)
14
16
18
20
22
24
26
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
CS
End−
Trea
tmen
t (%
)
14
16
18
20
22
24
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
CS
Follo
w−U
p (%
)
3
4
5
6
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
LVED
D B
asel
ine (
cm)
3
4
5
6
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
LVED
D E
nd−T
reat
men
t (cm
)
2
3
4
5
6
1.0 1.5 2.0 2.5 3.0log Concentration (pg/mL)
LVED
D Fo
llow−U
p (cm
)
R2: 0.026
R2: 0.003
R2: 0.003
R2: 0.049
R2: 0.002 R2: 0.017
R2: 0.011
R2: 0.003
R2: 0.036
R2: 0.001
R2: 0.001
R2: 0.084
88
4.3.2 High-sensitivity troponin T (hs-TnT)
Baseline hs-TnT samples were analyzed in 57 patients and 242 CALIPER controls had hs-TnT
measurements (Figure 5). The concentration range for hs-TnT in patients was from 3 pg/mL to
50 pg/mL while CALIPER controls displayed concentrations that ranged from 3 pg/mL to 90
pg/mL (Figure 14). Overall, patients at baseline were older than CALIPER controls (7.7 ± 5.4
versus 5.6 ± 6.2 years, p=0.014), but similar to the NT-proBNP observations, there was a wide
variability in hs-TnT levels in neonates up to age 1, especially in the CALIPER cohort (n=109,
45.0%). In contrast, only 2 patients (3.5%) with hs-TnT measurements at baseline were under 1
year of age. Therefore, to ensure appropriate comparisons between the two groups, subjects
under the age of 1 year were once again excluded from further analyses. Consequently, 55
patients and 133 CALIPER controls were included in our hs-TnT analyses.
Clinical characteristics of the two groups are depicted in Table 17. In comparison to CALIPER
controls, patients at baseline were younger (6.1 [IQR: 3.7 – 12.4] versus 10.1 [IQR: 4.9 – 14.7]
years, p=0.041) and had a higher median hs-TnT concentration (5.2 [IQR: 4.0 – 7.8] versus 3.0
[IQR: 3.0 – 3.6] pg/mL, p<0.0005). Overall, none of the CALIPER controls had hs-TnT levels in
the abnormal range of >14 pg/mL whereas 6 patients (10.9%) at baseline did (Aroney and Cullen
2016). A younger age correlated with a higher hs-TnT concentration in patients over 1 year of
age (p=0.011), but the same was not observed for the CALIPER group (p=0.193). The median
hs-TnT concentration at baseline did not differ significantly between patients who had prior
exposure to non-anthracycline chemotherapy (7.7 pg/mL [IQR: 4.3 – 8.1]) and those who did not
(4.8 pg/mL [IQR: 3.7 – 6.6]), p=0.138.
A positive correlation was demonstrated between hs-TnT levels assessed at baseline and 12-
month follow-up (p=0.042). In a paired analysis of patients with hs-TnT measurements from
both baseline and 12-month follow-up (n=30), no change in hs-TnT concentration over time was
observed (5.7 [IQR: 4.0 – 7.8] pg/mL at baseline to 5.4 [IQR: 4.8 – 7.3] pg/mL, p=0.813).
However, both measurements in the patient group were significantly higher than the median hs-
TnT level in the CALIPER cohort (3.0 pg/mL), p<0.0005 (Figure 15). No difference in baseline
hs-TnT concentration was shown between cancer diagnosis groups: leukemia (5.2 pg/mL [IQR:
4.0 – 8.0]), lymphoma (4.3 pg/mL [IQR: 3.8 – 6.5]), bone/soft tissue sarcoma (4.3 pg/mL [IQR:
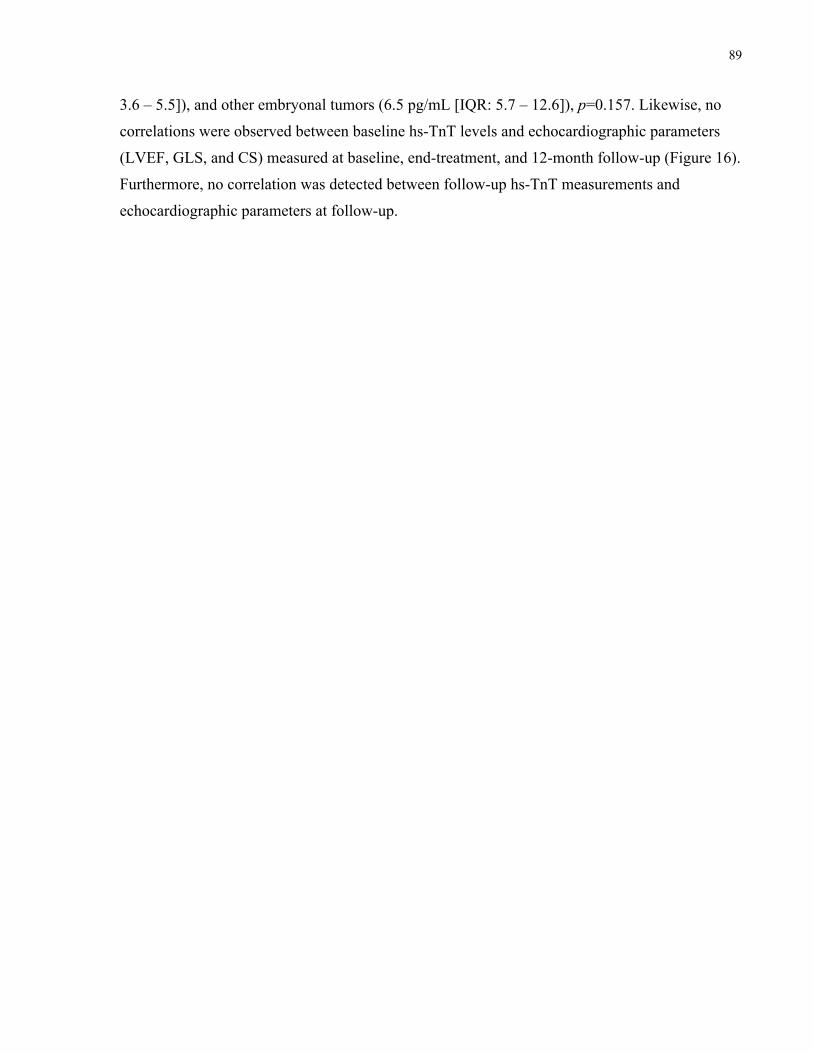
89
3.6 – 5.5]), and other embryonal tumors (6.5 pg/mL [IQR: 5.7 – 12.6]), p=0.157. Likewise, no
correlations were observed between baseline hs-TnT levels and echocardiographic parameters
(LVEF, GLS, and CS) measured at baseline, end-treatment, and 12-month follow-up (Figure 16).
Furthermore, no correlation was detected between follow-up hs-TnT measurements and
echocardiographic parameters at follow-up.
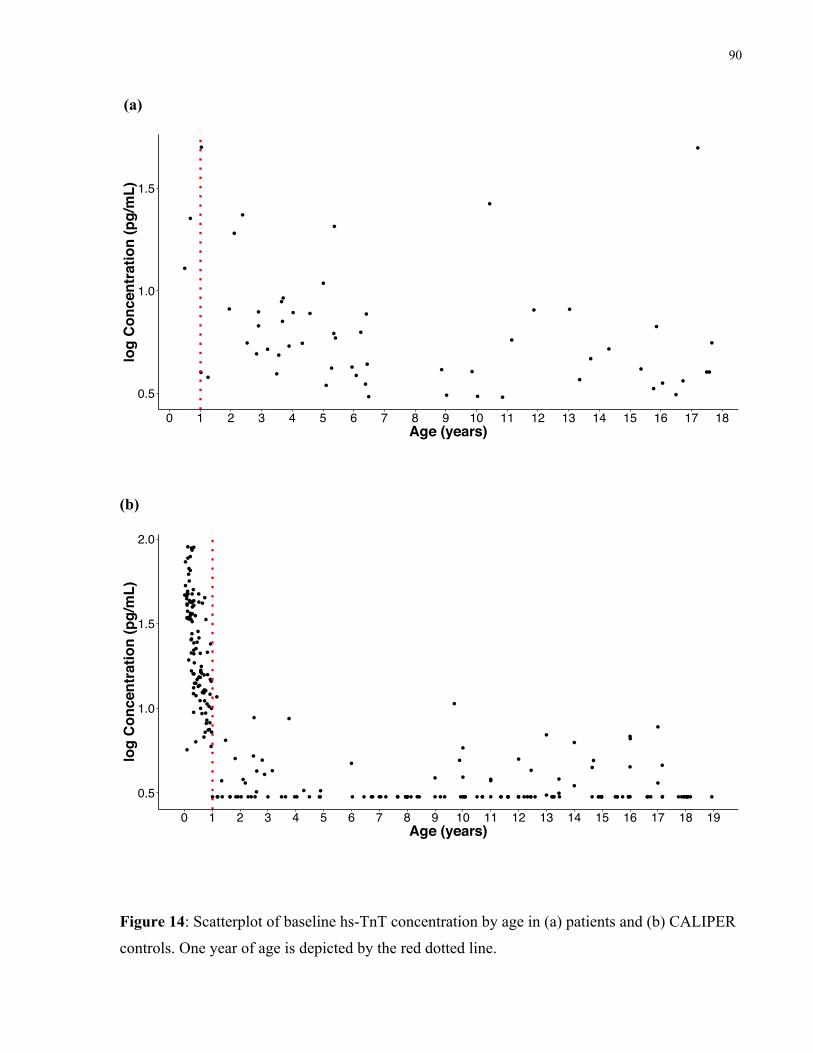
90
(a)
(b)
Figure 14: Scatterplot of baseline hs-TnT concentration by age in (a) patients and (b) CALIPER
controls. One year of age is depicted by the red dotted line.
0.5
1.0
1.5
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18Age (years)
log
Con
cent
ratio
n (p
g/m
L)
0.5
1.0
1.5
2.0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19Age (years)
log
Con
cent
ratio
n (p
g/m
L)
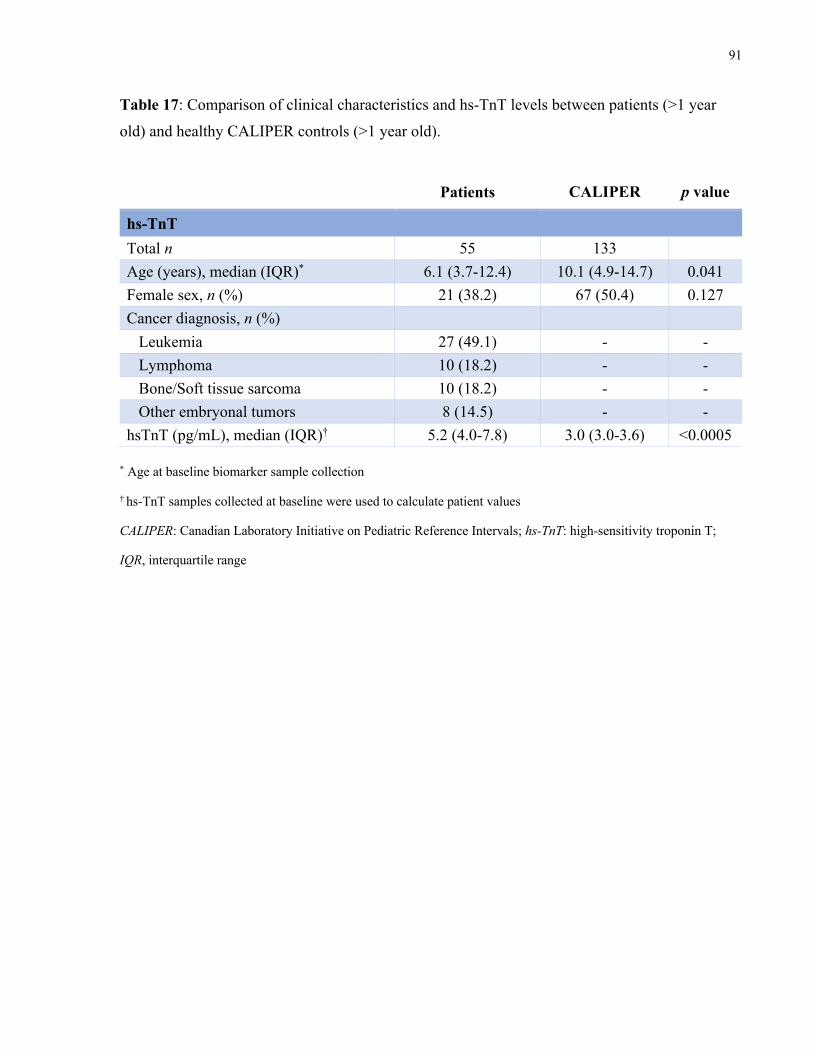
91
Table 17: Comparison of clinical characteristics and hs-TnT levels between patients (>1 year
old) and healthy CALIPER controls (>1 year old).
Patients CALIPER p value
hs-TnT Total n 55 133 Age (years), median (IQR)* 6.1 (3.7-12.4) 10.1 (4.9-14.7) 0.041 Female sex, n (%) 21 (38.2) 67 (50.4) 0.127 Cancer diagnosis, n (%) Leukemia 27 (49.1) - - Lymphoma 10 (18.2) - - Bone/Soft tissue sarcoma 10 (18.2) - - Other embryonal tumors 8 (14.5) - - hsTnT (pg/mL), median (IQR)† 5.2 (4.0-7.8) 3.0 (3.0-3.6) <0.0005
* Age at baseline biomarker sample collection
† hs-TnT samples collected at baseline were used to calculate patient values
CALIPER: Canadian Laboratory Initiative on Pediatric Reference Intervals; hs-TnT: high-sensitivity troponin T;
IQR, interquartile range
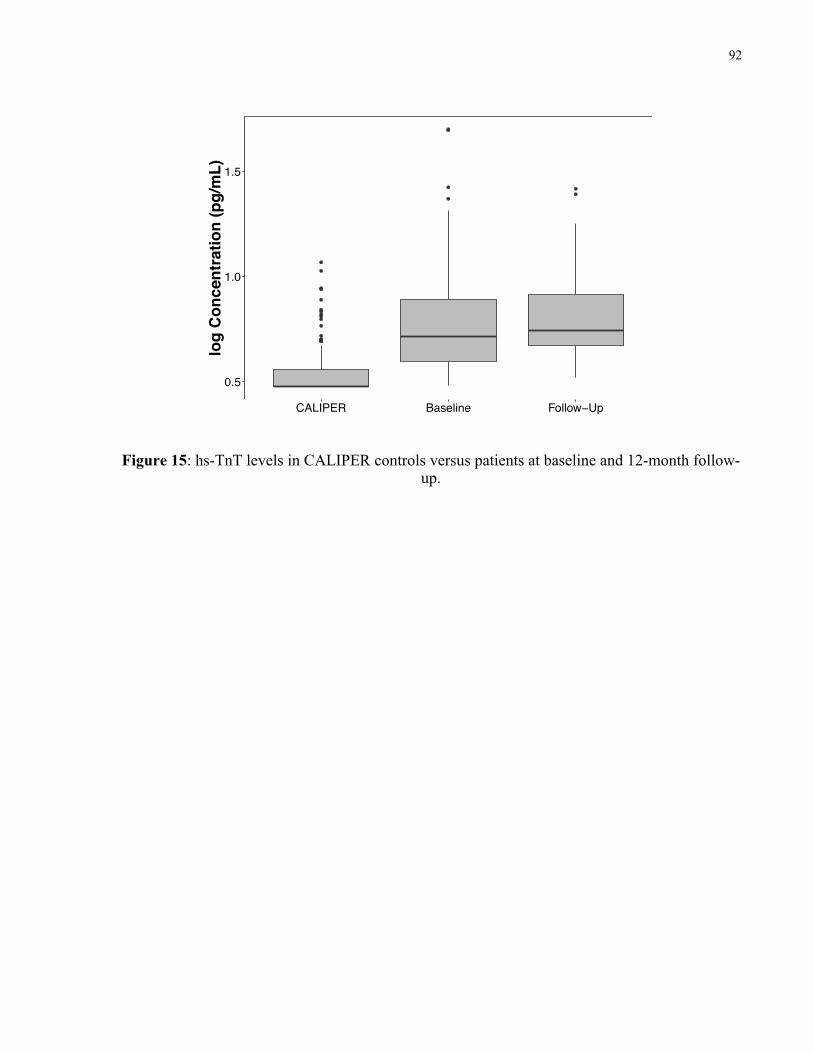
92
Figure 15: hs-TnT levels in CALIPER controls versus patients at baseline and 12-month follow-up.
0.5
1.0
1.5
CALIPER Baseline Follow−Up
log
Con
cent
ratio
n (p
g/m
L)
hs−TnT
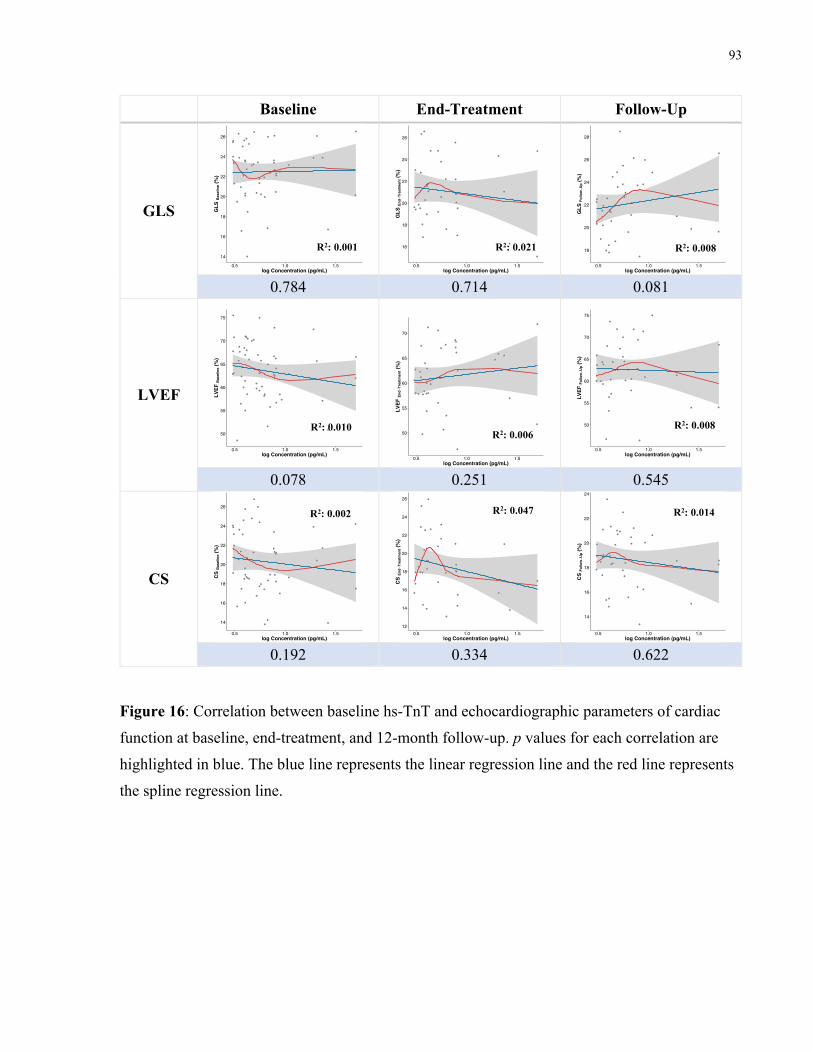
93
Baseline End-Treatment Follow-Up
GLS
0.784 0.714 0.081
LVEF
0.078 0.251 0.545
CS
0.192 0.334 0.622
Figure 16: Correlation between baseline hs-TnT and echocardiographic parameters of cardiac
function at baseline, end-treatment, and 12-month follow-up. p values for each correlation are
highlighted in blue. The blue line represents the linear regression line and the red line represents
the spline regression line.
14
16
18
20
22
24
26
0.5 1.0 1.5log Concentration (pg/mL)
GLS
Bas
elin
e (%
)
16
18
20
22
24
26
0.5 1.0 1.5log Concentration (pg/mL)
GLS
End
−Tre
atm
ent (
%)
18
20
22
24
26
28
0.5 1.0 1.5log Concentration (pg/mL)
GLS
Follo
w−U
p (%
)
50
55
60
65
70
75
0.5 1.0 1.5log Concentration (pg/mL)
LVEF
Bas
elin
e (%
)
50
55
60
65
70
0.5 1.0 1.5log Concentration (pg/mL)
LVEF
End
−Tre
atm
ent (
%)
50
55
60
65
70
75
0.5 1.0 1.5log Concentration (pg/mL)
LVEF
Follo
w−U
p (%
)
14
16
18
20
22
24
26
0.5 1.0 1.5log Concentration (pg/mL)
CS
Bas
elin
e (%
)
12
14
16
18
20
22
24
26
0.5 1.0 1.5log Concentration (pg/mL)
CS
End−
Trea
tmen
t (%
)
14
16
18
20
22
24
0.5 1.0 1.5log Concentration (pg/mL)
CS
Follo
w−U
p (%
)
R2: 0.010
R2: 0.001
R2: 0.002
R2: 0.006
R2: 0.021
R2: 0.047
R2: 0.008
R2: 0.008
R2: 0.014
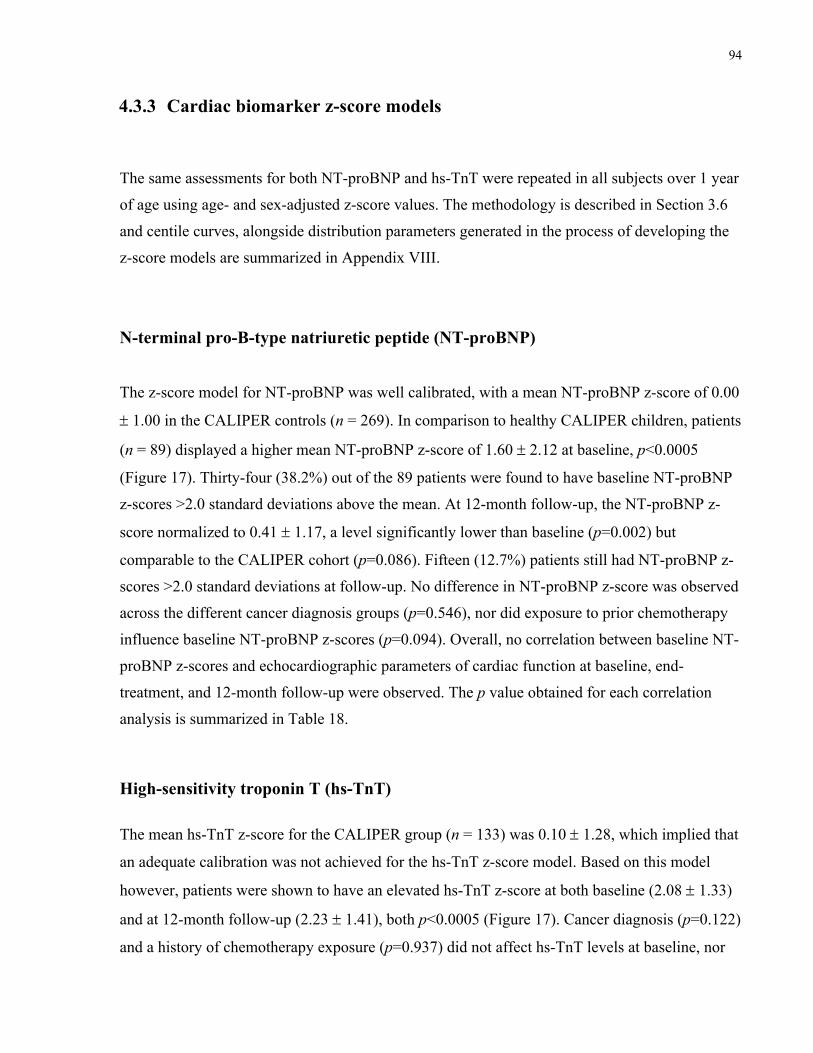
94
4.3.3 Cardiac biomarker z-score models
The same assessments for both NT-proBNP and hs-TnT were repeated in all subjects over 1 year
of age using age- and sex-adjusted z-score values. The methodology is described in Section 3.6
and centile curves, alongside distribution parameters generated in the process of developing the
z-score models are summarized in Appendix VIII.
N-terminal pro-B-type natriuretic peptide (NT-proBNP)
The z-score model for NT-proBNP was well calibrated, with a mean NT-proBNP z-score of 0.00
± 1.00 in the CALIPER controls (n = 269). In comparison to healthy CALIPER children, patients
(n = 89) displayed a higher mean NT-proBNP z-score of 1.60 ± 2.12 at baseline, p<0.0005
(Figure 17). Thirty-four (38.2%) out of the 89 patients were found to have baseline NT-proBNP
z-scores >2.0 standard deviations above the mean. At 12-month follow-up, the NT-proBNP z-
score normalized to 0.41 ± 1.17, a level significantly lower than baseline (p=0.002) but
comparable to the CALIPER cohort (p=0.086). Fifteen (12.7%) patients still had NT-proBNP z-
scores >2.0 standard deviations at follow-up. No difference in NT-proBNP z-score was observed
across the different cancer diagnosis groups (p=0.546), nor did exposure to prior chemotherapy
influence baseline NT-proBNP z-scores (p=0.094). Overall, no correlation between baseline NT-
proBNP z-scores and echocardiographic parameters of cardiac function at baseline, end-
treatment, and 12-month follow-up were observed. The p value obtained for each correlation
analysis is summarized in Table 18.
High-sensitivity troponin T (hs-TnT)
The mean hs-TnT z-score for the CALIPER group (n = 133) was 0.10 ± 1.28, which implied that
an adequate calibration was not achieved for the hs-TnT z-score model. Based on this model
however, patients were shown to have an elevated hs-TnT z-score at both baseline (2.08 ± 1.33)
and at 12-month follow-up (2.23 ± 1.41), both p<0.0005 (Figure 17). Cancer diagnosis (p=0.122)
and a history of chemotherapy exposure (p=0.937) did not affect hs-TnT levels at baseline, nor
95
were there any relationship between hs-TnT z-scores and cardiac function assessed at all three
time points (Table 18).
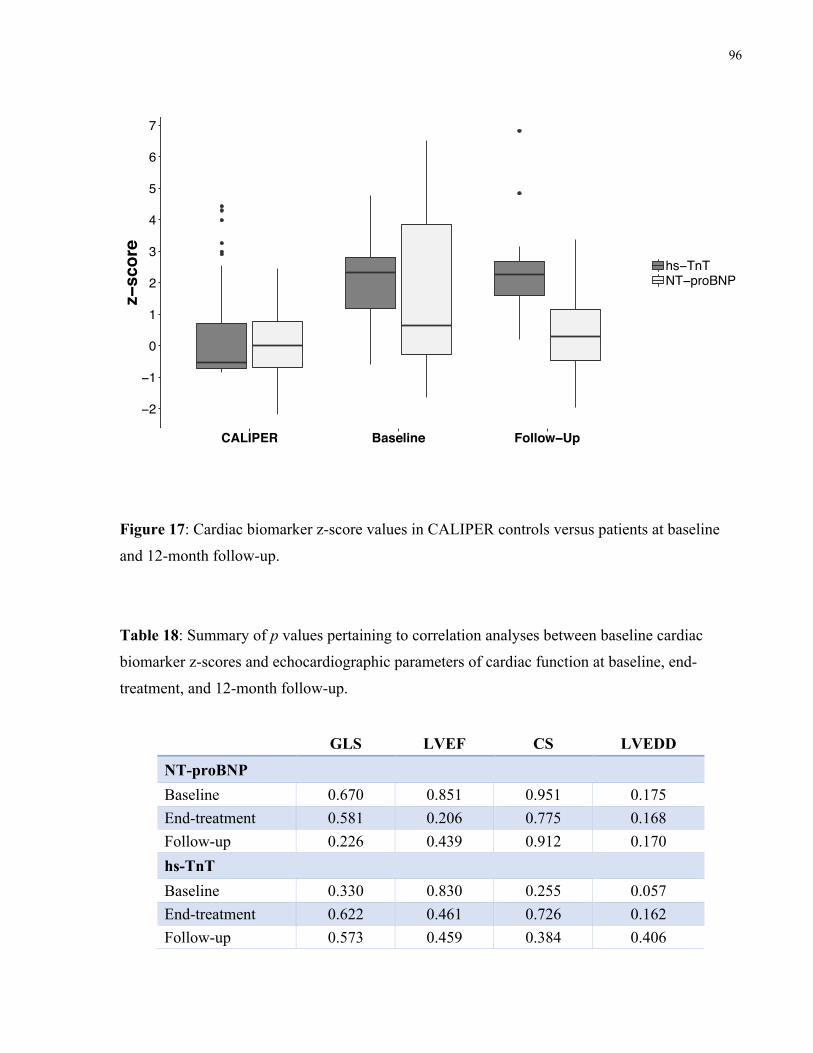
96
Figure 17: Cardiac biomarker z-score values in CALIPER controls versus patients at baseline
and 12-month follow-up.
Table 18: Summary of p values pertaining to correlation analyses between baseline cardiac
biomarker z-scores and echocardiographic parameters of cardiac function at baseline, end-
treatment, and 12-month follow-up.
GLS LVEF CS LVEDD
NT-proBNP Baseline 0.670 0.851 0.951 0.175 End-treatment 0.581 0.206 0.775 0.168 Follow-up 0.226 0.439 0.912 0.170 hs-TnT Baseline 0.330 0.830 0.255 0.057 End-treatment 0.622 0.461 0.726 0.162 Follow-up 0.573 0.459 0.384 0.406
−2
−1
0
1
2
3
4
5
6
7
CALIPER Baseline Follow−Up
z−sc
ore
hs−TnTNT−proBNP
Cardiac Biomarkers
97
Discussion
We examined the influence of baseline GLS measurements on left ventricular functional
outcomes during and one year after treatment with anthracycline chemotherapy in 176 pediatric
cancer patients with preserved LVEF. Baseline cardiac biomarker profiles alongside their
relationship with cardiac function before, during, and after anthracycline treatment were also
explored. The study cohort was drawn from the Acute Cohort of the PCS2 study. Leukemia was
the most common cancer diagnosis in our pediatric cohort and 41.5% were female. Accordingly,
our study population closely resembled the incidence trends observed in the general Canadian
population (Canadian Cancer Society 2019; Xie, Onysko, and Morrison 2018). A control cohort
of 151 children aged 4 to 18 years, without heart disease, was randomly recruited from the
broader Toronto community, and over 95% of subjects had strain measurements available for
evaluation. We further referenced data from the CALIPER project to define normal pediatric
values for our cardiac biomarkers of interest. As a nation-wide research initiative, data collected
in the context of the CALIPER project is also likely reflective of the general population in
Canada.
To address the first objective of this study, echocardiograms performed prior to the first dose of
anthracycline were examined. Specifically, we evaluated LVEF, GLS, and CS measurements
that were obtained before patients underwent anthracycline chemotherapy. Comparisons of
cardiac strain measurements were made between the patient cohort and control subjects to
elucidate whether pre-chemotherapy differences in cardiac strain exist in children with cancer.
Moreover, the effects of age and cancer diagnosis on baseline GLS and CS were examined in the
two pediatric groups.
The second objective of this study examined the influence of a lower GLS at baseline on the
cardiac response to anthracycline chemotherapy in pediatric cancer patients. To accomplish this,
a series of correlation analyses were conducted to assess whether a lower GLS at baseline was
associated with a lower GLS, LVEF, and CS at 12 months after anthracycline treatment
completion. We then identified 24 patients who had GLS <19% at baseline (‘low GLS group’)
and matched each subject to 2 patients who had a baseline GLS of >20% (‘high GLS group’,
n=48) based on age group and cancer diagnosis. Using paired analyses and standard comparative
methods, changes in LVEF, GLS, and CS were evaluated within each group as well as compared
98
between the two groups at baseline, end-treatment, and at 12-months post-anthracycline
chemotherapy.
Our final objective was to gain a better understanding of the concentration levels of cardiac
biomarkers in pediatric cancer patients prior to, and at 12-months after receiving anthracycline
treatment. NT-proBNP and hs-TnT were selected as candidate cardiac biomarkers for
investigation. Concentrations of biomarkers were evaluated using both raw values as well as z-
scores adjusted for age and sex. In specific, cardiac biomarkers in patients at baseline and
follow-up were compared against reference values obtained from the healthy CALIPER cohort.
Spline regression were also performed to explore the correlation between baseline biomarker
concentrations and LVEF, GLS, and CS measurements at baseline, end-treatment, and 12-month
follow-up.
99
5.1 Baseline cardiac strain in pediatric cancer patients (Objective 1)
The first objective of this study was to assess the baseline cardiac function, with an emphasis on
myocardial strain, in pediatric cancer patients with normal LVEF prior to exposure to
anthracycline chemotherapy. We hypothesized that there would be differences in cardiac strain
measurements between pediatric cancer patients prior to receiving anthracycline chemotherapy
and healthy controls. According to our findings, the mean GLS and CS in our patients at baseline
were 22.1 ± 2.8% and 20.0 ± 3.2% respectively. In control subjects, GLS was 21.8 ± 2.1% and
CS was 20.6 ± 2.6%. Thus, overall, no significant difference was observed between our patients
and healthy controls in terms of cardiac strain, even after taking into consideration the age
difference between the two groups. Moreover, GLS and CS in our patient cohort were both
within the normal range, based on published pediatric reference ranges (Levy et al. 2016; Jashari
et al. 2015; Tuzovic et al. 2018). While statistical differences in baseline cardiac function were
detected between certain cancer diagnosis groups and healthy controls, none were of clinical
significance. Altogether, we detected minimal differences in cardiac strain measurements
between pediatric cancer patients prior to receiving anthracycline chemotherapy and healthy
controls. Nonetheless, our findings provide added insight into the myocardial strain status in
pediatric cancer patients with preserved LVEF who are in line to receive anthracycline
chemotherapy.
There are two previous studies in children that support our finding of normal GLS measurements
in pediatric cancer patients prior to anthracycline exposure. Poterucha et al. performed standard
echocardiographic examinations and two-dimensional speckle-tracking echocardiographic
assessments in 19 pediatric cancer patients 24 hours before the first dose of doxorubicin, and at 4
and 8 months after the baseline study (Poterucha et al. 2012). Controls (n=19) matched for age,
sex, and body surface area were also recruited. The authors reported comparable GLS between
patients at baseline (19.9 ± 2.1%) and control subjects (20.5 ± 1.5%). Likewise, Agha et al.
examined LV function before and after doxorubicin treatment in a cross-sectional prospective
study of 30 asymptomatic children newly diagnosed with hematological malignancies (Agha et
al. 2016). The average GLS before chemotherapy in their cohort was measured to be 21.6 ±
2.5%.
100
In contrast to our findings, two recent studies reported lowered cardiac strain in cancer patients
before the administration of any cancer treatment. In the first study, Assuncao et al. specifically
examined cardiac alterations prior to chemotherapy in a cohort of 76 patients with acute
leukemia (Assuncao et al. 2017). None had received other chemotherapeutic agents or
radiotherapy prior to the echocardiographic assessment. A total of 76 matched control patients
without cancer nor cardiac disease were also included in the study for comparison purposes. The
median age of the acute leukemia patients was 51 years (IQR: 38 – 59) compared to 51 years
(IQR: 44 – 59) for the controls. Patients with acute leukemia had a lower GLS relative to
controls (19.3 ± 2.7% versus 20.9 ± 1.9%, p<0.001) at baseline but no difference in LVEF (62 ±
6% for patients; 62 ± 5% for controls) was observed between the two groups. The second study
involved 154 patients (age: 56 ± 9 years) with solid cancer (Tadic et al. 2018). Compared to
controls matched for age, sex and cardiovascular risk factors (e.g. arterial hypertension,
diabetes, and smoking), patients were found to have pre-existing abnormalities in GLS and CS
prior to chemotherapy exposure. In specific, baseline GLS was significantly lower in patients
(17.8 ± 3.5%) than in controls (19.1 ± 2.1%), p=0.022. Similarly, CS was lower in patients as
well (20.1 ± 4.1% versus 22.9 ± 3.5%, p<0.001). No difference in strain measurements were
observed between patients with different cancer types. These discrepancies may be related to the
fact that adult cancer patients are more likely to have comorbidities such as hypertension,
diabetes mellitus, dyslipidemia, anemia, and atrial fibrillation which may influence cardiac
function prior to anthracycline exposure. Indeed, up to 34% of patients enrolled in the two
aforementioned adult studies presented with some form of cardiac comorbidity. In comparison,
none of our pediatric patients had any major cardiac risk factors. Therefore, the impact of these
comorbidities on baseline cardiac function cannot be neglected.
It is interesting to highlight that 50 patients (28.4%) in our pediatric cohort had exposure to other
types of non-anthracycline chemotherapy prior to their baseline echocardiographic assessment.
Examples of chemotherapeutic agents used include methotrexate, cyclophosphamide, cytarabine,
etoposide, mercaptopurine, and vincristine. Some of these antineoplastic drugs have potential
cardiovascular effects (Senkus and Jassem 2011). Thus, we evaluated the impact of prior
chemotherapy exposure on baseline cardiac function. Subjects with a history of chemotherapy
exposure were found to be younger than those without such treatments (5.1 [IQR: 3.7 – 6.5]
versus 12.8 [6.4 – 15.5] years, p<0.0005). The former group also had a higher mean baseline
LVEF (65.5 ± 5.5% versus 63.4 ± 5.7%, p=0.033) as well as GLS (23.2 ± 2.3% versus 21.8 ±
2.9%, p=0.001). However, these differences were not of clinical significance. As such, the

101
findings suggest that a history of chemotherapy exposure has minimal influence on baseline
cardiac function. Nevertheless, further studies are required to confirm the effects of prior
chemotherapy on baseline cardiac function in pediatric cancer patients.
102
5.2 Cardiac outcomes in pediatric cancer patients with lower baseline GLS (Objective 2)
The second objective of this thesis was to examine whether a lower GLS at baseline impacts the
cardiac response to anthracycline chemotherapy in pediatric cancer patients with normal baseline
LVEF. We hypothesized that a lower GLS at baseline would be associated with worse cardiac
outcomes during, and 12 months after anthracycline chemotherapy compared to patients who
started with a higher GLS at baseline.
We successfully identified 24 patients with lower GLS (<19%) at baseline. The mean GLS of the
‘low GLS group’ was 17.2 ± 1.5%. Out of the 24 patients, 10 (41.7%) had a baseline GLS at the
lower limit of normal (i.e. 18% – 19%). The remaining 14 patients presented with GLS <18% at
baseline, which in the adult population, and especially during anthracycline chemotherapy,
represents a strain measurement with demonstrated predictive value for subsequent decreases in
LVEF (Plana et al. 2014; Armenian et al. 2017; Gripp et al. 2018). Despite the lower baseline
GLS in these patients, measures of baseline LVEF were in the normal range. This was expected
as only children with normal LVEF were eligible for enrolment in the PCS2 study. From the
correlation analysis, a strong positive correlation was observed between baseline GLS and
baseline LVEF. This was consistent with findings from a study of acute leukemia patients, where
a decrease in baseline GLS was associated with a reduction in LVEF at baseline (Assuncao et al.
2017). In terms of CS, the mean CS at baseline in the low GLS group was 17.6 ± 2.0%,
representing a diminished CS according to published reference ranges (Jashari et al. 2015; Levy
et al. 2016; Tuzovic et al. 2018). On one hand, this observation may be inaccurate due to the
small sample size and thus, have little clinical significance. However, in a study of myocardial
strain indices in 25 children receiving anthracycline chemotherapy, abnormal CS was detected in
19 (76%) patients as opposed to 15 (60%) patients with abnormal GLS (Pignatelli et al. 2015).
GLS was unaffected in the remaining four patients and thereby, the authors suggested that CS
may deteriorate earlier than GLS. Whether there is prognostic significance in a reduced baseline
CS in pediatric cancer patients requires further investigation.
The reason behind the lower baseline GLS measurements in the 24 patients of the low GLS
group was unclear, although it is most likely multifactorial. From our investigation, prior
chemotherapy exposure did not impact GLS at baseline as previously mentioned. Demographic
103
and clinical characteristics were similar between the low GLS group and the high GLS group as
well. Assuncao et al. found baseline GLS reduction to be associated with a decreased absolute
number of circulating lymphocytes/µL (b=-0.138, p=0.008), suggesting laboratory markers may
reflect tumor burden and cardiac function prior to chemotherapy (Assuncao et al. 2017).
Neoplastic cells are also known to produce pro-inflammatory cytokines and chemokines such as
tumor necrosis factor-α and interleukin-6, which may induce a immune response that ultimately
leads to myocardial depression and damage (Demers et al. 2012; Chechlinska, Kowalewska, and
Nowak 2010). Other general factors that may explain the lower GLS at baseline include anemia
(Horwich et al. 2002), sepsis (Fahmey et al. 2019; Abdel-Hady, Matter, and El-Arman 2012),
and hyperhydration (Valle et al. 2011). Additional studies are necessary to verify the association
between these factors and baseline myocardial strain status.
Comparisons of echocardiographic characteristics between the low GLS group and the high GLS
group uncovered that apart from differences in GLS, patients in the former group also had
significantly lower LVEF and CS at baseline. These were in line with our correlation analyses.
Interestingly, we observed a significant recovery in GLS in the low GLS group after exposure to
anthracycline chemotherapy whereas no major changes occurred in regard to LVEF and CS over
time. Five patients among the low GLS group remained with a reduced GLS at 12-month follow-
up. Unfortunately, due to the small number of observations, it was difficult to perform additional
analyses on these five patients. In contrast to the low GLS group, subjects in the high GLS group
displayed a significant decline in all three echocardiographic parameters following anthracycline
administration. At both end-treatment and 12 months after completion of anthracycline
treatment, differences in LVEF, GLS, and CS were in fact, negligible between the two patient
cohorts. Altogether, our analyses showed a regression to the mean in terms of cardiac function
over time in the two patient groups.
The finding of improved GLS after anthracycline treatment in the low GLS group was surprising
given that previous adult studies have identified a reduced baseline GLS to be an independent
predictor of LV dysfunction following anthracycline chemotherapy. Mousavi et al. reported that
a baseline GLS of ≤16% was associated with a 4.7-fold (95% CI: 1.5 – 16.0) increased risk of
major cardiac events in adult cancer patients following treatment with anthracycline
chemotherapy (Mousavi et al. 2015). Another study of adult patients with hematologic cancers
treated with anthracyclines found pre-chemotherapy GLS to be lower in patients who
developed subsequent cardiac events compared with those who did not (15.0 ± 2.8% versus
104
19.7 ± 2.7%, p<0.0001) (Ali et al. 2016). The authors also indicated that a baseline GLS of
<17.5% increased the hazard of subsequent cardiotoxicity by 1.47-fold (95% CI: 1.35 – 1.59).
More recently, Hatazawa et al. showed that baseline GLS in patients with malignant lymphoma
who developed LV dysfunction after anthracycline chemotherapy were lower compared to
those without LV dysfunction (18.5 ± 3.4% versus 21.6 ± 2.4%, p<0.001) (Hatazawa et al.
2018). Additionally, a multivariate logistic regression analysis identified a reduced baseline GLS
to be the only independent predictor of subsequent anthracycline-related cardiotoxicity (odds
ratio: 0.65, 95% CI 0.49 – 0.87, p=0.004). Nonetheless, caution must be excised when
interpreting pediatric data based on findings from adult literature. Around 20% of patients in
each of the above three studies presented with cardiac comorbidities such as hypertension,
diabetes mellitus, and hypercholesterolemia. As previously mentioned, these cardiac risk
factors may add a layer of complexity to the cardiac response to anthracycline chemotherapy.
Another fact that is worth highlighting is the longer follow-up period in the three
aforementioned studies. In the first study, Mousavi et al. followed patients for a median of 617
(IQR: 167 – 1,554) days. The median follow-up duration for the second study was even longer
at 1,593 (IQR: 13 – 2,891) days. Hatazawa et al. followed patients for 50 months. Therefore,
our current findings from the low GLS group may only represent a transient change in cardiac
function. Perhaps, deterioration in cardiac function may occur later on in time in the low GLS
group. If so, our hypothesis of worse cardiac outcomes in patients who present with a lower
GLS at baseline would be proven. On the contrary, the recovery of GLS in the low GLS group
after anthracycline exposure may simply be due to the ceiling effect, where extreme values will
tend to regress to the mean over time.
Findings from the high GLS group were consistent with a previous study by Poterucha et al.,
where cardiac function was prospectively evaluated in 19 children undergoing anthracycline
chemotherapy (Poterucha et al. 2012). The study found a significant reduction in GLS from
baseline (19.9 ± 2.1%) to 4 months after anthracycline chemotherapy (18.1 ± 2.5%), p<0.01. A
reduction in LVEF was also observed 8 months after the baseline study, but as with our findings,
the final LVEF remained in the normal range (59 ± 3%). More longitudinal studies in pediatric
cancer patients are required to elucidate the significance of these early changes in GLS.
Overall, we observed normal cardiac function in our cohort of pediatric cancer patients during,
and 12 months after anthracycline chemotherapy. The long-term significance of our findings,
and the true utility of GLS as a subclinical marker of LV systolic dysfunction in pediatric

105
cancer patients receiving anthracycline chemotherapy is yet to be determined. Nevertheless,
our findings suggest that a lower baseline GLS in pediatric cancer patients should not a reason
to preclude them from receiving anthracycline chemotherapy, especially when their baseline
LVEF measurements are in the normal range.
106
5.3 Cardiac biomarkers and cardiac function in pediatric cancer patients (Objective 3)
The third objective of this thesis was to examine cardiac biomarker levels in pediatric cancer
patients prior to anthracycline exposure, and to explore their relationship with echocardiographic
parameters before, during, and 12 months after receiving anthracycline treatment. We
specifically evaluated the concentrations of two biomarkers that are implicated in cardiac
damage: NT-proBNP and hs-TnT. Given that cancer patients may have worse cardiac function
before chemotherapy compared with healthy individuals, we hypothesized that pediatric cancer
patients would have higher levels of both NT-proBNP and hs-TnT prior to anthracycline
administration than healthy controls.
5.3.1 N-terminal pro-B-type natriuretic peptide (NT-proBNP)
A wide range of NT-proBNP levels (range: 11 – 4,046 pg/mL) was detected in our patient cohort
prior to anthracycline administration. However, this observation does not seem to be out of the
norm given that the healthy CALIPER cohort also displayed a large variability in NT-proBNP
concentrations (range: 5 – 5,756 pg/mL). In either group, NT-proBNP values were especially
high amongst the youngest individuals and decreased with age, suggesting an age effect on
plasma NT-proBNP concentration. A number of studies have addressed natriuretic peptide levels
in infants and children and reported similar findings where NT-proBNP levels were extremely
high immediately after birth followed by a drastic decline during the first few weeks of life
(Koch and Singer 2003; Mir et al. 2003; A Nir et al. 2004; Yoshibayashi et al. 1995). In a more
recent review of four studies evaluating NT-proBNP levels in infants and children, similar trends
were reported (Amiram Nir et al. 2009). Specifically, the 95th percentile for normal NT-proBNP
levels by age was highest in infants aged 0 to 2 days (11,987 pg/mL), decreasing to 5,918 pg/mL
for 3 to 11 days of age, 646 pg/mL for 1 month to 1 year of age, 413 pg/mL for 1 to 2 years of
age, 289 pg/mL for 2 to 6 years of age, 157 pg/mL for 6 to 14 years of age, and 158 pg/mL for
children aged 14 to 18 years. To date, the reason for the high levels of NT-proBNP shortly after
birth remains unclear. One possible explanation is that during the first few weeks of life, the
107
kidney undergoes progressive maturation and as a result, it may lead to physiological changes in
hemodynamics (Koch and Singer 2003). Along with the increase in pulmonary blood flow and
an increase in systematic vascular resistance due to the removal of the placenta, which has very
low resistance, the end result is an overall increase in left ventricular volume and pressure load.
In response to these perinatal circulatory changes, the ventricles may be stimulated to synthesize
BNP. Consequently, plasma BNP and NT-proBNP levels rise. In cancer patients, the increased
production of tumor necrosis factor-α, interleukin-1, interleukin-6, and other cytokines by tumor
cells could also contribute to the amplified secretion of NT-proBNP (Clerico et al. 2006). It is
proposed that with further maturation and closure of the ductus arteriosus, plasma NT-proBNP
levels gradually decline and eventually, stabilize at a new hemodynamic standard (Holmstrom,
Hall, and Thaulow 2001).
Exclusion of subjects <1 year of age from both our patient cohort and the CALIPER cohort
allowed us to perform more accurate and robust comparisons between the two groups. At
baseline, median plasma NT-proBNP concentrations were two times higher in patients than in
CALIPER controls. The younger median age in patients relative to CALIPER children may have
had some influence on NT-proBNP measurements. To account for the difference in age between
the two groups, NT-proBNP levels were compared against age-dependent 97.5th percentile
reference values published Albers et al. (Albers et al. 2006). We found elevated NT-proBNP
levels in a significantly higher proportion of patients (23.6%) than in CALIPER controls (2.2%).
Our results were consistent with findings from another prospective study conducted in 60
children with acute lymphoblastic leukemia treated with anthracycline chemotherapy
(Mavinkurve-Groothuis et al. 2013). In their study, NT-proBNP was assayed at baseline, and at
10 weeks and one year after start of treatment. Abnormal baseline NT-proBNP levels were
detected in 26% of their patients. The authors hypothesized that symptoms of severe anemia,
leukocytosis, and hyperhydration as a preventative measure for tumor lysis syndrome in children
with acute lymphoblastic leukemia may have caused the increased levels of NT-proBNP at
baseline. On the contrary, Lipshultz et al. reported in their study of 156 children with high-risk
acute lymphoblastic leukemia that approximately 90% of their patients had elevated NT-proBNP
concentrations prior to doxorubicin treatment (Lipshultz, Miller, Scully, et al. 2012). The
significantly higher percentage of abnormal NT-proBNP levels in their patients relative to our
cohort could be explained by the different reference values used to define abnormal NT-proBNP
concentrations. In their study, an increased NT-proBNP concentration was described as ≥100
pg/mL in patients ≥1 year of age and ≥150 pg/mL in patients <1 year old. As such, their
108
definition was much more simplistic compared to the one proposed by Albers et al. (Albers et al.
2006), which was the reference values used by Mavinkurve-Groothuis et al. and our study. The
difference in reference values hindered further comparisons of findings from their study with
ours. Interestingly, cancer diagnosis did not affect baseline NT-proBNP concentrations, a finding
that agrees with results published by Ekstein et al. (Ekstein et al. 2007). Moreover, exposure to
potentially cardiotoxic chemotherapy prior to the baseline study visit did not impact baseline
NT-proBNP levels either. Altogether, our findings suggest that, regardless of the type of
childhood cancer, baseline NT-proBNP levels may be elevated due to the burden of the cancer
itself.
A reduction in NT-proBNP levels relative to baseline was observed in our patients at 12 months
after completion of anthracycline chemotherapy. However, compared with CALIPER controls,
the follow-up NT-proBNP measurements still represented an elevated level. Additionally, 9.3%
of patients at follow-up were found to have NT-proBNP levels in the abnormal range. Similar
observations were made in the prospective study previously mentioned, where 20% of patients
were found to have increased levels of NT-proBNP at one year after start of anthracycline
treatment (Mavinkurve-Groothuis et al. 2013). In their study, an abnormal NT-proBNP at
baseline was also found to be predictive of abnormal NT-proBNP levels one year later. Our
findings support this observation as a higher NT-proBNP at baseline was associated with higher
levels of NT-proBNP at 12 months after anthracycline treatment in patients. Despite these
observations, it remains unclear whether an elevated NT-proBNP level after chemotherapy has
clinical value for detecting cardiotoxicity. In a study of 61 patients with breast cancer treated
with trastuzumab, NT-proBNP measured during treatment in fact, had no predictive value for
later trastuzumab-induced cardiac dysfunction. Further investigation is required to elucidate the
significance of elevated NT-proBNP levels before, during and after treatment on subsequent
cardiac outcomes.
Few studies have examined the relationship between NT-proBNP levels and echocardiographic
measures of cardiac function in pediatric cancer patients. From our spline regression analyses,
we found no relation between NT-proBNP levels at baseline and LVEF, GLS, CS, and LVEDD
measured at baseline, end-treatment, and 12-month follow-up. Nor were there any relationship
between NT-proBNP levels at 12-month follow-up and echocardiographic parameters assessed at
the same time point. Causal relationships between baseline NT-proBNP levels and subsequent
LV dysfunction could not be determined from our study.
109
Comparable observations have been reported in three previous studies. Ekstein et al. examined
NT-proBNP levels and assessed left ventricular function before, during, and after anthracycline
treatment in 25 children newly diagnosed with cancer (Ekstein et al. 2007). Measures of left
ventricular function were normal both at baseline and at the end of the follow-up period. The
authors observed no correlation between elevated NT-proBNP concentrations and cardiac
function. Mavinkurve-Groothuis et al. evaluated myocardial strain in asymptomatic long-term
survivors of childhood cancer and found no relation between abnormal NT-proBNP levels and
lower GLS (Mavinkurve-Groothuis et al. 2010). Zidan et al. evaluated biomarker levels and
cardiac function in 80 children treated with anthracycline and found abnormally high levels of
NT-proBNP in 30% of the study population (Zidan et al. 2015). Between the normal and
abnormal NT-proBNP groups, no significant difference in systolic or diastolic cardiac function
was detected. Overall, these observations reflect a potentially superior sensitivity of NT-proBNP
to early cardiac damage compared with routine echocardiographic measures. However, this
could not be fully verified in our study.
5.3.2 High-sensitivity troponin T (hs-TnT)
Given its novelty, limited data exist on the use of high-sensitivity troponin measures in pediatric
cancer patients treated with anthracycline chemotherapy. Therefore, our findings provide new
insights into the profile of hs-TnT in pediatric cancer patients before and 12 months after
anthracycline exposure.
Overall, findings from our hs-TnT analyses were analogous to those obtained for NT-proBNP.
Concentrations of hs-TnT at baseline varied from a low of 3 pg/mL to a high of 50 pg/mL in the
patient cohort and we detected concentrations of 3 pg/mL to 90 pg/mL in the CALIPER cohort.
Once again, the highest hs-TnT levels were primarily found in the youngest children, suggesting
that physiological remodeling of the heart may be occurring shortly after birth. An interesting
finding was that having a history of chemotherapy exposure had no impact on baseline hs-TnT
levels. Comparisons between patients and healthy CALIPER children revealed that patients had
elevated hs-TnT levels at baseline as well as at 12 months after anthracycline treatment.
Specifically, 10.9% of patients had hs-TnT levels in the abnormal range at baseline and 4.7% at
110
12 months after completion of anthracycline chemotherapy. A study of 219 doxorubicin-treated
pediatric patients with acute lymphoblastic leukemia obtained 2,377 serial measurements of
cardiac TnT and similarly documented elevated cardiac TnT concentrations of >10 ng/L in 10%
of patients prior to doxorubicin treatment (Lipshultz et al. 2004). In another study in adult study
involving mixed acute myeloid and non-Hodgkin lymphoma patients, 3.8% of 78 patients
displayed elevated cardiac troponin T levels of >70 ng/L at baseline (Auner et al. 2001;
McGowan et al. 2017). Similar results had also been published by Missov et al. where higher
levels of troponin were detected in cancer patients prior to receiving anthracycline treatment
compared to healthy controls (36.5 ± 27.5 pg/mL versus 19.5 ± 23.1 pg/mL, p<0.01) (Missov et
al. 1997). Altogether, these findings provide further evidence that cancer itself may cause injury
to cardiomyocytes even before any exposure to anthracycline chemotherapy. On the contrary,
Mavinkurve-Groothuis et al. did not find any abnormalities in cardiac TnT levels before the start
of anthracycline treatment (Mavinkurve-Groothuis et al. 2013). It was only after a cumulative
anthracycline dose of 120 mg/m2 that abnormal cardiac TnT levels were detected in 11% of
patients. At one year after start of chemotherapy, 2.5% of pediatric patients had elevated cardiac
TnT levels, an incidence comparable to our findings. As such, more studies are necessary to
determine the clinical significance of an elevated hs-TnT concentration before, during, and after
anthracycline chemotherapy in pediatric cancer patients.
Despite the elevation in baseline hs-TnT concentrations, no correlation was demonstrated
between hs-TnT levels at baseline and LVEF, GLS, and CS assessed at baseline, end-treatment,
and 12-month follow-up. Similarly, hs-TnT levels at follow-up had no relation with
echocardiographic measures of cardiac function. Our findings are consistent with those reported
by Cheung et al. in a study of 100 adult survivors of childhood leukemia previously treated with
anthracycline chemotherapy (Y. Cheung et al. 2013). In their study, longitudinal systolic strain
rate was lower in patients who had elevated hs-TnT levels, but no differences in LVEF, GLS and
CS were found between survivors with and without elevated hs-TnT concentrations. Future
research may help validate the utility of hs-TnT for the early detection of cardiotoxicity in
children with cancer.
111
5.3.3 Cardiac biomarkers z-score assessment
A z-score model adjusting for both age and sex was successfully constructed for NT-proBNP.
Overall, findings based on z-score values were consistent with results obtained from using raw
values. This signals that sex does not influence NT-proBNP levels in pediatric cancer patients
before, and shortly after receiving anthracycline chemotherapy. While our findings agree with
select previous studies (Ekstein et al. 2007; A Nir et al. 2004), others have reported the opposite
where clear sex differences in NT-proBNP concentrations could be observed (Koch and Singer
2003; Leosdottir et al. 2011). Kim et al. had reported sex differences in the prognostic value of
NT-proBNP in heart failure, where a higher NT-proBNP level at hospital admission was an
independent predictor of subsequent mortality only in men (hazard ratio: 1.74, 95% CI: 1.25 –
2.43, p=0.001) but not in women (Kim et al. 2017). We were not able to prove the prognostic
value of NT-proBNP as we did not detect any relation between baseline NT-proBNP z-scores
and abnormalities in cardiac function at 12 months after anthracycline completion. Perhaps, a
longer follow-up duration is required for relevant outcomes to be detected.
In contrast to NT-proBNP, an adequate z-score model was not generated for hs-TnT. Therefore,
our findings from the z-score analyses may not be accurate, although they were comparable to
results obtained from using raw hs-TnT values. The reason for the inadequate model could be
due to the relatively small CALIPER sample size (n=133) used to build the z-score model. More
importantly however, it could be attributed to the lack of variation in biomarker concentrations
among the CALIPER children who had hs-TnT measurements. In specific, 93 (69.9%) out of the
133 children had a hs-TnT level of 3.0 pg/mL, which represented the detection limit of the hs-
TnT assay used. This lack of variability in data was disadvantageous for generating robust z-
score models. Larger datasets from healthy children may help address this shortcoming.
112
5.4 Strengths and Limitations of the Study
5.4.1 Strengths of the study
The unique multidisciplinary design of the PCS2 study provides an unparalleled data resource for
longitudinal research of acute and late-onset cardiac dysfunction resulting from exposure to
anthracycline chemotherapy in children with cancer. As with all longitudinal studies, strengths
include the ability to follow select individuals within a given cohort over time and the capacity to
relate specific events to particular treatment exposures (Caruana et al. 2015). In the current
study, we were able to identify a subgroup of pediatric cancer patients with normal LVEF but
lower GLS at baseline, and obtain detailed information pertaining to their cardiac outcomes
during and following anthracycline chemotherapy. Comparisons with age- and cancer diagnosis-
matched ‘high baseline GLS’ patients allowed for a clean assessment of differences in changes in
cardiac function over time while accounting for the possible age effect on strain indices (Abou et
al. 2017; Alcidi et al. 2018). Multiple regression analyses, adjusting for age, were also performed
to confirm our findings. To our knowledge, this is the first prospective study that explored the
importance of baseline GLS measurements on left ventricular functional outcomes in a group of
pediatric cancer patients receiving anthracycline chemotherapy. Our findings may inspire future
research. Additionally, all echocardiograms and strain measurements were obtained according to
a standardized investigatory procedure. Thus, we were able to control for intervendor variability,
a key limitation to using strain parameters for longitudinal evaluations. By referencing data
collected by the CALIPER project, it also allowed us to compare cardiac biomarker
measurements in pediatric cancer patients against reference values that are highly reflective of
the general population. In addition, few studies have used high-sensitivity troponin assays in the
context of cardio-oncology; none that have investigated its utility in the pediatric cancer
population. Thus, our findings provide novel insights into the hs-TnT profile in children with
cancer. Altogether, our findings add to the understanding of the cardiac status, in relation to
select cardiac biomarkers, in pediatric cancer patients before and shortly after anthracycline
treatment.
113
5.4.2 Limitations of the study
Incomplete or interrupted follow-up of study participants represent a common limitation of
longitudinal studies. Beyond the challenges inherent to the study design, there are some
limitations to our study that merit consideration. First, the 12-month follow-up duration used in
our study is relatively short in the context of anthracycline-related cardiotoxicity, as important
myocardial changes often take years to decades after chemotherapy exposure to appear. In order
to address the long-term cardiac sequelae in pediatric cancer patients receiving anthracyclines, a
registry for our PCS2 participants has been established (Core 4 of the PCS2 study) to
longitudinally follow them well into their adult years. Second, of the 51 patients who were
excluded from our echocardiographic analyses due to quality issues with the scans for baseline
GLS measurement, some may have had unmeasured reduced GLS at baseline and severe cardiac
outcomes during and following anthracycline treatment. In addition, there were patients who
died before the 12-month follow-up visit. These may have led to an underestimation of the
incidence of cardiac dysfunction in our study cohort. However, no difference in baseline clinical
and echocardiographic characteristics were observed between the 176 patients included in our
study and the 127 Acute Cohort patients who were excluded due to aforementioned reasons
(Table 8). Baseline measures of cardiac function including LVEF, GLS, and CS were also in the
normal range as defined by the American Society of Echocardiography and the European
Association of Cardiovascular Imaging (Plana et al. 2014) for all patients who died prior to the
follow-up. Therefore, it is unlikely that the exclusion of these patients would have had a
significant effect on our findings. Third, a substantial number (45.1%) of patient biomarker
samples had to be excluded from analysis, either due to low sample quantity or because they
were yet to be assayed. As such, this may have limited the power of analyses to detect subtle, yet
important changes in cardiac biomarkers. In relation to this was the lack of variation in
CALIPER hs-TnT concentrations, which impeded the construction of an appropriate z-score
model. Further investigations using larger reference datasets are required to confirm our
biomarker findings.

114
5.5 Conclusion
Pediatric cancer patients with preserved LVEF presented with similar myocardial strain values
prior to anthracycline exposure compared to healthy controls. Patients with a lower GLS at
baseline exhibited improvements in GLS 12 months after completion of anthracycline
chemotherapy and cardiac function assessed before the last dose of anthracycline treatment
reflected that of the 12-month follow-up. NT-proBNP and hs-TnT were both elevated at baseline
in patients compared to healthy CALIPER controls, and remained elevated after anthracycline
chemotherapy completion, but no associations between baseline biomarker values and
echocardiographic parameters of LV systolic function were detected. Overall, our findings
suggest that a lower GLS at baseline is not a reason to preclude patients from receiving
anthracycline chemotherapy. There is also undefined value in cardiac biomarker measurements
obtained prior to anthracycline exposure.
115
5.6 Future Directions
Based on our findings, it appears that a lower GLS at baseline does not influence left ventricular
functional outcomes 12 months after anthracycline chemotherapy in children with cancer.
However, as cardiotoxicity related to anthracycline chemotherapy often takes years to decades to
appear, our findings may only represent a transient change in GLS. A longer follow-up duration
may uncover significant myocardial changes that can be explained by differences in baseline
GLS. It is important to note that many of our patients in the ‘low GLS group’ had a baseline GLS
measurement at the lower limit of normal, instead of being completely abnormal. All patients
had normal LVEF at baseline as well. Thus, our conclusions cannot be extended to children who
present with truly abnormal GLS values prior to receiving anthracycline chemotherapy. If
possible, future studies should attempt to assess cardiac outcomes in children with truly
abnormal GLS at baseline and compared the findings with our results. The findings would be
especially valuable in helping tailor chemotherapy regimens based on the cardiac strain status in
pediatric cancer patients and to optimize treatment efficacy as well as to improve long-term
cardiac health in childhood cancer survivors.
The reason behind the lower GLS measurements in our patients was unclear. Past exposure to
potentially cardiotoxic non-anthracycline chemotherapy did not have a significant impact on
baseline GLS from our investigation. As circulating lymphocytes (Assuncao et al. 2017), pro-
inflammatory cytokines and chemokines (Demers et al. 2012; Chechlinska, Kowalewska, and
Nowak 2010), anemia (Horwich et al. 2002), sepsis (Fahmey et al. 2019; Abdel-Hady, Matter,
and El-Arman 2012), and hyperhydration (Valle et al. 2011) have all been implemented in
myocardial depression and damage in cancer patients, it would be interesting to further explore
the impact of these factors on GLS in future pediatric studies.
In terms of cardiac biomarkers, we were not able to fully verify the importance of elevated NT-
proBNP levels before, during, and after treatment on subsequent cardiac damage. As for hs-TnT,
our investigations were purely exploratory since no other groups have studied this biomarker in
the context of pediatric cancer. Thus, additional studies with larger samples sizes are required to
verify our findings and to clarify the associations between cardiac biomarker levels and cardiac
function. Markers of myocardial ischemia or necrosis such as fatty acid binding protein and
glycogen phosphorylase isoenzyme-BB (Cardinale et al. 2017; Horacek et al. 2008), high-
116
sensitivity C-reactive protein (Onitilo et al. 2012), and myeloperoxidase (Ky et al. 2014) are
newer biomarkers with proposed predictive value for the development of LV dysfunction after
chemotherapy exposure. A closer examination of these biomarkers in pediatric cancer patients
may be of interest.
Overall, the prognostic value of a lower GLS at baseline remains to be determined. Cardiac
biomarkers may complement cardiac imaging for the early detection of cardiac dysfunction in
pediatric cancer patients, but their usefulness is still indeterminate. This thesis has contributed to
the understanding of the myocardial strain status in pediatric cancer patients prior to
anthracycline exposure and their cardiac outcomes 12 months after treatment. The future studies
suggested above will help elucidate the full spectrum of damage associated with curative cancer
therapy in children who present with different GLS and biomarker measurements. Altogether,
this work along with future studies will help devise possible interventions that may be integrated
into treatment and follow-up plans to mitigate potential cardiac complications. Such
advancements in pediatric cancer treatment and management will ensure that survivors can
continue to experience the best possible quality of life for decades following their childhood
cancer diagnosis.
117
References
(Lieke), Feijen E A M, Font‐Gonzalez Anna, Van der Pal Helena J H., Kok Wouter E M., Geskus Ronald B., Ronckers Cécile M., Bresters Dorine, et al. 2019. “Risk and Temporal Changes of Heart Failure Among 5‐Year Childhood Cancer Survivors: A DCOG‐LATER Study.” Journal of the American Heart Association 8 (1): e009122.
Abdel-Hady, Hesham E, Mohamed K Matter, and Mohamed M El-Arman. 2012. “Myocardial Dysfunction in Neonatal Sepsis: A Tissue Doppler Imaging Study.” Pediatric Critical Care Medicine : A Journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies 13 (3): 318–23.
Abiko, Masayuki, Kei Inai, Eriko Shimada, Seiji Asagai, and Toshio Nakanishi. 2018. “The Prognostic Value of High Sensitivity Cardiac Troponin T in Patients with Congenital Heart Disease.” Journal of Cardiology 71 (4): 389–93.
Abou, Rachid, Melissa Leung, Mand J H Khidir, Ron Wolterbeek, Martin J Schalij, Nina Ajmone Marsan, Jeroen J Bax, and Victoria Delgado. 2017. “Influence of Aging on Level and Layer-Specific Left Ventricular Longitudinal Strain in Subjects Without Structural Heart Disease.” The American Journal of Cardiology 120 (11): 2065–72.
Adams, M Jacob, and Steven E Lipshultz. 2005. “Pathophysiology of Anthracycline- and Radiation-Associated Cardiomyopathies: Implications for Screening and Prevention.” Pediatric Blood & Cancer 44 (7): 600–606.
Adeli, Khosrow. 2014. “Closing the Gaps in Pediatric Reference Intervals: An Update on the CALIPER Project.” Clinical Biochemistry 47 (9): 737–39.
Agha, Hala, Lobna Shalaby, Wael Attia, Gaser Abdelmohsen, Osama Abdel Aziz, and Mohamed Youssef Abdel Rahman. 2016. “Early Ventricular Dysfunction After Anthracycline Chemotherapy in Children.” Pediatric Cardiology 37 (3): 537–44.
Albers, Stefanie, Thomas S Mir, Munif Haddad, and Stephanie Laer. 2006. “N-Terminal pro-Brain Natriuretic Peptide: Normal Ranges in the Pediatric Population Including Method Comparison and Interlaboratory Variability.” Clinical Chemistry and Laboratory Medicine 44 (1): 80–85.
Alcidi, Gian Marco, Roberta Esposito, Vincenzo Evola, Ciro Santoro, Maria Lembo, Regina Sorrentino, Francesco Lo Iudice, et al. 2018. “Normal Reference Values of Multilayer Longitudinal Strain According to Age Decades in a Healthy Population: A Single-Centre Experience.” European Heart Journal Cardiovascular Imaging 19 (12): 1390–96.
Ali, Mohammed T, Evin Yucel, Souhila Bouras, Lin Wang, Hong-Wen Fei, Elkan F Halpern, and Marielle Scherrer-Crosbie. 2016. “Myocardial Strain Is Associated with Adverse Clinical Cardiac Events in Patients Treated with Anthracyclines.” Journal of the American Society of Echocardiography : Official Publication of the American Society of Echocardiography 29 (6): 522-527.e3.
118
Aminkeng, Folefac, Amit P Bhavsar, Henk Visscher, Shahrad R Rassekh, Yuling Li, Jong W Lee, Liam R Brunham, et al. 2015. “A Coding Variant in RARG Confers Susceptibility to Anthracycline-Induced Cardiotoxicity in Childhood Cancer.” Nature Genetics 47 (9): 1079–84.
Amzulescu, M S, M De Craene, H Langet, A Pasquet, D Vancraeynest, A C Pouleur, J L Vanoverschelde, and B L Gerber. 2019. “Myocardial Strain Imaging: Review of General Principles, Validation, and Sources of Discrepancies.” European Heart Journal - Cardiovascular Imaging 20 (6): 605–19.
Armenian, Saro H, Gregory T Armstrong, Gregory Aune, Eric J Chow, Matthew J Ehrhardt, Bonnie Ky, Javid Moslehi, et al. 2018. “Cardiovascular Disease in Survivors of Childhood Cancer: Insights Into Epidemiology, Pathophysiology, and Prevention.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 36 (21): 2135–44.
Armenian, Saro H, Melissa M Hudson, Renee L Mulder, Ming Hui Chen, Louis S Constine, Mary Dwyer, Paul C Nathan, et al. 2015. “Recommendations for Cardiomyopathy Surveillance for Survivors of Childhood Cancer: A Report from the International Late Effects of Childhood Cancer Guideline Harmonization Group.” The Lancet. Oncology 16 (3): e123-36.
Armenian, Saro H, Christina Lacchetti, Ana Barac, Joseph Carver, Louis S Constine, Neelima Denduluri, Susan Dent, et al. 2017. “Prevention and Monitoring of Cardiac Dysfunction in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 35 (8): 893–911.
Armstrong, Gregory T, Vijaya M Joshi, Kirsten K Ness, Thomas H Marwick, Nan Zhang, DeoKumar Srivastava, Brian P Griffin, et al. 2015. “Comprehensive Echocardiographic Detection of Treatment-Related Cardiac Dysfunction in Adult Survivors of Childhood Cancer: Results From the St. Jude Lifetime Cohort Study.” Journal of the American College of Cardiology 65 (23): 2511–22.
Armstrong, Gregory T, Toana Kawashima, Wendy Leisenring, Kayla Stratton, Marilyn Stovall, Melissa M Hudson, Charles A Sklar, Leslie L Robison, and Kevin C Oeffinger. 2014. “Aging and Risk of Severe, Disabling, Life-Threatening, and Fatal Events in the Childhood Cancer Survivor Study.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 32 (12): 1218–27.
Armstrong, Gregory T, Qi Liu, Yutaka Yasui, Joseph P Neglia, Wendy Leisenring, Leslie L Robison, and Ann C Mertens. 2009. “Late Mortality among 5-Year Survivors of Childhood Cancer: A Summary from the Childhood Cancer Survivor Study.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 27 (14): 2328–38.
Armstrong, Gregory T, Marilyn Stovall, and Leslie L Robison. 2010. “Long-Term Effects of Radiation Exposure among Adult Survivors of Childhood Cancer: Results from the Childhood Cancer Survivor Study.” Radiation Research 174 (6): 840–50.
Arola, O J, A Saraste, K Pulkki, M Kallajoki, M Parvinen, and L M Voipio-Pulkki. 2000. “Acute Doxorubicin Cardiotoxicity Involves Cardiomyocyte Apoptosis.” Cancer Research 60 (7):
119
1789–92.
Aroney, Constantine N, and Louise Cullen. 2016. “Appropriate Use of Serum Troponin Testing in General Practice: A Narrative Review.” The Medical Journal of Australia 205 (2): 91–94.
Asdahl, Peter H, Jeanette F Winther, Trine G Bonnesen, Sofie De Fine Licht, Thorgerdur Gudmundsdottir, Harald Anderson, Laura Madanat-Harjuoja, et al. 2015. “The Adult Life After Childhood Cancer in Scandinavia (ALiCCS) Study: Design and Characteristics.” Pediatric Blood & Cancer 62 (12): 2204–10.
Assuncao, Bruna Morhy Borges Leal, Mark D Handschumacher, Andrew M Brunner, Evin Yucel, Philipp E Bartko, Kai-Hung Cheng, Orlando Campos, Amir T Fathi, Timothy C Tan, and Marielle Scherrer-Crosbie. 2017. “Acute Leukemia Is Associated with Cardiac Alterations before Chemotherapy.” Journal of the American Society of Echocardiography : Official Publication of the American Society of Echocardiography.
Auner, H W, C Tinchon, W Linkesch, G Halwachs-Baumann, and H Sill. 2001. “Correspondence Re: O. J. Arola et Al., Acute Doxorubicin Cardiotoxicity Involves Cardiomyocyte Apoptosis. Cancer Res., 60: 1789-1792, 2000.” Cancer Research. United States.
Bhakta, Nickhill, Qi Liu, Kirsten K Ness, Malek Baassiri, Hesham Eissa, Frederick Yeo, Wassim Chemaitilly, et al. 2017. “The Cumulative Burden of Surviving Childhood Cancer: An Initial Report from the St Jude Lifetime Cohort Study (SJLIFE).” Lancet (London, England) 390 (10112): 2569–82.
Bhakta, Nickhill, Qi Liu, Frederick Yeo, Malek Baassiri, Matthew J Ehrhardt, Deo K Srivastava, Monika L Metzger, et al. 2016. “Cumulative Burden of Cardiovascular Morbidity in Paediatric, Adolescent, and Young Adult Survivors of Hodgkin’s Lymphoma: An Analysis from the St Jude Lifetime Cohort Study.” The Lancet. Oncology 17 (9): 1325–34.
Biasillo, Gina, Carlo M Cipolla, and Daniela Cardinale. 2017. “Cardio-Oncology: Gaps in Knowledge, Goals, Advances, and Educational Efforts.” Current Oncology Reports 19 (8): 55.
Biering-Sørensen, Tor, Sofie Reumert Biering-Sørensen, Flemming Javier Olsen, Morten Sengeløv, Peter Godsk Jørgensen, Rasmus Mogelvang, Amil M Shah, and Jan Skov Jensen. 2017. “Global Longitudinal Strain by Echocardiography Predicts Long-Term Risk of Cardiovascular Morbidity and Mortality in a Low-Risk General Population: The Copenhagen City Heart Study.” Circulation. Cardiovascular Imaging 10 (3): e005521.
Blanco, Javier G, Wendy M Leisenring, Vanessa M Gonzalez-Covarrubias, Toana I Kawashima, Stella M Davies, Mary V Relling, Leslie L Robison, Charles A Sklar, Marilyn Stovall, and Smita Bhatia. 2008. “Genetic Polymorphisms in the Carbonyl Reductase 3 Gene CBR3 and the NAD(P)H:Quinone Oxidoreductase 1 Gene NQO1 in Patients Who Developed Anthracycline-Related Congestive Heart Failure after Childhood Cancer.” Cancer 112 (12): 2789–95.
Blanco, Javier G, Can-Lan Sun, Wendy Landier, Lu Chen, Diego Esparza-Duran, Wendy Leisenring, Allison Mays, et al. 2012. “Anthracycline-Related Cardiomyopathy after
120
Childhood Cancer: Role of Polymorphisms in Carbonyl Reductase Genes--a Report from the Children’s Oncology Group.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 30 (13): 1415–21.
Bloom, Michelle W, Carine E Hamo, Daniela Cardinale, Bonnie Ky, Anju Nohria, Lea Baer, Hal Skopicki, et al. 2016. “Cancer Therapy-Related Cardiac Dysfunction and Heart Failure: Part 1: Definitions, Pathophysiology, Risk Factors, and Imaging.” Circulation. Heart Failure 9 (1): e002661.
Bradley, Nicole M E, Maria F Lorenzi, Zenaida Abanto, Sam Sheps, Anne Marie Broemeling, John J Spinelli, Karen Goddard, Sheila Pritchard, Paul Rogers, and Mary L McBride. 2010. “Hospitalisations 1998–2000 in a British Columbia Population-Based Cohort of Young Cancer Survivors: Report of the Childhood/Adolescent/Young Adult Cancer Survivors (CAYACS) Research Program.” European Journal of Cancer 46 (13): 2441–48.
Brewster, D H, D Clark, L Hopkins, J Bauer, S H Wild, A B Edgar, and W H Wallace. 2014. “Subsequent Hospitalisation Experience of 5-Year Survivors of Childhood, Adolescent, and Young Adult Cancer in Scotland: A Population Based, Retrospective Cohort Study.” British Journal of Cancer 110 (5): 1342–50.
Bulten, Ben F, Martina Sollini, Roberto Boni, Katrin Massri, Lioe-Fee de Geus-Oei, Hanneke W M van Laarhoven, Riemer H J A Slart, and Paola A Erba. 2019. “Cardiac Molecular Pathways Influenced by Doxorubicin Treatment in Mice.” Scientific Reports 9 (1): 2514.
Çağlar, Ayla Akca, Aynur Oğuz, Faruk Güçlü Pınarlı, Ceyda Karadeniz, Arzu Okur, Aysun Bideci, Ülker Koçak, and Hüseyin Bora. 2014. “Thyroid Abnormalities in Survivors of Childhood Cancer.” Journal of Clinical Research in Pediatric Endocrinology 6 (3): 144–51.
Canadian Cancer Society/National Cancer Institute of Canada. 2008. “Canadian Cancer Statistics 2008.” Toronto, ON, Canada.
Canadian Cancer Society. 2019. “Childhood Cancer Statistics.” 2019. http://www.cancer.ca/en/cancer-information/cancer-101/childhood-cancer-statistics/?region=on.
Cardinale, Daniela, Colombo Alessandro, Bacchiani Giulia, Tedeschi Ines, Meroni Carlo A., Veglia Fabrizio, Civelli Maurizio, et al. 2015. “Early Detection of Anthracycline Cardiotoxicity and Improvement With Heart Failure Therapy.” Circulation 131 (22): 1981–88.
Cardinale, Daniela, Gina Biasillo, Michela Salvatici, Maria Teresa Sandri, and Carlo Maria Cipolla. 2017. “Using Biomarkers to Predict and to Prevent Cardiotoxicity of Cancer Therapy.” Expert Review of Molecular Diagnostics 17 (3): 245–56.
Caruana, Edward Joseph, Marius Roman, Jules Hernández-Sánchez, and Piergiorgio Solli. 2015. “Longitudinal Studies.” Journal of Thoracic Disease 7 (11): E537-40.
Carver, Joseph R, Charles L Shapiro, Andrea Ng, Linda Jacobs, Cindy Schwartz, Katherine S Virgo, Karen L Hagerty, Mark R Somerfield, and David J Vaughn. 2007. “American Society of Clinical Oncology Clinical Evidence Review on the Ongoing Care of Adult Cancer Survivors: Cardiac and Pulmonary Late Effects.” Journal of Clinical Oncology :
121
Official Journal of the American Society of Clinical Oncology 25 (25): 3991–4008.
Çetin, Süha, Kadir Babaoğlu, Eviç Z Başar, Murat Deveci, and Funda Çorapçıoğlu. 2018. “Subclinical Anthracycline-Induced Cardiotoxicity in Long-Term Follow-up of Asymptomatic Childhood Cancer Survivors: Assessment by Speckle Tracking Echocardiography.” Echocardiography 35 (2): 234–40.
Charbonnel, Clement, Raphaele Convers-Domart, Sophie Rigaudeau, Anne Laure Taksin, Nicolas Baron, Juliette Lambert, Stephanie Ghez, et al. 2017. “Assessment of Global Longitudinal Strain at Low-Dose Anthracycline-Based Chemotherapy, for the Prediction of Subsequent Cardiotoxicity.” European Heart Journal Cardiovascular Imaging 18 (4): 392–401.
Chechlinska, Magdalena, Magdalena Kowalewska, and Radoslawa Nowak. 2010. “Systemic Inflammation as a Confounding Factor in Cancer Biomarker Discovery and Validation.” Nature Reviews Cancer 10 (January): 2.
Cheng, Susan, Martin G Larson, Elizabeth L McCabe, Ewa Osypiuk, Birgitta T Lehman, Plamen Stanchev, Jayashri Aragam, Emelia J Benjamin, Scott D Solomon, and Ramachandran S Vasan. 2013. “Reproducibility of Speckle-Tracking-Based Strain Measures of Left Ventricular Function in a Community-Based Study.” Journal of the American Society of Echocardiography : Official Publication of the American Society of Echocardiography 26 (11): 1258-1266.e2.
Cheung, Yin Ting, Tara M Brinkman, Chenghong Li, Yasmin Mzayek, Deokumar Srivastava, Kirsten K Ness, Sunita K Patel, et al. 2018. “Chronic Health Conditions and Neurocognitive Function in Aging Survivors of Childhood Cancer: A Report from the Childhood Cancer Survivor Study.” Journal of the National Cancer Institute 110 (4): 411–19.
Cheung, Yiu-fai, Wei Yu, Daniel Ka-leung Cheuk, Frankie Wai-tsoi Cheng, Janet Yee-kwan Yang, Jeffrey Ping-wa Yau, Karin Ka-huen Ho, et al. 2013. “Plasma High Sensitivity Troponin T Levels in Adult Survivors of Childhood Leukaemias: Determinants and Associations with Cardiac Function.” PLOS ONE 8 (10): e77063.
Childhood Cancer Survivor Study. 2017. “Demographic and Cancer Treatment of Participants in the Expansion, Original and Overall Cohorts.” https://ccss.stjude.org/content/dam/en_US/shared/ccss/documents/data/treatment-exposure-tables.pdf.
Children’s Oncology Group. 2013. “Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent and Young Adult Cancers, Version 4.0. Monrovia, CA: Children’s Oncology Group; October 2013.” www.survivorshipguidelines.org.
———. 2018. “Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent and Young Adult Cancers, Version 5.0. Monrovia, CA: Children’s Oncology Group; October 2018.” www.survivorshipguidelines.org.
Choi, Hyoung Soo, Eun Sil Park, Hyoung Jin Kang, Hee Young Shin, Chung Il Noh, Yong Soo Yun, Hyo Seop Ahn, and Jung Yun Choi. 2010. “Dexrazoxane for Preventing Anthracycline Cardiotoxicity in Children with Solid Tumors.” Journal of Korean Medical Science 25 (9): 1336–42.
122
Christiansen, Jon R, Richard Massey, Håvard Dalen, Adriani Kanellopoulos, Hanne Hamre, Sophie D Fosså, Ellen Ruud, Cecilie E Kiserud, and Svend Aakhus. 2016. “Utility of Global Longitudinal Strain by Echocardiography to Detect Left Ventricular Dysfunction in Long-Term Adult Survivors of Childhood Lymphoma and Acute Lymphoblastic Leukemia.” American Journal of Cardiology 118 (3): 446–52.
Cikes, Maja, and Scott D Solomon. 2015. “Beyond Ejection Fraction: An Integrative Approach for Assessment of Cardiac Structure and Function in Heart Failure.” European Heart Journal 37 (21): 1642–50.
Clerico, Aldo, Fabio A Recchia, Claudio Passino, and Michele Emdin. 2006. “Cardiac Endocrine Function Is an Essential Component of the Homeostatic Regulation Network: Physiological and Clinical Implications.” American Journal of Physiology. Heart and Circulatory Physiology 290 (1): H17-29.
Cohn, J N, R Ferrari, and N Sharpe. 2000. “Cardiac Remodeling--Concepts and Clinical Implications: A Consensus Paper from an International Forum on Cardiac Remodeling. Behalf of an International Forum on Cardiac Remodeling.” Journal of the American College of Cardiology 35 (3): 569–82.
Crone, Steven A, You-Yang Zhao, Lian Fan, Yusu Gu, Susumu Minamisawa, Yang Liu, Kirk L Peterson, et al. 2002. “ErbB2 Is Essential in the Prevention of Dilated Cardiomyopathy.” Nature Medicine 8 (5): 459–65.
Dallaire, Frederic, Cameron Slorach, Timothy Bradley, Wei Hui, Taisto Sarkola, Mark K Friedberg, Edgar Jaeggi, et al. 2016. “Pediatric Reference Values and Z Score Equations for Left Ventricular Systolic Strain Measured by Two-Dimensional Speckle-Tracking Echocardiography.” Journal of the American Society of Echocardiography : Official Publication of the American Society of Echocardiography 29 (8): 786-793.e8.
Dallaire, Frederic, Cameron Slorach, Wei Hui, Taisto Sarkola, Mark K Friedberg, Timothy J Bradley, Edgar Jaeggi, et al. 2015. “Reference Values for Pulse Wave Doppler and Tissue Doppler Imaging in Pediatric Echocardiography.” Circulation. Cardiovascular Imaging 8 (2): e002167.
Demers, Mélanie, Daniela S Krause, Daphne Schatzberg, Kimberly Martinod, Jaymie R Voorhees, Tobias A Fuchs, David T Scadden, and Denisa D Wagner. 2012. “Cancers Predispose Neutrophils to Release Extracellular DNA Traps That Contribute to Cancer-Associated Thrombosis.” Proceedings of the National Academy of Sciences of the United States of America 109 (32): 13076–81.
Ehrhardt, Matthew J, Joy M Fulbright, and Saro H Armenian. 2016. “Cardiomyopathy in Childhood Cancer Survivors: Lessons from the Past and Challenges for the Future.” Current Oncology Reports 18 (4): 22.
Ekstein, Sivan, Amiram Nir, Azaria J J T Rein, Zeev Perles, Benjamin Bar-Oz, Lea Salpeter, Nurit Algur, and Michael Weintraub. 2007. “N-Terminal-ProB-Type Natriuretic Peptide as a Marker for Acute Anthracycline Cardiotoxicity in Children.” Journal of Pediatric Hematology/Oncology 29 (7): 440–44.
El-Sherbeny, Wafaa S, Nesreen M Sabry, and Radwa M Sharbay. 2019. “Prediction of
123
Trastuzumab-Induced Cardiotoxicity in Breast Cancer Patients Receiving Anthracycline-Based Chemotherapy.” Journal of Echocardiography 17 (2): 76–83.
Ellison, Lawrence, and Teresa Janz. 2015. “Childhood Cancer Incidence and Mortality in Canada.” Statistics Canada; Catalogue no. 82-624-X; Health at a Glance.
Ewer, M S, M K Ali, B Mackay, S Wallace, M Valdivieso, S S Legha, R S Benjamin, and T P Haynie. 1984. “A Comparison of Cardiac Biopsy Grades and Ejection Fraction Estimations in Patients Receiving Adriamycin.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 2 (2): 112–17.
Fahmey, Sameh S, Mahmoud Hodeib, Khaled Refaat, and Walaa Mohammed. 2019. “Evaluation of Myocardial Function in Neonatal Sepsis Using Tissue Doppler Imaging.” The Journal of Maternal-Fetal & Neonatal Medicine : The Official Journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians, March, 1–5.
Felker, G M, R E Thompson, J M Hare, R H Hruban, D E Clemetson, D L Howard, K L Baughman, and E K Kasper. 2000. “Underlying Causes and Long-Term Survival in Patients with Initially Unexplained Cardiomyopathy.” The New England Journal of Medicine 342 (15): 1077–84.
Finck, Brian N, and Daniel P Kelly. 2007. “Peroxisome Proliferator-Activated Receptor Gamma Coactivator-1 (PGC-1) Regulatory Cascade in Cardiac Physiology and Disease.” Circulation 115 (19): 2540–48.
Franco, Vivian I, and Steven E Lipshultz. 2015. “Cardiac Complications in Childhood Cancer Survivors Treated with Anthracyclines.” Cardiology in the Young 25 Suppl 2 (August): 107–16.
Gan, Hoong-Wei, and Helen A Spoudeas. 2014. “Long-Term Follow-up of Survivors of Childhood Cancer (SIGN Clinical Guideline 132).” Archives of Disease in Childhood. Education and Practice Edition 99 (4): 138–43.
Giza, Dana Elena, Gloria Iliescu, Saamir Hassan, Konstantinos Marmagkiolis, and Cezar Iliescu. 2017. “Cancer as a Risk Factor for Cardiovascular Disease.” Current Oncology Reports 19 (6): 39.
Grabow, Desiree, Melanie Kaiser, Lars Hjorth, Julianne Byrne, Daniela Alessi, Rodrigue S Allodji, Francesca Bagnasco, et al. 2018. “The PanCareSurFup Cohort of 83,333 Five-Year Survivors of Childhood Cancer: A Cohort from 12 European Countries.” European Journal of Epidemiology 33 (3): 335–49.
Gripp, Eliza de Almeida, Gabriela Escudini de Oliveira, Luiz Augusto Feijo, Marcelo Iorio Garcia, Sergio Salles Xavier, and Andrea Silvestre de Sousa. 2018. “Global Longitudinal Strain Accuracy for Cardiotoxicity Prediction in a Cohort of Breast Cancer Patients During Anthracycline and/or Trastuzumab Treatment.” Arquivos Brasileiros de Cardiologia 110 (2): 140–50.
Gulati, Geeta, Siri Lagethon Heck, Anne Hansen Ree, Pavel Hoffmann, Jeanette Schulz-Menger, Morten W Fagerland, Berit Gravdehaug, et al. 2016. “Prevention of Cardiac Dysfunction
124
during Adjuvant Breast Cancer Therapy (PRADA): A 2 x 2 Factorial, Randomized, Placebo-Controlled, Double-Blind Clinical Trial of Candesartan and Metoprolol.” European Heart Journal 37 (21): 1671–80.
Hatazawa, Keiko, Hidekazu Tanaka, Akiko Nonaka, Hiroki Takada, Fumitaka Soga, Yutaka Hatani, Hiroki Matsuzoe, et al. 2018. “Baseline Global Longitudinal Strain as a Predictor of Left Ventricular Dysfunction and Hospitalization for Heart Failure of Patients With Malignant Lymphoma After Anthracycline Therapy.” Circulation Journal : Official Journal of the Japanese Circulation Society 82 (10): 2566–74.
Henriksen, Peter A. 2018. “Anthracycline Cardiotoxicity: An Update on Mechanisms, Monitoring and Prevention.” Heart (British Cardiac Society) 104 (12): 971–77.
Hequet, O, Q H Le, I Moullet, E Pauli, G Salles, D Espinouse, C Dumontet, et al. 2004. “Subclinical Late Cardiomyopathy after Doxorubicin Therapy for Lymphoma in Adults.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 22 (10): 1864–71.
Hoff, D D Von, M W Layard, P Basa, H L Jr Davis, A L Von Hoff, M Rozencweig, and F M Muggia. 1979. “Risk Factors for Doxorubicin-Induced Congestive Heart Failure.” Annals of Internal Medicine 91 (5): 710–17.
Holmstrom, H, C Hall, and E Thaulow. 2001. “Plasma Levels of Natriuretic Peptides and Hemodynamic Assessment of Patent Ductus Arteriosus in Preterm Infants.” Acta Paediatrica (Oslo, Norway : 1992) 90 (2): 184–91.
Horacek, J M, M Tichy, R Pudil, and L Jebavy. 2008. “Glycogen Phosphorylase BB Could Be a New Circulating Biomarker for Detection of Anthracycline Cardiotoxicity.” Annals of Oncology : Official Journal of the European Society for Medical Oncology. England.
Horwich, Tamara B, Gregg C Fonarow, Michele A Hamilton, W Robb MacLellan, and Jeff Borenstein. 2002. “Anemia Is Associated with Worse Symptoms, Greater Impairment in Functional Capacity and a Significant Increase in Mortality in Patients with Advanced Heart Failure.” Journal of the American College of Cardiology 39 (11): 1780–86.
Hudson, Melissa M, Kirsten K Ness, James G Gurney, Daniel A Mulrooney, Wassim Chemaitilly, Kevin R Krull, Daniel M Green, et al. 2013. “Clinical Ascertainment of Health Outcomes among Adults Treated for Childhood Cancer.” JAMA 309 (22): 2371–81.
Hudson, Melissa M, Shesh N Rai, Cesar Nunez, Thomas E Merchant, Neyssa M Marina, Nia Zalamea, Cheryl Cox, Sean Phipps, Ronald Pompeu, and David Rosenthal. 2007. “Noninvasive Evaluation of Late Anthracycline Cardiac Toxicity in Childhood Cancer Survivors.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 25 (24): 3635–43.
Jashari, Haki, Annika Rydberg, Pranvera Ibrahimi, Gani Bajraktari, Lindita Kryeziu, Fisnik Jashari, and Michael Y Henein. 2015. “Normal Ranges of Left Ventricular Strain in Children: A Meta-Analysis.” Cardiovascular Ultrasound 13 (1): 37.
Kadan-Lottick, Nina S, Lonnie K Zeltzer, Qi Liu, Yutaka Yasui, Leah Ellenberg, Gerard Gioia, Leslie L Robison, and Kevin R Krull. 2010. “Neurocognitive Functioning in Adult
125
Survivors of Childhood Non-Central Nervous System Cancers.” Journal of the National Cancer Institute 102 (12): 881–93.
Kalam, Kashif, Petr Otahal, and Thomas H Marwick. 2014. “Prognostic Implications of Global LV Dysfunction: A Systematic Review and Meta-Analysis of Global Longitudinal Strain and Ejection Fraction.” Heart (British Cardiac Society) 100 (21): 1673–80.
Kalay, Nihat, Emrullah Basar, Ibrahim Ozdogru, Ozlem Er, Yakup Cetinkaya, Ali Dogan, Tugrul Inanc, et al. 2006. “Protective Effects of Carvedilol against Anthracycline-Induced Cardiomyopathy.” Journal of the American College of Cardiology 48 (11): 2258–62.
Kang, Min Jae, and Jung Sub Lim. 2013. “Bone Mineral Density Deficits in Childhood Cancer Survivors: Pathophysiology, Prevalence, Screening, and Management.” Korean Journal of Pediatrics 56 (2): 60–67. https://doi.org/10.3345/kjp.2013.56.2.60.
Kang, Yu, Leilei Cheng, Lin Li, Haiyan Chen, Minmin Sun, Zheng Wei, Cuizhen Pan, and Xianhong Shu. 2013. “Early Detection of Anthracycline-Induced Cardiotoxicity Using Two-Dimensional Speckle Tracking Echocardiography.” Cardiology Journal 20 (6): 592–99.
Kaya, Mehmet G, Metin Ozkan, Ozgur Gunebakmaz, Hasan Akkaya, Esma G Kaya, Mahmut Akpek, Nihat Kalay, et al. 2013. “Protective Effects of Nebivolol against Anthracycline-Induced Cardiomyopathy: A Randomized Control Study.” International Journal of Cardiology 167 (5): 2306–10.
Kenborg, Line, Karen M Linnet, Sofie de Fine Licht, Andrea Bautz, Anna S Holmqvist, Laufey Tryggvadottir, Laura M Madanat-Harjuoja, et al. 2019. “Hospital Admission for Neurologic Disorders among 5-Year Survivors of Noncentral Nervous System Tumors in Childhood: A Cohort Study within the Adult Life after Childhood Cancer in Scandinavia Study.” International Journal of Cancer, April.
Khouri, Michel, Pamela Douglas, John Mackey, Martin Miguel, Scott Jessica M., Scherrer-Crosbie Marielle, and Jones Lee W. 2012. “Cancer Therapy–Induced Cardiac Toxicity in Early Breast Cancer.” Circulation 126 (23): 2749–63.
Kim, Hack-Lyoung, Myung-A Kim, Dong-Ju Choi, Seongwoo Han, Eun-Seok Jeon, Myeong-Chan Cho, Jae-Joong Kim, et al. 2017. “Gender Difference in the Prognostic Value of N-Terminal Pro-B Type Natriuretic Peptide in Patients With Heart Failure- A Report From the Korean Heart Failure Registry (KorHF).” Circulation Journal : Official Journal of the Japanese Circulation Society 81 (9): 1329–36.
Kirchhoff, Anne C, Mark N Fluchel, Jennifer Wright, Jian Ying, Carol Sweeney, Julia Bodson, Antoinette M Stroup, Ken R Smith, Alison Fraser, and Anita Y Kinney. 2014. “Risk of Hospitalization for Survivors of Childhood and Adolescent Cancer.” Cancer Epidemiology, Biomarkers & Prevention : A Publication of the American Association for Cancer Research, Cosponsored by the American Society of Preventive Oncology 23 (7): 1280–89.
Koch, A, and H Singer. 2003. “Normal Values of B Type Natriuretic Peptide in Infants, Children, and Adolescents.” Heart (British Cardiac Society) 89 (8): 875–78.
Kooijmans, Esmee Cm, Arend Bokenkamp, Nic S Tjahjadi, Jesse M Tettero, Eline van Dulmen-
126
den Broeder, Helena Jh van der Pal, and Margreet A Veening. 2019. “Early and Late Adverse Renal Effects after Potentially Nephrotoxic Treatment for Childhood Cancer.” The Cochrane Database of Systematic Reviews 3 (March): CD008944.
Koopman, Laurens P, Cameron Slorach, Cedric Manlhiot, Brian W McCrindle, Edgar T Jaeggi, Luc Mertens, and Mark K Friedberg. 2011. “Assessment of Myocardial Deformation in Children Using Digital Imaging and Communications in Medicine (DICOM) Data and Vendor Independent Speckle Tracking Software.” Journal of the American Society of Echocardiography 24 (1): 37–44.
Kremer, L C M, H J H van der Pal, M Offringa, E C van Dalen, and P A Voute. 2002. “Frequency and Risk Factors of Subclinical Cardiotoxicity after Anthracycline Therapy in Children: A Systematic Review.” Annals of Oncology : Official Journal of the European Society for Medical Oncology 13 (6): 819–29.
Krischer, J P, S Epstein, D D Cuthbertson, A M Goorin, M L Epstein, and S E Lipshultz. 1997. “Clinical Cardiotoxicity Following Anthracycline Treatment for Childhood Cancer: The Pediatric Oncology Group Experience.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 15 (4): 1544–52.
Kuehni, Claudia E, Corina S Rueegg, Gisela Michel, Cornelia E Rebholz, Marie-Pierre F Strippoli, Felix K Niggli, Matthias Egger, Nicolas X von der Weid, and for the Swiss Paediatric Oncology Group (SPOG). 2011. “Cohort Profile: The Swiss Childhood Cancer Survivor Study.” International Journal of Epidemiology 41 (6): 1553–64.
Kwok, J C, and D R Richardson. 2000. “The Cardioprotective Effect of the Iron Chelator Dexrazoxane (ICRF-187) on Anthracycline-Mediated Cardiotoxicity.” Redox Report : Communications in Free Radical Research 5 (6): 317–24.
Ky, Bonnie, Mary Putt, Heloisa Sawaya, Benjamin French, James L Jr Januzzi, Igal A Sebag, Juan Carlos Plana, et al. 2014. “Early Increases in Multiple Biomarkers Predict Subsequent Cardiotoxicity in Patients with Breast Cancer Treated with Doxorubicin, Taxanes, and Trastuzumab.” Journal of the American College of Cardiology 63 (8): 809–16.
L., Chow Sheryl, Maisel Alan S., Anand Inder, Bozkurt Biykem, de Boer Rudolf A., Felker G Michael, Fonarow Gregg C., et al. 2017. “Role of Biomarkers for the Prevention, Assessment, and Management of Heart Failure: A Scientific Statement From the American Heart Association.” Circulation 135 (22): e1054–91.
Landy, David C, Tracie L Miller, Gabriela Lopez-Mitnik, Stuart R Lipsitz, Andrea S Hinkle, Louis S Constine, Carol A French, Amy M K Rovitelli, M Jacob Adams, and Steven E Lipshultz. 2012. “Aggregating Traditional Cardiovascular Disease Risk Factors to Assess the Cardiometabolic Health of Childhood Cancer Survivors: An Analysis from the Cardiac Risk Factors in Childhood Cancer Survivors Study.” American Heart Journal 163 (2): 295-301.e2.
Laufer-Perl, Michal, Matthew Derakhshesh, Assi Milwidsky, Liat Mor, Dor Ravid, Nadav Amrami, Jack Sherez, Gad Keren, Yan Topilsky, and Yaron Arbel. 2018. “Usefulness of Global Longitudinal Strain for Early Identification of Subclinical Left Ventricular Dysfunction in Patients With Active Cancer.” The American Journal of Cardiology 122
127
(10): 1784–89.
Leger, Kasey, Tamra Slone, Matthew Lemler, David Leonard, Cindy Cochran, W Paul Bowman, Lisa Bashore, and Naomi Winick. 2015. “Subclinical Cardiotoxicity in Childhood Cancer Survivors Exposed to Very Low Dose Anthracycline Therapy.” Pediatric Blood & Cancer 62 (1): 123–27.
Legha, Sewa S, ROBERT S BENJAMIN, BRUCE MACKAY, MICHAEL EWER, SIDNEY WALLACE, MANUEL VALDIVIESO, SHELLEY L RASMUSSEN, GEORGE R BLUMENSCHEIN, and EMIL J FREIREICH. 1982. “Reduction of Doxorubicin Cardiotoxicity by Prolonged Continuous Intravenous Infusion.” Annals of Internal Medicine 96 (2): 133–39.
Leosdottir, Margret, Ronnie Willenheimer, Christian Hall, Solve Tjora, Johan Malm, Olle Melander, and Peter M Nilsson. 2011. “Age and Gender Differences in the Association between Nt-ProBNP and Glucometabolic Disturbances.” Scandinavian Cardiovascular Journal : SCJ 45 (5): 294–300.
Levy, Philip T, Aliza Machefsky, Aura A Sanchez, Meghna D Patel, Sarah Rogal, Susan Fowler, Lauren Yaeger, et al. 2016. “Reference Ranges of Left Ventricular Strain Measures by Two-Dimensional Speckle-Tracking Echocardiography in Children: A Systematic Review and Meta-Analysis.” Journal of the American Society of Echocardiography : Official Publication of the American Society of Echocardiography 29 (3): 209-225.e6.
Link, G, R Tirosh, A Pinson, and C Hershko. 1996. “Role of Iron in the Potentiation of Anthracycline Cardiotoxicity: Identification of Heart Cell Mitochondria as a Major Site of Iron-Anthracycline Interaction.” The Journal of Laboratory and Clinical Medicine 127 (3): 272–78.
Lipshultz. 1996. “Dexrazoxane for Protection against Cardiotoxic Effects of Anthracyclines in Children.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. United States.
Lipshultz, Jorge A Alvarez, and Rebecca E Scully. 2008. “Anthracycline Associated Cardiotoxicity in Survivors of Childhood Cancer.” Heart (British Cardiac Society) 94 (4): 525–33.
Lipshultz, S D Colan, R D Gelber, A R Perez-Atayde, S E Sallan, and S P Sanders. 1991. “Late Cardiac Effects of Doxorubicin Therapy for Acute Lymphoblastic Leukemia in Childhood.” The New England Journal of Medicine 324 (12): 808–15.
Lipshultz, Vivian I Franco, Tracie L Miller, Steven D Colan, and Stephen E Sallan. 2015. “Cardiovascular Disease in Adult Survivors of Childhood Cancer.” Annual Review of Medicine 66: 161–76.
Lipshultz, Adams M Jacob, Colan Steven D., Constine Louis S., Herman Eugene H., Hsu Daphne T., Hudson Melissa M., et al. 2013. “Long-Term Cardiovascular Toxicity in Children, Adolescents, and Young Adults Who Receive Cancer Therapy: Pathophysiology, Course, Monitoring, Management, Prevention, and Research Directions.” Circulation 128 (17): 1927–95.
128
Lipshultz, S R Lipsitz, S M Mone, A M Goorin, S E Sallan, S P Sanders, E J Orav, R D Gelber, and S D Colan. 1995. “Female Sex and Higher Drug Dose as Risk Factors for Late Cardiotoxic Effects of Doxorubicin Therapy for Childhood Cancer.” The New England Journal of Medicine 332 (26): 1738–43.
Lipshultz, Stuart R Lipsitz, Jeffery L Kutok, Tracie L Miller, Steven D Colan, Donna S Neuberg, Kristen E Stevenson, et al. 2013. “Impact of Hemochromatosis Gene Mutations on Cardiac Status in Doxorubicin-Treated Survivors of Childhood High-Risk Leukemia.” Cancer 119 (19): 3555–62.
Lipshultz, N Rifai, S E Sallan, S R Lipsitz, V Dalton, D B Sacks, and M E Ottlinger. 1997. “Predictive Value of Cardiac Troponin T in Pediatric Patients at Risk for Myocardial Injury.” Circulation 96 (8): 2641–48.
Lipshultz, Rebecca E Scully, Stuart R Lipsitz, Stephen E Sallan, Lewis B Silverman, Tracie L Miller, Elly V Barry, et al. 2010. “Assessment of Dexrazoxane as a Cardioprotectant in Doxorubicin-Treated Children with High-Risk Acute Lymphoblastic Leukaemia: Long-Term Follow-up of a Prospective, Randomised, Multicentre Trial.” The Lancet. Oncology 11 (10): 950–61.
Lipshultz, Steven E, Stuart R Lipsitz, Stephen E Sallan, Virginia M Dalton, Suzanne M Mone, Richard D Gelber, and Steven D Colan. 2005. “Chronic Progressive Cardiac Dysfunction Years after Doxorubicin Therapy for Childhood Acute Lymphoblastic Leukemia.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 23 (12): 2629–36.
Lipshultz, Steven E, Tracie L Miller, Stuart R Lipsitz, Donna S Neuberg, Suzanne E Dahlberg, Steven D Colan, Lewis B Silverman, et al. 2012. “Continuous Versus Bolus Infusion of Doxorubicin in Children With ALL: Long-Term Cardiac Outcomes.” Pediatrics 130 (6): 1003–11.
Lipshultz, Steven E, Tracie L Miller, Rebecca E Scully, Stuart R Lipsitz, Nader Rifai, Lewis B Silverman, Steven D Colan, et al. 2012. “Changes in Cardiac Biomarkers during Doxorubicin Treatment of Pediatric Patients with High-Risk Acute Lymphoblastic Leukemia: Associations with Long-Term Echocardiographic Outcomes.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 30 (10): 1042–49.
Lipshultz, Steven E, Nader Rifai, Virginia M Dalton, Donna E Levy, Lewis B Silverman, Stuart R Lipsitz, Steven D Colan, et al. 2004. “The Effect of Dexrazoxane on Myocardial Injury in Doxorubicin-Treated Children with Acute Lymphoblastic Leukemia.” New England Journal of Medicine 351 (2): 145–53.
Loar, Robert W, Cory V Noel, Hari Tunuguntla, John L Colquitt, and Ricardo H Pignatelli. 2018. “State of the Art Review: Chemotherapy-Induced Cardiotoxicity in Children.” Congenital Heart Disease 13 (1): 5–15.
Loonen, Jacqueline, Milanthy Pourier, Peter M Hoogerbrugge, Annelies M C Mavinkurve-Groothuis, Karen A Marcus, Livia Kapusta, Ton Feuth, and Chris L de Korte. 2012. “Myocardial 2D Strain Echocardiography and Cardiac Biomarkers in Children during and
129
Shortly after Anthracycline Therapy for Acute Lymphoblastic Leukaemia (ALL): A Prospective Study.” European Heart Journal - Cardiovascular Imaging 14 (6): 562–69.
Lopez, Leo, Steven D Colan, Peter C Frommelt, Gregory J Ensing, Kathleen Kendall, Adel K Younoszai, Wyman W Lai, and Tal Geva. 2010. “Recommendations for Quantification Methods during the Performance of a Pediatric Echocardiogram: A Report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council.” Journal of the American Society of Echocardiography : Official Publication of the American Society of Echocardiography 23 (5): 465–67.
Lyu, Yi Lisa, John E Kerrigan, Chao-Po Lin, Anna M Azarova, Yuan-Chin Tsai, Yi Ban, and Leroy F Liu. 2007. “Topoisomerase IIβ–Mediated DNA Double-Strand Breaks: Implications in Doxorubicin Cardiotoxicity and Prevention by Dexrazoxane.” Cancer Research 67 (18): 8839 LP – 8846.
Marshall, W A, and J M Tanner. 1969. “Variations in Pattern of Pubertal Changes in Girls.” Archives of Disease in Childhood 44 (235): 291–303.
———. 1970. “Variations in the Pattern of Pubertal Changes in Boys.” Archives of Disease in Childhood 45 (239): 13–23.
Mavinkurve-Groothuis, Annelies M C, Jacqueline Groot-Loonen, Karen A Marcus, Louise Bellersen, Ton Feuth, Jos P M Bokkerink, Peter M Hoogerbrugge, Chris de Korte, and Livia Kapusta. 2010. “Myocardial Strain and Strain Rate in Monitoring Subclinical Heart Failure in Asymptomatic Long-Term Survivors of Childhood Cancer.” Ultrasound in Medicine & Biology 36 (11): 1783–91.
Mavinkurve-Groothuis, Annelies M C, Karen A Marcus, Milanthy Pourier, Jacqueline Loonen, Ton Feuth, Peter M Hoogerbrugge, Chris L de Korte, and Livia Kapusta. 2013. “Myocardial 2D Strain Echocardiography and Cardiac Biomarkers in Children during and Shortly after Anthracycline Therapy for Acute Lymphoblastic Leukaemia (ALL): A Prospective Study.” European Heart Journal Cardiovascular Imaging 14 (6): 562–69.
McBride, Mary L, Paul C Rogers, Sam B Sheps, Victor Glickman, Anne-Marie Broemeling, Karen Goddard, Joan Hu, et al. 2010. “Childhood, Adolescent, and Young Adult Cancer Survivors Research Program of British Columbia: Objectives, Study Design, and Cohort Characteristics.” Pediatric Blood & Cancer 55 (2): 324–30.
McGowan, John V, Robin Chung, Angshuman Maulik, Izabela Piotrowska, J Malcolm Walker, and Derek M Yellon. 2017. “Anthracycline Chemotherapy and Cardiotoxicity.” Cardiovascular Drugs and Therapy 31 (1): 63–75.
Mertens, Ann C, Qi Liu, Joseph P Neglia, Karen Wasilewski, Wendy Leisenring, Gregory T Armstrong, Leslie L Robison, and Yutaka Yasui. 2008. “Cause-Specific Late Mortality among 5-Year Survivors of Childhood Cancer: The Childhood Cancer Survivor Study.” Journal of the National Cancer Institute 100 (19): 1368–79.
Mertens, Y Yasui, J P Neglia, J D Potter, M E Jr Nesbit, K Ruccione, W A Smithson, and L L Robison. 2001. “Late Mortality Experience in Five-Year Survivors of Childhood and Adolescent Cancer: The Childhood Cancer Survivor Study.” Journal of Clinical Oncology :
130
Official Journal of the American Society of Clinical Oncology 19 (13): 3163–72.
Michel, Lars, Tienush Rassaf, and Matthias Totzeck. 2018. “Biomarkers for the Detection of Apparent and Subclinical Cancer Therapy-Related Cardiotoxicity.” Journal of Thoracic Disease 10 (Suppl 35): S4282–95.
Mir, Thomas S, Reinhard Laux, Hans Henning Hellwege, Bozena Liedke, Cornelius Heinze, Helmut von Buelow, Stephanie Laer, and Jochen Weil. 2003. “Plasma Concentrations of Aminoterminal pro Atrial Natriuretic Peptide and Aminoterminal pro Brain Natriuretic Peptide in Healthy Neonates: Marked and Rapid Increase after Birth.” Pediatrics 112 (4): 896–99.
Missov, E, C Calzolari, J M Davy, F Leclercq, M Rossi, and B Pau. 1997. “Cardiac Troponin I in Patients with Hematologic Malignancies.” Coronary Artery Disease 8 (8–9): 537–41.
Moke, Diana J, Lynn E Schubert, Heather Y Sun, Beth F Printz, and Andrew C Dietz. 2018. “Utility of Echocardiography as Screening for Late-Onset Anthracycline-Induced Cardiotoxicity in Pediatric Cancer Survivors: Observations from the First Decade After End of Therapy.” Journal of Pediatric Hematology/Oncology 40 (5): e283–88.
Mordente, Alvaro, Elisabetta Meucci, Giuseppe Ettore Martorana, Daniela Tavian, and Andrea Silvestrini. 2017. “Topoisomerases and Anthracyclines: Recent Advances and Perspectives in Anticancer Therapy and Prevention of Cardiotoxicity.” Current Medicinal Chemistry 24 (15): 1607–26.
Mornos, Cristian, Athanasios J Manolis, Drago Cozma, Nikos Kouremenos, Ioanna Zacharopoulou, and Adina Ionac. 2014. “The Value of Left Ventricular Global Longitudinal Strain Assessed by Three-Dimensional Strain Imaging in the Early Detection of Anthracyclinemediated Cardiotoxicity.” Hellenic Journal of Cardiology : HJC = Hellenike Kardiologike Epitheorese 55 (3): 235–44.
Mousavi, Negareh, Timothy C Tan, Mohammed Ali, Elkan F Halpern, Lin Wang, and Marielle Scherrer-Crosbie. 2015. “Echocardiographic Parameters of Left Ventricular Size and Function as Predictors of Symptomatic Heart Failure in Patients with a Left Ventricular Ejection Fraction of 50-59% Treated with Anthracyclines.” European Heart Journal Cardiovascular Imaging 16 (9): 977–84. https://doi.org/10.1093/ehjci/jev113.
Mulla, Z D. 2007. “Spline Regression in Clinical Research.” The West Indian Medical Journal 56 (1): 77–79.
Mulrooney, DA, GT Armstrong, S Huang, and et al. 2016. “Cardiac Outcomes in Adult Survivors of Childhood Cancer Exposed to Cardiotoxic Therapy: A Cross-Sectional Study.” Annals of Internal Medicine 164 (2): 93–101.
Mulrooney, Mark W Yeazel, Toana Kawashima, Ann C Mertens, Pauline Mitby, Marilyn Stovall, Sarah S Donaldson, et al. 2009. “Cardiac Outcomes in a Cohort of Adult Survivors of Childhood and Adolescent Cancer: Retrospective Analysis of the Childhood Cancer Survivor Study Cohort.” BMJ 339.
Nagarajan, R, S R Rose, M M Rutter, J Correll, D Kent, M Kim, B Schnell, and K C Burns. 2010. “Osteopenia in Survivors of Childhood Cancer.” Journal of Clinical Oncology 28
131
(15_suppl): 9089.
Narayan, Hari K, Benjamin French, Abigail M Khan, Theodore Plappert, David Hyman, Akinyemi Bajulaiye, Susan Domchek, et al. 2016. “Noninvasive Measures of Ventricular-Arterial Coupling and Circumferential Strain Predict Cancer Therapeutics-Related Cardiac Dysfunction.” JACC. Cardiovascular Imaging 9 (10): 1131–41.
Narayan, Hari K, Wei Wei, Ziding Feng, Daniel Lenihan, Ted Plappert, Virginia Englefield, Michael Fisch, and Bonnie Ky. 2017. “Cardiac Mechanics and Dysfunction with Anthracyclines in the Community: Results from the PREDICT Study.” Open Heart 4 (1).
Nathan, Paul C, Eitan Amir, and Husam Abdel-Qadir. 2016. “Cardiac Outcomes in Survivors of Pediatric and Adult Cancers.” The Canadian Journal of Cardiology 32 (7): 871–80.
National Cancer Institute. 2001. “SEER Cancer Statistics Review 1973-1997 (NCI 2000).” Journal of the National Cancer Institute 93 (5): 341. http://jnci.oxfordjournals.org/content/93/5/341.full.
Nebigil, Canan G, and Laurent Désaubry. 2018. “Updates in Anthracycline-Mediated Cardiotoxicity.” Frontiers in Pharmacology 9: 1262.
Negishi, Kazuaki, Tomoko Negishi, James L Hare, Brian A Haluska, Juan Carlos Plana, and Thomas H Marwick. 2013. “Independent and Incremental Value of Deformation Indices for Prediction of Trastuzumab-Induced Cardiotoxicity.” Journal of the American Society of Echocardiography 26 (5): 493–98.
Nir, A, B Bar-Oz, Z Perles, R Brooks, A Korach, and A J J T Rein. 2004. “N-Terminal pro-B-Type Natriuretic Peptide: Reference Plasma Levels from Birth to Adolescence. Elevated Levels at Birth and in Infants and Children with Heart Diseases.” Acta Paediatrica (Oslo, Norway : 1992) 93 (5): 603–7.
Nir, Amiram, Angelika Lindinger, Manfred Rauh, Benjamin Bar-Oz, Stephanie Laer, Lynn Schwachtgen, Andreas Koch, Jan Falkenberg, and Thomas S Mir. 2009. “NT-pro-B-Type Natriuretic Peptide in Infants and Children: Reference Values Based on Combined Data from Four Studies.” Pediatric Cardiology 30 (1): 3–8.
Noone, AM, N Howlader, M Krapcho, D Miller, A Brest, M Yu, J Ruhl, et al. 2018. “SEER Cancer Statistics Review, 1975-2015, National Cancer Institute. Bethesda, MD.” Bethesda, MD. https://seer.cancer.gov/csr/1975_2015/, based on November 2017 SEER data submission, posted to the SEER web site, April 2018.
Oeffinger, KC, AC Mertens, CA Sklar, T Kawashima, MM Hudson, AT Meadows, DL Friedman, et al. 2006. “Chronic Health Conditions in Adult Survivors of Childhood Cancer.” New England Journal of Medicine 355 (15): 1572–82.
Onitilo, Adedayo A, Jessica M Engel, Rachel V Stankowski, Hong Liang, Richard L Berg, and Suhail A R Doi. 2012. “High-Sensitivity C-Reactive Protein (Hs-CRP) as a Biomarker for Trastuzumab-Induced Cardiotoxicity in HER2-Positive Early-Stage Breast Cancer: A Pilot Study.” Breast Cancer Research and Treatment 134 (1): 291–98.
Pal, Helena J van der, Elvira C van Dalen, Evelien van Delden, Irma W van Dijk, Wouter E Kok,
132
Ronald B Geskus, Elske Sieswerda, et al. 2012. “High Risk of Symptomatic Cardiac Events in Childhood Cancer Survivors.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 30 (13): 1429–37.
Pal, Helena J van der, Elvira C van Dalen, Michael Hauptmann, Wouter E Kok, Huib N Caron, Cor van den Bos, Foppe Oldenburger, Caro C Koning, Flora E van Leeuwen, and Leontien C Kremer. 2010a. “Cardiac Function in 5-Year Survivors of Childhood Cancer: A Long-Term Follow-up Study.” Archives of Internal Medicine 170 (14): 1247–55.
———. 2010b. “Cardiac Function in 5-Year Survivors of Childhood Cancer: A Long-Term Follow-up StudyCardiac Function in Childhood Cancer Survivors.” JAMA Internal Medicine 170 (14): 1247–55.
Pein, F, O Sakiroglu, M Dahan, J Lebidois, P Merlet, A Shamsaldin, E Villain, F de Vathaire, D Sidi, and O Hartmann. 2004. “Cardiac Abnormalities 15 Years and More after Adriamycin Therapy in 229 Childhood Survivors of a Solid Tumour at the Institut Gustave Roussy.” British Journal of Cancer 91 (1): 37–44.
Pignatelli, Ricardo H, Payam Ghazi, S Chandra-Bose Reddy, Patrick Thompson, Qiqiong Cui, Jacqueline Castro, Mehmet F Okcu, and John Lynn Jefferies. 2015. “Abnormal Myocardial Strain Indices in Children Receiving Anthracycline Chemotherapy.” Pediatric Cardiology 36 (8): 1610–16.
Plana, Juan Carlos, Maurizio Galderisi, Ana Barac, Michael S Ewer, Bonnie Ky, Marielle Scherrer-Crosbie, Javier Ganame, et al. 2014. “Expert Consensus for Multimodality Imaging Evaluation of Adult Patients during and after Cancer Therapy: A Report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging.” Journal of the American Society of Echocardiography : Official Publication of the American Society of Echocardiography 27 (9): 911–39.
Ponikowski, Piotr, Adriaan A Voors, Stefan D Anker, Hector Bueno, John G F Cleland, Andrew J S Coats, Volkmar Falk, et al. 2016. “2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC). Developed with the Special Contribution .” European Journal of Heart Failure 18 (8): 891–975.
Poterucha, Joseph T, Shelby Kutty, Rebecca K Lindquist, Ling Li, and Benjamin W Eidem. 2012. “Changes in Left Ventricular Longitudinal Strain with Anthracycline Chemotherapy in Adolescents Precede Subsequent Decreased Left Ventricular Ejection Fraction.” Journal of the American Society of Echocardiography : Official Publication of the American Society of Echocardiography 25 (7): 733–40.
Pourier, Milanthy S, Livia Kapusta, Aniek van Gennip, Jos P M Bokkerink, Jacqueline Loonen, Louise Bellersen, and Annelies M C Mavinkurve-Groothuis. 2015. “Values of High Sensitive Troponin T in Long-Term Survivors of Childhood Cancer Treated with Anthracyclines.” Clinica Chimica Acta; International Journal of Clinical Chemistry 441 (February): 29–32.
Rajic, Vladan, Richard Aplenc, Marusa Debeljak, Veronika Velensek Prestor, Natasa Karas-
133
Kuzelicki, Irena Mlinaric-Rascan, and Janez Jazbec. 2009. “Influence of the Polymorphism in Candidate Genes on Late Cardiac Damage in Patients Treated Due to Acute Leukemia in Childhood.” Leukemia & Lymphoma 50 (10): 1693–98.
Reinbolt, Raquel E, Roshan Patel, Xueliang Pan, Cynthia Dawn Timmers, Robert Pilarski, Charles L Shapiro, and Maryam B Lustberg. 2016. “Risk Factors for Anthracycline-Associated Cardiotoxicity.” Supportive Care in Cancer : Official Journal of the Multinational Association of Supportive Care in Cancer 24 (5): 2173–80.
Reulen, RC, DL Winter, C Frobisher, and Et Al. 2010. “Long-Term Cause-Specific Mortality among Survivors of Childhood Cancer.” JAMA 304 (2): 172–79.
Rhea, Isaac B, Sarada Uppuluri, Stephen Sawada, Bryan P Schneider, and Harvey Feigenbaum. 2015. “Incremental Prognostic Value of Echocardiographic Strain and Its Association With Mortality in Cancer Patients.” Journal of the American Society of Echocardiography 28 (6): 667–73. https://doi.org/10.1016/j.echo.2015.02.006.
Rigby, R, and D Stasinopoulos. 2005. “Generalized Additive Models for Location, Scale and Shape.” Journal of the Royal Statistical Society: Series C (Applied Statistics) 54 (3): 507–54. https://rss.onlinelibrary.wiley.com/doi/abs/10.1111/j.1467-9876.2005.00510.x.
Rigby, R, M Stasinopoulos, G Heller, and F De Bastiani. 2017. Distributions for Modelling Location, Scale and Shape: Using GAMLSS in R.
Robison, Leslie L, Gregory T Armstrong, John D Boice, Eric J Chow, Stella M Davies, Sarah S Donaldson, Daniel M Green, et al. 2009. “The Childhood Cancer Survivor Study: A National Cancer Institute-Supported Resource for Outcome and Intervention Research.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 27 (14): 2308–18.
Robison, Leslie L, Daniel M Green, Melissa Hudson, Anna T Meadows, Ann C Mertens, Roger J Packer, Charles A Sklar, Louise C Strong, Yutaka Yasui, and Lonnie K Zeltzer. 2005. “Long-Term Outcomes of Adult Survivors of Childhood Cancer.” Cancer 104 (S11): 2557–64.
Robison, Leslie L, and Melissa M Hudson. 2014. “Survivors of Childhood and Adolescent Cancer: Life-Long Risks and Responsibilities.” Nature Reviews. Cancer. England.
Robison, Leslie L, Ann C Mertens, John D Boice, Norman E Breslow, Sarah S Donaldson, Daniel M Green, Frederic P Li, et al. 2002. “Study Design and Cohort Characteristics of the Childhood Cancer Survivor Study: A Multi-Institutional Collaborative Project.” Medical and Pediatric Oncology 38 (4): 229–39.
Roche Diagnostics. 2019a. “Roche Elecsys® Troponin T-High Sensitive.” 2019. https://diagnostics.roche.com/global/en/products/params/elecsys-troponin-t-high-sensitive-tnt-hs.html.
———. 2019b. “Roche NT-ProBNP.” 2019. https://diagnostics.roche.com/global/en/products/params/elecsys-nt-probnp.html.
Rosa, Gian Marco, Lorenzo Gigli, Maria Isabella Tagliasacchi, Cecilia Di Iorio, Federico
134
Carbone, Alessio Nencioni, Fabrizio Montecucco, and Claudio Brunelli. 2016. “Update on Cardiotoxicity of Anti-Cancer Treatments.” European Journal of Clinical Investigation 46 (3): 264–84.
Sawaya, Heloisa, Igal A Sebag, Juan Carlos Plana, James L Januzzi, Bonnie Ky, Victor Cohen, Sucheta Gosavi, et al. 2011. “Early Detection and Prediction of Cardiotoxicity in Chemotherapy-Treated Patients.” The American Journal of Cardiology 107 (9): 1375–80.
Sawaya, Heloisa, Igal A Sebag, Juan Carlos Plana, James L Januzzi, Bonnie Ky, Timothy C Tan, Victor Cohen, et al. 2012. “Assessment of Echocardiography and Biomarkers for the Extended Prediction of Cardiotoxicity in Patients Treated with Anthracyclines, Taxanes, and Trastuzumab.” Circulation. Cardiovascular Imaging 5 (5): 596–603.
Schnabl, Kareena, Man Khun Chan, Yanping Gong, and Khosrow Adeli. 2008. “Closing the Gaps in Paediatric Reference Intervals: The CALIPER Initiative.” The Clinical Biochemist. Reviews 29 (3): 89–96.
Scholz-Kreisel, Peter, Claudia Spix, Maria Blettner, Susan Eckerle, Jorg Faber, Philipp Wild, Hiltrud Merzenich, and Ulrike Hennewig. 2017. “Prevalence of Cardiovascular Late Sequelae in Long-Term Survivors of Childhood Cancer: A Systematic Review and Meta-Analysis.” Pediatric Blood & Cancer 64 (7).
Senkus, Elzbieta, and Jacek Jassem. 2011. “Cardiovascular Effects of Systemic Cancer Treatment.” Cancer Treatment Reviews 37 (4): 300–311.
Shaikh, Furqan, L Lee Dupuis, Sarah Alexander, Abha Gupta, Luc Mertens, and Paul C Nathan. 2016. “Cardioprotection and Second Malignant Neoplasms Associated With Dexrazoxane in Children Receiving Anthracycline Chemotherapy: A Systematic Review and Meta-Analysis.” Journal of the National Cancer Institute 108 (4).
Sieswerda, Elske, Anna Font-Gonzalez, Johannes B Reitsma, Marcel G W Dijkgraaf, Richard C Heinen, Monique W Jaspers, Helena J van der Pal, et al. 2016. “High Hospitalization Rates in Survivors of Childhood Cancer: A Longitudinal Follow-Up Study Using Medical Record Linkage.” PloS One 11 (7): e0159518.
Simunek, Tomas, Martin Sterba, Olga Popelova, Michaela Adamcova, Radomir Hrdina, and Vladimir Gersl. 2009. “Anthracycline-Induced Cardiotoxicity: Overview of Studies Examining the Roles of Oxidative Stress and Free Cellular Iron.” Pharmacological Reports : PR 61 (1): 154–71.
Skitch, Amy, Seema Mital, Luc Mertens, Peter Liu, Paul Kantor, Lars Grosse-Wortmann, Cedric Manlhiot, Mark Greenberg, and Paul C Nathan. 2017. “Novel Approaches to the Prediction, Diagnosis and Treatment of Cardiac Late Effects in Survivors of Childhood Cancer: A Multi-Centre Observational Study.” BMC Cancer 17 (1): 519.
Sorensen, Gitte Vrelits, Jeanette Falck Winther, Sofie de Fine Licht, Klaus Kaa Andersen, Anna Sallfors Holmqvist, Laura Madanat-Harjuoja, Laufey Tryggvadottir, Andrea Bautz, Timothy L Lash, and Henrik Hasle. 2019. “Long-Term Risk of Hospitalization among Five-Year Survivors of Childhood Leukemia in the Nordic Countries.” Journal of the National Cancer Institute, February.
135
Statistics Canada. 2019. “Table 13-10-0394-01 Leading Causes of Death, Total Population, by Age Group.” https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039401&pickMembers%5B0%5D=2.21&pickMembers%5B1%5D=3.1.
Steinherz, L J, P G Steinherz, C T Tan, G Heller, and M L Murphy. 1991. “Cardiac Toxicity 4 to 20 Years after Completing Anthracycline Therapy.” JAMA 266 (12): 1672–77.
Stoodley, Paul W, David A B Richards, Rina Hui, Anita Boyd, Paul R Harnett, Steven R Meikle, Jillian Clarke, and Liza Thomas. 2011. “Two-Dimensional Myocardial Strain Imaging Detects Changes in Left Ventricular Systolic Function Immediately after Anthracycline Chemotherapy.” European Heart Journal - Cardiovascular Imaging 12 (12): 945–52.
Swain, Sandra M, Fredrick S Whaley, and Michael S Ewer. 2003. “Congestive Heart Failure in Patients Treated with Doxorubicin.” Cancer 97 (11): 2869–79.
Tadic, Marijana, Martin Genger, Ana Baudisch, Sebastian Kelle, Cesare Cuspidi, Evgeny Belyavskiy, Franziska Burkhardt, Lucia Venneri, Philipp Attanasio, and Burkert Pieske. 2018. “Left Ventricular Strain in Chemotherapy-Naive and Radiotherapy-Naive Patients With Cancer.” The Canadian Journal of Cardiology 34 (3): 281–87.
Tanaka, Hidekazu. 2019. “Echocardiography and Cancer Therapeutics-Related Cardiac Dysfunction.” Journal of Medical Ultrasonics 46 (3): 309–16.
Tewey, K M, T C Rowe, L Yang, B D Halligan, and L F Liu. 1984. “Adriamycin-Induced DNA Damage Mediated by Mammalian DNA Topoisomerase II.” Science (New York, N.Y.) 226 (4673): 466–68.
Thavendiranathan, Paaladinesh, Andrew D Grant, Tomoko Negishi, Juan Carlos Plana, Zoran B Popovic, and Thomas H Marwick. 2013. “Reproducibility of Echocardiographic Techniques for Sequential Assessment of Left Ventricular Ejection Fraction and Volumes: Application to Patients Undergoing Cancer Chemotherapy.” Journal of the American College of Cardiology 61 (1): 77–84.
Thavendiranathan, Paaladinesh, Frederic Poulin, Ki-Dong Lim, Juan Carlos Plana, Anna Woo, and Thomas H Marwick. 2014. “Use of Myocardial Strain Imaging by Echocardiography for the Early Detection of Cardiotoxicity in Patients during and after Cancer Chemotherapy: A Systematic Review.” Journal of the American College of Cardiology 63 (25 Pt A): 2751–68.
Tokarska-Schlattner, Malgorzata, Michael Zaugg, Christian Zuppinger, Theo Wallimann, and Uwe Schlattner. 2006. “New Insights into Doxorubicin-Induced Cardiotoxicity: The Critical Role of Cellular Energetics.” Journal of Molecular and Cellular Cardiology 41 (3): 389–405.
Trachtenberg, Barry H, David C Landy, Vivian I Franco, Jacqueline M Henkel, Elliot J Pearson, Tracie L Miller, and Steven E Lipshultz. 2011. “Anthracycline-Associated Cardiotoxicity in Survivors of Childhood Cancer.” Pediatric Cardiology 32 (3): 342–53.
Travis, Lois B, Andrea K Ng, James M Allan, Ching-Hon Pui, Ann R Kennedy, X George Xu, James A Purdy, et al. 2012. “Second Malignant Neoplasms and Cardiovascular Disease
136
Following Radiotherapy.” Journal of the National Cancer Institute 104 (5): 357–70.
Trudeau, Maureen, Flay Charbonneau, Karen Gelmon, Kara Laing, Jean Latreille, John Mackey, Deanna McLeod, Kathy Pritchard, Louise Provencher, and Shailendra Verma. 2005. “Selection of Adjuvant Chemotherapy for Treatment of Node-Positive Breast Cancer.” The Lancet. Oncology 6 (11): 886–98.
Tuzovic, Mirela, Pei-Tzu Wu, Samuel Kianmahd, and Kim-Lien Nguyen. 2018. “Natural History of Myocardial Deformation in Children, Adolescents, and Young Adults Exposed to Anthracyclines: Systematic Review and Meta-Analysis.” Echocardiography (Mount Kisco, N.Y.) 35 (7): 922–34.
Valle, Roberto, Nadia Aspromonte, Loredano Milani, Frank W Peacock, Alan S Maisel, Massimo Santini, and Claudio Ronco. 2011. “Optimizing Fluid Management in Patients with Acute Decompensated Heart Failure (ADHF): The Emerging Role of Combined Measurement of Body Hydration Status and Brain Natriuretic Peptide (BNP) Levels.” Heart Failure Reviews 16 (6): 519–29.
Vejpongsa, P, and E T H Yeh. 2014. “Topoisomerase 2beta: A Promising Molecular Target for Primary Prevention of Anthracycline-Induced Cardiotoxicity.” Clinical Pharmacology and Therapeutics 95 (1): 45–52.
Volkova, Maria, and Raymond Russell 3rd. 2011. “Anthracycline Cardiotoxicity: Prevalence, Pathogenesis and Treatment.” Current Cardiology Reviews 7 (4): 214–20.
Wadugu, Brian, and Bernhard Kuhn. 2012. “The Role of Neuregulin/ErbB2/ErbB4 Signaling in the Heart with Special Focus on Effects on Cardiomyocyte Proliferation.” American Journal of Physiology. Heart and Circulatory Physiology 302 (11): H2139-47.
Wandt, B, L Bojö, K Tolagen, and B Wranne. 1999. “Echocardiographic Assessment of Ejection Fraction in Left Ventricular Hypertrophy.” Heart (British Cardiac Society) 82 (2): 192–98.
Wang, Xuexia, Wei Liu, Can-Lan Sun, Saro H Armenian, Hakon Hakonarson, Lindsey Hageman, Yan Ding, et al. 2014. “Hyaluronan Synthase 3 Variant and Anthracycline-Related Cardiomyopathy: A Report from the Children’s Oncology Group.” Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology 32 (7): 647–53.
Xie, Lin, Jay Onysko, and Howard Morrison. 2018. “Childhood Cancer Incidence in Canada: Demographic and Geographic Variation of Temporal Trends (1992-2010).” Health Promotion and Chronic Disease Prevention in Canada : Research, Policy and Practice 38 (3): 79–115.
Yang, Fang, Qiao Lei, Lu Li, Jian Chang He, Jiajia Zeng, Chunxiang Luo, Sai-Ching Jim Yeung, and Runxiang Yang. 2017. “Delivery of Epirubicin via Slow Infusion as a Strategy to Mitigate Chemotherapy-Induced Cardiotoxicity.” PLOS ONE 12 (11): e0188025.
Yeh, Jennifer M, Larissa Nekhlyudov, Sue J Goldie, Ann C Mertens, and Lisa Diller. 2010. “A Model-Based Estimate of Cumulative Excess Mortality in Survivors of Childhood Cancer.” Annals of Internal Medicine 152 (7): 409–17, W131-8.
137
Yingchoncharoen, Teerapat, Shikhar Agarwal, Zoran B Popovic, and Thomas H Marwick. 2013. “Normal Ranges of Left Ventricular Strain: A Meta-Analysis.” Journal of the American Society of Echocardiography : Official Publication of the American Society of Echocardiography 26 (2): 185–91.
Yoshibayashi, M, T Kamiya, Y Saito, K Nakao, K Nishioka, S Temma, H Itoh, G Shirakami, and H Matsuo. 1995. “Plasma Brain Natriuretic Peptide Concentrations in Healthy Children from Birth to Adolescence: Marked and Rapid Increase after Birth.” European Journal of Endocrinology 133 (2): 207–9.
Yu, Anthony F, Jayant Raikhelkar, Emily C Zabor, Emily S Tonorezos, Chaya S Moskowitz, Roberto Adsuar, Elton Mara, et al. 2016. “Two-Dimensional Speckle Tracking Echocardiography Detects Subclinical Left Ventricular Systolic Dysfunction among Adult Survivors of Childhood, Adolescent, and Young Adult Cancer.” BioMed Research International 2016: 9363951.
Zamorano, Jose Luis, Patrizio Lancellotti, Daniel Rodriguez Muñoz, Victor Aboyans, Riccardo Asteggiano, Maurizio Galderisi, Gilbert Habib, et al. 2016. “2016 ESC Position Paper on Cancer Treatments and Cardiovascular Toxicity Developed under the Auspices of the ESC Committee for Practice Guidelines: The Task Force for Cancer Treatments and Cardiovascular Toxicity of the European Society of Cardiology (ESC.” European Heart Journal 37 (36): 2768–2801.
Zidan, Amal, Laila M Sherief, Amera El-sheikh, Safaa H Saleh, Doaa A Shahbah, Naglaa M Kamal, Hanan S Sherbiny, and Heba Ahmad. 2015. “NT-ProBNP as Early Marker of Subclinical Late Cardiotoxicity after Doxorubicin Therapy and Mediastinal Irradiation in Childhood Cancer Survivors.” Disease Markers 2015: 513219.
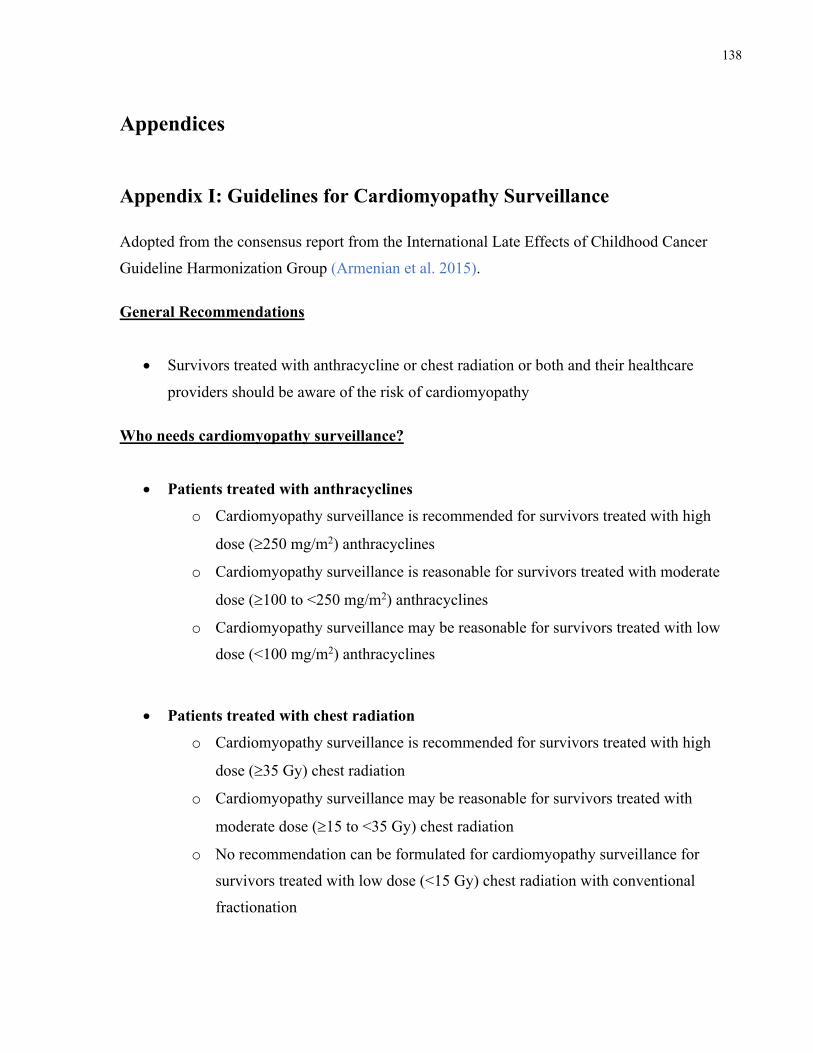
138
Appendices
Appendix I: Guidelines for Cardiomyopathy Surveillance Adopted from the consensus report from the International Late Effects of Childhood Cancer
Guideline Harmonization Group (Armenian et al. 2015). General Recommendations
• Survivors treated with anthracycline or chest radiation or both and their healthcare
providers should be aware of the risk of cardiomyopathy Who needs cardiomyopathy surveillance?
• Patients treated with anthracyclines
o Cardiomyopathy surveillance is recommended for survivors treated with high
dose (³250 mg/m2) anthracyclines
o Cardiomyopathy surveillance is reasonable for survivors treated with moderate
dose (³100 to <250 mg/m2) anthracyclines
o Cardiomyopathy surveillance may be reasonable for survivors treated with low
dose (<100 mg/m2) anthracyclines
• Patients treated with chest radiation
o Cardiomyopathy surveillance is recommended for survivors treated with high
dose (³35 Gy) chest radiation
o Cardiomyopathy surveillance may be reasonable for survivors treated with
moderate dose (³15 to <35 Gy) chest radiation
o No recommendation can be formulated for cardiomyopathy surveillance for
survivors treated with low dose (<15 Gy) chest radiation with conventional
fractionation
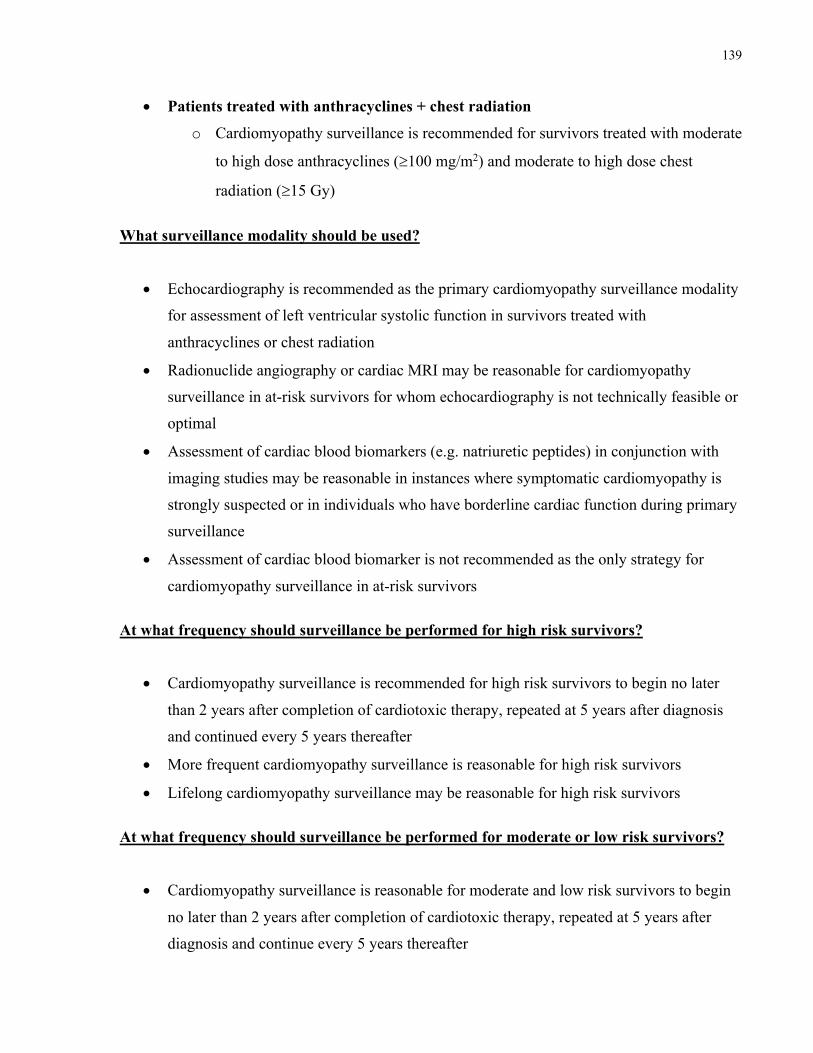
139
• Patients treated with anthracyclines + chest radiation
o Cardiomyopathy surveillance is recommended for survivors treated with moderate
to high dose anthracyclines (³100 mg/m2) and moderate to high dose chest
radiation (³15 Gy)
What surveillance modality should be used?
• Echocardiography is recommended as the primary cardiomyopathy surveillance modality
for assessment of left ventricular systolic function in survivors treated with
anthracyclines or chest radiation
• Radionuclide angiography or cardiac MRI may be reasonable for cardiomyopathy
surveillance in at-risk survivors for whom echocardiography is not technically feasible or
optimal
• Assessment of cardiac blood biomarkers (e.g. natriuretic peptides) in conjunction with
imaging studies may be reasonable in instances where symptomatic cardiomyopathy is
strongly suspected or in individuals who have borderline cardiac function during primary
surveillance
• Assessment of cardiac blood biomarker is not recommended as the only strategy for
cardiomyopathy surveillance in at-risk survivors At what frequency should surveillance be performed for high risk survivors?
• Cardiomyopathy surveillance is recommended for high risk survivors to begin no later
than 2 years after completion of cardiotoxic therapy, repeated at 5 years after diagnosis
and continued every 5 years thereafter
• More frequent cardiomyopathy surveillance is reasonable for high risk survivors
• Lifelong cardiomyopathy surveillance may be reasonable for high risk survivors
At what frequency should surveillance be performed for moderate or low risk survivors?
• Cardiomyopathy surveillance is reasonable for moderate and low risk survivors to begin
no later than 2 years after completion of cardiotoxic therapy, repeated at 5 years after
diagnosis and continue every 5 years thereafter
140
• More frequent cardiomyopathy surveillance may be reasonable for moderate and low risk
survivors
• Lifelong cardiomyopathy surveillance may be reasonable for moderate and low risk
survivors At what frequency should surveillance be performed for survivors who are pregnant or planning to become pregnant?
• Cardiomyopathy surveillance is reasonable before pregnancy or in the first trimester for
all female survivors treated with anthracyclines or chest radiation
• No recommendations can be formulated for the frequency of ongoing surveillance in
pregnant survivors who have normal left ventricular systolic function immediately before
or during the first trimester of pregnancy What should be done when abnormalities are identified?
• Cardiology consultation is recommended for survivors with asymptomatic
cardiomyopathy following treatment with anthracyclines or chest radiation What advice should be given regarding physical activity and other modifiable cardiovascular risk factors?
• Regular exercise, as recommended by the AHA and ESC, offers potential benefits to
survivors treated with anthracyclines or chest radiation
• Regular exercise is recommended for survivors treated with anthracyclines or chest
radiation who have normal left ventricular systolic function
• Cardiology consultation is recommended for survivors with asymptomatic
cardiomyopathy to define limits and precautions for exercise
• Cardiology consultation may be reasonable for high risk survivors who plan to participate
in high intensity exercise to define limits and precautions for physical activity
• Screening for modifiable cardiovascular risk factors (hypertension, dyslipidemia, and
obesity) is recommended for all survivors treated with anthracyclines or chest radiation
so that necessary interventions can be initiated to help avert the risk of symptomatic
cardiomyopathy
141
Appendix II: Echocardiographic Protocol All echocardiographic imaging to be performed on the GE Vivid 7/E9. Observe the following settings:
• High frame rates necessary for colour TDI (>150 fps) • 2D Frame rates should be 50-90 fps • Record 4 beat loops • Obtain BP (right arm) at the end of the study and enter into machine to calculate wall
stress
Parasternal Long Axis View
• Zoom LVOT and aortic valve • PLAX view with colour of aortic and mitral valves • M-mode aortic valve for LVET/LAd and R-R interval • VCFc • PLAX RV inflow 2D and colour and CW Doppler • RV outflow view from PLAX with colour and Doppler
Parasternal Short Axis View
• M-mode at level of mitral valve leaflet tips LV (SF and EF if possible) • Colour Doppler PV and TV • Obtain mean PA pressure when possible • PW Doppler of main PA • 2D PSAX views at MV/PAP/apical levels for 2D speckle strain • Corresponding colour tissue Doppler PSAX at MV/PAP/apical level for strain (using
appropriate TD Nyquist scale) Apical Views (cross sectional areas and long axis dimensions/volumes)
• 2D 4 chamber view for bi-plane Simpson’s and 2D Strain • 2D 2 chamber view for bi-plane Simpson’s and 2D Strain • CALCULATE Simpson’s EF • Colour MV/Aov and TV • Obtain RVsp • Obtain tricuspid valve inflow • Obtain pulsed Tissue Doppler traces optimizing alignment in the basal lateral LV, the
basal septal and basal lateral RV segment • Obtain pulsed Doppler traces in the basal anterior and posterior segments on the 2-
chamber view • Obtain 4-ch apical view of LA/ RA: 2D+ color TDI • Obtain 2-ch view of LA: 2D+ color TDI
142
Mitral valve Doppler/Pulmonary vein Doppler
• Record PW Doppler of Mitral inflow (MVe,a dt): between the valve leaflets (at tips of mitral leaflets)
• PW Doppler between inflow and outflow for IVRT and myocardial performance index • Obtain Color-Doppler M-Mode of LV inflow with adequate baseline shift • LV dp/dt: record CW Doppler of mitral regurgitation (RV dp/dt in single V) • Record PW Doppler RUPV: optimize tracing
LVOT + AO valve Doppler
• Record PW LVOT Doppler • Record CW Doppler through the aortic valve (gradient + aortic acceleration time)
Colour Tissue Doppler
• Broad sector views for colour TDI for LV desynchrony: include 4C + RV, (RV free wall and septum, LV lateral wall and septum, 3C and 2C-12 segments for analysis)
• Narrow sector views from 4-chamber for colour TDI of LV lateral wall, IVS and RV lateral wall for strain (narrow sector width= high frame rates), from two chamber view obtain narrow sector of anterior and posterior wall
IVC/Hepatic veins
• Image and Doppler hepatic venous flow and abdominal aorta • Image and Doppler of SVC from supra-sternal views - required in any patient who has or
had a PICC) At the end of study
• Obtain AFI
Measure BP and measure wall stress
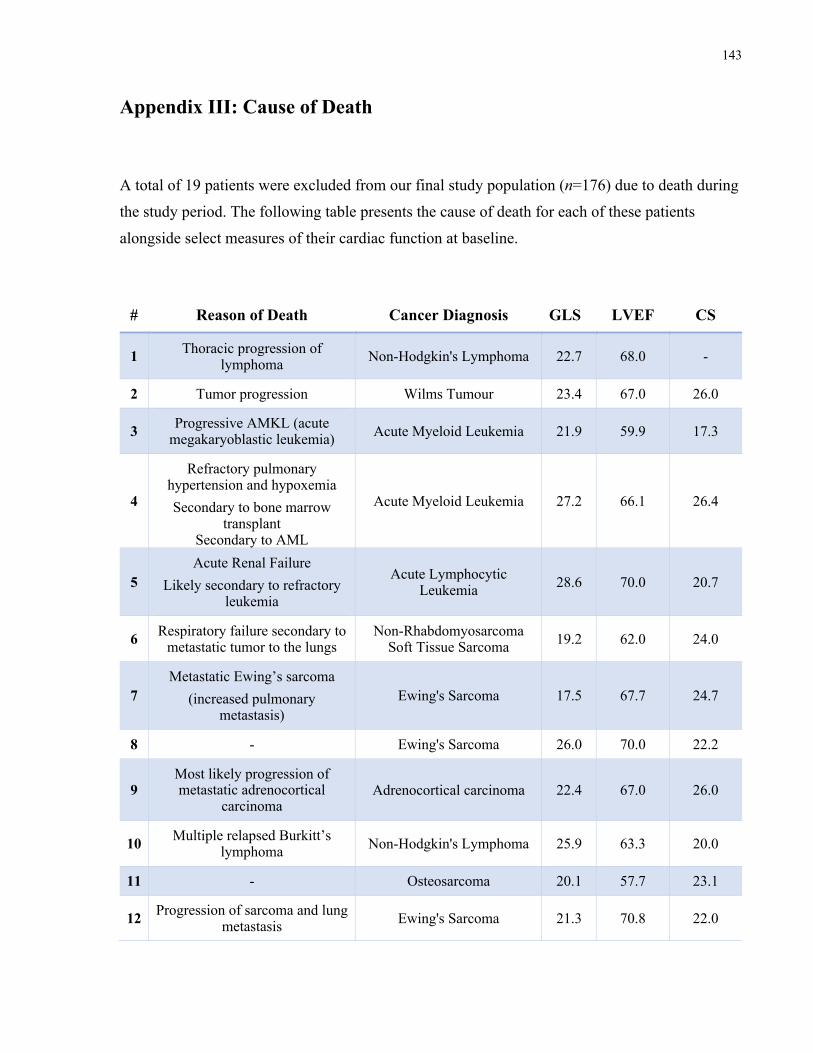
143
Appendix III: Cause of Death
A total of 19 patients were excluded from our final study population (n=176) due to death during
the study period. The following table presents the cause of death for each of these patients
alongside select measures of their cardiac function at baseline.
# Reason of Death Cancer Diagnosis GLS LVEF CS
1 Thoracic progression of lymphoma Non-Hodgkin's Lymphoma 22.7 68.0 -
2 Tumor progression Wilms Tumour 23.4 67.0 26.0
3 Progressive AMKL (acute megakaryoblastic leukemia) Acute Myeloid Leukemia 21.9 59.9 17.3
4
Refractory pulmonary hypertension and hypoxemia Secondary to bone marrow
transplant Secondary to AML
Acute Myeloid Leukemia 27.2 66.1 26.4
5 Acute Renal Failure
Likely secondary to refractory leukemia
Acute Lymphocytic Leukemia 28.6 70.0 20.7
6 Respiratory failure secondary to metastatic tumor to the lungs
Non-Rhabdomyosarcoma Soft Tissue Sarcoma 19.2 62.0 24.0
7 Metastatic Ewing’s sarcoma
(increased pulmonary metastasis)
Ewing's Sarcoma 17.5 67.7 24.7
8 - Ewing's Sarcoma 26.0 70.0 22.2
9 Most likely progression of metastatic adrenocortical
carcinoma Adrenocortical carcinoma 22.4 67.0 26.0
10 Multiple relapsed Burkitt’s lymphoma Non-Hodgkin's Lymphoma 25.9 63.3 20.0
11 - Osteosarcoma 20.1 57.7 23.1
12 Progression of sarcoma and lung metastasis Ewing's Sarcoma 21.3 70.8 22.0
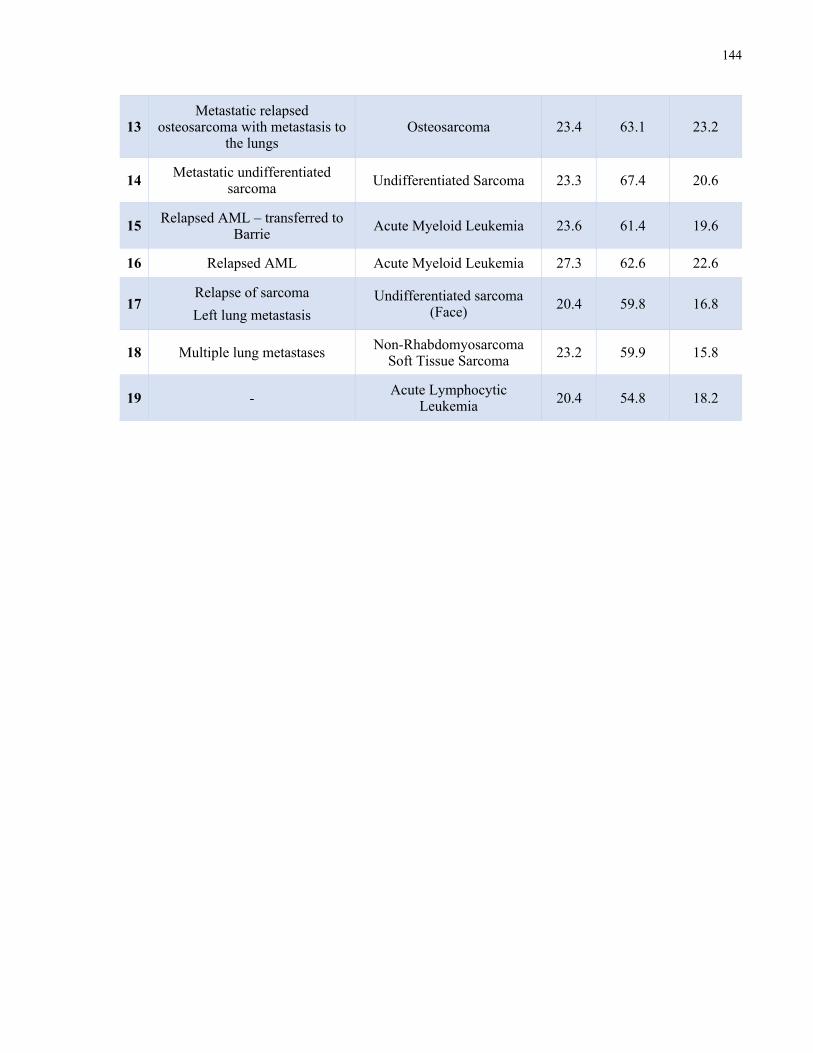
144
13 Metastatic relapsed
osteosarcoma with metastasis to the lungs
Osteosarcoma 23.4 63.1 23.2
14 Metastatic undifferentiated sarcoma Undifferentiated Sarcoma 23.3 67.4 20.6
15 Relapsed AML – transferred to Barrie Acute Myeloid Leukemia 23.6 61.4 19.6
16 Relapsed AML Acute Myeloid Leukemia 27.3 62.6 22.6
17 Relapse of sarcoma Left lung metastasis
Undifferentiated sarcoma (Face) 20.4 59.8 16.8
18 Multiple lung metastases Non-Rhabdomyosarcoma Soft Tissue Sarcoma 23.2 59.9 15.8
19 - Acute Lymphocytic Leukemia 20.4 54.8 18.2
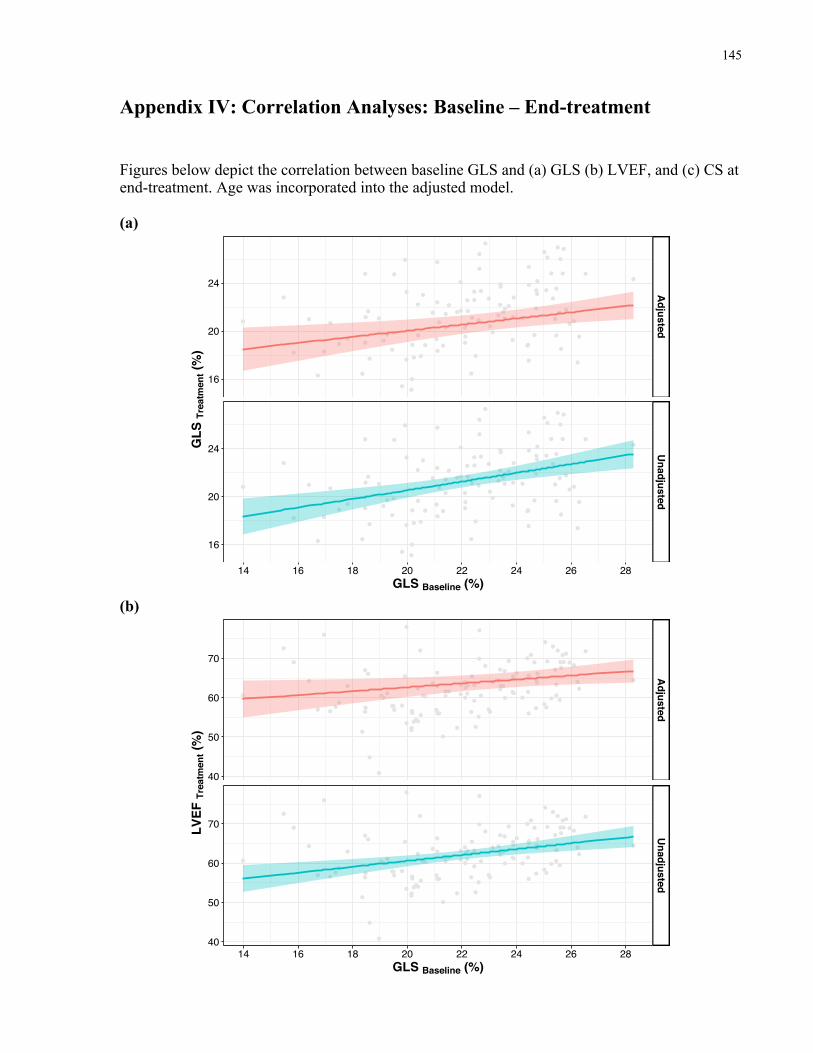
145
Appendix IV: Correlation Analyses: Baseline – End-treatment Figures below depict the correlation between baseline GLS and (a) GLS (b) LVEF, and (c) CS at end-treatment. Age was incorporated into the adjusted model. (a)
(b)
Adjusted
Unadjusted
14 16 18 20 22 24 26 28
16
20
24
16
20
24
GLS Baseline (%)
GLS
Tre
atm
ent (
%)
Adjusted
Unadjusted
14 16 18 20 22 24 26 28
40
50
60
70
40
50
60
70
GLS Baseline (%)
LVEF
Tre
atm
ent (
%)
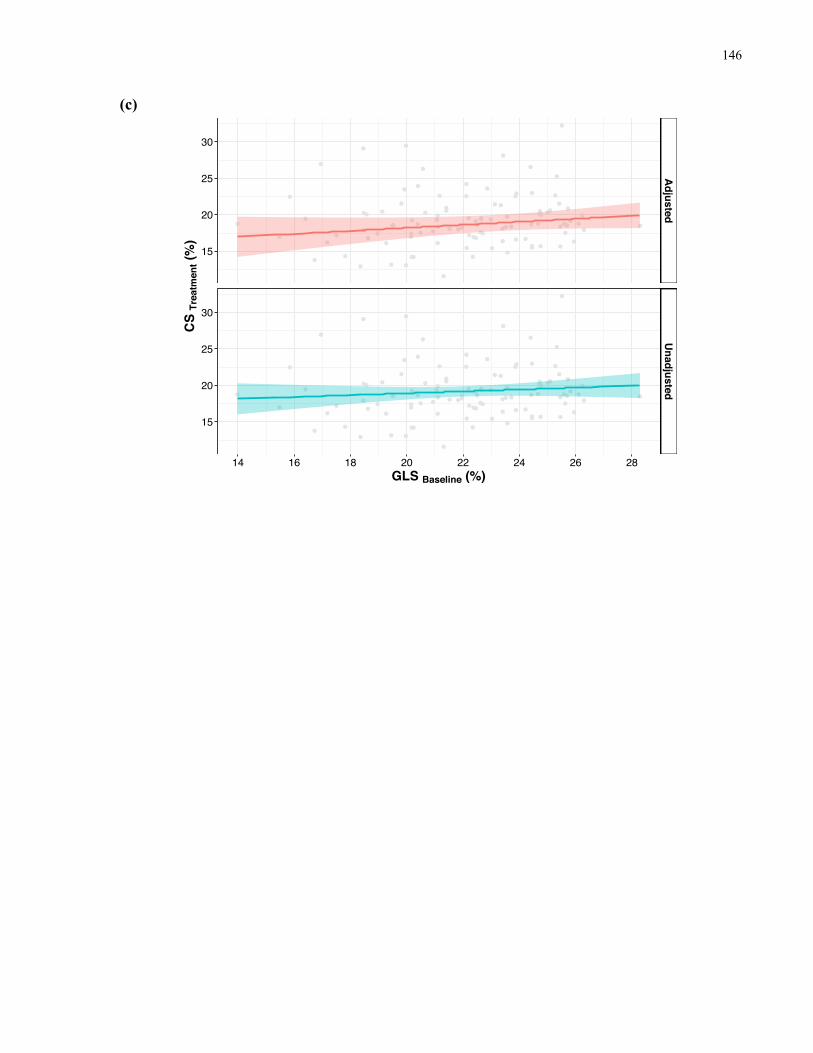
146
(c)
Adjusted
Unadjusted
14 16 18 20 22 24 26 28
15
20
25
30
15
20
25
30
GLS Baseline (%)
CS
Trea
tmen
t (%
)
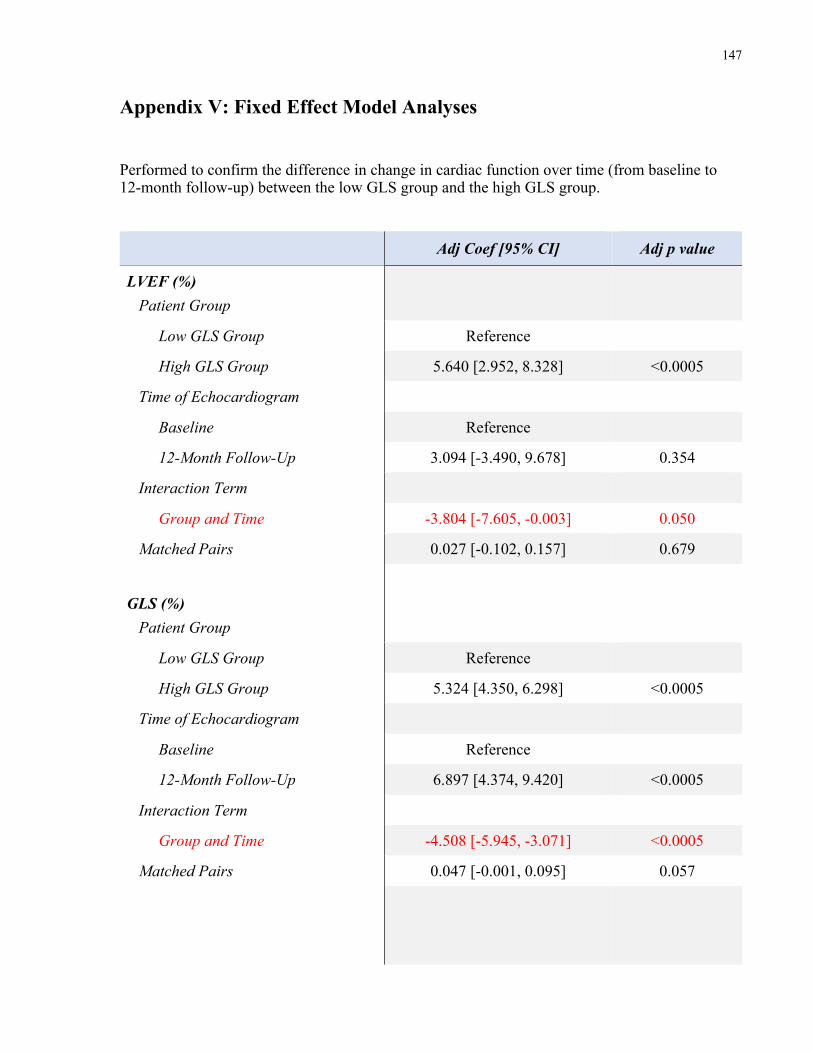
147
Appendix V: Fixed Effect Model Analyses Performed to confirm the difference in change in cardiac function over time (from baseline to 12-month follow-up) between the low GLS group and the high GLS group.
Adj Coef [95% CI] Adj p value
LVEF (%) Patient Group
Low GLS Group Reference
High GLS Group 5.640 [2.952, 8.328] <0.0005
Time of Echocardiogram
Baseline Reference
12-Month Follow-Up 3.094 [-3.490, 9.678] 0.354
Interaction Term
Group and Time -3.804 [-7.605, -0.003] 0.050
Matched Pairs 0.027 [-0.102, 0.157] 0.679
GLS (%) Patient Group
Low GLS Group Reference
High GLS Group 5.324 [4.350, 6.298] <0.0005
Time of Echocardiogram
Baseline Reference
12-Month Follow-Up 6.897 [4.374, 9.420] <0.0005
Interaction Term
Group and Time -4.508 [-5.945, -3.071] <0.0005
Matched Pairs 0.047 [-0.001, 0.095] 0.057
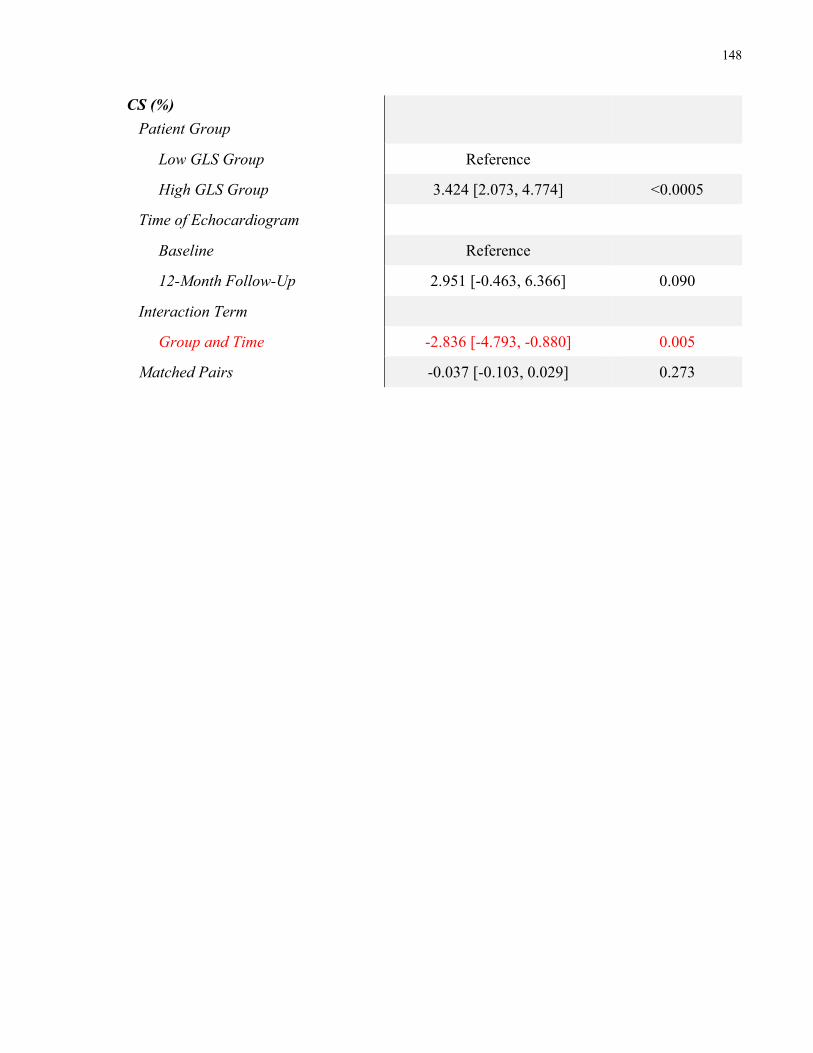
148
CS (%) Patient Group
Low GLS Group Reference
High GLS Group 3.424 [2.073, 4.774] <0.0005
Time of Echocardiogram
Baseline Reference
12-Month Follow-Up 2.951 [-0.463, 6.366] 0.090
Interaction Term
Group and Time -2.836 [-4.793, -0.880] 0.005
Matched Pairs -0.037 [-0.103, 0.029] 0.273
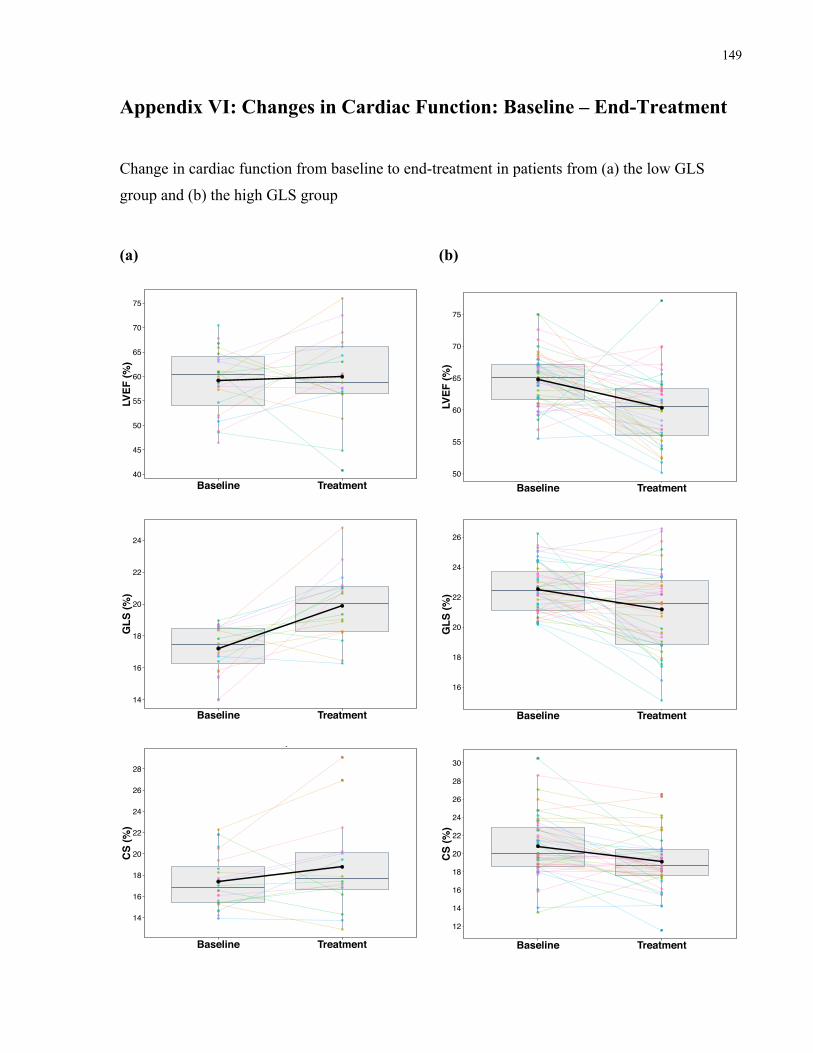
149
Appendix VI: Changes in Cardiac Function: Baseline – End-Treatment
Change in cardiac function from baseline to end-treatment in patients from (a) the low GLS
group and (b) the high GLS group
(a) (b)
40
45
50
55
60
65
70
75
Baseline Treatment
LVEF
(%)
Group 1
50
55
60
65
70
75
Baseline Treatment
LVEF
(%)
Group 2
14
16
18
20
22
24
Baseline Treatment
GLS
(%)
Group 1
16
18
20
22
24
26
Baseline Treatment
GLS
(%)
Group 2
14
16
18
20
22
24
26
28
Baseline Treatment
CS
(%)
Group 1
12
14
16
18
20
22
24
26
28
30
Baseline Treatment
CS
(%)
Group 2
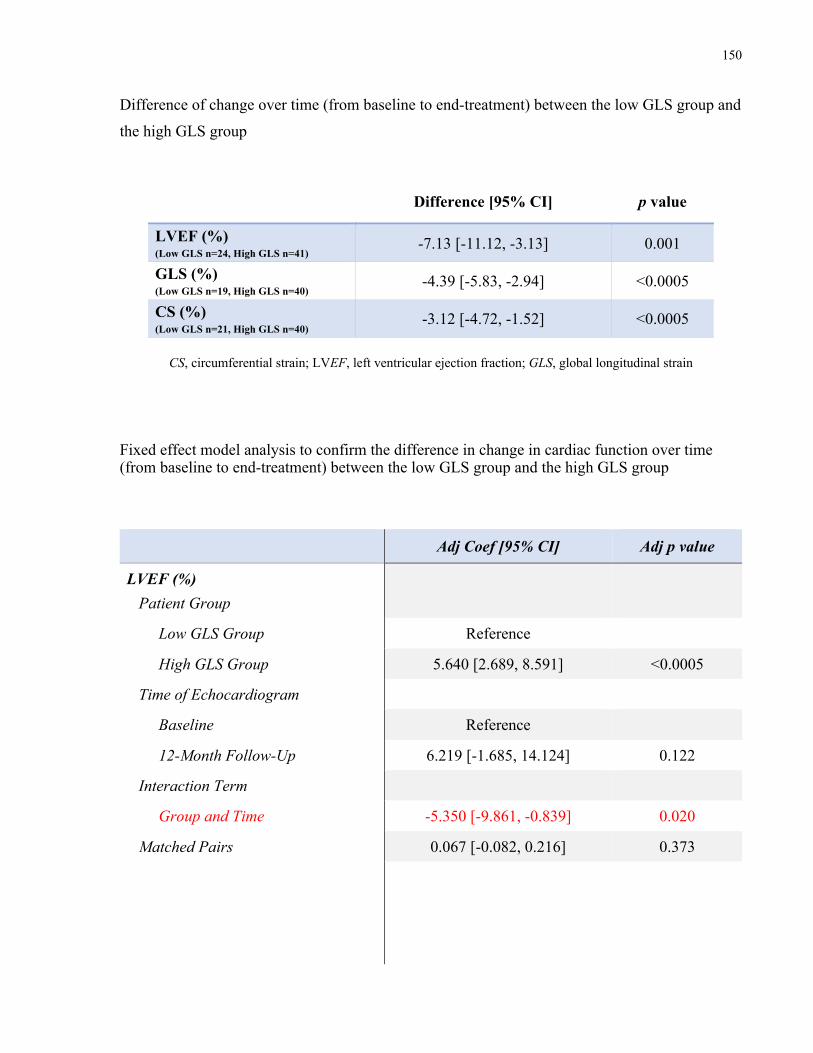
150
Difference of change over time (from baseline to end-treatment) between the low GLS group and
the high GLS group
Difference [95% CI] p value
LVEF (%) (Low GLS n=24, High GLS n=41) -7.13 [-11.12, -3.13] 0.001
GLS (%) (Low GLS n=19, High GLS n=40) -4.39 [-5.83, -2.94] <0.0005
CS (%) (Low GLS n=21, High GLS n=40) -3.12 [-4.72, -1.52] <0.0005
CS, circumferential strain; LVEF, left ventricular ejection fraction; GLS, global longitudinal strain
Fixed effect model analysis to confirm the difference in change in cardiac function over time (from baseline to end-treatment) between the low GLS group and the high GLS group
Adj Coef [95% CI] Adj p value
LVEF (%) Patient Group
Low GLS Group Reference
High GLS Group 5.640 [2.689, 8.591] <0.0005
Time of Echocardiogram
Baseline Reference
12-Month Follow-Up 6.219 [-1.685, 14.124] 0.122
Interaction Term
Group and Time -5.350 [-9.861, -0.839] 0.020
Matched Pairs 0.067 [-0.082, 0.216] 0.373
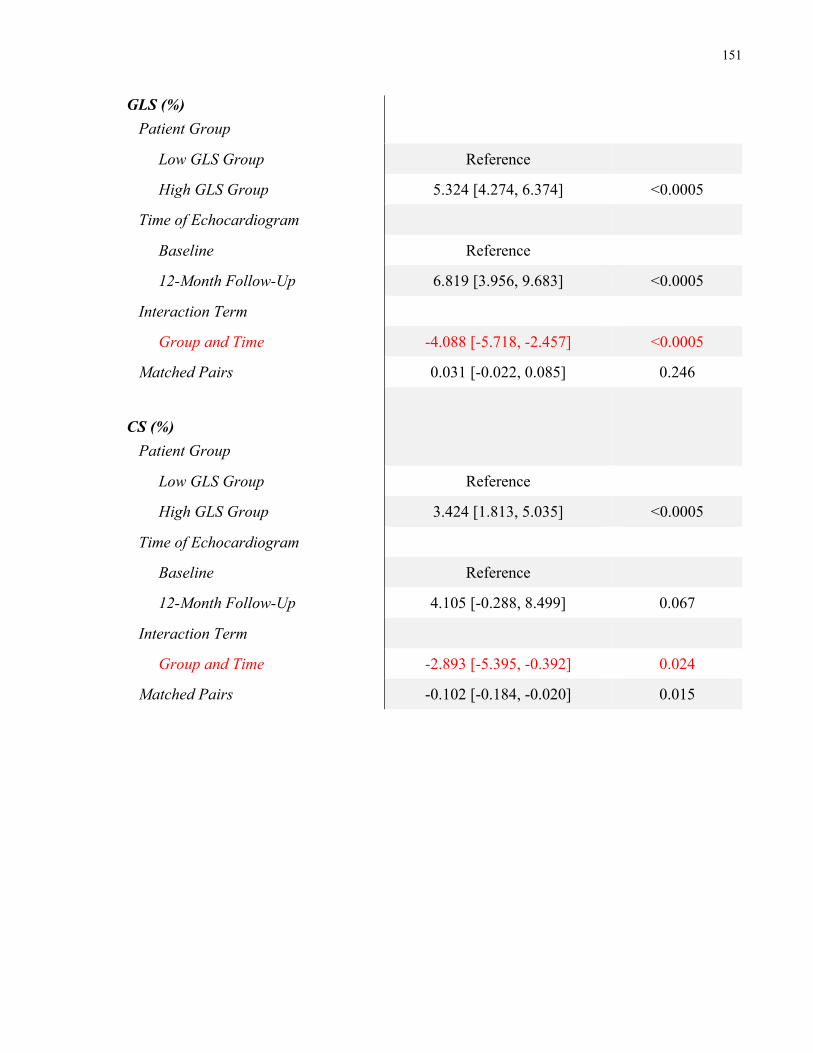
151
GLS (%) Patient Group
Low GLS Group Reference
High GLS Group 5.324 [4.274, 6.374] <0.0005
Time of Echocardiogram
Baseline Reference
12-Month Follow-Up 6.819 [3.956, 9.683] <0.0005
Interaction Term
Group and Time -4.088 [-5.718, -2.457] <0.0005
Matched Pairs 0.031 [-0.022, 0.085] 0.246
CS (%) Patient Group
Low GLS Group Reference
High GLS Group 3.424 [1.813, 5.035] <0.0005
Time of Echocardiogram
Baseline Reference
12-Month Follow-Up 4.105 [-0.288, 8.499] 0.067
Interaction Term
Group and Time -2.893 [-5.395, -0.392] 0.024
Matched Pairs -0.102 [-0.184, -0.020] 0.015
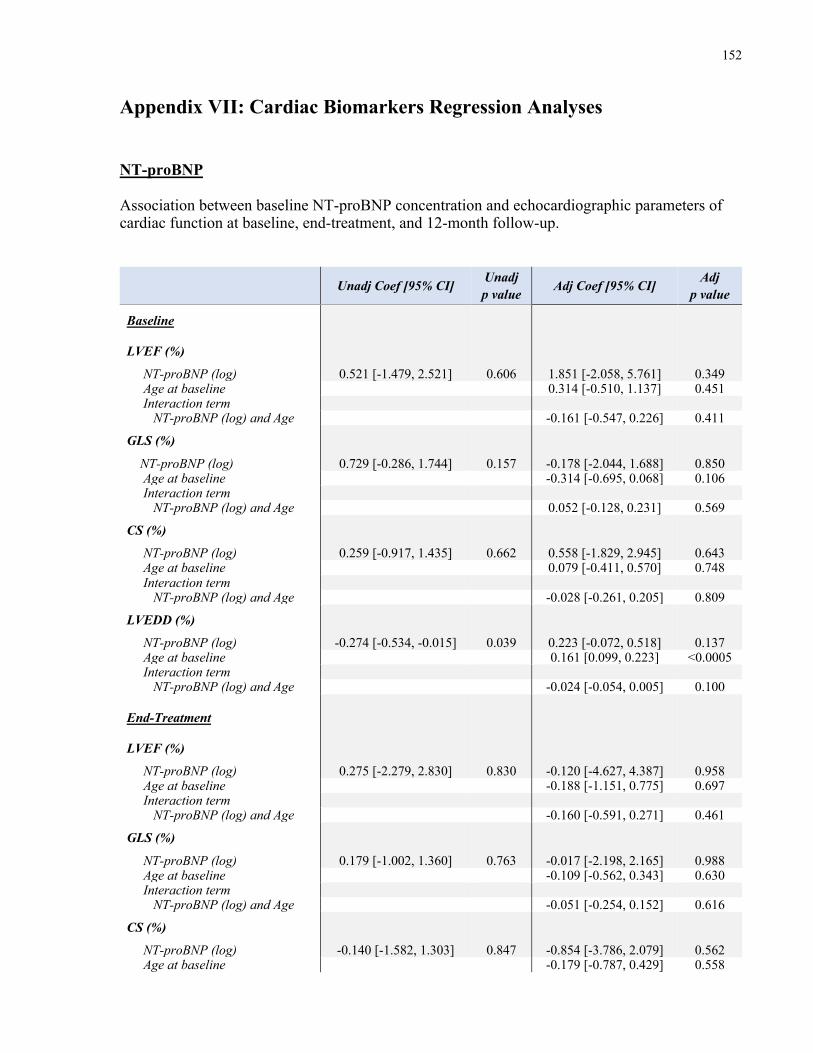
152
Appendix VII: Cardiac Biomarkers Regression Analyses NT-proBNP Association between baseline NT-proBNP concentration and echocardiographic parameters of cardiac function at baseline, end-treatment, and 12-month follow-up.
Unadj Coef [95% CI] Unadj p value Adj Coef [95% CI] Adj
p value
Baseline
LVEF (%)
NT-proBNP (log) 0.521 [-1.479, 2.521] 0.606 1.851 [-2.058, 5.761] 0.349 Age at baseline 0.314 [-0.510, 1.137] 0.451 Interaction term NT-proBNP (log) and Age -0.161 [-0.547, 0.226] 0.411
GLS (%)
NT-proBNP (log) 0.729 [-0.286, 1.744] 0.157 -0.178 [-2.044, 1.688] 0.850 Age at baseline -0.314 [-0.695, 0.068] 0.106 Interaction term NT-proBNP (log) and Age 0.052 [-0.128, 0.231] 0.569
CS (%)
NT-proBNP (log) 0.259 [-0.917, 1.435] 0.662 0.558 [-1.829, 2.945] 0.643 Age at baseline 0.079 [-0.411, 0.570] 0.748 Interaction term NT-proBNP (log) and Age -0.028 [-0.261, 0.205] 0.809
LVEDD (%)
NT-proBNP (log) -0.274 [-0.534, -0.015] 0.039 0.223 [-0.072, 0.518] 0.137 Age at baseline 0.161 [0.099, 0.223] <0.0005 Interaction term NT-proBNP (log) and Age -0.024 [-0.054, 0.005] 0.100
End-Treatment
LVEF (%)
NT-proBNP (log) 0.275 [-2.279, 2.830] 0.830 -0.120 [-4.627, 4.387] 0.958 Age at baseline -0.188 [-1.151, 0.775] 0.697 Interaction term NT-proBNP (log) and Age -0.160 [-0.591, 0.271] 0.461
GLS (%)
NT-proBNP (log) 0.179 [-1.002, 1.360] 0.763 -0.017 [-2.198, 2.165] 0.988 Age at baseline -0.109 [-0.562, 0.343] 0.630 Interaction term NT-proBNP (log) and Age -0.051 [-0.254, 0.152] 0.616
CS (%)
NT-proBNP (log) -0.140 [-1.582, 1.303] 0.847 -0.854 [-3.786, 2.079] 0.562 Age at baseline -0.179 [-0.787, 0.429] 0.558
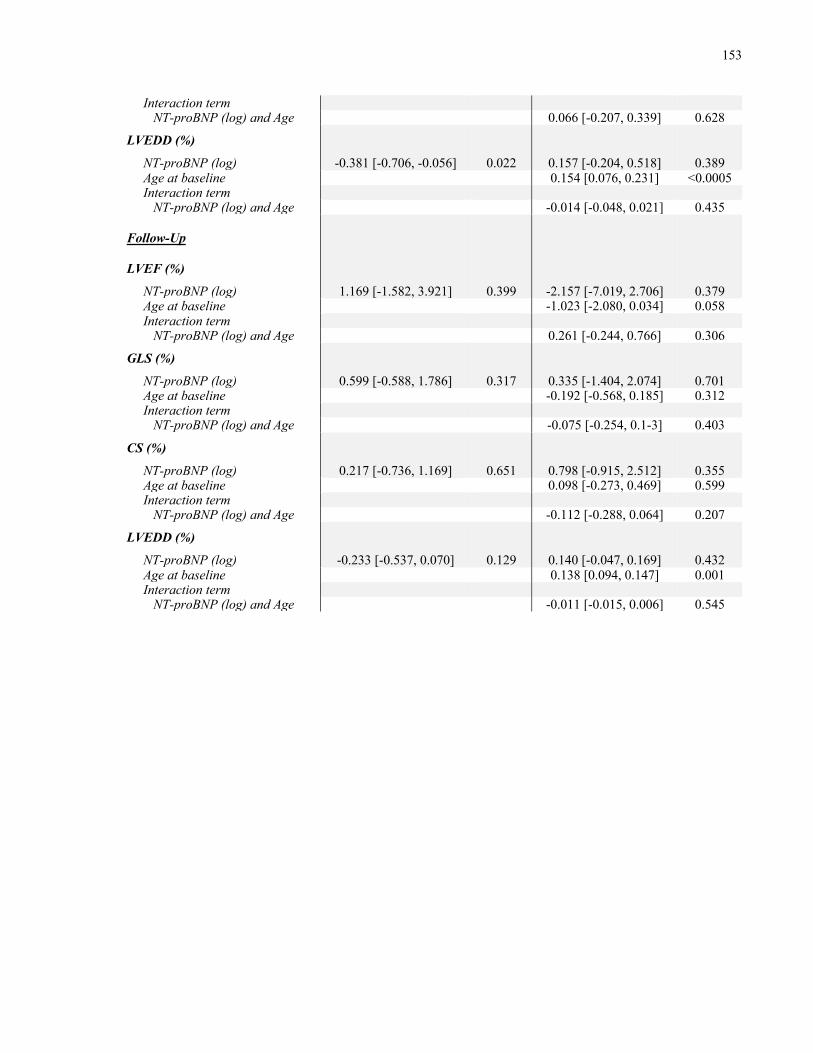
153
Interaction term NT-proBNP (log) and Age 0.066 [-0.207, 0.339] 0.628
LVEDD (%)
NT-proBNP (log) -0.381 [-0.706, -0.056] 0.022 0.157 [-0.204, 0.518] 0.389 Age at baseline 0.154 [0.076, 0.231] <0.0005 Interaction term NT-proBNP (log) and Age -0.014 [-0.048, 0.021] 0.435
Follow-Up
LVEF (%)
NT-proBNP (log) 1.169 [-1.582, 3.921] 0.399 -2.157 [-7.019, 2.706] 0.379 Age at baseline -1.023 [-2.080, 0.034] 0.058 Interaction term NT-proBNP (log) and Age 0.261 [-0.244, 0.766] 0.306
GLS (%)
NT-proBNP (log) 0.599 [-0.588, 1.786] 0.317 0.335 [-1.404, 2.074] 0.701 Age at baseline -0.192 [-0.568, 0.185] 0.312 Interaction term NT-proBNP (log) and Age -0.075 [-0.254, 0.1-3] 0.403
CS (%)
NT-proBNP (log) 0.217 [-0.736, 1.169] 0.651 0.798 [-0.915, 2.512] 0.355 Age at baseline 0.098 [-0.273, 0.469] 0.599 Interaction term NT-proBNP (log) and Age -0.112 [-0.288, 0.064] 0.207
LVEDD (%)
NT-proBNP (log) -0.233 [-0.537, 0.070] 0.129 0.140 [-0.047, 0.169] 0.432 Age at baseline 0.138 [0.094, 0.147] 0.001 Interaction term NT-proBNP (log) and Age -0.011 [-0.015, 0.006] 0.545
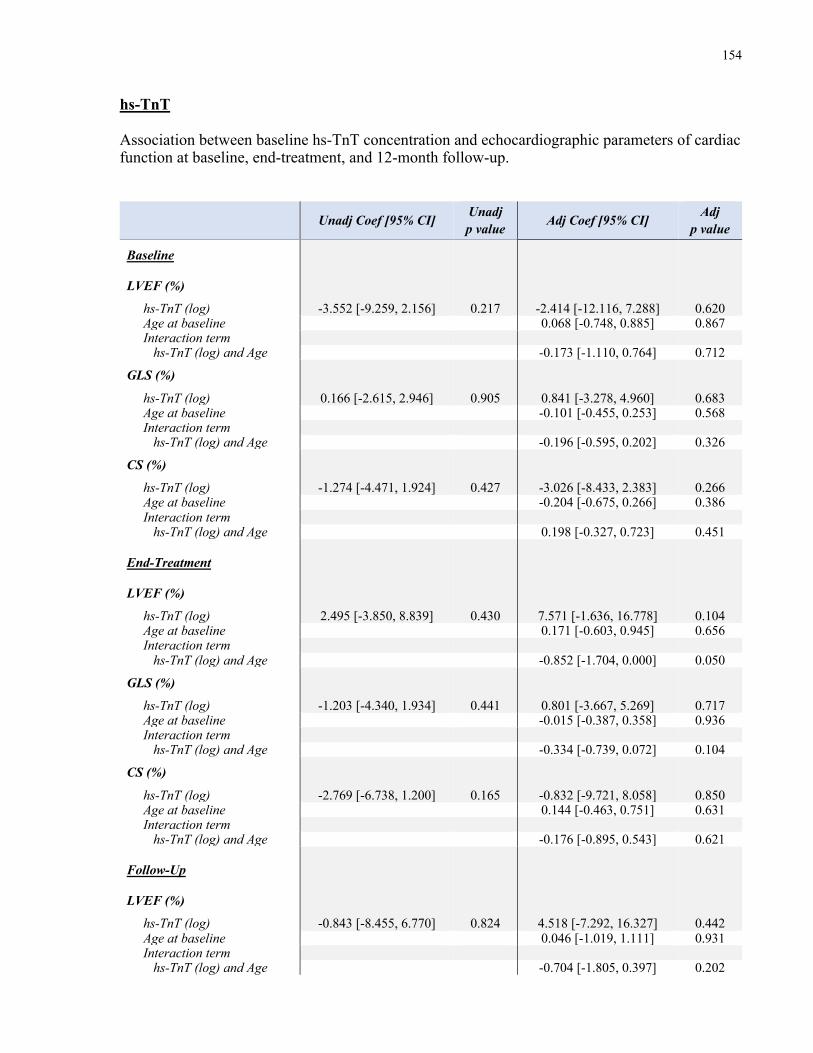
154
hs-TnT Association between baseline hs-TnT concentration and echocardiographic parameters of cardiac function at baseline, end-treatment, and 12-month follow-up.
Unadj Coef [95% CI] Unadj p value Adj Coef [95% CI] Adj
p value
Baseline
LVEF (%)
hs-TnT (log) -3.552 [-9.259, 2.156] 0.217 -2.414 [-12.116, 7.288] 0.620 Age at baseline 0.068 [-0.748, 0.885] 0.867 Interaction term hs-TnT (log) and Age -0.173 [-1.110, 0.764] 0.712
GLS (%)
hs-TnT (log) 0.166 [-2.615, 2.946] 0.905 0.841 [-3.278, 4.960] 0.683 Age at baseline -0.101 [-0.455, 0.253] 0.568 Interaction term hs-TnT (log) and Age -0.196 [-0.595, 0.202] 0.326
CS (%)
hs-TnT (log) -1.274 [-4.471, 1.924] 0.427 -3.026 [-8.433, 2.383] 0.266 Age at baseline -0.204 [-0.675, 0.266] 0.386 Interaction term hs-TnT (log) and Age 0.198 [-0.327, 0.723] 0.451
End-Treatment
LVEF (%)
hs-TnT (log) 2.495 [-3.850, 8.839] 0.430 7.571 [-1.636, 16.778] 0.104 Age at baseline 0.171 [-0.603, 0.945] 0.656 Interaction term hs-TnT (log) and Age -0.852 [-1.704, 0.000] 0.050
GLS (%)
hs-TnT (log) -1.203 [-4.340, 1.934] 0.441 0.801 [-3.667, 5.269] 0.717 Age at baseline -0.015 [-0.387, 0.358] 0.936 Interaction term hs-TnT (log) and Age -0.334 [-0.739, 0.072] 0.104
CS (%)
hs-TnT (log) -2.769 [-6.738, 1.200] 0.165 -0.832 [-9.721, 8.058] 0.850 Age at baseline 0.144 [-0.463, 0.751] 0.631 Interaction term hs-TnT (log) and Age -0.176 [-0.895, 0.543] 0.621
Follow-Up
LVEF (%)
hs-TnT (log) -0.843 [-8.455, 6.770] 0.824 4.518 [-7.292, 16.327] 0.442 Age at baseline 0.046 [-1.019, 1.111] 0.931 Interaction term hs-TnT (log) and Age -0.704 [-1.805, 0.397] 0.202
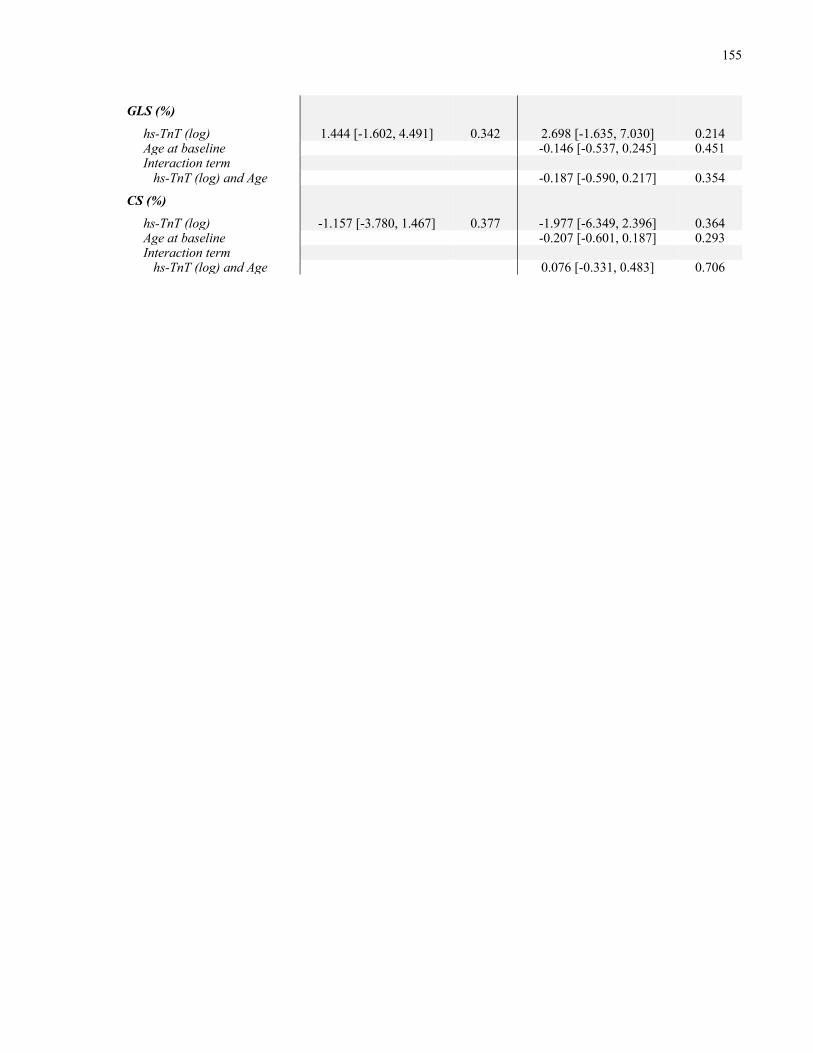
155
GLS (%)
hs-TnT (log) 1.444 [-1.602, 4.491] 0.342 2.698 [-1.635, 7.030] 0.214 Age at baseline -0.146 [-0.537, 0.245] 0.451 Interaction term hs-TnT (log) and Age -0.187 [-0.590, 0.217] 0.354
CS (%)
hs-TnT (log) -1.157 [-3.780, 1.467] 0.377 -1.977 [-6.349, 2.396] 0.364 Age at baseline -0.207 [-0.601, 0.187] 0.293 Interaction term hs-TnT (log) and Age 0.076 [-0.331, 0.483] 0.706
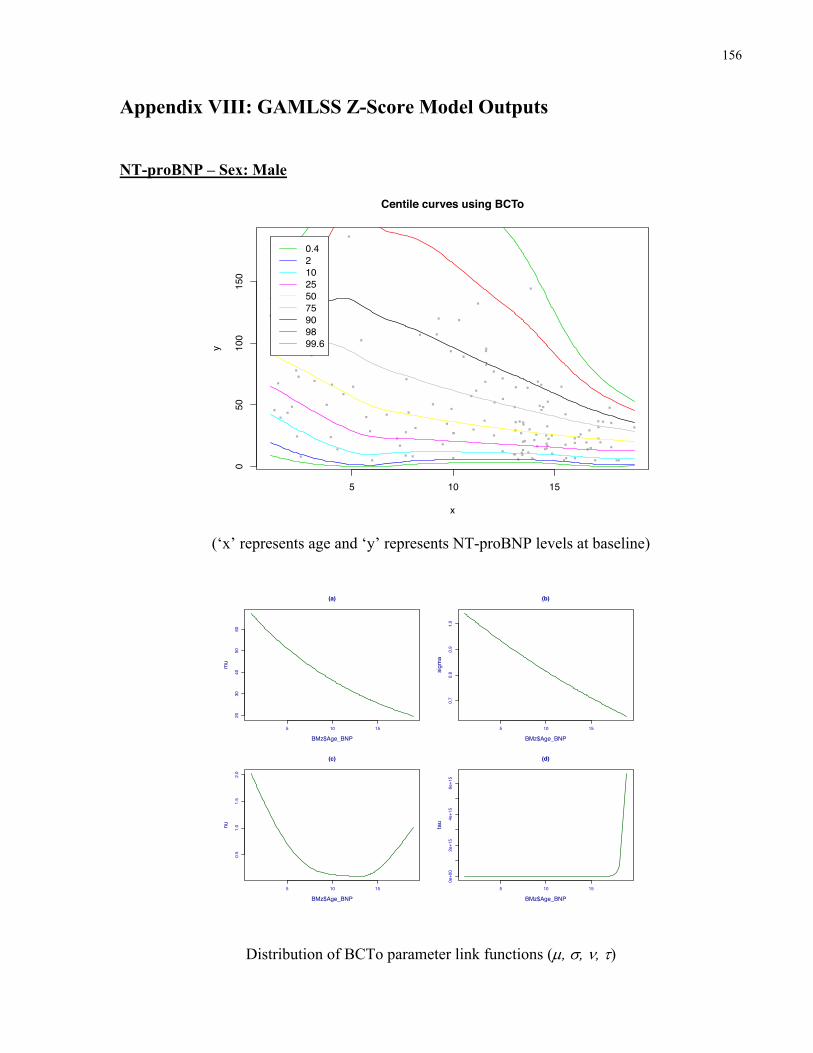
156
Appendix VIII: GAMLSS Z-Score Model Outputs NT-proBNP – Sex: Male
(‘x’ represents age and ‘y’ represents NT-proBNP levels at baseline)
Distribution of BCTo parameter link functions (µ, s, n, t)
5 10 15
050
100
150
x
yCentile curves using BCTo
0.4210255075909899.6
5 10 15
2030
4050
60
(a)
BMz$Age_BNP
mu
5 10 15
0.7
0.8
0.9
1.0
(b)
BMz$Age_BNP
sigm
a
5 10 15
0.5
1.0
1.5
2.0
(c)
BMz$Age_BNP
nu
5 10 15
0e+00
2e+15
4e+15
6e+15
(d)
BMz$Age_BNP
tau
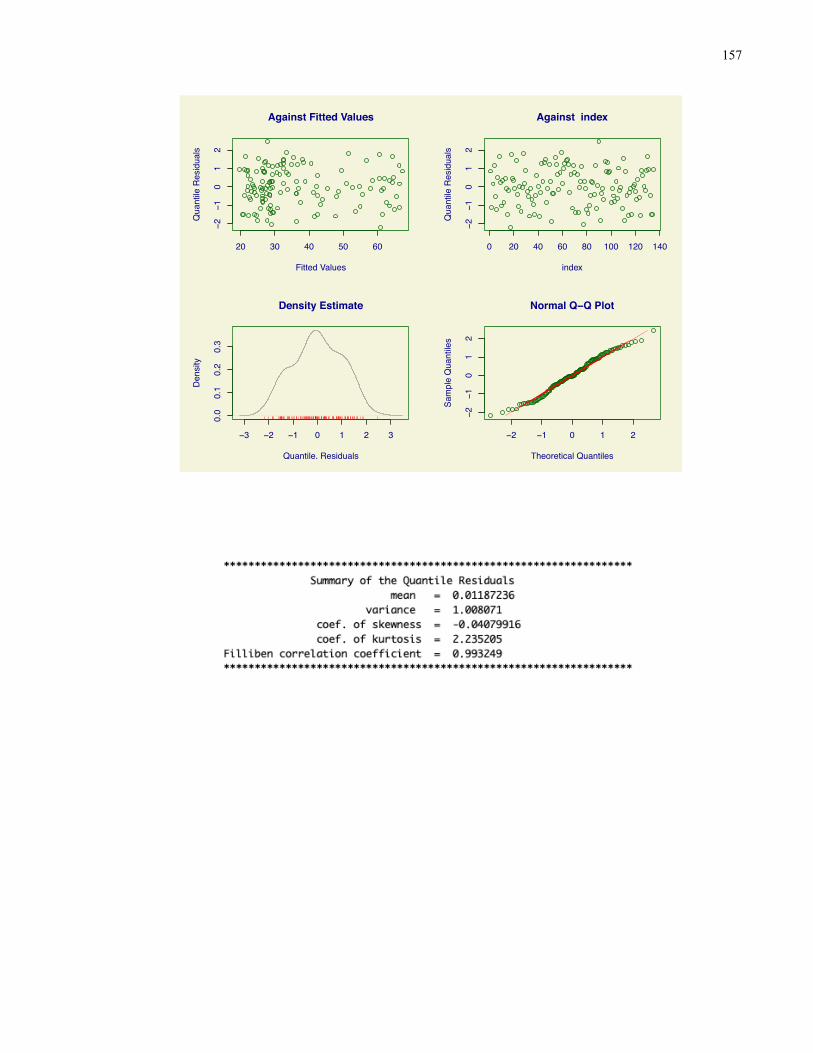
157
20 30 40 50 60
−2−1
01
2
Against Fitted Values
Fitted Values
Qua
ntile
Res
idua
ls
0 20 40 60 80 100 120 140
−2−1
01
2
Against index
index
Qua
ntile
Res
idua
ls−3 −2 −1 0 1 2 3
0.0
0.1
0.2
0.3
Density Estimate
Quantile. Residuals
Den
sity
−2 −1 0 1 2
−2−1
01
2
Normal Q−Q Plot
Theoretical QuantilesSa
mpl
e Q
uant
iles
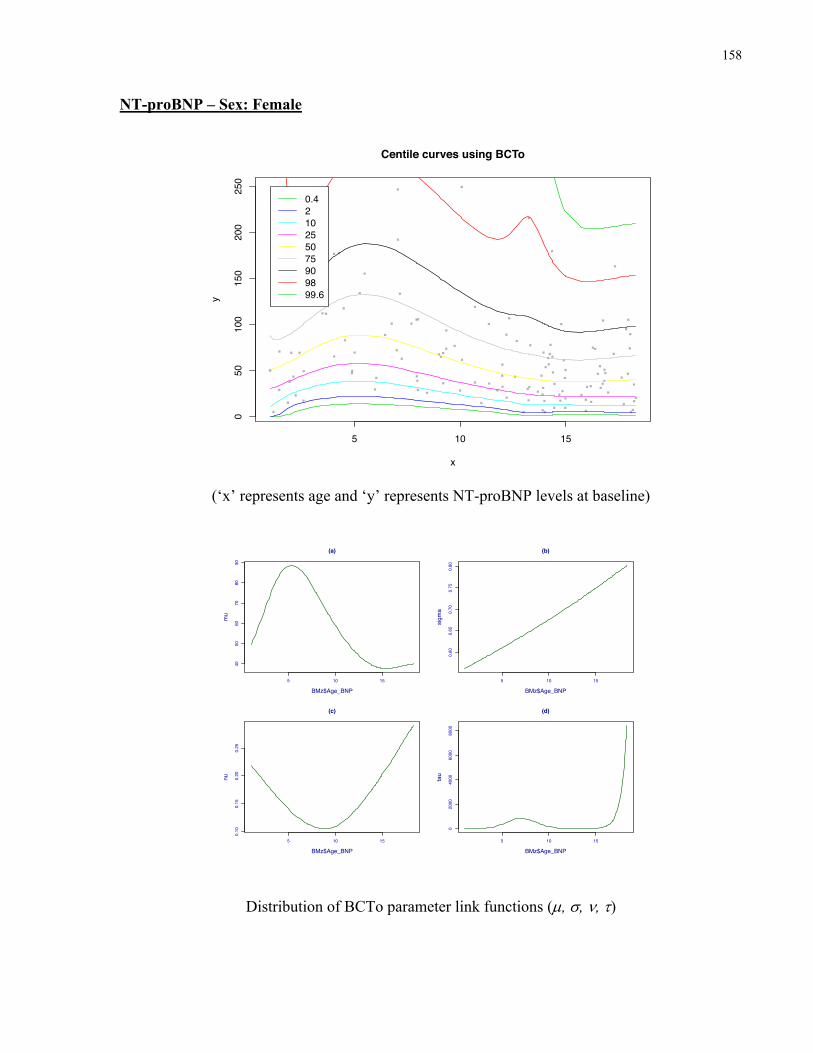
158
NT-proBNP – Sex: Female
(‘x’ represents age and ‘y’ represents NT-proBNP levels at baseline)
Distribution of BCTo parameter link functions (µ, s, n, t)
5 10 15
050
100
150
200
250
x
y
Centile curves using BCTo
0.4210255075909899.6
5 10 15
4050
6070
8090
(a)
BMz$Age_BNP
mu
5 10 15
0.60
0.65
0.70
0.75
0.80
(b)
BMz$Age_BNP
sigm
a
5 10 15
0.10
0.15
0.20
0.25
(c)
BMz$Age_BNP
nu
5 10 15
02000
4000
6000
8000
(d)
BMz$Age_BNP
tau
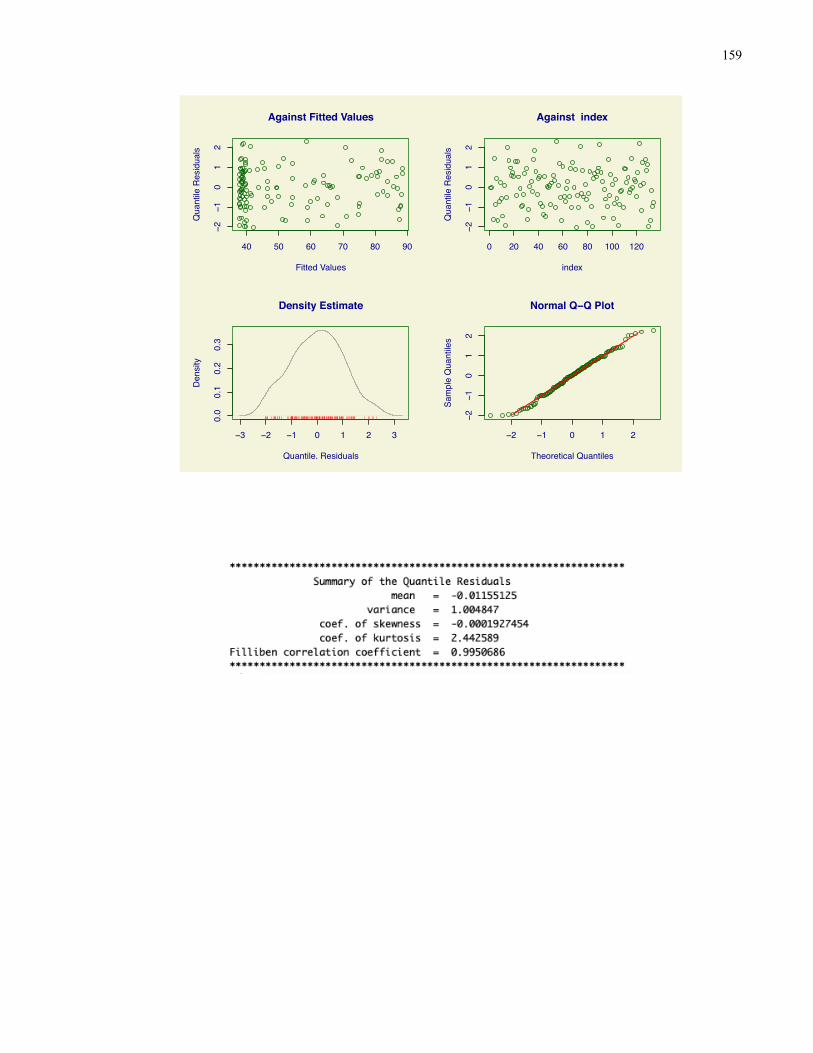
159
40 50 60 70 80 90
−2−1
01
2
Against Fitted Values
Fitted Values
Qua
ntile
Res
idua
ls
0 20 40 60 80 100 120
−2−1
01
2
Against index
index
Qua
ntile
Res
idua
ls−3 −2 −1 0 1 2 3
0.0
0.1
0.2
0.3
Density Estimate
Quantile. Residuals
Den
sity
−2 −1 0 1 2
−2−1
01
2
Normal Q−Q Plot
Theoretical QuantilesSa
mpl
e Q
uant
iles
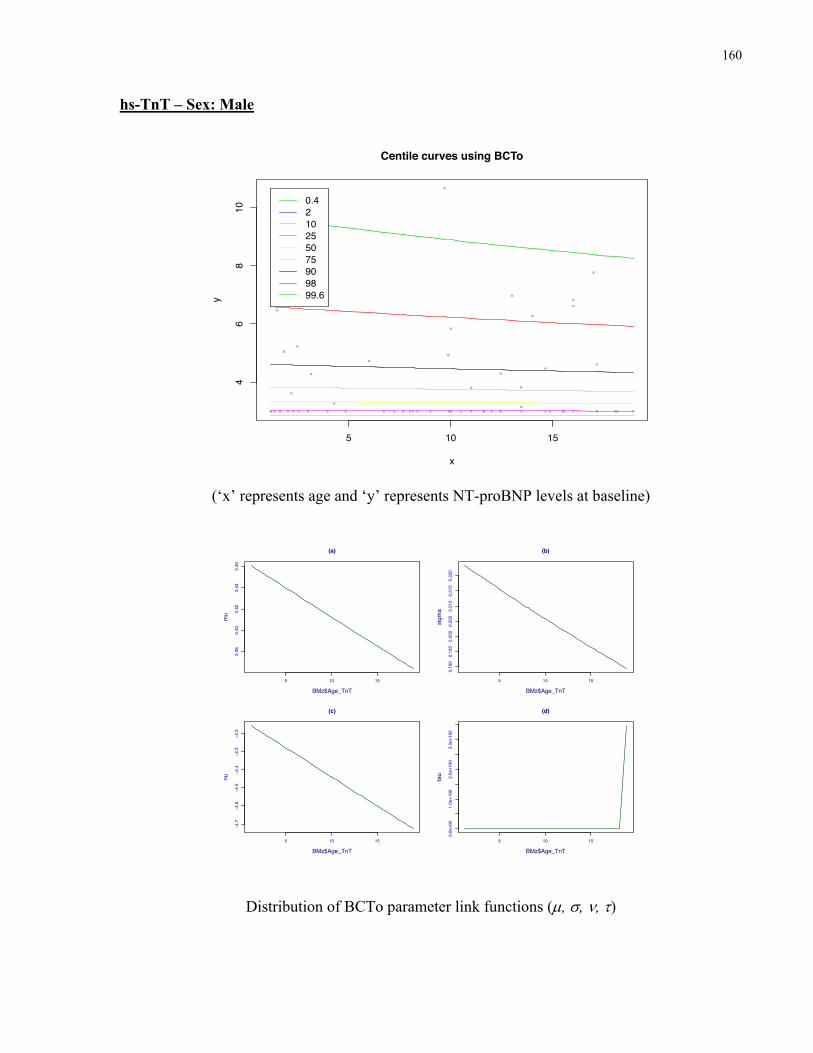
160
hs-TnT – Sex: Male
(‘x’ represents age and ‘y’ represents NT-proBNP levels at baseline)
Distribution of BCTo parameter link functions (µ, s, n, t)
5 10 15
46
810
x
y
Centile curves using BCTo
0.4210255075909899.6
5 10 15
3.38
3.40
3.42
3.44
3.46
(a)
BMz$Age_TnT
mu
5 10 15
0.190
0.195
0.200
0.205
0.210
0.215
0.220
(b)
BMz$Age_TnT
sigm
a
5 10 15
−4.7
−4.6
−4.5
−4.4
−4.3
−4.2
(c)
BMz$Age_TnT
nu
5 10 15
0.0e+00
1.0e+190
2.0e+190
3.0e+190
(d)
BMz$Age_TnT
tau
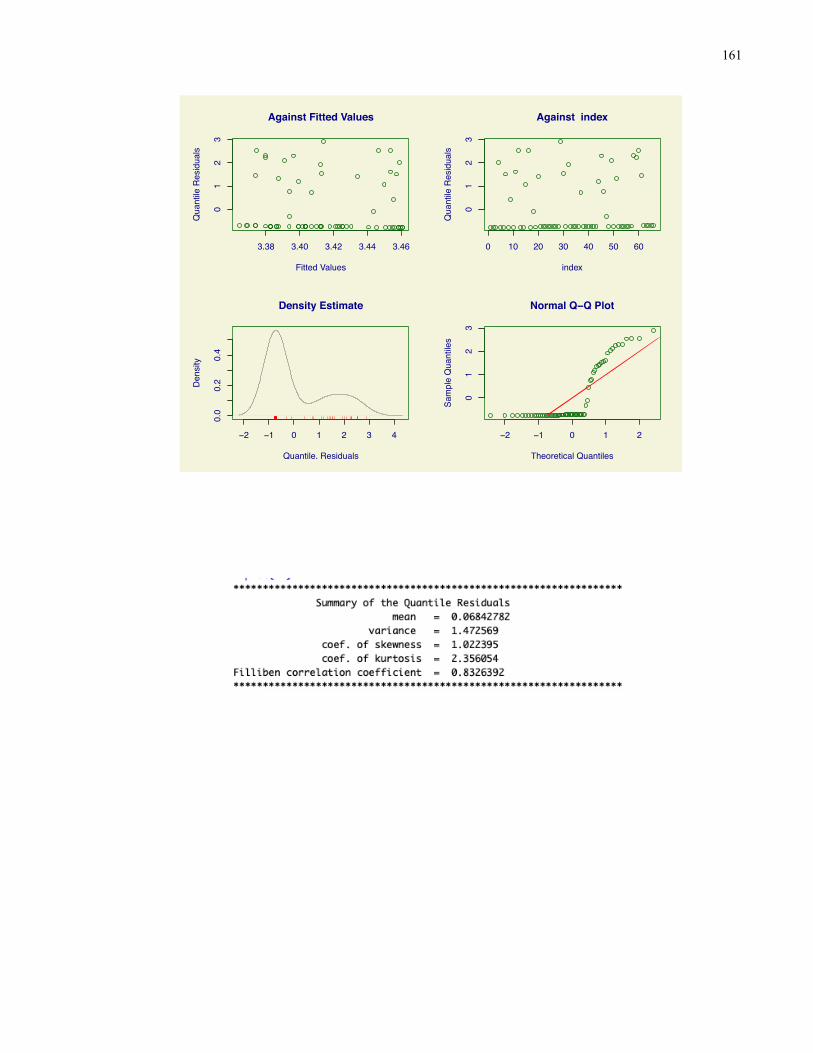
161
3.38 3.40 3.42 3.44 3.46
01
23
Against Fitted Values
Fitted Values
Qua
ntile
Res
idua
ls
0 10 20 30 40 50 60
01
23
Against index
index
Qua
ntile
Res
idua
ls−2 −1 0 1 2 3 4
0.0
0.2
0.4
Density Estimate
Quantile. Residuals
Den
sity
−2 −1 0 1 2
01
23
Normal Q−Q Plot
Theoretical QuantilesSa
mpl
e Q
uant
iles
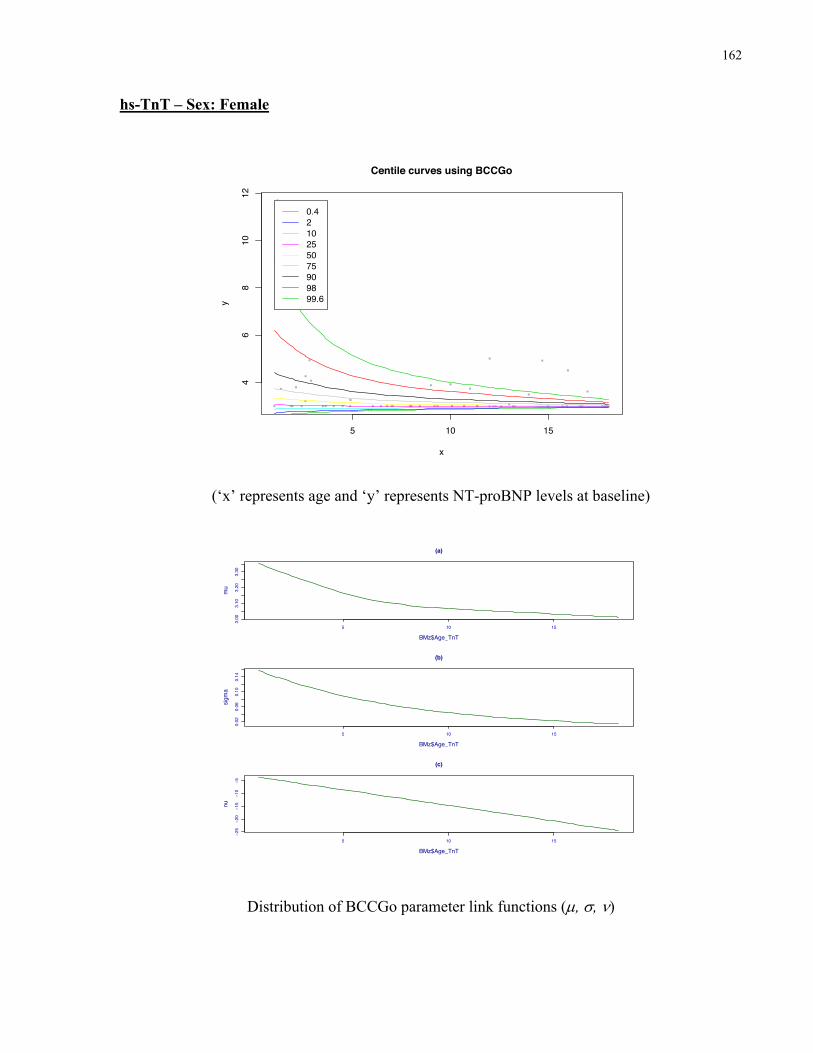
162
hs-TnT – Sex: Female
(‘x’ represents age and ‘y’ represents NT-proBNP levels at baseline)
Distribution of BCCGo parameter link functions (µ, s, n)
5 10 15
46
810
12
x
y
Centile curves using BCCGo
0.4210255075909899.6
5 10 15
3.00
3.10
3.20
3.30
(a)
BMz$Age_TnT
mu
5 10 15
0.02
0.06
0.10
0.14
(b)
BMz$Age_TnT
sigm
a
5 10 15
−25
−20
−15
−10
−5
(c)
BMz$Age_TnT
nu
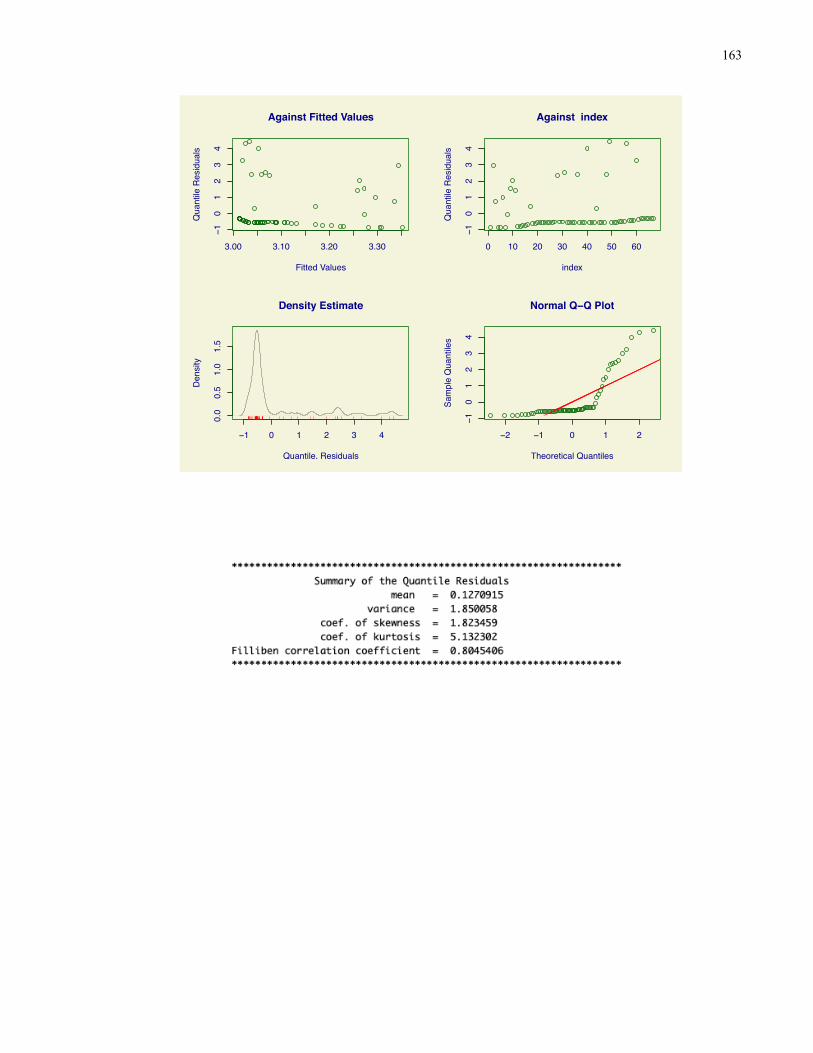
163
3.00 3.10 3.20 3.30
−10
12
34
Against Fitted Values
Fitted Values
Qua
ntile
Res
idua
ls
0 10 20 30 40 50 60
−10
12
34
Against index
index
Qua
ntile
Res
idua
ls−1 0 1 2 3 4
0.0
0.5
1.0
1.5
Density Estimate
Quantile. Residuals
Den
sity
−2 −1 0 1 2
−10
12
34
Normal Q−Q Plot
Theoretical QuantilesSa
mpl
e Q
uant
iles
Related Documents











