Shameem Ahmed, Ariful Islam, Parveen A Khanum, Barkat-e-Khuda Shameem Ahmed In memoriam This qualitative study was done in rural Bangladesh among the women seeking abortion-related care at six health facilities in two rural sub-districts of Bangladesh in 1996-1997. It looked at contraceptive use, why women had abortions, who made the abortion decision, who provided the abortions, the complications ofaborlion that developed, where and how soon the women sought treatment. A major@ of the women in this study availed abortion services from facilities where MR is provided. However, a quarter of the abortion procedures were dangerous or inadequate, and the number of women who developed complications was very high (43 per cent). Only 58 of 143 women attended only one provider, while 85 went on to attend a second provider. Of the 85, 37 went on to a third provider and 4 women had to be referred on to the district hospita1 with serious complications, of whom one died. About three-quarters of the women were not using contraception at the time of gettingpregnant. Many of the dangerous abortions were the most expensive to obtain, not least because of the tost of treatment for complications. Accessibility and availability of menstrual regulation and familyplanning services need to be strengthened in rural Bangladesh, and training for MR service needs to be improved, along with awareness-raising on the risks of unsafe procedures in the community. BOUT 40-60 million induced abortions are performed each year worldwide. Over half h a million women die each year due to regnancy-related complications, 99 per cent of them in developing c0untries.l Complica- tions of abortion are one of the five major causes of maternal mortality in the developing world. Fourteen per cent of all maternal deaths in South Asia can be attributed to unsafe abortions. Two out of five abortion procedures are unsafe, and one out of every 400 women who undergoes an unsafe abortion dies.’ In Bangladesh, women of childbearing age constitute about one fourth of the population.3 Women marry at a young age, a median of 14.2 years and have 3.3 children on average. The contraceptive prevalente rate is 49 per cent4 Although the Bangladesh Family Planning Pro- gramme has met with success, there are prob- lems such as like low contraceptive continuation rates, method failure and high unmet need for contraceptives, leading to unwanted pregnan- cies and abortions. Several studies have tried to estimate the number of abortions annually in Bangladesh. A study in 1978 estimated the number of abortions to be as high as 780,000.5 This figure was an extrapolation of 7,800 deaths due to complications of abortion, based on a case-fatality ratio of 1 per cent. More recent estimates were 241,442 in 1985’ j and 261,894 in 1991.7 The two later studies only considered abortions performed by trained providers and did not include those done by private practition- ers and traditional abortionists. A recent study in two rural areas of Bangladesh found that 9 per cent of 14,893 pregnancies were aborted inten- tionally or spontaneously.6 However, given that people have always been sensitive about abor- tion, due to associated social taboos, and that the majority of abortions are clandestine, these figures may be greatly underestimated. The mater& mortality ratio in Bangladesh is 450/100,000 live births.4 A total of 28,000 women die each year due to pregnancy-related causes,g 19

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Shameem Ahmed, Ariful Islam, Parveen A Khanum, Barkat-e-Khuda
Shameem Ahmed In memoriam
This qualitative study was done in rural Bangladesh among the women seeking abortion-related care at six health facilities in two rural sub-districts of Bangladesh in 1996-1997. It looked at contraceptive use, why women had abortions, who made the abortion decision, who provided the abortions, the complications ofaborlion that developed, where and how soon the women sought treatment. A major@ of the women in this study availed abortion services from facilities where MR is provided. However, a quarter of the abortion procedures were dangerous or inadequate, and the number of women who developed complications was very high (43 per cent). Only 58 of 143 women attended only one provider, while 85 went on to attend a second provider. Of the 85, 37 went on to a third provider and 4 women had to be referred on to the district hospita1 with serious complications, of whom one died. About three-quarters of the women were not using contraception at the time of gettingpregnant. Many of the dangerous abortions were the most expensive to obtain, not least because of the tost of treatment for complications. Accessibility and availability of menstrual regulation and familyplanning services need to be strengthened in rural Bangladesh, and training for MR service needs to be improved, along with awareness-raising on the risks of unsafe procedures in the community.
BOUT 40-60 million induced abortions are performed each year worldwide. Over half h a million women die each year due to
regnancy-related complications, 99 per cent of them in developing c0untries.l Complica- tions of abortion are one of the five major causes of maternal mortality in the developing world. Fourteen per cent of all maternal deaths in South Asia can be attributed to unsafe abortions. Two out of five abortion procedures are unsafe, and one out of every 400 women who undergoes an unsafe abortion dies.’
In Bangladesh, women of childbearing age constitute about one fourth of the population.3 Women marry at a young age, a median of 14.2 years and have 3.3 children on average. The contraceptive prevalente rate is 49 per cent4 Although the Bangladesh Family Planning Pro- gramme has met with success, there are prob- lems such as like low contraceptive continuation rates, method failure and high unmet need for contraceptives, leading to unwanted pregnan-
cies and abortions. Several studies have tried to estimate the number of abortions annually in Bangladesh. A study in 1978 estimated the number of abortions to be as high as 780,000.5 This figure was an extrapolation of 7,800 deaths due to complications of abortion, based on a case-fatality ratio of 1 per cent. More recent estimates were 241,442 in 1985’j and 261,894 in 1991.7 The two later studies only considered abortions performed by trained providers and did not include those done by private practition- ers and traditional abortionists. A recent study in two rural areas of Bangladesh found that 9 per cent of 14,893 pregnancies were aborted inten- tionally or spontaneously.6 However, given that people have always been sensitive about abor- tion, due to associated social taboos, and that the majority of abortions are clandestine, these figures may be greatly underestimated.
The mater& mortality ratio in Bangladesh is 450/100,000 live births.4 A total of 28,000 women die each year due to pregnancy-related causes,g
19
Ahmed, Islam, Khanum, Khuda
of w&h 8,00() deaths are estimated to be from abor+on-related comphcations.7 About 26 per cent of au pregnancy-related deaths are thought to be due to induced abortion in Bangladesh.‘O
The existing abortion law in Bangladesh, derived from the Penal Code of India 1860 and the British Offences against the Person Act 1861, prohibits abortion except to save a woman’s 1ife.t’ In 1972, the law was waived for women raped during the war of liberation. Although the law has been changed in both India and Britain, it is stil1 unchanged in Bangladesh. As early as 1976 the Bangladesh National Population Policy attempted to legalise first trimester abortion on broad medical and social grounds, but legislative action was not taken and restrictive legislation remains in effect.l* Yet scores of women, with the support and concurrence of their partners, stil1 choose pregnancy termination every day.
To make this choice safer, in 1974 the govern- ment of Bangladesh encouraged the introduction of menstrual regulation (MR) services in a few isolated family planning clinics. In 1978, an MR training and services programme was initiated in seven medical colleges and two government dis- trict hospitals. In 1979, the government included MR in the National Family Planning Programme and encouraged doctors and paramedics to provide MR services in al1 government hospitals and in health and family planning complexes.l* MR is accepted and widely practised throughout the country.t3 lt is also available in a limited number of NGO clinics as wel1 as in the private sector. MR is provided by paramedics who usually have 10-12 years of schooling and 18 months paramedic training, which includes 3 weeks of training in MR. In most cases these are the same providers who deliver family planning services. Physicians also provide these services.
MR is usually done within 6-10 weeks of amenorrhoea, without pregnancy confirmation. A 1990 study of more than 52,000 women seeking MR found that 17.2 per cent were turned away, of whom all but one per cent were over ten weeks of pregnancy. Of those turned away, almost al1 were sent away because the pregnancy was beyond that stage. l4 Apart from district and higher leve1 hospitals, the Health and Family Welfare Centers (H&FWC) are the service units providing MR at the union leve1 (consisting of 15-20 villages), and the rural hospitals or Thana Health Complexes (THCs) at the sub-district level.15
Deciding to terminate a pregnancy may not be easy for women in Bangladesh. Although this is a highly personal matter, it is not a private matter since women have to seek the agreement and financial support of their husbands or other relatives. In spite of the availability of MR in rural health facilities, many women in Bangladesh still depend on traditional methods of pregnancy termination, often performed by untrained pro- viders in unhygienic conditions.* Indeed, 83 per cent of induced abortidns are reported to be performed by traditional birth attendants and untrained practitioners. t6 The commonest method used by untrained providers is inserting roots into the uterus.5 Such procedures lead not only to appalling morbidity like perforation of the uterus and sterility, but also death.17 A sizeable propor- tion of admissions to obstetrics wards in the country are for complications of abortion; one study estimated that this was as high as 50 per cent.‘s Worse, women with abortion-related complications usually seek hospital care only after considerable suffering and as a last resort.1g,20
Many of the data above are from as long ago as 20 years. The present study was undertaken to find out where women go for induced abortion in rural Bangladesh today, their contraceptive practice prior to and after getting pregnant, their reasons for choosing abortion, who makes the decision for abortion, what complications they develop and where they go for treatment for these.
Materials and methods All the women who came to one of two rural hospitals (THCs) or four static clinics (H&FWCs) for an abortion-related reason in two rural sub- districts of Bangladesh (Mirsarai and Abhoyna- gar) from June 1996 to March 1997, were invited to participate in the study. One hundred and forty-three women agreed and gave verba1 consent; about five refused.
A semi-structured questionnaire was used, with scope to record responses as expressed by the women themselves. The interviews were conducted by women research assistants, who were trained, from the Operations Research Project which carried out the study.*l The women were interviewed at the facility itself, upon being discharged or upon leaving follow- ing a consultation. Privacy and confidentiality were always maintained.
Reproductive Health Matters, Vol. 7, No. 14, November 1999
Questions covered the women’s background, place and provider of abortion, reasons for abortion, decision-maker, complications that developed and treatment received, and contra- ceptive use prior to conception. Treatment provided at the THCs was validated from the hospita1 registers. Questions on reasons for abortion and decision-maker for abortion were open-ended. Though other questions were struc- tured, there was scope to record responses that did not fit in with the structured categories. The women were not prompted for any of the questions. Their sisters or sisters-in-law, who usually accompanied them, had no role when the women answered the questions.
It had originally been planned to follow up the women at their homes three months after the initial interview. However, only 81 of the 143 could be located at that stage, of whom one had died from abortion complications. The rest were lost to follow-up, mainly because they had deliberately given wrong addresses. This was not entirely unexpected, as most women under- going induced abortion prefer to keep it secret from relatives and neighbours. Although they had come to a health facility for abortion or for treatment, they did not wish to be traced later on. With a few exceptions, then, we do not to present the follow-up data here as we cannot be certain whether it is representative.
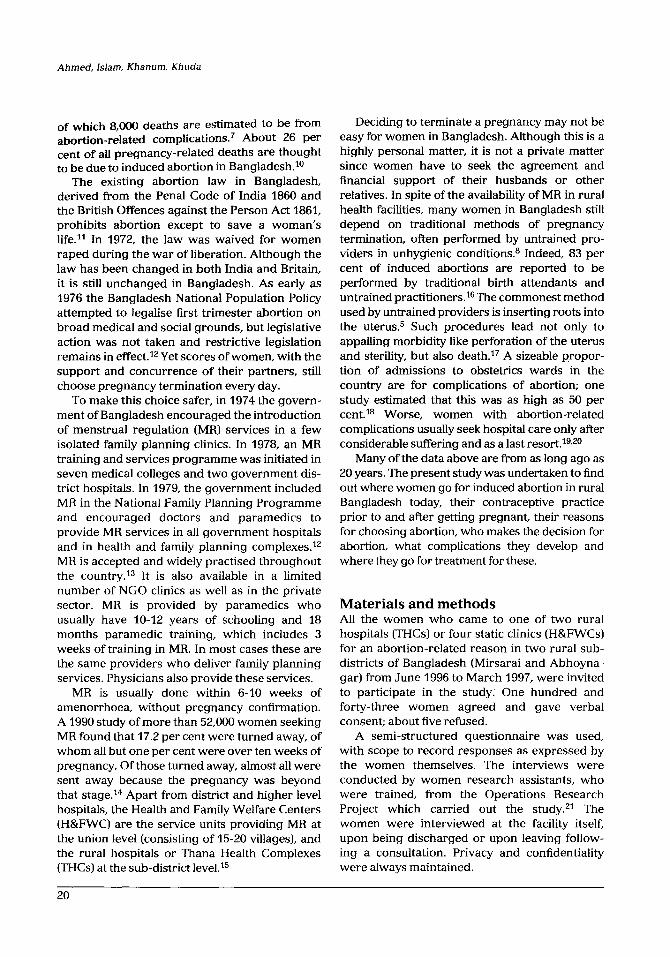
Characteristics of women in the study The ages of the women in the study ranged from 15 to 46 (average 28.3 years of age). Al1 but two were married, one was separated and the other widowed. Just over half (56 per cent) had more than two children and 73 per cent had at least one male child. Ten per cent were primiparae, while 11 per cent had children less than one year of age (Table 1).
Almost half the women had had no schooling, about a quarter had been to primary school (mean 3.4 years) and a quarter to secondary school. They worked either in smal1 businesses, e.g. making handicrafts, selling pickles and vegetables, or as day labourers. Almost half of the women’s husbands had had six or more years of schooling, while a third had had none (mean 5.2 years). More than half the husbands were either day labourers or involved in businesses such as selling fish and vegetables in the market,
Table 1. Socio-demographic characteristics of the women and their husbands (n=143)
Charactaristic
Aas (vars) < 20 ZO-24 25-29 30-34 35-46
Parily
None
1-2
3-4
5 or more
Age of last child (years)
NO children
Less than 1
1
2
3
4
5 or more
Woman’s education (years)
NO education
1-5
6-10
11 and above
Woman’s occupation
Housewife
Smal1 business
Dey labour
Service
Student
Husbands’ education (yaars)
NO education
1-5
6-10
11 and above
Husbands’ occupation
Works abroad/outside the thana
Business
Daylabour
Service
FarmerIandowner
Others
%
7
19
30
22
22
10
34
30
26
10
11
22
13
12
8
24
47
25
24
4
82
10
4
3
1
34
21
35
10
7
26
27
8
19
13
21
Ahmed, Islam, Khanum, Khuda
fruit-vending, working as barbers or owners of smal1 roadside tea shops. Seven per cent of the husbands were working abroad or outside the area at the time of the woman’s interview.
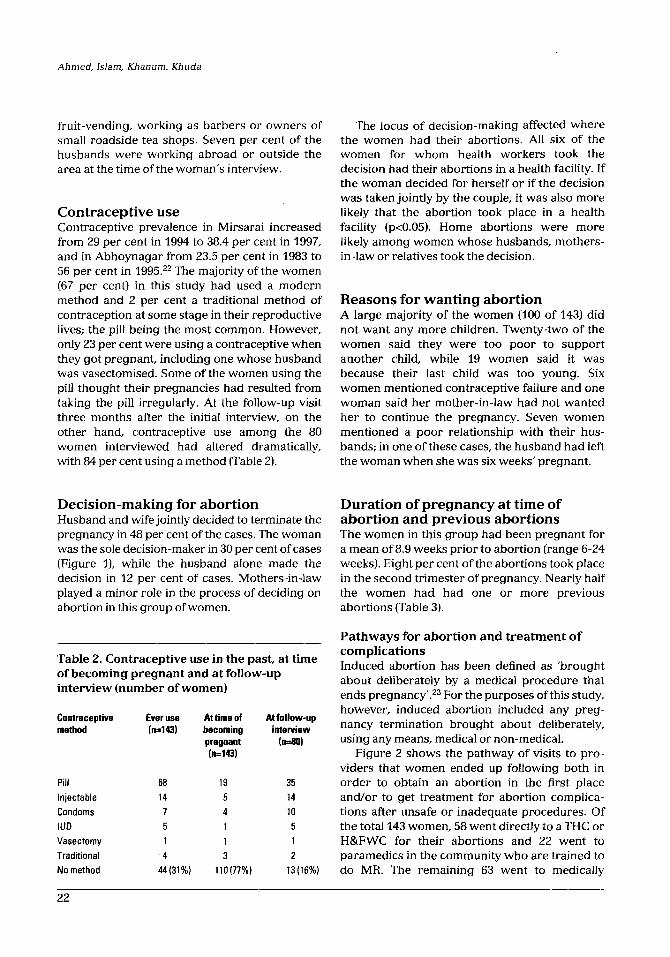
Contraceptive use Contraceptive prevalente in Mirsarai increased from 29 per cent in 1994 to 38.4 per cent in 1997, and in Abhoynagar from 23.5 per cent in 1983 to 56 per cent in 1995.“” The majority of the women (67 per cent) in this study had used a modern method and 2 per cent a traditional method of contraception at some stage in their reproductive lives; the pill being the most common. However, only 23 per cent were using a contraceptive when they got pregnant, including one whose husband was vasectomised. Some of the women using the pill thought their pregnancies had resulted fiom taking the pil1 irregularly. At the follow-up visit three months after the initial interview, on the other hand, contraceptive use among the 80 women interviewed had altered dramatically, with 84 per cent using a method (Table 2).
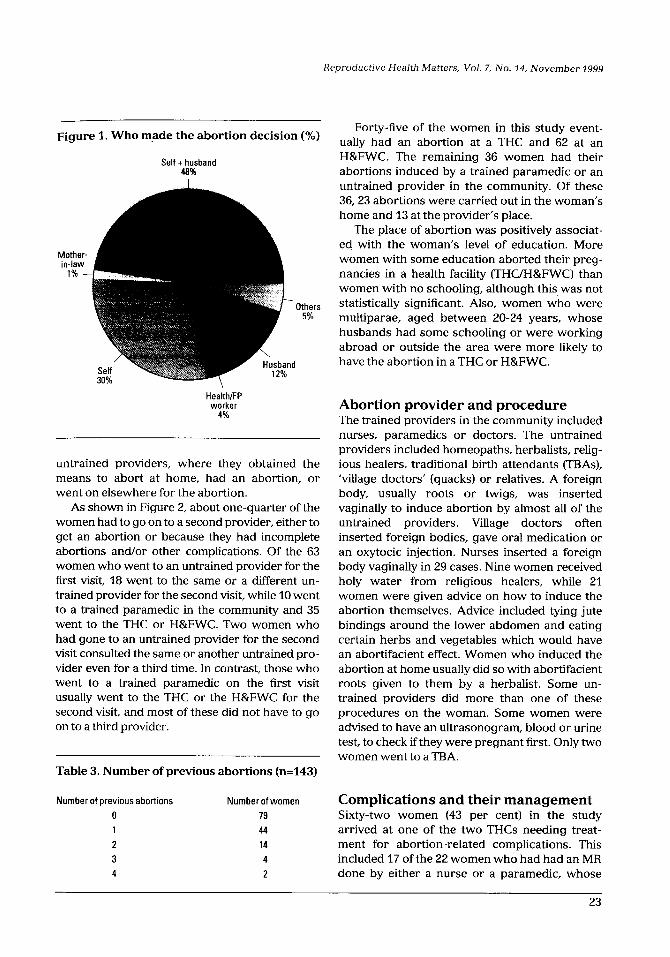
Decision-making for abortion Duration of pregnancy at time of Husband and wife jointly decided to terminate the abortion and previous abortions pregnancy in 48 per cent of the cases. The woman The women in this group had been pregnant for was the sole decision-maker in 30 per cent of cases a mean of 8.9 weeks prior to abortion (range 6-24 (Figure 1), while the husband alone made the weeks). Eight per cent of the abortions took place decision in 12 per cent of cases. Mothers-in-law in the second trimester of pregnancy. Nearly half played a minor role in the process of deciding on the women had had one or more previous abortion in this group of women. abortions (Table 3).
Table 2. Contraceptive use in the past, at time of becoming pregnant and at follow-up interview (number of women)
Contraceptive Ever use method (nd43)
At time of becoming pregnant (n=W)
At follow-up interview
MOl
Pil1 Injectable Condoms IUD Vasectomy
Traditional NO method
68 19 35 14 5 14 7 4 10 5 1 5 1 1 1
4 3 2
44(31%) 110(77%) 13(16%)
The lotus of decision-making affected where the women had their abortions. AU Six of the women for whom health workers took the decision had their abortions in a health facility. If the woman decided for herself or if the decision was taken jointly by the couple, it was also more likely that the abortion took place in a health facility (~~0.05). Home abortions were more likely among women whose husbands, mothers- in-law or relatives took the decísion.
Reasons for wanting abortion A large majority of the women (100 of 143) did not want any more children. Twenty-two of the women said they were too poor to support another child, while 19 women said it was because their last child was too young. Six women mentioned contraceptive failure and one woman said her mother-in-law had not wanted her to continue the pregnancy. Seven women mentioned a poor relationship with their hus- bands; in one of these cases, the husband had left the woman when she was six weeks’ pregnant.
Pathways for abortion and treatment of complications Induced abortion has been defined as ‘brought about deliberately by a medical procedure that ends pregnancy’.23 For the purposes of this study, however, induced abortion included any preg- nancy termination brought about deliberately, using any means, medical or non-medical.
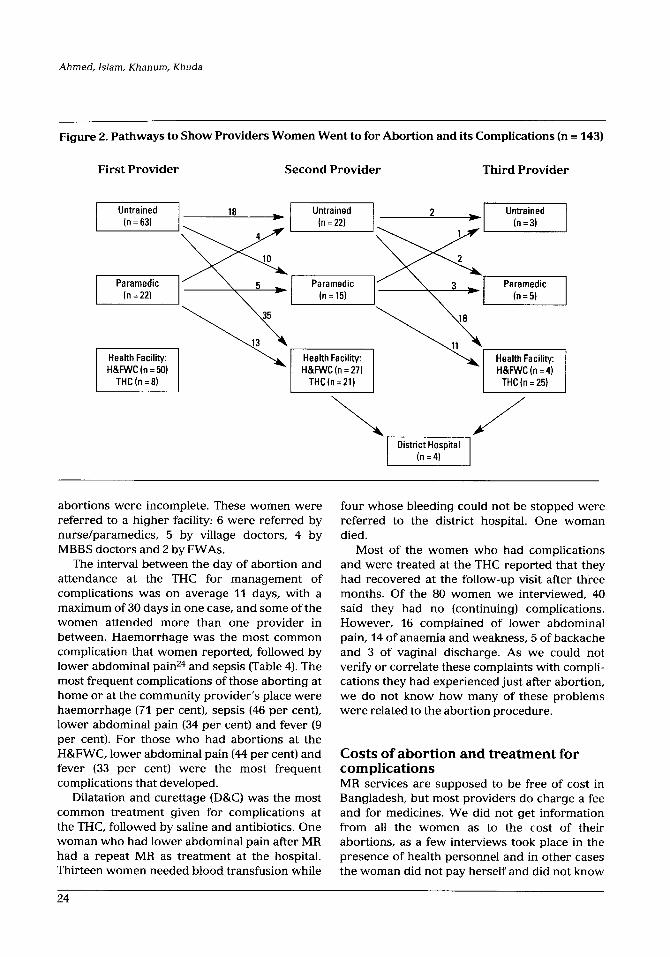
Figure 2 shows the pathway of visits to pro- viders that women ended up following both in order to obtain an abortion in the first place and/or to get treatment for abortion complica- tions after unsafe or inadequate procedures. Of the total 143 women, 58 went directly to a THC or H&FWC for theír abortions and 22 went to paramedics in the community who are trained to do MR. The remaining 63 went to medically
22
Reproductive Health Matters, Vol. 7, No. 14, November 1999
Figure 1. Who made the abortion decision (%)
Self + husband 48%
Moth in-la
1%
Others 5%
Health/FP worker
4%
untrained providers, where they obtained the means to abort at home, had an abortion, or went on elsewhere for the abortion.
As shown in Figure 2, about one-quarter of the women had to go on to a second provider, either to get an abortion or because they had incomplete abortions and/or other complications. Of the 63 women who went to an untrained provider for the first visit, 18 went to the same or a different un- trained provider for the second visit, while 10 went to a trained paramedic in the community and 35 went to the THC or H&FWC. Two women who had gone to an untrained provider for the second visit consulted the same or another untrained pro- vider even for a third time. In contrast, those who went to a trained paramedic on the first visit usually went to the THC or the H&FWC for the second visit, and most of these did not have to go on to a third provider.
Table 3. Number of previous abortions (n=143)
Number of previous abortions Number of women Complications and their management 0 79 Sixty-two women (43 per cent) in the study 1 44 arrived at one of the two THCs needing treat- 2 14 ment for abortion-related complications. This 3 4 included 17 of the 22 women who had had an MR 4 2 done by either a nurse or a paramedic, whose
Forty-five of the women in this study event- ually had an abortion at a THC and 62 at an H&FWC. The remaining 36 women had their abortions induced by a trained paramedic or an untrained provider in the community. Of these 36,23 abortions were carried out in the woman’s home and 13 at the provider’s place.
The place of abortion was positively associat- ecJ with the woman’s leve1 of education. More women with some education aborted their preg- nancies in a health facility (THC/H&FWC) than women with no schooling, although this was not statistically significant. Also, women who were multiparae, aged between 20-24 years, whose husbands had some schooling or were working abroad or outside the area were more likely to have the abortion in a THC or H&FWC.
Abortion provider and procedure The trained providers in the community included nurses, paramedics or doctors. The untrained providers included homeopaths, herbalists, relig- ious healers, traditional birth attendants (TRAS), ‘village doctors’ (quacks) or relatives. A foreign body, usually roots or twigs, was inserted vaginally to induce abortion by almost all of the untrained providers. Village doctors often inserted foreign bodies, gave oral medication or an oxytocic injection. Nurses inserted a foreign body vaginally in 29 cases. Nine women received holy water from religious healers, while 21 women were given advice on how to induce the abortion themselves. Advlce included tying jute bindings around the lower abdomen and eating certain herbs and vegetables which would have an abortifacient effect. Women who induced the abortion at home usually did so with abortifacient roots given to them by a herbalist. Some un- trained providers did more than one of these procedures on the woman. Some women were advised to have an ultrasonogram, blood or urine test, to check if they were pregnant first. Only two women went to a TRA.
23
Ahmed, Islam, Khanum, Khuda
Figure 2. Pathways to Show Providers Women Went to for Ahortion and its Complications (n = 143)
First Provider Second Provider Third Provider
abortions were incomplete. These women were referred to a higher facility: 6 were referred by nurse/paramedics, 5 by village doctors, 4 by MBBS doctors and 2 by FWAs.
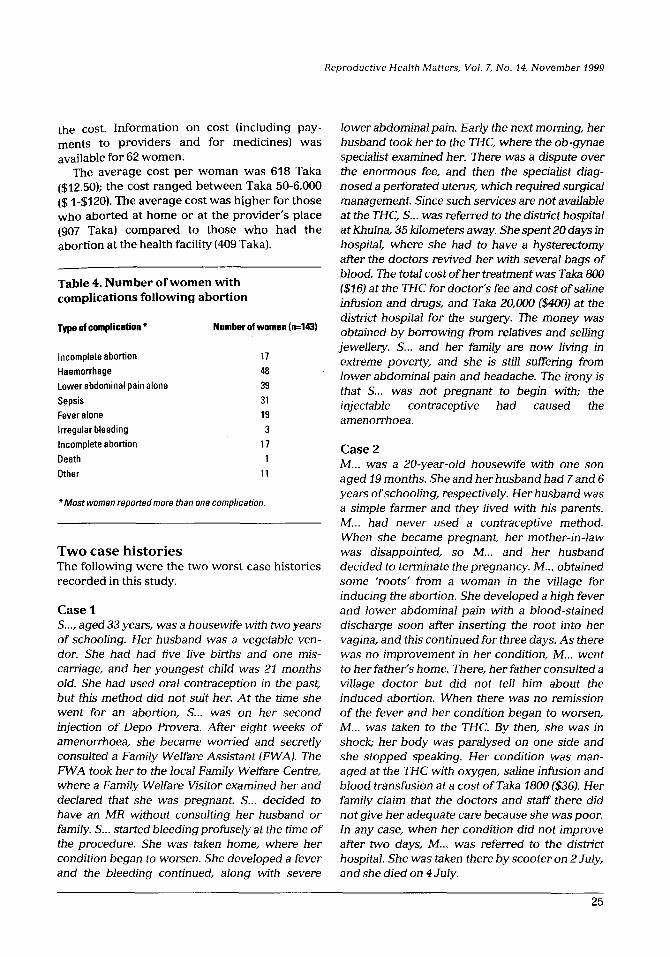
The interval between the day of abortion and attendance at the THC for management of complications was on average 11 days, with a maximum of 30 days in one case, and some of the women attended more than one provider in between. Haemorrhage was the most common complication that women reported, followed by lower abdominal painz4 and sepsis ffable 4). The most frequent complications of those aborting at home or at the community provider’s place were haemorrhage (71 per cent), sepsis (46 per cent), lower abdominal pain (34 per cent) and fever (9 per cent). For those who had abortions at the H&FWC, lower abdominal pain (44 per cent) and fever (33 per cent) were the most frequent complications that developed.
Dilatation and curettage (DK) was the most common treatment given for complications at the THC, followed by saline and antibiotics. One woman who had lower abdominal pain after MR had a repeat MR as treatment at the hospital. Thirteen women needed blood transfusion while
four whose bleeding could not be stopped were referred to the district hospital. One woman died.
Most of the women who had complications and were treated at the THC reported that they had recovered at the follow-up visit after three months. Of the 80 women we interviewed, 40 said they had no (continuing) complications. However, 16 complained of lower abdominal pain, 14 of anaemia and weakness, 5 of backache and 3 of vagina1 discharge. As we could not verify or correlate these complaints with compli- cations they had experienced just after abortion, we do not know how many of these problems were related to the abortion procedure.
Costs of abortion and treatment for complications MR services are supposed to be free of tost in Bangladesh, but most providers do charge a fee and for medicines. We did not get information from al1 the women as to the tost of their abortions, as a few interviews took place in the presence of health personnel and in other cases the woman did not pay herself and did not know
24
Reproductive Health Matters, Vol. 7, No. 14, November 1999
the tost. Information on tost (including pay- ments to providers and for medicines) was available for 62 women.
The average tost per woman was 618 Taka ($12.50); the tost ranged between Taka 50-6,000 ($ I-$120). The average tost was higher for those who aborted at home or at the provider’s place (907 Taka) compared to those who had the abortion at the health facility (409 Taka).
Table 4. Number of women with complications following abortion
Type ol complicetion ?? Number of women (n=l43)
Incomplete abortion Haemorrhage Lower abdominal pain alone
Sepsis Fever alone Irregular bleeding Incomplete abortion
Death Other
17 48 39 31 19
3 17
1 11
*Most women reported more than one complication.
Two case histories The following were the two worst case histories recorded in this study.
Case 1 S..., aged 33 years, was a housewife with two years of schooling. Her husband was a vegetable ven- dor. She had had 6ve live births and one mis- caniage, and her youngest child was 21 months old. She had used oral contraception in the past, but this method did not suit her. At the time she went for an abortion, S... was on her second injection of Depo Provera. Afier eight weeks of amenorrhoea, she became worried and secretly consulted a Family Welfare Assistant (FWA). The FWA took her to the local Family Welfare Centre, where a Family Welfare Visitor examined her and declared that she was pregnant. S... decided to have an MR without consulting her husband or family. S... started bleedingprofusely at the time of the procedure. She was taken home, where her condition began to worsen. She developed a fever and the bleeding continued, along with severe
lower abdominal pain. Early the next morning, her husband took her to the THC, where the ob-gynae specialist examined her. There was a dispute over the enormous fee, and then the specialist diag- nosed a perforated uterus, which required surgical management. Since such services are not available at the THC, S... was referred to the distn’ct hospital at khulna, 35 Iglometers away. She spent 20 days in hospital, where she had to have a hysterectomy atter the doctors revived her with several bags of blood. The total tost of her treatment was Taka 800 ($16) at the THC for doctor’s fee and tost of saline infusion and drugs, and Taka 20,000 ($400) at the district hospital for me surgery. The money was obtained by borrowing fiom relatives and selling jewellery. S... and her family are now living in extreme poverty, and she is stil1 suffering from lower abdominal pain and headache. The irony is that S... was not pregnant to begin with; the injectable contraceptive had caused the amenorrhoea.
Case 2 M... was a 20-year-oJd housewife with one son aged 19 months. She and herhusband had 7and 6 years of schooling, respectively. Her husband was a simple farmer and they Jived with his parents. M... had never used a contraceptive method. When she became pregnant, her mother-in-Jaw was disappointed, so M... and her husband decided to terminate the pregnancy. M... obtained some %oots’ from a woman in the village for inducing the abortion. She developed a high fever and lower abdominal pain with a blood-stained discharge soon afier inserting the root into her vagina, and this continued for three days. As there was no improvement in her condition, M... went to her father’s home. There, her father consulted a village doctor but did not tel1 him about the induced abortion. When there was no remission of the fever and her condition began to worsen, M.:. was taken to the THC. By then, she was in shock; her body was paralysed on one side and she stopped speaking. Her condition was man- aged at the THC with oxygen, saline infusion and blood transfusion at a tost of Taka 1800 ($36). Her family claim that the doctors and staff there did not g’ve her adequate care because she was poor. In any case, when her condition did not improve after two days, M... was referred to the district hospital. She was taken there by scooter on PJuly, and she died on 4July.
25
Ahmed, Islam, Khanum, Khuda
m majonty of the women in this study had an abortion because they did nOt want anY more children. Most of them already had two 01‘ more children, and 73 per cent had at least one male child. The primiparae women had an abortion mainly because they did not yet want a child, or because of poverty or a poor relationship with their husbands.
Although 67 per cent of the women in the study had used a modern method of contra- ception at some stage in their reproductive lives, 77 per cent were not using any contraceptive at the time they got pregnant. Their reluctance or failure to use contraception, or to use it effect- ively - whether because they did not have access to reliable methods, did not have adequate knowledge about methods (as in the case of irregular pill use), or were disillusioned with the services available to them - needs to be better studied and addressed by the national family planning programme. Condom use was also very low and a focus on increasing the use of ‘male’ as well as ‘female’ methods is to be recommended.
It is important to motivate women after an abortion to choose an appropriate method of fam- ily planning, thereby reducing the risk of anotber unwanted pregnancy. Almost half the women in this study had had one previous abortion and in a few cases more than one. Ross and Frankenberg have demonstrated that contraceptive use in- creases after abortion,a5 and the follow-up data we collected show this is the case in at least a good part of the group in this study. However, effective and sustained contraceptive use wil1 only occur if women have access to a range of methods and appropriate counselling and support.
For women who had an abortion because they did not want any more children, longer-acting and permanent methods of contraception are important to offer, to prevent further unwanted pregnancies. One in ten of the women in this group had a child aged less than one year old. This finding calls for the strengthening of post-partum contraceptive services, including support for exclusive breastfeeding for the first six months of infant life as a method of contraception.z6
Women were the sole decision-makers on whether to have an abortion in about 30 per cent of cases in this study, and about 48 per cent of the women made the decision jointly with their husbands. Mothers-in-law, usually the key
figure in the family, played a very negligible role in the decision-making process. This suggests that women are making more of their own choices for their reproductive lives. This same group of women also tended to go to a health facility for abortion, as compared to those for whom the decision was taken by others. This shows that women’s empowerment and inter- spousal communication is important for the improvement of reproductive health of women in rural Bangladesh.
A majority of the women in this study availed abortion services from facilities where MR is provided. This is indicative that women are now mobile and accessing services at static clinics and health facilities.
However, a quarter of the abortion procedures were dangerous or inadequate, particularly those induced by untrained providers and by women or their relatives, and the number of women who developed complications was very high (43 per cent). Although government-employed para- medics are supposed to provide free MR services in the community, a large proportion of rural women went to untrained village practitioners for abortion. This could be because of familiarity with these providers as well as easier access and confidentiality. On the other hand, it could also be due to the fact that some of the women were over ten weeks of pregnancy and knew or suspected that they might be turned away from MR services. The issue of what to do to help women in tbis position who are seeking abortion, whose plight is an important reason for the high abortion mortality and morbidity nationally in spite of accessible MR services, remains problematic in Bangladesh.
A few of the women saw up to three providers for abortion before they finally saw a sufficiently trained provlder. In all, only 58 of 143 women attended only one provider; while 85 went on to attend a second provlder. Of the 85, 37 went on to a third provider and 4 women had to be referred on to the district hospita1 with serious complications, of whom one died. Interventions by untrained providers appear to have been ineffective and to lead to complications; they caused many women to delay consulting a trained provider in the community or at a health facility. However, 22 of the 143 women chose a trained paramedic in the community as their first provider, and a high number of these women (17)
26
Reproductive Health Matters, Vol. 7, No. 14, November 1999
developed complications and had to go to the rural hospita1 for management.
Further, the tost of abortion was much higher when performed at the hands of untrained providers. Although we did not ask the women to give US a detailed breakdown of what they had paid, the higher amounts could be due to the charges that women had to pay to each of the several providers they had to go to. In addition to the fee for abortion were the costs of treating complications that developed. MR services are supposed to be free, however; the issue of charges for MR needs further investigation and possibly regulation.
MR is usually done without confirmation of pregnancy. However, if simple pregnancy tests were made available at local facilities, women and MR providers at community leve1 could at least be sure a woman is pregnant before doing MR. As shown in one of the case studies, a woman on an injectable contraceptive was misdiagnosed as being pregnant by a service provider, when both the provider and the woman should have known that amenorrhoea is a common side effect of the method. All these findings reflect the need to improve the quality of MR services in rural Bangladesh and the technical competente of MR service providers.
The major complications of abortion encount-
ered in this study were haemorrhage, lower abdominal pain and sepsis. These, along with other complications of abortion, are important causes of maternal death worldwide,27 and one maternal death occurred due to ruptured uterus in this group. The need to provide better training of paramedics for carrying out MR, so that the rate of incomplete abortions is reduced, is also critical. The two case studies point to the need to facilitate women’s access to treatment for complications of abortion when required. Further, the accessibility and availability of reproductive health and family planning services in rural Bangladesh need to be further improved. This includes better services for abortion clients and sympathetic post-abortion contraceptive counselling.
The fact that almost half the women in this study came to the rural hospita1 with complica- tions of abortion, calls for urgent attention to strengthen awareness-raising efforts in the community about the dangers of unsafe abortion. Health education for the grassroots workers also needs to be improved to enable them to convey appropriate messages to the community. They should be able to emphasise that when women do want an abortion they should go to a trained service provider for MR as early as possible, and that untrained providers and clandestine methods risk women’s health and lives.
27
Ahmed, Islam, Khanum, Khuda
Acknowledgments mis p&lication is funded by USAJD under CO- opemtive Agreement No. 388-A-00-97-00032-00 with the ZCDDR,B Centre for Health and Population Research. The Centre is supported by over 30 different countries and agencies which share its concern for the health and population problems of developing countn’es. The authors are gratefil to Prof Syeda Firoza Begum and Dr CP Maskey for their valuable comments on the paper.
The authors would also Jike to thank Dr Brute CaJdweJJ, Dr Abbas Uddin Bhuiyan and MS Nancy Piet-PeJon for their suggestions. Thanks also to Dr Sadia D Parveen for her assistance in the study.
Correspondence ArifuJ Islam, Senior Research Oftìcer, Operations Research Project, ZCDDR,B, CP0 Box 128, Dhaka- 1000, Bangladesh. Fax: 880-2-871-568. E-mail: [email protected]
References and Notes 1.
2.
3.
4.
5.
6.
7.
Revised 1990Estimates of Maternal Mortality: A New Approach by WHO and UNICEF. WHO, Geneva, 1996. Henshaw SK, 1990. Induced abortion: a world review. International Family Planning Perspectives. 22:76-89. Bangladesh Bureau of Statistics, 1996. Bangladesh Data Sheet 1996. Dhaka: Bangladesh Bureau of Statistics, Ministry of Planning, Government of Bangladesh. Data for women aged 20-49. From: Bangladesh Demographic and Health Survey 1996-1997. Dhaka: National Institute of Population Research and Training, Mitra and Associates, Demographic and Health Surveys, Macro International Inc, 1997. Measham AR, Obaidullah M, Rosenberg MJ et al, 1981. Complications from induced abortion in Bangladesh related to types of practitioners and methods and impact on mortal- ity. Lancet. 1124 Jan):199-202. Begum SF, Kamal H, Kamal GM, 1987. Evaluation ofMR Services in Bangladesh. Bangladesh Association for Prevention of Septic Abortion, Dhaka. Kamal H, Hussain A, Begum SF et al, 1993. Prospects of Menstrual Regulation Services in Bangladesh: Results ofan Operational Research. Bangladesh Association for Prevention of Septic Abortion. Publication No. 9, Dhaka.
8. Ahmed S, Haque 1, Barkat-e- Khuda et al, 1996. Abortion in Rural Bangladesh: evidente from the MCH-FP Extension Project. International Center for Diarr- hoeal Disease Research, Bangla- desh. Working paper 121, Dhaka.
9. UNICEF, 1993. Emergency Obstetrie care: intervention for the reduction ofmaternal mortality. Obstetrie and Gynaecological Society of Bangladesh. Dhaka: UNICEF.
10. Rochat RW, Jabeen S, Rosenberg M, 1981. Maternal and abortion related deaths in Bangladesh, 1978-1979. International Journal of Gynaecology and Obstetrics. 19:1554X.
ll. Bhiwandiwala PP, Cook RJ, Dickens BM et al, 1982. Menstrual therapies in Commonwealth Asia law. International Journal of Gynaecol- ogy and Obstetetrics. 20:273-78.
12. Akhter HH, 1996. Unsafe abortion: A situation Analysis. In: Akhter HH, Khan TF (eds). A Bibliography on Menstrual Regulation and Abortion Studies in Bangladesh. Bangladesh Institute of Research for Promotion of Essential & Reproductive Health and Technologies, Dhaka.
13. International Center for Diarrhoeal Disease Research, Bangladesh, 1995. Strengthen- ing maternal and neonatal health: improving linkages at all levels. A concept paper for ColIaborative project between Ministry of Health and Family
Welfare, Government of Bangla- desh, MCH-FP Extension Project (Rural). Dhaka: ICDDR,B.
14. Kamal MG, Kabir GM, Majumder MA et al, 1990. Study on interventions necessary for preventing rejection ofMR clients. Bangladesh Association for Prevention of Septic Abortion, Dhaka. This was a multi-facility study.
15. Akhter HH, 1986. Medical practice after legalization of abortion. Bangladesh prevention and treatment of contraceptive failure. In: Landy U, Ratnam SS. Prevention and Treatment of Contraceptive Failure -In Honour of Christopher Tietze. Plenum Press, New York.
16. Obaidullah M, Khan AR, 1996. Social dynamics of abortion services in rural Bangladesh. In: Akhter HH, Khan TF (eds). A Bibliography on Menstrual Regulation and Abortion Studies in Bangladesh. Bangladesh Institute of Research for Promotion of Essential & Reproductive Health and Technologies, Dhaka.
17. Kabir SM, 1989. Causes and consequences of unwanted pregnancy from Asian women’s perspectives. International Journal of Gynaecology and Obstetrics. 3(Suppl):9-14.
18. Begum SF et al, 1978. Experience with abortion-related admission in Dhaka Medical College Hospital. Bangladesh Fertility Research program. Technical Report No. 8, Dhaka.
28

Reproductive Health Matters, Vol. 7, No. 14, November 1999
lg. Jabeen S, Begum SF, Bhuiyan N, 1979. A study of the abortion- related admissions in the three hospitals ofBangladesh, 1977. 1979. Bangladesh Fertility Research Program, Dhaka.
20. Barua BB, Ahmed S, 1980. Characteristics of abortion cases admitted in Sylhet Medical College Hospital. Sylhet. (Unpublished).
21. These two sub-districts are field sites of the Operations Research Project (ORP) of the International Center for Diarrhoeal Disease Research, Bangladesh (ICDDR,B). Interventions in health and family planning are tested in
parts of these sub-districts. The Project has a surveillance system for collecting data on major demographic events and
abdominal pain in the same woman were considered to be sepsis during analysis of data.
25. Ross J, Frankenberg E, 1992. programmatic variables in both sites (since 1982 in Abhoynagar and 1994 in Mirsarai).
22. International Center for Diarrhoeal Disease Research, Bangladesh (ICDDR,B), 1996. Sample registration system reports, 1983-1995. Dhaka: MCH-FP Extension Project (Rural), Dhaka.
26
23. Dudley S, 1996. The truth about 27 abortion: A fact sheet series. Washington: National Abortion Federation, January.
24. Reported fever with lower
Induced Abortion: Findings From Two Decades ofFamily Planning Research. New York: Population Council. Salway S, Nurani S, 1997. T’he Contraceptive Potential of Breast- feedingin Bangladesh. Dhaka: International Centre for Diarr- hoeal Disease Research, Bangla- desh Working Paper No.83. Fauveau V; Koenig M, Chakroborty J et al, 1988. Causes of maternal mortality in rural Bangladesh, 1976-85. Bulletin of WHO. 66:643-51.
Résumé Resumen Cette étude a été réalisée dans des zones rurales du Bangladesh auprès de 143 femmes, afin de savoir où les femmes vont pour avorter, quelles sont les complications de l’avortement et où les femmes cherchent un traitement, les raisons de l’avortement et qui prend la décision sur l’avorte- ment, et l’utilisation de contraceptifs. Les partici- pantes à l’étude étaient des femmes qui étaient venues dans des centres de santé pour un avortement provoqué ou pour la gestion des complications, dans deux sous-districts ruraux du Bangladesh en 1996-1997. Bien qu’une régulation menstruelle soit proposée dans beaucoup de dispensaires, un quart des avortements chez les femmes étudiées avaient été provoqués par des praticiens non qualifiés ou pat- les femmes elles- mêmes. Au total, 43% de femmes ont connu des complications. Huit pour cent des femmes avaient eu leur avortement pendant le deuxième trimestre de grossesse. Environ les quatre cinquièmes n’utilisaient aucune contraception au moment de la conception. Cette étude suggère que des efforts de sensibilisation sont nécessaires afin que les femmes cessent de s’adresser à des praticiens non qualifiés et qu’elles aillent dans des dispensaires dotés de personnel compétent. Beaucoup des avortements à risque coûtent davantage, en particulier du fait des complica- tions. L’accessibilité et la disponibilité de services de régulation des menstruations et de planifica- tion familiale doivent être renforcées dans les zones rurales du Bangladesh.
Se realizó un estudio cualitativo entre 143 mujeres rurales en Bangladesh para determinar adónde acuden para abortar, las complicaciones de aborto que se presentan y dónde buscan tratamiento, las razones por las cuales abortan, y el uso anticonceptivo previo al aborto. Las participantes en el estudio eran mujeres que llegaron a los servicios de salud en 1996-97 solicitando un aborto inducido o tratamiento de complicaciones. Si bien se ofrece la regulación menstrual en muchas clínicas, un cuarto de los abortos entre las mujeres en este estudio fueron inducidos por personas sin capacitación o por las mujeres mismas. Un 43 por ciento de las mujeres sufrieron complicaciones. Un ocho por ciento de las mujeres habían abortado en el segundo trimestre del embarazo. Casi tres cuartos de las mujeres optaron por abortar porque no querían tener más hijos. Alrededor de un 80 por ciento de ellas no usaba ningún anticonceptivo al momento de concebir. Este estudio indicaría que es preciso un trabajo de concientización para que las mujeres dejen de recurrir a proveedores no capacitados. Muchas vetes cuestan más los abortos practicados en condiciones de riesgo al sumar el costo de tratar las complicaciones. Hay que fortalecer la provisión de los servicios de regulación menstrual y planificación familiar, y el acceso a ellos, en las áreas rurales de Bangladesh.
29
Related Documents