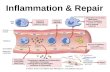
1 INFLAMMATION

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
INFLAMMATION

Topic OutcomesAt the end of this lecture, students are able to :1.Describe orally the signs of inflammation2.Describe and differentiate in written between
acute and chronic inflammation3.Explain the morphological of types of
inflammation4.Describe in written the mechanism of healing
and repairing

CONTENTS
2.1: Definitions & Concepts Of Inflammation
2.2: Stages Of Inflammation
2.3: Mediators Of Inflammation
2.4: Morphologic Pattern Of Acute & Chronic
Inflammation
2.5: Repair Or Healing
3

2.1: Definitions & Concepts Of Inflammation
• The local response of living mammalian tissues to injury due to any agent.
• Body defense reaction in order to eliminate or limit the spread of injurious agent as well as to remove the consequent necrosed cells and tissues.
4

• Causes of inflammation;
i. Physical agent e.g. mechanical trauma, radiation etc.
ii. Chemical agent e.g. simple chemical poisons, organic poisons
iii. Infective agents e.g. bacteria, viruses, parasites, their toxins
iv. Immunological agents e.g. Ag-Ab reaction, cell mediated
5

• Involves 2 basic processes (overlapping):
• Have protective role against injurious agents
• Cause considerable harm to the bodyeg; anaphylaxis, atherosclerosis etc
6
Inflammatory response
healing

Signs of Inflammation
• The famous 4 cardinal signs of inflammation:(i) rubor (redness)(ii) tumor (swelling)(iii) calor (heat)(iv) dolor (pain)
Added latest – functio laesa (loss of function)
7

Heat Redness Swelling Pain Loss Of Func.
8

2.2: Stages Of Inflammation
INFLAMMATION
ACUTE INFLAMMATION
CHRONIC INFLAMMATION
9

• Acute inflammation– Short duration & represents the early body
reaction and usually followed by repair– The main features :
(a) Accumulation of fluid & plasma at the affected site
(b) Intravascular activation of platelets(c) Polymorphonuclear neutrophils as
inflammatory cells
10

• Chronic Inflammation- longer duration and occurs either :
(a) after the causative agent of acuteinflammation persists for a long
time(b) Stimulus that induces chronic
inflammation from the beginning- main features :
presence of chronic inflammatory cells (lymphocytes, plasma cells and
macrophages)

I) ACUTE INFLAMMATION
• The changes can be conveniently described under:(i) Vascular events(ii) Cellular events
13
Infected toenail showing the characteristic redness and swelling associated with acute inflammation

(i) VASCULAR EVENTS• Alteration in the microvasculature (arterioles,
capillaries & venules)• Earliest response to tissue injury• Alterations includes:
(a) haemodynamic changes(b) changes in vascular permeability
14

(a) Haemodynamic Changes
• Earliest features of inflammatory response result from changes in the vascular flow and calibre of small blood vessels in the injured tissue
15

The sequence of these changes:
16
Transient vasoconstriction
Persistent progressive vasodilatation
Local hydrostatic pressure
Slowing or stasis
Leucocytic margination

• Lewis Triple Response/ red line response;
(Eg: form stroking with a blunt point)
i. Red line : Appears a few second; Capillary & venules
dilatation
ii. Flare : Bright reddish appearance/flush
surrounding the red line; Anteriolar dilation
iii. Wheal : Swelling or oedema of the surrounding skin
occurring due to transudation of fluid into the extravascular space
17

18
Triple response

(b) Altered vascular permeability• Vascular changes begin quickly after the
injury but may develop at variables rates, depending on the nature & severity of the original injury.
• The interchange of fluid between the vascular & extra vascular space results from balance of fluid into the vascular space or out into the tissues;
i. Hydrostatic pressure
ii. Oncotic pressure - protein
iii. Osmotic pressure
iv. Lymph flow
19

Fluid interchange between blood and extracellular fluid (ECF). (HP = Hydrostatic
pressure, OP = Osmotic pressure)
20
NO OEDEMA OEDEMA

Edema
21

• MECHANISMS OF INCREASED VASCULAR PERMEABILITY
(i) Endothelial cell contraction(ii) Endothelial cell retraction(iii) Direct injury to endothelial cells(iv) Endothelial injury mediated by leucocytes(v) Neovascularisation
23

a) Contraction of endothelial cells
• Microvasculature : venules• Response type :
Immediate transient (15-30 min)• Pathogenesis :
Histamine, bradykinin, other chemical mediators
• Examples : Mild thermal injury
24

b) Retraction of endothelial cells
• Microvasculature : venules• Response type :
somewhat delayed (in 4 – 6 hrs)prolonged (for 24 hrs or more)
• Pathogenesis :Interleukin-1(IL-1)Tumor Necrosis Factor (TNF)
• Examples : In vitro experimental work only25

c) Direct injury to endothelial cells• Microvasculature : Arteriols, venules,
capillaries• Response type :
Immediate sustained leakage (immediate after injury prolonged (hrs to days)Delayed sustained leakage (delayed (2-12hrs) prolonged (hrs-days))
26

• Pathogenesis :cell necrosis and detachment
• Examples : Moderate to severe burns, severe bacterial infection, radiation injury
27

d) Endothelial injury mediated by leucocytes
• Microvasculature : venules, capillaries• Response type :
delayed, prolonged• Pathogenesis :
Leucocyte activation• Examples : pulmonary venules and capillaries
28

e) Neovascularisation
• Microvasculature : All levels• Response type :
Any type• Pathogenesis :
Angiogenesis, vascular endothelial growth factor (VEGF)
• Examples : Healing, tumors
29

ii) CELLULAR EVENTS • Cellular events; cells of the acute
inflammatory response are the neutrophils, monocytes & macrophages.
Polymorphonuclear neutrophils (PMNs)(within 24 hrs; Life long 24-48 hrs)
MonocytesMacrophages
(24-48 hrs; Survive much longer)30

• The movements of neutrophils out of the vessels & their role in combat can be divided into 5 steps;
i. Margination = ?
ii. Adhesion = ?
iii. Emigration/ diapedesis=?
iv. Chemotaxis = ?
v. Phagocytosis & degranulation=?
31

• Concentrates the leucocytes adjacent to endothelial wall- Margination
• Adherence of inflammatory cell to the endothelium/ vascular basement membrane- Adhesion
• Neutrophil lodged between endothelial cell and basement membrane and escape out into the extravascular space- Diapedesis
• Chemotactic factor mediated transmigration of leucocytes to reach the interstitial tissue- Chemotaxis
• The process of engulfment of solid particulate material bt the cell (cell eating)- Phagocytosis 32

THE INFLAMMATION PROCESS
33

34

Neutrophil Margination
35

FATE OF ACUTE INFLAMMATION• Acute inflammation generally has one of
FOUR (4) outcomes;
i. Resolution – complete return to normal/ tissue changes are slight and cellular changes are reversible eg; resolution in lobar pneumonia
ii. Healing by scarrimg– tissue destruction is extensive, no tissue regeneration; healing by fibrosis
36

iii) Suppuration – the progression process of severe necrosis cause by pyogenic bacteria; neutrophilic infiltration; form an abcess; abcess – organised by dense fibrous tissue and get calcified
iv) Progression to chronic inflammation may follow acute inflammation, although signs of chronic inflammation may be present atthe onset of injury; healing proceed side by side.
37

An abscess on the skin, showing the redness and swelling characteristic of inflammation. Black rings of necrotic tissue surround central areas of pus
38

II) CHRONIC INFLAMMATION
• Chronic inflammation; prolonged process in which tissue destruction and inflammation occur at the same time.
39

• Caused one of the following 3 ways:i) Chronic inflammation following acute inflammation – the tissue destruction is extensive, or bacteria survive & persist in small numbers at the site of acute inflammation ii) Recurrent attacks of acute inflammation – repeated bouts of acute inflammation eg; repeated acute infection of gallbladder chronic cholecystitisiii) Starting de novo – infection with organisms of low pathogenecity (chronic from the beginning)
40

• General features of Chronic inflammation:
i. Infiltration with mononuclear cells
Infiltrated by mononuclear inflammatory cells : phagocytes & lymphoid cells
phagocytes : circulating monocytes, tissue macrophages, epithelioid cells,
multinucleated giants cells
ii. Tissue destruction
Central feature of lesions
iii. Proliferative changes
Result of necrosis, proliferation of small vessels and fibroblasts; healing by fibrosis and collagen 41

Systemic effects of chronic inflammation
Associated with following systemic features:1. Fever – mild fever, loss of weight and
weakness2. Anemia – varying degree of anemia3. Leucocytosis - general 4. ESR – elevated in all cases5. Amyloidosis – long term cases of chronic
suppurative inflammation (secondary systemic (AA) amyloidosis
42

Types of chronic inflammation
NON-SPECIFIC• Formation of granulation
tissue and healing by fibrosis
• Eg; Chronic osteomyelitis, Chronic ulcer
SPECIFIC• Injurious agent causes a
characteristic histologic tissue response
• Eg; tuberculosis, leprosy, syphilis
43

Types of chronic inflammation (based on histological classification)
CHRONIC NON-SPECIFIC INFLAMMATION
• Characterised by:(a) non-specific inflammatory cell infiltration eg; chronic osteomyelitis, lung abcess(b) Infiltration by polymorphs and abcess formation Eg; Actinomycosis
CHRONIC GRANULOMATOUS INFLAMMATION
• Formation of granulomas• Eg; tuberculosis, leprosy,
syphilis, sarcoidosis
44

Granulomatous Inflammation
• Granulomatous inflammation; mechanism whereby the body deals with certain “indigestible” bacteria, fungi, or foreign particles.
• Examples;
i. Bacteria e.g. Tuberculosis, Leprosy
ii. Parasitic e.g. Schistosomiasis
iii. Fungal e.g. Blastomycosis, Histoplasma capsulatum
iv. Inorganic metals or dusts e.g. Silicosis
v. Foreign body e.g. Vascular graft
vi. Unknown e.g. Sarcoidosis
45

46
INJURY(e.g; by M. tuberculosis,
talc
Failure to digest agent
Weak acute inflammatory response
Persistence of injurious agent
T cell-mediated immune response
Poorly digestible agent
• Activation of CD+4 T cells (release of lymphokines IL-1, IL-2. growth
factors IFN-ˠ and IFN-ɑ)
• Monocyte chemotactic factor

47
Accumulation of tissue macrophages (Increased recruitment from circulation, local
proliferation)
Macrophages activated by IFN-ˠ
Transformed to epithelioid cells, giant cells
GRANULOMA

Granuloma tissue
48

• Examples of disorders associated with inflammation include;
i. Asthma
ii. Autoimmune diseases
iii. Hypersensitivities
iv. Pelvic inflammatory disease
v. Rheumatoid arthritis
vi. Transplant rejection
49

2.3: Mediators Of Inflammation• What are mediators?
i. May be circulating in the plasma or may be produced
locally by cells at the site of inflammation.
ii. Induce their effects by binding to specific reactors on
target cells.
iii. May stimulate target cells to release secondary effector
molecules.
iv. May act on only one or a very few targets.
v. Function is generally tightly regulated.
50

• 2 types of chemical mediators of Acute inflammation;
i. Plasma-derived mediators e.g. kinin system,
coagulation & fibrinolytic system, complement
system.
ii. Cell-derived mediators e.g. vasoactive amines,
cytokines, platelet activating factor, growth factor.
51

• Chronic inflammatory cells & mediators;
i. Macrophages
ii. T & B-lymphocytes
iii. Eosinophils
iv. Mast cells
52

• Inflammatory cells release mediators such as;
i. Cytokines-
(IL-8, interferon-neutrophil)
ii. Vasoactive amines-
(histamine, serotinin- mast cell, basophil, platelet)
iii. Prostanoids-
(arachidonic acid metabolics)
iv. Reactive oxygen intermediates-
(released from activated neutrophil) 53

• If the mediators in the inflammatory response are successful;
i. Invading & infectious agents will be removed.
ii. Damaged tissues will be disposed of.
iii. New tissue will be induced to form.
iv. New blood supply to the area will be established.
54

Chronic inflammation cells
55

Chronic Inflammation – Lung Abscess56

2.4: Morphologic Patterns Of Acute & Chronic Inflammation
• Serous inflammation; excessive clear watery fluid with a variable protein content but no fibrin e.g. pleural effusion associated with tuberculosis.
57

Serous Inflammation - effusion58

Serous Inflammation - effusion59

• Fibrinous inflammation; the formation of fibrin is striking e.g. in acute pleurisy.
60

Fibrinous Inflammation61

• Purulent (Suppurative) inflammation; production of pus is the main characteristic e.g. abscess & acute apendicitis.
62

Purulent Inflammation - PUS
63

Purulent Inflammation - PUS64

• Ulceration; complication of many disease process
• Divided into 2 groups;
i. Simple ulcer
ii. Malignant (cancerous) ulcer
65

A skin ulcer resulting from infection with Corynebacterium diphtheriae
66

Mouth Apthus Ulcer
67

Gastric Ulcer
68

2.5: Repair Or Healing
• The processes that take place during & after the injury are;
i. Removal of dead & foreign material.
ii. Regeneration of injured tissue from cells
of the same type.
iii. Replacement of damage tissue by new
connective tissue.69

• Cells can be divided into 3 major groups;
i. Labile (continuous dividing) e.g. epithelial & blood cells.
ii. Stable (low level of replication; decrease or lose their ability to proliferate after adolescence) e.g. fibroblast, smooth muscle cells, bone & cartilage cells
iii. Permanent (never divide) e.g. nerve cells, cardiac myocytes.
70

HEALING
• 2 processes:(i) Granulation tissue formation(ii) Contraction of wounds
71

(i) Granulation tissue formation
• 3 phases :(a) PHASE OF INFLAMMATION
trauma, blood clots (site of injury)acute response :exudation of plasma,
neutrophils, monocytes (24 hours)
72

(b) PHASE OF CLEARANCE- proteolytic enzymes from neutrophils- Autolytic enzymes from dead tissue
cells- Phagocytic activity : macrophages(function : clear of the necrotic tissue,
debris & RBCs)
73

(c) PHASE OF INGROWTH OF GRANULATION2 main processes:i. Angiogenesis (neovascularisation) formation of new blood vesselsii. Fibrogenesis formation of fibrocytes and mitotic
division by fibroblasts; myofibroblasts In 6th days, more collagen is formed
74

ii) Contraction of wounds
• Start after 2 -3 days; completed: 14th day• Wound reduced 80% of its original size• Contraction occur: rapid healing process• Factors under mechanism of wound
contraction: (a) dehydration(b) contraction of collagen(c) myofibroblasts
75

WOUND HEALING
1. Healing by first intention (Primary union)characteristics:- clean & uninfected- surgical incised- without much loss of cells & tissue- edges of wound – surgical sutures
76

2. Healing by second intention (Secondary union)Characteristics:- Large tissue defect- extensive loss of cells & tissues- not approximated by surgical sutures but left open
77

• 5 stages of healing (primary Union);
i. Initial Haemorrhage
ii. Acute Inflammation response
iii. Epithelial changes
iv. Organization
v. Suture tracks
78

• 6 stages of healing (secondary Union);
i. Initial Hemorrhage
ii. Inflammation phase
iii. Epithelial changes
iv. Granulation tissue
v. Wound contraction
vi. Presence of infection79

• Repair; regeneration of injured tissue by parenchymal cells of the same type.
• Replacement by connective tissue occur when repair by parenchymal regeneration alone cannot be accomplished.
• Involves production of Granulation tissue.
• Replacement of parenchymal cells with proliferating fibroblasts & vascular endothelial cells.
80

Scars present on the skin, evidence of fibrosis & healing of a wound
81

Granulation tissue
82

Healing Skin wound
83

Healing - Skin scar84

• Factors affecting healing;
i. Systemic e.g. age, nutrition, immune
status.
ii. Local e.g. infection, blood supply,
mobility, foreign body.
85

"Each time you are honest and conduct yourself with honesty, a
success force will drive you toward greater success. Each time you lie, even with a little
white lie, there are strong forces pushing you toward failure."
86

THANK YOU
FOR YOUR ATTENTION
87
Related Documents