ORIGINAL ARTICLE Improvement in the visibility of colorectal polyps by using blue laser imaging Naohisa Yoshida, MD, PhD, 1 Takashi Hisabe, MD, PhD, 2 Ryohei Hirose, MD, 1 Kiyoshi Ogiso, MD, 1 Yutaka Inada, MD, PhD, 1 Hideyuki Konishi, MD, PhD, 1 Nobuaki Yagi, MD, PhD, 1 Yuji Naito, MD, PhD, 1 Yoshiaki Aomi, MD, 2 Kazeo Ninomiya, MD, 2 Go Ikezono, MD, 2 Masaaki Terasawa, MD, 2 Kenshi Yao, MD, PhD, 2 Toshiyuki Matsui, MD, PhD, 2 Akio Yanagisawa, MD, PhD, 3 Yoshito Itoh, MD, PhD 1 Kyoto, Fukuoka, Japan Background: Fujifilm developed blue laser imaging (BLI) via a laser light source with a narrow-band light obser- vation function. It has a brighter BLI bright mode for tumor detection. Objective: To investigate whether the BLI bright mode can improve the visibility of colorectal polyps compared with white light (WL). Design: We studied 100 colorectal polyps (protruding, 42; flat, 58; size, 2–20 mm) and recorded videos of the polyps by using the BLI bright mode and WL at Kyoto Prefectural University of Medicine and Fukuoka Chikushi University Hospital. The videos were evaluated by 4 expert endoscopists and 4 nonexperts. Each endoscopist eval- uated the videos in a randomized order. Each polyp was assigned a visibility score from 4 (excellent visibility) to 1 (poor visibility). Setting: Japanese academic units. Main Outcome Measurements: The visibility scores in each mode and their relationship to the clinical charac- teristics were analyzed. Results: The mean visibility scores of the BLI bright mode were significantly higher than those of WL for both experts and nonexperts (experts, 3.10 0.95 vs 2.90 1.09; P Z .00013; nonexperts, 3.04 0.94 vs 2.78 1.03; P ! .0001). For all nonexperts, the visibility scores of the BLI bright mode were significantly higher than those of WL; however, these scores were significantly higher in only 2 experts. For experts, the mean visibility scores of the BLI bright mode was significantly higher than those of WL for flat polyps, neoplastic polyps, and polyps located on the left side of the colon and the rectum. Limitations: Small sample size and review of videos. Conclusions: Our study showed that polyps were more easily visible with the BLI bright mode compared with WL. (Clinical trial registration number: UMIN000013770.) (Gastrointest Endosc 2015;-:1-8.) Colorectal cancer is a common GI malignancy in the United States, Europe, and Japan. According to the adenoma-carcinoma sequence concept, most colorectal cancers are thought to arise from preexisting adenomas. 1 Therefore, adenomatous polyps should be detected and resected by using endoscopic techniques such as endoscopic mucosal resection (EMR) and endoscopic submucosal dissection. 2-4 Colonoscopy is considered to be an effective examination for detecting colorectal neoplastic lesions. However, a meta-analysis of 6 studies found that the miss rate for polyps of any size was 22% with white light (WL) observation. 5 The reasons behind Abbreviations: BLI, blue laser imaging; FICE, flexible spectral imaging color enhancement; IEE, image-enhanced endoscopy; NBI, narrow- band imaging; WL, white light. DISCLOSURE: Dr Itoh received support from AstraZeneca Co, Ltd, Eisai Co, Ltd; Otsuka Pharmaceutical Co, Ltd; MSD KK; Dainippon Sumitomo Pharma Co, Ltd; Chugai Pharmaceutical Co, Ltd; FUJIFILM Medical Co, Ltd; Merck Serono Co; and Bristol-Myers KK. Dr Yagi received support from AstraZeneca Co, Ltd; Eisai Co, Ltd; Otsuka Pharmaceutical Co, Ltd; MSD KK; Dainippon Sumitomo Pharma Co, Ltd; Chugai Pharmaceutical Co, Ltd; Fujifilm Medical Co, Ltd; and Merck Serono Co. Dr Naito received support from Otsuka Pharmaceutical Co, Ltd (footnotes continued on last page of article) www.giejournal.org Volume -, No. - : 2015 GASTROINTESTINAL ENDOSCOPY 1 FLA 5.2.0 DTD ĸ YMGE9130_proof ĸ 7 April 2015 ĸ 4:13 pm

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ORIGINAL ARTICLE
Abbrcolorband
DISCCo, LPharLtd;
www
Improvement in the visibility of colorectal polyps by using bluelaser imaging
eviatioenhaimagi
LOSURtd; Otsuma CoMerck
.giejo
Naohisa Yoshida, MD, PhD,1 Takashi Hisabe, MD, PhD,2 Ryohei Hirose, MD,1 Kiyoshi Ogiso, MD,1
Yutaka Inada, MD, PhD,1 Hideyuki Konishi, MD, PhD,1 Nobuaki Yagi, MD, PhD,1 Yuji Naito, MD, PhD,1
Yoshiaki Aomi, MD,2 Kazeo Ninomiya, MD,2 Go Ikezono, MD,2 Masaaki Terasawa, MD,2
Kenshi Yao, MD, PhD,2 Toshiyuki Matsui, MD, PhD,2 Akio Yanagisawa, MD, PhD,3 Yoshito Itoh, MD, PhD1
Kyoto, Fukuoka, Japan
Background: Fujifilm developed blue laser imaging (BLI) via a laser light source with a narrow-band light obser-vation function. It has a brighter BLI bright mode for tumor detection.
Objective: To investigate whether the BLI bright mode can improve the visibility of colorectal polyps comparedwith white light (WL).
Design: We studied 100 colorectal polyps (protruding, 42; flat, 58; size, 2–20 mm) and recorded videos of thepolyps by using the BLI bright mode and WL at Kyoto Prefectural University of Medicine and Fukuoka ChikushiUniversity Hospital. The videos were evaluated by 4 expert endoscopists and 4 nonexperts. Each endoscopist eval-uated the videos in a randomized order. Each polyp was assigned a visibility score from 4 (excellent visibility) to 1(poor visibility).
Setting: Japanese academic units.
Main Outcome Measurements: The visibility scores in each mode and their relationship to the clinical charac-teristics were analyzed.
Results: The mean visibility scores of the BLI bright mode were significantly higher than those of WL for bothexperts and nonexperts (experts, 3.10 � 0.95 vs 2.90 � 1.09; P Z .00013; nonexperts, 3.04 � 0.94 vs 2.78 � 1.03;P! .0001). For all nonexperts, the visibility scores of the BLI bright mode were significantly higher than those ofWL; however, these scores were significantly higher in only 2 experts. For experts, the mean visibility scores of theBLI bright mode was significantly higher than those of WL for flat polyps, neoplastic polyps, and polyps located onthe left side of the colon and the rectum.
Limitations: Small sample size and review of videos.
Conclusions: Our study showed that polyps were more easily visible with the BLI bright mode compared withWL. (Clinical trial registration number: UMIN000013770.) (Gastrointest Endosc 2015;-:1-8.)
Colorectal cancer is a common GI malignancy in theUnited States, Europe, and Japan. According to theadenoma-carcinoma sequence concept, most colorectalcancers are thought to arise from preexisting adenomas.1
Therefore, adenomatous polyps should be detected andresected by using endoscopic techniques such as
ns: BLI, blue laser imaging; FICE, flexible spectral imagingncement; IEE, image-enhanced endoscopy; NBI, narrow-ng; WL, white light.
E: Dr Itoh received support from AstraZeneca Co, Ltd, Eisaika Pharmaceutical Co, Ltd; MSD KK; Dainippon Sumitomo
, Ltd; Chugai Pharmaceutical Co, Ltd; FUJIFILM Medical Co,Serono Co; and Bristol-Myers KK. Dr Yagi received support
urnal.org
FLA 5.2.0 DTD � YMGE9130_pr
endoscopic mucosal resection (EMR) and endoscopicsubmucosal dissection.2-4 Colonoscopy is considered tobe an effective examination for detecting colorectalneoplastic lesions. However, a meta-analysis of 6 studiesfound that the miss rate for polyps of any size was 22%with white light (WL) observation.5 The reasons behind
from AstraZeneca Co, Ltd; Eisai Co, Ltd; Otsuka Pharmaceutical Co,Ltd; MSD KK; Dainippon Sumitomo Pharma Co, Ltd; ChugaiPharmaceutical Co, Ltd; Fujifilm Medical Co, Ltd; and Merck SeronoCo. Dr Naito received support from Otsuka Pharmaceutical Co, Ltd
(footnotes continued on last page of article)
Volume -, No. - : 2015 GASTROINTESTINAL ENDOSCOPY 1
oof � 7 April 2015 � 4:13 pm

Detectability of colorectal polyps by using BLI Yoshida et al
the high miss rate were considered to be the quality ofbowel preparation, lesion characteristics (location, number,morphology, and size), and the endoscopist’s experience,especially insertion and withdrawal techniques.5 Recently,image-enhanced endoscopy (IEE) has been used to diagnoseGI tumors. This method is very different from conventionalchromoendoscopy and requires only the push of a buttonwithout the need to use a dye solution.
In IEE such as narrow-band imaging (NBI) (OlympusMedical Co, Tokyo, Japan), flexible spectral imaging colorenhancement (FICE) (Fujifilm Co, Tokyo, Japan), and auto-fluorescence imaging (Olympus Medical Co, Tokyo,Japan), many clinical studies, including randomized,controlled trials, have reported an improvement in thedetection rate in colonoscopy.6-11 However, the efficacyof these IEEs for tumor detection remains controversial.Recently, Fujifilm developed a new endoscope systemwith a semiconductor laser light source. The system has2 types of lasers with wavelengths of 410 nm and 450nm. It enables blue laser imaging (BLI) via narrow-bandlight observation.12-15 There are 2 modes such as BLI andBLI bright mode. The BLI mode is useful for magnified ob-servations and enables the acquisition of mucosal surfaceinformation about vascular and surface patterns. On theother hand, the BLI bright mode is brighter than the regu-lar BLI mode and is intended to improve the detection ofGI neoplastic lesions.
We believe that polyp detectability depends on manyfactors, and one of the most important factors is polyp vis-ibility. It is important to determine whether a new IEE canimprove polyp visibility. However, there are no reportsabout the visibility of colorectal polyps by using BLI. Inthis study, we aimed to investigate whether the BLI brightmode can improve the visibility of colorectal polypscompared with WL by using recorded polyp videos.
MATERIALS AND METHODS
This open, prospective, multicenter study was conduct-ed at the Department of Molecular Gastroenterology andHepatology, Kyoto Prefectural University of Medicine,and at the Department of Gastroenterology, Fukuoka Uni-versity Chikushi Hospital. We examined consecutive colo-rectal polyps and captured videos of the polyps by usingthe BLI mode, the BLI bright mode, and WL at Kyoto Pre-fectural University of Medicine from April 2013 toNovember 2013. The inclusion criterion was the presenceof a colorectal polyp between 2 and 20 mm in size that hadbeen detected by routine colonoscopy with the BLI brightmode or WL. A single expert (N.Y.) recorded 3 videos foreach polyp by using the BLI mode, the BLI bright mode,and WL. Each video included a range of 5 cm proximalfrom the polyp to 5 cm distal from the polyp. The evalua-tion of the visibility of the polyps was performed by usingthe following visibility scores: 4, excellent visibility (easily
2 GASTROINTESTINAL ENDOSCOPY Volume -, No. - : 2015
FLA 5.2.0 DTD � YMGE9130_pr
detectable); 3, good visibility (detectable with carefulobservation); 2, fair visibility (hardly detectable withoutcareful examination); and 1, poor visibility (not detectablewithout repeated careful examination) (Figs. 1 and 2;Supplemental Video 1, available online at www.giejournal.org). All videos were of the same polyprecorded under the same conditions to the best of ourabilities. We paid particular attention to the followingconditions: the presence of fluid, the amount ofinsufflation, the location of folds, and the withdrawalspeed. We excluded cases with noticeable variations inthe afore mentioned conditions. Videos were excludedwhen more than 2 polyps were present in the same movieclip. Videos with a Boston Bowel Preparation Score lessthan 2 were also excluded. Cases involving the presenceof recurrent lesions after the previous EMR and those ofadvanced colorectal cancer were also excluded. With re-gard to the morphology, polyps were divided into protrud-ing polyps and flat polyps in accordance with the Parisclassification.16 The size of a polyp was defined by itsmaximum diameter and was calculated relative to thesize of the injection needle and biopsy forceps.Histopathological diagnosis was performed by usingendoscopically resected specimens or biopsy specimens.Polyps were divided into neoplastic or non-neoplastic cat-egories based on the histopathological diagnosis. Thepolyp locations were divided into 3 segments, whichincluded the right side of the colon (from the cecum tothe transverse colon), the left side of the colon (from thedescending colon to the sigmoid colon), and the rectum.
All of the sets of videos during the study period werecollected. The evaluation was performed by 8 endoscopistswho had not viewed any of these videos before this study.Of the 8 endoscopists who participated in the study, 4were classified as nonexperts (had performed!5000 colo-noscopies) and 4 were classified as experts (hadperformed R5000 colonoscopies). All the videos wereviewed in random order. For example, the WL video ofpolyp A was shown as movie number 1, followed by aNBI video of polyp B. Participants assigned a visibility scoreto each polyp. The relationship between the visibilityscores and clinical characteristics including polyp location,size, histopathological diagnosis, and morphology was alsoinvestigated. The rates of polyps with poor visibility (scores1 or 2) were also compared for BLI bright mode and WLvideos.
With regard to colonoscopy preparation, patients fol-lowed a low-residue diet and took sodium picosulfate 1day before the examination; all patients also received 2 Lof polyethylene glycol solution (Niflec; Ajinomoto PharmaCo, Ltd, Tokyo, Japan) in the morning on the day of theexamination.
All patients provided written informed consent to un-dergo this study. The study was approved by the institu-tional review board and the ethics committees of KyotoPrefectural University of Medicine. In addition, this study
www.giejournal.org
oof � 7 April 2015 � 4:13 pm

print&web4C=FPO
Figure 1. Colorectal polyp visibility scores with the BLI bright mode and white light. A, BLI bright mode: visibility score, 4. B, BLI bright mode: visibilityscore: 3. C, BLI bright mode: visibility score, 2. D, BLI bright mode: visibility score, 1. E, WL: visibility score, 4. F, WL: visibility score, 3. G, WL: visibilityscore, 2. H, WL: visibility score, 1. BLI, blue laser imaging; WL, white light.
Yoshida et al Detectability of colorectal polyps by using BLI
was also performed in accordance with the World MedicalAssociation Helsinki Declaration and was registered in theUniversity Hospital Medical Information Network ClinicalTrials Registry (UMIN-CTR) as number UMIN000013770.
Histopathological diagnosisThe tumor specimens were obtained by endoscopic
biopsy, EMR, and endoscopic submucosal dissection.Thereafter, they were fixed with 10% formalin and wereevaluated histopathologically. Histopathological diagnosiswas performed by 1 clinical pathologist (A.Y.) accordingto the World Health Organization classification.17 Sessileserrated adenomas/polyps were defined as neoplasticlesions in this study.
BLI deviceThe BLI system used in this study was described in pre-
vious reports.12,13 In brief, this new endoscope system usesa semiconductor laser as the light source and has a narrow-band light observation function called BLI without acustomized optical filter. The system consists of the LL-4450 light source, the VP-4450HD processor, and a specialscope series. It has 2 types of lasers with 410-nm and 450-nm wavelengths. Both bandwidths are less than 2 nmcompared with the bandwidth of NBI (30 nm).12,13
The laser with a 450-nm wavelength makes phosphor irra-diate with an illumination similar to that produced by a
www.giejournal.org
FLA 5.2.0 DTD � YMGE9130_pr
xenon lamp. The combination of strong laser light with awavelength of 450 nm and fluorescent light provides anillumination that is almost equivalent to that of WL. TheBLI mode is produced through the combination of stronglaser light with a wavelength of 410 nm, weak laser lightwith a wavelength of 450 nm, and fluorescent light. TheBLI mode is useful for acquiring mucosal surface informa-tion such as surface blood vessels and surface structurepatterns. The BLI bright mode is set such that the powerof a laser with a wavelength of 450 nm is increased. Thismode is brighter than the BLI mode and is expected tobe useful in tumor detection.
Statistical assessmentIn a pilot study of the visibility of 151 colorectal polyps
by a single expert endoscopist, the BLI bright modeachieved visibility scores superior to those with WL in 69polyps (45.7%). By using a sign test, the a error was foundto be 5%, and the b error was found to be 80%. Thus, theminimum sample size was calculated to be 24. However,the pilot study was performed by only 1 endoscopist,and we decided to use a sample size of 90. Statisticalanalyses were performed by using the Mann-Whitney Utest, Wilcoxon signed rank test with Bonferroni correction,and the c2 test (SPSS version 22.0 for Windows; IBMJapan, Ltd, Tokyo, Japan). Continuous variables such aspatient age and tumor size were analyzed by using
Volume -, No. - : 2015 GASTROINTESTINAL ENDOSCOPY 3
oof � 7 April 2015 � 4:13 pm

print&
web4C=FPO
Figure 2. Case presentation. A, Colonic polyp, superficial, 15 mm on the cecum. WL: visibility score, 2. B, BLI bright mode: visibility score, 4. C, BLImode: visibility score, 3. BLI, blue laser imaging; WL, white light.
TABLE 1. Clinical characteristics of 100 colorectal polyps
No. of polyps 100
No. of patients 70
Male/female, no. 40/30
Detectability of colorectal polyps by using BLI Yoshida et al
the Mann-Whitney U test. The 4 phases of the evaluation(visibility scores 1-4) were used as ordered categorical vari-ables; comparisons between methods (WL, BLI, and BLIbright mode) were performed with the Wilcoxon signedrank test with Bonferroni correction. P! .05 was consid-ered statistically significant.
Median age, y (range) 67.9 (25–92)
Polyp size, mm (range) 9.7 (2–20)
Location (right sided:left sided:rectum) 52:33:15
Morphology (protruded or flat) 42:58
Histopathological diagnosis
Non-neoplastic:neoplastic 17:83
(SSAP:HP:Ad:M:SM) (2:15:64:14:5)
Right-sided, From the cecum to the transverse colon; left-sided, from the descendingcolon to the sigmoid colon; SSAP, sessile serrated adenoma/polyp; HP, hyperplasticpolyp; Ad, adenoma; M, intramucosal cancer, SM, submucosal cancer.
RESULTS
A total of 115 consecutive polyps were included inthe study. Fifteen polyps were excluded: 6 polyps hada different viewing angle and withdrawal speed betweenWL, BLI, and BLI bright mode. Six videos had more than2 polyps detected in the video. Three videos had a Bos-ton Bowel Preparation score less than 2. A total of 100colorectal polyps in 70 patients were investigated inthis study. There were 42 protruding polyps and 58flat polyps (Table 1). Fifty-two polyps were located inthe right side of the colon, 33 in the left side of the co-lon, and 15 in the rectum. The mean polyp size was9.7 mm (range 2–20 mm); 17 were non-neoplasticpolyps and 83 were neoplastic polyps. The mean visibil-ity scores of the BLI bright mode were significantlyhigher than those of WL for both expert (3.10 � 0.95vs 2.90 � 1.09, P Z .00013) and nonexpert (3.04 �0.94 vs 2.78 � 1.03, P Z 1.5 � 10�9) endoscopists. Incontrast, the BLI mode only improved the visibilityscores of nonexpert endoscopists (Table 2).
4 GASTROINTESTINAL ENDOSCOPY Volume -, No. - : 2015
FLA 5.2.0 DTD � YMGE9130_pr
The visibility scores of WL, the BLI bright mode, and theBLI mode from each endoscopist are shown in Table 3. Forall nonexperts, the visibility scores of the BLI bright modewere significantly higher than those of WL. However, foronly 2 experts, the visibility scores of the BLI brightmode were significantly higher than those of WL. Therewere significant differences between the WL and BLImode scores for 4 of the 8 endoscopists.
The mean visibility scores of WL, the BLI bright mode,and the BLI mode of experts in terms of various clinicalcharacteristics including location, size, histopathologicaldiagnosis, and morphology are shown in Table 4. The
www.giejournal.org
oof � 7 April 2015 � 4:13 pm

TABLE 2. Mean colorectal polyp visibility scores with WL, BLI bright mode, and BLI mode for experts and nonexperts
WL BLI bright mode BLIWL vs BLI brightmode, P value WL vs BLI, P value
Expert 2.90 � 1.09 3.10 � 0.95 3.02 � 1.03 .00013 NS
Nonexpert 2.78 � 1.03 3.04 � 0.94 2.94 � 1.03 1.5 � 10�9 .002
WL, White light; BLI, blue laser imaging; NS, not significant.
Expert
BLI bright
BLI bright
28 (7.0%)
45 (11.3%) 74 (18.5%)
76 (19.0%)
78 (19.5%)
51 (12.8%)
50 (12.5%)
80 (20.0%)
60 (15.0%)
39 (9.8%)
58 (14.5%)
62 (15.5%)
123 (30.8%)
109 (27.2%)
105 (26.3%)
165 (41.2%)
151 (37.8%)
143 (35.8%)
173 (43.2%)
172 (43.0%)
157 (39.2%)
145 (36.2%)
141 (35.2%)
115 (28.7%)
BLI
BLI
WL
WL
Nonexpert
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Visibility score 1 32 4
print&
web4C=FPO
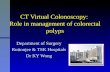
Figure 3. The ratio of visibility score in expert and nonexpert. BLI, Blue laser imaging; WL, white light.
Yoshida et al Detectability of colorectal polyps by using BLI
visibility scores of the BLI bright mode were significantlyhigher than those of WL for the left side of the colonand rectal lesions, any polyp size (both R10 and !10 mm polyp groups), neoplastic polyps, and flat polyps.The mean visibility scores of WL, BLI bright mode, andBLI mode of nonexperts in terms of the various clinicalcharacteristics are shown in Table 4. The visibility scoresof the BLI bright mode were significantly higher thanthose of WL for all the factors. The rates of poor visibility(score 1 or 2) of WL and BLI bright mode for eachendoscopist were analyzed (Fig. 3). For all 8endoscopists, the mean rates of poor visibility weresignificantly higher in WL (35.0%) than the BLI brightmode (24.3%). For the 4 nonexperts, the rates of poorvisibility of the BLI bright mode were significantly lowerthan those of WL. However, for only 2 experts, the ratesof poor visibility of WL and BLI bright mode weresignificantly different. BLI bright mode improved flatpolyp visibility for both experts and nonexperts.Interestingly, BLI bright mode also improved protrudingpolyp visibility of nonexperts. There were 3 lesions thatmore than 4 endoscopists rated a visibility score of 1 forall 3 modes. Two lesions were in the colon behind thefold, and 1 lesion was in the rectum. The first lesion wasa 3-mm protruding polyp in the ascending colon, the sec-ond polyp was an 18-mm protruding polyp also in the
www.giejournal.org
FLA 5.2.0 DTD � YMGE9130_pr
ascending colon, and the third polyp was a 12-mm flatpolyp in the rectum.
DISCUSSION
In the current study, we showed that BLI improved thevisibility of colorectal polyps compared with WL. Thus, ourstudy showed that the visibility of polyps was better underthe BLI bright mode compared with WL. Additionally, agreater improvement in visibility was observed in nonex-perts compared with experts.
Our previous multicenter study showed that the diag-nostic accuracy of BLI magnification of 104 neoplastic colo-rectal polyps was 74.0% (77/104), which was similar to thatof NBI magnification (77.8%).12 The concordance ratebetween BLI and NBI magnification in a published NBIclassification was 74.0%.18 Another study performed byour group showed that the overall diagnostic accuracy ofBLI with magnification for 314 neoplastic polyps andnon-neoplastic polyps was 84.3%.13 Additionally, thediagnostic accuracy of BLI without magnification fordifferentiating between neoplastic and non-neoplasticpolyps smaller than 10 mm in diameter was 95.2%, whichwas greater than that of WL (83.2%). Thus, BLI with orwithout magnification could predict the histopathological
Volume -, No. - : 2015 GASTROINTESTINAL ENDOSCOPY 5
oof � 7 April 2015 � 4:13 pm

TABLE 3. Mean visibility scores with WL, BLI bright mode, and BLI mode for each endoscopist
WL BLI bright mode BLIWL vs BLI brightmode, P value WL vs BLI, P value
Nonexpert A 2.50 � 1.1 2.72 � 0.3 2.57 � 1.1 .019 NS
Nonexpert B 2.63 � 1.1 2.89 � 1.0 2.69 � 1.1 .014 NS
Nonexpert C 3.20 � 0.8 3.40 � 0.7 3.38 � 0.7 .0071 .020
Nonexpert D 2.78 � 0.8 3.15 � 0.6 3.11 � 0.7 6.0 � 10�6 .00040
Expert A 2.90 � 1.0 3.16 � 0.9 3.25 � 0.9 .0090 .00061
Expert B 2.97 � 1.0 3.33 � 0.8 3.24 � 0.9 .00030 .0030
Expert C 2.70 � 1.1 2.89 � 1.0 2.72 � 1.1 NS NS
Expert D 3.01 � 1.0 3.03 � 0.8 2.87 � 0.9 NS NS
WL, White light; BLI, blue laser imaging; NS, not significant.
Detectability of colorectal polyps by using BLI Yoshida et al
diagnosis and invasion depth of colorectal neoplasms. Theprevious study also showed that endoscopic images of ves-sels and surface patterns obtained by using BLI magnifica-tion were different from those obtained with NBImagnification.12 This was likely related to differences inwavelength, bandwidth, and power. The bandwidths ofthe BLI and NBI systems used in that study were 2 nmand 30 nm, respectively.13 Moreover, the wavelengthsused in BLI were 410 nm and 450 nm, whereas thoseused in NBI were 415 nm and 540 nm. On uppergastroscopy, Miyaki et al14 reported the usefulness of aunique computer-based analysis system for early gastriccancer with clear BLI images.
With regard to endoscopist experience, greater improve-ment in visibility was observed in nonexperts comparedwith experts. Our group believes that the visibility of colo-rectal polyps is related to various clinical characteristics. Inthe current study, the differences in mean visibility scoresbetween WL and the BLI mode were significant for 4 of 8endoscopists, although those between WL and the BLIbright mode were significant for 6 of 8 endoscopists. Fornonexperts, the mean visibility scores for all clinical charac-teristics including location, size, histopathological diagnosis,and morphology in the BLI bright mode were significantlyhigher than those in WL, although some scores in the BLImode were not significantly higher than those in WL. For ex-perts, the scores for some characteristics (right-sidedpolyps, non-neoplastic polyps, protruding polyps) in theBLI-bright mode were not higher than those in WL. Apossible reason for this was that the visibility scores of pro-truding polyps were already high with WL, and, therefore,the possible improvement with the BLI bright mode wasminimal. In addition, a small number of non-neoplastic le-sions (NZ 17) may be responsible for this finding. Further-more, the right side of the colon is wider than the left side.Therefore, greater brightness and resolution may be neededto improve visibility in such cases.
A recent meta-analysis revealed that there was no signif-icant difference in the adenoma detection rate betweenNBI and WL.19 Furthermore, another systematic review
6 GASTROINTESTINAL ENDOSCOPY Volume -, No. - : 2015
FLA 5.2.0 DTD � YMGE9130_pr
including 8 randomized, controlled studies showed thatNBI did not improve the detection of colorectal polypscompared with WL.20 However, the withdrawal time is animportant confounding factor that may affect the validityof these studies. Withdrawal time is a difficult endoscopicfactor to regulate because we are not able to control thespeed of the colonoscope over a whole colonoscopicobservation, compared with video studies when only asmall segment of the whole colonoscopic observation isnormally recorded.
Certain studies reported longer withdrawal times forNBI observation because the NBI image was dark at acertain distance away from the polyps. Our study showedimproved visibility with the BLI bright mode comparedwith the BLI mode. Two randomized, controlled studieswith FICE showed that any improvement in FICE was notcorrelated with the adenoma detection rate.9,10 However,NBI and FICE systems have recently been enhanced. Abrighter NBI system named Elite in Japan (Olympus Co,Tokyo, Japan) or Exera III in America and Europe(Olympus Co) has been developed and may potentiallyimprove tumor detection.21 Similarly, the BLI brightmode may also potentially improve tumor detectionbecause of its higher resolution and brightness. Morestudies should be done to see whether higher visibilitywill lead to an improvement in overall polyp detection.
There were some limitations in our study. The samplesize was small, and therefore there may be some selec-tion bias. Additionally, it may limit the potential formultivariate analysis to show important factors for polypvisibility and/or risk factors for missed polyps. This studyinvolved the review of videos and may not reflect real-time prospective measures of detection (ie, during thetime of the procedure) because polyp detection isaffected not only by visibility, but also by various otherfactors. The study was conducted only in Japanese aca-demic centers and may lack generalizability in otherpractices around the world.
In conclusion, our study showed the visibility of the BLIbright mode was significantly better than that of WL for
www.giejournal.org
oof � 7 April 2015 � 4:13 pm

TABLE 4. Mean visibility scores of each clinical characteristic with WL, BLI bright mode, and BLI mode for experts and nonexperts
Nonexperts WL vs BLIbright mode
Experts WL vs BLIbright mode
Nonexperts WL vs BLI,P value
Experts WL vs BLI,P value
Right sided .0032 NS .038 NS
Left sided, rectum 1.4 � 10�7 0.00032 .045 .019
%10 mm 0.000028 0.017 .0056 NS
!10 mm 0.00025 0.0049 NS NS
Neoplastic 2.9 � 10�7 0.0013 .0015 NS
Non-neoplastic 0.0031 NS NS NS
Protruding 0.0050 NS NS NS
Flat 9.5 � 10�7 0.0015 .0030 .0047
WL, White light; BLI, blue laser imaging; right sided, from the cecum to the transverse colon; NS, not significant; left sided, from the descending colon to the sigmoid colon.
Yoshida et al Detectability of colorectal polyps by using BLI
both expert and nonexpert endoscopists. With respect totumor location (left side of the colon and rectal polyps), tu-mor size (any polyp size), histology (neoplastic polyps),and morphology (flat polyps), the visibility of the BLIbright mode for experts was significantly higher than thatof WL. On the other hand, the visibility of the BLI brightmode for nonexperts was significantly higher than that ofWL in all of the factors just listed. More studies shouldbe done to determine whether higher visibility will leadto a lower polyp miss rate.
ACKNOWLEDGMENTS
The authors thank Kewin Tien Ho Siah and all membersof the Department of Molecular Gastroenterology andHepatology, Kyoto Prefectural University of Medicine, forhelping with this study, and all members of the Depart-ment of Gastroenterology, Fukuoka University ChikushiHospital. The authors thank Dr Hironori Yamamoto andDr Mototsugu Kato for the study design and also KuboMasahiro and all other members who assisted in all proce-dures related to the Fujifilm LASEREO system.
REFERENCES
1. Vogelstein B, Fearon ER, Hamilton SR, et al. Genetic alterations duringcolorectal-tumor development. N Engl J Med 1988;319:525-32.
2. Saito Y, Fukuzawa M, Matsuda T, et al. Clinical outcome of endoscopicsubmucosal dissection versus endoscopic mucosal resection of largecolorectal tumors as determined by curative resection. Surg Endosc2010;24:343-52.
3. Kudo S, Tamegai Y, Yamano H, et al. Endoscopic mucosal resection ofthe colon: the Japanese technique. Gastrointest Endosc Clin N Am2001;11:519-35.
4. Yoshida N, Naito Y, Yagi N, et al. Safe procedure in endoscopic submu-cosal dissection for colorectal tumors focused on preventing complica-tions. World J Gastroenterol 2010;16:1688-95.
5. Su MY, Hsu CM, Ho YP, et al. Comparative study of conventionalcolonoscopy, chromoendoscopy, and narrow-band imaging systemsin differential diagnosis of neoplastic and nonneoplastic colonicpolyps. Am J Gastroenterol 2006;101:2711-6.
www.giejournal.org
FLA 5.2.0 DTD � YMGE9130_pr
6. Kaltenbach T, Friedland S, Soetikno R. A randomised tandem colonos-copy trial of narrow band imaging versus white light examination tocompare neoplasia miss rates. Gut 2008;57:1406-12.
7. Rastogi A, Bansal A, Wani S, et al. Narrow-band imaging colonoscopy–apilot feasibility study for the detection of polyps and correlation of sur-face patterns with polyp histologic diagnosis. Gastrointest Endosc2008;67:280-6.
8. East JE, Suzuki N, Guenther T, et al. Narrow band imaging (NBI) for ad-enoma detection in high risk patients: a randomized, controlled trial.Colorectal Dis 2012;14:e771-8.
9. Aminalai A, Rösch T, Aschenbeck J, et al. Live image processing doesnot increase adenoma detection rate during colonoscopy: a ran-domized comparison between FICE and conventional imaging (Ber-lin Colonoscopy Project 5, BECOP-5). Am J Gastroenterol 2010;105:2383-8.
10. Pohl J, Lotterer E, Balzer C, et al. Computed virtual chromoendoscopyversus standard colonoscopy with targeted indigocarmine chromo-scopy: a randomised multicentre trial. Gastrointest Endosc 2009;69:734-41.
11. Matsuda T, Saito Y, Fu KI, et al. Does autofluorescence imaging video-endoscopy system improve the colonoscopic polyp detection rate?–apilot study. Am J Gastroenterol 2008;103:1926-32.
12. Yoshida N, Hisabe T, Inada Y, et al. The ability of a novel blue laser im-aging system for the diagnosis of invasion depth of colorectal neo-plasms. J Gastroenterol 2014;49:73-80.
13. Yoshida N, Yagi N, Inada Y, et al. The ability of a novel blue laser im-aging system for the diagnosis of colorectal polyps. Dig Endosc2014;26:250-8.
14. Miyaki R, Yoshida S, Tanaka S, et al. A computer system to be used withlaser-based endoscopy for quantitative diagnosis of early gastric can-cer. J Clin Gastroenterol. Epub 2014 Feb 27.
15. Osawa H, Yamamoto H. Present and future status of flexible spectralimaging color enhancement and blue laser imaging technology. DigEndosc 2014;26(Suppl 1):105-15.
16. Participants in the Paris workshop. The Paris endoscopic classificationof superficial neoplastic lesions: esophagus, stomach, and colon–November 30 to December 1, 2002. Gastrointest Endosc2003;58(Suppl):S3-43.
17. Hamilton SR, Aaltonen LA, eds. World Health Organization classifica-tion of tumors. Pathology and genetics of tumours of the digestive sys-tem. Lyon, France: IARC Press; 2010. p. 104-9.
18. Kanao H, Tanaka S, Oka S, et al. Narrow-band imaging magnificationpredicts the histology and invasion depth of colorectal tumors. Gastro-intest Endosc 2009;69:631-6.
19. Jin XF, Chai TH, Shi JW, et al. A meta-analysis for evaluating the accu-racy of endoscopy with narrow band imaging in detecting colorectaladenomas. J Gastroenterol Hepatol 2012;27:882-7.
20. Sabbagh LC, Reveiz L, Aponte D, et al. Narrow-band imagingdoes not improve detection of colorectal polyps when compared
Volume -, No. - : 2015 GASTROINTESTINAL ENDOSCOPY 7
oof � 7 April 2015 � 4:13 pm

Detectability of colorectal polyps by using BLI Yoshida et al
to conventional colonoscopy: a randomized controlled trial andmeta-analysis of published studies. BMC Gastroenterol 2011;11:100.
21. Singh R, Jayanna M, Navadgi S, et al. Narrow-band imaging with dualfocus magnification in differentiating colorectal neoplasia. Dig Endosc2013;25(Suppl 2):16-20.
(J132003243) and Takeda Pharmaceutical Co, Ltd (J132003379 andJ132003384). All other authors disclosed no financial relationshipsrelevant to this article.
Copyright ª 2015 by the American Society for Gastrointestinal Endoscopy0016-5107/$36.00http://dx.doi.org/10.1016/j.gie.2015.01.030
8 GASTROINTESTINAL ENDOSCOPY Volume -, No. - : 2015
FLA 5.2.0 DTD � YMGE9130_pr
Received June 10, 2014. Accepted January 12, 2015.Current affiliations: Department of Molecular Gastroenterology andHepatology, Kyoto Prefectural University of Medicine, Graduate Schoolof Medical Science, Kyoto (1), Department of Gastroenterology, FukuokaUniversity Chikushi Hospital, Fukuoka (2), Department of Pathology,Kyoto Prefectural University of Medicine, Graduate School of MedicalScience, Kyoto (3), Japan.
Reprint requests: Naohisa Yoshida, MD, PhD, Department of MolecularGastroenterology and Hepatology, Kyoto Prefectural University ofMedicine, Graduate School of Medical Science, 465 Kajii-cho,Kawaramachi-Hirokoji, Kamigyo-ku, Kyoto 602-8566, Japan.
If you would like to chat with an author of this article, you may contactDr Yoshida at [email protected].
www.giejournal.org
oof � 7 April 2015 � 4:13 pm
Related Documents