Indentation Stiffness of Repair Tissue after Autologous Chondrocyte Transplantation Anna I. Vasara, MD*; Miika T. Nieminen, PhD†; Jukka S. Jurvelin, PhD‡; Lars Peterson, MD, PhD§; Anders Lindahl, MD, PhD ; and Ilkka Kiviranta, MD, PhD¶ Our main hypothesis was that indentation stiffness of the repair tissue approaches the values of adjacent cartilage 1 year after autologous chondrocyte transplantation. We also wanted to investigate the differences between osteochondritic lesions and full-thickness lesions. Thirty patients with carti- lage lesions were operated on with autologous chondrocyte transplantation. The repair was evaluated arthroscopically, indentation stiffness was measured, and clinical evaluations were done. The stiffness of the repair tissue improved to 62% (mean 2.04 ± 0.83 N, mean ± SD) of adjacent cartilage (3.58 ± 1.04 N). Fifty-three percent of the patients graded their knee as excellent or good and 47% of the patients graded their knee as fair at the followup. In six patients the normal- ized stiffness was at least 80%, suggesting hyaline-like re- pair. The indentation stiffness of the osteochondritis disse- cans lesion repairs (1.45 ± 0.46 N; n = 7) was less than that of the nonosteochondritis dissecans lesion repair sites (2.37 ± 0.72 N; n = 19). Gadolinium-enhanced magnetic resonance imaging of the cartilage (dGEMRIC) during followup of four patients suggested proteoglycan replenishment, although all grafts showed low indentation values. Low stiffness values may indicate incomplete maturation or predominantly fi- brous repair. The indentation analysis showed that the re- pair tissue stiffness could, in some cases, reach the same level as the adjacent cartilage, but there was a large variation among the grafts. Autologous chondrocyte transplantation is a widely used technique for treatment of cartilage injuries. 5 The clinical long-term results have been good. 7,28,33,34 The repair tis- sue after autologous chondrocyte transplantation is often hyaline-like cartilage with predominantly Type II colla- gen. 5,36,37 An animal study confirmed the viability of transplanted chondrocytes at least until 3 months. 12 How- ever, many aspects of the maturation of the repair tissue still are unknown. There are few data regarding the me- chanical integrity of the repair tissue even though biome- chanical properties affect the long-term durability of the repair tissue. 33 Arthroscopic indentation stiffness measurements have provided valuable information regarding cartilage biome- chanics and constituents even before macroscopic changes of cartilage can be detected. 24,25,26 Quantitative MRI tech- niques have been developed for structural characterization of articular cartilage composition, providing potential methodology for monitoring tissue degeneration and re- generation. 8 One of these techniques, delayed gadolinium- enhanced MRI of cartilage (dGEMRIC), enables estima- tion of relative proteoglycan (PG) concentration in carti- lage from T1 relaxation time measurements in the presence of the cationic contrast agent Gd-DTPA 2– . 3,9,29 The technique has been used for assessment of relative glycosaminoglycan (GAG) distribution in autologous chondrocyte transplantation grafts in vivo, 11 and it has been successfully correlated with mechanical properties of bovine articular cartilage in vitro. 31 Received: February 15, 2004 Revised: September 6, 2004 Accepted: October 26, 2004 From the *Department of Orthopedics and Traumatology, Helsinki Univer- sity Hospital, HUS; the †Department of Anatomy, University of Kuopio; the ‡Department of Clinical Physiology and Nuclear Medicine, Kuopio Univer- sity Hospital, Kuopio, Finland; the §Institute of Orthopedics, Göteborg Uni- versity, Sahlgrenska University Hospital; and the Institute of Laboratory Medicine, Department of Clinical Chemistry and Transfusion Medicine, Göteborg University, Sahlgrenska University Hospital, Go ¨teburg, Sweden; and the ¶Department of Orthopedics and Traumatology, Jyväskylä Central Hospital, Jyväskylä, Finland. Each author certifies that his or her institution has approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research, and that informed consent was obtained. Each author certifies that he or she has or may receive payments or benefits from a commercial entity related to this work. One or more of the authors has received funding from the Instrumentarium Science Foundation, Finnish Cultural Foundation (North-Savo Foundation), Jyväskylä Central Hospital (Söderholm grant and grant B51), Sigrid Juselius foundation, and Finnish Orthopaedics and Traumatology Research Founda- tion. Correspondence to: Anna Vasara, MD, Vilkenintie 16A, FIN-00640, Hel- sinki, Finland. Phone: 358-405261552; Fax: 358-962274750; E-mail: [email protected]. DOI: 10.1097/01.blo.0000150567.00022.2e CLINICAL ORTHOPAEDICS AND RELATED RESEARCH Number 433, pp. 233–242 © 2005 Lippincott Williams & Wilkins 233

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Indentation Stiffness of Repair Tissue after AutologousChondrocyte Transplantation
Anna I. Vasara, MD*; Miika T. Nieminen, PhD†; Jukka S. Jurvelin, PhD‡;Lars Peterson, MD, PhD§; Anders Lindahl, MD, PhD�; and Ilkka Kiviranta, MD, PhD¶
Our main hypothesis was that indentation stiffness of therepair tissue approaches the values of adjacent cartilage 1year after autologous chondrocyte transplantation. We alsowanted to investigate the differences between osteochondriticlesions and full-thickness lesions. Thirty patients with carti-lage lesions were operated on with autologous chondrocytetransplantation. The repair was evaluated arthroscopically,indentation stiffness was measured, and clinical evaluationswere done. The stiffness of the repair tissue improved to 62%(mean 2.04 ± 0.83 N, mean ± SD) of adjacent cartilage (3.58± 1.04 N). Fifty-three percent of the patients graded theirknee as excellent or good and 47% of the patients gradedtheir knee as fair at the followup. In six patients the normal-ized stiffness was at least 80%, suggesting hyaline-like re-pair. The indentation stiffness of the osteochondritis disse-cans lesion repairs (1.45 ± 0.46 N; n = 7) was less than thatof the nonosteochondritis dissecans lesion repair sites (2.37 ±0.72 N; n = 19). Gadolinium-enhanced magnetic resonance
imaging of the cartilage (dGEMRIC) during followup of fourpatients suggested proteoglycan replenishment, although allgrafts showed low indentation values. Low stiffness valuesmay indicate incomplete maturation or predominantly fi-brous repair. The indentation analysis showed that the re-pair tissue stiffness could, in some cases, reach the same levelas the adjacent cartilage, but there was a large variationamong the grafts.
Autologous chondrocyte transplantation is a widely usedtechnique for treatment of cartilage injuries.5 The clinicallong-term results have been good.7,28,33,34 The repair tis-sue after autologous chondrocyte transplantation is oftenhyaline-like cartilage with predominantly Type II colla-gen.5,36,37 An animal study confirmed the viability oftransplanted chondrocytes at least until 3 months.12 How-ever, many aspects of the maturation of the repair tissuestill are unknown. There are few data regarding the me-chanical integrity of the repair tissue even though biome-chanical properties affect the long-term durability of therepair tissue.33
Arthroscopic indentation stiffness measurements haveprovided valuable information regarding cartilage biome-chanics and constituents even before macroscopic changesof cartilage can be detected.24,25,26 Quantitative MRI tech-niques have been developed for structural characterizationof articular cartilage composition, providing potentialmethodology for monitoring tissue degeneration and re-generation.8 One of these techniques, delayed gadolinium-enhanced MRI of cartilage (dGEMRIC), enables estima-tion of relative proteoglycan (PG) concentration in carti-lage from T1 relaxation time measurements in thepresence of the cationic contrast agent Gd-DTPA2–.3,9,29
The technique has been used for assessment of relativeglycosaminoglycan (GAG) distribution in autologouschondrocyte transplantation grafts in vivo,11 and it hasbeen successfully correlated with mechanical properties ofbovine articular cartilage in vitro.31
Received: February 15, 2004Revised: September 6, 2004Accepted: October 26, 2004From the *Department of Orthopedics and Traumatology, Helsinki Univer-sity Hospital, HUS; the †Department of Anatomy, University of Kuopio; the‡Department of Clinical Physiology and Nuclear Medicine, Kuopio Univer-sity Hospital, Kuopio, Finland; the §Institute of Orthopedics, Göteborg Uni-versity, Sahlgrenska University Hospital; and the �Institute of LaboratoryMedicine, Department of Clinical Chemistry and Transfusion Medicine,Göteborg University, Sahlgrenska University Hospital, Goteburg, Sweden;and the ¶Department of Orthopedics and Traumatology, Jyväskylä CentralHospital, Jyväskylä, Finland.Each author certifies that his or her institution has approved the humanprotocol for this investigation and that all investigations were conducted inconformity with ethical principles of research, and that informed consent wasobtained.Each author certifies that he or she has or may receive payments or benefitsfrom a commercial entity related to this work.One or more of the authors has received funding from the InstrumentariumScience Foundation, Finnish Cultural Foundation (North-Savo Foundation),Jyväskylä Central Hospital (Söderholm grant and grant B51), Sigrid Juseliusfoundation, and Finnish Orthopaedics and Traumatology Research Founda-tion.Correspondence to: Anna Vasara, MD, Vilkenintie 16A, FIN-00640, Hel-sinki, Finland. Phone: 358-405261552; Fax: 358-962274750; E-mail:[email protected]: 10.1097/01.blo.0000150567.00022.2e
CLINICAL ORTHOPAEDICS AND RELATED RESEARCHNumber 433, pp. 233–242© 2005 Lippincott Williams & Wilkins
233

Our aim was to systematically investigate the biome-chanical stiffness of repair tissue with arthroscopic inden-tation in patients having knee injury 1 year after autolo-gous chondrocyte transplantation. Our main hypothesiswas that the indentation stiffness of the repair tissue ap-proaches the values of adjacent cartilage after 1 year. Inaddition, we investigated if the osteochondritis dissecanslesions and full-thickness cartilage lesions were differentin stiffness. We also investigated the correlation of stiff-ness with the patient outcome scores and in four patientswith delayed gadolinium-enhanced MRI of the cartilagefor the GAG content of the repair tissue.
MATERIALS AND METHODS
We treated 32 patients with symptomatic chondral lesions of theknee with autologous chondrocyte transplantation between 1997and 2000. One patient was not willing to return for followuparthroscopy, and another was treated with autologous chondro-cyte transplantation combined with periosteal transplantation
without chondrocytes. Both were excluded from the study. Con-sequently, the study group consisted of 30 patients (18 men, 12women; 30 ± 9.0 years of age (mean ± SD); range, 16-47 years)with symptomatic chondral lesions in the knee treated with au-tologous chondrocyte transplantation (Table 1). The local ethicaland research committee approved the study plan and all patientsgave informed consent. All patients had full-thickness cartilagelesions (International Cartilage Repair Society classificationGrades III-IV); the mean lesion size was 6.8 ± 4.2 cm2 (range,1.6–20.4 cm2).
Autologous chondrocyte transplantation was done as de-scribed previously.5 Two operative procedures were needed inthe treatment, and the followup arthroscopy was the third pro-cedure in the protocol. First, arthroscopy was done to assess thecartilage lesion and to harvest cartilage for cell culture. Inden-tation stiffness of the cartilage was measured with an arthro-scopic indentation device (Artscan 1000, Artscan Oy, Helsinki,Finland) (Fig 1). The instrument allows measurement of com-pressive stiffness of articular cartilage from all joint surfaces ofthe knee, and it is possible to compare the biomechanical prop-erties of the graft and adjacent normal-looking cartilage. The
TABLE 1. Patient Information
PatientNumber Gender
Age(years) Site
Size(cm2) Diagnosis
AdditionalProcedures
1 M 25 MFC 1.6 Trauma2 F 22 MFC 9.4 OCD + Trauma3 F 35 MFC 9.0 Trauma High tibial valgus osteotomy + ACL reconstruction4 F 35 MFC 10.8 Unknown High tibial valgus osteotomy5 F 19 Patella 8.0 Trauma Elmslie-Trillat procedure6 M 47 MFC 2.3 Trauma7 F 36 MFC 7.2 Trauma High tibial valgus osteotomy8 F 25 LFC 8.8 Trauma9 M 32 PSF 2.5 Trauma
10 F 33 MFC 3.0 Trauma11 F 37 MFC 5.8 Trauma12 F 17 MFC 6.5 OCD13 M 25 MFC 9.0 Trauma High tibial valgus osteotomy14 F 39 MFC 3.1 Trauma ACL reconstruction15 M 28 MFC 7.0 Trauma High tibial valgus osteotomy + ACL reconstruction16 M 39 MFC 3.6 Trauma High tibial valgus osteotomy17 M 27 LFC 7.7 Trauma18 F 43 MFC 3.0 Trauma19 M 17 MFC 5.8 OCD20 M 25 MFC 2.6 Trauma21 M 47 MFC 10.1 Trauma ACL reconstruction24 M 32 MFC 8.7 OCD High tibial valgus osteotomy25 M 32 MFC 12.7 OCD26 M 17 LFC 11.6 OCD27 M 40 MFC 2.5 Trauma28 M 34 MFC 3.1 OCD31 M 29 MFC + PSF 20.4 OCD32 M 30 LTP 3.1 Trauma33 F 16 LFC 3.1 Trauma35 F 17 Patella 11.8 Chondromalacia
Average 30 6.8
OCD = osteochondritis dissecans; MFC = medial femoral condyle; LFC = lateral femoral condyle; PSF = patellar surface of the femur; LTP = lateral tibial plateau
Clinical Orthopaedicsand Related Research234 Vasara et al

arthroscopic indenter (1 mm diameter) introduces a small (300�m), constant indentation to the cartilage, and as an index ofcartilage stiffness, measures the force by which the tissue resiststhe indentation.23,25 The indenter was pressed 3 to 5 timesagainst the cartilage or repair tissue to get constant 10 N instan-taneous compressions. The average of the three highest indenterforces was calculated. The technically inadequate measurementswhen the compression force was not 10 N, or when measure-ments were not repeatable, were excluded. In 88% of the mea-surements at least three adequate values were measured. Themeasurement can be done only on cartilage with normal ornearly normal surface structure. Very thin or uneven cartilagewill give incorrect stiffness values. For uneven cartilage it isdifficult to produce a constant 10 N compression on the cartilageand the measurements are not repeatable. For thin cartilage(<1.5 mm) the indenter senses the underlying bone and theindenter forces are increased artificially, as indicated by thetheoretical model.13 With typical human cartilage thickness(1.5 mm–5.0 mm), the effect of variable cartilage thickness ismaximally 27%. Approximately 200–300 mg of healthy carti-lage was taken arthroscopically from the less-weightbearing sur-face. The cartilage sample was placed in a sterile test tube withsaline solution and then shipped within 24 hours to SahlgrenskaUniversity Hospital in Gothenburg for cell culture.
Chondrocyte culture was done as described previously.5,33,34
Briefly, the harvested cartilage was minced, and the chondro-cytes were isolated by enzymatic digestion for 24 hours andsubsequently cultured for 2–3 weeks in DMEM/F12 culture me-dium with addition of 10% of the patients’ own serum, produc-ing a suspension of 6–18 million cells. The cells were subjectedto thorough quality control for sterility and quality of the mor-phologic features of the cells. The chondrocytes were eitherfrozen for future use or suspended in 0.3–0.4 mL of implantationmedium (30 million cells/mL) and sent for implantation.
The second operation to transplant the cultured chondrocytesusually was done 3–4 weeks after the biopsy. A medial or lateralparapatellar incision was used. The damaged cartilage was de-brided to the subchondral bone. Next, a periosteal flap was har-vested from the anterior surface of the tibia (n � 22) or fromfemoral condyles (n � 8), and sutured over the cartilage lesionwith 6–0 resorbable interrupted sutures, except for a small part,where the cultured chondrocytes obtained in a sterile syringewere injected underneath the periosteum. Approximately onemillion chondrocytes were used per cm2 of the lesion. Flap clo-sure was completed with one suture and sealed with fibrin glue(Tisseel Duo Quick, Immuno AG, Vienna, Austria). The woundwas closed in layers. After transplantation partial weightbearing
was allowed for 8–12 weeks and high-impact activities were notrecommended until 1 year after the procedure.
On average, 1 year (range, 8–18 months) after the autologouschondrocyte transplantation the third procedure, an arthroscopywas done. The repair tissue was evaluated and the stiffness wasmeasured with an arthroscopic indentation device. The indenta-tion of the adjacent cartilage 5–10 mm from the lesion and theother joint areas was done. The stiffness of the repair tissue wasnormalized by the adjacent cartilage stiffness. Normalized stiff-ness (percent) was calculated as the indentation stiffness of therepair tissue normalized by the value of the adjacent cartilage(Fig 1). Three lesions on a lateral condyle were so large thatpostoperatively the adjacent cartilage measurements could not bedone. In these cases the preoperative value of adjacent cartilagewas used to calculate the normalized stiffness.
The clinical results were evaluated with the score of Brittberget al (patients’ subjective evaluation),5 Lysholm functionalscore,22 Tegner activity score,38 and the International CartilageRepair Society (ICRS) standard evaluation (Cartilage StandardEvaluation Form/Knee) preoperatively and 1 year postopera-tively.
Four male patients (28 ± 12 years; range, 18–41 years) withautologous chondrocyte transplantation in the medial or lateralfemoral condyles were studied 12–18 months postoperativelywith indentation measurements and delayed gadolinium-enhanced MRI of cartilage that indirectly reflects the cartilagePG concentration.3 The delayed gadolinium-enhanced MRI ofcartilage experiments were done according to the publishedprotocol.9 Accordingly, an intravenous administration of 0.2mmol/kg (0.4 mL/kg; ie, double dose) of Gd-DTPA2- (Magne-vist, Schering AG, Berlin, Germany) was followed by 10 min-utes of knee-bending exercises. T1 relaxation time in the pres-ence of Gd-DTPA2– or the delayed gadolinium-enhanced MRI ofcartilage index, was determined from T1-weighted images mea-sured within 2–3 hours after injection using a single-slice inver-sion recovery fast spin echo sequence in coronal and sagittalorientations (3 mm slice; TE � 30 ms; TR � 2000; seven TIsbetween 25–1600 ms, echo train length of 7; FOV � 290 mm;512 * 512 matrix; imaging time of 17 minutes for one slice). Ithas been shown that the measured delayed gadolinium-enhancedMRI of cartilage index (T1) values are approximately linearlyrelated to the GAG content of the tissue.3,9,29 The values fordelayed gadolinium-enhanced MRI of cartilage index and inden-tation force of autologous chondrocyte transplantation graftswere compared with the values of the adjacent cartilage. In onecase no indentation measurement adjacent to the graft could bedone and the values of the other unoperated condyle were used.
Fig 1A–B. A drawing of the arthroscopiccartilage indentation device is shown. (B)The indentation stiffness measurement ofthe repair tissue site (small arrow) and ad-jacent tissue site (large arrow) are shown.
Number 433April 2005 Indentation Stiffness of Repair Tissue 235

Conventional MRI of the knee with T1-weighted (sagittal), T1-weighted fat-suppressed (coronal plane), T2-weighted protondensity fat-suppressed (sagittal), and T2-weighted proton density(transverse) images was done postoperatively for additional fivepatients, and the cartilage repair areas were analyzed for thefollowing characteristics: the signal characteristics of the repairtissue, the morphologic features of the graft and filling of thedefect, the degree of integration of the graft with the adjacentnative cartilage and subchondral bone, and the status of thesubchondral bone plate and marrow.1 All studies were done us-ing a Siemens Magnetom Impact 1.0 T system (Siemens, Erlan-gen, Germany).
Statistical analysis was done with SPSS 9.0 statistical soft-ware (SPSS Inc., Chicago, IL). Comparisons of the differencesbetween the groups were analyzed using the Wilcoxon matched-pairs signed-ranks test and the Mann-Whitney U test. Spear-man’s nonparametric correlation analysis was used to study theeffects of different factors on patient outcome. The level ofstatistical significance was set at a p of 0.05.
RESULTS
During the 1-year followup, the stiffness of the repair tis-sue improved to 62% of that in the adjacent cartilage(Table 2). In six patients the indentation force of the repairtissue was more than 80% of the adjacent cartilage, sug-gesting probably hyaline-like repair.33 The highest relativevalue was 141% which occurred owing to abnormally lowadjacent cartilage value (1.88 N) and repair tissue value(2.7 N) that approached normal cartilage stiffness. In thiscase, the medial femoral cartilage already was soft duringthe preoperative measurement. The indentation values ofthe cartilage adjacent to the repair site did not changeduring the followup (mean, 3.4 ± 1.12 N [n � 26] versus3.58 ± 1.04 N [n � 23]). The indentation stiffness of themedial tibial plateau decreased during the followup,whereas no changes were detected on other cartilage sur-
TABLE 2. International Cartilage Repair Society Arthroscopic Grading of the Grafts
PatientNumber
FollowupArthroscopy
(months)DefectFilling Integration
MacroscopicAppearance
Total Gradeat 1 Year
NormalizedStiffness
1 13 4 3 4 11 52%2 13 4 4 3 11 33%3 12 1 3 0 4 —3 (2 ACT) 12 2 3 4 9 85%4 15 3 2 3 8 70%5 12 4 3 3 10 —6 12 2 2 3 7 —7 6 2 1 3 6 —7 (2 ACT) 8 2 1 4 7 52%8 12 3 2 4 9 102%9 12 4 2 4 10 62%
10 13 3 3 2 8 141%11 12 4 3 3 10 75%12 12 4 3 3 10 82%13 12 4 3 3 10 39%14 12 4 3 3 10 31%15 12 4 3 3 10 55%16 13 4 4 4 12 97%17 12 4 3 3 10 47%18 12 4 4 4 12 94%19 18 4 2 3 9 38%20 12 4 3 4 11 48%21 12 3 3 3 9 51%24 15 4 3 3 10 56%25 13 4 3 3 10 79%26 12 3 4 4 11 31%27 12 4 3 4 11 31%28 12 4 3 3 10 27%31 MFC 12 3 2 4 9 31%31 PSF 12 4 4 4 12 —32 12 4 3 3 10 60%33 12 4 4 3 11 71%35 12 4 4 3 11 —Average 12 3.6 2.9 3.2 9.7 62%
ACT = autologous chondrocyte transplantation; MFC = medial femoral condyle; PSF = patellar surface of the femur
Clinical Orthopaedicsand Related Research236 Vasara et al
faces (Table 3). The mean indentation force of the repairtissue was 2.04 ± 0.83 N.
The indentation stiffness of the osteochondritis disse-cans lesion repairs (1.45 ± 0.46 N; n � 7) was less (p <0.01) than that of the non-osteochondritis dissecans lesionrepair sites (2.37 ± 0.72 N; n � 19). The mean normalizedcartilage stiffness of the osteochondritis dissecans lesionrepair sites was less (p � 0.06) than in the repair sites oftraumatic lesions (46% [n � 7] versus 68% [n � 19]).However, there were no differences in the arthroscopicICRS grades of the repairs between these two groups.
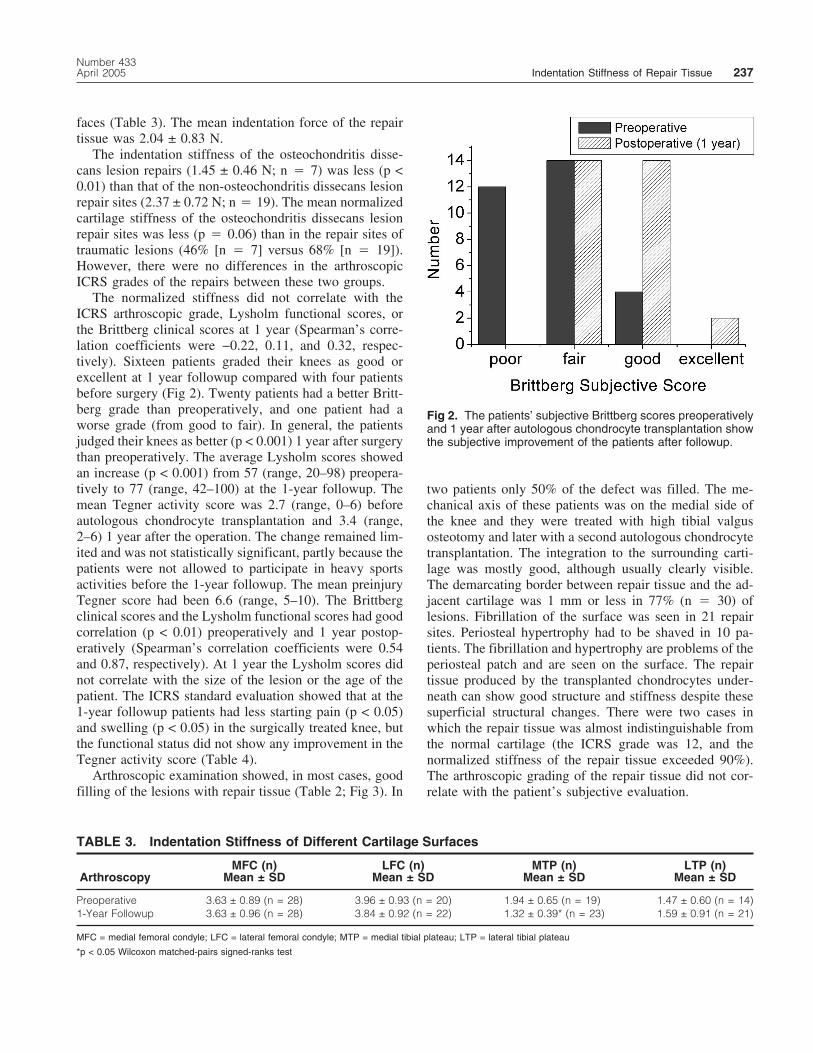
The normalized stiffness did not correlate with theICRS arthroscopic grade, Lysholm functional scores, orthe Brittberg clinical scores at 1 year (Spearman’s corre-lation coefficients were −0.22, 0.11, and 0.32, respec-tively). Sixteen patients graded their knees as good orexcellent at 1 year followup compared with four patientsbefore surgery (Fig 2). Twenty patients had a better Britt-berg grade than preoperatively, and one patient had aworse grade (from good to fair). In general, the patientsjudged their knees as better (p < 0.001) 1 year after surgerythan preoperatively. The average Lysholm scores showedan increase (p < 0.001) from 57 (range, 20–98) preopera-tively to 77 (range, 42–100) at the 1-year followup. Themean Tegner activity score was 2.7 (range, 0–6) beforeautologous chondrocyte transplantation and 3.4 (range,2–6) 1 year after the operation. The change remained lim-ited and was not statistically significant, partly because thepatients were not allowed to participate in heavy sportsactivities before the 1-year followup. The mean preinjuryTegner score had been 6.6 (range, 5–10). The Brittbergclinical scores and the Lysholm functional scores had goodcorrelation (p < 0.01) preoperatively and 1 year postop-eratively (Spearman’s correlation coefficients were 0.54and 0.87, respectively). At 1 year the Lysholm scores didnot correlate with the size of the lesion or the age of thepatient. The ICRS standard evaluation showed that at the1-year followup patients had less starting pain (p < 0.05)and swelling (p < 0.05) in the surgically treated knee, butthe functional status did not show any improvement in theTegner activity score (Table 4).
Arthroscopic examination showed, in most cases, goodfilling of the lesions with repair tissue (Table 2; Fig 3). In
two patients only 50% of the defect was filled. The me-chanical axis of these patients was on the medial side ofthe knee and they were treated with high tibial valgusosteotomy and later with a second autologous chondrocytetransplantation. The integration to the surrounding carti-lage was mostly good, although usually clearly visible.The demarcating border between repair tissue and the ad-jacent cartilage was 1 mm or less in 77% (n � 30) oflesions. Fibrillation of the surface was seen in 21 repairsites. Periosteal hypertrophy had to be shaved in 10 pa-tients. The fibrillation and hypertrophy are problems of theperiosteal patch and are seen on the surface. The repairtissue produced by the transplanted chondrocytes under-neath can show good structure and stiffness despite thesesuperficial structural changes. There were two cases inwhich the repair tissue was almost indistinguishable fromthe normal cartilage (the ICRS grade was 12, and thenormalized stiffness of the repair tissue exceeded 90%).The arthroscopic grading of the repair tissue did not cor-relate with the patient’s subjective evaluation.
TABLE 3. Indentation Stiffness of Different Cartilage Surfaces
ArthroscopyMFC (n)
Mean ± SDLFC (n)
Mean ± SDMTP (n)
Mean ± SDLTP (n)
Mean ± SD
Preoperative 3.63 ± 0.89 (n = 28) 3.96 ± 0.93 (n = 20) 1.94 ± 0.65 (n = 19) 1.47 ± 0.60 (n = 14)1-Year Followup 3.63 ± 0.96 (n = 28) 3.84 ± 0.92 (n = 22) 1.32 ± 0.39* (n = 23) 1.59 ± 0.91 (n = 21)
MFC = medial femoral condyle; LFC = lateral femoral condyle; MTP = medial tibial plateau; LTP = lateral tibial plateau
*p < 0.05 Wilcoxon matched-pairs signed-ranks test
Fig 2. The patients’ subjective Brittberg scores preoperativelyand 1 year after autologous chondrocyte transplantation showthe subjective improvement of the patients after followup.
Number 433April 2005 Indentation Stiffness of Repair Tissue 237

Quantitative MRI showed repair tissue delayed gado-linium-enhanced MRI of cartilage index values that werecomparable to the values of control tissue indicating re-plenished GAG concentration (Fig 5; Table 5). The MRIscans showed that in all 11 patients the lesions were com-pletely filled with repair tissue and the repair tissue waseither on the level of the surrounding cartilage or slightlythicker. In the osteochondritis dissecans lesions (n � 5),the repair tissue filled the bony defect and had returned thecontour of the condyle and the thickness of the cartilage(Fig 4). These MRI findings were verified by arthroscopyfindings. The signal intensity of the repair tissue was car-tilage-like, but mild heterogeneity of the signal was seen.The junction between repair tissue and adjacent cartilageappeared indistinguishable from cartilage in all repairs. Nodelamination of the grafts was seen. The subchondral boneplate beneath the repair tissue was normal or showed mini-mal bright signal in six patients. Edema-like signal in thebone marrow was seen in three patients 12 months aftercartilage repair.
DISCUSSION
The goal of cartilage repair is to obtain a mechanicallydurable graft that can resist high-impact loading and wearand tear in the joints. Consequently, the rationale in chon-drocyte transplantation is that the cells injected to the le-
sion site produce extracellular matrix, which matures withtime forming optimally a resilient, hyaline-like graft.5 Ourstudy showed that 1 year after autologous chondrocytetransplantation the stiffness of the graft can reach the stiff-ness level of the adjacent cartilage, but the variation in thestiffness of the repair tissue was great.
One of the major limitations of our study was the lackof histologic samples, and more studies are needed to cor-relate the stiffness with the histology or the graft. One-yearfollowup is relatively short for evaluation of clinical re-sults. The time of arthroscopy and indentation was set at 1year after surgery because it was shown that at 1 year thegraft can withstand more strenuous loading.5 However, itis possible that the graft maturation continues, and stiff-ness and the clinical results would change with longerfollowup. The indenter device was designed to be used ina clinical setting when the cartilage thickness informationis not available. Cartilage thickness can affect the stiffnessmeasurements especially when the thickness is less thanthe normal range (less than 1.5 mm). For thin cartilage (<1.5 mm), the indenter senses the underlying bone and theindenter forces are increased artificially, as indicated bythe theoretical model.13 With typical human cartilagethickness (1.5–5.0 mm) the effect of variable cartilagethickness is maximally 27%. Precision analysis of the in-dentation instrument with cartilage tissue has shown thatthe coefficient of variation is 11%.26,27 The indentationinstrument measures instantaneous stiffness characteris-tics, and it reflects sensitively alterations in the PG con-centration4,24 and superficial collagen layer of articularcartilage.21 It has been shown that indentation stiffness hasa good correlation with the histologic quality of cartilageand repair tissue.10,33 The Artscan 1000 instrument mustbe placed perpendicular to the cartilage, which sometimesis technically demanding. All measurements were done byone surgeon who is experienced with the instrument.Technically inadequate measurements were excluded. Themeasurements of the adjacent cartilage were done 5–10mm from the lesion on normal-looking cartilage. The mea-surement sites were variable because of the variability ofthe lesions. The stiffness values are instrument specificand cannot be directly compared with values from otherindentation instruments.
The great topographic and individual variation of car-tilage stiffness in human knees (from 2.4 ± 0.8 N in themedial plateau of the tibia to 5.6 ± 1.2 N in the lateralcondyle of the femur),26 made it necessary and practical tonormalize the indenter force values of the grafts with thestiffness of the adjacent cartilage outside the repair area.Biomechanical analysis showed that in six patients (20%),normalized stiffness of the graft was reestablished to 80%or greater. In these grafts the range of the indenter forcevalues was from 2.5–4.1 N, which is at or near the level of
TABLE 4. Subjective Results Evaluated with theCartilage Standard Evaluation Form/Knee (ICRS)
Parameter
Preoperative Postoperative
Mean Median Mean Median
Functional status* 3.4 4.0 2.8 3.0Compared to healthy
knee your knee isworth* 3.0 3.0 2.5 2.0
Visual analog scale,pain* 2.4 2.5 2.1 2.0
How does your kneefunction?* 3.0 3.0 2.0 2.0
Patients painassessment* 2.5 3.0 2.0 2.0
Pain at activity level† 3.8 4.0 3.1 3.0Swelling at activity
level† (p < 0.05) 3.5 4.0 2.5 3.0Giving way at activity
level† 3.2 4.0 2.4 2.0Starting pain at activity
level† (p < 0.05) 3.6 4.0 2.6 3.0
*All scores from 1–4 where 4 is severely abnormal, 3 is abnormal, 2 is nearlynormal, and 1 is normal or the †activity level of 4 is sedentary work (activities ofdaily living); 3 is light manual work, jogging, running; 2 is heavy manual work,skiing, tennis; 1 is jumping, pivoting, cutting, football, soccer
Statistical testing done with Wilcoxon matched-paired signed-ranks test, n = 17
Clinical Orthopaedicsand Related Research238 Vasara et al

normal cartilage stiffness.26 There was no correlation be-tween the ICRS arthroscopic grades and the stiffness mea-surements. The stiffness relates to the biochemical char-acters of the graft which can vary in the graft. The ICRSgrades, however, are dependent on the macroscopic quali-ties of the repair on the whole.
Earlier studies showing comparisons of the histologiccharacteristics of the repair tissue with the stiffness valuessuggested that the grafts, having indentation values nearthose of the adjacent cartilage, were histologically hyaline-like.20,33 The quantity of the grafts with optimal biome-chanical quality in this study is in accordance with theresults of Roberts et al,37 who reported that 22% of theirpatients who had autologous chondrocyte transplantationhad histologically hyaline-like repair. In the current study,
two patients had maximal ICRS scores and their normal-ized indentation values were greater than 90%. This mayindicate that, at its best, autologous chondrocyte transplan-tation can produce repair tissue that is visually and bio-mechanically similar to normal articular cartilage.
In eight patients (27%) the normalized stiffness valueswere less than 40%, and the indenter force values wereless than 1.8 N, suggesting incomplete maturation of thegraft, or fibrous type of repair.20,33 Five of these sevenpatients had osteochondritis dissecans lesions. We alsoobserved that cartilage stiffness was less in osteochondritisdissecans lesion repair sites than in grafts of the traumaticlesions. This can be explained partly by the larger tissuethickness of the osteochondritis dissecans lesion grafts.Macroscopically the repairs of osteochondritis dissecanslesions were similar to repairs of traumatic lesions. Thesofter graft may indicate slower maturation of the thickergrafts that fill the bony defect and the cartilage defect. It ispossible that the softer osteochondritis dissecans lesionrepair sites are more vulnerable to injuries than other re-pair types. It was shown that the maturation of the graftlasts more than 1 year and may vary.35 Also the subchon-dral bone formation continues for more than 2 years.35 Inrabbits the repair tissue showed significant maturation be-tween 12 and 52 weeks postoperatively, when full thick-ness chondral defects were repaired with autologous chon-drocyte transplantation.6 Also, the clinical results continueto improve as much as 2 years or more, which can bepartially attributable to the maturation of the repair tissuewith time.28,34 It also was shown that the repair tissue9–30 months after autologous chondrocyte transplantationstains for Type II collagen propeptide and Type II collagendenaturation product (Col2-3/4m), suggesting ongoingcollagen turnover.36
Fourteen patients (48%) had midrange stiffness valuesand the normalized stiffness of the grafts remained be-tween 40% and 80%. The corresponding indenter forcevalues varied from 1.7–2.5 N. Therefore, these compres-sive stiffness values were less than in the adjacent tissueand also less than those observed earlier in uninjured nor-mal cartilage,26 and the grafts may be susceptible to injuryin heavy loading. The maturation process might be incom-
Fig 4. A T1-weighted MRI scan of Patient 19 showed a thickgraft completely filling the bony and cartilage defects of osteo-chondritis dissecans with the autologous chondrocyte trans-plantation graft.
Fig 3A–C. (A) The cartilage lesion of Pa-tient 27 is shown via arthroscopy at thetime of the biopsy, (B) during the autolo-gous chondrocyte transplantation opera-tion after suturing the periosteum patchover the lesion, and (C) again 1 year afterthe autologous chondrocyte transplanta-tion. Good filling of the defect occurred.
Number 433April 2005 Indentation Stiffness of Repair Tissue 239

plete in these repairs, but it also is possible that these graftsconsisted of mixed fibrous and hyaline-like repair tissue.In an earlier report, 48% of patients treated with autolo-gous chondrocyte transplantation had histologically hya-line and fibrous mixed repair.37 This could be explainedpartly by the incorporation of periosteal fibrous tissue as asurface layer of the repair tissue. These figures show thevariability in the repair tissue quality and the ability of theindentation instrument to detect the differences in the bio-mechanical properties of the grafts.
Clinical outcome, as assessed with the Lysholm func-tional score and Tegner activity score, did not correlatewith the biomechanical properties of the graft. The re-stricted activity level of the patients during the first post-operative year may have contributed to this result. As all
lesions, except two, were completely covered with therepair tissue, it is probable that even a soft graft couldwithstand the nonstrenuous, low-impact type of loading.However, mechanical loading of the joint is essential forthe well-being of articular cartilage, and patients shouldparticipate in an individual physical therapy and exerciseprogram. Previous animal experiments showed that gradu-ally increased weightbearing and more impact type ofloading are necessary to increase PG content, collagenorientation, and biomechanical properties of articular car-tilage, although exercise that is too intensive may causedeterioration of articular cartilage.14–19 It would be ofenormous value to learn the optimal level of physical ac-tivity, which would improve the biomechanical propertiesof the repair tissue. Individual activity and rehabilitation
TABLE 5. Indentation Force Compared with Delayed Gadolinium-Enhanced MRI of Cartilage (dGEMRIC)Index (T1)
PatientNumber
ArthroscopicFinding
ICRS GradeGraft(N)
IndentationForce
Control (N)
Ratio(percent ofcontrol site)
Graft (ms)Mean ± SD
dGEMRICControl (ms)Mean ± SD
Ratio(percent ofcontrol site)
27 11 1.8 5.7 31 388 ± 54 426 ± 44 9126 11 1.2 4.0 31 421 ± 52 366 ± 55 11519 9 1.3 3.3 38 381 ± 60 422 ± 64 9028 10 0.9 3.2 27 470 ± 44 339 ± 67 139
Fig 5. A delayed gadolinium-enhanced MRI of cartilage map is shown (T1 relaxation time in milliseconds) of cartilage proteo-glycans in autologous chondrocyte transplantation (graft indicated with arrow) is shown. The repair tissue shows T1 valuescomparable to values of adjacent and remote control tissue indicating replenished GAG content of the graft.
Clinical Orthopaedicsand Related Research240 Vasara et al

profiles have been created and used for the first year basedon experience. The results of this 1-year evaluation ar-throscopy and indentation analysis support a gradual andindividual rehabilitation program after autologous chon-drocyte transplantation.
The quantitative MRI of the repair tissue showed de-layed gadolinium-enhanced MRI of cartilage indices com-parable to those of the control site. This suggests that thePG content of the repair tissue was replenished after theautologous chondrocyte transplantation. These results arein accordance with an earlier delayed gadolinium-enhanced MRI of cartilage study of autologous chondro-cyte transplantation grafts on humans showing that the PGcontent is less 2–6 months after autologous chondrocytetransplantation and is elevated to the level of the controlsites 12–24 months postoperatively.11 Despite the high PGcontent of the grafts in the four patients, the correspondingstiffness values of the repair tissue remained low. There-fore, the high PG content of the graft does not necessarilyindicate optimal biomechanical properties of the repair.Although PG is essential for compressive stiffness of ar-ticular cartilage, the collagen network is important for theelastic properties of the tissue.2 Not only collagen content,but also the structure and organization of collagen affectthe stiffness properties.21 It is possible that the reasons forthe poor mechanical characteristics of these grafts were anincomplete maturation process and insufficient organiza-tion of the collagen network. Three of the four samplesanalyzed by delayed gadolinium-enhanced MRI of carti-lage were deep osteochondritis dissecans lesion repairs, inwhich the repair tissue filled the bony and cartilage de-fects, and which most probably require a longer time formaturation. We assume that the closer the collagen net-work organization gets to normal cartilage structure themore likely the biomechanical properties approach thenormal values. This probably also would mean more du-rable repair tissue. However, additional investigations areneeded to evaluate the relationship between histologicanalysis and biomechanical properties of the grafts. T2relaxation time mapping, another quantitative MRI tech-nique that may provide information about the collagenintegrity and organization of the repair tissue might beused in future studies.30,32
The repair tissue stiffness could in some cases reach thesame level as the adjacent cartilage stiffness, but there wasgreat variation in the biomechanical properties of thegrafts and the osteochondritis dissecans lesions generallyhad softer grafts. Cartilage repair sites of the knee showedpredominantly good filling with repair tissue 1 year afterautologous chondrocyte transplantation. The stiffness didnot correlate with the macroscopic appearance of the graft.The patients experienced less pain and swelling of theknee than preoperatively, and the function of the knee was
better, but the activity level did not show improvement at1 year; partly because high-impact sports activities werenot allowed before the 1-year followup. The delayed gad-olinium-enhanced MRI of cartilage analysis of four pa-tients showed that the PG concentration of the repair tissuehad replenished during the followup. However, the samegrafts had very low stiffness values, indicating that PGconcentration does not necessarily fully characterize bio-mechanical properties of the graft. Additional studies areneeded to assess how the stiffness values at 1 year corre-late with the long-term durability of autologous chondro-cyte transplantation.
AcknowledgmentsWe thank physiotherapist Mirja Vuorenmaa from JyväskyläCentral Hospital for patient evaluation, Eeva Elomaa, MD,Jarmo Toivanen, PhD, and Tuija Järviluoma, MD, from the De-partment of Radiology, Jyväskylä Central Hospital for assistancewith MRI and radiograph analysis, and Mikko Laasanen, MSc,from Kuopio University for drawings.
References1. Alparslan L, Minas T, Winalski CS: Magnetic resonance imaging of
autologous chondrocyte implantation. Semin Ultrasound CT MR22:341–351, 2001.
2. Bader DL, Kempson GE, Egan J, Gilbey W, Barrett AJ: The effectsof selective matrix degradation on the short-term compressive prop-erties of adult human articular cartilage. Biochim Biophys Acta1116:147–154, 1992.
3. Bashir A, Gray ML, Hartke J, Burstein D: Nondestructive imagingof human cartilage glycosaminoglycan concentration by MRI.Magn Reson Med 41:857–865, 1999.
4. Brama PA, Barneveld A, Karssenberg D, Van Kampen GP, vanWeeren PR: The application of an indenter system to measure struc-tural properties of articular cartilage in the horse: Suitability of theinstrument and correlation with biochemical data. J Vet Med APhysiol Pathol Clin Med 48:213–221, 2001.
5. Brittberg M, Lindahl A, Nilsson A, et al: Treatment of deep carti-lage defects in the knee with autologous chondrocyte transplanta-tion. N Engl J Med 331:889–895, 1994.
6. Brittberg M, Nilsson A, Lindahl A, Ohlsson L, Peterson L: Rabbitarticular cartilage defects treated with autologous cultured chondro-cytes. Clin Orthop 326:270–283, 1996.
7. Brittberg M, Tallheden T, Sjögren-Jansson B, Lindahl A, PetersonL: Autologous chondrocytes used for articular cartilage repair: Anupdate. Clin Orthop 391(Suppl):S337–S348, 2001.
8. Burstein D, Gray M: New MRI techniques for imaging cartilage. JBone Joint Surg 85A(Suppl 2):70–77, 2003.
9. Burstein D, Velyvis J, Scott KT, et al: Protocol issues for delayedGd(DTPA)(2-)-enhanced MRI (dGEMRIC) for clinical evaluationof articular cartilage. Magn Reson Med 45:36–41, 2001.
10. Franz T, Hasler EM, Hagg R, et al: In situ compressive stiffness,biochemical composition, and structural integrity of articular carti-lage of the human knee joint. Osteoarthritis Cartilage 9:582–592,2001.
11. Gillis A, Bashir A, McKeon B, et al: Magnetic resonance imagingof relative glycosaminoglycan distribution in patients with autolo-gous chondrocyte transplants. Invest Radiol 36:743–748, 2001.
12. Grande DA, Pitman MI, Peterson L, Menche D, Klein M: The repairof experimentally produced defects in rabbit articular cartilage byautologous chondrocyte transplantation. J Orthop Res 7:208–218,1989.
Number 433April 2005 Indentation Stiffness of Repair Tissue 241

13. Hayes WC, Keer LM, Herrmann G, Mockros LF: A mathematicalanalysis for indentation tests of articular cartilage. J Biomech5:541–551, 1972.
14. Helminen HJ, Hyttinen MM, Lammi MJ, et al: Regular joint loadingin youth assists in the establishment and strengthening of the col-lagen network of articular cartilage and contributes to the preven-tion of osteoarthrosis later in life: A hypothesis. J Bone MinerMetab 18:245–257, 2000.
15. Jurvelin J, Kiviranta I, Tammi M, Helminen HJ: Effect of physicalexercise on indentation stiffness of articular cartilage in the canineknee. Int J Sports Med 7:106–110, 1986.
16. Kiviranta I, Jurvelin J, Tammi M, Säämänen AM, Helminen HJ:Weight bearing controls glycosaminoglycan concentration and ar-ticular cartilage thickness in the knee joints of young beagle dogs.Arthritis Rheum 30:801–809, 1987.
17. Kiviranta I, Tammi M, Arokoski J, et al: Effects of mechanicalloading and immobilization on the articular cartilage. Baillière’sClinical Orthopaedics 2:109–122, 1997.
18. Kiviranta I, Tammi M, Jurvelin J, et al: Articular cartilage thicknessand glycosaminoglycan distribution in the canine knee joint afterstrenuous running exercise. Clin Orthop 283:302–308, 1992.
19. Kiviranta I, Tammi M, Jurvelin J, Säämänen AM, Helminen HJ:Moderate running exercise augments glycosaminoglycans andthickness of articular cartilage in the knee joint of young beagledogs. J Orthop Res 6:188–195, 1988.
20. Kiviranta I, Vasara A, Lindahl A, Peterson L: Stiffness of the repairtissue one to seven years after autologous chondrocyte transplanta-tion of chondral lesions. Trans Orthop Res Soc 26:199, 2001.
21. Korhonen RK, Wong M, Arokoski J, et al: Importance of the su-perficial tissue layer for the indentation stiffness of articular carti-lage. Med Eng Phys 24:99–108, 2002.
22. Lysholm J, Gillquist J: Evaluation of knee ligament surgery resultswith special emphasis on use of a scoring scale. Am J Sports Med10:150–154, 1982.
23. Lyyra T: Development, Validation and Clinical Application of In-dentation Technique for Arthroscopic Measurement of CartilageStiffness. Kuopio, Finland: University of Kuopio, 1–99, 1997.
24. Lyyra T, Arokoski JP, Oksala N, et al: Experimental validation ofarthroscopic cartilage stiffness measurement using enzymaticallydegraded cartilage samples. Phys Med Biol 44:525–535, 1999.
25. Lyyra T, Jurvelin J, Pitkänen P, Väätäinen U, Kiviranta I: Indenta-
tion instrument for the measurement of cartilage stiffness underarthroscopic control. Med Eng Phys 17:395–399, 1995.
26. Lyyra T, Kiviranta I, Väätäinen U, Helminen HJ, Jurvelin JS: Invivo characterization of indentation stiffness of articular cartilage inthe normal human knee. J Biomed Mater Res 48:482–487, 1999.
27. Lyyra-Laitinen T, Niinimäki M, Töyräs J, et al: Optimization of thearthroscopic indentation instrument for the measurement of thincartilage stiffness. Phys Med Biol 44:2511–2524, 1999.
28. Minas T: Autologous chondrocyte implantation for focal chondraldefects of the knee. Clin Orthop 391(Suppl):S349–S361, 2001.
29. Nieminen MT, Rieppo J, Silvennoinen J, et al: Spatial assessment ofarticular cartilage proteoglycans with Gd-DTPA- enhanced T1 im-aging. Magn Reson Med 48:640–648, 2002.
30. Nieminen MT, Rieppo J, Töyräs J, et al: T2 relaxation revealsspatial collagen architecture in articular cartilage: A comparativequantitative MRI and polarized light microscopic study. Magn Re-son Med 46:487–493, 2001.
31. Nieminen MT, Töyräs J, Laasanen MS, et al: Prediction of biome-chanical properties of articular cartilage with quantitative magneticresonance imaging. J Biomech 37:321–328, 2004.
32. Nieminen MT, Töyräs J, Rieppo J, et al: Quantitative MR micros-copy of enzymatically degraded articular cartilage. Magn ResonMed 43:676–681, 2000.
33. Peterson L, Brittberg M, Kiviranta I, Akerlund EL, Lindahl A:Autologous chondrocyte transplantation: Biomechanics and long-term durability. Am J Sports Med 30:2–12, 2002.
34. Peterson L, Minas T, Brittberg M, et al: Two- to 9-year outcomeafter autologous chondrocyte transplantation of the knee. Clin Or-thop 374:212–234, 2000.
35. Peterson L, Minas T, Brittberg M, Lindahl A: Treatment of osteo-chondritis dissecans of the knee with autologous chondrocyte trans-plantation: Results at two to ten years. J Bone Joint Surg85A:17–24, 2003.
36. Roberts S, Hollander AP, Caterson B, Menage J, Richardson JB:Matrix turnover in human cartilage repair tissue in autologous chon-drocyte implantation. Arthritis Rheum 44:2586–2598, 2001.
37. Roberts S, McCall IW, Darby AJ, et al: Autologous chondrocyteimplantation for cartilage repair: Monitoring its success by mag-netic resonance imaging and histology. Arthritis Res Ther5:R60–R73, 2003.
38. Tegner Y, Lysholm J: Rating systems in the evaluation of kneeligament injuries. Clin Orthop 198:43–49, 1985.
Clinical Orthopaedicsand Related Research242 Vasara et al
Related Documents











