Incarcerated youth with personality disorders: Prevalence, comorbidity and convergent validity KATIE KASZYNSKI 1,3 , DIANA L. KALLIS 3 , NIRANJAN KARNIK 2 , MARIE SOLLER 4 , SCOTT HUNTER 2 , RUDY HAAPANEN 5 , JAMES BLAIR 6 AND HANS STEINER 7 , 1 Psychol- ogy, Illinois Institute of Technology, Chicago, IL, USA; 2 Department of Psychiatry and Behavioral Neuroscience, University of Chicago, Chicago, IL, USA; 3 Department of Psychiatry, Wright State University, Fairborn, OH, USA; 4 Wildwood Psychiatric Resource Center, Beaverton, OR, USA; 5 Center for Public Policy Research, University of California Davis, Davis, CA, USA; 6 Unit on Affective Cognitive Neuroscience, National Institute of Mental Health, Bethesda, MD, USA; 7 Department of Psychiatry & Behavioral Science, Stanford University School of Medicine, Stanford, CA, USA ABSTRACT Objective – The aims of this study were to examine the prevalence and comorbidities of personality disorders among incarcerated juveniles and to investigate the validity of these results. Method – A sample of 790 incarcerated youth (650 boys and 140 girls; mean age = 16.8 years) completed an assessment of Axis II diagnoses (Structured Interview for DSM-IV Personality). Subjects also completed secondary questionnaires assessing anger–irritability (Youth Self-Report (YSR)), aggression (YSR), delinquency (Massachusetts Youth Screening Instrument-2), and distress and restraint (Weinberger Adjustment Inventory). Results – Personality disorders can be found among incarcerated youth at high rates. Many meet the criteria for more than one personality disorder. Those with personality disorders have significant elevations of anger–irritability, aggression, delinquency, and distress and reduced restraint compared with incarcerated youth without a personality disorder. Conclusions – Results indicate that personality disorders can be found in incarcerated youth at high rates. These findings further our understanding of chronic psychiatric illness and possibly criminal recidivism in this at-risk population. Addition of personality measures in the assessment of delinquents may assist in the development of more effective interventions. Furthermore, the supportive convergent validity of these findings in a population younger than 18 years may indicate a need to reassess the current rationale for the diagnosis of Axis II disorders. Copyright © 2013 John Wiley & Sons, Ltd. Introduction Teplin, Abram, and McClelland (2002) found that as many as 75% of youth offenders in deten- tion have at least one diagnosable psychiatric disorder. Our group recently reported that exclud- ing conduct disorder (CD) or oppositional defiant disorder, over 88% of youths had a psychiatric dis- order and over 80% had a substance use disorder (Karnik et al., 2009, 2010). Although substance Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014) DOI: 10.1002/pmh Personality and Mental Health 8: 42–51 (2014) Published online 7 August 2013 in Wiley Online Library (wileyonlinelibrary.com) DOI 10.1002/pmh.1241

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Incarcerated youth with personality disorders:Prevalence, comorbidity and convergentvalidity
KATIE KASZYNSKI1,3, DIANA L. KALLIS3, NIRANJAN KARNIK2, MARIE SOLLER4,SCOTT HUNTER2, RUDY HAAPANEN5, JAMES BLAIR6 AND HANS STEINER7, 1Psychol-ogy, Illinois Institute of Technology, Chicago, IL, USA; 2Department of Psychiatry and BehavioralNeuroscience, University of Chicago, Chicago, IL, USA; 3Department of Psychiatry, Wright StateUniversity, Fairborn, OH, USA; 4Wildwood Psychiatric Resource Center, Beaverton, OR, USA;5Center for Public Policy Research, University of California Davis, Davis, CA, USA; 6Unit onAffective Cognitive Neuroscience, National Institute of Mental Health, Bethesda, MD, USA;7Department of Psychiatry & Behavioral Science, Stanford University School of Medicine,Stanford, CA, USA
ABSTRACTObjective – The aims of this study were to examine the prevalence and comorbidities of personality disordersamong incarcerated juveniles and to investigate the validity of these results.Method – A sample of 790 incarcerated youth (650 boys and 140 girls; mean age = 16.8 years) completed anassessment of Axis II diagnoses (Structured Interview for DSM-IV Personality). Subjects also completedsecondary questionnaires assessing anger–irritability (Youth Self-Report (YSR)), aggression (YSR), delinquency(Massachusetts Youth Screening Instrument-2), and distress and restraint (Weinberger Adjustment Inventory).Results – Personality disorders can be found among incarcerated youth at high rates. Many meet thecriteria for more than one personality disorder. Those with personality disorders have significant elevationsof anger–irritability, aggression, delinquency, and distress and reduced restraint compared with incarceratedyouth without a personality disorder.Conclusions – Results indicate that personality disorders can be found in incarcerated youth at high rates. Thesefindings further our understanding of chronic psychiatric illness and possibly criminal recidivism in this at-riskpopulation. Addition of personality measures in the assessment of delinquents may assist in the developmentof more effective interventions. Furthermore, the supportive convergent validity of these findings in a populationyounger than 18 years may indicate a need to reassess the current rationale for the diagnosis of Axis II disorders.Copyright © 2013 John Wiley & Sons, Ltd.
Introduction
Teplin, Abram, and McClelland (2002) foundthat as many as 75% of youth offenders in deten-tion have at least one diagnosable psychiatric
disorder. Our group recently reported that exclud-ing conduct disorder (CD) or oppositional defiantdisorder, over 88% of youths had a psychiatric dis-order and over 80% had a substance use disorder(Karnik et al., 2009, 2010). Although substance
Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014)DOI: 10.1002/pmh
Personality and Mental Health8: 42–51 (2014)Published online 7 August 2013 in Wiley Online Library(wileyonlinelibrary.com) DOI 10.1002/pmh.1241

use disorders are recognized in DSM-IV Text Re-vision (DSM-IV-TR) as psychiatric disorders, sub-stantial research discusses them separately. Thus,the current article will discuss substance use disor-ders as independent from other psychiatric disor-ders. Of the over 30 million youth processedeach year by the US juvenile justice system(JJS), about 100 000 end up in juvenile facilities.Institutionalized youth have a significantly highersaturation and comorbidity of psychiatric and sub-stance use disorders when compared with theircounterparts without institutional commitment(Lewis, Pincus, Lovely, Spitzer, & Moy, 1987;Puzzanchera et al., 2000).
The JJS, responsible for the rehabilitation ofincarcerated youth, is particularly interested inunderstanding how psychiatric illness may retardtheir efforts to effectively help these youth.Historically, clinical interventions have beenimplemented on the basis of easily identifiable riskfactors such as seriousness of offence, aggressivebehaviour and other externalizing behaviours(Barnum and Keilitz, 1992). Interventionalstrategies employed have included deterrenceprogrammes, vocational training and wilderness/challenge (Lipsey, Wilson, & Cothern, 2000).However, because most incarcerated delinquentsare repeat offenders (over 60% in one study), weare faced with evidence that traditional interven-tions are not working (Hollander & Turner,1985). In an updated meta-analysis from his1992 and 1995 works, Lipsey, Wilson, andCothern (2000) found that traditionalprogrammes did not decrease recidivism rates andthat other interventions such as academicprogrammes, family counselling and advocacy/socialwork had mixed or ambiguous evidence as to theirefficacy. He concluded, ‘…without understandingthe variables contributing to these differences, it isdifficult to know whether the effectiveness calcu-lated for this group of treatments was due to thetreatment or to another variable’ (Lipsey et al.,2000; p. 5).
Youth delinquency research seeks to betteridentify and understand the nature and causes of
delinquency. For example, the ubiquitous findingof CD and high rates of comorbidities with otherpsychiatric disorders in populations of incarcer-ated delinquents is well established within theliterature (Cocozza, 1992; Domalanta, Risser,Roberts, & Risser, 2003; Ruchkin, Schwab-Stone,Koposov, Vermeiren, & Steiner, 2002;Wasserman, McReynolds, Lucas, Fisher, &Santos, 2002). However, only about half ofindividuals showing behavioural characteristicsindicative of CD persist in the behaviour intoadulthood, suggesting that there may be otherfactors contributing to delinquent behaviour inyouth (Moffitt & Caspi, 2001; Moffitt, Caspi,Dickson, & Silva, 1996; Teplin, Abram, &McClelland, 1994). For instance, Moffitt andCaspi (2001) differentiated between predictors ofdelinquent behaviour that is limited to adoles-cence and that which persists into adulthood.They suggested that delinquent behaviour that islimited to adolescence is common, likely norma-tive and intended to facilitate autonomy and peeraffiliation during the period of biological andsocial maturity. Conversely, persistent delinquentbehaviour originates early in life and is shown torelate to individual factors such as cognitive defi-cits and hyperactivity, as well as environmentalfactors such as poor parenting, family disruptionand poverty (Moffitt & Caspi, 2001).
In the search to identify more stable, individualcharacteristics as potential contributors to delin-quency, many have begun to investigate theconcept of personality formation and personalitydisorders. Personality, as a developmental andintrinsic process, is associated with self-restraint(Farrell & Sullivan, 2000), impulsivity andpsychopathology (Swann, Bjork, Moeller, &Dougherty, 2002); all of which are characteristicsrelevant to delinquent youth populations.Disturbances in personality functioning have alsobeen shown in previous studies of delinquentyouth (Bowlby, 1944) and perhaps most problem-atic in the form of antisocial personality disorder(APD; Eppright, Kashani, Robison, & Reid,1993). In the latter study, 87% of detained youth
43Personality disorders in incarcerated youth
Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014)DOI: 10.1002/pmh

met the criteria for CD, and 86% of those youthmet the criteria for APD as a comorbid diagnosiswithout using the older than 18 years age require-ment for APD. According to the DSM-IV-TR,persons younger than 18 years cannot be given adiagnosis of APD. Results of recent researchsuggest that there are no clinically significantdifferences between adolescents and adults whomeet the criteria for APD (Jones & Westen,2010; Taylor, Elkins, Legrand, Peuschold, &Iacono, 2007). Additionally, one study found that54% of incarcerated juveniles met the criteria forAPD, 53% of whom also met the criteria forborderline personality disorder (BPD; McManus,Alessi, Grapentine, & Brickman, 1984). Infinding such a high incidence of individualsyounger than 18 years meeting the personalitydisorder criteria, DSM-IV-TR guidelines designat-ing an age cut-off for formally making such adiagnosis may warrant reconsideration.
Personality disorders, according to the DSM-IV-TR, are primarily diagnoses for adults due tothe need for one’s maladaptive behaviours to bepersistent over time and impacting a variety of lifedimensions (APA, 2000). The degree to whichpersonality disorders can be diagnosed in childrenand adolescents is an area of some debate(Kernberg & Shapiro, 2000). A reasonable onto-logical standard would posit that these disorderscould be diagnosed in persons younger than18 years if the particular maladaptive personalitytraits are unlikely to be limited to a developmentalstage or an Axis I disorder. For example, Chanen,Jovev, and Jackson (2007) found that presence ofBPD in a sample of adolescents was a more signif-icant predictor of psychopathology and generalfunctioning when compared with Axis I disorders.There is an explicit exception in the case of APDbecause the diagnosis is tied to the childhooddiagnosis of CD. The nature of this relationshipis vague and difficult to justify on the basis of ourcurrent understanding of the development ofdelinquent patterns and adolescent criminality.
Subpopulations of youth, particularly incarcer-ated youth, represent high-risk individuals in need
of more focused attention and understanding toidentify root causes of psychopathology. It isimportant for research in this area to remain clearin the terminology used to refer to sampled delin-quents. As a general rule, youth in detention facil-ities may or may not be guilty of offences they arecharged with and are instead held in detentionuntil an adjudicatory and/or dispositional hearing.This is an important distinction from incarcera-tion, which means the individual not only hasbeen found responsible but also has been giventhe disposition of an institutional commitmentto a juvenile prison for a determined length oftime. Additionally, incarcerated youth maysometimes be considered ‘detained youth’ as theyspend time in detention awaiting transfer to thecommitment site.
It is imperative that incarcerated youth beidentified by the system to implement propertreatment strategies that may ultimately reducerecidivism and provide rehabilitation, especiallybecause they may not just be syndromally ill butseverely compromised by chronic illness.Knowledge about their psychological well-beingis important not only in understanding the precur-sors to criminal behaviours as adults but also inunderstanding whether the characteristicsunderlying personality disturbances are appropri-ate targets for treatment within the JJS. Personal-ity disorders are notoriously difficult to treat inthe general population, largely due in part to thefailure of adults with personality disorders to seekout and/or follow through with treatment (Benderet al., 2001). Some studies have cited success inthe treatment of personality disorders (mainlyBPD), by pharmaceutically addressing mood orpsychotic symptoms and using psychotherapy toaffect long-term change (Hollander, Swann,Coccaro, Jiang, & Smith, 2005; Verheul &Herbrink, 2007). If incarcerated youth showcharacteristics indicative of personality disorders,targeted interventions within a highly structuredplacement may be more effective than with thegeneral population and could have far-reachingeffects on the health of society.
44 Kaszynski et al.
Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014)DOI: 10.1002/pmh

We hope to expand upon previous findingsthrough investigation of prevalence rates ofpersonality disorders in a large population ofincarcerated youth and their association withother psychopathological variables. To this end,we hypothesize the following: (1) consistent withprevious findings, incarcerated youth will meetthe criteria for at least one personality disorder,and (2) those meeting the personality disordercriteria will have significant elevations of angerand irritability, distress, and aggressive and delin-quent behaviours and reduced levels of restraintcompared with their counterparts not meetingthe personality disorder criteria.
Methods
Participants
Full details of the methods used in this studyhave been reported elsewhere (Karnik et al.,2009). Briefly, this study was conducted at theCalifornia Department of Corrections andRehabilitation, Division of Juvenile Justice(DJJ; at the time of the sampling named theCalifornia Youth Authority), one of the largestjuvenile correctional agencies in the USA. Anindependent Institutional Review Board andthe DJJ’s Research Project Approval Committeereviewed and approved project protocols,including protections of human subjects andconsent/assent forms and procedures. A totalof 1 012 youth met the study’s eligibilitycriteria. Fourteen refused participation, 156were released or paroled from the DJJ beforetheir interviews could be scheduled and 48could not be interviewed because of schedulingproblems. Diagnostic interviews were initiatedwith 794 participants and were completed with790 participants. These 790 participants included140 girls and had ages ranging from 13 to 22 years(x=16.8, standard deviation= 1.2 years). Thesample was ethnically diverse and representativeof the DJJ population: 224 (28.4%) were AfricanAmerican, 374 (47.3%) were Hispanic, 130
(16.5%) were Non-Hispanic White people and60 (7.8%) were of other ethnicities includingAsian American, Native American, FilipinoAmerican and Pacific Islander. Four hundredand thirty (54.4%) individuals were committedfor violent offences, 227 (28.7%) for propertyoffences, 50 (6.3%) for drug offences and 83(10.5%) for other offences. Prior to enteringthe DJJ, boys in the sample had an average of9.4 arrest charges each, and girls had an averageof 6.4, for an average of 8.9 for the total studypopulation.
Assessment of personality and psychiatric diagnoses
The Structured Clinical Interview for DSM-IV(SCID) was initially used to make diagnoses ofsubstance use, mood, anxiety and personalitydisorders (First, Gibbon, Spitzer, Williams, &Benjamin, 1997). We also used the specificmodules of the Diagnostic Interview for Chil-dren and Adolescents to determine the presenceof oppositional defiant disorder, attention deficithyperactivity disorder and separation anxiety, asthese disorders are not captured by the SCID(Reich, 2000). The Structured Interview forDSM-IV Personality (SIDP-IV; Pfohl, Blum, &Zimmerman, 1997) was used to determine thepresence of CD and personality disorders notcaptured by the SCID. The SIDP-IV is consid-ered a gold standard for the structured assess-ment of personality. Given the demographicsof our population with a mean age of 16.8 years,a third of our sample met the age criteria of theDSM-IV-TR for personality disorders. Theyounger participants were assessed in the samemanner as the older participants, because thevalidity of the instrument is retained on thebasis of reading level and availability of researchassistants to ensure proper comprehension(Ferdinand, Van Der Reijen, Verhulst, Fokko,& Giel, 1995; Myers, Burket, & Otto, 1993).
To further assess the validity of the SIDP-IVand to examine related dimensions of psychologi-cal functioning, we selected several additional
45Personality disorders in incarcerated youth
Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014)DOI: 10.1002/pmh
instruments to specifically measure traits, whichwe believed would be present in this population.Among these were the Achenbach Youth Self-Report (YSR), the Massachusetts Youth ScreeningInstrument-2 (MAYSI-2) and the WeinbergerAdjustment Inventory (WAI). These measures wereadministered at intake and again after 9months ofincarceration. The latter assessment was carried outconcurrently with the SIDP-IV. The inclusion ofthree diagnostic instruments in addition to the othermeasures of psychological functioning is beneficial asit will capture both the breadth and depth of psycho-logical factors influencing delinquency amongyouth. Using the SPSS version 14.0 software, (DanielA. Weinberger, PhD, Wellen Center, P.O. Box22807, Beachwood, OH 44122) we performed aseries of analyses of variance testing differencesbetween the mean scores of those with SIDP-IVmeeting the criteria for antisocial, borderline, narcis-sistic, schizotypal and schizoid personality disordersand those without these personality disorders onthe domains of anger and irritability (MAYSI-2),distress (WAI), restraint (WAI), aggressive (YSR)and delinquent behaviours (YSR).
Data collection procedures
Participants were excused from their regularschedules to learn about the study and to giveconsent/assent. The diagnostic interviews werethen scheduled as soon as possible after 9months’incarceration. Two trained raters, graduatestudents in social work, psychology and psychiatry,
were involved with each interview; one read thequestions from the standardized booklets whilethe other recorded answers on the answer sheet.After the sessions, both raters conferred, reviewedthe information obtained and arrived at a consen-sus of which ratings represented the best answersgiven by the subjects. This consensual protocolwas then copied and reviewed by the senior inves-tigator and his research staff. To further assess reli-ability, a portion of interviews were randomlyselected to be recorded and were reviewed by thesenior investigator.
Results
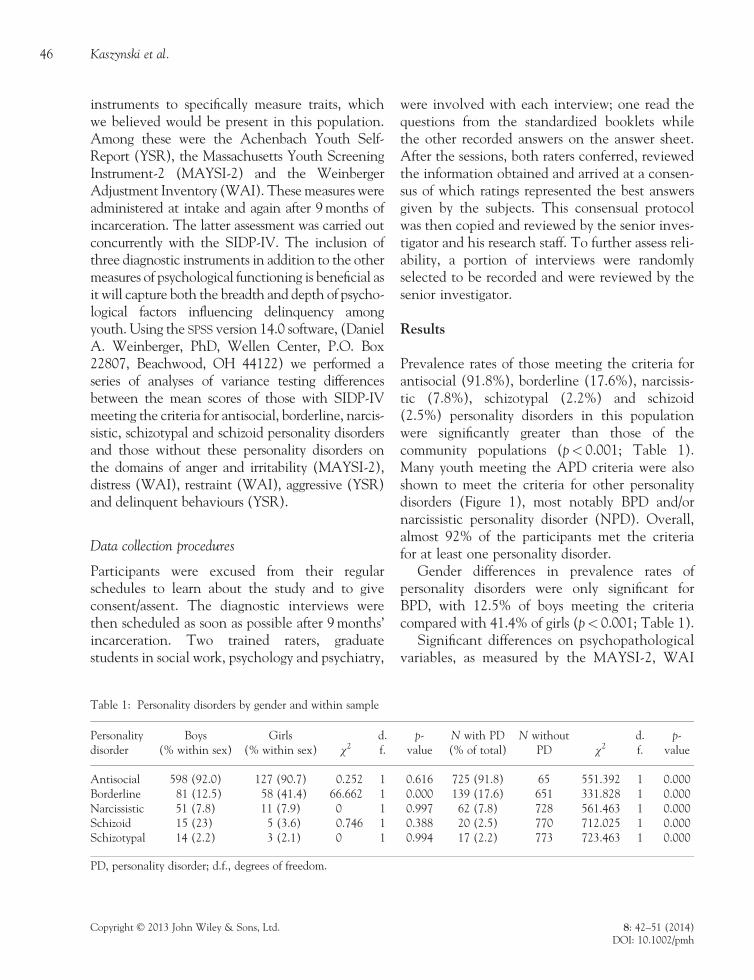
Prevalence rates of those meeting the criteria forantisocial (91.8%), borderline (17.6%), narcissis-tic (7.8%), schizotypal (2.2%) and schizoid(2.5%) personality disorders in this populationwere significantly greater than those of thecommunity populations (p< 0.001; Table 1).Many youth meeting the APD criteria were alsoshown to meet the criteria for other personalitydisorders (Figure 1), most notably BPD and/ornarcissistic personality disorder (NPD). Overall,almost 92% of the participants met the criteriafor at least one personality disorder.
Gender differences in prevalence rates ofpersonality disorders were only significant forBPD, with 12.5% of boys meeting the criteriacompared with 41.4% of girls (p< 0.001; Table 1).
Significant differences on psychopathologicalvariables, as measured by the MAYSI-2, WAI
Table 1: Personality disorders by gender and within sample
Personalitydisorder
Boys(% within sex)
Girls(% within sex) χ2
d.f.
p-value
N with PD(% of total)
N withoutPD χ2
d.f.
p-value
Antisocial 598 (92.0) 127 (90.7) 0.252 1 0.616 725 (91.8) 65 551.392 1 0.000Borderline 81 (12.5) 58 (41.4) 66.662 1 0.000 139 (17.6) 651 331.828 1 0.000Narcissistic 51 (7.8) 11 (7.9) 0 1 0.997 62 (7.8) 728 561.463 1 0.000Schizoid 15 (23) 5 (3.6) 0.746 1 0.388 20 (2.5) 770 712.025 1 0.000Schizotypal 14 (2.2) 3 (2.1) 0 1 0.994 17 (2.2) 773 723.463 1 0.000
PD, personality disorder; d.f., degrees of freedom.
46 Kaszynski et al.
Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014)DOI: 10.1002/pmh

and YSR, were also seen between those meetingthe criteria for antisocial, borderline, narcissisticand schizotypal personality disorders and thosewho did not meet the criteria for those specificdisorders (Table 2). Those meeting the criteriafor APD and NPD had statistically significantelevations of anger–irritability, aggression anddelinquency and significantly decreased restraint(p< 0.001). There were also significantelevations of distress for youth meeting thecriteria for APD and NPD (p< 0.05). Thosemeeting the criteria for BPD likewise hadsignificant elevations of anger–irritability,distress, aggression, delinquency and decreasedrestraint (p< 0.001). Finally, those meetingthe criteria for schizotypal personality disorderhad significantly more distress and aggressionand less restraint than those who did not meetthe criteria for schizotypal personality disorder(p< 0.005, p< 0.005 and p< 0.05 respectively).Our hypothesis was supported with the excep-tion of schizoid personality disorder, where wefound no significant differences between youthwith and without this personality disorder onany of the parameters specified.
Comorbidity is high in our sample with a largeproportion of youth meeting the criteria for multi-ple personality disorders (Table 3, Figure 1). Specif-ically, 18.6% of participants met the criteria for twopersonality disorders, the majority of which met thecriteria for APD and BPD (104 participants),followed by APD and NPD (29 participants). Over4% of the participants met the criteria for threepersonality disorders, including 20 of which whomet the criteria for APD, NPD and BPD. Fourparticipants met the criteria for four personalitydisorders, three of whichmet criteria for schizotypal,APD, NPD and BPD. One participant met thecriteria for all personality disorders measured, includ-ing schizotypal, schizoid, APD, NPD and BPD.
Discussion
Our findings extend the validity of the findings ofEppright et al. (1993) that incarcerated youthshow psychopathology of personality at a highrate. The findings of the present study indicatedthat almost all participants met the criteria for atleast one personality disorder, thus supportingour first hypothesis. APD was by far the mostcommon, followed by NPD and BPD. It is alsoimportant to realize that the findings in the studyof Eppright et al. (1993) were in accordance withthe more stringent criteria for APD found inDSM-III-R (‘…at least four of the following[ten]’ vs. the corresponding qualifier in DSM-IV-TR, ‘…indicated by three (or more) of thefollowing [seven]’). Thus, if this study wererepeated today, we might expect an evenincreased prevalence of the disorder over thatwhich was found previously.
Comorbidity rates of youth meeting the criteriafor multiple personality disorders were also propor-tionally high in this population, which providessupport for convergent validity between thesedisorders. Specifically, close to 25% of the partici-pants met the criteria for more than one personal-ity disorder. One-fifth of all the participants metthe criteria for two disorders, and less than 5% ofthe participants met the criteria for at least three
APD68.2%
13.2%
BPD0.1%
APD +BPD + NPD
2.5%
NPD3.7%
Sample Size100%
APD+NPD3.7%
A
Figure 1: Venn diagram of the percentage of subjectsmeeting the criteria for only antisocial personality disorder(APD), only borderline personality disorder (BPD), onlynarcissistic personality disorder (NPD) or a combination ofthese diagnoses in a sample of 790 incarcerated youth
47Personality disorders in incarcerated youth
Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014)DOI: 10.1002/pmh

Table
2:Meanscores
onmeasuresof
psycho
pathological
variables:significant
differences
betweenincarcerated
youthwithandwitho
utaperson
alitydisorder
MAYSI-2
domain
WAIdomain
YSR
domain
Anger–irritability(95%
CI)
Distress(95%
CI)
Restraint
(95%
CI)
Aggression(95%
CI)
Delinquency
(95%
CI)
Antisocial
4.040(3.830–4.250)
2.381(2.330–2.432)
3.249(3.196–3.302)
55.710
(55.06–56.35)
64.020
(63.26–64.78)
Not
antisocial
2.500(1.890–3.110)
2.191(2.008–2.374)
3.950(3.801–4.100)
51.610
(50.61–52.62)
57.160
(55.21–59.11)
Difference
betweenmeans
1.540
0.190
0.701
4.100
6.860
p-value
<0.001
<0.05
<0.001
<0.001
<0.001
Borderline
6.000(5.600–6.400)
2.865(2.741–2.972)
2.955(2.840–3.071)
60.890
(59.02–62.77)
67.350
(65.63–69.07)
Not
borderlin
e3.460(3.250–3.680)
2.256(2.205–2.306)
3.388(3.331–3.444)
54.160
(53.59–54.72)
62.610
(61.82–63.39)
Difference
betweenmeans
2.540
0.600
0.433
6.730
4.740
p-value
<0.001
<0.001
<0.001
<0.001
<0.001
Narcissistic
5.340(4.740–5.940)
2.542(2.379–2.705)
2.946(2.782–3.110)
59.890
(57.49–62.30)
68.070
(65.60–70.54)
Not
narcissistic
3.790(3.570–4.000)
2.350(2.298–2.401)
3.341(3.287–3.395)
54.980
(54.36–55.60)
63.060
(62.31–63.82)
Difference
betweenmeans
1.550
0.192
0.395
4.910
5.010
p-value
<0.001
<0.05
<0.001
<0.001
<0.001
Schizotypal
2.946(2.434–3.459)
2.933(2.493–3.374)
62.530
(55.90–69.17)
Not
schizotypal
2.353(2.304–2.402)
3.317(3.264–3.369)
55.220
(54.62–55.82)
Difference
betweenmeans
0.593
0.384
7.310
p-value
<0.005
<0.005
<0.05
<0.005
MAYSI-2,M
assachusettsYouth
ScreeningInstrument-2;
WAI,Weinb
ergerAdjustm
entInventory;YSR
,Youth
SelfReport;CI,confi
denceinterval.
48 Kaszynski et al.
Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014)DOI: 10.1002/pmh

personality disorders. These results are comparablewith the comorbidity rates of personality disordersfound among incarcerated juveniles by McManusand colleagues (1984).
Youth meeting the criteria for APD, BPD orNPD demonstrated significantly more anger andirritability, distress and aggressive and delinquentbehaviours, as well as significantly less restraintthan their counterparts not meeting the criteriafor these diagnoses. Those meeting the criteriafor schizotypal personality disorder have signifi-cant elevations in aggressive behaviour anddistress, with significant reductions in restraintcompared with those without this disorder. Youthmeeting the criteria for schizoid personality disor-der were not significantly different on any of thesedomains compared with their counterparts notmeeting this diagnosis. Our results supporthypothesis 2, indicating significant differences
between incarcerated individuals who did andthose who did not meet the criteria for personalitydisorders across domains, with the exception ofindividuals with schizoid personality disorder.One speculative explanation of this finding maybe that schizoid personality characteristics are lessaggressive or delinquent than those demonstratedby other personality disorders.
The findings of the current study not onlyemphasize the morbidity of pervasive psychiatricillnesses among this at-risk population but alsohighlight the need for treatment of such disorders.Treatment targeting underlying personalitydysfunction may be invaluable to the rehabilita-tion of incarcerated youth, which has thus farbeen ineffective (Hollander & Turner, 1985).The results tie into our previous prospective studythat personality traits predict criminologicaloutcomes up to 4.5 years after discharge (Steiner,
Table 3: Number of subjects meeting ≥1 personality disorder diagnosis
PD, personality disorder; APD, antisocial personality disorder; NPD, narcissistic personality disorder; BPD, borderlinepersonality disorder. Colors meant to distinguish between number of individuals meeting criteria for specified diagnoses.
49Personality disorders in incarcerated youth
Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014)DOI: 10.1002/pmh

Cauffman, & Duxbury, 1999). Our results suggestthat, in addition to Axis 1 diagnoses, Axis 2diagnoses need to be comprehensively evaluatedamong incarcerated youth with a history of delin-quent behaviour. In addition to the evaluation ofspecific characteristics, it is important to adminis-ter appropriate treatments targeting the persistentnature of delinquent behaviour characteristics sothat recidivism rates can be reduced. Given theincarcerated status of these youth, they may bemore able to participate and follow-through withtime-intensive therapy that has shown successamong other populations with personality disor-ders (Hollander et al., 2005; Verheul et al., 2007).
One limitation of this study is that it utilizes across-sectional design, and so longitudinal associa-tions cannot be determined. Additionally, becausewe only present rates at which individuals met thecriteria for personality disorders, it would behelpful to examine rates at which participantsmet various criteria. This information would helpinform interventions targeting behaviouralcharacteristics indicative of personality disorders,which would have long-term effects on rehabilita-tion. Despite that, there are several strengths to beacknowledged. First, the inclusion of threediagnostic instruments and several other measuresof psychological functioning helps to capture boththe breadth and depth of factors influencing delin-quency among youth. Second, the sample size wassubstantial enough to obtain adequate statisticalpower. Also, the participants sampled were demo-graphically diverse and representative of the DJJpopulation. Furthermore, this is the first study toour knowledge to establish the validity of Axis IIdisorders in a population younger than 18 years.
Our results provide support for future investiga-tions in several areas. First, these findings supportfuture research evaluating diagnostic differencesamong an at-risk population such as incarceratedyouth. Also, longitudinal research should evaluateendurance of personality dysfunction, self-restraint,distress, anger, aggression and irritability. Finally,this study will inform future research on developinginterventions treating personality disorders. In
summary, research identifying prevalence andcomorbidity of personality disorders is valuable,and further work is needed to inform interventionstargeting the rehabilitation of incarcerated youth.
References
American Psychiatric Association. (2000). Diagnostic and sta-tistical manual of mental disorders (4th edition – text revision).Washington, DC: Author.
Barnum, R. and Keilitz, I. (1992). Issues in systems interac-tions affescting mentally disordered juvenile offenders.In J.j. Cocozza (Ed.), Responding to the Mental HealthNeeds of Youth in Juvenile Justice System. Seattle, WA:The National Coalition for the Mentally Ill in the Crim-inal Justice System, pp. 49–91.
Bender, D. S., Dolan, R. T., Skodol, A. E., Sanislow, C. A.,Dyck, I. R., McGlashan, T. H., Shea M. T., Zanarini M.C., Oldham J. M., Gunderson, J. G. (2001). Treatmentutilization by patients with personality disorders. TheAmerican Journal of Psychiatry, 158(2), 295–302.
Bowlby, J. (1944). Forty-four juvenile thieves: Their characters andhome-life. The International Journal of Psychoanalysis, 25, 1–57.
Chanen, A. M., Jovev, M., & Jackson, H. J. (2007). Adaptivefunctioning and psychiatric symptoms in adolescents withborderline personality disorder. The Journal of ClinicalPsychiatry, 68(2), 297–306.
Cocozza, J. J. (1992). Responding to the mental health needsof youth in the juvenile justice system. In National coali-tion for the mentally ill in the criminal justice system. Seattle.
Domalanta, D. D., Risser, W. L., Roberts, R. E., & Risser, J. M.H. (2003). Prevalence of depression and other psychiatricdisorders among incarcerated youths. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 42(4), 477–484.
Eppright, T. D., Kashani, J. H., Robison, B. D., & Reid, J. C.(1993). Comorbidity of conduct disorder and personalitydisorders in an incarcerated juvenile population. TheAmerican Journal of Psychiatry, 150(8), 1233–1236.
Farrell, A. D., & Sullivan, T. N. (2000). Structure of theWeinberger Adjustment Inventory Self-Restraint Scaleand its relation to problem behaviors in adolescence.Psychological Assessment, 12(4), 394–401.
Ferdinand, R. F., Van Der Reijen, M., Verhulst, F. C., Fokko,J. N., Giel, R. (1995). Assessment of the prevalence ofpsychiatric disorders in young adults. The British Journalof Psychiatry, 166, 480–488.
First, M. B., Gibbon, M., Spitzer, R. L., Williams, J. B., & Benja-min, L. S. (1997). Structured Clinical Interview for DSM-IVAxis II personality disorders (SCID-II). New York, New York:American Psychiatric Publishing Incorporated.
Hollander, E., Swann, A. C., Coccaro, E. F., Jiang, P., &Smith, T. B. (2005). Impact of trait impulsivity and state
50 Kaszynski et al.
Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014)DOI: 10.1002/pmh

aggression on divalproex versus placebo response inborderline personality disorder. The American Journal ofPsychiatry, 162(3), 621–624.
Hollander, H. E., & Turner, F. D. (1985). Characteristics ofincarcerated delinquents: Relationship between develop-ment disorders, environmental and family factors, and pat-terns of offense and recidivism. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 24(2), 221–226.
Jones, M. & Westen, D. (2010). Diagnosis and subtypes ofantisocial personality disorder. Journal of Personality Disor-ders, 24(2), 217–243.
Karnik, N. S., Soller, M. V., Redlich, A., Silverman, M.,Kraemer, H. C., Haapanen, R., & Steiner, H. (2009).Prevalence rates and gender differences of psychiatricdisorders among juvenile delinquents nine months intoincarceration. Psychiatry Services, 60(6), 838–841.
Karnik, N. S., Soller, M. V., Redlich, A., Silverman, M.,Kraemer, H. C., Haapanen, R., & Steiner, H. (2010).Prevalence differences of psychiatric disorders amongyouth after nine months or more of incarceration byrace/ethnicity and age. Journal of Health Care for the Poorand Underserved, 21(1), 237–50.
Kernberg, P. F., & Shapiro, T. (2000). Resolved: Borderlinepersonality exists in children under twelve. In L. C. Terr(Ed.), Debate forum, Journal of the American Academy ofChild and Adolescent Psychiatry, 29(3), 478–483.
Lewis, D. O., Pincus, J. H., Lovely, R., Spitzer, E., & Moy, E.(1987). Biopsychosocial characteristics of matched samplesof delinquents and nondelinquents. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 26(5), 744–752.
Lipsey, M. W. (1992). Juvenile delinquency treatment: Ameta-analytic inquiry into the variability of effects. In T.Cook, H. Cooper, & D. S. Cordray (Eds.), Meta-analysisfor explanation: A casebook (pp. 83–127). New York:Russell Sage Foundation.
Lipsey, M.W. (1995). What do we learn from 400 researchstudies on the effectiveness of treatment with juveniledelinquents? In: What Works? J. McGuire (Eds.) ReducingReoffending, (63–78). New York, NY: John Wiley.
Lipsey, M. W., Wilson, D. B., & Cothern, L. (2000). Effectiveintervention for serious juvenile offenders. Nashville, TN:Juvenile Justice Bulletin: Office of Juvenile Justice andDelinquency Prevention.
McManus, M., Alessi, N. E., Grapentine, W. L., & Brickman,A. (1984). Psychiatric disturbance in serious delinquents.Journal of the American Academy of Child and AdolescentPsychiatry, 23(5), 602–615.
Moffitt, T. E., & Caspi, A. (2001). Childhood predictorsdifferentiate life-course persistent and adolescence-limited antisocial pathways among males and females.Developmental Psychopathology, 10, 355–375.
Moffitt, T. E., Caspi, A., Dickson, N., & Silva, P. (1996).Childhood-onset versus adolescent-onset antisocial
conduct problems in males: Natural history from ages 3to 18 years. Developmental Psychopathology, 8, 399–424.
Myers, W. C., Burket, R. C., & Otto, T. A. (1993). Conductdisorder and personality disorders in hospitalized adoles-cents. The Journal of Clinical Psychiatry, 54(1), 21–26.
Pfohl, B., Blum, N., & Zimmerman, M. (1997). StructuredInterview for DSM-IV Personality (Sid-P). Washington,D.C.: American Psychiatric Publishing, Inc.
Puzzanchera, C., Stahl, A. L., Finnegan, T. A., Snyder, H. N.,Poole, R. S., & Tierney, N. (2000). Juvenile court statistics1997. Washington, DC: Office of Juvenile Justice andDelinquency Prevention.
Reich, W. A. (2000). Diagnostic Interview for Children andAdolescents (DICA). Journal of the American Academy ofChild and Adolescent Psychiatry, 39(1), 59–66.
Ruchkin, V. V., Schwab-Stone, M., Koposov, R., Vermeiren,R., & Steiner, H. (2002). Violence exposure,posttraumatic stress, and personality in juvenile delin-quents. Journal of the American Academy of Child andAdolescent Psychiatry, 41(3), 322–329.
Steiner, H., Cauffman, E., & Duxbury, E. (1999). Personalitytraits in juvenile delinquents: Relation to criminalbehavior and recidivism. Journal of the American Academyof Child and Adolescent Psychiatry, 38, 256–262.
Swann, A. C., Bjork, J. M., Moeller, F. G., & Dougherty, D.M. (2002). Two models of impulsivity: Relationship topersonality traits and psychopathology. BiologicalPsychiatry, 51, 988–994.
Taylor, J., Elkins, I. J., Legrand, L., Peuschold, D., & Iacono, W.G. (2007). Construct validity of adolescent antisocial person-ality disorder. Journal of Youth andAdolescence, 36, 1048–1057.
Teplin, L. A., Abram, K. M., & McClelland, G. M. (1994).Does psychiatric disorder predict violent crime amongreleased jail detainees? A six-year longitudinal study.American Psychologist, 49, 335–342.
Teplin, L. A., Abram, K. M., & McClelland, G. M. (2002).Psychiatric disorders in youth in juvenile detention.Archives of General Psychiatry, 59(12), 1133–1143.
Verheul, R., & Herbrink, M. (2007). The efficacy of variousmodalities of psychotherapy for personality disorders: Asystematic review of the evidence and clinical recommen-dations. International Review of Psychiatry, 19, 25–38.
Wasserman, G. A., McReynolds, L. S., Lucas, C. P., Fisher, P.,& Santos, L. (2002). The voice DISC-IV with incarceratedmale youths: Prevalence of disorder. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 41(3), 314–21.
Address correspondence to: Niranjan Karnik,Department of Psychiatry and BehavioralSciences, University of Chicago, Chicago, IL,USA. Email: [email protected]
51Personality disorders in incarcerated youth
Copyright © 2013 John Wiley & Sons, Ltd. 8: 42–51 (2014)DOI: 10.1002/pmh
Related Documents








![Introduction to Comorbidity Auto Saved]](https://static.cupdf.com/doc/110x72/577d33b31a28ab3a6b8b7d51/introduction-to-comorbidity-auto-saved.jpg)


