Not for Release

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Not for R
elease

Indication, results, and long survival in DALK
Symposium 12: Anterior Lamellar Keratoplasty
Clinica degli occhi
Sarnicola
Vincenzo Sarnicola, MD Grosseto, Italy
Not for R
elease

No financial interest to disclose.
Not for R
elease

LONG TERM
GRAFT SURVIVAL
Not for R
elease
Not for R
elease
PURPOSE
• 10 years DALK graft survival
PARTICIPANTS
• 806 DALK/ 711 patients
• Between 2000-2009
• Exclusion criteria:
– Follow-up < 6 months
– Lost from follow-up visit
Not for R
elease
YEARS
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
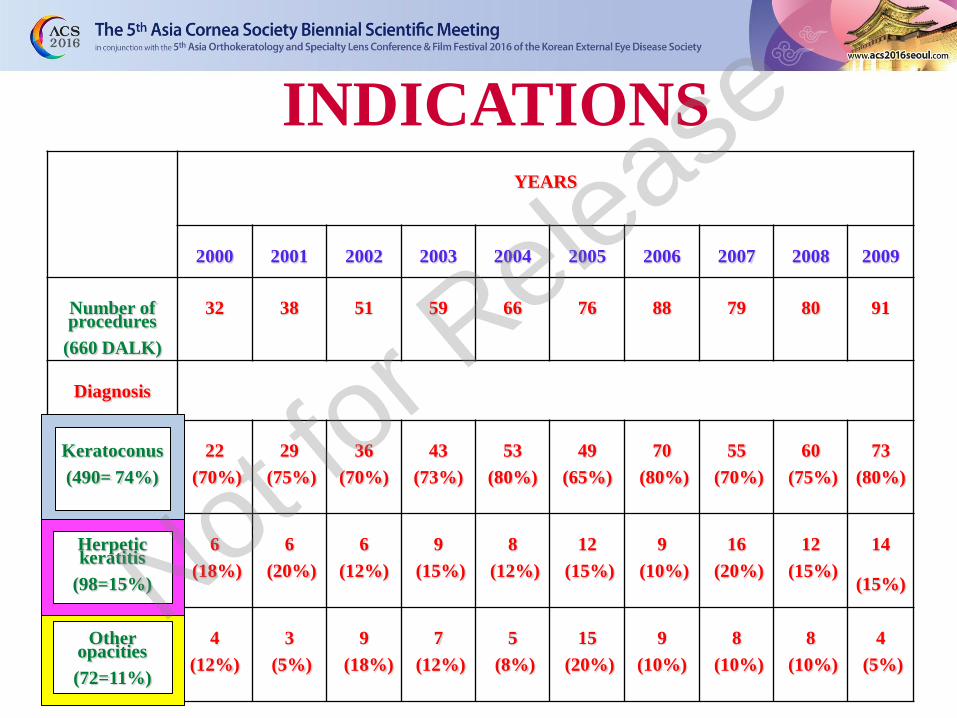
Number of procedures
(660 DALK)
32
38
51
59
66
76
88
79
80
91
Diagnosis
Keratoconus
(490= 74%)
22
(70%)
29
(75%)
36
(70%)
43
(73%)
53
(80%)
49
(65%)
70
(80%)
55
(70%)
60
(75%)
73
(80%)
Herpetic keratitis
(98=15%)
6
(18%)
6
(20%)
6
(12%)
9
(15%)
8
(12%)
12
(15%)
9
(10%)
16
(20%)
12
(15%)
14
(15%)
Other opacities
(72=11%)
4
(12%)
3
(5%)
9
(18%)
7
(12%)
5
(8%)
15
(20%)
9
(10%)
8
(10%)
8
(10%)
4
(5%)
INDICATIONS
Not for R
elease

Endothelial Cell Loss / 269 eyes
Preoperatively
(cells/mm2)
At 6 months
(cells/mm2)
At 1 year
(cells/mm2)
Mean 2705.9 2420.0 2403.8
ECL =
10-11%
Vincenzo Sarnicola
Not for R
elease
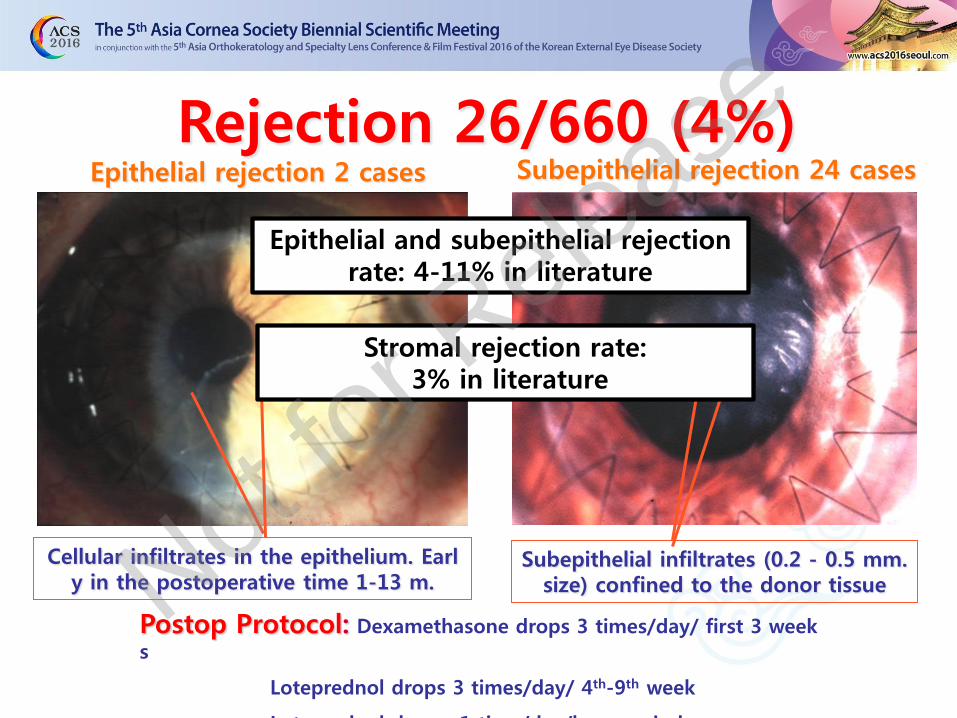
Rejection 26/660 (4%)
Subepithelial infiltrates (0.2 - 0.5 mm. size) confined to the donor tissue
Cellular infiltrates in the epithelium. Early in the postoperative time 1-13 m.
Epithelial rejection 2 cases Subepithelial rejection 24 cases
Postop Protocol: Dexamethasone drops 3 times/day/ first 3 week
s
Loteprednol drops 3 times/day/ 4th-9th week
Loteprednol drops 1 time/day/long period
Epithelial and subepithelial rejection rate: 4-11% in literature
Stromal rejection rate: 3% in literature
Not for R
elease
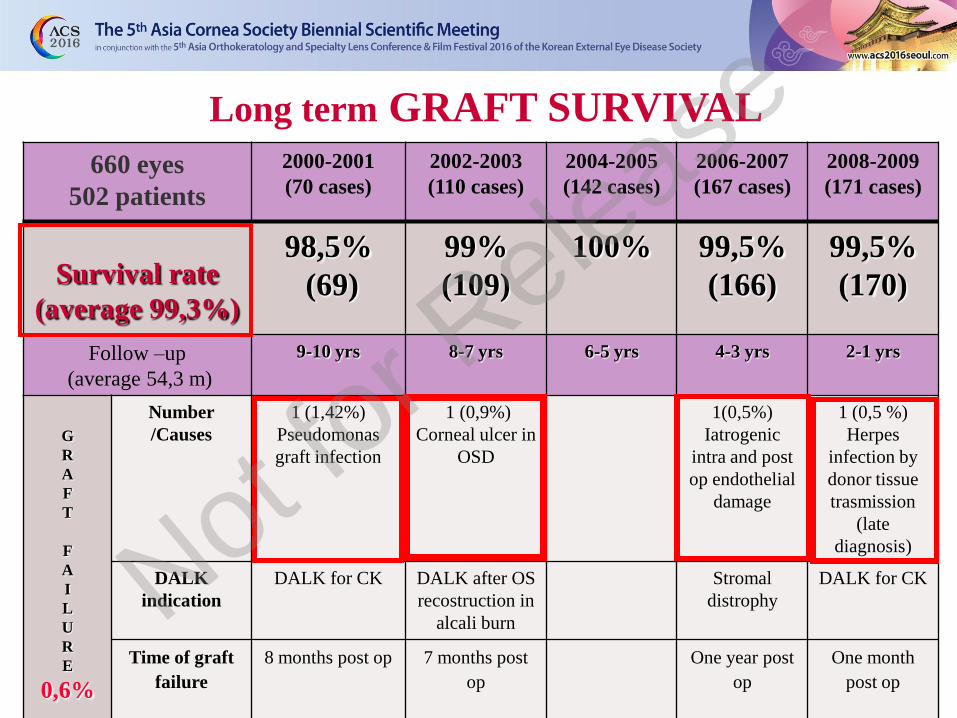
Long term GRAFT SURVIVAL
660 eyes
502 patients
2000-2001
(70 cases)
2002-2003
(110 cases)
2004-2005
(142 cases)
2006-2007
(167 cases)
2008-2009
(171 cases)
Survival rate
(average 99,3%)
98,5%
(69)
99%
(109)
100% 99,5%
(166)
99,5%
(170)
Follow –up
(average 54,3 m)
9-10 yrs 8-7 yrs 6-5 yrs 4-3 yrs 2-1 yrs
G
R
A
F
T
F
A
I
L
U
R
E
0,6%
Number
/Causes
1 (1,42%)
Pseudomonas
graft infection
1 (0,9%)
Corneal ulcer in
OSD
1(0,5%)
Iatrogenic
intra and post
op endothelial
damage
1 (0,5 %)
Herpes
infection by
donor tissue
trasmission
(late
diagnosis)
DALK
indication
DALK for CK DALK after OS
recostruction in
alcali burn
Stromal
distrophy
DALK for CK
Time of graft
failure
8 months post op 7 months post
op
One year post
op
One month
post op
Not for R
elease
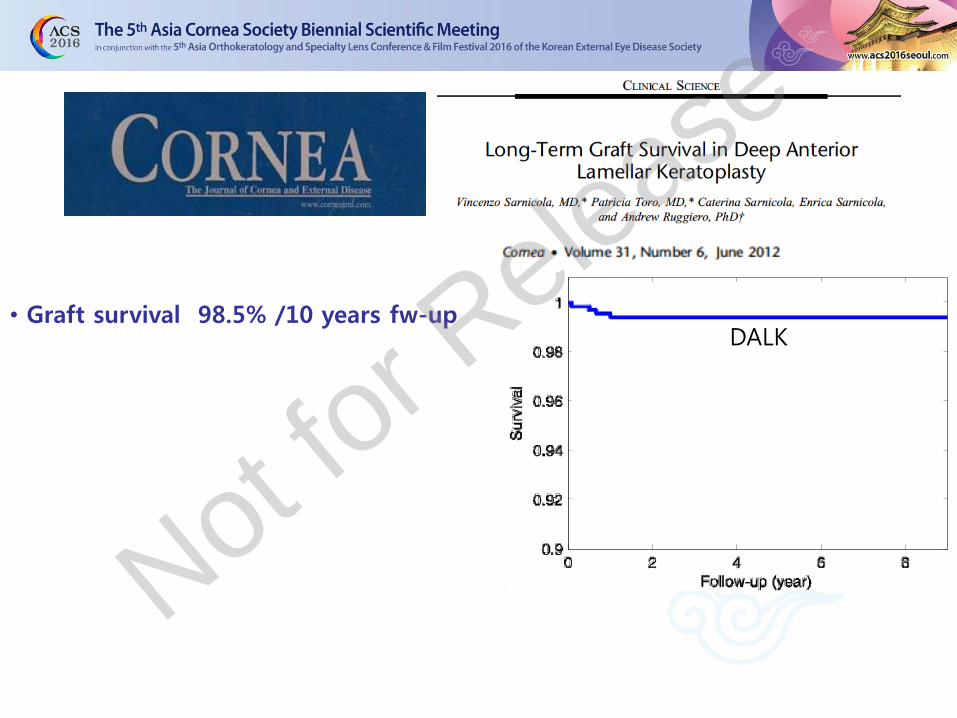
• Graft survival 98.5% /10 years fw-up DALK
Not for R
elease
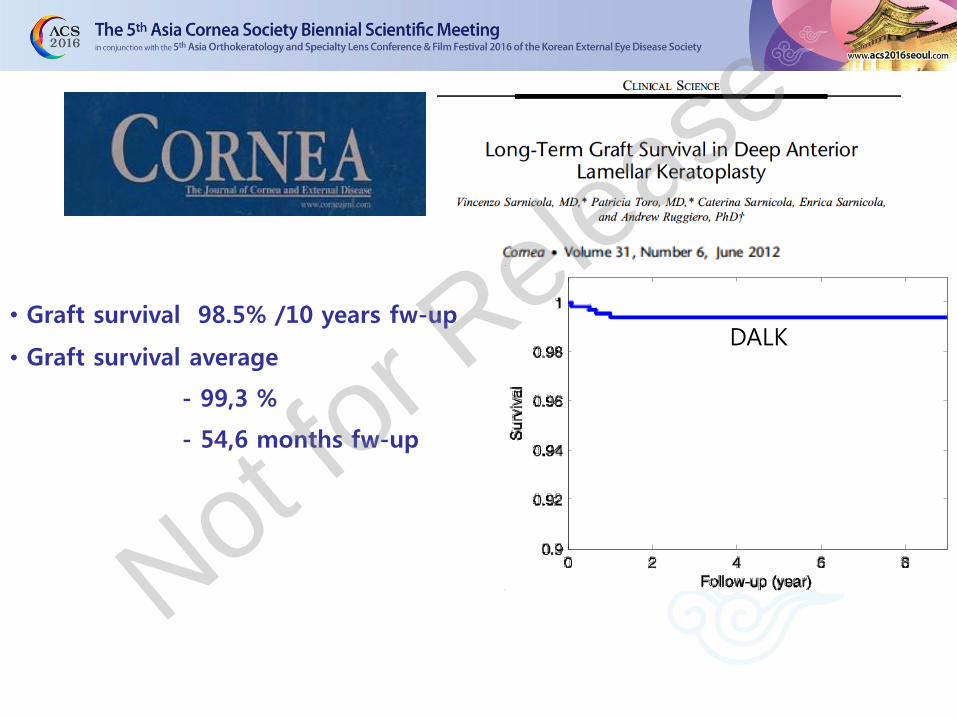
• Graft survival 98.5% /10 years fw-up
• Graft survival average
- 99,3 %
- 54,6 months fw-up
DALK
Not for R
elease

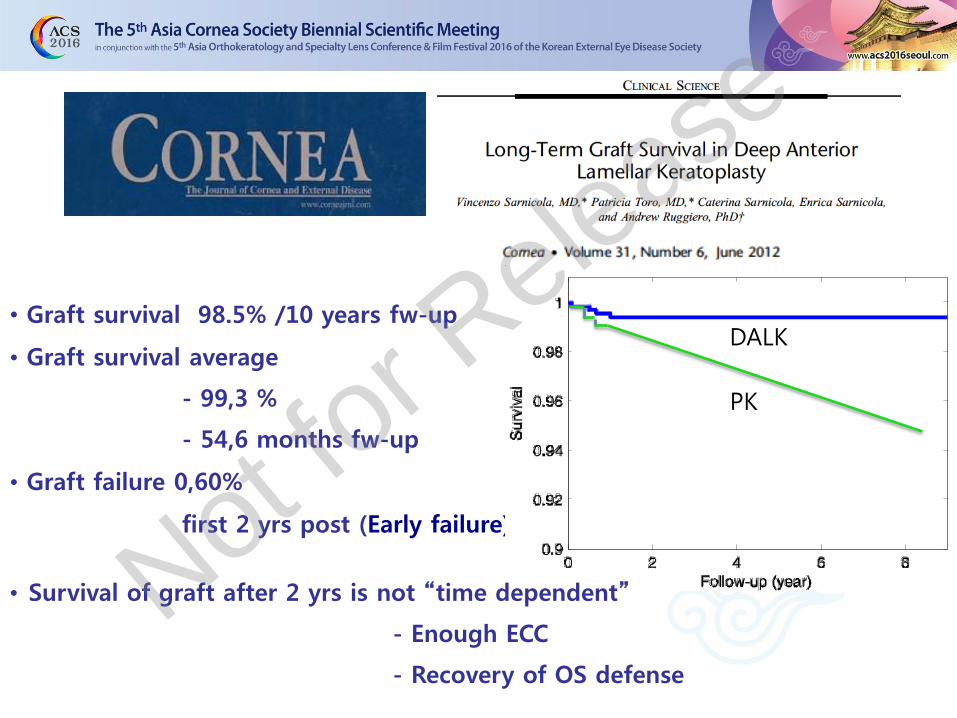
• Graft survival 98.5% /10 years fw-up
• Graft survival average
- 99,3 %
- 54,6 months fw-up
• Graft failure 0,60%
first 2 yrs post (Early failure)
DALK
Not for R
elease

• Graft survival 98.5% /10 years fw-up
• Graft survival average
- 99,3 %
- 54,6 months fw-up
• Graft failure 0,60%
first 2 yrs post (Early failure)
DALK
• Survival of graft after 2 yrs is not “time dependent”
Not fo
r Release

• Graft survival 98.5% /10 years fw-up
• Graft survival average
- 99,3 %
- 54,6 months fw-up
• Graft failure 0,60%
first 2 yrs post (Early failure)
DALK
• Survival of graft after 2 yrs is not “time dependent”
- Enough ECC Not fo
r Release
• Graft survival 98.5% /10 years fw-up
• Graft survival average
- 99,3 %
- 54,6 months fw-up
• Graft failure 0,60%
first 2 yrs post (Early failure)
DALK
PK
• Survival of graft after 2 yrs is not “time dependent”
- Enough ECC
- Recovery of OS defense
Not for R
elease
RESULTS
Not for R
elease
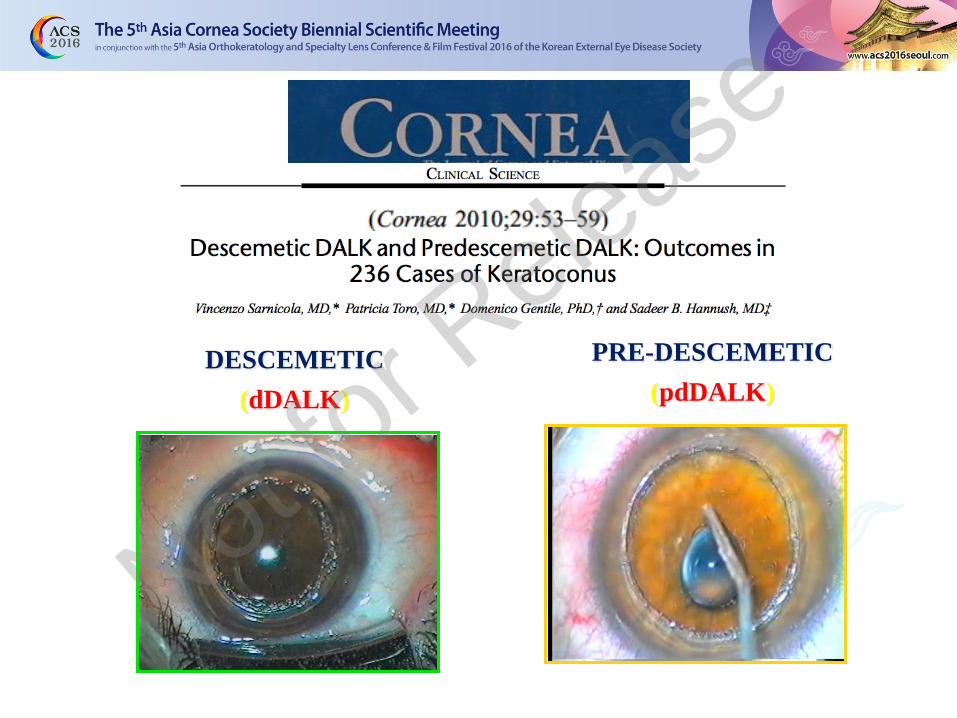
DESCEMETIC
(dDALK)
PRE-DESCEMETIC
(pdDALK)
Not for R
elease

Visual acuity dDALK / pdDALK
0
1
2
3
4
5
6
7
8
9
10
Preop UCVA 18,5 m BSCVA 30,4 m BSCVA
Follow up
Vis
ual
Acu
ity
pdDALK
dDALK
UCVA
Preop.
Postop.
UCVA
Postop.BSCVA At least 7/10
BSCVA
10/10
BSCVA
pdDALK 1,76/10 4.6/10 8.6/10 92/116(80%) 57/116(49%)
dDALK 1,85/10 4.9/10 8.8/10 186/219(85%) 107/219(49%)
48 months follow-up /120 eyes
Descemetic DALK and Predescemetic DALK: Outcomes in 236 Cases of Keratoconus. V.Sarnicola, P. Toro, D.Gentile, and S.Hannush. Cornea 2010;29:53-59
Not for R
elease
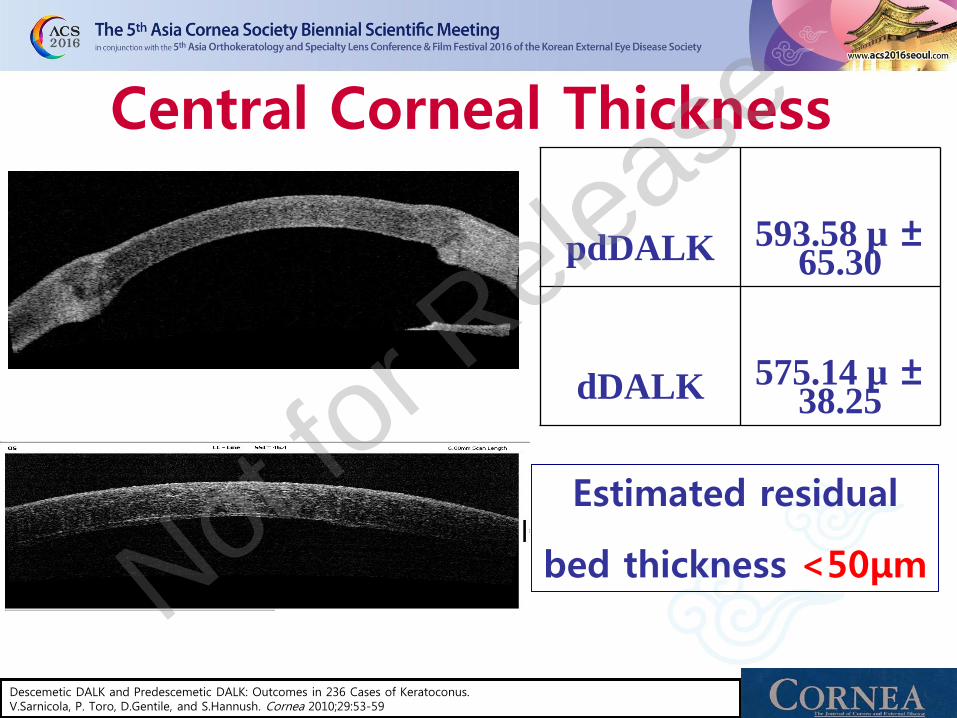
pdDALK 593.58 µ ± 65.30
dDALK 575.14 µ ± 38.25
Central Corneal Thickness
Estimated residual
bed thickness <50μm
Descemetic DALK and Predescemetic DALK: Outcomes in 236 Cases of Keratoconus. V.Sarnicola, P. Toro, D.Gentile, and S.Hannush. Cornea 2010;29:53-59
Not for R
elease

Paper Author Eyes DALK Residual bed thickness
BSCVA Follow-up
Am J Ophthalmol 2007;143:117-24
Fontana et al. 78 50 BB DALK - BB DALK > manual DALK
24months
28 manual DALK NO DATA
Am J Ophthalmol 2007;143:228-35
Ardjomand et al. (Larkin group)
17 6 DALK <20μ DALK ≅ PK 22 months
5 DALK 20-80μ DALK ≅ PK 22 months
6 DALK >80μ DALK < PK 22 months
Am J Ophthalmol 2009;148:744-51
Han et al. (Tan group)
25 14 aDALK - aDALK > mDALK
12 months 11 mDALK NO DATA
Ophthalmology 2011;118:209-218
Reinhart et al. AAO REVIEW
481 11 DALK/PK comparative studies
< 10 % DALK ≅ PK
Acta Ophthalmol Online 6Aug2012 DOI: 10.1111/j.1755-3 768.2012.4432.x
Fournie et al. 95 74 dDALK - dDALK > pdDALK dDALK ≅ pdDALK
2 years 5 years 21 pdDALK NO DATA
Am J Ophthalmol 2015;159:505-11
Romano et al. (Fontana group)
158 109 BB DALK BB DALK ≅ manual DALK
5 years
49 manual DALK
NO DATA
Not for R
elease
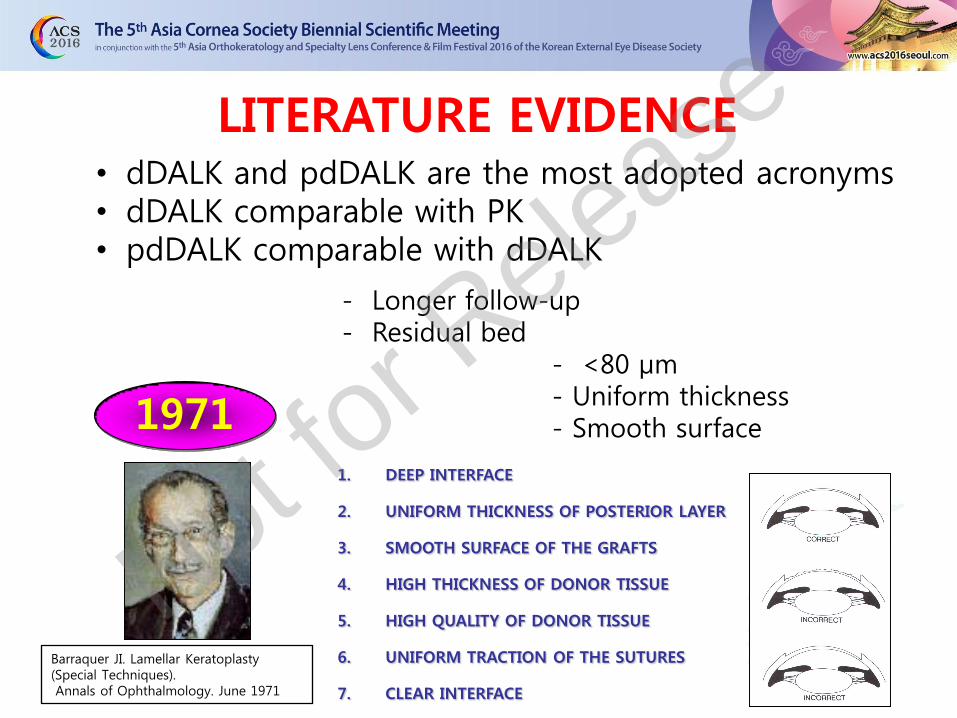
• dDALK and pdDALK are the most adopted acronyms • dDALK comparable with PK • pdDALK comparable with dDALK
- Longer follow-up - Residual bed - <80 μm - Uniform thickness - Smooth surface 1971 1. DEEP INTERFACE
2. UNIFORM THICKNESS OF POSTERIOR LAYER
3. SMOOTH SURFACE OF THE GRAFTS
4. HIGH THICKNESS OF DONOR TISSUE
5. HIGH QUALITY OF DONOR TISSUE
6. UNIFORM TRACTION OF THE SUTURES
7. CLEAR INTERFACE
LITERATURE EVIDENCE
Barraquer JI. Lamellar Keratoplasty (Special Techniques). Annals of Ophthalmology. June 1971
Not for R
elease
Clinica degli occh
i Sarnicola
Vincenzo Sarnicola
• Big bubble DALK (BB DALK)
• Maximum depth DALK (MD-DALK)
• Anwar DALK (aDALK)
• Descemet bared DALK
• Manual DALK (mDALK)
• Etc.
NOMENCLATURE
Not for R
elease
Clinica degli occh
i Sarnicola
Vincenzo Sarnicola
• Big bubble DALK (BB DALK)
• Maximum depth DALK (MD-DALK)
• Anwar DALK (aDALK)
• Descemet bared DALK
• Manual DALK (mDALK)
• Etc.
• Predescemetic DALK (pdDALK)
• Descemetic DALK (dDALK)
NOMENCLATURE
Not for R
elease
Clinica degli occh
i Sarnicola
Vincenzo Sarnicola
• Big bubble DALK (BB DALK)
• Maximum depth DALK (MD-DALK)
• Anwar DALK (aDALK)
• Descemet bared DALK
• Manual DALK (mDALK)
• Etc.
• Predescemetic DALK (pdDALK)
• Descemetic DALK (dDALK)
• Dua’s layer
NOMENCLATURE
Not for R
elease
Not for R
elease

“...BB 1 cleaves off a distinct layer at the posterior surface of the corneal stroma
BB Type 1
• Well circumscribed • White egde • Up to 8.5mm diameter (max 9.0 mm and then pops) • Startes in the center and enlarge circumferentially • Popping pressure 1.4-1.5 bar • It is possible to peel off the DM witho
ut deflating the BB Not for R
elease
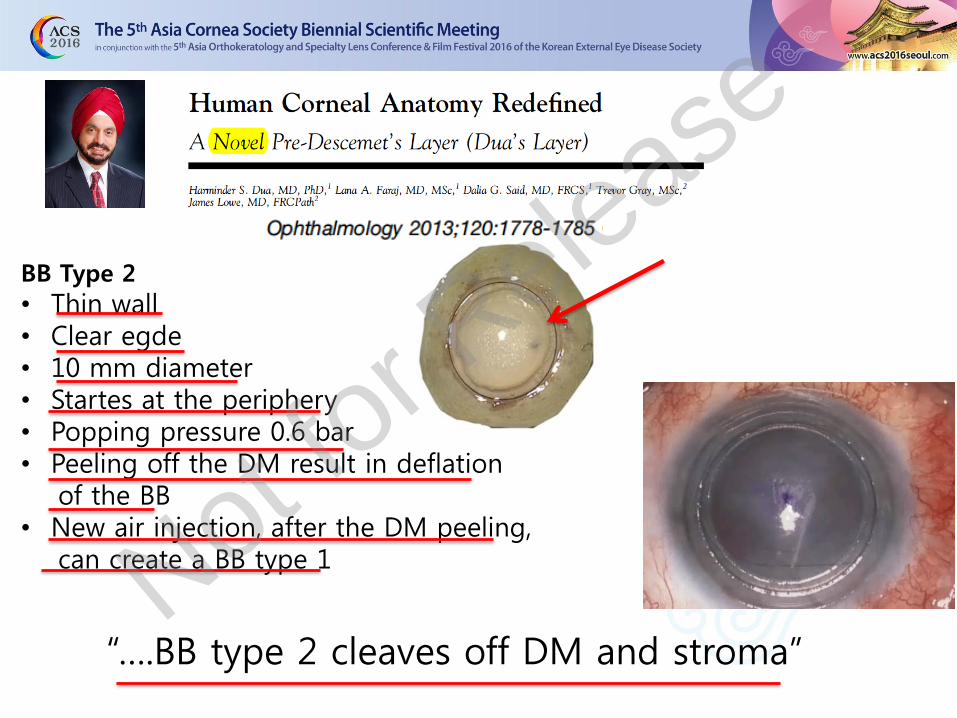
“….BB type 2 cleaves off DM and stroma”
BB Type 2
• Thin wall • Clear egde • 10 mm diameter • Startes at the periphery • Popping pressure 0.6 bar • Peeling off the DM result in deflation of the BB • New air injection, after the DM peeling, can create a BB type 1 Not fo
r Release

DUA’S LAYER
….BB 1 cleaves off a distinct layer at the posterior surface of the corneal stroma,
which is not “residual stroma”…… (Dua’s Layer)
- HISTOLOGY: • This layer is acellular • Measured 10.15±3.6 microns • Composed of 5 to 8 lamellae of predominantly type 1 • collagen arranged in trasverse, longitudinal and oblique directions
Not for R
elease
Not for R
elease

“…..anathomic descriptions….demonstrate the presence of keratocytes within 5 μm of the posterior lamina. This observation runs counter to a supposed hallmark of this so-called new layer, that is acellularity.”
“Although the observations presented are novel and illuminate an important mechanical response to acutley introduced nonphysiologic strain, in our opinion, The data presented do not warrant the assignation of a new anatomic layer to the cornea.”
Not for R
elease

Not for R
elease
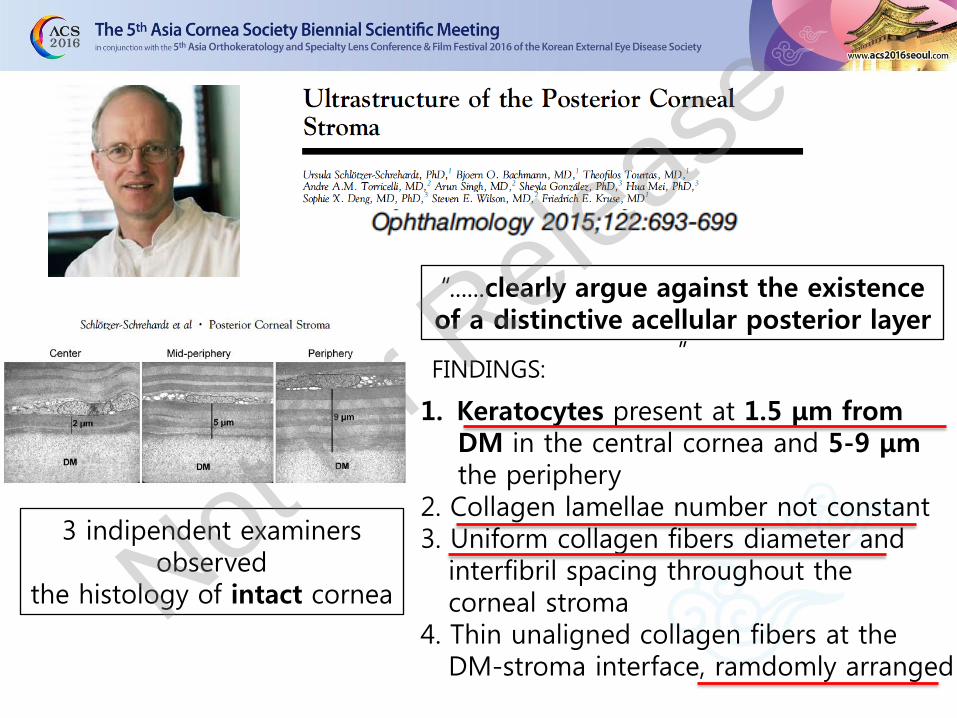
3 indipendent examiners observed
the histology of intact cornea
“......clearly argue against the existence of a distinctive acellular posterior layer
” FINDINGS:
1. Keratocytes present at 1.5 μm from DM in the central cornea and 5-9 μm the periphery 2. Collagen lamellae number not constant 3. Uniform collagen fibers diameter and interfibril spacing throughout the corneal stroma 4. Thin unaligned collagen fibers at the DM-stroma interface, ramdomly arranged
Not for R
elease
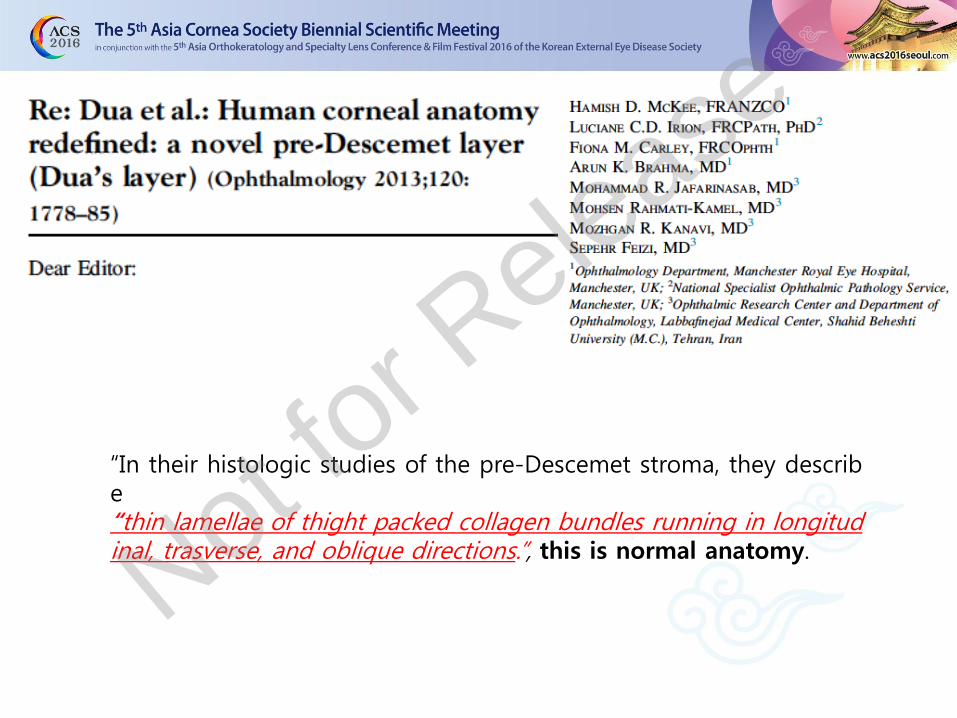
“In their histologic studies of the pre-Descemet stroma, they describe “thin lamellae of thight packed collagen bundles running in longitudinal, trasverse, and oblique directions.”, this is normal anatomy. Not fo
r Release
Not for R
elease
“Even though…
the existence of a new corneal anatomic layer is not
fully acctepted in literature….”
“Everybody should agree that…
Harminder Dua described, at least, the characteristics of a new surgical plane!!”
Vincenzo Sarnicola Asia Cornea Society, Seoul December 2016
Not fo
r Release
UNDOUBTED ADVANTAGES OF DUA’S INVESTIGATION
1- Classification of BB Type 1, Type2 and Type 3
• Dangerousness of BB Type2 • Maximum diameter of BB Type 1 • Visual outcomes • Characetristics of DM ruptures
2- Understanding of corneal biomechanics
• DALK better resistence following trauma vs PK • Acute hydrops in keratoconus • Resistance of Descemetocele before perforation • Recurrence of Macular dystrophy after BB Type 1 • Ect.
VERY IMPORTANT PRACTICAL APPLICATION
Not for R
elease
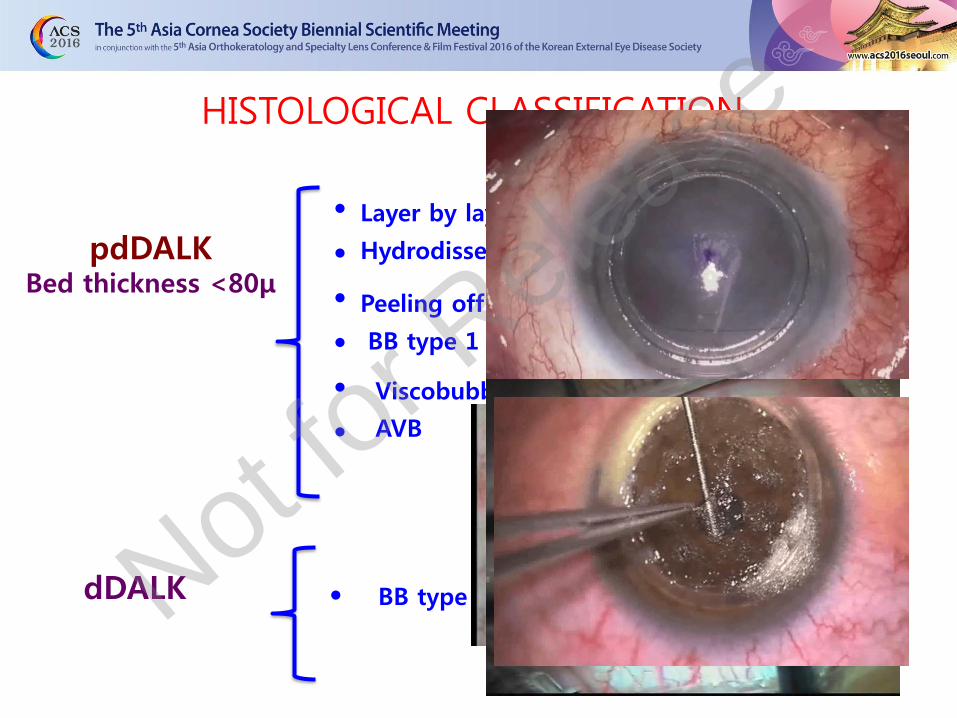
HISTOLOGICAL CLASSIFICATION
pdDALK Bed thickness <80μ
dDALK BB type 2
•Layer by layer •Hydrodissection
•Peeling off
• • • • • •
•
Layer by layer
Hydrodissection
Peeling off
•BB type 1
BB type 1
Viscobubble
AVB
•Viscobubble •AVB
• BB type 2
Not for R
elease
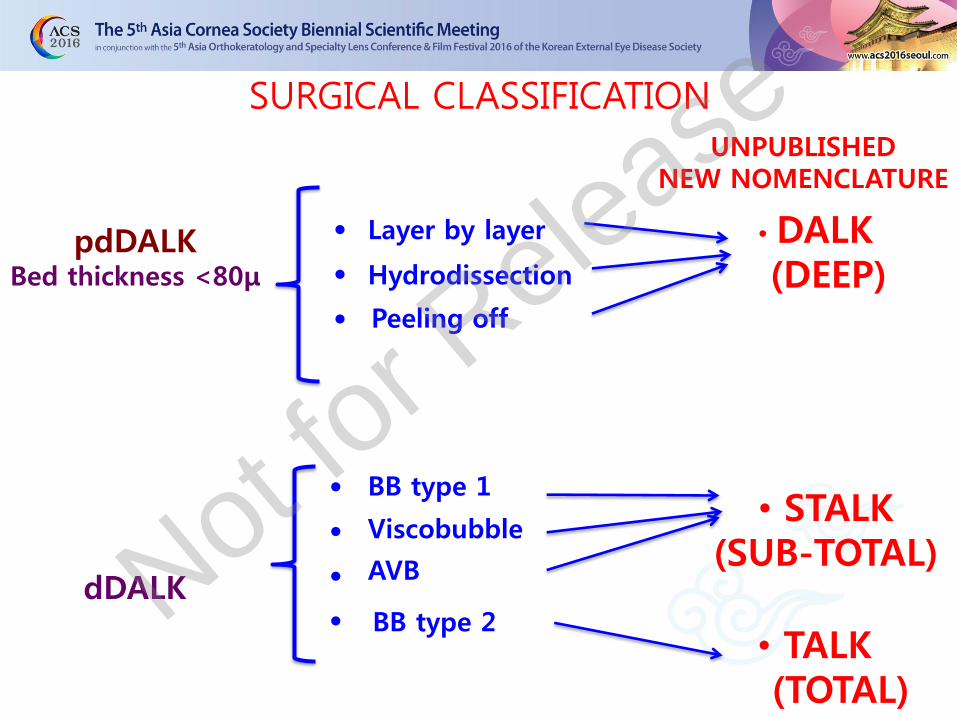
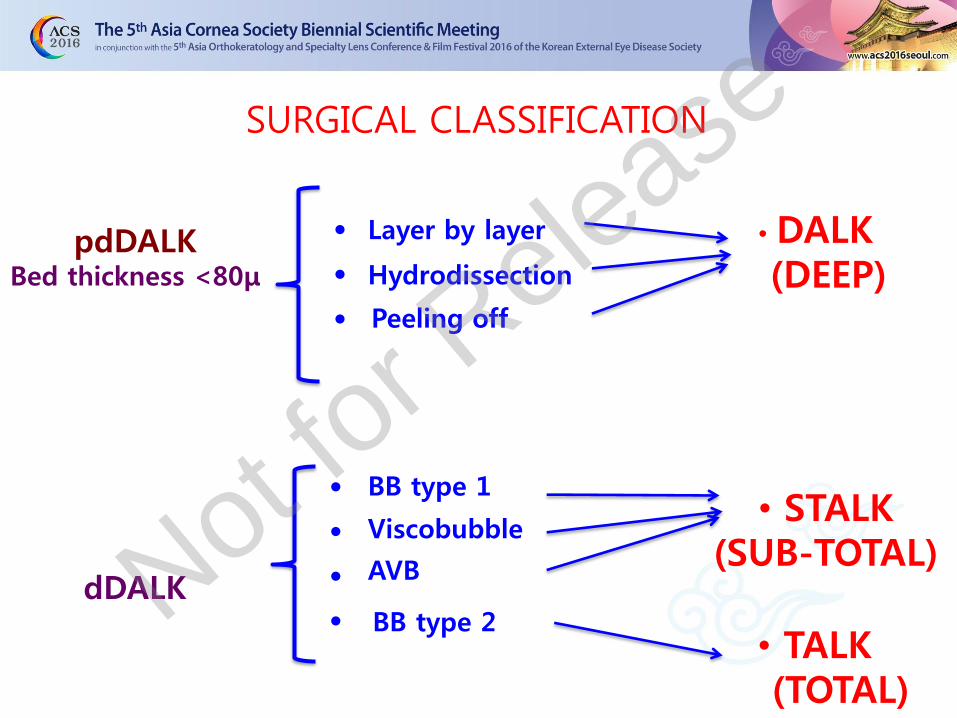
SURGICAL CLASSIFICATION
pdDALK Bed thickness <80μ
dDALK BB type 2
• • •
• • • •
Layer by layer
Hydrodissection
Peeling off
BB type 1
Viscobubble
AVB
• TALK (TOTAL)
• STALK (SUB-TOTAL)
• DALK (DEEP)
UNPUBLISHED NEW NOMENCLATURE
Not for R
elease

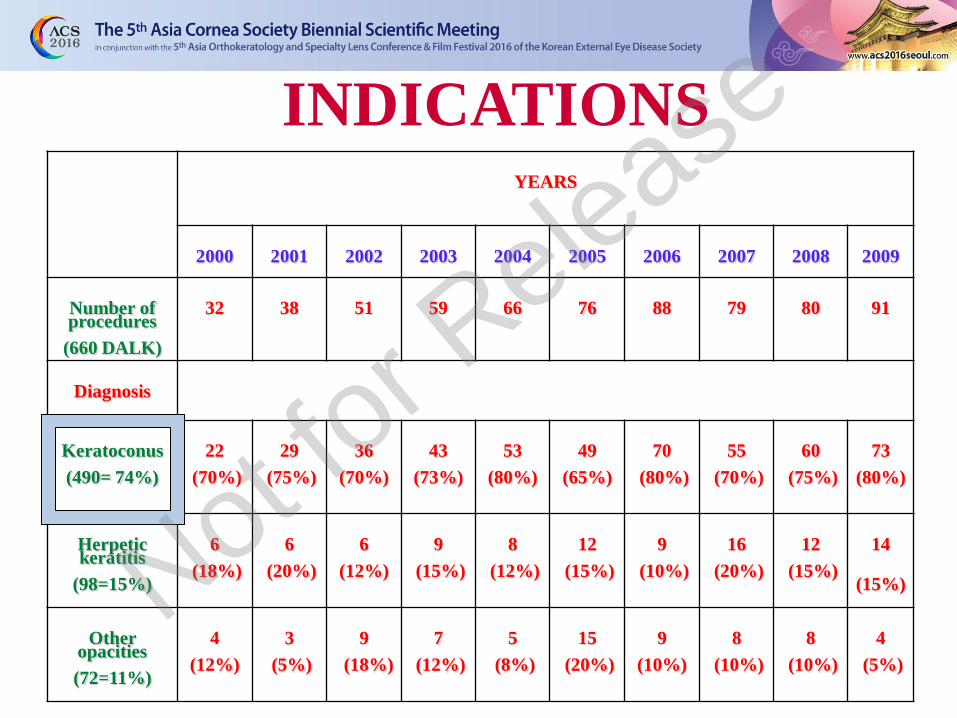
INDICATIONS
Not for R
elease
YEARS
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
Number of procedures
(660 DALK)
32
38
51
59
66
76
88
79
80
91
Diagnosis
Keratoconus
(490= 74%)
22
(70%)
29
(75%)
36
(70%)
43
(73%)
53
(80%)
49
(65%)
70
(80%)
55
(70%)
60
(75%)
73
(80%)
Herpetic keratitis
(98=15%)
6
(18%)
6
(20%)
6
(12%)
9
(15%)
8
(12%)
12
(15%)
9
(10%)
16
(20%)
12
(15%)
14
(15%)
Other opacities
(72=11%)
4
(12%)
3
(5%)
9
(18%)
7
(12%)
5
(8%)
15
(20%)
9
(10%)
8
(10%)
8
(10%)
4
(5%)
INDICATIONS
Not for R
elease
1.- DALK in EXTREME ECTASIA
2.- DALK in INFECTIONS
3.- DALK in CORNEAL PENETRATING WOUNDS
4.- DALK in OCULAR SURFACE DISEASES
DALK OTHER INDICATIONS
• Keratoglobus
• Scar • Active infections
Not for R
elease

KERATOGLOBUS
Vincenzo Sarnicol
Not for R
elease

pdDALK in KERATOGLOBUS
Vincenzo Sarnicola, ASCRS, Boston 2014
Not for R
elease
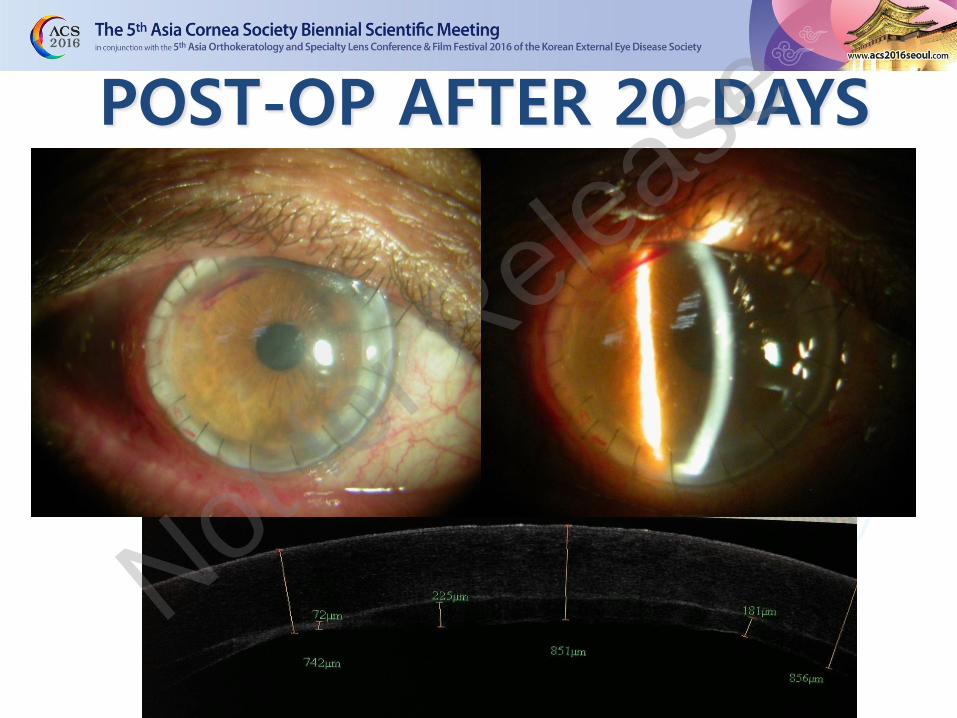
POST-OP AFTER 20 DAYS
Not for R
elease
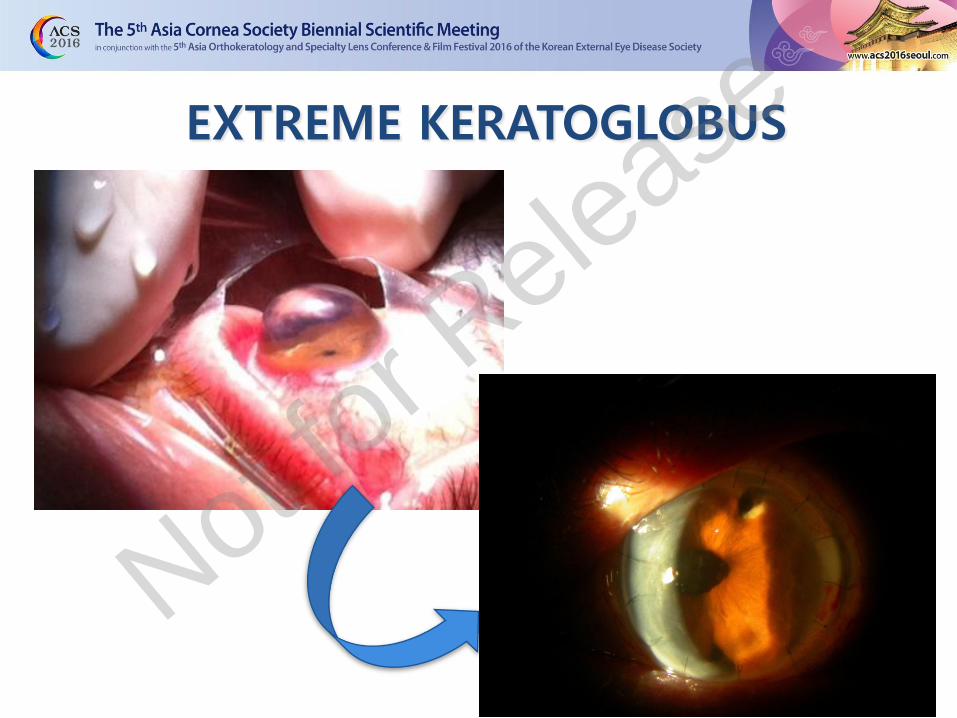
EXTREME KERATOGLOBUS
Not for R
elease

1.- DALK in EXTREME ECTASIA
2.- DALK in INFECTIONS
3.- DALK in CORNEAL PENETRATING WOUNDS
4.- DALK in OCULAR SURFACE DISEASES
DALK OTHER INDICATIONS
• Keratoglobus
• Scar • Active infections
Not for R
elease

Preop UCVA: 1/10 (20/200) BSCVA: NI Ph: 3/10 (20/63)
1 year postop UCVA: 5/10 (20/40) BSCVA: 8/10 (20/25) -1.50 cyl 180 Ph: 10/10 (20/20)
HSV SCAR
Not for R
elease
DALK
SYSTEMIC ACYCLOVIR
LOCAL LOTEPREDNOL
Not for R
elease
Not for R
elease

Vincenzo Sarnicola, ASCRS, Boston 2014
5 MONTHS THERAPY (ORAL ACYCLOVIR, LOTEPREDNOL EYE DROPS)
Not for R
elease

Preop One year post-op
UCVA 20/100 BSCVA 20/25 (+2cyl x 90°)
Not for R
elease
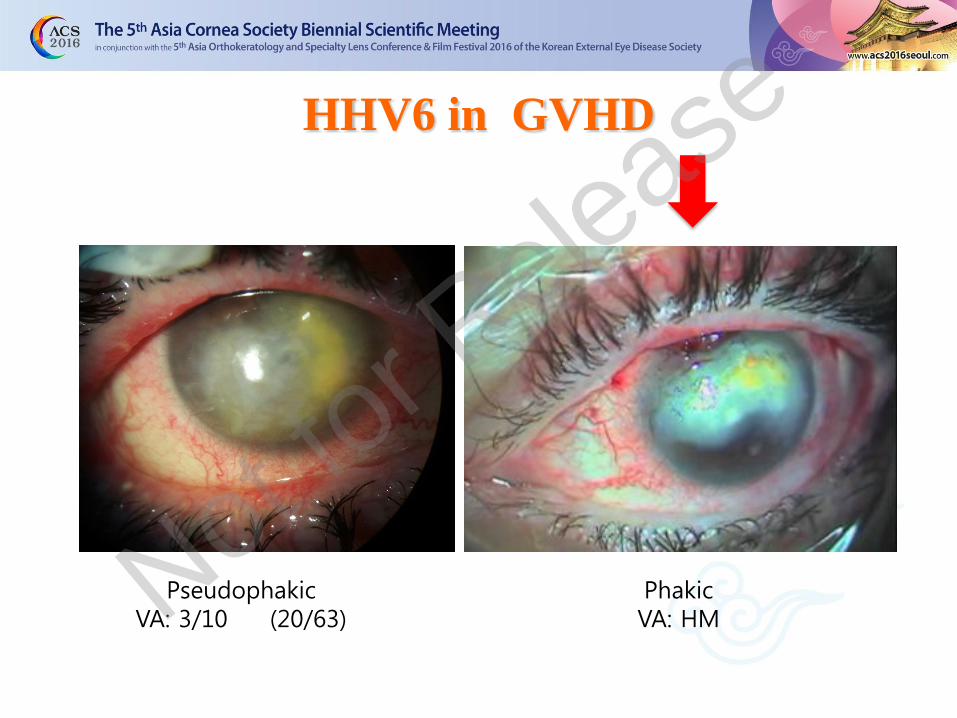
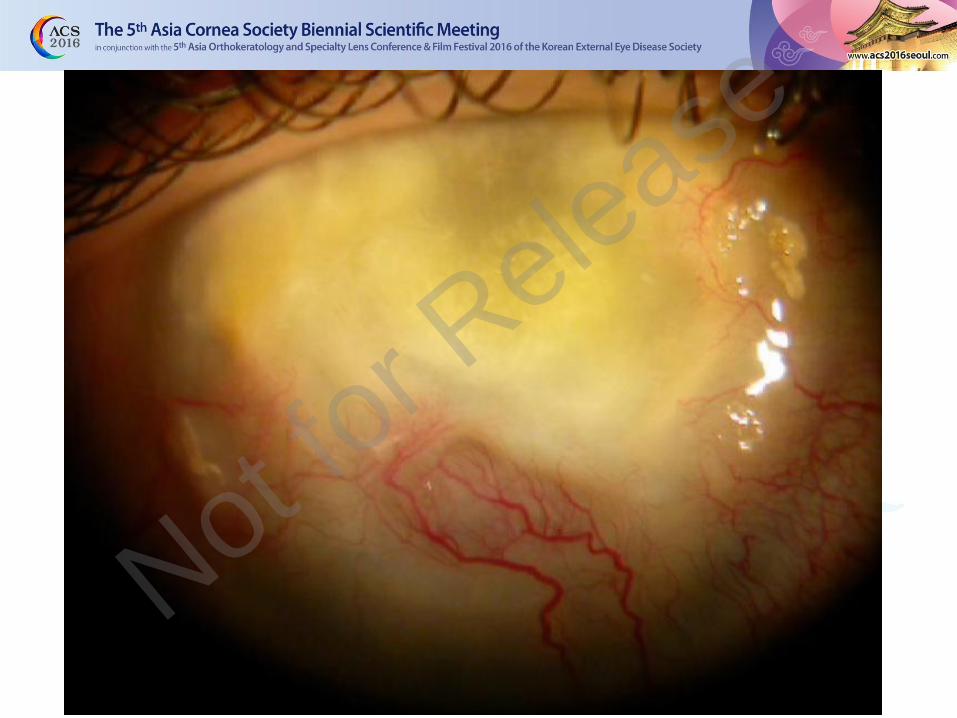
HHV6 in GVHD
Phakic VA: HM
Pseudophakic VA: 3/10 (20/63) Not fo
r Release
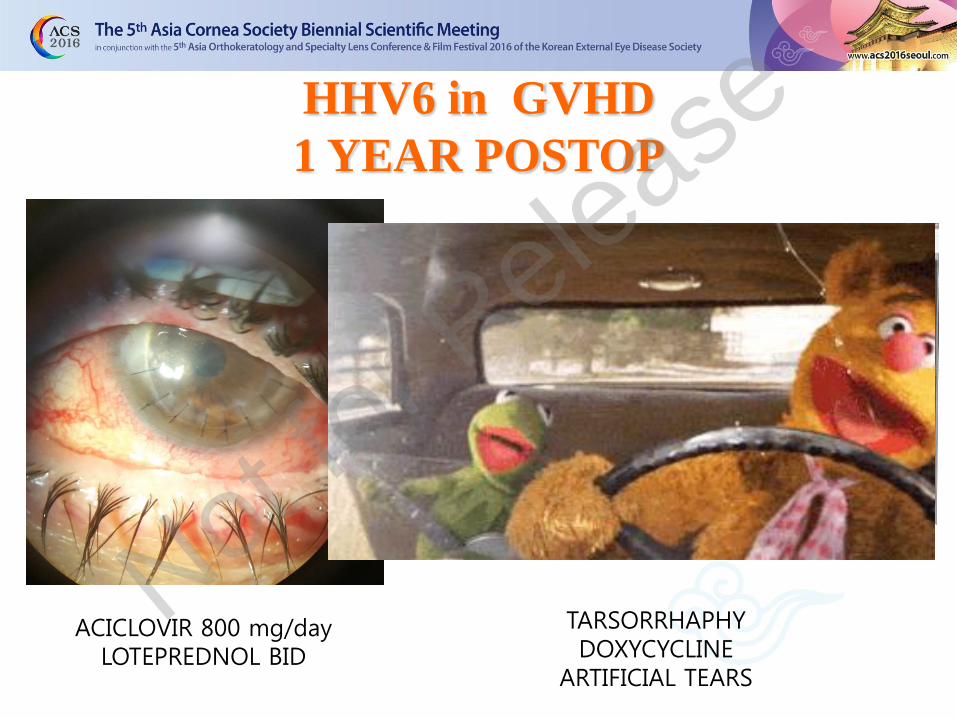
HHV6 in GVHD
1 YEAR POSTOP
ACICLOVIR 800 mg/day LOTEPREDNOL BID
TARSORRHAPHY DOXYCYCLINE
ARTIFICIAL TEARS
Not for R
elease
1.- DALK in EXTREME ECTASIA
2.- DALK in INFECTIONS
3.- DALK in CORNEAL PENETRATING WOUNDS
4.- DALK in OCULAR SURFACE DISEASES
DALK OTHER INDICATIONS
• Keratoglobus
• Scar • Active infections
Not for R
elease
Not for R
elease
EARLY DALK in infectious keratitis
poorly responsive to medical treatment
• Significant ulcer (>150) in optical zone : (Presumed scar penalizing VA)
• Dangerousness of infection (Fungal and Acanthamoeba keratitis)
• Absence of prompt medical therapy response (NO reduction, or at least stabilization, of size lesion and/ or symptoms, after 1 week of targeted therapy)
• Patient’s compliance
Clinica degli occhi
Sarnicola
Vincenzo Sarnicola
Not for R
elease
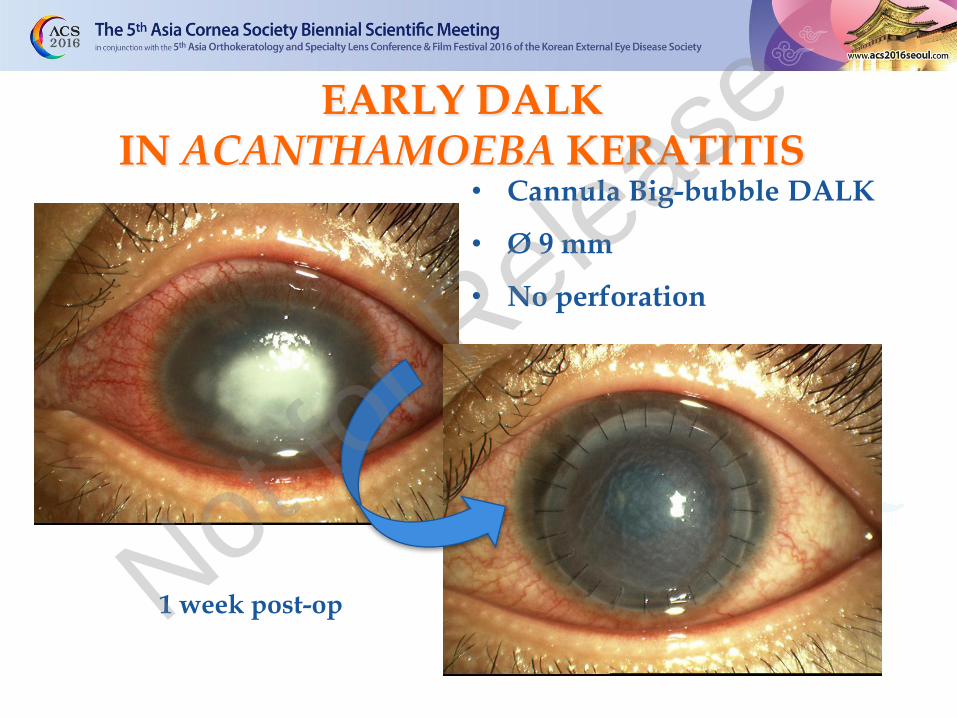
1 week post-op
• Cannula Big-bubble DALK
• Ø 9 mm
• No perforation
EARLY DALK IN ACANTHAMOEBA KERATITIS
Not for R
elease
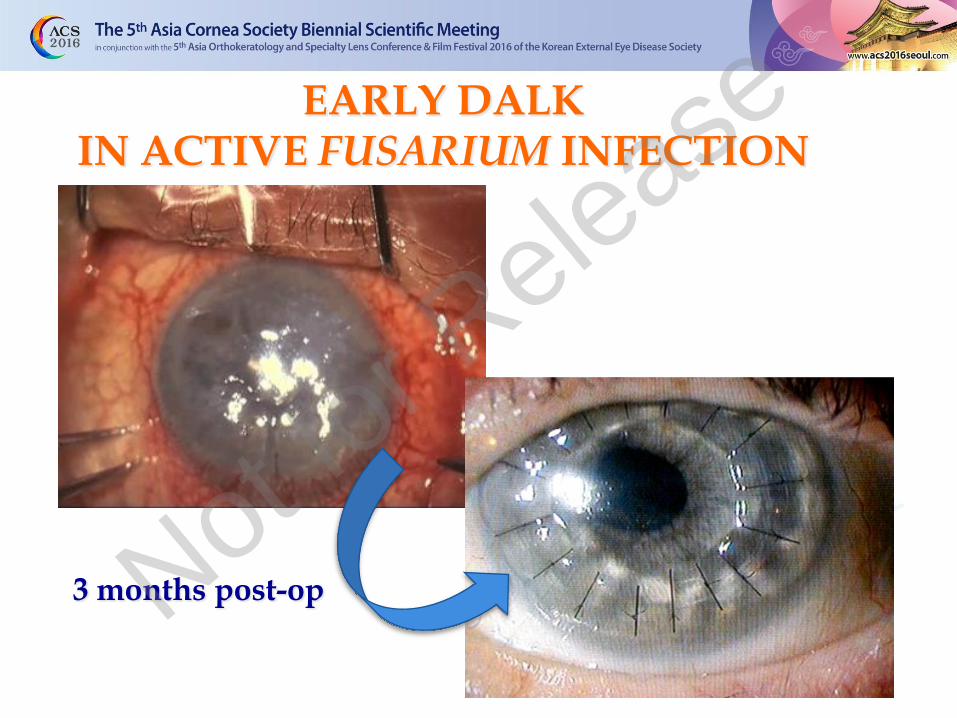
EARLY DALK IN ACTIVE FUSARIUM INFECTION
3 months post-op Not for R
elease
1.- DALK in ECTASIA
2.- DALK in INFECTIONS
3.- DALK in CORNEAL PENETRATING WOUNDS
4.- DALK in OCULAR SURFACE DISEASES
INDICATIONS
• Keratoconus • Keratoglobus
• Scar • Active infections
Not for R
elease

PENETRATING WOUND -Man, 16 years old
- Penetrating corneal trauma OD (February, 2012)
- Visual acuity OD:
•20/200 -1 sph
- pdDALK March, 2013
Not for R
elease
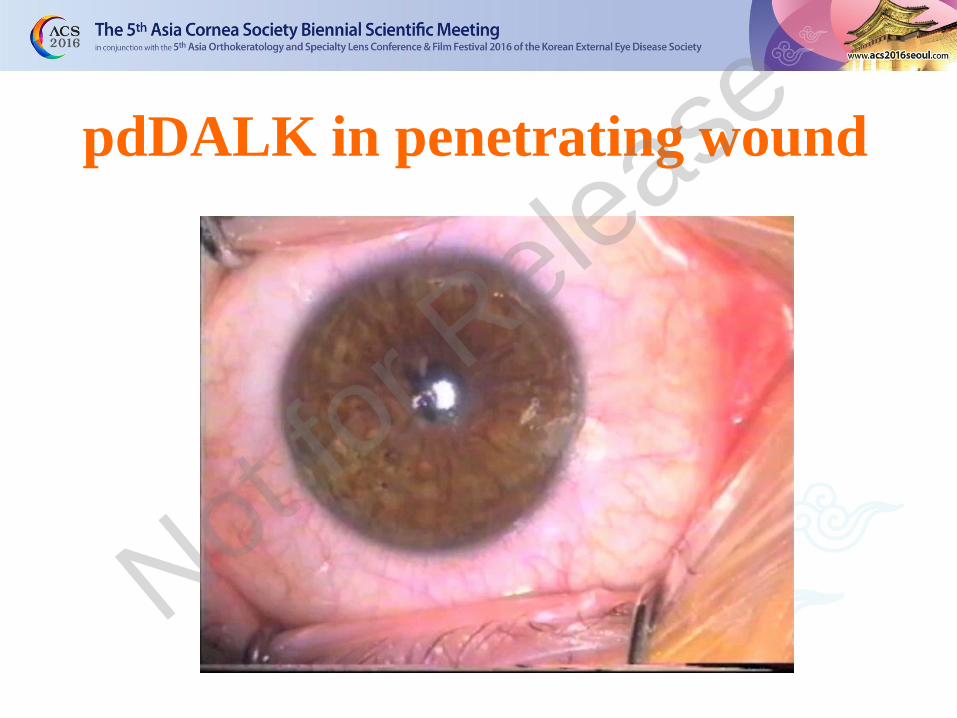
pdDALK in penetrating wound
Not for R
elease
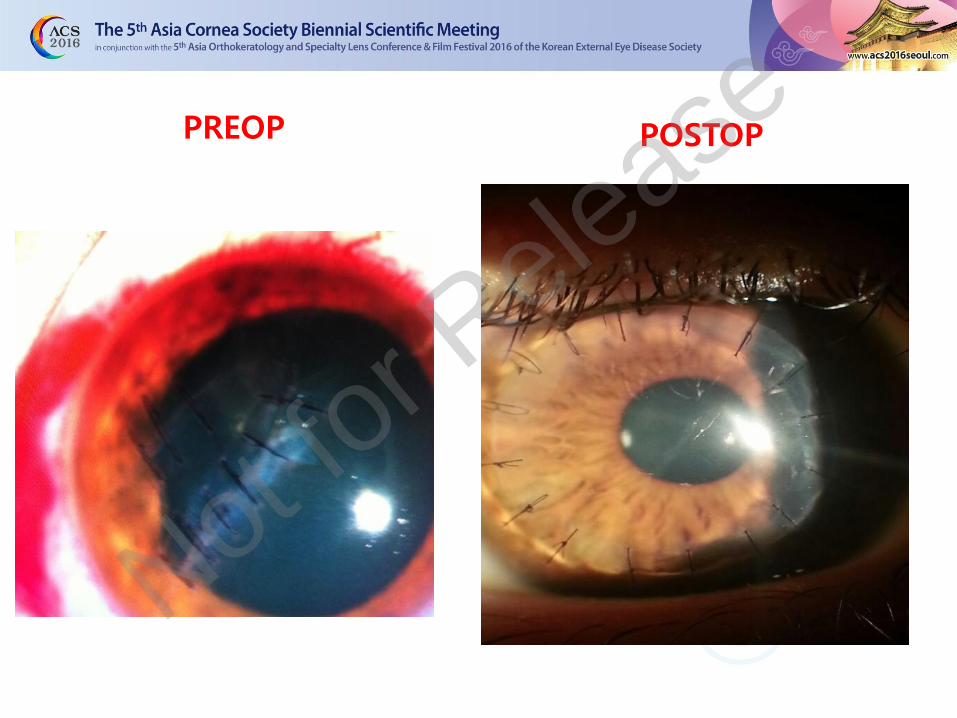
PREOP POSTOP
Not for R
elease

1.- DALK in ECTASIA
2.- DALK in INFECTIONS
3.- DALK in CORNEAL PENETRATING WOUNDS
4.- DALK in OCULAR SURFACE DISEASES
INDICATIONS
• Keratoconus • Keratoglobus
• Scar • Active infections
Not for R
elease

Chemical burn
V. Sarnicola, 2012
After autolimbal t
ransplantation
Not for R
elease

“ ….the corneal endothelium and Descemet’s
membrane must remain intact if a corneal graft
was to succeed……”
Leber 1911
Mannis M, Mannis A. Corneal transplantation: a history in profiles. The monographs. 1999
Not for R
elease

Grosseto (Tuscany) Italy
22-24 June 2017
The I nternational Congressof the I tal ian
Society of Stem Cellsand Surface
XVISI CSSO Congress
www.sicsso.org/congress2017
Mobile: +39 331 7073818 - Email: [email protected]
SAVE TH E D ATE
Teatro degli Industri
Clinica degli occhi S
arnicola
Grosseto (Tuscany) Italy
22-24 June 2017
The I nternational Congressof the I tal ian
Society of Stem Cellsand Surface
XVISI CSSO Congress
www.sicsso.org/congress2017
Mobile: +39 331 7073818 - Email: [email protected]
SAVE TH E D ATE
Teatro degli Industri
Not for R
elease

Not for R
elease
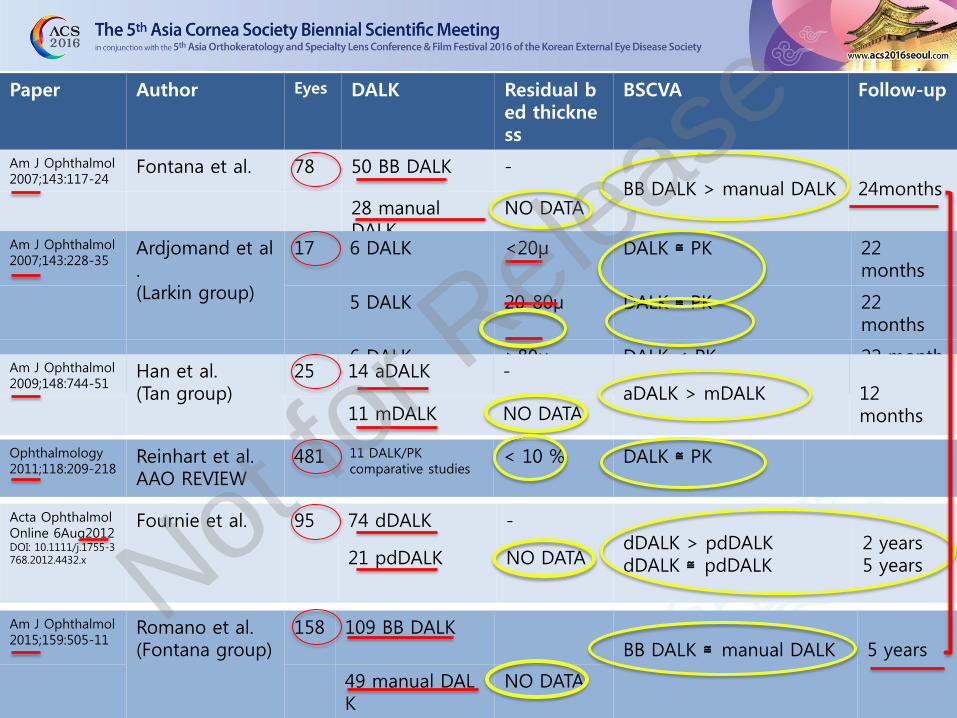
Paper Author Eyes DALK Residual bed thickness
BSCVA Follow-up
Am J Ophthalmol 2007;143:117-24
Fontana et al. 78 50 BB DALK - BB DALK > manual DALK
24months
28 manual DALK
NO DATA
Am J Ophthalmol 2007;143:228-35
Ardjomand et al. (Larkin group)
17 6 DALK <20μ DALK ≅ PK 22 months
5 DALK 20-80μ DALK ≅ PK 22 months
6 DALK >80μ DALK < PK 22 months
Am J Ophthalmol 2009;148:744-51
Han et al. (Tan group)
25 14 aDALK - aDALK > mDALK
12 months 11 mDALK NO DATA
Ophthalmology 2011;118:209-218
Reinhart et al. AAO REVIEW
481 11 DALK/PK comparative studies
< 10 % DALK ≅ PK
Acta Ophthalmol Online 6Aug2012 DOI: 10.1111/j.1755-3 768.2012.4432.x
Fournie et al. 95 74 dDALK - dDALK > pdDALK dDALK ≅ pdDALK
2 years 5 years 21 pdDALK NO DATA
Am J Ophthalmol 2015;159:505-11
Romano et al. (Fontana group)
158 109 BB DALK BB DALK ≅ manual DALK
5 years
49 manual DALK
NO DATA
Not for R
elease
Clinica degli occh
i Sarnicola
Vincenzo Sarnicola
• Big bubble DALK (BB DALK)
• Maximum depth DALK (MD-DALK)
• Anwar DALK (aDALK)
• Descemet bared DALK
• Manual DALK (mDALK)
• Etc.
NOMENCLATURE
Not for R
elease
Clinica degli occh
i Sarnicola
Vincenzo Sarnicola
• Big bubble DALK (BB DALK)
• Maximum depth DALK (MD-DALK)
• Anwar DALK (aDALK)
• Descemet bared DALK
• Manual DALK (mDALK)
• Etc.
• Predescemetic DALK (pdDALK)
• Descemetic DALK (dDALK)
VISUAL OUTCOME
Not for R
elease
Clinica degli occh
i Sarnicola
Vincenzo Sarnicola
• Big bubble DALK (BB DALK)
• Maximum depth DALK (MD-DALK)
• Anwar DALK (aDALK)
• Descemet bared DALK
• Manual DALK (mDALK)
• Etc.
• Predescemetic DALK (pdDALK)
• Descemetic DALK (dDALK)
VISUAL OUTCOME
Not for R
elease
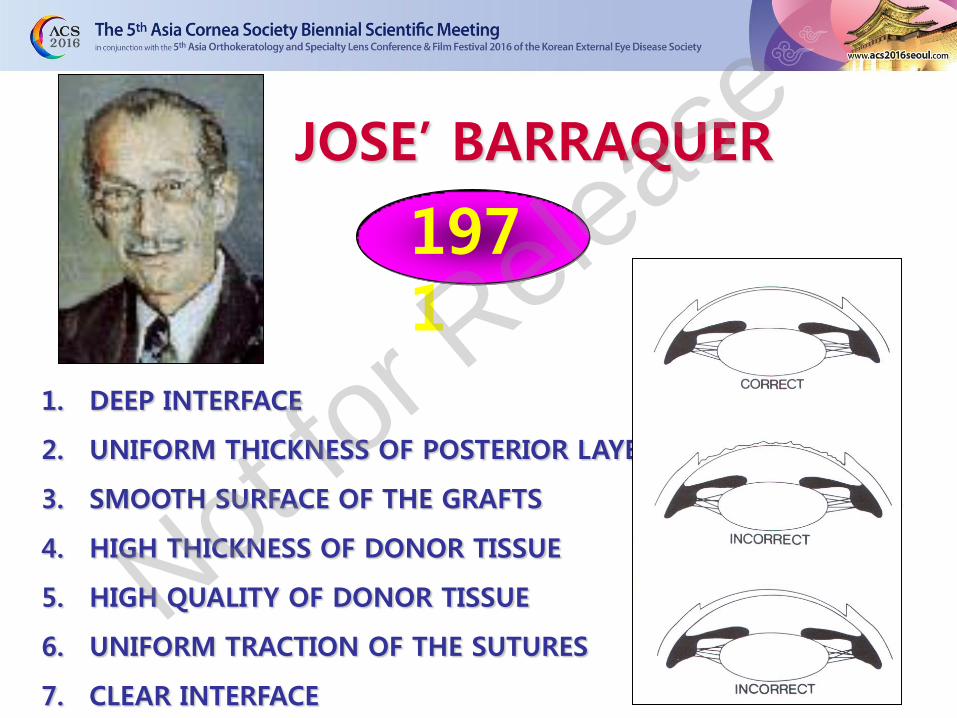
JOSE’ BARRAQUER
1971
1. DEEP INTERFACE
2. UNIFORM THICKNESS OF POSTERIOR LAYER
3. SMOOTH SURFACE OF THE GRAFTS
4. HIGH THICKNESS OF DONOR TISSUE
5. HIGH QUALITY OF DONOR TISSUE
6. UNIFORM TRACTION OF THE SUTURES
7. CLEAR INTERFACE
Not for R
elease
Clinica degli occh
i Sarnicola
Vincenzo Sarnicola
• Big bubble DALK (BB DALK)
• Maximum depth DALK (MD-DALK)
• Anwar DALK (aDALK)
• Descemet bared DALK
• Manual DALK (mDALK)
• Etc.
• Predescemetic DALK (pdDALK)
• Descemetic DALK (dDALK)
VISUAL OUTCOME
Not for R
elease
ADAM EVE
Not for R
elease

HISTOLOGICAL CLASSIFICATION
pdDALK Bed thickness <80μ
dDALK BB type 2
•Layer by layer •Hydrodissection
•Peeling off
• • • • • •
•
Layer by layer
Hydrodissection
Peeling off
•BB type 1
BB type 1
Viscobubble
AVB
•Viscobubble •AVB
• BB type 2
Not for R
elease
SURGICAL CLASSIFICATION
pdDALK Bed thickness <80μ
dDALK BB type 2
• • •
• • • •
Layer by layer
Hydrodissection
Peeling off
BB type 1
Viscobubble
AVB
• TALK (TOTAL)
• STALK (SUB-TOTAL)
• DALK (DEEP)
Not for R
elease
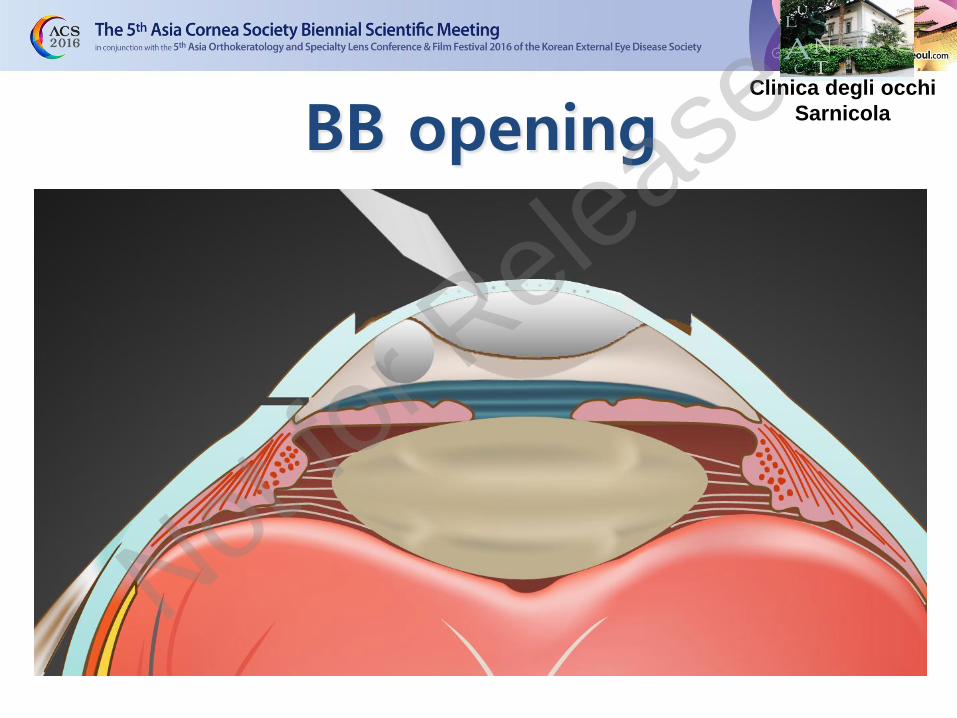
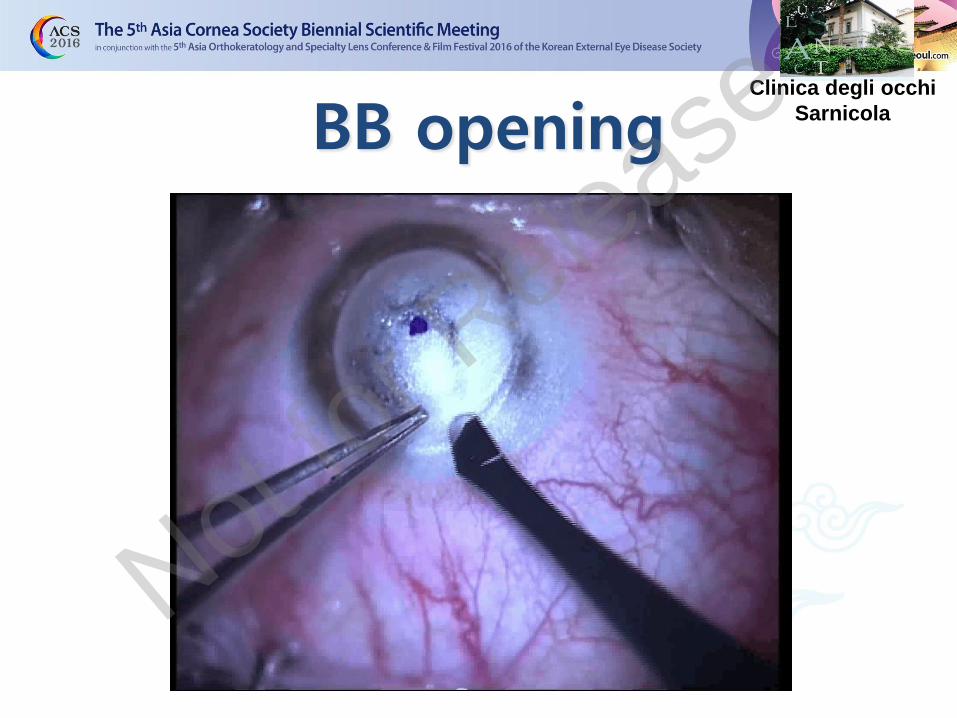
BB opening Clinica degli occhi
Sarnicola
Not for R
elease

BB opening Clinica degli occhi
Sarnicola
Not for R
elease

BB opening Clinica degli occhi
Sarnicola
Not for R
elease
BB opening Clinica degli occhi
Sarnicola
Not for R
elease

DALK for KERATOCONUS: STANDARD TECHNIQUE
TODAY
Clinica degli occhi
Sarnicola
Not for R
elease
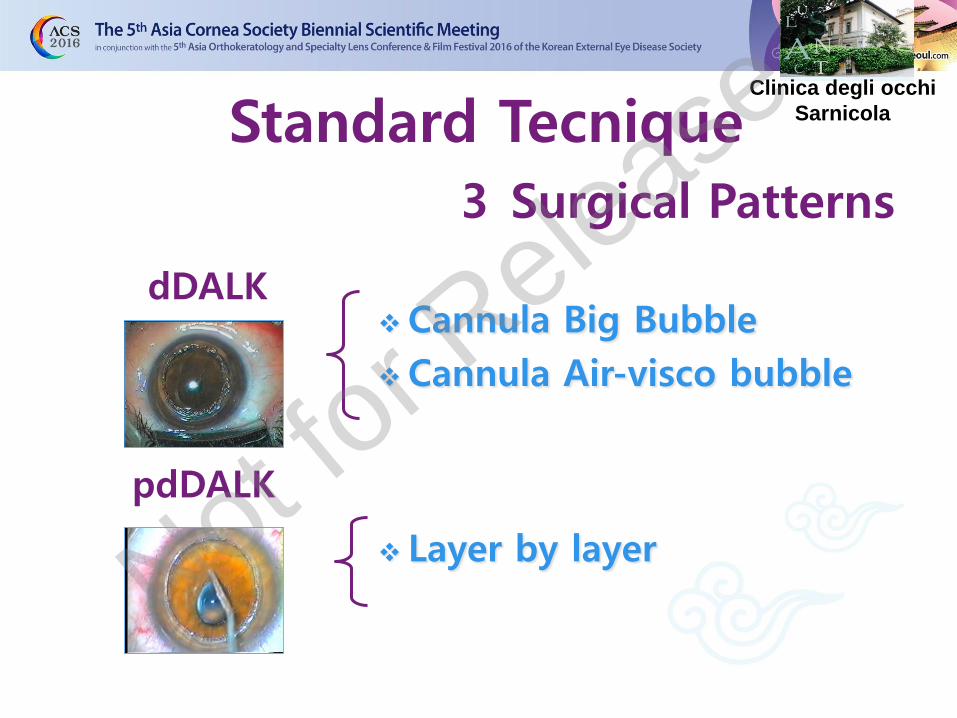
Standard Tecnique
3 Surgical Patterns
Cannula Big Bubble
Cannula Air-visco bubble
Layer by layer
dDALK
pdDALK
Clinica degli occhi
Sarnicola
Not for R
elease
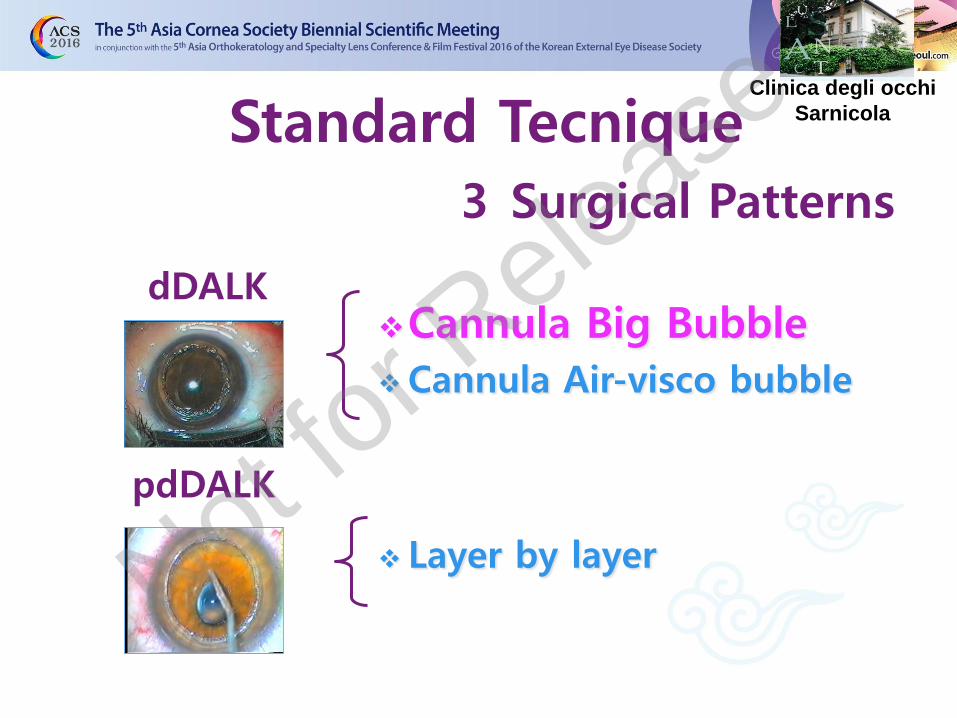
Standard Tecnique
3 Surgical Patterns
Cannula Big Bubble
Cannula Air-visco bubble
Layer by layer
dDALK
pdDALK
Clinica degli occhi
Sarnicola
Not for R
elease
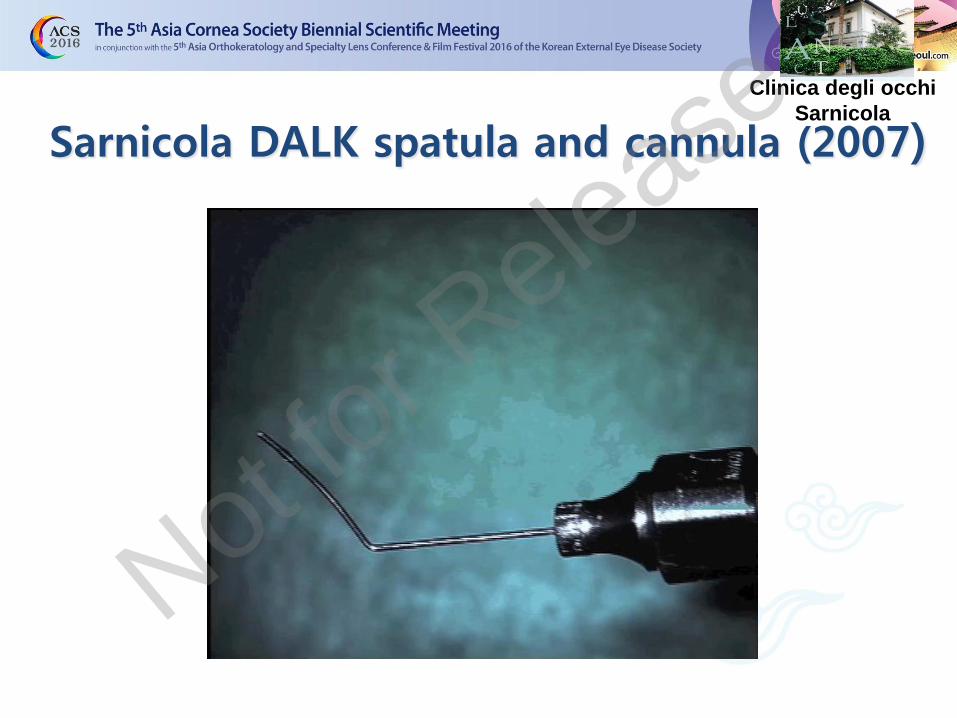
Sarnicola DALK spatula and cannula (2007)
Clinica degli occhi
Sarnicola
Not for R
elease
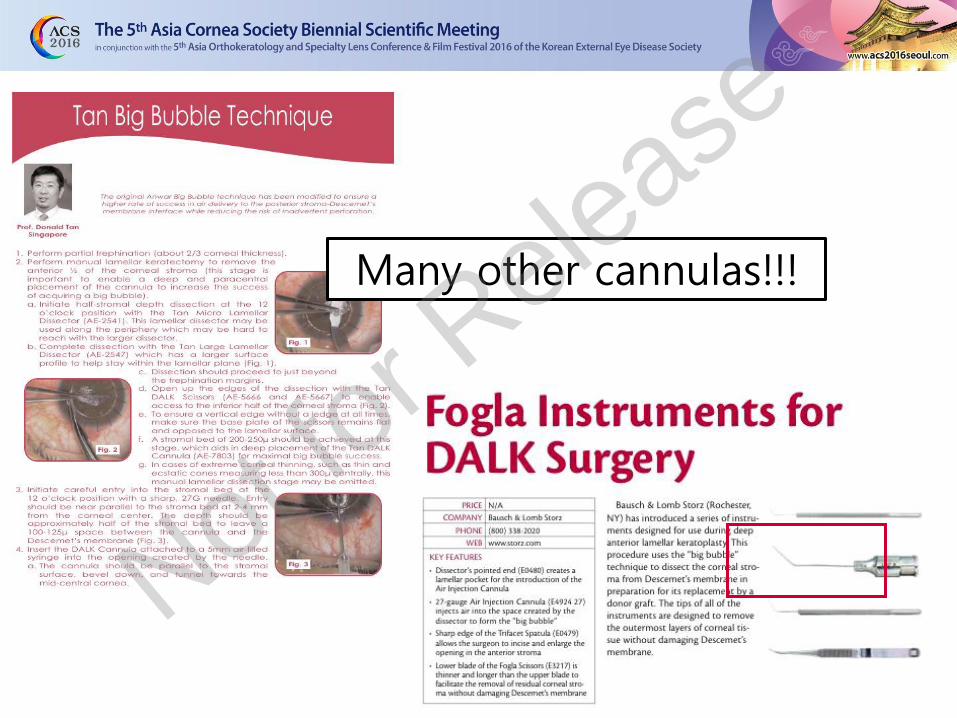
Many other cannulas!!!
Not for R
elease

Cannula BB Clinica degli occhi
Sarnicola
Not for R
elease

Cannula 27G
Clinica degli occhi
Sarnicola
Not for R
elease
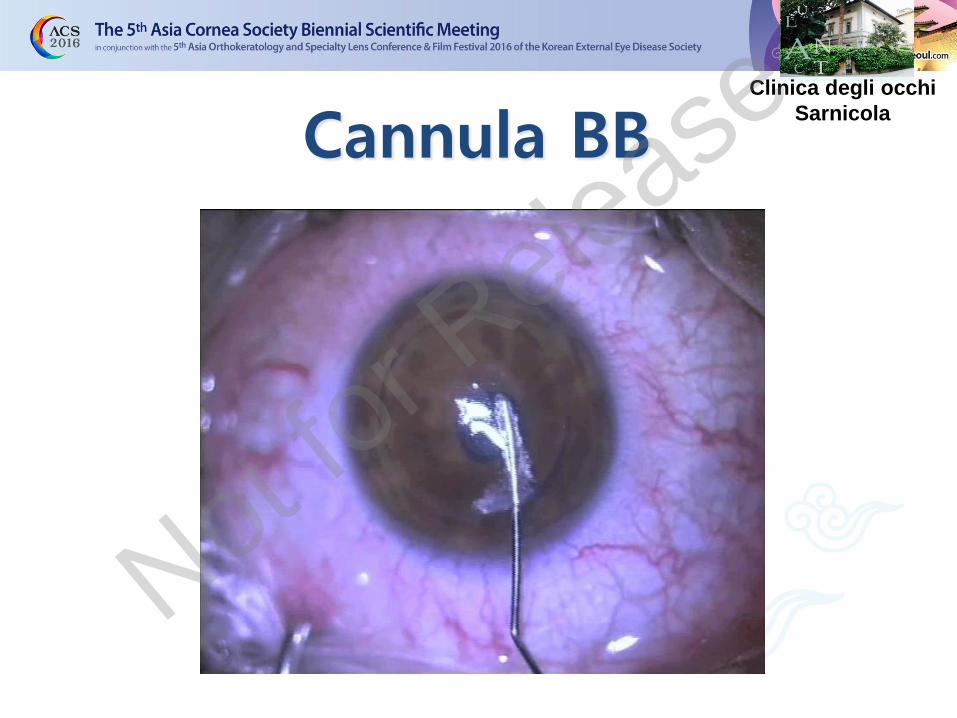
Cannula BB Clinica degli occhi
Sarnicola
Not for R
elease
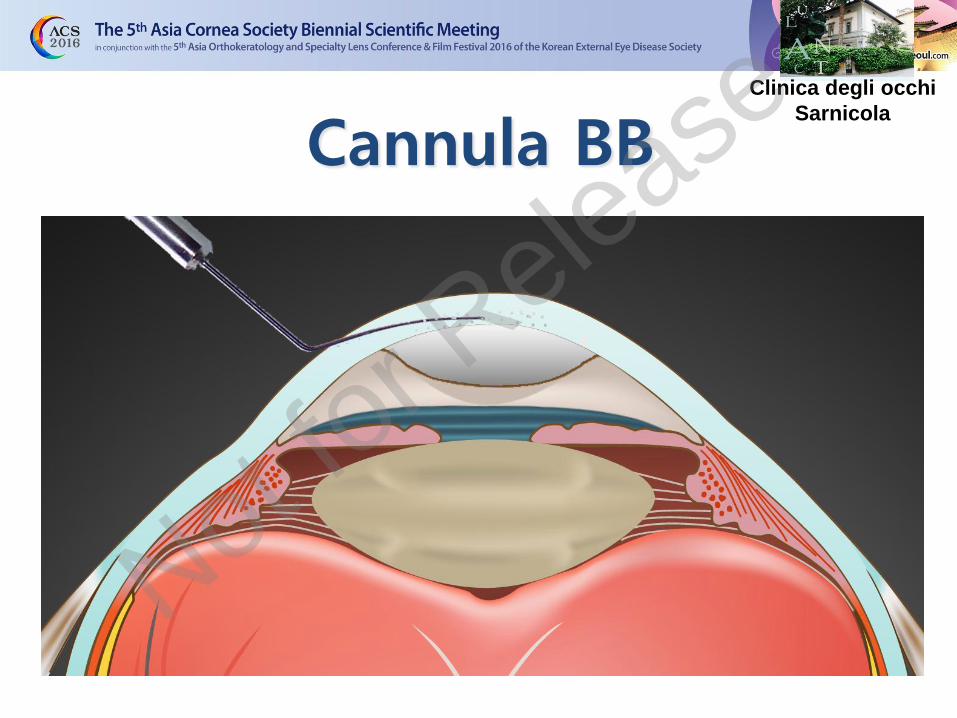
Cannula BB Clinica degli occhi
Sarnicola
Not for R
elease

Bubble test Clinica degli occhi
Sarnicola
Not for R
elease

BB Test Clinica degli occhi
Sarnicola
Not for R
elease
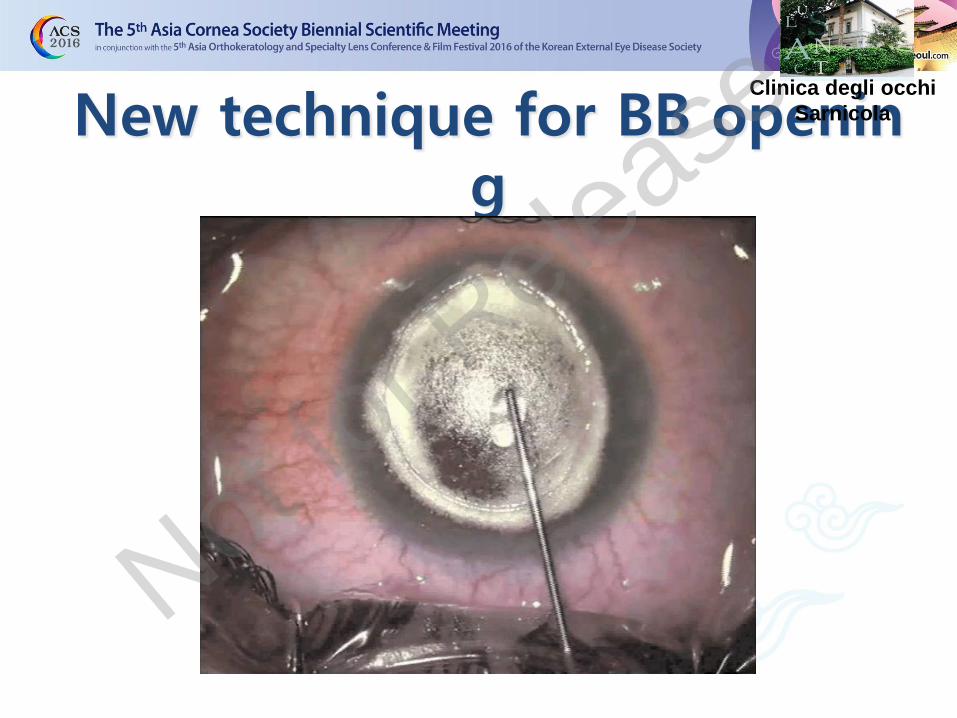
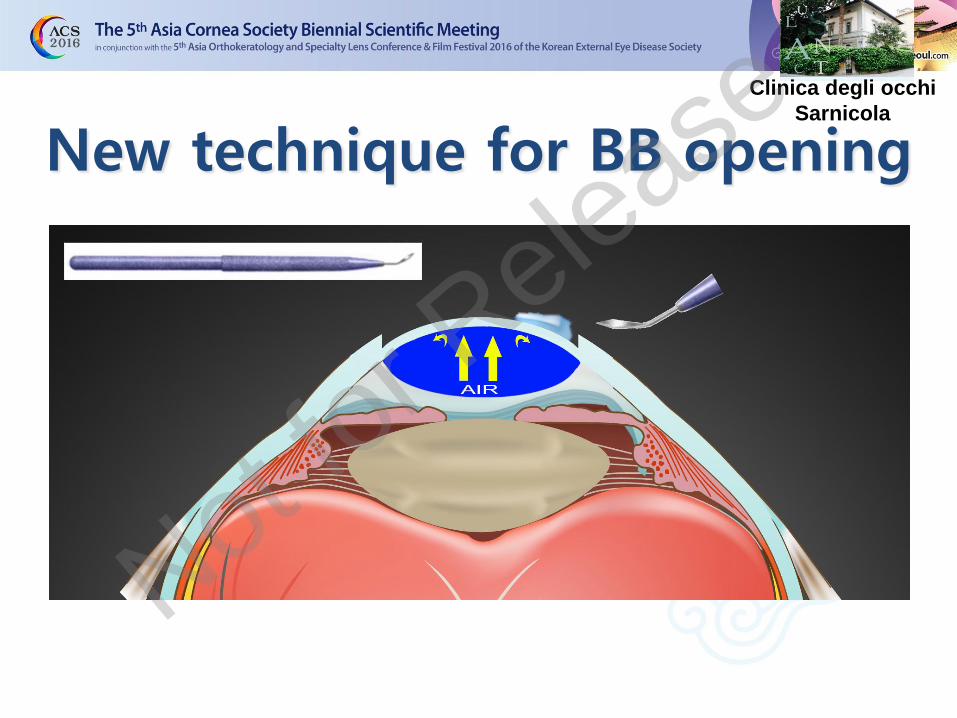
New technique for BB opening
Clinica degli occhi
Sarnicola
Not for R
elease
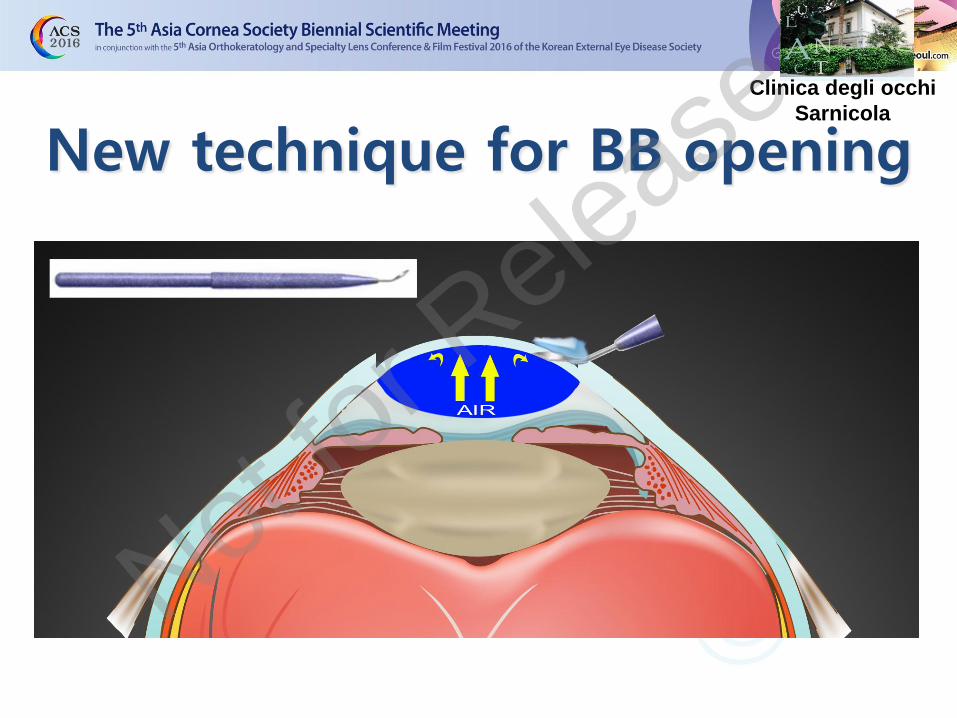
Clinica degli occhi
Sarnicola
New technique for BB opening
Not for R
elease

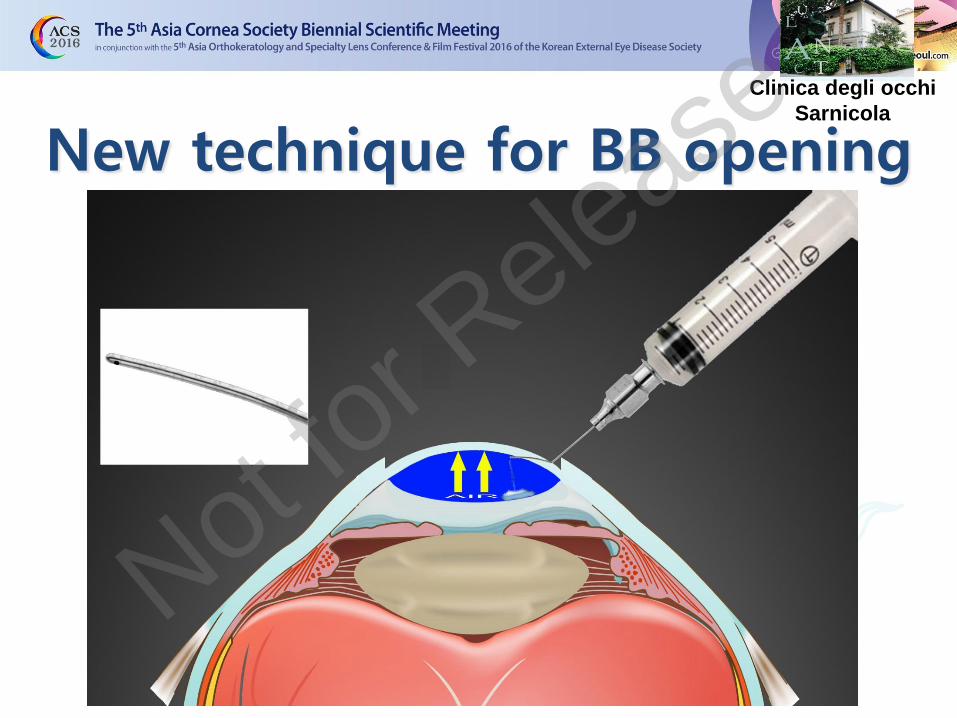
Clinica degli occhi
Sarnicola
New technique for BB opening
Not for R
elease
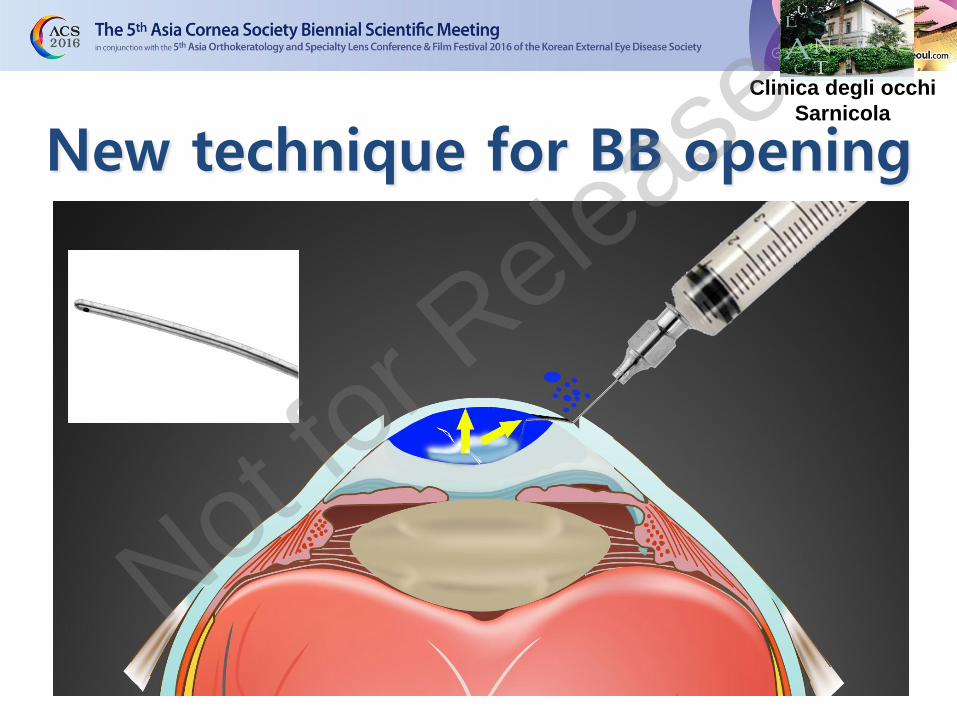
Clinica degli occhi
Sarnicola
New technique for BB opening
Not for R
elease

Clinica degli occhi
Sarnicola
New technique for BB opening
Not for R
elease

Clinica degli occhi
Sarnicola
New technique for BB opening
Not for R
elease
Clinica degli occhi
Sarnicola
New technique for BB opening
Not for R
elease
Clinica degli occhi
Sarnicola
New technique for BB opening
Not for R
elease

Clinica degli occhi
Sarnicola
New technique for BB opening
Not for R
elease

Clinica degli occhi
Sarnicola
New technique for BB opening
Not for R
elease
Standard Tecnique
3 Surgical Patterns
Cannula Big Bubble
Cannula Air-visco bubble
Layer by layer
dDALK
pdDALK
Clinica degli occhi
Sarnicola
Not for R
elease
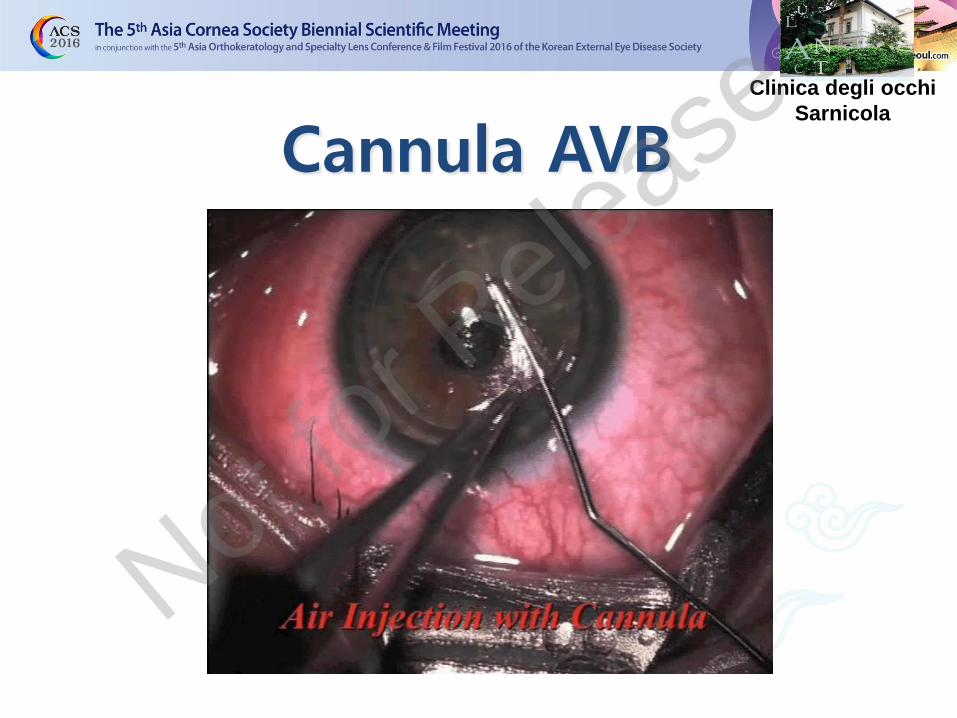
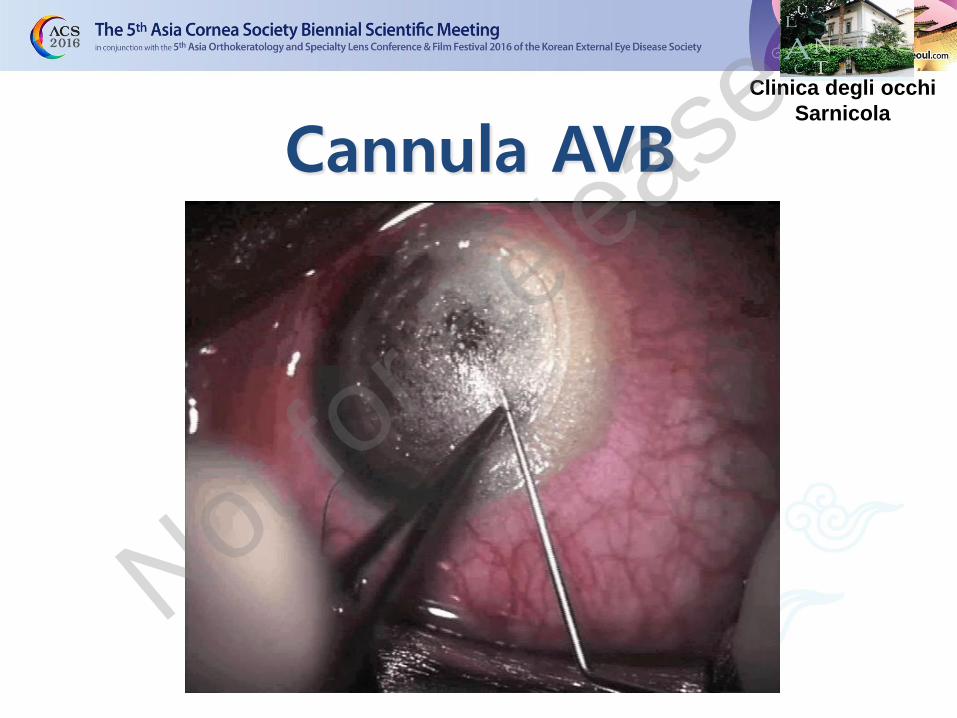
Cannula AVB Clinica degli occhi
Sarnicola
Not for R
elease
Cannula AVB Clinica degli occhi
Sarnicola
Not for R
elease
Standard Tecnique
3 Surgical Patterns
Cannula Big Bubble
Cannula Air-visco bubble
Layer by layer
dDALK
pdDALK
Clinica degli occhi
Sarnicola
Not for R
elease
pdDALK Clinica degli occhi
Sarnicola
Not for R
elease

1.- DALK in EXTREME ECTASIA
2.- DALK in INFECTIONS
3.- DALK in CORNEAL PENETRATING WOUNDS
4.- DALK in OCULAR SURFACE DISEASES
DALK OTHER INDICATIONS
• Keratoglobus
• Scar • Active infections
Not for R
elease
Related Documents