Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript


Implications of Immunotherapy for the Clinic – TODAY!
AZMN Roundtable
March 2016
Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida
Joseph Mikhael, MD, MEd, FRCPC
Staff Hematologist, Mayo Clinic Arizona
Joseph Mikhael, MD, MEd, FRCPC, FACP
Associate Dean, Mayo School of Graduate Medical Education
Professor of Medicine, Mayo Clinic Arizona

Objectives
1. Review the recently approved immunotherapy agents by the FDA for relapsed multiple myeloma
2. Discuss the overall strategy of risk stratification in deciding which agents to select in myeloma
3. Provide a practical algorithm for relapsed myeloma based on disease based and patient based factors
4. Place immunotherapy in the context of the overall approach myeloma

Managing myeloma: the components
Supportive Care
Initial
Therapy
Consolidation Maintenance
Treatment
of Relapsed
disease
Transplant
Eligible
Patients
Transplant
Ineligible
patientsConsolidation/ Maintenance/
Continued therapy

Three New Agents in One Month!
Daratumumab Darzalex©–
Anti CD38 Monoclonal Antibody (11/16)
Ixazomib – Ninlaro©
Oral Proteasome Inhibitor (11/20)
Elotuzumab – Emplicity©
Anti SLAMF7 Monoclonal Antibody (12/1)
Panobinostat – Farydak©
HDAC inhibitor (February 2015)

Phase 2 Study of Daratumumab (DARA) in
Patients with ≥3 Lines of Prior Therapy or
Double Refractory Multiple Myeloma:
54767414MMY2002 (Sirius)*
Sagar Lonial,1 Brendan Weiss,2 Saad Usmani,3 Seema Singhal,4 Ajai Chari,5 Nizar Bahlis,6 Andrew Belch,7 Amrita Krishnan,8 Robert Vescio,9 Maria Victoria Mateos,10 Amitabha Mazumder,11 Robert Z. Orlowski,12 Heather Sutherland,13 Joan Blade,14 Emma C. Scott,15 Huaibao Feng,16 Clarissa Uhlar,17
Imran Khan,16 Tahamtan Ahmadi,17 Peter Voorhees,18.
1Department of Hematology and Medical Oncology, Winship Cancer Institute, Emory University, Atlanta, GA; 2Division of Hematology & Oncology, Department of Medicine, Abramson Cancer Center and Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA; 3Levine Cancer Institute/Carolinas Healthcare System, Charlotte, NC; 4Robert H. Lurie Comprehensive Cancer Center, Division of Hem./Onc.,
Northwestern University Feinberg School of Medicine, Chicago, IL; 5Tisch Cancer Institute, Mount Sinai School of Medicine, New York, NY; 6Tom Baker Cancer Center - University of Calgary, Calgary, AB, Canada; 7Cross Cancer Institute, Edmonton, AB, Canada; 8Department Hematology and Hematopoietic Stem Cell Transplant, City of Hope, Duarte, CA; 9Cedars-Sinai Outpatient Cancer Center at the Samuel
Oschin Comprehensive Cancer Institute, Los Angeles, CA; 10University Hospital of Salamanca/IBSAL, Salamanca, Spain; 11NYU PerlmutterCancer Center, New York, NY; 12Department of Lymphoma/Myeloma, The University of Texas MD Anderson Cancer Center, Houston, TX;
13Leukemia/Bone Marrow Transplant Program, University of British Columbia, Vancouver, BC, Canada; 14IDIBAPS, Hospital Clinic de Barcelona, Barcelona, Spain; 15Knight Cancer Institute, Oregon Health and Science University, Portland, OR; 16Janssen Research & Development, Raritan, NJ; 17Janssen Research & Development, Spring House, PA; 18Division of Hematology/Oncology, Lineberger
Comprehensive Cancer Center, University of North Carolina at Chapel Hill, Chapel Hill, NC
*NCT01985126

Background• CD38 is highly and ubiquitously
expressed on myeloma cells and at
low levels on normal lymphoid and
myeloid cells, making it a promising
therapeutic target in multiple
myeloma (MM)1,2
• Daratumumab (DARA) is a human
monoclonal antibody (mAb) that
binds to CD38-expressing malignant
cells, inducing cell death through
multiple pathways including CDC,3
ADCC,3 ADCP4 and apoptosis5
1. Lin P, et al. Am J Clin Pathol. 2004;121:482-88.
2. Laubach JP, et al. Expert Opin Investig Drugs. 2014;23:445-52.
3. de Weers M, et al. J Immunol. 2011;186:1840-48.
4. Overdijk MB, et al. MAbs. 2015;7:311-21.
5. Jansen JH, et al. Blood.2012; 120. 2974.
DARA Mechanism of Action
CDC, complement-dependent cytotoxicity; ADCC, antibody-dependent cell-mediated
cytotoxicity; ADCP, antibody-dependent cellular phagocytosis; NK, natural killer cell; NAD,
nicotinamide adenine dinucleotide; cADPR, cyclic adenosine diphosphate-ribose; NAADP,
nicotinic acid adenine dinucleotide phosphate.
Adapted from Laubach JP, et al. Expert Opin Investig Drugs. 2014;23:445-52.

Study Design
• Open-label, international, multicenter study
of Simon-2-stage design
• Initially, patients randomized 1:1 to receive
DARA
– 8 mg/kg every 4 weeks (Q4W) or
– 16 mg/kg every week (QW) for 8 weeks,
every 2 weeks (Q2W) for 16 weeks, then
Q4W thereafter
• 16 mg/kg DARA was established as the
recommended dose for further study
• Results are reported for all patients who
were treated with 16 mg/kg DARA (n = 106)
16 mg/kg
(n = 16)
8 mg/kg
(n = 18)
16 mg/kg
(n = 106)
Response evaluated
Randomization
Additional 90
patients enrolled at
16 mg/kg DARA

Patient Disposition
• Patients were enrolled between October 2013 and May 2014
• Data cutoff January 9th 2015
• Of 106 patients treated with 16 mg/kg DARA, 16 (15%) patients remained on
study at data cutoff
• Discontinuations predominantly due to disease progression
– 82 (77%) due to progressive disease
– 3 (3%) withdrew consent due to symptoms related to disease progression
– 5 (5%) due to adverse events (not related to DARA)
o General physical health deterioration (n = 2)
o H1N1 influenza (n =1)
o Hypercalcemia (n =1)
o Spinal cord compression (n =1)

Baseline Refractory Status
Refractory to, n (%) n = 106
Last prior therapy 103 (97)
PI and IMiD 101 (95)
BORT 95 (90)
CARF 51 (48)
LEN 93 (88)
POM 67 (63)
Alkylating agent 82 (77)
BORT+LEN 87 (82)
BORT+LEN+CARF 42 (40)
BORT+LEN+POM 57 (54)
BORT+LEN+CARF+POM 33 (31)
BORT+LEN+CARF+POM+TH
AL
12 (11)
• Patients were heavily pretreated, and
most patients were refractory to multiple
lines of PI and IMiD treatment
– 97% were refractory to their last line
of therapy
– 77% were refractory to alkylating
agents
– 95% were double refractory
– 66% were refractory to 3 of 4
therapies (BORT, LEN, CARF, and
POM)
– 63% were refractory to POM
– 48% were refractory to CARF

Overall Response Rate
• ORR was 29% (95% CI, 21–39) in
patients receiving 16 mg/kg DARA
• Stringent complete response (sCR) in 3%
of patients (95% CI, 0.6–8.0)
• VGPR or better achieved in 12% (95% CI,
7–20) of patients
• Clinical benefit rate (ORR + MR) was 34%
(95% CI, 25–44)
0
5
10
15
20
25
30
35
16 mg/kg
Ove
rall
re
sp
on
se
ra
te, %
ORR = 29%
sCR
n = 3 (3%)
VGPR
n = 10 (9%)
PR
n = 18 (17%)

ORR by Subgroup
33 3330
21 20
30 29 28 2826
21
0
5
10
15
20
25
30
35
40
OR
R, %
Refractory to

Progression-free and Overall Survival
• 29 of 31 responders are still alive
• The 1-year survival rate was 65% (95% CI, 51.2–75.5)
96106 85 82 64 23 10 2 0Patients at risk
80
100
60
40
20
0
0 42 6 8 16141210
Months from start of treatment
Pa
tie
nts
aliv
e (
%)
Median OS = NE
(95% CI, 13.7–NE)Median PFS = 3.7 months
(95% CI, 2.8–4.6)
63106 38 32 17 5 4 1 0Patients at risk
80
100
60
40
20
0
0 42 6 8 16141210
Months from start of treatment
Pa
tie
nts
pro
gre
ssio
n-f
ree a
nd
aliv
e (
%)

Infusion-related Reactions (IRRs)
• Occurred in 43% of patients
• Predominantly Grade 1 or 2
– Grade 3: 5%; no Grade 4
• >90% of IRRs occurred during the
first infusion
• 7% of patients had an IRR at >1
infusion
• Most common IRRs included nasal
congestion (12%); throat irritation
(7%); cough, dyspnea, chills, and
vomiting (6% each)
• No patients discontinued treatment
due to IRRs
0
5
10
15
20
25
30
35
40
45
Overall 1st infusion 2nd infusion 3rd or laterinfusion
Incid
en
ce o
f IR
R, %

Conclusions
• DARA is a fully human mAb with remarkable single-agent activity in heavily
pretreated and refractory MM patients who exhausted other therapeutic options
• Efficacy was consistent across all subgroups
• Responses were rapid, durable, and deepened over time
– 3 sCRs
– 10 VGPR
– Depth of response may translate to prolonged OS
• DARA was well tolerated
– No patients discontinued treatment due to AEs related to DARA
• IRRs predominantly occurred during the first infusion, were usually Grade 1 or 2,
and were manageable
• DARA represents a new standard of care in this setting

My Take - Daratumumab
• Will have the greatest impact of the drugs approved in 2015
• Ideal partner to combine with PIs or IMiDsdue to lack of overlapping toxicity
• Single agent activity impressive (“rituximab” of myeloma)
• Infusional reactions are real and infusion is LONG
• Watch for the next CD38 MoAb = Isatuximab

ELOQUENT-2: a phase 3, randomized, open-label study
of lenalidomide/dexamethasone with/without elotuzumab
in patients with relapsed/refractory multiple myeloma
Sagar Lonial,1 Meletios Dimopoulos,2 Antonio Palumbo,3 Darrell White,4
Sebastian Grosicki,5 Ivan Spicka,6 Adam Walter-Croneck,7 Philippe Moreau,8
Maria‐Victoria Mateos,9 Hila Magen,10 Andrew Belch,11 Donna Reece,12 Meral Beksac,13
Masafumi Taniwaki,14 Christoph Röllig,15 Anil Singhal,16 Jessica Katz,17 Eric Bleickardt,18
Valerie Poulart,19 and Paul Richardson,20 on behalf of the ELOQUENT-2 Investigators
1Winship Cancer Institute, Emory University School of Medicine, Atlanta, GA; 2National and Kapodistrian University of Athens, Athens, Greece; 3A.O.U. San Giovanni Battista di Torino–Ospedale Molinette, Torino, Italy; 4QEII Health Science Center and Dalhousie University, Halifax, Canada; 5Silesian Medical University, Katowice, Poland; 6Prague General Hospital, Prague, Czech Republic; 7Medical University of Lublin, Lublin, Poland;
8University Hospital, Nantes, France; 9University Hospital of Salamanca–IBSAL, Salamanca, Spain; 10Tel Aviv University, Ramat Aviv, Israel; 11Cross Cancer Institute and University of Alberta, Edmonton, Canada; 12Princess Margaret Hospital, Toronto, Canada; 13Ankara University, Ankara, Turkey; 14Kyoto Prefectural University of Medicine, Kyoto, Japan; 15Universitatsklinikum der TU, Dresden, Germany; 16AbbVie Biotherapeutics
Inc. (ABR), Redwood City, CA; 17Bristol‐Myers Squibb, Princeton, NJ; 18Bristol-Myers Squibb, Wallingford, CT; 19Bristol-Myers Squibb, Braine-l'Alleud, Belgium; 20Dana-Farber Cancer Institute, Boston, MA
Presented at the American Society of Clinical Oncology (ASCO) Annual Meeting; Chicago, Illinois; May 29–June 2, 2015
8508

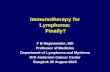
Dual Mechanism of Action of Elotuzumab
• Humanized IgG1 immunostimulatory monoclonal antibody targeted against SLAMF7, a glycoprotein
highly expressed on myeloma and natural killer cells but not on normal tissues1
• Direct activation: Binding to SLAMF7
directly activates natural killer cells,2
but not myeloma cells3
• Tagging for recognition:
Elotuzumab activates natural killer cells
via CD16, enabling selective killing of
myeloma cells via antibody-dependent
cellular cytotoxicity (ADCC) with minimal
effects on normal tissue2
1. Hsi ED et al. Clin Cancer Res 2008;14:2775–84
2. Collins SM et al. Cancer Immunol Immunother 2013;62:1841–9
3. Guo H et al. Mol Cell Biol 2015;35:41–51
Direct activationA
B
Myeloma
cell death
EAT-2
Downstream
activating
signaling
cascade
Degranulation
Perforin,
granzyme B
release
Tagging for
recognition
Elotuzumab
SLAMF7
Natural killer cell
Granule synthesis
Polarization
Elotuzumab
SLAMF7
Myeloma cell
SLAMF7 = Signaling Lymphocyte Activation Molecule-F7

ELOQUENT-2 Study Design
• Open-label, international, randomized, multicenter, phase 3 trial (168 global sites)
• Endpoints:
– Co-primary: PFS and ORR
– Other: overall survival (data not yet mature); duration of response, quality of life, safety
• All patients received premedication to mitigate infusion reactions prior to Elo administration
Key inclusion criteria
• RRMM
• 1–3 prior lines of therapy
• Prior Len exposure permitted in 10% of study population (patients not refractory to Len)
Elo plus Len/Dex (E-Ld) schedule (n=321)
Elo (10 mg/kg IV): Cycle 1 and 2: weekly;
Cycles 3+: every other week
Len (25 mg PO): days 1–21
Dex: weekly equivalent, 40 mg
Len/Dex (Ld) schedule (n=325)
Len (25 mg PO): days 1–21;
Dex: 40 mg PO days 1, 8, 15, 22
Repeat every 28 days
Assessment
• Tumor response: every 4 wks until progressive disease
• Survival: every 12 wks after disease progression

CharacteristicE-Ld
(n=321)Ld (n=325)
Age (years), median (range) 67 (37–88) 66(38–91)
≥65 years 187 (58) 183 (56)
Region, n (%)
Europe 196 (61) 194 (60)
North America 66 (21) 68 (21)
Rest of the world 59 (18) 63 (19)
International Staging System disease stage, n (%)
I 141 (44) 138 (43)
II 102 (32) 105 (32)
III 66 (21) 68 (21)
Not reported 12 (4) 14 (4)
Cytogenetics (FISH)del(17p)
Yes 102 (32) 104 (32)
No 213 (66) 218 (67)
Not reported 6 (2) 3 (1)
t(4;14)
Yes 30 (9) 31 (10)
No 285 (89) 290 (89)
Not reported 6 (2) 4 (1)
1q21
Yes 147 (46) 163 (50)
No 169 (53) 159 (49)
Not reported 5 (2) 3 (1)
Baseline Demographics and Disease Characteristics

Treatment Summary
*At the time of the data cut-off for the interim analysis
E-Ld (n=321) Ld (n=325)
Number of treatment cycles,
median (range)19 (1–42) 14 (1–40)
Patients on treatment, n (%)* 113 (35) 66 (21)
Relative dose intensity (≥90%), n (%)
Elotuzumab 264 (83) -
Lenalidomide 163 (51) 161 (51)
Dexamethasone 146 (46) 148 (47)

Co-Primary Endpoint: Progression-Free Survival
PFS analysis used the primary definition of PFS
E-Ld-treated patients had a 30% reduction in the risk of disease progression or
death; treatment difference at 1 and 2 years was 11% and 14%, respectively
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
380 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36
No. of patients at risk:
E-Ld
Ld321
325
303
295
279
249
259
216
232
192
215
173
195
158
178
141
157
123
143
106
128
89
117
72
85
48
59
36
42
21
32
13
12
7
7
2
57%
68%
27%
41%
1-year PFS 2-year PFS
PFS (months)
Pro
ba
bilit
y p
rog
res
sio
n f
ree
E-Ld
Ld
From N Engl J Med, Lonial, S et al, Elotuzumab Therapy for Relapsed or Refractory Multiple Myeloma. Copyright © (2015) Massachusetts Medical Society. Reprinted with permission
0
0
1
0
E-Ld Ld
Hazard ratio = 0.70 (95% CI:
0.57, 0.85) P=0.0004
Median
PFS
(95% CI)
19.4 mo
(16.6,
22.2)
14.9 mo
(12.1,
17.2)

Co-Primary Endpoint: Overall Response Rate
P=0.0002‡
*Defined as partial response or better; †Complete response rates in the E-Ld group may be underestimated due to
interference from therapeutic antibody in immunofixation and serum protein electrophoresis assay
P=0.0002‡
0
20
40
60
80
100
Re
sp
on
se
ra
te (
%)
E-Ld Ld
p=0.0002
79
66
Overall
response rate*
Complete response
(sCR + CR)†Very good
partial response
Combined response
(sCR + CR + VGPR)Partial response
47
21
2833
28
38
46

Progression-Free Survival According to Age
100
Pro
gre
ss
ion
-fre
e p
ati
en
ts (
%)
Time (months)
Pro
gre
ss
ion
-fre
e p
ati
en
ts (
%)
Time (months)
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38
<65 years ≥65 years
Hazard ratio: 0.75
(95% CI: 0.55, 1.02)Hazard ratio: 0.65
(95% CI: 0.50, 0.85)
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38
90
80
70
60
50
40
30
20
10
0
100
90
80
70
60
50
40
30
20
10
0
2-year
PFS
2-year
PFS
40%
30%
42%
25%
Ld
ELd
Ld
ELd

Key Adverse Events Reported in ≥30% of Patients
Adverse event, n (%)
E-Ld (n=318) Ld (n=317)
Any
grade
Grade
3/4
Any
grade
Grade
3/4
Common non-hematologic adverse events
Fatigue 149 (47) 27 (9) 123 (39) 26 (8)
Pyrexia 119 (37) 8 (3) 78 (25) 9 (3)
Diarrhea 149 (47) 16 (5) 114 (36) 13 (4)
Constipation 113 (36) 4 (1) 86 (27) 1 (0.3)
Muscle spasms 95 (30) 1 (0.3) 84 (27) 3 (1)
Cough 100 (31) 1 (0.3) 57 (18) 0
Common hematologic toxicities
Lymphopenia 316 (99) 244 (77) 311 (98) 154 (49)
Neutropenia 260 (82) 107 (34) 281 (89) 138 (44)
Infections 259 (81) 89 (28) 236 (74) 77 (24)
• Exposure-adjusted infection rate was 197 (incidence rate per 100 person–years of exposure) in both arms
• There was no detriment to overall health-related quality of life with the addition of Elo to Ld

Infusion Reactions
• Infusion reactions occurred in 10% of patients
• 70% of infusion reactions occurred with the first dose
• No Grade 4 or 5 infusion reactions
• Elotuzumab infusion was interrupted in 15 (5%) patients due to an infusion reaction (median interruption duration 25 minutes)
• 2 (1%) patients discontinued the study due to an infusion reaction
Events, n (%)
E-Ld (n=318)
Grade
1/2Grade 3
Grade
4/5
Infusion reaction 29 (9) 4 (1) 0
Pyrexia 10 (3) 0 0
Chills 4 (1) 0 0
Hypertension 3 (1) 1(<1) 0

Summary and Conclusions
• Elotuzumab is a novel immunostimulatory monoclonal antibody (mAb) with a dual
mechanism of action elicited via natural killer cells
• In relapsed and refractory patients, in combination with Len/Dex, elotuzumab
demonstrated a significant and clinically meaningful increase in PFS and ORR
– 30% reduction in the risk of progression or death compared with Len/Dex alone
– Difference in PFS was greater at 2 years for E-Ld compared with Ld
– Benefit for PFS in elotuzumab group was consistent across key subgroups, including
elderly and high risk patients
– Absolute difference in overall response rate favored elotuzumab group
• Elotuzumab in combination with Len/Dex did not increase the incidence of adverse events
compared to Len/Dex alone
• Elotuzumab is the first mAb demonstrating PFS benefit in combination with Len/Dex in a
large randomized phase 3 study in RRMM


My Take - Elotuzumab
• No single agent activity, but unique mechanism of action
• True “immune effect” of tail of durable response yet to be fully proven
• Limited now by need of lenalidomide –future use with pomalidomide could be important
• Results with bortezomib less impressive

Treatment sequence in Myeloma
Induction Consolidation
Front line treatment
Post
consolidation
Maintenance
Rescue
Relapsed
NewCarfilzomib Combos
“more” induction
Lenalidomide 2 mths? Ixazomib
Oprozomib
Isatuximab
Bendamustine
PD/PDL-1 Inhibition
++++++++
Now
VD
Rev/Dex
CyBorD
VTD
VRD
SCTNothing
Thalidomide?
Bortezomib
Lenalidomide
Bortezomib
Lenalidomide
Thalidomide
Carfilzomib
Pomalidomide
Panobinostat
Daratumumab
Ixazomib
Elotuzumab

The Future of Myeloma
• Other Conventional Chemo (Bendamustine, DPACE)
• Others?
• Steroids• Doxorubicin, Panobinostat, Steroids
Proteasome Inhibitors
(Bortezomib, Carfilzomib, Ixazomib…)
Immuno-modulatory
Agents (Thalidomide, Lenalidomide, Pomalidomide)
Alkylators(melphalan,
cyclophospha-mide)
Monoclonal Antibodies
(Elotuzumab, Daratumumab,
Isatuximab)

Mayo Stratification for Myeloma And Risk-adapted Therapy
Relapsed Myeloma
mSMART
v3 //last reviewed Dec 2015

mSMART 2.0: Classification of Relapsed MM
Relapse <12 months from transplant or progression within first year of diagnosis
FISH Del 17p t(14;16) t(14;20)
High risk GEP
All others including:
Trisomies
t(11;14)
t(6;14)
FISH t(4;14)
1q gain
High PC S-phase
High-Risk Intermediate-Risk Standard-Risk
Dispenzieri et al. Mayo Clin Proc 2007;82:323-341; Kumar et al. Mayo Clin Proc 2009 84:1095-1110; Mikhael et al. Mayo Clin
Proc 2013;88:360-376.
v4 //last reviewed Dec 2015

mSMART 2.0: Classification of Relapsed MM
Relapse <12 months from transplant or progression within first year of diagnosis
FISH Del 17p t(14;16) t(14;20)
High risk GEP
All others including:
Trisomies
t(11;14)
t(6;14)
FISH t(4;14)
1q gain
High PC S-phase
High-Risk 20% Intermediate-Risk 20% Standard-Risk 60%
Dispenzieri et al. Mayo Clin Proc 2007;82:323-341; Kumar et al. Mayo Clin Proc 2009 84:1095-1110; Mikhael et al. Mayo Clin
Proc 2013;88:360-376.
v4 //last reviewed Dec 2015
3 years 4-5 years 8-10 years
FISH= fluorescence in situ hybridization; GEP= gene expression profiling; PCLI= plasma cell labeling index

• KRd, carfilzomib, lenalidomide, dexamethasone
• KPd, carfilzomib, pomalidomide, dexamethasone
• CyBorD, cyclophosphamide, bortezomib, dexamethasone
• IRd, ixazomib, lenalidomide, dexamethasone
• ICd, ixazomib, cyclophosphamide, dexamethasone
• Rd-Elo, lenalidomide, dexamethasone, elotuzumab
• Pom-dex, pomalidomide, dexamethasone
• PVd, pomalidomide, bortezomib, dexamethasone
• Dara, daratumumab
Abbreviations for Major Regimens
v4 //last reviewed Dec 2015

ICd if Rev
maintenance*
IRd or Rd-Elo if Vel
maintenance*
KPd or CyBord if
Rev maintenance*
KRd or KPd if Vel
maintenance*
Indolent Relapse
or Frail patients
Fit PatientsFit Patients
On maintenance
Indolent Relapse
or Frail patients
Off-therapy/ Unmaintained
*Consider salvage auto SCT in patients eligible for ASCT who have not
had transplant before; Consider 2nd auto SCT if eligible and >18 months
unmaintained or >36 months maintained response to first auto;
First Relapse Off-Study
v4 //last reviewed Dec 2015
IRd or Rd-Elo*KRd*

Not Plasma Cell Leukemia (PCL) or Similar extramedullary disease (EMD)
Second or later Relapse* Off-Study
Dual-Refractory
(Bortezomib and
Lenalidomide)**
Triple-Refractory
(Bortezomib, Lenalidomide
and Carfilzomib)**
Triple-Refractory
(Bortezomib, Len, and
Pomalidomide)**
Pom-Dex plus daratumumab Dara-based regimen; or
Alkylator-based regimen if
alkylator naïve; or
Proteasome inhibitor plus
panobinostat
* If single refractory, refer to First Relapse algorithm; **Auto transplant is an option, if transplant
candidate and feasible
v4 //last reviewed Dec 2015

Second or later Relapse – Off-Study
Quadruple-refractory (Lenalidomide, Pomalidomide, Bortezomib,
and Carfilzomib)
VDT-PACE* x 2 cycles if possible.*
Auto transplant if transplant candidate; if not, treat with regimens that the patient is not
known to be refractory to (eg., daratumumab-containing regimen; KRd, KPd, IRd, or PVd -
plus moAB; panobinostat-containing regimen; bendamustine; alkylator-containing
combination if not alkylator refractory; or anthracycline containing regimen such as RAD,
VDD, PAD, or CHOP)
*CVAD or similar regimen can be used in place of VDT-PACE in older patients or patients with poor functional status
v4 //last reviewed Dec 2015

Secondary PCL or extensive EMD
VDT-PACE x 2 cycles;*
Auto transplant if transplant candidate; if not maintain with one of the regimens listed
that the patient is not known to be refractory to (eg., daratumumab-containing
regimen; KRd, KPd, IRd, or PVd - plus moAB; alkylator-containing combination if not
alkylator refractory; or anthracycline containing regimen such as RAD, VDD, PAD, or
CHOP)
Second or later Relapse – Off-Study
*CVAD or similar regimen can be used in place of VDT-PACE in older patients or patients with poor functional status
v4 //last reviewed Dec 2015

Conclusions
• Therapy for myeloma has radically changed in the last year with more options
• Monoclonal antibody therapy has become a critical aspect of relapsed therapy but likely across the spectrum of therapy soon
• Oral proteasome inhibition can now be delivered orally with reduced toxicity
• Optimal combinations and sequencing of therapy have yet to be determined but the ability to individualize therapy is truly here

Mayo Clinic Myeloma Consultants
Rochester
• V. Rajkumar, MD
• Francis Buadi, MD
• David Dingli, MD
• Angela Dispenzieri, MD
• Morie Gertz, MD
• Suzanne Hayman, MD
• Shaji Kumar, MD
• Robert Kyle, MD
• Nelson Leung, MD
• John Lust, MD
• Steve Russell, MD
• Steven Zeldenrust, MD
• Prashant Kapoor, MD
• Wilson Gonsalves, MD
• Yi Lin, MD, PhD
• Martha Lacy, MD
Arizona
•Joseph Mikhael, MD
•Leif Bergsagel, MD
•Rafael Fonseca, MD
•Craig Reeder, MD
•Keith Stewart, MD
Florida
•Vivek Roy, MD
•Asher Chanan Khan, MD
•Taimur Sher, MD
•Sikander Ailawadhi, MD
MSMART.org

Related Documents