Indian Kidney Exchange Program: A Game Theoretic Perspective Arghya Bandyopadhyay * and Sajal Mukhopadhyay † December 7, 2021 Abstract We propose a ways in which Kidney exchange can be feasibly, economically and efficiently implemented in Indian medical space, named as Indian Kidney Ex- change Program(IKEP) along with Indian specific in- fluences on compatibility and final outcomes. Kidney exchange is a boon for those suffering from renal kid- ney failure and do have a donor with an incompatible kidney (compatible kidney also encouraged for better matches). In such situations the patient, donor pair is matched to another patient, donor pair having the same problem and are compatible to each other. Hos- pitals put up their patient-donor data. Using the bio- logical data, compatibility scores(or weights) are gen- erated and preferences are formed accordingly. Indian influences on weights, modify the compatibility scores generated and hence, the preferences. The pairs are then allocated using game theoretic matching algo- rithms for markets without money. Keywords: Kidney exchange, kidney paired donation, donor-recipient pair, living donor kidney transplant. * Department of Computer Science and Engineering, Na- tional Institute of Technology, Durgapur, West Bengal, India; Email:[email protected] † Department of Computer Science and Engineering, Na- tional Institute of Technology, Durgapur, West Bengal, India; Email:[email protected] 1 Introduction We hereby, propose a centralized, matching algo- rithm and a framework for a national kidney ex- change program in India, named as Indian kidney exchange program(IKEP) motivated from Singh N P et al. 2016[14] which discusses the challenges and future of kidney transplantation in India and states that kidney exchanges programs(KEPs) can be ben- eficial in Indian kidney transplantation market. Lec- ture 10 of Tim Roughgarden[20] provides a brief idea on kidney exchange paradigm and various mechanism designs deployed. 1.1 Overview The patients who are suffering from EKSD and have a donor 1 are supposed to see for the hospitals associ- ated with IKEP 2 . The patient will then report to the nearest hospital and get themselves enrolled into the IKEP pool of patient-donor pairs. After successful registration of patient-donor pair in IKEP program, preferences are generated based on the information provided by them (here, the patients and the donors, in realistic sense, are strategic in nature and hence, the generated preferences will be treated in strate- gic setting) and then, the patients and the donors are matched by a mechanism designed specifically for 1 The donor should be eligible to donate to the patient under the Indian act of Organ donation 1994. 2 We expect all the hospitals to get themselves associated to IKEP, which would help in getting a much more thicker pool. Page 1 of 30 arXiv:2112.02932v1 [cs.GT] 6 Dec 2021

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Indian Kidney Exchange Program: A GameTheoretic Perspective
Arghya Bandyopadhyay∗and Sajal Mukhopadhyay†
December 7, 2021
Abstract
We propose a ways in which Kidney exchange canbe feasibly, economically and efficiently implementedin Indian medical space, named as Indian Kidney Ex-change Program(IKEP) along with Indian specific in-fluences on compatibility and final outcomes. Kidneyexchange is a boon for those suffering from renal kid-ney failure and do have a donor with an incompatiblekidney (compatible kidney also encouraged for bettermatches). In such situations the patient, donor pairis matched to another patient, donor pair having thesame problem and are compatible to each other. Hos-pitals put up their patient-donor data. Using the bio-logical data, compatibility scores(or weights) are gen-erated and preferences are formed accordingly. Indianinfluences on weights, modify the compatibility scoresgenerated and hence, the preferences. The pairs arethen allocated using game theoretic matching algo-rithms for markets without money.
Keywords: Kidney exchange, kidney paireddonation, donor-recipient pair, living donorkidney transplant.
∗Department of Computer Science and Engineering, Na-tional Institute of Technology, Durgapur, West Bengal, India;Email:[email protected]
†Department of Computer Science and Engineering, Na-tional Institute of Technology, Durgapur, West Bengal, India;Email:[email protected]
1 Introduction
We hereby, propose a centralized, matching algo-rithm and a framework for a national kidney ex-change program in India, named as Indian kidneyexchange program(IKEP) motivated from SinghN P et al. 2016[14] which discusses the challenges andfuture of kidney transplantation in India and statesthat kidney exchanges programs(KEPs) can be ben-eficial in Indian kidney transplantation market. Lec-ture 10 of Tim Roughgarden[20] provides a brief ideaon kidney exchange paradigm and various mechanismdesigns deployed.
1.1 Overview
The patients who are suffering from EKSD and havea donor1 are supposed to see for the hospitals associ-ated with IKEP2. The patient will then report to thenearest hospital and get themselves enrolled into theIKEP pool of patient-donor pairs. After successfulregistration of patient-donor pair in IKEP program,preferences are generated based on the informationprovided by them (here, the patients and the donors,in realistic sense, are strategic in nature and hence,the generated preferences will be treated in strate-gic setting) and then, the patients and the donorsare matched by a mechanism designed specifically for
1The donor should be eligible to donate to the patient underthe Indian act of Organ donation 1994.
2We expect all the hospitals to get themselves associated toIKEP, which would help in getting a much more thicker pool.
Page 1 of 30
arX
iv:2
112.
0293
2v1
[cs
.GT
] 6
Dec
202
1

Indian Kidney Exchange Program: A Game Theoretic Perspective
markets without money (mechanism design withoutmoney is a subtopic of game theory[12]).
Hospital 1
Hospital 2
Can matchinternally?
Can matchinternally?
Based of severalfeatures of patientsand donors ,a centralrepository will bemaintained.
P1, D1
P2, D2
P19, D19
P20, D20
Pn, Dn
P1
P2
Pn
P3
P4
P5
P6
D1 D2 D3 D4 D5 D6 Dn
No
No
A large two dimen-sional matrix will becreated signifing com-patibility score.
Figure 1: Overview of IKEP
All the patients, along with their donors, approachthe respective hospitals for enrolling themselves inIKEP. Although not promoted3, the hospitals try tomatch pairs internally and enroll its remaining, un-matched pairs in IKEP. As soon as the pairs are en-rolled, a central repository is created based on severalfeatures of patients and donors as discussed in theSection 1.2. After that, the compatibility score4 of allthe patients with each and every donor participatingin the IKEP is calculated and stored in a n× n ma-trix. The calculations of compatibility scores/weightsare discussed in the Section 2.1. Fig. 1 describes theoverview of IKEP where Pi and Di denotes patientand donor respectively.
From the matrix generated, IKEP analyzes the topmost preference of the pairs on the donors. And thesepreferences are used to generate stable matches be-tween pairs and donors.
In the remaining parts of paper, Section 2 describesthe system model of IKEP and Section 3, present thealgorithmic implementation of the mechanism pro-posed. We then paint a picture of how indian in-fluences on weights(Societal acceptance score) affectsthe compatibility matrix generated to form a prefer-
3Because, more number of pairs in the IKEP will lead toincrease in the number of patients getting matched to theirpreferred donor.
4Compatibility scores and weights are used interchangeablythroughout this paper.
ence list in Section 4.In Section 5, we describe the way in which, the
preferences are made strict and non-ambiguous. Sec-tion 6 speaks about the way in which the cycles pro-posed by IKEP could be deployed in a distributedbut simultaneous manner. Section 7 states the limi-tations of IKEP and how they could be solved. Sec-tion 9 and Section 10 provides insights for future workand concludes the paper.
Appendix A gives an idea of the current situationof KEPs in India and things related to that. andAppendix B provides necessary background detailsabout kidney exchange and biological terms used inthis paper.
1.2 Prerequisites
Before enrolling a patient into the Indian kidney ex-change program, the hospitals are required to keepthe following details of the donor and patients re-spectively:
1. Age. The age of the donor matters[11], It hasbeen observed that patients getting a kidneyfrom an age group of 18-34 years has 62% of graftsurvival and 59% for kidneys from age group 35-49 and so on.5
2. Blood Group. (Ex: A, B, AB, O) It is collectedto decide ABO type compatibility discussed inAppendix B.4.
3. List of Human leukocyte antigens -A, -B,-DR antigens The list helps in calculating thecompatibility score of a patient from pair 1 withthe a donor from pair 2.
4. Kidney Size The size of kidney also plays a rolein increasing the survival of the patient after thegraft.
5. Panel Reactive Antibodies(PRA) percent-age. The PRA is crucial in deciding the waitingtime of a particular patient. The PRA points tothe level of sensitization of the patient. Patientswith higher PRA, face more difficulty in gettingmatched.
5Referred from National Kidney Registry USA.
Page 2 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
6. Pin code. If the pin-code is found same, it in-creases the acceptance and feasibility of the ex-change and reduces with increase in the distancebetween two pin-codes.
7. Has ever donated a kidney. This data willhelp in prioritizing the patients in the pool.
8. Societal preference. It is basically a rankedlist of acceptable societal distributions6, withmost preferred being the first element and leastpreferred being the last element. The societaldistributions, not present in the list are assumedunacceptable. If the societal preference is found∅, it is assumed that the patient is indifferent toall the kidneys present in the pool in terms ofsocietal distributions.
9. Societal distribution of donor. The societaldistribution of donor is noted down in order tocheck the acceptance of his/her kidney by anypatients according to their societal preference.
10. Distance from dialysis center. This parame-ter is used to allocate the marginal priority whichis used for breaking the ties described in Sec-tion 5.
11. Economic slab. The patient falling in lowereconomic slab are marginally prioritized over thehigher economic slabs.
1.3 Timeline
The timeline of IKEP basically consists three stepswhich will provide a clear picture of the entire pro-cess.
1.4 Submitting medical data
Hospitals submit their patient donor pair medical de-tails to enroll them as soon as the patients approachtheir hospitals.
6The term societal distribution is self explanatory. Everysociety is distributed by factors like, Religion, caste and creed.
1.5 Matching and exchange proposals
Matching Algorithm 1 is carried out after a particu-lar interval and exchange cycles are proposed to thehospitals for final verdicts.
1.6 Offer reviews and transplants
As soon as the matching cycles are proposed by thealgorithm, a cross match test is performed by the cen-tral testing center for IKEP and based of the resultsfinal matching results are presented to the concernedhospitals. The hospitals review the exchanges offered.On approval, the the next step of transplantation istaken, else the pairs remain in the exchange pool andget considered for next match.
2 System Model
We hereby, propose the system model of IKEP whichis a variant of Top-trading cycle used for House allo-cation problem by Shapley and Scarf et al. 1974 [21].Roth et al.(2004)[17] proposes that kidney exchangeproblem can be understood as a special case of houseallocation problem.
The basic idea was to replace the residents whohave preferences over houses available with the pa-tients, who have preferences over the kidneys avail-able. And patients point towards their most preferredkidney and it has been observed that, a cycle coulddefinitely be found(always). These cycles are markedout and removed from the graph.
After the removal of the patients participating inthe previous cycles, the remaining patients reassigntheir most preferred kidney over the remaining kid-neys and cycles are reformed and eliminated. It alsospeaks about the inclusion of chains and there for-mation at times when no cycles can be found. Butin India, Non directed donors(NDD) are prohibitedwhich in turn prohibits formation and carrying outchains.
The entire preference list is generated based on theIKEP Compatibility Graph. It is a weighted directedgraph(E,V,W). Let Vi, Vj ∈ V be two vertices, andwij ∈ W be the weight for the edge eij ∈ E from Vi
Page 3 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
to Vj representing how compatible7 is the donor of Vito the patient of Vj . wij = 0, means that donor of Vican’t donate to the patient of Vj .
Before every algorithm run, the weights are recal-culated and edges are redrawn to and from the pre-vious members to the new pair. It is assumed thatthe pair arrive consecutively.
2.1 Weight calculation.
IKEP calculate the weights(wij) on the basis ofHLA matching score(hij), PRA percentage, Bloodgroup(bij) and some others. The following are thegeneral influences on the weights. Section 4 state theinfluences on the weights in Indian perspective.
2.1.1 Age score(aij)
Age score is the measurement of age based compati-bility of donor of node i and patient of node j. Sincethe improvement of graft survival rate and quality islinear with the reduction in age difference, the calcu-lation of weight need to be linear too.
Aged ← Agei −Agej (1)
Where, Aged, Agei and Agej are difference in ages,age of the donor of node i and age of the patient ofnode j respectively.
aij ←
Va, if Aged < 0
Va − αa ×Aged, if Aged ≤ Da
0, otherwise
(2)
Where Va is the maximum value generated byEq. (2) and αa ∈ (0, 1) such that, the increase inAged linearly generates aij ∈ [0, Va]. Da is a limitto the age difference, beyond which the age score be-comes 0.
We take Va to be 6, αa to be 0.15 and Da to be40. The Eq. (2) has been inspired by from UtkarshVerma et al. 2020[24].
7the rate of graft survival of the transplantation.
2.1.2 ABO score(bij)
ABO score is the measurement of Blood group typecompatibility of donor of node i and patient of nodej.
bij ←
{Vb, if compatible(Bi, Bj)
0, otherwise(3)
Where Vb is the maximum value that could be as-signed to bij in Eq. (3). Vb ∈ (0,∞). We take Vb as6.
2.1.3 HLA score(hij)
HLA score depends on the cardinality of humanleukocyte antibodies matches8 among the donor ofthe node i and patient of the node j. Basu et al.2008[4] states the benefits of considering HLAs inmatching of Kidneys. It speaks about how HLA mis-match calculations can lead to better graft survival.
mij ← Hi ∩Hj (4)
where Hi and Hj is the set of human leukocyteantibodies of the donor of node i and the patient ofnode j respectively. And, mij is the set of matchedantibodies.
hij ← |mij | (5)
H∗ is the number of HLAs being recorded at thetime of data input. In this paper, we consider thelength of HLA to be 6. Larger the H∗, larger is willbe the distribution of weights and the preferences willbe more strict.
2.1.4 Kidney size score(kij)
Kidney score is the measurement of Kidney size com-patibility of donor of node i and patient of node j.
Kd ← Ki −Kj (6)
8Here, 2 entries each of 3 human leukocyte antibodies typesare taken into consideration for the weight calculation andscoring, namely - HLA -A, -B, -DR antigens.
Page 4 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
Where, Kd, Ki and Kj are difference in kidneysizes, kidney size of the donor of node i and kidneysize of the patient of node j respectively.
kij ←
{Vk −Kd, if Kd ≤ Dk
0, otherwise(7)
Where Vk, is the maximum value generated byEq. (7) which is reduced by Kd. Dk is the differ-ence in the kidney sizes, beyond which kidney scorereduces to zero. We take Vk as 6 and Dk as 3.
2.1.5 Pincode score(pij)
Pincode score is a measure of the logistical compat-ibility. In the pincodes, the first digit signify zones,the second digit signify sub-zones. Although not ofmuch significance, is calculated by the Algorithm 11.
pij ← pinScore(Pini, P inj) (8)
where, Pini and Pinj be the pincode of node i andj respectively.
2.1.6 General Perspective Weight(gwij)
General perspective weight is the summation of allthe above mentioned scores. This, for edge eij iscalculated as:
gwij ← hij + bij + kij + aij + pij (9)
The values of the constants Va, Vb, Vk, H∗ andVp should be kept identical in order to give equalsignificance to all the scores. And to assign differentpriorities to the scores, the values assigned to theconstants need to be altered accordingly9.
The best way to select an identical value for theconstants is to decide the number of HLAs to be con-sidered for matching i.e. H∗. When decided, set thevalue of Va, Vb, Vk and Vp to H∗. And eventually theother depending constants.
9The constants with greater values than the remaining ones,would eventually become more significant in compatibility cal-culation.
3 Proposed Algorithm
The Algorithm 1 is the main/core of IKEP allocationsystem which returns the list of exchanges proposedby the algorithm. A loop runs until and unless all thevertices10 are removed or no more cycles can be de-rived from the remaining vertices and their respectivepreferences. In the loop, firstly it generates the com-patibility graph using the Algorithm 2. After thata queue is formed from the participating vertices forthe particular iteration.
Algorithm 1 IKEPA
1: procedure IKEPA(V,A,R) . Generates cyclesfor IKEP Exchanges
2: initialize C ← new ArrayList <> ()3: while V 6= null do . End, if no vertices left4: W ←GenCompatibilityMatrix(V )5: Q←ArrayToQueue(V )6: c←FindCycle(W,V.size,Q)7: if c 6= null then8: RemoveCycle(C, V,W )9: C.add(c)
10: else11: Break12: end if13: end while14: return C . List of cycles15: end procedure
Algorithm 14 assigns a priority based on the fac-tors discussed at the starting of each algorithm run.It takes one argument, the set of vertices in thepair. If isInitial member variable of any vertex istrue, the Algorithm 14 sets the value of waiting timescore(WTScore) to zero, add all other scores to cal-culate priority and set isInitial to false. However, ifisInitial is false, WTScore is incremented by a unitand then the priority is recalculated.
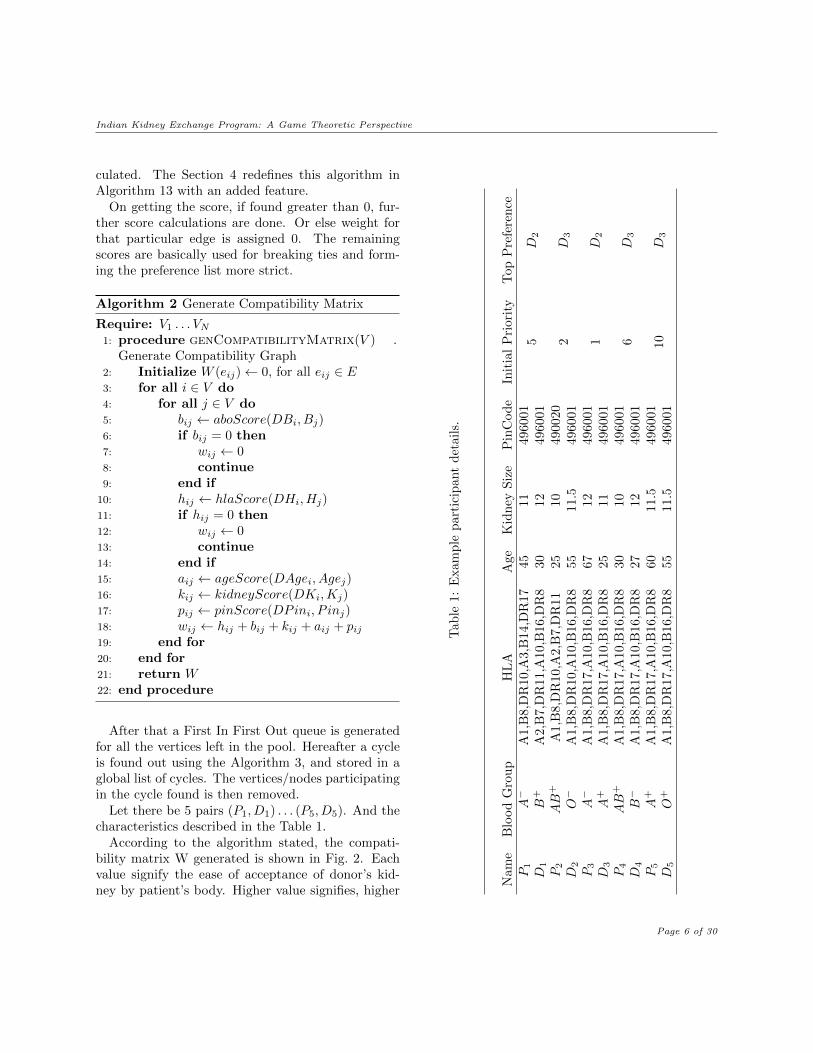
The Algorithm 2 is responsible for generating thecompatibility matrix as stated earlier. For everynode, it determines the blood group compatibilityand if found compatible, HLA compatibility is cal-
10The Vertex class is defined in the Appendix C.
Page 5 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
culated. The Section 4 redefines this algorithm inAlgorithm 13 with an added feature.
On getting the score, if found greater than 0, fur-ther score calculations are done. Or else weight forthat particular edge is assigned 0. The remainingscores are basically used for breaking ties and form-ing the preference list more strict.
Algorithm 2 Generate Compatibility Matrix
Require: V1 . . . VN1: procedure genCompatibilityMatrix(V ) .
Generate Compatibility Graph2: Initialize W (eij)← 0, for all eij ∈ E3: for all i ∈ V do4: for all j ∈ V do5: bij ← aboScore(DBi, Bj)6: if bij = 0 then7: wij ← 08: continue9: end if
10: hij ← hlaScore(DHi, Hj)11: if hij = 0 then12: wij ← 013: continue14: end if15: aij ← ageScore(DAgei, Agej)16: kij ← kidneyScore(DKi,Kj)17: pij ← pinScore(DPini, P inj)18: wij ← hij + bij + kij + aij + pij19: end for20: end for21: return W22: end procedure
After that a First In First Out queue is generatedfor all the vertices left in the pool. Hereafter a cycleis found out using the Algorithm 3, and stored in aglobal list of cycles. The vertices/nodes participatingin the cycle found is then removed.
Let there be 5 pairs (P1, D1) . . . (P5, D5). And thecharacteristics described in the Table 1.
According to the algorithm stated, the compati-bility matrix W generated is shown in Fig. 2. Eachvalue signify the ease of acceptance of donor’s kid-ney by patient’s body. Higher value signifies, higher
Tab
le1:
Exam
ple
part
icip
ant
det
ail
s.
Nam
eB
lood
Gro
up
HL
AA
ge
Kid
ney
Siz
eP
inC
od
eIn
itia
lP
riori
tyT
op
Pre
fere
nce
P1
A−
A1,
B8,
DR
10,A
3,B
14,D
R17
45
11
496001
5D
2D
1B
+A
2,B
7,D
R11,A
10,B
16,D
R8
30
12
496001
P2
AB
+A
1,B
8,D
R10,A
2,B
7,D
R11
25
10
490020
2D
3D
2O−
A1,
B8,
DR
10,A
10,B
16,D
R8
55
11.5
496001
P3
A−
A1,
B8,
DR
17,A
10,B
16,D
R8
67
12
496001
1D
2D
3A
+A
1,B
8,D
R17,A
10,B
16,D
R8
25
11
496001
P4
AB
+A
1,B
8,D
R17,A
10,B
16,D
R8
30
10
496001
6D
3D
4B−
A1,
B8,
DR
17,A
10,B
16,D
R8
27
12
496001
P5
A+
A1,
B8,
DR
17,A
10,B
16,D
R8
60
11.5
496001
10
D3
D5
O+
A1,
B8,
DR
17,A
10,B
16,D
R8
55
11.5
496001
Page 6 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
acceptance.
P1
P2
P3
P4
P5
D1 D2 D3 D4 D5
0 25 0 0 0
22 19 23 22 18
0 29 0 0 0
2528292425
0 29 30 0 30
Figure 2: Compatibility Matrix
The graph representation of the compatibility ma-trix is shown in Fig. 3
P1, D1
P2, D2
P3, D3
P5, D5P4, D4
Figure 3: Compatibility Graph
Let us assume the priorities11 assigned to the pa-tients be as described in the Table 1. And the toppreferences are derived from the compatibility ma-trix.
The Graph class defined in Algorithm 15, has mem-ber variables n and adj holds the number of nodes inthe graph and the list of adjacent nodes respectively.The member method addEdge adds directed edgesfrom source node i to destination node j. The con-structor initializes the graph by taking the number ofnodes and initialize the list of adjacent nodes.
11It is actually assigned and modified with time according tovarious time dependent characteristics like results of previousalgorithm runs, ease to match a pair and many others describedin Section 5
Algorithm 3 Find Cycles
1: procedure findCycle(W,S,Q, V ) . Finds outthe cycle including the top prioritized patients.
2: g ←genGraphMaxRowVal(W,S, V )3: while Q.isNotEmpty() do4: v ← Q.poll()5: c←dfsCycle(g, v)6: if c 6= null then7: return c . proposed cycle8: end if9: end while
10: return null . no cycles possible11: end procedure
IKEP finds the cycles with the help of adjacencymatrix that is being passed to the algorithm. The cellwith the highest value assigned in a particular rowis considered as the most preferred kidney for thatparticular patient. In case of a tie, the tie breakingis done using priorities assigned to the patients asdescribed in Section 5. The tie breaking algorithm isinculcated in the max function.
The cycles are formed using Algorithm 5 which isa modified version of DFS algorithm.
Algorithm 4 Generate Graph Using Max Row Value
1: procedure genGraphMaxRowVal(W,S, V ).Generates graph based on highest prioritized kid-ney for a patient.
2: initialize G←new Graph(S)3: for all wi ∈W do . wi is ith row in
adjacency matrix4: i, j ←max(w) . if max is non-distinct,
use pair priority to break ties.5: if max(w) > F ∗ then6: G.addEdge(i, V [j])7: else8: G.addEdge(i, null)9: end if
10: end for11: return G . graph with max row values12: end procedure
F* is the filter constant which removes the edges
Page 7 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
having weights less than itself. IKEP adds all thevertices it comes across, in to a hash-set and keepson checking if the node is repeated. As soon as arepeated node is found, it signifies a cycle. Hence thehash-set is converted into a list and returned back.
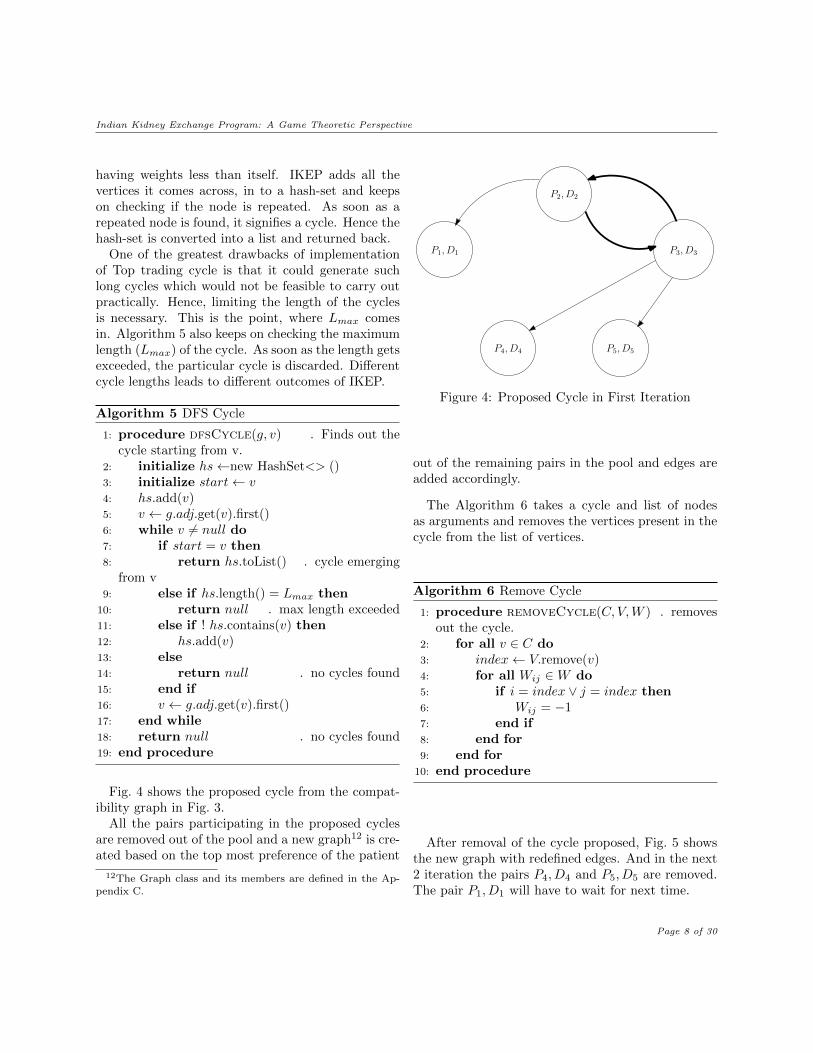
One of the greatest drawbacks of implementationof Top trading cycle is that it could generate suchlong cycles which would not be feasible to carry outpractically. Hence, limiting the length of the cyclesis necessary. This is the point, where Lmax comesin. Algorithm 5 also keeps on checking the maximumlength (Lmax) of the cycle. As soon as the length getsexceeded, the particular cycle is discarded. Differentcycle lengths leads to different outcomes of IKEP.
Algorithm 5 DFS Cycle
1: procedure dfsCycle(g, v) . Finds out thecycle starting from v.
2: initialize hs←new HashSet<> ()3: initialize start← v4: hs.add(v)5: v ← g.adj.get(v).first()6: while v 6= null do7: if start = v then8: return hs.toList() . cycle emerging
from v9: else if hs.length() = Lmax then
10: return null . max length exceeded11: else if ! hs.contains(v) then12: hs.add(v)13: else14: return null . no cycles found15: end if16: v ← g.adj.get(v).first()17: end while18: return null . no cycles found19: end procedure
Fig. 4 shows the proposed cycle from the compat-ibility graph in Fig. 3.
All the pairs participating in the proposed cyclesare removed out of the pool and a new graph12 is cre-ated based on the top most preference of the patient
12The Graph class and its members are defined in the Ap-pendix C.
P1, D1
P2, D2
P3, D3
P5, D5P4, D4
Figure 4: Proposed Cycle in First Iteration
out of the remaining pairs in the pool and edges areadded accordingly.
The Algorithm 6 takes a cycle and list of nodesas arguments and removes the vertices present in thecycle from the list of vertices.
Algorithm 6 Remove Cycle
1: procedure removeCycle(C, V,W ) . removesout the cycle.
2: for all v ∈ C do3: index← V.remove(v)4: for all Wij ∈W do5: if i = index ∨ j = index then6: Wij = −17: end if8: end for9: end for
10: end procedure
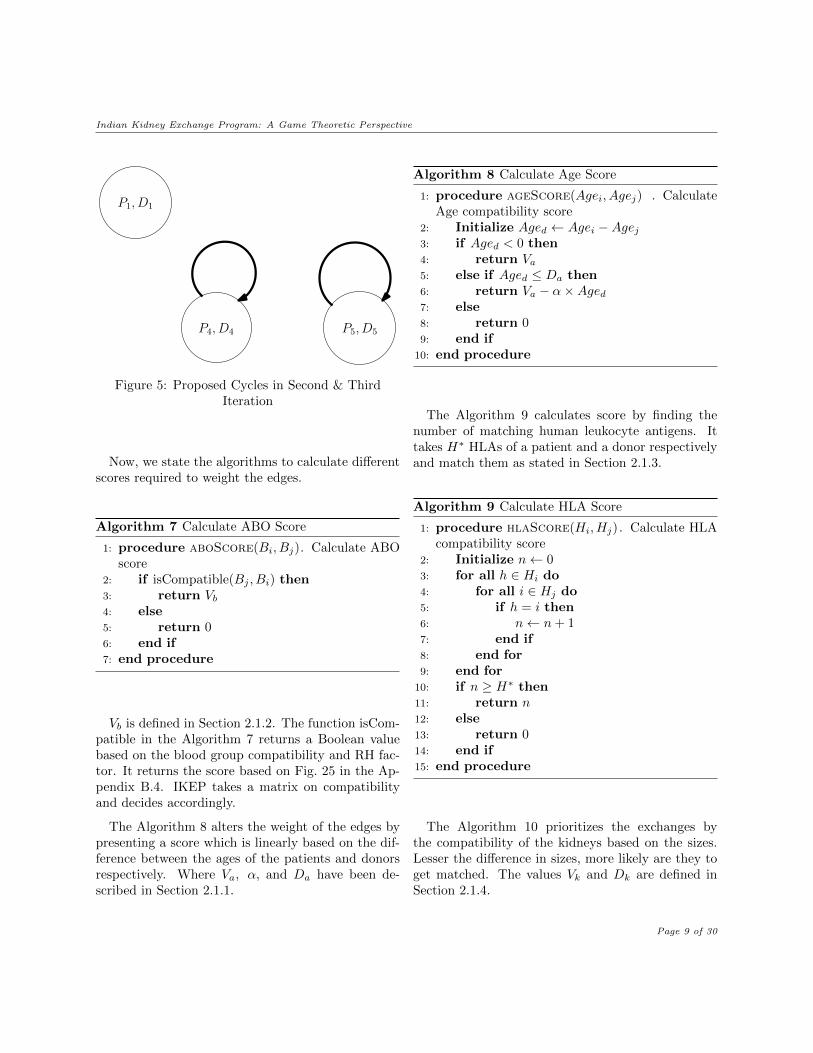
After removal of the cycle proposed, Fig. 5 showsthe new graph with redefined edges. And in the next2 iteration the pairs P4, D4 and P5, D5 are removed.The pair P1, D1 will have to wait for next time.
Page 8 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
P1, D1
P5, D5P4, D4
Figure 5: Proposed Cycles in Second & ThirdIteration
Now, we state the algorithms to calculate differentscores required to weight the edges.
Algorithm 7 Calculate ABO Score
1: procedure aboScore(Bi, Bj). Calculate ABOscore
2: if isCompatible(Bj , Bi) then3: return Vb4: else5: return 06: end if7: end procedure
Vb is defined in Section 2.1.2. The function isCom-patible in the Algorithm 7 returns a Boolean valuebased on the blood group compatibility and RH fac-tor. It returns the score based on Fig. 25 in the Ap-pendix B.4. IKEP takes a matrix on compatibilityand decides accordingly.
The Algorithm 8 alters the weight of the edges bypresenting a score which is linearly based on the dif-ference between the ages of the patients and donorsrespectively. Where Va, α, and Da have been de-scribed in Section 2.1.1.
Algorithm 8 Calculate Age Score
1: procedure ageScore(Agei, Agej) . CalculateAge compatibility score
2: Initialize Aged ← Agei −Agej3: if Aged < 0 then4: return Va5: else if Aged ≤ Da then6: return Va − α×Aged7: else8: return 09: end if
10: end procedure
The Algorithm 9 calculates score by finding thenumber of matching human leukocyte antigens. Ittakes H∗ HLAs of a patient and a donor respectivelyand match them as stated in Section 2.1.3.
Algorithm 9 Calculate HLA Score
1: procedure hlaScore(Hi, Hj). Calculate HLAcompatibility score
2: Initialize n← 03: for all h ∈ Hi do4: for all i ∈ Hj do5: if h = i then6: n← n+ 17: end if8: end for9: end for
10: if n ≥ H∗ then11: return n12: else13: return 014: end if15: end procedure
The Algorithm 10 prioritizes the exchanges bythe compatibility of the kidneys based on the sizes.Lesser the difference in sizes, more likely are they toget matched. The values Vk and Dk are defined inSection 2.1.4.
Page 9 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
Algorithm 10 Calculate Kidney Score
1: procedure kidneyScore(Ki,Kj) . CalculateKidney compatibility score
2: Initialize Kd ← |Ki −Kj |3: if Kd ≤ Dk then4: return Vk −Kd
5: else6: return 07: end if8: end procedure
The Algorithm 11 prioritizes the exchanges by theease of logistical feasibility of the exchanges. Lesserthe distance between the pairs, more likely are theyto get matched.
Algorithm 11 Calculate Pincode Score
1: procedure pinCode(Pini, P inj) . CalculatePincode compatibility score
2: if Pini=Pinj then3: return Vp4: else if city(Pini)=city(Pinj) then5: return Vp −Dp
6: else if subzone(Pini)=subzone(Pinj) then7: return Vp − αp1 ×Dp
8: else if zone(Pini)=zone(Pinj) then9: return Vp − αp2 ×Dp
10: else11: return 012: end if13: end procedure
Where Vp is the maximum value Algorithm 11 canreturn and Dp is the rate at which pinScore is dete-riorated in successive if statements. Dp is multipliedby αp1 ∈ (1,∞) in order to regulate the rate of dete-rioration, when sub-zones are identical. Similarly Dp
is multiplied by αp2 ∈ (αp1,∞) in order to regulatethe rate of deterioration, when zones are identical.We take Vp as 6, Dp as 1, αp1 as 2 and αp2 as 3.
4 Indian Influences On Weights
The compatibility scores/weights generated in Sec-tion 2.1 are biologically driven and do portray theideal preferences on kidneys. But in India, Societaldistribution compatibility act as a significant In-dian influence on weights. In this section, we mecha-nise an algorithm to take it into account and modifythe preferences previously generated and redefine Al-gorithm 2.
In India, religion, caste and other forms of diversityplays a significant role in Indian healthcare system.Roger P Worthington et al. 2011[29] describes, howIndian medicare and healthcare systems are being in-fluenced and effected by the religious and cultural as-pects. India is culturally and societally highly diversein nature. These poses a huge challenge in forming anationalized kidney exchange paradigm in India.
Let patient Pi belong to a societal distribution13
represented by sdi and let patient Pj belong to sdj .Where, sdi 6= sdj and sdi, sdj ∈ SD. Where, SDis the set of nsd societal distribution prevailing in asociety such that,
SD ← {sd1, sd2, . . . sdnsd}
Let us assume, that there is a prevailing hate orsocietal discrimination for sdj from sdi. There couldbe an incidence where Pi denies kidney from Dj andturns down the offer.
In order to solve this problem, we ask for accept-able communities from patients in the initial stagesof IKEP.
Societal acceptance score(sasij) is the mea-surement of the societal acceptance of donor’s kidneyby the patient. It is calculated by the Eq. (10).
sasij ←
1, if sPrefj = ∅1
k, if sdi ∈ sPrefj
1
k∗, otherwise
(10)
Where, k is index of donor’s societal distributionin patient’s preference list. And k∗ is any numberwhich is greater than nsd.
13Societal distributions in terms of religious, caste, creed andany other form of diversity.
Page 10 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
The Algorithm 12 implements SAS calculation. Itchecks the length of preference list. If found 0, it re-turns 1 or else, it traverses through the preference listof the patient. The element at index k of the prefer-ence list which matches with the societal distributionof donor is returned as 1
k . In case the donor’s societaldistribution doesn’t exist in the preference list14, thevalue returned 1
k∗ .
Algorithm 12 Calculate Societal Acceptance Score
1: procedure sas(sdi, sPrefj) . Calculate societalacceptance score
2: Initialize k ← 13: if sPrefj .length()= 0 then4: return 15: else6: for all s ∈ sPrefj do7: if s = sd′i then8: return 1
k9: end if
10: k ← k + 111: end for12: return 1
k∗
13: end if14: end procedure
The value returned by the Algorithm 12 is multi-plied with the general perspective weight calculatedin Eq. (9).
The final weight of edge eij is calculated as:
wij ← gwij × sasij (11)
For example, let a patient P1 has sPref1 ←[sd3, sd1] and a donor D3 belonging to a societaldistribution sd1. Let the general perspective weightw31 ← 30. Since the index of societal distribution ofD3 in the societal preference of patient sPref1 is 2,the sas31 ← 1
2 . Hence, the final weight w31 ← 30× 12 ,
i.e, 15.The Algorithm 13 shows, how the final weight is
been calculated. The Algorithm 13 needs to replaceAlgorithm 2 stated in Section 3.
14It is assumed that, if any patient has a set of preferences,∀sd ∈ SD−sPrefj is unacceptable for that particular patient.
IKEP at the time of edge selection in Algorithm 4,checks wij to be greater than F ∗. Here F ∗ is thefiltering constant to remove ”not up to the mark”edges. The not up to the mark value is dependentupon the thickness of the patients. In situations withscarce participants, F ∗ will go down and vice-versafor a surplus in participants.
Algorithm 13 Final Generate Compatibility Matrix
Require: V1 . . . VN1: procedure genCompatibilityMatrix(V ) .
Generate Compatibility Graph2: Initialize W (eij)← 0, for all eij ∈ E3: for all i ∈ V do4: for all j ∈ V do5: bij ← aboScore(DBi, Bj)6: if bij = 0 then7: wij ← 08: continue9: end if
10: hij ← hlaScore(DHi, Hj)11: if hij = 0 then12: wij ← 013: continue14: end if15: aij ← ageScore(DAgei, Agej)16: kij ← kidneyScore(DKi,Kj)17: pij ← pinScore(DPini, P inj)18: gwij ← hij + bij + kij + aij + pij19: sasij ← sas(Dsdi, sPrefj)20: wij ← gwij × sasij21: end for22: end for23: return W24: end procedure
Let there be 3 societal distributions prevailing inIndia.
SDInd ← {sd1, sd2, . . . sd3}
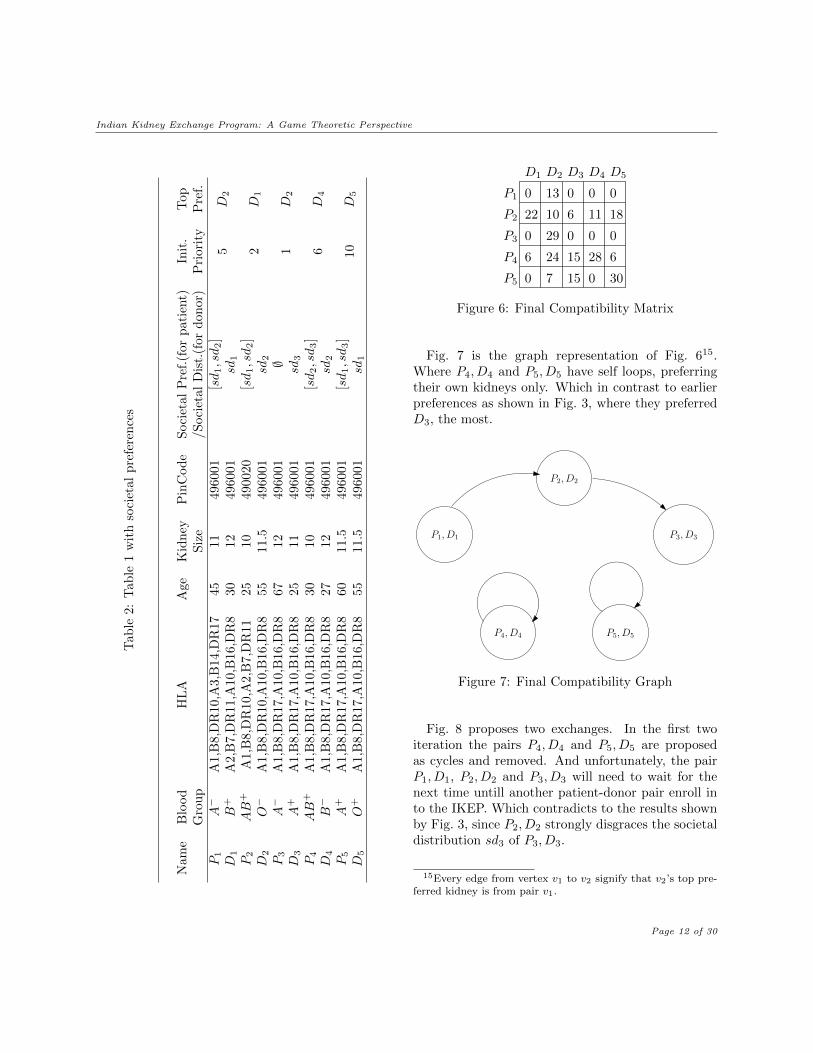
Let the Table 2 be the extended version of Table 1with added patients’ societal preferences and societaldistribution of donors. Fig. 6 is the modified compat-ibility matrix of Fig. 3 with final weights calculatedby Eq. (11).
Page 11 of 30
Indian Kidney Exchange Program: A Game Theoretic PerspectiveT
able
2:T
able
1w
ith
soci
etal
pre
fere
nce
s
Nam
eB
lood
HL
AA
geK
idn
eyP
inC
od
eS
oci
etal
Pre
f.(f
or
pati
ent)
Init
.T
op
Gro
up
Siz
e/S
oci
etal
Dis
t.(f
or
don
or)
Pri
ori
tyP
ref.
P1
A−
A1,
B8,
DR
10,A
3,B
14,D
R17
4511
4960
01[sd1,sd2]
5D
2D
1B
+A
2,B
7,D
R11
,A10
,B16
,DR
830
1249
6001
sd1
P2
AB
+A
1,B
8,D
R10
,A2,
B7,
DR
1125
1049
0020
[sd1,sd2]
2D
1D
2O−
A1,
B8,
DR
10,A
10,B
16,D
R8
5511
.549
6001
sd2
P3
A−
A1,
B8,
DR
17,A
10,B
16,D
R8
6712
4960
01∅
1D
2D
3A
+A
1,B
8,D
R17
,A10
,B16
,DR
825
1149
6001
sd3
P4
AB
+A
1,B
8,D
R17
,A10
,B16
,DR
830
1049
6001
[sd2,sd3]
6D
4D
4B−
A1,
B8,
DR
17,A
10,B
16,D
R8
2712
4960
01sd
2
P5
A+
A1,
B8,
DR
17,A
10,B
16,D
R8
6011
.549
6001
[sd1,sd3]
10
D5
D5
O+
A1,
B8,
DR
17,A
10,B
16,D
R8
5511
.549
6001
sd1
P1
P2
P3
P4
P5
D1 D2 D3 D4 D5
0 13 0 0 0
22 10 6 11 18
0 29 0 0 0
62815246
0 7 15 0 30
Figure 6: Final Compatibility Matrix
Fig. 7 is the graph representation of Fig. 615.Where P4, D4 and P5, D5 have self loops, preferringtheir own kidneys only. Which in contrast to earlierpreferences as shown in Fig. 3, where they preferredD3, the most.
P1, D1
P2, D2
P3, D3
P5, D5P4, D4
Figure 7: Final Compatibility Graph
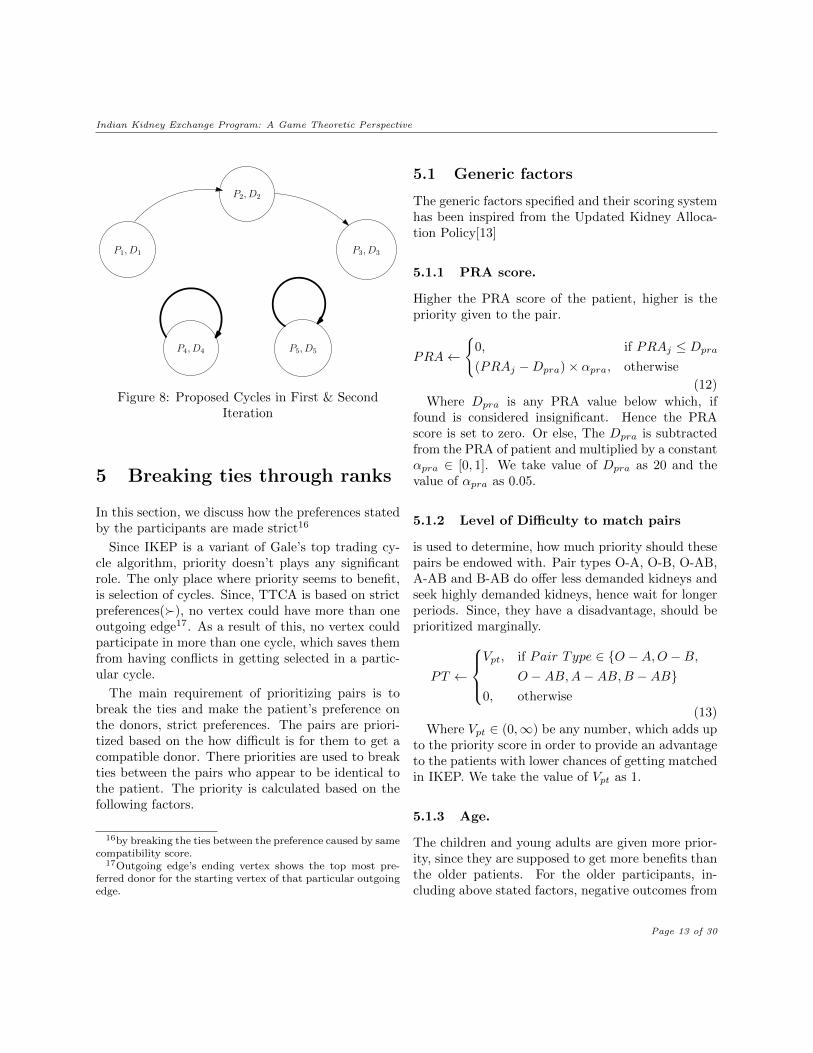
Fig. 8 proposes two exchanges. In the first twoiteration the pairs P4, D4 and P5, D5 are proposedas cycles and removed. And unfortunately, the pairP1, D1, P2, D2 and P3, D3 will need to wait for thenext time untill another patient-donor pair enroll into the IKEP. Which contradicts to the results shownby Fig. 3, since P2, D2 strongly disgraces the societaldistribution sd3 of P3, D3.
15Every edge from vertex v1 to v2 signify that v2’s top pre-ferred kidney is from pair v1.
Page 12 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
P1, D1
P2, D2
P3, D3
P5, D5P4, D4
Figure 8: Proposed Cycles in First & SecondIteration
5 Breaking ties through ranks
In this section, we discuss how the preferences statedby the participants are made strict16
Since IKEP is a variant of Gale’s top trading cy-cle algorithm, priority doesn’t plays any significantrole. The only place where priority seems to benefit,is selection of cycles. Since, TTCA is based on strictpreferences(�), no vertex could have more than oneoutgoing edge17. As a result of this, no vertex couldparticipate in more than one cycle, which saves themfrom having conflicts in getting selected in a partic-ular cycle.
The main requirement of prioritizing pairs is tobreak the ties and make the patient’s preference onthe donors, strict preferences. The pairs are priori-tized based on the how difficult is for them to get acompatible donor. There priorities are used to breakties between the pairs who appear to be identical tothe patient. The priority is calculated based on thefollowing factors.
16by breaking the ties between the preference caused by samecompatibility score.
17Outgoing edge’s ending vertex shows the top most pre-ferred donor for the starting vertex of that particular outgoingedge.
5.1 Generic factors
The generic factors specified and their scoring systemhas been inspired from the Updated Kidney Alloca-tion Policy[13]
5.1.1 PRA score.
Higher the PRA score of the patient, higher is thepriority given to the pair.
PRA←
{0, if PRAj ≤ Dpra
(PRAj −Dpra)× αpra, otherwise
(12)
Where Dpra is any PRA value below which, iffound is considered insignificant. Hence the PRAscore is set to zero. Or else, The Dpra is subtractedfrom the PRA of patient and multiplied by a constantαpra ∈ [0, 1]. We take value of Dpra as 20 and thevalue of αpra as 0.05.
5.1.2 Level of Difficulty to match pairs
is used to determine, how much priority should thesepairs be endowed with. Pair types O-A, O-B, O-AB,A-AB and B-AB do offer less demanded kidneys andseek highly demanded kidneys, hence wait for longerperiods. Since, they have a disadvantage, should beprioritized marginally.
PT ←
Vpt, if Pair Type ∈ {O −A,O −B,
O −AB,A−AB,B −AB}0, otherwise
(13)
Where Vpt ∈ (0,∞) be any number, which adds upto the priority score in order to provide an advantageto the patients with lower chances of getting matchedin IKEP. We take the value of Vpt as 1.
5.1.3 Age.
The children and young adults are given more prior-ity, since they are supposed to get more benefits thanthe older patients. For the older participants, in-cluding above stated factors, negative outcomes from
Page 13 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
previous algorithm runs and the patient who was pre-viously a donor are some of the significant factors forprioritization.
Age←
{Vap − αap ×Dap, if Agej ∈ ListAge
0, otherwise
(14)Where Vap is the upper limit of Age priority score.ListAge is the list of Age groups. Dap be the indexof Age group in which Agej lies in.αap is the regulator of the decrease in the value of
Age priority score with the increase in the index ofthe age group in which Agej lies in, such that.
αap ∈ (0,Vap
ListAge.length())
We assume the value of Vap as 3 and αap as 1. Thelist of age groups taken is ListAge ← [< 6, < 12,< 18].
5.1.4 Waiting Time.
Time is expensive, hence need to be used to prioritizepatients. Higher the waiting time of patient, higher isthe priority. For every algorithm run with negativeresult, there will be an increase in priority by Vwt
units. The initial waiting time priority for new par-ticipants will be zero. Although, a provision shouldbe made for those who have been in the waiting listfor deceased kidney in order to unify the two models.We take value Vwt as 1.
5.1.5 Is undergoing temporary vascular ac-cess
There are two situations prevailing among the pa-tients already undergoing hemodialysis.
Situation 1: One, who has failed on all AV Fistulasites.
Situation 2: One, who has failed AV Graft afterfailing all AV Fistula sites.
V A←
Vvap, if Situation 2 applies
Vvap1, if Situation 1 applies
0, otherwise
(15)
Where, Vvap, Vvap1 be the scores assigned to VApriority score according to the conditions they fulfilsuch that, Vvap ≥ Vvap1. We assume the values ofVvap and Vvap1 as 6 and 2 respectively.
5.1.6 Patient who was previously a donor
One who had been a donor and has now lost thesecond kidney needs to be prioritized.
IPD ←
{Vipd, if Patient was once a donor
0, otherwise(16)
Where Vipd ∈ (0,∞) is the maximum score allo-cated to the IPD priority. We take Vipd as 5.
5.2 IKEP specific factors:
The above stated factors are commonly used in kid-ney exchange/deceased kidney waiting list prioritiesfor the participants. There are some additional fac-tors, which will influence the scoring system for pri-oritizing the patients in IKEP.
5.2.1 Distance from dialysis center.
In India, a huge amount18 of population resides inrural distant villages with insignificant health caresystems and tedious transport system.
Dist←
{Vd − αd ×Dd, if Distj ∈ ListDist
0, otherwise(17)
Where Vd is the upper limit of distance priorityscore. ListDist is the list of distance ranges. Dd bethe index of distance group in which Distj lies in.αd is the regulator of the decrease in the value of
distance priority score with the increase in the indexof the distance group in whichDistj lies in, such that.
αd ∈ (0,Vd
ListDist.length())
18According to the census in 2001 , 72% of the Indian pop-ulation resided in urban areas.
Page 14 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
We assume the value of Vd as 3 and αd as 1. Thelist of age groups taken is ListDist ← [≥ 50, > 10 &< 50].
All the values presented are in kilometers.
5.2.2 Economic slab of the patient.
There is also an increasing economic gap in India.Rural people with limited income and lesser knowl-edge and availability of insurance and other aids, findit difficult to stay on dialysis. And hence need to beprioritized marginally.
Eco←
{Veco − αeco ×Deco, if Ecoj ∈ Listeco0, otherwise
(18)
Where Veco is the upper limit of economic priorityscore. Listeco is the list of economic slab. Deco bethe index of economic slab in which Ecoj lies in.
αeco is the regulator of the decrease in the value ofeconomic priority score with the increase in the indexof the economic slab in which Ecoj lies in, such that.
αeco ∈ (0,Veco
Listeco.length())
We assume the value of Veco as 4 and αeco as 1.The list of age groups taken is
ListEco ← [< 1, > 1 & < 5, > 5 & < 10, ≥ 10].
All the values presented are in Lakhs.
5.2.3 Priority Allocation
The initial priority Priorityv of the pair is calculatedwith the help of the following formula. And for thesubsequent calculations, we need to increment thevalue of Waiting time score(WTScore).
priorityij ← Age+PRA+PT+V A+IPD+Dist+Eco(19)
Algorithm 14 Assigns Priority
Require: V1 . . . VN1: procedure calculatePriority(V ) . Assigns
Priority2: for all v ∈ V do3: if isInitialv then4: WTScorev ← 05: isInitialv ← false6: else7: WTScorev ←WTScorev + Vwt
8: end if9: Priorityv ← Age + PRA + PT + V A +IPD +Dist+ Eco+WTScorev
10: end for11: return V12: end procedure
Where Vwt is the incrementor for wait time score.We take Vwt as 1.
5.3 Lexicographic VS IKEP Methodof Tie Breaking
In lexicographic tie breaking, the donors are eithersequenced based on the name of patients or based onfirst come first serve. And the one which is placedearlier among the pairs, who form a tie is selected asthe most preferred pair. The other way of tie break-ing has been described in Section 5.
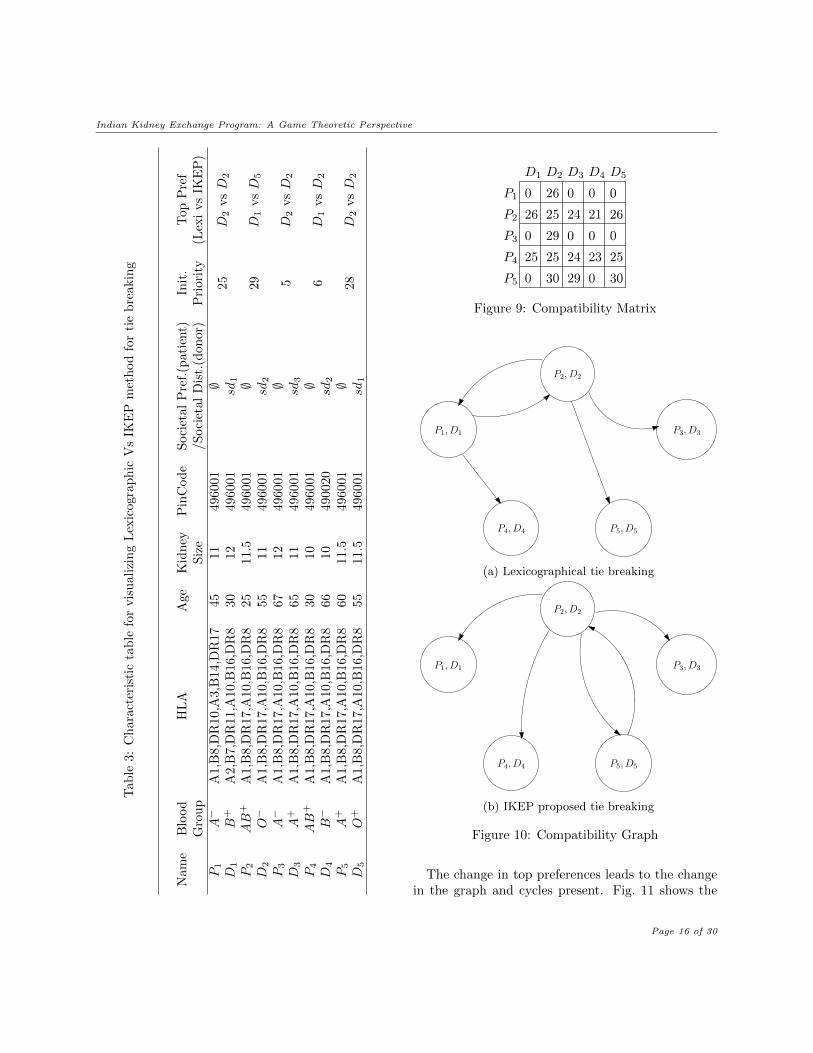
Let Table 3 be another characteristic table withinitial priorities as defined in the second last column.The last column describes the most preferred donorsusing lexicographic tie breaking versus IKEP statedtie breaking methodology.
Fig. 9 is the compatibility matrix, calculated forTable 3.
Fig. 10 is the graphical representation of Fig. 9.Fig. 10a is generated when the tie breaking methodused is lexicographic where as, Fig. 10b is generatedwhen tie breaking is done using priority as describedin Section 5.
Page 15 of 30
Indian Kidney Exchange Program: A Game Theoretic PerspectiveT
able
3:C
har
acte
rist
icta
ble
for
vis
ual
izin
gL
exic
ogra
ph
icV
sIK
EP
met
hod
for
tie
bre
akin
g
Nam
eB
lood
HL
AA
geK
idney
Pin
Cod
eS
oci
etal
Pre
f.(p
ati
ent)
Init
.T
op
Pre
fG
rou
pS
ize
/S
oci
etal
Dis
t.(d
on
or)
Pri
ori
ty(L
exi
vs
IKE
P)
P1
A−
A1,
B8,
DR
10,A
3,B
14,D
R17
4511
4960
01∅
25
D2
vsD
2D
1B
+A
2,B
7,D
R11
,A10
,B16
,DR
830
1249
6001
sd1
P2
AB
+A
1,B
8,D
R17
,A10
,B16
,DR
825
11.5
4960
01∅
29
D1
vsD
5D
2O−
A1,
B8,
DR
17,A
10,B
16,D
R8
5511
4960
01sd
2
P3
A−
A1,
B8,
DR
17,A
10,B
16,D
R8
6712
4960
01∅
5D
2vsD
2D
3A
+A
1,B
8,D
R17
,A10
,B16
,DR
865
1149
6001
sd3
P4
AB
+A
1,B
8,D
R17
,A10
,B16
,DR
830
1049
6001
∅6
D1
vsD
2D
4B−
A1,
B8,
DR
17,A
10,B
16,D
R8
6610
4900
20sd
2
P5
A+
A1,
B8,
DR
17,A
10,B
16,D
R8
6011
.549
6001
∅28
D2
vsD
2D
5O
+A
1,B
8,D
R17
,A10
,B16
,DR
855
11.5
4960
01sd
1
P1
P2
P3
P4
P5
D1 D2 D3 D4 D5
0 26 0 0 0
26 25 24 21 26
0 29 0 0 0
2523242525
0 30 29 0 30
Figure 9: Compatibility Matrix
P1, D1
P2, D2
P3, D3
P5, D5P4, D4
(a) Lexicographical tie breaking
P1, D1
P2, D2
P3, D3
P5, D5P4, D4
(b) IKEP proposed tie breaking
Figure 10: Compatibility Graph
The change in top preferences leads to the changein the graph and cycles present. Fig. 11 shows the
Page 16 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
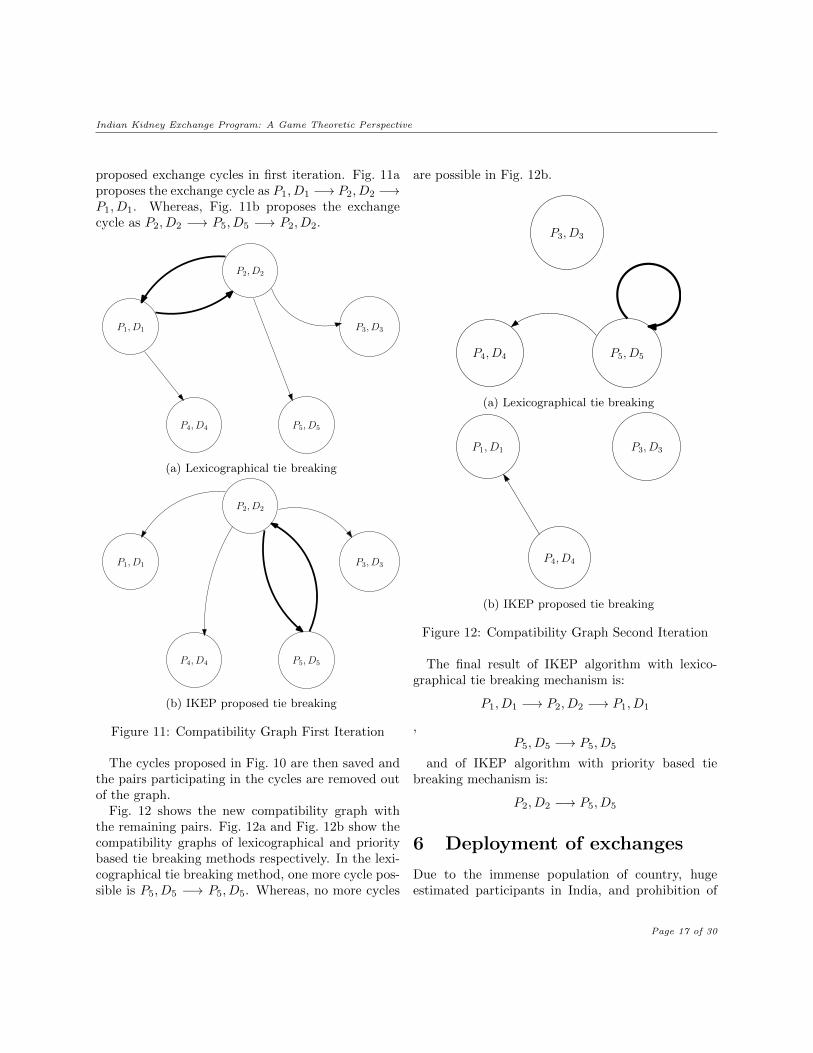
proposed exchange cycles in first iteration. Fig. 11aproposes the exchange cycle as P1, D1 −→ P2, D2 −→P1, D1. Whereas, Fig. 11b proposes the exchangecycle as P2, D2 −→ P5, D5 −→ P2, D2.
P1, D1
P2, D2
P3, D3
P5, D5P4, D4
(a) Lexicographical tie breaking
P1, D1
P2, D2
P3, D3
P5, D5P4, D4
(b) IKEP proposed tie breaking
Figure 11: Compatibility Graph First Iteration
The cycles proposed in Fig. 10 are then saved andthe pairs participating in the cycles are removed outof the graph.
Fig. 12 shows the new compatibility graph withthe remaining pairs. Fig. 12a and Fig. 12b show thecompatibility graphs of lexicographical and prioritybased tie breaking methods respectively. In the lexi-cographical tie breaking method, one more cycle pos-sible is P5, D5 −→ P5, D5. Whereas, no more cycles
are possible in Fig. 12b.
P3, D3
P5, D5P4, D4
(a) Lexicographical tie breaking
P1, D1 P3, D3
P4, D4
(b) IKEP proposed tie breaking
Figure 12: Compatibility Graph Second Iteration
The final result of IKEP algorithm with lexico-graphical tie breaking mechanism is:
P1, D1 −→ P2, D2 −→ P1, D1
,P5, D5 −→ P5, D5
and of IKEP algorithm with priority based tiebreaking mechanism is:
P2, D2 −→ P5, D5
6 Deployment of exchanges
Due to the immense population of country, hugeestimated participants in India, and prohibition of
Page 17 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
chains, encourages non-simultaneous cycles, whichrequires socialization to encourage trust. A priori, so-cialization becomes difficult when the number of peo-ple, financial structure, diversity and logistics chal-lenged by geography comes into existence.
6.1 Cycle Implementation
Instead of following the common paradigm of con-ducting the procurement and transplantation simul-taneously in the same hospital, which takes 2x sur-gical teams and operation theatre . IKEP takes outthe kidneys simultaneously in the same hospital andwould require 1x surgical teams and operation the-atre. Hence, a cycle length could be increased to 2x.The execution of the cycles in the matching can bedone by following steps.
Step 1. Donors travel to the location of recipients.Step 2. Kidneys are procured from the donor at
each center simultaneously. And operation theatre inall the centers act in a synchronised manner.
Step 3. Transplant the procured kidneys into thepatients.
7 Limitations of IKEP
Most of the limitations of IKEP is either due to theliteracy or due to legal restrictions19. And hence canonly be solved by government reforms and actions.
7.1 Anonymity
Since the pairs need to get themselves a permis-sion to go for a transplant from the gazetted offi-cers, and IKEP will also require to keep a track ofthe data, so that it could prove the legitimacy of thepatient-donor pair in times of audits by government.Anonymity can only be conserved to a particular ex-tent only.
7.2 Prohibition of Altruistic Donors
According to the laws in India for organ donations, itis illegal to donate organ without an intended recipi-
19As described in Appendix A.3.
ent. This prohibition, indirectly removes the presenceof chains in the KEPs. It has been observed that,KEPs without chains would eventually increase theaverage waiting time for the under demanded pairsand leads to accumulation. This is a serious limita-tion to IKEP, and proper amendments are needed tolegalize it.
7.2.1 Allowing chains will be revolutionary
Let there be 5 pairs (P1, D1) . . . (P5, D5). And thecharacteristics described in the Table 4. We haveassumed for the ease of solution, that every patientdon’t have a preference on societal distributions.
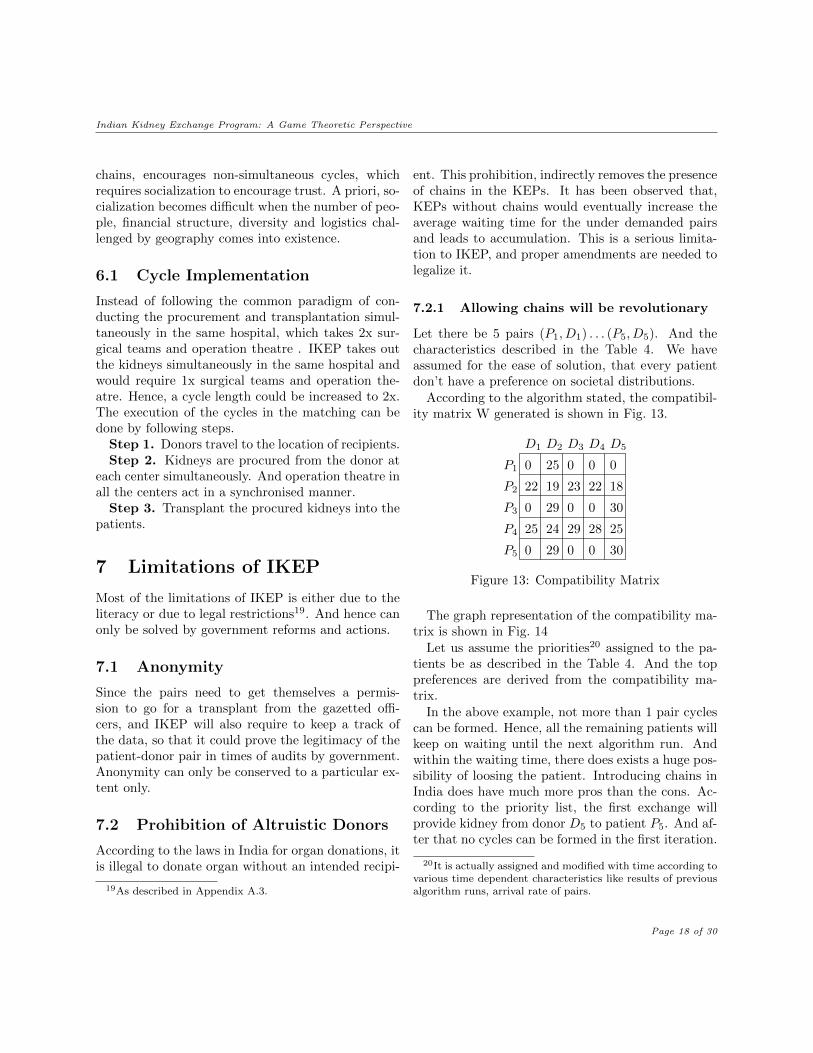
According to the algorithm stated, the compatibil-ity matrix W generated is shown in Fig. 13.
P1
P2
P3
P4
P5
D1 D2 D3 D4 D5
0 25 0 0 0
22 19 23 22 18
0 29 0 0 30
2528292425
0 29 0 0 30
Figure 13: Compatibility Matrix
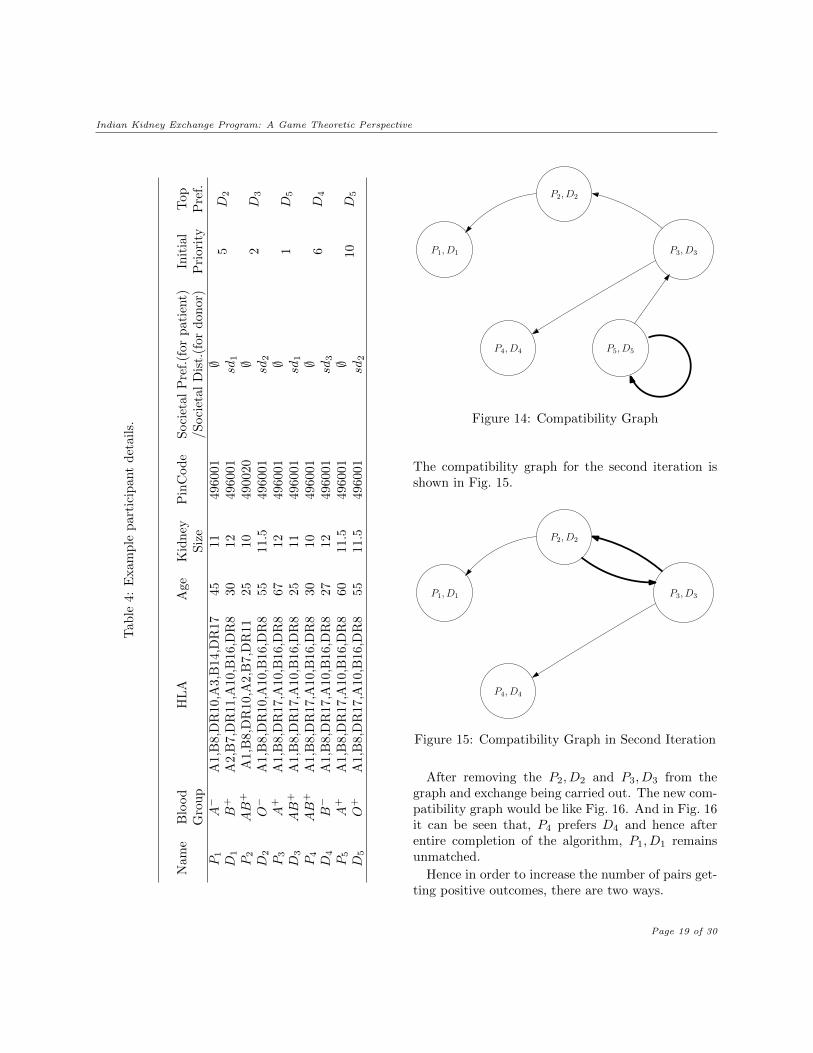
The graph representation of the compatibility ma-trix is shown in Fig. 14
Let us assume the priorities20 assigned to the pa-tients be as described in the Table 4. And the toppreferences are derived from the compatibility ma-trix.
In the above example, not more than 1 pair cyclescan be formed. Hence, all the remaining patients willkeep on waiting until the next algorithm run. Andwithin the waiting time, there does exists a huge pos-sibility of loosing the patient. Introducing chains inIndia does have much more pros than the cons. Ac-cording to the priority list, the first exchange willprovide kidney from donor D5 to patient P5. And af-ter that no cycles can be formed in the first iteration.
20It is actually assigned and modified with time according tovarious time dependent characteristics like results of previousalgorithm runs, arrival rate of pairs.
Page 18 of 30
Indian Kidney Exchange Program: A Game Theoretic PerspectiveT
able
4:E
xam
ple
par
tici
pan
td
etail
s.
Nam
eB
lood
HL
AA
geK
idn
eyP
inC
od
eS
oci
etal
Pre
f.(f
or
pati
ent)
Init
ial
Top
Gro
up
Siz
e/S
oci
etal
Dis
t.(f
or
don
or)
Pri
ori
tyP
ref.
P1
A−
A1,
B8,
DR
10,A
3,B
14,D
R17
4511
4960
01∅
5D
2D
1B
+A
2,B
7,D
R11
,A10
,B16
,DR
830
1249
6001
sd1
P2
AB
+A
1,B
8,D
R10
,A2,
B7,
DR
1125
1049
0020
∅2
D3
D2
O−
A1,
B8,
DR
10,A
10,B
16,D
R8
5511
.549
6001
sd2
P3
A+
A1,
B8,
DR
17,A
10,B
16,D
R8
6712
4960
01∅
1D
5D
3AB
+A
1,B
8,D
R17
,A10,
B16
,DR
825
1149
6001
sd1
P4
AB
+A
1,B
8,D
R17
,A10
,B16
,DR
830
1049
6001
∅6
D4
D4
B−
A1,
B8,
DR
17,A
10,B
16,D
R8
2712
4960
01sd
3
P5
A+
A1,
B8,
DR
17,A
10,B
16,D
R8
6011
.549
6001
∅10
D5
D5
O+
A1,
B8,
DR
17,A
10,B
16,D
R8
5511
.549
6001
sd2
P1, D1
P2, D2
P3, D3
P5, D5P4, D4
Figure 14: Compatibility Graph
The compatibility graph for the second iteration isshown in Fig. 15.
P1, D1
P2, D2
P3, D3
P4, D4
Figure 15: Compatibility Graph in Second Iteration
After removing the P2, D2 and P3, D3 from thegraph and exchange being carried out. The new com-patibility graph would be like Fig. 16. And in Fig. 16it can be seen that, P4 prefers D4 and hence afterentire completion of the algorithm, P1, D1 remainsunmatched.
Hence in order to increase the number of pairs get-ting positive outcomes, there are two ways.
Page 19 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
P1, D1
P4, D4
Figure 16: Compatibility Graph in Third Iteration
• Increasing number of participants by wait-ing: Let us assume a patient donor pair P6, D6
with priority 4 which arrives at a particularpoint of time. The properties of the new pairsare given in Table 5. And for ease of under-standing, let the societal preference be ∅ and thesocietal distribution be sd1.
Table 5: Details of additional pairs
Name ABO HLA Age Size PinCode
P6 B+ A2,B7,DR11, 25 11 496001A10,B16,DR8
D6 A+ A1,B8,DR17, 67 11.5 496001A10,B16,DR8
the new compatibility matrix W generated isshown in Fig. 17.
P1
P2
P3
P4
P5
D1 D2 D3 D4 D5
0 25 0 0 0
22 19 23 22 18
0 29 0 0 30
2528292425
0 29 0 0 30
P6
D6
29
28 22 0 26 22 0
23
30
17
0
Figure 17: Extended Compatibility Matrix
The new graph representation of the compatibil-
ity matrix is shown in Fig. 18. In this graph, thefirst iteration provides P5 the kidney from D5
which in turn modifies the graph into Fig. 19.
P1, D1
P2, D2
P3, D3
P5, D5P4, D4P6, D6
Figure 18: Compatibility Graph With More Pairs
In the second iteration, the cycle goes likeP1, D1 −→ P2, D2 −→ P3, D3 −→ P4, D4 −→P1, D1. After removal of all the participatingvertices, the modified compatibility graph forthird iteration is shown in Fig. 20.
P1, D1
P2, D2
P3, D3
P4, D4P6, D6
Figure 19: Second Iteration Compatibility Graph
Page 20 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
P4, D4
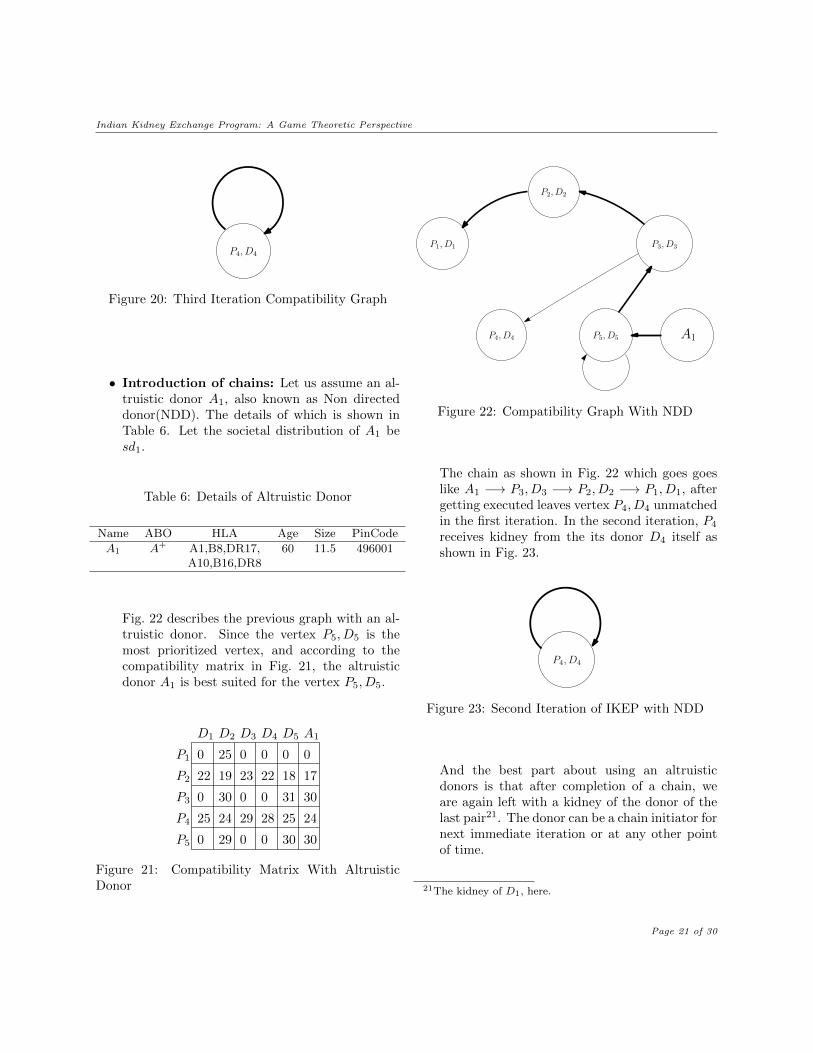
Figure 20: Third Iteration Compatibility Graph
• Introduction of chains: Let us assume an al-truistic donor A1, also known as Non directeddonor(NDD). The details of which is shown inTable 6. Let the societal distribution of A1 besd1.
Table 6: Details of Altruistic Donor
Name ABO HLA Age Size PinCode
A1 A+ A1,B8,DR17, 60 11.5 496001A10,B16,DR8
Fig. 22 describes the previous graph with an al-truistic donor. Since the vertex P5, D5 is themost prioritized vertex, and according to thecompatibility matrix in Fig. 21, the altruisticdonor A1 is best suited for the vertex P5, D5.
P1
P2
P3
P4
P5
D1 D2 D3 D4 D5
0 25 0 0 0
22 19 23 22 18
0 30 0 0 31
2528292425
0 29 0 0 30
A1
30
24
30
17
0
Figure 21: Compatibility Matrix With AltruisticDonor
P1, D1
P2, D2
P3, D3
P5, D5P4, D4 A1
Figure 22: Compatibility Graph With NDD
The chain as shown in Fig. 22 which goes goeslike A1 −→ P3, D3 −→ P2, D2 −→ P1, D1, aftergetting executed leaves vertex P4, D4 unmatchedin the first iteration. In the second iteration, P4
receives kidney from the its donor D4 itself asshown in Fig. 23.
P4, D4
Figure 23: Second Iteration of IKEP with NDD
And the best part about using an altruisticdonors is that after completion of a chain, weare again left with a kidney of the donor of thelast pair21. The donor can be a chain initiator fornext immediate iteration or at any other pointof time.
21The kidney of D1, here.
Page 21 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
8 Helicopter View Of IKEP
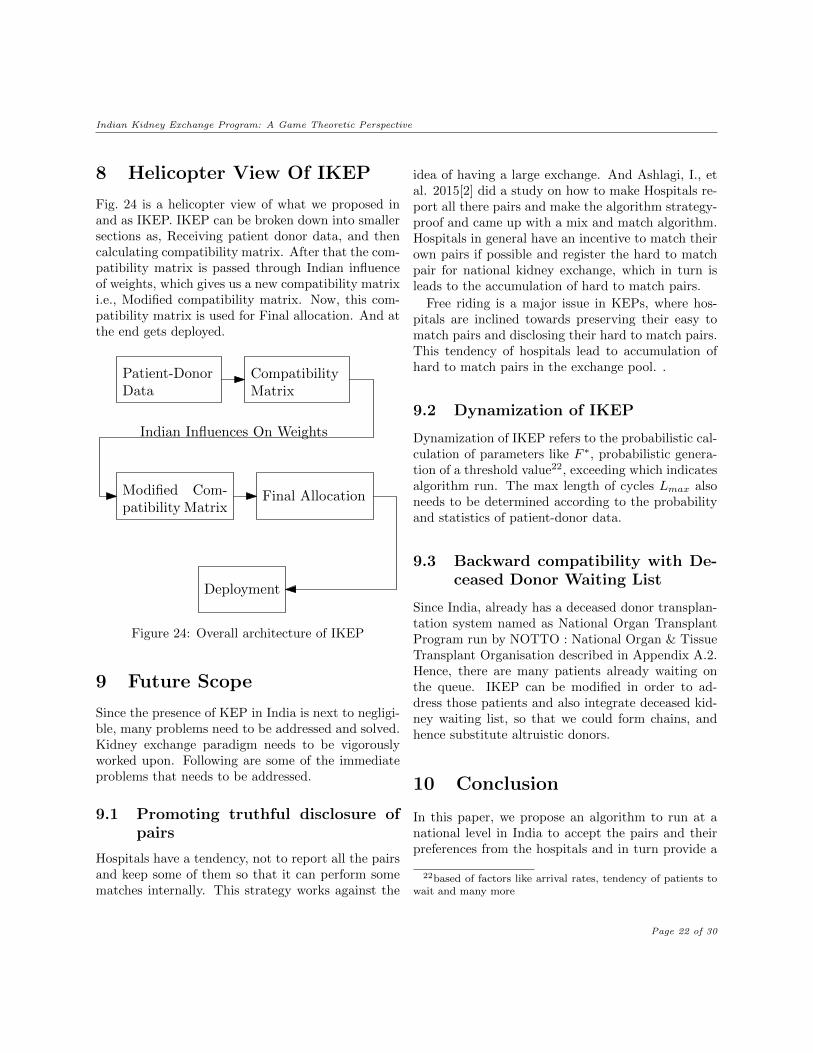
Fig. 24 is a helicopter view of what we proposed inand as IKEP. IKEP can be broken down into smallersections as, Receiving patient donor data, and thencalculating compatibility matrix. After that the com-patibility matrix is passed through Indian influenceof weights, which gives us a new compatibility matrixi.e., Modified compatibility matrix. Now, this com-patibility matrix is used for Final allocation. And atthe end gets deployed.
Patient-DonorData
CompatibilityMatrix
Modified Com-patibility Matrix
Final Allocation
Indian Influences On Weights
Deployment
Figure 24: Overall architecture of IKEP
9 Future Scope
Since the presence of KEP in India is next to negligi-ble, many problems need to be addressed and solved.Kidney exchange paradigm needs to be vigorouslyworked upon. Following are some of the immediateproblems that needs to be addressed.
9.1 Promoting truthful disclosure ofpairs
Hospitals have a tendency, not to report all the pairsand keep some of them so that it can perform somematches internally. This strategy works against the
idea of having a large exchange. And Ashlagi, I., etal. 2015[2] did a study on how to make Hospitals re-port all there pairs and make the algorithm strategy-proof and came up with a mix and match algorithm.Hospitals in general have an incentive to match theirown pairs if possible and register the hard to matchpair for national kidney exchange, which in turn isleads to the accumulation of hard to match pairs.
Free riding is a major issue in KEPs, where hos-pitals are inclined towards preserving their easy tomatch pairs and disclosing their hard to match pairs.This tendency of hospitals lead to accumulation ofhard to match pairs in the exchange pool. .
9.2 Dynamization of IKEP
Dynamization of IKEP refers to the probabilistic cal-culation of parameters like F ∗, probabilistic genera-tion of a threshold value22, exceeding which indicatesalgorithm run. The max length of cycles Lmax alsoneeds to be determined according to the probabilityand statistics of patient-donor data.
9.3 Backward compatibility with De-ceased Donor Waiting List
Since India, already has a deceased donor transplan-tation system named as National Organ TransplantProgram run by NOTTO : National Organ & TissueTransplant Organisation described in Appendix A.2.Hence, there are many patients already waiting onthe queue. IKEP can be modified in order to ad-dress those patients and also integrate deceased kid-ney waiting list, so that we could form chains, andhence substitute altruistic donors.
10 Conclusion
In this paper, we propose an algorithm to run at anational level in India to accept the pairs and theirpreferences from the hospitals and in turn provide a
22based of factors like arrival rates, tendency of patients towait and many more
Page 22 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
considerably stable, individually rational and maxi-mum cardinal exchanges. We propose some parame-ters which crucial to Indian perspective.
Appendix
A Current Situation in India
It has been noticed that kidney failures are becominga leading cause for many deaths. Number of deathshappening due to Chronic Kidney Disease(CKD) inIndia raised from 0.6 million in 1990 to 1.18 millionin 2016 [30]. According to an article by India Todaythere are approximately 1,00,000 people who are di-agnosed with End-stage kidney disease(EKSD) everyyear. And shows the burden of CKD in Indian med-ical space. And one of the best method to cope upwith this burden is Kidney transplantation. Manypatients rely on dialysis(two to three times a week)for there life, which is much more costlier than bothin terms of money, time and effort. And more impor-tantly quality of life degrades considerably.
Kidney exchange(KE) is essential for India sinceits absence leads to a considerable number of pa-tients get matched with incompatible kidneys whichin turn needs to be treated with immunosuppres-sants23 in large amounts.[3] The use of immunosup-pressants add to a lifelong monthly expenditure onmedicines which is approximately near about |10,000to |15,000. This expense can also be reduced throughKEPs by getting more compatible kidneys throughthem. A considerable amount of work24 needs tobe done in the direction of adaptation of kidney ex-change in India to reduce fatalities mentioned above.
One good thing about the kidneys are that everyperson on this planet are are born with two kid-neys(excluding those in case born with one). Andcan live perfectly fine with any one of them. There-fore, people can donate one of their kidneys to thereloved ones, making themselves a living donor. Andwith the advent of living donors in the field of kidney
23Immunosuppressants are those medical drugs given to thepatients in order to stop there body from rejecting the newkidney transplanted.
24Although there are some people working in this domain.
transplant, comes a situation in which living donor isincompatible to donate to the patient, he/she wantsto donate to. This problem is addressed by kidneyexchange.
There was an estimate in 2018 stating that in In-dia, there were near about 175,000 patients depen-dent on chronic dialysis. Which turns out to be129 per million population.[25] According to a blogby Narayana Health in the year 2019, there were200,000 recipient awaiting kidneys, and only 15,000donors willing to donate kidneys. Moreover, accord-ing to a calculation by Ministry of Health, out of arange of 2-3 lakhs transplant requirements, only 6000are getting accomplished. The burden of fatalities onIndia is larger than other low-middle income coun-tries.
And in order to combat the burden, kidney trans-plants act as a boon. Kidney transplants are far in-expensive to dialysis. According to a study[1], 60%of the dialysis patients resides more than 50km awayfrom Hemodialysis(HD) station, and nearly 25% re-sides more than 100km away. A huge amount ofmoney in transportation itself.25 Total cost per dial-ysis is approximately |4148($64), which accounts for|8296($128) per week26[6]. There are portals for de-ceased kidney transplantation, but the chances arevery thin27.
A.1 Related Work
The factor behind the success of single centered KEPdepends on the formation central registry of theincompatible pairs and the literacy about KEPs28
(Kute VB et al 2017[27]). Single center KE were per-formed by Pahwa et al[10], Waigankar et al[22], Jha
25At an average, in India there are 2 dialysis per week.26In India, there are people working at a salary of
|8296($128) per month.27The number of deceased kidneys extracted are very less in
number because of less time span between the arrival of kid-ney to the selection of recipient, large recipient waiting pooland less number of deceased kidneys being eligible to be trans-planted.
28Most of the people in India don’t have information re-garding KEPs. This is a new paradigm, which needs to beimplemented massively to reduce a significant part of deaths.Discussed more specifically in Appendix A.4.1
Page 23 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
et al [16], Kute et al[28], Kute et al[26] for the du-rations 2006-2011, 2008-2011, 2010-2013, 2000-2012,2013 respectively. Utkarsh Verma et al 2020[24] anal-ysed how multiple registries of KEPs in India workand how can they be brought together and performmatching in coalition with individual rationality con-straints.
A.2 National Organ Transplant Pro-gram
National organ transplant program is an Indian pro-gram run by Directorate General of Health Servicesunder the Ministry of Health & Family Welfare, toprocure deceased donor kidneys, maintain EKPD pa-tients waiting list and allot kidneys accordingly. It’sobjective is to improve the ease of transplantationby promoting deceased organ donations. NOTP alsoprotects vulnerable patients from organ trafficking.NOTTO : National Organ & Tissue Transplant Or-ganisation act as an apex organisation for coordinat-ing and procuring deceased kidney and providing itto the wait-listed candidates.
A.3 Legal Framework in India
The fist act governing the transplantation in India isTransplantation of Human Organ Act(THO)1994.
• It was passed in order to regulate the organ pro-curement, storage and transplantation.
• It also prohibited commercial trading of humanorgans.
In 2011, an amendment was passednamed as Transplantation of Human Or-gan(Amendment) Act(THO) 2011.
• It legalizes swap donations, i.e., kidney ex-changes are legalized by this act.
• It specifies that patients are only allowed to re-ceive an organ(here, kidney) from their first rela-tives only. In situations when there is no first rel-ative, the patient and the donor need to get per-mission from government appointed authoriza-
tion committee, which finds out the genuinenessof the donor.
• The Kidney exchanges need to be approvedby the concerned authorities before conductingthem.
A.4 Issues
There are several issues, prevailing in India which arehindering the progress of kidney exchange paradigmin India.
A.4.1 Literacy
Literacy of KEPs in India is very less. There is alsoa shortage of living donor due to the fear of con-sequences of not having a kidney which actually isnone. Recently, Indian government faced a huge re-sistance from rural part of the country in order toget themselves vaccinated. Hence getting more andmore people to participating in organ donation, evento there loved ones will be a big checkpoint.
A.4.2 Restrictions on NDD
According to the legal restrictions discussed above inAppendix A.3, non directed donors are not allowedwhich in turn prohibits chains. And there prohibi-tions will lead to accumulation of hard to match pairs.Chains have been acting as a boon for those pairs incountries like UK, USA, etc.
A.4.3 Poor Infrastructure
India spends approximately 1.5% of its GDP inhealthcare sector. For a vast and populated countrylike India, the mentioned expenditure is very less. Asa result of this, there are significantly huge cardinal-ity of hospitals unmaintained. The government runhospitals do not have adequate surgical facilities. In-frastructure would add to the resistance towards theimplementation of IKEP.
A.4.4 Abundance of uninsured patients
Since, India is a developing nation, there is a signifi-cant amount of poverty prevailing in the country. The
Page 24 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
poverty stricken population will obviously not con-sider purchasing insurances. And hence, there wouldbe a section of population, tending towards dying athome than to enroll in a dialysis initially and then inIKEP.
A.5 Existing Kidney Registry
There are basically two significant kidney registriesin India.
A.5.1 ASTRA
Apex Swap Transplant Registry29 - Apex KidneyFoundation, situated in Mumbai performs simulta-neous KEPs30 in India. It is a paired kidney registry,established in 2011.
A.5.2 IKDRC
Dr. HL Trivedi Institute of Trans-plantation Sci-ences (IKDRC-ITS)31, Ahmedabad, India carried out10 pair non-simultaneous cycles32 in the year 2020[7] and a simultaneous 10 pair cycle in 2013 [8].They have significantly contributed towards spread-ing awareness about KEP in India. Form January2000 to July 2016, the same hospital carried out3616 live donor renal transplants and 561 deceasedkidney transplants, out to which 300 were kidneyexchanges[27].
B Background and Definitions
Some of the basic information regarding kidney ex-change and its history are discussed in the followingsections.
29http://www.apexkidneyfoundation.org/astra/30Discussed earlier, way in which procurement and trans-
plantation is carried our simultaneously31http://www.ikdrc-its.org/32Non Simultaneous cycles are not allowed in many coun-
tries because of the risk of patient not getting a kidney afterproviding one by its incompatible donor
B.1 History
The paradigm of kidney exchange was first suggestedand published by Felix Rapaport in Rapaport FT etal. 1986[5]and was first, successfully carried out inSouth Korea[9]. After this, several KEPs were carriedout in Switzerland[9], USA[23] and England[15]. Theparadigm of KEPs were popularized by Roth et al.(2004)[17], Roth et al. (2005)[18], and Roth et al.(2007)[19]
B.2 Kidney Exchange
A problem in which at-least two patient-donor33
pairs34, who are incapable of exchanging kidneyamong themselves due to incompatibilities discussedbriefly in upcoming subsections. But, are compati-ble among each other. Suppose there are two pairs(P1, D1), (P2, D2) and D1 can’t donate her kidney toP1 rather can donate to P2. Similarly can D2 do-nate her kidney to P1. And in this way, the exchangehappens in a 2-way exchange. KE can accumulaten-way exchanges35, but comes with huge costs. Vari-ous ways of matching are used for matching the pairsand forming cycles and chains.
B.3 Cycles and Chains.
Cycles are formed when there are finite pairs in thepool which can exchange kidneys among themselves.All the matched pairs are brought into a same placeand the exchange(operation) takes place simultane-ously.
There are some people who voluntarily come up inorder to donate a kidney, but in turn don’t have anypatient along with them. And hence introduce a free-undirected kidney in the system. These people areknown as Non-directed Donors(NDD)36. Presence of
33Sometimes there are patients with their loved ones willingto donate a kidney but are incompetent to receive that kidney.
34For a patient to participate and benefit from a KE pro-gram, it is compulsory to have a donor.
35Many countries don’t allow more than 3-way exchange.Where as some countries like Germany don’t even allow KidneyExchange.
36India, France, Poland, Greece, Switzerland are some of themany countries that don’t allow live donation of organs
Page 25 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
these donors lead to the formation of chains. Form-ing a chain, results into exchanges taking place atdifferent times. Formation of chains reduces logisti-cal constraints, and hence involve large exchanges.
B.4 Biological constraints
The basic factors for matching a pair to another aredependent on blood group, tissue compatibility andsensitization.
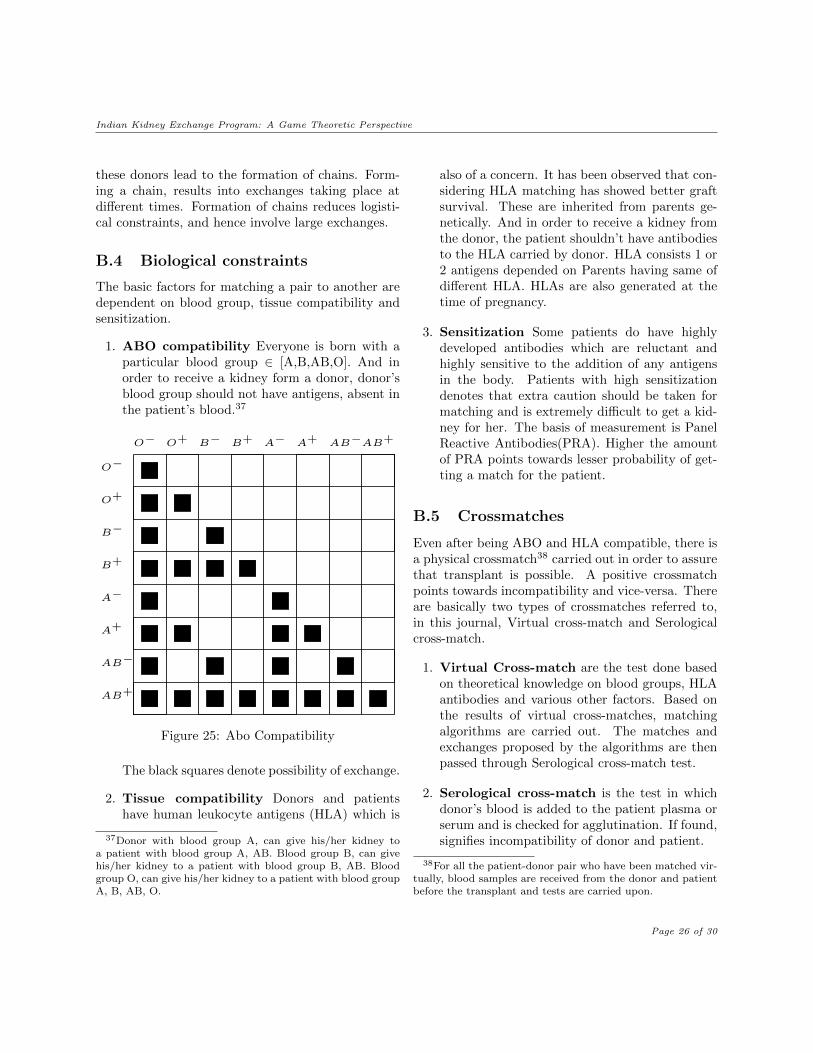
1. ABO compatibility Everyone is born with aparticular blood group ∈ [A,B,AB,O]. And inorder to receive a kidney form a donor, donor’sblood group should not have antigens, absent inthe patient’s blood.37
O− O+ B− B+ A− A+ AB−AB+
O−
O+
B−
B+
A−
A+
AB−
AB+
Figure 25: Abo Compatibility
The black squares denote possibility of exchange.
2. Tissue compatibility Donors and patientshave human leukocyte antigens (HLA) which is
37Donor with blood group A, can give his/her kidney toa patient with blood group A, AB. Blood group B, can givehis/her kidney to a patient with blood group B, AB. Bloodgroup O, can give his/her kidney to a patient with blood groupA, B, AB, O.
also of a concern. It has been observed that con-sidering HLA matching has showed better graftsurvival. These are inherited from parents ge-netically. And in order to receive a kidney fromthe donor, the patient shouldn’t have antibodiesto the HLA carried by donor. HLA consists 1 or2 antigens depended on Parents having same ofdifferent HLA. HLAs are also generated at thetime of pregnancy.
3. Sensitization Some patients do have highlydeveloped antibodies which are reluctant andhighly sensitive to the addition of any antigensin the body. Patients with high sensitizationdenotes that extra caution should be taken formatching and is extremely difficult to get a kid-ney for her. The basis of measurement is PanelReactive Antibodies(PRA). Higher the amountof PRA points towards lesser probability of get-ting a match for the patient.
B.5 Crossmatches
Even after being ABO and HLA compatible, there isa physical crossmatch38 carried out in order to assurethat transplant is possible. A positive crossmatchpoints towards incompatibility and vice-versa. Thereare basically two types of crossmatches referred to,in this journal, Virtual cross-match and Serologicalcross-match.
1. Virtual Cross-match are the test done basedon theoretical knowledge on blood groups, HLAantibodies and various other factors. Based onthe results of virtual cross-matches, matchingalgorithms are carried out. The matches andexchanges proposed by the algorithms are thenpassed through Serological cross-match test.
2. Serological cross-match is the test in whichdonor’s blood is added to the patient plasma orserum and is checked for agglutination. If found,signifies incompatibility of donor and patient.
38For all the patient-donor pair who have been matched vir-tually, blood samples are received from the donor and patientbefore the transplant and tests are carried upon.
Page 26 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
B.6 Pair types.
Patient-donor pairs are classified based on the diffi-culty to be matched. The easy to match pairs arethose which are highly demanded and vice versa.Mostly ABO compatible pairs(AB-A, AB-B, A-O,AB-O, B-O) are highly demanded as compared tothe ABO incompatible pairs(A-AB, B-AB, O-A, O-B, O-AB), because ABO compatible pairs offer moreacceptable kidneys than they themselves require.39
Another reason for a pair to be a hard to match pairis high sensitization of the patient.
B.7 Matching
Whenever a suitable pool is formed, matching algo-rithms are carried out in order to match maximumnumber of pairs. There are basically two types ofmatching in kidney exchange paradigm.
B.7.1 Static Matching
The static matching conducts matching on the pairspresent in the pool at a particular timestamp. Pairsparticipating in successful exchanges are removedfrom the pool and rest remain in the pool for nexttime. The probability of getting better matches onwaiting is not taken in to account.
B.7.2 Dynamic Matching
Dynamic matching takes probability of getting amatch for the pairs in the pool by waiting in to con-sideration.
It accounts for arrival rates, probability of compat-ible, incompatible pairs opting out of IKEP after notgetting matched or get matched in an easier manner,outside.
There are different policies used in matching pairsin the market using dynamic matching.
39Eg., B-O pair offers a O blood group kidney, which ishighly demanded for O blood group patients whereas wantsan B blood group kidney in return which is considerably easyto get. Moreover pairs like B-O don’t generally appear in thepool since they are ABO compatible whereas O-B does accu-mulate.
• Greedy policy. In this policy, the pairs arematched as soon as they arrive in the market.
• Batching policy. In this policy, the pairs arematched in batches at a particular time interval.The time interval varies from programs to pro-grams. Programs wait from one day to weeklyto monthly.
There is a trade off between the possibility of get-ting a match for the pair by waiting and taking therisk of losing the life of the patient.
C Class Definitions
Firstly, we describe the Graph class in Algorithm 15,its member variables and member functions.
Algorithm 15 Graph
1: class Graph2: n : Integer3: adj : List<List<Vertex>>4: procedure Graph(n)5: this.n← n6: adj ←new ArrayList<> (n)7: for all i ∈ {0, 1, . . . n} do8: adj.add(new LinkedList<> ())9: end for
10: end procedure11: procedure addEdge(i, j) . adds directed
edge from i to j12: adj.get(i).add(j)13: end procedure14: end class
We now describe the Vertex class in Algorithm 16,its member variables. The member variables are sameas described in the Section 1.2.
Page 27 of 30
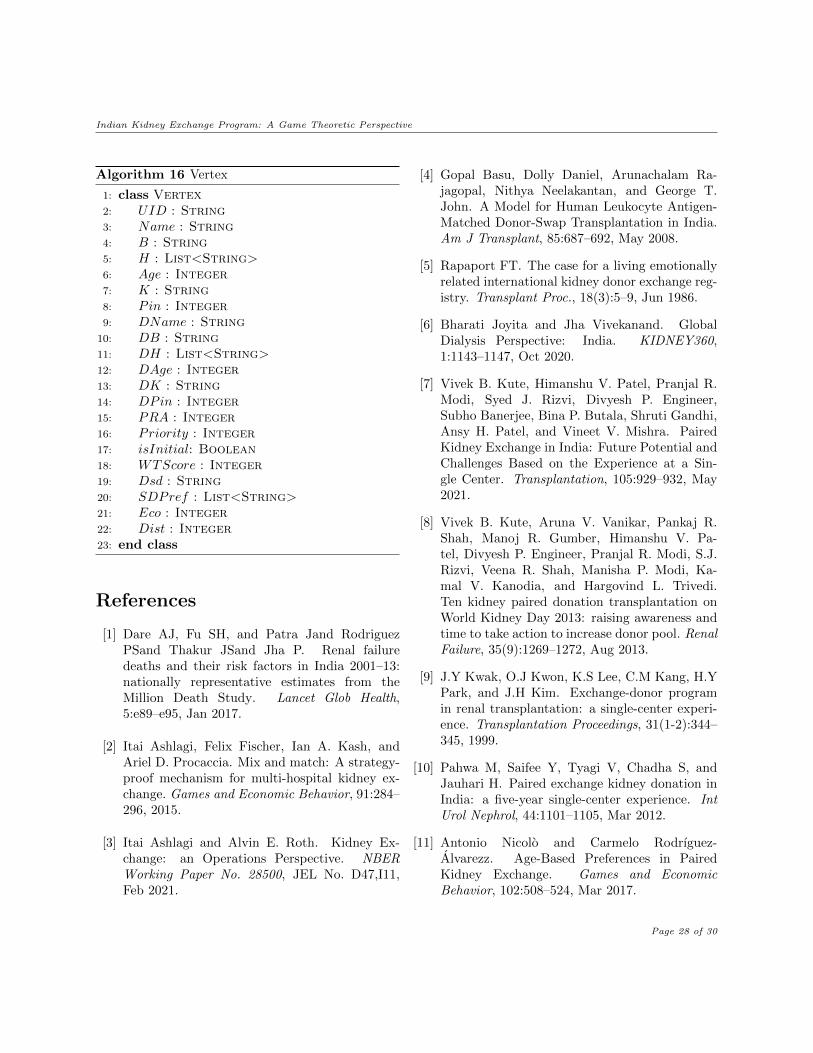
Indian Kidney Exchange Program: A Game Theoretic Perspective
Algorithm 16 Vertex
1: class Vertex2: UID : String3: Name : String4: B : String5: H : List<String>6: Age : Integer7: K : String8: Pin : Integer9: DName : String
10: DB : String11: DH : List<String>12: DAge : Integer13: DK : String14: DPin : Integer15: PRA : Integer16: Priority : Integer17: isInitial: Boolean18: WTScore : Integer19: Dsd : String20: SDPref : List<String>21: Eco : Integer22: Dist : Integer23: end class
References
[1] Dare AJ, Fu SH, and Patra Jand RodriguezPSand Thakur JSand Jha P. Renal failuredeaths and their risk factors in India 2001–13:nationally representative estimates from theMillion Death Study. Lancet Glob Health,5:e89–e95, Jan 2017.
[2] Itai Ashlagi, Felix Fischer, Ian A. Kash, andAriel D. Procaccia. Mix and match: A strategy-proof mechanism for multi-hospital kidney ex-change. Games and Economic Behavior, 91:284–296, 2015.
[3] Itai Ashlagi and Alvin E. Roth. Kidney Ex-change: an Operations Perspective. NBERWorking Paper No. 28500, JEL No. D47,I11,Feb 2021.
[4] Gopal Basu, Dolly Daniel, Arunachalam Ra-jagopal, Nithya Neelakantan, and George T.John. A Model for Human Leukocyte Antigen-Matched Donor-Swap Transplantation in India.Am J Transplant, 85:687–692, May 2008.
[5] Rapaport FT. The case for a living emotionallyrelated international kidney donor exchange reg-istry. Transplant Proc., 18(3):5–9, Jun 1986.
[6] Bharati Joyita and Jha Vivekanand. GlobalDialysis Perspective: India. KIDNEY360,1:1143–1147, Oct 2020.
[7] Vivek B. Kute, Himanshu V. Patel, Pranjal R.Modi, Syed J. Rizvi, Divyesh P. Engineer,Subho Banerjee, Bina P. Butala, Shruti Gandhi,Ansy H. Patel, and Vineet V. Mishra. PairedKidney Exchange in India: Future Potential andChallenges Based on the Experience at a Sin-gle Center. Transplantation, 105:929–932, May2021.
[8] Vivek B. Kute, Aruna V. Vanikar, Pankaj R.Shah, Manoj R. Gumber, Himanshu V. Pa-tel, Divyesh P. Engineer, Pranjal R. Modi, S.J.Rizvi, Veena R. Shah, Manisha P. Modi, Ka-mal V. Kanodia, and Hargovind L. Trivedi.Ten kidney paired donation transplantation onWorld Kidney Day 2013: raising awareness andtime to take action to increase donor pool. RenalFailure, 35(9):1269–1272, Aug 2013.
[9] J.Y Kwak, O.J Kwon, K.S Lee, C.M Kang, H.YPark, and J.H Kim. Exchange-donor programin renal transplantation: a single-center experi-ence. Transplantation Proceedings, 31(1-2):344–345, 1999.
[10] Pahwa M, Saifee Y, Tyagi V, Chadha S, andJauhari H. Paired exchange kidney donation inIndia: a five-year single-center experience. IntUrol Nephrol, 44:1101–1105, Mar 2012.
[11] Antonio Nicolo and Carmelo Rodrıguez-Alvarezz. Age-Based Preferences in PairedKidney Exchange. Games and EconomicBehavior, 102:508–524, Mar 2017.
Page 28 of 30
Indian Kidney Exchange Program: A Game Theoretic Perspective
[12] Noam Nisan, Tim Roughgarden, Eva Tardos,and Vijay V. Vazirani i. Algorithmic Game The-ory. Cambridge University Press, 32 Avenue ofthe Americas, New York, NY 10013-2473, USA”,Sep 2007.
[13] National Organ and Tissue Transplant Organ-isation. Updated Kidney Allocation Policy.www.notto.gov.in.
[14] Singh N P and Kumar A. Kidney transplanta-tion in India: Challenges and future recommen-dation. MAMC J Med Sci, 2:12–17, Jan 2016.
[15] Zarsadias P, Monaco AP, and Morrissey PE.A pioneering paired kidney exchange. StudentBMJ, 18:c1562, 2010.
[16] Jha PK, Sethi S, Bansal SB, Jain M, SharmaR, Phanish MK, Duggal R, Ahlawat R, andKher V. Paired kidney exchange transplanta-tion: Maximizing the donor pool. Indian JNephrol, 25:349–354, 2015.
[17] Alvin E. Roth, Tayfun Sonmez, and M. UtkuUnver. Kidney Exchange. The Quarterly Jour-nal of Economics, 119:457–488, May 2004.
[18] Alvin E. Roth, Tayfun Sonmez, and M. UtkuUnver. Pairwise kidney exchange. Journal ofEconomic Theory, 125:151–188, May 2005.
[19] Alvin E. Roth, Tayfun Sonmez, and M. UtkuUnver. Efficient Kidney Exchange: Coinci-dence of Wants in Markets with Compatibility-Based Preferences. American Economic Review,97(3):828–851, Jun 2007.
[20] Tim Roughgarden. Lecture 10: Kidney Ex-change and Stable Matching. CS364A: Algorith-mic Game Theory, Oct 2013.
[21] Lloyd Shapley and Herbert Scarf. On coresand indivisibility. Journal of Mathematical Eco-nomics, 1(1):23–37, 1974.
[22] Waigankar SS, Kamat MH, Joshi S, Gandhi BV,Bahadur M, and Deshpande RV. Living donor
transplant options in end-stage renal disease pa-tients with ABO incompatibility. Indian J Urol,29:114–118, 2013.
[23] G Thiel, P Vogelbach, L Gurke, T Gasser,K Lehmann, T Voegele, A Kiss, and G Kirste.Crossover renal transplantation: hurdles to becleared! Transplantation Proceedings, 33:811–816, 2001.
[24] Verma Utkarsh and Rangaraj Narayan. Analysisof multi-registry kidney exchange program withindividual rationality constraints. Dec 2020.
[25] Jha V, Ur-Rashid H, Agarwal SK, Akhtar SF,Kafle RK, and Sheriff R. ISN South Asia Re-gional Board: The state of nephrology in SouthAsia. Kidney Int, 95:31–37, Jan 2019.
[26] Kute VB, Vanikar AV, Shah PR, Gumber MR,Patel HV, Engineer DP, Modi PR, Shah VR, andTrivedi HL. Increasing access to kidney trans-plantation in countries with limited resources:the Indian experience with kidney paired do-nation. Nephrology (Carlton), 19:599–604, Jul2014.
[27] Kute VB, Patel HV, Shah PR, Modi PR, ShahVR, Rizvi SJ, Pal BC, Modi MP, Shah PS,Varyani UT, Wakhare PS, Shinde SG, GhodelaVA, Patel MH, Trivedi VB, and Trivedi HL.Past, present and future of kidney paired do-nation transplantation in India. World Journalof Transplantation, 7(2):134–143, Apr 2017.
[28] Kute VB, Gumber MR, Patel HV, Shah PR,Vanikar AV, Modi PR, Shah VR, Patel MP, andTrivedi HL. Outcome of kidney paired dona-tion transplantation to increase donor pool andto prevent commercial transplantation: a single-center experience from a developing country. IntUrol Nephrol, 45:1171–1178, Aug 2013.
[29] Roger P Worthington and Anupriya Gogne. Cul-tural aspects of primary healthcare in India:A case- based analysis. Asia Pacific familymedicine, 10(1):8, Jan 2011.
Page 29 of 30

Indian Kidney Exchange Program: A Game Theoretic Perspective
[30] Xie Y, Bowe B, Mokdad AH, Xian H, Yan Y,Li T, Maddukuri G, Tsai CY, Floyd T, and Al-Aly Z. Analysis of the Global Burden of Diseasestudy highlights the global, regional, and na-tional trends of chronic kidney disease epidemi-ology from 1990 to 2016. Kidney Int, 94:567–581,Aug 2018.
Page 30 of 30
Related Documents











