Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Increased blood troponin levels in ICU patients Nikolaos Markou a , Leonidas Gregorakos b and Pavlos Myrianthefs b Introduction Serum levels of cardiac troponins T and I (cTnT, cTnI) represent an exquisite marker of myocardial injury, with high myocardial tissue specificity and high sensitivity. Thus troponins have succeeded creatine phosphokinase- MB (CPK-MB) as the preferred biomarkers for the diagnosis of myocardial infarction (MI) and for risk stratification in acute coronary syndromes (ACS) [1–3]. Currently, for types 1 and 2 of MI, diagnosis requires a changing pattern of cardiac troponin (a rise or fall within hours), with at least one value above the upper reference limit of the assay [1,2,4]. With sensitive assays now in use, up to 80% of patients presenting with MI can be identified within 2–3 h, whereas exclusion of MI can take as little as 6 h [5]. The recent development of newer assays with even lower cut-off points, promises further improvement in the early diagnosis and risk stratification of acute MI [6,7]. Yet, an elevated troponin does not automatically equate with diagnosis of MI as it may also be associated with a multitude of nonischemic causes (given below) [2,3,8,9]. Elevations of troponin in the absence of overt ischemic heart disease: (1) Cardiac contusion. (2) Ablation, pacing, cardioversion, endomyocardial biopsy. (3) Congestive heart failure (acute, chronic). (4) Aortic dissection, aortic valve disease or hyper- trophic cardiomyopathy. (5) Tachyarrhythmias or bradyarrhythmias. (6) Apical ballooning syndrome. (7) Rhabdomyolysis. (8) Pulmonary embolism. (9) Severe pulmonary hypertension. (10) Renal failure. (11) Acute neurological disease (stroke, subarachnoid hemorrhage). (12) Infiltrative myocardial diseases: amyloidosis, hemo- chromatosis, sarcoidosis, scleroderma. (13) Myocarditis or myocardial extension of pericarditis or endocarditis. (14) Drug toxicity: adriamycin, 5-fluorouracil, herceptin, snake venoms. a ICU, ‘Thriasio’ Hospital and b Athens University School of Nursing, ICU at «Agioi Anargyroi» General Hospital, Athens, Greece Correspondence to Nikolaos Markou, 24 Sholiou St, 15342 Agia Paraskevi, Greece Tel: +30 6973404627; e-mail: [email protected] Current Opinion in Critical Care 2011, 17:454–463 Purpose of review Cardiac troponins in serum have become the biomarkers of choice for the diagnosis of myocardial infarction. Yet, troponin can also be elevated by a multitude of causes in the absence of overt myocardial ischemia. Such nonspecific elevations are particularly common in the critically ill. This article aims to provide information on the significance of troponin elevations in unselected critically ill patients and in patients with sepsis or septic shock. Recent findings Recent studies reconsider the possible association of troponin elevations with myocardial infarction in unselected critically ill patients. There are also more data on the prognostic significance of troponin in this population. In patients with sepsis, recent studies suggest that troponin may be a reliable index of sepsis-induced myocardial dysfunction, although the implications of this finding in the management of sepsis remain unclear for the time being. Troponin also appears to be a predictor of short and possibly also long-term outcome in septic patients. The advent of newer assays with even higher sensitivity, may lead to further redefinition of the role of troponin in the ICU. Summary Troponin is frequently elevated in critically ill patients. More research is needed on the diagnostic and prognostic significance and possible clinical applications of troponin measurements in patients with sepsis and critical illness. Keywords critical illness, diastolic dysfunction, myocardial infarction, prognosis, sepsis, systolic dysfunction, troponin Curr Opin Crit Care 17:454–463 ß 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins 1070-5295 1070-5295 ß 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins DOI:10.1097/MCC.0b013e3283491f0d

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

C
Increased blood troponin levels
in ICU patientsNikolaos Markoua, Leonidas Gregorakosb and Pavlos MyrianthefsbaICU, ‘Thriasio’ Hospital and bAthens University Schoolof Nursing, ICU at «Agioi Anargyroi» General Hospital,Athens, Greece
Correspondence to Nikolaos Markou, 24 Sholiou St,15342 Agia Paraskevi, GreeceTel: +30 6973404627;e-mail: [email protected]
Current Opinion in Critical Care 2011,17:454–463
Purpose of review
Cardiac troponins in serum have become the biomarkers of choice for the diagnosis of
myocardial infarction. Yet, troponin can also be elevated by a multitude of causes in the
absence of overt myocardial ischemia. Such nonspecific elevations are particularly
common in the critically ill. This article aims to provide information on the significance of
troponin elevations in unselected critically ill patients and in patients with sepsis or
septic shock.
Recent findings
Recent studies reconsider the possible association of troponin elevations with
myocardial infarction in unselected critically ill patients. There are also more data on the
prognostic significance of troponin in this population. In patients with sepsis, recent
studies suggest that troponin may be a reliable index of sepsis-induced myocardial
dysfunction, although the implications of this finding in the management of sepsis
remain unclear for the time being. Troponin also appears to be a predictor of short and
possibly also long-term outcome in septic patients. The advent of newer assays with
even higher sensitivity, may lead to further redefinition of the role of troponin in the ICU.
Summary
Troponin is frequently elevated in critically ill patients. More research is needed on the
diagnostic and prognostic significance and possible clinical applications of troponin
measurements in patients with sepsis and critical illness.
Keywords
critical illness, diastolic dysfunction, myocardial infarction, prognosis, sepsis, systolic
dysfunction, troponin
Curr Opin Crit Care 17:454–463� 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins1070-5295
Introduction
Serum levels of cardiac troponins T and I (cTnT, cTnI)
represent an exquisite marker of myocardial injury, with
high myocardial tissue specificity and high sensitivity.
Thus troponins have succeeded creatine phosphokinase-
MB (CPK-MB) as the preferred biomarkers for the
diagnosis of myocardial infarction (MI) and for risk
stratification in acute coronary syndromes (ACS) [1–3].
Currently, for types 1 and 2 of MI, diagnosis requires a
changing pattern of cardiac troponin (a rise or fall within
hours), with at least one value above the upper reference
limit of the assay [1,2,4]. With sensitive assays now in use,
up to 80% of patients presenting with MI can be identified
within 2–3 h, whereas exclusion of MI can take as little as
6 h [5]. The recent development of newer assays with even
lower cut-off points, promises further improvement in the
early diagnosis and risk stratification of acute MI [6,7].
Yet, an elevated troponin does not automatically
equate with diagnosis of MI as it may also be associated
with a multitude of nonischemic causes (given below)
[2,3,8,9].
opyright © Lippincott Williams & Wilkins. Unauth
1070-5295 � 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins
Elevations of troponin in the absence of overt ischemic
heart disease:
(1) C
oriz
ardiac contusion.
(2) A
blation, pacing, cardioversion, endomyocardialbiopsy.
(3) C
ongestive heart failure (acute, chronic).(4) A
ortic dissection, aortic valve disease or hyper-trophic cardiomyopathy.
(5) T
achyarrhythmias or bradyarrhythmias.(6) A
pical ballooning syndrome.(7) R
habdomyolysis.(8) P
ulmonary embolism.(9) S
evere pulmonary hypertension.(10) R
enal failure.(11) A
cute neurological disease (stroke, subarachnoidhemorrhage).
(12) I
nfiltrative myocardial diseases: amyloidosis, hemo-chromatosis, sarcoidosis, scleroderma.
(13) M
yocarditis or myocardial extension of pericarditisor endocarditis.
(14) D
rug toxicity: adriamycin, 5-fluorouracil, herceptin,snake venoms.
ed reproduction of this article is prohibited.
DOI:10.1097/MCC.0b013e3283491f0d

Increased blood troponin levels in ICU patients Markou et al. 455
(15) C
Cop
Key points
ritically ill patients especially with respiratory fail-ure or sepsis.
� Troponin elevation is common in critically ill (16) Bpatients and is not specific for myocardial ischemia.
urns, especially more than 30% of body surfacearea (BSA).
� In these patients, regardless of the presence of (17) E xtreme exertion.myocardial ischemia, elevation of troponin seems
to be associated with both short- and long-term
prognosis.
� In patients with sepsis, elevations of troponin seem
to be associated with reversible sepsis-induced
myocardial infarction.
It should be noted that in most of these cases troponin
elevation probably still signifies myocardial injury (but
not necessarily necrosis) [4]. Thus diagnosis of myo-
cardial necrosis of ischemic cause in a patient with
increased troponin depends on the clinical context
(symptoms of ischemia, ECG findings, imaging) [1,2].
Increased troponin levels in the absence of ACS should
prompt an evaluation for an alternative, nonthrombotic
mechanism of troponin elevation and direct management
at the underlying cause [6].
A recent study highlights that troponin elevations may
often be unrelated to MI even in acute patients present-
ing with increased clinical likelihood for MI: among 991
consecutive troponin-positive patients presenting with a
clinical suspicion of ACS to the emergency department,
83% of the troponin elevations were retrospectively
attributed to MI, 7.9% were related to other cardiac
causes, and 9.1% to noncardiac diseases. The leading
noncardiac causes were pulmonary embolism, renal fail-
ure, pneumonia, and sepsis [10�]. The specificity for MI
of low-level troponin elevations (one to five times the
upper limit of normal) is probably much lower (�49%)
[11�]. It seems that with sensitive troponin assays cur-
rently in use such low-level elevations represent a gray
zone, when evaluation of the clinical context as well as of
changes of troponin over time becomes even more
imperative for correct diagnosis.
It is well recognized that the levels of troponin are of
prognostic significance in ACS [4]. This prognostic sig-
nificance seems also to extend to patients with acute
noncoronary events (e.g. pulmonary embolism) and to
patients with chronic heart failure and chronic renal
failure [4,9]. Interestingly, in the study of Ilva et al.[10�] noncardiac patients with elevated troponin I at
admission showed significantly higher in-hospital
mortality (26.7 vs. 13.4%) compared to cardiac patients.
The use of recent high-sensitivity assays with very low
cut-offs may aggravate the problem of specificity for MI,
but on the contrary it may offer valuable prognostic
information. It has been recently shown that most
patients with stable coronary artery disease and preserved
left-ventricular function have detectable levels of tropo-
nin with a high-sensitivity troponin T assay, whereas
elevated values are found in 11.1% of patients. In these
patients, troponin concentrations were independently
associated with long-term incidence of cardiovascular
death and heart failure. This association persisted even
yright © Lippincott Williams & Wilkins. Unaut
for values of troponin within normal range of the assay
and below the limit of detection of conventional cardiac
troponin T assays [12].
Cardiac troponin elevation is common in the ICU and can
be observed in up to 40–50% of critically ill patients.
The interpretation, clinical significance and appropriate
management of an elevated troponin measurement in
critically ill patients are uncertain. In these patients,
the pretest probability for ACS is much lower than in
coronary care, whereas nonischemic causes of troponin
elevation (shock, sepsis, pulmonary embolism, renal
failure) are very often encountered. Regardless of cause,
elevated levels of troponin are probably of prognostic
value in critically ill patients, although such associations
are less unequivocal than in ACS [13,14].
We will review the significance of troponin elevations in
the general critically ill patient, with particular emphasis
in more recent findings. We will not discuss the role of
troponin in trauma, cardiac and noncardiac surgery, the
postsurgical setting, revascularization processes or in the
coronary care unit, neither its significance in entities
such as stroke, pulmonary embolism, chronic obstructive
pulmonary disease (COPD), decompensated heart failure
or renal failure.
Troponin in mixed critical care patientsTroponin is commonly increased in critically ill patients,
although the exact frequency varies considerably
between studies, because of differences in patient selec-
tion, case-mix, heterogeneity of assays and different
cut-off values [15–31,32��,33��]. A few years ago, a
meta-analysis of 20 studies with a total of 3278 critically
ill patients, reported that elevated troponin was present
with a median frequency of 43% [interquartile range
(IQR) 21–59%]. Elevated cardiac troponin (cTn) levels
were more frequently found among patients admitted
with sepsis or septic shock. The median frequency of
elevated troponin measurement was higher among
medical ICU patients, somewhat lower in mixed
medical-surgical ICU patients and even lower in surgi-
cal-trauma ICU patients [15]. It should be noted that
horized reproduction of this article is prohibited.

C
456 Cardiovascular system
many of the studies in this meta-analysis concerned not
only unselected critically ill patients but cohorts with
more specific problems (trauma, sepsis, COPD). Table 1
presents data from studies of troponin in unselected
critically ill patients [16–31,32��,33��]. Troponin levels
seem to be higher in more severe disease [22,30,34].
Associations have also been reported with age, cardio-
vascular risk factors and previous cardiovascular history
[30].
Troponin elevation in these patients is not necessarily
indicative of ACS, as many of the entities listed above are
also commonly observed in the ICU. On the other hand,
aggravation of pre-existing coronary artery disease in the
context of extreme stress associated with critical illness
can also lead to increases in troponin because of MI [35].
It has been observed that among patients admitted
to the ICU for gastrointestinal bleeding, those with risk
factors for ischemic heart disease developed ACS more
frequently than those without [36]. It can be easily
postulated that an imbalance in pro and anticoagulant
mechanisms can predispose to thrombotic (type 1) MI
in these patients, whereas endothelial dysfunction might
also play a role in limiting coronary blood flow in patients
with critical coronary lesions. In addition, tachycardia,
hypoxemia, diminished oxygen delivery, may tip the
balance of regional myocardial oxygen consumption over
the critical edge. Thus, in some cases, troponin elevation
might represent not only plaque rupture (type 1 MI) but
also a type 2 MI due to underlying coronary artery disease
and increased myocardial oxygen demand [27,28,35].
Nevertheless, the exact contribution of MI or ACS to
troponin increase in unselected critically ill patients
remains debatable.
In an older prospective study by Ammann et al. [22] in
58 consecutive patients admitted to the ICU for reasons
other than ACS, flow-limiting coronary artery disease
could be excluded with stress echocardiography or
autopsy in 72% of troponin-positive patients. On the
contrary, studies with prospective screening of critically
ill patients with 12-lead electrocardiography (ECG)
and troponin measurements conclude that troponin
elevations are associated with events of myocardial
ischemia in approximately 50% of cases [20,31,32��].
Booker et al. [20] prospectively screened 76 consecutive
patients admitted to a general ICU with 12-lead ECGs for
the first 24–48 h of admission and troponin assays 8–12 h
after the ECG monitoring period. ECG-defined ischemic
events together with troponin I elevation were observed
in six patients, who accounted for 50% of all troponin-
positive results [20].
Lim et al. [31,32��] applied on all patients admitted to a
general ICU over a 2-month period a systematic screen-
opyright © Lippincott Williams & Wilkins. Unauth
ing protocol (with troponin T and 12-lead ECG) over the
whole duration of hospitalization. Patients were screened
at ICU admission and then once daily for the first week;
on alternate days for up to 1 month; then weekly until
ICU death or discharge or for a maximum of 2 months.
Two adjudicators retrospectively reviewed patient charts
to determine the likely cause of troponin elevation. It
should be noted that in their institution patients with
primary cardiac diagnoses but requiring mechanical
ventilation or inotropes/vasopressors were admitted to
the ICU and not to the coronary care unit and thus were
not excluded from the study. Cardiovascular diagnosis
was present in 13.8% of patients but only one of nine
patients with cardiovascular diagnosis had an admission
diagnosis of acute MI, whereas the other eight were
surgical patients.
Of 103 patient admissions, 52 (50.5%) had one or more
elevated troponin measurements. Troponin elevation
was attributed to MI in 53.1% of patients, sepsis in
18.4%, renal failure in 12.2%, and to other causes in
16.3% (cardiac contusion/cardiopulmonary resuscitation
in 6.1%, COPD in 6.1%, congestive heart failure in 4.1%).
Of patients with MI, 61.5% were adjudicated as having
type 1 MI (plaque rupture) on the basis of a history of
coronary artery disease with typical ECG evidence of
progression of infarction (Q waves). A 38.5% of patients
were adjudicated as having type 2 MI (no risk factors or
history of coronary artery disease and presence of a
condition possibly associated with supply–demand
imbalance in the coronary circulation – for example
hypotension, hypovolemia, supraventricular tachycardia).
Interestingly, no significant difference in hospital
mortality was observed between the two types of MI
(25 vs. 40%), although this lack of significance may be
associated with limited number of events [32��].
Diagnosis of MI in these prospective studies was based
on current guidelines, recommending a rise and/or fall in
serum levels of troponin, together with evidence of
myocardial ischemia (clinical, electrocardiographical or
by imaging of new regional wall motion abnormalities)
[2,3]. Yet, diagnosing MI in unselected critically ill
patients remains a challenge. In these patients, not only
is chest pain a rare finding and the significance of troponin
elevation unclear, but interpretation of 12-lead ECG can
be problematic, as even ST-segment elevation has
been reported to be a nonspecific finding that is fre-
quently the result of a variety of nonischemic processes
[20,37,38,39�].
Rennyson et al. [39�] retrospectively studied all cases with
electrocardiographic ST-segment elevation in an ICU: in
23 patients with ST elevation and borderline elevation of
troponin, who should have been classified as MI according
to current guidelines, echocardiographic evaluation could
orized reproduction of this article is prohibited.

Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Increased blood troponin levels in ICU patients Markou et al. 457
Ta
ble
1T
rop
on
inin
un
se
lecte
dcri
tica
lly
ill
pa
tie
nts
Ref
eren
ceS
tud
yd
esig
nN
umb
eran
dty
pe
of
pat
ient
scT
nty
pe
Sam
plin
gp
roto
col
Fre
que
ncy
of
elev
ated
cTn
(%)
Ass
oci
atio
no
fcT
nw
ithm
ort
ality
LOS
(una
dju
sted
anal
ysis
)
Gue
stet
al.
[16
]P
rosp
ectiv
e,co
nsec
utiv
e2
09
Med
ical
ICU
cTnI
Dai
ly1
5IC
Um
ort
ality
incr
ease
d(u
niva
riate
anal
ysis
)IC
ULO
Sin
crea
sed
Ko
llef
etal
.[1
7]
Pro
spec
tive,
cons
ecut
ive
26
0M
edic
alIC
UcT
nID
aily
16
Ho
spita
lm
ort
ality
–no
effe
ctin
mul
tivar
iate
anal
ysis
No
ble
etal
.[1
8]
Pro
spec
tive,
case
cont
rol,
cons
ecut
ive
10
9C
ases
and
58
cont
rols
(hea
lthy
volu
ntee
rs)
med
ical
-sur
gic
alIC
U
cTnI
Dai
ly7
1(0
inco
ntro
ls)
Ho
spita
lm
ort
ality
–no
effe
ct(u
niva
riate
anal
ysis
)
Kle
inG
unne
wie
kan
dva
nd
eLe
ur[1
9]
Pro
spec
tive,
cons
ecut
ive
34
Sur
gic
alcT
nTA
dm
issi
on,
next
mo
rnin
gan
d2
4h
late
r3
2N
oas
soci
atio
nw
ithm
ort
ality
No
asso
ciat
ion
with
LOS
Bo
oke
ret
al.
[20
]P
rosp
ectiv
e,co
nsec
utiv
e7
6M
edic
al-s
urg
ical
cTnI
8–
12
haf
ter
24
–4
8h
of
EK
Gm
oni
torin
g1
6A
sso
ciat
ion
with
hosp
ital
mo
rtal
ity(u
nad
just
edan
alys
is)
Rel
os
etal
.[2
1]
Ret
rosp
ectiv
e,no
nco
nsec
utiv
e8
69
Sur
gic
alIC
UcT
nIN
ot
spec
ified
No
tsp
ecifi
edIn
crea
sed
ICU
mo
rtal
ityin
unad
just
edan
alys
isA
mm
ann
etal
.[2
2]
Pro
spec
tive,
cons
ecut
ive.
CA
Dex
clud
edw
ithst
ress
EC
HO
or
auto
psy
58
Med
ical
ICU
cTnI
,cT
nTE
nro
llmen
t,3
,1
2,
24
,4
6,
96
,1
92
h5
5A
sso
ciat
ion
with
ICU
,ho
spita
lm
ort
ality
(uni
varia
tean
alys
is)
Wu
etal
.[2
3]
Pro
spec
tive,
cons
ecut
ive
10
8M
edic
alIC
UcT
nIA
dm
issi
on
45
Incr
ease
dIC
Um
ort
ality
,In
crea
sed
hosp
ital
mo
rtal
ityIn
crea
sed
ICU
LOS
Que
not
etal
.[2
4]
Pro
spec
tive,
cons
ecut
ive
21
7M
edic
alIC
UcT
nIA
dm
issi
on
32
Incr
ease
dho
spita
lm
ort
ality
Incr
ease
dIC
Uan
dho
spita
lLO
SLi
met
al.
[25
]P
rosp
ectiv
e,no
nco
nsec
utiv
e(8
1%
of
all
ICU
adm
issi
ons
)9
3M
edic
al-s
urg
ical
ICU
cTnT
Day
of
adm
issi
on
47
No
tin
dep
end
ent
pre
dic
tor
of
ICU
or
hosp
ital
mo
rtal
ityM
inki
net
al.
[26
]R
etro
spec
tive,
nonc
ons
ecut
ive
13
2/2
21
13
2M
edic
alIC
UcT
nIA
dm
issi
on
31
Una
dju
sted
asso
ciat
ion
with
ICU
but
not
hosp
ital
mo
rtal
ityK
ing
etal
.[2
7]
Pro
spec
tive,
cons
ecut
ive
21
5M
edic
alIC
UcT
nIA
dm
issi
on
(with
in6
h)2
7,
3A
sso
ciat
ion
inun
ivar
iate
anal
ysis
but
not
ind
epen
den
tp
red
icto
ro
f2
8-d
aym
ort
ality
No
asso
ciat
ion
with
ICU
LOS
Land
esb
erg
etal
.[2
8]
Pro
spec
tive.
Pat
ient
sw
ithkn
ow
nst
able
CA
Do
rhi
gh
risk
for
CA
D
10
1G
ener
alIC
UcT
nTD
aily
38
Ass
oci
ated
with
1-m
ont
h,6
-mo
nth
and
2-y
ear
mo
rtal
ityin
univ
aria
teb
utno
tm
ultiv
aria
tean
alys
isLi
met
al.
[29
]R
etro
spec
tive.
Pat
ient
sw
ithex
pec
ted
stay
inIC
U>
72
h;no
nco
nsec
utiv
e
Ear
lysa
mp
ling
(<4
8h)
:1
71
;la
tesa
mp
ling
(>4
8h)
:1
36
;m
edic
al-
surg
ical
ICU
cTnI
As
need
edE
arly
sam
plin
g:
42
;la
tesa
mp
ling
:1
2In
univ
aria
tean
alys
is,
asso
ciat
ion
with
ICU
but
not
hosp
ital
mo
rtal
ity.
No
tin
dep
end
ent
pre
dic
tor
of
surv
ival
Bab
uin
etal
.[3
0]
Ret
rosp
ectiv
e,no
nco
nsec
utiv
e9
29
Med
ical
ICU
cTnT
Ad
mis
sio
n6
1,
4In
dep
end
ent
asso
ciat
ion
with
:3
0-d
aym
ort
ality
,in
-ho
spita
lm
ort
ality
,lo
ng-t
erm
mo
rtal
ityLi
met
al.
[31
,32��
]P
rosp
ectiv
e,co
nsec
utiv
e1
03
Med
ical
surg
ical
ICU
14
%ha
dca
rdio
vasc
ular
dia
gno
sis
on
adm
issi
on,
1ha
dM
I
cTnT
Scr
eene
dat
ICU
adm
issi
on
and
then
onc
ed
aily
for
the
first
wee
k;o
nal
tern
ate
day
sfo
rup
to1
mo
nth;
then
wee
kly
until
ICU
dea
tho
rd
isch
arg
efo
ra
max
imum
of
2m
ont
hs
50
.5In
dep
end
ent
pre
dic
tor
of
hosp
ital
mo
rtal
ityb
utno
to
fIC
Um
ort
ality
Vas
ileet
al.
[33��
]R
etro
spec
tive,
nonc
ons
ecut
ive
20
78
Med
ical
ICU
cTnT
Ad
mis
sio
n4
2,
3In
dep
end
ent
asso
ciat
ion
with
:3
0-d
aym
ort
ality
,in
-ho
spita
lm
ort
ality
,lo
ng-t
erm
mo
rtal
ity
LOS
,le
ngth
of
stay
.D
ata
fro
m[1
6–
31
,32��
,33��
].

C
458 Cardiovascular system
detect regional or global wall motion abnormalities in only
four cases. Given the fact that the prevalence of both
troponin elevation and of ECG abnormalities in the
ICU is high and that both findings are relatively non-
specific for MI, there is high probability that at least some
patients in the cohort of Lim et al. [32��] with both elevated
troponin and ECG abnormalities did not actually have MI.
Unluckily, neither Booker et al. nor Lim et al. routinely
performed echocardiograms as part of their screening
protocol, whereas angiography was also not part of the
protocol. Thus an unequivocal determination of the exact
frequency of MI in the ICU setting is not possible
at present.
Lim et al. [31] report that in less than half of their MI
patients was a clinical diagnosis possible by ICU staff and
only screening provided 62.2% of MIs ultimately diag-
nosed. They conclude that MI in the ICU can be an
elusive diagnosis in the absence of systematic screening
with troponin and ECGs. An alternative explanation
might be that their screening protocol resulted in over-
diagnosis of MI. Yet, if the findings of Lim et al. are
confirmed by further studies, and the prevalence of MI in
unselected critically ill patients is indeed as high as that
reported by these investigators, then one can ask whether
all critically ill patients should undergo screening (with
troponin and ECG or imaging) for MI. For the time
being, the answer is probably negative: it is currently
unknown whether higher detection rates of MI will
translate into better clinical outcomes through targeted
therapy. The results of the study by Lim et al. also do not
support a strategy of systematic screening: there was
no difference in outcome between patients with MI
detected by staff and MI detected solely by screening.
With clinicians blinded as to the screening diagnosis
which did not affect patient management in their cohort,
this casts doubt to the hypothesis that a diagnosis of MI
can improve outcome in the critically ill [31]. On the
contrary, further prospective studies with screening
(including troponin, ECG and probably echocardiogra-
phy as well) to further clarify the cause of troponin
elevations in the ICU would be highly welcome.
The prognostic significance of troponin inunselected critically ill patientsThere is no unanimity on the prognostic significance
of troponin in unselected critically ill patients [16–31,
32��,33��] (Table 1). Some investigators report that
troponin is an independent predictor of ICU or hospital
mortality [24,30,31,33��] and others find no association
whatever [18,19]. Other studies report associations with
mortality, but they either do not control for other vari-
ables [16,20–23,26] or these associations do not persist in
multivariate analysis [17,25,27].
opyright © Lippincott Williams & Wilkins. Unauth
Associations have also been reported with length of ICU
[16,21,24] and hospital stay [24,40], although in this case
there is no adjustment for other variables.
A meta-analysis concluded that troponin was a univariate
predictor of death in the ICU (eight studies with no
adjustment for confounding variables, with a total of
1019 patients), whereas cumulative data from six more
studies with adjustment for confounding variables (a total
of 1706 patients) demonstrated that troponin was an
independent predictor of death [odds ratio (OR) 2.5;
95% confidence interval (CI) 1.9–3.4]. Moreover, this
meta-analysis concluded that troponin was associated
with an increased length of ICU stay of 3.0 days and
an increased length of hospital stay of 2.2 days (unad-
justed data) [15].
Reaffirmation of a prognostic significance for troponin is
provided by a large retrospective study by Babuin et al.[30]. They reviewed the files of 1657 consecutive unse-
lected patients admitted to medical ICU, 929 of whom
had a cTnT measurement within 6 h of admission.
Cardiovascular causes of admission were not excluded.
Troponin was elevated in 61.3% of the patients, with
mostly small to modest increases. Troponin was an inde-
pendent predictor of 30-day and in-hospital mortality
with no difference observed between cardiovascular
and noncardiovascular admissions.
A recent retrospective study of 240 critically ill patients
with normal (<0.1 ng/ml) or intermediate (0.1–1.49 ng/ml)
cTnI levels, concludes that even borderline elevations
of cTnI are independently associated with in-hospital
mortality and length of ICU stay (but not length of
hospital stay, readmission rate, or postdischarge mortality
at 6 months) [40].
Surprisingly, in the study of Babuin et al. [30] elevated
cTnT on admission was independently associated with
long-term mortality even at 3 years of follow-up, with no
difference observed between cardiovascular and noncar-
diovascular admissions. Two more retrospective studies
from the same group [33��,41] support an association of
troponin at admission to the ICU with long-term out-
come. Elevated troponin upon admission was indepen-
dently associated with in-hospital, short-term and long-
term mortality (up to 3 years follow-up) in a cohort of
2078 patients who had troponin measurement out of a
total of 4433 consecutive admissions to the ICU for a
respiratory condition [33��]. In another retrospective
cohort of 754 patients who had troponin measurements
out of a total of 1076 consecutive ICU admissions for
acute gastrointestinal bleeding, troponin levels on admis-
sion were independently associated with long-term
mortality (though not with short-term mortality) [41].
These findings suggest that even after hospital discharge
orized reproduction of this article is prohibited.

Increased blood troponin levels in ICU patients Markou et al. 459
there might be an opportunity to intervene in patients
who were troponin-positive on admission to the ICU, in
an effort to improve long-term outcome.
An older study by Lim et al. suggests that the prognostic
significance of troponin elevations in the ICU may vary
depending on the cause of troponin elevation, for example
myocardial ischemia vs. nonischemic origin: they con-
cluded that MI during ICU stay is an independent pre-
dictor of hospital mortality [odds ratio (OR) 3.2], whereas
an isolated increase in troponin was not independently
predictive of ICU or hospital mortality [25]. Later high-
quality prospective data from the same group [31,32��]
indeed confirmed that prognostic significance depends on
the cause of troponin elevation, but the implications
on prognosis were different, with troponin elevation in
the absence of MI appearing to favor a worse outcome. In
this cohort, ICU mortality was 2.0% for patients with no
troponin elevation, 23.1% in patients with MI, and 39.1%
in patients with troponin elevation not due to MI. Elevated
troponin in the absence of MI was independently associ-
ated with hospital (but not ICU) mortality. Associations
of elevated troponin in the presence of MI with mortality
did not persist in multivariate analysis [31].
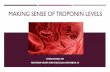
Troponin in sepsisTroponin elevation is a common finding in patients with
sepsis [42–57,58��,59��] (Table 2). Troponin levels in
these patients seem to be associated with disease severity
[42–47,50,58��,59��] and presence of shock [47,55,59��],
whereas a study of hospitalized bacteremic patients
also reports associations with kidney function, severity
of the underlying infection, and underlying cardiac
disease [60].
The close association of high-sensitivity troponin T
(hs-TnT) with N-terminal pro b-type natriuretic peptide
(NT-proBNP) suggests myocardial origin of troponin
elevation in sepsis [59��]. Although some septic patients
with elevated troponin may have either nonspecific ECG
changes [46,50] or regional wall motion abnormalities
[47], on the whole, neither objective testing [22,45,46]
nor the high occurrence of elevated troponin in a popu-
lation of pediatric sepsis [48] supports the concept that
flow-limiting coronary artery disease is the main cause of
troponin release in sepsis. Troponin release in this
population is most probably the result of low-grade
cytokine-mediated cardiomyocyte injury with transient
loss in membrane integrity and troponin leakage. Sepsis-
related factors like apoptosis, increase in intracellular
calcium, oxidative stress or uncoupling of oxidative phos-
phorylation may also contribute, whereas microvascular
thrombotic injury or systemic hypotension resulting in
suboptimal coronary artery blood flow cannot be excluded
as additive factors in some cases [61–63,64�].
Copyright © Lippincott Williams & Wilkins. Unaut
A recent study concludes that thrombus-associated myo-
cardial damage is unlikely to have a major role in troponin
release in sepsis. The authors studied 38 consecutive
patients with sepsis without evidence of ACS, 58% of
whom were cTnI-positive. Extensive investigation of
coagulation parameters could not demonstrate differences
between cTnI-positive and negative patients in the extrin-
sic, intrinsic or common pathway of coagulation [64�].
It has long been observed that troponin may be associated
with nonischemic systolic dysfunction, mainly in patients
with sepsis [43,45,47,49] but also in unselected critically ill
patients [22]. The more recent findings of Bouhemad et al.[54,65] expand this association to nonischemic diastolic
dysfunction as well, with troponin featuring as a reliable
index of sepsis-induced myocardial dysfunction.
Bouhemad et al. studied prospectively 54 patients with
septic shock: at days 1, 2, 3, 4, 7, and 10 after onset of
septic shock they performed echocardiography with
tissue Doppler and measurement of cTnI and cytokines.
An increase in cTnI was observed in 22 patients, half of
whom had both systolic and diastolic dysfunction
together with acute and left-ventricular dilation, whereas
the rest had isolated impairment of left-ventricular re-
laxation. Echocardiographic findings in patients with
increased cTnI were reversible with reversal of shock.
Improvement of diastolic dysfunction went in parallel with
a progressive decrease in cTnI values and with decreases in
tissue necrosis factor-alpha (TNF-a), IL-8, and IL-10.
The observed improvement in impaired myocardial per-
formance after disease recovery, speaks against major
myocardial cell death in sepsis. On the contrary, patients
with normal cTnI values had either normal systolic and
diastolic function, or in some cases, diastolic dysfunction
that persisted after reversal of shock (and most probably
pre-existed) [54,65]. Associations with mortality were not
assessed in this cohort [54,65], but according to other
investigators diastolic dysfunction is an independent
predictor of hospital survival in septic shock [57].
Although measurements of troponin may facilitate recog-
nition of sepsis-induced myocardial dysfunction, the lack
of established treatment for this entity limits the role of
troponin in the management of sepsis at this time. On the
contrary, troponin can be utilized in the context of
future therapeutic trials in order to target patients with
possible sepsis-induced myocardial dysfunction.
A single-center study by John et al. [50] suggests that
troponin can be used to guide treatment with activated
protein C (APC). In this study patients were prospec-
tively defined but cTnI was measured at the discretion of
the primary physician. The same study group in a retro-
spective analysis of data from the PROWESS study could
not replicate this finding [58��]. Further study is needed
horized reproduction of this article is prohibited.
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
460 Cardiovascular system
Ta
ble
2T
rop
on
inin
se
psis
Ref
eren
ceS
tud
yd
esig
nN
umb
eran
dty
pe
of
pat
ient
scT
nty
pe
Sam
plin
gp
roto
col
Fre
que
ncy
of
elev
ated
cTn
(%)
Ass
oci
atio
nw
ithm
ort
ality
Sp
ies
etal
.[4
2]
Pro
spec
tive.
Enr
ollm
ent
not
spec
ified
26
-sur
gic
alIC
UcT
nTE
very
4h
on
day
1.
The
nd
aily
for
7d
ays
69
No
tad
dre
ssed
Fer
nand
eset
al.
[43
]P
rosp
ectiv
e.E
nro
llmen
tno
tsp
ecifi
ed1
0-m
edic
alsu
rgic
alcT
nIW
ithin
12
hfr
om
adm
issi
on
60
Incr
ease
dse
psi
sm
ort
ality
(uni
varia
te)
Tur
ner
etal
.[4
4]
Pro
spec
tive,
cons
ecut
ive.
Cas
e-co
ntro
lM
edic
al-s
urg
ical
;1
5p
atie
nts
with
sep
tican
d6
nons
eptic
sho
ckco
ntro
ls
cTnI
Dai
lyun
tilen
do
fse
psi
s8
0vs
.1
7in
cont
rols
No
tad
dre
ssed
ver
Els
tet
al.
[45
]P
rosp
ectiv
e,co
nsec
utiv
eM
edic
al-s
urg
ical
.4
6p
atie
nts
with
sep
ticsh
ock
cTnI
,cT
nTE
nro
llmen
t,2
4an
d4
8h
50
cTnI
,3
6cT
nTA
sso
ciat
ion
with
hosp
ital
mo
rtal
ity(u
niva
riate
anal
ysis
)A
mm
ann
etal
.[4
6]
Pro
spec
tive,
cons
ecut
ive.
Cas
e-co
ntro
l2
0p
atie
nts
with
sep
sis,
20
nons
eptic
criti
cally
illco
ntro
lscT
nIW
ithin
24
fro
mo
nset
85
vs.
0in
cont
rols
No
tad
dre
ssed
Meh
taet
al.
[47
]P
rosp
ectiv
e,co
nsec
utiv
eM
edic
alsu
rgic
al.
37
sep
ticsh
ock
cTnI
Enr
ollm
ent,
24
,4
8h
43
Incr
ease
dIC
Um
ort
ality
(uni
varia
te)
Fen
ton
etal
.[4
8]
Pro
spec
tive.
Enr
ollm
ent
not
spec
ified
23
child
ren
with
sep
ticsh
ock
cTnI
Initi
al7
2h
57
Briv
etet
al.
[49
]P
rosp
ectiv
e;en
rollm
ent
not
spec
ified
No
tsp
ecifi
ed.
11
8cT
nIN
ot
spec
ified
No
tsp
ecifi
edN
oas
soci
atio
nw
ithho
spita
lm
ort
ality
(mul
tivar
iate
anal
ysis
)Jo
hnet
al.
[50
]P
rosp
ectiv
e;no
nco
nsec
utiv
e1
05
pat
ient
sw
ithse
vere
sep
sis
cTnI
Enr
ollm
ent
46
Incr
ease
dse
psi
sm
ort
ality
(uni
varia
te)
Sco
ttet
al.
[51
]P
rosp
ectiv
e.C
ons
ecut
ive
pat
ient
sre
qui
ring
pul
mo
nary
arte
ryca
thet
er6
6;
surg
ical
ICU
.S
ever
ese
psi
s,se
ptic
sho
ckcT
nIA
tca
thet
eriz
atio
nan
dev
ery
6–
8h
ther
eaft
er6
4N
oas
soci
atio
nw
ithm
ort
ality
Yuc
elet
al.
[52
]P
rosp
ectiv
e,co
nsec
utiv
e4
0p
atie
nts
adm
itted
with
sep
sis
tom
edic
al-s
urg
ical
ICU
cTnI
At
adm
issi
on,
day
2,
day
of
dis
char
ge
No
tsp
ecifi
edA
sso
ciat
ion
(uni
varia
tean
alys
is)
afte
rd
ay1
with
ICU
mo
rtal
ityC
hoo
n-ng
arm
and
Par
tpis
anu
[53
]4
0w
ithse
ptic
sho
ckcT
nT4
2,
5A
sso
ciat
ion
with
mo
rtal
ity(u
niva
riate
anal
ysis
)B
ouh
emad
etal
.[5
4]
Pro
spec
tive.
Enr
ollm
ent
not
spec
ified
Sur
gic
alIC
U.
Sep
ticsh
ock
54
cTnI
.D
ays
1,2
,3
,4
,7,
10
40
Incr
ease
d(u
niva
riate
anal
ysis
)O
livei
raet
al.
[55
]P
rosp
ectiv
e.C
ons
ecut
ive
21
8P
edia
tric
ICU
cTnI
With
in2
4h
fro
men
rollm
ent
4.5
No
asso
ciat
ion
with
hosp
ital
mo
rtal
ity(m
ultiv
aria
tean
alys
is)
Kan
get
al.
[56
]Lo
ng-t
erm
follo
w-u
pfo
rse
psi
so
fa
coho
rto
f3
05
ES
RD
pat
ient
s1
21
ES
RD
pat
ient
sw
ithse
psi
scT
nIO
nset
of
sep
sis
41
.3In
dep
end
ent
asso
ciat
ion
with
3-m
ont
han
d6
-mo
nth
mo
rtal
ityS
turg
ess
etal
.[5
7]
Pro
spec
tive
cons
ecut
ive
Med
ical
-sur
gic
alIC
U2
1se
ptic
sho
ckcT
nTW
ithin
72
ho
fsh
ock
67
No
asso
ciat
ion
with
hosp
ital
mo
rtal
ity(m
ultiv
aria
tean
alys
is)
John
etal
.[5
8��
]R
etro
spec
tive
dat
afr
om
PR
OW
ES
Sst
udy.
No
nco
nsec
utiv
e5
98
of
16
90
pat
ient
s(t
hose
who
had
avai
lab
lere
sults
)cT
nIE
nro
llmen
t7
5In
dep
end
ent
pre
dic
tor
of
28
-day
mo
rtal
ityR
øsj
øet
al.
[59��
]N
onc
ons
ecut
ive;
pat
ient
sad
mitt
edto
ICU
with
seve
rese
psi
sS
ubg
roup
fro
mF
INN
SE
PS
ISst
udy
25
4C
onv
entio
nal
cTnT
assa
y;hs
-cT
nTas
say
Ad
mis
sio
nto
ICU
,7
2h
Ad
mis
sio
n:4
2w
ithfo
urth
-gen
erat
ion
assa
y,8
0w
ithhs
-cT
nIas
say
No
asso
ciat
ion
with
hosp
ital
mo
rtal
ity(m
ultiv
aria
tean
alys
is)
Dat
afr
om
[42
–5
7,5
8��
,59��
].

Increased blood troponin levels in ICU patients Markou et al. 461
to determine whether troponin can serve as a simple,
readily available marker to identify which patients with
severe sepsis will benefit from APC, or possibly from
other innovative treatments of sepsis.
Prognostic significance of troponin in septicpatientsSeveral [43,45,47,52], but not all [49,51,55] studies con-
clude that troponin is an independent predictor of
adverse short-term outcome in sepsis (Table 2), whereas
it has also been associated with length of ICU stay in
sepsis patients [47]. Reasons for differences in the pre-
dictive role of troponins in sepsis may be related to small
sample size in some studies or to differences in the
characteristics of troponin assays utilized.
Recently, three sepsis studies reporting on associations
between elevated troponin and outcome were published
[56,58��,59��].
The study of John et al. [58��] was a retrospective analysis
of material from the PROWESS study: baseline cTnI
data were available in 598 nonconsecutive patients from
this cohort. Troponin-positive patients had a significantly
higher 28-day mortality (32 vs. 14%) and this difference
was observed in both the APC-treated and placebo-treated
groups. Elevated cTnI was also an independent predictor
of mortality (OR 2.020; 95% CI 1.153–3.541) [58��].
In a retrospective cohort of 121 patients with end-stage
renal disease (ESRD) and sepsis, cTnI was an indepen-
dent predictor of mortality at 90 days from onset of sepsis
(OR 5.13) and of mortality at more protracted follow-up
(180 days) (hazard ratio 5.90; 95% CI 2.06–16.9) [56].
It should be noted that the cut-off value for troponin
in this study was defined as the value providing the best
diagnostic accuracy for mortality based on receiver
operating characteristic curve (ROC) analysis and not
the cut-off by the manufacturer.
The study by Røsjø et al. [59��] reported on a subgroup of
patients from the prospective FINNSEPSIS study. From
a total of 470 patients who were enrolled with severe
sepsis or septic shock in this cohort, 254 consented for
blood sampling for troponin: cTnT levels were measured
by a novel hs-cTnT assay at two time points (inclusion
and 72 h thereafter). Results for the hs-cTnT assay were
compared to those of the established fourth-generation
cTnT assay (lower limit of detection 0.003 mg/l vs.
0.01 mg/l for fourth-generation assay). At inclusion in
the study, cTnT was detectable in 60% of patients with
the conventional assay and in 100% with the hs-cTnT
assay, whereas increased levels were found in 42% with
the standard assay and in 80% with hs-cTnT assay. At
72 h, troponin was still detected in 57% of patients with
the conventional assay and in 100% with hs-cTnT assay,
Copyright © Lippincott Williams & Wilkins. Unaut
whereas it remained elevated in 7% of patients with the
conventional assay and in 79% with the hs-cTnT assay.
Survivors had higher levels of hs-cTnT on inclusion,
whereas no difference in troponin values was observed
with the conventional assay. Troponin was not indepen-
dently associated with in-hospital mortality, regardless of
assay but, interestingly, hs-cTnT on inclusion was inde-
pendently associated with development of shock during
hospitalization (OR 2.45; 95% CI 1.09–5.53) and could
predict development of septic shock with a sensitivity of
86% and specificity of 33% [59��]. This role of cTnT as an
index of impending shock in early sepsis needs to be
confirmed in further studies.
The study by Røsjø et al. highlights the importance of
the characteristics of troponin assays which may be a
partial explanation for the divergence of results between
existing studies of troponin in critical illness and sepsis.
ConclusionTroponin is frequently elevated in the critically ill, and
recent data suggest that MI is the underlying (and often
unrecognized) cause of such elevations in a large pro-
portion of these patients. Recent studies also reinforce
the impression that troponin may be an independent
predictor of short-term outcome in critical illness and
expand the predictive role of troponin to the long-term
outcome of this patient population.
In sepsis, troponin elevations do not seem to be com-
monly related to ACS, but are probably associated with
reversible sepsis-induced myocardial dysfunction. There
are newer data on the predictive role of troponin in sepsis,
although the verdict on this question is not unanimous.
Recent findings on troponin need to be confirmed in
larger and more systematic prospective trials enrolling
consecutive patients. More research is also needed on the
possible implications of these findings in the clinical
management of mixed critically ill patients and patients
with severe sepsis or septic shock.
AcknowledgementsConflicts of interestThere are no conflicts of interest.
References and recommended readingPapers of particular interest, published within the annual period of review, havebeen highlighted as:� of special interest�� of outstanding interest
Additional references related to this topic can also be found in the CurrentWorld Literature section in this issue (p. 539).
1 Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction rede-fined-a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardialinfarction. J Am Coll Cardiol 2000; 36:959–969.
horized reproduction of this article is prohibited.

C
462 Cardiovascular system
2 Thygesen K, Alpert JS, White HD, Joint ESC/ACCF/AHA/WHF Task Forcefor the Redefinition of Myocardial Infarction. Universal definition of myocardialinfarction. Circulation 2007; 116:2634–2653.
3 Thygesen K, Alpert JS, Jaffe AS, White HD. Diagnostic application of theuniversal definition of myocardial infarction in the intensive care unit. CurrOpin Crit Care 2008; 14:543–548.
4 Bertsch T, Braun SL, Giannitis E, et al. Conference on clinical use of troponinT high sensitive (TnThs) on September 8, 2009 at the airport conferencecenter, Frankfurt/Main. Clin Lab 2010; 56:355–358.
5 Mac Rae AR, Kavsak PA, Lustig V. Assessing the requirement for the 6-hourinterval between specimens in the American Heart Association Classificationof Myocardial Infarction in epidemiology and clinical research studies. ClinChem 2006; 52:812–818.
6 Keller T, Zeller T, Peetz D, et al. Sensitive troponin I assay in early diagnosis ofacute myocardial infarction. N Engl J Med 2009; 361:868–877.
7 Reichlin T, Hochholzer W, Bassetti S, et al. Early diagnosis of myocardialinfarction with sensitive cardiac troponin assays. N Engl J Med 2009;361:858–867.
8 Jeremias A, Gibson CM. Narrative review: alternative causes for elevatedcardiac troponin levels when acute coronary syndromes are excluded. AnnIntern Med 2005; 142:786–791.
9 Agzew Y. Elevated serum cardiac troponin in nonacute coronary syndrome.Clin Cardiol 2009; 32:15–20.
10
�Ilva TJ, Eskola MJ, Nikus KC, et al. The etiology and prognostic significanceof cardiac troponin I elevation in unselected emergency department patients.J Emerg Med 2010; 38:1–5.
Large prospective study of causes of troponin elevation in the emergency depart-ment.
11
�Lee HM, Kerr D, O’H Ici D, Kelly AM. Clinical significance of initial troponin I inthe grey zone in emergency department chest pain patients: a retrospectivepilot study. Emerg Med J 2010; 27:302–304.
A retrospective study of patients assessed for ACS in emergency department.
12 Omland T, de Lemos JA, Sabatine MS, et al. Prevention of Events withAngiotensin Converting Enzyme Inhibition (PEACE) Trial Investigators. Asensitive cardiac troponin T assay in stable coronary artery disease. N EnglJ Med 2009; 361:2538–2547.
13 Fromm RE Jr. Cardiac troponins in the intensive care unit: common causesof increased levels and interpretation. Crit Care Med 2007; 35:584–588.
14 Lim W. JOE DOUPE LECTURE: cardiac troponin in the intensive care unit.Clin Invest Med 2009; 32:E405–E410.
15 Lim W, Qushmaq I, Devereaux PJ, et al. Elevated cardiac troponin measure-ments in critically ill patients. Arch Intern Med 2006; 166:2446–2454.
16 Guest TM, Ramanathan AV, Tuteur PG, et al. Myocardial injury in critically illpatients. A frequently unrecognized complication. J Am Med Assoc 1995;273:1945–1949.
17 Kollef MH, Ladenson JH, Eisenberg PR. Clinically recognized cardiac dys-function: an independent determinant of mortality among critically ill patients.Is there a role for serial measurement of cardiac troponin I? Chest 1997;111:1340–1347.
18 Noble JS, Reid AM, Jordan LV, et al. Troponin I and myocardial injury in theICU. Br J Anaesth 1999; 82:41–46.
19 Klein Gunnewiek JM, van de Leur JJ. Elevated troponin T concentrations incritically ill patients. Intensive Care Med 2003; 29:2317–2322.
20 Booker KJ, Holm K, Drew BJ, et al. Frequency and outcomes of transientmyocardial ischemia in critically ill adults admitted for noncardiac conditions.Am J Crit Care 2003; 12:508–516.
21 Relos RP, Hasinoff IK, Beilman GJ. Moderately elevated serum troponinconcentrations are associated with increased morbidity and mortalityrates in surgical intensive care unit patients. Crit Care Med 2003; 31:2598–2603.
22 Ammann P, Maggiorini M, Bertel O, et al. Troponin as a risk factor for mortalityin critically ill patients without acute coronary syndromes. J Am Coll Cardiol2003; 41:2004–2009.
23 Wu TT, Yuan A, Chen CY, et al. Cardiac troponin I levels are a risk factor formortality and multiple organ failure in noncardiac critically ill patients and havean additive effect to the APACHE II score in outcome prediction. Shock 2004;22:95–101.
24 Quenot JP, Le Teuff G, Quantin C, et al. Myocardial injury in critically illpatients: relation to increased cardiac troponin I and hospital mortality. Chest2005; 128:2758–2764.
25 Lim W, Qushmaq I, Cook DJ, et al., Troponin T Trials Group. Elevated troponinand myocardial infarction in the intensive care unit: a prospective study. CritCare 2005; 9:R636–R644.
opyright © Lippincott Williams & Wilkins. Unauth
26 Minkin R, Cotiga D, Noack S, et al. Use of admission troponin in critically illmedical patients. J Intensive Care Med 2005; 20:334–338.
27 King DA, Codish S, Novack V, et al. The role of cardiac troponin I as aprognosticator in critically ill medical patients: a prospective observationalcohort study. Crit Care 2005; 9:R390–R395.
28 Landesberg G, Vesselov Y, Einav S, et al. Myocardial ischemia, cardiactroponin, and long-term survival of high-cardiac risk critically ill intensive careunit patients. Crit Care Med 2005; 33:1281–1287.
29 Lim W, Cook DJ, Griffith LE, et al. Elevated cardiac troponin levels in criticallyill patients: prevalence, incidence, and outcomes. Am J Crit Care 2006;15:280–288.
30 Babuin L, Vasile VC, Rio Perez JA, et al. Elevated cardiac troponin is anindependent risk factor for short- and long-term mortality in medical intensivecare unit patients. Crit Care Med 2008; 36:759–765.
31 Lim W, Holinski P, Devereaux PJ, et al. Detecting myocardial infarction incritical illness using screening troponin measurements and ECG recordings.Crit Care 2008; 12:R36.
32
��Lim W, Whitlock R, Khera V, et al. Etiology of troponin elevation in critically illpatients. J Crit Care 2010; 25:322–328.
Prospective study applying systematic screening with troponin and ECG inunselected critically ill patients and searching for causes of elevation of troponin.
33
��Vasile VC, Chai HS, Khambatta S, et al. Significance of elevated cardiactroponin T levels in critically ill patients with acute respiratory disease. Am JMed 2010; 123:1049–1058.
Large retrospective study of troponin in patients admitted to the ICU for respiratoryconditions. Associations with both short-term and long-term mortality were ob-served.
34 Arlati S, Brenna S, Prencipe L, et al. Myocardial necrosis in ICU patients withacute noncardiac disease: a prospective study. Intensive Care Med 2000;26:31–37.
35 King DA, Almog Y. Myocardial infarction complicating critical illness. Crit Care2005; 9:634–635.
36 Bhatti N, Amoateng-Adjepong Y, Qamar A, Manthous CA. Myocardialinfarction in critically ill patients presenting with gastrointestinal hemor-rhage: retrospective analysis of risks and outcomes. Chest 1998; 114:1137–1142.
37 Lim W, Qushmaq I, Cook DJ, et al. Reliability of electrocardiogram interpreta-tion in critically ill patients. Crit Care Med 2006; 34:1338–1343.
38 Lim W, Tkaczyk A, Holinski P, et al. The diagnosis of myocardial infarction incritically ill patients: an agreement study. J Crit Care 2009; 24:447–452.
39
�Rennyson SL, Hunt J, Haley MW, et al. Electrocardiographic ST-segmentelevation myocardial infarction in critically ill patients: an observational cohortanalysis. Crit Care Med 2010; 38:2304–2309.
A retrospective study evaluating the significance of ST-segment elevation in theICU, in association with troponin levels.
40 Stein R, Gupta B, Agarwal S, et al. Prognostic implications of normal(<0.10 ng/ml) and borderline (0.10 to 1.49 ng/ml) troponin elevation levelsin critically ill patients without acute coronary syndrome. Am J Cardiol 2008;102:509–512.
41 Vasile VC, Babuin L, Rio Perez JA, et al. Long-term prognostic significance ofelevated cardiac troponin levels in critically ill patients with acute gastro-intestinal bleeding. Crit Care Med 2009; 37:140–147.
42 Spies C, Haude V, Fitzner R, et al. Serum cardiac troponin T as a prognosticmarker in early sepsis. Chest 1998; 113:1055–1063.
43 Fernandes CJ Jr, Akamine N, Knobel E. Cardiac troponin: a new serummarker of myocardial injury in sepsis. Intensive Care Med 1999; 25:1165–1168.
44 Turner A, Tsamitros M, Bellomo R. Myocardial cell injury in septic shock. CritCare Med 1999; 27:1775–1780.
45 ver Elst KM, Spapen HD, Nguyen DN, et al. Cardiac troponins I and T arebiological markers of left ventricular dysfunction in septic shock. Clin Chem2000; 46:650–657.
46 Ammann P, Fehr T, Minder EI, et al. Elevation of troponin I in sepsis and septicshock. Intensive Care Med 2001; 27:965–969.
47 Mehta NJ, Khan IA, Gupta V, et al. Cardiac troponin I predicts myocardialdysfunction and adverse outcome in septic shock. Int J Cardiol 2004; 95:13–17.
48 Fenton KE, Sable CA, Bell MJ, et al. Increases in serum levels of troponin I areassociated with cardiac dysfunction and disease severity in pediatric patientswith septic shock. Pediatr Crit Care Med 2004; 5:533–538.
49 Brivet FG, Jacobs FM, Colin P, et al. Cardiac troponin level is not anindependent predictor of mortality in septic patients requiring medicalintensive care unit admission. Crit Care 2006; 10:404.
orized reproduction of this article is prohibited.

Increased blood troponin levels in ICU patients Markou et al. 463
50 John J, Awab A, Norman D, et al. Activated protein C improves survival in severesepsis patients with elevated troponin. Intensive Care Med 2007; 33:2122–2128.
51 Scott EC, Ho HC, Yu M, et al. Preexisting cardiac disease, troponin I elevationand mortality in patients with severe sepsis and septic shock. AnaesthIntensive Care 2008; 36:51–59.
52 Yucel T, Memis D, Karamanlioglu B, et al. The prognostic value of atrial andbrain natriuretic peptides, troponin I and C-reactive protein in patients withsepsis. Exp Clin Cardiol 2008; 13:183–188.
53 Choon-ngarm T, Partpisanu P. Serum cardiac troponin-T as a prognosticmarker in septic shock. J Med Assoc Thai 2008; 91:1818–1821.
54 Bouhemad B, Nicolas-Robin A, Arbelot C, et al. Isolated and reversibleimpairment of ventricular relaxation in patients with septic shock. Crit CareMed 2008; 36:766–774.
55 Oliveira NS, Silva VR, Castelo JS, et al. Serum level of cardiac troponin I inpediatric patients with sepsis or septic shock. Pediatr Crit Care Med 2008;9:414–417.
56 Kang EW, Na HJ, Hong SM, et al. Prognostic value of elevated cardiactroponin I in ESRD patients with sepsis. Nephrol Dial Transplant 2009;24:1568–1573.
57 Sturgess DJ, Marwick TH, Joyce C, et al. Prediction of hospital outcome inseptic shock: a prospective comparison of tissue Doppler and cardiacbiomarkers. Crit Care 2010; 14:R44.
58
��John J, Woodward DB, Wang Y, et al. Troponin-I as a prognosticator ofmortality in severe sepsis patients. J Crit Care 2010; 25:270–275.
Retrospective analysis of material from the PROWESS study. Troponin was anindependent predictor of mortality in patients with sepsis.
Copyright © Lippincott Williams & Wilkins. Unaut
59
��Røsjø H, Varpula M, Hagve TA, et al., FINNSEPSIS Study Group. Circulatinghigh sensitivity troponin T in severe sepsis and septic shock: distribution,associated factors, and relation to outcome. Intensive Care Med 2011;37:77–85.
Retrospective analysis of data from the prospective FINNSEPSIS study. Compar-ison of a conventional cTnT assay, with a novel hs-cTnT assay in patients withsepsis.
60 Kalla C, Raveh D, Algur N, et al. Incidence and significance of a positivetroponin test in bacteremic patients without acute coronary syndrome. Am JMed 2008; 121:909–915.
61 Maeder M, Fehr T, Rickli H, Ammann P. Sepsis-associated myocardialdysfunction. Diagnostic and prognostic impact of cardiac troponins andnatriuretic peptides. Chest 2006; 129:1349–1366.
62 Fernandes CJ Jr, Akamine N, Knobel E. Myocardial depression in sepsis.Shock 2008 (Suppl 1):S14–S17.
63 Favory R, Neviere R. Significance and interpretation of elevated troponin inseptic patients. Crit Care 2006; 10:224.
64
�Altmann DR, Korte W, Maeder MT, et al. Elevated cardiac troponin I in sepsisand septic shock: no evidence for thrombus associated myocardial necrosis.PLoS One 2010; 5:e9017.
Prospective study investigating the association of troponin elevation in sepsis withcoagulation abnormalities.
65 Bouhemad B, Nicolas-Robin A, Arbelot C, et al. Acute left ventricular dilatationand shock-induced myocardial dysfunction. Crit Care Med 2009; 37:441–447.
horized reproduction of this article is prohibited.
Related Documents