10.5731/pdajpst.2015.01037 Access the most recent version at doi: 123-139 69 , 2015 PDA J Pharm Sci and Tech Stan Bukofzer, John Ayres, Anna Chavez, et al. Injectable Drug Products Industry Perspective on the Medical Risk of Visible Particles in on August 15, 2018 journal.pda.org Downloaded from on August 15, 2018 journal.pda.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
10.5731/pdajpst.2015.01037Access the most recent version at doi: 123-13969, 2015 PDA J Pharm Sci and Tech
Stan Bukofzer, John Ayres, Anna Chavez, et al. Injectable Drug ProductsIndustry Perspective on the Medical Risk of Visible Particles in
on August 15, 2018journal.pda.orgDownloaded from on August 15, 2018journal.pda.orgDownloaded from

PDA PAPER
Industry Perspective on the Medical Risk of VisibleParticles in Injectable Drug Products
Authors
Stan Bukofzer*, MD, Hospira, Inc (Chair)John Ayres, MD, Eli Lilly and CompanyAnna Chavez, MD, BaxterMinerva Devera, DBA, QSM, EmergentJahanvi Miller, MBA, Parenteral Drug Association (PDA)
Douglas Ross, MD, PfizerJohn Shabushnig, PhD, Insight Pharma Consulting, LLCSusan Vargo, MS, PhD, AmgenHarry Watson, MTSC, CMQ/OE, Hospira, IncRick Watson, Merck
Executive Summary
Sterile injectable products are used extensively inhealth care. Patients, caregivers, manufacturers, andregulators have an inherent expectation for safe andeffective injectable drug products. This expectation re-quires injectable pharmaceuticals to be produced tostandards of quality, purity, and sterility that includebeing essentially free of extraneous matter such as par-ticles. Despite guidance in producing product that is“essentially free” of particles, manufacturing such prod-uct is very challenging. In many instances, the observa-tion of particles in pharmaceutical products has resultedin product recalls. While medical warnings have accom-panied these recall notices, the specifics of these warn-ings have varied. The medical literature is sparse withrespect to case reports and experimental studies provid-ing data to support the safety risk of particles (intrinsicor extrinsic) in humans. A gap exists between the obser-vation of small quantities of particles in injectable phar-maceutical products and patient-documented safety con-cerns resulting from the inadvertent administration ofparticles to patients. Thus, a need exists to create aframework to describe and assess the potential risk ofadministering particles to patients.
This paper provides a review of current compendialinspection requirements for visible particles along with areview of the medical literature associated with anyobserved harm from such particles. Guidance is pro-vided on the assessment of risk in such circumstances
including consideration of the following key attributes;patient factors, route of administration and use of filtra-tion at the point of administration, the volume adminis-tered, particle size and their fate in body, particle type,source and amount, manufacturing process mitigationand the frequency of detection.
Globally, clinicians and patient populations are fac-ing drug shortages in part due to inconsistent productrelease and recall decisions related to the presence ofparticles and a lack of understanding of the impact topatient risk. The decision to recall product from themarket should be based on context of the manufactur-ing trend history, complaint rate trending, and medi-cal risk assessment. Unless there are specific specialcircumstances, there should be no automatic require-ment to recall a product lot for a single particle foundin a single unit. Notwithstanding high risk clinicalcircumstances and acknowledging there are limita-tions to reporting clinical events to particle infusion,the existing data suggest the overall risk to patients isgenerally low and the benefit of these treatments isgenerally significant.
Introduction
Sterile injectable products are used extensively inhealth care; in fact, more than 15 billion injectabledoses are administered annually worldwide (1). Pa-tients, caregivers, manufacturers, and regulatorshave an inherent expectation for safe and effectiveinjectable drug products. This expectation requiresinjectable pharmaceuticals to be produced to stan-dards of quality, purity, and sterility that includebeing essentially free of extraneous matter such asparticles. (For the purposes of this paper, the mean-ing of the term particle includes particulate andparticulate matter) The standards of producingpharmaceutical products are described within thevarious pharmacopeias. Manufacturers strive to pro-
*Corresponding Author: Stan Bukofzer, MD, CorporateVice President and Chief Medical Officer, Hospira, Inc, 275North Field Drive, Lake Forest, IL 60045, USA. Tele-phone: (�1) 224-212.4524; Fax: 224-212-5223; Mobile:224-209-9061; e-mail: [email protected]
doi: 10.5731/pdajpst.2015.01037
PDA Paper Disclaimer: The following paper is a special contribution from the Parenteral Drug Association (PDA). Thisarticle was internally reviewed by PDA and the task force members and not peer-reviewed by the PDA Journal. Note: ThisPDA Paper is protected by copyright and unauthorized distribution or use is prohibited.
123Vol. 69, No. 1, January–February 2015
on August 15, 2018journal.pda.orgDownloaded from

duce injectable products with the requisite qualityoutlined in these standards to ensure their safe andeffective use.
Despite guidance in producing product that is “essen-tially free” of particles, manufacturing such product isvery challenging (2). For example, over the period of2008 –2012, particle-related issues led to 22% of prod-uct recalls for injectable products (3). In 2007, theEuropean Medicines Agency (EMA) performed ananalysis of product quality defects reported in 2005and noted that 6% of all product quality defects wereattributed to particles (4). Those particle defects thatresulted in a recall would have been classified by EMAas either a class 2 (defects which could cause illness ormistreatment, but are not Class 1, e.g., mislabelingsuch as incorrect text) or class 3 (defects which maynot pose a significant hazard to health, but where arecall has been initiated for other reasons e.g., faultypackaging) (EU recall) (4, 5). Between January 2013and June 2014, the Medicines and Healthcare ProductsRegulatory Agency (MHRA) Drug Alert website is-sued forty-two drug alerts, with eleven alerts relatingto particles (6). Of these, alerts reported in 2014 wereall class 2 and included metal particles, small whiteparticles, fiber and glass particles, and silicone frag-ments (7–11). Other agencies, such as FDA, havedifferent class definitions for recalls: Class I Recall -A situation in which there is a reasonable probabilitythat use of, or exposure to, a violative product willcause serious adverse health consequences or death.(21 C.F.R. § 7.3(m)(1)); Class II Recall - A situationin which use of, or exposure to, a violative productmay cause temporary or medically reversible ad-verse health consequences or where the probabilityof serious adverse health consequences is remote.(21 C.F.R. § 7.3(m)(2)); and Class III Recall - Asituation in which use of, or exposure to, a violativeproduct is not likely to cause adverse health conse-quences (21 C.F.R. § 7.3(m)(3)) (12).
Parenteral solutions withdrawn from glass ampoulesroutinely expose patients to numerous glass particlesof variable size. As an example, a 1972 study by Turcoand Davis showed that opening a single 2 mL glassampoule and withdrawing the medicine included 292glass particles between 5 �m and 50 �m and 21particles that were greater than 50 �m (13). Vialpresentations may contain particles from the rubberclosure, a risk that is present with every injection (14).These are known risks that may result from the pack-aging and use of the product and are not manufactur-
ing related. The technology to produce, package, andstore completely particle-free products on a large scaleis not currently available. Additionally, Davis et al.identified 86 to 2,200 particles of �5 �m per literfollowing filtration from a wide variety of sterile in-fusion solutions in glass and plastic containers (15).Based on the study by C.M. Backhouse et al., intensivecare patients would likely often receive more than 107
foreign particles �2�m per 24 hours with their intra-venous therapy (16).
In many instances, the observation of particles inpharmaceutical products has resulted in product re-calls (3). While medical warnings have accompaniedthese recall notices, the specifics of these warningshave varied (17–22). Typically, these warnings aredescribed as “potential” and are not accompanied bypublished reports of patient harm. The medical litera-ture is sparse with respect to case reports and exper-imental studies providing data to support the safetyrisk of particles (intrinsic or extrinsic) in humans.Turco and others have demonstrated mechanisms forthe inadvertent introduction of particles, sometimes inlarge quantities, to parenteral fluids prior to adminis-tration (13). The in-line filter articles suggest a poten-tial relationship of the reduction of particles and de-crease in rate on infusion site phlebitis when filters areused (16). The older literature on large volume infu-sion and parenteral nutrition and the literature onintravenous drug addicts (IVDA), which have verylimited general use for current medical practice showthat mass, chronicity and unique characteristics of theparticle may have a role in these special situations (23,24). The paucity of current medical literature detailingharms from particulate in pharmaceutical productsmight in part reflect the high standards of currentmanufacturing processes.
A recently observed exception is the reaction of sub-visible (�10 �m) protein aggregates to form anti-drugantibodies. Such antibodies have been observed inboth preclinical and clinical studies with protein baseddrug products (25–28). These particles are typicallybelow the visual threshold, unless present in largequantity to be observed as a haze in the solution. Withthis exception, a gap exists between the observation ofsmall quantities of particles in injectable pharmaceu-tical products and patient-documented safety concernsresulting from the administration of particles to pa-tients. Thus, a need exists to create a framework todescribe and assess the potential risk of administeringparticles to patients.
124 PDA Journal of Pharmaceutical Science and Technology
on August 15, 2018journal.pda.orgDownloaded from

Current written expectations for limits on particles ininjectable products can be found in the national orregional pharmacopeias. These requirements aremore fully described in the section “Current DefinedRules” that follows. Historically, these expectationshave required significant interpretation to translateinto a usable numerical limit for product release andongoing compliance considerations. This has led toa broad range of differing practices and decisions byindividual pharmaceutical manufacturers and regu-latory authorities. The evolving standards and abetter understanding of patient risk will help todeliver consistent and safe products across the phar-maceutical industry.
With these considerations in mind, the medical offi-cers and industry experts authoring this paper reachedconsensus on considerations to be used when assessinghealth hazards of particles in injectable solutions. Thepurpose of this paper, which purposely limits scope tofocus on non-product particles (e.g., fibers, glass, rub-ber, metal), is to provide a scientific, medical risk-based approach for evaluating patient safety if a par-ticle contained within injectable drug products isinadvertently administered to a patient. The paper issupplemented by a literature review of describedharms to patients as well as a number of animal studiesthat have tried to evaluate the physiological effect; ingeneral these studies have been highly experimentaland used excessive quantities of particles (29 –31).Specific approaches to risk mitigation are not ad-dressed in this paper.
To assess risk to health, consideration needs to includeproduct sterility, patient factors as well as the vari-ability in route of product administration and variabil-ity in particle type, size, and volume of any productwithin which the particle exists. The clinical impactcan then be adequately assessed by understanding thelikelihood and severity of the pathophysiological con-sequences if particles are administered to patients. Byunderstanding the health risks, regulators and manu-facturers will be better able to develop standards thatsupport delivering high-quality drug products. Theseperspectives underlie the creation of a risk-based ap-proach when assessing health hazards associated withparticles.
Despite varying sources and types of inert particles,only four basic pathogenic mechanisms for potentialharm exist: 1. Infection and inflammation due to localor systemic infections caused by the presence of mi-
croorganisms or endotoxins. 2. Physical presence of aparticle may cause inflammatory response directly orthrough associated leachates that cause direct tissueinjury. 3. Particles might also stimulate untoward im-mune responses such as allergic reactions or anaphy-laxis. 4. Tissue damage can arise from the occlusion ofthe affected vasculature (thromboembolism). Symp-toms and signs can manifest locally or systemically(e.g., temperature, feeling weak). As part of the baserequirements for a quality system, the manufactur-ing environment is monitored for potential sourcesof microorganisms or endotoxin contamination.Product is routinely tested at final release to ensureproduct requirements (e.g., sterility) are met. Al-though microorganisms and endotoxins represent apotential concern, these risks are addressed throughother commonly used compendial tests. Thus, thispaper focuses on the concerns surrounding irritatinginflammation or reaction, local tissue damage, andthromboembolism.
The routes of administration considered for the pur-pose of this paper are limited to drugs administeredthrough direct injection or infusion. As defined inTable 1 later in this paper, the examples of the types ofinjections considered within scope include subcutane-ous, intramuscular, intravenous, high-volume/pressureinfusions, intrathecal, intraarticular, intraocular, in-traarterial, and intraperitoneal. Examples of producttypes included are antibiotics, antitoxins, antivenums,blood, blood derivatives, immune serums, immuno-logic diagnostic aids, therapeutic proteins, toxoids, IVsolutions, and vaccines. Out of scope of this documentare drug-release products that are implanted, even ifimplantation occurs through injection, as well as allroutes of administration other than injection, includinginhalation, topical, and ophthalmic. Furthermore, thepaper does not include gross contamination, wherebyparticles may be included across a significant propor-tion of vials of a product lot or lots or a single vialwith a large quantity of particles, and the product doesnot meet the expectation for “essentially free.”
Current Defined Rules
The current inspection methods and acceptance crite-ria for particle matter in injectable products may befound in the national or regional pharmacopeias. Forthe U.S. market, the U.S. Pharmacopeia (USP) Gen-eral Chapter �788� Particulate Matter in Injectionshas been official for many years. It defines two meth-ods for counting subvisible particles and sets limits of
125Vol. 69, No. 1, January–February 2015
on August 15, 2018journal.pda.orgDownloaded from

6,000 and 600 particles per container for �10 �m and�25 �m particles, respectively. These limits apply tocontainers �100 mL. For containers larger than 100mL, limits are set on a per milliliter basis. As this is aharmonized chapter, the same methods and limits arefound in the European Pharmacopeia (EP) and theJapanese Pharmacopeia (JP).
Requirements for visible particles are found in USPGeneral Chapter �1� Injections. The requirement setin this chapter is that every final container is inspectedfor particles to the extent possible, and any showingthe presence of observable foreign and particulatematter are rejected. It further requires that “the inspec-tion process shall be designed and qualified to ensurethat every lot of parenteral preparations is essentiallyfree from visible particulates” (32). General Chapter�790� Visible Particulates in Injections was pub-lished in the first supplement to USP 37 and becameofficial August 1, 2014 (2). This chapter establishesreference inspection conditions and provides quantita-tive limits based on acceptance sampling to meet theexpectation for every lot to be essentially free fromvisible particles. The inspection conditions are harmo-nized with those found in the EP (33).
Additional requirements for products marketed in Eu-rope can be found in the Finishing of Sterile Productssection of the European Medicines Agency Annex 1.This section sets the requirement that “filled contain-ers of parenteral products should be inspected individ-ually for extraneous contamination or other defects.”It also sets an expectation that inspectors pass regularvision tests and that frequent breaks be given to avoidfatigue. The EP, in Parenteral Preparations-Injections(0520), specifies “solutions for injection, examinedunder suitable conditions of visibility, are clear andpractically free from particles.” It follows with aninspection method described in 2.9.20 ParticulateContamination: Visible Particles. This section speci-fies illumination intensity, background, and pace forthe conditions suitable for inspection. The EP mono-graph Monoclonal Antibodies for Human Use (2013)aligns with the EP monograph Parenteral Preparationsfor Injections, allowing for an appearance specifica-tion of “practically free from particles.” The specifi-cation must be “justified and authorized” (34).
The requirements for product marketed in Japan arecontained within the JP. It specifies inspection withthe unaided eye with light coming from an incandes-cent source with intensity below that stated in the EP
and USP. The acceptance criterion for this inspectionis “injections or vehicles must be clear and free fromreadily detectable foreign insoluble matters” (35).
All of the pharmacopeias establish the need to perform100% inspection of units in a batch or lot of productunder controlled condition, but they recognize theprobabilistic nature of the inspection process in theacceptance criteria.
Evolving Stances and Drivers
Particles represent an ongoing challenge in drug prod-uct manufacturing. The use of clear and colorlessinjectable liquids and containers permits continuous,nondestructive inspection throughout the drug productlife cycle for most products. Where product formula-tion (e.g., powders, suspensions and strongly coloredsolutions) and/or the container (e.g., amber glass ortranslucent plastic) limit visual inspection, supplemen-tal destructive testing of a small sample is recom-mended to further assess the risk of particles in thebatch (2). Points of failure, based on particle presence,include in-process waste (rejects) and customer com-plaints. As seen in a recent benchmarking study, themost common cause for rejections was the presence ofparticles (28). Sources of particles include the manu-facturing environment, primary packaging compo-nents, processing equipment, and the drug productitself. Together with cosmetic and other appearancedefects, particles continue to impact product qualityand availability.
The presence of visible particles in injectable drugproducts has been a matter of intense discussion,both from a regulatory and a compliance perspec-tive, within global regulatory agencies as well asindustry over recent years (35). There is an expec-tation to not only reduce particles but also controlthem, including those in the subvisible range. Tobetter understand the particles’ source, and thus aidin their reduction, particle detection and identifica-tion are important parts of regulatory complianceand product quality assurance. Lot release accep-tance criteria such as “free from”, “without” or “novisible particles” risk the rejection of entire batchesof drug product should a single particle be detectedin a single container of product. Further, currentinspection methods and technologies, including hu-man manual inspection and fully automated inspec-tion systems, cannot provide this level of absoluteassurance. Visual inspection is a probabilistic pro-
126 PDA Journal of Pharmaceutical Science and Technology
on August 15, 2018journal.pda.orgDownloaded from

cess (36, 37), with detection probabilities less than100%, especially for particles less than 200 �m indiameter (27, 28, 38). This 100% inspection is sup-ported by acceptance sampling methodology (“AQLinspection”), which again does not support absoluteassurance of the absence of all particles. Thesepractical limitations should be considered when es-tablishing any visual inspection limit.
Industry has been working with regulatory agenciesworldwide to update guidelines and monographs toreflect these pharmaceutical developments and to gainimprovements in control and methods for identifica-tion of visible particles. Industry has begun to advo-cate for regulatory distinction between particles intro-duced into a product as an intrinsic or extrinsiccontaminant versus the formation of inherent particlesfrom the drug product, recognizing that inherent par-ticles should have been fully characterized by theapplication holder during product development anddescribed in the product application.
Despite these efforts, the published guidance fromregulatory bodies has limited specificity on allowableparticle size, numbers, and types of visible particles(2, 29, 32, 34, 40), or on visible particle investigations(41). There is no published guidance on the potentialimpact of small numbers of visible particles to patientsafety. In a general sense, this is the most commonissue facing manufacturers. While the published liter-ature contains a number of anecdotal reports describ-ing exposure to large numbers of particles, none ofthese reports reflect the potential hazards of moretypical particle administration via large- or small-volume parenteral pharmaceutical administration topatients. There continues to be emotional stances lack-ing data around the subject; a clear understanding ofthe facts to benefit all is required.
Particle Matter Consideration
The European, Japanese, and US Pharmacopeias sharethe following harmonized definition for particulatematter in injectable products:
Particulate matter in injections and paren-teral infusions consists of extraneous mobileundissolved particles, other than gas bubbles,unintentionally present in the solutions.
Identification of the composition of the particulatematter is the first step in characterizing particulate
matter risk. Based on this information, particles can befurther classified into one of three subcategories: ex-trinsic, intrinsic, and inherent. Both extrinsic and in-trinsic particles are considered within the scope of thispaper, while inherent particles are not. The followingdiscussion provides definitions and examples of ex-trinsic, intrinsic, and inherent particles.
Extrinsic particles are defined as those that are not partof the formulation, package, or assembly process, butrather are foreign and unexpected. Examples of extrin-sic particles include fibers (e.g., cellulous), clothingfragments, hair, rubber, metal, plastic, and paint. Ma-terials such as rubber, metal, and plastic are definedas extrinsic in cases where the specific materialidentified is not a product-contact material andtherefore not considered part of the formulation,package, or assembly process. Extrinsic particlespresent a greater risk to sterility assurance, espe-cially for aseptically filled products, as their biobur-den is unknown and uncontrolled.
Intrinsic particles are defined as those that arise fromsources related to the formulation, packaging, or as-sembly processes. Examples of intrinsic particle ma-terials include glass, stainless steel, rubber from stop-pers, and gasket material. In each of these cases, theparticle material should be a known product-contactmaterial to be considered intrinsic. Such materialsare chosen because they are inert and unreactive tothe drug product. Intrinsic particles can also berelated to changes in the product over time or due tophysical and chemical reactions between the prod-uct and the components (e.g., oxidation, incompat-ibility between admixture drug and the carriersolution). Such reactions may form a visible precip-itate or glass lamellae. While these are formed inpart from the drug formulation, they are not consid-ered inherent particles, as discussed below, becausethey are indicative of an unexpected reaction and alack of product stability.
Inherent particles are defined as materials that areexpected from the drug formulation, and thus repre-sent a generally accepted characteristic of the product.Examples of inherent matter include the following:adjuvant material in suspension products, certain ex-cipients such as human serum albumin, proteinaceousaggregates in therapeutic proteins, and mannitol crys-tallization (38). Inherent particles, although antici-pated, should be handled as a particle defect whenfound to exceed expected levels. Because inherent
127Vol. 69, No. 1, January–February 2015
on August 15, 2018journal.pda.orgDownloaded from

particle by its nature is product specific, assessing itssafety is considered out of the scope of this document.Importantly, products with inherent particles shouldbe characterized fully and both the product quality andthe patient safety impacts should be analyzed withsimilar risk assessment considerations as laid out inthis document.
Particle Size
While particles of varying size have been observed ininjectable drug products, they are generally classifiedinto one of two categories; visible and subvisible.Visible particles are defined as those that can bedetected under controlled conditions by the unaidedhuman eye (i.e., without supplemental magnification)(2, 33, 35). As a reference, studies have demonstratedthat under idealized conditions, trained inspectors per-forming the pharmacopeia inspection method will be-gin to have reliable detection of near 70% efficiencywhen particle sizes reach 150 �m (38). The 150 �mthreshold should be considered a best-case thresholdfor human visual identification of particles in inject-able drug products given that it represents idealizedinspection conditions. Any changes in product, con-tainer, or particle material from those idealized con-ditions will cause the visible detection threshold toshift above 150 �m. There are specific nonzero limitsin the pharmacopeias for subvisible particles �10 �mand �25 �m. The subvisible particle category coversmaterials ranging in size from submicron up to thevisible threshold. The limits are harmonized in theUSP, EP, and JP and are 6,000 and 600 per container,respectively, for containers � 100 mL.
Pathophysiological Considerations andClinical Implications
The effects of particles in injectable drug productshave been discussed in the medical literature for de-cades (42– 47), and are based on in vitro studies, someanimal data, human case reports, and small observa-tional studies. Human data is limited because it isethically impossible to prospectively test the impact ofparticles in injections. Further, even if particulate mat-ter is administered to a patient, the clinical impact canbe hard to assess or even may be unnoticed or asymp-tomatic. Potential clinical sequella could, in somecircumstances, be indistinguishable from an underly-ing disease or other treatment impact. The literatureoften contains the most extreme examples from intra-venous drug abuse and hyperalimentation. Given these
limitations, it’s best to understand potential harm topatients based on an understanding of the pathophys-iology of particle infusion.
The type and degree of clinical impact is dependent onmultiple factors, including the route of administration,the size and amount of the particle(s) injected, andpatient factors such as underlying health status. Al-though there are limited data on human exposure toinfused particles, it is estimated that “patients in in-tensive care units may receive more than a millioninjected particles �2 �m daily” (48). As such, parti-cles could theoretically have meaningful clinicalimpact if highly experimental animal studies areconsidered appropriate surrogates (49, 50, 51). Asan example, ICU patients are at greater risk ofconsequences of particle infusion, due to their needfor continuous infusion of parenteral solution, in-cluding that for hyperalimentation.
Many injectable drugs are administered intramuscu-larly and subcutaneously. Intramuscularly and subcu-taneously administered drugs containing particlesgenerally have minimal impact on patient health.Complications from subcutaneous and intramuscularmedications generally arise from the irritating proper-ties of the drug product and are often drug-specific(52). For particles that are primarily mechanical ob-structions and inert (e.g., cellulose, metal, or glass),the composition of a particle is not critical to clinicalimpact except for impact on sterility, which is dis-cussed below. Subcutaneous administration of small,inert, sterile particles would not be expected to inducea clinically significant reaction beyond minor irritationor perhaps a small granuloma (53). Likewise for in-tramuscular injections, Greenblatt and Allen looked at26,294 hospitalized medical patients, 46% of whomreceived at least one intramuscular injection, findingthat clinically apparent local complications are un-commonly (less than 0.4%) associated with IM injec-tions (54). In consideration of glass particles in par-ticular, glass fragments from tubular and molded glasscan generally be considered inert, and in small quan-tities they are not likely to cause significant injuries.However, the special case of glass lamellae which canbe either visible or subvisible can be present in largenumbers and can increase in number with time, canhave a higher clinical impact if administered in largevolumes.
Whenever a drug is injected into a contained space, forexample, intraocular or intrathecal use, there may be
128 PDA Journal of Pharmaceutical Science and Technology
on August 15, 2018journal.pda.orgDownloaded from

more risk for inflammation from particles or a particlemay serve as a nidus for infection, causing harm (55).There are limited data, but the presence of particles insolutions for intrathecal use has been reported fromuse of drugs within glass ampoules (56). The averagenumber of particles was 17 (7–38) with a range in sizefrom 15 �m to 80 �m. At the time of the study, theincidence of central nervous system complication fol-lowing subarachnoid anesthesia was low. The authorsnote that a foreign body reaction may have resultedand may account for the reported events of chemicalmeningitis.
Intravenous infusion of particles might result in phle-bitis due to particles causing direct traumatic damageto the vein, or chemical damage from undissolvedparticles, or infection if the particle is non-sterile.Non-dissolvable particle matter will become trappedin small vessels or capillary beds, when the introducedparticle is larger than the vessel. The diameter of thesmallest capillary or blood vessel is about 7 �m in anadult (57) and the diameter of a pulmonary capillary,which is approximately 10-15 �m, just larger than thesize of red blood cells which are responsible for oxy-genation of blood as they travel through the pulmo-nary vasculature. Therefore any intravenously admin-istered particles greater than 7 �m but less than 10 �mmay occlude some capillaries. If pulmonary capillariesare compromised in the presence of microemboli (pul-monary embolism), the clinical consequence is im-paired oxygen transfer and compromised respiratoryfunction (58). Smaller particles (�7 �m) will gener-ally be phagoctised by macrophages and ultimatelydeposited in spleen or liver. Massive amounts of sub-visible particles might not be phagocystosed andmight then be deposited in other organs, especially thekidney. In general the clinical consequences are neg-ligible because most organ systems have significantreserve capacity (30, 31).
The clinical impact from an occluded vessel is depen-dent on many variables, including the size of thevessel affected as well as the number of vessels sup-plying a particular organ. In many instances, theremay be no clinical impact as some tissues or organshave extensive blood vasculature so that numerousvessels may be feeding the same tissue. Therefore, oneor numerous occluded small vessels may have noclinical significance or patient symptoms. In fact, solidparticle microemboli are a recognized complication ofextracorporeal circulation in open-heart surgery (59 –62). Microsphere infusion during bypass in laboratory
animals showed pulmonary ultrastructure damage wasproportionally related to particles increasing in sizefrom 20 �m to 75 �m. After simple perfusion of theextracorporeal circuit, Liu reported that the 15 to 80�m particle count reached 199 � 69 per mL (63).Despite these risks, the clinical benefits outweigh therisks, justifying why extracorporeal circulation hascontinued to be used in open-heart surgery. This high-lights that risk alone is but one consideration whenassessing the use of products and should not be theonly consideration when assessing impact.
Numerous animal studies have been conducted to de-termine the fate of intravenous particles of differingsize and composition (29, 51, 64, 65). Most studieshave focused on subvisible particles, with a diameterof less than 50 �m. In these studies, the infusion ofmassive quantities of particles has been accompaniedby histologic evidence of injury to pulmonary capil-lary endothelial cells (63), microscopic thrombi in thepulmonary capillaries (66), microscopic pulmonarygranulomata (67), and hepatic inflammatory effects(68). In a hamster model using antibiotics with sub-visible and visible particles, capillary perfusion wasjeopardized in posthypoxic tissue but not in normallyperfused tissue (24). While useful in understanding thepathophysiologic response to intravenous particle ex-posures, the large mass of particles employed in theseanimal studies provides little guidance on the risk ofsmall numbers of macroscopic particles to human pa-tients.
There are limited data on human exposure to infusedparticles. Clinically detectable patient harms from par-ticle injection are difficult to detect even if suspected,suggesting minimal short-term impact. Garvin andGunner were among the first to report a concern aboutthe effects of particles in human patients, findingpostmortem pulmonary vasculature granulomas (cel-lulose fiber) in the lungs of patients who had receivedlarge volumes of IV fluids (69, 70). For obvious eth-ical reasons, there is a lack of controlled human stud-ies on the effect of particles in human patients. How-ever, clinical events from total parenteral nutrition(TPN) complications, intravenous drug use, and car-diopulmonary bypass provide relevant information onthe effects of high (and prolonged) particle exposure(these are specific and not necessarily generalizablecircumstances).
The American Society of Parenteral and Enteral Nu-trition (ASPEN) Guidelines note particles of 5 to 20
129Vol. 69, No. 1, January–February 2015
on August 15, 2018journal.pda.orgDownloaded from

�m and larger are capable of obstructing blood flowthrough the pulmonary capillaries, which could lead tocomplications such as pulmonary embolism (42). Areview of the literature reveals a case report of adyspneic patient receiving TPN who had diffuse �1mm micronodules on computerized tomography exam-ination, elevated pulmonary artery pressures, and, onpostmortem, amorphous material microemboli in thepulmonary vasculature (71). This finding highlightsthat particles may have a clinical impact when admin-istered over an extended period of time with multipleexposures (72). Hyperalimentation associated with in-herent particles (calcium and phosphate) administeredto pigs has been shown to cause respiratory distressand sudden death with amorphous calcium-phosphateprecipitant debris (71).
Additional anecdotal information for human patientrisk may be obtained from the examination of casereports involving intravenous drug abusers (68, 73,74). In these cases, a powder or pulverized tablet issuspended in a vehicle, then variably filtered throughcotton (75). These patients may develop dyspnea andshow reduced pulmonary function testing (72). Cut-ting agents or excipients such as microcrystalline cel-lulose, talc, and starch have been identified in pulmo-nary, foreign-body emboli and granulomas in theseindividuals (75–77). In one instance, the particleslodged in the pulmonary arteriole, causing inflamma-tion and thrombosis, subsequently eroding through thearteriolar wall and becoming a giant cell granuloma(77). Talc granulomas in organs other than the lungswere found to be of negligible clinical significance(78). Niden and Aviado (1956) found that experimen-tal intravenous injection of a given mass of glass beadsproduced greater pulmonary dysfunction with smallerparticle sizes suggesting systemic effects might berelated to surface area rather than size of particles(58). Importantly, the meaningful clinical risks to hu-man patients are difficult to infer from these observa-tions of extreme cases of particle infusion that result inchronic exposure, extremes in mass, number, and di-versity of foreign particles, as well as the uncontrolledconditions in which they were administered.
In another paper where embolization events resulted ina less extreme case in regards to number of events,Baydur et al. demonstrated that prolonged indwellingcentral venous catheter use may degrade and lead toembolization of catheter material (79). This occurredin a patient where the catheter particles entered thepulmonary circulation. This patient required a central
venous catheter for more than five years, and numer-ous catheters were utilized in this time period. Thepatient was clinically asymptomatic throughout thattime and four years later developed symptoms ofsarcoidosis that included granuloma formation of theskin. The patient required further evaluation, includ-ing an open-lung biopsy, which revealed pulmonarygranulomas of two distinct types, that from sarcoidosisand the other of catheter material. The author reportsthe two granulomatous processes were unrelated. Thispaper and case reports of IV drug abusers highlightthat a localized pulmonary inflammatory response maybe more likely to result from particles than pulmonaryembolism or clinically symptomatic tissue damage.
Perhaps more relevant are clinical results of arterialembolization procedures performed using materialssuch as polyvinyl alcohol embolic agents (80), colla-gen-coated acrylic microspheres, and gelatin spheres(81). These procedures provide us some insight on thepotential human pathophysiologic outcomes due tonon-target embolization within intravenous infusions(82). These procedural reported cases involved mas-sive, 300 –500 �m particle loads moving from thearterial injection site into the venous circulation.While these embolization procedures did result in theintended thromboembolic event, they have not re-sulted in significant long-term consequences from ma-terial that would be considered extrinsic particles formost, if not all, drug products (27, 83– 87).
In the presence of an abnormal communication be-tween the venous and arterial systems, intravenouslyadministered particles can bypass the lung and itsvasculature. Aberrant anatomy might be known, forexample fistulae for renal dialysis, or unknown forexample, up to 30% of the adult population has apatent foramen ovale that allows for a right to left shiftof the blood circulation within the heart and bypassesthe lungs (38). This allows for the possibility of par-ticles to enter directly into the central vascular system,with potential complications to include ischemicstroke and myocardial ischemia, or into the peripheralvascular system, where peripheral vascular ischemiamay result. In addition, end organ damage can occurthrough deposition or embolism of particle into theorgan vasculature. Further, even with an intact normalvascular anatomy, particles less than 10 �m may passthrough the lung’s circulation, into the peripheral cir-culation, and deposit in other organs, such as the liver,kidney, and spleen. Patients with existing end-organ
130 PDA Journal of Pharmaceutical Science and Technology
on August 15, 2018journal.pda.orgDownloaded from

disease and small-vessel disease may be considered atgreater risk.
In summary, particle administration has a low proba-bility of clinically significant injury on the vascularsystem, and current hypothetical assessments are over-estimated. Clearly some impact can exist, but cases areinfrequent and often associated with extreme risk sit-uations. Data suggest administration of a large volumeof particles over time, the use of hyperalimentationand large volumes of small size particles may causeclinical damage. Small amounts of inert particles areunlikely to cause clinically meaningful patient harm.In addition, intramuscular and subcutaneous injections ofsterile inert particles are very unlikely to cause meaning-ful patient injury. Further consideration should howeverbe given to patients with end-organ disease, immune-compromised, or neonates and infants, as well as whenparticles are injected into closed spaces (e.g., intrathecal,intraocular, intraarticular) as these situations may have agreater potential for harm.
Risk Assessment
To assess the potential impact of the particle to thepatient, a risk assessment should be performed inaccordance with recognized guidance documents andstandards (88). In the International Conference onHarmonisation Quality Guideline Q9: Quality RiskManagement, “risk is defined as the combination ofthe probability of occurrence of harm and the severityof that harm” (89). In relation to particles, whenassessing the risk to the patient population, the assess-ment can be reduced into the likelihood for the hazardto occur and the severity of the harm or clinicallysignificant outcome that might occur to the patient dueto the hazard. The risk is derived after assessing thelikelihood of the harm against the severity of the harmunder specific circumstances. Differentiation shouldbe made between the likely general population and asubset of patients who might be most at risk.
Noting that post-hoc process controls should not beused as a safety-net for poor manufacturing methods,the risk assessment needs to consider the possibletypes of clinical impact the patient might experienceand assess whether the harm would be likely to occurgiven the specific circumstances. Some products areknown to have a risk for precipitant, and labeling andstandard use reflect this understanding and the impor-tance for product inspection prior to use within thepharmacy as well as at patient bedside. The assess-
ment should account for standard clinical practice toreflect real-world use.
The severity of harm is determined based on thepotential clinical impact that the patient will experi-ence due to administering product from the affectedlot. Severity can be rated as temporary discomfort allthe way to patient death. Potential harms, as discussedin the Pathophysiology section, may include phlebitis,granuloma, and occlusion or thromboembolic events,each with differing severity levels of harm. For exam-ple, an otherwise healthy individual receiving a sub-cutaneous or intramuscular injection containing a sin-gle sterile extraneous inert particle would likelyexperience no adverse effect or at worst develop asmall granuloma. The severity of the harm may beconsidered minor with no need for medical interven-tion. By comparison, a critically ill premature infantreceiving a particle-laden infusion directly through anumbilical catheter might suffer permanent or life-threatening injury (47, 90). This outcome may beconsidered critical, as a life-threatening situationarose. In some situations, permanent injury may resultand should be considered in determining the degree ofseverity of the harm.
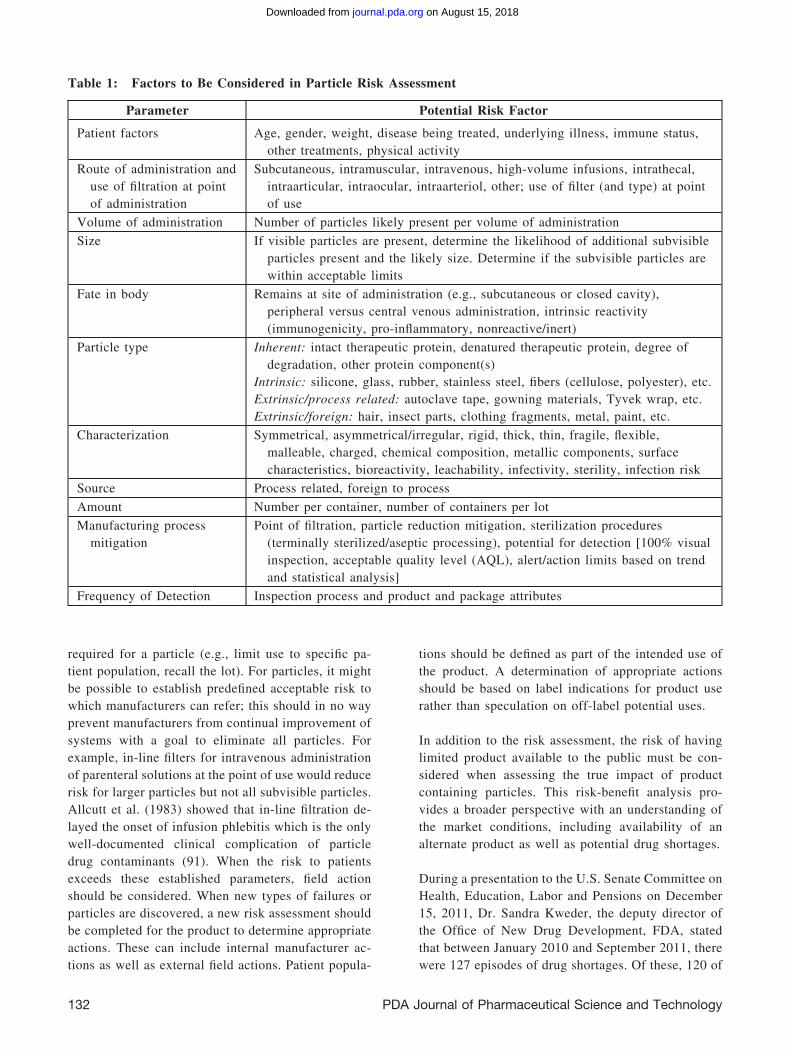
The scope of this paper does not allow the creation ofa specific template to consider risk; however, thefactors presented in Table 1 should be taken intoconsideration in such an assessment.
A key consideration is to assess the source of theparticle and to assess the risk to the sterility of thedrug product in this regard. The impact might bemodified by additional manufacturing variables, suchas terminal sterilization (as compared to aseptic fill-ing) for determination of possible microbial contami-nation. Thus, understanding the manufacturing pro-cess and where the particles were introduced into theproduct is important in understanding the overall riskto the sterility assurance of the product. Microbialcontamination and/or endotoxin introduction into theproduct should be considered in addition to patho-physiological considerations for particles in order forhealth care professionals to have a comprehensiveunderstanding of potential impact to the patient.
As previously stated, the overall risk is determined byassessing the likelihood of harm, which may be deter-mined qualitatively or quantitatively, occurringagainst the severity of the harm. Based on the assess-ment, a determination can be made as to the actions
131Vol. 69, No. 1, January–February 2015
on August 15, 2018journal.pda.orgDownloaded from
required for a particle (e.g., limit use to specific pa-tient population, recall the lot). For particles, it mightbe possible to establish predefined acceptable risk towhich manufacturers can refer; this should in no wayprevent manufacturers from continual improvement ofsystems with a goal to eliminate all particles. Forexample, in-line filters for intravenous administrationof parenteral solutions at the point of use would reducerisk for larger particles but not all subvisible particles.Allcutt et al. (1983) showed that in-line filtration de-layed the onset of infusion phlebitis which is the onlywell-documented clinical complication of particledrug contaminants (91). When the risk to patientsexceeds these established parameters, field actionshould be considered. When new types of failures orparticles are discovered, a new risk assessment shouldbe completed for the product to determine appropriateactions. These can include internal manufacturer ac-tions as well as external field actions. Patient popula-
tions should be defined as part of the intended use ofthe product. A determination of appropriate actionsshould be based on label indications for product userather than speculation on off-label potential uses.
In addition to the risk assessment, the risk of havinglimited product available to the public must be con-sidered when assessing the true impact of productcontaining particles. This risk-benefit analysis pro-vides a broader perspective with an understanding ofthe market conditions, including availability of analternate product as well as potential drug shortages.
During a presentation to the U.S. Senate Committee onHealth, Education, Labor and Pensions on December15, 2011, Dr. Sandra Kweder, the deputy director ofthe Office of New Drug Development, FDA, statedthat between January 2010 and September 2011, therewere 127 episodes of drug shortages. Of these, 120 of
Table 1: Factors to Be Considered in Particle Risk Assessment
Parameter Potential Risk Factor
Patient factors Age, gender, weight, disease being treated, underlying illness, immune status,other treatments, physical activity
Route of administration anduse of filtration at pointof administration
Subcutaneous, intramuscular, intravenous, high-volume infusions, intrathecal,intraarticular, intraocular, intraarteriol, other; use of filter (and type) at pointof use
Volume of administration Number of particles likely present per volume of administration
Size If visible particles are present, determine the likelihood of additional subvisibleparticles present and the likely size. Determine if the subvisible particles arewithin acceptable limits
Fate in body Remains at site of administration (e.g., subcutaneous or closed cavity),peripheral versus central venous administration, intrinsic reactivity(immunogenicity, pro-inflammatory, nonreactive/inert)
Particle type Inherent: intact therapeutic protein, denatured therapeutic protein, degree ofdegradation, other protein component(s)
Intrinsic: silicone, glass, rubber, stainless steel, fibers (cellulose, polyester), etc.Extrinsic/process related: autoclave tape, gowning materials, Tyvek wrap, etc.Extrinsic/foreign: hair, insect parts, clothing fragments, metal, paint, etc.
Characterization Symmetrical, asymmetrical/irregular, rigid, thick, thin, fragile, flexible,malleable, charged, chemical composition, metallic components, surfacecharacteristics, bioreactivity, leachability, infectivity, sterility, infection risk
Source Process related, foreign to process
Amount Number per container, number of containers per lot
Manufacturing processmitigation
Point of filtration, particle reduction mitigation, sterilization procedures(terminally sterilized/aseptic processing), potential for detection [100% visualinspection, acceptable quality level (AQL), alert/action limits based on trendand statistical analysis]
Frequency of Detection Inspection process and product and package attributes
132 PDA Journal of Pharmaceutical Science and Technology
on August 15, 2018journal.pda.orgDownloaded from

the product shortages involved sterile injectable drugs(92). Further, 54% of these had product quality issues(particles, microbiologic contaminants, impurities,and stability concerns). The availability of injectabledrug products to patients due to potential risk from asingle vial containing a particle creates an additionalconcern for patient safety. An outcome of a seriousadverse event may be the exception and not the rulefor injectable drug products with limited numbers ofparticles present in product released as “essentiallyfree” of particles.
Quality Risk Management
The frequency or rate at which the particle is likely tooccur should be determined and based on objectivedata. The presence of particles, for example, can occuras a single particle or as multiple particles containedwithin a single unit. One must consider the distribu-tion of these particles, that is, whether the particle isan isolated event or its detection may implicate otherunits or batches. Further consideration should also begiven to other products manufactured on the sameproduction line.
A determination needs to be made as to how often thehazard, particles in this case, is likely to occur withina lot of product or across product lots. This assessmentneeds to take into account how widespread the particlehazard might be (e.g., one particle in one vial of onebatch of product or ten particles in two hundred vialswithin twenty batches of product). To make this de-termination, a manufacturing site needs to conserva-tively assess the potential causes of the hazard anddetermine how long these potential causes have beenoccurring. Ultimately, even if the product is within thespecified AQL, it is incumbent on the manufacturer tounderstand leading and lagging trends over time.
Manufacturers are encouraged to take a life-cycle ap-proach to understand where particles may be gener-ated, detected, and removed in a production process.Characterization of defects at the time of manufacturecan provide valuable insights into the overall under-standing of particle generation and subsequent mitiga-tion to reduce the level of particles in products. Ex-amples of items to review to determine a failure rateinclude, but are not limited to, the following: com-plaint data (trends or spikes), exception report/CAPArecords, manufacturing batch records, supplier incom-ing reports/data, and inspection results of inventory aswell as of retained samples. From this analysis, the
manufacturing site can estimate at a base level thelikelihood of occurrence for particles within the af-fected lot or lots of product.
Conclusion: Overall Medical Risk
Advances in process capability to reduce the particleburden, and continued vigilance for particles, haveresulted in reported injuries being rare and mostappear limited to the case reports associated with theinfusion of significant quantities of precipitated ad-mixtures. Additionally, macroscopic particles aremore likely to be discovered prior to administration orcan be too large to pass through the lumen of a needle.Further, even when larger particles are used purpose-fully to occlude AVMs (and they have been shown tocross into the venous circulation), there is rarely sig-nificant sequelae observed for these patients who areunder close observation. However, clinical data sug-gests that product conforming to compendial particlelimits can contain subvisible particles, which, canresult in patients being exposed to low levels of par-ticles as part of the practice of routine health care. Theintravenous infusion of rigid particles greater than the10-12 �m diameter of a pulmonary capillary will beocclusive. Once infused or injected an aggregate num-ber of subvisible particles might impart a similarpathophysiological effect as a macroscopic particle,but more importantly, it is increasingly recognizedthat subvisible aggregates might induce an untowardimmune response (27). Thus, the often prevailing as-sumption, that larger particles pose a greater risk topatients rather than smaller particles, maybe a miscon-ception.
An estimated 15 billion injectable doses of medicinesare administered worldwide each year (1). The evi-dence in this paper suggests that true patient harmassociated with injections is extremely limited at thecurrent level of particle matter contained therein.While manufacturing processes, recall procedures, andclinical practices all contribute to this current state,current processes and procedures seem adequate.Small amounts of inert particles are unlikely to causeclinically meaningful patient harm. In addition, intra-muscular and subcutaneous injections of sterile inertparticles are very unlikely to cause meaningful patientinjury. Further consideration should however be givento patients with end-organ disease, immune-compro-mised, or neonates and infants, as well as when par-ticles are injected into closed spaces (e.g., intrathecal,intraocular, intraarticular) as these situations may have
133Vol. 69, No. 1, January–February 2015
on August 15, 2018journal.pda.orgDownloaded from

a greater potential for harm. There is insufficient ev-idence to conclude that intravenous injection of inertvisible particles results in harm to patients (47, 71,93).
As there is limited direct evidence of patient risk dueto sterile, inert particles, it is reasonable to concludezero tolerance should not be the requirement, butinstead considered as the goal in manufacturing inject-able drug products (72, 90, 93). Despite manufacturingprocess improvements and an increased surveillancewith improved detection methodology, the manufac-ture of particle-free injectable product is not techni-cally feasible, but continuous process improvement isan expectation.
A pragmatic approach ensuring high-quality drugs areavailable to patients is provided by USP �790�. Thischapter requires a robust quality management systemwith a 100% inspection process, particle identificationprocess, and a good investigation and monitoring pro-cess to ensure the occurrence and composition ofparticulates are understood. The composition of theparticulate matter is very important when consideringthe medical significance when performing a risk as-sessment. To understand the composition, a firmwould need a system to identify the particulate matterfound in the drug product. USP �790�, together witha medical risk-based approach, offers a practical strat-egy to ensure manufacturers meet expectations forvisible particles. This standard was written consider-ing both current manufacturing capability and patientrisk. Following the recommendations in USP �790�will provide the minimum expectations for manufac-turing standards. For low-risk routes of administra-tion, such as intramuscular and subcutaneous injec-tions, the acceptance criterion of an AQL of 0.65%based on USP �790�, ensures the adequate safety ofthe product. There may be clinical circumstanceswhere tighter AQL values (limits) may be appropriatefor high-risk patients and for other routes of adminis-tration based on an evaluation of patient risk.
Globally, clinicians and patient populations are facingdrug shortages, in part due to inconsistent productrelease and recall decisions related to the presence ofparticles and a lack of understanding of the impact topatient risk. Safety considerations related to particlesin injectable drug products must be assessed on thebasis of the factors identified in this paper, whichinclude the intended patient population and method ofadministration. The decision to recall product from the
market should be based on the context of the manu-facturing trend history, complaint rate trending, andmedical assessment of patient risk. Unless there arespecific special circumstances, there should be no au-tomatic requirement to recall a product lot for a singleparticle found in a single unit. While manufacturersstrive to remove particles from injectable products,this paper has outlined considerations important toassessing the risk-benefit ratio of administering prod-uct to a patient. In general, notwithstanding high riskclinical circumstances and acknowledging there arelimitations to reporting clinical events to particle in-fusion, the existing data suggest the overall risk topatients is generally low and the benefit of thesetreatments is generally significant.
References
1. Injectable Drug Delivery: Probing the Route toGrowth. Datamonitor, January 2004. http://www.datamonitor.com/Products/Free/Report/DMHC1964/010DMHC1964.pdf (accessed July9, 2014).
2. General Chapter �790� Visible Particulates inInjections. USP 37/NF 32; U.S. Pharmacopeia:2014. www.usp.org.
3. Lynn, S. Drug Defects. Presented at the 37thInternational Good Manufacturing Practices Con-ference. Mar 14, 2013, Athens, GA.
4. EudraLex, Inspections. An Analysis of Quality Prod-uct Defects in the Centralised Procedure; EuropeanCommission: 2007. http://www.ema.europa.eu/docs/en_GB/document_library/Regulatory_and_procedural_guideline/2009/10/WC500004420.pdf(accessed July 9, 2014).
5. EudraLex, Standard Operating Procedure—Annex4, Crisis Management Regarding Defects of Cen-trally Authorised Products: Classification of BatchRecalls for Quality Defects; European Commission:2012. http://www.ema.europa.eu/docs/en_GB/document_library/Regulatory_and_procedural_guideline/2009/10/WC500004404.pdf (accessedJune 30, 2014).
6. MHRA Drug Alerts website. http://www.mhra.gov.uk/Publications/Safetywarnings/DrugAlerts/index.htm (accessed June 30, 2014).
134 PDA Journal of Pharmaceutical Science and Technology
on August 15, 2018journal.pda.orgDownloaded from
7. MHRA Publications and Consultations, SafetyWarnings, Drug Alerts. Class 2 Medicines Recall(action within 48 hours): Fybogel Hi-Fibre and Fy-bogel Orange manufactured by Reckitt BenckiserHealthcare (UK) Limited (EL (14)A/08). http://www.mhra.gov.uk/Publications/Safetywarnings/DrugAlerts/CON426907 (accessed June 30,2014).
8. MHRA Publications and Consultations, SafetyWarnings, Drug Alerts. Class 2 Medicines Recall(action within 48 hours): Fybogel Orange—Reckitt Benckiser Healthcare (UK) Limited (EL(14)A/04). http://www.mhra.gov.uk/Publications/Safetywarnings/DrugAlerts/CON392875 (ac-cessed June 30, 2014).
9. MHRA Publications and Consultations, SafetyWarnings, Drug Alerts. Class 2 Medicines Recall(action within 48 hours): Clarithromycin 500mgPowder for Solution for Infusion in Agila liverymanufactured by Strides Arcolab InternationalLimited (EL (14)A/07). http://www.mhra.gov.uk/Publications/Safetywarnings/DrugAlerts/CON426899 (accessed June 30, 2014).
10. MHRA Publications and Consultations, SafetyWarnings, Drug Alerts. Class 2 Medicines Recall(action within 48 hours): Vancomycin Powder forConcentrate for Solution for Infusion manufacturedby Actavis Group PTC ehf (EL (14)A/06). http://www.mhra.gov.uk/Publications/Safetywarnings/DrugAlerts/CON425132 (accessed June 30, 2014).
11. MHRA Publications and Consultations, SafetyWarnings, Drug Alerts. Class 2 Medicines Recall(action within 48 hours): Viread 245 mg Film-Coated Tablets—Gilead Sciences Limited (EL(14)A/03). http://www.mhra.gov.uk/Publications/Safetywarnings/DrugAlerts/CON391205 (ac-cessed June 30, 2014).
12. U.S. Code of Federal Regulations Title 21 Part7.3(m): Definitions. ecfr.gpoaccess.gov (accessedSep. 2, 2014).
13. Turco, S.; Davis, N. Glass Particles in IntravenousInjections. New Engl. J. Med. 1972, 287, 1204 –1205.
14. Dempsey, G. Hazards of Particle Injection.Pharm. J. 1983, July 16, 63– 64.
15. Davis, N. M.; Turco, S.; Sivelly, E. A Study ofParticulate Matter in I.V. Infusion Fluids. Am. J.Hosp. Pharm. 1970, 27, 822– 826.
16. Backhouse, C. M.; Ball, P. R.; Booth S.; Kelshaw,M. A.; Potter, S. R.; McCollum, C. N. ParticulateContaminants of Intravenous Medications and In-fusions. J. Pharm. Pharmacol. 1987, 39, 241-245.
17. U.S. Food and Drug Administration (FDA). Multi-ple product recall notifications, 2009–2012. http://www.fda.gov/Drugs/DrugSafety/DrugRecalls/default.htm (accessed March–April 2012).
18. FDA Recalls, Market Withdrawals, and SafetyAlerts. Bedford Laboratories Issues a VoluntaryNationwide Patient Level Recall of Acetylcys-teine Solution, USP, LOT 1877093. Press release,February 2, 2012. http://www.fda.gov/Safety/Recalls/ucm290204.htm (accessed June 19, 2014).
19. FDA Recalls, Market Withdrawals, & Safety Alerts.American Regent Initiates Nationwide VoluntaryRecall of Methyldopate HCL Injection, USP 5 mLSingle Dose Vial Due to Glass Particulates. Pressrelease, June 6, 2011. http://www.fda.gov/Safety/Recalls/ucm258064.htm (accessed June 19, 2014).
20. FDA Recalls, Market Withdrawals, and SafetyAlerts. American Regent Initiates NationwideVoluntary Recall of Caffeine & Sodium BenzoateInjection, USP 250 mg/mL, 2 mL Single DoseVial Due to Visible Particulates. Press release,May 5, 2011. http://www.fda.gov/Safety/Recalls/ArchiveRecalls/2011/ucm254287.htm (accessedJune 19, 2014).
21. MHRA Publications and Consultations, SafetyWarnings, Drug Alerts. Class 4 Drug Alert: B.BraunMedical Ltd—NuTRIflex Lipid Products (EL(11)A/32). http://www.mhra.gov.uk/Publications/Safetywarnings/DrugAlerts/CON137913 (accessedJune 19, 2014).
22. MHRA Publications and Consultations, SafetyWarnings, Drug Alerts. Class 2 Drug Alert (Ac-tion within 48 hours): Abraxis BioScience Ltd—Abraxane 5mg/ml powder for suspension for in-fusion (EL (09)A/28). http://www.mhra.gov.
135Vol. 69, No. 1, January–February 2015
on August 15, 2018journal.pda.orgDownloaded from
uk/Publications/Safetywarnings/DrugAlerts/CON062632 (accessed June 19, 2014).
23. Schroeder H.G.; DeLuca, P.P. Particulate MatterAssessment of a Clinical Investigation on Filtrationand Infusion Phlebitis. AJHP. 1976, 33, 543–546.
24. Lehr, H.-A.; Brunner, J.: Rangoonwala, R.; Kirk-patrick, C. J. Particulate Matter Contamination ofIntravenous Antibiotics Aggravates Loss of Func-tional Capillary Density in Postischemic StriatedMuscle. Am. J. Respir. Crit. Care Med. 2002, 165,514 –520.
25. Macdougall, I. C.; Roger, S. D.; de Francisco, A.;Goldsmith, D. J. A.; Schellekens, H.; Ebbers, H.;Jelkmann, W.; London, G.; Casadevall, N.; Hörl,W. H.; Kemeny, D. M.; Pollock, C. Antibody-Mediated Pure Red Cell Aplasia in Chronic Kid-ney Disease Patients Receiving Erythropoiesis-Stimulating Agents: New Insights. Kidney Int.2012, 81 (8), 727–732.
26. Singh, K. S. Impact of Product-Related Factors onImmunogenicity of Biotherapeutics. J. Pharm.Sci. 2011, 100, 354 –387.
27. Carpenter, J. F.; Randolph, T. W.; Jiskoot, W.;Crommelin, D, J.; Middaugh, R. C.; Winter, G.;Fan, Y.-X.; Kirshner, S.; VerthelyI, D.; Kozlow-ski, S.; Clouse, K. A.; Swann, P. G.; Roseberg, A.;Cherney, B. Overlooking Subvisible Particles inTherapeutic Protein Products: Gaps That MayCompromise Product Quality. J. Pharm. Sci.2009, 98 (4), 1201–1205.
28. Watson, R.; Strab, J. Manual Inspection Capabil-ity to Detect Particulate in Parenterals. Presentedat the 2013 PDA Visual Inspection Forum, Oct7– 8, 2013, Bethesda, MD.
29. Brewer, J. H.; Dunning, J. H. F. An In Vitro andIn Vivo Study of Glass Particles in Ampules.J. Am. Pharm. Assoc. 1947, 36 (10), 289 –293.
30. Stehbens, W.E.; Florey, H.W. The Behaviour ofIntravenously Injected Particles Observed inChambers in Rabbits’ Ears. Q.J. Exp. Physiol.1960, 45, 252–264.
31. Schoenberg, M.D.; Gilman, P.A.; Mumaw, V.R.;Moore, R.D. The Phagocytosis of Uniform Poly-
styrene Latex Particles (PLP) by the Reticulo-Endothelial System (RES) in the Rabbit. Brit. J.Exp. Pathol. 1961, 42 (5), 486 – 495.
32. General Chapter �1� Injections. USP 36/NF 31;U.S. Pharmacopeia: 2013. www.usp.org.
33. Chapter 2.9.20, Particulate Contamination: Visi-ble Particles; European Pharmacopeia: 2013.
34. Eudralex, Guideline on Production and QualityControl of Monoclonal Antibodies and Related Sub-stances; European Commission: 2007. http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003073.pdf (accessed July 9, 2014).
35. Chapter 6.06, Foreign Insoluble Matter Test forInjections; Japanese Pharmacopeia: 2011 http://db.yaozh.com/foreign/JP15/jp1/F1_70.pdf (ac-cessed July 9, 2014).
36. Knapp, J. Z; Kushner, H. R. Generalized Meth-odology for Evaluation of Parenteral InspectionProcedures. PDA J. Pharm. Sci. Tech. 1980, 34(1), 14 – 61.
37. Knapp, J. Z; Kushner, H. R. Implementation andAutomation of a Particle Detection System forParenteral Products. PDA J. Pharm. Sci. Tech.1980, 34 (5), 369 –393.
38. Shabushnig, J. G.; Melchore, J. A.; Geiger, M.;Chrai, S.; Gerger, M. E. A Proposed Working Stan-dard for Validation of Particulate Inspection in Ster-ile Solutions. Paper presented at the PDA AnnualMeeting, Philadelphia, November 2–4, 1995.
39. General Chapter �788� Particulate Matter in In-jections; USP 37/NF 32; U.S. Pharmacopeia:2011. www.usp.org.
40. Monograph for Monoclonal Antibodies for Hu-man Use; European Pharmacopeia: 2013.
41. Circulaire N°10-0224 Direction Des AffairesScientifiques, Pharmaceutiques Et MedicalesAFSSAPS Form n° 2 – Complaints “glass parti-cles in injectable products,” (Notification of“glass particles in injectable products”) April 19,2010.
136 PDA Journal of Pharmaceutical Science and Technology
on August 15, 2018journal.pda.orgDownloaded from
42. Mirtallo, J.; Canada, T.; Johnson, D.; Kumpf, V.;Petersen, C.; Sacks, G.; Seres, D.; Guenter, P.Special Report: Safe Practices for Parenteral Nu-trition. JPEN J. Parenter. Enteral Nutr. 2004, 28(6), S39 –S70.
43. Thomas, W. H.; Lee, Y. K. Particles in Intrave-nous Solutions: A Review. New Zeal. Med. J.1974, 80, 170 –178.
44. Borchert, S. J.; Abe, A.; Aldrich, S. D.; Fox, L. E.;Freeman, J. E.; White, R. D. Particulate Matter inParenteral Products: A Review. PDA J. Pharm.Sci. Tech. 1986, 40 (5), 212–241.
45. Groves, M. J.; De Malka, S. R. The Relevance ofPharmacopeial Particulate Matter Tests. Drug De-velopment Communications, 1976, 2, 285–324.
46. Groves, M. J. Parenteral Products: The Prepara-tion and Quality Control of Products for Injec-tion; William Heinemann Medical Books: Lon-don, 1973.
47. Groves, M. J. Particulate Matter: Sources andResources for Healthcare Manufacturers; Interp-harm Press: Buffalo Grove, IL, 1993.
48. Langille, S. E. Particulate Matter in InjectableDrug Products. PDA J. Pharm. Sci. Tech. 2013,67, 186 –200.
49. Xie, Guangping; Sun, Jiao; Zhong, Gaoren; Shi,Liyi; Zhang, Dawei. Biodistribution and Toxicityof Intravenously Administered Silica Nanopar-ticles in Mice. Arch Toxicol. 2010, 84, 183–190.
50. Cho, M.; Cho, W.-S.; Choi, M.; Kim, S. J.; Han,B. S.; Kim, S. H.; Kim, H. O.; Sheen, Y. Y.;Jeong, J. The Impact of Size on Tissue Distribu-tion and Elimination by Single Intravenous Injec-tion of Silica Nanoparticles. Toxicol Lett. 2009,189, 177-183.
51. Hozumi, K.; Kitamura, K.; Kitade, T.; Iwagami,S. Localization of Glass Particles in Animal Or-gans Derived from Cutting of Glass AmpoulesBefore Intravenous Injections. Microchem. J.1983, 28, 215–226.
52. Hay, J. Complications at Site of Injection of De-pot Neuroleptics. BMJ 1995, 311, 421.
53. Miliauskas, J. R.; Mukherjee, T.; Dixon. B.Postimmunization (Vaccination) Injection-SiteReactions: A Report of Four Cases and Review ofthe Literature. Am. J. Surg. Pathol. 1993, 17 (5),516 –524.
54. Greenblatt, D.; Divoll-Allen, M. IntramuscularInjection-Site Complications. JAMA 1978, 240(6), 542–544.
55. Drews, R.C. Use of Millipore Filters in Ophthal-mic Surgery. Am J Ophthalmol. 1960, 50, 159 –160.
56. Pinnock, C. A. Particulate Contamination of So-lutions for Intrathecal Use. Ann. R. Coll. Surg.Engl. 1984, 66 (6), 423.
57. Akers, M. J.; Larrimore, D. S.; Guazzo, D. M.Parenteral Quality Control: Sterility, Pyrogen,Particulate, and Package Integrity Testing. MarcelDekker: New York, 1994; p. 179.
58. Niden, A. H.; Aviado, D. M. Effects of PulmonaryEmbolism on the Pulmonary Circulation withSpecial Reference to Arteriovenous Shunts in theLungs Circulation Res. 1956, 4, 67–73.
59. Groom, R. C.; Quinn, R. D.; Lennon, P.; Done-gan, D. J.; Braxton, J. H.; Kramer, R. S.; Weldner,P. W.; Russo, L.; Blank, S. D.; Christie, A. A.;Taenzer, A. H.; Forest, R. J.; Clark, C.; Welch, J.;Ross, C. S.; O’Connor, G. T.; Likosky, D. S.Detection and Elimination of Microemboli Re-lated to Cardiopulmonary Bypass. Circ. Cardio-vasc. Qual. Outcomes 2009, 2, 191–198.
60. Blauth, C. I. Macroemboli and Microemboli Dur-ing Cardiopulmonary Bypass. Ann. Thorac. Surg.1995, 59, 1300 –1303.
61. Stump, D. A.; Rogers, A. T.; Hammon, J. W.;Newman, S. P. Cerebral Emboli and CognitiveOutcome After Cardiac Surgery. J. Cardiothorac.Vasc. Anesth. 1996, 10 (1), 113–119.
62. Liu, Y.-H.; Wang, D.-X.; Li, L.-H.; Wu, X.-M.;Shan, G.-J.; Su, Y.; Li, J.; Yu, Q.-J.; Shi, C.-X.;Huang, Y.-N.; Sun, W. The Effects of Cardiopul-monary Bypass on the Number of Cerebral Mi-croemboli and the Incidence of Cognitive Dys-function After Coronary Artery Bypass Graft
137Vol. 69, No. 1, January–February 2015
on August 15, 2018journal.pda.orgDownloaded from
Surgery. Anesth. Analg. 2009, 109 (4), 1013–1022.
63. Liu, J.-F.; Su, Z.-K.; Ding, W.-X. Quantitation ofParticulate Microemboli During CardiopulmonaryBypass: Experimental and Clinical Studies. Ann.Thorac. Surg. 1992, 54, 1196 –1202.
64. Schoenberg, M. D.; Gilman, P. A.; Mumaw, V.;Moore, R. D. Proliferation of the Reticuloendo-thelial System and Phagocytosis. Exp. Mol.Pathol. 1962, 2, 126 –143.
65. Brekkan, A.; Lexow, P. E.; Woxholt, G. GlassFragments and Other Particles Contaminatng [sic]Contrast Media. Acta Radiol.: Diagnosis, 1975,16 (6), 600 – 608.
66. Walpot, H.; Frank, R. P.; Burchard, W. G.,Agternkamp, C.; Muller, F. G.; Mittermayer, C.;Kalff, G. Particulate Contamination of Intrave-nous Solutions and Drug Additives During Long-Term Intensive Care. Anaesthesist, 1989, 38, 617–621.
67. Jones, M. L.; Warren, J. S. Monocyte Chemoat-tractant Protein 1 in a Rat Model of PulmonaryGranulomatosis. Laboratory Investigation 1992,66 (4), 498 –503.
68. Bautista, A. P.; Schuler, A.; Spolarics, Z.; Spitzer,J. J. In Vivo Latex Phagocytosis Primes theKupffer Cells and Hepatic Neutrophils to Gener-ate Superoxide Anion. J. Leukoc. Biol. 1992, 51,39 – 45.
69. Garvan, J. M.; Gunner, B. W. The Harmful Ef-fects of Particles in Intravenous Fluids. Med. J.Aust. 1964, 2 (1), 1– 6.
70. Garvan, J. M.; Gunner, B.W. Intravenous Fluids:“A Solution Containing Such Particles Must NotBe Used.” Med. J. Aust. 1963, 2, 140 –145.
71. Hill, S. E.; Heldman, L. S.; Goo, E. D. H.;Whippo, P. E.; Perkinson, J. C. Fatal Microvas-cular Pulmonary Emboli from Precipitation of aTotal Nutrient Admixture Solution. JPEN J. Par-enter. Enteral Nutr. 1996, 20 (1), 81– 86.
72. Reedy, J. S.; Kuhlman, J. E.; Voytovich, M. Mi-crovascular Pulmonary Emboli Secondary to Pre-
cipitated Crystals in a Patient Receiving TotalParenteral Nutrition: A Case Report and Descrip-tion of the High-Resolution CT Findings. Chest1999, 115, 892– 895.
73. Burton, J. F.; Zawadzki, E. S.; Wetherell, H. R.;Moy, T. W. Mainliners and Blue Velvet. Paperpresented at 17th Annual Meeting of the Ameri-can Academy of Forensic Sciences, Chicago, Feb-ruary 25, 1965.
74. Douglas, F. G.; Kafilmount, K. J.; Patt, N. L.Foreign Particle Embolism in Drug Addicts: Re-spiratory Pathophysiology. Ann. Intern. Med.1971, 75 (6), 865– 872.
75. Jones, B. S.; Brancaccio, F. A.; Rodriguez, G. A.Dyspnea and Bilateral Interstitial Pulmonary In-filtrates in an Intravenous Drug User. Proc. (Bayl.Univ. Med. Cent.) 2002, 15, 430 – 432.
76. Richman, H. S. Acute Pulmonary Edema Associ-ated with Librium Abuse. Radiology, 1972, 103,57–58.
77. Jorens, P. G.; Van Marck, E.; Snoeckx, A.; Pari-zel, P. M. Nonthrombotic Pulmonary Embolism.Eur. Respir. J. 2009, 34, 452– 474.
78. Kringsholm, B.; Christoffersen, P. The Nature andthe Occurrence of Birefringent Material in Differ-ent Organs in Fatal Drug Addiction. Forensic Sci.Int. 1987, 34, 53– 62.
79. Baydur, A.; Koss, M. N.; Sharma, O. P.; Dal-gleish, G. E.; Nguyen, D. V.; Mullick, F. G.;Murakata, L. A.; Centeno, J. A. Microscopic Pul-monary Embolisation of an Indwelling CentralVenous Catheter with Granulomatous Inflamma-tory Response. Eur. Respir. J. 2005, 26, 351–353.
80. Wijeyaratne, S. M.; Ubayasiri, R. A.; Weerasinghe,C. Fatal Pulmonary Embolism of Polyvinyl AlcoholParticles Following Therapeutic Embolisation of aPeripheral Arteriovenous Malformation. BMJ CaseReports. http://casereports.bmj.com/content/2009/bcr.02.2009.1635.full?sid�c744e316-4da4-4584-8d8e-1dd9ba2ca9e3 (accessed March 12, 2014).
81. Brown, K. T. Fatal pulmonary complications afterarterial embolization with 40 –120-�m tris-acryl
138 PDA Journal of Pharmaceutical Science and Technology
on August 15, 2018journal.pda.orgDownloaded from

gelatin microspheres. J Vasc Interv Radiol. 2004,15 (2), 197–200.
82. Plasencia, A. R.; Santillan, A. Embolization andRadiosurgery for Arteriovenous Malformations.Surg Neurol Int. 2012, 2 (Supple 2), S90 –S104.
83. Mahler, H.-C.; Friess, W.; Grauschopf, U.; Kiese,S. Protein Aggregation: Pathways, Induction Fac-tors and Analysis. J. Pharm. Sci. 2009, 98 (9),2909 –2934.
84. Narhi, L. O.; Jiang, Y.; Cao, S.; Benedek, K.;Shnek, D. A Critical Review of Analytical Meth-ods for Subvisible and Visible Particles. Curr.Pharm. Biotechnol. 2009, 10 (4), 373–381.
85. Sharma, D. K.; King, D.; Oma, P.; Merchant, C.Micro-Flow Imaging: Flow Microscopy Appliedto Sub-visible Particulate Analysis in Protein For-mulations. AAPS J. 2010, 12 (3), 455– 464.
86. Gentile, F.; Curcio, A.; Indolfi, C.; Ferrari, M.; De-cuzzi, P. The Margination Propensity of SphericalParticles for Vascular Targeting in the Microcircu-lation. J. Nanobiotechnology 2008, 6 (9), 1–9.
87. Shannon, P.; Billbao, J.M.; Marotta, T.; Terbrugge,K. Inadvertent Foreign Body Embolization in Diag-nostic and Therapeutic Cerebral Angiography. Am J.Neuroradiol. 2006, 27, 278–282.
88. Technical Report No 44: Quality Risk Managementfor Aseptic Processes; Parenteral Drug Association:2008. https://store.pda.org/ProductCatalog/Product.aspx?ID�1220 (Accessed July 21, 2014).
89. Quality Guideline Q9: Quality Risk Manage-ment; International Conference on Harmionisa-tion: 2005. www.ich.org (accessed March 11,2014).
90. Newton, D. W.; Driscoll, D. F. Calcium and Phos-phate Compatibility: Revisited Again. Am. J.Health Syst. Pharm. 2008, 65, 73– 80.
91. Allcutt, D. A.; Lort, D.; McCollum, C. N. FinalInline Filtration for Intravenous Infusions: A Pro-spective Hospital Study. Br. J. Surg. 1983, 70,111–113.
92. Kweder, S. Deputy director, Office of New DrugDevelopment, FDA. Presentation to U.S. SenateCommittee on Health, Education, Labor, and Pen-sions, December 15, 2011.
93. Parikh, M. J.; Dumas, G.; Silvestri, A.; Bistrian,B. R.; Driscoll, D. F. Physical Compatibility ofNeomatal Total Parenteral Nutrient AdmixturesContaining Organic Calcium and Inorganic Phos-phate Salts. Am. J. Health Syst. Pharm. 2005, 62,1177–1183.
139Vol. 69, No. 1, January–February 2015
on August 15, 2018journal.pda.orgDownloaded from
Authorized User or for the use by or distribution to other Authorized Users·Make a reasonable number of photocopies of a printed article for the individual use of an·Print individual articles from the PDA Journal for the individual use of an Authorized User ·Assemble and distribute links that point to the PDA Journal·Download a single article for the individual use of an Authorized User·Search and view the content of the PDA Journal permitted to do the following:Technology (the PDA Journal) is a PDA Member in good standing. Authorized Users are An Authorized User of the electronic PDA Journal of Pharmaceutical Science and
copyright information or notice contained in the PDA Journal·Delete or remove in any form or format, including on a printed article or photocopy, anytext or graphics·Make any edits or derivative works with respect to any portion of the PDA Journal including any·Alter, modify, repackage or adapt any portion of the PDA Journaldistribution of materials in any form, or any substantially similar commercial purpose·Use or copy the PDA Journal for document delivery, fee-for-service use, or bulk reproduction orJournal or its content·Sell, re-sell, rent, lease, license, sublicense, assign or otherwise transfer the use of the PDAof the PDA Journal ·Use robots or intelligent agents to access, search and/or systematically download any portion·Create a searchable archive of any portion of the PDA JournalJournal·Transmit electronically, via e-mail or any other file transfer protocols, any portion of the PDAor in any form of online publications·Post articles from the PDA Journal on Web sites, either available on the Internet or an Intranet,than an Authorized User· Display or otherwise make any information from the PDA Journal available to anyone otherPDA Journal·Except as mentioned above, allow anyone other than an Authorized User to use or access the Authorized Users are not permitted to do the following:
on August 15, 2018journal.pda.orgDownloaded from
Related Documents











