Implications of Advances in Hypertension Pathophysiology: Darryl M. Nomura PharmD Viva Health 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Implications of Advances in Hypertension Pathophysiology
Darryl M Nomura PharmD
Viva Health1
Primary Program GoalTo describe advances in a model outlining hypertension pathophysiology identifying existing roles of sensors processors and
effectors as well as updates in central nervous system control of blood pressure in
hypertension
2
Primary Objective 18
bull State the leading theories physiologic factors and physical vascular tissue remodeling conditions that results in hypertension and related macrovascular complications such as stroke and myocardial infarction
3
Pathophysiology Arterial Vessel RemodelingFatty Streaks
Adapted from httpwwwfimperialacuk~ajm8BioFluidsPictures
4
Pathophysiology of CeVDCVD
5
Pathophysiology of CeVDCVDOxidized-LDL
6
Pathophysiology of CeVDCVD
7
8
Pathophysiology Cross-Section of a Labile Plaque
9
PathophysiologyHigher BP Increases Shear Stress amp Risk of Rupture
10
PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Primary Program GoalTo describe advances in a model outlining hypertension pathophysiology identifying existing roles of sensors processors and
effectors as well as updates in central nervous system control of blood pressure in
hypertension
2
Primary Objective 18
bull State the leading theories physiologic factors and physical vascular tissue remodeling conditions that results in hypertension and related macrovascular complications such as stroke and myocardial infarction
3
Pathophysiology Arterial Vessel RemodelingFatty Streaks
Adapted from httpwwwfimperialacuk~ajm8BioFluidsPictures
4
Pathophysiology of CeVDCVD
5
Pathophysiology of CeVDCVDOxidized-LDL
6
Pathophysiology of CeVDCVD
7
8
Pathophysiology Cross-Section of a Labile Plaque
9
PathophysiologyHigher BP Increases Shear Stress amp Risk of Rupture
10
PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Primary Objective 18
bull State the leading theories physiologic factors and physical vascular tissue remodeling conditions that results in hypertension and related macrovascular complications such as stroke and myocardial infarction
3
Pathophysiology Arterial Vessel RemodelingFatty Streaks
Adapted from httpwwwfimperialacuk~ajm8BioFluidsPictures
4
Pathophysiology of CeVDCVD
5
Pathophysiology of CeVDCVDOxidized-LDL
6
Pathophysiology of CeVDCVD
7
8
Pathophysiology Cross-Section of a Labile Plaque
9
PathophysiologyHigher BP Increases Shear Stress amp Risk of Rupture
10
PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Pathophysiology Arterial Vessel RemodelingFatty Streaks
Adapted from httpwwwfimperialacuk~ajm8BioFluidsPictures
4
Pathophysiology of CeVDCVD
5
Pathophysiology of CeVDCVDOxidized-LDL
6
Pathophysiology of CeVDCVD
7
8
Pathophysiology Cross-Section of a Labile Plaque
9
PathophysiologyHigher BP Increases Shear Stress amp Risk of Rupture
10
PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Pathophysiology of CeVDCVD
5
Pathophysiology of CeVDCVDOxidized-LDL
6
Pathophysiology of CeVDCVD
7
8
Pathophysiology Cross-Section of a Labile Plaque
9
PathophysiologyHigher BP Increases Shear Stress amp Risk of Rupture
10
PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Pathophysiology of CeVDCVDOxidized-LDL
6
Pathophysiology of CeVDCVD
7
8
Pathophysiology Cross-Section of a Labile Plaque
9
PathophysiologyHigher BP Increases Shear Stress amp Risk of Rupture
10
PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Pathophysiology of CeVDCVD
7
8
Pathophysiology Cross-Section of a Labile Plaque
9
PathophysiologyHigher BP Increases Shear Stress amp Risk of Rupture
10
PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

8
Pathophysiology Cross-Section of a Labile Plaque
9
PathophysiologyHigher BP Increases Shear Stress amp Risk of Rupture
10
PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Pathophysiology Cross-Section of a Labile Plaque
9
PathophysiologyHigher BP Increases Shear Stress amp Risk of Rupture
10
PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

PathophysiologyHigher BP Increases Shear Stress amp Risk of Rupture
10
PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

PathophysiologyTurbulent flow rupturing plaques can lead to occlusion MI
Seimiya K et al Significance of Plaque Disruption Sites in Acute Coronary Syndrome J Nippon Med Sch 73141-148 200611
Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Primary Objective 28
bullDescribe the three primary areas that form the foundational basis of essential hypertension and provide at least three factors supporting each primary area
12
Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Primary Area 1 Systemic Vascular Resistance
Primary Area 2Cardiac Output
Primary Area 3 Blood Volume
1 Vascular Anatomy Heart Rate Renal Na Handling
2 Vascular Factors Stroke Volume H2O Handling
3 Tissue Factors Neuro-hormonal Factors Neuro-hormonal Factors
12
3
httpwwwcvphysiologycomBlood20PressureBP02213
14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

14
Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Source Table 28-3 in httpsbasicmedicalkeycomwp-contentuploads201609f0302-01jpg
Drug solutions to controlling BP (see the 3 primary issues) but what do we know about ldquoSNS System Activationrdquo
1
2
3
15
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term reflex controlbull Long-term stability and control
bull Requires ldquocalibrationrdquo to know what is the target
Smooth Muscle Vascular EffectorsCardiac Muscle EffectorsRenal SodiumVolume EffectorsRenin-Angiotensin-Aldosterone System
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
16
Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Pressure and
Chemo-receptor Sensors
17
18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

18
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60
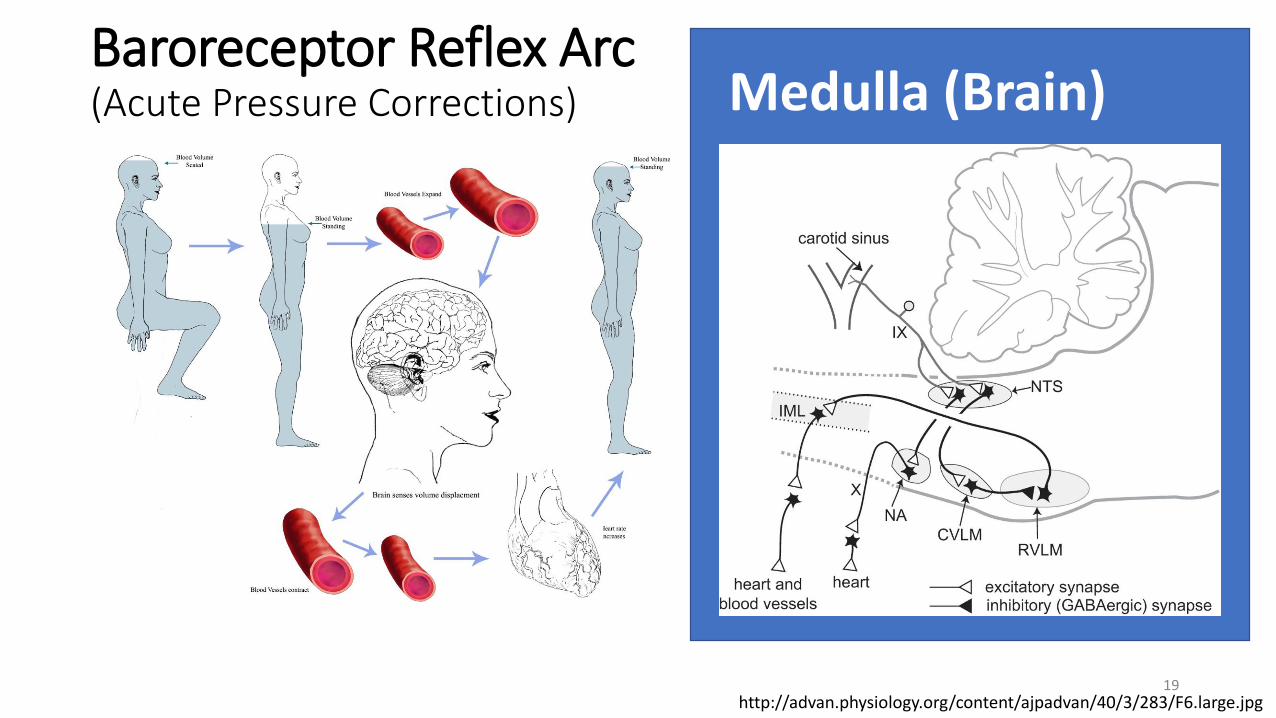
httpadvanphysiologyorgcontentajpadvan403283F6largejpg
Baroreceptor Reflex Arc (Acute Pressure Corrections) Medulla (Brain)
19
Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Zanutto et al Blood pressure long term regulation A neural network model of the set point development BioMedical Engineering OnLine 2011 1054 httpwwwbiomedical-engineering-
onlinecomcontent10154
Cardio-Inhibitory Center
Cardio-Accelerator Center
Vaso-Motor Center(medulla oblongata)
Comparator (NTS)
Error Signal After the difference from
Baro- Cardiopulmonary- Chemo-Receptors
Transducers (Neural-side to CV-side)
Pacemaker (myocardial)Contractile Elements (myocardial cardiac muscle)
Cardiac Output
Multipliers
NeuralReference
(R)
Contractile Elements (arterial vascular smooth muscle)
Signals fromBaro- Cardiopulmonary-
Chemo-Receptors
Heart Rate
Stroke Volume
Peripheral Resistance
BLOOD PRESSURE RESULT
Error Signal From Vaso-Motor Center
SNS
PSNS
Medulla (Brain)
20
httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

httpdoctorlibinfophysiologymedicalmedicalfilesimage822jpg
Question Why is SNS innervation so
important Why do we need ldquohigh-voltage
electricityrdquo carried by the SNS neurons
21
Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Without the ldquohigh voltagerdquo carried
by the SNS the L-type and T-type
calcium channels cannot openhellipand
no smooth muscle or cardiac
muscle contraction is
possiblehttpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 22
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 23
httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

httpdroualbfacultymjceduCourse20MaterialsPhysiology20101Chapter20NotesFall202011chapter_1320Fall202011htm 24
httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

httpwwwpathophysorgphysiology-of-cardiac-conduction-and-contractility25
The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

The SNS and Innervation of the HeartSA Node drives Heart Rate (pulse) ndash Cardiac Output
26
The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

The SNS and Innervation of Arteries and
Arterioles
27
da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

da Silva AA do Carmo JM Wang Z Hall JE The Brain Melanocortin System Sympathetic Control and Obesity Hypertension Physiology Published 1 May 2014 Vol 29 no 3 196-202 DOI 101152physiol000612013
The Role of Obesity and Leptin
in Hypertension mediated by the
Brain and the SNS
Pro-opiomelanocortin (POMC) neurons and consequent stimulation of melanocortin-4 receptors (MC4R) in brain regions involved in cardiovascular regulation
28
Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Reactive Oxygen Species (ROS) in the CNS
Loperena R Harrison DG Oxidative Stress and Hypertensive Diseases Research Gate October 2016 DOI 101016jmcna20160800429
NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

NEWDietary Salt the Cerebrospinal Fluid
and Central SNS StimulationA New Paradigm Shift in Thinking about Sodium The Endogenous
Ouabain (EO) increases hypothalamic ANG-II type-1 receptor and NADPH
oxidase (ROS) and decreases neuronal nitric oxide (NOS) synthase protein
expression The aldosterone-epithelial Na+ channel-EO-
α2 Na+ pump-ANG-II pathway modulates the activity of brain
cardiovascular control centers that regulate the BP set point and induce
sustained changes in SNA
Blaustein MP Leenen FHH Chen L Golovina VA Hamlyn JM Pallone TL Van Huysse JW Zhang J Wier WG How NaCl raises blood pressure a new paradigm for the pathogenesis of salt-dependent hypertension American Journal of Physiology -Heart and Circulatory Physiology 1 March 2012 Vol 302 no 5 H1031-H1049 DOI 101152ajpheart008992011
30
Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Ang Richard amp Opel Aaisha amp Tinker Andrew (2012) The Role of Inhibitory G Proteins and Regulators of G Protein Signaling in the in vivo Control of Heart Rate and Predisposition to Cardiac Arrhythmias Frontiers in physiology 3 96 103389fphys201200096
Higher Centers of the Brain and SNS stimulation
of the Heart and Blood Vessels Note the lack of
any parasympathetic innervation on blood
vessels
31
ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

ldquoComputer to Renal Effectorrdquo SNS Innervation
Triggers the JGA to Release of Reninhellipand constrict the afferent arteriole smooth
muscle
32
RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

RAAS Angiotensin II Stimulation of Effectors Five Major Systems Affected
33
Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Summary Higher Brain Center Issues
bull Role of Excess Sodium and HTN from SNS stimulation
bull Role of Oxidative Stress and HTNbull Excess Reactive Oxygen Species (ROS) generation by AII in the hypothalamus
bull Role of Obesity and Excess Leptinbull POMC stimulation of melanocortin-4 receptors (MC4R) brain pro-
opiomelanocortin (POMC) neurons
bull Role of Sleep Apnea (Chronic Intermittent Hypoxia) on PVN sympathetic tone signals to the NTSbull Increasing the carotid body O2 chemoreceptor sensitivity drives the next day
keeping BP up
34
Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Blood Volume Impact on BP by Guytonrsquos work
Osborn JW Averina VA Fink GD Current computational models do not reveal the importance of the nervous system in long-term control of arterial pressure Exp Phys 944 pp381-397 2009 35
Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Primary Objective 38
bullOutline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension
36
Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Outline the three major abnormal processes in the kidney resulting in a salt-sensitive kidney that has been proposed as the principle and dominant cause of essential salt-sensitive hypertension (see Oparil)Phase Process 1 Process 2 Process 3
1 Normal Kidney Functioning
Increased SNS activity
Increased RAAS activity
2A Subtle Renal Injury Tubular ischemia amp interstitial inflammation
Increased vasoconstrictor expression and decreased vasodilator expression
Increased sodium reabsorption
2B Decreased Na excretion
Decreased sodium filtration
2C Increased blood pressure
Na retentionIncreased BP
3 Hypertensive Kidney Tubular ischemia diminishes
Sodium handling returns to normal
37
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60
Primary Objective 48
bullDescribe the mechanism of long-term stress and sleep apnea on blood pressure control
38
Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Long-term Stress and Sleep Apnea
Sharpe AL Calderon AS Andrade MA Cunningham JT Mifflin SW Toney GM Chronic intermittent hypoxia increases sympathetic control of blood pressure role of neuronal activity in the hypothalamic paraventricular nucleus American Journal of Physiology - Heart and Circulatory Physiology Published 15 December 2013 Vol 305 no 12 H1772H1780 DOI 101152ajpheart005922013
Chemo-receptors
39
Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Primary Objective 58
bull Outline the counter-regulatory mechanisms of regulating sodium in salt-sensitive nocturnal overnight BP ldquodippersrdquo and non-salt sensitive BP ldquonon-dippersrdquo Relate pathophysiologic processes that can promote recovery of nocturnal overnight circadian rhythm blood pressure dipping
40
Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Facts Describe the mechanism of long-term stress and sleep apnea on blood pressure control
41
Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Kario K Morning Hypertension A Pitfall of Current Hypertension Management JMAJ 48234-240 2005
42
Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Primary Objective 68
bull Describe the basis for the JNC-8 recommendations that made specific recommendations for this guideline regarding age and blood pressure targets
43
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
Jin J New Guideline for Treatment of High Blood Pressure in Adults JAMA 2014311(5)538
44
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
45
Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Process Compare and contrast the medication treatment algorithms described in the JNC-8 British Hypertension Societyrsquos (BHS-NHS) and American Diabetes Association hypertension guidelines
James PA et al 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults Report From the Panel Members Appointed to the Eight Joint National Committee (JNC 9) JAMA 311507-520 2014
46
Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Dr Paul A James Lead JNC-8 Guideline Author Explainshellip
We wanted to make the message very simple for physicians treat to 15090 mm Hg in patients over age 60 and 14090 for everybody else Monitor them track them re-monitor themThats a very simple message We wanted to be crystal clear
about where the evidence is to support these recommendations We are not saying that if youve gotten someones [systolic] BP to 140 or 135 mm Hg on medicine and they are doing well that you need to take them off medicines and get their BP closer to 150
We are simply saying if you can consistently get peoples BP below 150 you really are improving their health outcomes
47
Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Primary Objective 78
bullRelate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
48
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60
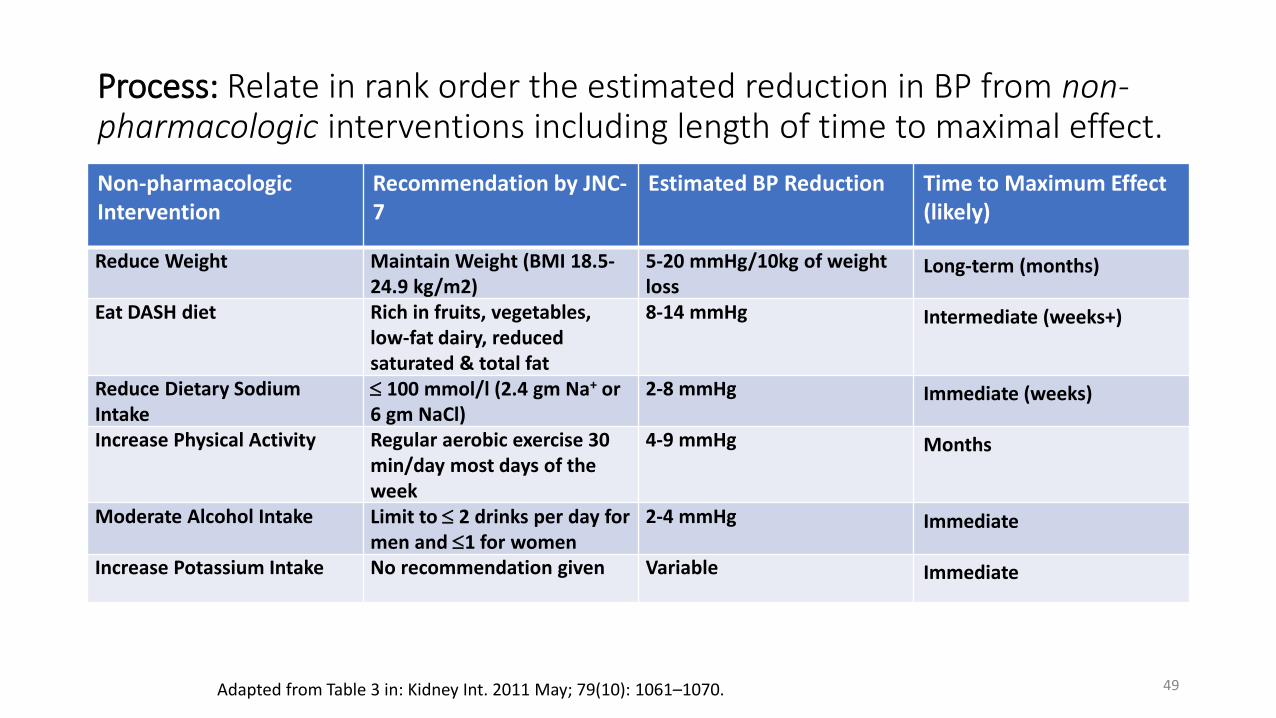
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Increase Potassium Intake No recommendation given Variable Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070 49
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Reduce Weight Maintain Weight (BMI 185-249 kgm2)
5-20 mmHg10kg of weight loss
Long-term (months)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Ideal Body Weight Calories per lb(kg) fat loss
Calorie Expenditure for Exercise MinWeek Cal ExpendedWeekly
Time to weight loss (weeks)
Example165 pounds (75 kg)
ideal current weight
200 pounds (91 kg)35 pounds to lose
(26 kg)
3500(7700)
145 calhrbiking lt 17
kph
295 calhrbiking gt 17
kph
30 x 5 = 150
minutes
15060 = 25 hours x 145 (363
calweek)X 295 (738week)
1kg 7700cal363week =
21 weeks(295hr 105
weeks)
140 calhrwalking lt 6
kph
230 calhrwalking gt 6
kph
30 x 5 = 150
minutes
15060 = 25 hours
(350calwk)(575calwk)
5kg x7700 =38500 cal=
38500575=1067 weeks
50
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction Time to Maximum Effect (likely)
Eat DASH diet Rich in fruits vegetables low-fat dairy reduced saturated amp total fat
8-14 mmHg Intermediate (weeks+)
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
51
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7 Estimated BP Reduction
Time to Maximum Effect (likely)
Reduce Dietary Sodium Intake
100 mmoll (24 gm Na+ or 6 gm NaCl)
2-8 mmHg Immediate (weeks)30 days for DASH STUDY
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Sacks FM Svetkey LP Vollmer WM Appel LJ Bray GA Harsha D Obarzanek E Conlin PR Miller III ER Simons-Morton DG Karanja N Pao-Hwa L for the DASH Sodium Collaborative Research Group Effects on Blood Pressure of Reduced Dietary Sodium and the Dietary Approaches to Stop Hypertension (DASH) Diet N Engl J Med 3443-10 2001)
52
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Increase Physical Activity Regular aerobic exercise 30 minday most days of the week
4-9 mmHg Months
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
Results The weighted net reduction of blood pressure in response to dynamic physical training averaged 3424 mm Hg (P 1113090 0001) Inter-study differences in the changes in pressure were not related to weekly frequency time per session or exercise intensity which ranged from approximately 45ndash85 these three characteristics combined explained less than 5 of the variance of the blood pressure response The response of diastolic blood pressure was not different according to training intensity in studies that randomized patients to training programs with different intensities Some studies reported a greater reduction of systolic blood pressure when intensity was about 40 than when participants exercised at about 70 but this finding was not consistent neither within nor between studies Conclusion Training from three to five times per week during 30 ndash 60 min per session at an intensity of about 40 ndash50 of net maximal exercise performance appears to be effective with regard to blood pressure reduction
Fagard RG Exercise characteristics and the blood pressure response to dynamic physical training Medicine and Science in Sports amp Exercise S484-S4922001
53
Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Process Relate in rank order the estimated reduction in BP from non-pharmacologic interventions including length of time to maximal effect
Non-pharmacologic Intervention
Recommendation by JNC-7
Estimated BP Reduction Time to Maximum Effect (likely)
Moderate Alcohol Intake Limit to 2 drinks per day for men and 1 for women
2-4 mmHg Immediate
Adapted from Table 3 in Kidney Int 2011 May 79(10) 1061ndash1070
The overall effect size estimates in our meta-analysis were impressive 331 mm Hg reduction in systolic BP and 204 mm Hg reduction in diastolic BP The effect of alcohol reduction on BP was consistent across subgroups including those defined by presence or absence of hypertension
Xue X Jiang H Frontini MG Ogden LG Motsamai OI Whelton PK Effects of Alcohol Reduction on Blood Pressure A Meta-Analysis of Randomized Controlled Trials Hypertension 381112-1117 2001
54
Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Primary Objective 88
bullRelate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
55
Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Process Relate the specific CVD event risk reduction if patients eliminate smoking use HTN medications and takes low-dose aspirin both alone and in combination
Viera AJ Sheridan SL Global Risk of CoronaryHeart Disease Assessment and Application AmFam Physician 82265-274 2010
56
A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

A Conceptual Model
Homeostasis
Master Computer Pressure ControllerldquoAKA the BRAINrdquo
bull Short-term (baro-reflex)Long-term BP controlbull Impacted by external sensors internal stresses (ROS Leptin AII) amp set-point recalibration
Vascular Smooth Muscle Contraction EffectorsCardiac Muscle ChronoInotropy EffectorsKidney Sodium Effectors (AII Aldosterone)Kidney Water Volume Effectors (ADH)Kidney RAAS - JGA Effectors (Renin)
Blood Pressure SensorsBlood Volume Stretch SensorsBlood Chemo Sensors (O2 amp CO2)
57
Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60

Summary Advances in HTN Pathophysiology
bull The role of the NTS and RVLM of the medulla oblongata is significantly greater than simple correction of sudden pressure change as in standing or sitting
bull Signaling molecules in the medulla oblongata such as leptin reactive oxygen species (ROS) dietary salt in the CNS itself and Angiotensin II in addition to pressure and chemoreceptor inputs affect SNS stimulation of the heart blood vessels Pituitary (ADH) renal JGA adrenal cortex (aldosterone) and adrenal medula
bull Lifestyle issues such as Obstructive Sleep Apnea affect chemo-receptor sensitivity to oxygen and CO2 for extended periods afterwards even through the next day
bull Improvements in regular exercise can help to improve baro-receptor sensitivity but is unlikely to fully correct BP to normal values
bull Improvements in sodium intake can help to improve BP as has been seen with the DASH diet but alone are unlikely to dramatically lower BP in HTN patients
bull Improvements in BP for older patients as per JNC-8 guidelines do not always require correction to 14090 mmHg or less
58
59
END
60
59
END
60

END
60
Related Documents











