Infective Endocarditis

Infective Endocarditis. Is due to microbial infection of a heart valve, the lining of cardiac chamber or blood vessel, or a congenital anomaly (septal.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Infective Endocarditis
• Is due to microbial infection of a heart valve, the lining of cardiac chamber or blood vessel, or a congenital anomaly (septal defect).
• The causative agent is usually abacterium, but may be any organisms.
Pathophysiology
• Typically occurs at site of pre-existing endocardial damage.
• But virulence organism like staph.aureus can affect normal valve.
• Tricusped valve endocarditis in i.v. drug abuser.• Defect associated with high jet like PDA and VSD >
liable while defect with low jet less likely as in ASD.• Vegetation (organism,fibrin & platelete).• Extracardiac manifestations such as vasculitis & skin
lesion are due to emboli or immune complex deposition.Mycotic aneurysm may develop in arteries at sites of emboli .
Microbiology
• *Streptococci ;• Viridans gr. 30-40 %.• Entrococci 10-15 %.• Other streptococci 20-25 %.• *Staph. :• Staph.aureus 9-27 %• Coagulase –negative 1-3 %• *Gram –ve, Haemophilus & Anaeroes 3-8 %.• *Rickettsiae & fungi < 2 %.
Clinical features • Could be divided in to Acute and subacute with overlap between
them .• The clinical pattern influenced by the type of organism, the site of
infection and prior antibiotic therapy .• Sub acuteBacterial Endocarditis : persistent fever, un usual
tiredness, night sweating or weight loss ,or new signs of valve dysfunction or heart failure.Less often embolic phenomenon.
• Osler nodes a painfull tender nodes at finger tips probably due to vasculitis (rare).
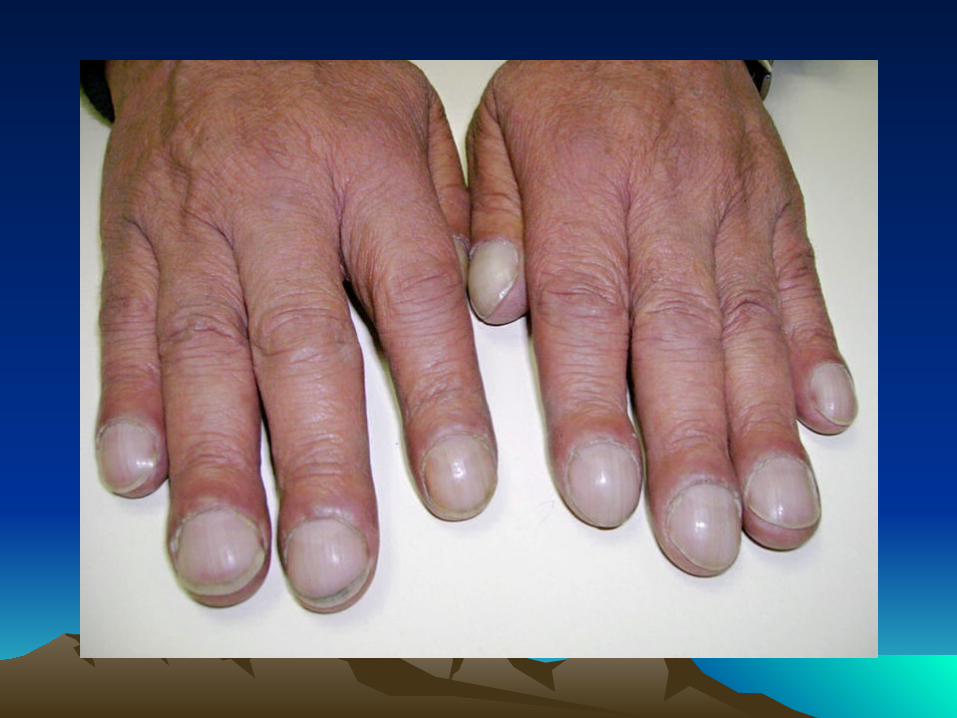
• Digital clubbing is a late sign .• The spleen frequently palpable .In Qoxiella infection the spleen and
liver may be considerably enlarged..Microscopic haematuria is common.

• Acute endocarditis : sever febrile illness, with prominent and changing murmur and petichiae . Embolic phenomenon is common , and cardiac and renal failure may develop rapidly. Abscesses may be detected on echocardiography.clinical features of chronic endocarditis usually abscent.
Post operative endocarditis : any un explained fever in a patient who has had heart valve surgery should be investigated for possible endocarditis.
The infection usually affect valve ring & may resemble sub acute or acute endocarditis, depending on virulence of the organism. Morbidity and mortality is high and redo
surgery usually required .
Investigations :• Blood culture :3 samples for culture should be obtained on aseptic
technique on different sites, aerobic and anaerobic culture are required . • Echocardiography :Is the key tool for detecting vegetations and following its
progress, as small as 3-5 mm can be detected on TTE and as smaller as 1-1.5 mm on TEE. the later specially important in identifying abscess formation and endocarditis of the prosthetic valve.
• Elevation of ESR and a normochromic ,normocytic anaemia ,with leuckocytosis are common.
• Measurement of CRP(C-reactive Protein ) is more reliable for monitoring the treatment than ESR.
• Proteinurea & microscpic haematuria may occur and usually is the only positive finding.
• ECG is important t for monitoring the development of conduction defect and aortic root abscess by showing P-R prolongation.
• Chest X-ray show evidence of cardiac failure and cardiomegaly.
Management
• Mortality rate is about 20 % and may be higher in special cases (prosthetic valve endocarditis and resistant microorganism).
• A 2 week treatment regimen may be sufficient for fully sensitive strains of Streptococcal viridans and Strep.bovis.
• For empirical treatment of bacterial endocarditis ,Penicillin plus gentamicin is the treatment of choice for most of the cases.
• However when staphylococcal infection is suspected vancomycin plus gentamicine is recommended.
• Cardiac surgery (debridement of infected material & valve replacement) is advisable for the following conditions ;
• 1-Heart failure due to valve damage.• 2-failure of antibiotic therapy.• 3-Large vegetation on left sided valve.• 4-Abscess formation.• 5-prosthetic valve endocarditis.• 6-Fungal endocarditis.
Related Documents