Infection Control of Aerosol Transmissible Diseases

Infection Control of Aerosol Transmissible Diseases.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Infection Control ofAerosol Transmissible Diseases
Overview Transmission of Communicable Diseases
Principles of Infection Control
Application to Aerosol Transmissible Diseases (ATDs)
Interactive exercises
Resources in packet
The Chain Model of Communicable Diseases
• Infectious agent
• Reservoirs and/or sources
• Portals of exit
• Modes of transmission
• Portals of entry
• Susceptible hosts
The Chain Model of Communicable Diseases• Infectious agent
• Reservoirs and/or sources– human– animal– Environment
• Portal(s) of exit:– Respiratory tract– GI tract– Genital/urinary tract– Breaks in skin
The Chain Model of Communicable Diseases
• Modes of transmission– Direct contact– Indirect contact
• Portals of entry
• Susceptible hosts
Modes of Transmission
• Direct Transmission
Direct Contact Droplet
• Indirect Transmission
Vehicle-borne Vector-borne Airborne
• Vertical transmission (mother to infant)
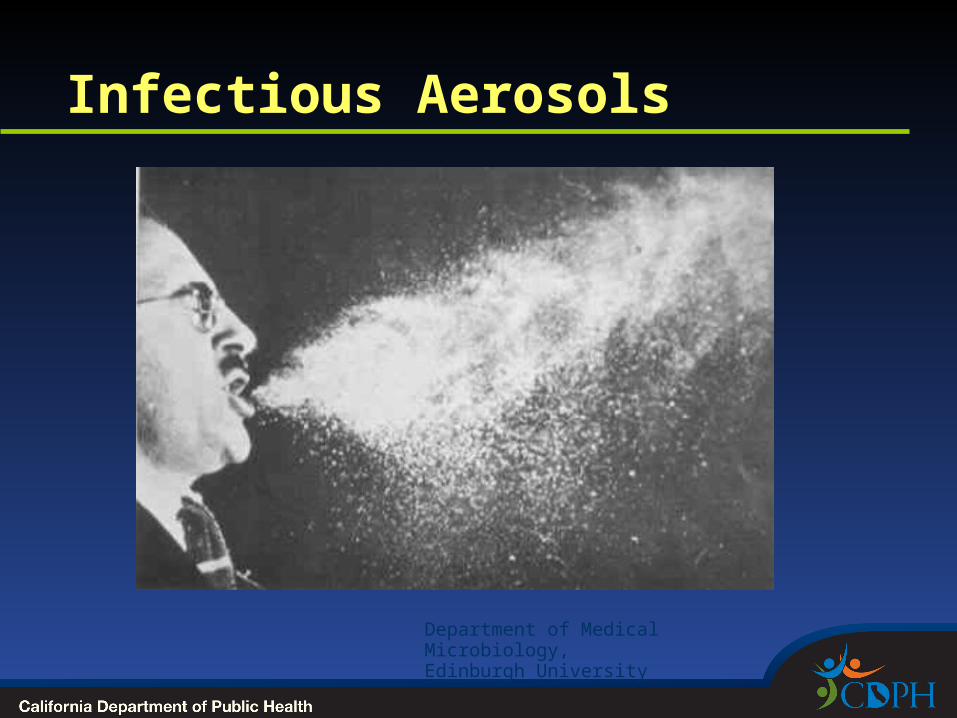
Infectious Aerosols
Department of Medical Microbiology,Edinburgh University
Transmission of Infections by Respiratory Aerosols• Droplets: land directly on mucosal lining of nose,
mouth, eyes of nearby persons or can be inhaled.• Highest exposures within 3-6 feet.
• Airborne: aerosols become smaller by evaporation; small aerosols (≤ 10 microns) remain suspended for longer periods, if inhaled travel deep into the lungs.
• Contact: Aerosols/ secretions contaminate nearby surface. Touch surfaces can infect self or others.
Relative contribution of three routes varies with agent.
Modes of Transmission viaInfectious Respiratory Secretions• Airborne: tuberculosis, measles, varicella,
smallpox, SARS, avian influenza
• Droplet: meningococcal meningitis, rubella, pertussis, common cold, SARS, influenza*
• Indirect contact: (fomite) RSV, SARS
*Influenza traditionally droplet, increasing evidence for airborne component
Infection Control in aHealth Care Setting
Review
Infection Control in a Health Care Setting
• Basic principles
• Standard precautions
• Transmission-based precautions
• Seasonal influenza in health care settings
• Vaccination of HCWs
• TB screening of HCWs
• Proper donning and doffing
• Choose your PPE
Basic Principles • All body fluids are potentially infectious
(except sweat)
blood and blood-tinged fluids including open-wounds stool, urine, vomit, respiratory secretions, saliva,
semen, vaginal secretions, breast milk, other body fluids such as pericardial and synovial fluids
• Minimize exposure to potentially infectious body fluids
• Infection control measures designed to “break the chain” of transmission

Standard Precautions in Health Care Settings
1. Appropriate hand hygiene
2. Barrier protective equipment:
if splash, splatter, or sprays can be reasonably anticipated
choose appropriate PPE as needed: gloves, gown, mask, eye protection (face shield, goggles)
3. Proper use and handling of patient care equipment
Standard Precautions in Health Care Settings
4. Proper environmental cleaning and disinfection
5. Proper Handling of Linen
6. Adherence to Bloodborne Pathogens Standards
7. Proper patient placement
8. Respiratory Hygiene/Cough Etiquette
9. Safe injection practices
Expanded Isolation Precautions:Transmission-based Standards
When standard precautions are not enough
Additional measures based on mode of transmission
Contact Precautions Droplet Precautions Airborne Precautions
Transmission-Based Precautions: Contact Precautions
For known or suspected infections that represent an increased risk of spread by direct or indirect contact with the patient or the patient’s environment
Transmission-Based Precautions: Contact Precautions
Personal Protective Equipment
Gown & Gloves for all patient interactions
Don PPE on entry, discard before exiting room. (in addition to Standard Precautions)
Examples: MRSA, C difficile, Norovirus, other GI pathogens, RSV, antibiotic-resistant pathogens
Transmission-Based Precautions: Droplet Precautions Single room preferred, no special
ventilation
Patient: Mask if transport necessary. Instruct on respiratory hygiene/cough etiquette
HCWs wear surgical or procedure mask within 6 feet of patient. Eye protection if splash, spray anticipated (in addition to Standard Precautions)
Transmission-Based Precautions: Airborne Precautions
Airborne Infection Isolation Room (AIIR) if available
Patient: Mask if transport necessary (as tolerated).
Health care workers (HCWs):
N95 respirator prior to entry into room, discarded after exit. Higher level respirators for aerosol-gen procedure. Careful attention
to proper putting on & taking off (don/doff) respirator, including seal check.
Hand hygiene before & after don/doff. Alert others if need to transfer
(in addition to Standard Precautions)
Seasonal Influenza in Healthcare Settings
• CDC and CDPH guidelines updated 2010
• Multi-faceted approach
Flu vaccine for HCWs Implementation of respiratory hygiene and
cough etiquette HCWs with ILI stay home Source Control
Seasonal Influenza in Healthcare Settings: Isolation Precautions• Droplet precautions for all patients with
suspect influenza (ILI)
ILI Temp >37.8 C (100 F) plus new cough or sore throat
Ideally, place patients in single room Surgical mask for close patient contact
• Employer may allow N95 during routine care as option
Patient should be transported with surgical mask.
Seasonal Influenza in Healthcare Settings: Isolation Precautions• For aerosol-generating procedures: N95
respirator + standard precautions (gown, gloves, goggles for spray/splash)
• Aerosol generated procedures
Sputum induction, bronchoscopy, elective intubation and extubation, autopsies
CPR, emergent intubation, open suctioning of airways
Vaccination of HCWs
• Protect patients, protect yourself and other HCWs
• CDC recommends
Measles, mumps, rubella (MMR): vaccinate unless documentation of immunity or previous vaccination
Varicella: vaccinate unless documentation of immunity or previous vaccination
Tdap
Yearly influenza vaccination
Hepatitis B: vaccinate unless documentation of previous vaccination

Vaccination of HCWs
• Cal/OSHA ATD & Bloodborne Pathogen Standard
Employer must offer to those who are not vaccinated or immune:
• MMR and varicella vaccination • Tdap• Seasonal influenza vaccination• Hepatitis B vaccination
No cost to employee
Employer must maintain on file: records of immunity, vaccine, or declinations
Tuberculosis Screeningfor Health Care Workers
• Title 22 and Cal/OSHA ATD Standard
• TB screening at hire and then annually for all licensed healthcare facilities in CA (e.g., acute care hospitals, skilled nursing facilities, primary care clinics)
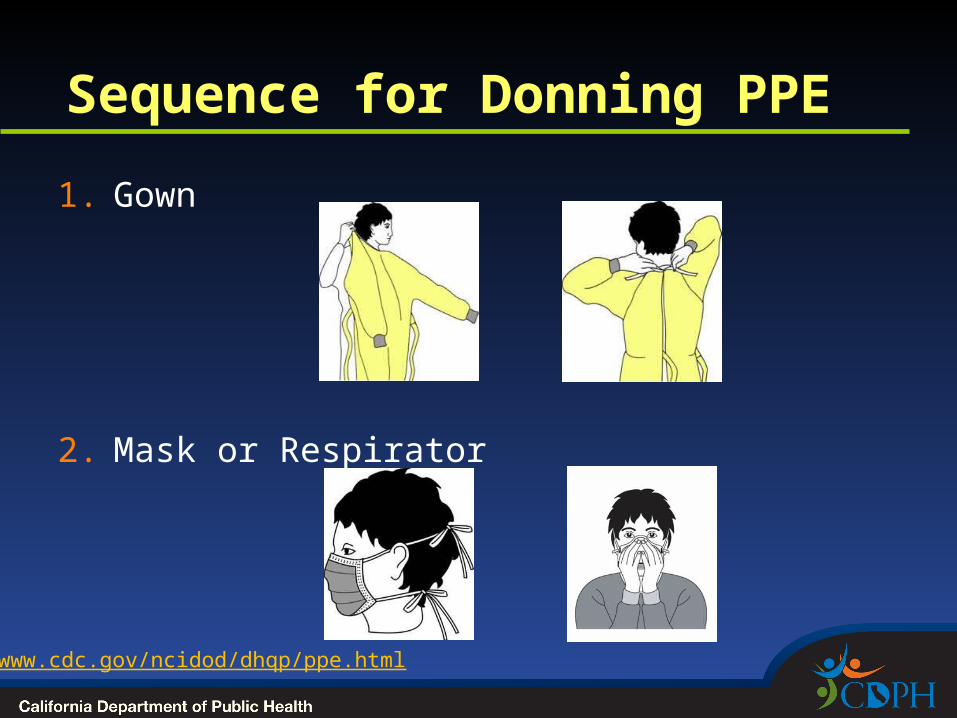
Sequence for Donning PPE
1. Gown
2. Mask or Respirator
www.cdc.gov/ncidod/dhqp/ppe.html
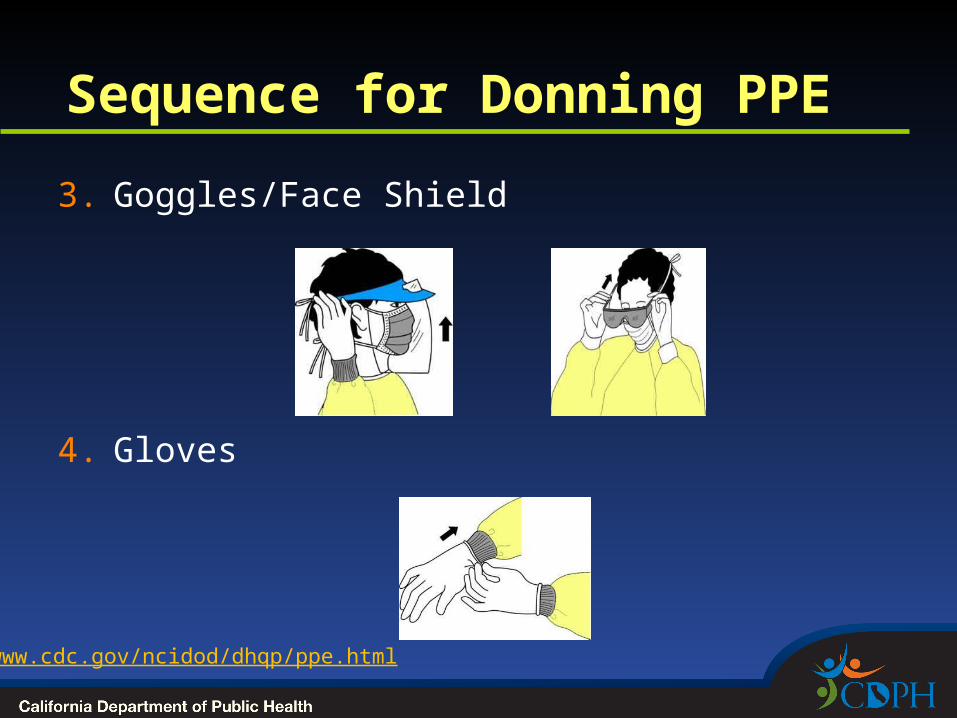
Sequence for Donning PPE
3. Goggles/Face Shield
4. Gloves
www.cdc.gov/ncidod/dhqp/ppe.html
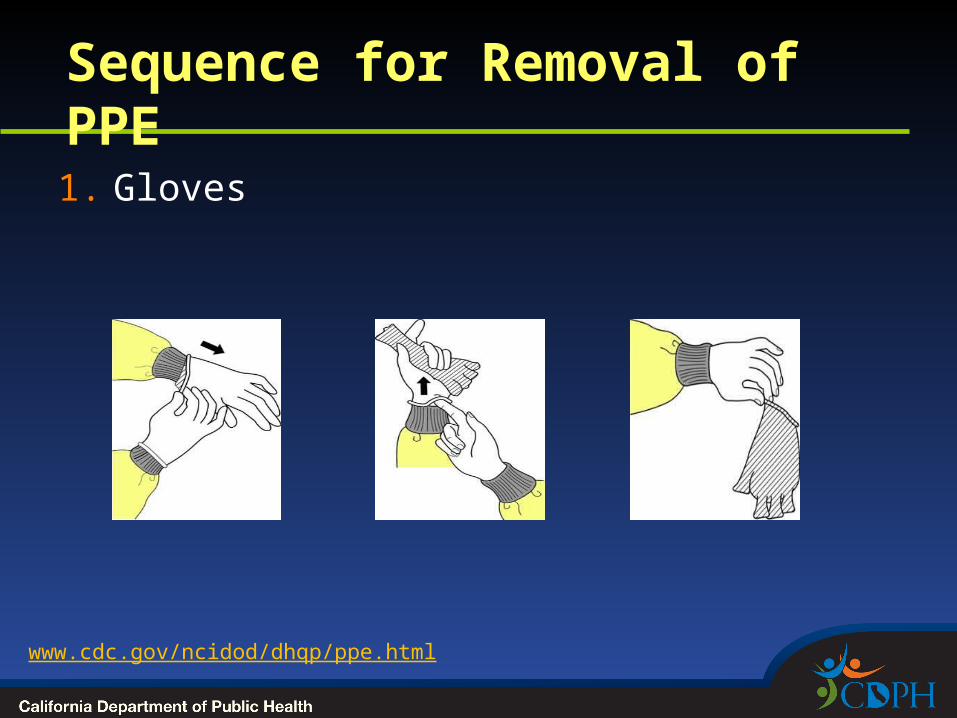
Sequence for Removal of PPE1. Gloves
www.cdc.gov/ncidod/dhqp/ppe.html
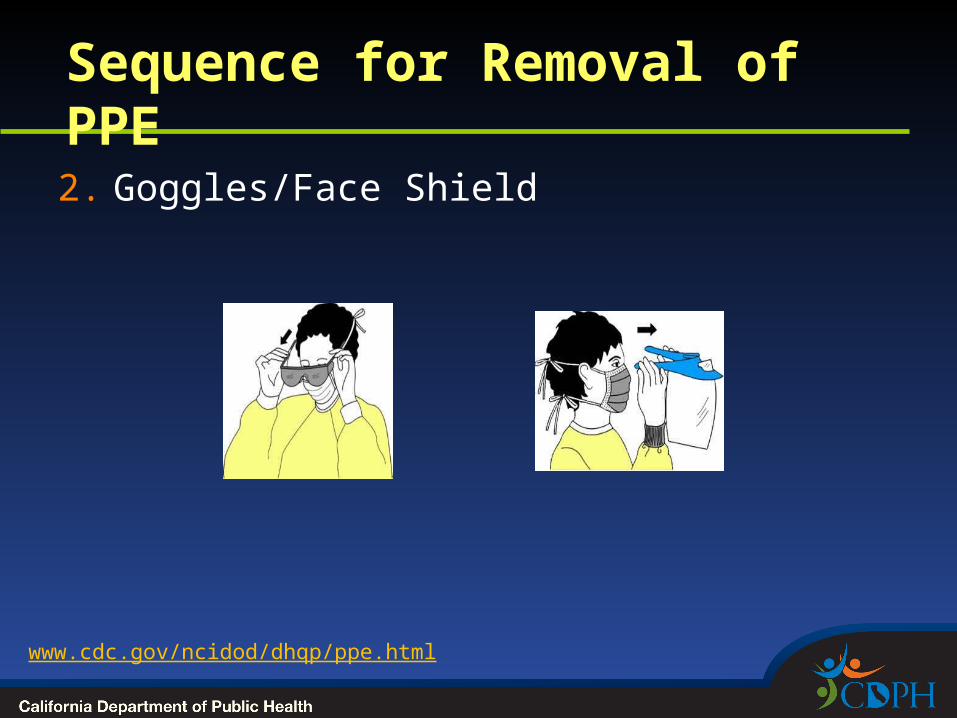
Sequence for Removal of PPE2. Goggles/Face Shield
www.cdc.gov/ncidod/dhqp/ppe.html
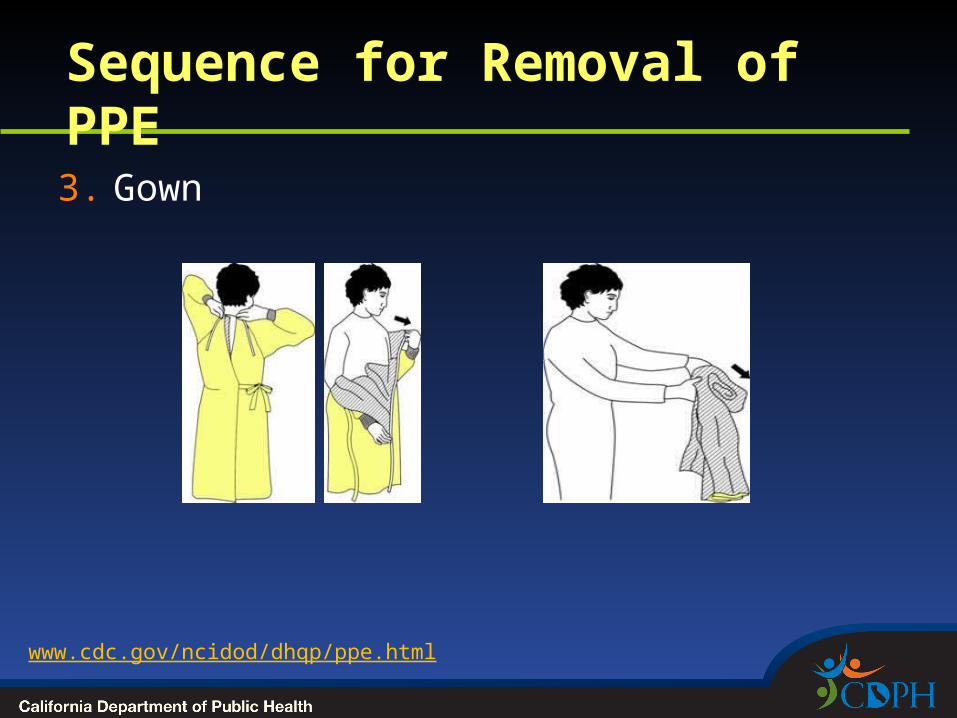
Sequence for Removal of PPE3. Gown
www.cdc.gov/ncidod/dhqp/ppe.html
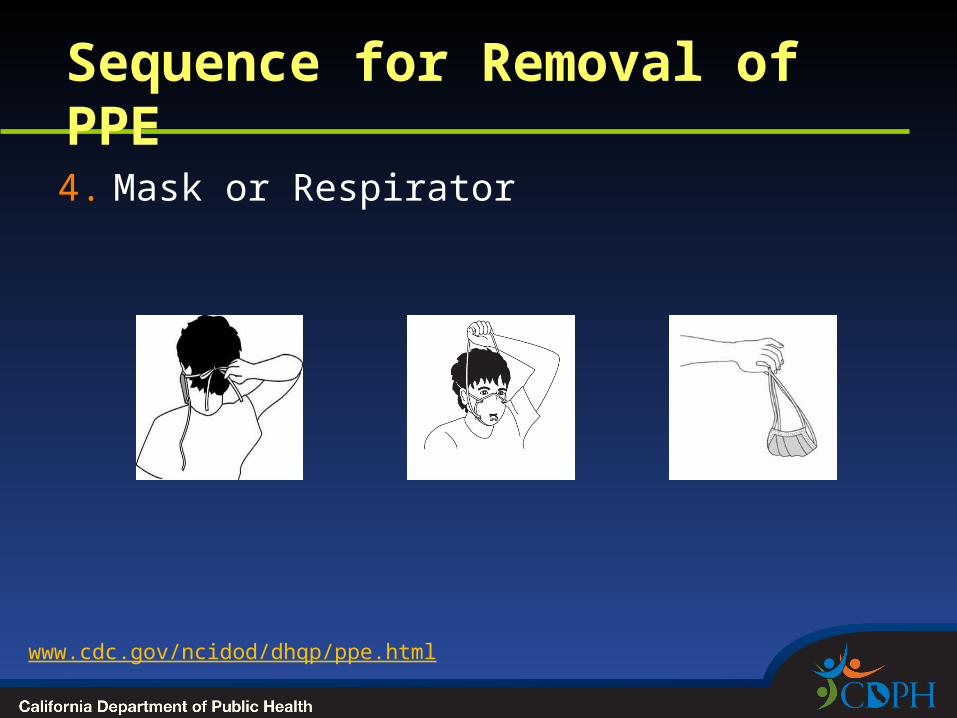
Sequence for Removal of PPE4. Mask or Respirator
www.cdc.gov/ncidod/dhqp/ppe.html
What Type of PPE Would You Wear?
• Giving a bed bath?
Generally none
• Suctioning oral secretions?
Gloves and mask/goggles or a face shield – sometimes gown
www.cdc.gov/ncidod/dhqp/ppe.html
What Type of PPE Would You Wear?
• Transporting a patient in a wheel chair?
Generally none required
• Responding to an emergency where blood is spurting?
Gloves, fluid-resistant gown, mask/goggles
www.cdc.gov/ncidod/dhqp/ppe.html
What Type of PPE Would You Wear?
• Taking vital signs
Generally none
• Drawing blood from a vein?
Gloves
www.cdc.gov/ncidod/dhqp/ppe.html
What Type of PPE Would You Wear?
• Cleaning an incontinent patient with diarrhea?
Gown, gloves
• Taking vitals on a patient with suspect TB?
N95 respirator
www.cdc.gov/ncidod/dhqp/ppe.html
Controlling the Spread of Aerosol Transmissible
Diseases in Health Care Settings
Breaking the Chain
Health care and public safety settings
• Unique challenges for control of ATDs
Diversity of job titles and duties Unique “business” of caring for the ill Societal behaviors related to caregiving Exotic and unique exposures Suspension of usual self protection behaviors Emphasis on confidentiality
Aerosol Transmissible Diseases in Health Care and Public Safety Settings
• Droplet
Meningococcal meningitis
Pertussis Mumps Rubella (German
measles) Strep pharyngitis Influenza
• Airborne
Tuberculosis Varicella
(chickenpox) Measles SARS Avian influenza Smallpox Influenza
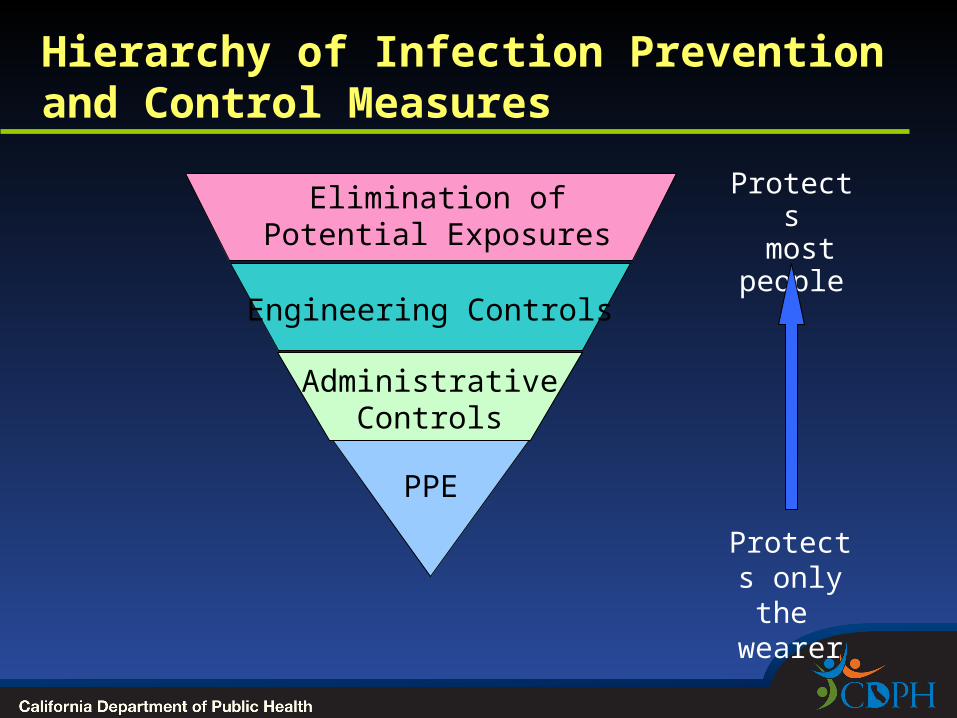
Hierarchy of Infection Prevention and Control Measures
PPE
Engineering Controls
Protects only the wearer
Elimination of Potential Exposures
Administrative Controls
Protects most
people
Hierarchy of Control Technologies
• Goal is to reduce exposures to a hazard
• Order in which these elements are selected to control exposure is important
Elimination of Potential Exposures Engineering controls Administrative and work practice controls Personal protective equipment/apparel
Elimination of Potential Exposures
• Example: patients with mild influenza like illness stay home
Engineering Controls
• Physically separates the employee from the hazard
• Does not require employee compliance to be effective
• Examples:
physical barriers at triage airborne infection isolation room for patients
with known or suspect airborne infectious diseases
Administrative Controls/ Workplace Practices
• Policies, procedures, and programs that minimize intensity or duration of exposure
Examples: • signs on door of an airborne isolation room• triage, mask symptomatic patient• provide tissues/ masks/hand sanitizer to public
• Standard procedures/ behaviors in caring for patients e.g. hand hygiene, HCW vaccination
• Only as good as enforcement
Personal Protective Equipment• Lowest level of hierarchy - requires employee
compliance for efficacy
• Means higher elements of hierarchy fail to adequately protect employee
• May involve use of gowns, gloves, eye/splash protection or respirators
• Last line of defense
Face Masks vs. N95 Respirators
• Loose fitting, not designed to filter out small aerosols
• Place on coughing patient (source control)
• HCW should wear mask to protect patient during
certain procedures (e.g., surgery, LP)
protect HCW• droplet precautions• Mask + goggles for
anticipated spray/splash
• Tight fitting respirator, designed to filter the air
• Protects the wearer
• HCW should wear when concerned about transmission by airborne route

Reasons for Respiratory Protection• Engineering controls not feasible or sufficient
• Employees must wear N95 respirators (or higher level of protection) in the following circumstances
Entering a room with patient with suspect or confirmed airborne infectious disease
When performing high-hazard (aerosol-generating) procedures on persons with suspect/confirmed airborne infectious disease or influenza
When emergency response employees/others must transport in a closed vehicle, a patient with suspect/confirmed airborne infectious disease
Aerosol-Generating Procedures• Sputum induction, bronchoscopy, elective
intubation and extubation, autopsies
• CPR emergent intubation, open suctioning of airways
What you should do when you hear Ah-choo!
• Likely communicable?
airborne vs. droplet ?
• Choose appropriate source control and PPE
• Reportable Disease? Contact local health department. Some require immediate action
Title 17 reporting requirement
Aerosol Transmissible DiseasesBreaking the Chain• Source control
stay home, isolate or separate mask patient
• Respiratory hygiene, cough etiquette
• Hand hygiene
• HCW protection
• Vaccinate• Droplet – Mask• Airborne- N95 respirator
References
• CDC
2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Healthcare Settings http://www.cdc.gov/hicpac/2007IP/2007isolationPrecautions.html
Guideline for Hand Hygiene in Health-Care Settings MMWR 2002; vol. 51, no. RR-16 http://www.cdc.gov/mmwr/PDF/rr/rr5116.pdf
References
• Cal/OSHA
Aerosol Transmissible Disease Standard http://www.dir.ca.gov/Title8/5199.html
Appendix A http://www.dir.ca.gov/Title8/5199a.html
References
• Seasonal Influenza Infection Control Guidelines 2010
CDC: http://www.cdc.gov/flu/professionals/infectioncontrol/index.htm
CDPH http://www.cdph.ca.gov/programs/immunize/Documents/CDPHGuidanceFluPreventionHCS20101105.pdf
Cal/OSHA http://www.dir.ca.gov/dosh/Cal-OSHA_influenza_guidance_11-5-10.pdf
Questions?
Related Documents











