Infection Control in hospital settings. Influenza. Piroska Orosi M.D., Ph.D Faculty of Public Health

Infection Control in hospital settings. Influenza. Piroska Orosi M.D., Ph.D Faculty of Public Health.
Dec 19, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Infection Control in hospital settings. Influenza.
Piroska Orosi M.D., Ph.D
Faculty of Public Health
Definition
• Infection prevention and control is a quality standard and is essential for the well-being and safety of patients, staff and visitors.
Infection Control Committee:
• An ICC provides a forum for multidisciplinary input, cooperation, and information sharing.
• The ICC is responsible for the planning, implementation, priorisation, and resource allocation of all matters relating to IC.
Who is the member of Infection Control Committee
• Its membership shall include representation from the medical staff, microbiology section of the laboratory, epidemiologie department, nursing services.
Infection Control Committee• The ICC gives structure, direction and
administrative power of the infection control program. During regular meetings the group serves as a review and recommendation board. Policies, protocols, and results of any survaillance programs are reviewed and recommendations are passed on to other committees, of hospital admininistration and medical staff.
The ICC reviews the following:
• Surveillance data. Any data collected on nosocomial infections in patients or employees, environmental monitoring, and the results of outbreak investigations must be reviewed by the committee.
• Policies and procedures. All departments and areas must have infection control policies and procedures, which are reviewed by the ICC and approved or modified.
• Protocols
Infection control team
• Epidemiologyst
• Microbiologyst
• Infectologyst
• Infection control nurses
The role of the Infection Control Team
• To develop an annual infection control plan.• To supervise and monitor daily practices of
patient care designed to prevent infection.• To organise epidemiological surveillance for
Healthcare-associated infections.• To investigate outbreaks.• To educate all grades of staff in IC policy,
practice and procedures.
Pathogens Important to Infection Prevention and Control
• Tuberculosis is spread by droplet nuclei in the air when somone with active diseases.
• Diagnosis is microscopy of stained smears( sputum, cerebrospinal fluid, pus).
• Isolation and prompt treatment of active cases.
• The use of N-95/FFP masks for healthcare workers.
Antibiotic Resistant Microorganisms
• Gram positive: MRSA, hVISA, VRSA, VRE
• Sreening: swab of nares, rectal, wounds
• Contact route of transmission
• Isolation precaution
• Discontinuation of precautions: 3 consecutive negative cultures taken at least one week apart in the absence of antibiotic therapy
Clostridium difficile infection
• Gram positive spore-forming, anaerob bacillus it is widely distibuted in the enviroment.The vegetative form produce toxins (ToxinA, ToxinB).
• This strain causes a severe illness colitis, diarrhoea, abdominal pain, and pseudomemrans in the gut.
• Sporocidal agents should be used for cleaning.• Soap and water are effectivein hand hygiene.
Multi-drug resistant Gram-negative microorganisms
• ESBL producing Enterobacteriaceae
• Carbapenem resistant Pseudomonas aeruginosa
• Acinetobacter species
• Patients at risk: previous antibiotic use, severe underlying illness, prolonged hospital stay
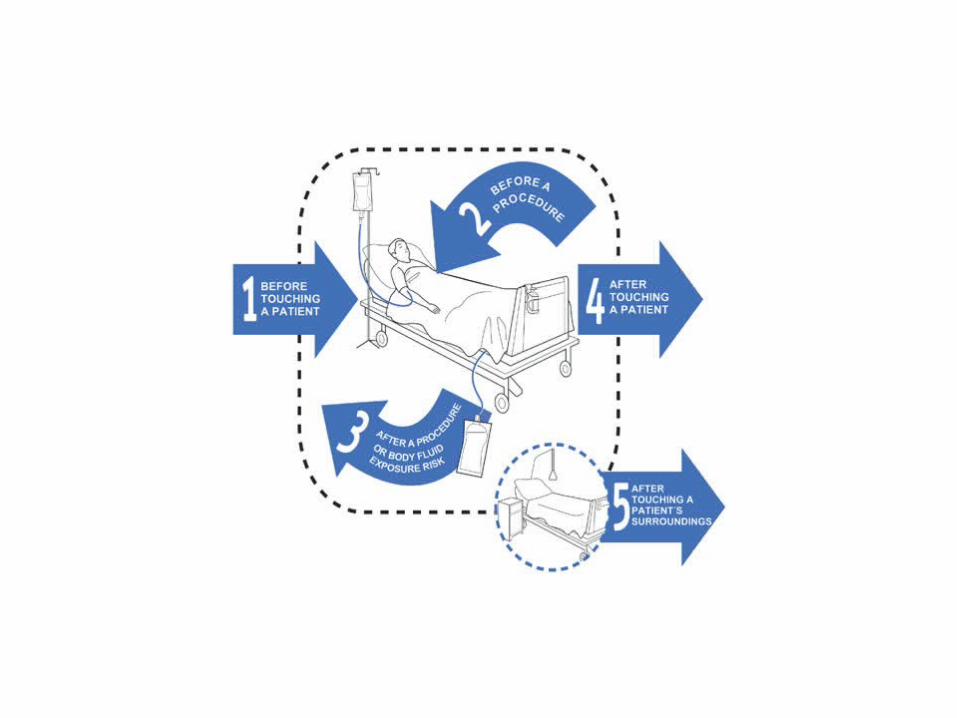
Preventive strategies of hospital-acquired infecion
• Isolation policy• Hand hygiene• Cleaning• Desinfection• Sterilization• Antibiotic profilaxis• Increasing the resistance of the recipient host
against the infectious agent
Prevention of Urinary Tract Infections
• Limit the use of invasive urinary tract procedures• Urinary catheterisation should be performed with
sterile equipment. • Aseptic maintenance of the device• The catheter should be removed as soon as
clinically possible, preferably within 5 days.• The drainage bag should be emptied once per
nursing session.
Prevention of wound infections
• Preoperative preparation of patients
• Aseptic operative process: sterilisation of instruments, aseptic technique, clean air
• Antibiotic profilaxis
• Aseptic wound care
Prevention of pneumonia
• Treat lung diseases prior to surgery, if possible.
• Elevate head of the bed.• Avoid unnecessary suctioning of airways.• Oral cavity care at least 6 times a day.
Prevention of Pneumonia
• Deep breathing and coughing exercises before and after operation.
• Percussion and postural drainage to stimulate coughing.
• Mobilise early after operation.
Prevention of bloodstream infection
• Insertion of device (sterilisation of inserted device, sterile medication, steril gloves,mask)
• Maintain a closed system. Protect the insertion site with a sterile dressing.Inspect insertion site daily.
• Remove the catheter as early as possible and immediatly if any signs of infection are present.
H7
H5
H9*
1980
1997
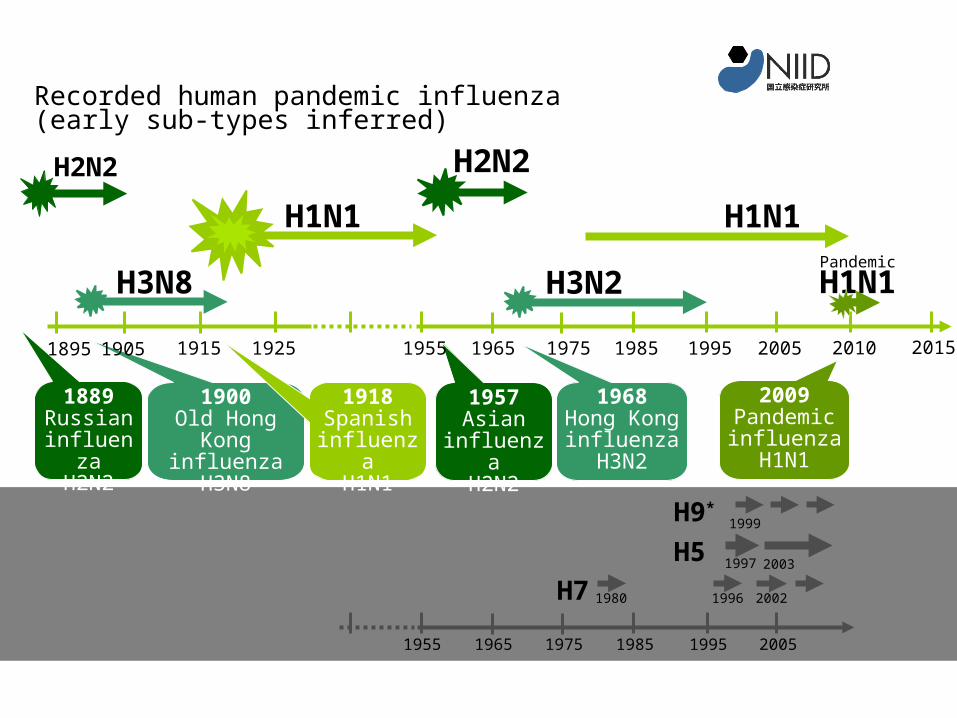
Recorded new avian influenzas
1996 2002
1999
2003
1955 1965 1975 1985 1995 2005
H1N1
H2N2
1889Russianinfluenz
aH2N2
H2N2
1957Asian
influenzaH2N2
H3N2
1968Hong Konginfluenza
H3N2
H3N8
1900Old Hong
Kong influenza
H3N8
1918Spanishinfluenza
H1N1
1915 1925 1955 1965 1975 1985 1995 20051895 1905 2010 2015
2009Pandemicinfluenza
H1N1
Recorded human pandemic influenza(early sub-types inferred)
Reproduced and adapted (2009) with permission of Dr Masato Tashiro, Director, Center for Influenza Virus Research, National Institute of Infectious Diseases (NIID), Japan.
Animated slide: Press space bar
H1N1Pandemic
H1N1
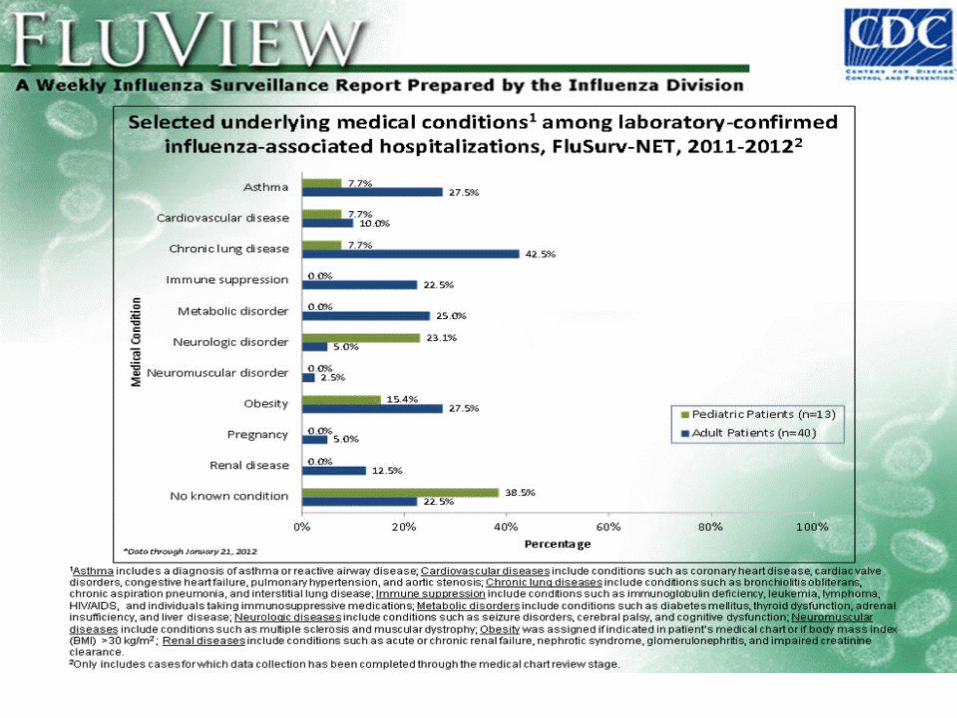
Risk groups for the lastA(H1N1) pandemic 2009
• People with chronic conditions in the following categories: – chronic respiratory diseases; – chronic cardiovascular diseases (though not isolated mild hypertension); – chronic metabolic disorders (notably diabetes); – chronic renal and hepatic diseases; – persons with deficient immunity (congenital or acquired); – chronic neurological or neuromuscular conditions; and– any other condition that impairs a person’s immunity or prejudices their respiratory (breathing)
function, including severe or morbid obesity.
Pregnant women.
• Young children (especially those under two years).
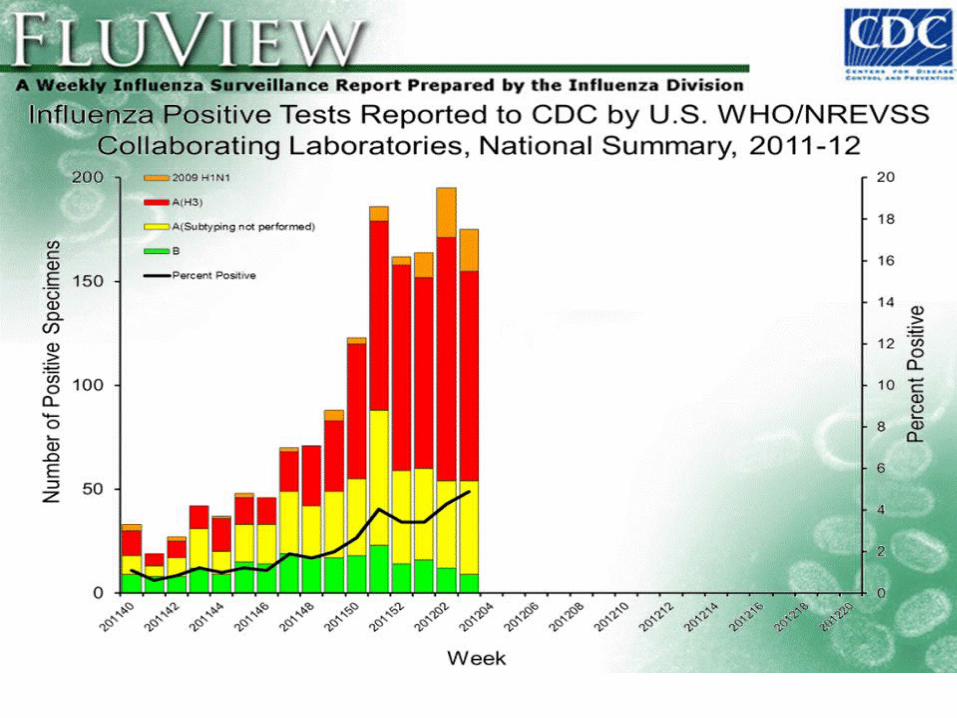
Data of influenza cases of USA in 2011/2012 influenza season
• Week 3 • No. of specimens tested 3,572 • No. of positive specimens (%) 175 (4.9%) • Positive specimens by type/subtype • Influenza A 166 (94.9%) • A (2009 H1N1) 20 (12%) • A (subtyping not performed) 45 (27.1%) • A (H3) 101 (60.8%) • Influenza B 9 (5.1%)

Impact of Influenza
• >20,000 excess deaths in each of 9 epidemics from 1972-1991
• >90% of deaths among persons 65 years of age or older
Seasonal Influenza Vaccine
• Composition: inactivated virus
trivalent(H3N2,H1N1,B)
Efficacy: Varies by similarity to circulating strain, age, underlying illnes
Duration of Immunity: <1year
Schedule: 1 dose annually
Are there other ways to prevent the spread of illness?
• Cover your nose and mouth with a tissue when you cough or sneeze. Throw the tissue in the trash after you use it.
• Wash your hands often with soap and water, especially after you cough or sneeze. If soap and water are not available, use an alcohol-based hand rub.
• Avoid touching your eyes, nose or mouth. Germs spread that way.
• Stay home if you get sick. CDC recommends that you stay home from work or school and limit contact with others to keep from infecting them.
•
Related Documents











