UPMC Cardiovascular Institute Improving D2B Time in ST-Elevation Myocardial Infarction Sun Scolieri, MD Assistant Professor of Medicine UPMC Cardiovascular Institute

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

UPMC Cardiovascular Institute
Improving D2B Time in ST-Elevation Myocardial Infarction
Sun Scolieri, MDAssistant Professor of Medicine
UPMC Cardiovascular Institute

UPMC Cardiovascular Institute
History at UPMC Presbyterian
Data collection began in Jan 2004 and analysis revealed:• Average time to intervention first 6 months: 447 minutes• No standardization of process• Multiple layers involved in facilitating a patient from the
Emergency Department door to the Cardiac Catheterization Laboratory with successful intervention.
• Commitment to minimize D2B time at UPMC Presbyterian• Original goal <120 minutes, later reduced to <90 minutes• Variety of measures implemented July through September
2006 at UPMC Presbyterian ED/Cardiology

UPMC Cardiovascular Institute
Process Flow Pre Initiative
Patient arrives in ED with Chest Pain
Triage via ED RN
EKG Completed
Assessment by ED Physician
Chest Pain Team Called
Assessment by Cardiology Attending/Fellow
Cardiology Assessment Team contacts
Interventional Cardiologist
Decision for Cardiac Catheterization
Cath Lab Call Team notified – 30 minute window to
arrive at hospital
Transported to Cath Lab
Procedure and Intervention

UPMC Cardiovascular Institute
Improvement Plan
Task force initiated including:• ED and Cardiology Physicians• ED and Cardiology Management and Staff
• Emergency Medical Services Personnel and Management Team
• MedCall Referral Management

UPMC Cardiovascular Institute
Tracking System Initiated
Tracking form developed and implemented.
2. Emergency Department initiates form as soon as patient arrives.
3. ED staff completes form and sends with patient upon transport.
4. Cath Lab Staff completes remaining portion of the form and Manager collects and tallies information.

UPMC Cardiovascular Institute
Acute Myocardial Infarct Tracking Log
Pt Name__________________________
Medical Record #___________________
Date______________________________
Procedure Time Comments 1. Prearrival Activation- Chest Pain
Team
2. Arrival to ED
3. First EKG
4. Chest Pain Team activated by ED
5. Arrival of Cardiology fellow in ED
6. Decision for cath/on-call staff
paged
7. CCU attending called by fellow
8. Cath attending called by fellow
9. Time ED ready
10. Time Cath ready.
(Call Cath Lab to clear transport 30
min after page/allow 20 rings)
2-4745
Ready? Y or N
11. If no, second attempt to call Cath
Lab (5min later) 2-4745
Ready? Y or N
12. If no, page Kitty Zell #3446
13. Transported to Cath Lab
14. Time into lab
15. Time case began
16. Time of access
17. Time of Angiojet
18. Time wire across lesion
19. Time first balloon inflation

UPMC Cardiovascular Institute
Before and After D2B Initiative Emergency Department
BEFORE
• Patient (pt) arrives with c/o CP EKG was done by ED staff and presented to either the resident, ED attending or left in room awaiting MD evaluation
• Upon PCI decision; pt waited in ED for cath lab team arrival before further preparation
• RN would go to McKesson to retrieve cardiac medications many times during ED treatment phase
AFTER
• After initial EKG is completed, EKG is taken immediately to ED attending physician for review
• Upon PCI decision; pt is changed to gown, procedural translucent EKG leads are placed, and groin prepped by ED staff
• All Cardiac meds for AMI are available in one box in the McKesson called “AMI Kit” to increase efficiency

UPMC Cardiovascular Institute
Before and After Decision-Making Process
BEFORE
• Assessment by the ED Physician• Chest Pain Team called• Assessment by Cardiology
Fellow• Cardiology Fellow pages
Cardiology attending on-call• Cardiology Attending on-call
makes decision to contact Interventional Cardiologist
• Interventional Cardiologist pages Cath Lab on-call Team
AFTER
• Assessment by ED Physician• Chest Pain Team,
Interventional Cardiologist, Cardiology Fellow and Cath Lab on-call team paged simultaneously.

UPMC Cardiovascular Institute
Before and After Cath Lab ProtocolsBEFORE
• Cath Lab paged only after full ED and Cardiology assessment
• Travel time 30 minutes• Search for Parking in PUH
Garage• Prepare procedure room• Call for patient when all three
staff members as well as Cardiologist and Fellow have arrived
AFTER
• Cath Lab called in based on ED physician assessment.
• Travel time 30 minutes• Park in Emergency Department
spaces• No room preparation needed –
room left “ready” for emergency patient
• First staff member present calls for patient – ED staff will stay and assist if patient transported before rest of call team arrives.

UPMC Cardiovascular Institute
Assessment Post Event
Acute MI Logs collected and analyzed within 24-48 hours of procedure
Immediate feedback to all Physicians, Staff members, EMS staff and MedCall Staff providing a “report card” of
Outcome.
UPMC Cardiovascular Institute
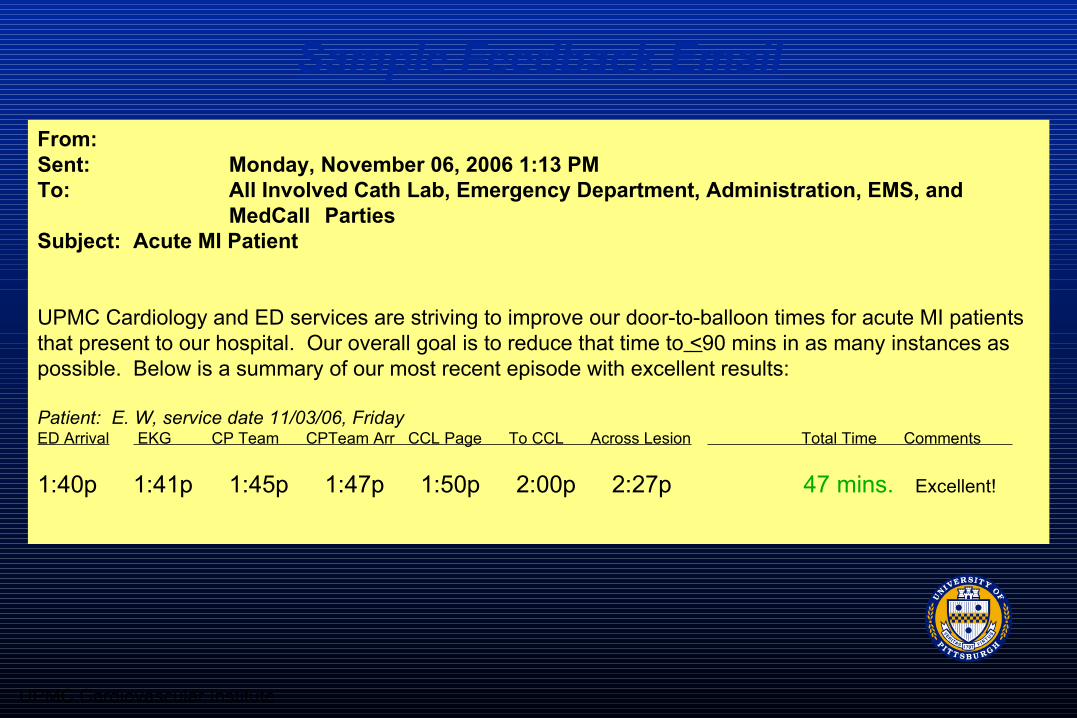
From: Sent: Monday, November 06, 2006 1:13 PM To: All Involved Cath Lab, Emergency Department, Administration, EMS, and
MedCall Parties Subject: Acute MI Patient
UPMC Cardiology and ED services are striving to improve our door-to-balloon times for acute MI patients that present to our hospital. Our overall goal is to reduce that time to <90 mins in as many instances as possible. Below is a summary of our most recent episode with excellent results:
Patient: E. W, service date 11/03/06, Friday ED Arrival EKG CP Team CPTeam Arr CCL Page To CCL Across Lesion Total Time Comments
1:40p 1:41p 1:45p 1:47p 1:50p 2:00p 2:27p 47 mins. Excellent!
Sample Feedback Email

UPMC Cardiovascular Institute
Guideline Applied Practice~Door-To-Balloon GAP-D2B Goal
• To achieve a door-to-balloon time of
< 90 minutes for at least 75% of non-transfer primary PCI patients with ST-segment elevation myocardial infarction in all participating hospitals performing primary PCI.

UPMC Cardiovascular Institute
Difference?• We analyzed non-transfer patients with STEMI
presenting between July 2005 and May 2007 at UPMC Presbyterian Hospital.
• The baseline group consisted of 63 consecutive STEMI patients between July 2005 and August 2006, and we compared these to 31 consecutive STEMI patients enrolled after protocol implementation, between September 2006 and May 2007.

UPMC Cardiovascular Institute
UPMC Presbyterian Time to PCIJuly 2005 -May 2007
020406080
100120140160180200
Ju
l-0
5
Au
g-0
5
Se
p-0
5
Oct-
05
De
c-0
5
Ja
n-0
6
Fe
b-0
6
Ma
r-0
6
Ma
r-0
6
Ap
r-0
6
Ju
n-0
6
Ju
l-0
6
Au
g-0
6
Se
p-0
6
Oct-
06
No
v-0
6
Ja
n-0
7
Fe
b-0
7
Ap
r-0
7
Min
ute
s
Time to PCI Target 90 Minutes Trend
Full implementation of D2B initiative
Data based on admission date available as of June 15, 2007

UPMC Cardiovascular Institute
UNDER 90 MINUTES
87.1%
28.6%
0
20
40
60
80
100
Pre Post
Initiation
Pe
rce
nt
7/05-8/06 9/06-5/07
N=63 N=31
p<0.00001

UPMC Cardiovascular Institute
MEAN D2B TIME
108.3
72.2
0
20
40
60
80
100
120
Pre Post
Initiation
Tim
e (m
inu
tes)
N=63 N=31
p<0.00001
7/05-8/06 9/06-5/07

UPMC Cardiovascular Institute
MEAN D2B TIME
108.3
72.270.7
0
20
40
60
80
100
120
Pre Post Updated
INITIATION
TIM
E (
Min
ute
s)
7/05-8/06 9/06-5/07 9/06-8/07
N=63 N=31 N=37
p<0.00001
Data based on admission date available as of September 15, 2007

UPMC Cardiovascular Institute
ACC: Evidence-based Strategies
1.Pre-hospital ECG to activate the cath lab
2.ED physician activates the cath lab3.One call activates the cath lab4.Cath lab team ready in 20-30 minutes5.Prompt data feedback6.Senior management commitment7.Team-based approach

UPMC Cardiovascular Institute
How to make it work
1) Commitment from leadership of involved departments to make improvement of D2B highest priority.
2) Empowerment of emergency physician to directly activate cardiac cath team
3) Single call activation system for in-house cardiology, cath lab staff, interventional fellow and attending.
4) Defined time expectations for triage to ECG time, decision to activate cath lab, transfer time.
5) Detailed real time feedback of each component of D2B to all caregivers involved within 1 day of patient encounter.
UPMC Cardiovascular Institute
Thank You
• Joon Sup Lee, MD• Suresh Mulukutla, MD• Vincent Mosesso, MD• Donald Yealy, MD• Charissa Pacella, MD
• Kitty Zell, BSN• Peg Richards, BSN
• MedCall/ Referral center
• Emergency Services • ER staff and personnel• Cath lab staff and
personnel• Administrative support
Related Documents











