39' INFECTION IN THE -NEWBORN INFANT By J. L. HENDERSON, M.D., F.R.C.P.E. Senior Lecturer, Department of Child Life and Health, Edinburgh University This article is a review of the immunological peculiarities of the newborn infant and the in- cidence, clinical features, treatment, epidemiology and prophylaxis of neonatal infections. Infective disorders are very common in the first month of life and are the principal cause of mor- bidity and mortality after the first few days. In the first few days after birth obstetrical factors are the chief cause of morbidity and mortality, and infections are uncommon since there has not been time for most of them to cause illness. Infective disorders are more amenable to preventive measures than any other cause of morbidity in the neonatal period,' and the efforts being made to reduce their incidence are yielding very encourag- ing results, particularly in maternity hospitals and infants' institutions where the risk of contracting infections is so much greater than in the home. Since the unduly high neonatal mortality rate can most easily be reduced by measures which will curtail the incidence of infections in the newborn, a better and more general understanding of the epidemiology and clinical features of such infec- tions is of prime importance. Immunological Considerations It was for long believed that the newborn infant has an enhanced resistance to infection. This is a fallacious and dangerous doctrine. The con- ception probably arose from the fact that the exanthematous infections are uncommon in the first few months of life. The tissues of the newborn infant, immature and unaccustomed to infection, react to contact with bacteria in a different manner from those of older age groups. There is a lack of specific active immunity and local tissue response is poor. These handicaps are, however, compensated for in the early weeks by inheritance from the mother of specific passive immunity to numerous organisms and the occurrence of a defensive physiological leucocvtosis. In mammals such as man, with a haemochorial placenta, providing a thin placental barrier, gamma globulin, which carries the antibodies, passes across the placenta from the maternal to the foetal circulation. Most antibodies have the same titre in both individuals and others a lower titre in the' foetal than in the maternal blood. Specific coliform antibodies have a much lower titre in the foetal than in the maternal blood anac, con- sequently, are absent unless the mother's titre is fairly high. Only about one-third of pregnant women possess pertussis antibodies. The lack of these two forms of specific passive immunity in the majority of the newborn accounts for the prevalence of coliform infections and whooping cough in young infants. In mammals with- a thick placental barrier, and such constitute the majority of species, virtually no antibody-carrying gamma globulin passes across the placenta to the foetal circulation. It is a natural corollary to these anatomical and physiological facts that the colost- rum in the anthropoids and other mammals with a thin placental barrier which permits the passage of antibodies, should have a minimal antibody content, and the colostrum of mammals with a thick placental barrier, not permitting the passage *of antibodies, an abundant supply of antibodies. Nature thus ensures, by one means or the other, that all newborn mammals shall have some humoral antibody protection against bacteria to which they had not previously been exposed, and to which they would otherwise be easy prey. It must be emphasized that the antibodies which the human foetus or newborn animal acquires from the mother confer a passive and therefore a short-lived immunity persisting for only a matter of weeks or, at most, a few months. It should also be reiterated that some antibodies are transmitted only to a small extent, if at all, and consequently afford no worthwhile protection. Active immunity to the common organisms with which the infant- comes in contact after birth is gradually acquired and immunity to the various epidemic diseases is acquired as a result of clinical or sub-clinical infection at'any time. The develop- ment of active immunity is a slow process at any age, but much more so in the first six months- of life at which period the immature reiiculo- endothelial system responds poorly to. antigenic stimulation, and produces a low level of lmoral antibodies. This poor response td jan`igenic stimulation can be compensated for to consider- able extent when inducing immunity-in the early months by increasing the strength of the antigenic stimulus. For instance, a satisfactory antibody response can be obtained in the first few 'months of life by giving larger immunizing doses of vaccine than are necessary at a later age.- copyright. on March 21, 2022 by guest. Protected by http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.24.274.391 on 1 August 1948. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

39'
INFECTION IN THE -NEWBORN INFANTBy J. L. HENDERSON, M.D., F.R.C.P.E.
Senior Lecturer, Department of Child Life and Health, Edinburgh University
This article is a review of the immunologicalpeculiarities of the newborn infant and the in-cidence, clinical features, treatment, epidemiologyand prophylaxis of neonatal infections.
Infective disorders are very common in the firstmonth of life and are the principal cause of mor-bidity and mortality after the first few days. Inthe first few days after birth obstetrical factors arethe chief cause of morbidity and mortality, andinfections are uncommon since there has not beentime for most of them to cause illness. Infectivedisorders are more amenable to preventivemeasures than any other cause of morbidity in theneonatal period,' and the efforts being made toreduce their incidence are yielding very encourag-ing results, particularly in maternity hospitals andinfants' institutions where the risk of contractinginfections is so much greater than in the home.Since the unduly high neonatal mortality ratecan most easily be reduced by measures which willcurtail the incidence of infections in the newborn,a better and more general understanding of theepidemiology and clinical features of such infec-tions is of prime importance.
Immunological ConsiderationsIt was for long believed that the newborn infant
has an enhanced resistance to infection. This isa fallacious and dangerous doctrine. The con-ception probably arose from the fact that theexanthematous infections are uncommon in thefirst few months of life.The tissues of the newborn infant, immature
and unaccustomed to infection, react to contactwith bacteria in a different manner from those ofolder age groups. There is a lack of specific activeimmunity and local tissue response is poor. Thesehandicaps are, however, compensated for in theearly weeks by inheritance from the mother ofspecific passive immunity to numerous organismsand the occurrence of a defensive physiologicalleucocvtosis.
In mammals such as man, with a haemochorialplacenta, providing a thin placental barrier, gammaglobulin, which carries the antibodies, passesacross the placenta from the maternal to the foetalcirculation. Most antibodies have the same titrein both individuals and others a lower titre in the'foetal than in the maternal blood. Specificcoliform antibodies have a much lower titre in the
foetal than in the maternal blood anac, con-sequently, are absent unless the mother's titre isfairly high. Only about one-third of pregnantwomen possess pertussis antibodies. The lack ofthese two forms of specific passive immunity inthe majority of the newborn accounts for theprevalence of coliform infections and whoopingcough in young infants. In mammals with- athick placental barrier, and such constitute themajority of species, virtually no antibody-carryinggamma globulin passes across the placenta to thefoetal circulation. It is a natural corollary to theseanatomical and physiological facts that the colost-rum in the anthropoids and other mammals witha thin placental barrier which permits the passageof antibodies, should have a minimal antibodycontent, and the colostrum of mammals with athick placental barrier, not permitting the passage*of antibodies, an abundant supply of antibodies.Nature thus ensures, by one means or the other,that all newborn mammals shall have somehumoral antibody protection against bacteria towhich they had not previously been exposed, andto which they would otherwise be easy prey.
It must be emphasized that the antibodieswhich the human foetus or newborn animalacquires from the mother confer a passive andtherefore a short-lived immunity persisting foronly a matter of weeks or, at most, a few months.It should also be reiterated that some antibodiesare transmitted only to a small extent, if at all, andconsequently afford no worthwhile protection.
Active immunity to the common organismswith which the infant- comes in contact after birthis gradually acquired and immunity to the variousepidemic diseases is acquired as a result of clinicalor sub-clinical infection at'any time. The develop-ment of active immunity is a slow process at anyage, but much more so in the first six months- oflife at which period the immature reiiculo-endothelial system responds poorly to. antigenicstimulation, and produces a low level of lmoralantibodies. This poor response td jan`igenicstimulation can be compensated for to consider-able extent when inducing immunity-in the earlymonths by increasing the strength of the antigenicstimulus. For instance, a satisfactory antibodyresponse can be obtained in the first few'months oflife by giving larger immunizing doses of vaccinethan are necessary at a later age.-
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from
392 POST GRADUATE MEDICAL JOURNAL August I948
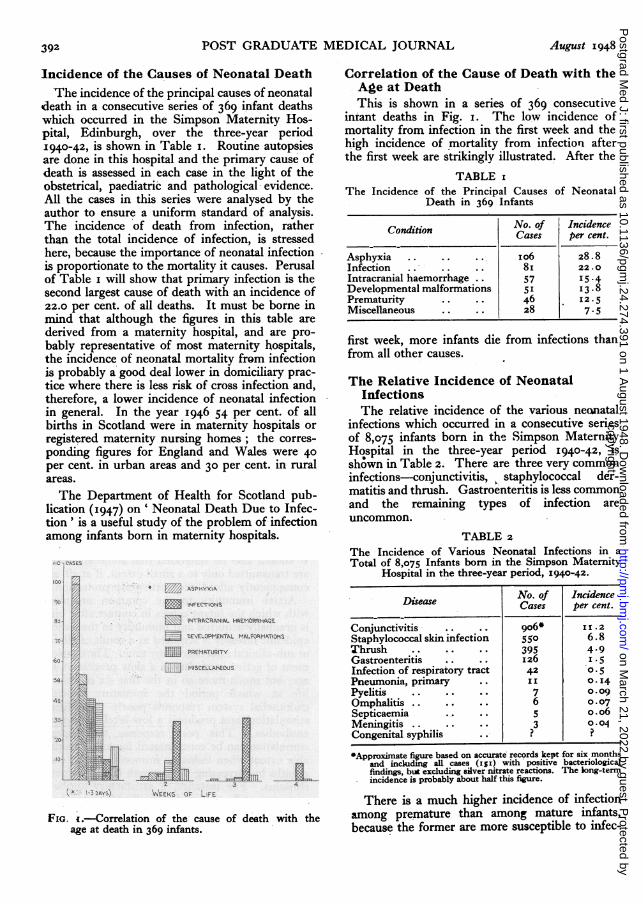
Incidence of the Causes of Neonatal DeathThe incidence of the principal causes of neonatal
death in a consecutive series of 369 infant deathswhich occurred in the Simpson Maternity Hos-pital, Edinburgh, over the three-year period1940-42, is shown in Table i. Routine autopsiesare done in this hospital and the primary cause ofdeath is assessed in each case in the light of theobstetrical, paediatric and pathological evidence.All the cases in this series were analysed by theauthor to ensure a uniform standard of analysis.The incidence of death from infection, ratherthan the total incidence of infection, is stressedhere, because the importance of neonatal infectionis proportionate to the mortality it causes. Perusalof Table i will show that primary infection is thesecond largest cause of death with an incidence of22.0 per cent. of all deaths. It must be borne inmind that although the figures in this table arederived from a maternity hospital, and are pro-bably representative of most maternity hospitals,the incidence of neonatal mortalitv from infectionis probably a good deal lower in domiciliary prac-tice where there is less risk of cross infection and,therefore, a lower incidence of neonatal infectionin general. In the year 1946 54 per cent. of allbirths in Scotland were in maternity hospitals orregistered maternity nursing homes; the corres-ponding figures for England and Wales were 40per cent. in urban areas and 30 per cent. in ruralareas.The Department of Health for Scotland pub-
lication (I947) on' Neonatal Death Due to Infec-tion' is a useful study of the problem of infectionamong infants born in maternity hospitals.
FiG. ;.-Correlation of the cause of death with theage at death in 369 infants.
Correlation of the Cause of Death with theAge at DeathThis is shown in a series of 369 consecutive
iniant deaths in Fig. i. The low incidence ofmortality from infection in the first week and thehigh incidence of mortality from infection afterthe first week are strikingly illustrated. After the
TABLE IThe Incidence of the Principal Causes of Neonatal
Death in 369 Infants
Condition No. of IncidenceCases per cent.
Asphyxia .. .. .. Io6 28.8Infection .. .. .. 8i 22.0Intracranial haemorrhage .. 57 15 .-4Developmental malformations 5 I 13.8Prematurity .. 46 I 12.5Miscellaneous .. 28 7.5
first week, more infants die from infections thanfrom all other causes.
The Relative Incidence of NeonatalInfectionsThe relative incidence of the various neanatal
infections which occurred in a consecutive seriesof 8,075 infants born in the Simpson MaternityHospital in the three-year period I940-42, iSshown in Table 2. There are three very commoninfections-conjunctivitis, staphylococcal der-matitis and thrush. Gastroenteritis is less commonand the remaining types of infection areuncommon.
TABLE 2The Incidence of Various Neonatal Infections in aTotal of 8,075 Infants born in the. Simpson Maternity
Hospital in the three-year period, 1940-42.
Disease No. of IncidenceCases per cent.
Conjunctivitis .. .. 906* 11.2Staphylococcal skin infection 55° 6.8Thrush .. .. .. 395 4-9Gastroenteritis .. .. 26.5Infection of respiratory tract 42 0.5Pneumonia, primary .. I I 0.1I4Pyelitis .. .. .. 7 o.ogOmphalitis .. .. .. 6 0.07Septicaemia .. 5 o. o6Meningitis .. .. .. 3 0.04Congenital syphilis . ? ?
*Approximate figure based on accurate records kept for six monthsand including all cases (Is') with 'positive bacteriologicalfindings, but excluding silver nitrate reactions. The long-termincidence is probably about half this figure.
There is a much higher incidence of infectionamong premature than among mature infants,because the former are more susceptible to inlfec-
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from

August 1948 HENDERSON: Infection in the Newborn Infant 393
tion than the latter, while in maternity hospitalsan even more important cause of the higher in-cidence in premature infants is the much longerduration of their stay in hospital with a propor-tionate increase in the risk of cross infection.
Grouping of Infections according to theTime of the Initial InfectionInfections in the newborn may be classified
according to whether they are contracted before,during or after birth.
Antenatal Infections. These are few in numberbecause of the protection from infection enjoyedby the foetus in utero. It is generally believedthat the healthy placenta is impermeable to micro-scopic organisms and that such organisms caninfect the foetus only when they produce placentallesions. Some believe, however, that in excep-tional circumstances any organisms that producea matemal blood infection mav pass the placentalbarrier and infect the foetal blood stream. Moreevidence on this fascinating question is needed,but it is extremely difficult to obtain.
Syphilis is the only common antenatal infectionand infection of the foetus seems to depend on thedevelopment of preceding placental lesions. Con-genital tuberculosis, of which there have beenalmost ioo cases recorded in the literature, ap-parently arises from placental tubercles, and notfrom tuberculous bacillaemia if the placenta ishealthy.
Ultra-microscopic viruses, unlike microscopicorganisms, are small enough to pass the placentalbarrier and infect the foetus. Since the humanfoetus is not protected from maternal virus diseasessuch as measles, rubella, smallpox, chickenpoxand mumps it is providential that these diseasesare rare in pregnant women. They are uncommonin adults because the vast majority of people areimmunized in childhood, either through havinga clinical, or more likely, a sub-clinical infection.The effect of a virus disease on the foetus dependson the type of the disease and the stage of foetaldevelopment. It is now known that foetal organsduring the stage of differentiation, in the secondmonth of gestation, are particularly susceptible todamage by noxious influences such as specificforms of nutritional deficiency or infection withthe rubella virus. In I94I, Gregg, in Australia,discovered that women who develop rubella inthe second month of pregnancy usually give birthto infants with congenital malformations, par-ticularly cataract, which have been produced bythe rubella virus damaging the relevant tissues inthe organogenetic stage of development. Maternalrubella does not cause foetal malformations whencontracted after the second month of pregnancy.
This is the only infection known, so far, to pro-duce congenital malformations, but there may beothers. Some virus diseases mav cause intra-uterine death with miscarriage, and it is of interestthat women who develop measles in later preg-nancy tend to have a premature labour, and theirinfants may be born with measles or develop itwithin a few days of birth.
Natal Infections. Infections are more oftencontracted during birth than before, though theirmanifestation does not usually occur until a fewdays later. Prolonged labour favours vaginal anduterine infection, particularly when the membranesrupture earlv. Inoculation of the baby's eyes,respiratory passages and areas of traumatized skinis facilitated. A variety of organisms may infectinfants in this way and cause infections such asconjunctivitis, pneumonia and dermatitis in theearly days of life. The chief are staphylococci,streptococci and B. coli.
Other intrapartum infections may arise which aredependent on preceding infection of the maternalpassages. Gonococcal conjunctivitis is usuallycontracted in this way, and oral thrush may be so.Inoculation with the spirochaete of syphilis froma primary lesion on the maternal vulva is a rareoccurrence.
Post-Natal Infections. This is much the largestand most important of these three groups ofinfection, and epidemiological considerationsassume great importance in the common infectionscontracted during the neonatal period. Conjunc-tivitis, staphylococcal dermatitis and oral thrush,the three common neonatal diseases, are all con-tracted after birth in the great majority of instances.
Staphylococcal InfectionsIncreasing attention has been given in recent
years to the prevalence of staphylococcal disease inmaternity hospitals, where its, endemicity is aconstant menace to infants and adults alike.The Staphylococcus aureus is much the most
common cause of neonatal infection, particularlyin maternity hospitals. The chief manifestationsare dermatitis, of which there are several forms,and conjunctivitis, but omphalitis, septicaemia,pneumonia and otitis media may all be caused bythis organism. Staphylococcal infections also com-monly affect mothers and nurses, and the pre-valence of virulent strains is usually shown bya rise in the incidence of both neonatal and adultcases of staphylococcal disease.Staphylococcal Dermatitis
Staphyloccal lesions of the skin are very com-mon in the newborn and there are several varieties.The common forms, in order of frequency, arepustules, paronychia and bullous impetigo. Less
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from

394- POST GRADUATE MEDICAL JOURNAL August 98.
TABLE 3The Inpidence of the Various Types of StaphylococcalInfection' (Based, on the Type of the Initial Lesion),
in 424 Infants in the year 1942.
Tyfie of Lesion No. of IncidenceCases per cent.
Conjunctivitis .. .. 2I2 50o.0Pustules 27.527.Paronychia .53 12.5Bullous impetigo Io226 ,62Boils 212. 2.4Cellulitis and abscesses . I .2PneUmonia .. .. .. 3J 0.7
*Equivalent o6f i0o6 in sixK months of accurate recording.
common forms are furuncles, cellulitis with abscess'formation,' mastitis and pemphigus. The relativefrequency of the various types of lesion in a con-secutive series of infants at the' Simpson MaternityHospital is shown in Table 3.
CLINICAL FEATURES. Pustules may occur singlyor in small or large numbers and they usually occurin'groups, but may be discretely distributed.Large ones are unmistakable, but small ones ma'be confused with (a)' miliaria, (b) small milialsebaceous concretiois which are. particularlycommon on the face' in the newborn, or (c) urti-caria, the lesions of which often show a smallcentral vesicle in newborn infants.
Paronychiais usually multiple, affecting several'fingers, and it'often occurs on both hands. Bpthsides' of'the-finger are affected as a rule. Infectionprobably enters at the torn' base of a tag Qf skin.The condition may not progress beyond a. smallarea of inamm,ation,. though a small focu's of.suopuration often develops in the centre of thearea. This focus usually drie,s up and, forms alittle scab which eventually separates, but oc-casionally a larger pustule will form. which 'my,burst '(Fig. 2). Infrequently, the infection may.spread and caiMse complications. It may inv,ade.the nail fold,`prducing a true onychia or involvethe' nail Jbed, in which case the nail may' be shed.Somietimes the infection spreads. in the skin. of the.finger,causien, septic blistering. Thrombosis ofthe terminal digital arteries is a rare but..dangerouscomplication, for it produces necrosis of the, ter-'mina,l phalanx. and gangrene of the. tip of the.finger.
JBuious Impetigo is less common than the twopreceding infections, but more liable to occur inepidemic form, a fact which. suggests-that it is. amanifestation of exalted virulence or of the.,pre-valence of an unusually virulent straih. Theremay be. one lesion, but there are usually a few(Fig. 3) and they are often widely;.dispersed. Theyappear without the warning of preceding 'inflam-mation and vary: in size' from a few mm. in diameter
to' an inch or two. They contain clear or slightlyturbid.fluid which soon becomes more purulentand the fluid is not under much tension. If un-treated. the vesicles increase in size and numberand when they rupture the underlyinig moistreddish dermis is exposed. When large areas ofskin become. affected the condition is known aspemphiguis. In b6enign yesiculation of the 'new-born, small blisters, seldom exceeding i 'cm. indiameter, arise in the first few days of life, usuallyon the fingers, and they.do not enlargc, are moretense and contain bright yellow sterile fluid.
Pemphigus is the septic vesiculation' and ex-foliationv of large areas of skin. It is a grave con--dition'associated with severe toxaemia and is nowrarely seen in maternity hospitals. In derm'atitisexfoliativa (Ritter's Disease) which is usuallystreptococcal, there is no vesiculation, but ex-foliation of 'large areas of skin occurs. Thiscondition is equally serious.
Furuncles sometimes 6occur in' the -newborn.They"'usually look more like small abscesses thahboils.' The occipital region is 'one 'of the' mostt'common sites, but they may occur in any situation,are usually multiple 'and often widespread.
Cellulitis and abscess formation are occasionalmanifestations of staphyloCoccal infection. It maydevelop under'a superficial' infection such 'as apustule, but there is often 'no apparent 'portal ofentry. The area involved 'iS sometimes large.Suppuration develops quickly in the 'newborn'unless vigorous and prompt. penicillin therapy isadopted.
M sii is bMastitisis by 'no means rare and arises in thephysiologically enlarge.d'breast. It usually pro'gresses to suppuration.TREATMENT. Prophylaxis is very important.
The practice of not bathing newborn babies untilafter discharge from hospital, which is increasing,probably reduces the incidence of staphylococcalskin infections. The face is cleaned if necessaryafter -birth and the buttocks as indicated, andthere is. no, unpleasant aroma such as might, be.expected. The. risk' of contact infection is muchreduced, the skin is subjected to much lesstrauma, the,-infant is less exposed, and.-there is a.great saving of nurses' time.The importance of immediate isolation of- all
infants who develop.a staphylococcal lesion, how-ever small, cannot-be over-emphasized. Moreover,all lesions, 'even the most -trivial, should beassiduously. treated, owing to the ever-presentdanger, of a much more serious local lesion or ofa generalized infection developing.
Therapy will 'depend on the type and severity ofthe lesion. Any loose skin, as'in bullous impetigo,should. be completely removed and affected areas
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from
August 1948 HENDERSON: Infection in the Newborn Infant 395
should always be covered with a dry dressing toprevent contacting clothes or the baby's fingersfrom infecting other areas of the skin. Superficial-lesions should be treated locally with 5 per cent.penicillin cream or i per cent. gentian violet inaqueous solution twice daily. Systemic penicillinshould be given in all cases, giving 20,000 unitsorally in each feed, and four-hourly during thenight in a little milk.
It has been shown by Henderson and McAdam(I946); and other workers, that the administrationof penicillin by the oral route is reliable in thefirst month of life when given in larger doses thanwould be adequate if given intramuscularly. Tenthousand units usually produces a therapeuticlevel in the blood which is maintained for. fivehours. Twenty thousand-units given in each feedprovides an ample therapeutic margin. In hos-pital practice penicillin for oral administration ,is'usually dispensed in i drachm of normal saline,but in domiciliarv practice it is more convenientto crush and dissolve in each feed two io,ooo-unittablets.
It is disturbing to find a. poor response topenicillin therapy in a considerable minority ofcases of staphylococcal infection. The. staphy-lococcal strains in these cases a're found to bepenicillin-resistant, some moderately and othershighly, and very, large doses up to io or 2o timesthe normal dose may be necessary to overcome theresistance of the organism and cure the disease in'such cases. Surgical procedures, such as incisionand drainage,' will be necessary when an abscessforms andl in some cases with mastitis, boils oronychia.
ConjunctivitisStaphylococcal infection is much the most
common cause of in'fective conjunctivitis in theneonatal period and accounts'for more cases thanall other forms of infection combined. Con-junctivitis iri the newborn will be described ind'etail in a later section.'
Other Staphylococcal InfectionsThe Staphylococcus aureus may cause infection
in several parts of the body, in addition to theeyes and skin, which are the most common' sitesof infection by this organism. It is often foundin omphalitis, broncho-pneumonia, aspiration orprimary, otitis media and septicaemia, 'whileosteomyelitis is essentially a staphylococcal disease.
Epidemiology of Staphylococcal InfectionsEpidemiological studies of staphylococcal
disease are hampered by the lack of a'satisfactorymethod of identifying the various strains of 'theorganism. The 'method now' most commonly
used for detecting pathogenicity is that based onthe capacity of pathogenic staphylococci tocoagulate plasma. -The term coagulase-positiveis, therefore, synonymous with pathogenicity, butthis test gives no indication of the degree ofpathogenicity. There is no simple method ofidentifying the most virulent strains, but it is nowpossible to classify pathogenic staphylococci intoa large number of types by means of highly specificstaphylococcal phages, and some relation may befound between these types and the degree ofpathogenicity. Chapman et al. (I937) have beenexperimenting with the production of mediaselective for pathogenic staphylococci. A reliableand simple method of identifying the variousstrains of staphylococci would greatly facilitateepidemiological studies. The recent developmentof serological and phage typing has made it possibleto relate infection in nurses to infection in infantsin a number of epidemics.The infant at birth has about the same titre of
staphylococcal antitoxin as the mother, but itseems to have little protective value. Experimentalwork suggests that the chief value of the antitoxinis to assist in combating systemic infection, but itseems unable to prevent the organism fromcausing local lesions. When the skin is inoculatedwith a culture of Staphylococcus aureus theorganisms diminish rapidly owing to a well-markedbactericidal action which the skin has been shownto have on many organisms, but the st'aphylococcimay not completely disappear. Moreover, it isclear that staphylococcal lesions develop veryreadily at the site of small traumatic lesions onthe skin.About 30 per cent. of adults are nasal carriers
of Staphylococcus aureus- and individuals''withstaphylococcal skin lesions have a much highernasal carrier rate.' Recent work has shown thatthe infants in maternity hospital nurseries may beexpected to show a high incidence of pathogenicstaphylococci 'in the nose; the incidence ofSt'aphylococcus aureus rises from zero at birth toa figure that appears usually to be well over 50per cent. and may approximate to ioo per cent.It is important to remember that the faeces inmany cases are infected and also the skin. Themost important sources of infection, however, arethose infants with slight superficial infections suchas a few small pustules, a ' sticky' eye or' damp'umbilicus. In such circumstances, the organismis multiplying rapidly, is present in greater num-bers, is more virulent and p'ossibly increasing invirulence. Benians (iX94) found at the height'ofan epidemic 'of bullous 'impetigo' and other'staphylococcal skin lesions in the newborn, ina maternity hospital, that 85 per cent. of the
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from

396 POST GRADUATE MEDICAL JOURNAL August 1948
maternity nurses were nasal carriers. The ratefell to 25 per cent. six months after the outbreak.
Spread from one individual to another is eitherby direct contact or through the agency of objects,such as clothing, instruments and ointment. Ithas been shown, for instance, that infected clothesmay not be sterilized in laundries and that infectedpersonnel in laundries may contaminate them.The air and dust may become infected throughshaking infected clothing and the organisms byaerial dissemination settle directly on babies or,more likely, on all manner of objects which will behandled by nurses and thus contaminate theirhands. Clearly then infection must be regardedas coming from direct or indirect contact withnurses, domestic staff, doctors, mothers, otherinfants or visitors.
It has been stated above that under presentconditions most infants in maternity hospitals areinfected with potentially pathogenic staphylococciby the time they are discharged, showing that thepresent methods of preventing the spread of con-tact infection are ineffective. Fortunately, themajority of the strains are of low virulence, so thatmost of the infants remain healthy and only a fewsuffer from trivial lesions, but these trivial infec-tions may be the forerunners of serious epidemicswhen more serious staphylococcal lesions, such asbullous impetigo, pemphigus, cellulitis or staphy-lococcal pneumonia may develop in some of theinfants; mastitis, staphylococcal infection of thegenital tract or other staphylococcal lesions insome of the mothers; and staphylococcal lesions inmembers of the staff. Ludlam (I947), from whoseexcellent review of the epidemiology of staphy-lococcal infections much of the foregoing informa-tion has been obtained,'believes the most practicalway of finding the adult source of staphylococcalinfection is to examine all adults who enter amaternity unit for septic lesions and to take a nasalswab from each, paying particular attention to anyadult contact who repeatedly yields a profusegrowth of pathogenic staphylococci. Nurses inthese circumstances should be debarred fromentering a maternity unit and transferred, ifpossible, or, less desirably, carry out a particularlyrigid hygienic regime. Ludlam emphasizes -thata more effective but more arduous way of identify-ing adult sources of infection is to type the staphy-lococci isolated from adults by routine nasalswabbing as described above, and at the sametime the staphylococci isolated from infants,mothers or nurses with staphylococcal lesions.
Knott and Blaikley (i944) in the MaternityUnit at Guy's Hospitaj investigated the epidemi-ology of staphylococcal infections over a period oftwo years, and by introducing a more enlightened
routine were able to reduce the incidence. ofstaphylococcal infection greatly, and to bring toan end the occurrence of repeated epidemics ofstaphylococcal infection which had previouslyhampered the smooth functioning of the unit.They emphasized three main epidemiologicalpoints:
(a) The more virulent strains of Staphylococcusaureus which are responsible for active lesions areusually introduced to a previously clean depart-ment by human carriers, skin, respiratory orvaginal, temporary or permanent.
(b) Since masks were worn at all times, andinfection spread rapidly in spite of them, directcontact, especially hand contact, must be extremelyimportant.
(c) Frequently handled ward equipment such asfeeding bottles were often infected, and muchmore likely to pass on infection than ward dust,which was surprisingly free from pathogenicstrains even during epidemics.The following are the principal prophylactic
measures recommended and successfully adoptedby Knott and Blaikley:
(i) To avoid contact spread the routinenursing of both mother and baby should be guidedstrictly by all those principles accepted as essentialin performing surgical dressings.
(2) All nurses have their nose, throat and handscultured before commencing work in the mater-nity department. All whose cultures containpathogenic staphylococci are debarred, given non-surgical and non-septic work and re-examined atintervals until free.
(3) All nurses working, in the department havethese cultures repeated each fortnight and whenthey develop colds. All growing staphylococciare at once debarred, but allowed to return if theorganisms are shown to be non-pathogenic onfurther investigation.
(4) All mothers are swabbed immediately onadmission. The nose, throat, hands and thevagina are all swabbed. Also any inflammatorylesion, however small. They remain in a smalladmission ward until the results are known. Ifnegative, they pass into the main wards. Ifpositive, they go to a small separation unit wherethey remain until the organism is shown to benon-pathogenic. If pathogenic, they are admittedto an isolation unit.
(5) Babies are handled only when absolutelynecessary.
(6) Always before and after handling a baby,or tending a recently confined mother, nursesmust invariably wash their hands and forearmsunder a strong spray of water turned on by foot orelbow as in a surgical theatre. They then dry the
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from

August I948 HENDERSON: Infection in the Newborn Infant 397
hands on small sterile towel squares which areused only once, thrown into a basket and thenlaundered.
(7) To reduce handling of babies and damage totheir skin, the babies are bathed as infrequentlyas possible, only at birth and when the -cordseparates.
(8) After each baby is bathed the whole of thebath and its equipment is very thoroughly washeddown before being used again.
(g) Each day's supply of dusting powder, olive,oil or similar applications is sterilized.
(io) Only fathers are allowed to see babies andthey must wear masks. They may not handlebabies. Babies are not kept in the ward duringvisiting hours.
(ii) Mothers and babies infected with patho-genic strains of Staphylococcus aureus are re-moved to an isolation unit away from the maindepartment.
Knott and Blaikley also recommend that nursesshould always wear masks when attending tobabies and mothers and whenever they are in thenurseries, but I believe that this practice, thougha useful additional precaution, is less importantthan the i i precautions enumerated above.
Such a routine conscientiously carried outwould greatly reduce the incidence of staphy-lococcal and other forms of cross infection such asthrush and epidemic gastroenteritis in our mater-nity hospitals, and epidemics would be rare.Epidemics are always a serious reflection on hos-pital conditions and management. The Guy'sunit is small and the preventive routine so success-fully operated there is, therefore, relatively easy tocarry out, but the experiment has proved howsuccessful such a routine can be, and is a challengeto larger maternity units in general to leave nostone unturned and make a determined attemptto introduce a prophylactic routine based on thesame fundamental principles. The shortage ofnurses at the present time is a serious obstacle,but a clear conception of preventive principles bythe responsible authorities would ensure a notablereduction in the present rate of staphylococcalinfection in particular and neonatal infection ingeneral. Knott and Blaikley believe that ' con-tinuous bacteriological control in a maternitydepartment far exceeds in' value intermittent bac-teriological testing, and does not involve a pro-hibitive amount of work or number of exclusionsof either staff or patients.'
ConjunctivitisConjunctivitis is the most common neonatal
infection. It is usually very mild. A moderatedegree with a little sero-purulent discharge, but
no swelling or inflammation of the eyelids, iscommon. Only a small minority of cases isacute, with palpebral oedema and inflammationand a profuse discharge.
Conjunctivitis in the first two days of life iscommon when irritating prophylactic instillationsare used at birth. Silver nitrate, which is theprincipal agent used for this purpose, is veryirritating when used in the standard i per cent.solution, and not infrequently causes an acutechemical conjunctivitis with blepharospasm anda profuse serous discharge. It subsides spon-taneously within two or three days. A i per cent.silver nitrate solution is quite strong enough forprophylactic purposes. This should be kept in awell-stoppered bottle to prevent concentration byevaporation.The incidence of the various organisms isolated
in a consecutive series of infective conjunctivitisin the Simpson Matemnity Hospital is shown inTable 4. Direct inoculation of a blood-agarplate was made from the conjunctival sac and adirect smear was also made. Organisms wereisolated in i 5i cases and none in 63 cases. Therewas a great preponderance of Staphylococcusaureus, 72 per cent. of cases with a pure culturebeing due to this organism, and 70.2 per cent. ofall cases, whether pure or mixed infection, beinginfected with it. Staphylococcus albus wasisolated from 9.9 per cent. of cases, and diph-theroids from i 1.9 per cent., both these organismsbeing associated with others in most cases. Eightother organisms were isolated on a few occasions,including Streptococcus viridans in 5.3 per cent.,B. coli in 4.6 per cent. and pneumococcus in 4per cent. The gonococcus was isolated from onlytwo of the r5I cases, in pure culture in bothinstances. Though relatively uncommon, andmuch less often seen than in former- times,gonococcal conjunctivitis remains the most im-portant form of conjunctivitis in the newborn,since it is the only form which may destroy aneye- in a few days if treatment is neglected. Virusconjunctivitis was not looked for and some ofthe negative cases may have been of this nature.
TREATMENT. The introduction of sulphonamideand penicillin has revolutionized the therapy ofconjunctival infections. Treatment is muchsimpler and more effective. Since 8o per cent. ofcases yielding a positive culture are staphylococcal,initial treatment should always be with penicillin,and this agent should be continued until eithera penicillin-resistant and sulphonamide-sensitiveorganism, such as B. coli or a diphtheroid, isisolated on culture-2I.9 per cent. of the casesin this study yielded such organisms in mixed orpure culture-or until, in the absence of bac-
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from
398 POST GRADUATE MEDICAL JOURNAL August i948
TABLE 4The Incidence of the Various Types of Infective Conjunctivitis in the Newborn.
No. of Cases IncidenceBactriumPure Mixedpecnt
Culture Culture Total per ce
Staphylococcus aureus *. .. .. .. .. 95 II Io6 70.2albus .. .. .. 5 Io 15 9.9
Diphtheroids .. ..- . 9 9 i8 II.9Streptococcus viridans .. .. .. .. .. 6 2 8 5 .3Pneumococcus .. .. .. .. .. .. 3 3 6 4.0Gonococcus .. .. .. .. .. .. 2 0 2 1.3Bacillus coli .. .. .. .. .. .. 6 I 7 4. 6
proteus . .. .. .. .. 2 I 3 2.0
pyocyaneus .. . .. .. .. 2 I 3 2.0lactis aerogenes .. .. .. .. I 0.7Morax-Axenfeld .. .. .. .. I 0.7
Negative film and culture .. .. .. .. - 63
Infants with a pure culture .............. ....132,mixed ................. .......I9negative ................. .....63
Total of infants with infective conjunctivitis .. I5IIncidence of infective conjunctivitis .. .. I 2 per cent.
teriological investigation, the conjunctivitis fails toshow much improvement in three days-pre-sumably because the infecting organism is apenicillin-resistant bacillus. In both of thesecircumstances the treatment should be changed tosulphonamide, usually with success.
In mild cases crystalline penicillin should beadministered locally by instilling one or two dropsinto the conjunctival sac before and after eachfeed. In cases of moderate or severe degree itshould be instilled as often as possible, at leasthourly in a moderately severe case, and everyfew minutes in the early stages of treating a severecase. In severe cases systemic penicillin shouldalso be given. The penicillin solution for instilla-tion should contain 2,500 Oxford units per cc. ofnormal saline in the less severe cases, and I0,000units per cc. in severe cases, and 20,000 unitsshould be given three- or four-hourly in each feedand four-hourly in a little milk during the nightwhen systemic administration is also considerednecessary.
Sulphonamides can be given locally or sys-temically according to the severity of the condition.Sodium sulphacetamide, io per cent. solution innormal saline, or 2-4 per cent. in ointment, isthe form in general use for local treatment, andit should be instilled before and after each feedin mild cases. Sulphacetamide is soluble andnon-irritating, whereas most of the other sulphona-mides are insoluble and alkaline and are, therefore,unsuitable for local treatment. In more severecases sulphonamide should be given orally in aform such as sulphamezathine or sulphadiazine indoses of i gr. four-hourly. When the in-
fecting organism is susceptible to sulphonamidetherapy, as in gonococcal or pneumococcal con-junctivitis, which are both acute and severe, as arule, the response to sulphonamide given by theoral route is dramatic and the disease is cured intwo to four days.When the eyelids tend to adhere in conjunc-
tivitis and impede the free drainage of dischargea drop of liquid paraffin instilled into the sac willensure free drainage. Conjunctival lavage, whichwas the bulwark of treatment in the pre-chemo-therapeutic era, is unnecessary.
Chronic ConjunctivitisRecurrent conjunctivitis and unduly' indolent'
conjunctivitis which may persist for months inyoung infants in spite of persistent treatment arecommon. They are usually caused by poordrainage from the conjunctival sac owing to acongenital stenosis of the naso-lachrymal duct.Ophthalmologists advise conservative treatment inthese cases and seldom attempt to dilate the duct,because adequate canalization and drainage willoccur within a few months when the tendency to,conjunctivitis will subside. In the meantime themild conjunctivitis should be minimized by in-stillation of the solution appropriate to the infect-ing organism. Dacryocystitis occasionally developsin, such cases; firm pressure over the sac atregular intervals evacuates accumulated muco-pusinto the conjunctival sac from which it escapes.
ThrushOral thrush is a common infection in young
infants, particularly in maternity hospitals and
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from
August 1948 HENDERSON: Infection in the Newborn Infant 399
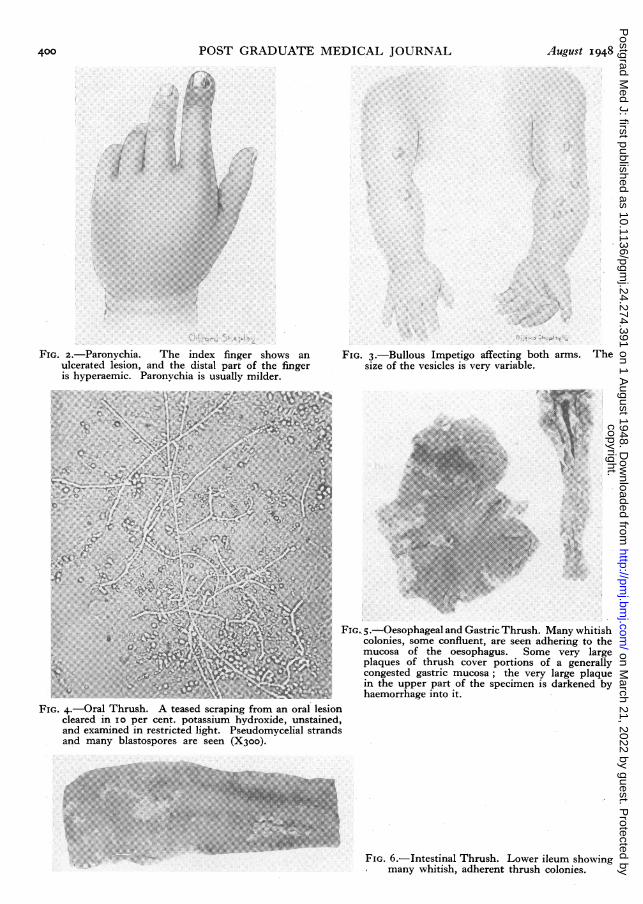
other institutions. The incidence in the SimpsonMaternity Hospital in the period I940-42 was4.9 per cent. (Table 2), but a better understandingof the disease and increased vigilance reduced it toi.8 per cent. in the period 1944-46. It is causedby the fungus Monilia albicans, a generally dis-tributed organism which occurs in the mouth inabout I4 per cent. of the adult population (Todd,I937). The incubation period is about four daysor more. A photomicrograph of a specimenobtained from a thrush lesion in the mouth of aninfant in a maternity hospital is shown in Fig. 4.Fortunately, the organism is pathogenic only inthe early months of life in health, but may becomeso in older infants and children, and even in adults,as a secondary invader in local conditions, such asulcerative stomatitis or in conditions of severegeneral debility.
CLINICAL FEATURES. Thrush seldom developsbefore the latter part of the first week and mayoccur at any time in the following few months.It is much more common in bottle-fed than inbreast-fed babies, and also in those who staylonger in hospital, such as premature babies.The lesions begin as whitish-grey, pin-head
colonies on any part of the buccal mucosa or onthe dorsum of the tongue. They are adherentbecause the mycelial strands of the organismpenetrate the mucosa. If untreated, the coloniesmultiply and enlarge and they may coalesce toform large plaques. The tongue is the mostcommonly affected part of the mouth, and thepalate is more often affected than the inside of thecheeks. Severe infection may lead to ulcerationand secondary infection. The pharynx also maybecome involved; one cannot say in what pro-portion, but probably in a minority of cases.Invasion of the oesophageal wall occurs oc-casionally and is a serious complication, and thedisease may spread even further and involve thegastric mucosa. In a series of 20 cases of oeso-phageal thrush, Ludlam and Henderson (1942)found gastric involvement in four. Fig. 5 showsnumerous thrush lesions of the oesophagus andstomach in a pathological specimen. Intestinalthrush appears to be rare, though it is likely to bemissed ; it may occur in the small intestine,usually the lower ileum (Fig. 6) or in the colon.Macgregor and Henderson (1943) published twocases of thrush in the lower ileum in which thecondition was found at autopsy.
Oral thrush is usually a mild and somewhat'indolent' infection and the oral lesions usuallydo not cover much of the mucous membrane. Ifuntreated, the lesions will cease to spread, inmost cases, after reaching such a stage and usuallypersist for many weeks before gradually subsiding
without ever having interfered with the feeding orprogress of the infant. Nevertheless, it is dan-gerous ever to regard thrush as a benign condition,and it is generally so regarded, because it doesbecome a severe and serious disease in a consider-able minority of cases. It may then prove fatal,as in 13 of the 20 cases of thrush oesophagitis towhich I have referred. Severe oral thrush, withinflammation, ulceration and secondary infectionof the buccal mucosa, causes some degree ofanorexia and malaise, while oesophageal involve-ment produces severe anorexia and vomiting and,in fatal cases, aspiration broncho-pneumonia.Thrush oesophagitis cannot be diagnosed withcertainty during life and it is not known, therefore,what proportion of the less severe cases recover.Similarly, thrush ileitis and colitis, which causediarrhoea, can only be diagnosed post mortem,and the death rate cannot be determined. Itshould be borne in mind, however, that carefulinspection of the mouth reveals oral lesions in ahigh proportion of cases with involvement lowerdown the alimentary tract.
DIAGNOSIS. Oral thrush must be differentiatedfrom milk curds which are not adherent, whitefibrous nodules which are a normal feature in thegums, and the median raphe of the palate, andfrom furring of the tongue which is uniform,unlike the granular appearance of thrush. Alsofrom a sloughing traumatic ulcer following injuryto the palate by a mucous extractor. When indoubt, the diagnosis should be confirmed byscraping off a colony or plaque and teasing it outon a slide in io per cent. potassium hydroxide.Microscopic examination with minimal illumina-tion will show the mycelium and spores and t4edebris will have been dissolved (Fig. 4).TREATMENT. Prophylaxis is fundamental in
institutions. The babies of mothers who sufferedfrom vaginal thrush in pregnancy should bespecially carefully watched for the development oforal thrush. All infants who develop thrush shouldbe isolated immediately to prevent cross-infection.It is a rule in well-run maternity hospitals for themouth of every baby to be carefully inspected forthrush each morning by the sister-in-charge ora responsible staff nurse.
Therapy consists of the application of i percent. gentian violet in aqueous solution to themouth twice a day until the lesions have prac-tically disappeared, and then once a day for anotherweek to prevent relapse. This is necessary becausethe spores persist in the mouth for a week or twoafter disappearance of the lesions, which, inciden-tally, usually linger longest between the corruga-tions on the fore-part of the hard palate. Suchpersistence of infection after clinical recovery
D.
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from
400 POST GRADUATE MEDICAL JOURNAL August 1948
...... ... ...... ................... ......... .... ..
....... ;...''..
FIG. 2.-Paronychia. The index finger shows anulcerated lesion, and the distal part of the fingeris hyperaemic. Paronvchia is usually milder.
B: :! :e:':: :' ::!: ....g.r; ... j.:.!:.',S -.> B.e, ,, |s. ::: :. , .. e. - 8: cS oWB ,, l. r . l .. S: .. ;.:,. y . l .. : :.:.;: .:We m- H. ;S |colS ......... - : : :: .. ;.|l, . j. ; ,.: .' .'., i;. '': ::.: :::.:.:: > .!. .S....i,:<.,::.::<..-..,.:..:..: :: i:i .i -.:
::::::...:..:.: .:..::!j :.: .: :::.::. j.:. .: ..:: j: .: ...:,. :-:.:j... ':,.':.': i.:.::: .: .. ::: :': :' .:;.:.,.' .. ., .'a.. ',.,' ... .S,X,';;: ,. g":: :: :: ::;.: :: :::::}.:- .. ::::2 e.'B :'.,.:C:::::: ..:: : :.: . ; - :-i ; .. ,; . - e 2, . :: : .. :e < .:: ....... : ',-: ^ '- .2 . :. -'.:. ':
FIG. 3.-Bullous Impetigo affecting both arms. Thesize of the vesicles is very variable.
t M /
~I
FIG. 4.-Oral Thrush. A teased scraping from an oral lesioncleared in Io per cent. potassium hydroxide, unstained,and examined in restricted light. Pseudomycelial strandsand many blastospores are seen (Xioo).
4pa
FIG.. 5.-Oesophageal and Gastric Thrush. Many whitishcolonies, some confluent, are seen adhering to themucosa of the oesophagus. Some very largeplaques of thrush cover portions of a generallycongested gastric mucosa; the very large plaquein the upper part of the specimen is darkened byhPemorrhnaee intn it.
I I
FIG. 6.-Intestinal Thrush. Lower ileum showingmany whitish, adherent thrush colonies.
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from

August I948 HENDERSON: Infection in the Newborn Infant 401
necessitates continued isolation until discharge,unless bacteriological cure is demonstrated.
EPIDEMIOLOGY. Thrush vaginitis is one of theprincipal causes of leucorrhoea in pregnancy andthe infants of infected mothers may developthrush within a few days of birth, though theyusually seem to escape infection. Most of thecases in maternity hospitals are caused by cross-infection via the hands of nurses. Ludlam andHenderson (1942) isolated Monilia albicans fromthe throat of 33 per cent. of a series of 6o nursesin the Simpson Maternity Hospital, and from thefingers of three out of 42 nurses swabbed whenbottle-feeding infants. The disease developed inall infants from whose mouths the organism hadpreviously been isolated, though relapse did notalways occur when the organism was isolatedafter thrush lesions had disappeared. Oral thrushwas accompanied by infection of the infants' handsin 50 per cent. of cases and by infection of thefaeces in all cases. It was also isolated from 50per cent. of samples of pooled breast milk. Ex-posure of culture plates in the nursery and chang-ing rooms for long periods did not produce asingle thrush colony, which seemed to eliminateair-borne infection as an important epidemio-logical factor.The nurses' hands appear to be the main vehicle
in the dissemination of thrush, as in the dis-semination of the Staphylococcus aureus and theprophylactic principles and routine are the samein both infections.
GastroenteritisThis is much the most serious of the common
neonatal infections. It may be primary and causedby a variety of organisms, known and unknown,or it may be secondary. Infective gastroenteritisis always potentially an epidemic disease whateverthe causal organism, and its gravity makes it themost dreaded of all neonatal infections in maternityhospitals. In most epidemics no casual organismcan be found and many have, therefore, assumedthat a virus is the probable cause, but this is adebatable hypothesis. Some believe that sinceyoung infants tend to react to various types ofinfection by diarrhoea, epidemic neonatal diar-rhoea may be produced by a variety of organisms.Some suspect certain strains of Bact. coli whichare normally non-pathogenic in older children, butwhich readily cause a number of neonatal infectionssuch as meningitis and pneumonia. McClure(1943), for instance, found haemolytic B. coli ina greater proportion of sick than of healthy infantsin an epidemic he investigated. Moreover, thebeneficial effect of sulphonamide in epidemicgastroenteritis reported by Henderson (I943) and
numerous other workers is more suggestiveof a bacterial than a virus aetiology. A few yearsago Light and Hodes (I943) claimed to haveisolated a virus in four outbreaks of neonataldiarrhoea, but no confirmatory evidence hasbeen obtniined since from other epidemics,Epidemics have been described in which thefollowing organisms have been suspected-B. colimutabile, B. mucosus, B. protes and B. pyocyaneus,while Gale et al. (i944) have isolated beta-haemolytic group D streptococci in large, numbersfrom some epidemics and believe that the hightyrosine decarboxylase activity of these organismsmay cause severe toxaemia and diarrhoea in veryyoung infants, as in very young rats. Clearlythere is much speculation about the aetiology ofepidemic diarrhoea in the newborn, but few con-crete facts have yet emerged from the manyattempts to elucidate this baffling disease. It isprobable that there are several distinct aetiologicalorganisms and that some of these cause ageneralized disease of which gastroenteritis is oneof the features. The great variability of theincubation period in different epidemics alsosuggests an inconstant aetiology. It varies froma few to 2I days. In a small proportion ofepidemics known pathogens such as Salmonellaeand B. dysenteriae Sonne have been isolated, andthese can usually be linked up with adult carriers,The incidence and mortality in the Simpson
Maternity Hospital in the two four-year periods1939-42 and 1943-46 are shown in Table 5,Increased vigilance and earlier diagnosis reducedthe incidence by half in the latter period, whileimproved methods of treatment, and possibly lesssevere forms of the disease, caused a steep fall inthe mortality from 43.1 per cent. to 17.5 per cent.(II.3 per cent. in the two-year period I945-46),
CLINICAL FEATURES. Infective gastroenteritisis much more common in bottle-fed than in breast.fed infants. It seldom develops until the secondpart of the first week, but. usually after the firstweek. The affected infant develops malaise, withanorexia, listlessness and pallor. Diarrhoea is notthe first symptom and it may not begin for I2 to36 hours. The severity of the diarrhoea variesgreatly. It may be watery with an uncountablenumber of stools in the day when the diagnosiswill no longer be in doubt, or there may be onlyslightly increased frequency and looseness of thestools. In the latter circumstances, the diagnosismay remain uncertain for a few days, particularlyin sporadic cases where there is less reason tosuspect the disease. A noticeable increase ofmucus in the stools is seen in only a minority ofcases, as a rule, and blood is seldom seen. Vomit,ing is a feature in about half of tlw gases, also
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from

402 POST GRADUATE MEDICAL JOURNAL August 1948
TABLE 5
The Incidence and Mortality Rate of Gastroenteritis in the two Four-Year Periods 1939-42 and 1943-46
Cases DeathsPeriod Live - Incidence Incidence
Births Number per cent. Number per cent.
I939-42 .1. I 0,484 i88 1.79 8i 43 .'I1943-46 I. .. 12,241 120 o.98 21* 17.5*
* In the two-year period I945-46 there were eight deaths with a mortality rate of I 1.3 per cent.
pyrexia. Signs of dehydration appear within aday or two in all cases except the mildest, andprogress very rapidly in acute cases. Theweight falls steeply, except in mild cases. Scream-ing sometimes occurs, presumably because ofcolic. Abdominal distension may occur inadvanced cases and is a serious sign, and scleremais a grave development.
TREATMENT. Prophylaxis is much the mostimportant aspect of the handling of this disease.Suitable isolation facilities should be available inall maternity hospitals to isolate immediately, asa precautionary measure, all infants who develop-malaise, particularly anorexia, a lagging or fallingweight or any looseness of the stools. Most suchinfants will not have gastroenteritis, but only byprompt precautionary action will epidemics ofgastroenteritis in nurseries be prevented. Whengastroenteritis is diagnosed in such an isolatedbaby, all the babies in the nursery from whichthat baby came should be presumed to be in-fected, and no further babies admitted to thatnursery until all have been discharged or for aperiod of three weeks.
Therapy consists of the complete withdrawal.of milk feeding for a variable number of days untilthe appetite returns, and half normal saline con-taining 5 per cent. glucose is given two-hourlyad lib.; a daily intake of 3 oz. per lb. body weightmust be ensured. This fluid is usually taken welland gavage feeding is not often necessary. Sulpha-succidine or sulphaguanidine should always begiven from the outset in a dose of 5 gr. per lb.per day. Improvement with a return of appetite-occurs in one to four days when these measuresare adopted. Dilute milk feeding with half-strength breast milk, or a low fat artificial milk,such as sweetened condensed or half-cream dried,is then commenced at alternate feeds and, if welltolerated, the mixture is given at every feed thefollowing day and then gradually strengthened.
In severe cases with much dehydration ortoxaemia, intravenous fluid and electrolyte therapyshould be inaugurated without delay. Oral salineand glucose should be continued ad lib. in these
circumstances as advised, but if there is muchvomiting, oral feeding should be completelystopped until vomiting ceases and general improve-ment occurs. Lack of space forbids a detailedaccount of current practice in parenteral fluid,electrolyte and maintenance therapy. This canbe obtained from paediatric textbooks and articleson the subject by Darrow (I946), Govan andDarrow (1946), Butler and Talbot (I944) andHenderson (I947).
Penicillin, 20,-000 units four-hourly by mouth,should be given in all cases to minimize thepossibility of secondary infection.
Respiratory Tract InfectionsNasopharyngitis is not uncommon. It is most
often contracted from a mother who has a ' cold,'but sometimes from one of the staff or a visitor.The chief symptom is nasal obstruction whichreadily occurs in the narrow passages of the infant.The infant becomes snuffly and feeding is rendereddifficult and is subject to repeated interruptions.Immediate isolation is necessary because colds arehighly infectious. Failure to do this may causean epidemic in which some infants will be likelyto develop complications, such as otitis media,infection of the lower respiratory tract or broncho-pneumonia. Penicillin and sulphonamide shouldbe given in all these complications, but it is evenmore important to endeavour to avoid these com-plications by commencing these drugs as soon asthe naso-pharyngeal catarrh shows signs of becom-ing purulent. Nasal' obstruction can often berelieved and feeding assisted by instilling into thenostrils before feeds drops consisting of ephedrine1 per cent., sodium chloride I.3 per cent., Aq.Dest. ad. ioo per cent. Oily drops should neverbe used, since aspiration may cause pneumonia.
Otitis MediaThis infection is difficult to diagnose in the
newborn unless otorrhoea develops, becau;e theeardrums are very difficult to see at this age evenby otologists. It occurs not infrequently, es-pecially in upper respiratory tract infection,
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from
August I948 HENDERSON: Infection in the Newborn Infant 4O3
because the eustachian tubes are short and wideat this age and infection easily passes along them.It should always be borne in minid as a possiblecause of obscure illness, as in older infants. Theorganism is usually either a pneumococcus orStaphylococcus aureus, but may be a haemolyticstreptococcus. Penicillin should be given sys-temically by the method advocated elsewhere.
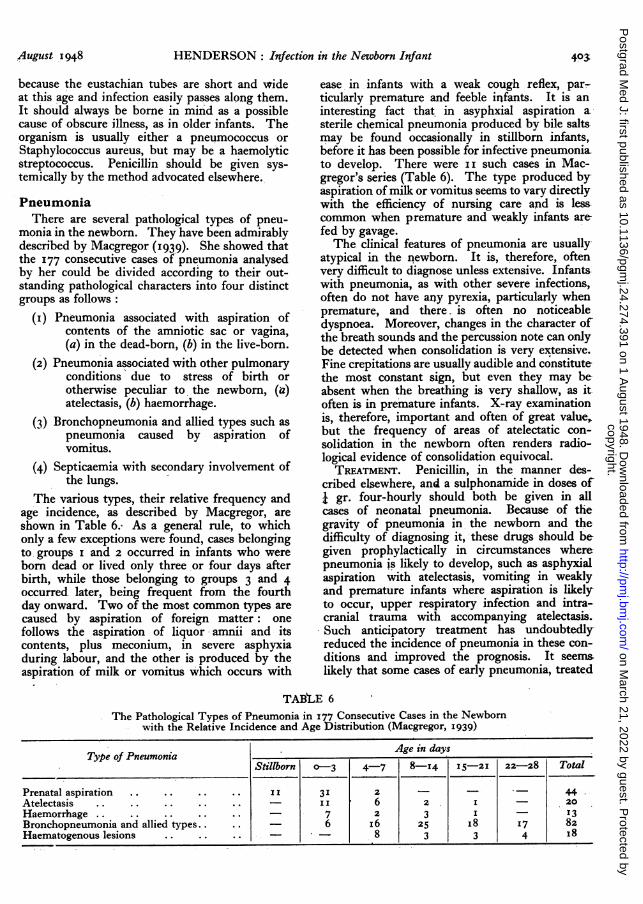
PneumoniaThere are several pathological types of pneu-
monia in the newborn. They have been admirablydescribed by Macgregor (1939). She showed thatthe 177 consecutive cases of pneumonia analysedby her could be divided according to their out-standing pathological characters into four distinctgroups as follows:
(i) Pneumonia associated with aspiration ofcontents of the amniotic sac or vagina,(a) in the dead-born, (b) in the live-born.
(2) Pneumonia associated with other pulmonaryconditions due to stress of birth orotherwise peculiar to the newborn, (a)atelectasis, (b) haemorrhage.
(3) Bronchopneumonia and allied types such aspneumonia caused by aspiration ofvomitus.
(4) Septicaemia with secondary involvement ofthe lungs.
The various types, their relative frequency andage incidence, as described by Macgregor, areshown in Table 6. As a general rule, to whichonly a few exceptions were found, cases belongingto groups i and 2 occurred in infants who wereborn dead or lived only three or four days afterbirth, while those belonging to groups 3 and 4occurred later, being frequent from the fourthday onward. Two of the most common types arecaused by aspiration of foreign matter: onefollows the aspiration of liquor amnii and itscontents, plus meconium, in severe asphyxiaduring labour, and the other is produced by theaspiration of milk or vomitus which occurs with
ease in infants with a weak cough reflex, par-ticularly premature and feeble infants. It is aninteresting fact that. in asyphxial aspiration asterile chemical pneumonia produced by bile salts-may be found occasionally in -stillborn infants,before it has been possible for infective pneumoniato develop. There were i i such cases in Mac-gregor's series (Table 6). The type produced byaspiration of milk or vomitus seems to vary directlywith the efficiency of nursing care axid is less,common when premature and weakly infants arefed by gavage.The clinical features of pneumonia are usually
atypical in the newborn. It is, therefore, oftenvery difficult to diagnose unless extensive. Infants.with pneumonia, as with other severe infections,often do not have any pyrexia, particularly whenpremature, and there- is often no noticeabledyspnoea. Moreover, changes in the character ofthe breath sounds and the percussion note can onlybe detected when consolidation is very extensive.Fine crepitations are usually audible and constitutethe most constant sign, but even they may be-absent when the breathing is very shallow, as itoften is in premature infants. X-ray examinationis, therefore, important and often of great value,but the frequency of areas of atelectatic con-solidation in the newborn often renders radio-logical evidence of consolidation equivocal.TREATMENT. Penicillin, in the manner des-
cribed elsewhere, and a sulphonamide in doses ofj gr. four-hourly should both be given in allcases of neonatal pneumonia. Because of thegravity of pneumonia in the newborn and thedifficulty of diagnosing it, these drugs should begiven prophylactically in circumstances wherepneumonia is likely to develop, such as asphyxialaspiration with atelectasis, vomiting in weaklyand premature infants where aspiration is likelyto occur, upper respiratory infection and intra-cranial trauma with accompanying atelectasis.Such anticipatory treatment has undoubtedlyreduced the incidence of pneumonia in these con-ditions and improved the prognosis. It seems.likely that some cases of early pneumonia, treated
TABtLE 6
The Pathological Types of Pneumonia in I77 Consecutive Cases in the Newbornwith the Relative Incidence and Age Distribution (Macgregor, I939)
Type of Pneumonia Age_in daysStillborn o-3 4-7 8-14 15-21 22-28 Total
Prenatal aspiration .. .. .. .. I 3I 2 - 44.Atelectasis I.. .. .. .. .. - I 6 2 I 20Haemorrhage .. .. .. .. .. 7 2 3 I 13Bronchopneumonia and allied types. .. 6 i6 25 I8 I7 82Haematogenous lesions .. .. .. - - 8 3 3 4 I8
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from

404 POST GRADUATE MEDICAL JOURNAL August I948
with these drugs, now recover. Oxygen shouldbe given if there is any cyanosis.
OmphalitisSerious umbilical infection is now very un-
common, thanks to the strict aseptic techniquepractised when dressing the cord and umbilicus.Tetanus neonatorum is now extremely rare exceptin backward communities. The most dangerousinfection under modem conditions is haemolyticstreptococcal infection of the umbilical stump inthe first few days, as the infection may enter thecirculation before the vascular channels havebecome thrombosed. This rarely occurs andlocal omphalitis, occasionally complicated by peri-umbilical cellulitis, is the type most often seennowadays. Haemolytic streptococci and Staphy-lococcus aureus, often in combination, are theprincipal causes of acute local infection. Treat-ment consists of the application of penicillinpowder locally and the administration of penicillinorally, giving 20,000 units in each feed.
Mild infection of the unhealed umbilicus oftenoccurs after separation of the cord, particularlywhen separation of a thick cord leaves a large rawarea. In such circumstances, there is a slight sero-purulent discharge and a reactive excrescence ofgranulation tissue usually develops. The friabilityof the latter may cause a few drops of blood tocontaminate the discharge occasionally in a smallproportion of cases. The infection is usually lowgrade and mixed in these circumstances, buthaemolytic streptococci and Staphylococcus aureus*often play a part, and the relatively indolent lesion-tends to persist for a few weeks if untreated. Theexcrescence seems to be the chief cause of suchpersistence, for once it is removed complete heal-ing occurs spontaneously in a couple of days.Treatment in the earlier days consists of washingand drying the umbilicus thoroughly twice a dayand then dusting it with penicillin powder. When-a polypus is found it should be removed as soon aspossible, by torsion with Alliss' forceps if verysmall, by ligation and strangulation if pedun-,culated and by repeated cauterization with coppersulphate if sessile.
PeritonitisThis uncommon infection is most often a com-
plication of omphalitis, but it may be a manifesta-tion of septicaemia, or complicate alimentarydisease, such as untreated volvulus or other causeof unrelieved obstruction, or a perforationassociated with enteritis, colitis or faulty surgical-technique.
SepticaemiaThis is uncommon, but by no means rare. It
may be the only manifestation of infection or beassociated with infection elsewhere, such asstaphylococcal dermatitis or omphalitis. It isusually either streptococcal or staphylococcal.
Infants with septicaemia usually have a highremittent temperature, but may have none,especially if premature. Embolic manifestations,such as skin abscesses and osteomyelitis, mayoccur. The diagnosis is established by bloodculture. If blood culture were performed muchmore often in ill infants with no local signs ofdisease, septicaemia would be found to be morecommon than many at present suppose. Promptchemotherapy gives a reasonable chance ofrecovery.
MeningitisNeonatal meningitis is not uncommon. The
most common cause is B. coli, yet this type isvirtually unknown after the first month or two oflife. This remarkable phenomenon is no doubta manifestation of the peculiar immunologicalcharacteristics of the newborn. Craig (1936) inhis series of 2I cases found B. coli in 14 cases, theinfection being mixed in four of them. Nextcame Staphylococcus aureus with six cases, twobeing mixed, then Streptococcus viridans withthree cases. A pneumococcus, haemolytic strep-tococcus and an atypical salmonella were eachfound once. Meningitis is usually part of ageneralized septicaemia, but one cannot alwaysdetermine whether infection arose from haemato-genous spread or by direct extension from a localfocus. There is a greater tendency for it to occurin infants with local infections, particularly of thenasopharynx and mouth.The classical signs of meningitis are often
absent. Signs of intracranial disturbance arisingafter the first week of life should always suggest it;ocular signs, increased tension of the fontanelleand mental restlessness are the -most common.Fever may not occur, especially in prematureinfants, but is usual in advanced cases. Convul-sions are rare.
Diagnosis is by lumbar puncture and cerebro-spinal fluid features. Treatment depends on thecausal organism, and since B. coli is the mostcommon cause a sulphonamide is usually in-dicated in doses of 4 gr. four-hourly. If noorganism is found, penicillin should also be given.Recovery usually occurs with prompt treatment.Hydrocephalus is a not uncommon complication,so the cranial circumference should be watchedby daily measurement.
PyelitisThis acute infection is relatively uncommon,
and is practically always caused by B. coli. There
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from

August I948 HENDERSON: Infection in the Newborn Infant 405
seems to be no definite sex incidence at this age.The principal clinical features are high remittentfever, irritability and thirst, while convulsions mayoccur. Recurrent circulatory collapse, with pallorand a sub-normal temperature, are regarded asvery suggestive of this disease in young infants.
Examination of the urine, which should beobtained with the aid of a test-tube in a male andby catheter in a female, will confirm the diagnosis.Treatment is along the usual lines. Abundantfluid, with alkalinization of the urine, which mayrequire the administration of as much as onedrachm of sodium citrate in the first day or two,and i gr. of sulphamezathine, four-hourly, willsoon effect improvement.The prognosis is very good. When relapse
occurs, especially more than once, the possibilityof a congenital abnormality of the tract causingstagnation of urine should be considered, and ifpossible eliminated, since malformations are acommon cause of urinary tract infection in infants.
Congenital SyphilisIt is unusual for congenital syphilis to reveal
itself in the first month of life. When it does themost common manifestation is snuffles withprofuse sanguineo-purulent rhinorrhoea. Skinmanifestations may be observed as early as thefirst few days, particularly scaly exfoliation of theskin of the soles and the appearance of reddish ormilky macules which soon develop a bronze tint.Splenomegaly and hepatomegaly can be demon-strated in the more seVere cases, but are usuallymissed until other manifestations appear. Thereis a variable degree of anaemia and it is oftenaccompanied by erythroblastaemia. Muco-cutaneous lesions are uncommon in the firstmonth. Roentgenography of the skeleton mayshow characteristic osteochondritis. It is usuallypresent at birth, but may not be seen for severalmonths. Chondroepiphysitis is the most commonlesion, but periostitis is also frequently seen. Thegeneral condition of infants with manifest con-genital syphilis in the first month is good, as arule, but it may be indifferent or poor, andoccasionally death may occur before any effectivetreatment can be given.The placenta in congenital syphilis may not
look remarkable on cursory examination, but insevere cases it has a pale pink colour, and anincreased thickness and weight. Infarction inthe form of multiple small infarcts, which may bemissed on superficial examination, are a constantfeature, but large infarcts are often found whenintra-uterine death occurs. In erythroblastosiswith hydrops foetalis or maceration the placenta ismuch larger and paler than in syphilis. Histo-logically thickening and clubbing of the villi, and
diminished vascularity with obliterating endar-teritis and perivascular fibrosis are the principalfeatures. The spirochaeta paliida may not bedemonstrable in fresh placental tissue in which itis much more difficult to find than in macerate4tissue.The mother's Wassermann and Kahn tests are
positive in a high proportion of cases, but mayoccasionally be negative. The infant's serologicaltests are unreliable in the first few months beca,useof the immunological peculiarities of the newborninfant which have been discussed elsewhere.TREATMENT. The introduction of penicillin has
revolutionized and simplified treatment. The fol-lowing is an outline of current therapeutic practicein the Department of Venereal Diseases, Edin-burgh Royal Infirmary:
(i) The infant of a mother who has been treatedin pregnancy and has a negative Wassermannreaction at parturition is given a course of 300,000units of penicillin, receiving eight three-hourlyinjections of 5,000 units per day. Mother andchild are examined at three-monthly intervals forthe next two years and no failures have yet beenencountered.
(2) The infant of a mother who has been treatedin pregnancy and has a positive Wassermannreaction at parturition is given a course of i ,000,000units of penicillin, receiving eight injections of5,000 units on the first day of treatment, eightinjections of io,ooo units on the second day andeight injections of 20,ooo units on the third andsubsequent days. A weekly injection of arsenicand bismuth for a period of ten weeks is also givento the infants in this category, as complete curewas not being obtained in all cases treated withpenicillin alone.
(3) The infant of a mother who has not receivedany treatment is given a course of 2,000,000 unitsof penicillin along the lines detailed above. Alsoa course of arsenic and bismuth as recommendedin category 2.
General Measures to Reduce the Incidenceof Neonatal InfectionsImproved. social and hygienic standards and a
strengthening of aseptic technique have steadilyreduced the incidence of infection in the newborn,but much more could be done to safeguard infantsfrom the risks of infection in the newborn period.The following reforms would all contribute
towards a further reduction in the incidence ofneonatal infection:
(i) Improvement in the general health standardand physique of the people through the attainmentof more universally satisfactory economic andsocial standards, particularly better housing cmn-ditions and nutrition.
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from

406 POST GRADUATE MEDICAL JOURNAL August 1948
(2) More universal and thorough supervision ofthe expectant mother, with special emphasis onan optimum diet.
(3) Much more widespread and attractivemothercraft teaching and propaganda throughmothercraft clinics, films and publications. Thisshould be directed particularly to women expectingtheir first child.
(4) A general raising of obstetrical standards,with a reduction in the number of complicatedand prolonged labours which often predispose toinfection.
(5) A reversal of the trend towards confine-ment in maternity hospitals which, though some-times of advantage to the mother, greatly enhancesthe possibility of the baby contracting an infection.
(6) More rigid precautions against introductionof infection to maternity units by adults. Nursesparticularly should report the commencement ofany infection such as a cold, diarrhoea or skininfection immediately, and be debarred from workin a maternity unit for as long as there is anydanger of spreading infection.
(7) More enlightened up-to-date planning ofmaternity hospitals to diminish the risk of cross-infection among infants, by adopting a policy ofdispersal, in small units of one to four beds, withtheir mothers, rather than crowding them intosmall nurseries as usually practised at the presenttime.
(8) Better teaching of medical students andpost graduates and of nurses, midwives and healthvisitors in the physiology and care of the' newborn,and particularly in the clinical features, epidemi-ology and prevention of infections.
(g) A more adequate establishment of ex-perienced senior nursing staff and enough pupilnurses to ensure a high standard of nursing at alltimes.
(io) A reversal of the most regrettable declinein the incidence of breast feeding.
(ii) The provision of greatly improved childwelfare services in every locality, particularly agreat increase in the number of well-trained health
visitors, who constitute the backbone of theservice.
In the section on epidemiology of staphylococcalinfections I have discussed the principal bac-teriological and nursing measures which arenecessary to minimize the incidence of staphy-lococcal infections in a maternity unit. Theseprinciples apply to the control of all forms. ofinfection in the newborn. A detailed account ofthe measures necessary to prevent cross-infectionin maternity hospitals has recently been writtenby Ludlam (I947) in his excellent publication on'The Bacteriology and Epidemiology of Infectionsof Early Infancy.' The Medical Research Councilpublication (I944) on the ' Control of CrossInfection in Hospitals,' and the Department ofHealth for Scotland publication (1947) on ' Neo-natal Deaths Due to Infection' contain muchvaluable information and advice about the controlof infection in infancy and childhood.
BIBLIOGRAPHYBENIANS, T. H. C. (I923), Brit. Med. ., I, 623BUTLER, A. M., and TALBOT, N. B. (ig44), New. Engi. J7. Med.,
23I, 585, 62I.CHAPMAN, G. H., LIEB, C. W., BERENS, C., and CURCIO,
L. G. (I9V7), J. Bact., 33, 533.CRAIG, W. S. (1936), Arch. Dis. Childh., iI, I7I.DARROW, D. C. (1946), J. Pediat., 28, 515.Department of Health for Scotland, Report of the Scientific Ad-
visory Committee (I947), 'Neonatal Deaths Due to Infection.'GALE, E. F. (1944), Lancet, I, 567.GOVAN, C. D., and DARROW, D. C. (1946), J. Pediat., 28, 541.GREGG, N. M. (1942), Trans. Ophth. Soc. Austral., 3, 35.HENDERSON, J. L. (i943), Brit. Med. J., I, 410.HENDERSON, J. L. (i947), Practitioner, I58, 83.HENDERSON, J. L., and McADAM, I. W. J. (1946), Lancet, I,
922.KNOTT, F. A., and BLAIKLEY, J. B. (I944), J. Obstet. Gynaec.,
52, 386.LIGHT, J. S., and HODES, H. L. (I943), Am. J7. Pubi. Hlth., 33,
145I.LUDLAM, G. B. (I947), Health Bulletin issued by the Chief
Medical Officer of the Department of Health for Scotland, 5,40, 49, 79. ' Bacteriology and Epidemiology of Infections ofEarly Infancy.'
LUDLAM, G. B., and HENDERSON, J. L. (1942), Lancet, I, 64.McCLURE, W. B. (I943), J. Pediat., 22, 6o.MAcGREGOR, A. R. (I939), Arch. Dis. Childh., 14, 323.MAcGREGOR, A. R., and HENDERSON, J. L. (I943), Arch. Dis.
Childh., Ig, I86.Medical Research Council, War Memorandum No. 1I (I944), 'The
Control of Cross Infection in Hospitals.'TODD, R. L. (I937), Am. J. Hyg., 25, 212.
RUTHI CASTLE@|, NORTH WALES---
A Clinic for the diagnosis and treatment of Internal Diseases (except Mental or Infectious Diseases). TheClinic is provided with a staff of doctors, technicians and nurses.
The surroundings are beautiful. The climate is mild. There is central heating throughout.' The annualrainfall is 30.5 inches, that is, less than the average for England-.
The Fees are inclusive and vary according to the room occupied.
For particulars apply to THE SECRETARY, Ruthin Castle, North Wales.
Teleirams: CIle, Ruthin. Telephone: Ruthin6
copyright. on M
arch 21, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.274.391 on 1 A
ugust 1948. Dow
nloaded from
Related Documents











