Improving Patient Hand-Over ABMS QI Forum - May 2015 Iahn Gonsenhauser

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Improving Patient Hand-Over ABMS QI Forum - May 2015
Iahn Gonsenhauser

Consider the Case
2
Covering a hospital service overnight you are paged that your patient is having increased respiratory difficulty. Scanning her EMR, the procedure note is still pending and is unreadable The admission note indicates she was admitted for lethargy and difficult to wean oxygen, post procedure from a pacemaker placement for what was supposed to be an outpatient procedure. While reading… the code blue alarm sounds…
Presenter
Presentation Notes
Consider the case of covering a hospital service overnight. A few hours into your shift you are paged that your patient is having increased respiratory difficulty. You are not familiar with the patient. You knew there was a late admission, transferred from another service, this sounds like it must be the one. Briefly scanning her EMR, finding the procedure note still pending completion and unreadable you see her admission note that she was admitted post procedure from the EP lab for what was supposed to be an outpatient procedure. She was admitted for lethargy and difficult to wean oxygen following procedure. Standard workup with basic labs and imaging had been ordered. As you are thinking to yourself, those EP guys are always so aggressive with the sedatives its amazing they can extubate anybody… at that time the code blue alarm sounds…

Consider the Case
3
Cardiac Arrest, CPR, Intubation Distant breath sounds, needle-decompression, bilateral chest tubes and transfer to the ICU for an extended stay…
Presenter
Presentation Notes
The scene on your arrival is familiar, CPR, ACLS, intubation in progress and along the way absent breath sounds noted, needle-decompression, bilateral chest tubes and transfer to the ICU for an extended stay… If any communication had taken place to sign this patient out at end of day – You were unaware. The procedure note, only available some time after the event, mentions difficult access and some respiratory difficulty. At the subsequent M&M the Cardio fellow describes his verbal signout which referred to the complication, and to the CXR that was pended following the procedure. A CXR you would have reviewed hours prior to the radiology read, had you known it was pending. No hand-over from the original team. No visible sign-out in the EMR from the EP Fellow.

We Know This Is A Problem
4
Multiple regulatory groups and professional organizations have identified significant shortcomings in transitions of care, including end-of-shift inpatient hand-overs.
Presenter
Presentation Notes
This is not altogether unfamiliar. Transitions of care have been implicated in avoidable patient harm events since we started paying attention to avoidable patient harm. Transitions at shift change are at the heart of the debate regarding duty hour restrictions. No doubt the IOM, the ACGME, ABIM, the SHM and many others have all stressed how critical these transitions are and how crucial effective communication is at these junctures.

What Exactly is the Problem?
5
Variability in Methods Lack of Structure No Documentation Poor Efficiency Failure to Confirm
Presenter
Presentation Notes
We know where our deficits are: Variability in basic methods: are hand-overs done at all and if so are they done in-person by telephone or by email Lack of structure or order No physical document summarizing patient’s data is included. Lack of efficiency Lack of provider insight of whether or not their practices are truly effective. Everyday we employ methods to structure communication when discussing patients: History and Physical or the Progress Note The structure helps the listener know what to expect and where to focus their attention. This standardized communication is advantageous to both the presenter and the listener. So why then is this still such a deficit?

The Hand Off Problem
6
• How effective are you at communicating critical elements of the plan of care?
• Do you use a standard method?
• Do they know what to expect from you as they receive sign-out? • Would you be willing to adopt a set of basic inclusions/principles to
your current approach?
Presenter
Presentation Notes
So we asked a series of simple questions. We asked attendings, residents, interns, nurses and pharmacists on multiple inpatient services medical, surgical, general and subspecialty - - to self-reflect We asked: Are their methods effective? Do they use a standard method, and if so is anyone aware of that? Are expectations clear And would they be willing to adopt any additional basic principles to improve? We developed simple tools to ask these questions in more detail. Tools that allow for actionable self-reflection. Tools that can be completed in very little time and allow providers to compare their personal perception of competency and the perceived quality of patient hand-over as rated by their colleagues.
The Hand Off Problem
7
• Efficient – Length/Amount of Information/Efficiency • Effective – Clear/Structured/Results as Expected • Sufficient – Preparedness/Expectation/Safety
Presenter
Presentation Notes
We focused on specific domains within the hand-over process. Efficiency, effectiveness and sufficiency. The goal being, a transition that was all of these things, the worst case scenario being a transition that was at least sufficient in that it adequately prepared the accepting provider, yielded reasonable expectations and was safe. Our answer was not at all surprising. Individual providers all thought they were doing a great job. They felt that their personal approach was very high functioning across all domains. Specifically our providers felt that their own transitions were Safe 96% of the time. When we polled their peers, high-functioning began to look more like sort of ok functioning & even at times, unsafe, in fact unsafe about 25% of the time.
Improving Your Golf Game
8
‘I won’t rebuild your swing, I will take your swing and improve it enough that you can play the game successfully.’ Chip Inks – Golf Instructor
Presenter
Presentation Notes
‘I won’t rebuild your swing, I will take your swing and improve it enough that you can play the game successfully.’ Yes… His name really is Chip, and he is a terrific guy, but what does he have to do with patient transitions? The key is his philosophy… As we have learned recently, loudly if not clearly, there are many physicians and other providers out there that are staunchly opposed to being forced to practice, or improve practice in a prescribed way. Flexibility and personalization are key drivers of success. So we went back to our previous question - Would you be willing to adopt a set of basic inclusions/principles to your current approach? Now with Chip’s philosophy, recognizing that providers have their own way of doing this, and that’s fine, we ask that you consider adopting some simple add-ons to what you already do? And we offered a simple intervention using simple tools. We offered two sets of guideline principles, Macro - one set for your handover as a whole, and Micro - one set for your individual patient descriptions.

Hand Off – Macro Level
9
Level 1 • Perform a Hand Over Level 2 • Summary Document & Consistent Environment Level 3 • Prioritize Patient List • Follow Up Questions • Occasionally solicit feedback
Presenter
Presentation Notes
The macro levels are a way of creating the foundation for safe and effective transitions of care. Level 1 is very simple. If you do not engage in any hand off, start doing something. Anything is better than nothing Level 2 consists of a three basic principles, #1 if you conduct some sort of hand off but do not generate any physical document summarizing your hand-over, start. Hand something to whoever you are transitioning with. #2 If you don’t consistently conduct hand over in the same environment of form, ie sometimes email, sometimes phone, get consistent. #3 Prioritize patient list from most critical/complex to least critical/complex patient when handing over the service. No one pays attention for 15-20 minutes of sign-out. Important items first, while you still have some attention. Level 3 adds some finer points that allow for continuous improvement

Hand Off – Micro Level
10
O-H-I-O – Individual Patient Summary Structure Overview – Name/Location/Code Status History- Status (New/Hand-Back/Discharge) (Sick/Not) (Stable/Improving/Declining) & One Line Summary or Principal Dx Interval History – Pertinent recent changes/events Ongoing – Action Summary - Things to do/expect overnight
Presenter
Presentation Notes
The Micro Level – This is the real content and the finer structure. The goals – Just 3 really 1 - Remove extraneous information. The hand-over and document are not a replacement for the patient chart. This is high-yield, pertinent, potential action items. 2 - Give the green light to save time. Its OK to skip a patient who you have discharged. Its OK to save time on a patient that is known to your colleague with no significant updates. 3 – Increased awareness of the patient’s current condition For examples of what this looks like in practice please visit the poster session. This is a very flexible structure, for medicine, these can be quite long. For Surgery, per their feedback, the entire signout fits on a single line.
The Hand Off Checklist - Macro
11
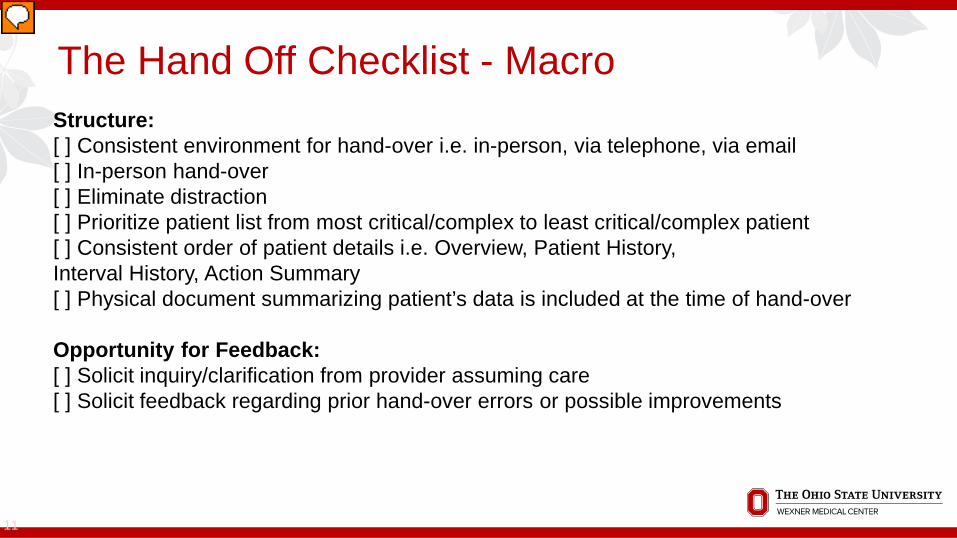
Structure: [ ] Consistent environment for hand-over i.e. in-person, via telephone, via email [ ] In-person hand-over [ ] Eliminate distraction [ ] Prioritize patient list from most critical/complex to least critical/complex patient [ ] Consistent order of patient details i.e. Overview, Patient History, Interval History, Action Summary [ ] Physical document summarizing patient’s data is included at the time of hand-over Opportunity for Feedback: [ ] Solicit inquiry/clarification from provider assuming care [ ] Solicit feedback regarding prior hand-over errors or possible improvements
Presenter
Presentation Notes
Because this was a lot of very discrete information, yes/no items, we employed a checklist. Used as an inventory it is a quick way of itemizing what your current practice is. We found that many of the most crucial items on the checklist are consistently missing. As an intervention we found that providers employed the principles very easily with minimal preparation or experience.
The Hand Off Checklist - Micro
12
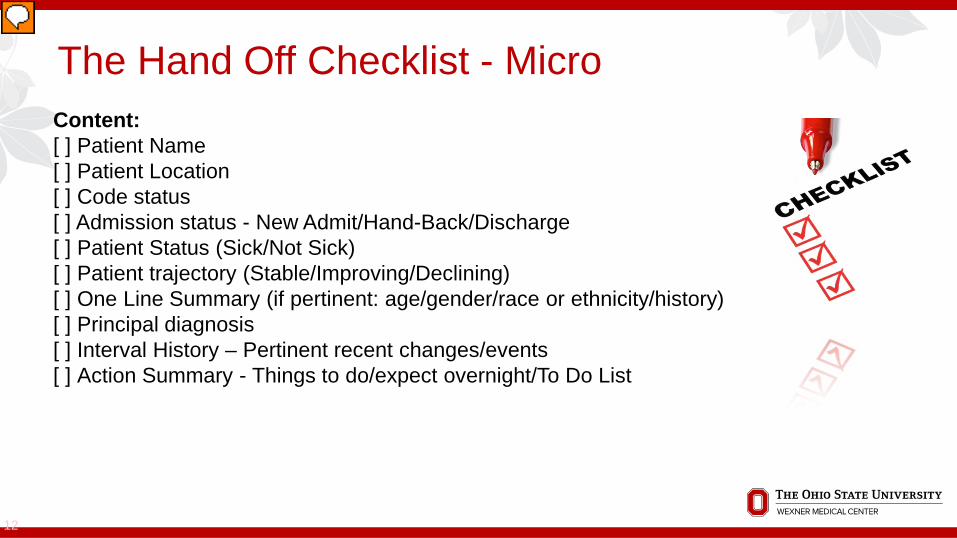
Content: [ ] Patient Name [ ] Patient Location [ ] Code status [ ] Admission status - New Admit/Hand-Back/Discharge [ ] Patient Status (Sick/Not Sick) [ ] Patient trajectory (Stable/Improving/Declining) [ ] One Line Summary (if pertinent: age/gender/race or ethnicity/history) [ ] Principal diagnosis [ ] Interval History – Pertinent recent changes/events [ ] Action Summary - Things to do/expect overnight/To Do List
Presenter
Presentation Notes
We suggested to our providers that discrete items presented within the checklist should be added to current hand-over communication if missing. We suggest that the order and content areas remain preserved, but can be flexible. In the case of the Patient History – if the preference is for a simple principal diagnosis or surgical procedure that fine. We also developed an EMR smartphrase as an algorithm to automate as much of the product as possible. All of our assessment and intervention tools are available in greater detail at our poster.
Remember that Case
13
CXR – Bilateral Pneumothorax Late result Preventable complication leading to prolonged hospitalization All we needed to know was to follow up on the CXR Could have easily avoided the arrest, the intubation Lack of hand-over prevented relay of critical information
Presenter
Presentation Notes
So thinking back to our case of respiratory difficulty in an unfamiliar patient. We ask if this system would have changed anything. No signout of any kind took place. We had little if any knowledge of the patient until we were paged about them. Had we known that an XR had been completed and that the patient was unstable and worsening we, hopefully, would have personally reviewed the image hours before. Hours before cardiac arrest.

Hand Off – The Intervention
14
With the help of the tools created for this project we can improve hospital transitions of care and patient outcomes. The implementation of these tools requires limited resources and takes very little time. In 15-30 minutes providers can improve the quality and safety of inpatient transitions of care using a simple toolset
Presenter
Presentation Notes
So what do we hope for with this? We believe that by reviewing and implementing a simple toolset, a toolset that takes 15 min to read through and a little bit of practical application, we can improve the quality of inpatient transitions of care and improve the quality and safety of multi-provider coverage schemes. Our intervention is focused on the inpatient setting but is broadly applicable across disciplines.
Next Steps
15
Educate • Performance Improvement Module • Teaches QI/Safety (DMAIC) methodology and satisfies both Part 2 and
Part 4 criteria for MOC • Project choice within our proposed Multi-Specialty Portfolio Program
Measure • Outcomes data to demonstrate value – Ongoing, multidisciplinary • Improved performance on inpatient services • Semi-automated generation of service transition lists with appropriate
prioritization
Presenter
Presentation Notes
Educate This project has been developed as a self-directed performance improvement module. The module instructs on the use of DMAIC methodology and satisfies both Part 2 and Part 4 criteria for MOC We hope to implement it as a project choice within MSPP eventually Measure Currently we are collecting outcomes data to demonstrate value – We are collecting We expect to show improved preparedness and decreased unexpected events overnight on inpatient services at multiple levels of care delivery Currently we are working to implement this system within the EMR and add discrete variables that will allow for the semi-automated generation of service transition lists with appropriate prioritization

Thank You - ABMS, Dr. Lois Nora
Very Special Thanks To: Dr. Shelly Horowitz Marty Daiga Tom Granatir Dr. David Price and all of the ABMS Visiting Scholars Shepherds!
16
Related Documents










