Practice of Epidemiology Infant Feeding Survival and Markov Transition Probabilities Among Children Under Age 6 Months in Uganda Lumbwe Chola*, Lars T. Fadnes, Ingunn M. S. Engebretsen, James K. Tumwine, Thorkild Tylleskar, Bjarne Robberstad, and the PROMISE EBF Study Group * Correspondence to Lumbwe Chola, Centre for International Health, Universityof Bergen, Box 7804, N-5020 Bergen, Norway (e-mail: [email protected]). Initially submitted February 3, 2013; accepted for publication May 7, 2012. Infant feeding studies are typically presented as single-event models, without considering the dynamic nature of feeding. We analyzed the determinants of infant feeding duration using both single- and multiple-event Cox regression models. The Cox model was compared with parametric survival models, which were used to estimate feeding-state transition probabilities. Data were taken from a community randomized trial promoting exclusive breastfeeding (EBF) in Uganda from 2005 to 2008. Peer counselors visited intervention mothers once antenatally and 4 times after birth. Results showed that children in the control group were more likely to be switched from exclusive breastfeeding (EBF)/predominant breastfeeding (PBF) to mixed feeding (MF)/replacement feeding (RF). Children in intervention clusters (hazard ratio = 0.33, 95% confidence interval: 0.26, 0.42) and rural areas (hazard ratio = 0.79, 95% confidence interval: 0.63, 0.99) had a lower risk of EBF/PBF cessation. Based on the Akaike Information Criterion, parametric models were better fitted than the Cox model. The analytical approach to assessing infant feeding duration used in this study takes into account transitions between feeding categories, allowing for multiple events. This will enhance understanding of infant feeding practices and give policy-makers a better picture of the versatility of infant feeding. breastfeeding; Markov transition; survival analysis Abbreviations: CI, confidence interval; EBF, exclusive breastfeeding; MDM, midpoint approximation method; MF, mixed feeding; PBF, predominant breastfeeding; RF, replacement feeding; SD, standard deviation. Promotion of optimal infant feeding is a global health priority because it can save the lives of approximately 1 million children annually (1). The World Health Organiza- tion recommends that infants be exclusively breastfed for 6 months and thereafter given breast milk in addition to other foods up to age 2 years (2). However, actual feeding prac- tices are dynamic, and many infants are given different types of feedings daily (3–5). In the current study, infant feeding is categorized into 4 different patterns: exclusive breastfeeding (EBF), predominant breastfeeding (PBF), mixed feeding (MF), and replacement feeding (RF) (see Table 1). Several studies have assessed the health effects of various infant feeding patterns (6–8), but few have modeled how infants might change back and forth between feeding categories. In this regard, Markov processes can be useful for analyzing infant feeding behavior, because they allow understanding of changing states over time where there is a known probability of change from one state to another (9). These changes are referred to as transition probabilities. Apart from being used in planning, feeding-state transition probabilities might add prognostic information on the long- term health status of children, since infant feeding patterns affect health outcomes (10, 11). In this study, we used longitudinal data to perform a sur- vival analysis of infant feeding and to model Markov tran- sition probabilities between feeding states among children under age 6 months in Uganda. Data were interval- censored, which is common in longitudinal studies with oc- casional follow-up, and thus we used a midpoint solution to 1 American Journal of Epidemiology © The Author 2013. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: [email protected]. DOI: 10.1093/aje/kws254 American Journal of Epidemiology Advance Access published February 5, 2013 at Universitetsbiblioteket i Bergen on February 7, 2013 http://aje.oxfordjournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Practice of Epidemiology
Infant Feeding Survival and Markov Transition Probabilities Among Children
Under Age 6 Months in Uganda
Lumbwe Chola*, Lars T. Fadnes, Ingunn M. S. Engebretsen, James K. Tumwine,
Thorkild Tylleskar, Bjarne Robberstad, and the PROMISE EBF Study Group
* Correspondence to Lumbwe Chola, Centre for International Health, University of Bergen, Box 7804, N-5020 Bergen, Norway
(e-mail: [email protected]).
Initially submitted February 3, 2013; accepted for publication May 7, 2012.
Infant feeding studies are typically presented as single-event models, without considering the dynamic nature
of feeding. We analyzed the determinants of infant feeding duration using both single- and multiple-event Cox
regression models. The Cox model was compared with parametric survival models, which were used to estimate
feeding-state transition probabilities. Data were taken from a community randomized trial promoting exclusive
breastfeeding (EBF) in Uganda from 2005 to 2008. Peer counselors visited intervention mothers once antenatally
and 4 times after birth. Results showed that children in the control group were more likely to be switched from
exclusive breastfeeding (EBF)/predominant breastfeeding (PBF) to mixed feeding (MF)/replacement feeding
(RF). Children in intervention clusters (hazard ratio = 0.33, 95% confidence interval: 0.26, 0.42) and rural areas
(hazard ratio = 0.79, 95% confidence interval: 0.63, 0.99) had a lower risk of EBF/PBF cessation. Based on the
Akaike Information Criterion, parametric models were better fitted than the Cox model. The analytical approach
to assessing infant feeding duration used in this study takes into account transitions between feeding categories,
allowing for multiple events. This will enhance understanding of infant feeding practices and give policy-makers
a better picture of the versatility of infant feeding.
breastfeeding; Markov transition; survival analysis
Abbreviations: CI, confidence interval; EBF, exclusive breastfeeding; MDM, midpoint approximation method; MF, mixed feeding;
PBF, predominant breastfeeding; RF, replacement feeding; SD, standard deviation.
Promotion of optimal infant feeding is a global healthpriority because it can save the lives of approximately 1million children annually (1). The World Health Organiza-tion recommends that infants be exclusively breastfed for 6months and thereafter given breast milk in addition to otherfoods up to age 2 years (2). However, actual feeding prac-tices are dynamic, and many infants are given differenttypes of feedings daily (3–5). In the current study, infantfeeding is categorized into 4 different patterns: exclusivebreastfeeding (EBF), predominant breastfeeding (PBF),mixed feeding (MF), and replacement feeding (RF) (seeTable 1).
Several studies have assessed the health effects ofvarious infant feeding patterns (6–8), but few have modeledhow infants might change back and forth between feeding
categories. In this regard, Markov processes can be usefulfor analyzing infant feeding behavior, because they allowunderstanding of changing states over time where there is aknown probability of change from one state to another (9).These changes are referred to as transition probabilities.Apart from being used in planning, feeding-state transitionprobabilities might add prognostic information on the long-term health status of children, since infant feeding patternsaffect health outcomes (10, 11).
In this study, we used longitudinal data to perform a sur-vival analysis of infant feeding and to model Markov tran-sition probabilities between feeding states among childrenunder age 6 months in Uganda. Data were interval-censored, which is common in longitudinal studies with oc-casional follow-up, and thus we used a midpoint solution to
1
American Journal of Epidemiology
© The Author 2013. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of
Public Health. All rights reserved. For permissions, please e-mail: [email protected].
DOI: 10.1093/aje/kws254
American Journal of Epidemiology Advance Access published February 5, 2013 at U
niversitetsbiblioteket i Bergen on February 7, 2013
http://aje.oxfordjournals.org/D
ownloaded from
first model infant feeding behavior using both single- andmultiple-event analysis. Single-event models, which allowonly 1-way transitions between feeding states, are commonlyused in survival analysis of infant feeding (12). However,multiple-/repeated-event models may be more suited to cap-turing feeding behavior, since infants often gravitatebetween feeding states (3–5). Second, we estimated the de-terminants of feeding duration using the Cox proportionalhazards model. Many researchers use this model in survivalanalyses, mainly because it requires few assumptions. Itassumes that covariates are multiplicatively related to thehazard rate. However, in instances where this assumptiondoes not hold, it is recommended to use parametric models,which estimate parameters more efficiently (13, 14). Third,we compared the results of the Cox model with those ob-tained from parametric survival models. We used theWeibull and exponential models, which are the only para-metric models that can be specified as either proportional
hazards or accelerated failure time models. The latterassume a linear relationship between latent survival timeand covariates. The Weibull model allows for more flexibil-ity because the associated hazard rate is not constant withrespect to time. Finally, we used the best-fitting parametricmodel to estimate transition probabilities between infantfeeding states.Data were taken from the PROMISE-EBF Study (“Pro-
moting Infant Health and Nutrition in Sub-Saharan Africa:Safety and Efficacy of Exclusive Breastfeeding Promotionin the Era of HIV”), a multicenter community randomizedtrial (http://clinicaltrials.gov/ct2/show/NCT00397150) un-dertaken in Burkina Faso, South Africa, and Uganda. Theobjective of the PROMISE-EBF trial was to promote EBFamong infants under age 6 months through maternal peersupport. The main results of this trial have been reportedelsewhere (3).
MATERIALS AND METHODS
PROMISE-EBF trial
In Uganda, the PROMISE-EBF trial was undertakenbetween 2005 and 2008 in Mbale District, situated about230 km east of the capital Kampala, with a population ofabout 400,000 (15). The study was conducted in 2 of the 7counties in the district: the urban municipality of Mbaleand the rural Bungokho County. Bungokho County sur-rounds Mbale Municipality, and the population consistsmainly of subsistence farmers. The majority are Bagisu,using Lumasaba as their main language.In the district, 24 clusters were selected if they were
along the main road leading out of Mbale or were on thefirst or second branch off the main road, had a populationof at least 1,000 inhabitants, and represented a social andadministrative unit. Clusters were stratified on the basis ofurban or rural settlement and were randomized 1:1 to eithera control group or an intervention group. Pregnant womenresiding in selected clusters were identified by community-based recruiters. Those intending to breastfeed were as-sessed for study participation. Preinclusion criteria werethat a woman provided consent, resided in the selectedcluster, was 7 months pregnant or visibly pregnant, and hadno intention to move to another community. After birth,
Table 1. Definitions of Infant Feeding Patterns in the PROMISE-
EBF Study, Uganda, 2005–2008
Infant Feeding Pattern Definition
Exclusive breastfeeding Only breast milk is given to thechild, except for medicines,vitamins, or mineralsupplements.
Predominantbreastfeeding
Breast milk is nutritionally dominantwhile being given in addition towater-based fluids, including fruitjuices, tea without milk, or oralrehydration salts.
Complementary feedingincluding breast milk(partial breastfeedingor mixed feeding)
Nonhuman milk, semisolids, orother solids are given to the childin addition to breast milk. Theterm “mixed feeding” normallyrefers to the feeding practicespecified above during the firsthalf of infancy (under 6 monthsof age).
Replacement feeding The feeding strategy employedwhen breastfeeding has beenstopped, or if the child has neverbeen given any breast milk.Exclusive replacement feedingwas defined as never havingbeen given any breast milk.
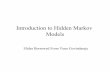
Figure 1. Markov models of infant feeding states illustrating the difference between single- and multiple-event models. A) Unidirectional modelof infant feeding transitions; B) multidirectional model of infant feeding transitions. αi = (α1, α2, α3, α4) is a set of events describing the transitionbetween feeding patterns, that is, the probability of moving from one feeding state to another. The probability α1 represents the likelihood that achild who is receiving exclusive breastfeeding (EBF)/predominant breastfeeding (PBF) in a particular month will still be receiving EBF/PBF inthe following month. α2 represents the chance that a child who is receiving EBF/PBF in a given month will be receiving mixed feeding (MF)/replacement feeding (RF) in the following month. Therefore, α1 + α2 = 1.
2 Chola et al.
at Universitetsbiblioteket i B
ergen on February 7, 2013http://aje.oxfordjournals.org/
Dow
nloaded from
preincluded mother-infant pairs were kept in the study ifthere was a single birth with no severe malformation thatcould interfere with breastfeeding. Exclusion criteria formothers were severe psychological illness, giving birth morethan a week before preinclusion, or intention to replacement-feed. The number of mother-infant pairs included in theanalysis was 396 in intervention groups and 369 in controlgroups.
In intervention clusters, mothers were visited by a peercounselor at least 5 times, once prenatally and at 1, 4, 7,and 10 weeks after birth. Women in control clusters did notreceive peer counseling but could visit standard antenatalclinics. Data collection was scheduled at 3, 6, 12, and 24
weeks postpartum. Study approval was obtained from theFaculty of Medicine of Makerere University (Kampala,Uganda), the Research and Ethics Committee of theUganda National Council for Science and Technology(Kampala, Uganda), and regional committees for medicaland health research ethics in Norway. Details of thePROMISE-EBF trial are provided elsewhere (3, 16).
Modeling infant feeding behavior
We used a 2-state Markov model to depict changesin feeding patterns (Figure 1). Children were categorizedinto 2 feeding states: exclusive/predominant breastfeeding
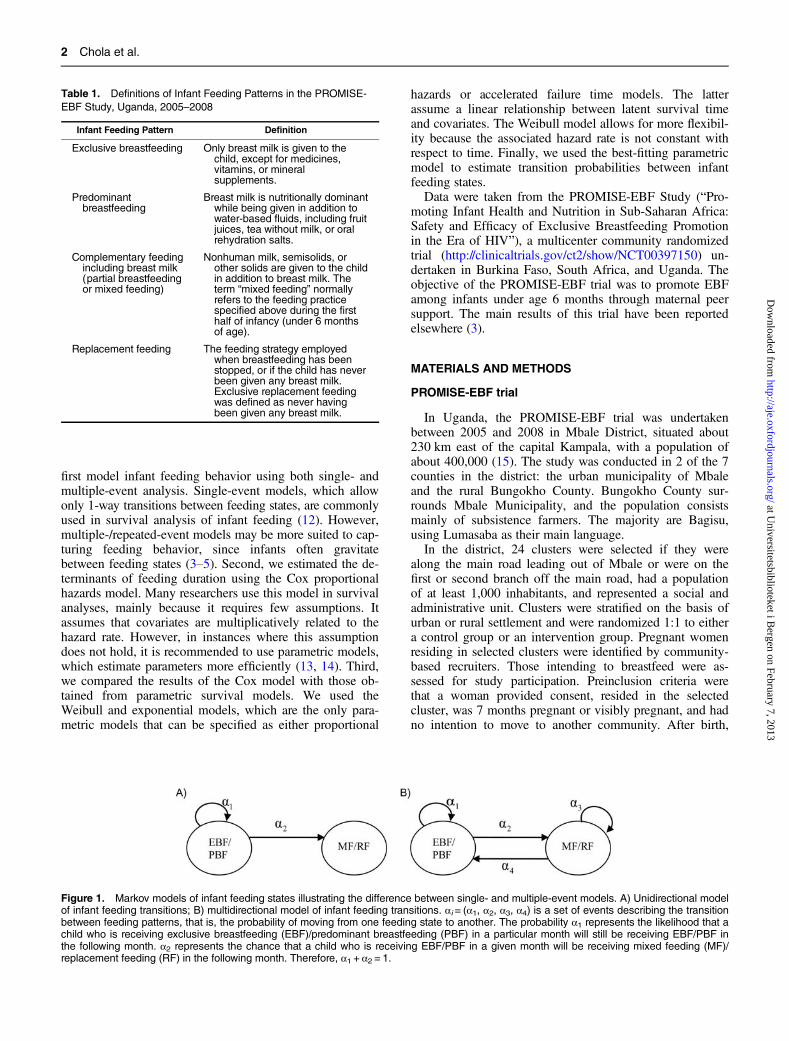
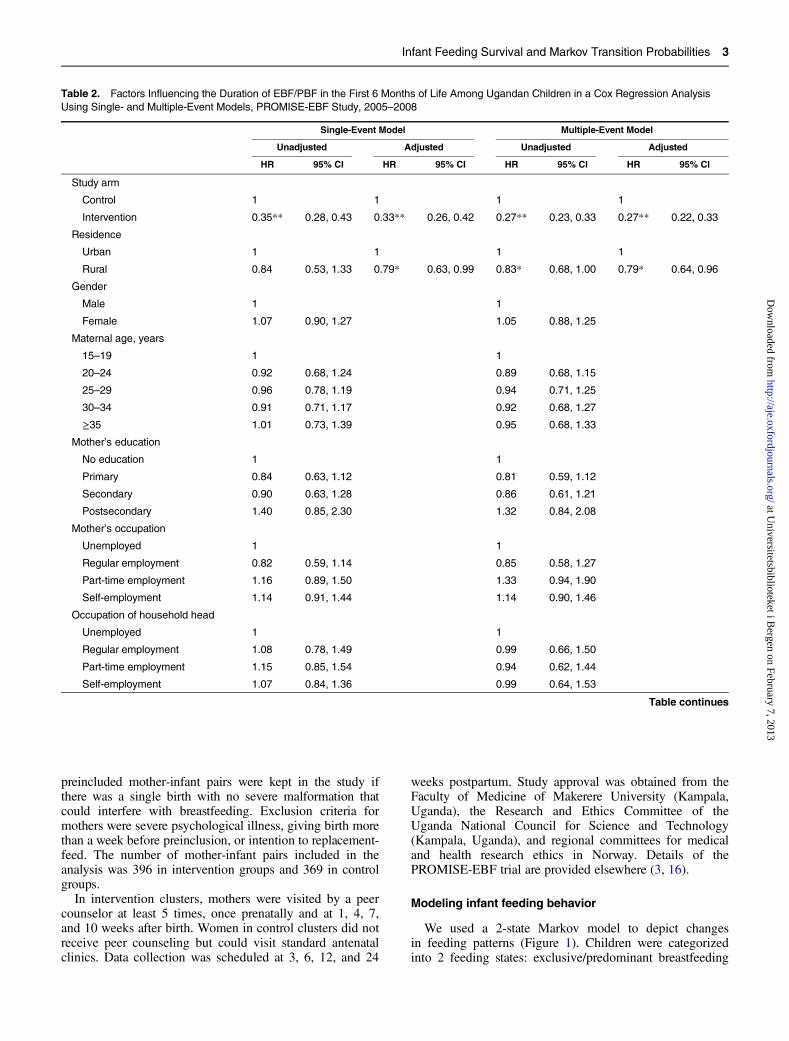
Table 2. Factors Influencing the Duration of EBF/PBF in the First 6 Months of Life Among Ugandan Children in a Cox Regression Analysis
Using Single- and Multiple-Event Models, PROMISE-EBF Study, 2005–2008
Single-Event Model Multiple-Event Model
Unadjusted Adjusted Unadjusted Adjusted
HR 95% CI HR 95% CI HR 95% CI HR 95% CI
Study arm
Control 1 1 1 1
Intervention 0.35** 0.28, 0.43 0.33** 0.26, 0.42 0.27** 0.23, 0.33 0.27** 0.22, 0.33
Residence
Urban 1 1 1 1
Rural 0.84 0.53, 1.33 0.79* 0.63, 0.99 0.83* 0.68, 1.00 0.79* 0.64, 0.96
Gender
Male 1 1
Female 1.07 0.90, 1.27 1.05 0.88, 1.25
Maternal age, years
15–19 1 1
20–24 0.92 0.68, 1.24 0.89 0.68, 1.15
25–29 0.96 0.78, 1.19 0.94 0.71, 1.25
30–34 0.91 0.71, 1.17 0.92 0.68, 1.27
≥35 1.01 0.73, 1.39 0.95 0.68, 1.33
Mother’s education
No education 1 1
Primary 0.84 0.63, 1.12 0.81 0.59, 1.12
Secondary 0.90 0.63, 1.28 0.86 0.61, 1.21
Postsecondary 1.40 0.85, 2.30 1.32 0.84, 2.08
Mother’s occupation
Unemployed 1 1
Regular employment 0.82 0.59, 1.14 0.85 0.58, 1.27
Part-time employment 1.16 0.89, 1.50 1.33 0.94, 1.90
Self-employment 1.14 0.91, 1.44 1.14 0.90, 1.46
Occupation of household head
Unemployed 1 1
Regular employment 1.08 0.78, 1.49 0.99 0.66, 1.50
Part-time employment 1.15 0.85, 1.54 0.94 0.62, 1.44
Self-employment 1.07 0.84, 1.36 0.99 0.64, 1.53
Table continues
Infant Feeding Survival and Markov Transition Probabilities 3
at Universitetsbiblioteket i B
ergen on February 7, 2013http://aje.oxfordjournals.org/
Dow
nloaded from
(EBF/PBF) and mixed/replacement feeding (MF/RF). Themerging of EBF and PBF was made on the basis that fewstudies indicate clear prognostic differences between EBFand PBF (3, 4). MF and RF were merged because fewmothers in our study population were practicing replace-ment feeding (0.3%). The transition from EBF/PBF to MF/RF was either unidirectional, depicting a single-eventmodel (Figure 1A), or multidirectional, defining a multiple-event model (Figure 1B). Feeding status was based onmothers’ recall of infant feeding 7 days prior to the inter-view. In constructing the unidirectional feeding model, astrict definition of feeding was adopted; for example, chil-dren stopping EBF at age 3 weeks could not be categorizedas receiving EBF in subsequent weeks. In the multidirec-tional model, children could be categorized differently insubsequent weeks.
Estimating infant feeding survival
The survival model of infant feeding was fitted usingSTATA, version 11 (StataCorp LP, College Station, Texas).The aims were to assess the duration of EBF/PBF amongchildren under age 6 months and to examine factors influ-encing this duration. The dependent variable was cessation
of EBF/PBF, a time-dependent factor indicating the age atwhich EBF/PBF was stopped. The exact time of EBF/PBFcessation was unknown; it was assumed to have takenplace between birth and a date recalled by the mother. Acontinuous time variable was created by assuming that anevent occurred midway between the start of EBF/PBF andan interview date.Children were censored when they were lost to follow-up
or the last valid interview was missed. Survival estimateswere specified using both single-event (Figure 1A) andmultiple-event (Figure 1B) models. Relapse into EBF/PBFwas assumed to occur midway between 2 follow-up visits.Factors influencing child feeding (Table 2) were identifiedfrom the literature. The “arm” variable denoted member-ship in an intervention or control group (3). Residence wasdichotomized into rural and urban clusters (17). Genderwas included as an inherent biological factor (18–20). Soci-oeconomic status was created with multiple correspondenceanalysis based on a set of assets including house type andtoilet facilities (3, 21).We used the household dependency ratio as a proxy for
family size, measured as the ratio of children to adults in ahousehold (22). Contact with health personnel during preg-nancy was determined by the mother’s possession of an
Table 2. Continued
Single-Event Model Multiple-Event Model
Unadjusted Adjusted Unadjusted Adjusted
HR 95% CI HR 95% CI HR 95% CI HR 95% CI
Tertile of socioeconomic statusa
Low 1 1 1
Medium 0.91 0.70, 1.19 1.19 0.97, 1.45 0.90 0.73, 1.12
High 0.92 0.74, 1.15 1.21* 1.03, 1.42 0.87 0.71, 1.08
Tertile of household dependencyb
Low 1 1
Medium 0.95 0.78, 1.15 0.99 0.80, 1.21
High 0.88 0.72, 1.06 0.88 0.70, 1.10
Parity
Primipara 1 1
Multipara 0.92 0.79, 1.06 0.90 0.74, 1.10
Possession of antenatal care card
No 1
Yes 1.12 0.96, 1.31 1.10 0.91, 1.32
Place of delivery
Home 1
Health facility 1.21* 1.01, 1.44 1.20 0.99, 1.44
Feeding advice
No 1 1 1
Yes 0.81* 0.67, 0.97 0.76** 0.63, 0.91 0.83* 0.69, 0.99
Abbreviations: CI, confidence interval; EBF, exclusive breastfeeding; HR, hazard ratio; PBF, predominant breastfeeding.
* P < 0.05; **P < 0.001.a Socioeconomic status was based on a set of assets including house type and toilet facilities (3, 21).b Household dependency (a proxy for family size) was measured as the ratio of children to adults in the household (22).
4 Chola et al.
at Universitetsbiblioteket i B
ergen on February 7, 2013http://aje.oxfordjournals.org/
Dow
nloaded from
antenatal care card and place of delivery. Additionally,mothers were asked whether they received any advice fromhealth personnel about infant feeding before or after birth,referred to as breastfeeding advice. Other variables includedwere mother’s age, education, and parity (23, 24).
Statistical analysis
Kaplan-Meier survival estimates were used to determineEBF/PBF duration and were compared using a log-ranktest. Turnbull’s nonparametric estimator (25) and flexibleparametric analyses (26) are recommended for interval-censored data; however, we used the standard Kaplan-Meier approach because it has been shown to be sufficientwhen intervals are short, as was the case in our study (27).To characterize the determinants of EBF/PBF duration,we used the midpoint approximation method (MDM) in aCox proportional hazards model accounting for intervalcensoring.
The MDM was also used to fit parametric survivalmodels, the Weibull and exponential models, whose resultswere compared with those obtained in the Cox regression.MDM has been shown to be relatively adequate and usefulin estimating parameters for fairly large data sets withminimal amounts of missing data (28, 29). However, theMDM may not always be the best solution and can lead tobiased estimates. Therefore, to test its usefulness, we fitteda discrete survival-time model with a random intercept andcompared the results.
Model fit was assessed using the Akaike InformationCriterion. This test helps to select the best fit from a set ofmodels (30, 31). The chosen model is the one that minimizesthe Kullback-Leibler distance between the model and a truemeasurement. Data were analyzed longitudinally with 4panels corresponding to the data collection time pointsscheduled at 3, 6, 12, and 24 weeks postpartum. A variance-corrected model (repeated-event model with unorderedfailures of the same type) was used to account for depen-dencies between failure times. This approach does notinclude dependencies between failure times in the model,but it adjusts the covariance matrix of estimators to accountfor additional correlation (32). Since data were randomizedat the community level, we adjusted for cluster randomiza-tion during analysis.
Individual model effects were measured in univariateanalyses. Collinearity, hazard plots, and residual plots werechecked. In multivariable analysis, a backward stepwiseapproach was used with removal set at P = 0.1. Effect mod-ification was tested, and since no interaction terms werestatistically significant at P = 0.05, they were excluded fromthe final model. Results were presented for both single- andmultiple-event models, with predictive power evaluated bycomputing the Harrell’s C concordance statistic. This mea-sures the agreement of predictions with observed failureorder (33). Markov state transition probabilities of infantfeeding were estimated from the best-fitting parametric sur-vival model using the methods described by Briggs et al.(13). In this method, a Markov model of given cycle lengthis specified, and the baseline transition probability isdefined as 1 minus the ratio of the survivor function at the
end of a Markov cycle to the survivor function at the begin-ning of the cycle.
RESULTS
Background characteristics
There were 765 mother-infant pairs in the study. Ofthese, 52% of pairs were in intervention clusters and 26%were in urban areas. Approximately 52% of the childrenwere girls. The mean age of mothers was 25.7 (standarddeviation (SD), 6.6) years. Approximately 22% of motherswere primiparas. Most women delivered their infants athealth facilities (53%) and were in possession of antenatalcare cards (65%). Approximately 48% of the mothersreceived advice on infant feeding from a health practitionereither before or after birth. The mean number of years ofschooling for mothers was 6.3 (SD, 3.3). Most women (74%)did not have salaried work or formalized employment.
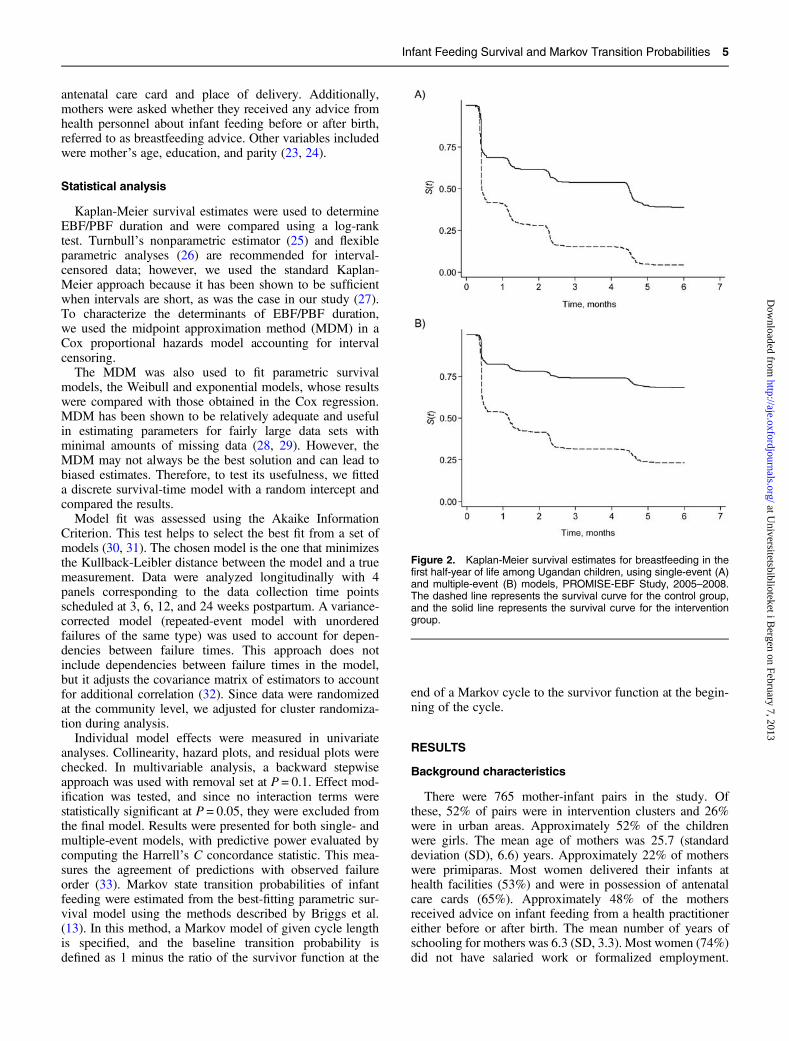
Figure 2. Kaplan-Meier survival estimates for breastfeeding in thefirst half-year of life among Ugandan children, using single-event (A)and multiple-event (B) models, PROMISE-EBF Study, 2005–2008.The dashed line represents the survival curve for the control group,and the solid line represents the survival curve for the interventiongroup.
Infant Feeding Survival and Markov Transition Probabilities 5
at Universitetsbiblioteket i B
ergen on February 7, 2013http://aje.oxfordjournals.org/
Dow
nloaded from
Formal employment was more common among householdheads (43%). The mean household dependency ratio was1.2 (SD, 1.1).
Distribution of survival time
In both single-event (log-rank test: χ2 = 177; P < 0.001)and multiple-event (χ2 = 149; P < 0.001) models, childrenwere breastfed exclusively/predominantly longer in inter-vention clusters than in control clusters (Figure 2). At anygiven time, children in intervention clusters had a lowerprobability of discontinuing EBF/PBF. Survival in thisfeeding state was different in single- and multiple-eventmodels. For example, at age 2 months, the probability forcontrol children to continue EBF/PBF was 39% in single-event models and 44% in multiple-event models. However,at age 6 months, more children were receiving EBF/PBF insingle-event models (>30%) than in multiple-event models(<10%).
Cox regression analysis
In the single-event model, the unadjusted effects of inter-vention arm, place of delivery, and advice on infantfeeding from health personnel were significant predictors ofEBF/PBF duration (Table 2). The peer counseling interven-tion arm had a hazard ratio of 0.35 (95% confidence inter-val (CI): 0.28, 0.43), indicating that children in interventionclusters had a 65% lower risk of EBF/PBF cessation. In themultiple-event model, the unadjusted effects of the inter-vention arm, residence, and advice on infant feeding fromhealth personnel were significant predictors of EBF/PBFduration. The direction of the effects between single- and
multiple-event analysis was the same for most variables,though the hazard ratios from the multiple-event modelwere smaller and the confidence intervals were narrower.Based on the multiple-event model, children in the inter-vention arm had a 73% lower risk of stopping EBF/PBF(hazard ratio = 0.27, 95% CI: 0.23, 0.33).After adjustment for all factors in the single-event
model, intervention arm, residence, and socioeconomicstatus were significant predictors of EBF/PBF duration.Children in intervention clusters and those in rural areashad lower risks of stopping EBF/PBF. In the multiple-eventmodel, the predictors of EBF/PBF duration were interven-tion arm, residence, and advice from health personnel.Harrell’s C statistic for the single-event model was esti-
mated to be 0.61 (95% CI: 0.58, 0.66), as compared with0.70 (95% CI: 0.66, 0.72) in the multiple-event model.This implies that the single-event model correctly identifiedthe order of survival times for pairs of subjects approxi-mately 60% of the time, compared with 70% in the multiple-event model.
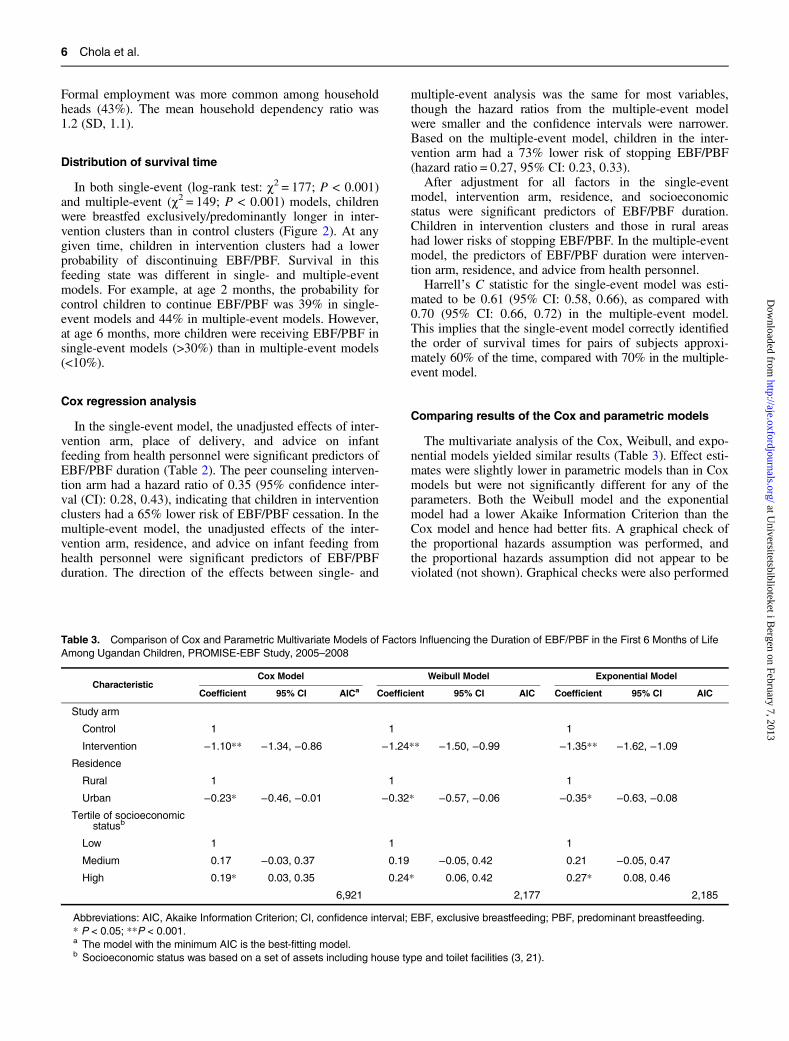
Comparing results of the Cox and parametric models
The multivariate analysis of the Cox, Weibull, and expo-nential models yielded similar results (Table 3). Effect esti-mates were slightly lower in parametric models than in Coxmodels but were not significantly different for any of theparameters. Both the Weibull model and the exponentialmodel had a lower Akaike Information Criterion than theCox model and hence had better fits. A graphical check ofthe proportional hazards assumption was performed, andthe proportional hazards assumption did not appear to beviolated (not shown). Graphical checks were also performed
Table 3. Comparison of Cox and Parametric Multivariate Models of Factors Influencing the Duration of EBF/PBF in the First 6 Months of Life
Among Ugandan Children, PROMISE-EBF Study, 2005–2008
CharacteristicCox Model Weibull Model Exponential Model
Coefficient 95% CI AICa Coefficient 95% CI AIC Coefficient 95% CI AIC
Study arm
Control 1 1 1
Intervention −1.10** −1.34, −0.86 −1.24** −1.50, −0.99 −1.35** −1.62, −1.09
Residence
Rural 1 1 1
Urban −0.23* −0.46, −0.01 −0.32* −0.57, −0.06 −0.35* −0.63, −0.08
Tertile of socioeconomicstatusb
Low 1 1 1
Medium 0.17 −0.03, 0.37 0.19 −0.05, 0.42 0.21 −0.05, 0.47
High 0.19* 0.03, 0.35 0.24* 0.06, 0.42 0.27* 0.08, 0.46
6,921 2,177 2,185
Abbreviations: AIC, Akaike Information Criterion; CI, confidence interval; EBF, exclusive breastfeeding; PBF, predominant breastfeeding.
* P < 0.05; **P < 0.001.a The model with the minimum AIC is the best-fitting model.b Socioeconomic status was based on a set of assets including house type and toilet facilities (3, 21).
6 Chola et al.
at Universitetsbiblioteket i B
ergen on February 7, 2013http://aje.oxfordjournals.org/
Dow
nloaded from
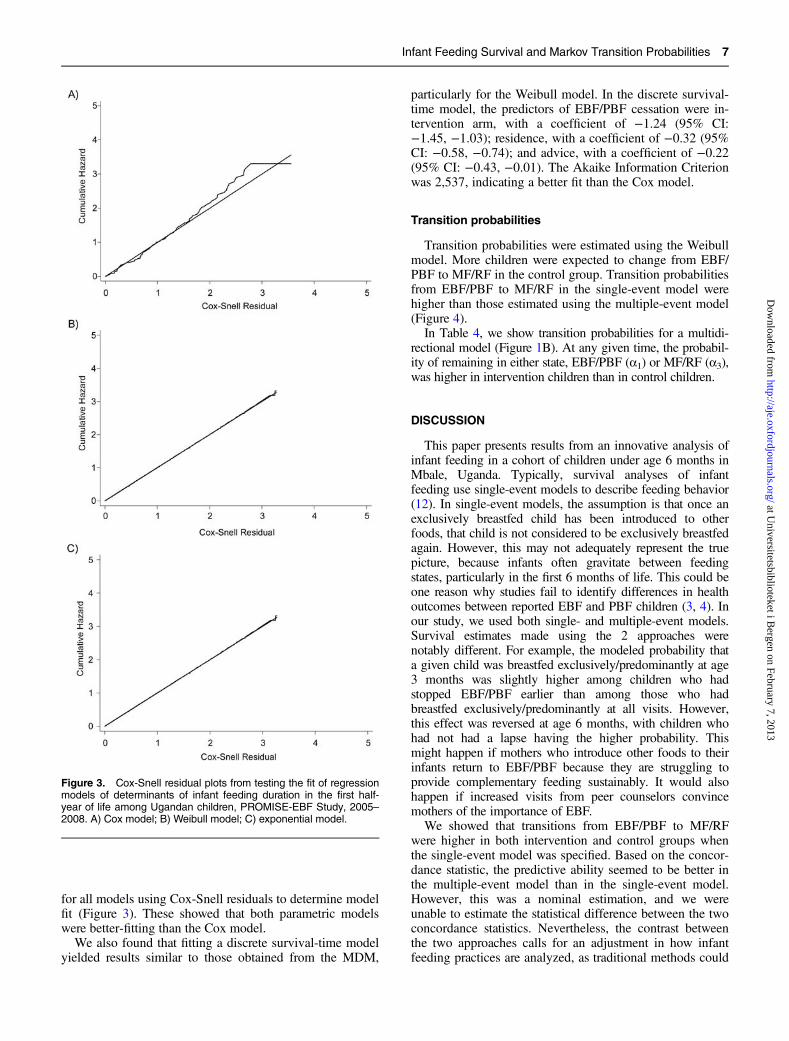
for all models using Cox-Snell residuals to determine modelfit (Figure 3). These showed that both parametric modelswere better-fitting than the Cox model.
We also found that fitting a discrete survival-time modelyielded results similar to those obtained from the MDM,
particularly for the Weibull model. In the discrete survival-time model, the predictors of EBF/PBF cessation were in-tervention arm, with a coefficient of −1.24 (95% CI:−1.45, −1.03); residence, with a coefficient of −0.32 (95%CI: −0.58, −0.74); and advice, with a coefficient of −0.22(95% CI: −0.43, −0.01). The Akaike Information Criterionwas 2,537, indicating a better fit than the Cox model.
Transition probabilities
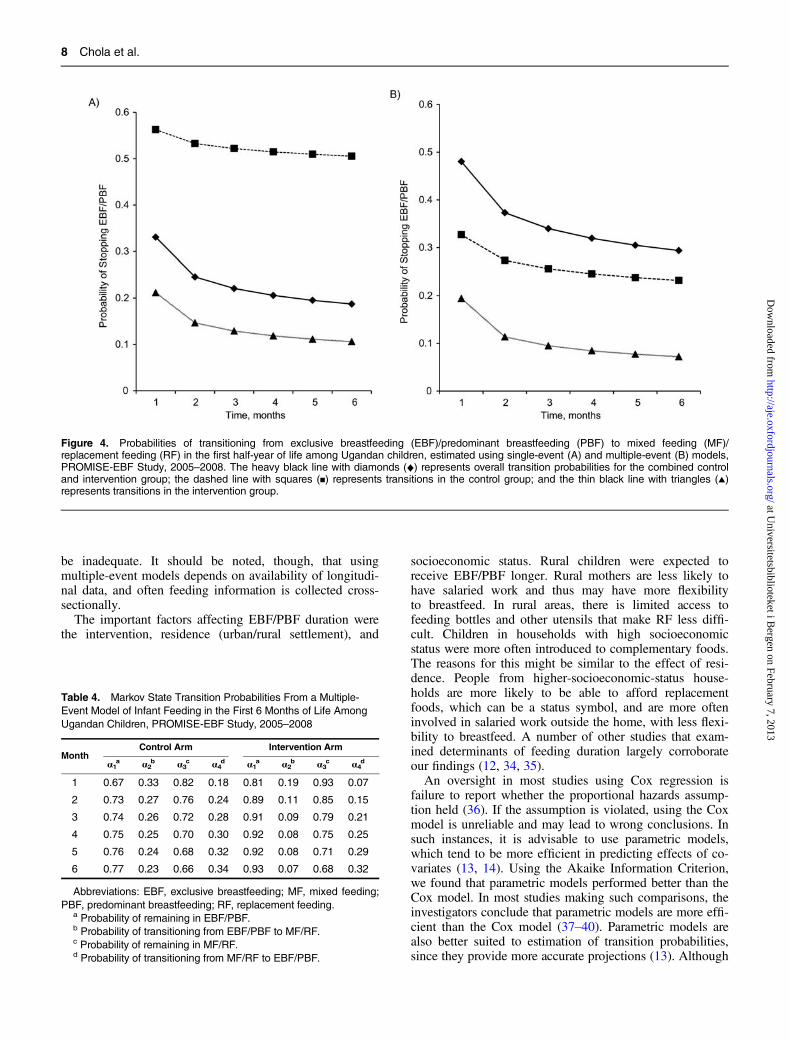
Transition probabilities were estimated using the Weibullmodel. More children were expected to change from EBF/PBF to MF/RF in the control group. Transition probabilitiesfrom EBF/PBF to MF/RF in the single-event model werehigher than those estimated using the multiple-event model(Figure 4).
In Table 4, we show transition probabilities for a multidi-rectional model (Figure 1B). At any given time, the probabil-ity of remaining in either state, EBF/PBF (α1) or MF/RF (α3),was higher in intervention children than in control children.
DISCUSSION
This paper presents results from an innovative analysis ofinfant feeding in a cohort of children under age 6 months inMbale, Uganda. Typically, survival analyses of infantfeeding use single-event models to describe feeding behavior(12). In single-event models, the assumption is that once anexclusively breastfed child has been introduced to otherfoods, that child is not considered to be exclusively breastfedagain. However, this may not adequately represent the truepicture, because infants often gravitate between feedingstates, particularly in the first 6 months of life. This could beone reason why studies fail to identify differences in healthoutcomes between reported EBF and PBF children (3, 4). Inour study, we used both single- and multiple-event models.Survival estimates made using the 2 approaches werenotably different. For example, the modeled probability thata given child was breastfed exclusively/predominantly at age3 months was slightly higher among children who hadstopped EBF/PBF earlier than among those who hadbreastfed exclusively/predominantly at all visits. However,this effect was reversed at age 6 months, with children whohad not had a lapse having the higher probability. Thismight happen if mothers who introduce other foods to theirinfants return to EBF/PBF because they are struggling toprovide complementary feeding sustainably. It would alsohappen if increased visits from peer counselors convincemothers of the importance of EBF.
We showed that transitions from EBF/PBF to MF/RFwere higher in both intervention and control groups whenthe single-event model was specified. Based on the concor-dance statistic, the predictive ability seemed to be better inthe multiple-event model than in the single-event model.However, this was a nominal estimation, and we wereunable to estimate the statistical difference between the twoconcordance statistics. Nevertheless, the contrast betweenthe two approaches calls for an adjustment in how infantfeeding practices are analyzed, as traditional methods could
Figure 3. Cox-Snell residual plots from testing the fit of regressionmodels of determinants of infant feeding duration in the first half-year of life among Ugandan children, PROMISE-EBF Study, 2005–2008. A) Cox model; B) Weibull model; C) exponential model.
Infant Feeding Survival and Markov Transition Probabilities 7
at Universitetsbiblioteket i B
ergen on February 7, 2013http://aje.oxfordjournals.org/
Dow
nloaded from
be inadequate. It should be noted, though, that usingmultiple-event models depends on availability of longitudi-nal data, and often feeding information is collected cross-sectionally.The important factors affecting EBF/PBF duration were
the intervention, residence (urban/rural settlement), and
socioeconomic status. Rural children were expected toreceive EBF/PBF longer. Rural mothers are less likely tohave salaried work and thus may have more flexibilityto breastfeed. In rural areas, there is limited access tofeeding bottles and other utensils that make RF less diffi-cult. Children in households with high socioeconomicstatus were more often introduced to complementary foods.The reasons for this might be similar to the effect of resi-dence. People from higher-socioeconomic-status house-holds are more likely to be able to afford replacementfoods, which can be a status symbol, and are more ofteninvolved in salaried work outside the home, with less flexi-bility to breastfeed. A number of other studies that exam-ined determinants of feeding duration largely corroborateour findings (12, 34, 35).An oversight in most studies using Cox regression is
failure to report whether the proportional hazards assump-tion held (36). If the assumption is violated, using the Coxmodel is unreliable and may lead to wrong conclusions. Insuch instances, it is advisable to use parametric models,which tend to be more efficient in predicting effects of co-variates (13, 14). Using the Akaike Information Criterion,we found that parametric models performed better than theCox model. In most studies making such comparisons, theinvestigators conclude that parametric models are more effi-cient than the Cox model (37–40). Parametric models arealso better suited to estimation of transition probabilities,since they provide more accurate projections (13). Although
Figure 4. Probabilities of transitioning from exclusive breastfeeding (EBF)/predominant breastfeeding (PBF) to mixed feeding (MF)/replacement feeding (RF) in the first half-year of life among Ugandan children, estimated using single-event (A) and multiple-event (B) models,PROMISE-EBF Study, 2005–2008. The heavy black line with diamonds (♦) represents overall transition probabilities for the combined controland intervention group; the dashed line with squares (▪) represents transitions in the control group; and the thin black line with triangles (▴)represents transitions in the intervention group.
Table 4. Markov State Transition Probabilities From a Multiple-
Event Model of Infant Feeding in the First 6 Months of Life Among
Ugandan Children, PROMISE-EBF Study, 2005–2008
MonthControl Arm Intervention Arm
α1a α2
b α3c α4
d α1a α2
b α3c α4
d
1 0.67 0.33 0.82 0.18 0.81 0.19 0.93 0.07
2 0.73 0.27 0.76 0.24 0.89 0.11 0.85 0.15
3 0.74 0.26 0.72 0.28 0.91 0.09 0.79 0.21
4 0.75 0.25 0.70 0.30 0.92 0.08 0.75 0.25
5 0.76 0.24 0.68 0.32 0.92 0.08 0.71 0.29
6 0.77 0.23 0.66 0.34 0.93 0.07 0.68 0.32
Abbreviations: EBF, exclusive breastfeeding; MF, mixed feeding;
PBF, predominant breastfeeding; RF, replacement feeding.a Probability of remaining in EBF/PBF.b Probability of transitioning from EBF/PBF to MF/RF.c Probability of remaining in MF/RF.d Probability of transitioning from MF/RF to EBF/PBF.
8 Chola et al.
at Universitetsbiblioteket i B
ergen on February 7, 2013http://aje.oxfordjournals.org/
Dow
nloaded from

parallel in many respects, parametric models might appearunfamiliar to many. Still, according to our findings, para-metric tests could be more efficient.
Analytically, the models presented in this paper do nottake into account frequency, amount, and quality offeeding. This is useful for understanding infant health andcalls for further research. The strength of this study is thatit was a community-based prospective cohort study withmedium intensity. As a result, relatively few mother-infantpairs were lost to follow-up. However, the frequency andtiming of data collection were not optimal for estimation ofmean feeding duration. Data were collected cross-sectionallyat 4 time points during the follow-up period. More frequentfollow-up—for example, on a monthly basis—would haveenriched the analyses. Furthermore, some mothers missedscheduled interviews, and consequently some interviewswere held much later than the scheduled dates. Such inter-views were censored. This could have led to underestima-tion of feeding duration. However, the number of untimelyinterviews was relatively low and did not differ by arm.During data analysis, we used the MDM to obtain survivalestimates. This is adequate for estimating parameters, par-ticularly when data sets are fairly large and have minimalamounts of missing data (28, 29). However, it may notalways be the best solution, and it can lead to biased esti-mates (41). We fitted a discrete survival-time model andfound that results were not intuitively different from thoseobtained using the MDM.
In conclusion, the analytical approach using transitionsbetween different infant feeding categories and allowingfor multiple events gave us an extended understanding ofinfant feeding practices. This approach is believed toprovide a better picture than single-event models of longi-tudinal infant feeding data and is consequently preferablewhen the goal is informing public health policy or conduct-ing economic evaluations.
ACKNOWLEDGMENTS
Author affiliations: Central Statistical Office, Lusaka,Zambia (Lumbwe Chola); Centre for International Health,University of Bergen, Bergen, Norway (Lumbwe Chola,Lars T. Fadnes, Ingunn M. S. Engebretsen, ThorkildTylleskar, Bjarne Robberstad); Department of Medicine,Haukeland University Hospital, Bergen, Norway (LarsT. Fadnes); Department of Child and Adolescent Psychia-try, Haukeland University Hospital, Bergen, Norway(Ingunn M. S. Engebretsen); and Department of Paediatricsand Child Health, School of Medicine, Makerere Universi-ty, Kampala, Uganda (James K. Tumwine).
This study was supported by the European Union-fundedproject PROMISE-EBF (contract INCO-CT 2004-003660).It was also financially supported by the Research Councilof Norway’s Programme for Global Health and VaccinationResearch (grant 172226); the Norwegian Programme forDevelopment, Research and Education; and the Universityof Bergen.
Members of the PROMISE-EBF Study Group—SteeringCommittee: Thorkild Tylleskär (Principal Investigator (PI)),Philippe Van de Perre, Eva-Charlotte Ekström, NicolasMeda, James K. Tumwine, Chipepo Kankasa, DebraJackson; Norway: Thorkild Tylleskär (PI), Ingunn M.S.Engebretsen, Lars Thore Fadnes, Eli Fjeld, Knut Fylkesnes,Jørn Klungsøyr, Anne Nordrehaug-Åstrøm, Øystein EvjenOlsen, Bjarne Robberstad, Halvor Sommerfelt; France:Philippe Van de Perre (PI); Sweden: Eva-Charlotte Ekström(PI), Barni Nor; Burkina Faso: Nicolas Meda (PI), A. HamaDiallo, Thomas Ouedrago, Jeremi Rouamba, BernadetteTraoré Germain Traoré, Emmanuel Zabsonré; Uganda:James K. Tumwine (PI), Caleb Bwengye, Charles Karamagi,Victoria Nankabirwa, Jolly Nankunda, Grace Ndeezi,Margaret Wandera; Zambia: Chipepo Kankasa (PI), MaryKatepa-Bwalya, Lumbwe Chola, Chafye Siuluta, SeterSiziya; South Africa: Debra Jackson (PI), Carl Lombard,Mickey Chopra, Mark Colvin, Tanya Doherty, AmeenaE. Googa, Lyness Matizirofa, Lungiswa Nkonki, DavidSanders, Rebecca Shanmugam, Wanga Zembe.
Conflict of interest: none declared.
REFERENCES
1. Jones G, Steketee RW, Black RE, et al. How many childdeaths can we prevent this year? Lancet. 2003;362(9377):65–71.
2. World Health Organization. HIV and Infant Feeding: RevisedPrinciples and Recommendations—Rapid Advice. Geneva,Switzerland: World Health Organization; 2009.
3. Tylleskar T, Jackson D, Meda N, et al. Exclusivebreastfeeding promotion by peer counsellors in sub-SaharanAfrica (PROMISE-EBF): a cluster-randomised trial. Lancet.2011;378(9789):420–427.
4. Bahl R, Frost C, Kirkwood BR, et al. Infant feeding patternsand risks of death and hospitalization in the first half ofinfancy: multicentre cohort study. Bull World Health Organ.2005;83(6):418–426.
5. Bhandari N, Bahl R, Mazumdar S, et al. Effect ofcommunity-based promotion of exclusive breastfeeding ondiarrhoeal illness and growth: a cluster randomised controlledtrial. Lancet. 2003;361(9367):1418–1423.
6. Arifeen SE, Black RE, Caulfield LE, et al. Determinants ofinfant growth in the slums of Dhaka: size and maturity atbirth, breastfeeding and morbidity. Eur J Clin Nutr. 2001;55(3):167–178.
7. Diallo FB, Bell L, Moutquin JM, et al. The effects ofexclusive versus non-exclusive breastfeeding on specificinfant morbidities in Conakry. Pan Afr Med J. 2009;2:2.
8. Kuhn L, Aldrovandi GM, Sinkala M, et al. Effects of early,abrupt weaning on HIV-free survival of children in Zambia.N Engl J Med. 2008;359(2):130–141.
9. Sonnenberg FA, Beck JR. Markov models in medicaldecision making: a practical guide. Med Decis Making.1993;13(4):322–338.
10. Scholtens S, Gehring U, Brunekreef B, et al. Breastfeeding,weight gain in infancy, and overweight at seven years of age:the prevention and incidence of asthma and mite allergy birthcohort study. Am J Epidemiol. 2007;165(8):919–926.
11. Rzehak P, Sausenthaler S, Koletzko S, et al. Period-specificgrowth, overweight and modification by breastfeeding in the
Infant Feeding Survival and Markov Transition Probabilities 9
at Universitetsbiblioteket i B
ergen on February 7, 2013http://aje.oxfordjournals.org/
Dow
nloaded from

GINI and LISA birth cohorts up to age 6 years. Eur JEpidemiol. 2009;24(8):449–467.
12. Abada TS, Trovato F, Lalu N. Determinants of breastfeedingin the Philippines: a survival analysis. Soc Sci Med. 2001;52(1):71–81.
13. Briggs A, Claxton K, Sculpher M. Decision Modelling forHealth Economic Evaluation. New York, NY: OxfordUniversity Press; 2006.
14. May M, Sterne J, Egger M. Parametric survival models maybe more accurate than Kaplan-Meier estimates [letter]. BMJ.2003;326(7393):822.
15. Uganda Bureau of Statistics. Uganda Population andHousing Census. Kampala, Uganda: Uganda Bureau ofStatistics; 2002.
16. Nankunda J, Tylleskar T, Ndeezi G, et al. Establishingindividual peer counselling for exclusive breastfeeding inUganda: implications for scaling-up. Matern Child Nutr.2010;6(1):53–66.
17. Grummer-Strawn LM. The effect of changes in populationcharacteristics on breastfeeding trends in fifteen developingcountries. Int J Epidemiol. 1996;25(1):94–102.
18. Drevenstedt GL, Crimmins EM, Vasunilashorn S, et al. Therise and fall of excess male infant mortality. Proc Natl AcadSci U S A. 2008;105(13):5016–5021.
19. Wamani H, Astrom AN, Peterson S, et al. Boys are morestunted than girls in sub-Saharan Africa: a meta-analysis of16 demographic and health surveys. BMC Pediatr. 2007;7:17.
20. Fuse K, Crenshaw EM. Gender imbalance in infant mortality:a cross-national study of social structure and femaleinfanticide. Soc Sci Med. 2006;62(2):360–374.
21. Howe LD, Hargreaves JR, Huttly SR. Issues in theconstruction of wealth indices for the measurement of socio-economic position in low-income countries. Emerg ThemesEpidemiol. 2008;5:3.
22. Agboado G, Michel E, Jackson E, et al. Factors associatedwith breastfeeding cessation in nursing mothers in a peersupport programme in Eastern Lancashire. BMC Pediatr.2010;10:3.
23. Ekstrom A, Widstrom AM, Nissen E. Duration ofbreastfeeding in Swedish primiparous and multiparouswomen. J Hum Lact. 2003;19(2):172–178.
24. Fadnes LT, Engebretsen IM, Wamani H, et al. Need tooptimise infant feeding counselling: a cross-sectional surveyamong HIV-positive mothers in Eastern Uganda. BMCPediatr. 2009;9:2.
25. Turnbull BW. The empirical distribution function witharbitrarily grouped, censored and truncated data. J R Stat SocSeries B Stat Methodol. 1976;38(3):290–295.
26. Royston P. Flexible parametric alternatives to the Cox model,and more. Stata J. 2001;1(1):1–28.
27. Alioum A, Cortina-Borja M, Dabis F, et al. Estimating theefficacy of interventions to prevent mother-to-childtransmission of human immunodeficiency virus inbreastfeeding populations: comparing statistical methods. AmJ Epidemiol. 2003;158(6):596–605.
28. Odell PM, Anderson KM, D’Agostino RB. Maximumlikelihood estimation for interval-censored data using aWeibull-based accelerated failure time model. Biometrics.1992;48(3):951–959.
29. Ng HKT, Wang Z. Statistical estimation for the parameters ofWeibull distribution based on progressively type-I intervalcensored sample. J Stat Comput Simul. 2009;79(2):145–159.
30. Glatting G, Kletting P, Reske SN, et al. Choosing the optimalfit function: comparison of the Akaike information criterionand the F-test. Med Phys. 2007;34(11):4285–4292.
31. Wager C, Vaida F, Kauermann G. Model selection forpenalized spline smoothing using Akaike information criteria.Aust N Z J Stat. 2007;49(2):173–190.
32. Ezell ME, Land KC, Cohen LE. Modeling multiple failuretime data: a survey of variance-corrected proportional hazardsmodels with empirical applications to arrest data. SociolMethodol. 2003;33(1):111–167.
33. Newson RB. Comparing the predictive powers of survivalmodels using Harrell’s C or Somers’ D. Stata J. 2010;10(3):339–358.
34. Kimani-Murage EW, Madise NJ, Fotso JC, et al. Patterns anddeterminants of breastfeeding and complementary feedingpractices in urban informal settlements, Nairobi Kenya. BMCPublic Health. 2011;11:396.
35. Agampodi SB, Agampodi TC, Piyaseeli UK. Breastfeedingpractices in a public health field practice area in Sri Lanka: asurvival analysis. Int Breastfeed J. 2007;2:13.
36. Altman DG, De Stavola BL, Love SB, et al. Review ofsurvival analyses published in cancer journals. Br J Cancer.1995;72(2):511–518.
37. Nakhaee F, Law M. Parametric modelling of survivalfollowing HIV and AIDS in the era of highly activeantiretroviral therapy: data from Australia. East MediterrHealth J. 2011;17(3):231–237.
38. Moghimi-Dehkordi B, Safaee A, Pourhoseingholi MA, et al.Statistical comparison of survival models for analysis ofcancer data. Asian Pac J Cancer Prev. 2008;9(3):417–420.
39. Pourhoseingholi MA, Hajizadeh E, Moghimi Dehkordi B,et al. Comparing Cox regression and parametric models forsurvival of patients with gastric carcinoma. Asian Pac JCancer Prev. 2007;8(3):412–416.
40. Nardi A, Schemper M. Comparing Cox and parametricmodels in clinical studies. Stat Med. 2003;22(23):3597–3610.
41. Williamson JM, Satten GA, Hanson JA, et al. Analysis ofdynamic cohort data. Am J Epidemiol. 2001;154(4):366–372.
10 Chola et al.
at Universitetsbiblioteket i B
ergen on February 7, 2013http://aje.oxfordjournals.org/
Dow
nloaded from
Related Documents