Improving Accrual to Improving Accrual to Clinical Trials Clinical Trials Saving patients and $aving Saving patients and $aving Time Time Daniel Weisdorf October 2011 Thanks to Mary Horowitz

Improving Accrual to Clinical Trials Saving patients and $aving Time Daniel Weisdorf October 2011 Thanks to Mary Horowitz.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Improving Accrual to Clinical Improving Accrual to Clinical Trials Trials
Saving patients and $aving Saving patients and $aving TimeTime
Daniel Weisdorf
October 2011
Thanks to Mary Horowitz

Clinical ResearchClinical Research
Basic Biomedical Research
Human Studies of Safety/Efficacy –
Clinical Trials
Clinical Science
and Knowledge
Clinical Practice and Health Decision
Making
Improved Health
From: Sung et al. Central challenges facing the national clinical research enterprise. JAMA 2003;289:1278-87.
Effectiveness vs. Efficacy
Quality/Access
Improvement
ImpairedHealth

Major frequent problems in Clinical Trials
1. Bad idea
2. Poor study design--masks true test of a good idea
competing hazards, co-variates, wrong patient group
3. Too few patients--statistically invalid.
May not observe great response in subset.
4. Too short a trial.
5. Wrong analysis. ,ß...….. errors
CLINICAL TRIALS ARE DIFFICULTCLINICAL TRIALS ARE DIFFICULT
2003 Institute of Med Report High research costs/lack of funding Regulatory burden Fragmented infrastructure/ incompatible databases Lack of willing participants (informed consent issues+
) Lack of qualified investigators Career disincentives
True for all disciplines – but especially in HCT

Distribution of Transplant Volumes Distribution of Transplant Volumes among 181 US Centers Reporting Data to among 181 US Centers Reporting Data to
CIBMTR-2008CIBMTR-2008
34%
15%22%
25%
4%
<3030-4950-99100-299>300
Mmh06_6.ppt
29% >100/y
HCT is really uncommon
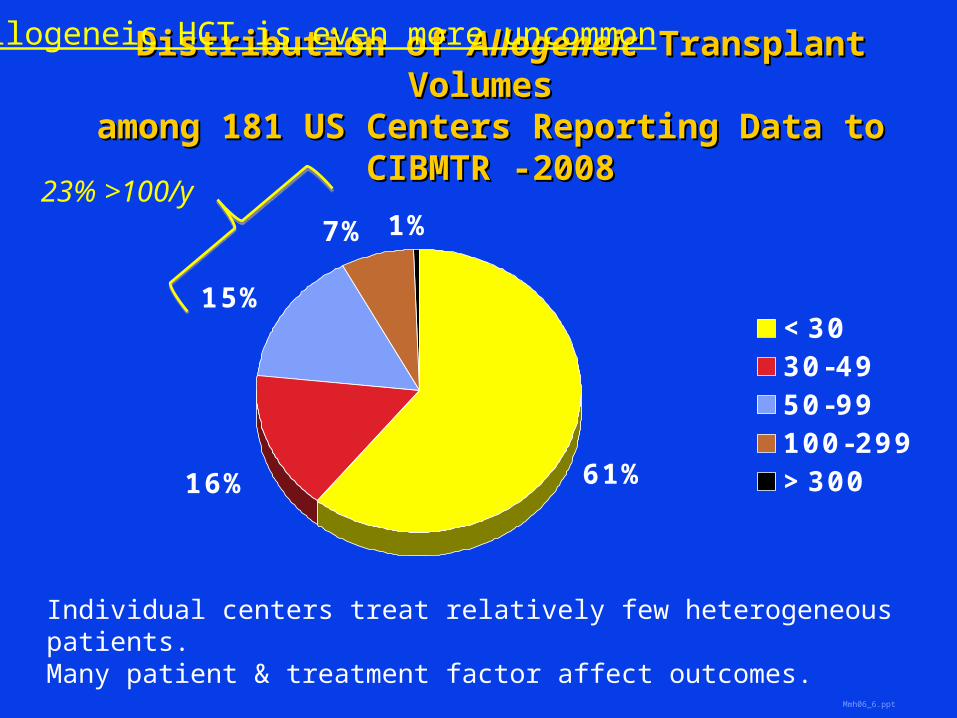
Distribution of Distribution of AllogeneicAllogeneic Transplant Volumes Transplant Volumes
among 181 US Centers Reporting Data to among 181 US Centers Reporting Data to CIBMTR -2008CIBMTR -2008
61%16%
15%
7% 1%
<3030-4950-99100-299>300
Mmh06_6.ppt
Individual centers treat relatively few heterogeneous patients. Many patient & treatment factor affect outcomes.
23% >100/y
Allogeneic HCT is even more uncommon
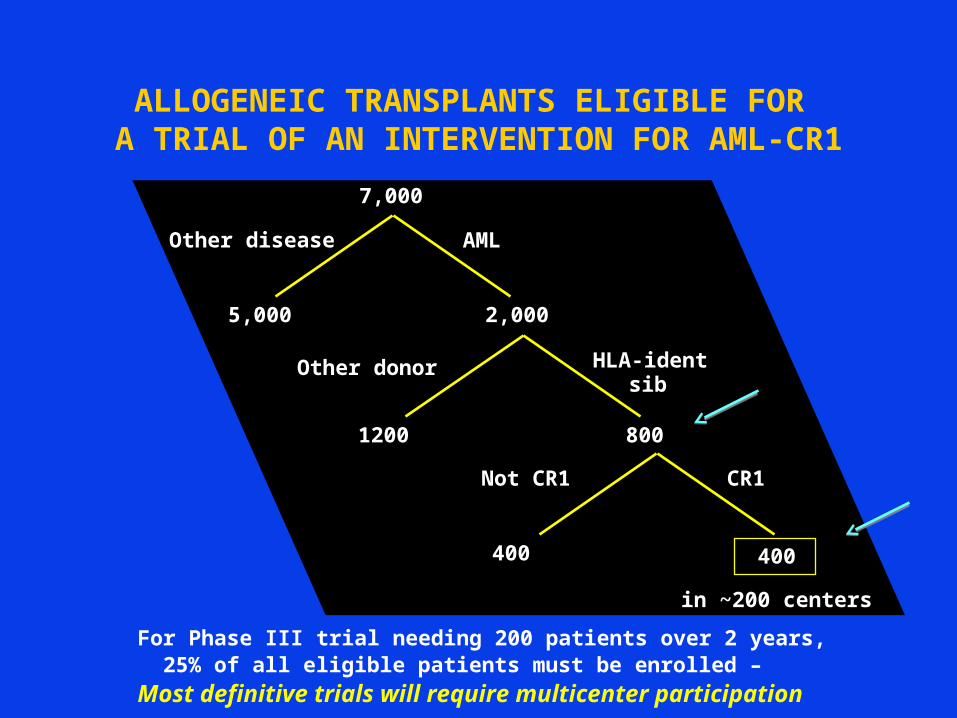
ALLOGENEIC TRANSPLANTS ELIGIBLE FOR A TRIAL OF AN INTERVENTION FOR AML-CR1
For Phase III trial needing 200 patients over 2 years, 25% of all eligible patients must be enrolled – Most definitive trials will require multicenter
participation
7,000
2,0005,000
AMLOther disease
8001200
HLA-ident sibOther donor
400
in ~200 centers
400
CR1Not CR1
HCT Trials are difficultHCT Trials are difficult
Complex therapy for life-threatening diseases Long, involved informed scary consent documents Patients are very sick
Everyone [patient/referring MD/transplant MD] wants to believe they know the best treatment
Competing risks complicate the primary endpoint How do you interpret patients who die before reach a
primary endpoint? Death before engraftment or GVHD
Need more patients to make up for drop-out Two subjects – donor and recipient
Increases complexity and costs Decreases numbers eligible for studies

BMT endpoints occur at varying times
Engraftment at 20-45 days;
GVHD by 100+ days; Chronic GVHD 2-24 months
Relapse 1-2 years;
Survival long term.
Quit for early endpoint likely makes sample too small to see
late endpoint.
Followup is costly but well designed early trial can be
informative later on
DBV06_21.ppt
Small NumbersSmall Numbers Tests our willingness to collaborate.
Large collaborative observational databases – a unique feature of our field CIBMTR EBMT
Usable for study planning—control and eligible pts
Collaboration for clinical trials
– 2001 – Blood and Marrow Transplant Clinical Trials Network BMT CTN – infrastructure for large Phase II and III trials
– 2005 – Resource for Clinical Investigations in BMT RCI BMT – smaller Phase I/II trials

What makes a good Protocol?What makes a good Protocol? Important question
Can the result change practice? How many people might it affect?
What is a realistic effect size? How to estimate baseline outcomes
and treatment effects Affects target enrollment
How many patients are there that might be eligible to enroll? Who is treating them now and how?
What makes a good Protocol?What makes a good Protocol? Important question
Can the result change practice? How many people might it affect?
What is a realistic effect size? What are realistic baseline outcomes
and treatment effects Determines target enrollment
How many patients are there that might be eligible to enroll? Who is treating them now and how?

What makes a good Protocol?What makes a good Protocol? Important question
Can the result change practice? How many people might it affect?
What is a realistic effect size? How to estimate baseline outcomes and
treatment effects Affects target enrollment
How many patients are there eligible to enroll? Who is treating them now; and how? Are they interested in a new HCT trial?

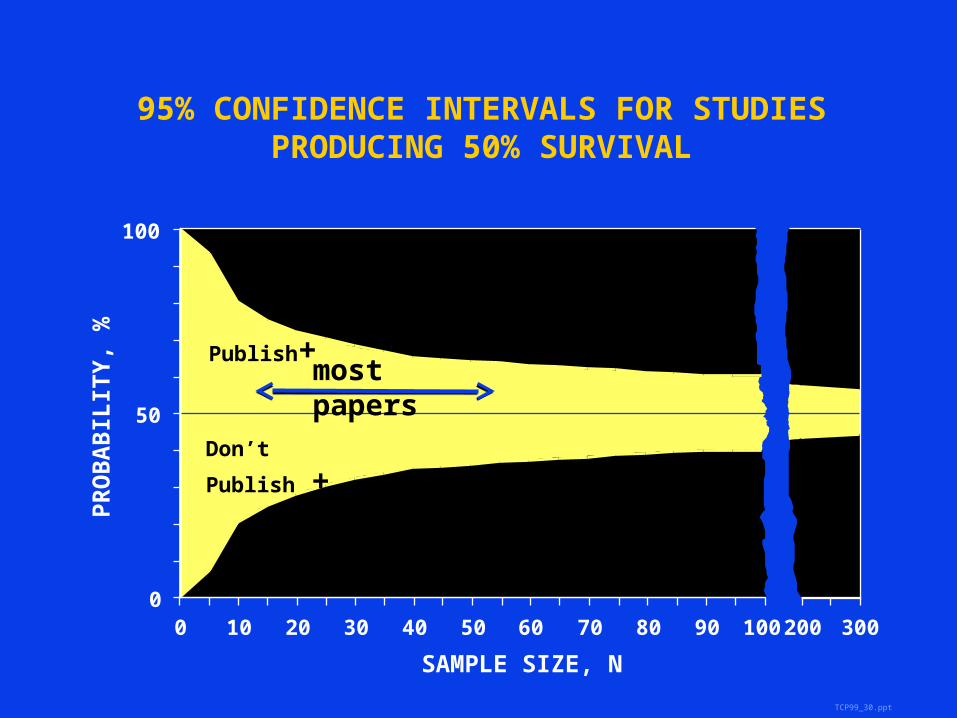
Baseline Outcomes and Effect SizesBaseline Outcomes and Effect Sizes
Publication bias – results may be misleading Single center study – examine your own
data Multicenter study – CIBMTR database
TCP99_30.ppt
95% CONFIDENCE INTERVALS FOR STUDIES PRODUCING 50% SURVIVAL
SAMPLE SIZE, N
0 20 30 40 50 60 70 80 90 10010
PR
OB
AB
ILIT
Y,
%
0
50
100
300200
Publish
+
Don’t
Publish +
most papers

TCP99_30.ppt
SAMPLE SIZE, N
0 20 30 40 50 60 70 80 90 10010
PR
OB
AB
ILIT
Y,
%
0
50
100
300200
Publish
+
Don’t
Publish +Most trials
95% CONFIDENCE INTERVALS FOR STUDIES PRODUCING 50% SURVIVAL

Not all have equipoise
Baseline Outcomes and Effect SizesBaseline Outcomes and Effect Sizes
Publication bias – results may be misleading Single center study – examine your own data Multicenter study – CIBMTR/EBMT databases
Consider randomized Phase II study
Allows consideration of broader eligiblity and selection to judge worthiness for followup study
Can use pick the winner design-not the best, but the best to study
Randomized Phase II TrialsRandomized Phase II Trials Single arm Phase II designs assume historical rate is
“fixed” and efficacy based on a one sample comparison to that a fixed rate
A randomized control arm may be helpful if historical rate is uncertain Especially useful when inclusion criteria are variable:
VOD syndrome, high risk GVHD
BMT CTN 0302 – randomized 4 arm Phase II of treatment for high-risk acute GVHD Response rate in eligible population was not well
understood—and 4 agents were promising
Cautions when you write the Cautions when you write the protocolprotocol
Treatment regimen – How closely does it mimic practice? Is it unnecessarily complex?
Supportive care Fussy (single institution habit)
requirements can prevent centers from participating
Too many restrictions can prevent patients from participating
Treatment regimen – How closely does it mimic practice? Is it unnecessarily complex?
Supportive care Fussy (single institution habit)
requirements can prevent centers from participating
Too many restrictions can prevent patients from participating
Collect only what you need forSafety; analysis; planning next trial
CautionsCautions when you write the when you write the protocolprotocol

BMT CTN Protocol 0302 BMT CTN Protocol 0302 Randomized Phase II Trial of Combined Randomized Phase II Trial of Combined
Therapy with Prednisone with Either MMF, Therapy with Prednisone with Either MMF, Etanercept, Pentostatin or Ontak for Newly Etanercept, Pentostatin or Ontak for Newly
Diagnosed AGVHDDiagnosed AGVHD
020406080
100120140160180200
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9 Q10 Q11
Actual
RevisedProjection
OriginalProjection
Looser eligibilityEasier start 72 not 48hWider Pred dose range

Writing a good protocolWriting a good protocol
How many patients are there that might be eligible to enroll? Who is treating them now and how?

Approximate Annual Number of US Approximate Annual Number of US Transplants Fulfilling Eligibility Criteria Transplants Fulfilling Eligibility Criteria
for BMT CTN Trialsfor BMT CTN Trials
0
500
1000
1500
2000
2500Not Enrolled Enrolled
Rapid accrual
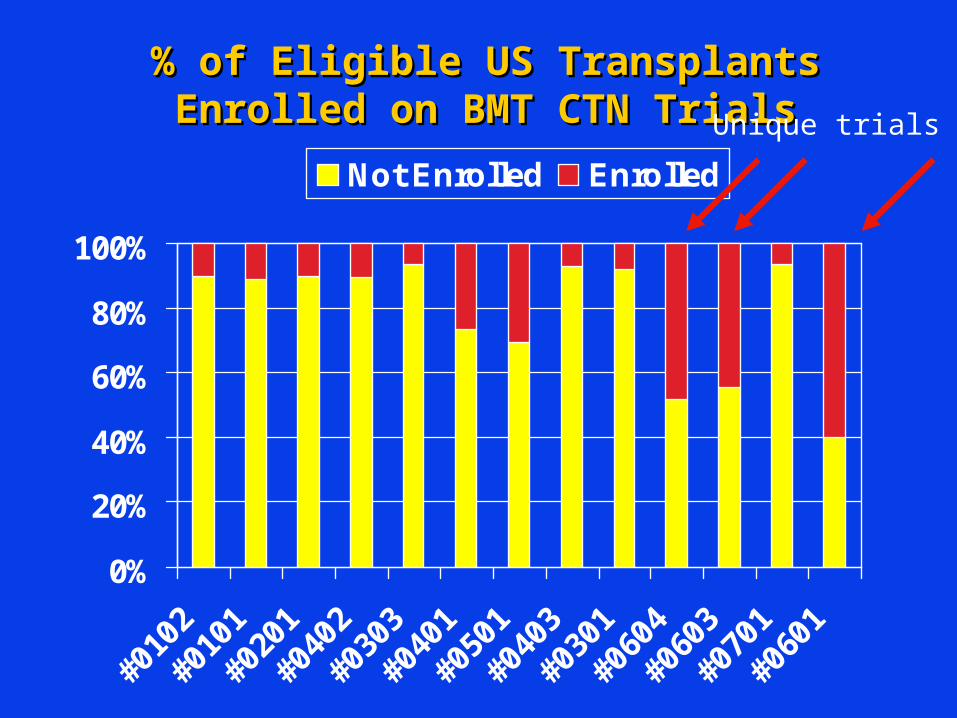
% of Eligible US Transplants % of Eligible US Transplants Enrolled on BMT CTN TrialsEnrolled on BMT CTN Trials
0%
20%
40%
60%
80%
100%
#010
2
#010
1
#020
1
#040
2
#030
3
#040
1
#050
1
#040
3
#030
1
#060
4
#060
3
#070
1
#060
1
Not Enrolled Enrolled
Unique trials

Understanding the Potential Patient Understanding the Potential Patient PopulationPopulation
Is the study feasible? Does accrual require capture of 10% [or
50%] of all transplants Number of centers Collaboration Timeline Accrual goal
Are there competing protocols?

CALGB 100104 CALGB 100104 Revlimid After AutotransplantRevlimid After Autotransplant
Monthly AccrualMonthly Accrual
0
5
10
15
20
25
30
Apr-
05
Jun-0
5
Aug-0
5
Oct-
05
Dec-0
5
Feb-0
6
Apr-
06
Jun-0
6
Aug-0
6
Oct-
06
Dec-0
6
Feb-0
7
Apr-
07
Jun-0
7
Aug-0
7
Oct-
07
Dec-0
7
Feb-0
8
Apr-
08
Jun-0
8
Aug-0
8
Oct-
08
Launched 18 months into accrual of BMT CTN 0102 (auto-auto vs auto-allo transplants) which targeted same patient population

CALGB 100104 CALGB 100104 Revlimid After AutotransplantRevlimid After Autotransplant
Monthly AccrualMonthly Accrual
0
5
10
15
20
25
30
Apr-
05
Jun-0
5
Aug-0
5
Oct-
05
Dec-0
5
Feb-0
6
Apr-
06
Jun-0
6
Aug-0
6
Oct-
06
Dec-0
6
Feb-0
7
Apr-
07
Jun-0
7
Aug-0
7
Oct-
07
Dec-0
7
Feb-0
8
Apr-
08
Jun-0
8
Aug-0
8
Oct-
08
Complete accrual 2009; results released early

Don’t design protocol to failDon’t design protocol to fail
Eligibility criteria Balance between maximizing accrual
and minimizing heterogeneity that confounds outcomes
Examine the impact of specific criteria

Easy enrollment
Unbiased population
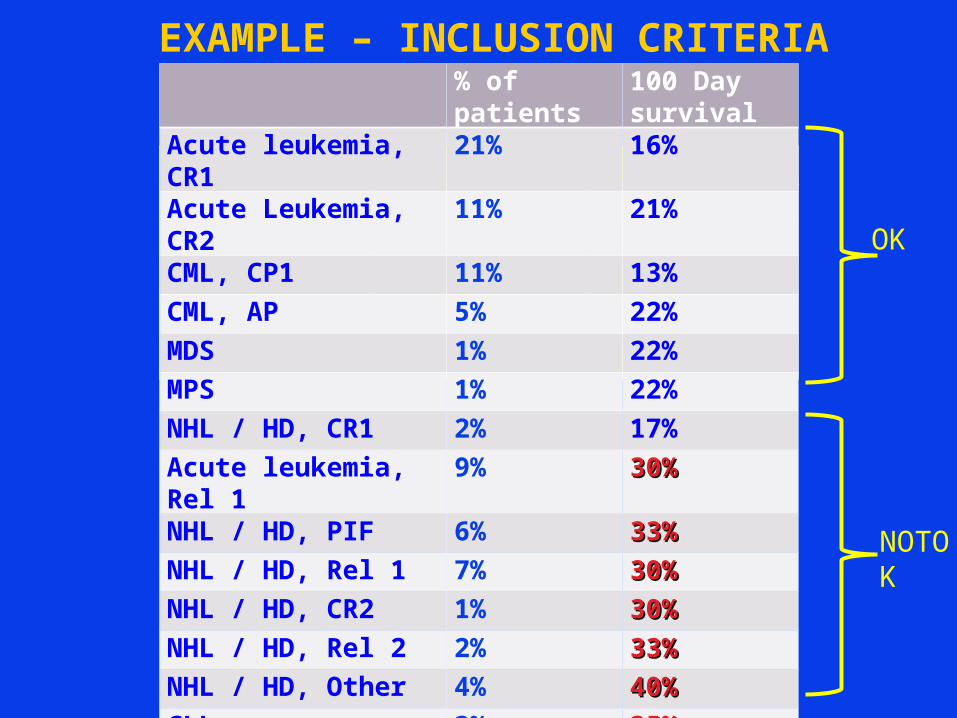
EXAMPLE – INCLUSION CRITERIA% of patients
100 Day survival
Acute leukemia, CR1
21% 16%
Acute Leukemia, CR2
11% 21%
CML, CP1 11% 13%CML, AP 5% 22%MDS 1% 22%MPS 1% 22%NHL / HD, CR1 2% 17%Acute leukemia, Rel 1
9% 30%30%
NHL / HD, PIF 6% 33%33%NHL / HD, Rel 1 7% 30%30%NHL / HD, CR2 1% 30%30%NHL / HD, Rel 2 2% 33%33%NHL / HD, Other 4% 40%40%CLL 3% 35%35%Multiple Myeloma 8% 40%40%
OK
NOTOK
Biological assignment trial-sometimes Biological assignment trial-sometimes necessary for a successful trialnecessary for a successful trial
Randomized trial: A random method is used to assign the treatment group, All patients must be eligible to receive
either treatment Balances unknowns that influence outcome
Biological assignment trial: Treatment group is assigned by availability of therapy HLA-identical Sib vs. Auto Sib vs. alternative donor Related vs. unrelated Related vs. auto
Biological assignment – Biological assignment – WHY?WHY?
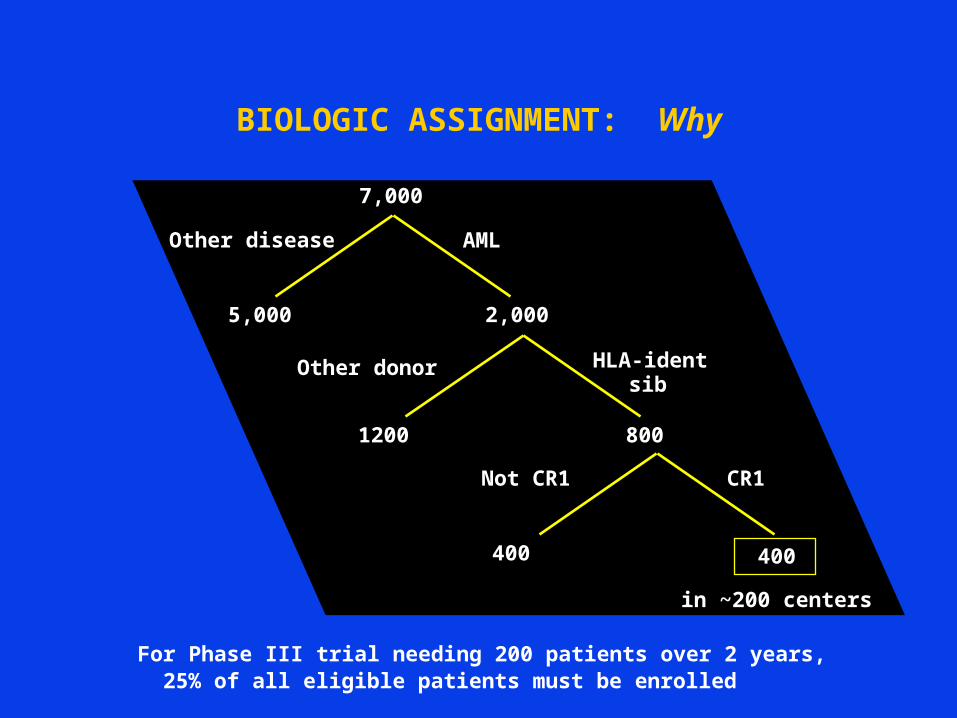
BIOLOGIC ASSIGNMENT: Why
For Phase III trial needing 200 patients over 2 years, 25% of all eligible patients must be enrolled
7,000
2,0005,000
AMLOther disease
8001200
HLA-ident sibOther donor
400
in ~200 centers
400
CR1Not CR1

BMT CTN 0102: BMT CTN 0102: Auto-auto vs auto-allo HCT for MyelomaAuto-auto vs auto-allo HCT for Myeloma
NEED a Sib donorNEED a Sib donor% With Donor
Trial DesignAnnual Accrual
Sample Size Required
Years of Accrual
20%Randomized trial
(Matched sibling donors only)
51 462 9.1
Biological Assignment (all patients) 254 720 2.8
25%Randomized trial
(Matched sibling donors only)
63 462 7.3
Biological Assignment (all patients) 254 615 2.4
30%Randomized trial
(Matched sibling donors only)
76 462 6.1
Biological Assignment (all patients) 254 550 2.2
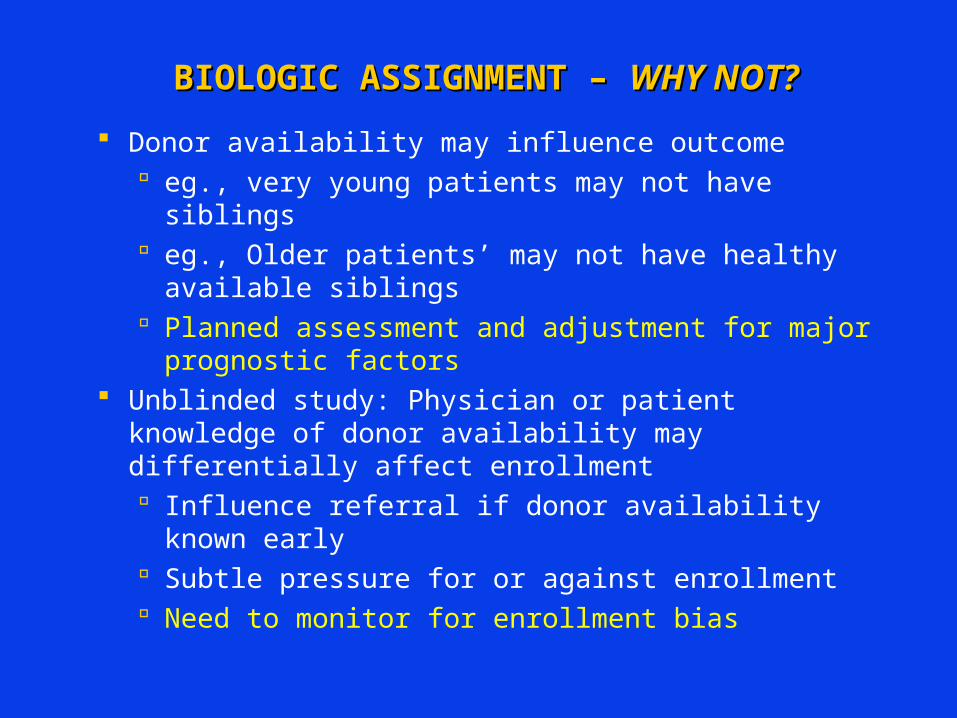
BIOLOGIC ASSIGNMENT – BIOLOGIC ASSIGNMENT – WHY NOT?WHY NOT?
Donor availability may influence outcome eg., very young patients may not have siblings eg., Older patients’ may not have healthy
available siblings Planned assessment and adjustment for major
prognostic factors Unblinded study: Physician or patient knowledge
of donor availability may differentially affect enrollment Influence referral if donor availability known
early Subtle pressure for or against enrollment Need to monitor for enrollment bias

Biologic Assignment: 0102Biologic Assignment: 0102
Number of Living SiblingsP value
0-1 ≥2
Age 0.001
≤55 45% 59%
>55 55% 41%
Race 0.3
Caucasian
82% 78%
Other 18% 22%

AFTER YOU OPEN THE PROTOCOLAFTER YOU OPEN THE PROTOCOL
Cheerleading – an essential element Personal communication is powerful
Get others to champion your protocol Acknowledge that accrual is difficult and
needs focused attention Figure out how to provide help Balance praise, cajoling, enticements,
appeal to higher calling
Accrual Plan
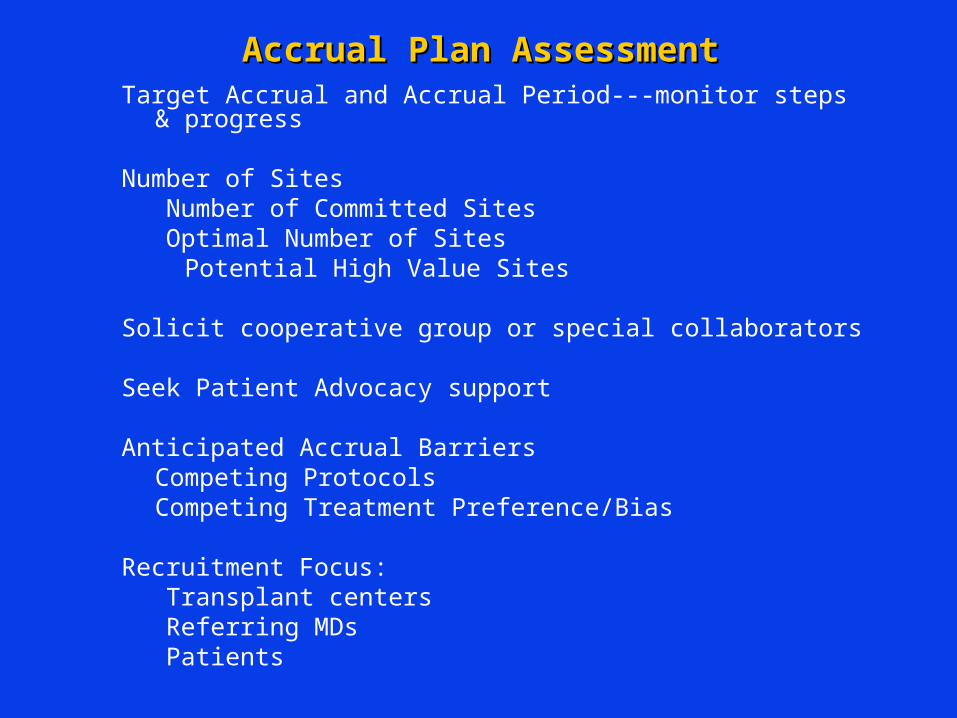
Accrual Plan AssessmentAccrual Plan AssessmentTarget Accrual and Accrual Period---monitor steps &
progress
Number of Sites Number of Committed SitesOptimal Number of Sites
Potential High Value Sites
Solicit cooperative group or special collaborators
Seek Patient Advocacy support
Anticipated Accrual BarriersCompeting ProtocolsCompeting Treatment Preference/Bias
Recruitment Focus:Transplant centersReferring MDsPatients
Never forgetAvoid the most annoying CROs
Tend to press detail over quality
If they don’t like the trial, they won’t enrollWork on inclusiveness prior to openingAnticipate accrual barriers
Pay enough to cover the costsSlow accrual is more costly than more $$/patient
Don’t be complacent; Ongoing communication helps. Guilt helps too

AFTER YOU OPEN THE PROTOCOLAFTER YOU OPEN THE PROTOCOL
Pay attention Identify problems early and correct them
quickly
Trial success is collaborative Listen to centers—before & after trial opens
Limit amendments Only those needed for safety or accrual

Confirmatory trials are essential !!!
-Reduce likelihood of false +
-Verify original results
-Expands the number of observations, perhaps allowing subgroup effects to be seen in combined analysis (Meta-analysis)
BUT-- only one trial doesn’t teach us the truth
Related Documents











