C 2009, the Authors Journal compilation C 2009, Wiley Periodicals, Inc. DOI: 10.1111/j.1540-8175.2009.00952.x RESEARCH FROM THE UNIVERSITY OF ALABAMA AT BIRMINGHAM Incremental Value of Live/Real Time Three-Dimensional Transthoracic Echocardiography in the Assessment of Right Ventricular Masses Venkataramana K. Reddy, M.D., ∗ Michael Faulkner, M.D., ∗ Naveen Bandarupalli, M.D., ∗ Navin C. Nanda, M.D., ∗ Preeti Singh, M.D., ∗ Rajarshi Dutta, M.B.B.S., ∗ Anurag Singh, M.D., ∗ Koteswara R. Pothineni, M.D., M.P.H., ∗ Harvinder S. Dod, M.D.,† Ravindra Bhardwaj, M.B.B.S., M.P.H.,† Bradford E. Warden, M.D.,† Robert J. Beto, M.D.,† and Abnash C. Jain, M.D. ∗ ∗ Division of Cardiovascular Disease, University of Alabama at Birmingham, Birmingham, Alabama, and †Department of Medicine, Section of Cardiology, WestVirginia University, Morgantown, West Virginia This case series demonstrates the incremental value of three-dimensional transthoracic echocardio- graphy (3D TTE) over two-dimensional transthoracic echocardiography (2D TTE) in the assessment of 11 patients with right ventricular (RV) masses or mass-like lesions (three cases of RV thrombus, one myxoma, one fibroma, one lipoma, one chordoma, and one sarcoma and three cases of RV non- compaction, which are considered to be mass-like in nature). 3D TTE was of incremental value in the assessment of these masses in that 3D TTE has the capacity to section the mass and view it from multiple angles, giving the examiner a more comprehensive assessment of the mass. This was particu- larly helpful in the cases of thrombi, as the presence of echolucencies indicated clot lysis. In addition, certainty in the number of thrombi present was an advantage of 3D TTE. Also, sectioning of cardiac tumors allowed more confidence in narrowing the differential diagnosis of the etiology of the mass. In addition, 3D TTE allowed us to identify precise location of the attachments of the masses as well as to determine whether there were mobile components to the mass. Another noteworthy advantage of 3D TTE was that the volumes of the masses could be calculated. Additionally, the findings by 3D TTE correlated well with pathologic examination of RV tumors, and some of the masses measured larger by 3D TTE than by 2D TTE, which was also validated in one case by surgery. As in the case of RV fibroma, another advantage was that 3D TTE actually identified more masses than 2D TTE. RV noncompaction was also well studied, and the assessment with 3D TTE helped to give a more definitive diagnosis in these patients. (ECHOCARDIOGRAPHY, Volume 26, May 2009) real time three-dimensional transthoracic echocardiography, three-dimensional echocardiography, two-dimensional echocardiography, right ventricular noncompaction, right ventricular mass, chor- doma, myxoma, lipoma, fibroma, right ventricular thrombus Real time two-dimensional transthoracic echocardiography (2D TTE) has proven use- ful in the detection of cardiac masses. 1 More recently, three-dimensional transthoracic echo- Address for correspondence and reprint requests: Navin C. Nanda, M.D., University of Alabama at Birmingham, Heart Station, SWB/S102, 619 19th Street South, Birmingham, AL 35249. Fax: 205-934-6747; E-mail: [email protected] cardiography (3D TTE) has also been utilized to evaluate these mass lesions. 2–4 In this study, we report 11 cases of right ventricular (RV) masses and mass-like lesions that were eval- uated by 2D TTE and also with 3D TTE. The cases include three cases of RV thrombus, one myxoma, one fibroma, one lipoma, one chor- doma, one sarcoma, and three cases of RV noncompaction. 598 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 26, No. 5, 2009

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
C© 2009, the AuthorsJournal compilation C© 2009, Wiley Periodicals, Inc.DOI: 10.1111/j.1540-8175.2009.00952.x
RESEARCH FROM THE UNIVERSITY OF ALABAMA ATBIRMINGHAM
Incremental Value of Live/Real TimeThree-Dimensional TransthoracicEchocardiography in the Assessmentof Right Ventricular MassesVenkataramana K. Reddy, M.D.,∗ Michael Faulkner, M.D.,∗ Naveen Bandarupalli, M.D.,∗
Navin C. Nanda, M.D.,∗ Preeti Singh, M.D.,∗ Rajarshi Dutta, M.B.B.S.,∗ Anurag Singh, M.D.,∗
Koteswara R. Pothineni, M.D., M.P.H.,∗ Harvinder S. Dod, M.D.,†Ravindra Bhardwaj, M.B.B.S., M.P.H.,† Bradford E. Warden, M.D.,† Robert J. Beto, M.D.,†and Abnash C. Jain, M.D.∗
∗Division of Cardiovascular Disease, University of Alabama at Birmingham, Birmingham,Alabama, and †Department of Medicine, Section of Cardiology, West Virginia University,Morgantown, West Virginia
This case series demonstrates the incremental value of three-dimensional transthoracic echocardio-graphy (3D TTE) over two-dimensional transthoracic echocardiography (2D TTE) in the assessmentof 11 patients with right ventricular (RV) masses or mass-like lesions (three cases of RV thrombus,one myxoma, one fibroma, one lipoma, one chordoma, and one sarcoma and three cases of RV non-compaction, which are considered to be mass-like in nature). 3D TTE was of incremental value inthe assessment of these masses in that 3D TTE has the capacity to section the mass and view it frommultiple angles, giving the examiner a more comprehensive assessment of the mass. This was particu-larly helpful in the cases of thrombi, as the presence of echolucencies indicated clot lysis. In addition,certainty in the number of thrombi present was an advantage of 3D TTE. Also, sectioning of cardiactumors allowed more confidence in narrowing the differential diagnosis of the etiology of the mass.In addition, 3D TTE allowed us to identify precise location of the attachments of the masses as wellas to determine whether there were mobile components to the mass. Another noteworthy advantageof 3D TTE was that the volumes of the masses could be calculated. Additionally, the findings by 3DTTE correlated well with pathologic examination of RV tumors, and some of the masses measuredlarger by 3D TTE than by 2D TTE, which was also validated in one case by surgery. As in the caseof RV fibroma, another advantage was that 3D TTE actually identified more masses than 2D TTE.RV noncompaction was also well studied, and the assessment with 3D TTE helped to give a moredefinitive diagnosis in these patients. (ECHOCARDIOGRAPHY, Volume 26, May 2009)
real time three-dimensional transthoracic echocardiography, three-dimensional echocardiography,two-dimensional echocardiography, right ventricular noncompaction, right ventricular mass, chor-doma, myxoma, lipoma, fibroma, right ventricular thrombus
Real time two-dimensional transthoracicechocardiography (2D TTE) has proven use-ful in the detection of cardiac masses.1 Morerecently, three-dimensional transthoracic echo-
Address for correspondence and reprint requests: Navin C.Nanda, M.D., University of Alabama at Birmingham, HeartStation, SWB/S102, 619 19th Street South, Birmingham,AL 35249. Fax: 205-934-6747; E-mail: [email protected]
cardiography (3D TTE) has also been utilizedto evaluate these mass lesions.2–4 In this study,we report 11 cases of right ventricular (RV)masses and mass-like lesions that were eval-uated by 2D TTE and also with 3D TTE. Thecases include three cases of RV thrombus, onemyxoma, one fibroma, one lipoma, one chor-doma, one sarcoma, and three cases of RVnoncompaction.
598 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 26, No. 5, 2009
3D TTE IN RV MASSES
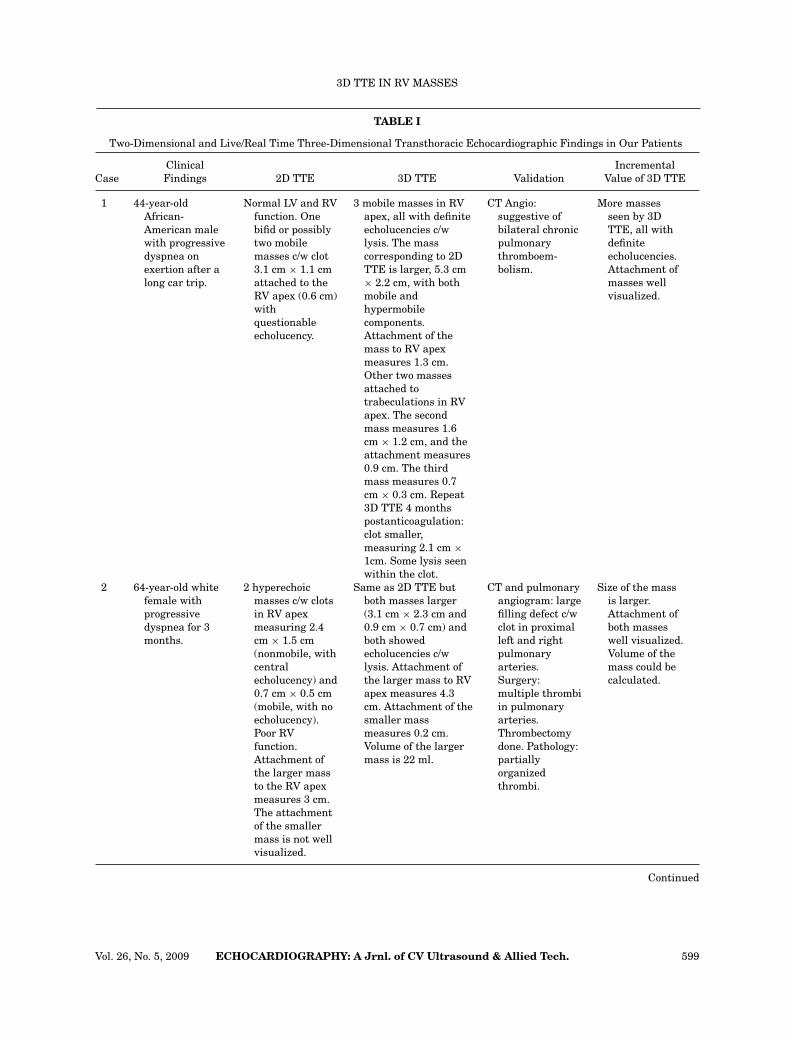
TABLE I
Two-Dimensional and Live/Real Time Three-Dimensional Transthoracic Echocardiographic Findings in Our Patients
Clinical IncrementalCase Findings 2D TTE 3D TTE Validation Value of 3D TTE
1 44-year-oldAfrican-American malewith progressivedyspnea onexertion after along car trip.
Normal LV and RVfunction. Onebifid or possiblytwo mobilemasses c/w clot3.1 cm × 1.1 cmattached to theRV apex (0.6 cm)withquestionableecholucency.
3 mobile masses in RVapex, all with definiteecholucencies c/wlysis. The masscorresponding to 2DTTE is larger, 5.3 cm× 2.2 cm, with bothmobile andhypermobilecomponents.Attachment of themass to RV apexmeasures 1.3 cm.Other two massesattached totrabeculations in RVapex. The secondmass measures 1.6cm × 1.2 cm, and theattachment measures0.9 cm. The thirdmass measures 0.7cm × 0.3 cm. Repeat3D TTE 4 monthspostanticoagulation:clot smaller,measuring 2.1 cm ×1cm. Some lysis seenwithin the clot.
CT Angio:suggestive ofbilateral chronicpulmonarythromboem-bolism.
More massesseen by 3DTTE, all withdefiniteecholucencies.Attachment ofmasses wellvisualized.
2 64-year-old whitefemale withprogressivedyspnea for 3months.
2 hyperechoicmasses c/w clotsin RV apexmeasuring 2.4cm × 1.5 cm(nonmobile, withcentralecholucency) and0.7 cm × 0.5 cm(mobile, with noecholucency).Poor RVfunction.Attachment ofthe larger massto the RV apexmeasures 3 cm.The attachmentof the smallermass is not wellvisualized.
Same as 2D TTE butboth masses larger(3.1 cm × 2.3 cm and0.9 cm × 0.7 cm) andboth showedecholucencies c/wlysis. Attachment ofthe larger mass to RVapex measures 4.3cm. Attachment of thesmaller massmeasures 0.2 cm.Volume of the largermass is 22 ml.
CT and pulmonaryangiogram: largefilling defect c/wclot in proximalleft and rightpulmonaryarteries.Surgery:multiple thrombiin pulmonaryarteries.Thrombectomydone. Pathology:partiallyorganizedthrombi.
Size of the massis larger.Attachment ofboth masseswell visualized.Volume of themass could becalculated.
Continued
Vol. 26, No. 5, 2009 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 599
REDDY, ET AL.
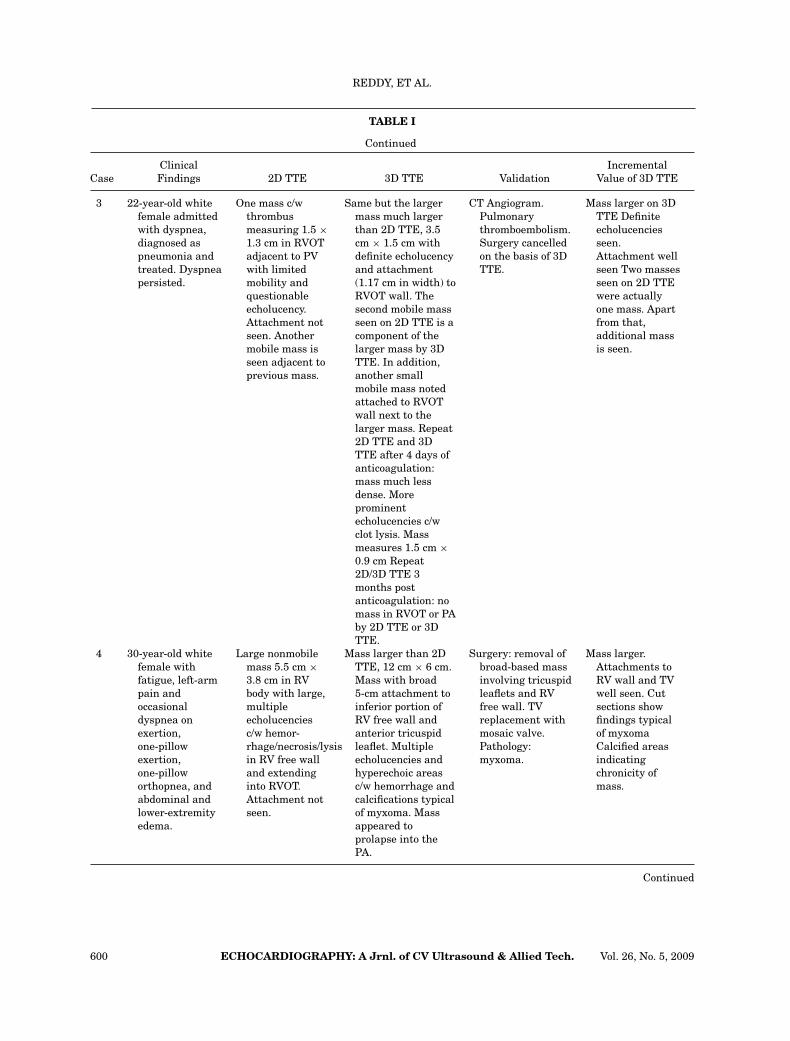
TABLE I
Continued
Clinical IncrementalCase Findings 2D TTE 3D TTE Validation Value of 3D TTE
3 22-year-old whitefemale admittedwith dyspnea,diagnosed aspneumonia andtreated. Dyspneapersisted.
One mass c/wthrombusmeasuring 1.5 ×1.3 cm in RVOTadjacent to PVwith limitedmobility andquestionableecholucency.Attachment notseen. Anothermobile mass isseen adjacent toprevious mass.
Same but the largermass much largerthan 2D TTE, 3.5cm × 1.5 cm withdefinite echolucencyand attachment(1.17 cm in width) toRVOT wall. Thesecond mobile massseen on 2D TTE is acomponent of thelarger mass by 3DTTE. In addition,another smallmobile mass notedattached to RVOTwall next to thelarger mass. Repeat2D TTE and 3DTTE after 4 days ofanticoagulation:mass much lessdense. Moreprominentecholucencies c/wclot lysis. Massmeasures 1.5 cm ×0.9 cm Repeat2D/3D TTE 3months postanticoagulation: nomass in RVOT or PAby 2D TTE or 3DTTE.
CT Angiogram.Pulmonarythromboembolism.Surgery cancelledon the basis of 3DTTE.
Mass larger on 3DTTE Definiteecholucenciesseen.Attachment wellseen Two massesseen on 2D TTEwere actuallyone mass. Apartfrom that,additional massis seen.
4 30-year-old whitefemale withfatigue, left-armpain andoccasionaldyspnea onexertion,one-pillowexertion,one-pilloworthopnea, andabdominal andlower-extremityedema.
Large nonmobilemass 5.5 cm ×3.8 cm in RVbody with large,multipleecholucenciesc/w hemor-rhage/necrosis/lysisin RV free walland extendinginto RVOT.Attachment notseen.
Mass larger than 2DTTE, 12 cm × 6 cm.Mass with broad5-cm attachment toinferior portion ofRV free wall andanterior tricuspidleaflet. Multipleecholucencies andhyperechoic areasc/w hemorrhage andcalcifications typicalof myxoma. Massappeared toprolapse into thePA.
Surgery: removal ofbroad-based massinvolving tricuspidleaflets and RVfree wall. TVreplacement withmosaic valve.Pathology:myxoma.
Mass larger.Attachments toRV wall and TVwell seen. Cutsections showfindings typicalof myxomaCalcified areasindicatingchronicity ofmass.
Continued
600 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 26, No. 5, 2009
3D TTE IN RV MASSES
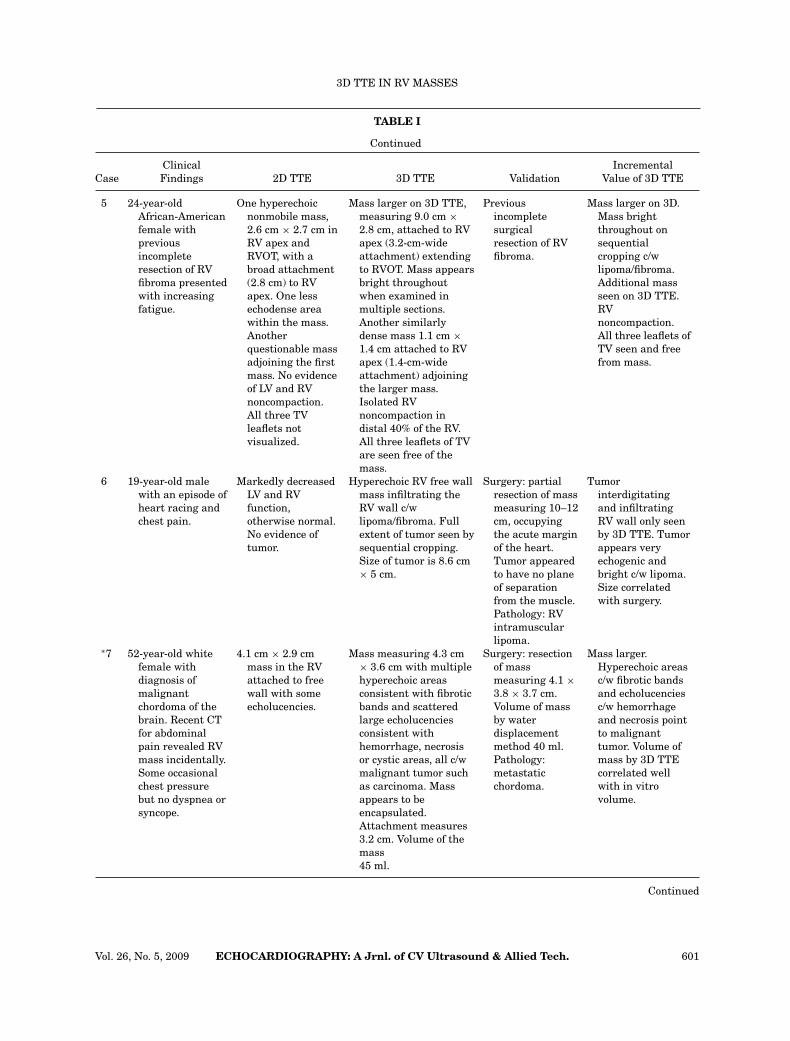
TABLE I
Continued
Clinical IncrementalCase Findings 2D TTE 3D TTE Validation Value of 3D TTE
5 24-year-oldAfrican-Americanfemale withpreviousincompleteresection of RVfibroma presentedwith increasingfatigue.
One hyperechoicnonmobile mass,2.6 cm × 2.7 cm inRV apex andRVOT, with abroad attachment(2.8 cm) to RVapex. One lessechodense areawithin the mass.Anotherquestionable massadjoining the firstmass. No evidenceof LV and RVnoncompaction.All three TVleaflets notvisualized.
Mass larger on 3D TTE,measuring 9.0 cm ×2.8 cm, attached to RVapex (3.2-cm-wideattachment) extendingto RVOT. Mass appearsbright throughoutwhen examined inmultiple sections.Another similarlydense mass 1.1 cm ×1.4 cm attached to RVapex (1.4-cm-wideattachment) adjoiningthe larger mass.Isolated RVnoncompaction indistal 40% of the RV.All three leaflets of TVare seen free of themass.
Previousincompletesurgicalresection of RVfibroma.
Mass larger on 3D.Mass brightthroughout onsequentialcropping c/wlipoma/fibroma.Additional massseen on 3D TTE.RVnoncompaction.All three leaflets ofTV seen and freefrom mass.
6 19-year-old malewith an episode ofheart racing andchest pain.
Markedly decreasedLV and RVfunction,otherwise normal.No evidence oftumor.
Hyperechoic RV free wallmass infiltrating theRV wall c/wlipoma/fibroma. Fullextent of tumor seen bysequential cropping.Size of tumor is 8.6 cm× 5 cm.
Surgery: partialresection of massmeasuring 10–12cm, occupyingthe acute marginof the heart.Tumor appearedto have no planeof separationfrom the muscle.Pathology: RVintramuscularlipoma.
Tumorinterdigitatingand infiltratingRV wall only seenby 3D TTE. Tumorappears veryechogenic andbright c/w lipoma.Size correlatedwith surgery.
∗7 52-year-old whitefemale withdiagnosis ofmalignantchordoma of thebrain. Recent CTfor abdominalpain revealed RVmass incidentally.Some occasionalchest pressurebut no dyspnea orsyncope.
4.1 cm × 2.9 cmmass in the RVattached to freewall with someecholucencies.
Mass measuring 4.3 cm× 3.6 cm with multiplehyperechoic areasconsistent with fibroticbands and scatteredlarge echolucenciesconsistent withhemorrhage, necrosisor cystic areas, all c/wmalignant tumor suchas carcinoma. Massappears to beencapsulated.Attachment measures3.2 cm. Volume of themass45 ml.
Surgery: resectionof massmeasuring 4.1 ×3.8 × 3.7 cm.Volume of massby waterdisplacementmethod 40 ml.Pathology:metastaticchordoma.
Mass larger.Hyperechoic areasc/w fibrotic bandsand echolucenciesc/w hemorrhageand necrosis pointto malignanttumor. Volume ofmass by 3D TTEcorrelated wellwith in vitrovolume.
Continued
Vol. 26, No. 5, 2009 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 601
REDDY, ET AL.
TABLE I
Continued
Clinical IncrementalCase Findings 2D TTE 3D TTE Validation Value of 3D TTE
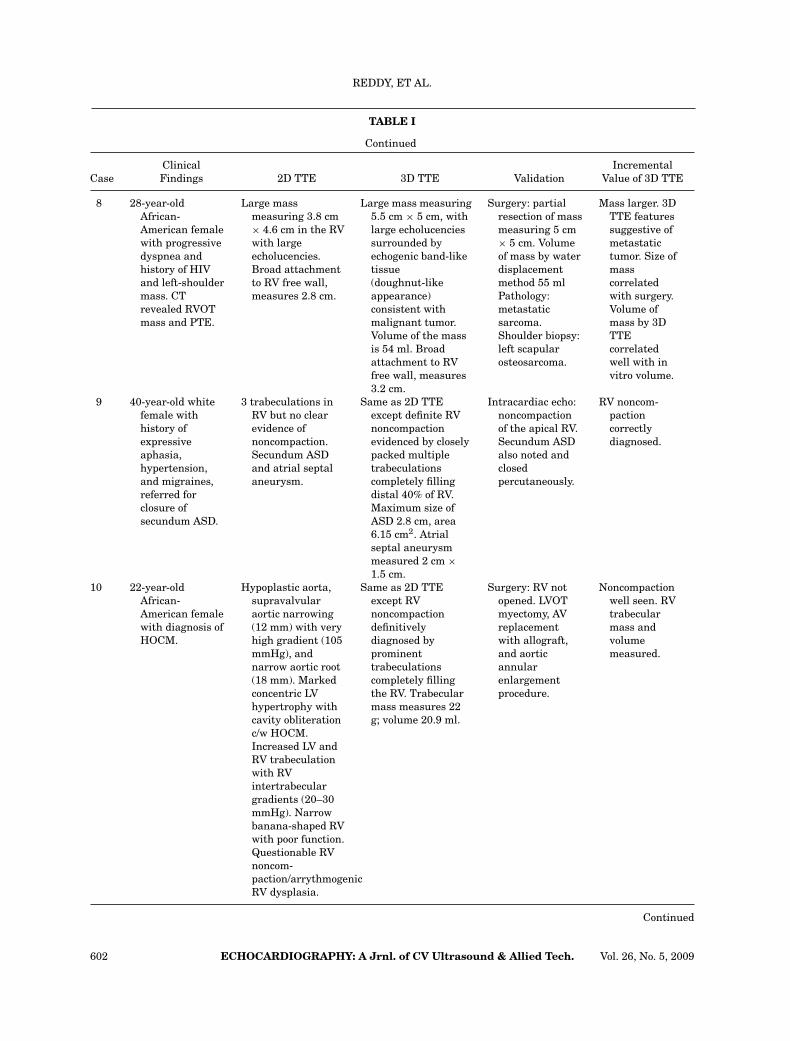
8 28-year-oldAfrican-American femalewith progressivedyspnea andhistory of HIVand left-shouldermass. CTrevealed RVOTmass and PTE.
Large massmeasuring 3.8 cm× 4.6 cm in the RVwith largeecholucencies.Broad attachmentto RV free wall,measures 2.8 cm.
Large mass measuring5.5 cm × 5 cm, withlarge echolucenciessurrounded byechogenic band-liketissue(doughnut-likeappearance)consistent withmalignant tumor.Volume of the massis 54 ml. Broadattachment to RVfree wall, measures3.2 cm.
Surgery: partialresection of massmeasuring 5 cm× 5 cm. Volumeof mass by waterdisplacementmethod 55 mlPathology:metastaticsarcoma.Shoulder biopsy:left scapularosteosarcoma.
Mass larger. 3DTTE featuressuggestive ofmetastatictumor. Size ofmasscorrelatedwith surgery.Volume ofmass by 3DTTEcorrelatedwell with invitro volume.
9 40-year-old whitefemale withhistory ofexpressiveaphasia,hypertension,and migraines,referred forclosure ofsecundum ASD.
3 trabeculations inRV but no clearevidence ofnoncompaction.Secundum ASDand atrial septalaneurysm.
Same as 2D TTEexcept definite RVnoncompactionevidenced by closelypacked multipletrabeculationscompletely fillingdistal 40% of RV.Maximum size ofASD 2.8 cm, area6.15 cm2. Atrialseptal aneurysmmeasured 2 cm ×1.5 cm.
Intracardiac echo:noncompactionof the apical RV.Secundum ASDalso noted andclosedpercutaneously.
RV noncom-pactioncorrectlydiagnosed.
10 22-year-oldAfrican-American femalewith diagnosis ofHOCM.
Hypoplastic aorta,supravalvularaortic narrowing(12 mm) with veryhigh gradient (105mmHg), andnarrow aortic root(18 mm). Markedconcentric LVhypertrophy withcavity obliterationc/w HOCM.Increased LV andRV trabeculationwith RVintertrabeculargradients (20–30mmHg). Narrowbanana-shaped RVwith poor function.Questionable RVnoncom-paction/arrythmogenicRV dysplasia.
Same as 2D TTEexcept RVnoncompactiondefinitivelydiagnosed byprominenttrabeculationscompletely fillingthe RV. Trabecularmass measures 22g; volume 20.9 ml.
Surgery: RV notopened. LVOTmyectomy, AVreplacementwith allograft,and aorticannularenlargementprocedure.
Noncompactionwell seen. RVtrabecularmass andvolumemeasured.
Continued
602 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 26, No. 5, 2009
3D TTE IN RV MASSES
TABLE I
Continued
Clinical IncrementalCase Findings 2D TTE 3D TTE Validation Value of 3D TTE
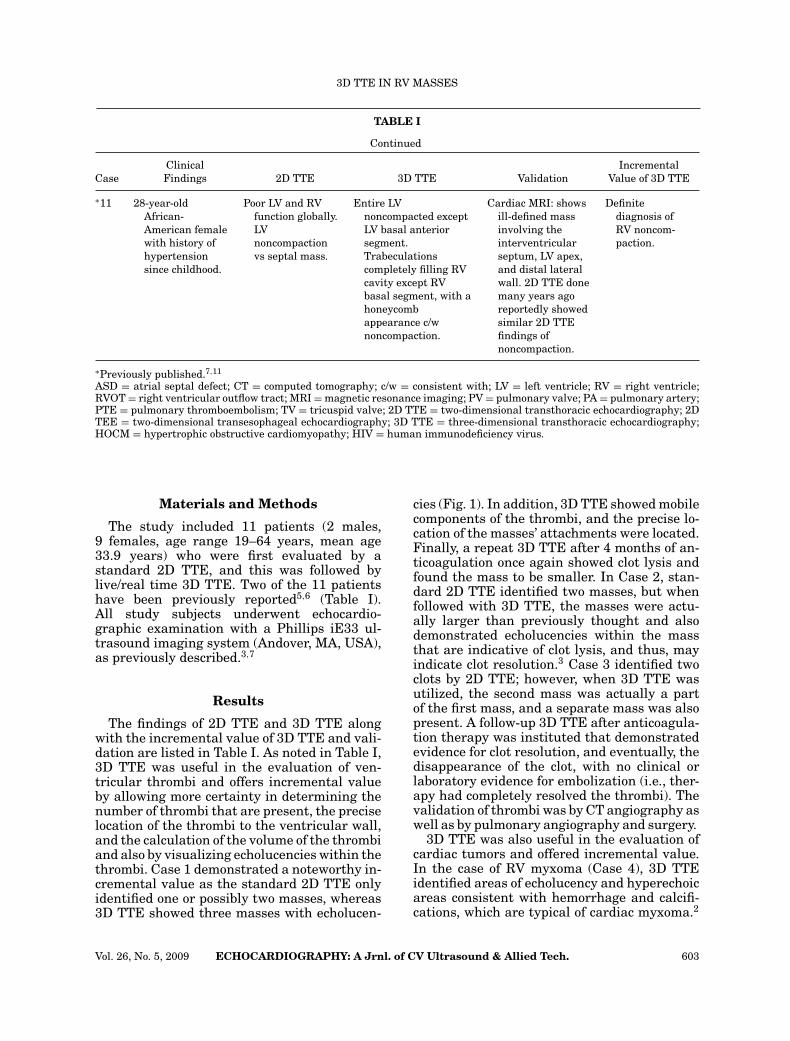
∗11 28-year-oldAfrican-American femalewith history ofhypertensionsince childhood.
Poor LV and RVfunction globally.LVnoncompactionvs septal mass.
Entire LVnoncompacted exceptLV basal anteriorsegment.Trabeculationscompletely filling RVcavity except RVbasal segment, with ahoneycombappearance c/wnoncompaction.
Cardiac MRI: showsill-defined massinvolving theinterventricularseptum, LV apex,and distal lateralwall. 2D TTE donemany years agoreportedly showedsimilar 2D TTEfindings ofnoncompaction.
Definitediagnosis ofRV noncom-paction.
∗Previously published.7,11
ASD = atrial septal defect; CT = computed tomography; c/w = consistent with; LV = left ventricle; RV = right ventricle;RVOT = right ventricular outflow tract; MRI = magnetic resonance imaging; PV = pulmonary valve; PA = pulmonary artery;PTE = pulmonary thromboembolism; TV = tricuspid valve; 2D TTE = two-dimensional transthoracic echocardiography; 2DTEE = two-dimensional transesophageal echocardiography; 3D TTE = three-dimensional transthoracic echocardiography;HOCM = hypertrophic obstructive cardiomyopathy; HIV = human immunodeficiency virus.
Materials and Methods
The study included 11 patients (2 males,9 females, age range 19–64 years, mean age33.9 years) who were first evaluated by astandard 2D TTE, and this was followed bylive/real time 3D TTE. Two of the 11 patientshave been previously reported5,6 (Table I).All study subjects underwent echocardio-graphic examination with a Phillips iE33 ul-trasound imaging system (Andover, MA, USA),as previously described.3,7
Results
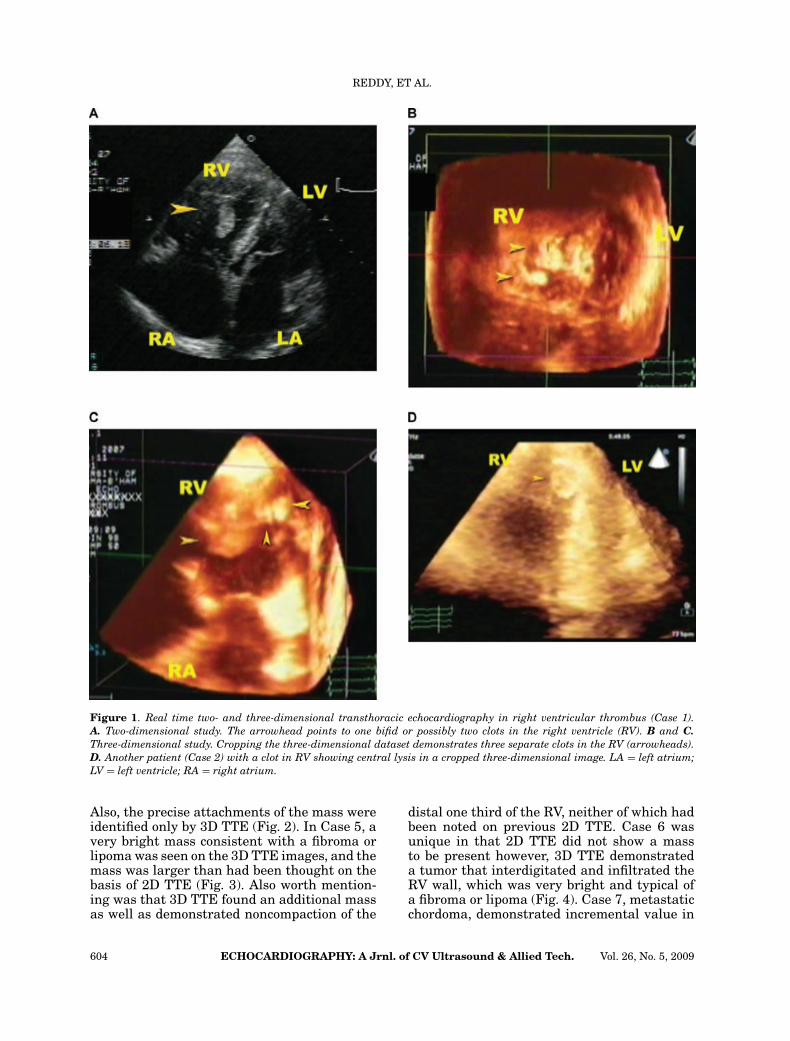
The findings of 2D TTE and 3D TTE alongwith the incremental value of 3D TTE and vali-dation are listed in Table I. As noted in Table I,3D TTE was useful in the evaluation of ven-tricular thrombi and offers incremental valueby allowing more certainty in determining thenumber of thrombi that are present, the preciselocation of the thrombi to the ventricular wall,and the calculation of the volume of the thrombiand also by visualizing echolucencies within thethrombi. Case 1 demonstrated a noteworthy in-cremental value as the standard 2D TTE onlyidentified one or possibly two masses, whereas3D TTE showed three masses with echolucen-
cies (Fig. 1). In addition, 3D TTE showed mobilecomponents of the thrombi, and the precise lo-cation of the masses’ attachments were located.Finally, a repeat 3D TTE after 4 months of an-ticoagulation once again showed clot lysis andfound the mass to be smaller. In Case 2, stan-dard 2D TTE identified two masses, but whenfollowed with 3D TTE, the masses were actu-ally larger than previously thought and alsodemonstrated echolucencies within the massthat are indicative of clot lysis, and thus, mayindicate clot resolution.3 Case 3 identified twoclots by 2D TTE; however, when 3D TTE wasutilized, the second mass was actually a partof the first mass, and a separate mass was alsopresent. A follow-up 3D TTE after anticoagula-tion therapy was instituted that demonstratedevidence for clot resolution, and eventually, thedisappearance of the clot, with no clinical orlaboratory evidence for embolization (i.e., ther-apy had completely resolved the thrombi). Thevalidation of thrombi was by CT angiography aswell as by pulmonary angiography and surgery.
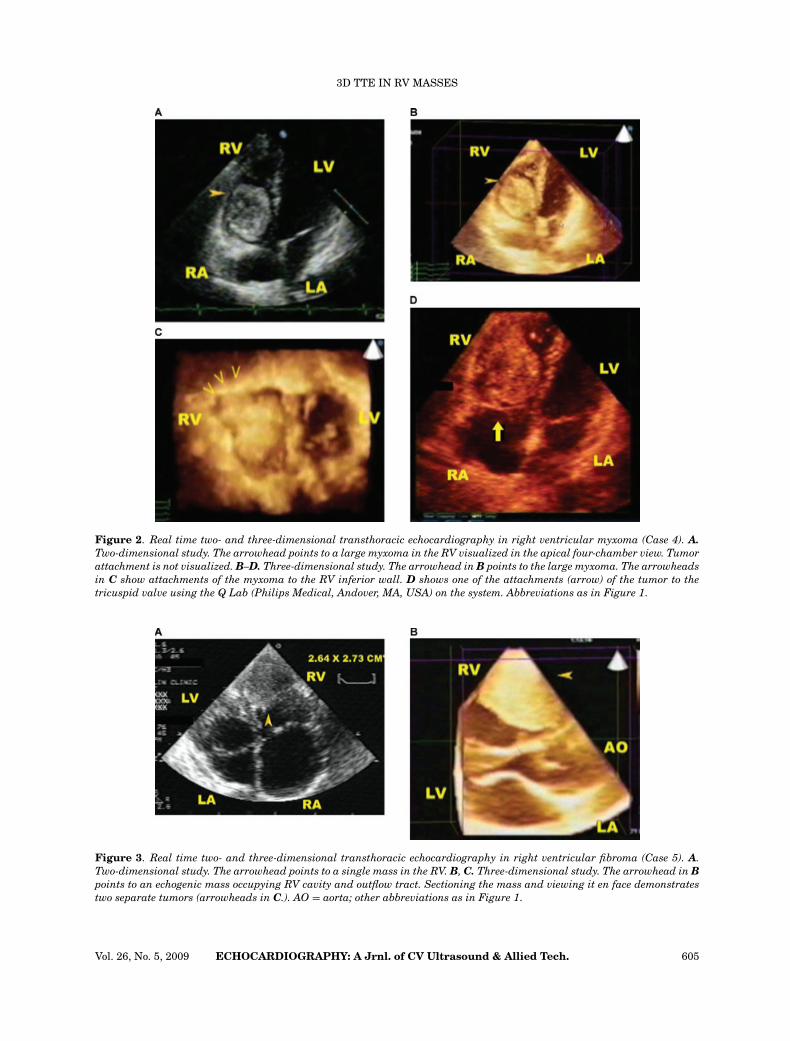
3D TTE was also useful in the evaluation ofcardiac tumors and offered incremental value.In the case of RV myxoma (Case 4), 3D TTEidentified areas of echolucency and hyperechoicareas consistent with hemorrhage and calcifi-cations, which are typical of cardiac myxoma.2
Vol. 26, No. 5, 2009 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 603
REDDY, ET AL.
Figure 1. Real time two- and three-dimensional transthoracic echocardiography in right ventricular thrombus (Case 1).A. Two-dimensional study. The arrowhead points to one bifid or possibly two clots in the right ventricle (RV). B and C.Three-dimensional study. Cropping the three-dimensional dataset demonstrates three separate clots in the RV (arrowheads).D. Another patient (Case 2) with a clot in RV showing central lysis in a cropped three-dimensional image. LA = left atrium;LV = left ventricle; RA = right atrium.
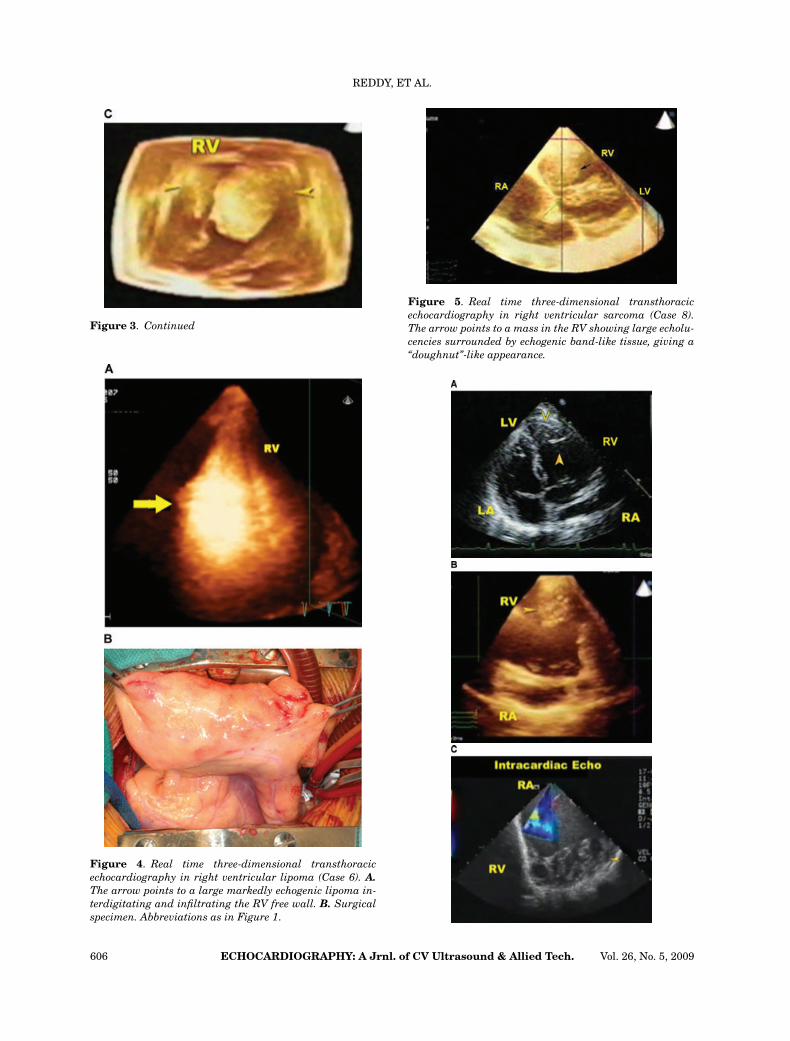
Also, the precise attachments of the mass wereidentified only by 3D TTE (Fig. 2). In Case 5, avery bright mass consistent with a fibroma orlipoma was seen on the 3D TTE images, and themass was larger than had been thought on thebasis of 2D TTE (Fig. 3). Also worth mention-ing was that 3D TTE found an additional massas well as demonstrated noncompaction of the
distal one third of the RV, neither of which hadbeen noted on previous 2D TTE. Case 6 wasunique in that 2D TTE did not show a massto be present however, 3D TTE demonstrateda tumor that interdigitated and infiltrated theRV wall, which was very bright and typical ofa fibroma or lipoma (Fig. 4). Case 7, metastaticchordoma, demonstrated incremental value in
604 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 26, No. 5, 2009
3D TTE IN RV MASSES
Figure 2. Real time two- and three-dimensional transthoracic echocardiography in right ventricular myxoma (Case 4). A.Two-dimensional study. The arrowhead points to a large myxoma in the RV visualized in the apical four-chamber view. Tumorattachment is not visualized. B–D. Three-dimensional study. The arrowhead in B points to the large myxoma. The arrowheadsin C show attachments of the myxoma to the RV inferior wall. D shows one of the attachments (arrow) of the tumor to thetricuspid valve using the Q Lab (Philips Medical, Andover, MA, USA) on the system. Abbreviations as in Figure 1.
Figure 3. Real time two- and three-dimensional transthoracic echocardiography in right ventricular fibroma (Case 5). A.Two-dimensional study. The arrowhead points to a single mass in the RV. B, C. Three-dimensional study. The arrowhead in Bpoints to an echogenic mass occupying RV cavity and outflow tract. Sectioning the mass and viewing it en face demonstratestwo separate tumors (arrowheads in C.). AO = aorta; other abbreviations as in Figure 1.
Vol. 26, No. 5, 2009 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 605
REDDY, ET AL.
Figure 3. Continued
Figure 4. Real time three-dimensional transthoracicechocardiography in right ventricular lipoma (Case 6). A.The arrow points to a large markedly echogenic lipoma in-terdigitating and infiltrating the RV free wall. B. Surgicalspecimen. Abbreviations as in Figure 1.
Figure 5. Real time three-dimensional transthoracicechocardiography in right ventricular sarcoma (Case 8).The arrow points to a mass in the RV showing large echolu-cencies surrounded by echogenic band-like tissue, giving a“doughnut”-like appearance.
606 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 26, No. 5, 2009

3D TTE IN RV MASSES
Figure 6. Schematics. The horizontal arrowhead in Apoints to central lysis in a clot, in B, it points to an areaof hemorrhage/necrosis in a myxoma, and in C, it pointsto an area of necrosis surrounded by a thick band-liketissue containing collagen, giving a doughnut-like appear-ance seen with chordoma and sarcoma. The vertical arrow-head in B points to dense calcification in the myxoma. Ddemonstrates a hemangioma that is completely vascular,and the echolucensies involve the whole tumor, including theperiphery.
that, in addition to showing that the mass waslarger than previously thought, the volume cal-culated by 3D TTE correlated with that foundat surgical resection of the mass. This find-ing was also present in Case 8, metastatic sar-coma, as the size noted on 3D TTE correlatedwell with the surgical specimen (Fig. 5). Bothpatients showed areas of echolucencies consis-tent with hemorrhage or necrosis, which werebordered by bright bands of tissue consistentwith collagen/fibrosis (Fig. 6). There was vali-
←−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−Figure 7. Real time two- and three-dimensional transtho-racic echocardiography in isolated right ventricular non-compaction (Case 9). A. Two-dimensional study. The ar-rowheads point to a few muscle bands in the RV apex,but there is no clear-cut evidence for noncompaction. B.Three-dimensional study. Cropping of the image reveals ahoneycomb appearance typical of RV noncompaction. C.Intracardiac echocardiography shows RV noncompaction(arrowhead). Abbreviations as in Figure 1.
dation of the tumors by surgical resection andpathology.
Finally, 3D TTE showed incremental value inthe evaluation of RV noncompaction. 3D TTE,when used as an adjunct, was able to help inmaking the proper diagnosis of RV noncom-paction in Cases 9, 10, and 11 (Fig. 7). Priorto 3D TTE images, the exact diagnosis wasnot clearly known. 2D TTE in Case 9 showedsome trabeculations but no clear evidence ofnoncompaction. On the other hand, with 3DTTE, the distal 40% of RV was noted to becompletely filled with trabeculations, resultingin a definitive diagnosis of RV noncompaction.Case 11 did demonstrate left ventricular (LV)noncompaction on 2D TTE, but when followedwith 3D TTE, it was found that the trabecula-tions were completely filling the RV cavity also,and that there was typical honeycomb appear-ance to the RV that is consistent with noncom-paction. In Case 10, the trabecular mass andvolume could also be calculated with the use of3D TTE.
Discussion
This case series clearly demonstrates that 3DTTE is a useful adjunct in the evaluation of RVmasses and mass-like lesions and offers incre-mental value in their assessment. RV thrombiare often formed in the presence of poor RVfunction and this aids in their diagnosis. By sec-tioning thrombi, echolucencies within the clotwere identified, which have shown to be con-sistent with clot liquefaction and clot lysis3,4
(Fig. 6). This finding can signify important ther-apeutic and prognostic implications, as it mayindicate that anticoagulation therapy is help-ing in clot dissolution. Furthermore, 3D TTEallows for better identification of the preciseattachments as well as of the mobile compo-nents of a clot. It has been previously thoughtthat if a thrombus was firmly attached to theventricular wall, it might have less propensityfor detachment and subsequent embolization.3In addition, 3D TTE offers incremental valuein determining the precise number of thrombipresent, as in Case 1.
The present study demonstrates that 3D TTEhas incremental value in the assessment of RVtumors. One of the inherent properties of 3DTTE is its ability to sequentially section the tu-mor and view it from multiple angles, giving thephysician a look at the inner part of the tumor.6Examining the inner structure of the tumor by3D TTE, and noting the characteristics of the
Vol. 26, No. 5, 2009 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 607

REDDY, ET AL.
mass, has been shown to correlate well with thefindings of pathologic analysis of the tumor.6Large echolucencies, possibly representingnecrosis or hemorrhage, together with scat-tered bright, punctate areas that are consis-tent with calcification, favor a myxoma. Masseswith bright echogenic areas, typically repre-senting fibrosis or fibro-fatty tissue and colla-gen, are likely to be a lipoma or fibroma. Closelypacked echolucencies involving the mass com-pletely and extending all the way to the pe-riphery have been reported in a highly vascularmass such as a hemangioma2 (Fig. 6). However,the present series does not include any RV he-mangioma. Both the malignant tumors seen byus in the RV (Cases 7 and 8) demonstrated,when the 3D datasets were sectioned, discreteecholucencies surrounded by bright band-liketissue, often giving a doughnut-like appearance(Fig. 6). These echolucencies correlate withhemorrhages or necrosis, and the bright areasrepresent bands of collagen/fibrosis. These find-ings were not seen in other nonmalignant tu-mors. Further experience with a large num-ber of cases would be needed to determinethe exact sensitivity and specificity of these3D TTE findings in the diagnosis of these twotypes of malignant tumors. Metastatic chor-doma may be differentiated from a sarcomabecause the primary tumor most commonlyarises in the axial skeleton. Tumors in theRV were easily differentiated from clots bythe associated absence of poor RV function,which serves as a substrate for clot forma-tion. When combined with the clinical andother 2D TTE findings the addition of 3D TTEhelps to narrow the differential diagnosis of RVmasses. Also, in the present study, the findingsat 3D TTE correlate well with the pathologicfindings.
Ventricular noncompaction is often suspectedwhen echocardiographic examination shows in-creased trabeculations with deep intertrabecu-lar recesses and a “honeycomb” appearance tothe myocardium.5 In the present study, the di-agnosis of noncompaction was made when therewere thought to be “excessive” trabeculations inthe RV. For example, in Case 9, the distal 40%of the RV was completely filled with trabecu-lations (Fig. 1). Cases 10 and 11 demonstratedprominent trabeculations virtually completelyfilling the RV. Thus, in these cases, there wasthought to be excessive trabeculations, and thediagnosis of RV noncompaction was made. Thedifferential diagnosis in a patient with noncom-
paction is quite broad.5,8,9 The addition of 3DTTE to the workup of such patients can helpto make a more definitive diagnosis. In addi-tion, trabecular mass and volume can also beassessed with 3D TTE.
In conclusion, the addition of 3D TTE in theevaluation of the RV masses has demonstratedincremental value over standard 2D TTE in theevaluation of these masses.
Acknowledgments: We sincerely thank Jaya PrakashManda, M.B.B.S., Sai Sravanthi Palakodety, M.B.B.S., andRohini Prashar, M.B.B.S., for their help in this study.
References
1. Moses HW, Nanda NC: Real time two-dimensionalechocardiography in the diagnosis of left atrial myx-oma. Chest 1980;78:788–791.
2. Mehmood F, Nanda NC, Vengala S, et al: Livethree-dimensional transthoracic echocardiographic as-sessment of left atrial tumors. Echocardiography2005;22:137–143.
3. Sinha A, Nanda NC, Khanna D, et al: Morphologicalassessment of left ventricular thrombus by live three-dimensional transthoracic echocardiography. Echocar-diography 2004;7:649–655.
4. Duncan K, Nanda NC, Foster WA, et al: Incrementalvalue of live/real time three dimensional transthoracicechocardiography in the assessment of left ventricularthrombi. Echocardiography 2006;23:68–72.
5. Bodiwala K, Miller A, Nanda N, et al: Live threedimensional transthoracic echocardiographic assess-ment of ventricular noncompaction. Echocardiography2005;22:611–619.
6. Pothineni KR, Nanda NC, Burri MV, et al: Live/realtime three-dimensional transthoracic echocardio-graphic description of chordoma metastatic to theheart. Echcardiography 2008;25:440–442.
7. Rajdev S, Singh A, Nanda NC, et al: Comparison of two-and three-dimensional transthoracic echocardiographyin the assessment of trabeculations and trabecularmass in left ventricular noncompaction. Echocardio-graphy 2007;24:760–767.
8. Cavusoglu Y, Ata N, Timuralp B, et al: Noncompactionof the ventricular myocardium: Report of two caseswith bicuspid aortic valve demonstrating poor progno-sis and with prominent right ventricular involvement.Echocardiography 2003;20:379–383.
9. Eilen D, Patterson N, Karkut C, et al: Isolated non-compaction of the left ventricular myocardium: Acase report and literature review. Echocardiography2008;25:755–761.
Supporting Information
Additional Supporting Information may befound in the online version of this article:
Video clip for Figure 1A.Video clip for Figures 1B and C, parts 1–4.
608 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. Vol. 26, No. 5, 2009
3D TTE IN RV MASSES
Video clip for Figure 1D.Video clip for Figures 2B–D, parts 1 and 2.Video clip for Figures 3B and C, parts 1–3.Video clip for Figure 4, parts 1–3.Video clip for Figure 5B.Video clip for Figures 7A–C.
Please note: Wiley-Blackwell is not respon-sible for the content or functionality of anysupporting information supplied by the au-thors. Any queries (other than missing mate-rial) should be directed to the correspondingauthor for the article.
Vol. 26, No. 5, 2009 ECHOCARDIOGRAPHY: A Jrnl. of CV Ultrasound & Allied Tech. 609
Related Documents











