1 Report on The 5 th Annual AAAH Conference Human Resources for Health Challenges for Achieving MDGs 3-6 October, 2010 Sanur, Bali, Indonesia Reported by AAAH Secretariat Team International Health Policy Program (IHPP) Ministry of Public Health, Thailand With support from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Report on
The 5th Annual AAAH Conference
Human Resources for Health Challenges for Achieving MDGs
3-6 October, 2010
Sanur, Bali, Indonesia
Reported by
AAAH Secretariat Team
International Health Policy Program (IHPP)
Ministry of Public Health, Thailand
With support from
2
Table of content
Page
1. Introduction 3
2. Objectives of the conference 3
3. Structure of the 5th Annual AAAH Conference 4
4. The Asia-Pacific HRH Awards 2010 6
5. Short and keynote addresses 20
6. Main messages of the Conference 22
7. The way forward for AAAH 25
8. Acknowledgment 26
Annex 1: Conference Program 27
Annex 2: Rapporteur Team 34
Annex 3: Summary of the sessions 37
Annex 4: Suggestions from participants on the way forward of AAAH 72
31
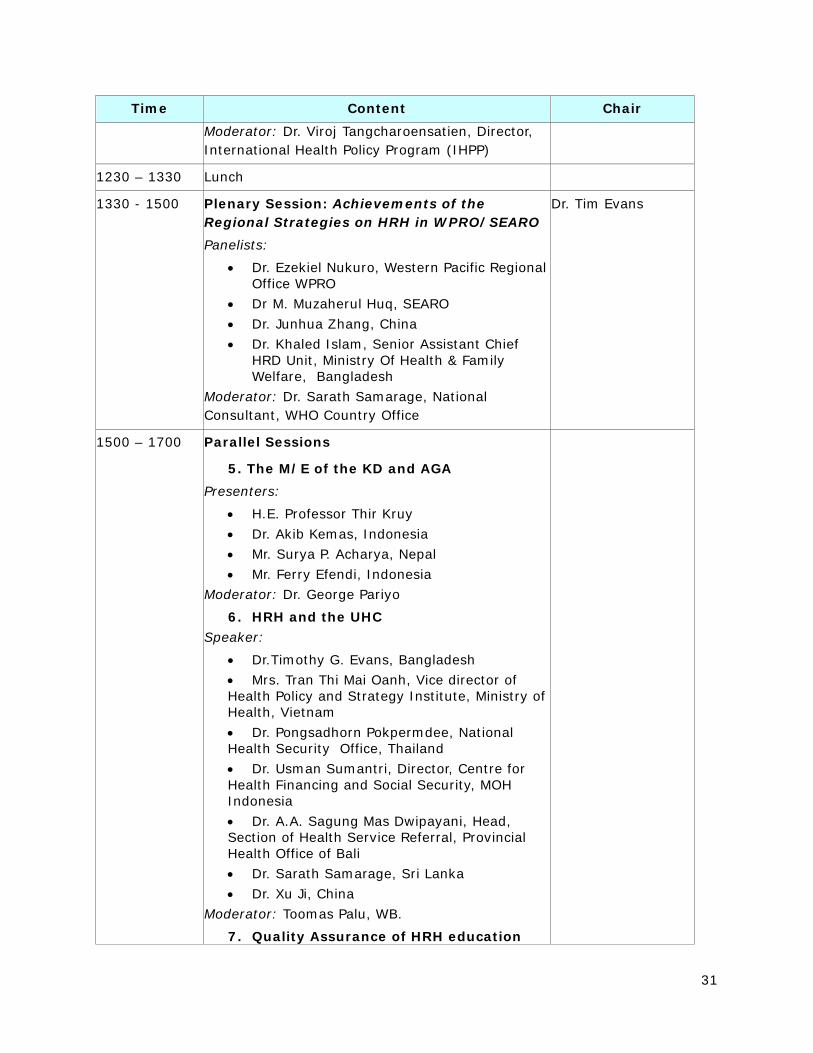
Time Content Chair Moderator: Dr. Viroj Tangcharoensatien, Director, International Health Policy Program (IHPP)
1230 – 1330 Lunch
1330 - 1500 Plenary Session: Achievements of the Regional Strategies on HRH in WPRO/SEARO Panelists:
Dr. Ezekiel Nukuro, Western Pacific Regional Office WPRO Dr M. Muzaherul Huq, SEARO Dr. Junhua Zhang, China Dr. Khaled Islam, Senior Assistant Chief HRD Unit, Ministry Of Health & Family Welfare, Bangladesh
Moderator: Dr. Sarath Samarage, National Consultant, WHO Country Office
Dr. Tim Evans
1500 – 1700 Parallel Sessions
5. The M/E of the KD and AGA Presenters:
H.E. Professor Thir Kruy Dr. Akib Kemas, Indonesia Mr. Surya P. Acharya, Nepal Mr. Ferry Efendi, Indonesia
Moderator: Dr. George Pariyo
6. HRH and the UHC Speaker:
Dr.Timothy G. Evans, Bangladesh Mrs. Tran Thi Mai Oanh, Vice director of
Health Policy and Strategy Institute, Ministry of Health, Vietnam
Dr. Pongsadhorn Pokpermdee, National Health Security Office, Thailand
Dr. Usman Sumantri, Director, Centre for Health Financing and Social Security, MOH Indonesia
Dr. A.A. Sagung Mas Dwipayani, Head, Section of Health Service Referral, Provincial Health Office of Bali
Dr. Sarath Samarage, Sri Lanka Dr. Xu Ji, China
Moderator: Toomas Palu, WB.
7. Quality Assurance of HRH education
57
Parallel Session 5 Monitoring and evaluation of the Kampala Declaration and Agenda for Global Actions
Moderator: Dr. Georgo Pariyo, GHWA Case presentation: Mr. Ferry Efendi –IndonesiaPanelists:
1. Dr. Akib Kemas -Indonesia, 2. Prof. Thir Kruy-Cambodia 3. Mr. Surya Acharya—Nepal,
Rapporteur team members: Pen Participants: 19
Moderator, George
Government plays key role in implementing the KD/AGA:
Use of evidence is very important so we know what is being done is achieving results. Scale up education and training. Retaining an effective, responsive and equitably distributed health workforce. Manage pressures of the international health workforce market and impact on migration. Securing additional and more productive investment in the health workforce.
Key Points of presentations
Prof Thir Kruy: Cambodia progress of KD/AGA
Made great efforts to meet country needs
KD/AGA most relevant to Cambodia is scaling up health workers through education and training. Focus on education, deployment, staff retention and resource mobilization to address the shortage of staff at remote and rural areas.
Enabling factors: commitment from decision makers, clear policy and strategy framework of MOH, harmonization and alignment from stakeholders and partners for resource mobilization, monitoring and follow up.
Dr. Akib: Overcoming the health workforce crisis in Indonesia –
Indonesia have completed nearly all of the agenda except for No. 2, informed response based on evidence. Need strong commitment of stakeholders to overcome this problem.
Best practices are enabling factors – incentive scheme for contract doctors and midwives, scholarship program with bonding. There are strong commitment from MOH, MOF, MONE, MOIA, health education institutions and local governments. Sustained funding also helps.
58
Mr. Surya:
AGA 1 leadership – stakeholders involved in development, implementation and evaluation. Civil society will examine impact of program.
AGA 2 informed responses – stakeholders will scale up investment in capacity building, - need to do in Nepal
AGA 4 – Retention – various incentives. Nepal has problems in terms of this. Should incentives be given just for retention or linked to performance?
AGA 5 – international health workforce market – every country should monitor their health workforce.
Relevancy of KD/AGA in Nepal: all are important but need to prioritize agenda. Which do you choose? Important one or urgent one?
Enabling factors: National Health Policy of 1991 provided enabling environment in Nepal. Large number of private institutions (17) established to train health care professionals. Access to essential health care services was increased by establishing health posts in villages and had an extensive network of female community health volunteers. Professional associations, trade unions, academic and research institutions are in existence and their participation in the process is proposed. Gov’t of Nepal has stipulated the skill mix in the health workforce. Have evidence of scale up of education and training quickly and effectively.
Learned: initiations are there, but scattered and small in scale. Commitment from each level of leadership is a must. Other ministries need to be adequately involved. Bringing all stakeholders to one table generates much, including creating ownership, maintaining transparency.
Mr. Ferry
KD AGA 3 reviewed.
Case of Indonesia – district hospitals – most have four basic medical specialist services OB/GYN, internal med, surgery, and .. But on 71.8% have these in the country. The gap is getting higher. There is a shortage in nurses in district hospitals.
Scholarship program – long term program providing financial support to attend specialist education for doctors who are willing to serve all over Indonesia.

59
Key Challenges:
Cambodia – alignment of resources, leadership role is still weak in staff management, regulatory framework related to quality of profession and education is limited.
Indonesia – decentralization is a challenge. Districts must be aware and responsible for health personnel in their areas. Maintaining regular supervision can improve motivation of health personnel working in remote areas. Production of certain types of health workers especially some areas of med doctors are limited in certain regions. Leads to maldistribution.
Mr. Ferry: most provinces don’t have working groups to address the issues of shortages and other KD/AGA related issues.
Recommendations:
Cambodia: Plan to focus on KD/AGA 1 and 4 (build leadership and retain and equitably distributed health workforce) AAAH initiatives are key of success as can bring awareness to global trends and directions., exchange strengths and weaknesses.
Indonesia – strengthen M/E, improve HRH plan with evidence based, clear indicators and costed. Strengthen CCF mechanism. Institutionalize policies on international recruitment of HRH, incentive scheme, award system for HRH in relation to its performance, privileging of health workers with adequate training to provide necessary medical actions in remote areas.
Nepal: quality control, coordination and networking, insufficient competencies in providing services, narrow skill mix of the health workforce, retention. Way forward: - institutionalization of KD/AGA at country level, harmonization of agenda, planning of HRH by July 2011, next two years will be on implementation, monitoring, reporting and feedback, after that the HRH plan will be reviewed, updated and continue implementation.
Mr. Ferry: Need to conduct analysis of contribution of the program to achieve MDGs as well as the outcomes and impact of the program. Convene a high level committee of the MoH, MONE and others.
Establish a tracking system to monitor progress on HR programs. Support from donors for Gov’t commitment to taking direct action for securing financial needs. Accelerate production of traditional cadres.
Discussion:
Dr. Karki – incentive package for health workers in rural areas in Indo – what is this? Elaborate also on bonding for scholarships.
Who funds the incentives in Indonesia, and for how long?
Dr. Akib response: incentives include transportation from original school to the areas. Monthly incentive for med docs – 7.5 million rupiahs which is a 100% increase from normal salary if they go to rural areas. Bonding depends on the length of the scholarship, if start from first year and for all years, they are bonded for the same period.
60
Wanda: what methods were used to select the specific incentives used?
Nepal – 9 districts that are difficult to reach, compared public sector salary with private sector. Decided to give 1000 Nepali rupiah per night to doctors.
Indo – have financial and non-financial incentives. Transportration in rural areas – small motorbikes. Non-financial –priority is given to them that they will be hired as a government/civil employee which is under the local government.
CHWs –purely volunteers or receive incentives? M/E of progress – what are some of the challenges in terms of monitoring and information systems on the workforce? Nepal – have been increasing reliability of information systems, in some areas still some duplication. Retention of staff in remote areas – after finishing contracts, doctors might go back to original areas. How are they retained? Are there any difficulties in linkages between central and local governments? Any constraints in strengthening health systems in one site over another site? Nepal – most power is still now decentralized, national system still working in transition to decentralization.
Cambodia – has policy to strengthen capacity and quality of training in all public and private universities. Have budget to give something to students who are from regional areas. Incentives provided to midwives – USD 10 per delivery case in order to improve services. Involve private sector in establishing regulatory framework. Projects to strengthen capacity of teaching staff.
George – Cambodia raised good point regarding the attempt to scale up training, there has been a mushrooming of private institutions. Need standards not only for the public but private institutions as well.
Ferry – decentralization is seen as creating opportunities for creating retention in remote areas. Local gov’t has authority to hire and recruit = good opportunity to get workers in the district. Another issue to be addressed is the HR information system – various data about the health workforce between central and local gov’t, need to harmonize.
Summary
Importance of ownership was highlighted by all. Monitoring, if not in place needs to be done. Incentives are keys. Cannot bring about long lasting change without regulatory support
1
Report on
The 5th Annual AAAH Conference
Human Resources for Health Challenges for Achieving MDGs
3-6 October, 2010
Sanur, Bali, Indonesia
Reported by
AAAH Secretariat Team
International Health Policy Program (IHPP)
Ministry of Public Health, Thailand
With support from
2
Table of content
Page
1. Introduction 3
2. Objectives of the conference 3
3. Structure of the 5th Annual AAAH Conference 4
4. The Asia-Pacific HRH Awards 2010 6
5. Short and keynote addresses 20
6. Main messages of the Conference 22
7. The way forward for AAAH 25
8. Acknowledgment 26
Annex 1: Conference Program 27
Annex 2: Rapporteur Team 34
Annex 3: Summary of the sessions 37
Annex 4: Suggestions from participants on the way forward of AAAH 72
3
1. Introduction
In September 2000, 189 heads of state adopted the UN Millennium Declaration and endorsed a framework for development. The plan was for countries and development partners to work together to increase access to the resources needed to reduce poverty and hunger, and tackle ill-health, gender inequality, lack of education, lack of access to clean water and environmental degradation.
Reporting on progress towards the MDGs has underscored the importance of working with countries to generate more reliable and timely data. Currently available data show that while some countries have made impressive gains in achieving health-related targets, others are falling behind. Human resources for health are viewed as major challenges to the achievement of the health-related MDGs.
For this reason, the Ministry of Health Indonesia and Asia-Pacific Action Alliance on Human Resources for Health (AAAH) are organizing the 5th AAAH Annual Conference on 3-6 October 2010, in Kuta, Bali, Indonesia with the theme of “Human Resources for Health Challenges for Achieving MDGs” which will address various issues regarding human resources for health to accelerate progress towards MDGs by 2015, in particular the context of developing countries.
2. Objectives of the conference 2.1 General objectives This Conference aims to gain an in-depth understanding of the current situation and strategies to tackle the problems of inequitable distribution of health workforces, especially those in the underserved areas. It will also discuss and refine a set of draft global recommendations, initiated by WHO, to support countries in formulating and implementing appropriate, comprehensive and feasible interventions to get committed health workers to underserved areas. These draft recommendations will be further refined by the WHO expert group, with a view to launch the final recommendations in spring 2010. This conference will also allow more intensive networking and capacity building of institutes and researchers and policy makers interested in the area of human resources for health.
2.2 Specific objectives
1. To describe the current situation regarding the distribution of committed health workforces to underserved areas, including selection and pre-service education, continuous education, recruitment, regulatory measures, financial and non-financial incentives, working and living conditions, management environment, and social and spiritual motivation.
2. To understand the factors which encourage or discourage health workforces to go and continue to work in the underserved areas.
3. To learn experiences from different countries/continents concerning the distribution and retention of health workers in underserved areas, and to foster networking among partners.
4
4. To discuss a set of draft WHO recommendations for appropriate retention strategies that will support health workers in remote and rural areas
3. Structure of the 5th Annual AAAH Conference
Activities during the 5th Annual AAAH Conference include: 1. The side meetings on Sunday 3 October 2010 2. The field visits in the afternoon of Monday 4 October 2010 afternoon 3. The main conference on 4-6 October 2010 with keynote addresses, the plenary
sessions, parallel sessions and the discussions on the futures of AAAH The Conference program is in annex 1. 3.1 The side meeting Four side meetings were organized by partner organizations included the following topics:
• Implementing the HRH Action Framework (HAF) within the GHWA Country Coordination Facilitation (CCF) Mechanism (GHWA and CapacityPlus)
• Taking action on the WHO’s recommendations for rural retention (WHO and CapacityPlus)
• HRH Education Network (AAAH Secretariat) • AAAH Steering Committee Meeting (AAAH Secretariat)
3.2 The field visits Three sites focusing on different issues were arranged by the Indonesian colleagues. Participants would choose to visit either of them, including a) HRH Education Institutions at Denpasar Health Polytechnic, b) Health Service Delivery at Puskesmas III Denpasar Selatan, and c) Universal Health Care Coverage at Tabanan hospital The objectives of the field visits were:-
• To provide an opportunity for the Conference Participants to learn about health professional education system in Indonesia, the role of public and private sector in HRH production and health service delivery, and the local health authority strategies in achieving toward Universal Health Coverage
• To provide an opportunity to the national and international experts for sharing experiences
5
3.3 The main conference There were three plenary sessions and a total of 10 parallel sessions. Three plenary sessions covered issues including:-
PL1: Dialogue on HRH Challenges to Achieve MDGs PL2: HRH Education in the 21st Century PL3: Achievements of the Regional Strategies on HRH in WPRO/SEARO
There were a total of 10 parallel sessions which included those covering the following topics:
PS1: Innovative education to support MDGs PS2: HRH key challenges and responses of countries in Asia PS3: Private sector and HRH education towards MDGs PS4: The Code of Practice for International Recruitment of Health Personnel PS5: The M/E of the KD and AGA PS6: HRH and UHC PS7: Quality assurance of HRH education and regulation PS8: Continuing professional development PS9: Teaching of public health PS10: Community health workers
6
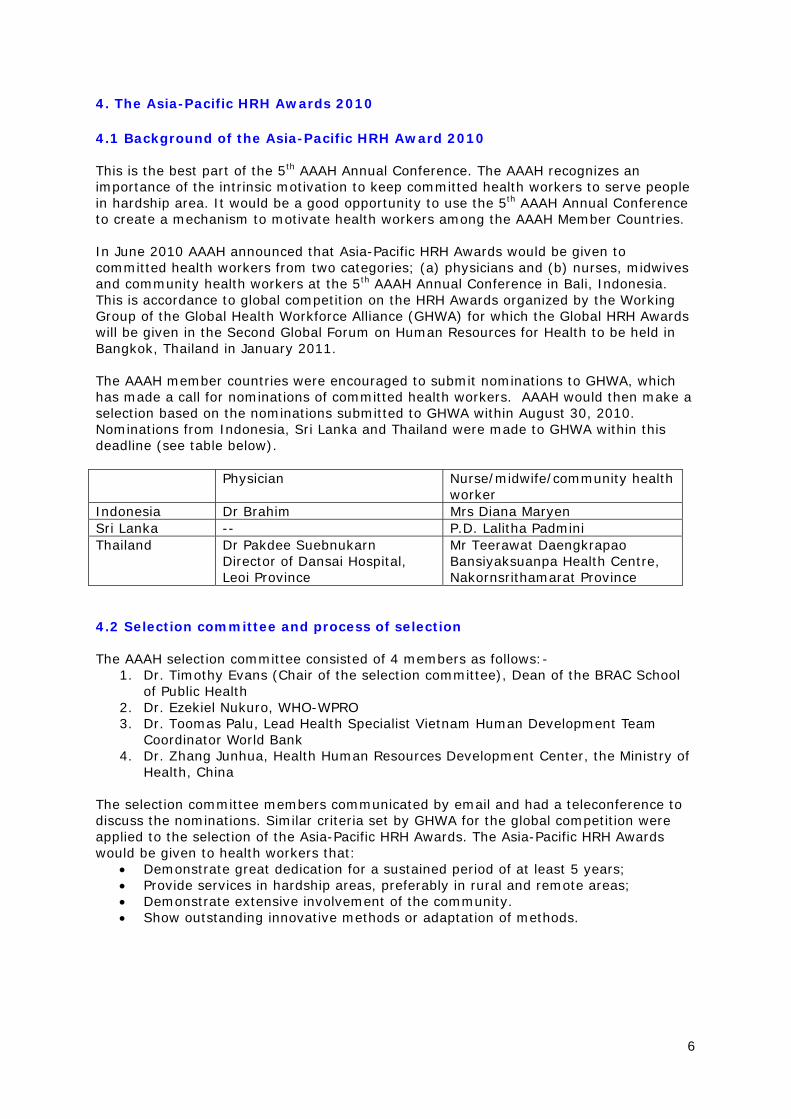
4. The Asia-Pacific HRH Awards 2010 4.1 Background of the Asia-Pacific HRH Award 2010 This is the best part of the 5th AAAH Annual Conference. The AAAH recognizes an importance of the intrinsic motivation to keep committed health workers to serve people in hardship area. It would be a good opportunity to use the 5th AAAH Annual Conference to create a mechanism to motivate health workers among the AAAH Member Countries. In June 2010 AAAH announced that Asia-Pacific HRH Awards would be given to committed health workers from two categories; (a) physicians and (b) nurses, midwives and community health workers at the 5th AAAH Annual Conference in Bali, Indonesia. This is accordance to global competition on the HRH Awards organized by the Working Group of the Global Health Workforce Alliance (GHWA) for which the Global HRH Awards will be given in the Second Global Forum on Human Resources for Health to be held in Bangkok, Thailand in January 2011. The AAAH member countries were encouraged to submit nominations to GHWA, which has made a call for nominations of committed health workers. AAAH would then make a selection based on the nominations submitted to GHWA within August 30, 2010. Nominations from Indonesia, Sri Lanka and Thailand were made to GHWA within this deadline (see table below). Physician Nurse/midwife/community health
worker Indonesia Dr Brahim Mrs Diana Maryen Sri Lanka -- P.D. Lalitha Padmini Thailand Dr Pakdee Suebnukarn
Director of Dansai Hospital, Leoi Province
Mr Teerawat Daengkrapao Bansiyaksuanpa Health Centre, Nakornsrithamarat Province
4.2 Selection committee and process of selection The AAAH selection committee consisted of 4 members as follows:-
1. Dr. Timothy Evans (Chair of the selection committee), Dean of the BRAC School of Public Health
2. Dr. Ezekiel Nukuro, WHO-WPRO 3. Dr. Toomas Palu, Lead Health Specialist Vietnam Human Development Team
Coordinator World Bank 4. Dr. Zhang Junhua, Health Human Resources Development Center, the Ministry of
Health, China
The selection committee members communicated by email and had a teleconference to discuss the nominations. Similar criteria set by GHWA for the global competition were applied to the selection of the Asia-Pacific HRH Awards. The Asia-Pacific HRH Awards would be given to health workers that:
• Demonstrate great dedication for a sustained period of at least 5 years; • Provide services in hardship areas, preferably in rural and remote areas; • Demonstrate extensive involvement of the community. • Show outstanding innovative methods or adaptation of methods.

7
4.3 The Asia-Pacific HRH Awardees 2010 The selection committee came to the following decisions:-
• The Asia-Pacific HRH Award 2010 for committed physician is given to Dr Pakdee Suebnukarn from Thailand for his distinctive innovative thinking and approaches of involving community participation especially children to work for their communities.
• The Asia-Pacific HRH Award 2010 for committed nurses/midwives/community health worker is given to Mrs Diana Maryen from Indonesia for her work in the community which is addressing the MDGs such as through maternal and child health surveillance. She also worked with the strong traditional beliefs in the communities when educating mothers on health and child health issues.
Other nominated health workers were given the recognition trophy and invited to the 5th AAAH Annual Conference in Bali, Indonesia, between 3 and 6 October 2010. All Asia-Pacific HRH Awards and recognition 2010 are summarized in table below. Physician Nurse/midwife/community health
worker Asia-Pacific HRH Award
Dr Pakdee Suebnukarn, Thailand Mrs Diana Maryen, Indonesia
Asia-Pacific HRH Recognition
Dr Brahim, Indonesia P.D. Lalitha Padmini, Sri Lanka Mr Teerawat Daengkrapao, Thailand
4.4 Awarding Ceremony All nominated health workers were invited to join the 5th AAAH Annual Conference in Bali, Indonesia, between 3 and 6 October 2010. The Awarding Ceremony was held in the morning of Wednesday 6 October 2010. The Asia-Pacific HRH Award and Recognition trophies were given to all five committed health workers. Their speech/reflection right after the Awarding Ceremony is shown below.
The Asia-Pacific HRH Award 2010 for committed physician is given to Dr Pakdee Suebnukarn from Thailand. Unfortunately, Dr Pakdee Suebnukarn was not able to join the Awarding Ceremony due to prior obligation. Dr. Pattapong Kessomboon received the award on behalf of Dr. Pakdee Suebnukarn.

8
The Asia-Pacific HRH Award 2010 for committed nurses/midwives/community health worker is given to Mrs Diana Maryen from Indonesia. Asia-Pacific HRH Recognition
The Asia-Pacific HRH Recognition 2010 for committed physician: Dr Brahim, Indonesia

9
The Asia-Pacific HRH Recognition 2010 for committed nurse/midwife/community health worker: P.D. Lalitha Padmini, Sri Lanka Unfortunately, P.D. Lalitha Padmini was not able to join the Awarding Ceremony due to prior obligation. Dr. Sarath Samarage received the award on behalf of P.D. Lalitha Padmini.
The Asia-Pacific HRH Recognition 2010 for committed nurse/midwife/community health worker: Mr Teerawat Daengkrapao
10
4.4.1 The Asia-Pacific HRH Award 2010 for committed physician: Dr Pakdee Suebnukarn from Thailand Unfortunately, Dr Pakdee Suebnukarn was not able to join the Awarding Ceremony due to prior obligation. His background and works were presented in the ppt slides below. Slide 1
Slide 1 Dr Pakdee Suebnukarn is the Director of Dansai hospital, 60 bed district hospital. He serves as a rural doctor at this hospital for 23 years. His thought is really impress. “Health service with essence of being human, from my experience, the key is that you treat your patients as good as you want your mother to be treated, that's it”
Slide 2
Slide 2 Dr Pakdee revitalizes Dansai Hospital to be living organization.
Slide 3
Slide 3 System would be effective and efficient because of wisdom and spirituality. This would lead to sustainable healthcare organization
11
Slide 4 and 5
Slide 4 and 5 He makes health workers in Dansai Hospital to provide humanized health service to the patient without discrimination
Slide 6
Slide 6 At the same time, he could apply international guideline like Ottawa Charter for Health Promotion to suit the local context.
Slide 7 Slide 7 Culture of voluntarism is gradually cultivated into health staff of Dansai Hospital
12
Slide 8 and 9
Slide 8 and 9 Three main strategies are applied for gradually revitalizing the remote district hospital. First strategy is ‘personal transformation’ to truly understand yourself and find appropriate job to happily work and to be role model for other persons.
Slide 10 Slide 10 Second strategy is ‘organization transformation’ by improving environment with participatory of multi-stakeholders, especially student and children
13
Slide 11
Slide 11 Third strategy is ‘social transformation’ by nurturing children who are the future of the community and the nation
Slide 12
Slide 12 Dr Pakdee would like to say again his thought “the key is that you treat your patients as good as you want your mother to be treated, that's it”

14
4.4.2 The Asia-Pacific HRH Award 2010 for committed health worker: Mrs Diana Maryen, Indonesia Mrs Diana Maryen and her husband joined the 5th AAAH Annual Conference in Bali, Indonesia. After receiving the Award; she gave her speech in Indonesian language and after that a translator translated in English. Mrs Diana Maryen, Indonesia The Outstanding Midwives from Eastern Indonesia As we all know, providing a good public health services requires a lot of effort and sacrifices. Mrs Diana, one of Indonesia’s Kartini performing her tasks as a midwives in Pustu Anggaduber, Puskesmas Marauw, Kab. Biak Numfor, Papua Province in the Eastern Indonesia. Bidan Diana constantly and continuously supports and assists the community. Her principle of “if not I who else” made her become one of the most devoted midwives in Indonesia. In spite of difficult conditions with minimum infrastructure and facilities, she still able to perform her tasks well. In her view, if community is happy she is happy. Her wish is that someday she will have the opportunity to learn and increase her knowledge and skills to that she can contribute more to the community.

15
4.4.3 The Asia-Pacific HRH Recognition 2010 for committed physician: Dr Brahim, Indonesia Dr Brahim gave his speech at the Conference. Dr Brahim, Indonesia
Assalamu’alaikum warahmatullahi wabarakatuh,
May the blessings of God always be with us,
Distinguished guests and participants, from the deepest side of my heart, I will introduce myself and my work that have transformed me and my character. I also thank God for the opportunity to be here and to stand in front of this most honorable forum.
My name is doctor Brahim, born from an ordinary family in Brakharang, a small village in Binjai city, Deli Serdang District, North Sumatra on 8 March 1961. I studied at Tarumanegara Medical School, Jakarta. After having graduated in 1988, I work at Abdi Waluyo Cardiac Hospital, Jakarta.
The memory of my childhood spent in a village close to rivers and forest, even though I had been a young medical doctor. I started missing my rural life, and start searching for future site of my service. From so many sources, I knew that many doctors were not willing to work in Papua (previously known as Irian Jaya) for different reasons. This challenged me to serve there; and therefore, I work as a contracted doctor in Karas village, Fakfak District, Irian Jaya Province, that become Karas Subdistrict of Fakfak District, Papua Barat Province.
I arrived in Karas having strong motivation, carving in my heart. I thought about words that can inspire me to live and struggle in a challenging situation, happiness, sadness, and loneliness day and night. After having been there for some time, in the middle of my life, I realized that all of my experiences had taught me to accept and thanked God, the Creator of my life. The inspiring words are: “Come, stay with them, love them, learn from them, plan everything with them and help them. You must start from what they know; you must build something from what they have”.
The biggest challenge of serving people in coastal areas and outer islands, far from the capital city of the district, is that the area is so large covering 21 villages, far from each other, inhabited by people which are unevenly distributed. I decided to meet people more often, and taught them how to live in a clean and healthy lifestyle, since I believe that “health service by the people themselves is the cheapest and justified given the condition of Papua”.
My toughest challenge in the beginning of my job was the different views of the people about diseases. In the past, the important thing was not what, but who caused diseases. In this situation, the influence of magicians or traditional healers could not be ignored. For example, when a traditional birth attendant assisted a mother to deliver a baby causing heavy bleeding because of her inappropriate massage, I was the last person to be asked for help. Although the baby was saved, the mother had died because of the bleeding. It was hard for me to be accused as causing the death of the mother.
16
Another story was about mothers who refused to have her baby’s umbilical cord cut after delivery. They thought that the placenta was the baby’s brother or sister. At that time, I struggled to cope with this custom and people’s opinion for years. The results are that now community health centre, sub- community health centre and village birthing place (polindes) become the only place that people seek health services. In addition, integrated community health posts become community-based health efforts with full participation of the people. The people can now seek health services whenever they need through report and act mechanism. Moreover, this leads me to know which traditional healers are cooperative and which ones need some efforts, so that they will add the people’s burden.
The results of my long struggle can be seen now. However, am an ordinary person, who feel lonely because of separated from my children and wife. It is for my children’s best education, I am separated far away from them, between remote Papua and Java islands. In order to visit them, I have to wait until I have an official job in Java. Most of the time, I cannot go for Idul Fitri celebration with my family. Because of financial constraint, I had to write letters to Fakfak District Health Office and others to ask for help, when my father was severely ill in Java.
I have started my work in Karas, and I really want to end it in Karas. I have never been moving to any other places, and do not want to leave until the people there do not need me anymore. That was why I refused all offerings that would gave me the opportunity for further study or promotion, because I just want to serve in Papua. I am aware and believe in my own destiny by working and providing health service, that here in Papua I have a peaceful and happy life more than anything else.
I believe that my God always be with me. He always help me in my struggle and have raised me to this higher stage here today. When I learn how much God has given me, I then know that “We (I and my friends in the Community Health Centre) plant, we water the plants, but only God grows them”.
Thank you.
Dr. Brahim
17
4.4.4 The Asia-Pacific HRH Recognition 2010 for committed health worker: Mr Teerawat Daengkrapao, Thailand Speech of Mr Teerawat Daengkrapao, Thailand Mr Teerawat Daengkrapao Honorable colleagues, Nowadays, “health” is complex and inter-related with all other determinants. Solving health problems is increasingly complex. Demographic and health transition and increase demand for health services result in rapid increase health expenditures. How to control healthcare cost is a challenging question. Solution should be a participatory process. Our team contributes to “create health awareness for all people in the community”. We believe that “health is everyone’s business”. We design module to train and empower village health volunteers applying life long self learning process. They gradually become powerful volunteers and closely collaborate with health workers at the local level. In addition, health empowerment at the community level has proved that members are able to lead a healthy life style and manage not only their own health problems but also their friend, relatives and neighbors. Therefore, “self learning, empowerment and management of own health problems”, a fundamental platform towards healthy community, should be one of the solutions which at the end lead to a sustainable “good health at low cost”. Thank you very much Thai version คาํกลา่วของคณุธรีะวฒัน ์แดงกะเปา ทา่นผูม้เีกยีรตทิกุทา่น ทกุวันน ี“สขุภาพ” เชอมโยงเกยีวขอ้งกบัทกุเรอืง มคีวามซบซอนจนยากทจีะแยกออกจากกนัื ั ้ ได ้แนวโนม้ในการจัดการสขุภาพจงึยากขนึเรอืยๆ สงผลใหค้า่ใชจา่ยเรอืงสขุภาพสงูขนึตลอดเวลา่ ้ ทําอยา่งไรให ้“ตน้ทนุดา้นสขุภาพตําลง” เป็นคําถามทน่ีาจะหาทางออกรว่มกนั ชองทางหนงึททีมี่กระผมไดดํ้าเนนิการอยู ่คอื ทําใหเ้รอืงสขุภาพเป็นเรอืงของทกุคน ทกุคนเป็นเจา้ของสขุภาพ โดยการสรา้งโรงเรยีนสอนอาสาสมัครสาธารณสขุขนึมา จัดกระบวนการเรยีนรูต้ลอดชวติ จนเป็นอาสาสมัครทีีทรงพลัง แลว้รว่มมอืกบับคุลากรสาธารณสขุ โดยเฉพาะระดับพนืท ีจัดกจิกรรมสรา้งการเรยีนรูใ้นชมุชน ใหส้ามารถจัดการสขุภาพตนเอง ครอบครัว ญาตมิติร และคนในชมุชน กนัเองได ้ “การเรยีนรู ้ส ูการจัดการสขุภาพ ดว้ยตนเอง่ ” จงึน่าจะเป็นทางออกหนงึทจีะนําพาเรอืงสขุภาพกา้วสยูคุ่ใหม ่คอื ยคุแหง่ “สขุภาพดตีน้ทนุตํา” ขอบพระคณุครับ
18
4.4.5 The Asia-Pacific HRH Recognition 2010 for committed health worker: P.D. Lalitha Padmini, Sri Lanka P.D. Lalitha Padmini, Sri Lanka Slide 1
Slide 2
Slide 3
Slide 4

19
Slide 5
20
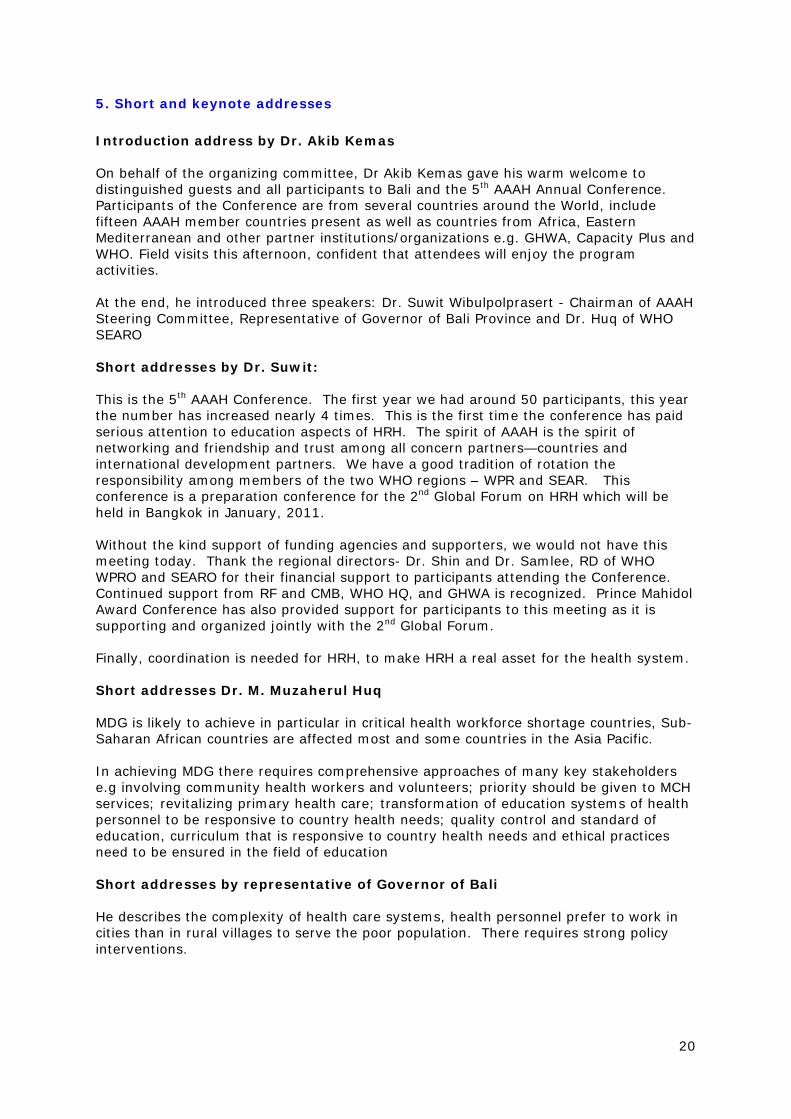
5. Short and keynote addresses Introduction address by Dr. Akib Kemas On behalf of the organizing committee, Dr Akib Kemas gave his warm welcome to distinguished guests and all participants to Bali and the 5th AAAH Annual Conference. Participants of the Conference are from several countries around the World, include fifteen AAAH member countries present as well as countries from Africa, Eastern Mediterranean and other partner institutions/organizations e.g. GHWA, Capacity Plus and WHO. Field visits this afternoon, confident that attendees will enjoy the program activities. At the end, he introduced three speakers: Dr. Suwit Wibulpolprasert - Chairman of AAAH Steering Committee, Representative of Governor of Bali Province and Dr. Huq of WHO SEARO Short addresses by Dr. Suwit: This is the 5th AAAH Conference. The first year we had around 50 participants, this year the number has increased nearly 4 times. This is the first time the conference has paid serious attention to education aspects of HRH. The spirit of AAAH is the spirit of networking and friendship and trust among all concern partners—countries and international development partners. We have a good tradition of rotation the responsibility among members of the two WHO regions – WPR and SEAR. This conference is a preparation conference for the 2nd Global Forum on HRH which will be held in Bangkok in January, 2011. Without the kind support of funding agencies and supporters, we would not have this meeting today. Thank the regional directors- Dr. Shin and Dr. Samlee, RD of WHO WPRO and SEARO for their financial support to participants attending the Conference. Continued support from RF and CMB, WHO HQ, and GHWA is recognized. Prince Mahidol Award Conference has also provided support for participants to this meeting as it is supporting and organized jointly with the 2nd Global Forum. Finally, coordination is needed for HRH, to make HRH a real asset for the health system. Short addresses Dr. M. Muzaherul Huq MDG is likely to achieve in particular in critical health workforce shortage countries, Sub-Saharan African countries are affected most and some countries in the Asia Pacific. In achieving MDG there requires comprehensive approaches of many key stakeholders e.g involving community health workers and volunteers; priority should be given to MCH services; revitalizing primary health care; transformation of education systems of health personnel to be responsive to country health needs; quality control and standard of education, curriculum that is responsive to country health needs and ethical practices need to be ensured in the field of education Short addresses by representative of Governor of Bali He describes the complexity of health care systems, health personnel prefer to work in cities than in rural villages to serve the poor population. There requires strong policy interventions.
21
Keynote addresses by Mrs Diana Maryen, Indonesia and Dr Brahim, Indonesia
The Indonesian host of the Conference recommended to invite Mrs Diana Maryen and Dr Brahim from Indonesia to provide keynote addresses at the opening session of the Conference. This is to give high recognition to the committed health workers in the remote area. Apart from keynote address, both of them got Asia-Pacific HRH Award and recognition, accordingly (see section 4.3 Asia-Pacific HRH Awardees 2010). Their keynote addresses can be seen in section 4.4 Awarding ceremony above.
In order to pay high recognition to committed health workers in underserved area, there is a recommendation by the AAAH Steering Committee and supported by many participants that keynote address can be reserved for 1-2 committed health workers of the local host country of the AAAH Annual Conference.
22
6. Main messages of the Conference
There are approximately 195 participants registered for the Conference who are 50 Indonesian health workers, 125 registered participants from the AAAH country members and its partners and 20 from countries in African and Eastern Mediterranean Region and international development partners.
The Conference program includes three plenary sessions and ten parallel sessions. Main contents of each session were summarized by the Rapporteur Team and synthesized by the Lead Rapporteur, Dr Viroj Tangcharoensathien, the director of International Health Policy Program (IHPP), Ministry of Public Health, Thailand. Name list of the Rapporteur Team is in annex 2.
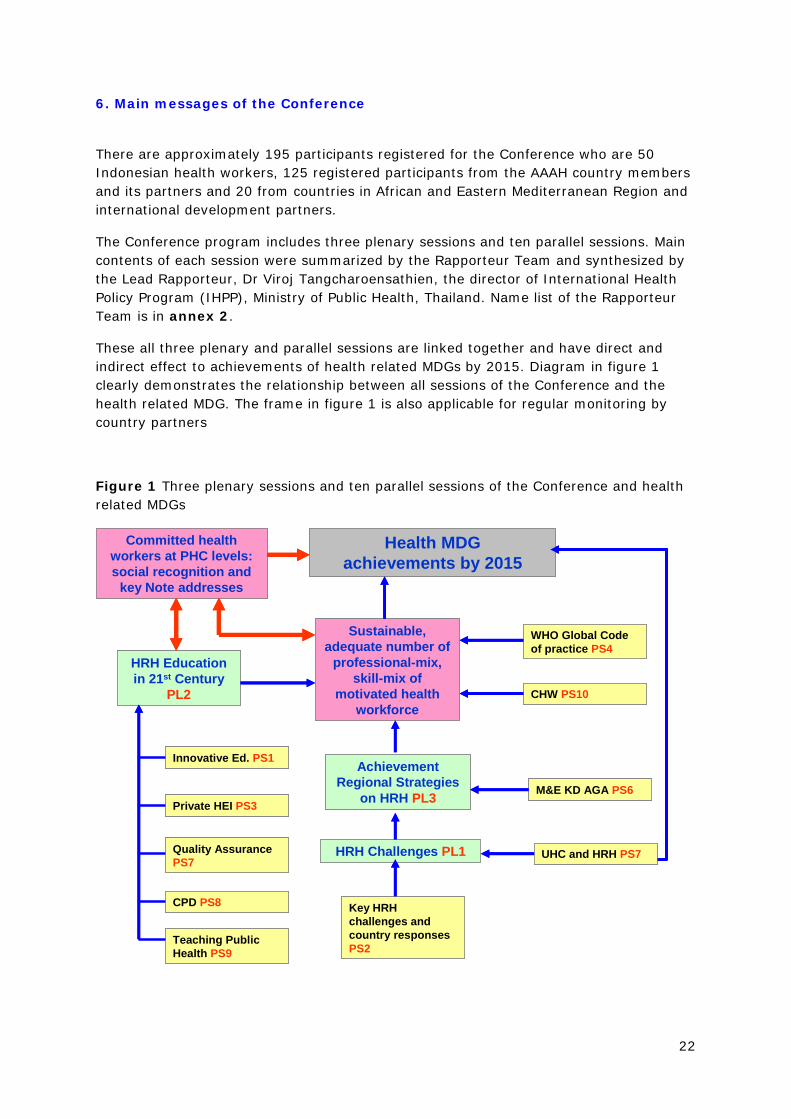
These all three plenary and parallel sessions are linked together and have direct and indirect effect to achievements of health related MDGs by 2015. Diagram in figure 1 clearly demonstrates the relationship between all sessions of the Conference and the health related MDG. The frame in figure 1 is also applicable for regular monitoring by country partners
Figure 1 Three plenary sessions and ten parallel sessions of the Conference and health related MDGs
HRH Challenges PL1
Health MDG achievements by 2015
HRH Education in 21st Century
PL2
M&E KD AGA PS6
Innovative Ed. PS1
Private HEI PS3
Quality Assurance PS7
CPD PS8
Teaching Public Health PS9
WHO Global Code of practice PS4
CHW PS10
UHC and HRH PS7
Key HRH challenges and country responses PS2
Sustainable, adequate number of
professional-mix, skill-mix of
motivated health workforce
Achievement Regional Strategies
on HRH PL3
Committed health workers at PHC levels: social recognition and
key Note addresses
HRH Challenges PL1
Health MDG achievements by 2015
HRH Education in 21st Century
PL2
M&E KD AGA PS6
Innovative Ed. PS1
Private HEI PS3
Quality Assurance PS7
CPD PS8
Teaching Public Health PS9
WHO Global Code of practice PS4
CHW PS10
UHC and HRH PS7
Key HRH challenges and country responses PS2
Sustainable, adequate number of
professional-mix, skill-mix of
motivated health workforce
Achievement Regional Strategies
on HRH PL3
Committed health workers at PHC levels: social recognition and
key Note addresses

23
Main findings from the synthesis
Evidences from many forums and activities clearly indicate that HRH is high on the political agenda at all levels, global, regional and national levels. At the global level, in the Tokyo G8 summit in 2008, human resources for health (HRH) is highlighted as one main issue apart from other two issues of health information system and health financing. All WHO member states put efforts together to endorse the WHA resolution on WHO Global Code of Practice on International Recruitment of Health Personnel in May 2010 to support better and ethical management of international flows. The First Global Forum on HRH was held in Kampala and the Second Global Forum on HRH will be held in Bangkok in Jan 2011. At regional level, it can be seen from the regional strategies on HRH of the WHO regional offices in South East Asia and Western Pacific. Country Coordinating Framework is launched and implemented to promote multi-sectoral ownership and ensure evidence based for the development of national strategies in many countries.
Know-how on HRH development is adequate for further improvement. Evidence, tool kits and best practice can be found in both developed and developing countries. Examples of evidence are WHO rural retention publication which provides interventions that work and do not work; the Commission on Medical Education in the 21st Century and ample experience on task shifting in international peer review journals. Many tool kits are useful for example DCE, Discrete Choice Experiment, on stated job preferences for effective policy designs, participatory priority settings for policy interventions and HRH planning and projection which needs regular update and adjustment to changing context. Variety of health and non-health reforms can be seen in many countries. These reforms can be either threats or opportunities for HRH development. Examples of the reforms are Chinese policy towards Universal Health Coverage (UHC) stimulate production and distributions of HRH; Vietnam UHC achievement pending strong primary health care and deployment of HRH and Thai UHC prompts to rapid production of family physicians.
Many countries, especially developing countries, have faced many challenging problems both conventional and emerging problems. Unresolved critical shortage, inadequate skills and mal-distribution are classic problems of many countries. Private sector growths and trade in health service can be opportunity of the country and at the same time can be threat when it is not good plan and management. Some other main challenges are international and national migration of well trained health personnel, international movement of patients seeking care in high quality at lower cost. The situation would be worse when there is a weak coordination and constructive dialogue between trade and health; public and private production and employment sector; dissociation between curriculum design and national and sub-national/community needs; bio-medical and social interventions and contributions of various determinants to health of population. In many countries, there is incoherence between policies for trade and health. Health education institutes are driven by international market demand, export oriented, and at times not responsive to community health needs. There continue to be poorly equipped and low motivated faculties. Problem based learning is seen as a key entry point of reform. Public health curriculum needs included needing to adapt to national and global health contexts in the 21st century, and understanding the complex dynamics of Social Determinants of Health. In terms of in-service capacity development, re-licensing may be applied. Reorientation towards transformative professional education including quality assurance, licensing and accreditation should perform. Faculty development is needed as well as staff retention.

24
There was the view that “health personnel are technically competent and socially accountable to respond to priority health needs of the country.” Detail of each session can be seen in annex 3, summary by the rapporteur team.

25
7. The way forward for AAAH
Method used and process In the morning of 5th of October 2010, during the second plenary session, all participants of the 5th AAAH Annual Conference were asked to write down his/her idea on the most important suggestion on what they expect from the AAAH, apart from an annual conference and existing activities of the AAAH. One participant was asked for only one suggestion. At the end of the second plenary session, there were 60 respondents submitted their suggestions to the AAAH Secretariat. Majority of respondents shared one most important point while some respondents shared more than one issue. Results All suggestions and comments from 60 respondents were listed in annex 4. Similar suggestions were merged and then classified into 6 groups as can been seen in Appendix 2. These six groups are (A) networking and collaborating, (B) research/evidence generation, (C) Information sharing and knowledge exchange, (D) Institutional Strengthening and Capacity Development or Supporting implementation at country level, (E) assessment of the AAAH and (F) others. These main six groups are voted by a total of 25 meeting tables in the Conference room. One table has one vote. The results of the voting shows that majority of the Conference would prefer the way forward of the AAAH on networking and collaborating (9 out of 25 scores), follows by information sharing & knowledge exchange and institutional strengthening & capacity development or supporting implementation at country level (7 scores each). See detail in table 1. Table 1 Voting results of the way forward for the AAAH
Topic Vote (A) Networking and collaborating 9 (B) Collaborative Research/evidence generation 1 (C) Information sharing and knowledge exchange 7 (D) Institutional Strengthening and Capacity Development
or Supporting implementation at country level (technical support)
7
(E) Systematic Assessment of the AAAH 1 Total 25
26
8. Acknowledgment
• The host country – Indonesia MOH and other local/international partners for their hospitality
and conference organization • The conference is supported by
– WHO WPRO, SEARO – China Medical Board – GHWA – Rockefeller Foundation – Prince Mahidol Award Conference
• Active contributions and active participation – Chairs, moderators, speakers, panellists, – Participants
• Conference summary and proceeding synthesis – Rapporteur team of 4 Indonesian, 1 Rockefeller, 2 Thai and 4 AAAH
secretariat staffs – Lead rapporteur, Dr Viroj Tangcharoensathien, the director of International
Health Policy Program (IHPP), Ministry of Public Health, Thailand
==============================
27
Annex 1: Conference Program
AAAH 5th Annual Conference Program
Date: 3-6 October 2010
Venue: The Sanur Paradise Plaza Hotel Bali, Indonesia
Theme: HRH Challenges for Achieving MDGs
Objectives: To address and discuss HRH challenges to achieving MDGs and provide input to the planning for the 2nd Global Forum The Conference program has several activities: 4. The side meetings on Sunday Oct 3rd. 5. The field visits on Monday Oct 4th afternoon. 6. The main conference Oct 4-6th with keynote addresses, the plenary sessions, parallel
sessions and the discussions on the futures of AAAH. 7. The AAAH awards in response to the GHWA awards.
1. Pre-conference side meetings(Optional) Sunday 3 October 2010
Time Content Coordinators of the session
0830 – 1230
1400 – 1700
1400 – 1600
1700 – 2000
Side meeting topics
• Implementing the HRH Action Framework (HAF) within the GHWA Country Coordination Facilitation (CCF) mechanism
• Taking action on the WHO’s recommendations for rural retention
• AAAH Steering Committee Meeting
• HRH Education Network
GHWA/AAAH Secretariat/Capacity Plus
WHO/Capacity Plus /Indonesia
AAAH
AAAH
0800 onward Registration for the conference Local host and AAAH Secretariat
28
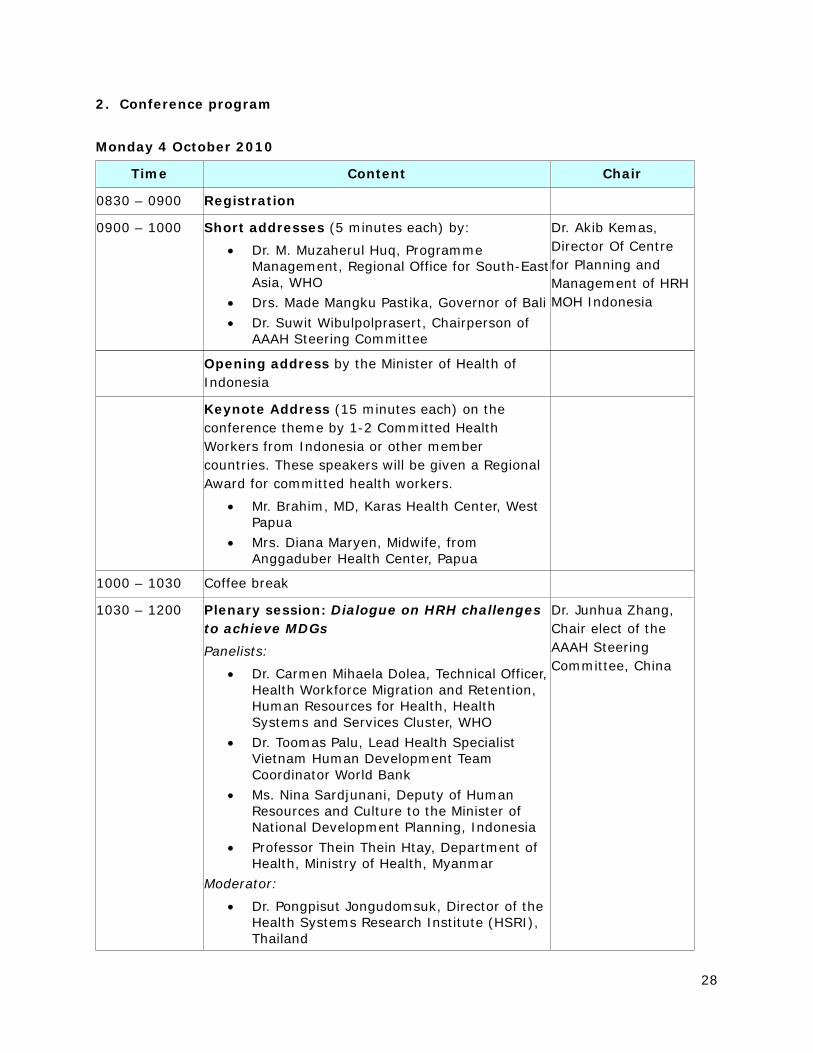
2. Conference program Monday 4 October 2010
Time Content Chair
0830 – 0900 Registration
0900 – 1000 Short addresses (5 minutes each) by:
• Dr. M. Muzaherul Huq, Programme Management, Regional Office for South-East Asia, WHO
• Drs. Made Mangku Pastika, Governor of Bali • Dr. Suwit Wibulpolprasert, Chairperson of
AAAH Steering Committee
Dr. Akib Kemas, Director Of Centre for Planning and Management of HRH MOH Indonesia
Opening address by the Minister of Health of Indonesia
Keynote Address (15 minutes each) on the conference theme by 1-2 Committed Health Workers from Indonesia or other member countries. These speakers will be given a Regional Award for committed health workers.
• Mr. Brahim, MD, Karas Health Center, West Papua
• Mrs. Diana Maryen, Midwife, from Anggaduber Health Center, Papua
1000 – 1030 Coffee break
1030 – 1200 Plenary session: Dialogue on HRH challenges to achieve MDGs Panelists:
• Dr. Carmen Mihaela Dolea, Technical Officer, Health Workforce Migration and Retention, Human Resources for Health, Health Systems and Services Cluster, WHO
• Dr. Toomas Palu, Lead Health Specialist Vietnam Human Development Team Coordinator World Bank
• Ms. Nina Sardjunani, Deputy of Human Resources and Culture to the Minister of National Development Planning, Indonesia
• Professor Thein Thein Htay, Department of Health, Ministry of Health, Myanmar
Moderator:
• Dr. Pongpisut Jongudomsuk, Director of the Health Systems Research Institute (HSRI), Thailand
Dr. Junhua Zhang, Chair elect of the AAAH Steering Committee, China
29
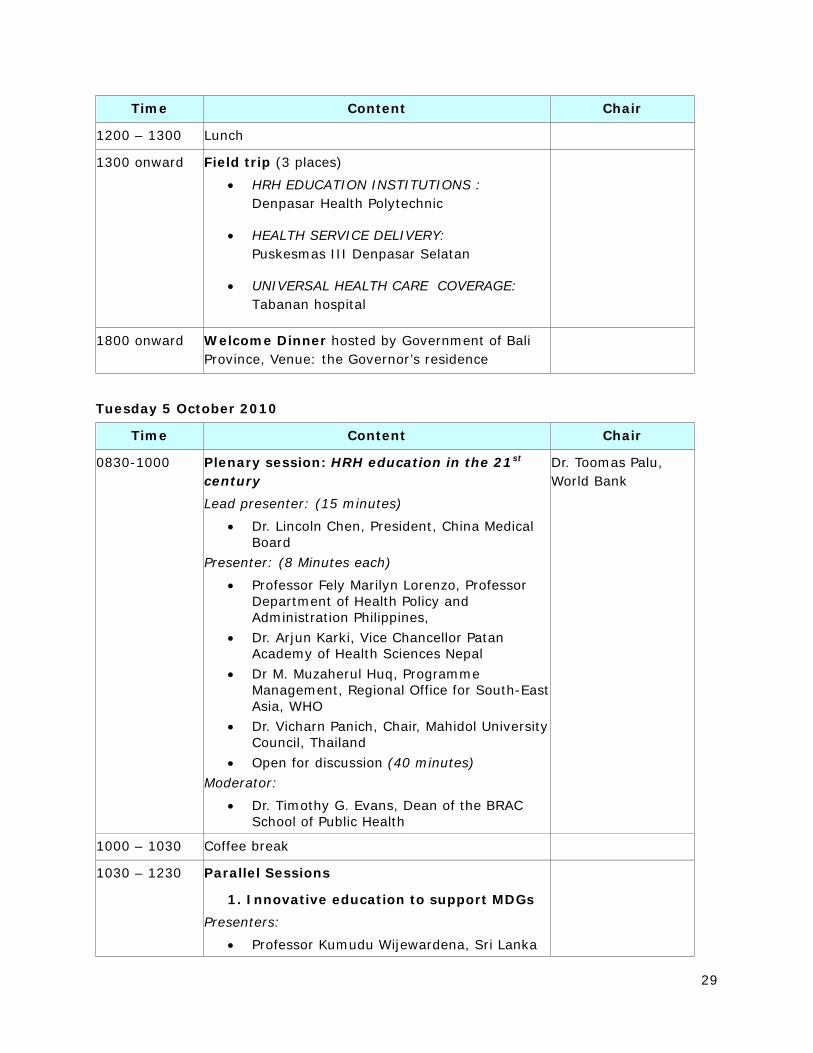
Time Content Chair
1200 – 1300 Lunch
1300 onward Field trip (3 places)
• HRH EDUCATION INSTITUTIONS : Denpasar Health Polytechnic
• HEALTH SERVICE DELIVERY: Puskesmas III Denpasar Selatan
• UNIVERSAL HEALTH CARE COVERAGE: Tabanan hospital
1800 onward Welcome Dinner hosted by Government of Bali Province, Venue: the Governor’s residence
Tuesday 5 October 2010
Time Content Chair
0830-1000 Plenary session: HRH education in the 21st century Lead presenter: (15 minutes)
• Dr. Lincoln Chen, President, China Medical Board
Presenter: (8 Minutes each)
• Professor Fely Marilyn Lorenzo, Professor Department of Health Policy and Administration Philippines,
• Dr. Arjun Karki, Vice Chancellor Patan Academy of Health Sciences Nepal
• Dr M. Muzaherul Huq, Programme Management, Regional Office for South-East Asia, WHO
• Dr. Vicharn Panich, Chair, Mahidol University Council, Thailand
• Open for discussion (40 minutes) Moderator:
• Dr. Timothy G. Evans, Dean of the BRAC School of Public Health
Dr. Toomas Palu, World Bank
1000 – 1030 Coffee break
1030 – 1230 Parallel Sessions
1. Innovative education to support MDGs Presenters:
• Professor Kumudu Wijewardena, Sri Lanka
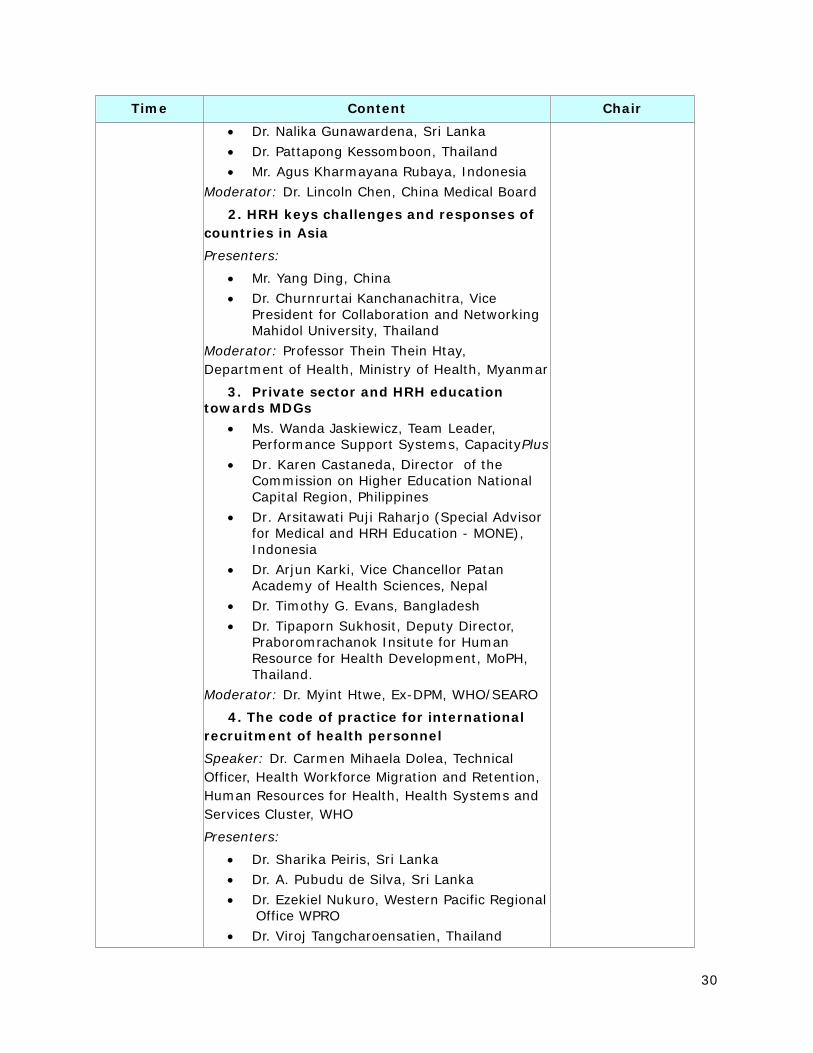
30
Time Content Chair • Dr. Nalika Gunawardena, Sri Lanka • Dr. Pattapong Kessomboon, Thailand • Mr. Agus Kharmayana Rubaya, Indonesia
Moderator: Dr. Lincoln Chen, China Medical Board
2. HRH keys challenges and responses of countries in Asia Presenters:
• Mr. Yang Ding, China • Dr. Churnrurtai Kanchanachitra, Vice
President for Collaboration and Networking Mahidol University, Thailand
Moderator: Professor Thein Thein Htay, Department of Health, Ministry of Health, Myanmar
3. Private sector and HRH education towards MDGs
• Ms. Wanda Jaskiewicz, Team Leader, Performance Support Systems, CapacityPlus
• Dr. Karen Castaneda, Director of the Commission on Higher Education National Capital Region, Philippines
• Dr. Arsitawati Puji Raharjo (Special Advisor for Medical and HRH Education - MONE), Indonesia
• Dr. Arjun Karki, Vice Chancellor Patan Academy of Health Sciences, Nepal
• Dr. Timothy G. Evans, Bangladesh • Dr. Tipaporn Sukhosit, Deputy Director,
Praboromrachanok Insitute for Human Resource for Health Development, MoPH, Thailand.
Moderator: Dr. Myint Htwe, Ex-DPM, WHO/SEARO
4. The code of practice for international recruitment of health personnel Speaker: Dr. Carmen Mihaela Dolea, Technical Officer, Health Workforce Migration and Retention, Human Resources for Health, Health Systems and Services Cluster, WHO
Presenters:
• Dr. Sharika Peiris, Sri Lanka • Dr. A. Pubudu de Silva, Sri Lanka • Dr. Ezekiel Nukuro, Western Pacific Regional
Office WPRO • Dr. Viroj Tangcharoensatien, Thailand
31
Time Content Chair Moderator: Dr. Viroj Tangcharoensatien, Director, International Health Policy Program (IHPP)
1230 – 1330 Lunch
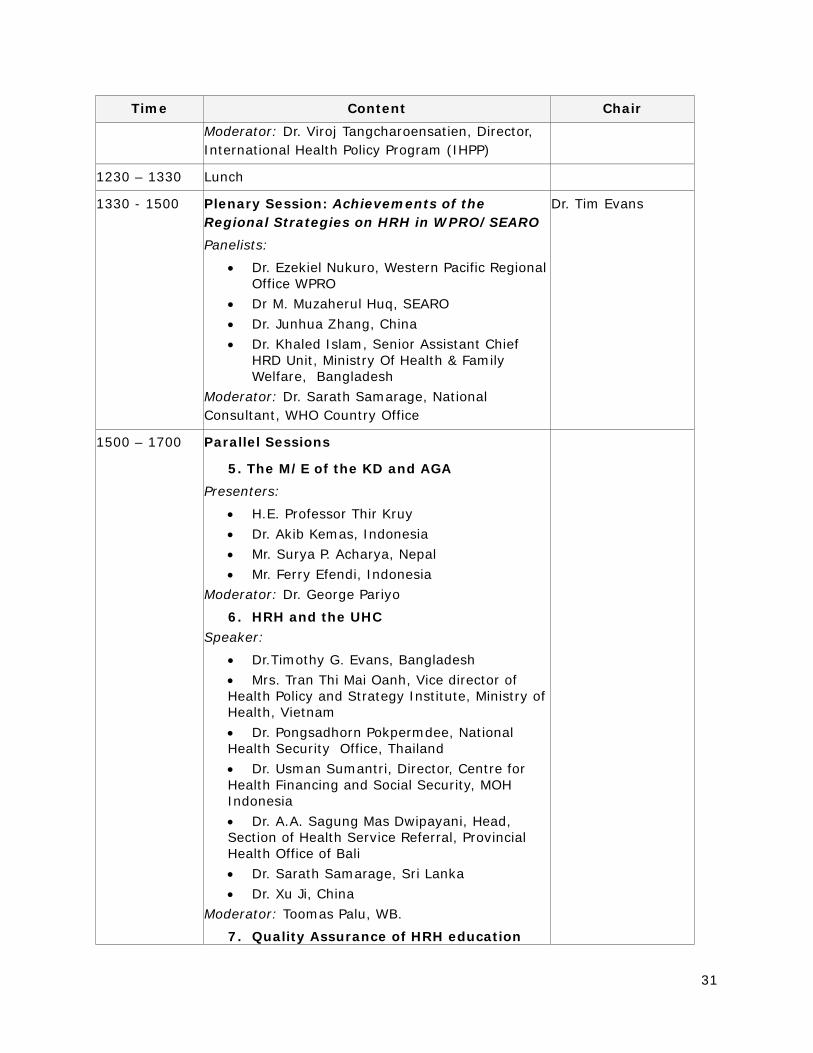
1330 - 1500 Plenary Session: Achievements of the Regional Strategies on HRH in WPRO/SEARO Panelists:
• Dr. Ezekiel Nukuro, Western Pacific Regional Office WPRO
• Dr M. Muzaherul Huq, SEARO • Dr. Junhua Zhang, China • Dr. Khaled Islam, Senior Assistant Chief
HRD Unit, Ministry Of Health & Family Welfare, Bangladesh
Moderator: Dr. Sarath Samarage, National Consultant, WHO Country Office
Dr. Tim Evans
1500 – 1700 Parallel Sessions
5. The M/E of the KD and AGA Presenters:
• H.E. Professor Thir Kruy • Dr. Akib Kemas, Indonesia • Mr. Surya P. Acharya, Nepal • Mr. Ferry Efendi, Indonesia
Moderator: Dr. George Pariyo
6. HRH and the UHC Speaker:
• Dr.Timothy G. Evans, Bangladesh • Mrs. Tran Thi Mai Oanh, Vice director of Health Policy and Strategy Institute, Ministry of Health, Vietnam • Dr. Pongsadhorn Pokpermdee, National Health Security Office, Thailand • Dr. Usman Sumantri, Director, Centre for Health Financing and Social Security, MOH Indonesia • Dr. A.A. Sagung Mas Dwipayani, Head, Section of Health Service Referral, Provincial Health Office of Bali • Dr. Sarath Samarage, Sri Lanka • Dr. Xu Ji, China
Moderator: Toomas Palu, WB.
7. Quality Assurance of HRH education
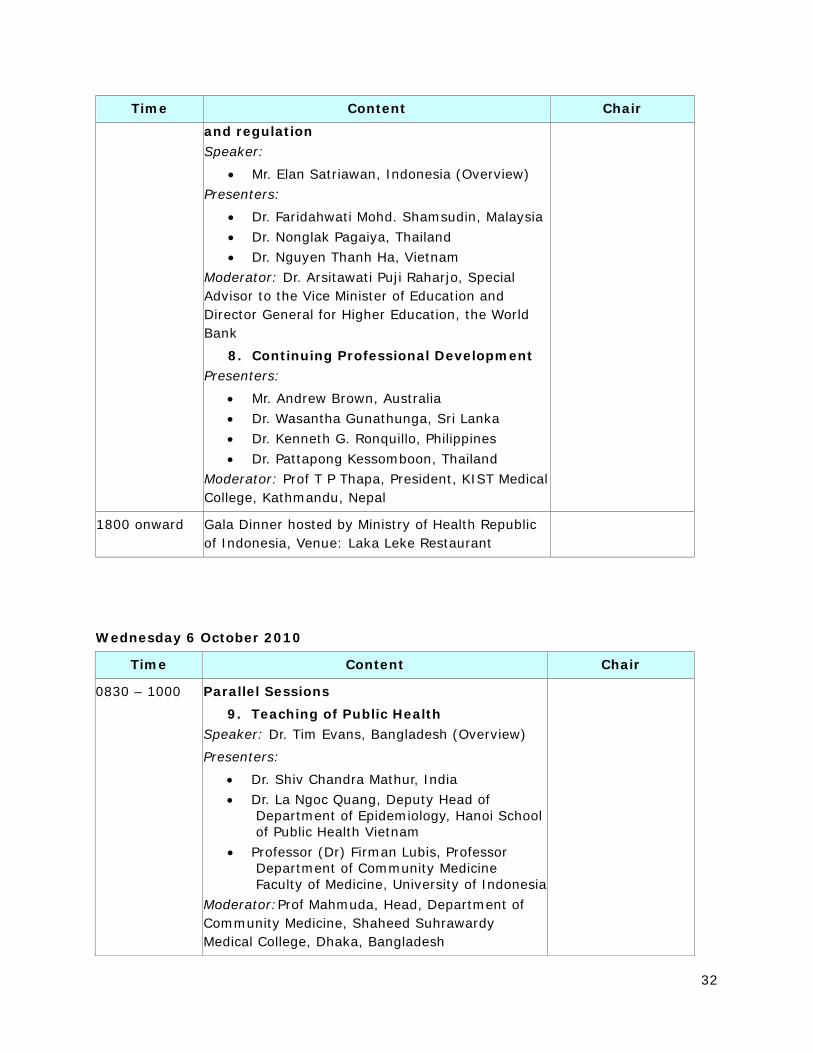
32
Time Content Chair and regulation Speaker:
• Mr. Elan Satriawan, Indonesia (Overview) Presenters:
• Dr. Faridahwati Mohd. Shamsudin, Malaysia • Dr. Nonglak Pagaiya, Thailand • Dr. Nguyen Thanh Ha, Vietnam
Moderator: Dr. Arsitawati Puji Raharjo, Special Advisor to the Vice Minister of Education and Director General for Higher Education, the World Bank
8. Continuing Professional Development Presenters:
• Mr. Andrew Brown, Australia • Dr. Wasantha Gunathunga, Sri Lanka • Dr. Kenneth G. Ronquillo, Philippines • Dr. Pattapong Kessomboon, Thailand
Moderator: Prof T P Thapa, President, KIST Medical College, Kathmandu, Nepal
1800 onward Gala Dinner hosted by Ministry of Health Republic of Indonesia, Venue: Laka Leke Restaurant
Wednesday 6 October 2010
Time Content Chair
0830 – 1000 Parallel Sessions 9. Teaching of Public Health
Speaker: Dr. Tim Evans, Bangladesh (Overview)
Presenters:
• Dr. Shiv Chandra Mathur, India • Dr. La Ngoc Quang, Deputy Head of
Department of Epidemiology, Hanoi School of Public Health Vietnam
• Professor (Dr) Firman Lubis, Professor Department of Community Medicine Faculty of Medicine, University of Indonesia
Moderator:Prof Mahmuda, Head, Department of Community Medicine, Shaheed Suhrawardy Medical College, Dhaka, Bangladesh
33
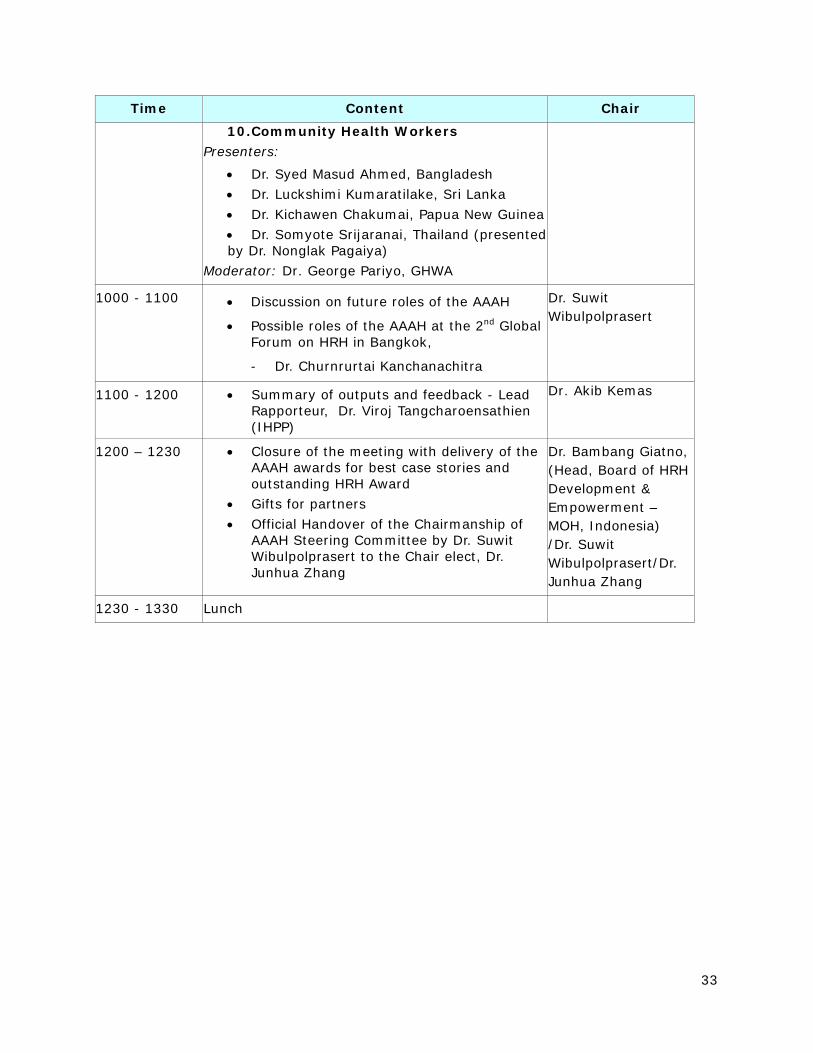
Time Content Chair 10. Community Health Workers
Presenters:
• Dr. Syed Masud Ahmed, Bangladesh • Dr. Luckshimi Kumaratilake, Sri Lanka • Dr. Kichawen Chakumai, Papua New Guinea • Dr. Somyote Srijaranai, Thailand (presented by Dr. Nonglak Pagaiya)
Moderator: Dr. George Pariyo, GHWA
1000 - 1100 • Discussion on future roles of the AAAH
• Possible roles of the AAAH at the 2nd Global Forum on HRH in Bangkok,
- Dr. Churnrurtai Kanchanachitra
Dr. Suwit Wibulpolprasert
1100 - 1200 • Summary of outputs and feedback - Lead Rapporteur, Dr. Viroj Tangcharoensathien (IHPP)
Dr. Akib Kemas
1200 – 1230 • Closure of the meeting with delivery of the AAAH awards for best case stories and outstanding HRH Award
• Gifts for partners • Official Handover of the Chairmanship of
AAAH Steering Committee by Dr. Suwit Wibulpolprasert to the Chair elect, Dr. Junhua Zhang
Dr. Bambang Giatno, (Head, Board of HRH Development & Empowerment – MOH, Indonesia) /Dr. Suwit Wibulpolprasert/Dr. Junhua Zhang
1230 - 1330 Lunch
34
Annex 2: Rapporteur Team
Expected deliverables from Session Rapporteur As of 3 October 2010
Summary major findings from each of the session in the Conference, not more than 500 words, reflecting the following topics:
o Key messages from the presentations by speakers, panellists
o Major issues or problems being discussed by participants
o Conclusion
o Recommendations
Please report in word document and send electronic file to the lead Rapporteur [Viroj Tangcharoensathien] at [email protected]
• For short address, key note address, and plenary session 1 by Monday 4 October 1700 hr.
• For plenary session 2 and 3 and Parallel sessions 1-4 and 5-8 by Tuesday 5 October 1800 hr.
• For Parallel sessions 9-10, by Wednesday 6 October 1030 hr.
Please kindly save in word file 2003 using the name as followed: Parallel 2.doc or plenary 3.doc
The lead Rapporteur will synthesize inputs from session Rapporteur and report to the Conference on Wednesday 6 October 1130-1230 hr.
The voluntary contributions by all session Rapporteurs are significant, not only reflecting Regional solidarity and voluntarism, it forms the Conference proceeding. The proceeding will be posted on the AAAH website by end October 2010 and circulate to all participants.
AAAH secretariat recognizes and pays high tributes to your contributions.
35
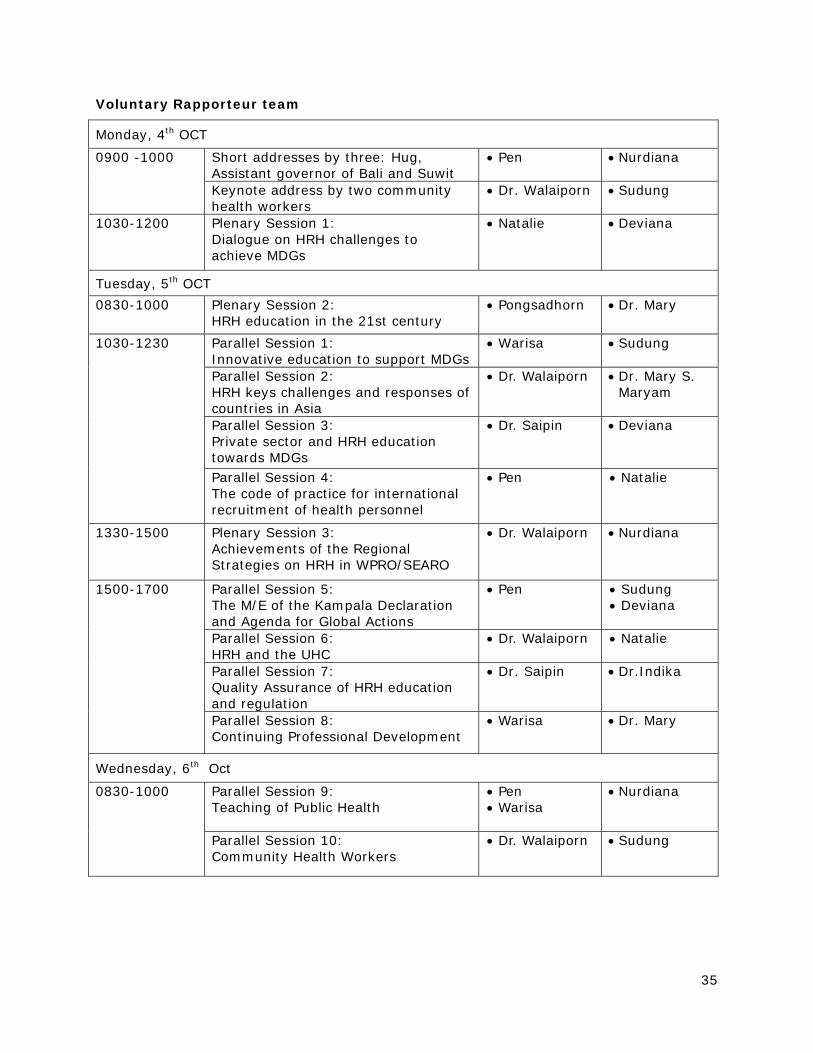
Voluntary Rapporteur team
Monday, 4th OCT
Short addresses by three: Hug, Assistant governor of Bali and Suwit
• Pen
• Nurdiana
0900 -1000
Keynote address by two community health workers
• Dr. Walaiporn • Sudung
1030-1200 Plenary Session 1: Dialogue on HRH challenges to achieve MDGs
• Natalie • Deviana
Tuesday, 5th OCT 0830-1000 Plenary Session 2:
HRH education in the 21st century • Pongsadhorn
• Dr. Mary
Parallel Session 1: Innovative education to support MDGs
• Warisa
• Sudung
Parallel Session 2: HRH keys challenges and responses of countries in Asia
• Dr. Walaiporn
• Dr. Mary S. Maryam
Parallel Session 3: Private sector and HRH education towards MDGs
• Dr. Saipin • Deviana
1030-1230
Parallel Session 4: The code of practice for international recruitment of health personnel
• Pen
• Natalie
1330-1500 Plenary Session 3: Achievements of the Regional Strategies on HRH in WPRO/SEARO
• Dr. Walaiporn
• Nurdiana
Parallel Session 5: The M/E of the Kampala Declaration and Agenda for Global Actions
• Pen
• Sudung • Deviana
Parallel Session 6: HRH and the UHC
• Dr. Walaiporn • Natalie
Parallel Session 7: Quality Assurance of HRH education and regulation
• Dr. Saipin
• Dr.Indika
1500-1700
Parallel Session 8: Continuing Professional Development
• Warisa
• Dr. Mary
Wednesday, 6th Oct
Parallel Session 9: Teaching of Public Health
• Pen • Warisa
• Nurdiana
0830-1000
Parallel Session 10: Community Health Workers
• Dr. Walaiporn
• Sudung
36
Template of session Rapporteur report Short addresses or
Key note or
plenary session X or
Parallel session Y
Date_____________
Chair ______________
Moderator________________
Speakers______________
Panellist __________________
Rapporteur team members _______________
Key messages from the presentations by speakers, panellists
Major issues or problems being discussed by participants
Conclusions
Recommendations

37
Annex 3: Summary of the sessions
Plenary Session I Dialogue on HRH challenges to achieve MDGs Date October 4, 2010 Chair Dr. Junhua Zhang –China Moderator Dr. Pongpisut Jongudomsuk—Thailand Panellists
1. Dr. Carmen Mihaela Dolea –WHO 2. Dr. Toomas Palu – World Bank 3. Ms. Nina Sardjunani- Indonesia 4. Prof. Thein Thein Htay –Myanmar
Rapporteur team members: Deviana, Natalie Key messages from the panellists The session focuses on how to retain health personnel, financial and non-financial incentives, how to motivate and how to educate them and retain them to provide health services in rural areas. It can be observed that there is a basic correlation between higher health personnel/capita and improved health outcomes i.e. lower MMR and IMR. However, globally, there is a critical global shortage using a benchmark of 2.28 doctors, nurses and midwives per 1,000 populations; there are 57 countries in critical shortage of healthcare personnel. The central question is what kind of health professionals are most needed to be produced to achieve MDGs in 2015? Major issues discussed by the panellists What kind of health professionals are most needed to achieve MDGs—doctor versus nurses and paramedics, Given the limited resources in low income countries, what is the trade-off between quantity and productivity of health workforce? What reforms in other sectors that may have impact on health workforce policies?
38
Conclusions Panellists agreed that, given limited resources in low income countries, priority should be given to equitable allocation of current HRH instead of produce more. Once mobilized to primary healthcare, incentive system, financial and non-financial for rural retention should be well in place. To achieve efficiency and effectiveness, appropriate manpower-mix and skills-mix are important policy issues. Health need assessment and the context of health systems determine balance in health workforce mix and skill-mix. Not only producing more, distribution of health workforce to serve the majority population is essential for MDG achievement. Reform in other sector has impact on health workforce, for example, civil service and public sector reforms may have either positive and negative impact on health workforce. Although most countries in Asia Pacific are progressing well to achieve MDG targets, inequity gaps associated with low level of human resources and service provision are major MDG challenges. Recommendations • More flexible recruitment structure of health personnel such as through contracting
basis. • Decentralization result in more responsiveness to people health needs, but government
should prevent fragmentation and ensure equalization of resource to poorer localities. • Health workforce policy is affected by other sectoral policies in particular civil service
reform. Appropriate incentives system is important in human resource management in light of the interaction between public and private health sectors.
39
Plenary Session II HRH education in the 21st century Date 5th October 2010
Moderator Dr.Toomus Palu
Speakers; Professor Fely Marilyn Lorenzo, Philippines
Dr. Arjun Karki, Nepal
Dr M. Muzaherul Huq, Regional Office for South-East Asia, WHO
Dr. Vicharn Panich, Thailand
Rapporteur team members; Warisa and Mary
Key messages from the presentations by panellists
Dr.Chen has point out that though MDGs give a focus, emphasize the grassroots community health workers. MDGs are misleading for health as they are too focused, too short term – only five years until 2015. Health is much longer and much more comprehensive process than the MDGs. However, care is now fragmented rather than continuous. Hospital rather than community based.
Profession is also facing ethical challenges, corruption and lack of leadership. There is maldistribution of medical schools around the world; lack of school among poor countries. With this reason, poorer countries must rely much more on community health workers rather than other health professionals.
He believes that we will witness a third generation of reform: the first one was science based, the second generation was problem based and now it is the generation of systems based.
Finally, he suggests set of recommendations which include 1) competency based approach which can break out of professional silos, 2) local-global, 3) IT empowered, 4) education resources and 5) new professionalism.
Prof Marilyn shares experience from Philippines that we need to innovate and train teams of skill mixes workers that can work together in teams, train early enough tends to be socialized and can work together in a friendly manner.
Dr.Karki raises 3 main points. The first one is that the curriculum is still technocentric, focusing on sciences though we should educate students about social determinants of health. The second, we have to make the med schools socially accountable. The third is about potential value to create synergy between national health system and universities. Medical schools under Ministry of Education while health services are under MOH, this results in misalignment between the two forces.
Dr.Huq points out that while doctors come from good socioeconomic background, urban based communities. Four important questions are Who are we training, Where are we training them, Who are training them, and Are they quality trainers. If not, then don’t get proper training.
Dr.Vicharn; Complex and active system, always evolve. Thus, we need to understand change in the long term andbase understanding on the real context. AAAH should serve as research bank, link research questions that will provide understanding and how to address and achieve recommendations by Commission Report.
40
Major issues or problems being discussed by participants
As education for health personnel is issues between education and health, coordination between these two Ministries is a major problem in many countries. Thus, cooperation is important factor. In China, there is coordinating development of HRH requires health and education departments to jointly develop the rural health workforce plan.
Another point is relevancy of teaching to the real situation, for example, relevancy between professions, between education and community needs, education and the health systems.
Conclusions
Health systems and professions will change and need to respond responsibly to society. The priority should be given to improve knowledge base, mapping of what is actually happening.
41
Plenary Session 3 Achievements of the Regional Strategies on HRH in WPRO/SEARO Date October 5, 2010 Chair: Dr. Tim Evans Moderator: Dr. Sarath Samarage Panellists
1. Dr. Ezekiel Nukuro WHO WPR 2. Dr. Muzaherul Huq WHO SEAR 3. Dr. Junhua Zhang China 4. Dr. Khaled Islam Bangladesh
Rapporteur team members: Pen Keys: Resources, committed funding is important. Cohesiveness of sectoral and national policies Dr. Nukuro There are 8 member countries from WPRO as AAAH members Purpose, Objectives of Western Pacific Regional Strategy:
• Providing member states with policy options and guidance with which they may want to develop strategies and polices
• Regional strategies should not and cannot replace country specific strategies. • Strategy includes indicators for M/E
Achievements
• Reaffirmation of political and stakeholder commitment to HRH • Use of regional strategy as guide for national HRH policy and strategy development • Wide range of country initiatives and efforts to overcome health workforce challenges
Challenges
• Limited capacity for HR management • Lack of cohesiveness of sectoral and national policies and strategies • Low levels of funding for the health sector and for HRH in particular • Quantity, quality, distribution of health workforce
Way forward:
• Facilitating implementation • Focused country actions • Alignment with renewal of PHC reforms and health system strengthening
Dr. Huq Challenges in SEA:
• Imbalance of production • Maldistribution
42
• Improper management • Inadequate functioning of HRH regulatory bodies • Access, migration and retention
Priority activities:
• Implementing the WHO Global Code of Practice on international recruitment of health personnel
• Networking and partnership building Achievements
• Guidelines on accreditation of medical schools • Regional guidelines for CPD/CME continued professional development, continued
medical education • Module of Teaching of Ethics to undergraduates • Networking and partnerships collaboration
Conclusion and way forward:
• WHO CCs and other partners including AAAH are working in collaboration and coordination in country capacity building on HRH.
• Asia Pacific Observatory on Health System and Policy –make information available to everyone, namely information on HS and HRH.
Dr. Junhua Zhang:
• MDGs and achievements in China • Medical graduates should attend training programs in hospitals for another 3-5 years
Dr. Khaled
• Received the SEARO guidelines in 2007. Countries in region are faced with the same challenges and issues.
• Policy formulation, adoption • In 2008 – followed regional guidelines –national health policy, national population
policy • Bangladesh doing good, particularly on MDGs 4 and 5.
Dr. Suwit – question to the Chair
• So many WHO global /regional strategies, has WHO ever assessed achievement of these strategies?
• Tim – fundamental question related to institutional mechanisms of WHO.
43
Parallel session 1 Innovative education to support MDGs Date 5th October 2010 Moderator: Dr.Lincoln Chen Speakers; Professor Kumudu Wijewardena, Sri Lanka
Dr. Nalika Gunawardena, Sri Lanka Dr. Pattapong Kessomboon, Thailand Mr. Agus Kharmayana Rubaya, Indonesia
Rapporteur team members; Sudung and Warisa Panichkriangkrai Key messages from the presentations by speakers Professor Kumudu has addressed the current knowledge gap concerning provider’s roles and relationships in the area of adolescent sexual and reproductive health care in Sri Lanka. Though, there are multi-sectoral interventions from both education and health side, there is a lack of a coordinated approach to the provision of services. Recommendations are that there is a need for a sustained multi sectoral approach in ASRH with policy directives and financial commitment that are woven into the action plans of the ministries of health, education and youth affairs. Dr. Nalika show the result that curricula of most medical faculties in Sri Lanka were not adequately ‘gender sensitive’ in terms of content teaching/ learning strategies, timing of inputs, duration allocated. In addition, few faculties aimed at developing skills to promote gender equality at work. Dr. Pattapong introduces a solution to increase the number of family doctors in rural areas, there is three year in-service training program in Family Medicine in Khon kaen province which started in 2009. This program got support from the top which includes budget for tuition and travel fee for trainees. This program can attract more doctors than the past. Mr. Agus did a literature review to compile the current issues related to the education of human resources in public health. He found that two of important health professions produced by Polytechnic of Health: Midwife and Sanitarian contribute to improve maternal health, reduce of child mortality as well as increase women empowerment. Major issues or problems being discussed by participants
• Counselling (Education )(Health) • Peer education • Competencies of health workers • Curriculum of most medical faculties • Concepts and principles of Family Medicine

44
Conclusions The 4 I’s has been raised; innovation in multidimensional (as referred by Dr.Kumudu), intervention of curricula in gender sensitivity and equity of the faculty (by Dr.Nalika), inventory of public health education (by Mr.Agus), and inequalities in family health coverage for rural areas (by Dr.Pattapong).
Recommendations 1. A sustained multi sectoral approach in ASRH is needed. 2. A comprehensive analyses of curricula of all health professionals is needed in all
countries in the region 3. The principles and values of Family Medicine are unique and can help equip trainees
with new concepts and lead to better practice behaviors. 4. The Midwife and Sanitarian are contributed to the improvement of maternal health,
reduction of child mortality and increasing women empowerment, and combating environmental-based diseases as the major causes of childhood mortality and providing safe water and basic sanitation facility.
45
Parallel Session 2 HRH challenges and responses of countries in Asia Date 5 October 2010, 10.30-12.30
Moderator: Professor Thein Thein Htay, Myanmar
Presenters:
1. Mr. Yang Ding, China 2. Dr Sita Naik, India 3. Dr. Churnrurtai Kanchanachitra, Thailand
Rapporteur team: Walaiporn and Mary
Participants: 23
Key messages from the presentations and discussion by speakers and participants
China (Power Point presentation)
• China had achieved MDG on reducing chid mortality by 2007 (18.1/1,000) as well as MMR
• HRH challenges and responses:
1. Shortage and mal-distribution local recruitment and local support, at least one doctor in one township,
2. Quality of health worker training enhancement (regulation of the training course and certification), upgrading of professional qualification, training for urban community health centre to deal with NCD
3. Weak governance on HRH management skill improvement
4. Lack of senior level health professionals training and promotion the senior level
• Further development: National Medium to long term HRH development framework for 2010-2020 will be issued in 2010. Now is the process of working on this framework.
India (no power point)
• Challenges are similar to other countries. Shortage, if go with normal rate of production; India cannot solve the problem for both medical doctor and nurse. Other problems are
o Government structure: Large (like China), structure of the government due to large and divided central level introduced the guideline and the local level has to apply, less efficient government, less effectiveness in implementing program
o Huge problems of life style change due to multi-factors e.g. zero pop growth, rapid economic growth, huge migration between urban and rural (40-50% live in urban) and then lead to urban poor
• Some responses from government to solve the HRH problems
o Next few month regulations on “hospital accreditation” otherwise health insurance company won’t reimburse medical bill to the hospital
46
o Modification of training course for three year for bachelor program on medical services.
o Reform on healthcare financing will improve health care service delivery to patients and indirectly solve HRH
Pregnant women will get financial subsidies for transportation when travel to healthcare provider to get ANC – demand side financing
Targeting the poor – premium is paid 70% by local government and 30% by state government. Provider payment mechanism is ‘deduction from the health card’. BPL program
• There are number of intentions and policy intervention to solve the problems but effective policy implementation is the main challenges. One main problem is ‘governance’. Monitoring and evaluation are essential tools to improve the intervention implementation.
Presentation by Dr Churnrurthai (Power point presentation)
• This presentation is on data of South East Asia Region – 11 countries on two main sections:- within country problem on shortage and mal-distribution and international trade and health
• Shortage and mal-distribution
o Main problems are similar – shortage and mal-distribution. HRH problems on shortage is directly related to U5MR
o Main factors leading to shortage are low production capacity e.g. Lao, Cambodia and low employment capacity (only half of nursed graduated in Indo employed).
o Mal-distribution of doctor is more serious than nurse, except in VN. Factor leading to mal-distribution: distribution of health infrastructure, poor working and living conditions and opportunities to earn extra income in urban area
• International threats:
o Mode 2: providing services. International patients seek health care services. Some factors are (1) high quality medical services (JCI accredited hospitals 16 in Singapore, 11 in Thailand, 6 in Malaysia and 3 in Philippines and one in Indonesia and one in VN), (2) long queue and supply shortage in home countries and (3) lower cost for foreign patients
o Mode 4: doctors and nurses working in OECD countries. Philippine nurses mainly go to UK, USA, South Arabia
• Example of responses to the challenges
o Shortage: (1) increase production quickly to compensate for the shortages but may compromise quality, (2) upgraded assistant doctors to be doctor (VN), (3) rotate high qualified staff to work in rural area (VN), (3) increase role of private sector in production of HRH (Philippines and Indo) for which must have effective regulation mechanism and (4) applying skill-mix, professional mix and task shifting approaches. Points to consideration are (a) quality vs quantity trade-off, especially in resource poor setting scale up lower cadres may need to take into consideration – shorter time and lower investment and (b) employment opportunity for newly graduated.
47
o Mal-distribution: (1) rural recruitment and hometown placement, (2) compulsory placement and (3) financial and non-financial incentive. Point of consideration are comprehensive strategies, effective implementation and monitoring and evaluation on the impact of those interventions
o Policy on trade in health services:
Policy to promote medical hub to encourage more patients to seek health care
Impact on health care to the local people in term of require more HRH especially super-specialists
Policy to promote export of HRH change from individual to bilateral and multilateral
Studies are needed to assess on impact on health care to the local people
• Summary and recommendations
o Challenges are similar to other countries in terms of shortage and mal-distribution
o Uniqueness is in the active engagement in trade in health services
o To cope with shortages in resource poor countries, scale up of lower cadres and apply task shifting in a possible way
o Appropriate training is necessary to ensure quality
o Balance between trade and health has to take into account when develop policy on medical hub or export of HRH and the coordination among several Ministers e.g. Health, Foreign, Commerce
Conclusions
1. HRH problems are there and not easy to solve in short period due to its complexity and dynamic.
2. The chronic problems still remain in many countries and at the same time new threats on trade and globalization intrude quickly. There are several factors involved of HRH problems:-not only in health sector but also out side health sector e.g. government structure, demography, living condition, trade in bad (e.g. tobacco and alcohol and regional trade agreements in favour of trade rather than health of the population) and globalization.
3. In many countries; there are policy intentions and various interventions to deal with the chronic problems on HRH and new challenges like trade and globalization. Several lessons can be drawn from country experiences.
4. Effective policy implementation on the comprehensive interventions is needed.
5. Monitoring & evaluation of those interventions implementation are necessary to feed back the policy and to improve the solution. Studies and researches are also needed in HRH issues.
48
Parallel session 3 Private sector and HRH education towards MDGs Date October 5th, 2010 (10.30-12.30)
Moderator Dr. Myint Htwe, WHO/SEARO
Speakers
• Ms. Wanda Jaskiewicz, Team Leader, Performance Support Systems, CapacityPlus
• Dr. Karen Castaneda, Director of the Commission on Higher Education National Capital Region, Philippines
• Dr. Arsitawati Puji Raharjo, Special Advisor for Medical and HRH Education - MONE, Indonesia
• Dr. Arjun Karki, Vice Chancellor Patan Academy of Health Sciences, Nepal
• Dr. Timothy G. Evans, Bangladesh
• Dr. Tipaporn Sukhosit, Deputy Director, Praboromrachanok Insitute for Human Resource for Health Development, MoPH, Thailand.
Rapporteur team members
• Dr. Saipin Hathirat, Thailand
Key messages from the presentations by speakers
• Ms. Wanda, CapacityPlus
Show the Joint-collaboration of world bank, health Africa initiative by capacity plus project in private contribute to HRH production
In Africa, private sector heath care is 50% of formal health care delivery and has role as sponsor institutions and private donors
Case study from Africa on semi-structured interviews with senior key officials to document the role in increasing capacity of HWs, identify characteristics of successful + quality private institution, challenging scaling up educational model
8-10 case studies from 4-6 countries would be produced soon by Capacity Plus on the role of private education institutes.
• Dr. Karen, Philippines
Agency of higher education has roles in regulation whole education institutes, 88% private schools.
Problem: Proliferation of higher education, too many franchise schools, producing too many nurses with no jobs, underproducing other HCW areas, not enough incentive to send to rural and local hospital
Control by publicizing the ranking the qualified institute, only 1/3 of institute pass the licencing national exam
49
• Dr. Arsitawati, Indonesia
Indonesia education in health: private growth rapidly 35 times of public institutes. Growth of midwife education is higher
Number of health HEI lecturers [Faculty development] still need to be empowered. Public university lecturer decrease every year, private is increasing. [tapping limited faculty resources from public to private-jeopardize quality of public training institutes]
Growth of disparity between poor and rich student, MD come from rich one
Problems: need new regulation and supervision, equity on accessibility for high education; accreditation system to find the minimal competence of each HCP, how competence mix with population demand; certification system; Continuous professional development – need to strengthen the profession organization; inter-professional collaboration; public – private partnership sharing learning resources
• Dr. Arjun, Nepal
Human resources in health: critical shortage in Nepal with private challenges.
Private challenges:
1. HRH policy in national level is in need that what should be the basic need of people health.
2. No regulatory mechanism, such as tuition fee
3. Most medical schools primary focus to attract med student to go abroad, not local people
• Dr. Timothy, Bangladesh
Not to see as black and white of public or private site in HRH production; they’re closely link
Positive side from various countries shows massive growth in demand of HRH production both local and global need
Negative side “degree mills” to produce massive numbers of HCW in very cheap but low quality. Students receive very shallow knowledge and get certification although low standard in career experience.
Have to balance positive and negative sides of private sector
Research for comprehensive assessment HRH production is in need
Higher education is neglect to invest by the government although it’s fundamental for HRH production
Need to develop tool, evaluation criteria for both private/public audit mechanism.
50
Need national accreditation standard to confront the cross-border global market need for HRH
• Dr. Tipaporn, Thailand
Thailand confronts many challenging situations: rapid chronic and non-communicable diseases, economic growth, universal coverage, and huge influx of international patients due to medical hub policy
Clarify the data on distribution of HRH stock of Thailand: MD, dentist, nurse, pharmacist
In each professional institutes, private university has limited contribution to HRH production such only 5% in medical doctors, 13% for dentist, 25% for pharmacist and nurses.
The regulatory mechanism in national level and professional council is by law. However only nursing council can forces to have 5-year re-licensing of nurse.
We need to see private sector as a friend rather than a foe. They can reduce government invest in HRH production and increase number of HRH in the health system.
Negative impact is inequity in education opportunity gap, widening gap of rural/urban distribution, commercialize of health care system, create brain-drain situation
Convert private production to be friend.
Major issues or problems being discussed by participants
• Because of under-investment of public HRH production, private can be resource, not only problem
• We need to project what kind of HRH we need in future, rather than let the market drives the demand of HRH production
• Growth of private sectors shows how finance of public HRH production is under invested.
• There are differences in market HRH production, such as south Asia focus on MD production, Philippines focuses on nurse production, Indonesia focus on midwifery production. These may show market-driven differently in each country.
• Need private contribution in HRH production in health system by using higher level of policy such as government not to support, (not to kill) private to involve in HRH production. Need strong regulatory mechanism to close down the poor-quality professional schools. Then these can make good private practice to serve the country.
Conclusions
51
• Public should learn from private how they become successful and have good operational management
• Regulate policy to control private sector.
• Set guideline to control proliferative growth of private sectors. And need the compulsory time to work in rural areas for both public and private graduates
• Need consensus and regulatory body to control institute function in HRH education. Not just public or private is needed to follow.
• Financing professional education is needed to be considered. Otherwise students have to carry debt in tuition fee and expensive professional education. Then impacts on their freedom of career choice.
• In-service education is over-looked.
Recommendations
• Need to assess advantages and disadvantages of private sector contribution to HRH production
• Need regulatory mechanism/body for quality assurance and make use of private sector in contribution to population need
• Each professional council needs to regulate quality of their graduates
• Each country need to make the national policy to regulate and quality control in private sector contribution to HRH production
• In-service training need to be considered more to order to achieve MDGs
• More transparent criteria for accreditation is in need
52
Parallel session 4 WHO Global Code of Practice on international recruitment of health personnel (about 20 participants) Date October 5, 2010 Moderator: Viroj Tangcharoensathien Panellists
5. Dr. Carmen Mihaela Dolea, WHO HQ 6. Dr. Sharika Peiris, Sri Lanka 7. Dr. A Pubudu de Silva, Sri Lanka 8. Dr. Ezekiel Nukoro, WHO WPRO 9. Dr. Viroj Tangcharoensathien
Rapporteur team members: Pen and Natalie Carmen • Evidence shows a huge out-migration from some of African and Caribbean as measured
by expatriation rate for nurses and doctors in OECD countries. Also internal rural urban migrations posted serious problems on health systems in poor countries and rural areas.
• The WHO Global Code of practice on international recruitment of health personnel intends to address the backdrop of critical shortages of health workers through ethical management of the international migration.
• The code is an outcome of systematic consultations with member states as well as deliberation in various Regional Committee meetings in 2009; prior to the final deliberations in WHA63 in May 2010. Altogether there are 10 Articles in the Code and preamble statements.
• The WHO Global Code is voluntary in nature and provides ethical principles applicable to the international recruitment of health personnel, ensuring rights to migrate and obligations the country health systems.
• Five main implementation strategies were proposed, including communication and advocacy, development of institutional mechanisms, partnerships, resource mobilization and support at regional and country level.
• The WHA Resolution request the WHO to rapidly develop, in consultation with Member States, guidelines for minimum data set, information exchange and reporting on the implementation of the WHO Global Code. This is an ongoing process and participants voice concern that this process should be quickly finalized.
Dr. Sharika Sri Lanka took lead in developing migration friendly health policies at WHA. To gain remittance, the government policy will support migration of skill labourers which also cover skill health workforce to boost the Sri Lankan economy. A number of challenges were highlighted in Sri Lanka including rural-urban and outbound migration, mal-distribution, inappropriate skill mix, ageing of the health workers and needs for post-conflicts health systems development. There was a large provincial inequity gap in the distributions of medical officers, nurses and specialists, measured by professional to population ratio.
53
Data cannot capture accurate figures on various profiles of outbound and internal migration. However, in the MOH Post-doctoral training programme sponsored by the government, 11.2% loss to the country of training institutes, a majority returned, 88% To solve intra-country and international migration, a national steering committee on migration health was established with 13 line ministries involved, this is supported by Migration task force and Migration health secretariat. Dr. Pubudu Temporary migration of health workers for continued training is a must, but need to go back to their countries. Every post grad who goes to train abroad must sign a bond to secure coming back to SL. Saw an increase in number of migration to train, however all bonds were paid back as if do not come back on time, legal action is taken. SL promotes temporary migration for training is seen as “knowledge economy” Other incentives are given – provide facilities for healthcare workers, economic gains include opportunity to engage in unlimited private practice after hours, higher salary, etc. to keep them in SL. Improved living conditions are provided. Opportunity to get better schooling for children. Dr. Nukuro Pacific Code of Practice – Rational and aspects of Pac Code:
• See a loss of highly trained workers to Aus, NZ. Issue is critical as may lose only anesthetist on the island.
• There was a Commonwealth Code of Practice, which the Pac Islands countries did not accept. Needed own Pac Code.
Guiding principles
• Achieving the correct balance between the rights, obligations and expectations of all parties
• Respecting the principles of transparency, fairness and mutuality of benefit. Improvements from previous codes – need for M/E, support for source countries bonding/obligations Countries need to train workers that are unlikely to leave and to meet needs. Pacific code provides information about the provisions of the Code including some case examples Links with WHO Code
• Similarity in rationale • Pacific Code – included among codes examined when developing WHO global code • WHO code is bigger than the Pacific code, more comprehensive and unanimously
adopted by members. Only second code to be adopted. Lessons learned
54
• Advocacy about the code. Found that the dissemination has not gone beyond the Ministry of Health and even in MOH, some senior managers did not know about it.
• No longer see active recruitment from outside/other countries following passing of the Code.
• Recruitment is personal, people apply for jobs abroad. • Code only covers formal recruitment process and not the personal process. • No incentives to be tied to the Code. • M/E is a long standing problem even in small populations. Difficult to track people
when they leave. Challenges:
• No concrete implementation plan with resource mobilization • No buy-in from stakeholders • Global labor markets – people will move
Way forward: • Code is not the magic bullet • Trainings relevance to country/local needs, kinds of workers that are more likely to
be retained • Have a referral system • What happens on the ground matters • Should be a level playing field for all partners
Dr. Viroj Draw lessons from the negotiation of the Code in WHA63 in May 2010. He draws lessons learned from history of soft law – the case of the 1981 Code of marketing breast milk substitutes, at that time USA has objection to the Code while three member states abstained. Codes are not legally binding, but a soft law. Negotiating partners can be classified into three groups:
• Source countries who lose their well trained health workforce • Destination countries – US, UK, NZ, Switzerland, France, Spain who gained from
international migration • No gain-no loss countries – support legitimate position of losers: Thailand, Brazil.
Do we need a code? – Everyone “yes”, this is to stimulate the spirit of compromise and moving towards an adoption of the Code. Data capturing is important at the destination countries for which source countries cannot adequately capture. The drafting group agreed to have a “good enough” code rather than “the best” Code which will be ignored and violated at the implementation phase. Major achievement – consensus around contentious issue, unanimously adopted, second code adopted by WHO, most challenging on implementation. Challenges – foreseeable violation of code by private recruiters Discussions 1. What are the effective processes to start implementation of the Code in your country?
• Philippines has effective management of migration well before the Code was adopted. Some best practices – one is multi-agency approach towards migration management. HRH network headed by DOH in collaboration with agencies responsible for migration. Department of Foreign Affairs and Budget and Management also involved.
• The Government actively pursuit towards bilateral agreements with destination countries. Used commonwealth code as a basis of the bilateral agreements.
55
• Looking at work conditions, win-win situations, investing in health systems, health education, health facilities
• Critical is the network with not only the government agencies but engaging the private sector especially the recruiters. All recruiters are licensed/registered by Trade Ministry
• Looking at migration management – not just deployment and then migrate, but looking at the scope from production of health workforce to deployment and monitor what happens after that.
• Migration of health workers are trade issues, not just a health issue. Health workers seen as commodities, not seen as important health workers to beef-up the system in other countries. Presents a different approach and issues toward recruitment. How can trade negotiations be improved to ensure that health workers are not seen as a commodity but as part of the health systems.
2. What are the three critical success factors in implementation of this Code? Indonesia -commitment of all stakeholders, coordination and effective implementation. Dr. Tushara – move strongly and swiftly. Implementation plans will provide countries with adequate flexibility. Situation in each country is a little different and complex. 40% of doctors trained in Nepal are foreign student and returned to their home country after completion. Do we count this event as international migration? Need to analyze the real situation in each country, identify key problems specific to each country and then move forward in a way that is flexible. Barbara –does mutual recognition of curricula stimulate international migration of health workforce? Why is UK such a popular destination for doctors from Africa? It is the geo-proximity, recognition of curricula of many former British colonies in Africa with similar curricula. Dr. Nukuro –ANZ are investing in training institution in Pacific island countries such as medical school in Fiji. Providing aid to health systems strengthening is increasing. Good experiences on sharing of nurses among Pacific island countries. Carmen – recognition of qualification: facilitates migration but also stresses education, changing curricula towards destination countries. Timeline for guidelines – is quite long. Idea is to have more consultations with member countries. Dr. Nukuro: concerned about brain waste – recruited as nurses but then when they get to the destination, wind up doing something else. Mechanisms need to be in place to ensure that workers do what they were hired to do – ILO already provides protection for this. Summary • Good experience on time sharing from SL presentation, active management of
temporary migration. • Code is one of the many pillars, don’t totally rely on the Code. Retention must be
addressed through various ways, CCF facilitates a good national HRH plan and effective implementation is important.
• Migration will be in a more systematic and transparent manner embraced by the Code. • Engagement with stakeholder in the implementation of the Code is important and not
less than evidence and data capturing.

56
• Creating public awareness among stakeholder and recognition of the Code is the major entry point of implementation.
• WHO and partners are working on implementation of this, progress report is mandated in WHA2013.
57
Parallel Session 5 Monitoring and evaluation of the Kampala Declaration and Agenda for Global Actions Moderator: Dr. Georgo Pariyo, GHWA Case presentation: Mr. Ferry Efendi –Indonesia Panelists:
1. Dr. Akib Kemas -Indonesia, 2. Prof. Thir Kruy-Cambodia 3. Mr. Surya Acharya—Nepal,
Rapporteur team members: Pen Participants: 19
Moderator, George
Government plays key role in implementing the KD/AGA:
• Use of evidence is very important so we know what is being done is achieving results. • Scale up education and training. • Retaining an effective, responsive and equitably distributed health workforce. • Manage pressures of the international health workforce market and impact on migration. • Securing additional and more productive investment in the health workforce.
Key Points of presentations
Prof Thir Kruy: Cambodia progress of KD/AGA
Made great efforts to meet country needs
KD/AGA most relevant to Cambodia is scaling up health workers through education and training. Focus on education, deployment, staff retention and resource mobilization to address the shortage of staff at remote and rural areas.
Enabling factors: commitment from decision makers, clear policy and strategy framework of MOH, harmonization and alignment from stakeholders and partners for resource mobilization, monitoring and follow up.
Dr. Akib: Overcoming the health workforce crisis in Indonesia –
Indonesia have completed nearly all of the agenda except for No. 2, informed response based on evidence. Need strong commitment of stakeholders to overcome this problem.
Best practices are enabling factors – incentive scheme for contract doctors and midwives, scholarship program with bonding. There are strong commitment from MOH, MOF, MONE, MOIA, health education institutions and local governments. Sustained funding also helps.
58
Mr. Surya:
AGA 1 leadership – stakeholders involved in development, implementation and evaluation. Civil society will examine impact of program.
AGA 2 informed responses – stakeholders will scale up investment in capacity building, - need to do in Nepal
AGA 4 – Retention – various incentives. Nepal has problems in terms of this. Should incentives be given just for retention or linked to performance?
AGA 5 – international health workforce market – every country should monitor their health workforce.
Relevancy of KD/AGA in Nepal: all are important but need to prioritize agenda. Which do you choose? Important one or urgent one?
Enabling factors: National Health Policy of 1991 provided enabling environment in Nepal. Large number of private institutions (17) established to train health care professionals. Access to essential health care services was increased by establishing health posts in villages and had an extensive network of female community health volunteers. Professional associations, trade unions, academic and research institutions are in existence and their participation in the process is proposed. Gov’t of Nepal has stipulated the skill mix in the health workforce. Have evidence of scale up of education and training quickly and effectively.
Learned: initiations are there, but scattered and small in scale. Commitment from each level of leadership is a must. Other ministries need to be adequately involved. Bringing all stakeholders to one table generates much, including creating ownership, maintaining transparency.
Mr. Ferry
KD AGA 3 reviewed.
Case of Indonesia – district hospitals – most have four basic medical specialist services OB/GYN, internal med, surgery, and .. But on 71.8% have these in the country. The gap is getting higher. There is a shortage in nurses in district hospitals.
Scholarship program – long term program providing financial support to attend specialist education for doctors who are willing to serve all over Indonesia.

59
Key Challenges:
Cambodia – alignment of resources, leadership role is still weak in staff management, regulatory framework related to quality of profession and education is limited.
Indonesia – decentralization is a challenge. Districts must be aware and responsible for health personnel in their areas. Maintaining regular supervision can improve motivation of health personnel working in remote areas. Production of certain types of health workers especially some areas of med doctors are limited in certain regions. Leads to maldistribution.
Mr. Ferry: most provinces don’t have working groups to address the issues of shortages and other KD/AGA related issues.
Recommendations:
Cambodia: Plan to focus on KD/AGA 1 and 4 (build leadership and retain and equitably distributed health workforce) AAAH initiatives are key of success as can bring awareness to global trends and directions., exchange strengths and weaknesses.
Indonesia – strengthen M/E, improve HRH plan with evidence based, clear indicators and costed. Strengthen CCF mechanism. Institutionalize policies on international recruitment of HRH, incentive scheme, award system for HRH in relation to its performance, privileging of health workers with adequate training to provide necessary medical actions in remote areas.
Nepal: quality control, coordination and networking, insufficient competencies in providing services, narrow skill mix of the health workforce, retention. Way forward: - institutionalization of KD/AGA at country level, harmonization of agenda, planning of HRH by July 2011, next two years will be on implementation, monitoring, reporting and feedback, after that the HRH plan will be reviewed, updated and continue implementation.
Mr. Ferry: Need to conduct analysis of contribution of the program to achieve MDGs as well as the outcomes and impact of the program. Convene a high level committee of the MoH, MONE and others.
Establish a tracking system to monitor progress on HR programs. Support from donors for Gov’t commitment to taking direct action for securing financial needs. Accelerate production of traditional cadres.
Discussion:
Dr. Karki – incentive package for health workers in rural areas in Indo – what is this? Elaborate also on bonding for scholarships.
Who funds the incentives in Indonesia, and for how long?
Dr. Akib response: incentives include transportation from original school to the areas. Monthly incentive for med docs – 7.5 million rupiahs which is a 100% increase from normal salary if they go to rural areas. Bonding depends on the length of the scholarship, if start from first year and for all years, they are bonded for the same period.
60
Wanda: what methods were used to select the specific incentives used?
Nepal – 9 districts that are difficult to reach, compared public sector salary with private sector. Decided to give 1000 Nepali rupiah per night to doctors.
Indo – have financial and non-financial incentives. Transportration in rural areas – small motorbikes. Non-financial –priority is given to them that they will be hired as a government/civil employee which is under the local government.
• CHWs –purely volunteers or receive incentives? • M/E of progress – what are some of the challenges in terms of monitoring and
information systems on the workforce? Nepal – have been increasing reliability of information systems, in some areas still some duplication.
• Retention of staff in remote areas – after finishing contracts, doctors might go back to original areas. How are they retained?
• Are there any difficulties in linkages between central and local governments? Any constraints in strengthening health systems in one site over another site? Nepal – most power is still now decentralized, national system still working in transition to decentralization.
Cambodia – has policy to strengthen capacity and quality of training in all public and private universities. Have budget to give something to students who are from regional areas. Incentives provided to midwives – USD 10 per delivery case in order to improve services. Involve private sector in establishing regulatory framework. Projects to strengthen capacity of teaching staff.
George – Cambodia raised good point regarding the attempt to scale up training, there has been a mushrooming of private institutions. Need standards not only for the public but private institutions as well.
Ferry – decentralization is seen as creating opportunities for creating retention in remote areas. Local gov’t has authority to hire and recruit = good opportunity to get workers in the district. Another issue to be addressed is the HR information system – various data about the health workforce between central and local gov’t, need to harmonize.
Summary
Importance of ownership was highlighted by all. Monitoring, if not in place needs to be done. Incentives are keys. Cannot bring about long lasting change without regulatory support
61
Parallel session 6: HRH and the UHC Tuesday 5 October 2010, 15.00-17.00
Moderator: Toomas Palu, World Bank Speakers:
• Dr. Timothy G. Evans, Bangladesh • Mrs. Tran Thi Mai Oanh, Vietnam • Dr. Pongsadhorn Pokpermdee, Thailand • Dr. Usman Sumantri, Indonesia • Dr. A.A. Sagung Mas Dwipayani, Bali, Indonesia • Dr. Sarath Samarage, Sri Lanka • Dr. Xu Ji, China
Rapporteur team members Natalie and Walaiporn
Participants: 40 approximately
Key messages from the presentations and discussion by speakers and participants
Dr. Timothy G. Evans, Bangladesh
• Discussion on three dimensions of UHC
o Breadth: population coverage
o Depth: service coverage depends on quality of HRH and other health systems factors
o Height: financial risk protection depends on HRH who might charge the patients
• Another dimension of universal health coverage is the ‘effective coverage’.
• HRH is the most important determinants for effective implementation of UHC, especially HRH management knowledge and skill, e.g. revenue raising & pooling – how to collect premium and purchasing – how to set up the benefit package and how to deliver it effectively.
Dr. Pongsadhorn Pokpermdee, Thailand
• Thailand has long history on the development of health insurance schemes for different groups of population, until it reached UHC by 2001
• Implication on HRH
o Incentive for HRH because of services expansion and then more workload e.g. cataract program with the number of patient got operation, CAPD program,
o Another purpose of incentive is for quality assurance improvement e.g. hospital accreditation.
• In sum: UHC policy creates demand for health services and HRH. There is a need to have strong HRH policy and strategy to support UC policy. UHC creates incentives for staff through disease management initiative to expand service and improve quality of care.
62
Dr. Usman Sumantri, Indonesia and Dr. A.A. Sagung Mas Dwipayani, Bali
• Two Indonesian presenters present the movement in Indonesia and Bali towards UHC
• Bali is the new and young scheme
Dr. Sarath Samarage, Sri Lanka
• Population about 21 million. GDP at 2,100 USD per capita, low tax base at 17% of GDP
• Sri Lanka is the national health services free of charge at public healthcare providers, but OOP = 43.5% of THE, GGHE = 49.2% of THE, 0.1% on social health insurance.
• Challenges in SLK:
o Demographic transition, NCD burden (already higher than in the rich countries.
o Financing issues: service package at different levels of care, fiscal space
o HRH related issues: workload, financing, regulation, skill of HRH e.g. PHC, malnutrition problem of children, rehabilitation (in the service package), NCD primary prevention, holistic approach, a family practice approach at primary level.
Dr. Xu Ji, China • History; there are several rounds of health reform. In 2009, China has 283,800
hospitals, 4.41 million beds, 6.73 million health workers. China is in the process of development health insurance system towards UHC.
• Some challenges: uninsured people especially urban migrants, lack of integration of several health insurance schemes and benefit package.
• HRH production in China is still far below needs. Capacity building for senior HRH is needed.
• Further interventions need to balance the HRH distribution, to enhance the HRH capacity, to increase number of HRH.
• Adequate HRH is needed to support the UHC development for which health promotion and disease prevention knowledge and skill are essential.
Mrs. Tran Thi Mai Oanh, Vice director of Health Policy and Strategy Institute, Ministry of Health, Vietnam
• Three issues facing Vietnam in expanding UHC: Ensure availability; Eliminate barriers to access; Organize social protection
• Moving towards UHC in VN: to ensure availability by improving PHC network, to eliminate barriers to access essential health services by issuing Health Insurance Law in 2009 and to organize financial protection by ensuring free health care for the vulnerable people.
• Current health system in VN: 31 hospital at central level, 409 provincial hospitals, 640 district hospital and 10,748 commune health centers. UHC needs to strengthen district hospitals and commune health centers [primary health care focus].
• Nevertheless, Vietnam still has a problem of shortage including medical doctors (7 doctors per 10,000 populations) and mal-distribution especially at district and commune
63
level (only 59% of commune level has doctors). One more issue is lack of doctors who work in health promotion and disease prevention. [dis-integration of curative, health promotion and diseases preventions]
Discussion
• Referral system should be good enough to support the proper health care services (both up and down refer, primary <-> secondary <-> tertiary care)
• Equity issues will have to be addressed upon implementing UHC. Equity to access and equity to quality healthcare.
• Ability to provide health service: the UHC system will allow both public and private providers to join or not. Private healthcare providers in Thailand could join but still minority. Private health sector could help reducing workload of public hospitals. However, private providers might be not available at the grass root level and have limitation in providing disease prevention and health promotion services.
• Satisfaction of health worker under UHC (because of more workload) is questionable. One model under UHC is on contractual model. Doctor-patient relationship:-are there still good or more law suit. There are several factors influenced the doctor-patient relationship. UHC might be only one while many other factors are outside health sectors e.g. media. In China, patients can access more information on health and then lead to higher expectation. Whereas VN health workers feel satisfied with secured funding to the hospital and health personnel.
• UHC and its financial implication; financial incentives according to different activities. This leads to differential incentive among different professionals. Homogenous scheme is better and more effective. Fragmented system creates more administrative hurdles which more workload and costly.
Conclusions
• This session started by Dr Tim Evans on general concept of UHC on three dimensions:-breadth, depth and height on population coverage, service package and financial protection and UHC policy have impacts on HRH for both clinical services and management knowledge and skill.
• Many countries are moving towards UHC with various approaches. SLK and Thailand use general tax financing system whereby Indonesia, China and VN apply mandatory contribution system to finance health care delivery system and to protect patient from catastrophic health expenditure.
• UHC definitely has implication on HRH not only who work on clinical services but also non-clinical services. Regarding clinical services, many presenters highlighted the comprehensive service package in UHC for which requires comprehensive knowledge and skill on public health services at primary care level (i.e. mal-nutrition, health promotion, NCD primary prevention interventions).
• Experiences from countries show some innovative under the UHC to provide more financial incentive directly to health workers and to healthcare providers e.g. Disease Management Incentive, hospital incentives where got hospital accreditation, pay for performance.
64
Parallel session 7 Quality assurance of HRH education and regulation Date October 5th, 2010 (15.00-17.00)
Moderator
Dr. Arsitawati Puji Raharjo, Special Advisor to the Vice Minister of Education and Director General for Higher Education, the World Bank
Speakers
• Mr. Elan Satriawan, Indonesia
Presenters:
• Ms. Faridahwati Shamsudin, Malaysia
• Dr. Nonglak Pagaiya, Thailand
• Dr. Nguyen Thanh Ha, Vietnam
Rapporteur team members
• Dr. Saipin Hathirat, Thailand
• Dr. Indika Karunathilake, Sri Lanka
Key messages from the presentations by speakers
• Mr. Elan Satriawan, Indonesia
Case Vignettes can be used as tool to measure the quality of the health workforce. Using three case vignattes on basic health issues (Pre-natal care, child curative, adult curative), a statistically significant increase was found out in the quality of care both public and private sectors. The knowledge of midwife was found to be as good as doctors in pre-natal care.
• Dr. Faridahwati Shamsudin, Malaysia
A survey conducted among primary care managers of health centers in Southern Thailand found that humanistic culture is more important than leadership culture and leads to improve competencies.
• Dr. Nonglak Pagaiya, Thailand
Survey study among newly graduated MD in 2010 showed that even though the majority of medical students are from urban and upper-middle class/educated family background, they would have positive attitudes towards rural practice.
Another study found that less than 20% doctors remain in rural areas after three years of compulsory service. Professional isolation, been away from home, low income are factors against deciding to remain in rural practice.
• Dr. Nguyen Thanh Ha, Vietnam
65
A survey among students and teachers showed that Problem-based learning is appropriate teaching/learning method in public health curriculum. Lack of availability of trained facilitators and logistics can affect the quality of training.
Major issues or problems being discussed by participants
• Quality Assurance in medical education and the quality of service delivery are not similar. However there are inter-linkages between MDG, QA of education systems and quality of service delivery.
• The knowledge is not the only determinant of quality. To assess the quality of health workforce, the direct observation of their actual practice is essential.
Conclusions
• Humanistic culture is more important than leadership culture and leads to improve competencies. Health workforce education need also to focus on humanistic culture.
• In spite of have positive attitudes towards rural practice among newly graduated Thai MDs, only a minority remain in rural practice after three years of compulsory service.
Recommendations
• Training of managerial skills for health workers is important
• It is important to ensure the quality of HRH education and regulation.
• The examples of QA in medical education in the region should be studied and good practices should be shared. In the future AAAH conferences, more emphasis should be given to QA in HRH education.
• AAAH should arrange the training program on QA.
66
Parallel session 8 Continuing Professional Development Date 5th October 2010
Moderator Prof T P Thapa
Speakers; Mr. Andrew Brown, Australia
Dr. Wasantha Gunathunga, Sri Lanka
Dr. Kenneth G. Ronquillo, Philippines
Dr. Pattapong Kessomboon, Thailand
Rapporteur team members; Mary
Warisa Panichkriangkrai
Key messages from the presentations by speakers
• Mr. Andrew shares his experiences working with Pacific Island countries. He introduces a new approach that has been developed involving a three year partnership between UNFPA, the University of Canberra and representative countries in the region. The approach considers the impact of culture in developing novel approaches to competency development using a participation action framework. So, they use systematic approach or “Seven steps” to assess competencies of countries including competencies, culture, as well as budget and material available, and develop appropriate approach for countries.
• Lessons learnt from the approach:
o CPD needs to be linked with cultural and local ways to implement
o Competency requirements for different countries or localities may differ, but they must be practical-work-based
o The approach engages local practitioners
• Dr.Wasantha presents a mind skills development program using Noble Eightfold Path(NEP) to medical students, and developing and validating a tool to measure characteristics of the mind. It is found out that NEP is effective in improving professional and personal performance in terms of quantity and quality.
o The generic skills needed for health workers: patience, concentration, satisfaction and freedom from stress in order to be efficient and professional
o This CPD program is a transferable skills with lifestyle approach by rediscovering generic skills of mind useful for HRH development
• Dr. Kenneth presents the Masters in Public Management majoring in Health Systems and Development (MPM-HSD) that was developed to solve a problem of limited financial resources and lack of healthcare workers in rural areas. It is a degree course that is composed of a series of independent unit-earning short courses including governance, financing, regulation, and service delivery. This program is part of the Continuing Professional Education Program within 2 year rural service.
o Short courses are strategically phased and based on the need of the health services in the field
67
o The course is designed for healthcare providers, policy makers and planners Initially done for CPD, but it becomes an institutional partnership for
strategic courses cost effective o The participants continue to participate in learning after finishing the course
as a response to their felt needs of health sector reform
• Dr.Pattapong describes an innovative postgraduate program or Leaderships in Primary Care Management. This program focuses on primary care managerial skills of hospital directors in rural areas. Key features are modular systems, case-based learning, workshops, adult learning, study visits and research. The first batch was just graduated and satisfied this program.
o Medical graduates are mostly inadequately trained in managerial skills
o CPD must be feasible & practical
Major issues or problems being discussed by participants
• In-service training is different from CPD
• E-learning can be a supplement combined with web-based learning
• Be cautious on e-learning should be in module fashion
• CPD can be creative towards improvement
• Sustainability can be done through network
Conclusions
• Different kind and approaches of CPD had been discussed, including those in managerial as well as in practical and technical skills for different types and levels of health workers in the community, primary health care institutions and hospital setting
• CPD can improve skills of HRH and enhance learning in order to develop HRH capacity in their workplace
• Different media can be used, but need to be adjusted to local condition or capacity and needs
Recommendations
• Although CPD can be creative towards improvement, it need sustainability, which can be done through networking among stakeholders
• Different media can be used for CPD, but need to be adjusted to local condition or capacity and needs
68
Parallel session 9: Teaching of Public Health Date October 6th, 2010 (8.30-10.00)
Moderator Prof Mahmuda, Head, Department of Community Medicine, Shaheed Suhrawardy Medical College, Dhaka, Bangladesh
Speakers
• Dr. Tim Evans, Bangladesh (Overview)
Presenter
• Dr. Shiv Chandra Mathur, India • Dr. La Ngoc Quang, Deputy Head of Department of Epidemiology, Hanoi School of
Public Health Vietnam • Professor (Dr) Firman Lubis, Professor. Department of Community Medicine, Faculty
of Medicine, University of Indonesia
Rapporteur team members
• Dr. Saipin Hathirat, Thailand
• Ms. Nurdiana . Indonesia
Key messages from the presentations by speakers
• Dr. Tim Evans
Focus on how to teach public health in the change of 21st global health
3 assets of PH teaching areas/contextual challenges
1. Security : social element, environment / climate change
2. Solidality : create equity across country, within country
3. System : growing reality on patient behaviours, multi-feedback loop, working in PH in 21st cen.
3 dimensions of training:
1. Content : Identify of 3 major gaps in content of PH curriculum; Policy trap, ecologic trap, analytic trap - change linear thinking to system thinking or complex adaptive system analysis
2. Who : use the life cycle-based learning ; Trainee : Not to give certificate in early stage, in-service training is more important after they learn from their practice and then they have mid-career change to PH; Faculty need to be trained ; move from pedagogy to problem solving skill
3. How: Corporate approach(have people engage in reality of practice environment), Bring training site came close to their life, decentralize, instead of city training, Continuing education (providing accessible to update information to frontline people, center of excellence, research in action and teaching together in reality topics)
Health workforce is new area in PH and need leadership - actively engage policy maker to alliance and to generate system.
69
• Dr. Shiv Chandra Mathur
Community health fellowship program in Madhya Pradesh and Rajasthen, India. 2-year program, weekly program with cluster meeting and collective teaching. Then feedback at national conference.
Objective of scholarship: to strengthen the motivation, interest and commitment of young person’s for community health, to sharpen the analytic skills and to deepen the understanding of the societal paradigm of community health
• Dr. La Ngoc Quang
Field training experiences for MPH at the Hanoi School of PH(HSPH), Vietnam: alumni survey of MPH training
MPH started in 1995 plus the cooperating with international experts in 2-year innovative program field training “PHSWOW – public health school without wall”
Combined qualitative and quantitative study on 187 MPH alumni (90% general MD) on the appropriateness of the program in different competencies of learning.
• Professor (Dr) Firman Lubis
Normally teaching public health separate from clinical science in medical school. While clinical teaching is developed rapidly, PH is not changed much.
Present using PBL discussion to revitalize public health in clinical curriculum in medical school
Major issues or problems being discussed by participants
• There are maybe enough innovative teaching methods but how to sustain in reality.
• Every patient comes with not only body but whole context with him. Social issues should be in the medical teaching.
• Because PH is not only quantitative, how to teach qualitative approach in PH teaching
• Any school assess using case study in PH in medical student and master student
Conclusions
• Need to reorient PH curriculum to change and adapt to global health change in 21st century
Recommendations
• Need tips for PH teaching in future teachers
70
Parallel session 10: Community health workers Integrating community health workers into national health systems Wednesday 6 October 2010, 8:30-10:30 Coordinators: George Pariyo Speakers:
Dr. Syed Musad Ahmed, Bangladesh Dr. Luckshimi Kumaratilake, Sri Lanka Mrs. Mary Roroi, Papua New Guinea, Papua New Guinea Dr. Nonglak Pagaiya, Thailand
Rapporteur team members Dr. PongsadhornPokpermdee, Sudong Participants: 50 approximately Key messages from the presentations and discussion by speakers and participants George Pariyo He presented the key messages of GHWA on integrating community health workers in national health workforce plan. This includes 3 main issues as follows:
1. Planning, production and deployment such as Integrating Community Health Workers (CHWs) into national HRH plans and health systems and involve key HRH stakeholders in the decision-making process, and ensure monitoring and evaluation throughout the policy and implementation process. It should have an adequate provision of the additional costs and resources required for supporting the cadre
2. Attraction and retention Preparing and engaging the community from the start in planning, selecting, implementing, monitoring and supporting CHWs and ensure a regular and sustainable remuneration stipend and, complement it with other rewards, which may include financial and non-financial incentives.
3. Performance management Performance management should be based on a minimum standardized set of skills that responds to community needs and appraisal of strategies, and is context-specific. The management and supervision of CHWs should be integrated with that of other health workers, using a team approach, and should be developmental, systematic, planned and budgeted for accordingly, in order to achieve the desired service delivery and health outcomes.
Dr. Syed Musad Ahmed, Bangladesh
• CMH in Bangladesh provide essential healthcare services to the community voluntarily.
• The attraction and retention of CMH are opportunity to serve the community and access to privileged knowledge, motivation by BRAC staff, benefits both the community (door-step services) and the SS (empowerment) and a reasonable, fixed, monthly remuneration
• The lesson learnt are volunteering is a culture-sensitive concept and western concept of volunteering may not be applicable in LMICs context. It should be linked to the livelihood strategies of the poor women in LICs.
• Opportunity cost of the poor women should be taken into consideration while developing ‘voluntary’ health workers. Monetary incentives based on performance should be given to improve income and satisfy economic motivation. A career path with the possibility of being promoted to the next level of cadre of health workers will increase retention.
71
Dr. Luckshimi Kumaratilake, Sri Lanka
• CMH is an important part of Sri Lanka health system which has constrains of resources. Each CMH response for 3,000 populaiton and focus on preventive area only.
• There is a need for continuous professional development reaching all and training curriculum revision needed for training of new CMH. In addition, CMH should be allocated higher proportions to provinces with poor health indicators.
• The attraction and retention of CMH in Sri Lnaka are government salary with pensions and allowances, facilities: quarters, transport, and schooling for children.
• The suggestions on the performance management include: supervision of CHW at all levels, monthly conferences, discuss performance, integrated information system and national indicators for performance assessment.
Mrs. Mary Roroi, Papua New Guinea • The Community Health Workers (CHW) is a major provider of the health services in
Papua New Guinea. They are the first contact at the Aid Post health facilities providing primary care to the rural majority. They provide primary health care and primary curative care due to shortage of the nurses in the hospital setting.
• Lesson learnt and practice: The designing of the program should met the National Health Plan needs, equipped the graduate to be competent to practice in the employment setting. Stakeholder should involve throughout the process, HR, training, the tutors to ensure support for implementation.
• Attraction and retention: There is employment available for them and they have associate with the Department for better employment terms and conditions.
• Performance management: assure that they are skilled, motivated and productive in activities carried out and also to create career pathway for the CHW (HRH Policy), capacity building for Managers in areas of use of information system to strengthen the supervision and monitoring to ensure achieve good health outcomes at all levels. It should have documentation of management systems at all levels in particular, local levels in way of reporting to strengthen the performance management.
Dr. Nonglak Pagaiya and Dr. Somyote Srijaranai, Thailand
• After Thailand implemeted PHC, health seeking behavior has been changed from last 3 decades from self care and traditional healer to seek care in the system including health center, public and private sector. As a result, infant mortality has decline dramatically from 81.3 in1964 to 11.3 in 2006.
• CMH plays important roles in PHC in Thailand for many decades. Currently, Thailand develops the strategic road map to train CMH in order to response on the dynamic situation such as chronic diseases. Case study of Kalasin province (middle income in NE region) is shown as a case study.
• Strategies road map could be used to redress the problem of health workforce shortages, in such a sustainable approach, shifts care from curative to health promotion, empower communities; explore social capital to develop healthy communities and gather multi-stakeholder to participate in this process.
Conclusions This section put emphasis on the need to support countries in the decision to integrate and implement community health worker (CHM) activities on a national scale and selecting appropriate strategies for the use CHMs as an integral component of their HRH and national health system. The experiences from different countries in a different context in this section are useful for other countries to strengthen the CMH as major part of national health workforce.
72
Annex 4: Suggestions from participants on the way forward of AAAH
List of all 60 suggestions and comments on the way forward of AAAH ID Suggestions 1 Assist in providing T.A. to help in setting up of “Direct entry midwifery” course for
assuring in Samoa 2 To provide the opportunity to debate the fixation on planning and to strengthen the
focus on strategic thinking in HRH 3 Create a platform for sharing experiences, particularly on innovations & success
stories in the area of HRH education and management. 4 To develop creative of innovative medical education to improve MDGs goals (in
those area manner) 5 It is very much appreciated if the AAAH resources could be used & focused towards
the implementation strategies and facilitate implementation processes of the member states
6 Facilitate implementation of curriculum revisions in individual country 7 Provide assistance in HRH in terms of survey with where we are in Fiji and in
achieving on MDG 8 To enroll individual members or organization for AAAH. If so, I would like to be
Reg, or NHSRC of Government of Indonesia to be registered. Is that regular inputs can be contributed for HRH.
9 1. Individuals active in HRH area need to be promoted by AAAH 2. Leadership of Medical schools should be in the hosts who can strengthen
“Generalist” education 3. Privatization should be promoted with stringent regulation
10 Work with universities to help them engage with MoH and industry to determine competency requirements for health care workers by doctors, nurses, health practitioner, ect.
11 AAAH should be mase in action as implementation of all the issues and recommendations that have been mentioned since many years ago. For this AAAH should build a strong network among all stakeholders and pressure to health policy workers and political leaders.
12 AAAH to further involve education department and institution to promote synergy between health and education in development of HRH
13 Catalyst to global converter of HRH development Facilitates of various dynamics in HRH development Promote HRH development
14 Evolve a common guideline for quality evaluation of health professionals and para-professionals at all levels- doctors, nurses, technicians, pharmacists, health workers, midwives etc, especially in view of the growing role of private trainers/educators.
15 Networking and addressing inter-regional HRH issues to enhance joint learning and collaboration between countries with MRE framework to check progress
16 AAAH in the coming year should enhance upon producing/devising methodology for counties the national health professional education account This tool will help in mapping resources in term of who pays including household, who manage these resources, who provides the education services, and for work discipline By mapping this, inequalities in health professional education can be determined
73
at country level as well as globally by cross- country comparison 17 Do countries have the competence to analyse the HR situation design a system
covering both public and private sector conduct research on HR? Comprehensive change in a systems complex is necessary. Are counties prepared for the huge task?
18 AAAH should evaluation their 5 years performance and obviously more participation from nursing & paramedic workforce groups
19 AAAH should be leaded in preparing or identify common core competency that could include in curriculum for all categories of health profession like M.D., nurse, midwife, etc. for Asian countries. Whereas others specific subject will be manage by individual countries
20 Follow up activities among AAAH countries on action plan related with HRH especially health education
21 The AAAH should assist in developing a monitoring & evaluation program for rural retention of health professional by -Sharing experiences in other countries -Providing tool that can be used -How to analyse the results.
22 Inequalities in Human resources for health Social determinants of human resources for health
23 What can AAAH do? Top private sector (companies & agencies) to finance more workshops, develops, summary especially training program to really make a dust in local & international efforts.
24 Share of information and experiences with similar forum across other regions 25 Set panel for sharing experiences of success small story of each country on linkage
of medical education and health system. This panel should be in next conference 26 Maintain the network education, updated with HRH and HRH related uses and
engaged 27 Summary well the recommendation and sent to all country members by email or
by well sets of AAAH 28 AAAH needs to push forward the discussions that we have made in the past time
years into real actions. Wish to listen to more resolutions and policies that member countries conducted in the coming future
29 AAAH should act as a regional coordination organization for research and training activities and financial support provider in Asia-pacific region
30 Database of education institution in order to improve health professional education among AAAH members
31 AAAH serve as research bank for achieving the third HRH revolution. 32 The role of AAAH should be
‐ Providing standard for HRH education regarding the competencies of Health workers.
‐ Providing standard ratio for each Health worker specification (Doctors, Nurses, Midwives) according the country of the population and providing recommendation to achieve the acceptable ratio.
33 For specialist & sub specialist education – it should be spiral based and the colleague from each professional society should be active in this education or training. In Indonesia now this education is university based and the trainee has to paid instead of being paid
‐ Less growth of specialist and sub specialist ‐ World Bank should help financial for Physician, nurse and technician
education in Indonesia the program should well prepare
74
34 AAAH should push for HRH research to inform HRH policy through networks or by funding / commissioning research
35 To assist member countries in achieving HRH challenges in terms of ‐ Enhancing evidence based research ‐ Providing technical and financial assistance in solving HRH problems in each
country ‐ Strengthening Health systems in the countries
36 ‐ As a catalyst in shaping global, reproval and country HRH balance ‐ To be instrumental in advocating policy makers to get aware of the
importance of HRH as the human for global health system ‐ To find a change agent / champion of country level and guide them more.
37 ‐ The role of AAAH will be improve coordination and reduce 10% HRH crisis ‐ Please invite the same people again
38 Influence change in Human Resource for health production and deployment to action–chronic disease in developing country
39 ‐ Shaping the information : policy for HR for health, changing education for the priority of the problem/problem in health
‐ Making minimum standardization of education in health in Asia Pacific 40 Development of institution of HRH education is not difficult but for making
standardize of institution of HRH education is very difficult and assure to quality of HRH is very difficult too
41 Build some like “A board” to synchronize between Ministry of Education and Ministry of Health to link “Health system with human resource for health production & distribution”
42 Creative with the network capacitate 43 Be health sensitive
‐ To provide infrastructure in strategic policy formulation and regulation skill Fiji
‐ I would like AAAH to provide information and consultancy assistance to the Ministry of Health that will assist it to address of human resource challenge in relative to returning its health worker; in relative to university the administrative, and financial carder of official to be knowledge based in health system that is to be empowered to PTO be health sensitive
‐ To provide infrastructure in strategic policy formulation and regulation skills. 44 ‐ The AAAH can work very closely with institutions specializing in
management (or junctional management) to train health sector professionals on non-medical aspect of institutional management
‐ Research collaboration between health professional bodies and educational institutions needs to be promoted and encouraged
45 How can AAAH to support health strategies and formation of Health authorities 46 The AAAH should assist the Pacific island countries in setting up a reliable date
system which is sustainable 47 To assist and facilitate the HRH needs of countries based on their country
context/regional context – Pacific island countries share similar issues- Help build capacity and institution content
48 To carry out a survey on the institution their status towards the new innovative measures What strategies depending on the context
49 More opportunity to help and Pic because we are facing the same problem in regards to human resources for health
75
50 Develop a theme for each year and manage the discussion at regional & global level e.g. Brain drain of Health workforce from LIC, to HIC for coming year
51 AAAH should seriously consider has to work in a concerted and coordinated with various stakeholders. HRH to obtain an action and output and outcome oriented framework or actions point to be carried and by individual member countries is line with the epidemiological and other scenario of the countries Then there will be monitored and share their experience Future AAAH annual meeting/conference
52 ‐ Produce an evidence –based report that can convince that there is a dire need for reform in health education in order to meet MDGs and ensure equity
‐ AAAH can share finding at global conferences and publish it 53 The “King pin” of a motor car which will coordinated all different HRH activities in
the region 54
The AAAH should be able to : Facilitate the co operation not only between G to G but also I to I (Health Education Institute
55 Psychological transportation Strategies to impress professional
56 AAAH should work more closely with the Govts. For taking knowledge on HRH where practice is.
57 The way forward: 1. Evaluation(External/Internal) Revise working plan 2. Country Blog: update news/articles/case studies on HRH 3. Member countries to develop National HRH medium and Long Term Strategies
(2010-1020) 4. Member Countries to submit a brief on the Current HRH situation 5. A core active HRH team with 3-5 members, consisting of 6. Fulfill the roles on the Second Global Forum
• Organizing participants from AAAH member countries to attending the forum.
• Coordinating member countries to submit case-stories and recommend HRH award nominees to GHWA by the end of November
• Select rapporteor and speakers for plenary and parallel session 7. CCF: to coordinate the Five most priority countries to complete: National
Health Workforce Strategies’ 8. Workshop: HRH Planning 9. Participants go back to your countries please report the conference HRH to
your boss, the Ministry of Health and the Ministry of Education 10. The 6th AAAH Conference theme:HRH and UHC Venue: Philippines Dates late Sept 2011
58 Cannot read
59 Cannot read
60 The next meeting of AAAH on HRH,should considering or including other health professionals such as nutritionist/dietious sonitarian, pharmacist, public health wirkers,etc. So it is not medical science bias. We need more on promotive + preventive aspects and it is not only a culative aspects. The maternal health & maternal mortality is related to onder nutrition
76
Grouping of all 60 suggestions into six groups All 60 suggestions and comments were listed below. Similar suggestions were merged and then classified into 6 groups:- (A) networking and collaborating, (B) research/evidence generation, (C) Information sharing and knowledge exchange, (D) Institutional Strengthening and Capacity Development or Supporting implementation at country level, (E) assessment of the AAAH and (F) others. (A) Networking and collaborating
1. Work in a concerted and coordinated with various stakeholders 2. Networking and addressing inter-regional HRH issues to enhance joint learning
and collaboration between countries 3. CCF: to coordinate the Five most priority countries to complete: National Health
Workforce Strategies. 4. Promote synergy between health system and education for develop HRH
(B) Research/evidence generation 5. Providing assistance in HRH in term of survey with where we are? and in
achieving on MDG. 6. AAAH should assist in developing a monitoring and evaluation program for rural
retention of health professional 7. Promote and encourage research collaboration between health professional
bodies and education institutions. 8. Collect database of education institution in order to improve health professional
educating among AAAH members. 9. Mapping resources in term of who pays, who manage, who provides the
education services 10. Produce an evidence based report 11. Providing standard ratio for each health worker specification according to the
country and providing recommendation to achieve the acceptable ratio. 12. AAAH should act as a regional coordination organization for research and training
activities and financial support provider in Asia-pacific region (C) Information sharing and knowledge exchange
13. Create a platform for sharing experiences, particularly on innovations & success stories in HRH education and management.
14. Provide the opportunity to debate the fixation on planning and to strengthen the focus on strategic thinking in HRH.
15. Set panel for sharing success stories of each country on linkage of medical education and health system.
16. Country blog: update news/articles/case studies on HRH 17. Shaping information: policy for HRH, changing education for the priority of the
problem in health sector. 18. AAAH should work more closely with the Gov. for taking knowledge on HRH
where the practice is? (D) Institutional Strengthening and Capacity Development or Supporting
implementation at country level 19. Providing information and consultancy assistance to the MoH that will assist it to
address of HRH challenge in relative to returning its health workers, in relative to university and administrative, and financial carder of official to be knowledge based in health system that is to be empowered to PTO.
77
20. AAAH resources& focused towards the implementation strategies and facilitate implementation processes of the member states.
21. Making and providing standardize of institution of HRH education. 22. Developing guideline for quality evaluation of health professionals and para-
professionals at all levels especially in view of the growing role of private trainers/educators.
23. AAAH can work very closely with institution specializing in management (or functional management) to train health sector professionals on non-medical aspect of institutional management.
24. Providing infrastructure??? in strategic policy formulation and regulation skills. 25. The role of AAAH will be improved coordination and reduce 10% HRH crisis.
(E) Assessment of the AAAH 26. AAAH should evaluate their 5 years performance and obviously more participation
from nursing and paramedic workforces groups. 27. AAAH should evaluate themselves (both external/internal), revise working plan.
(F) Others, unclassified 28. The next meeting of AAAH on HRH should considering or including other health
professionals such as nutritionist/pharmacist, public health workers, etc. So it is not medical science bias. We need more on promotive and preventive aspects and it is not only a curative aspects. The maternal health & maternal mortality is related to under nutrition.
29. Participants report the conference HRH to their boss after go back to their countries.
30. The 6th AAAH theme: HRH and UHC: the venue: Philippines, dates late September 2011. Select rapporteur and speaker for plenary and parallel session.
31. Please invite the same people again. 32. Coordinating member countries to submit case stories and recommend HRH
award nominees to GHWA by the end of November.
Related Documents











