IN THE NAME OF GOD

IN THE NAME OF GOD. Oral Hypoglycemic Agents.
Dec 31, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
IN THE NAME OF GOD

Oral Hypoglycemic Agents
Recommendations:Glycemic Goals in Adults
• Hb A1C < 7%
• Hb A1C < 6.5%
• Hb A1C < 8%
Recommendations:Glycemic Goals in Adults (1)
• Lowering A1C to below or around 7% has been shown to reduce microvascular complications and, if implemented soon after the diagnosis of diabetes, is associated with long-term reduction in macrovascular disease. Therefore, a reasonable A1C goal for many nonpregnant adults is <7% . B
Recommendations:Glycemic Goals in Adults (2)
• Providers might reasonably suggest more stringent A1C goals (such as <6.5%) for selected individual patients, if this can be achieved:
• without significant hypoglycemia • or other adverse effects of treatment.
Appropriate patients might include those• with short duration of diabetes, • long life expectancy, • and no significant CVD. C
Recommendations:Glycemic Goals in Adults (3)
• Less stringent A1C goals (such as <8%) may be appropriate for patients with (B):
• History of severe hypoglycemia, limited life expectancy, advanced microvascular or macrovascular complications, extensive comorbid conditions.
• Those with longstanding diabetes in whom the general goal is difficult to attain despite DSME, appropriate glucose monitoring, and effective doses of multiple glucose lowering agents including insulin
Oral Hypoglycemic Agents
• 1-Insulin Sensitizers with Predominant Action in the Liver
• 2- Insulin Sensitizers with Predominant Action in Peripheral Insulin-Sensitive Tissues
• 3-Insulin Secretagogues• 4-Incretin-Related Therapies(DPP4 Inhibitors)• 5-Sodium-glucose cotransporters type 2 inhibitors• 6-Alpha-glucosidase inhibitors • 7-Colesevelam• 8-Bromocriptine
PHARMACOLOGICAL THERAPY FOR TYPE 1 DIABETES(Slide1)
• Most people with type 1 diabetes should be treated with multiple-dose insulin (MDI) injections (three to four injections per day of basal and prandial insulin)
• or continuous subcutaneous insulin infusion (CSII). A (Diabetes Care)
ORAL HYPOGLYCEMIC AGENT THERAPY FOR TYPE 1
DIABETES(Slide2)• 1- Metformin• 2- ALPHA-GLUCOSIDASE INHIBITORS
PHARMACOLOGICAL THERAPY FOR TYPE 1 DIABETES(Slide3)
• Adding metformin to insulin therapy:• 1- may reduce insulin requirements• 2- and improve metabolic control in overweight/obese
patients with poorly controlled type 1 diabetes. • In a meta-analysis, metformin in type 1 diabetes was
found to reduce insulin requirements (6.6 U/day, P , 0.001) and led to small reductions in weight and total and LDL cholesterol but not to improved glycemic control (absolute A1C reduction 0.11%, P = 0.42) (Diabetes Care).
PHARMACOLOGICAL THERAPY FOR TYPE 1 DIABETES(4)
• Incretin-Based Therapies• Therapies approved for the treatment of type 2
diabetes are currently being evaluated in type 1 diabetes.
• Glucagon-like peptide 1 (GLP-1) agonists and dipeptidyl peptidase 4 (DPP-4) inhibitors are not currently FDA approved for those with type 1 diabetes, but are being studied in this population.
PHARMACOLOGICAL THERAPY FOR TYPE 1 DIABETES(4)
• Sodium–Glucose Cotransporter 2 Inhibitors• Sodium–glucose cotransporter 2 (SGLT2) inhibitors
provide insulin-independent glucose lowering by blocking glucose reabsorption in the proximal renal tubule by inhibiting SGLT2. These agents provide modest weight loss and blood pressure reduction. Although there are two FDAapproved agents for use in patients with type 2 diabetes, there are insufficient data to recommend clinical use in type 1 diabetes at this time (Diabetes Care).
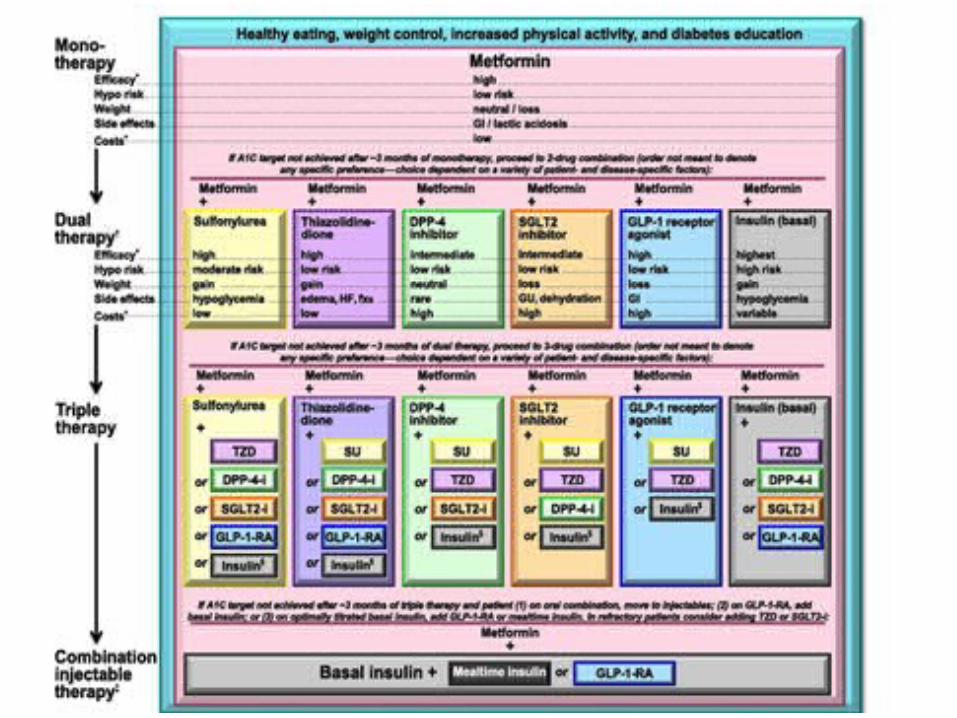
PHARMACOLOGICAL THERAPY FORTYPE 2 DIABETES
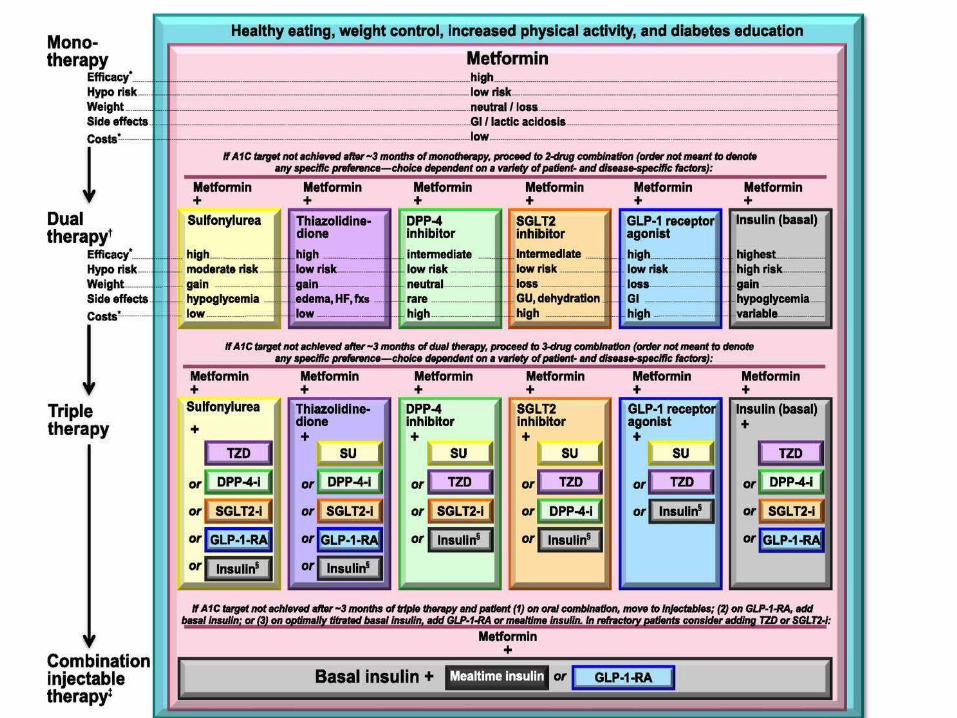
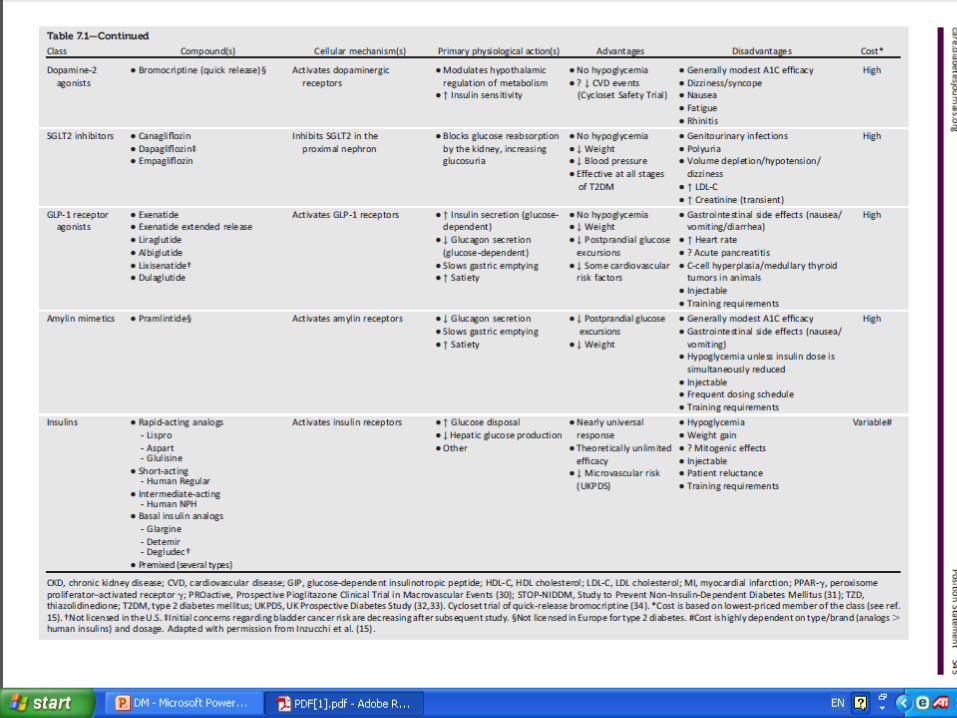
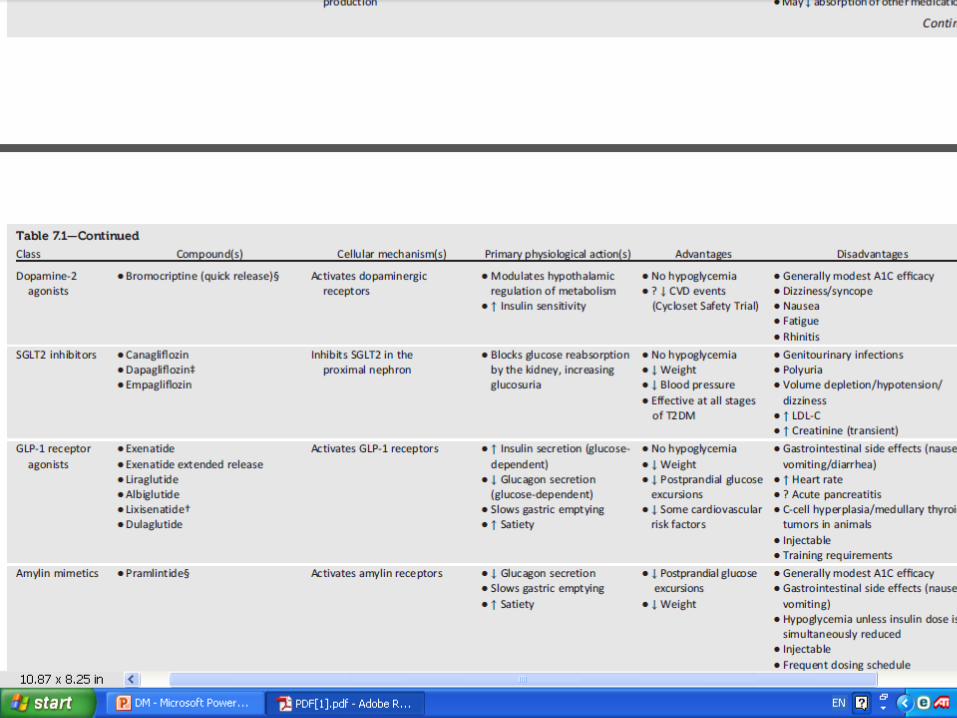
ADA. 7. Approaches to Glycemic Treatment. Diabetes Care 2015;38(suppl 1):S43. Figure 7.1; adapted with permission from Inzucchi SE, et al. Diabetes Care, 2015;38:140-149
Choiceof Pharmacological Agents
• Considerations include: • efficacy• cost• potential side effects • weight• comorbidities • hypoglycemia risk• and patient preferences. E• Due to the progressive nature of type 2 diabetes, insulin
therapy is eventually indicated for many patients with type 2 diabetes. B (Diabetes Care).
Dual Therapy
• For all patients, consider initiating therapy with a dual combination when A1C is 9% to more expeditiously achieve the target A1C level. (Diabetes Care).
Insulin
• When hyperglycemia is severe, especially if symptoms are present or any catabolic features (weight loss, ketosis) are in evidence.
• Consider initiating combination insulin injectable therapy when blood glucose is 300–350 mg/dL and/or A1C is 10–12%.
• As the patient’s glucose toxicity resolves, the regimen can, potentially, be subsequently simplified. (Diabetes Care)
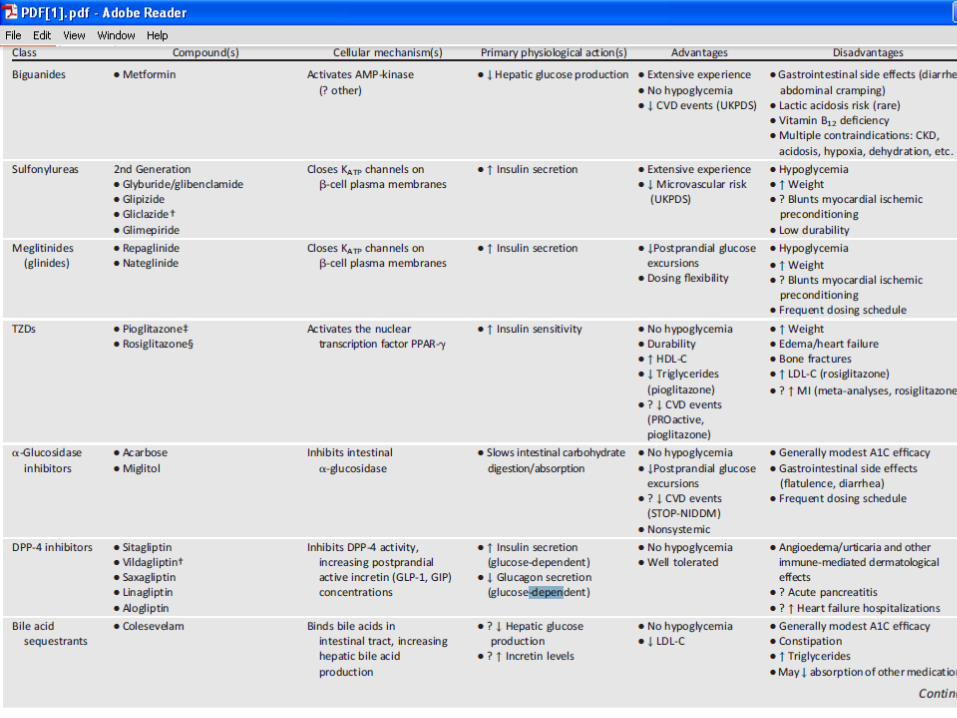
Metformin
• Metformin, if not contraindicated and if tolerated, is the preferred initial pharmacological agent for type 2 diabetes. A
• In patients with newly diagnosed type 2 diabetes and markedly symptomatic and/or elevated blood glucose levels or A1C, consider initiating insulin therapy (with or without additional agents). E
• If noninsulin monotherapy at maximum tolerated dose does not achieve or maintain the A1C target over 3 months, add a second oral agent, a GLP-1 receptor agonist, or basal insulin. A
Metformin(MECHANISM OF ACTION(1))
• Is effective only in the presence of insulin• its major effect is to decrease hepatic glucose output• In addition, metformin increases insulin-mediated
glucose utilization in peripheral tissues (such as muscle and liver), particularly after meals, and has an antilipolytic effect that lowers serum free fatty acid concentrations, thereby reducing substrate availability for gluconeogenesis.
• As a result of the improvement in glycemic control, serum insulin concentrations decline slightly.
Metformin(MECHANISM OF ACTION(2))
• The molecular mechanisms of metformin action are not fully known.
• Activation of the enzyme AMP-activated protein kinase (AMK) appears to be the mechanism by which metformin lowers serum lipid and blood glucose concentrations.
• Metformin works through the Peutz-Jeghers protein, LKB1, to regulate AMPK. LKB1 is a tumor suppressor and activation of AMPK through LKB1 may play a role in inhibiting cell growth. In case-control and cohort studies in patients with type 2 diabetes, metformin use has been associated with a reduced risk of cancer and lower cancer mortality?
Metformin
• HbA1c Lowering >1 (%) • Fasting & Postprandial effect • Usual Dosing Frequency (1-3 Doses/Day)• Maximum effective dose (1000 mg bid)
Agent -Specific AdvantagesMetformin
• 1- May be less likely to cause hypoglycemia.(Careful blood glucose monitoring is still needed during the first weeks or months of treatment with metformin to avoid this problem.)
• 2- Weight neutral• 3- (LDL &TG), HDL• 4-Inexpensive• 5-Decreased all-cause mortality and decreased rate
of myocardial infarction .
• SIDE EFFECTS — The most common side effects of metformin are gastrointestinal, including a metallic taste in the mouth, mild anorexia, nausea, abdominal discomfort, and soft bowel movements or diarrhea [4]. These symptoms are usually mild, transient, and reversible after dose reduction or discontinuation of the drug. In clinical trials, only 5 percent of study subjects discontinue metformin because of the gastrointestinal side effects.
• Metformin reduces intestinal absorption of vitamin B12 in up to 30 percent of patients, and lowers serum vitamin B12 concentrations in 5 to 10 percent, but only rarely causes megaloblastic anemia. The dose and duration of use of metformin correlates with the risk of vitamin B12 deficiency [21]. This reduction appears to be due to absorption in the ileum and can be corrected by administration of oral calcium [22]
Agent -Specific Disadvantages
• The most common side effects:– Metallic taste in the mouth,– mild anorexia – nausea – abdominal discomfort– soft bowel movements or diarrhea
• Reduces intestinal absorption of vitamin B12
• lactic acidosis (Rare problem){anorexia, nausea, vomiting, abdominal pain, lethargy, hyperventilation, and hypotension}
Contraindications
• 1-Serum Cr >1.5 mg/dL (men) >1.4 mg/dL (women)• 2- CHF• 3-radiographic contrast studies • 4-seriously ill patients• 5-acidosis• 6-Concurrent liver disease or alcohol abuse• 7-Past history of lactic acidosis
Contraindications• 1-intravenous contrast administration• 2-Predisposing factors for lactic acidosis related to
metformin– Impaired renal function, which has been variably defined; one
definition is serum creatinine concentration above 1.4 mg/dL in women and 1.5 mg/dL in men
• 3-Concurrent liver disease or alcohol abuse• 4-Heart failure; however, despite safety concerns,
metformin use has been common and well tolerated in diabetic patients with heart failure
• 5-Past history of lactic acidosis• 6-Decreased tissue perfusion or hemodynamic instability
due to infection or other causes
parenteral administration of iodinated contrast
• should be discontinued immediately prior to and for 48 hours after any radiologic procedure involving parenteral administration of iodinated contrast material. The rationale for this recommendation is to avoid the potential for high plasma metformin concentrations (and lactic acidosis) if the patient develops contrast-induced acute renal failure.
Metformin(protect against hypoglycemia)
• Metformin also increases intestinal glucose utilization via nonoxidative metabolism, at least in experimental animals.
• The lactate produced by this process is largely metabolized in the liver as a substrate for gluconeogenesis. The latter effect could protect against hypoglycemia.
DOSING
• Tab 500, 850, 1000 mg• Metformin is absorbed rapidly from the small intestine,
with peak plasma concentrations attained in two hours. It is not bound to plasma proteins, is not metabolized, and is rapidly excreted in the urine .
• and should be taken with meals• We begin with 500 mg once daily with the evening
meal and, if tolerated, add a second 500 mg dose with breakfast.
• The dose can be increased slowly (one tablet every one to two weeks) as necessary .
• The usual effective dose is 1500 to 2000 mg/day per day; the maximum dose of 2550 mg/day
• A comparative effectiveness meta-analysis suggests that overall each new class of noninsulin agents added to initial therapy lowers A1C around 0.9–1.1%.(ADA)
combination of metformin and one of these …
• If the A1C target is not achieved after
approximately 3 months, consider a combination of metformin and one of these six treatment options: • sulfonylurea,• thiazolidinedione,• DPP-4 inhibitors,• SGLT2 inhibitors, • GLP-1 receptor agonists, • or basal insulin.
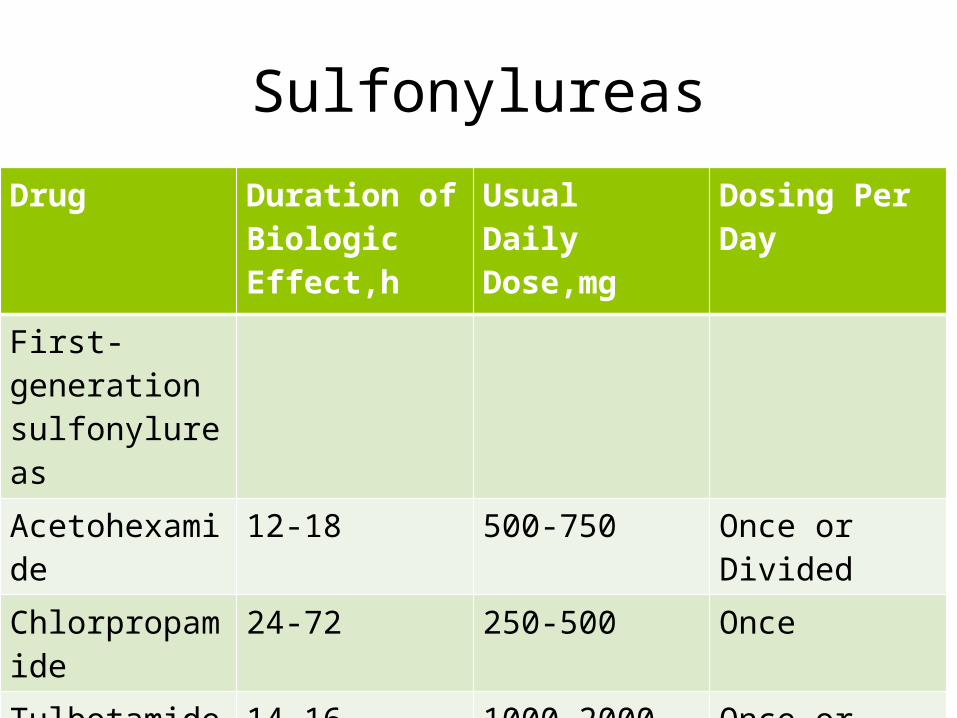
Sulfonylureas
Drug Duration of Biologic Effect,h
Usual Daily Dose,mg
Dosing Per Day
First-generation sulfonylureas
Acetohexamide 12-18 500-750 Once or Divided
Chlorpropamide 24-72 250-500 Once
Tulbotamide 14-16 1000-2000 Once or Divided
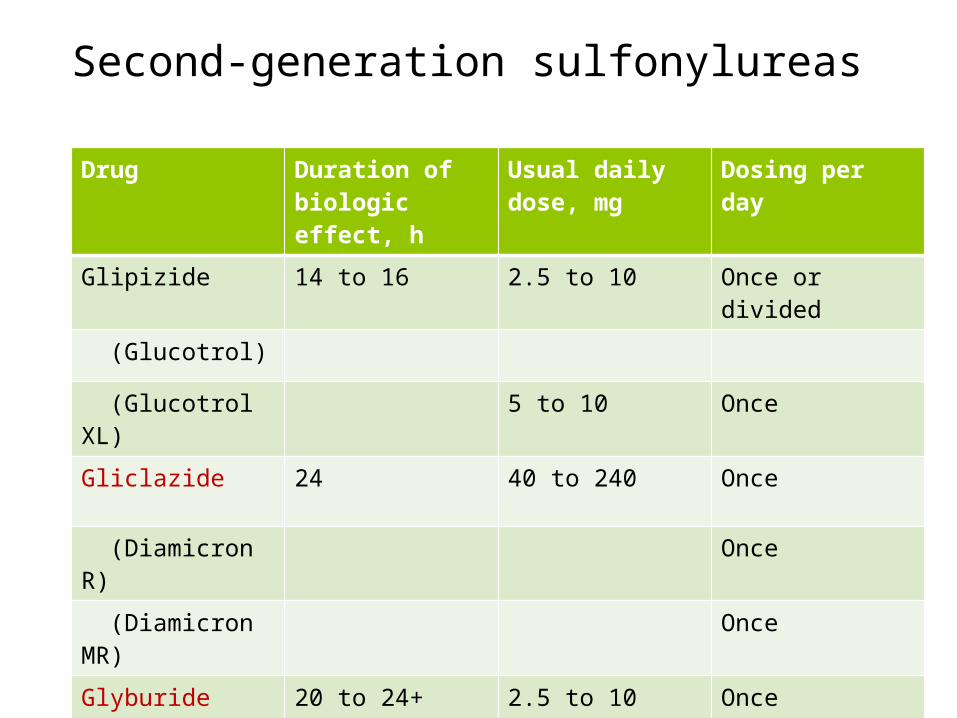
Second-generation sulfonylureas
Drug Duration of biologic effect, h
Usual daily dose, mg
Dosing per day
Glipizide 14 to 16 2.5 to 10 Once or divided
(Glucotrol)
(Glucotrol XL) 5 to 10 Once
Gliclazide 24 40 to 240 Once
(Diamicron R) Once
(Diamicron MR) Once
Glyburide (Glibenclamide)
20 to 24+ 2.5 to 10 Once
Glimepiride (Amaryl)
24+ 2 to 4 Once
Gliclazide
• Tablet, oral:Immediate release tablet• Diamicron®: 80 mg• Tablet, modified release, oral:• Diamicron® MR: 30 mg, 60 mg
Gliclazide:Administration
• Administration Patients that are • NPO or• require decreased caloric intake may need doses held to
avoid hypoglycemia.• Administer with meals (modified release tablet should be
administered with breakfast). May split the 60 mg modified release tablets in half; however, the 30 mg modified release tablets must be swallowed whole. Modified release tablets should not be crushed or chewed.
• Administer with meals (modified release tablet should be administered with breakfast).
Gliclazide:Dosing:
• Immediate release tablet:• Recommended initial: • 80 mg twice daily; titrate based on blood glucose levels.
Usual dosage range 80-320 mg/day (maximum dose: 320 mg/day); dosage of ≥160 mg should be divided into 2 equal parts for twice-daily administration
• Modified release tablet:• Initial:• 30 mg once daily; titrate in 30 mg increments every 2
weeks based on blood glucose levels. Maximum dose: 120 mg once daily
Conversion from Insulin to Gliclazide
• Maturity-onset diabetes: Oral: May consider conversion from insulin to gliclazide therapy in patients receiving <40 units/day insulin. Prior to conversion, discontinue insulin for 48-72 hours with close monitoring (≥3 times/day) of urine for glucose and ketones. Patients with ketonuria and glycosuria 12-24 hours after discontinuing insulin should not be converted to gliclazide therapy and should remain on insulin therapy.
gliclazide Dosing: Renal Impairment
• Mild-moderate impairment (Clcr ≥15 mL/minute): Dose reductions may be necessary. There are no dosage adjustments provided in manufacturer's labeling.
• Severe impairment: Use is contraindicated.
GliclazideDosing: Hepatic Impairment
• Mild-moderate impairment: Dose reductions may be necessary. There are no dosage adjustments provided in manufacturer's labeling.
• Severe impairment: Use is contraindicated.
Drug Interactions of Gliclazide
• Alcohol (Ethyl)• Beta-Blockers• Chloramphenicol• Cimetidine• Corticosteroids (Orally Inhaled), (Systemic)• Cyclic Antidepressants• Fibric Acid Derivatives• Fluconazole• GLP-1 Agonists• Miconazole (Oral )
Contraindications• 1-Hypersensitivity to gliclazide, other sulfonylureas or
sulfonamides, or any component of the formulation;• 2-Type 1 diabetes mellitus (insulin dependent, IDDM); • 3-Diabetic ketoacidosis with or without coma; • 4-Severe renal impairment; • 5-Severe hepatic impairment• 6-stress conditions (eg, serious infection, trauma,
surgery);• 7- concurrent use with miconazole (systemic or
oromucosal gel);
Disease-related concerns:
• Glucose-6-phosphate dehydrogenase (G6PD) deficiency: Patients with G6PD deficiency may be at an increased risk of sulfonylurea-induced hemolytic anemia; however, cases have also been described in patients without G6PD deficiency during postmarketing surveillance. Use with caution and consider a nonsulfonylurea alternative in patients with G6PD deficiency.

DPP-4 inhibitors
Discovery of DPP-4 Inhibitors as Antidiabetic Agents
Tesfaye BiftuMerck & Co., Inc.
Incretin-Related Therapies(SLIDE 1)
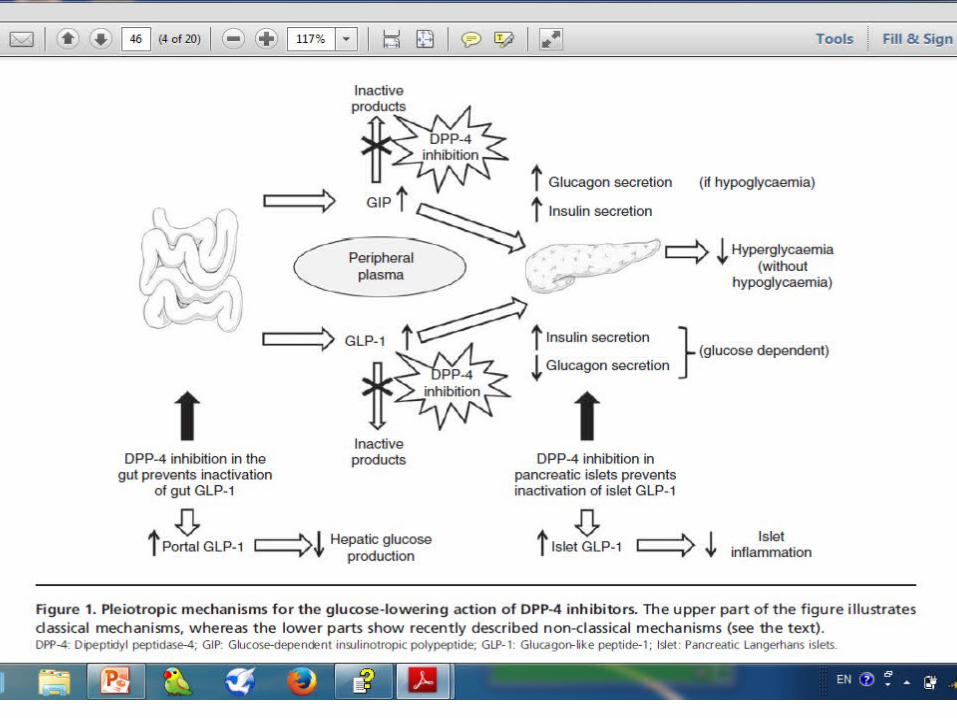
• The incretin effect describes the observation that oral glucose has a greater stimulatory effect on insulin secretion than does intravenous glucose at the same circulating glucose concentration. In humans, this effect seems to be primarily mediated by GLP1 and GIP(Glucose-dependent insulinotropic polypeptide) . GLP1 is produced from the proglucagon gene in intestinal L cells and is secreted in response to nutrients. (Williams)
Incretin-Related Therapies(SLIDE 2)
• GLP1: • 1-Stimulates insulin secretion in a glucose-
dependent fashion • 2-Inhibits inappropriate hyperglucagonemia • 3-Slows gastric emptying • 4-Reduces appetite and improves satiety • 5-Beta-cell proliferative, antiapoptotic, and
differentiation effects at least in vitro and in preclinical models. (Williams)
Incretin-Related Therapies(SLIDE 3)
• GLP1 has a very short half-life in plasma (1 to 2 minutes) due to aminoterminal degradation by the enzyme dipeptidyl peptidase IV (DPP4). (Williams)
Incretin-Related Therapies(SLIDE 4)
• GLP1 receptor agonists, which are peptides that produce increases of 10-fold or higher in GLP1 activity
• DPP4 inhibitors, which are small molecule inhibitors of the degradation of GLP1 and GIP as well as other hormones.
• DPP-4 inhibitors may be used in the:• full spectrum of type 2 diabetes (T2DM):
– monotherapy in drug-naive patients, – dual or triple oral therapies– or even as add-onto insulin. (Andre J Scheen)
special populations
• Because of their favourable efficacy/safety profile, DPP-4 inhibitors are best suited for special populations of T2DM patients such as
• elderly people,• patients with renal impairment • or patients at risk of hypoglycaemia
(‘personalized medicine’). (Andre J Scheen)
• The pancreatic safety remains a matter of debate and requires careful post-marketing surveillance,
whereas the • cardiovascular safety of DPP-4 inhibitors is
already better known and will be even more extensively demonstrated in further ongoing trials.
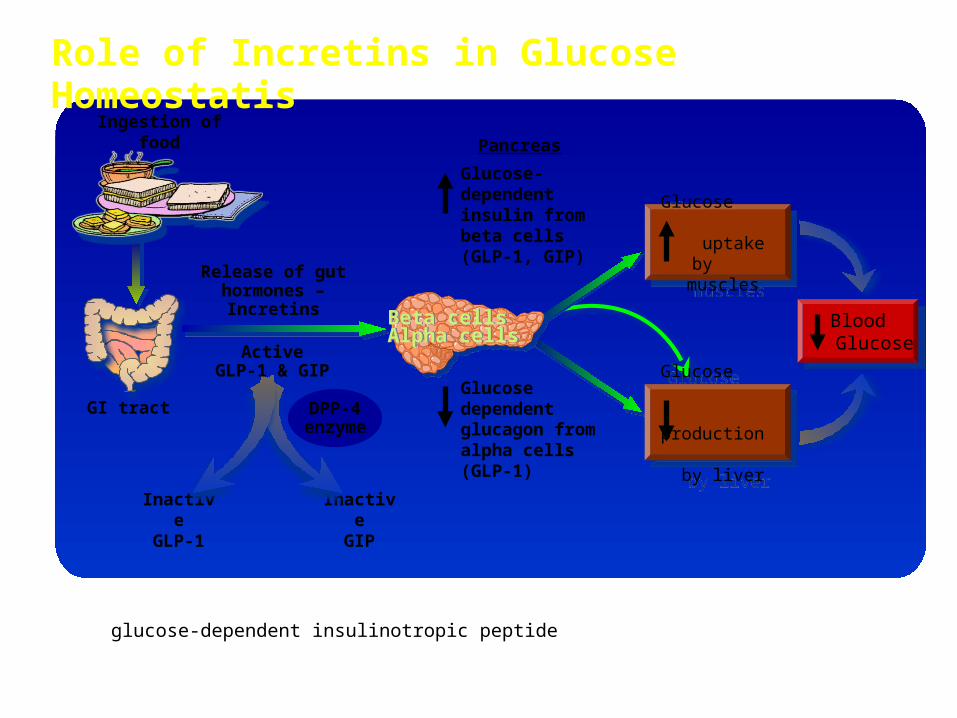
Role of Incretins in Glucose Homeostatis
DPP-4=dipeptidyl peptidase–4GIP=glucose-dependent insulinotropic peptideGLP-1=glucagon-like peptide–1
Beta cellsAlpha cellsBeta cellsAlpha cells
InactiveGLP-1
Blood Glucose
Blood Glucose
GI tract
Release of gut hormones –
Incretins
Ingestion of food
Glucose uptake by
muscles
Glucose uptake by
muscles
Glucose production
by liver
Glucose production
by liver
InactiveGIP
DPP-4enzyme
Glucose dependent glucagon from alpha cells (GLP-1)
Glucose-dependent insulin from beta cells (GLP-1, GIP)
ActiveGLP-1 & GIP
Pancreas
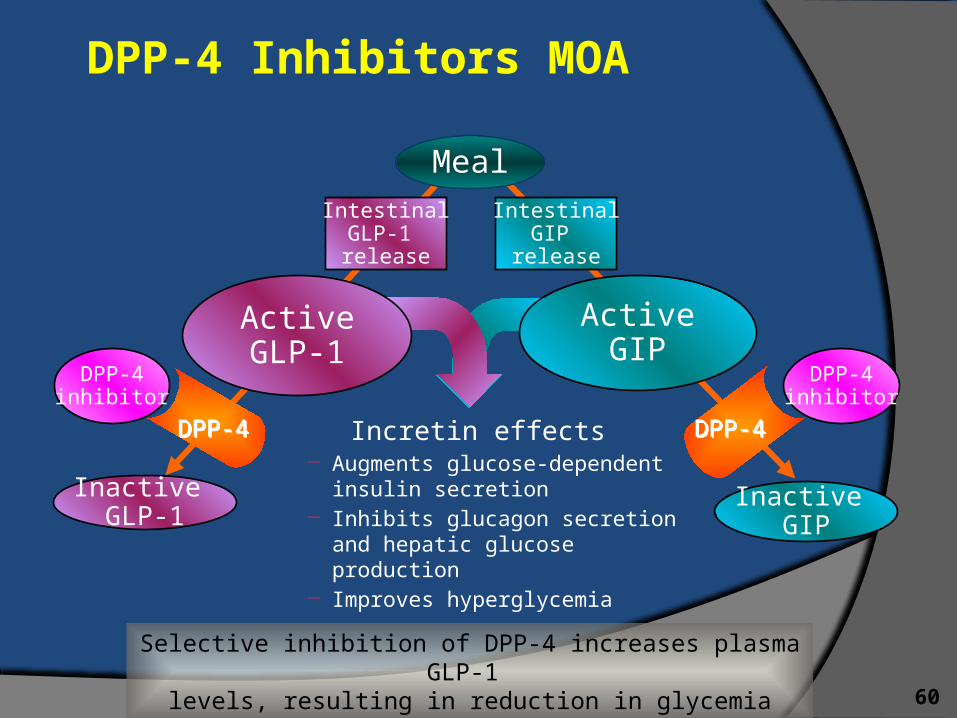
DPP-4 Inhibitors MOA
60
Incretin effects – Augments glucose-dependent
insulin secretion– Inhibits glucagon secretion
and hepatic glucose production– Improves hyperglycemia
Meal
Inactive GLP-1
ActiveGIP
DPP-4DPP-4
IntestinalGIP
release
IntestinalGLP-1 release
DPP-4DPP-4
DPP-4inhibitor
Inactive GIP
DPP-4inhibitor
ActiveGLP-1
Selective inhibition of DPP-4 increases plasma GLP-1 levels, resulting in reduction in glycemia
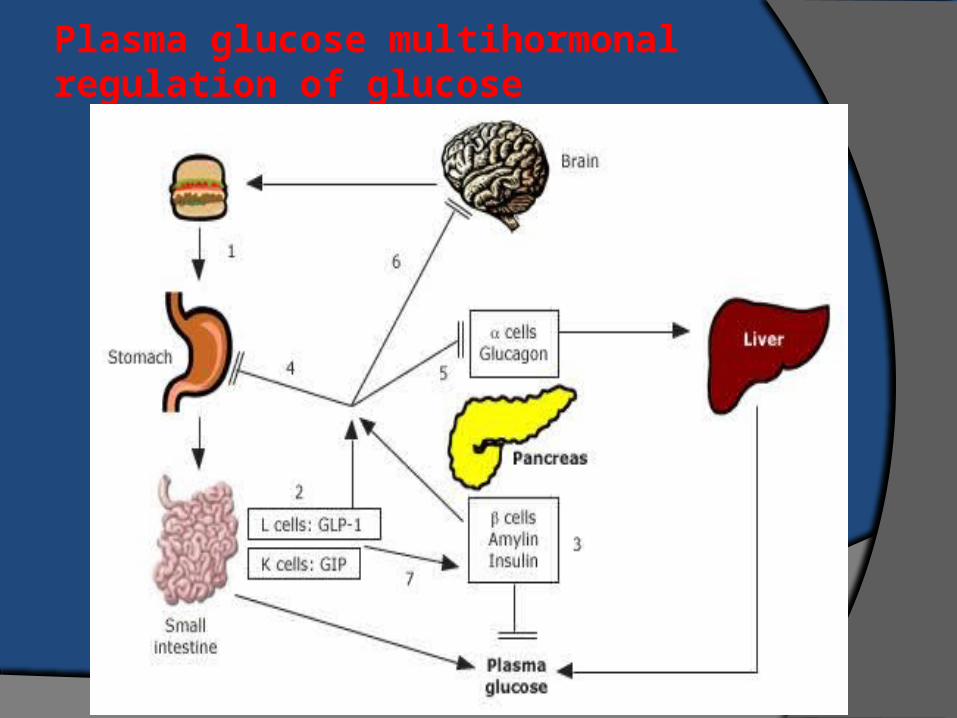
Plasma glucose multihormonal regulation of glucose
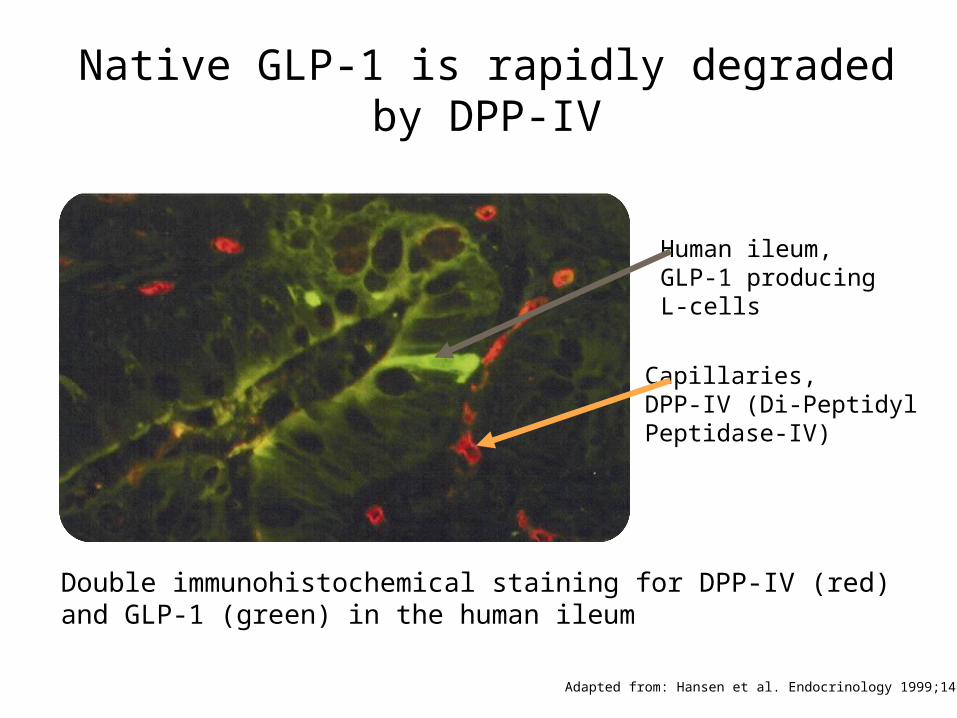
Native GLP-1 is rapidly degraded by DPP-IV
Human ileum, GLP-1 producingL-cells
Capillaries,DPP-IV (Di-Peptidyl Peptidase-IV)
Adapted from: Hansen et al. Endocrinology 1999;140:5356–5363.
Double immunohistochemical staining for DPP-IV (red) and GLP-1 (green) in the human ileum
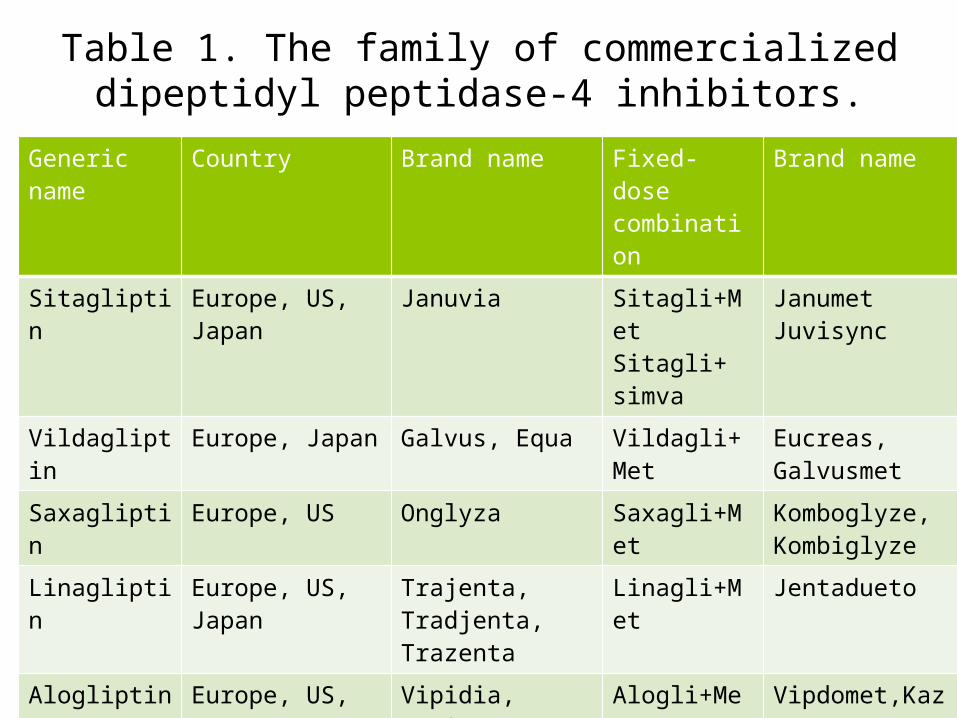
Table 1. The family of commercialized dipeptidyl peptidase-4 inhibitors.
Generic name Country Brand name Fixed-dose combination
Brand name
Sitagliptin Europe, US, Japan Januvia Sitagli+MetSitagli+ simva
JanumetJuvisync
Vildagliptin Europe, Japan Galvus, Equa Vildagli+Met Eucreas, Galvusmet
Saxagliptin Europe, US Onglyza Saxagli+Met Komboglyze, Kombiglyze
Linagliptin Europe, US, Japan Trajenta, Tradjenta, Trazenta
Linagli+Met Jentadueto
Alogliptin Europe, US, Japan Vipidia, Nesina Alogli+MetAlogli+ piogli
Vipdomet,KazanoOseni
Anagliptin Japan Suiny
Teneligliptin Japan Tenelia
Gemigliptin Korea Zemiglo
Clinical indications of DDP4 inhibitors for the management of
hyperglycaemia in type 2 diabetes.
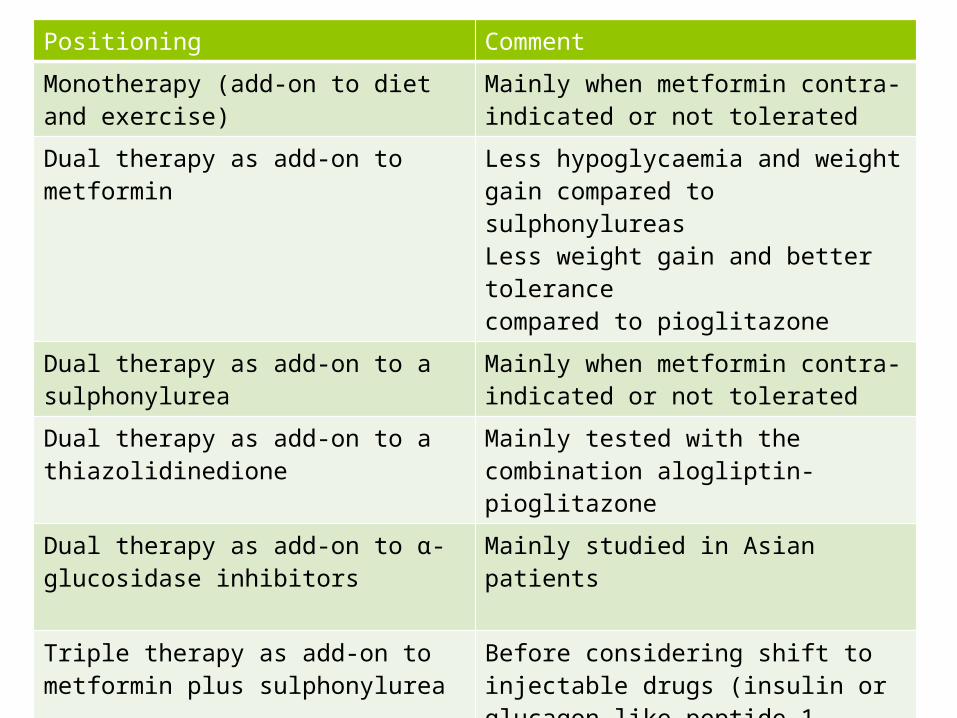
Positioning Comment
Monotherapy (add-on to diet and exercise) Mainly when metformin contra-indicated or not tolerated
Dual therapy as add-on to metformin Less hypoglycaemia and weight gain compared to sulphonylureasLess weight gain and better tolerance compared to pioglitazone
Dual therapy as add-on to a sulphonylurea Mainly when metformin contra-indicated or not tolerated
Dual therapy as add-on to a thiazolidinedione
Mainly tested with the combination alogliptin-pioglitazone
Dual therapy as add-on to α-glucosidase inhibitors
Mainly studied in Asian patients
Triple therapy as add-on to metformin plus sulphonylurea
Before considering shift to injectable drugs (insulin or glucagon-like peptide-1 receptor agonists)
Triple therapy as add-on to metformin plus pioglitazone
Less hypoglycaemia and weight gain compared to sulphonylureas
As add-on to insulin therapy Better glucose control with less insulin and no increase of hypoglycaemia
DDP4 inhibitors
• These agents produce approximately twofold increases in fasting and postprandial GLP1 and GIP levels, with subsequent HbA1c reductions of approximately 0.7%.
• well tolerated• Specifically, they are not associated with nausea.• because of the lesser increase in GLP1 activity than
with the GLP1 receptor agonists, there is no weight loss with DPP4 inhibitors; they tend to be weight neutral
Sitagliptin
• Dosing: Adult Type 2 diabetes: Oral: 100 mg once daily
• Concomitant use with insulin and/or insulin secretagogues (eg, sulfonylureas): Reduced dose of insulin and/or insulin secretagogues may be needed
• Tablet, oral: • Januvia®: 25 mg, 50 mg, 100 mg
SitagliptinDosing: Renal Impairment
• Clcr ≥50 mL/minute: No adjustment required
• Clcr ≥30 to <50 mL/minute: 50 mg once daily
• Scr: Males: >1.7 to ≤3.0 mg/dL; Females: >1.5 to ≤2.5 mg/dL: 50 mg once daily
• Clcr<30 mL/minute: 25 mg once daily
• Scr: Males: >3.0 mg/dL; Females: >2.5 mg/dL: 25 mg once daily
• ESRD requiring hemodialysis or peritoneal dialysis: 25 mg once daily; administered without regard to timing of hemodialysis
Dosing: Hepatic Impairment
• Mild-to-moderate impairment (Child-Pugh score 7-9): No dosage adjustment required
• Severe impairment (Child-Pugh score >9): Not studied
• Pregnancy Risk Factor B• Breast-Feeding Considerations It is not known
if sitagliptin is excreted in breast milk. The manufacturer recommends that caution be used if administered to breast-feeding women.
• Dietary Considerations May be taken with or without food.
• Monitoring Parameters Hb A1c, serum glucose; renal function prior to initiation and periodically during treatment
Contraindication
• Postmarketing cases of pancreatitis have been reported for the DPP4 inhibitors, and they are contraindicated for use in those with a prior history.
• Specificity for DPP4 appears to be crucial, because less specific inhibitors have demonstrated adverse effects on immune function and cancer growth in animal studies.
• The usual dose is the maximum marketed dose; because these drugs are cleared renally, smaller doses are recommended in the setting of stage 3 or greater chronic kidney disease.
hypersensitivity reactions
• Serious hypersensitivity reactions have been reported, including:
• anaphylaxis, • angioedema,• and exfoliative skin conditions with sitagliptin,
but causality has not been substantiated due to the rarity of events.

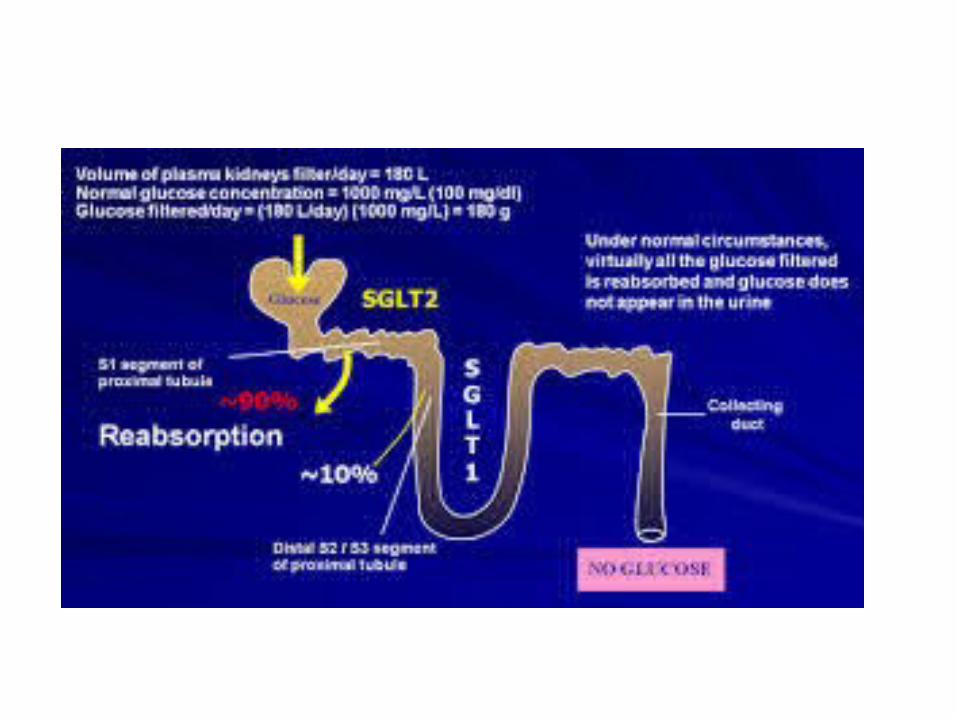
sodium glucose cotransporter
• SGLT2 is a member of the sodium glucose cotransporter family which are sodium-dependent glucose transport proteins. SGLT2 is the major cotransporter involved in glucose reabsorption in the kidney.
• Dapagliflozin, approved in the United States.• Canagliflozin, approved in the United States• Ipragliflozin (ASP-1941), in Phase III clinical trials• Tofogliflozin, in Phase III clinical trials• Empagliflozin (BI-10773), approved in the United
States.• Sergliflozin etabonate, discontinued after Phase II trials• Remogliflozin etabonate, in phase IIb trials• Ertugliflozin (PF-04971729 / MK-8835), in phase III
trials
Clinical significance
• Mutations in this gene are also associated with renal glucosuria
Dapagliflozin
• Mechanism of action• Dapagliflozin inhibits subtype 2 of the
sodium-glucose transport proteins (SGLT2) which are responsible for at least 90% of the glucose reabsorption in the kidney. Blocking this transporter mechanism causes blood glucose to be eliminated through the urine. In clinical trials, dapagliflozin lowered HbA1c by 0.90 percentage points when added to metformin.
DapagliflozinSide effects
• Since dapagliflozin leads to heavy glycosuria (sometimes up to about 70 grams per day) it can lead to rapid weight loss and tiredness. The glucose acts as an osmotic diuretic (this effect is the cause of polyuria in diabetes) which can lead to dehydration. The increased amount of glucose in the urine can also worsen the infections already associated with diabetes, particularly urinary tract infections and thrush (candidiasis). Dapagliflozin is also associated with hypotensive reactions.
DYSLIPIDEMIA/LIPIDMANAGEMENT
• Screening• In adults, a screening lipid profile is• reasonable at the time of first diagnosis,• at the initial medical evaluation,• and/or at age 40 years and• periodically (e.g., every 1–2 years) thereafter. E
Dyslipidemia/Lipid Management
• – Screening• In most adult patients with diabetes, measure
fasting lipid profile at least annually (B)• In adults with low-risk lipid values
– (LDL cholesterol <100 mg/dL, – HDL cholesterol >50 mg/dL, and – triglycerides <150 mg/dL), – lipid assessments may be repeated every 2 years
(E)
Dyslipidemia/Lipid ManagementTreatment Recommendations and Goals
• To improve the lipid profile in patients with diabetes, recommended Lifestyle modification (A) focusing on– Reduction of saturated fat, trans fat, and cholesterol intake
• Increase of omega-3 fatty acids, viscous fiber (such as in oats, legumes, and citrus), and plant stanols/sterols
• Weight loss (if indicated)• Increased physical activity should be recommended to
improve the lipid profile in patients with diabetes (A)• Glycemic control can also beneficially modify
plasmalipid levels, particularly in patients with very high triglycerides and poor glycemic control.
• Intensify lifestyle therapy and optimize glycemic control for patients with elevated triglyceride levels (≥150 mg/dL) and/or low HDL cholesterol (<40 mg/dLfor men, <50 mg/dL for women). C
• For patients with fasting triglyceride levels ≥500 mg/dL,evaluate for secondary causes and consider medical therapy to reduce risk of pancreatitis. C
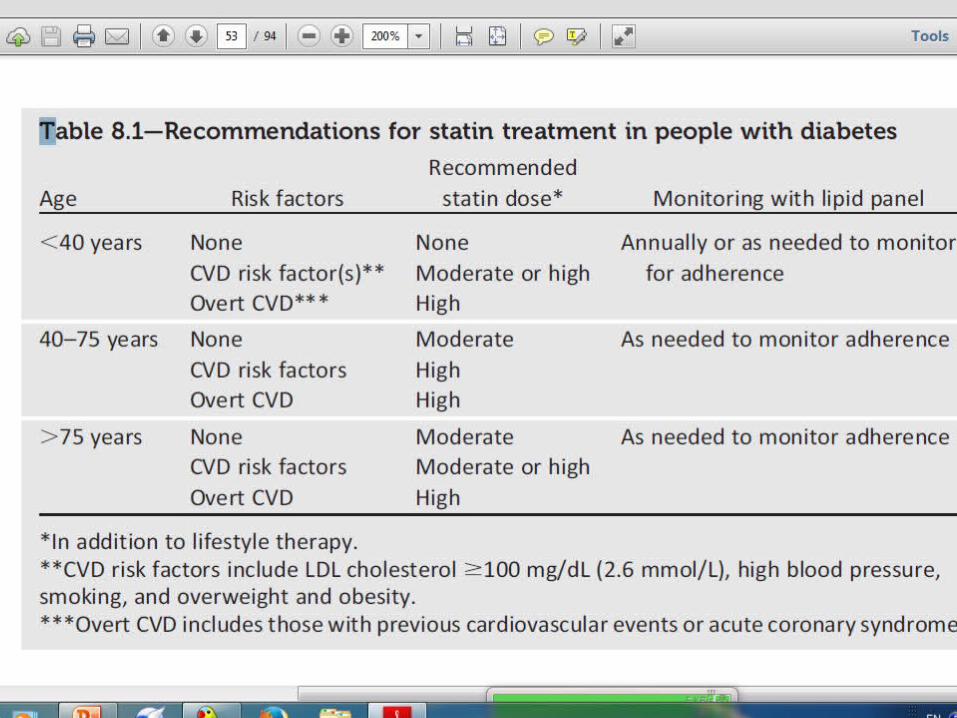
• For patients of all ages with diabetes and overt CVD:
• high-intensity statin therapy should be added to lifestyle therapy. A
• For patients with diabetes aged,40 years with additional CVD risk factors, consider using moderateor high-intensity statin and lifestyle therapy. C
Statin therapy should be added to lifestyle therapy
• 1-regardless of baseline lipid levels, for diabetic patientsa-With overt CVD (A)
b- Without CVD who are over the age of 40 years and have one or more other CVD risk factors (A) 2-For patients at lower risk (e.g., without overt CVD and younger than age 40 years)
a-LDL cholesterol remains >100 mg/dL
b-In those with multiple CVD risk factors (C)
• For patients with diabetes aged• 40–75 years without additional• CVD risk factors, consider using• moderate-intensity statin and lifestyle• therapy. A
• Therefore, in• patients with increased cardiovascular• risk (e.g., LDL cholesterol $100 mg/dL• [2.6 mmol/L], high blood pressure, smoking,• and overweight/obesity) or with overt• CVD, high-dose statins are recommended
• Combination therapy (statin/• fibrate and statin/niacin) has not• been shown to provide additional• cardiovascular benefit above statin• therapy alone and is not generally• recommended. A
• Statin therapy is contraindicated• in pregnancy. B
Treatment Recommendations and Goals
• In individuals without overt CVD, the goal is:
LDL cholesterol <100 mg/dL (B)• In individuals with overt CVD,
– a lower LDL cholesterol goal of <70 mg/dL , with a high dose of a statin, is an option (B)
Treatment Recommendations and Goals
• If targets not reached on maximal tolerated statin therapy
• Alternative therapiotic goal: reduce in LDL cholesterol ~30-40% from baseline (B)
• Triglyceride levels <150 mg/dl, HDL cholesterol >40 mg/dL in men and >50 mg/dL in women, are desirable (C).
However, LDL cholesterol-targeting statin therapy remains the preferred strategy (A)
Treatment Recommendations and Goals
• Combination therapy has been shown not to provide additional cardiovascular benefit above statin therapy alone and is not generally recommended (A)
• Statin therapy is contraindicated in pregnancy (B)
• If severe hypertriglyceridemia is absent, then
therapy targeting HDL cholesterol or triglycerides
lacks the strong evidence base of statin therapy. • If HDL cholesterol is ,40 mg/dL and LDL
cholesterolis between100 and 129 mg/dL, a fibrate or niacin might be used, especially if a patient is intolerant to statins.
Combination Therapy
• Statin and Fibrate• may be efficacious for treatment for LDLcholesterol, HDL
cholesterol, and triglycerides,• but this combination is associated with an increased risk for
abnormal transaminase levels, myositis, or rhabdomyolysis.• The risk of rhabdomyolysis is more common with• 1-higher doses of statins and
2-with renal insufficiency and
3-seems seems to belower when statins are combined with
fenofibrate than gemfibrozil.
In the ACCORD study
• in patients with type 2 diabetes who were at high risk for CVD, the combination of fenofibrate and simvastatin did not reduce the rate of
• fatalcardiovascular events, • nonfatalMI, • or nonfatal stroke, • as compared with simvastatin alone.
Benefit of CombinationTherapy
• for men • and possible harm for women, • and a possible benefit for patients with
both triglyceride level ≥204mg/dL • and HDL cholesterol level ≤34 mg/dL
Statin and Niacin
• Combination therapy with niacin is not recommended given the lack of efficacy on
• major CVD outcomes, possible increase in• risk of ischemic stroke, and side effects.
Diabetes With Statin Use
• There is an increased risk of incident diabetes
with statin use , which may be limited to those
with diabetes risk factors.• These patients may benefit from diabetes
screening when on statin therapy.• The absolute risk increase was small (over 5 years
of follow-up, 1.2%of participants on placebo
developed diabetes and 1.5% on rosuvastatin).• while simultaneously preventing 5.4 vascular
events


Recommendations:Glycemic,Blood Pressure, Lipid Control in Adults
• A1C <7.0%• Blood Preshure <140/90 mmHg• Lipids: LDL <100 mg/dl • cholestrol• Statin therapy for those with history of MI or
age < 40 + other risk factors, or age > 40
ANTIPLATELET AGENTS• Consider aspirin therapy (75–162mg/day) as a
primary prevention strategy in those with type 1 or type 2 diabetes at increased cardiovascular risk (10-year risk>10%). This includes most men aged >50 years or women aged>60 years who have at least one additional major risk factor (family history of CVD, hypertension, smoking, dyslipidemia, or albuminuria). C
• Aspirin should not be recommendedfor CVD prevention for adults with diabetes at low CVD risk (10-year CVD risk ,5%, such as in men aged ,50 years and women aged ,60 years with no major additional CVD risk factors),
• since the potential adverse effects from bleeding likely offset the potential benefits. C
• In patients in these age-groups with multiple other risk factors (e.g., 10-year risk 5–10%), clinical judgment is required. E
• Use aspirin therapy (75–162mg/day) as a secondary prevention strategy in those with diabetes and a history of CVD. A
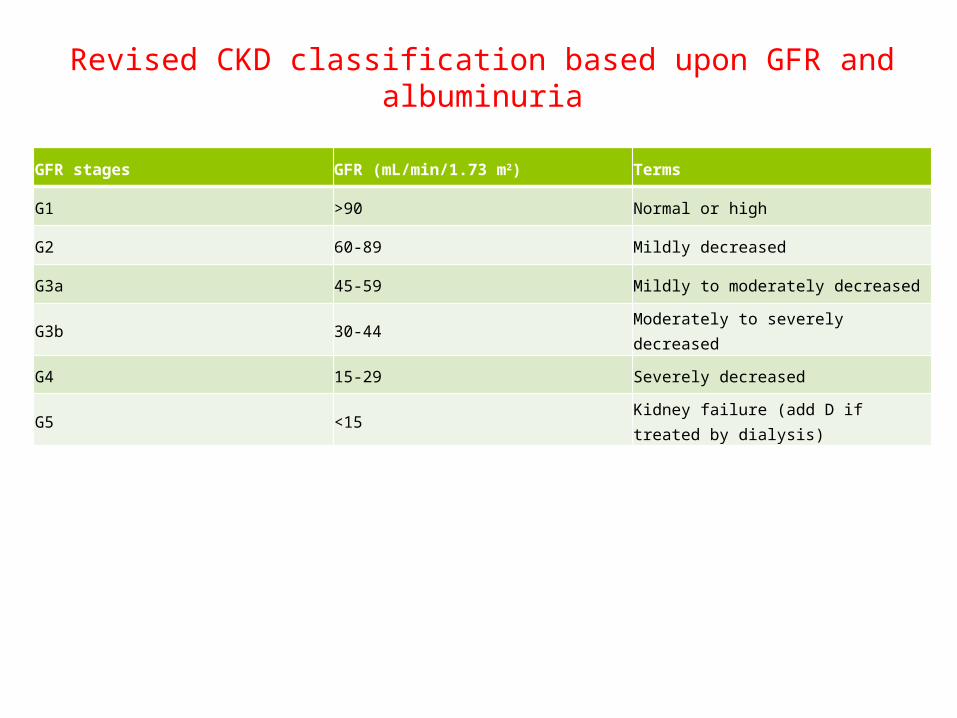
Revised CKD classification based upon GFR and albuminuria
GFR stages GFR (mL/min/1.73 m2) Terms
G1 >90 Normal or high
G2 60-89 Mildly decreased
G3a 45-59 Mildly to moderately decreased
G3b 30-44 Moderately to severely decreased
G4 15-29 Severely decreased
G5 <15 Kidney failure (add D if treated by dialysis)
CVD risk factors
• family history of CVD• hypertension• Smoking• Dyslipidemia• albuminuria
Low Risk For CVD
• without overt CVD and younger than age 40 years), statin therapy should be considered in addition to lifestyle therapy if LDL cholesterol remains >100 mg/dL or in those with multiple CVD risk factors (C)

Related Documents