-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
1/103
PREPARED BY;DR. SYED FAHAD HAMID
INFLAMMATORY BOWELDISEASE
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
2/103
Major forms
Two major forms;
1) Crohns disease
2) Ulcerative colitis
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
3/103
CROHNS DISEASE
Definition;Crohns disease is a chronic recurrent disease
characterized by patchy transmural
inflammation involving any segment of the
gastrointestinal tract from mouth to the anus.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
4/103
ULCERATIVE COLITIS
Definition;Ulcerative colitis is a chronic, recurrent disease
characterized by diffuse mucosal inflammationinvolving only the colon. It invariably involvesthe rectum and may extend proximally in a
continuous fashion to involve part or all of thecolon.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
5/103
Crohns Disease
Incidence
4 10 per 100 000 per yearPrevalence
27 106 per 100 000
September 2004
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
6/103
Ulcerative Colitis
Incidence6 15 per 100 000 per year
Prevalence
80 150 per 100 000
September 2004
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
7/103
Jews are more prone than other ethnicgroups.
Crohns is slightly more commoner infemales.
Highest incidence and prevalence rates arefrom Northern Europe, UK and NorthAmerica.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
8/103
Aetiopathogenesis
Three major interactive co-factors.
1) Genetic susceptibility
2) The environment (both local
microenvironment and nutritional
environment
3) Host immune response
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
9/103
Familial
Family history is the largest independent
risk factor.
1 in 5 with crohns and 1 in 6 with UC will
have a first degree relative with the
disease.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
10/103
Genetic
Increase concordance for the disease inmonozygotic twins than dizygotic twins.
Susceptibilty loci have been found onchromosome 16(IBD1), 12, 6, 14, 5, 19, 1,16(IBD8) and 3,These have been renamed IBD1-9respectively.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
11/103
Genetic; contd.
Significant loci also found on chromosome13q and in jewish families on 1p and 3q.
Linkage mutations on Card 15(NOD2), theunderlying gene on chromosome 16 (IBD1),and genes underlying IBD5 and IBD3 loci.The Card 15 (NOD2) gene is associated;Crohns disease in whites and stricturingsmall bowel crohns disease.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
12/103
Genetic; contd.
Recent SNP (single nucleotide polymorphism)scans have identified a locus for UC andCrohns disease at ECM1 (extracellular matrix
protein 1).Other risk loci; on IL23R, IL12B, NKX2-3 andMST1.
The autophagy genes ATG16L1 and IRGM,(along with CARD 15) are specific for Crohns disease.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
13/103
Genetic; contd.
HLA genes involved:HLA genes on chromosome 6 also appear tohave a role in modifying the disease.DRB 0103 allele- linked to aggressive courseof Ulcerative colitis and the need for surgery,and with colonic crohns disease.
DRB*0103 and MICA*010- perianal diseaseDRB*0701- ilealCrohns disease
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
14/103
Environmental Factors
Good domestic hygiene has been shown to
be a risk factor for Crohns disease.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
15/103
Life style
Nutritional factors: Higher sugar and fat intake.
Smoking exacerbates Crohns disease.
Smoking improves Ulcerative colitis. Nicotine is
effective treatment of Ulcerative colitis.
Adverse life events and psychological factors
increase relapses in patients with quiescent
disease
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
16/103
Appendicectomy
Is protective for Ulcerative colitis before 20
years of age.
Increases the risk of Crohns disease.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
17/103
Intestinal microflora
IBD is characterized by an overaggressive
immune response to luminal bacterial
antigens and other products in the
genetically susceptible.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
18/103
Intestinal microflora;contd.
Alteration in the bacterial flora :Increase in anaerobic bacteria in Crohns disease and aerobic in UC.
Bacterial antigens :Exert their pro-inflammatory influence byproducing toll like receptor ligands, whichinteract with the normal intestine withsurface toll like receptors (TLRs).The disruption of the surface TLR signallingprevents the mucosa to withstand bacterialinsults.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
19/103
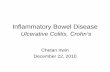
September 2004
Medzhitov, R. et al. N Engl J Med 2000;343:338- 344
Toll-like Receptors
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
20/103
Intestinal microflora;contd.
Intestinal mucosal invasion;The intestinal wall in IBD patientsis contaminated by adherent and invading
bacteria.e.g. there is increased E.coli adherence tothe ileal-epithelial cells in Crohns disease.This occurs via E.colis type 1 pilli to a proteincalled carcinoembryonic antigen related celladhesion molecule 6 (CEACAM 6). The lattermay become a marker for inflammation.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
21/103
Intestinal microflora;contd.
Defective chemical barrier or intestinaldefensins
Evidence suggests a decrease in human alphadefensin-1 (HD-1) in both Crohns disease andUC and lack of induction of HD-2 and HD-3,HD-5 in Crohns disease
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
22/103
Intestinal microflora;contd.
Impaired mucosal barrier function;
It explains the presence of unusual and
potentially pathogenic bacteria, e.g.
Mycobacterium paratuberculosis (MAP),
Listeria and mucosal adherent E.coli.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
23/103
Intestinal microflora;contd.
Butyrate :
Sulphate producing bacteria increase luminal
levels of hydrogen sulphide resulting in
reduction of butyrate oxidation in colonic
mucosa, producing energy deficient state andleading to mucosal inflammation
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
24/103
Pathogenesis
Defective mucosal immune system producingan inappropriate response to luminalantigens such as bacteria .Bacterial ligands interact with toll likereceptors TLRs expressed on epithelialmembranes via co-stimulatory moleculeswhich enable the epithelial cells to act asantigen presenting cells to the myeloiddendritic cells.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
25/103
Pathogenesis; contd..
Then follows the cascade of stimulation of thenaive Th 0 cells to the effector Th 1, Th2, andTh17 which predominate over the regulatory Tcells.Cytokines released from the above cellsstimulate the macrophages to secrete TNF-alpha, IL-1 & IL-6 in large quantitiesMacrophages are also stimulated by
plasmacytoid dendritic cells via natural killer cellswhich themselves can cause direct cytotoxiceffects on cells and secrete inflammatorycytokines.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
26/103
All the above result in leucocytes leaving thecirculation and releasing cytokines(lymphokines, arachidonic acid metabolites,neuropeptides, and free o2 radicals leading totissue damage and also attract moreinflammatory cells like a viscious circle.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
27/103
September 2004
Medzhitov, R. et al. N Engl J Med 2000;343:338- 344
Toll-like Receptors
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
28/103
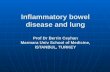
Pathology; Chrons disease
Any part can be affected.
Increase tendency to involve the terminal
ileum and ascending colon.
Can involve single(e.g. terminal ileum) or
multiple areas(skip lesions)
Can involve whole of the colon (total colitis)
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
29/103
Pathology Ulcerative Colitis
Proctitis ( the rectum alone)
left sided colitis (Sigmoid and descending
colon)
Total colitis
backwash ilietis (inflammation of the
terminal ileum )
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
30/103
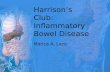
Macroscopic changes; Crohns Disease
Small bowel is thickened and narrowedDeep fissures and ulcers in the mucosa
Cobble stone appearanceColon : fistulae and abscessesInitially the ulcers are aphthoid but laterlarger and deep ulcers appear in patchydistribution.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
31/103
September 2004
Copyright Science Press Internet Services
Aphthae
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
32/103
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
33/103
September 2004
Ileitis
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
34/103
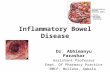
Macroscopic changes;Ulcerative Colitis
Mucosa looks redenned, inflammed andbleeds easily
Severe disease -extensive ulceration and themucosa adjacent to it looks like inflammatorypolypsFulminant disease of either type- loss of mostof the mucosa leaving a few islands ofoedematous mucosa and toxic dilatationoccurs.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
35/103
September 2004
Ulcerative Colitis
Copyright Science Press Internet Services
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
36/103
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
37/103
Microscopy; Crohns disease
Inflammation extends through all three layers
(transmural).
Increase in chronic inflammatory cells and
lymphoid hyperplasia
Non caseating granulomas in 50-60 %
G l
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
38/103
September 2004Copyright Science Press Internet Services
Granuloma
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
39/103
Microscopy; Ulcerative
colitisSuperficial inflammation.
Chronic inflammatory cell infiltrate in the
lamina propria
Crypt abscesses and goblet cell depletion
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
40/103
September 2004
Ulcerative Colitis
Copyright Science Press Internet Services
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
41/103
Differentiation
Sometimes it becomes difficult to diffrentiatebetween the two so in those cases,serological testing might help.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
42/103
Extragastrointestinalmanifestations
Occur in both the diseasesJoint complications are the commonest
The peripheral arthropathies are classified asType 1 (pauci articular) acute self limiting(
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
43/103
EXTRAGASTROINTESTINALMANIFESTATIONS
ULCERATIVE COLITS(Percent cases)
CROHNS DISEASE(Percent cases)
EYESUveitisEpiscleritis,Conjunctivitis
25-8
53-10
JOINTSType 1(pauci-articular)ArthropathyType 2(polyarticular)arthropathyArthralgiaAnkylosing SponylitisInflammatory backpain
4
2.5
513.5
6
4
141.29
SKINErythema nodosum
Pyodermaan renosum
1
1
4
2
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
44/103
Association of HLAs
HLA DRB1*0103 with pauci articular large
joint arthritis in Ulcerative Colitis and Chrons
disease
HLA-B44 Small joint symmetrical arthritis
HLA-B27 with sacroilietis
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
45/103
Differential Diagnosis
All causes of diarrhoea should be excluded
Ileo colonic tuberculosis
Lymphomas
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
46/103
CROHNS DISEASE
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
47/103
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
48/103
Clinical presentation:
15% have no GI symptomsPatients with extensive disease have morefrequent recurrences30 % present with ilietis25 % present as anal and perianal disease
In 20-40 % enteric fistulae form, i.e. bladderor vagina.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
49/103
Clinical presentation:
Acute or insidiousClinical features are variable and depend on the region ofthe bowel affectedThe abdominal pain can be colicky suggesting obstruction.
80 percent present with diarrhoea and in colonicinvolvement, will contain blood.Can present with steatorrea in small bowel diseaseCan present as an emergency mimicking appendicitisCan be complicated by anal and perianal disease in 25%preceding colonic and small intestinal symptoms by manyyears.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
50/103
Examination
Weight loss and general ill healthAphthous ulcers
Tenderness in RIF, although mostlyabdominal examination is normalMass (abscess or matted inflammed bowelloops)Oedematous anal tags, fissures or perianalabscess
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
51/103
Extragastrointestinal featuresSigmoidoscopy : Rectum may appear normal,
but a biopsy must be taken to findnonspecific inflammatory changes. Inextensive colonic disease the rectum may bespared but there still can be patchyinvolvement with an oedematoushemorrhagic mucosa.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
52/103
Investigations
Blood tests Normochromic normocytic anemia of chronic
disease.
Iron or folate deficiency. Megaloblastic anemia due to B-12 deficiency is
unusual despite terminal ileum involvement. Hypoalbuminemia(in severe disease) Blood cultures (if septicemic) Raised ESR, CRP and TLC.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
53/103
Liver biochemistry may be abnormal Serological tests (saccharomyces cerevisiae
antibody) is usually present pANCA is negative
Stools cultures
Should always be performed if diarrhoea ispresent.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
54/103
Radiology and imaging Ba follow through or CT scan with oral
contrast, in every patient with crohns
disease.
Findings -asymmetrical alteration inmucosal pattern with deep ulceration andareas of narrowing and thickening.Terminal ileum is the most common site.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
55/103
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
56/103
Magnetic resonance enteroclysis ( forimaging of the small bowel)
Colonoscopy, if colonic involvement issuspected, except in severe acute disease.
Plain abdominal X-rays, U/S or CT in patientspresenting acutely with colonic symptoms,
High resolution U/S and CT scan are helpful indefining the thickness of the bowel wall andmesnetry as well as intraabdominal and paraintestinal abscesses.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
57/103
Endoanal US and MRI for perianal disease
Radionuclide scans with gallium labelled
polymorphs or indium or technetium
labelled leucocytes, to identify small
intestinal and colonic disease and to localiseextraintestinal abscesses
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
58/103
Disease activity
Assessed by using simple parameters such asHb, white cell count .Inflammatory markers (ESR, CRP, and platletcount) and serum albumin.Calprotectin is a calcium binding protein andaccounts for 60 % of cytosolic protein ofneutrophils.
Faecal calprotectin is cheap noninvasive markerof disease activity in IBD and may be of help inpredicting response to and failure of treatment.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
59/103
Medical management
AimInducing remission
Maintaining remission
M f ild
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
60/103
Management of mild symptoms
Mild symptoms- symptomatic treatment
Stop smokingDiarrhoea : anti diarrhoeals ( loperamide, codeinphosphate or co-phenotropeCholestyramine if diarrhoea is due to bile acid
malabsorptionAnemia depending on the cause should be treatedAnemia of chronic disease will improve as thedisease improves (erythropoetin can be used)Active (moderate to severe) disease may requirehospital admissionModerate to severe chrons colitis are treated as forUC
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
61/103
Remission induction
Glucocorticoids oral or IV (30-60 mg/day)Slow realease formulations such asbudesonide in ileocaecal diseaseIt has a high topical activity and is rapidlyeliminated by the liver so less suppression ofthe cortisol and least adverse effectsRemission response rates vary(60-90 %)depending upon the site and extent of thedisease.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
62/103
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
63/103
Unresponsive patients - raise the dose ofazathioprine to levels that make patientsleucopenic.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
64/103
Remission maintenance
Flareups occur on tapering steroids orstopping enteral diets. They can be treated bytemporarily increasing steroid doses for
inducing remission.Aminosalicylates for treating remission incrohns colitis.Immunosuppressives (azathioprine,6mercaptopurine, methotrexate andmycophenolate mofetil) are used in all otherpatients for maintaining remission.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
65/103
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
66/103
Biological agents
Failure to induce or maintain remission,biological agents can be used.Infliximab a chimeric anti TNF-alphamonoclonal antibody Is the most widely used biological agent.Most successful at inducing remission incortocosteroid/immunosuppressive resistantpatients and also maintaining it.Efficacy is reduced due to formation ofantibodies
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
67/103
Two other TNF-alpha antibodies are nowwidely used.Adalimumab fully human anti-TNFmonoclonal antibodiesUsed in patients who fail to respond toinfliximab as well as those who have notreceived it.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
68/103
Certolizumab pegol is a pegylated Fab fragment of humanized anti-TNF-alphamonoclonal antibody.Short-term and longer-term efficacy hasbeen demonstrated.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
69/103
Other new anti-TNF antibody therapie sinclude CDP571, etanercept and onercept.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
70/103
Surgical management
Approximately 80% require an operation atsome time in their life during the course of theirdisease
Nevertheless surgery should be avoided ifpossible and only minimal resection should beundertaken as recurrence(15%) is almostinevitable.
Chances of recurrences can be reduced inpatients undergoing their second surgery bytreating them with Azathiprine and 6-Mercaptopurine.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
71/103
Indication for surgeryFailure of medical therapy, with acute orchronic symptoms producing ill health.Complications (e.g. toxic dilatation,obstruction, perforation, abscesses andenterocutaneous fistula)Failure to grow in children despite medicaltreatment
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
72/103
Surgical approachStricturoplasty(some strictures)Resection and end to end anastamosis(others)Subtotal colectomy and ileorectal anastamosiswhen entire colon is involved and rectum isspared.
Panproctocolectomy with an ileostomy is thestandard procedure for whole colonic and rectalinvolvement.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
73/103
ULCERATIVE COLITIS
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
74/103
Ulcerative colitis
Clinical featuresMajor symptoms (diarrhoea with blood andmucous)General features include malaise, lethargy,anorexia and weight lossAphthous ulceration in mouth
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
75/103
Can be classified as mild moderate andsevereRuns a course of remissions andexacerbations10% have persistent chronic symptomsOthers have only a single attackIn proctitis urgency, tenesmus, are common
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
76/103
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
77/103
Toxic megacolon is a serious complication.On plain abdominal a dilated thin walledcolon with a diameter of >6cm will be seen.Serious complication and may result inperforation and high mortality(15-25%).Urgent surgery is required in all patients inwhom toxic dilatation has not resolved within48 hours.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
78/103
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
79/103
Severe attack; contd
Management
Admitt to hospital
Assess IV fluids
Monitor daily:Stool frequecyAbdominal X rayFBC, CRPalbumin
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
80/103
Examination
Generally no specific signsSlight distention and tenderness on palpation
Rectal examination: blood will be seenRigid sigmoidoscopic examination:inflammed bleeding and friable mucosa. canbe normal in cases of rectal sparing.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
81/103
Investigations
Blood testsIron deficiency anemia
White cells and platlet counts are raisedESR and CRP are raisedLiver biochemistry may be abnormal
Hypoalbuminemia occurs in severe diseasepANCA may be positive
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
82/103
Stool cultures
Should always be performed to excludeinfective causes of colitis
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
83/103
ImagingPlain abdominal xrays with an abdominalultrasound : key investigations in moderateto severe attacksThe extent of the disease can be assessed bythe degree of air distribution in the colon.Thickening of the colonic wall can bedetected on ultrasound as can the degree ofhyperemia in the colonic wall.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
84/103
Radionuclide scansUsed to assess colonic inflammation
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
85/103
ColonoscopyShould not be performed in acute attacksbecause of the risk of perforation.Can be performed in long standing chronicdiseases in defining the extent and activity ofthe disease and excluding the onset ofdysplasia and carcinoma in patients withlongstanding disease of 10 years duration ormore
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
86/103
Medical management
All patients should be treated with anaminosalicylate.The active moiety is 5-aminosalicylic acid(5-ASA).The 5-ASA is absorbed in the small intestine (andmay be nephrotoxic) so the design of variousaminosalicylate preparation is based on the bindingof 5-ASA by an azo bond tosulphapyridine(sulphasalizine), 4 amino benzyl betaalanine(balsalazide), or to 5-ASA itself(olsalazine),coating with a PH sensitive polymer(Asacol), orpackaging of 5-ASA in microspheres(pentasa)
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
87/103
Proctitis : Oral amino salicylates +local rectal steroidpreparation are the first line treatement .Mesalazine enemas and budesonide enemascan be tried.Resistant cases: oral cortiocosteroids alone orcombination with azathioprine can be tried
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
88/103
Left sided proctocolitis:Oral aminosalicylates + local rectal steroidpreparationModerate to severe attacks: oralprednisolone.Unresponsive patient: to be admitted to thehospital
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
89/103
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
90/103
Monitor clinical status (fever, tachycardia,abdominal signs). Daily FBC, ESR, CRP, electrolytes, urea,
LFTS, X-ray erect abdomen and stool weight.Persistent fever, tachycardia, falling Hb, risingTLC, falling potassium, falling Albumin, andpersistently raised stool weight(>500gm/day)with loose blood stained stool shows nonresponsiveness and is an indication forsurgery.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
91/103
Rescue therapy to avoid colectomy: (forpatients with poor prognostic signs and a CRPmore than 45mg/L after 3 days of IV
hydrocortisone)Hydrocortisone + IV cyclosporin 2mg/kg/dayor TNF- alpha antibody therapyOther agents: visilizumab andleucocytapheresis(selective removal of whitecells from blood and reinfusion of RBCs andleucocyte poor plasma)
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
92/103
Patients responding to i.v. hydrocortisonetreatement, oral prednisolone therapy shouldbe substituted and doses should be tailedoff(5-10mg/weekly)Maintenace of remission is withaminosalicylates.
In patients in whom it is not possible toreduce the dose without a flareup,azathioprine is used.
S i l M
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
93/103
Surgical ManagementTreatment of Ulcerative colitis is mainlymedical, but surgery has a very central role aswell.Indications for surgery in Ulcerative colitis
areFulminant acute attack:Failure of medical treatment (3 days)
Toxic dilatationHaemorrhageperforation
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
94/103
Chronic diseaseIncomplete response to medical treatment
Excessive steroid requirementNon-compliance with medicationRisk of cancer
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
95/103
Surgical approachSubtotal colectomy with end ileostomy andpreservation of the rectum is the operation ofchoice in acute diseaseLater a number of options can be tried. Theseinclude, proctectomy with a permanent
ileostomy orIleorectal anastomosis if a permanentileostomy is to be avoided
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
96/103
Annual biopsies of the rectal mucosa must becarried out to detect dysplasia.With ileoanal anastomosis, a pouch of theileum is formed that acts as a reservoir.A third patients will experience pouchitiswhich is characterized by the pouch mucosa
with clinical symptoms of diarrhoea,bleeding, fever and at times exacerbationwith extracolonic manifestations
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
97/103
Pouchitis is twice as high in primarysclerosing cholangitis.Two thirds will recur as acute relapsing orchronic unremitting forms.Treatment is not always satisfactory andincludes topical and oral 5-ASA,
corticosteroids, metronidazole andciprofloxacin.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
98/103
Probiotics (four strains of lactobacillus,three strains of bifidobacterium, and one ofstreptococcus) have been shown to prevent
the onset of pouchitis and to maintainremission. Short chain fatty acid enemas andalicaforsen( a selective inhibitor ofintercellular adhesion molecule 1, ICAM-1,expression) enemas have shown promise inpouchitis treatment.
C d P g i
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
99/103
Course and Prognosis
Third of the patients with distal inflammatoryproctitis due to Ulcerative colitis will developemore proximal disease, with 5-10%developing total colitis.A third will have a single attackOthers will have relapsing course
A third will undergo colectomy within 20years of diagnosis
C d IBD
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
100/103
Cancer and IBD
There is an increased riskScreening strategiesScreening colonoscopy with multiple biopsiesshould be done every 2 years in patients with
total UC andcrohns
colitis of 10 years and everyyear after 20 yearsLeft sided UC and those with less than totalcrohns colitis should have a screeningcolonoscopy at 15 years and therafter biannuallyPatients with Ulcerative colitis and primarysclerosing cholangitis are particularly at risk ofdeveloping colon cancer and should have yearlyscreening
Pregnancy and Inflammatory
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
101/103
bowel disease
Women with inactive IBD have normalfertilityFertility however may be decreased in activediseaseSpotaneous abortions are twice as likely inthose with active disease than those with
inactive disease.Relapse rates in pregnancy are similar tothose of non pregnant patients.
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
102/103
Flareups in the first trimester enhances therisk of flareups in puerperial period.There is no risk of flareup in pregnancy forboth Crohns disease and ulcerative colitisRelapse if it does occur is however more likelyin the first trimester.
Amino salicylates, steroids, and azathiprineare safe at the time of conception and duringpregnancy
-
8/13/2019 Inflammatory Bowel Disease Ward Ppt
103/103
THANKYOU FOR YOUR PATIENCE